the effects of massage therapy on suspected fetal alcohol ... · therapy on suspected fetal alcohol...
TRANSCRIPT

The Effects of Massage
Therapy on Suspected Fetal Alcohol Spectrum Disorder; A
Case Study
THE IMPACT OF MASSAGE THERAPY ON A TWO YEAR OLD WITH SUSPECTED FETAL ALCOHOL SPECTRUM DISORDER RELATIVE
TO BEHAVIOUR
ALYSSA HOFMANN 2144 Fleetwood Ave, Kamloops, BC, V2B 4S5
(250)8190689 [email protected]
Okanagan Valley College of Massage Therapy 200 3400 30th Avenue Vernon BC V1T 2E
Alyssa Hofmann
Table of Contents…………………………………..page 1
Abstract………….……………………………….....page 3
Introduction…………………………………….….page 5
Client Profile……………………………………....page 6
Assessment.……….…………………………….….page 8
Treatment……………………………….……...…...page 11
Results……………………………………...……...page 13
Conclusion…………...……………………..……..page 19
References………...……………………………….page 21
1

Alyssa Hofmann
ACKNOWLEDGEMENTS
I would like to take this time to thank my wonderful patient for being
willing to participant in this case study. I would also like to thank his
guardians for helping to keep track of the outcomes on a daily log and being
willing to incorporate aspects of this case study into their lives. Another thank
you to Robynne Kingswood for being the helping handed that was needed
anytime there was a question or concern about this research project. I
appreciate the help from Anastasia Dikareva who taught us how to research
and also the importance it has in the Massage Therapy field. And most of all a
thank you to my family and friends who were moral support throughout this
project and stuck by even when the going got tough.
2

Alyssa Hofmann
ABSTRACT
Background: Fetal Alcohol Spectrum Disorder (FASD) a term used for a
wide array of growth, mental, and physical problems that can occur to a baby
if the mother drinks while pregnant. There is currently no specific treatment
for FASD however parents of children suffering with FASD are able to seek
help from doctors, specialists, massage, and pharmaceuticals for their
symptoms.
Objectives: To determine if swedish massage will have a lasting effect on a
two year old boys behaviour.
Methods: The patient was given ten swedish massage treatments. Before the
first treatment, after the fifth treatment, after the last treatment and one week
later the patient was measured for the outcome. The therapist was looking to
affect the way the child interacted with others,whether that be the child’s
guardian or sibling, the amount he was distracted while doing specific tasks
and the child’s need to walk on his toes.
3

Alyssa Hofmann
Results: Overall, five of the seven specific outcomes the therapist was testing
for decreased and two of the seven outcomes stayed the same. The therapist
also noticed a decrease in hypertonicity in the child’s bilateral Tricep Surae
group.
Conclusion: Although the findings from this case study proved the therapist’s
hypothesis more research is need to determine whether massage alone can
have a statistical significance on helping improve the behaviour of a child with
Fetal Alcohol Spectrum Disorder.
Keywords: Massage, Child, Fetal Alcohol Spectrum Disorder, Behaviour
4

Alyssa Hofmann
INTRODUCTION
Fetal Alcohol Spectrum Disorder (FASD) also known as Fetal Alcohol
Syndrome (FAS) describes an abundance of disabilities including certain
facial, intellectual and growth defects resulting from exposure to alcohol while
in utero, that can last throughout a lifetime.¹ Adults that are suffering with
FASD have daily struggles, like uncontrollable aggression, that prevent them
from being able to hold down a stable job, live independently, and avoid
conflict with authority figures⁴. Because of these problems, many of these
adults end up dropping out of school, having to spend time serving community
service for minor offenses and some even end up going to prison.³
FASD reportedly affects 330,000 Canadians or approximately 1 in
every 100 people¹. Specific physical and emotional criteria is set out to
determine if a child can be clinically diagnosed with FASD. These diagnostic
features can include but are not limited to: a flat philtrum, small upper lip,
microcephaly, speech delays, adaptive behaviour problems, Learning delays,
difficulty at mealtimes, developmental motor delays, and ear formation
abnormalities² ⁸.
Currently, massage has been used in conjunction with a medical team
at an early age to help try to counteract the emotional, physical, and social
aspects of FASD² ⁶. Many people suffering with FASD are also dealing with
5

