the communication initiative summaries of change theories and models
TRANSCRIPT

The Communication Initiative
Summaries of
Change Theories and Models

Health Belief Model
“Two major factors influence the likelihood that a person will adopt a recommended preventive health action
First they must feel personally threatened by the disease i.e. they must feel personally susceptible to a disease with serious or severe consequences
Second they must believe that the benefits of taking the preventive action outweigh the perceived barriers to
(and/or costs of) preventive action”
Source: Fishbein summarising Becker [1974, 1984], Janz and Becker [1984], Rosenstock, Strecher and Becker [1994]page 3 in Developing Effective Behavior Change Interventions, Fishbein M, Univ Of Illinois
Theory of Reasoned Action
“…there is one primary determinant of behavior, namely the person’s intention to perform it. This intention is itself viewed as a function of two determinants
- the person’s attitude toward performing the behavior ( based on his/her beliefs about the consequences of performing the behavior, i.e. his or her beliefs about the costs and benefits of performing the behavior) and
- the person’s perception of he social (or normative) pressure exerted upon him or her to perform the behavior.”
Source: Fishbein summarising Fishbein and Ajzen [1975], Ajzen and Fishbein [1980] Fishbein, Middlestadt and Hitchcock [1991], page 4 in Developing Effective Behavior Change Interventions, Fishbein M, Univ Of Illinois

Theory of Subjective Culture and Interpersonal Relations
“…the likelihood of performing a given behavior is determined by intentions, habits and facilitating factors.
Intentions are, in turn, viewed as a function of
- perceived consequences of performing the behavior (outcome expectancies) - social influences (including norms, roles and the self concept) and- emotions
Source: Fishbein summarising Triandis [1972, 1977, 1980], page 4 in Developing Effective Behavior Change Interventions, Fishbein M, Univ Of Illinois

Social Cognitive Theory
“Two major factors influencing the likelihood that one will take preventive action:
First, like the Health Belief Model, a person believe that the benefits of performing the behavior outweigh the costs (i.e. a person should have more positive than negative outcome expectancies)
Second, and perhaps most important, the person must have
a sense of personal agency, or self-efficacy with respect to performing thepreventive behaviour…….must believe that he or she has the skills and abilities necessary for performing the behavior under a variety
of circumstances”
Source: Fishbein summarising Bandura [1986, 1989, 19991, page 3 in Developing Effective Behavior Change Interventions, Fishbein M, Univ Of Illinois

Variables Underlying Behavioral Performance
- summary by Martin Fishbein“Generally speaking it appears that in order for a person to perform a given behavior one or more of the following must be true:
1. The person must have formed a strong positive intention (or made a commitment) to perform the behavior;2. There are no environmental constraints that make it impossible to perform the behavior;3. The person has the skills necessary to perform that behavior;4. The person believes that the advantages (benefits, anticipated positive outcomes) of performing the behavior outweigh the disadvantages (costs, anticipated negative outcomes);5. The person perceives more social (normative) pressure to perform the behavior than to not perform the behavior;6. The person perceives that performance of the behavior is more consistent than inconsistent with his or her self image, or that it’s performance does not violate personal standards that activate negative self-actions;7. The persons emotional reaction to performing the behavior is more positive than negative; and8. The person perceives that he or she has the capabilities to perform the behavior under a number of different circumstances…”
Source: Fishbein summarising on page 5/6 in Developing Effective Behavior Change Interventions, Fishbein M, Univ Of Illinois

Community-level Structural Modelsas summarised by Robert Hornick with examples from the field of STD control
“Suggests that environmental forces beyond the control of the individual constrain or help the knowledge-behavior link:[for example]
•Presence or absence of legal restrictions - eg availability of condoms
•Wage scales - which define what proportion of people will have the resources to purchase STD medication
•Access - to clinics capable of diagnosing and treating STDs
Each of these would make it either harder or easier for an individual who learned about a practice to realize it.
Programming Implication
Also suggests that while individual education may be one strategy for achieving behavior change, change in societal level structures may be a more effective starting point - eg availability of condoms”
Source: Alternative Models of Behavior Change - by Robert Hornick, Annenburg School for Communication, Working Paper 131, 1990, p 3/4

