the doubled-suture nice knot - semantic scholar · abstract: the authors describe a novel suture...
TRANSCRIPT
e382 Copyright © SLACK inCorporAted
n tips & techniquesSection Editor: Steven F. Harwin, MD
The Doubled-Suture Nice KnotPascal Boileau, MD; Ghassan Alami, MD, FRCS(C); Adam Rumian, MD, FRCS; Daniel G. Schwartz, MD; Christophe Trojani, MD, PhD; Adam J. Seidl, MD
Secure fixation is crucial for tissue healing, whether it
is bone or soft tissue. A knot is considered to be of good quality
if it is easy to learn and tie, has a low profile, has good loop and knot security, and allows accu-rate control of the tension ap-
plied.1-4 Traditionally, flat non-sliding knots, such as square knots, have been used in open surgery because they have been perceived to be more secure than sliding knots. With the de-velopment of arthroscopic and endoscopic surgery, the techni-cal challenges of tying intracor-poreal flat knots have contribut-ed to the development of many effective sliding knots.5-15
Besides the knot itself, the type of suture used and its configuration are also impor-tant biomechanical parameters that should be taken into ac-count at the time of soft tissue and bone repair. It has been the authors’ experience that doubling the suture on itself provides a stronger means of fixation for both soft tissue and bone repair. However, the use of a doubled suture means that a specific knot must be done to provide both progressive tensioning and secure fixa-tion. For the past 10 years, the authors have been using the doubled-suture Nice knot for the fixation of bone fragments and soft tissues alike, in vari-ous surgical contexts.
In this article, the authors describe a novel fixation tech-nique that combines a doubled suture with a sliding knot that is self-stabilizing (nonslip-ping), adjustable, easy to per-form, and solid. The doubled-suture Nice knot can be tied in both open and arthroscopic surgery to fix torn tendons/ligaments and fractured/oste-otomized bones. Its use with a doubled high-strength suture also makes it applicable in a variety of contexts involving large displacement forces.
TechniqueA high-caliber (at least No.
1), braided, absorbable or non-absorbable suture is used. The suture is doubled over itself to obtain 2 free limbs on one end and a loop on the other (Fig-ure 1A). The suture is passed around the tissues to be fixed, using a suture shuttle or a re-movable needle mounted on the loop end. Alternatively, a com-mercially available “looped” suture with needle can be used (Figure 2). A simple square knot is thrown using the loop on 1 hand and the 2 free
The authors are from the Department of Orthopaedic Surgery and Sports Traumatology (PB, DGS, CT), L’Archet2 Hospital, University of Nice- Sophia-Antipolis, Nice, France; Saint Jérôme Hospital (GA), Montreal, Que-bec, Canada; Spire Harpenden Hospital (AR), Hertfordshire, United King-dom; and the Department of Orthopaedics (AJS), University of Colorado, Aurora, Colorado.
Drs Alami, Rumian, Schwartz, Trojani, and Seidl have no relevant finan-cial relationships to disclose. Dr Boileau is an unpaid consultant for Smith & Nephew, is on the speaker’s bureau of Smith & Nephew, receives royalties from Wright Medical, receives travel expenses from Smith & Nephew and Wright Medical, and holds stock in Imascap.
Correspondence should be addressed to: Pascal Boileau, MD, Depart-ment of Orthopaedic Surgery and Sports Traumatology, L’Archet2 Hospital, University of Nice-Sophia-Antipolis, 151 Route de St Antoine de Ginestière, 06200 Nice, France ([email protected]).
Received: March 29, 2016; Accepted: June 14, 2016. doi: 10.3928/01477447-20161202-05
Abstract: The authors describe a novel suture fixation tech-nique that combines a doubled suture with a sliding knot. The knot can be tied in both open and arthroscopic surgery to fix torn tendons/ligaments and fractured/osteotomized bones. The advantages of the doubled-suture Nice knot include strength, adjustability, simplicity, and versatility. This technique, which has proven useful in the authors’ practice for the past 10 years, has replaced metallic wires and cables for bone fixation. The doubled-suture Nice knot can also be tied over a double-button and has been used for ankle syndesmosis, acromioclavicular joint separation repair, and coracoid bone block fixation. [Or-thopedics. 2017; 40(2):e382-e386.]

