the effect of upper trapezius taping on electromyographic activity …€¦ · ·...
TRANSCRIPT
Journal of Sport Rehabilitation, 1997, 6, 309-318 O 1997 Human Kinetics Publishers, lnc.
The Effect of Upper Trapezius Taping on Electromyographic Activity in the Upper
and Middle Trapezius Region
Gary E. Morin, David Tiberio, and Gary Austin
A characteristic of scapulothoracic dysfunction is the tendency for the upper regions of the trapezius to hypertrophy in relation to its middle and lower portions. This creates a muscular imbalance that can alter scapular position and subsequently the length-tension relationship of the shoulder muscles. Tape was applied over the right upper trapezius to inhibit electrical activity in the muscles of 10 uninjured subjects. EMG activity was recorded in two locations of the upper trapezius and one location in the middle to lower trapezius region while each subject maintained an isometric contraction designed to activate both muscles. With the tape applied, there was a statistically significant reduc- tion in EMG activity of the upper trapezius with a corresponding increase in the middle/lower trapezius. The ability of the tape to alter trapezius activity in this fashion may help correct muscular imbalances in the trapezius muscle.
Chronic shoulder pain can prevent full participation in physical activity in the athletic as well as the occupational setting. Pain can be centered in the area of the rotator cuff or elsewhere in the shoulder. Symptoms may be felt in the area between the cervical spine and the superior border of the scapula. Athletes as well as office workers often complain of pain, spasm, and "knots" in the upper trape- zius, superior to the medial angle of the scapula. Quite often, this pain must be managed as impingement or shoulder instability is treated.
Cervicobrachial conditions have been primarily studied in the occupational setting. Investigators have characterized the condition as stiff muscles often asso- ciated with discomfort and palpable tender spots in the muscle (1,6,7). The cause of this discomfort has not yet been fully determined (1,7), but there appears to be
Gary E. Morin is with the Department of Exercise Science, Southern Connecticut State University, New Haven, CT 065 15. David Tiberio is with the Department of Physical Therapy, University of Connecticut, Storrs, CT 06269. Gary Austin is with the Department of Sport, Leisure, and Exercise Sciences, University of Connecticut, Storrs.
31 0 Morin, Tiberio, and Austin
a correlation between repetitive mechanical stress on the musculoskeletal system and subsequent injury (6).
To determine the potential cause of this cervicobrachial pain, shoulder girdle function must be understood. Certain axioscapular muscles are important in the total function of the shoulder joint (3). The trapezius, rhomboids, serratus anterior, and levator scapulae appear to play a dominant role in the proper function of the shoulder girdle. These muscles elevate, depress, and rotate the scapula during shoul- der motion, helping to maintain proper alignment of the humeral head in the gle- noid fossa during arm motion and the appropriate length-tension relationship of the rotator cuff muscles (5).
The trapezius can be broken down into four distinct sections, with the lower three each directly acting on the scapula (10). The most superior section of the trapezius that inserts into the scapula elevates and upwardly rotates the scapula. Its motion is countered by the pull of the most inferior section of the trapezius, which originates on the lower nine thoracic vertebrae and inserts into the root of the scapular spine. This lower portion of the trapezius acts as a scapular depressor and down- ward rotator along with the latissimus dorsi. The middle trapezius, via its origin on C7 and TI-3, provides the mostly linear motion of scapular adduction and retrac- tion. The different alignments of the various sections of the trapezius muscle re- quire them to work together and to be balanced in strength for the scapula to be positioned properly during motion. However, certain activities tend to stress cer- tain sections of this muscle more than others.
The different sections of the trapezius have important roles in scapular mo- tion. Most occupational activities and overhead sports are characterized by consid- erable activity in this muscle (1, 5, 9). However, the amount of muscle activity present in each section of the muscle is not necessarily equal. The upward rotators of the scapula, particularly the upper elements of the trapezius, show greater EMG activity than its lower portion and other muscles of the region (1,5,7).
