the diabetic athlete - american college of sports …forms.acsm.org/tpc/pdfs/43 bayes.pdf• discuss...
TRANSCRIPT

The Diabetic Athlete
Matt Bayes, MD, CAQSM BlueTail Medical Group
St. Louis, MO

Thanks to:
David Olson, MD
University of Minnesota
Objectives At the conclusion of this lecture you will be able to:
• Discuss where to find clinical guidelines • Define diabetes mellitus • Define risks and benefits of exercise in the diabetic
athlete, including diabetic emergencies • Understand sport physiology and diabetes • Discuss pre-participation evaluation and
participation issues in the diabetic athlete • Know specific management issues in Type I and II
DM
Clinical Guidelines Position statements via American Diabetes
Association
– Standards of Medical Care for Patients with Diabetes Mellitus. Diabetes Care. Vol. 27, Supplement 1, January 2004
– Physical Activity/Exercise and Diabetes. Diabetes Care. Vol. 27, Supplement 1, January 2004
– www.diabetes.org – great site for Physician info!

Clinical Guidelines
Clinical Review Articles
– Harris GD, White RD: Diabetes in the Competitive Athlete. Curr Sports Med Rep 2012 Nov;11(6):309-15
– Weiland DA, White RD: Clinics in Family Practice 2002;4(3)
– The daily management of athletes with diabetes. Clin Sports Med, Jul 2009

Defining Diabetes
“Diabetes mellitus is a group of metabolic diseases characterized by hyperglycemia resulting from defects in insulin secretion,
insulin action, or both.”
•~90% Type II •~10% Type I
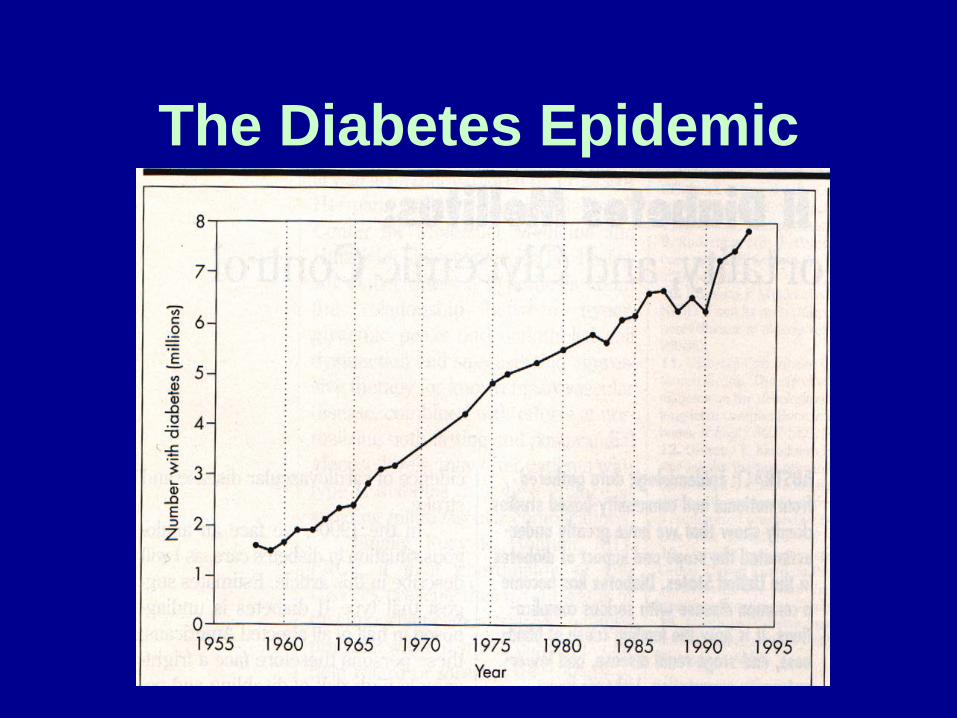
The Diabetes Epidemic
Type I Diabetes/IDDM • Can occur at any age, typical onset < 30 yo
therefore many athletic encounters involve athletes with this condition
• Autoimmune mediated decrease in insulin production in the islet cells of the pancreas
• Demonstrate hyperglycemia and weight loss
• Prone to ketoacidosis, with death occurring if exogenous insulin is not administered and the acidosis is reversed
Type II Diabetes: NIDDM
• Impairment in insulin production and release by pancreatic beta cells
• Reduced sensitivity to insulin in muscle, liver and fat tissues
• Excessive hepatic glucose production in the basal state
• Rare to see Type II in elite athletes • Seen in “weekend warrior” athletes or
with higher BMI: football linemen, rugby, ageing first basemen

