the digestive system the alimentary canal or gastrointestinal (gi) tract digests and absorbs food...
TRANSCRIPT
The Digestive system
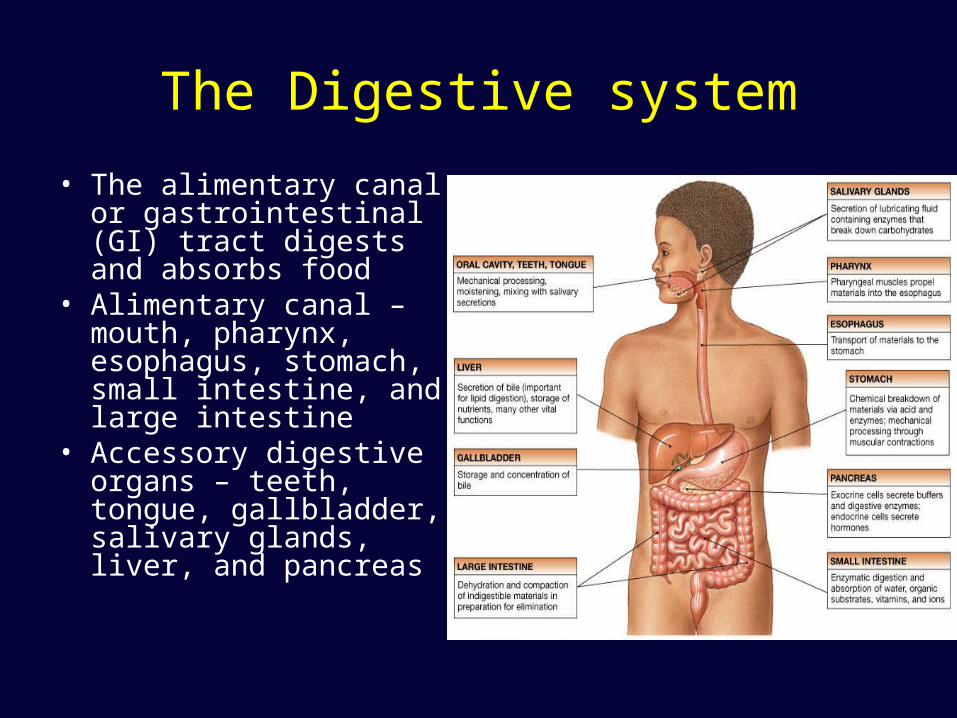
• The alimentary canal or gastrointestinal (GI) tract digests and absorbs food
• Alimentary canal – mouth, pharynx, esophagus, stomach, small intestine, and large intestine
• Accessory digestive organs – teeth, tongue, gallbladder, salivary glands, liver, and pancreas
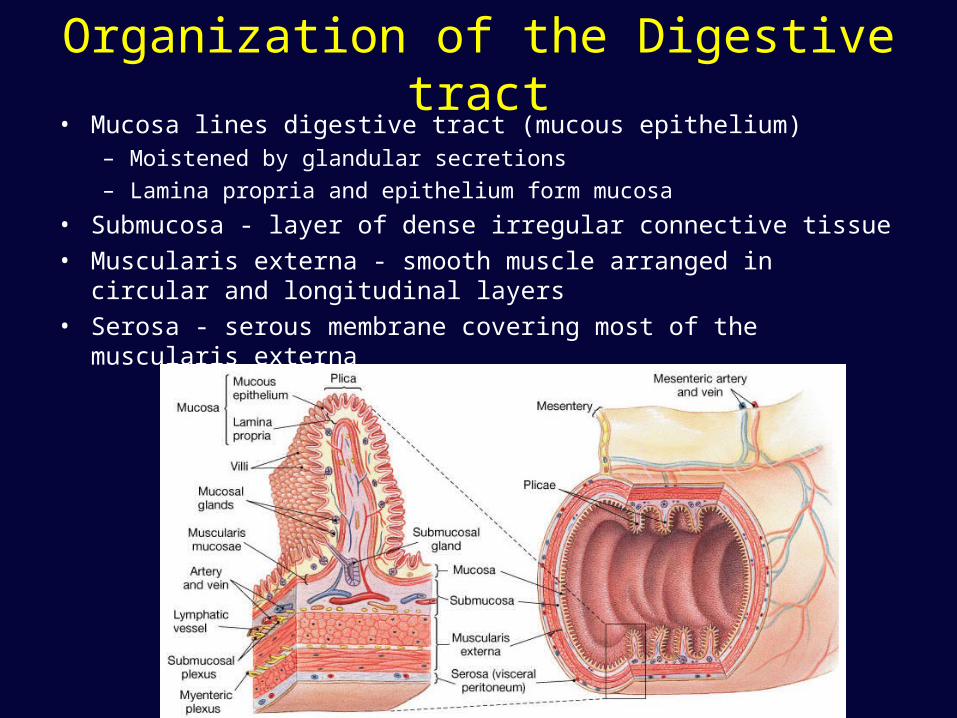
Organization of the Digestive tract• Mucosa lines digestive tract (mucous epithelium)
– Moistened by glandular secretions
– Lamina propria and epithelium form mucosa
• Submucosa - layer of dense irregular connective tissue• Muscularis externa - smooth muscle arranged in circular and
longitudinal layers• Serosa - serous membrane covering most of the muscularis externa

Figure 21-2c
Digestive System Anatomy
Digestive System Anatomy
Digestive System Activities
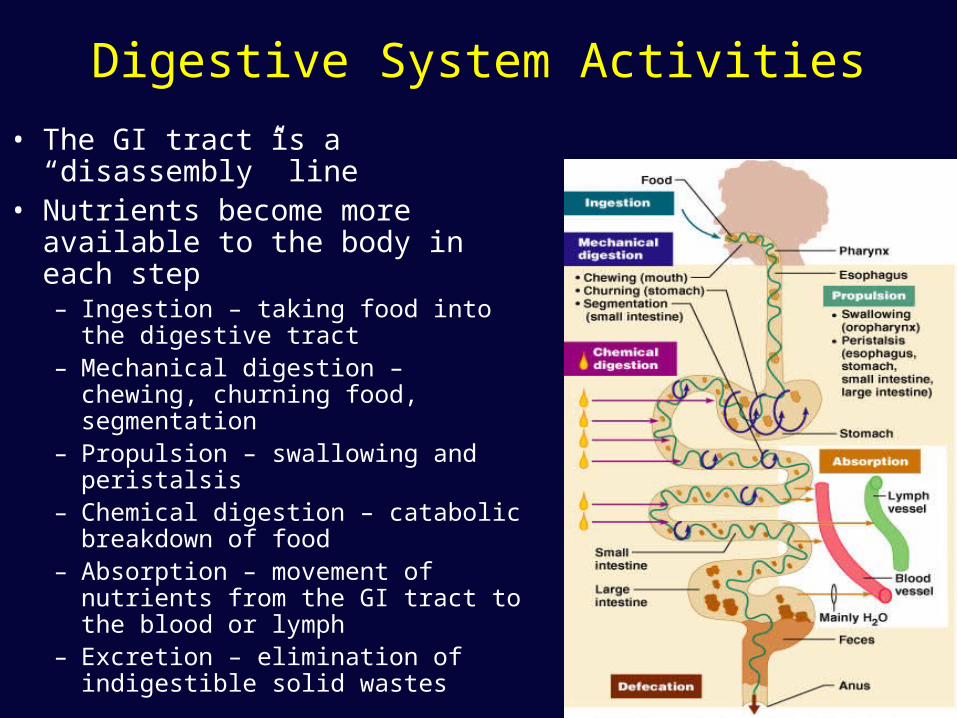
• The GI tract is a “disassembly” line
• Nutrients become more available to the body in each step– Ingestion – taking food into the
digestive tract – Mechanical digestion – chewing,
churning food, segmentation – Propulsion – swallowing and
peristalsis– Chemical digestion – catabolic
breakdown of food– Absorption – movement of nutrients
from the GI tract to the blood or lymph
– Excretion – elimination of indigestible solid wastes
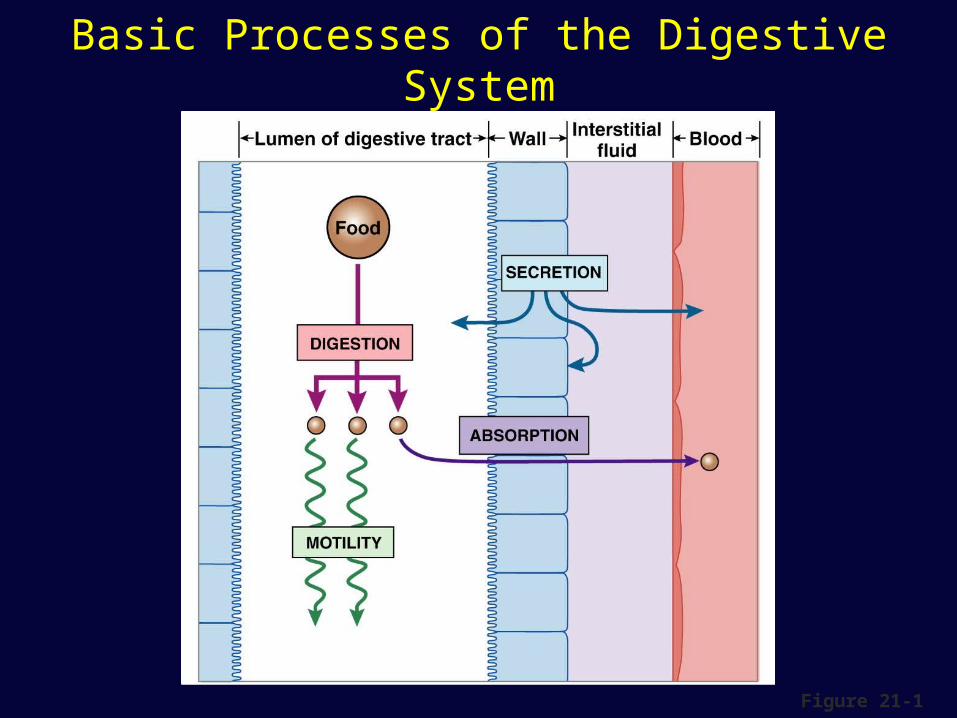
Basic Processes of the Digestive System
Figure 21-1
Motility
• Movement of digestive materials
• Visceral smooth muscle– Tonic contractions
• Sustained• Smooth muscle sphincters and stomach
– Phasic contractions • Rhythmic cycles of activity - pacemaker cells• Last a few seconds• Peristalsis moves bolus forward• Segmentation mixes
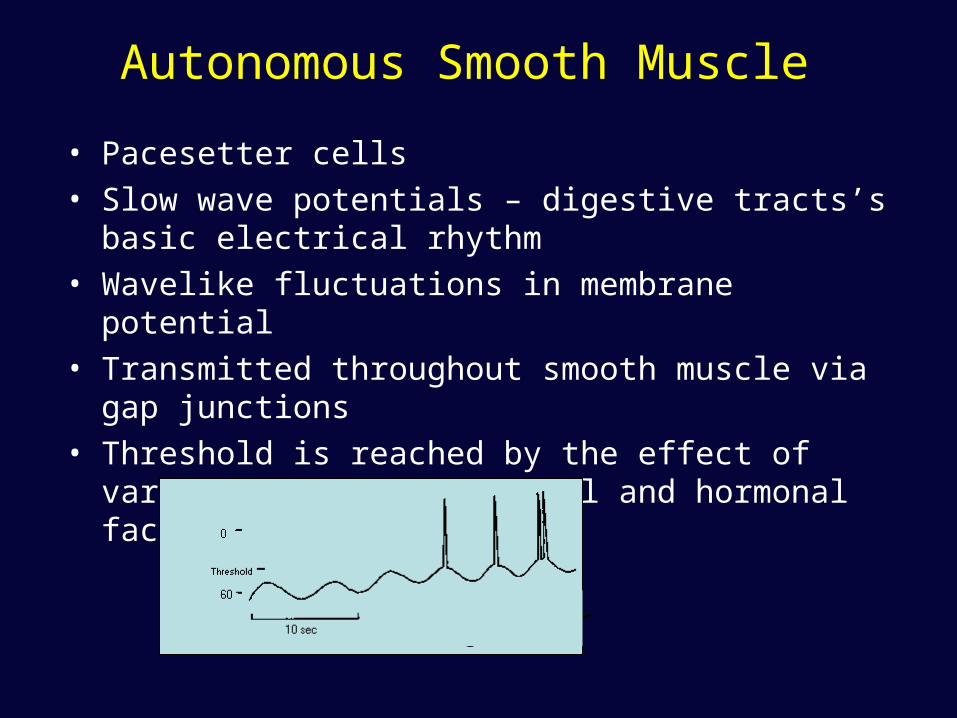
Autonomous Smooth Muscle
• Pacesetter cells• Slow wave potentials – digestive tracts’s basic electrical
rhythm • Wavelike fluctuations in membrane potential • Transmitted throughout smooth muscle via gap junctions• Threshold is reached by the effect of various
mechanical, neural and hormonal factors
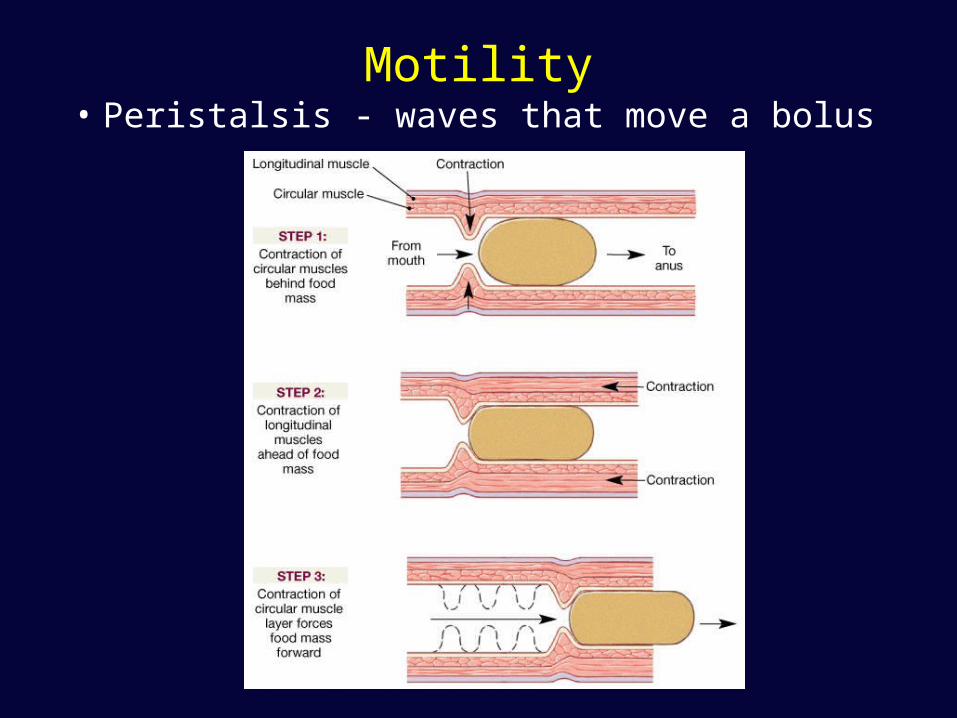
Motility• Peristalsis - waves that move a bolus
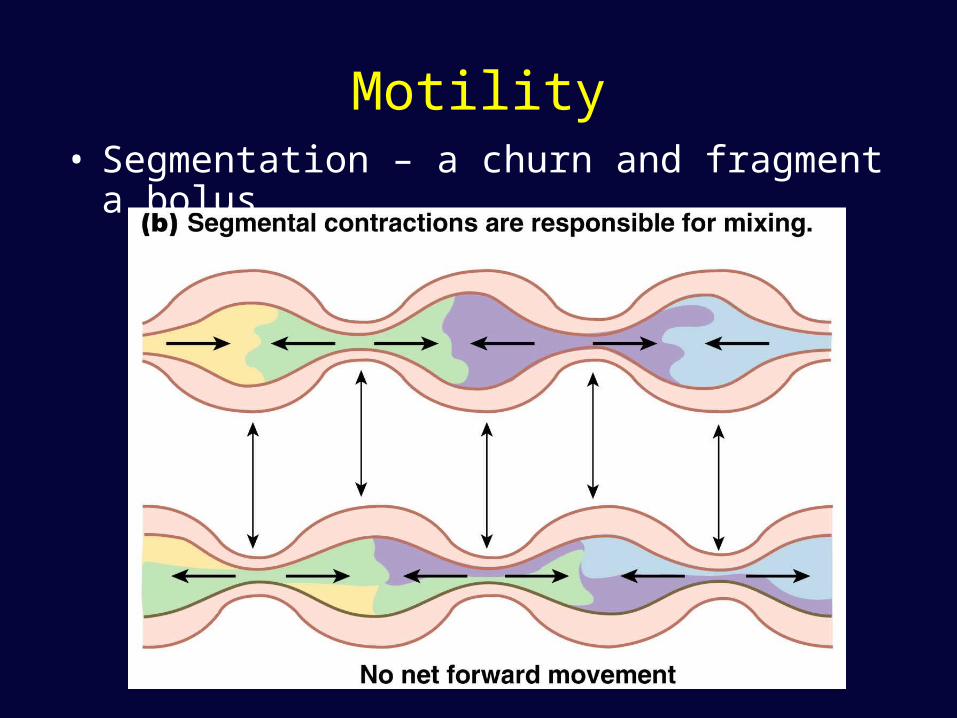
Motility• Segmentation – a churn and fragment a bolus
Ingestion and Mechanical Digestion
• Food is ingested• Mechanical digestion begins (chewing)• Propulsion is initiated by swallowing• Salivary amylase begins chemical breakdown of
starch• The pharynx and esophagus serve as conduits
to pass food from the mouth to the stomach• Uvula guards opening to pharynx
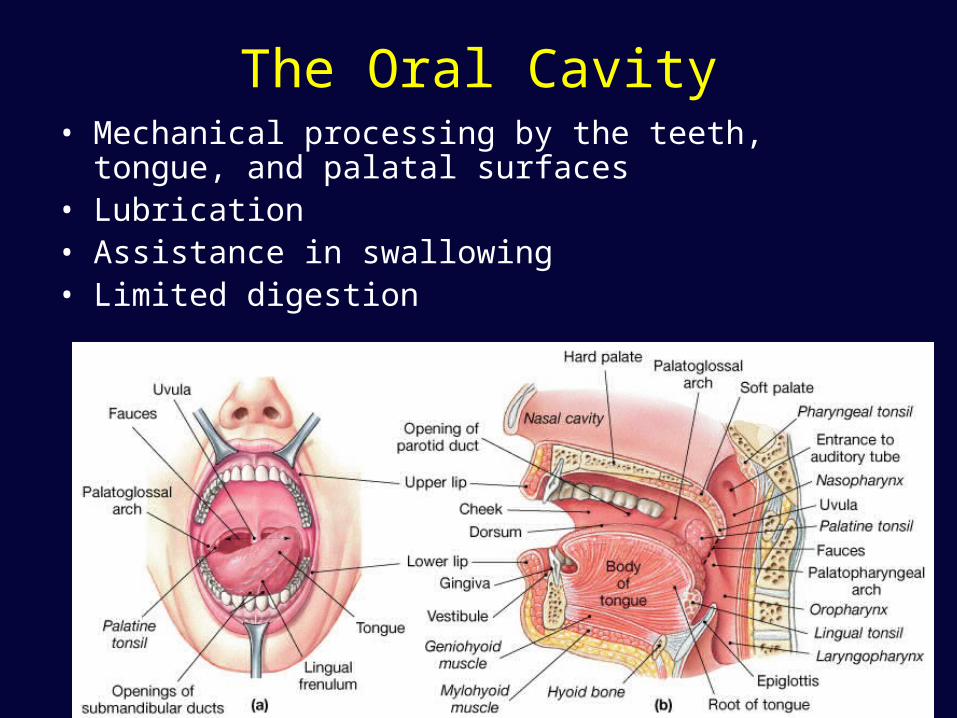