The upper sections of the trapezius, due to their suspensory roles, are con- stantly active during ambulation (lo), creating a constant tension overload in these fibers. The lower sections of the trapezius muscle do not exhibit similar activity. Therefore, the upper trapezius tends to hypertrophy more easily. Also, in individu- als with elevated scapulae, higher EMG activity is seen although its cause is uncer- tain.
In addition, there tends to be an overcompensation of the scapular elevators, like the upper trapezius, in sports involving significant overhead motion (4,9). The heightened upper trapezius activity can invariably lead to hypertrophy. Unfortu- nately, the lower to middle trapezius regions do not experience the same use and subsequently tend to be weaker in relation to the upper section, producing an im- balance. As a result, the scapula tends to become or remain elevated in these indi- viduals, possibly leading to shoulder joint pathology.
Fatigue of the shoulder girdle muscles may be one contributor to certain cervicobrachial pathologies. Hansson et al. (1) found that subjects experiencing

Upper Trapezius Taping 31 1
pain in the upper trapezius displayed less muscular endurance compared to sub- jects who performed the same occupation without pain.
The cause of pain in the upper trapezius and cervicobrachial region remains uncertain. However, scapular elevators appear to be more active during many ac- tivities and tend to become overdeveloped (4,9). Therefore, it would be helpful to determine a method of clinically decreasing muscle activity at the upper trapezius to lessen fatigue within the muscle and potentially return the scapula to its proper position.
Inhibition of the upper trapezius may also be helpful in rehabilitation of scapular dysfunction. Authors have reported the need to strengthen and shorten the lower fibers of the trapezius (4,8). Unfortunately, therapy may be prolonged un- less the scapular elevators can be prevented from becoming stronger and can be effectively lengthened to permit proper positioning of the scapula. An effective way of preventing additional strength gains and possibly reducing existing strength levels is to inhibit the muscle from maximally contracting. Prolonged inhibition of the upper trapezius, combined with shortening and strengthening of the lower tra- pezius, may restore proper balance between the muscle sections and decrease the time necessary for a successful return to physical activity.
Host (2) reported success with the application of tape to a symptomatic shoul- der. Using 8-10 strips of Leukosport Tape applied over protective Cover-Roll strips, she attempted to realign the shoulder to its proper position. The author applied additional strips to compress the upper fibers of the trapezius muscle. The subject was found to have pain-free motion with the tape applied. With prolonged use of the shoulder taping, muscle length imbalances improved with lengthening of the pectoralis minor. Host felt that scapular taping could be used to alleviate symp- toms of pain due to scapulothoracic dysfunction. However, her work was based on the results of one patient, and she did not determine the exact role of the tape in the treatment of the shoulder.
Therefore, we undertook to evaluate the effect of applying compressive shoul- der taping on the muscle activity of the upper trapezius. We hypothesized that muscle activity of the upper trapezius would decrease and activity of the lower trapezius would increase with shoulder taping. The results of this study will deter- mine if a method to inhibit upper trapezius activity can be devised. This could be of potential benefit in designing programs to prevent cervicobrachial syndromes and may also help to partially explain Host's success in treating shoulder pain with a taping procedure (2).
Methods
Ten active and healthy adult subjects (9 males, 1 female) participated in this study. Prior to testing, all subjects signed an informed consent document in accordance with University policy. All subjects were free of any significant shoulder injury at the time of the study.

31 2 Morin, Tiberio, and Austin
The subjects were seated upright and instructed to grasp the handles of an exercise tubing (Pro-Cord, Pro Orthopedics, Tucson, AZ), which was attached to a wall, 4 in. from the floor. Subjects were instructed to place their shoulders at 90" abduction and 45" internal rotation and to hold this position until the trial was completed (Figure 1). The upright position of the subject and 45" internal rotation created a right triangle arrangement, with one side created by the chair, the second side created by an imaginary line running 4 in. above and parallel to the floor, and the third side created by the exercise cord and the subject's forearms. Data collec- tion was initiated after the subject successfully attained the proper position for the isometric muscle contraction. Three trials were used for each a taped and a no-tape condition, with a 30-s rest provided between trials and approximately 3 min be- tween conditions.