Social Expectation Modelsas summarised by Robert Hornick with examples from the field of STD control
“Suggests that behavior which appears to be individual may be viewed as a social behavior..Individual practices are substantially the result of conformity to the expectations of others.
Two paths through which private acts may be socially influenced:
• Direct Experience - the social network communicates the private experience - for example expected and acceptable sexual practices through sexual experience with particular partners
• Outside of Direct Experience - for example through conversation amongst those in asocial network, mass media, books, observation of others, all may provide as to what is expected or acceptable
May be that people are unable to articulate, or example, why they use condoms, they just do it. Theirconformity reflects the demands of their social network without any reflective process producing awareness of those demands.
Need to ask the question - ‘how do groups change their behavior?’ rather than ‘how do individuals change their behavior?’
Source: Alternative Models of Behavior Change - by Robert Hornick, Annenburg School for Communication, Working Paper 131, 1990, p 5/6

Audiences along a Behavior Change Continuum:Possible Communication Strategies
Unaware
Aware, concerned,knowledgeable
Motivated to Change
Tries New Behavior
Sustains New Behavior
• Raise awareness• Recommend a solution
• Identify perceived barriers and benefits to behavior change
• Provide logistical information• Use community groups to counsel and motivate
• Provide information on correct use• Encourage continued use by emphasising benefits• Reduce barriers through problem solving• Build skills through behavioral trials• Social support
• Remind them of benefits of new behavior• Assure them of their ability to sustain new behavior• Social support
Source: Communication forBehavior Change - The WorldBank, 1996, by Cecilia Cabanero-Verzosa p 4 - Figure 2

The Behavior Change SpiralSource: The Behavior Changespiral from “What do they want us to do now?”AFAO 1996
Pre
-con
tem
pla
tion
Con
tem
pla
tion
Pre
par
atio
n
Act
ion
Mai
nte
nan
ce
Precontemplation: changing a behavior has not been considered;person might not realise that change is possible or that it might be of interestto them
Contemplation: something happens to prompt the person to start thinking about change - perhaps hearing that someone has made changes - or something else has changed - resulting in the need for further change
Preparation: person prepares to undertake the desired change - requires gathering information, finding out how to achieve the change, ascertaining skills necessary, deciding when change should take place - may include talking with others to see how they feel about the likely change, considering impactchange will have and who will be affected
Action: people make changes, acting on previous decisions, experience, information, new skills, and motivations for making the change
Maintenance: practice required for the new behavior to be consistently maintained, incorporated into the repertoire of behaviors available to a person at any one time

The Behavior Change Spiralin the context of the Enabling Environment
Source: The Behavior Changespiral from “What do they want us to do now?”AFAO 1996
Pre-c
onte
mpla
tion
Contemplatio
n
Prepa
ratio
n
Act
ion
Mai
nten
anceSocial features
eg nature of personal relationships; expectationsof class, position, age, gender; access to knowledge,information.
Cultural features- the behaviors and attitudes considered acceptable in given contexts - eg relating to sex, gender, drugs, leisure, participation
Ethical and spiritual features - influence of personal and shared values and discussion about moral systems from which those are derived - can include rituals,religion and rights of passage
Legal Features - laws determining what people can do and activities to encourage observance of those laws
Political features - systems of governance in which change will have to take place - can, for example, limit access to information and involvement insocial action
Resource features - affect what is required to make things happen - covers human, financial and material resources;community knowledge and skills; and items for exchange
6 Features of the E
nabling Environm
ent
Per
son
al B
ehav
ior
Ch
ange
Sp
iral

Steps to Behavior ChangeAs developed by Population Communication Services for communication programmes appropriate for
family planning and reproductive health.
Knowledge1. Recalls family planning messages.2. Understands what family planning means.3. Can name family planning method(s) and/or source of supply.
Approval4. Responds favorably to family planning messages.5. Discusses family planning with personal networks (family, friends)6. Thinks family, friends, and community approve of family planning.7. Approves of family planning.
Intention8. Recognizes that family planning can meet a personal need.9. Intends to consult a provider.10. Intends to practice family planning at some time.
Practice11. Goes to a provider of information/supplies/services.12. Chooses a method and begins family planning use.13. Continues family planning use.
Advocacy14. Experiences and acknowledges personal benefits of family planning.15. Advocates practice to others.16. Supports programs in the community.
SOURCE: Health Communication - Lessons from Family Planning and Reproductive Health, Johns Hopkins School of Public Health, Center for Communication Programs, 1997, by Phyllis Tilson Piotrow, D. Lawrence Kincaid, Jose G. Rimon II, and Ward Rinehart. P. 23