The Oral Cavity• Mechanical processing by the teeth, tongue, and palatal
surfaces• Lubrication• Assistance in swallowing• Limited digestion
Figure 24.6a, b
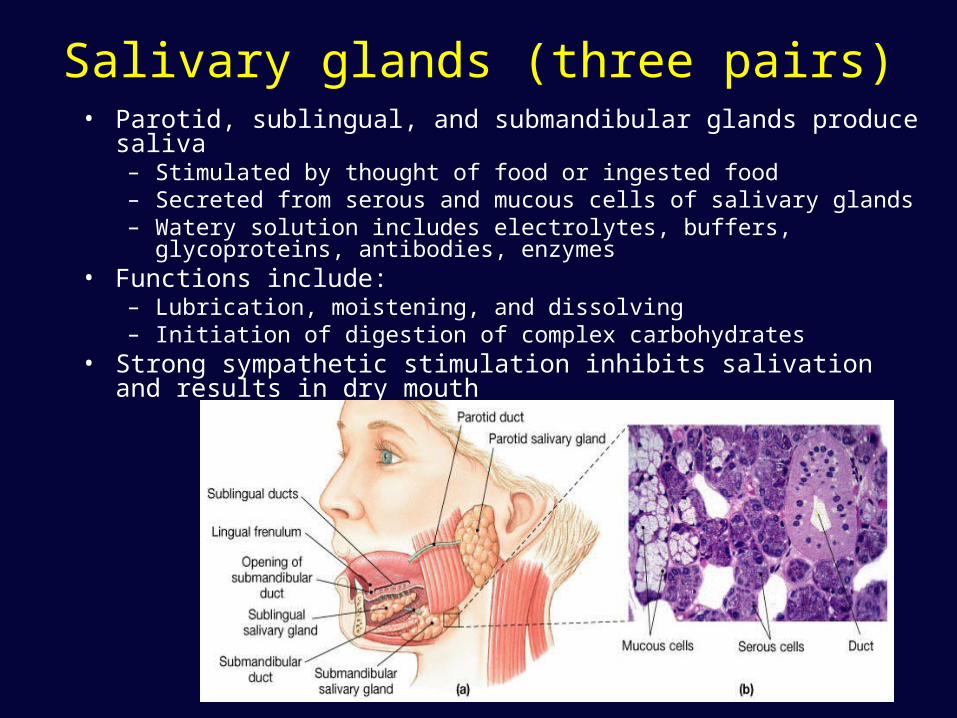
Salivary glands (three pairs)• Parotid, sublingual, and submandibular glands produce saliva
– Stimulated by thought of food or ingested food– Secreted from serous and mucous cells of salivary glands – Watery solution includes electrolytes, buffers, glycoproteins, antibodies,
enzymes • Functions include:
– Lubrication, moistening, and dissolving– Initiation of digestion of complex carbohydrates
• Strong sympathetic stimulation inhibits salivation and results in dry mouth
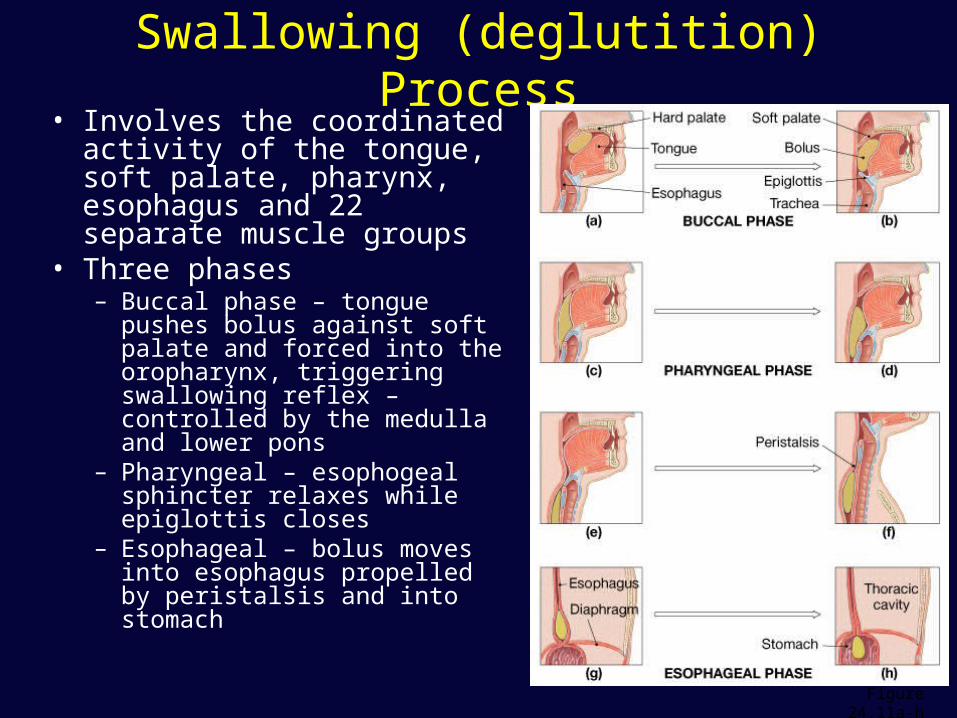
Swallowing (deglutition) Process• Involves the coordinated
activity of the tongue, soft palate, pharynx, esophagus and 22 separate muscle groups
• Three phases– Buccal phase – tongue pushes
bolus against soft palate and forced into the oropharynx, triggering swallowing reflex – controlled by the medulla and lower pons
– Pharyngeal – esophogeal sphincter relaxes while epiglottis closes
– Esophageal – bolus moves into esophagus propelled by peristalsis and into stomach
Figure 24.11a-h

Functions of the stomach
• Holds ingested food• Degrades this food both
physically and chemically• Delivers chyme to the
small intestine• Enzymatically digests
proteins with pepsin• Secretes intrinsic factor
required for absorption of vitamin B12
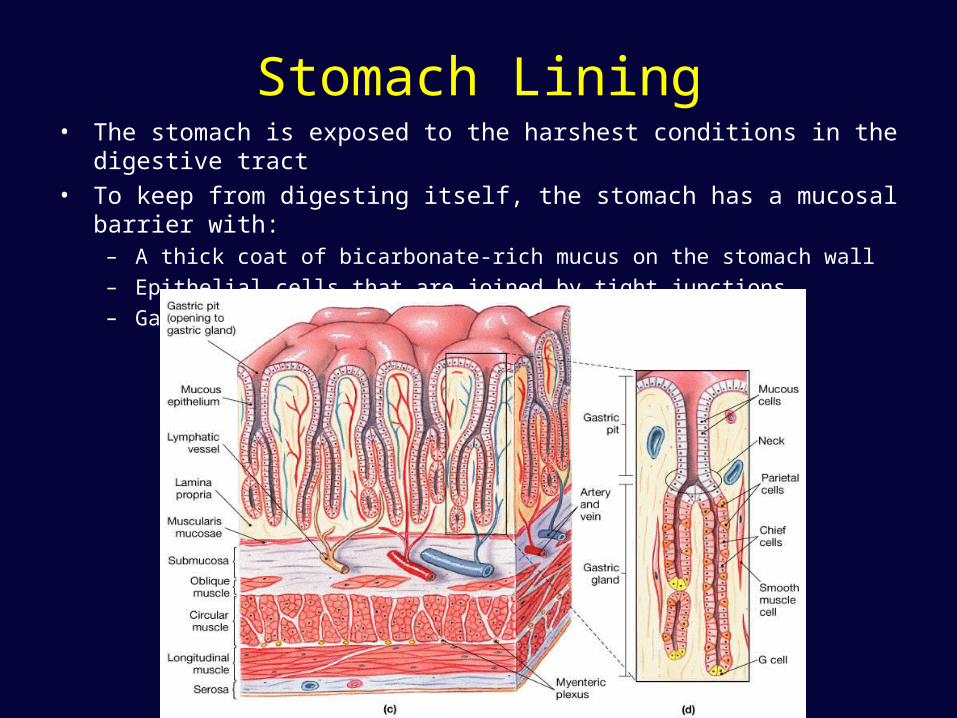
Stomach Lining• The stomach is exposed to the harshest conditions in the digestive tract
• To keep from digesting itself, the stomach has a mucosal barrier with:– A thick coat of bicarbonate-rich mucus on the stomach wall– Epithelial cells that are joined by tight junctions– Gastric glands that have cells impermeable to HCl
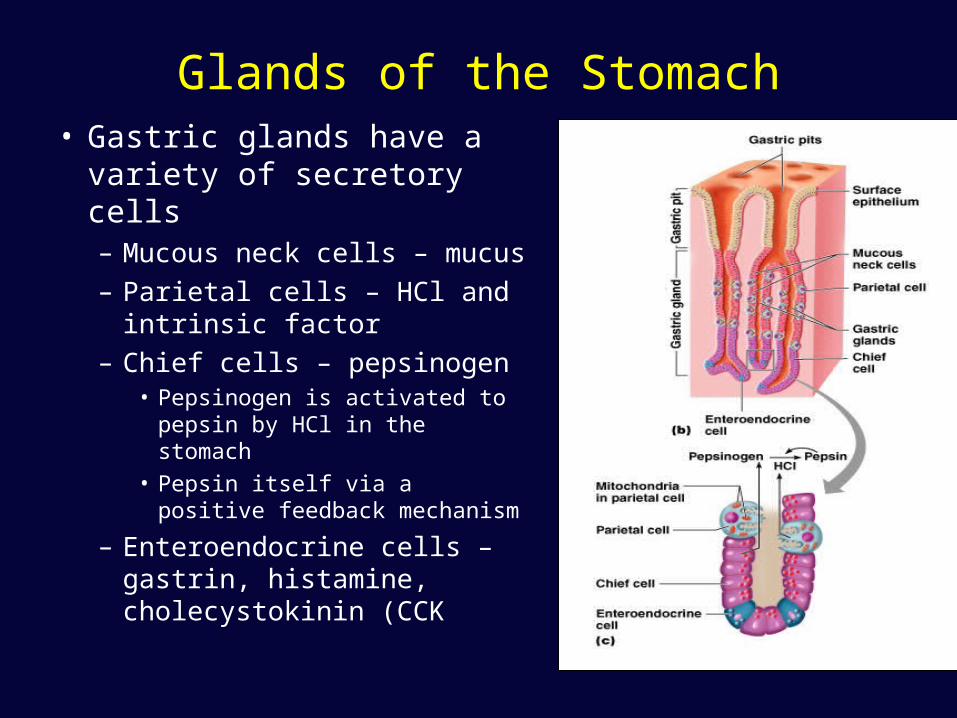
Glands of the Stomach• Gastric glands have a
variety of secretory cells– Mucous neck cells – mucus– Parietal cells – HCl and
intrinsic factor– Chief cells – pepsinogen
• Pepsinogen is activated to pepsin by HCl in the stomach
• Pepsin itself via a positive feedback mechanism
– Enteroendocrine cells – gastrin, histamine, cholecystokinin (CCK

Regulation of Gastric Secretion• Neural and hormonal mechanisms
regulate the release of gastric juice
• Stimulatory and inhibitory events occur in three phases– Cephalic (reflex) phase: prior to food entry– Gastric phase: once food enters the stomach– Intestinal phase: as partially digested food
enters the duodenum
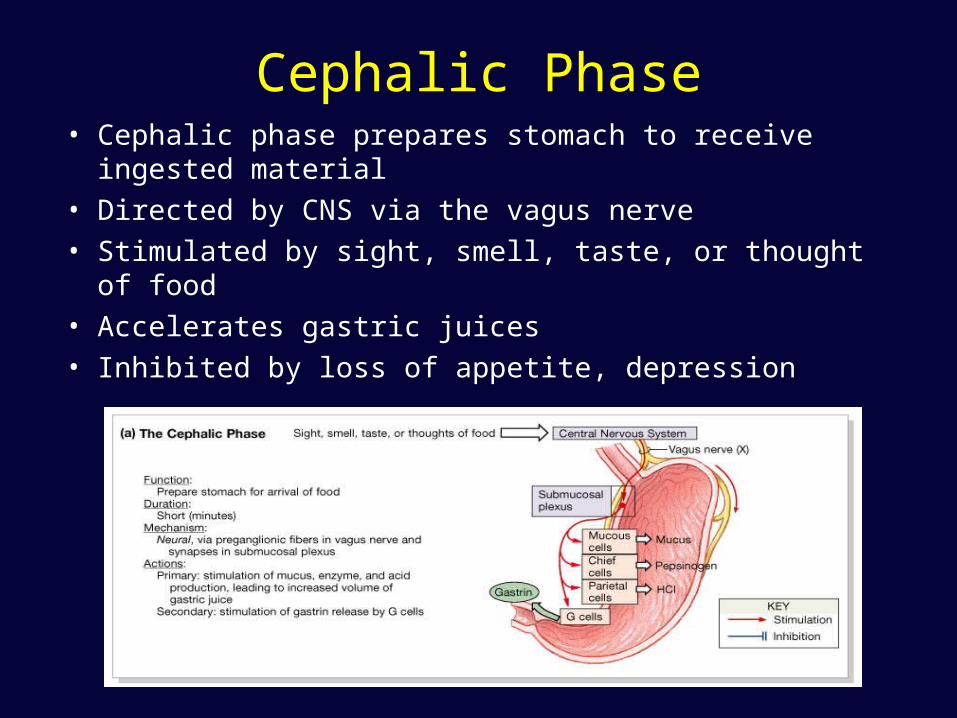
Cephalic Phase• Cephalic phase prepares stomach to receive ingested