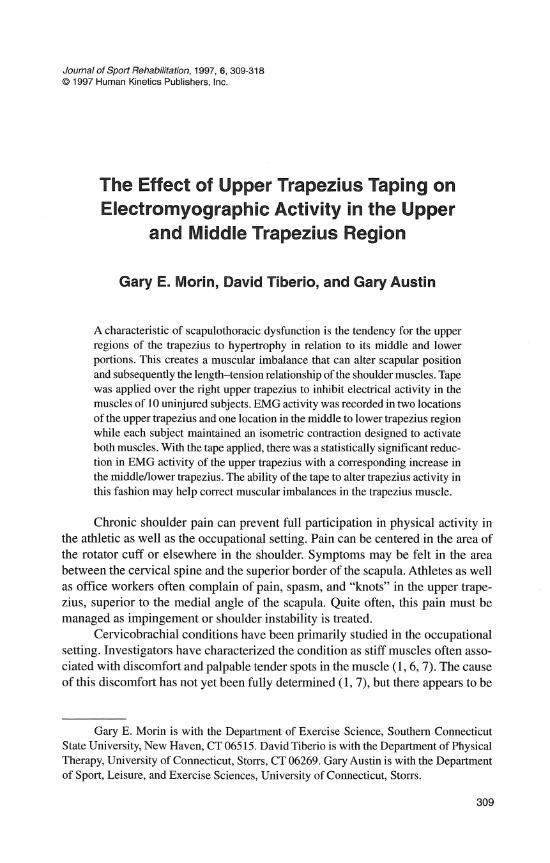
Jayshield (Jaybird, Lawrence, MA) was used to protect the subject's skin during the taped condition, and a strip of Leukotape P (Beiersdorf, Nonvalk, CT) was applied over it. The application consisted of one 2 in. wide strip of the Jayshield applied over the muscle belly of the right upper trapezius (Figure 2). The Jayshield extended inferiorly 6-7 in. down the anterior and posterior chest walls. One strip of 1.5-in. Leukotape P was applied over the Jayshield with equal force applied to both ends of the tape to compress the upper trapezius. The subject was asked if the tape felt snug, and if the response was negative, a second strip was applied over the first in a posterior to anteriorlinferior direction, ensuring adequate compression to the muscle belly. All of the taping procedures were done by the same researcher,
Figure. 1 - Simulated testing set-up for subject.

.snuada.q y@p 03 plagsLaf jo Map ~ouquv (q) .uogmgdde p~aysdef JO Map .roua$sod (a) -sraqg snuada~~ ~addn aq3 30 uo~ssa.~du~o~ JOJ 'dqdw rappoqs - z ad^
-uogmydde d adqoyna~ 30 Mapi Jo!.xa)uv (p) .uo!$ea
Upper Trapezius Taping 315
who made no effort to alter the position of the scapula on the posterior thorax while applying the tape.
Bipolar, preamplified surface electrodes (Therapeutics Unlimited, Iowa City, IA) were attached to the skin of the right shoulder at three locations (Figure 1). Two electrodes were placed over the upper trapezius, with one located between the clavicle and scapular spine approximately 1 in. medial to the acromioclavicular joint and the second attached 1-1.5 in. lateral to C4-5. A third electrode was placed between the medial scapular border and the thoracic spine halfway between the superior and inferior angles. The three electrodes were aligned parallel to the re- spective muscle fibers. A common ground electrode was placed on the subject's right wrist just proximal to the styloid process of the ulna styloid process. Elec- trode placement was maintained with a nonelastic tape.
EMG data were collected during 4-s time intervals beginning after each sub- ject was properly positioned. Root mean square (RMS) signal was used to assess the activity of the upper and lower trapezius muscles. EMG signals were pro- cessed with a time constant of 11.75 ms at a sampling rate of 1 ms using a 20 Hz low-cutoff filter. The main amplifier (Therapeutics Unlimited, Iowa City, IA) was linked to an IBM-compatible computer for data collection. Computerscope En- hanced Graphics Acquisition and Analysis Software (RC Electronics Inc., Santa Barbara, CA, 1992 version) was used for data analysis.