Alyssa Hofmann
other disorders like depression, anxiety, and different personalities disorders⁵.
At this time there is no cure for FASD and because of that many parents turn
to prescription drugs and therapy to help balance out the effects of FASD
however, these treatments can only help manage some aspects. Massage has
been shown to decrease the effects of depression, decrease stress, increase
relaxation, and increase immune function. Massage can also be used to help
decrease some of the behavioural and psychological symptoms that go along
with FASD⁷. There has not been enough studies performed on whether
massage can improve behaviour on FASD children to confirm if it alone is an
effective treatment.
As a result of the lacking research, the goal of this study is to
determine if swedish massage on a two year old child with FASD will help to
have an impact his behaviour.
CLIENT PROFILE
The client for this case study is a two year old First Nations male that
was diagnosed by a physician with suspected Fetal Alcohol Spectrum
Disorder. The child is currently on the waitlist to be tested with his medical
specialist. He has not yet reached the minimum age for which testing can
begin. He has been with his current guardian, his aunt and uncle, since
6

Alyssa Hofmann
September 25th 2015 after being in a stable foster care home since he was five
months old.
Since birth, the child had suffered with chronic repetitive ear infections
which in turn resulted in tubes being placed in both ears to aid in drainage. At
this point, both tubes have fallen out and the holes have closed up however,
because of the increase of ear pressure the child developed a small foramen in
his right ear just below the eardrum. Additionally, the child did not starting
walking until approximately fifteen months old and could only say between
five and ten words at seventeen months. When the child was taken to the
doctor for a regular checkup in November 2015 the guardian was told he was
in the 80th percentile for his age in weight and height. As of April 2016 the
child is thirtytwo pounds and thirty six inches tall.
The child’s most irrefutable FASD traits include small eyes, speech
delays, a small upper lip, motor delays, and chronic ear problems. The child’s
birth mother has also admitted to drinking all throughout her pregnancy.
The child’s guardian has been actively seeking help for the child so he
does not fall too far behind the average milestones. Therefore he is currently
visiting both a hearing and speech specialist. The hearing specialist
determined that the child is not able to fully hear out of this right ear. The
percentage of hearing that is present is unavailable based on the child’s age.
Every six months the child returns to the specialist to be retested and an
7

Alyssa Hofmann
accurate percentage for his hearing should be available when the child is
around seven years old. The speech therapist has come to the conclusion that
because of the child’s lack of hearing for the first eighteen months of his life,
he is verbally delayed by approximately ten to twelve months. Not only is the
specialist working with the child’s guardian but is also working with the
Developmental Daycare that he attends. Currently, after every three months
the child returns to get retested and the guardian is given new activities to
encourage his speech.
ASSESSMENT
One week before the first treatment the child was introduced to a
Visual Analog Scale(VAS) that was incorporated into aspects of his daily life.
When the child would mimic bad behaviour, throws toys on the floor, takes a
toy away from their sibling, fidgets at meals, get over emotional, or show
aggressive behaviour, the guardian would ask the child to point on the VAS
image to show his anger level or pick the picture that he related to most in that
situation. This VAS was used before and after his massage to record the way
he was feeling. The VAS scale was also implemented to measure his anger
when the child would spit, yell, pinch, hit or grab someone’s hair.
8

Alyssa Hofmann
Before the first treatment the therapist also performed bilateral muscle
testing (Dorsiflexion Maneuver) to test for both a Gastrocnemius or Soleus
contracture and the special tests (Thompson’s or Simmond’s) bilaterally to
rule out an Achilles tendon rupture. The therapist also performed a Tibialis
Anterior resisted muscle test before the first treatment, after the fifth
treatment, and then again after the last treatment.
Throughout the ten treatments, the child’s guardian was also keeping
track of certain aspects of the child’s behaviour on a daily basis and recording
these on a tally chart. The following were the aspect that the guardian was
asked to record: when the child would be walking on his toes, throwing toys
on the floor during a tantrum, have aggressive behaviour (pinching, hitting,
grabbing hair), take a toy away from a sibling, get unnecessarily over
emotional, fidgets at meal time, and mimics bad behaviour from their sibling
(spitting, yelling). These charts were then averaged out to show one week
before the first treatment, during days one through five of treatment, days five
through ten of treatment, and for a week after the last treatment.
Along with Resisted Muscle Tests and Special Tests the therapist also
performed a full body palpation of the client and modified postural
examination. This palpation found hypertonicity in the bilateral low arm
extensors, upper fiber Trapezius, and bilateral Tricep Surae group. The
postural examination showed that the child had a slight head forward posture,
9