material• Directed by CNS via the vagus nerve• Stimulated by sight, smell, taste, or thought of food• Accelerates gastric juices• Inhibited by loss of appetite, depression
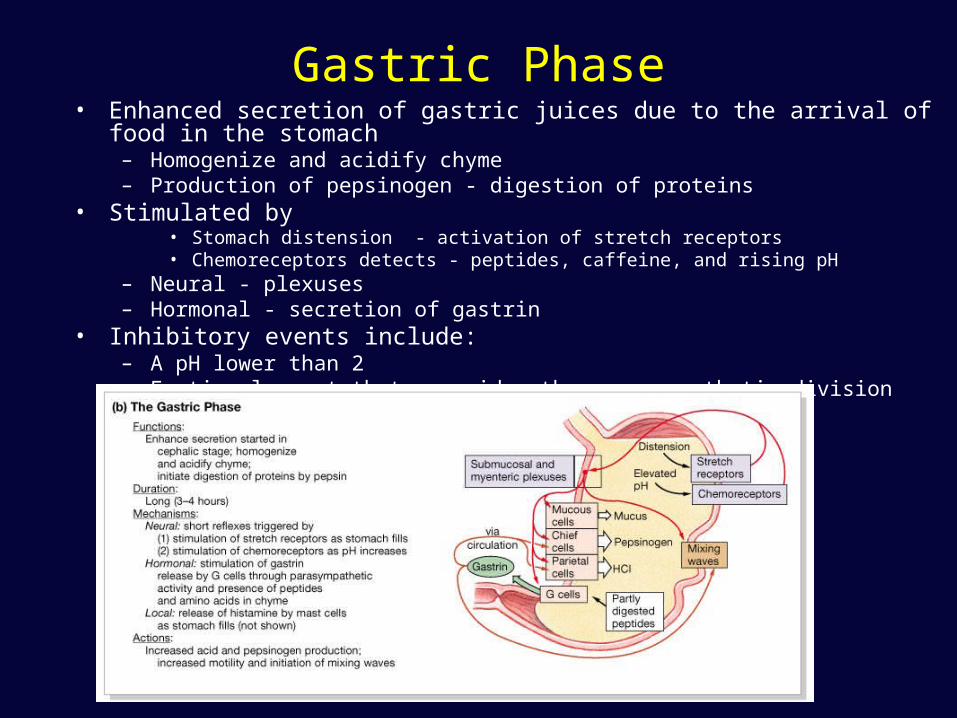
Gastric Phase• Enhanced secretion of gastric juices due to the arrival of food in the stomach
– Homogenize and acidify chyme – Production of pepsinogen - digestion of proteins
• Stimulated by • Stomach distension - activation of stretch receptors • Chemoreceptors detects - peptides, caffeine, and rising pH
– Neural - plexuses– Hormonal - secretion of gastrin
• Inhibitory events include:– A pH lower than 2 – Emotional upset that overrides the parasympathetic division
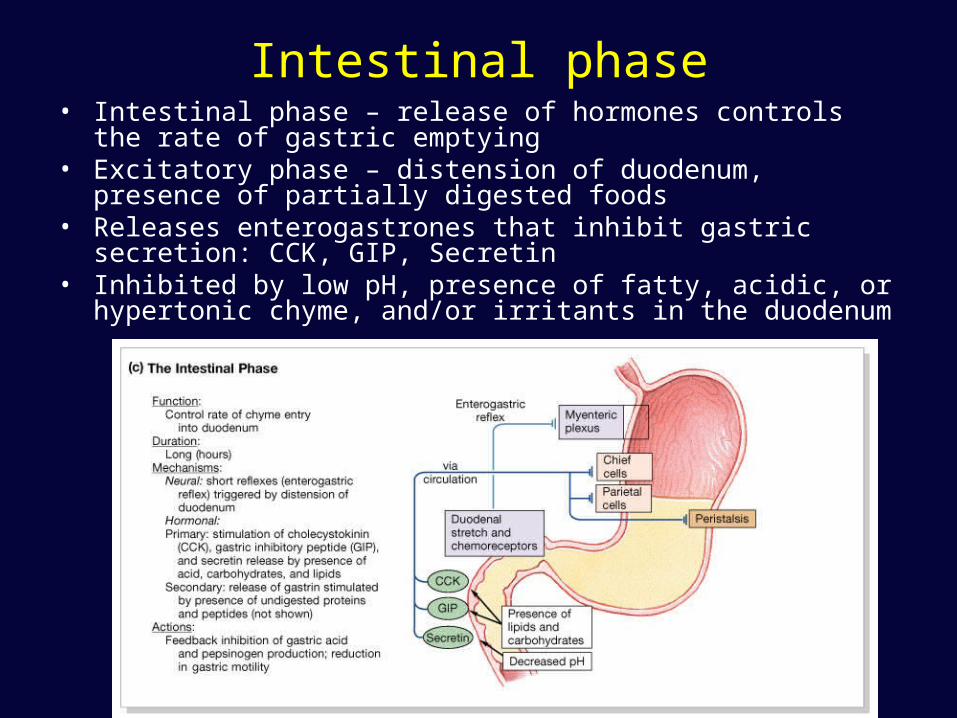
Intestinal phase• Intestinal phase – release of hormones controls the rate of gastric
emptying • Excitatory phase – distension of duodenum, presence of partially
digested foods • Releases enterogastrones that inhibit gastric secretion: CCK, GIP,
Secretin • Inhibited by low pH, presence of fatty, acidic, or hypertonic chyme,
and/or irritants in the duodenum
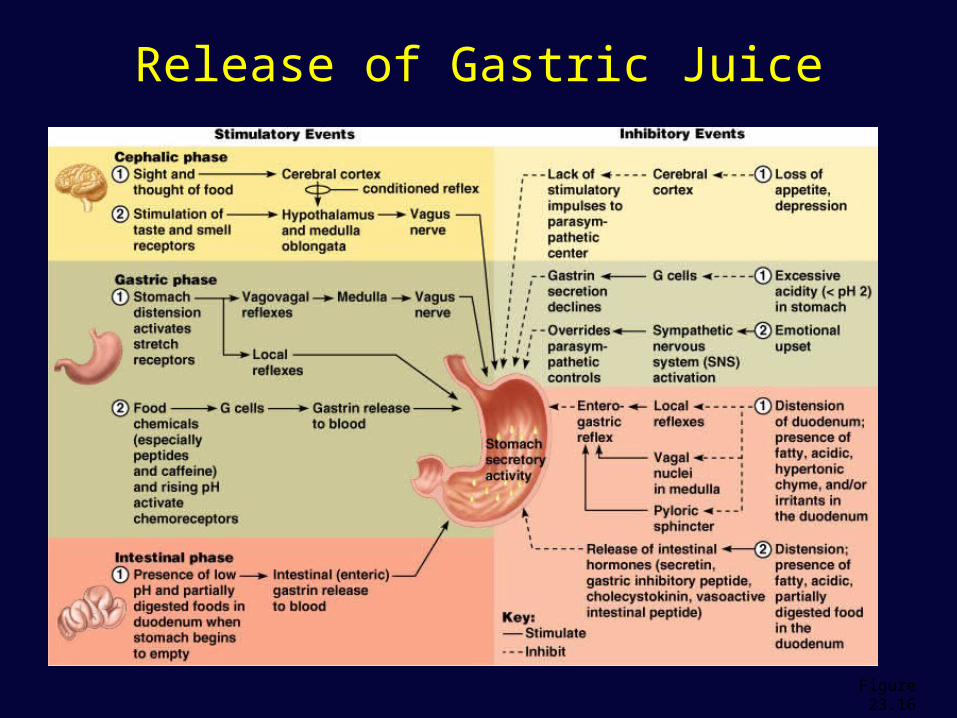
Release of Gastric Juice
Figure 23.16

Regulation of HCl Secretion
• HCl secretion is stimulated by ACh, histamine, and gastrin through second-messenger systems
• Release of hydrochloric acid:– Is low if only one ligand binds to
parietal cells– Is high if all three ligands bind to
parietal cells
• Antihistamines block H2 receptors and decrease HCl release
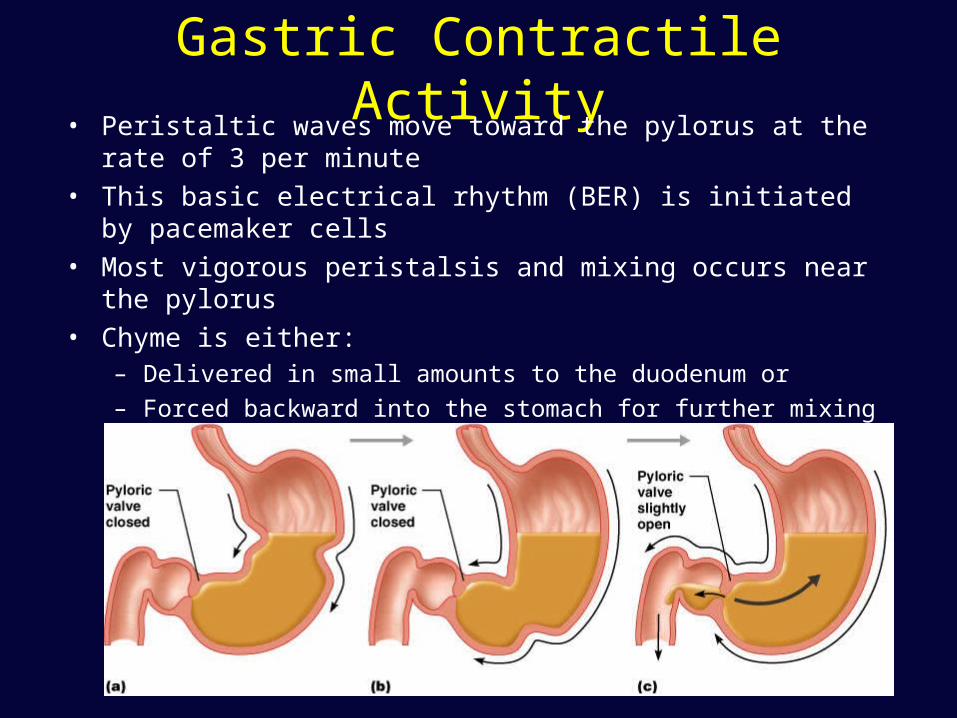
Gastric Contractile Activity• Peristaltic waves move toward the pylorus at the rate of 3 per
minute• This basic electrical rhythm (BER) is initiated by pacemaker cells • Most vigorous peristalsis and mixing occurs near the pylorus• Chyme is either:
– Delivered in small amounts to the duodenum or
– Forced backward into the stomach for further mixing
Regulation of Gastric Emptying• Gastric emptying is regulated by:
– The neural enterogastric reflex– Hormonal (enterogastrone) mechanisms
• These mechanisms inhibit gastric secretion and duodenal filling
• Carbohydrate-rich chyme quickly moves through the duodenum
• Fat-laden chyme is digested more slowly causing food to remain in the stomach longer
Gastrointestinal Hormones• Gastrin
– Release is stimulated by presence of protein in stomach
– Secretion inhibited by accumulation of acid in stomach
• Acts in several ways to increase secretion of HCl and pepsinogen
• Enhances gastric motility, stimulates ileal motility, relaxes ileocecal sphincter, induces mass movements in colon
• Helps maintain well-developed, functionally viable digestive tract lining
Gastrointestinal Hormones• Secretin