Prevalence of Non-Insulin Dependent Diabetes by Age

Type II DM: Initial Conservative Therapy
• A 3-4 month trial of dietary counseling • Regular exercise regimen to improve
insulin sensitivity and glucose utilization • Lack of improvement in blood sugars
and glycosylated hemoglobin with lifestyle changes reflects the need for oral agents or insulin
Exercise benefits both Type I and II DM
• Reduced cardiovascular disease risk • Enhancement of physical fitness • Improved social and emotional well-
being
Exercise Risks in DM • General: If external goals outweigh the
importance of blood glucose control and avoidance of complications
• Specific to weight category sports (wrestling, boxing): common to omit insulin to lose weight prior to weigh-in, leading to poor glucose control and risk of ketoacidosis
Potential Complications of Exercise in Diabetics
• Hypoglycemia • Hyperglycemia (with and without ketosis) • Dehydration • Hypotension • Foot ulcers (with peripheral neuropathy) • Orthopedic injuries • Accelerated DJD
Contraindications in Diabetic Athletes
• Contraindications are based on potential risks of a particular activity in the presence of specific complications of DM
• Patients without complications, steady control and knowledge can participate in most activities
• Must be careful with scuba, sky diving, auto racing and others where hypoglycemia could cause disaster

Diabetes Control and Complication Trial
• Study by the Diabetes Control and Complications Trial Research Group
• Clearly demonstrated the beneficial affects of tight glucose control in the development and progression of complications in Type I diabetes
• Hypoglycemic episodes are 3 times more likely in intensively controlled patients than those more traditionally treated
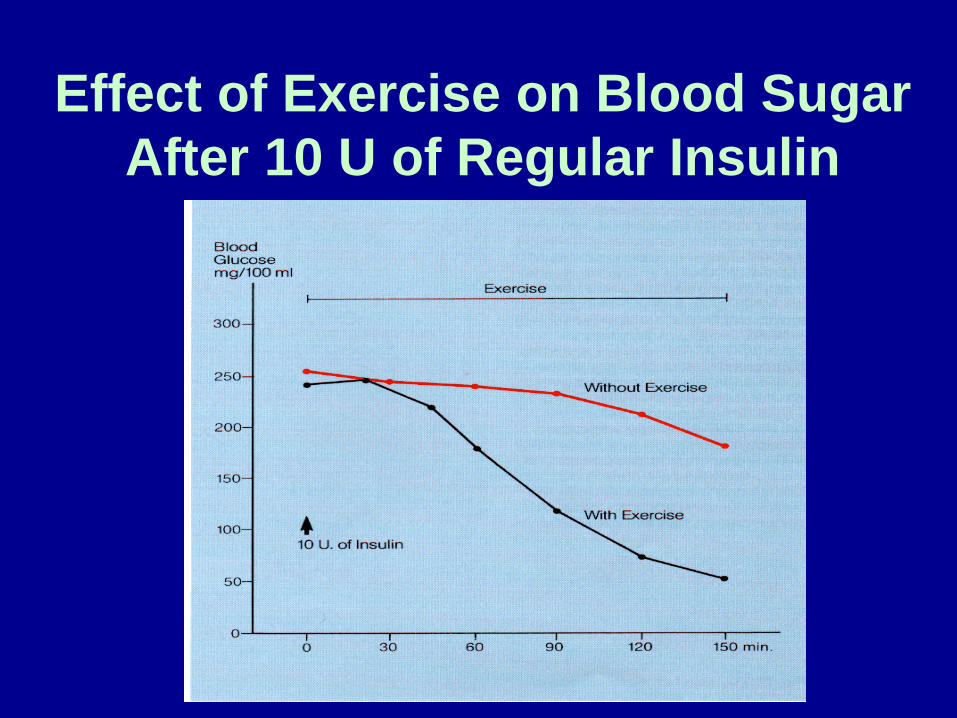
Effect of Exercise on Blood Sugar After 10 U of Regular Insulin