Cultivation Theory of Mass Mediaproposed by George Gerbner
“…specifies that repeated, intense exposure to deviant definitions of ‘reality’ in the mass media leads to perception of the ‘reality’ as normal. The result is a social legitimisation of the ‘reality’ depicted in the mass media, which can influence behavior. (Gerbner, 1973 & 1977; Gerbner et al., 1980.)”
SOURCE: Health Communication - Lessons from Family Planning and Reproductive Health, Johns Hopkins School of Public Health, Center for Communication Programs, 1997, by Phyllis Tilson Piotrow, D. Lawrence Kincaid, Jose G. Rimon II, and Ward Rinehart. P. 22
“Cultivation analysis concentrates on the enduring and common consequences of growing up and living with television. Theories of the cultivation process attempt to understand and explain the dynamics of television as the distinctive and dominant cultural force of our age. Cultivation analysis uses a survey instrument, administered to representative samples of respondents. The responses are analyzed by a number of demographic variables including gender, age, race, education, income, and political self-designation (liberal, moderate, conservative). Where applicable, other controls, such as urban-rural residence, newspaper reading, and party affiliation are also used.Cultivation analysis is a part of the Cultural Indicators (CI) research project. CI is a data base and a series of reports relating recurrent features of the world of television to viewer conceptions of reality. Its cumulative content data archive contains observations on over 4,500 programmes and 40,000 characters coded according to many thematic, demographic and action categories.”
SOURCE: Letter from George Gerbner to The Communication Initiative, 12 December 1998.

The Knowledge Filterpage 1 of 2
SUBJECTIVEUNRELIABLE
TIM
E
ALL HUMAN TRAITS
CONVENTIONAL
WISDOM
WISDOM
IGNORANCEDEDICATION
COMPETENCE
AMBITION
LAZINESS
GREED
CONSERVATISM IMAGINATION
INSPIRATION
JEALOUSY
INCOMPETENCECARE
HUNCHES
PIG-HEADEDNESS
SLOPPINESS
WILD IDEAS
ANARCHY
PERSISTENCE
Gra
duat
e
Und
ergr
adua
te
Trai
ning
Educ
atio
n
NONSENSE
STUPIDITYPSUEDO-SCIENCE
“WHAT WILL THEY THINK?”Proposal reviewing.Grant funding.
BRIGHT
IDEAS
SILLY IDEAS
TRIAL & ERROR
IDEOSYNCRACY
MIXED MOTIVES
STUBBORNESSCONFLICTS OF INTEREST
LUCK
RUTHLESSNESS
HUNCHES
INGENUITY
QUICK & DIRTY EXPERIMENTS
GENEROSITY
CUTTING CORNERS
“CAN THIS GET PUBLISHED?”Replicate & clean up. Seminars & preprints.Editors & referees.
FRONTIERSCIENCE
BIASERROR
DISHONESTY
PRIMARYLITERATURE
RESEARCH PAPERS
MOSTLY NOT OBVIOUS WRONG
PUTATIVESCIENCE
ABSTRACTSMIGHT BE RIGHT
MISTAKES
UNINTERESTING STUFF
FRAUD
Testing & use by others.Modification & extension.Citation of useful work.
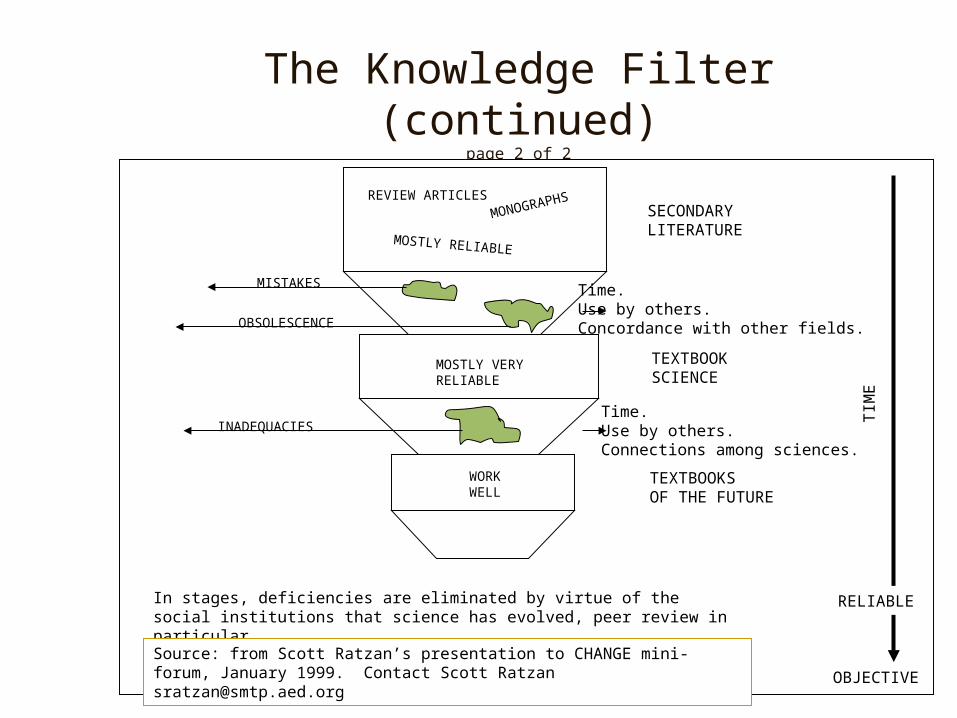
The Knowledge Filter (continued)page 2 of 2
RELIABLE
OBJECTIVE
TIM
E
REVIEW ARTICLES
MONOGRAPHS
MOSTLY RELIABLE
MISTAKES
OBSOLESCENCE
SECONDARYLITERATURE
Time.Use by others.Concordance with other fields.
MOSTLY VERYRELIABLE
TEXTBOOKSCIENCE
INADEQUACIESTime.Use by others.Connections among sciences.
WORKWELL
TEXTBOOKSOF THE FUTURE
In stages, deficiencies are eliminated by virtue of the social institutions that science has evolved, peer review in particular.
Source: from Scott Ratzan’s presentation to CHANGE mini-forum, January 1999. Contact Scott Ratzan [email protected]