– Presence of acid in duodenum stimulates release– Inhibits gastric emptying in order to prevent further acid
from entering duodenum until acid already present is neutralized
– Inhibits gastric secretion to reduce amount of acid being produced
– Stimulates pancreatic duct cells to produce large volume of aqueous NaHCO3 secretion
– Stimulates liver to secrete NaCO3 rich bile which assists in neutralization process
– Along with CCK, is trophic to exocrine pancreas

Gastrointestinal Hormones• CCK
– Inhibits gastric motility and secretion– Stimulates pancreatic acinar cells to increase secretion of
pancreatic enzymes– Causes contraction of gallbladder – Along with secretin, is trophic to exocrine pancreas– Implicated in long-term adaptive changes in proportion of
pancreatic enzymes in response to prolonged diet changes– Important regulator of food intake
• GIP– Glucose-dependent insulinotrophic peptide– Stimulates insulin release by pancreas
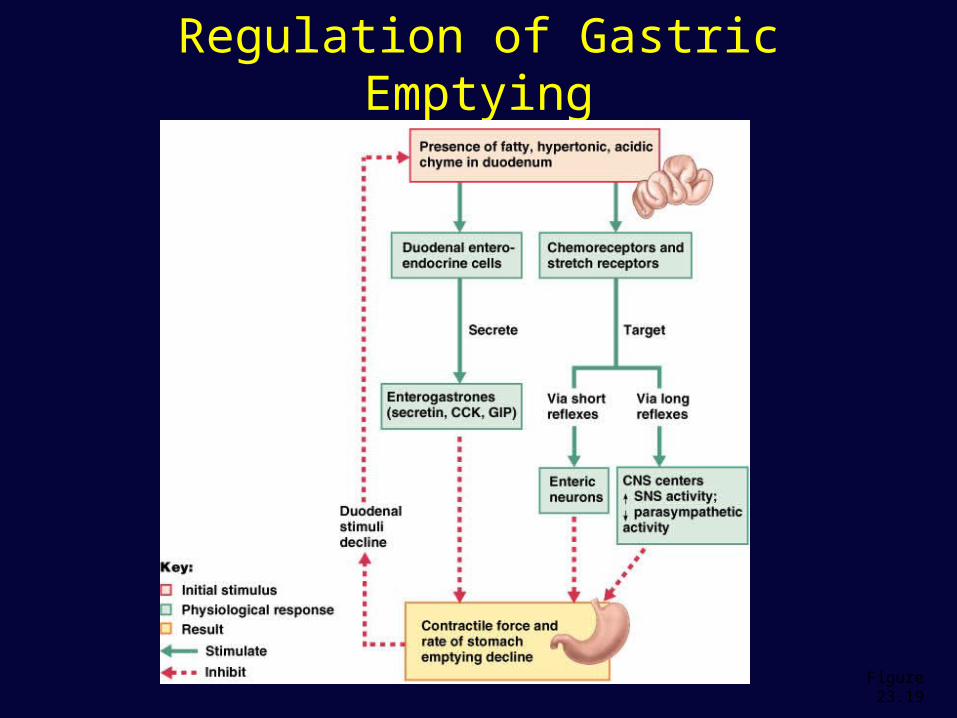
Regulation of Gastric Emptying
Figure 23.19
Digestion And Absorption In The Stomach
• Preliminary digestion of proteins - pepsin
• Permits digestion of carbohydrates
• Very little absorption of nutrients – Some drugs, however, are absorbed
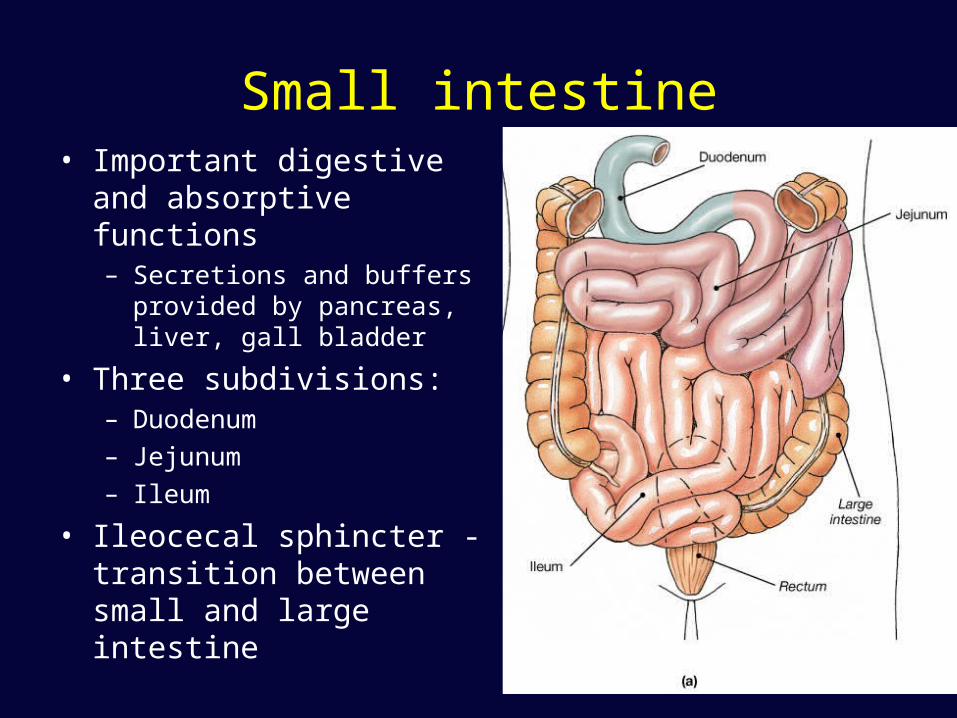
Small intestine• Important digestive and
absorptive functions– Secretions and buffers
provided by pancreas, liver, gall bladder
• Three subdivisions:– Duodenum – Jejunum – Ileum
• Ileocecal sphincter - transition between small and large intestine
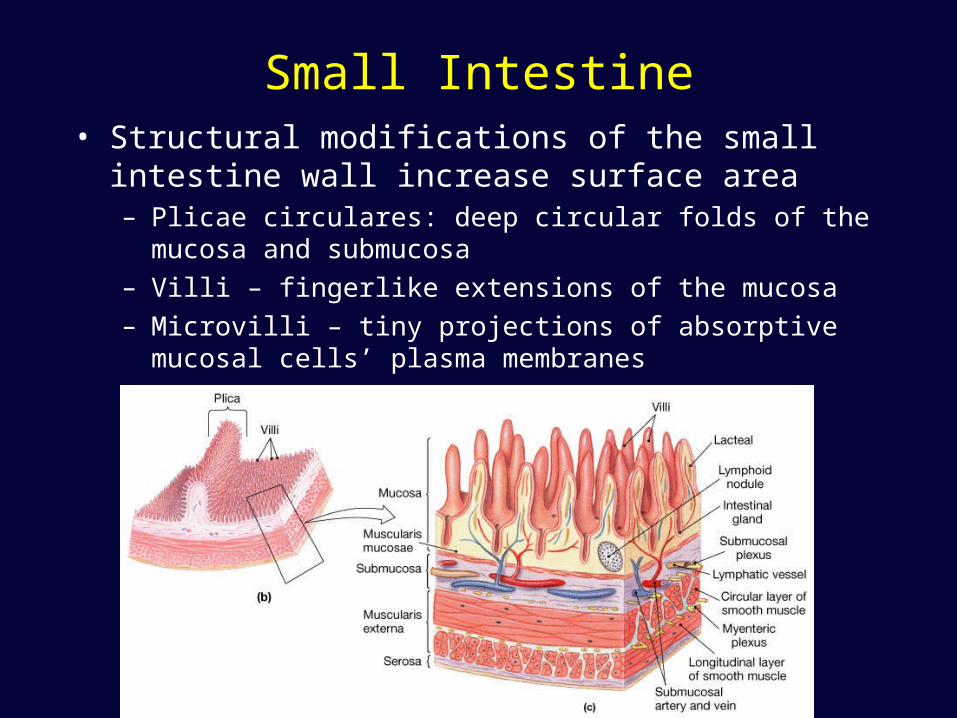
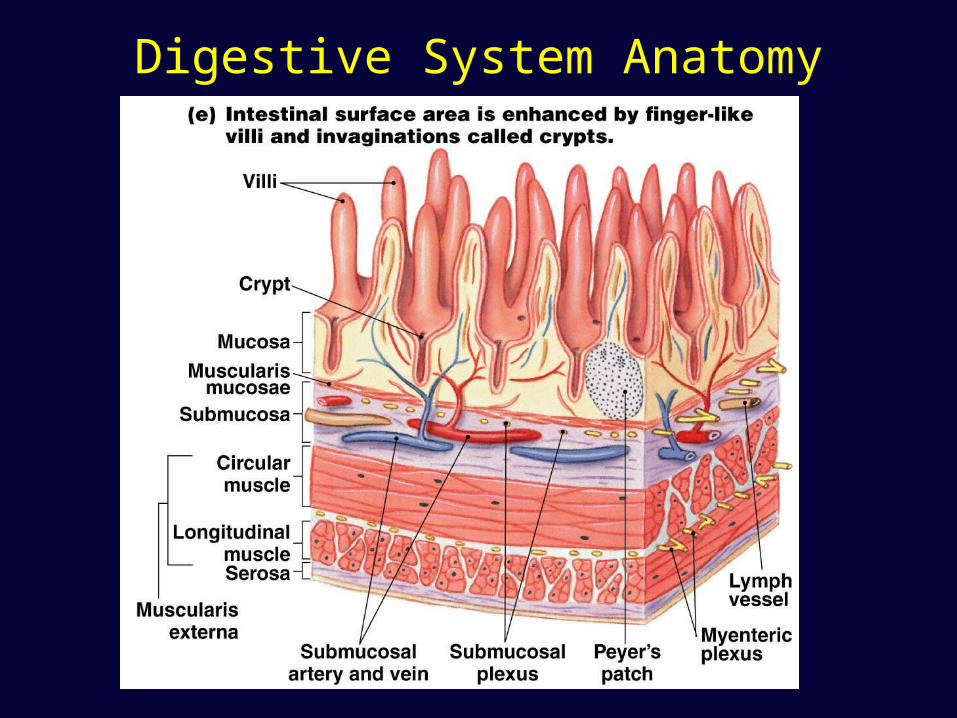
Small Intestine• Structural modifications of the small intestine wall
increase surface area– Plicae circulares: deep circular folds of the mucosa and
submucosa– Villi – fingerlike extensions of the mucosa– Microvilli – tiny projections of absorptive mucosal cells’
plasma membranes
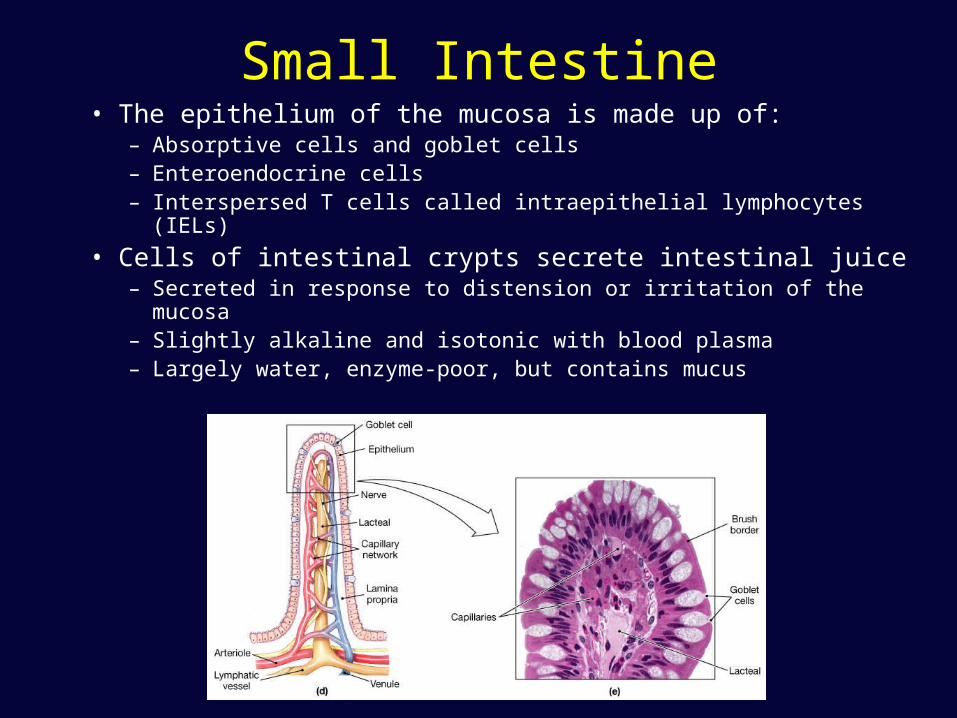
Small Intestine• The epithelium of the mucosa is made up of:
– Absorptive cells and goblet cells – Enteroendocrine cells – Interspersed T cells called intraepithelial lymphocytes (IELs)
• Cells of intestinal crypts secrete intestinal juice– Secreted in response to distension or irritation of the mucosa– Slightly alkaline and isotonic with blood plasma– Largely water, enzyme-poor, but contains mucus

Small Intestine
• Glands of the duodenum– Moisten chyme– Help buffer acids– Maintain digestive material in solution
• Hormones– Secretin - produces alkaline buffers, increase bile by
liver and pancreas – Cholecystokinin – increase pancreatic enzymes,
stimulates contraction of gall bladder, reduces hunger sensation
– GIP – stimulates release of insulin, inhibits gastric secretion and motility