Sport Physiology and Diabetes
• Augments the effects of insulin: Increases 20x the muscle’s ability to take up glucose
• 40 min exercise session can insulin sensitivity by 40% and continue for the subsequent 48 hours
• These are not diminished in the diabetic condition, benefits Type II > Type I
Metabolic response to exercise • Can be various release patterns and
insulin absorption from SC insulin • Increased exposure of insulin to
receptors on muscle cells as blood flow increases
• Thus risk of hyperglycemia during initial exercise and hypoglycemia later as the injected insulin does not regulate to the falling level of glucose

Preparticipation Assessment • History
– Length of known diabetes (Type) – Medication regimen – Discuss any secondary medical
problems related to their diabetes – Type of exercise planned – Previous exercise – Goals of patient (Weight loss, BS
control)

Pre-exercise Evaluation
• History and Physical must check for: – Cardiovascular disease – Peripheral Vascular Disease – Retinopathy – Nephropathy – Neuropathies (Autonomic/Peripheral) – Hyper/Hypoglycemic episodes and
frequency
Pre-exercise Evaluation – Base line fasting blood glucose,
HBA1c, lipid profile – Before beginning intense exercise
program should be doing frequent glucose monitoring & urine ketone monitoring
– Transition from sedentary to trained athlete poses the greatest risk of hypoglycemia

Glucose monitoring and exercise
• 2-3 readings 30 min apart pre-exercise to trend blood glucose direction
• Every 30 min during exercise • Every 2 hours for up to 4 hours post
exercise to monitor for delayed hypoglycemia

Pre-Exercise Blood Glucose
• 100-250 mg/dl: Safe to begin exercise • Most athletes prefer 120-180 mg/dl • <100 mg/dl: Administer glucose (tablet
or juice) • >250 mg/dl: Check for urine ketones
+ ketones: Avoid exercise, hydrate, recheck - ketones: Proceed cautiously, hydrate, recheck
Cardiac/Peripheral Vascular Systems
– Diabetics >35yo or >25yr history of DM should have screening for silent ischemia & cardiac response to exercise w/ graded exercise test
– Contraindications to exercise: CAD (untreated), SBP > 200, claudication
– Graded Exercise Test: Provides estimation of fitness level
– Especially important in previously sedentary patient
– Check feet closely and treat aggressively

Retinopathy • Screen all athletes • Diabetic athletes
need yearly exam • If present: avoid
sports that increase pressure (weightlifting, scuba)
• Clear via Optho if retinopathy is present
Autonomic Dysfunction
– May have abnormal HR & BP response to exercise & position change causing orthostatic hypotension
– Impaired temperature regulation – Prone to dehydration

Nephropathy
• Control hypertension • Regular evaluation of
renal function (BUN/Cr) and presence of proteinuria (micro- albumin)
Musculoskeletal
• May show decreased flexibility: caused by glycosylation of connective tissue in poorly controlled DM
• Proprioceptive issues putting them at risk if athlete has peripheral neuropathy

Medications
• Many forms of insulin injections • Many types of oral hypoglycemic meds • Insulin pumps • Continuous glucose monitoring • www.diabetes.org

Preventing/Managing Hypoglycemia
• In the athlete hypoglycemia is immediate or delayed
• Immediate: during or shortly after exercise, most common in Type I due to inadequate glucose intake to meet metabolic demands
• Other causes: Excessive exogenous insulin, or injection of insulin into site of exercising muscle causing increased absorption rate

Prevention of Hypoglycemia • Inject insulin into the abdominal area • Replace calories continuously during
prolonged activity • Careful glucose monitoring to adjust as
needed • More calories required if in cold weather or
lower intensity exercise • Hot environment: risk due to poor appetite
and decreased caloric intake