Stages of Change Model
CONCEPT DEFINITITION APPLICATION
Pre-contemplation Unaware of the problem Increase awareness of need for change,hasn’t thought about change personalize information on risks and
benefits.
Contemplation Thinking about change, Motivate, encourage to make specificin the near future. plans
Decision/Determination Making a plan to change Assist in developing concrete actionplans, setting gradual goals
Action Implementation of specific Assist with feedback, problem solving,action plans social support, reinforcement
Maintenance Continuation of desirable Assist in coping, reminders, findingactions, or repeating periodic alternatives, avoiding slips/relapsesrecommended step(s) (as applies)
Source: “Theory at a Glance: A Guide for Health Promotion Practice” National Institutes of Health, National Cancer Institute.

Consumer Information Processing Model of Change
MotivationGoal Hierarchy
Attention
InformationAcquisition and
Evaluation
DecisionProcesses
Consumption andLearning Processes
PerceptualEncoding
InternalSearch
ExternalSearch
ProcessingCapacity
Source: “Theory at a Glance: A Guide for Health Promotion Practice” National Institutes of Health, National Cancer Institute.

Consumer Information Processing Model
Concept Definition Application
Information Processing Individuals’ limitations in the Choose the most important and usefulCapacity amount of information they points to communicate, whether orally or
can acquire, use, and remember in print materials
Information Search Processing of acquiring and Provide information so it takes little effortevaluating information; to obtain, draws consumer’s attention,affected by motivation, attention and is clearand perception
Decision Rules/ Rules of thumb, developed and Learn key ways to synthesize informationHeuristics used to help consumers select in ways that have meaning and appeal for
among alternatives your audience
Consumption and Internal feedback based on Keep in mind that people have probablyLearning outcomes of choices, and use in made related choices in the past, and
future decisions are not “empty vessels”
Information Amount, location, format Design information tailored to theEnvironment readability, and processability audience; place it conveniently for use
of relevant information
Source: “Theory at a Glance: A Guide for Health Promotion Practice” National Institutes of Health, National Cancer Institute.