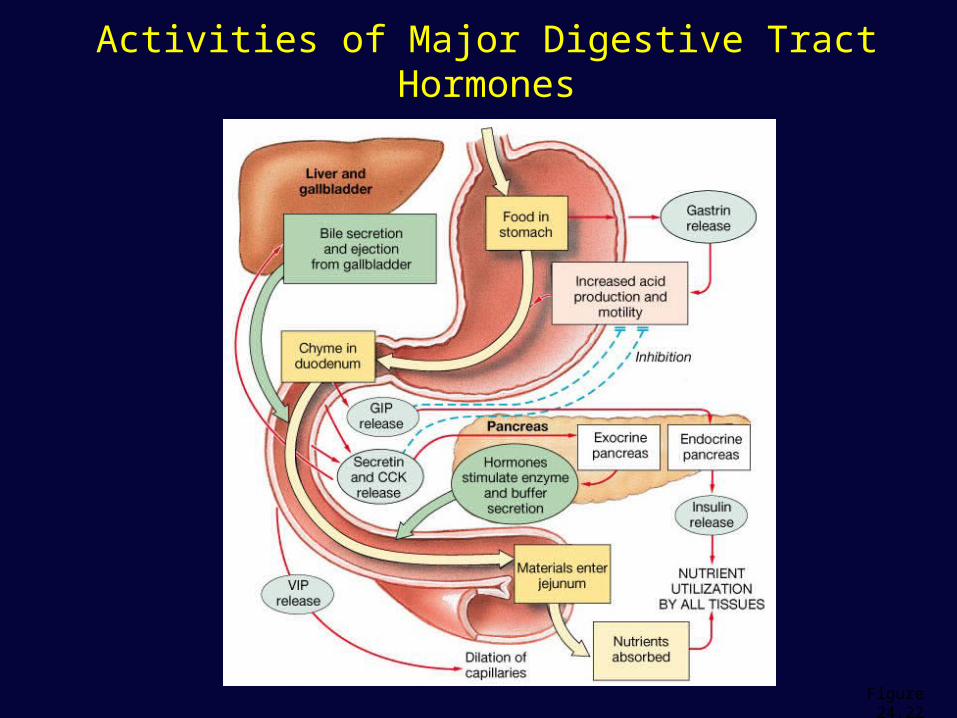
Activities of Major Digestive Tract Hormones
Figure 24.22
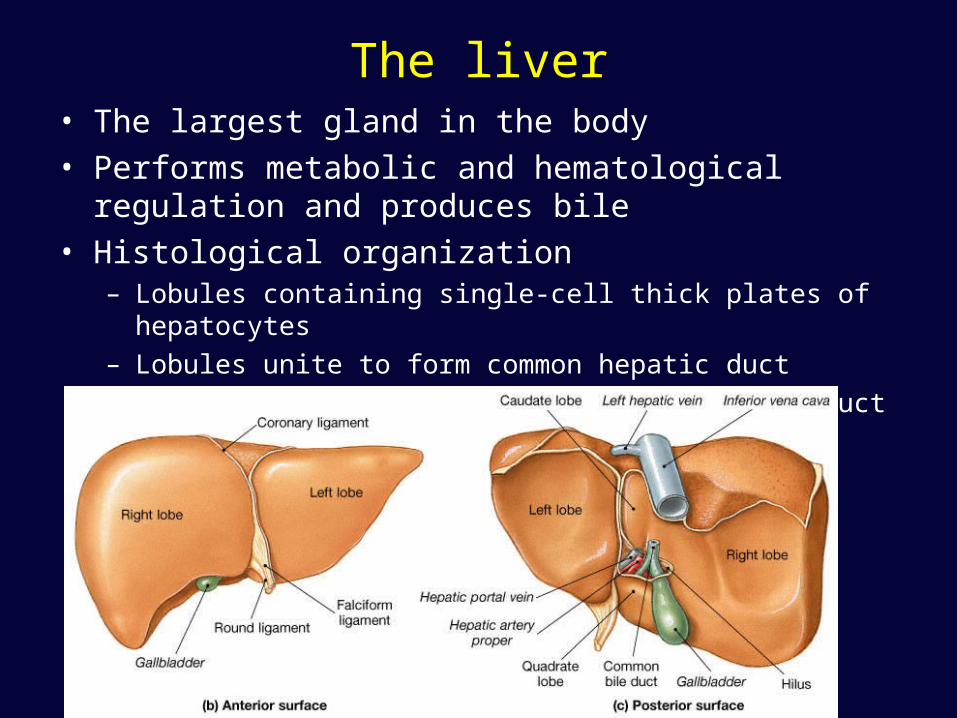
The liver• The largest gland in the body• Performs metabolic and hematological regulation and
produces bile• Histological organization
– Lobules containing single-cell thick plates of hepatocytes– Lobules unite to form common hepatic duct– Duct meets cystic duct to form common bile duct
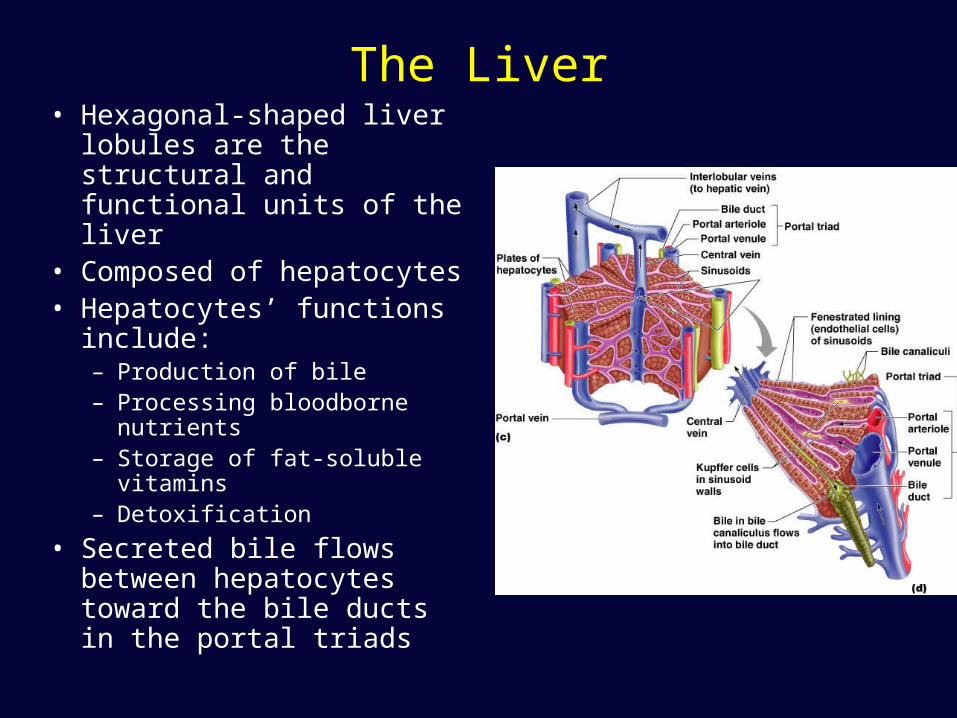
The Liver• Hexagonal-shaped liver
lobules are the structural and functional units of the liver
• Composed of hepatocytes• Hepatocytes’ functions
include:– Production of bile– Processing bloodborne
nutrients– Storage of fat-soluble vitamins– Detoxification
• Secreted bile flows between hepatocytes toward the bile ducts in the portal triads

Composition of Bile• A yellow-green, alkaline solution containing bile
salts, bile pigments, cholesterol, neutral fats, phospholipids, and electrolytes
• Bile salts are cholesterol derivatives that:– Emulsify fat– Facilitate fat and cholesterol absorption– Help solubilize cholesterol
• Enterohepatic circulation recycles bile salts • The chief bile pigment is bilirubin, a waste
product of heme
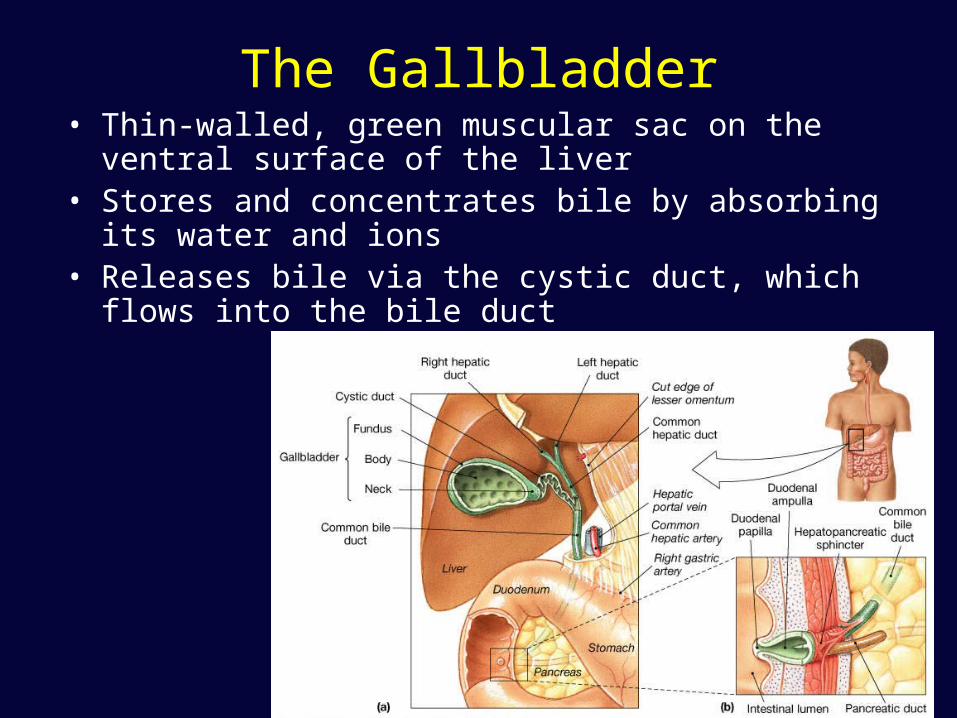
The Gallbladder• Thin-walled, green muscular sac on the ventral surface
of the liver• Stores and concentrates bile by absorbing its water and
ions• Releases bile via the cystic duct, which flows into the
bile duct

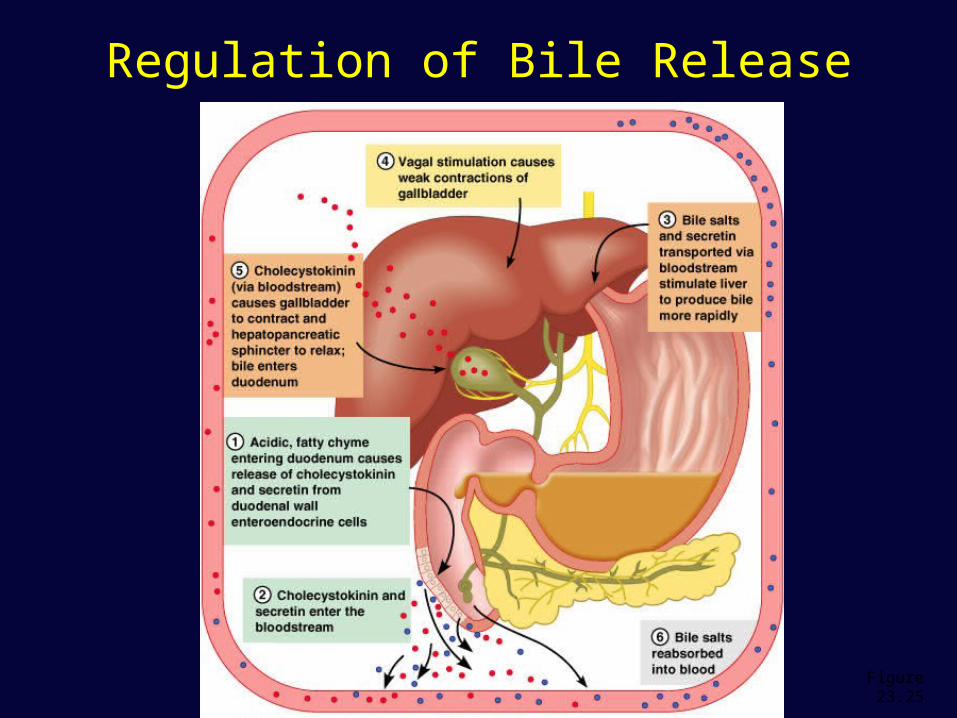
Regulation of Bile Release• Acidic, fatty chyme causes the duodenum to
release:– Cholecystokinin (CCK) and secretin into the
bloodstream• Bile salts and secretin transported in blood
stimulate the liver to produce bile• Vagal stimulation causes weak contractions of
the gallbladder• Cholecystokinin causes:
– The gallbladder to contract– The hepatopancreatic sphincter to relax
• As a result, bile enters the duodenum
Regulation of Bile Release
Figure 23.25
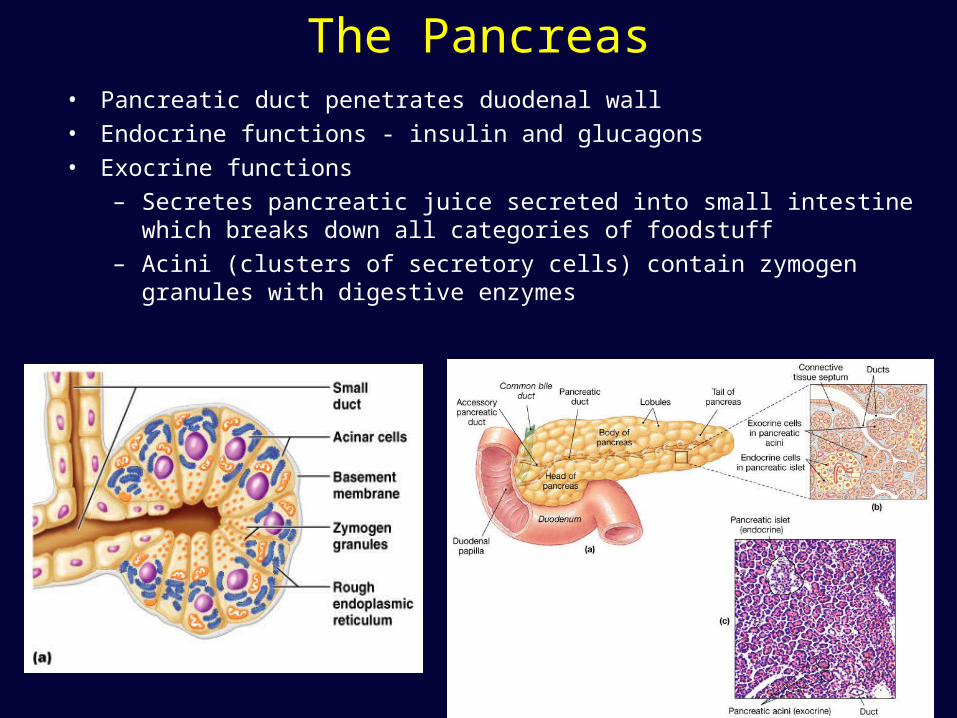
The Pancreas• Pancreatic duct penetrates duodenal wall
• Endocrine functions - insulin and glucagons
• Exocrine functions
– Secretes pancreatic juice secreted into small intestine which breaks down all categories of foodstuff
– Acini (clusters of secretory cells) contain zymogen granules with digestive enzymes
Composition of Pancreatic Juice
• Water solution of enzymes and electrolytes (primarily HCO3–)– Neutralizes acid chyme– Provides optimal environment for pancreatic enzymes
• Enzymes are released in inactive form and activated in the duodenum
• Examples include– Trypsinogen is activated to trypsin– Procarboxypeptidase is activated to carboxypeptidase