Alyssa Hofmann
an anterior pelvic tilt, fallen arch on the right foot, and bilateral supination in
his feet.
Figure 1: Graph showing the average number of times the child showed the outcomes during the week
before the first treatment.
Figure 2:Visual Analog Scale used to show client’s anger levels and emotions.
10

Alyssa Hofmann
TREATMENT
The massage started with the child lying their back and the therapist
working on the right leg with fifteen seconds of Indian milking from the thigh
down to the ankle which was then followed with compression points of the
foot fanning outwards with the therapist’s thumbs starting by the heel and
working up to the toes repeating the stroke three times. Next, the therapist
used the palm of their hand and slowly stroked upwards from the heel to the
toes, stretching the toes in extension and holding for five seconds. From there,
the therapist used fingertip movement in small circles around the child’s ankle
for five seconds. Next moving into rolling of the leg between the palms of the
therapists hands starting at the ankle and moving to the upper thigh for ten
seconds. The therapist ended with feather stroking from the thigh to the toes
and repeated this three times. The leg was then placed onto the ground and the
same massage was performed on the left leg. Once both legs were complete
the therapist moved onto the stomach starting with paddling downwards with
the palms on the child’s stomach making water wheel motions down to the
hips for fifteen seconds. The therapist then used their palms in clockwise
circular motion repeating the circle five times with their fingers walking
11

Alyssa Hofmann
horizontally across the child’s stomach below and above the belly button
twice. The therapist then flexed and extended the child’s legs in a bicycle
motion, repeating this three times for each leg and then moved into a
clockwise knees to chest circle for fifteen seconds. To end the stomach
treatment the therapist put their hands on either side of the child’s stomach and
gently rocked the child back and forth for fifteen seconds. Next, the therapist
moved to the child’s chest, placing their thumbs on the child’s sternum and
stroked outwards, repeating this motion three times. Afterwards, the therapist
used their palms to draw three large hearts on the child’s chest. The therapist
then placed both hands on the child’s hips and rhythmically brought one hand
to the child’s opposite shoulder repeating this four times for both hands. The
therapist then moved on to the right arm, starting with fifteen seconds of
Indian milking followed by stretching of the child’s palm and fingers into
extension with the therapist thumbs for five seconds. After, the therapist rolled
the child’s arm between their palms starting from the wrist and working up to
the shoulder for ten seconds. Then, the therapist finished the arm with light
feather stroking repeating the stroke three times. The therapist then had the
child turn onto their stomach and initiated treatment by drawing three large
hearts on the child’s back. This was followed with paddling down from the
neck to the sacrum for fifteen seconds. Finally, the therapist used their
fingertips in a rake like position to perform running vibrations from the child’s
12
Alyssa Hofmann
neck down to the feet three times. The therapist ended the massage with one
hand on the child’s upper back and the other on the lower back in resting
position. The therapist excluded the face and head from the massage as the
child does not tolerate having this body part being touched. Throughout the
massage the therapist was calmly talking to the child about what was being
done.
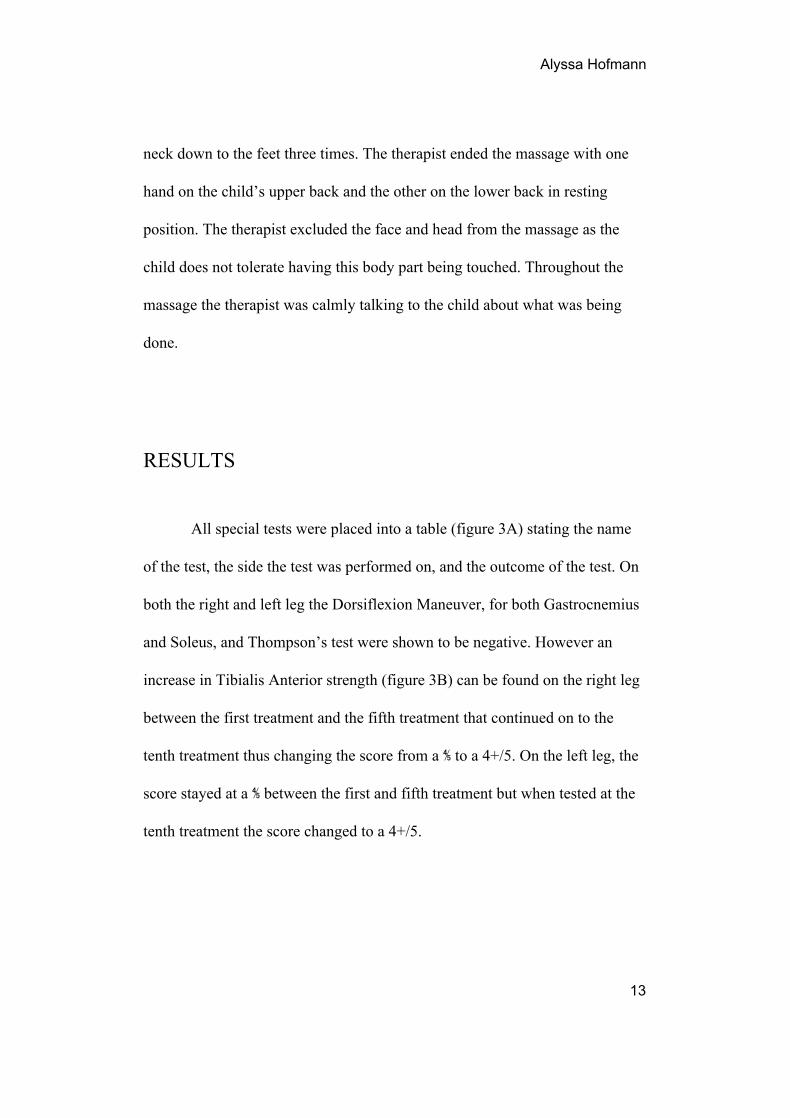
RESULTS
All special tests were placed into a table (figure 3A) stating the name
of the test, the side the test was performed on, and the outcome of the test. On
both the right and left leg the Dorsiflexion Maneuver, for both Gastrocnemius
and Soleus, and Thompson’s test were shown to be negative. However an
increase in Tibialis Anterior strength (figure 3B) can be found on the right leg
between the first treatment and the fifth treatment that continued on to the
tenth treatment thus changing the score from a ⅘ to a 4+/5. On the left leg, the
score stayed at a ⅘ between the first and fifth treatment but when tested at the
tenth treatment the score changed to a 4+/5.
13