Social Learning Theoryor
Social Cognitive TheoryConcept Definition Application
Reciprocal Determinism Behavior changes result from Involve the individual and relevant others;interaction between person work to change the environment, ifand environment; change is warrantedbi-directional
Behavioral Capability Knowledge and skills to Provide information and training aboutinfluence behavior action
Expectations Beliefs about likely results Incorporate information about likely resultsof action of action in advice
Self-Efficacy Confidence in ability to take Point out strengths; use persuasion andaction and persist in action encouragement; approach behavior
change in small steps
Observational Learning Beliefs based on observing Point out others’ experience, physicalothers like self and/or visible changes; identify role models to emulatephysical results
Reinforcement Responses to a person’s Provide incentives, rewards, praise;behavior that increase or encourage self-reward; decreasedecrease the chances of possibility of negative responses thatrecurrence deter positive changes
Source: “Theory at a Glance: A Guide for Health Promotion Practice” National Institutes of Health, National Cancer Institute.

Community Level Models
Designing health promotion initiatives to serve communities and targeted populations, and not just single individuals, is at the heart of a public health orientation. The collective well-being of communities can be fostered by creating structures and policies that support healthy lifestyles, and by reducing or eliminating hazards in social and physical environments. Community-level models are frameworks for understanding how social systems function and change, and how communities and organisations can be activated.
Community-level models are essential for comprehensive health promotion efforts. These models embody an ecological perspective and are the foundations for pursuing goals of better health for individuals, groups, institutions, and communities. They complement individually oriented behavior change goals with broad aims that include advocacy and policy development. Community-level models suggest strategies and initiatives that are planned and led by organisations and institutions whose missions are to protect and improve health: schools, worksites, health care settings, community groups, and government agencies.
Ideally, comprehensive health promotion efforts build on strategies that have been tried and found effective for reaching health and health behavior goals. However, while strategies have been shown to be effective in many behavioral arenas (e.g., marketing, political), there are currently few health issues for which a variety of demonstrably effective strategies are known.
Source: “Theory at a Glance: A Guide for Health Promotion Practice” National Institutes of Health, National Cancer Institute.
PRECEDE - PROCEED
PRECEDE-PROCEED is a planning model designed by Lawrence Green and Marshall Kreuter for health education and health promotion programmes. Its overriding principle is that most enduring health behavior change is voluntary in nature. This principle is reflected in a systematic planning process which seeks to empower individuals with understanding, motivation, and skills and active engagement in community affairs to improve their quality of life.
This is also practical:
Much research shows that behavior change is most likely and lasting when people have actively participated in decisions about it. In the process, they make healthy choices easier by changing their behavior and by changing the policies and regulations which influence their behavior.
Source: “Theory at a Glance: A Guide for Health Promotion Practice” National Institutes of Health, National Cancer Institute.

PRECEDE - PROCEEDPhases
PRECEDEPhase 5 Phase 4 Phase 3 Phase 2 Phase 1Administration Educational & Behavioral & Epidemiological Social& Policy Organisational Environmental Diagnosis DiagnosisDiagnosis Diagnosis Diagnosis
HealthEducation
Policyregulation
organisation
Predisposingfactors
Reinforcingfactors
Enablingfactors
Behavior andlifestyle
Environment
HealthQualityof life
HEALTHPROMOTION
Phase 6 Phase 7 Phase 8 Phase 9Implementaion Process Impact Outcome
Evaluation Evaluation Evaluation
PROCEED
Source: “Theory at a Glance: A Guide for Health Promotion Practice” National Institutes of Health, National Cancer Institute.