• Active enzymes secreted– Amylase, lipases, and nucleases – These enzymes require ions or bile for optimal activity
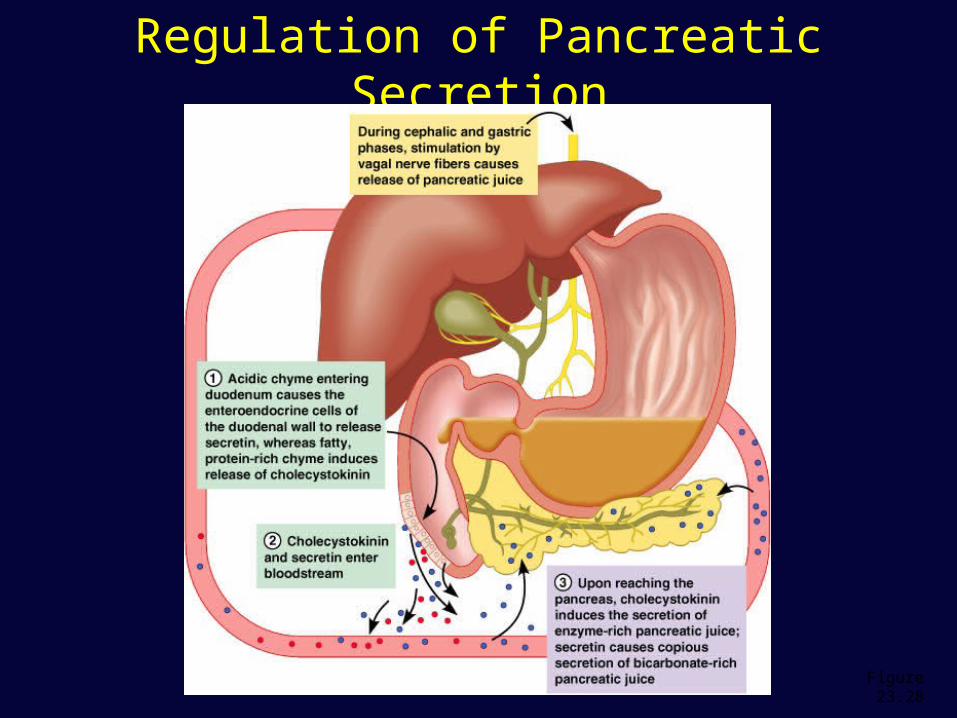
Regulation of Pancreatic Secretion• Secretin and CCK are released when fatty or
acidic chyme enters the duodenum• CCK and secretin enter the bloodstream• Upon reaching the pancreas:
– CCK induces the secretion of enzyme-rich pancreatic juice
– Secretin causes secretion of bicarbonate-rich pancreatic juice
• Vagal stimulation also causes release of pancreatic juice
Regulation of Pancreatic Secretion
Figure 23.28
Digestion in the Small Intestine
• As chyme enters the duodenum: – Carbohydrates and proteins are only partially digested– No fat digestion has taken place
• Digestion continues in the small intestine– Chyme is released slowly into the duodenum – Because it is hypertonic and has low pH, mixing is
required for proper digestion– Required substances needed are supplied by the liver – Virtually all nutrient absorption takes place in the
small intestine
Motility in the Small Intestine
• The most common motion of the small intestine is segmentation– It is initiated by intrinsic pacemaker cells (Cajal cells)– Moves contents steadily toward the ileocecal valve
• After nutrients have been absorbed:– Peristalsis begins with each wave starting distal to the
previous – Meal remnants, bacteria, mucosal cells, and debris
are moved into the large intestine
Control of Motility
• Local enteric neurons of the GI tract coordinate intestinal motility
• Cholinergic neurons cause:– Contraction and shortening of the circular muscle
layer– Shortening of longitudinal muscle– Distension of the intestine
• Other impulses relax the circular muscle• The gastroileal reflex and gastrin:
– Relax the ileocecal sphincter– Allow chyme to pass into the large intestine
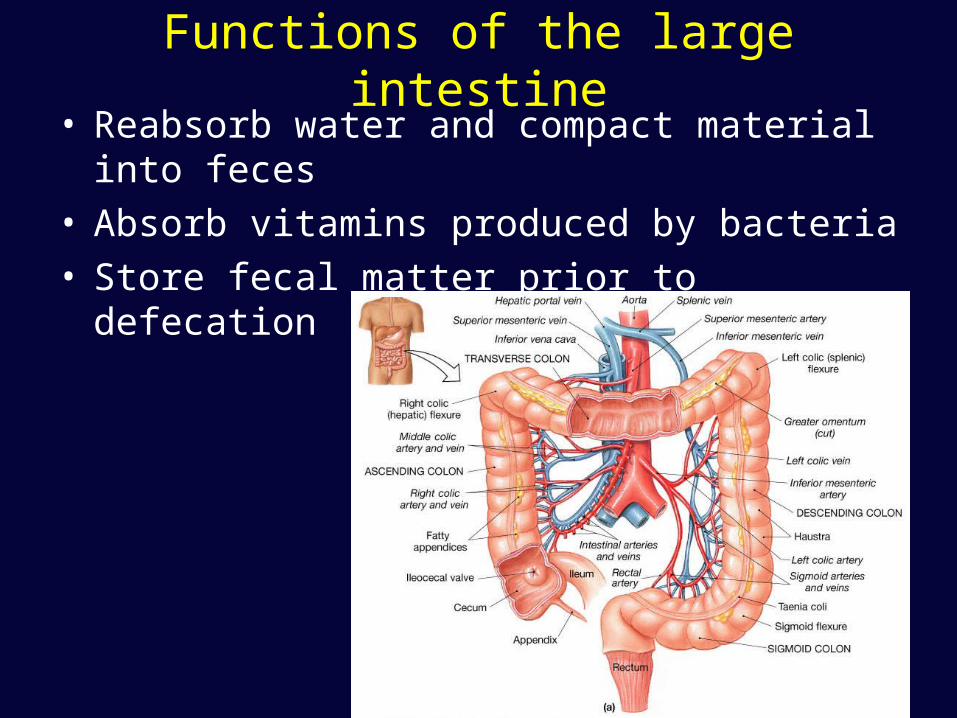
Functions of the large intestine• Reabsorb water and compact material into feces• Absorb vitamins produced by bacteria• Store fecal matter prior to defecation
Functions of the Large Intestine
• Other than digestion of enteric bacteria, no further digestion takes place
• Vitamins, water, and electrolytes are reclaimed
• Its major function is propulsion of fecal material toward the anus
• Though essential for comfort, the colon is not essential for life

Motility of the Large Intestine
• Haustral contractions– Slow segmenting movements that move the
contents of the colon– Haustra sequentially contract as they are
stimulated by distension
• Presence of food in the stomach:– Activates the gastrocolic reflex– Initiates peristalsis that forces contents toward
the rectum