Management of Hypoglycemia
• Best approach: Prevent! • Be ready: Athletes have varying levels
of maturity, commitment to the sport, and personal accountability
• If suspected: Remove from play, immediate fingerstick glucose

Management of Hypoglycemia • Treat with 15-20g fast acting carb:
glucose tablet or juice, repeat in 15 min if no improvement in symptom or level
• If conditions suggest recurrent hypoglycemia add complex carbs before return to play
• Avoid excess carb: hypoglycemia provokes a counter-regulatory hormonal response

Management of Hypoglycemia
• Severe hypoglycemia with LOC or sz is life threatening: Alert 911
• Avoid forced PO glucose • Glucagon SC, IM, or IV • D50 1-3 ampules
Delayed Hypoglycemia
• AKA: Nocturnal Hypoglycemia • 6-12 hrs after exercise, up to 28 hrs • Associated with sz, arrhythmia, death
as it often occurs in sleep • Vigorous exercise severely depletes
body glycogen stores, followed by poor replacement of glycogen in the postexercise interval (‘Golden Period’)

Delayed Hypoglycemia • In ensuing hours liver and muscle
extract blood glucose to replenish depleted glycogen stores and glycogen synthetase is activated
• Muscle tissue is more sensitive to any available insulin postexercise
• Subsequent severe and persistent delayed hypoglycemia often requires assistance of another person, glucagon, and hours of continuous caloric intake
Type I DM: Sprinters • Anaerobic short distance sprint activities
rarely cause problems • Proper hydration and glycemic control
maximizes performance • Hyperglycemia may occur due to acute
catecholamine release • Delayed hypoglycemia is rare • Usually unnecessary to adjust insulin
dose
Type I DM: Endurance Athlete
• Attain a steady state balance between basal insulin rate, carb intake, and exercise requirement to keep glucose level ~130-150 mg/dl
• If sprint/ effort needed then carb intake or basal rate during that short period
Type I DM: Endurance Athlete: To Avoid Hypoglycemia
• Short bursts of anaerobic exercise before or after aerobic exercise can prevent subsequent hypoglycemia
• Critical ‘Golden Period’: Replace glycogen stores post-race to prevent delayed hypoglycemia (1.5 g carb/kg body weight)
Type II DM
• Management depends on sport and severity/duration of diagnosis
• Early in diagnosis: Still producing insulin, little to no exogenous insulin needed
• Later: Exogenous insulin needed, with adjustment to prevent hypoglycemia

Type II DM
• With active training it is not uncommon for exogenous insulin requirement to decrease by 50% or greater
• Some fit athletes with Type II DM note a plateau in medicine requirements for treating their disease
Travel Requirements • Labeled travel kit, hand carried • 2x needed supplies • Syringes, glucose meter, lancet, test
strips, alcohol swabs, insulin, insulin pump with supplies, glucagon emergency kit, ketone testing supplies
• Physician letter and extra prescriptions • Prepackaged meals and snacks • Diabetes medical bracelet worn
Conclusion • Team physician must understand the
pathophysiology of diabetes • Important to understand the different
risks in athletes with diabetes • Education and assessing an athlete’s
comfort with their diabetes must be done at the pre-participation exam (game/practice is too late)
• Need to have plan in advance for checking athletes prior to game/event and plan of action for potential emergencies

Thank You!
Bibliography • Harris GD, White RD: Diabetes in the Competitive
Athlete. Curr Sports Med Rep 2012 Nov;11(6):309-15 • American Diabetes Association. Diabetes Care. Vol.
27, Supplement 1, January 2004 • American Diabetes Association. Information for
Medical Professionals. www.diabetes.org. 2007 • Kerr C: Improving outcomes in diabetes: A review of
the outpatient care of NIDDM patients. J Fam Pract 40(1):63-74,1995
• Gordon NF: Diabetes: Your complete exercise guide. Champaign, Human Kinetics, 1993
• Peterson KA, Smith CK: The DCCT findings and standards of care for diabetes. Am Fam Physician 52(4):1092-1126, 1995