n tips & techniques
MARCH/APRIL 2017 | Volume 40 • Number 2 e383
limbs on the other (treated as a simple, undoubled suture) (Figure 1B). The loop is opened and both free limbs are passed through it (Figure 1C). The knot is then dressed by making the loop smaller (Figure 1D). When ready to secure the involved tissues, sur-geons tighten down the sliding knot by either pulling the 2 free limbs apart (Figure 1E)—as done during open surgery—or pulling the free limbs (acting as the post) back toward them, which is most useful during ar-throscopic surgery. As with oth-er sliding knots, while the post is being pulled back, the knot can be helped down either man-ually or with an arthroscopic knot pusher to reduce the trac-tion forces seen by the tissues around which the sutures are sliding. Another way to reduce such traction forces is to pull the 2 free limbs of the post sep-arately in alternation (but still in the same axis). Finally, 3 alter-
nating half-hitches or surgeon’s knots are performed using the 2 separated free limbs (Figure 1F). This precludes the pos-sibility that the free limbs will slide back out of the loop, thus securing the knot definitively. As excellent as its loop security and holding capacity may be, the authors consider the knot provisional until secured de-finitively with the 3 alternating half-hitches.16,17
ApplicATionsThe following are a few
examples of the various con-texts, open and arthroscopic, in which the doubled-suture Nice knot has proven useful.
Tuberosity Fixation During Fracture Treatment With Humeral Hemiarthroplasty or Reverse Shoulder Arthroplasty
The authors’ technique for tuberosity fixation using 4 horizontal cerclages and 2 ver-tical tension-band sutures has
been published previously.18 The authors have modified their technique in that each cerclage and tension-band su-tures are now made using the Nice knot with strong (eg, No. 5 Ethibond [Ethicon, Somer-ville, New Jersey] or No. 2 Or-thocord [DePuy Mitek, War-saw, Indiana]) nonabsorbable sutures. As explained above, the knots can be tightened in stages without slipping. This allows provisional fixation while the tuberosity positions are adjusted to achieve an ana-tomic reduction (Figures 3-4).
Fixation of an Isolated Greater Tuberosity After Acute Fracture, Nonunion, or Malunion
For fixation of an isolated greater tuberosity after acute fracture, nonunion, or mal-union, the horizontal cerclage double sutures are passed through the hard bone of the bicipital groove (or through
the lesser tuberosity) on one side and through the tendons of the infraspinatus and teres minor distally on the other side. This technique can also be used for the treatment of 3- or 4-part fractures, together with a lateral locking plate or intramedullary humeral nail.
Cerclage Sutures for Humerotomy or Femorotomy Fixation During Revision Arthroplasty
Multiple doubled sutures can be shuttled around the diaphysis and used for cerclage. This is
A B C
DFigure 1: Knot technique. A doubled-over suture is passed around the tissue (A). A single square knot is thrown (B). The 2 free limbs are passed through the loop (C). The knot is dressed (D). The knot is slid down by pulling the 2 free limbs apart (E). (The 2 limbs can also be pulled back toward the surgeon at once or alternately. A knot pusher can also be used to help the knot down while the limbs are being pulled.) The tightened knot is ready to be secured with 3 alternating half-hitches or surgeon’s knots (F).
E F
Figure 2: A doubled-over suture with a needle.
e384 Copyright © SLACK inCorporAted
n tips & techniques
much easier than passing wires or cables and is less traumatic to
the surrounding soft tissues, both during insertion and in case of an
unexpected breakage. Two, 3, or 4 cerclages are set up and, again,
partially and progressively tight-ened while the osteotomy frag-ment is reduced anatomically. Suture is less likely than wires or cables to irritate the surrounding tissues; yet, if for any reason the doubled-suture cerclage needs to be removed, it is much easier to cut with scissors and pull out (Figure 5).