The testing order was counterbalanced, with the first subject and subsequent odd-numbered subjects beginning with the no-tape condition and ending with the taped condition. The second and subsequent even-numbered subjects began with the taped condition and ended with the no-tape condition. The RMS EMG results of the three electrodes were compared for the no-tape and taped conditions. A repeated-measures ANOVA was used to analyze changes in electrode RMS and the effect of the tape on the muscles. These ANOVAs were followed by a series of planned comparison t tests to determine differences between the individual elec- trodes due to condition. Significance was set at p < .05 for the ANOVA, with the significance level for the subsequent t tests set a tp < .0125 based on a Bonfferoni adjustment for the four multiple comparisons of the data.
Results
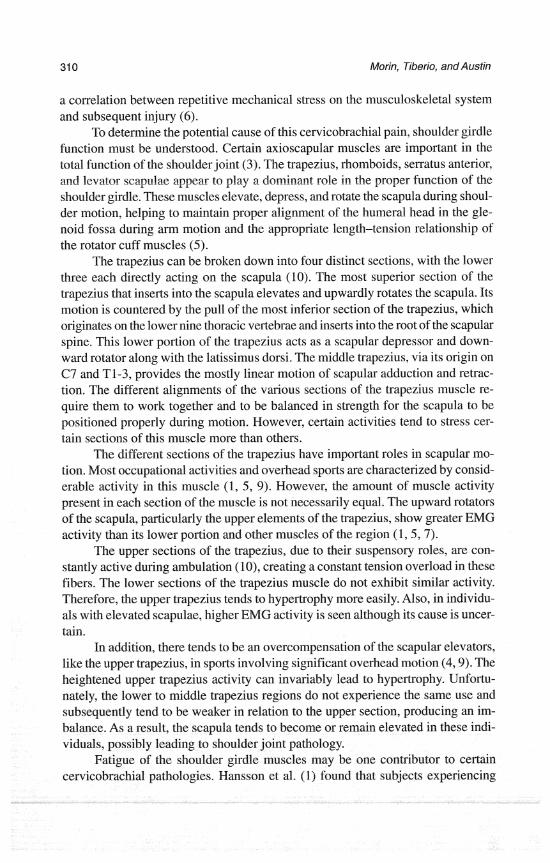
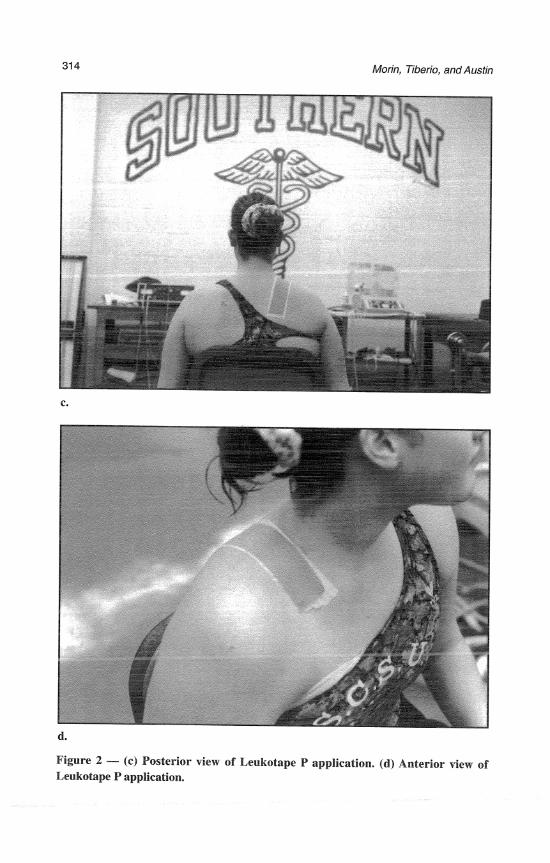
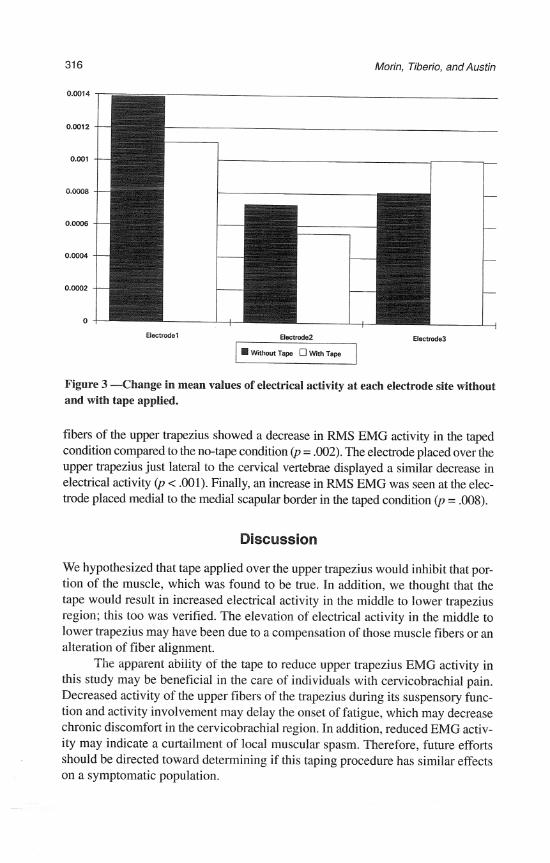
The mean differences for the three electrodes over the two conditions are pre- sented in Figure 3. There was a difference in the amount of RMS activity among the three attachment sites, F(2, 58) = 20.71, p < .001. No significant difference between conditions, F(1, 29) = 3.33, p = .0782, was found. However, a strong interaction between the electrodes and conditions, F(2,58) = 18.99, p < .001, was seen due to decreased activity at the two electrodes over the upper trapezius and increased activity at the lower trapezius electrode for the taped condition.
Planned comparison t tests revealed statistically significant differences for all three electrodes due to conditions. The electrode located over the lateral distal
31 6 Morin, Tiberio, and Austin
Electradel Electrode2 Electrode3 . Withart T a p W a T a p
Figure 3 -Change in mean values of electrical activity at each electrode site without and with tape applied.