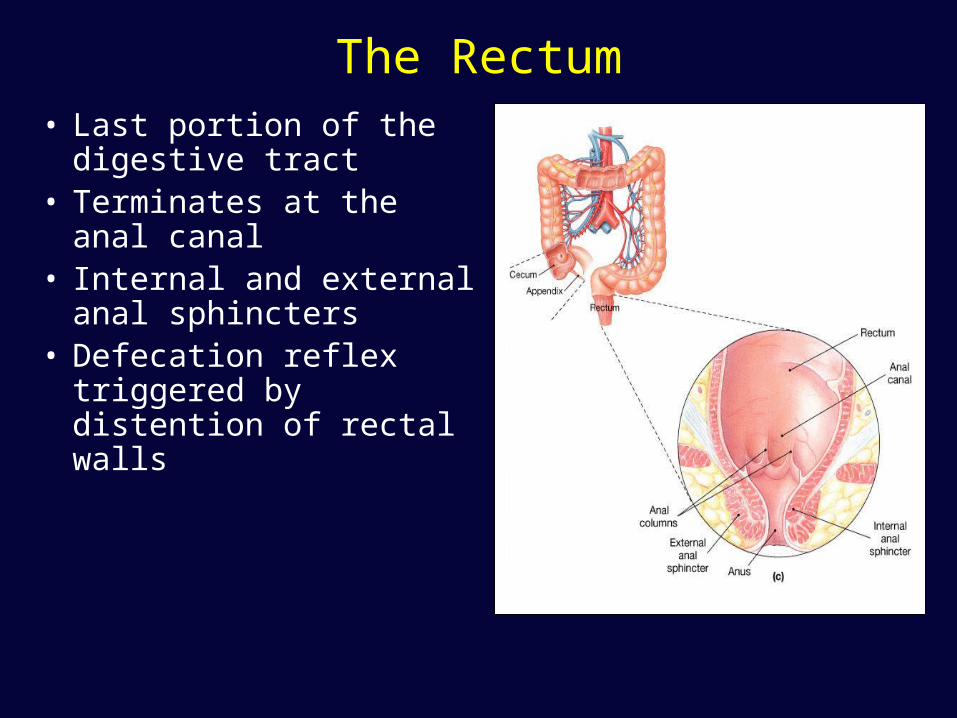
The Rectum• Last portion of the
digestive tract• Terminates at the anal
canal• Internal and external
anal sphincters• Defecation reflex
triggered by distention of rectal walls
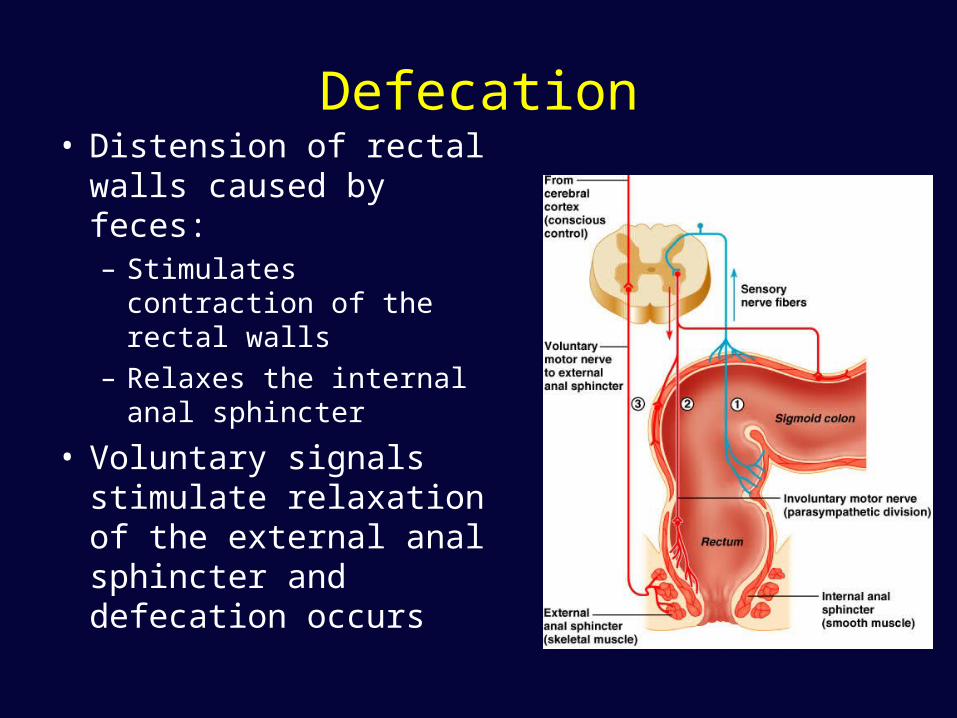
Defecation• Distension of rectal
walls caused by feces:– Stimulates contraction of
the rectal walls– Relaxes the internal anal
sphincter
• Voluntary signals stimulate relaxation of the external anal sphincter and defecation occurs
Regulation of digestion
• Intrinsic control by local centers– Autonomous smooth muscle pacesetter
cells– Intrinsic nerve plexuses and sensory
receptors
• Extrinsic control– ANS– GI hormones
Regulation of digestion
• Mechano- and chemoreceptors respond to:– Stretch, osmolarity, and pH– Presence of substrate, and end products of
digestion
• They initiate reflexes that:– Activate or inhibit digestive glands – Mix lumen contents and move them along
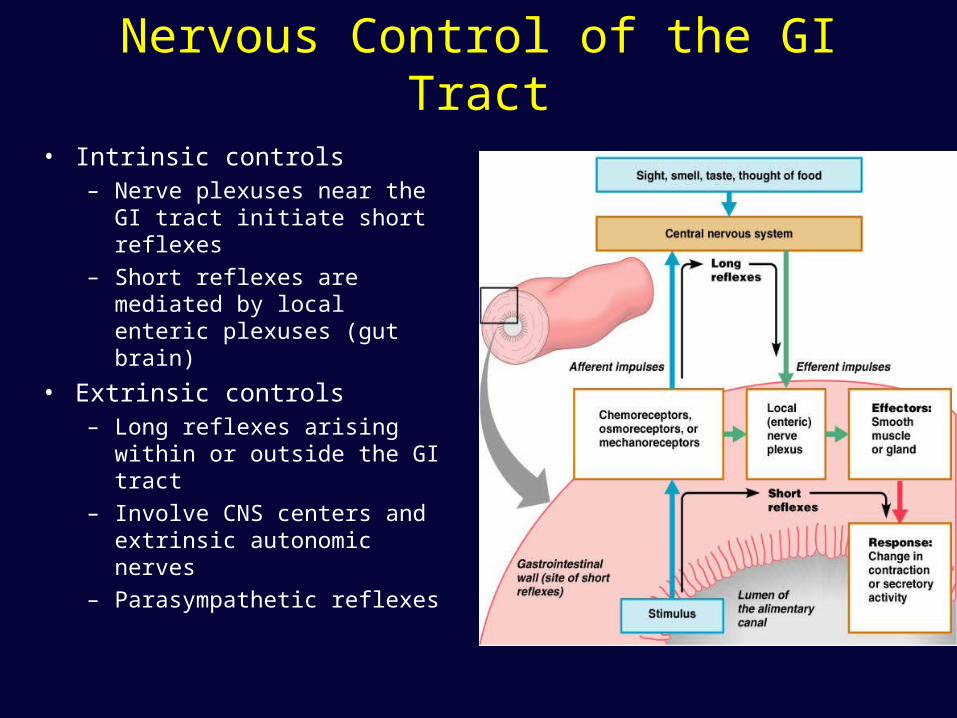
Nervous Control of the GI Tract
• Intrinsic controls– Nerve plexuses near the GI
tract initiate short reflexes
– Short reflexes are mediated by local enteric plexuses (gut brain)
• Extrinsic controls– Long reflexes arising within or
outside the GI tract
– Involve CNS centers and extrinsic autonomic nerves
– Parasympathetic reflexes
Enteric Nervous System• Composed of two major intrinsic nerve plexuses
– Submucosal nerve plexus – regulates glands and smooth muscle in the mucosa
– Myenteric nerve plexus – Major nerve supply that controls GI tract mobility
• Segmentation and peristalsis are largely automatic involving local reflex arcs
• Linked to the CNS via long autonomic reflex arc
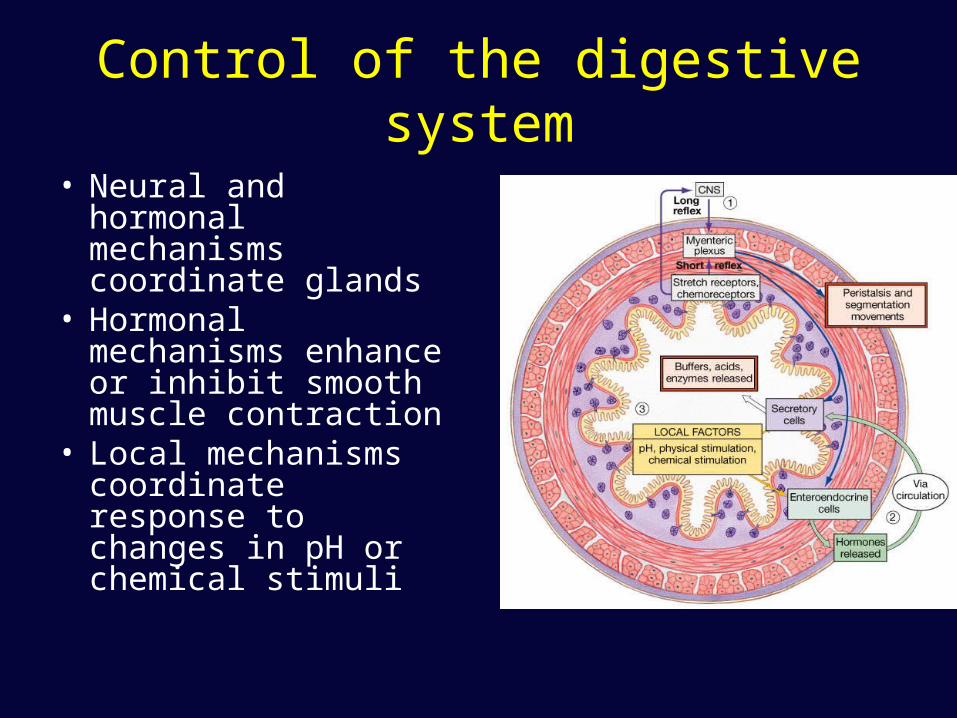
Control of the digestive system
• Neural and hormonal mechanisms coordinate glands
• Hormonal mechanisms enhance or inhibit smooth muscle contraction
• Local mechanisms coordinate response to changes in pH or chemical stimuli
Digestion And Absorption Of Nutrients
• Disassembling organic food into smaller fragments
• Hydrolyzing carbohydrates, proteins, lipids and nucleic acids for absorption
Chemical Digestion: Carbohydrates
• Begins in the mouth – Salivary and pancreatic enzymes catabolize into disaccharides
and trisaccharides– Brush border enzymes catabolize into monosaccharides
• Absorption of monosaccharides occurs across the intestinal epithelia
• Absorption: via cotransport with Na+, and facilitated diffusion– Enter the capillary bed in the villi– Transported to the liver via the hepatic portal vein
• Enzymes used: salivary amylase, pancreatic amylase, and brush border enzymes
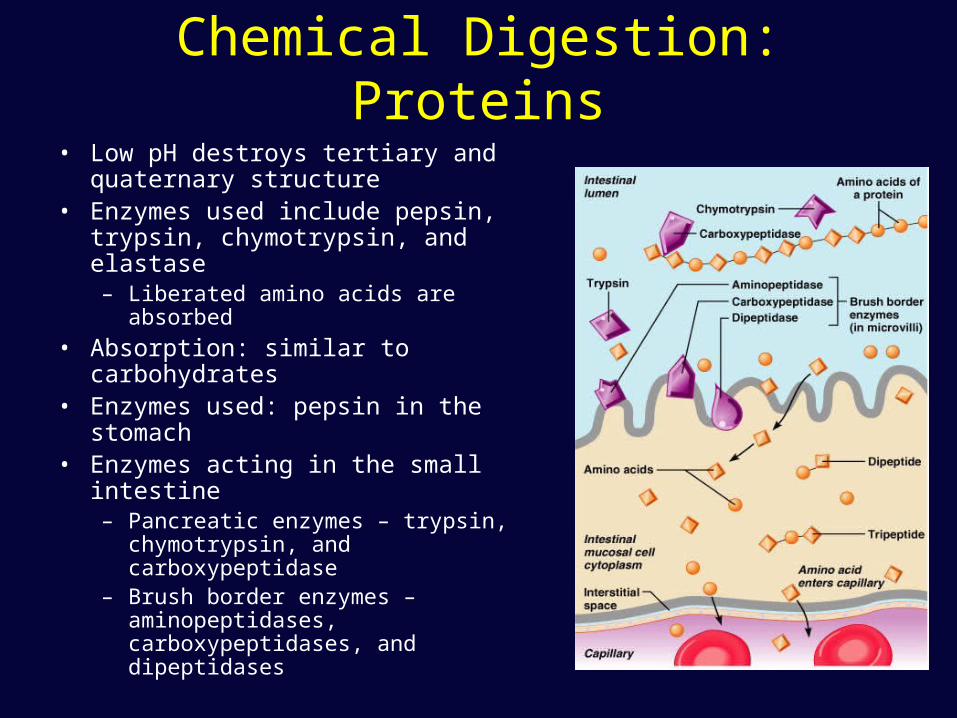
Chemical Digestion: Proteins