Fixation of Small Butterfly Fragments
A butterfly (wedge) frac-ture fragment is often encoun-tered when performing open reduction and internal fixation of fractures of, for instance, the clavicle or distal fibula. An attempt to fix such a butterfly fragment with a lag screw can result in its fragmentation or devitalization. However, it is a simple matter to pass 1 or 2 doubled sutures around it and secure it with the Nice knot.
Arthroscopic ApplicationsThe authors systematically
use the Nice knot when per-forming side-to-side rotator cuff repairs or anchorless, transos-seous repairs (Figure 6).19 In some situations, they also pass a doubled suture through the eye-let of an anchor and use it with the Nice knot as they would any other sliding arthroscopic knot. The authors have also used this technique in the fixation of both posterior and anterior bone blocks for the treatment of shoulder instability. Finally, the doubled-suture Nice knot can also be tightened over a double-button for anterior cruciate liga-ment graft fixation, ankle syn-desmosis, or all-arthroscopic reconstruction of acromiocla-vicular joint disruptions.20
A B
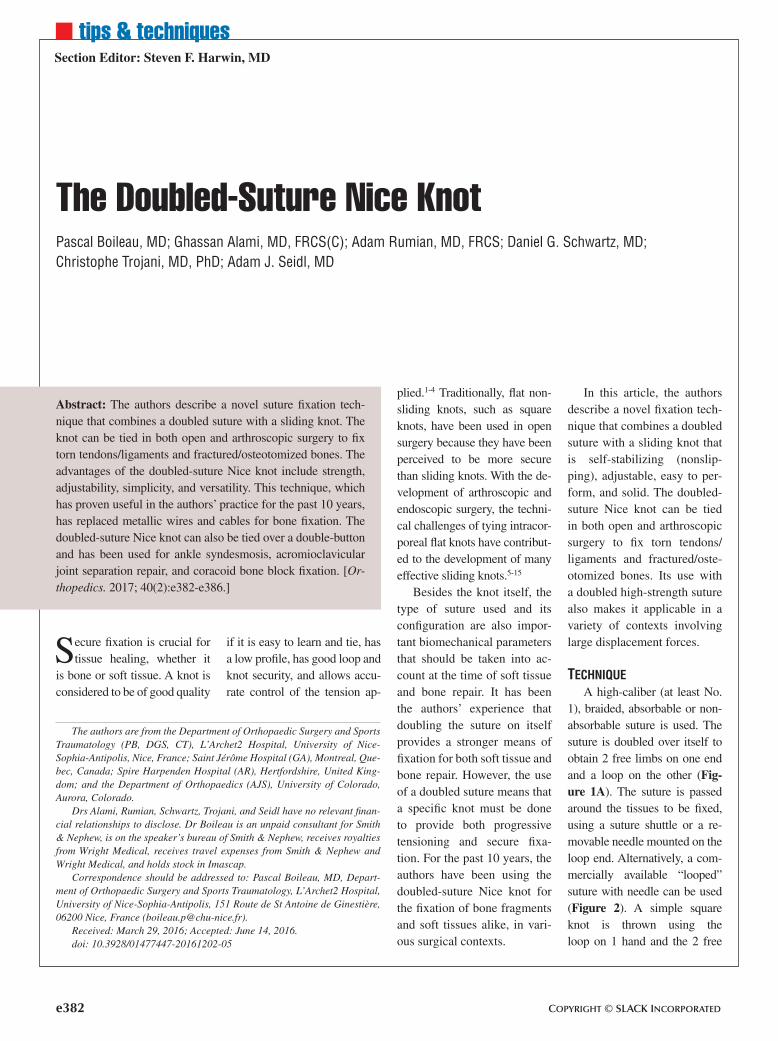
CFigure 3: Tuberosity fixation during hemiarthroplasty for proximal humerus fracture (left shoulder, anterosuperior “sa-ber” incision). Note that 2 cerclages have already been placed to fix the greater tuberosity to the prosthesis (after bring-ing the arm into external rotation for anatomic tuberosity reduction). This figure illustrates the 2 final cerclages around both tuberosities, their doubled sutures having been shuttled around with a regular needle-loaded suture. With the lower blue cerclage, a Nice knot is prepared and left loose; on the upper green cerclage, a Nice knot is tightened provisionally (A). The tuberosity reduction is adjusted as required, then the lower blue cerclage Nice knot is tightened (B). The upper green cerclage can now be tightened definitively, then both knots are secured and cut (C). Final appearance with all 4 cerclages and 2 vertical tension bands in place (D).