Alyssa Hofmann
Test Side Outcomes
Dorsiflexion Maneuver Right Negative Gastrocnemius Negative Soleus
Dorsiflexion Maneuver Left Negative Gastrocnemius Negative Soleus
Thompson’s (Simmond’s) Right Negative
Thompson’s (Simmond’s) Left Negative Figure 3A: Table showing the tests performed on the client during the assessment.
Figure 3B: Graph showing the results of Tibialis Anterior resisted muscle test throughout the
treatments.
14

Alyssa Hofmann
Figure 4 is an average between treatments five and ten showing the
number of times per day that an outcome would occur. Between the week
before treatment and the first five treatments there was change in four of the
outcomes measures. The child’s aggressive behaviour and the amount of time
spent walking on his toes decreased by one, the amount of time spent fidgeting
at meals decreased by three and the amount the child gets over emotional
emotional decreased a total of five. However the amount the child throws toys
on floor, takes a toy away from someone, and mimics bad behaviour all stayed
the same.
Figure 4: Graph showing the average number of times the child showed the outcomes during the first five days after the first treatment.
15

Alyssa Hofmann
Figure 5 is showing the outcomes between the fifth and tenth
treatments. The amount of aggressive behaviour had increased by one and the
amount the child became over emotional increased by five. Outcomes that
stayed the same include the amount of fidgeting at meal times and the amount
of bad behaviour. The amount the child walks on his toes, throws toys on the
floor and takes a toy away from someone all decreased by one.
Figure 5: Graph showing the average number of times the child showed the outcomes during days five
through ten after the first treatment.
Figure 6 occurred in the week after the last treatment. During this week
the amount the client throws toys on the floor, his aggressive behaviour, and
16

Alyssa Hofmann
the amount the client got over emotional during situations all decreased.
However the amount the child walked on his toes and the amount he
mimicked bad behaviour both stayed the same while the amount of fidgeting
at meal time and the amount of times the child took toys away from someone
else both increased by one.
Figure 6: Graph showing the average number of times the child showed the outcomes during the week
after the last treatment.
The therapist also performed a full body palpation after the last
treatment in which they found no hypertonicity in the bilateral Tricep Surae
group although there was still slight hypertonicity in the upper fiber Trapezius.
17