fibers of the upper trapezius showed a decrease in RMS EMG activity in the taped condition compared to the no-tape condition @ = .002). The electrode placed over the upper trapezius just lateral to the cervical vertebrae displayed a similar decrease in electrical activity (p < .001). Finally, an increase in RMS EMG was seen at the elec- trode placed medial to the medial scapular border in the taped condition (p = .008).
Discussion
We hypothesized that tape applied over the upper trapezius would inhibit that por- tion of the muscle, which was found to be true. In addition, we thought that the tape would result in increased electrical activity in the middle to lower trapezius region; this too was verified. The elevation of electrical activity in the middle to lower trapezius may have been due to a compensation of those muscle fibers or an alteration of fiber alignment.
The apparent ability of the tape to reduce upper trapezius EMG activity in this study may be beneficial in the care of individuals with cervicobrachial pain. Decreased activity of the upper fibers of the trapezius during its suspensory func- tion and activity involvement may delay the onset of fatigue, which may decrease chronic discomfort in the cervicobrachial region. In addition, reduced EMG activ- ity may indicate a curtailment of local muscular spasm. Therefore, future efforts should be directed toward determining if this taping procedure has similar effects on a symptomatic population.

Upper Trapezius Taping 31 7
Perhaps more importantly, the apparent inhibition of the upper trapezius may have allowed the lower sections of the trapezius to increase activity to compensate for the decreased upper trapezius involvement. In this study, middle to lower tra- pezius EMG increased with the tape applied to the upper trapezius, even though the same exercise was done. This would facilitate an increase in middle to lower trapezius strength without a similar increase of the upper trapezius, potentially preventing a muscle imbalance. It is possible that an imbalance among the differ- ent sections of the trapezius could be corrected, which would in turn correct scapu- lar positioning and restore the normal length-tension relationship of the rotator cuff.