D
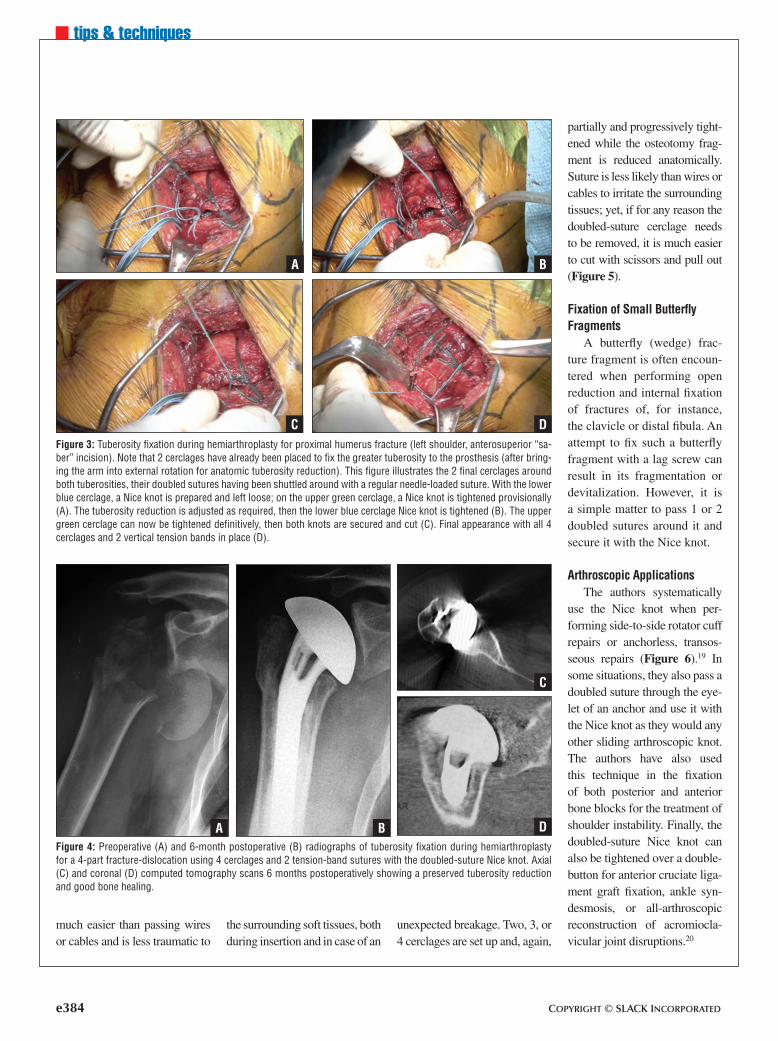
Figure 4: Preoperative (A) and 6-month postoperative (B) radiographs of tuberosity fixation during hemiarthroplasty for a 4-part fracture-dislocation using 4 cerclages and 2 tension-band sutures with the doubled-suture Nice knot. Axial (C) and coronal (D) computed tomography scans 6 months postoperatively showing a preserved tuberosity reduction and good bone healing.
C
DBA

n tips & techniques
MARCH/APRIL 2017 | Volume 40 • Number 2 e385
Other Possible ApplicationsThe authors have also used
the doubled-suture Nice knot for tension banding of olecra-non fracture and for patellar fracture fixation. This novel fixation technique has proven useful in their practice for the past 10 years, replacing metal-lic wires and cable fixation.
DiscussionAdvantages
The doubled-suture Nice knot has several advantages. First, its use of a doubled-over suture theoretically doubles the suture’s strength. The ten-sion in each strand is halved, as is the risk of breakage. The doubling of the suture also re-sults in increased internal fric-tion, which translates into ex-cellent loop and knot security.1
Second, tightening the knot by pulling the free limbs apart results in a feel similar to that of flattening a half-hitch or surgeon’s knot, allowing more accurate and adjustable ten-sioning of the suture.