Alyssa Hofmann
Overall from the week before the first treatment to the week after the
last treatment, the amount the child walks on his toes, throws toys on the floor,
and fidgets at meals all decreased by two. The amount the child showed
aggressive behaviour had decreased overall by one while the amount that the
child gets over emotional decreased by four. However the amount the child
mimicked bad behaviour and the amount of times he took toys away from
someone else both stayed the same throughout.
Figure 7: Graph showing side by side comparison of first treatment versus last treatment.
Throughout the massage treatments the child was asked to point on the
VAS scale whenever he would show the attributes that the therapist was
18

Alyssa Hofmann
monitoring. Although these VAS scores were recorded the therapist did not
deam them reliable enough to include in the study. Instead they were used to
present an opportunity for the child to reflect on his feelings and being able to
use the VAS as a method of communicating his feeling with adults.
CONCLUSIONS
The purpose of this case study was to determine if swedish massage
would impact a two year old’s behaviour. By the end of the treatments the
child walked on his toes less, throwed toys less, had less aggressive behaviour,
fidgeted at meals less and did not get as over emotional. The amount that the
child mimicked bad behaviour and took toys away from others both stayed the
same. These results however are casespecific because there is currently not
enough research available to support the fact that massage alone made the
changes. The results found in this case study could have been influenced by
visits with specialists, the child’s day care, and regular development. Another
factor that could have had influence would be the guardians work with the
child throughout the treatments. When talking with the child’s guardians two
weeks after the last massage they were pleased to report that the child was
asking for more massages and had an easier time accepting healthy touch,
whether in the form of tickling or hugging. They are planning to continue with
19
Alyssa Hofmann
at home massages as they hope to grow the relationship between themselves
and the child in a healthy manner.
However the results found from this case study were supported by
some of the research that has already been done on massage related to
developmentally delayed children⁶. If the study was performed again it would
be beneficial to use a larger case study with a control. The therapist could also
use a larger sample size therefore relating the study to a wider audience.
Hopefully in the future more research will be done to determine the effects
massage has on children with Fetal Alcohol Spectrum Disorder.
20

Alyssa Hofmann
REFERENCES 1. Cook J, Green C, Lilley C, Anderson S, Baldwin M, Chudley A, Conry J, LeBlanc N, Loock C, Lutke J, Mallon B, McFarlane A, Temple V, Rosales T. Fetal alcohol spectrum disorder: a guideline for diagnosis across the lifespan. Canadian Medical Association Journal. 2015;188(3):191197. 2. Sekhar SVyas N. Fetal Alcohol Spectrum Disorders. Sudanese Journal of Public Health [Internet]. 2012 [cited 2016 May 1];7(1). Available from: http://www.sjph.net.sd/files/Vol7N1/Original%20Article2.pdf
3.STREISSGUTH A, BOOKSTEIN F, BARR H, SAMPSON P, O'MALLEY K, YOUNG J. Risk Factors for Adverse Life Outcomes in Fetal Alcohol Syndrome and Fetal Alcohol Effects. Journal of Developmental & Behavioral Pediatrics. 2004;25(4):228238.
4. Freunscht IFeldmann R. Young Adults With Fetal Alcohol Syndrome (FAS): Social, Emotional and Occupational Development. Klinische Pädiatrie. 2010;223(01):3337.
5. Famy C, Streissguth A, Unis A. Mental Illness in Adults With Fetal Alcohol
Syndrome or Fetal Alcohol Effects. American Journal of Psychiatry.
1998;155(4):552554.
6. Tsuji S, Yuhi T, Furuhara K, Ohta S, Shimizu Y, Higashida H. Salivary
Oxytocin Concentrations in Seven Boys with Autism Spectrum Disorder
21

Alyssa Hofmann
Received Massage from Their Mothers: A Pilot Study. Frontiers in Psychiatry.
2015;6.
7. Field T. Massage therapy effects. American Psychologist.
1998;53(12):12701281.
8. Peadon E, RhysJones B, Bower C, Elliott E. Systematic review of
interventions for children with Fetal Alcohol Spectrum Disorders. BMC
Pediatrics. 2009;9(1):35.
22