However, the mechanism behind the alteration in electrical activity is not known. Smith and Gilleard found that patellofemoral taping to correct anteroposterior tilt altered muscle activity in the vastus medialis oblique and the vastus lateralis (11). They found a delayed onset of vastus lateralis activity due to the presence of the tape, with a corresponding facilitation of the vastus medialis oblique. The authors postu- lated that this might indicate a change in direction of the muscle fibers as the mecha- nism of improvement. Compression of the upper trapezius may have altered align- ment of the muscle fibers enough to change the angle of muscle pull; however, a direct reduction in muscle activity due to compression cannot be ruled out.
The results of the present study may help to explain some of Host's (2) suc- cess. Her patient experienced relief when tape was applied to his shoulder and upper trapezius despite the failure of previous rehabilitation protocols. A decrease in muscle activity may have disrupted the pain cycle by inhibiting contraction of the involved musculature. However, it should be noted that Host used additional strips of tape in an effort to correct for improper scapular positioning. This may have created a certain amount of "slack" in the posterior shoulder girdle muscles and an increase in space between the acromion and humeral head. This aspect of the taping procedure remains to be examined.
CervicobrachiaVupper trapezius pain is often difficult to treat, and there may be a link with dysfunction in this area and other shoulder joint problems. There- fore, methods must be devised to correct this condition. Compressive taping of the upper trapezius appears to help reduce muscle activity and permit an increase in the activity of the lower to middle trapezius.
The results of this study were based on the effects of taping on healthy sub- jects. Taping procedures of this type may result in similar effects in individuals experiencing cervicobrachial pain and scapulothoracic dysfunction and may serve as a helpful adjunct modality in their treatment. Therefore, studies should be de- veloped using individuals suffering from similar cervicobrachial pain. Suggested future topics include whether a similar taping procedure can decrease upper trape- zius activity in subjects experiencing pain, and whether pain can be alleviated with the shoulder taped. If the taping protocol benefits affected subjects, follow-up work will be needed to help incorporate this modality into rehabilitation protocols for similar dysfunctions.

References
Morin, Tiberio, and Austin
1. Hansson, G., U. Stromberg, B. Larsson, K. Ohlsson, I. Balogh, and U. Moritz. Elec- tromyographic fatigue in necklshoulder muscles and endurance in women with repeti- tive work. Ergonomics 35: 1341-1352,1992.
2. Host, H. Scapular taping in the treatment of anterior shoulder impingement. Phys. Dzer. 75:803-812, 1995.
3. Inman, V., M. Saunders, and L. Abbott. Observations on the function of the shoulder joint. J. Bone Joint Surg. 26: 1-30, 1994.
4. Kelley, M. Anatomic and biomechanical rationale for rehabilitation of the athlete's shoulder. J. Sport Rehabil. 4: 121-154, 1995.
5. Kibler, W.B. Role of the scapula in the overhead throwing motion. Orthopedics 22525- 532,1991.
6. Nieminen, H., and S. Hameenoja. Quantification of the static load component in muscle work using nonlinear filtering of surface EMG. Ergonomics 38: 11 72-1 183, 1995.
7. Oberg, T., L. Sandsjo, and R. Kadefors. Subjective and objective evaluation of shoulder muscle fatigue. Ergonomics 37:1323-1333, 1994.
8. Paine, R., and M. Voight. The role of the scapula. J. Orthop. Sports Phys. Ther. 18:386- 391,1993.
9. Pink, M., J. Peny, and A. Browne. The normal shoulder during freestyle swimming. Am. J. Sports Med. 19569-575, 1991.
10. Schenkman, M., and V. Rugo De Cartaya. Kinesiology of the shoulder complex. J. Orthop. Sports Phys. Thel: 8:438-450, 1987.
I I. Smith, M.D., and W.L. Gilleard. Electromyography assessment of quadriceps activa- tion when using McConnell taping for inferior patella pain. In Proceedings of the First Australasian Biomechanics Conference, Sydney, Australia, 1996.