Third, the tightening pro-cess can be stopped and re-sumed at any stage, as the loop security of the knot prevents it from slipping. Thus, when repairing a tissue under ten-sion, 2 or more sutures can be placed an appropriate distance apart and the Nice knot can be prepared on each of them (Fig-ure 4). Provisional tightening can then be performed and the reduction adjusted as required before the knots are finally tightened and secured. This is in stark contrast to tying a sim-ple knot, which requires imme-diate and irreversible locking, constant tension on the limbs,
or other extra (and sometimes unreliable) maneuvers by an assistant to prevent slippage.
Fourth, as long as it has not yet been secured, the knot can be completely undone by sim-ply pulling the free limbs back out of it. Once that is done, the knot unravels automatically and the doubled suture can be reused immediately.
Fifth, despite the above advantages, the Nice knot re-mains a low-profile, simple knot compared with other ex-isting sliding knots. By com-bining a relatively simple ini-tial knot with equally simple security knots, the Nice knot provides knot security with-out excessive complexity and bulkiness. Bulkiness is espe-cially undesirable when a knot made with nonabsorbable su-ture is left adjacent to articular cartilage or moving tendons.12
Needled double sutures are available and can be used with either an absorbable (Doubled PDS; Ethicon) or a nonabsorb-able (NiceLoop; Tornier Inc, Bloomington, Minnesota) su-ture (Figure 2).
Comparison With Related Knots
The closest relative to the doubled-suture Nice knot is the “modified racking hitch” knot. Although derived from the same “cow hitch” prede-cessor, the modified racking hitch is less straightforward and symmetric.21 Thus, in ad-dition to being more difficult to perform, the internal friction and interference is increased in the modified racking hitch knot, making it also relatively more difficult to slide. The
simpler “racking hitch” knot, which the senior author (P.B.) used prior to the Nice knot, had too little internal interfer-
ence and therefore not enough holding power.
An even more complex knot, the “giant knot,” is re-
Figure 5: Nice knot for humerotomy fixation. Preoperative anteroposterior ra-diograph of an uncemented humeral stem requiring revision. A humerotomy was required for stem extraction (A). Anteroposterior radiograph of the revised prosthesis showing good fixation of the humerotomy. The subtle notches seen on the outside of the diaphysis (arrows) are the radiographic evidence of the presence (and strength) of the doubled-suture Nice knots (B).
BA
Figure 6: Two doubled-suture Nice knots secured and cut after being used in a transosseous, anchorless rotator cuff repair.
e386 Copyright © SLACK inCorporAted
n tips & techniques
ported to have enough inter-nal interference after being “flipped” to not require se-curing with additional knots.8 Concern has previously been expressed regarding the effect of such post switching on knot tightness and tissue apposi-tion.12 In addition, this knot is performed with a single, not a double, suture.
Comparisons between these various knots have yet to be made with objective laboratory testing. The mentioned phe-nomena and the authors’ clini-cal experience with all of the above knots together support their conclusion that the Nice knot strikes the best balance among all of the attributes of the ideal sliding knot.
LimitationsThe strength of this tech-
nique may be underestimated while the knot is tightened. This may lead to ischemia of the tissues being fixed. Fur-thermore, later on, the weak-est link in the construct may be the bone or soft tissues themselves. Thus, the sur-geon should not subject them to unreasonable biomechani-cal conditions (eg, acceler-ated weight bearing or resisted
range of motion) simply be-cause a stronger fixation tech-nique has been employed.
conclusionThe doubled-suture Nice
knot is helpful and remarkably easy to execute. The authors encourage other surgeons to employ it. Whether in trauma or elective surgery, in open surgery or arthroscopy, its ap-plications are numerous. Its strength and effectiveness can provide the surgeon with con-fidence and efficiency in vari-ous critical surgical situations.
RefeRences 1. Burkhart SS, Wirth MA, Si-
monich M, Salem D, Lanctot D, Athanasiou K. Knot security in simple sliding knots and its re-lationship to rotator cuff repair: how secure must the knot be? Arthroscopy. 2000; 16(2):202-207.