• Low pH destroys tertiary and quaternary structure
• Enzymes used include pepsin, trypsin, chymotrypsin, and elastase– Liberated amino acids are absorbed
• Absorption: similar to carbohydrates• Enzymes used: pepsin in the
stomach• Enzymes acting in the small
intestine– Pancreatic enzymes – trypsin,
chymotrypsin, and carboxypeptidase– Brush border enzymes –
aminopeptidases, carboxypeptidases, and dipeptidases
Lipid digestion and absorption
• Lipid digestion utilizes lingual and pancreatic lipases– Bile salts improve chemical digestion by
emulsifying lipid drops– Lipid-bile salt complexes called micelles are
formed– Micelles diffuse into intestinal epithelia which
release lipids into the blood as chylomicrons
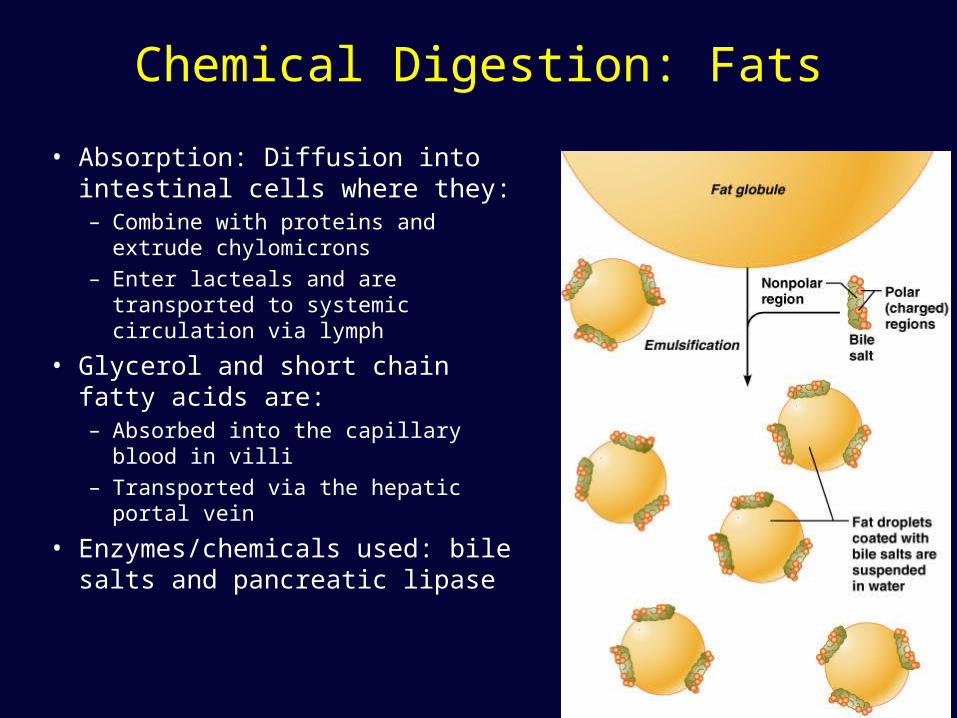
Chemical Digestion: Fats
• Absorption: Diffusion into intestinal cells where they:– Combine with proteins and extrude
chylomicrons– Enter lacteals and are transported to
systemic circulation via lymph
• Glycerol and short chain fatty acids are:– Absorbed into the capillary blood in
villi– Transported via the hepatic portal
vein
• Enzymes/chemicals used: bile salts and pancreatic lipase
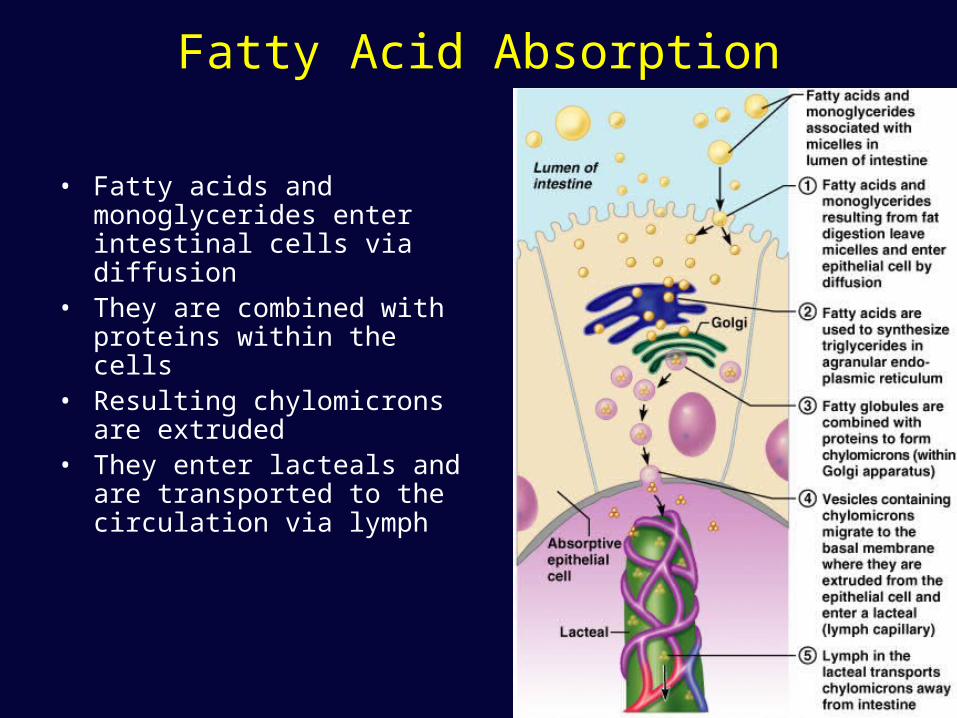
Fatty Acid Absorption
• Fatty acids and monoglycerides enter intestinal cells via diffusion
• They are combined with proteins within the cells
• Resulting chylomicrons are extruded
• They enter lacteals and are transported to the circulation via lymph
Chemical Digestion: Nucleic Acids
• Absorption: active transport via membrane carriers
• Absorbed in villi and transported to liver via hepatic portal vein
• Enzymes used: pancreatic ribonucleases and deoxyribonuclease in the small intestines
Absorption
• Water - nearly all (95%) that is ingested is reabsorbed– Net osmosis occurs whenever a concentration
gradient is established by active transport of solutes into the mucosal cells
– Water uptake is coupled with solute uptake, and as water moves into mucosal cells, substances follow along their concentration gradients
• Vitamins – Water soluble vitamins are absorbed by diffusion– Fat soluble vitamins are absorbed as part of micelles
• Vitamin B12 requires intrinsic factor
Electrolyte Absorption
• Most ions are actively absorbed along the length of small intestine – Na+ is coupled with absorption of glucose and amino acids– Ionic iron is transported into mucosal cells where it binds to
ferritin
• Anions passively follow the electrical potential established by Na+
• K+ diffuses across the intestinal mucosa in response to osmotic gradients
• Ca2+ absorption:– Is related to blood levels of ionic calcium– Is regulated by vitamin D and parathyroid hormone (PTH)