2. Lo IK, Burkhart SS, Chan KC, Athanasiou K. Arthroscopic knots: determining the opti-mal balance of loop security and knot security. Arthroscopy. 2004; 20(5):489-502.
3. Nottage WM, Lieurance RK. Arthroscopic knot tying tech-niques. Arthroscopy. 1999; 15(50):515-521.
4. Tera H, Aberg C. Strength of knots in surgery in relation to type of knot, type of suture ma-terial and dimension of suture thread. Acta Chir Scand. 1977; 143(2):75-83.
5. Babetty Z, Sumer A, Altintas S. Knot properties of alternat-ing sliding knots with differ-ent patterns in comparison to alternating and simple sliding knots. J Am Coll Surg. 1998; 186(4):485-489.
6. Balg F, Boileau P. The Mid-Ship knot: a new simple and secure sliding knot. Knee Surg Sports Traumatol Arthrosc. 2007; 15(2):217-218.
7. De Beer JF, van Rooyen K, Boezaart AP. Nicky’s knot: a new slip knot for arthroscopic surgery. Arthroscopy. 1998; 14(1):109-110.
8. Fleega BA, Sokkar SH. The gi-ant knot: a new one-way self-locking secured arthroscopic slip knot. Arthroscopy. 1999; 15(4):451-452.
9. Jo CH, Yoon KS, Lee JH, Kang SB, Lee MC. The slippage-proof knot: a new, nonstacking, arthroscopic, sliding locking knot with a lag bight. Orthope-dics. 2007; 30(5):349-350.
10. Karahan M, Akgun U, Espreg-ueira-Mendes J. The Pretzel knot: a new simple locking slip-knot. Knee Surg Sports Traumatol Arthrosc. 2010; 18(3):412-414.
11. Klobucar H, Delimar D, Cicak N, Korzinek K. A secure lock-ing knot for microsuturing. J Reconstr Microsurg. 2001; 17(5):331-334.
12. Pallia CS. The PC knot: a se-cure and satisfying arthroscopic slip knot. Arthroscopy. 2003; 19(5):558-560.
13. Ramirez OM, Tezel E, Ersoy B. The Peruvian fisherman’s knot: a new, simple, and versatile self-locking sliding knot. Ann Plast Surg. 2009; 62(2):114-117.
14. Tera H, Aberg C. Tensile strengths of twelve types of knot employed in surgery, using different suture materials. Acta Chir Scand. 1976; 142(1):1-7.
15. Thacker JG, Rodeheaver G, Moore JW, et al. Mechani-cal performance of surgical sutures. Am J Surg. 1975; 130(3):374-380.
16. Chan KC, Burkhart SS, Thiaga-rajan P, Goh JC. Optimization of stacked half-hitch knots for arthroscopic surgery. Arthros-copy. 2001; 17(7):752-759.
17. Loutzenheiser TD, Harry-man DT II, Yung SW, France MP, Sidles JA. Optimizing ar-throscopic knots. Arthroscopy. 1995; 11(2):199-206.
18. Boileau P, Walch G, Krishnan SG. Tuberosity osteosynthesis and hemiarthroplasty for four-part fractures of the proximal humerus. Tech Shoulder Elbow Surg. 2000; 1(2):96-109.
19. Boileau P, Brassart N, Watkin-son DJ, Carles M, Hatzidakis AM, Krishnan SG. Arthroscop-ic repair of full-thickness tears of the supraspinatus: does the tendon really heal? J Bone Joint Surg Am. 2005; 87(6):1229-1240.
20. Boileau P, Old J, Gastaud O, Brassart N, Roussanne Y. All-arthroscopic Weaver-Dunn-Chuinard procedure with double-button fixation for chronic acromioclavicular joint dislocation. Arthroscopy. 2010; 26(2):149-160.
21. Chokshi BV, Ishak C, Iesaka K, Jazrawi LM, Kummer FJ, Rosen JE. The modified rack-ing hitch (MRH) knot: a new sliding knot for arthroscopic surgery. Bull NYU Hosp Jt Dis. 2007; 65(4):306-307.