PRECEDE - PROCEEDas an Organising Framework for Application Theory
Diagnostic Phase
PHASE 1 PHASE 2 PHASE 3 PHASE 4 PHASE 5 Social Diagnosis Epidemiological Behavioral & Educational & Administrative & Diagnosis Environmental Organisational Policy
Diagnosis Diagnosis Diagnosis
THEORY
STAGES OF CHANGE X X
HEALTH BELIEF MODEL X
CONSUMER INFORMATION XPROCESSING
SOCIAL LEARNING X XTHEORY
COMMUNITY X XORGANISATION
ORGANISATIONAL X XCHANGE
DIFFUSION OF X XINOVATIONS
Source: “Theory at a Glance: A Guide for Health Promotion Practice” National Institutes of Health, National Cancer Institute.
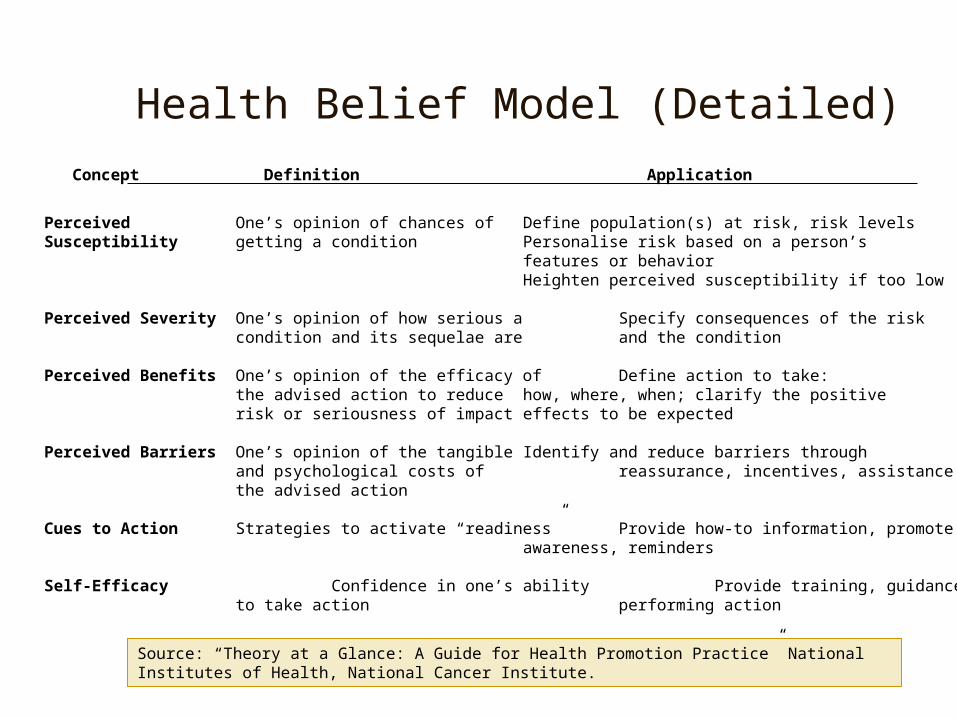
Health Belief Model (Detailed)Concept Definition Application
Perceived One’s opinion of chances of Define population(s) at risk, risk levelsSusceptibility getting a condition Personalise risk based on a person’s
features or behaviorHeighten perceived susceptibility if too low
Perceived Severity One’s opinion of how serious a Specify consequences of the riskcondition and its sequelae are and the condition
Perceived Benefits One’s opinion of the efficacy of Define action to take:the advised action to reduce how, where, when; clarify the positiverisk or seriousness of impact effects to be expected
Perceived Barriers One’s opinion of the tangible Identify and reduce barriers throughand psychological costs of reassurance, incentives, assistancethe advised action
Cues to Action Strategies to activate “readiness” Provide how-to information, promoteawareness, reminders
Self-Efficacy Confidence in one’s ability Provide training, guidance into take action performing action
Source: “Theory at a Glance: A Guide for Health Promotion Practice” National Institutes of Health, National Cancer Institute.

Health Belief Model (Visual)
Perceived Susceptabilityto Disease “X”
Perceived Severityof Disease “X”
Demographic variable[age, sex, raceethnicity, etc.]
Socio-psychological variables
Perceived Threat ofDisease “X”
Cues To ActionMass Media Campaigns
Advice from othersReminder postcard from physician or dentist
Illness of family member or friendNewspaper of magasine article
Perceived benefits ofpreventative action
minus
Perceived barriers to preventative action
Likelihood of TakingRecommended Preventative
Health Action
INDIVIDUAL PERCEPTIONS MODIFYING FACTORS LIKELIHOOD OF ACTION

Robinson’s “Two Step” Model
MASS MEDIA
OPINION GIVERS
OPINION RECEIVERS
Information
InfluenceInfluence
Source: “Communication and Community Development for Health Information: Constructs and Models for Evaluation” by John E. Bowes, Review prepared for the National Network of Libraries of Medicine, Pacific Northwest Region, Seattle, December 1997. [email protected]

Diffusion Model
COMMUNICATION CHANNELS
I. KNOWLEDGE II. PERSUASION III. DECISION IV. IMPLEMENTATION V. CONFIRMATION
PRIORCONDITIONS1. Previous practice2.Felt needs/problems3.Innovativeness4.Norms of the socialsystems
Characteristics ofthe Decision-Making Unit:1. Socioeconomiccharacteristics2. Personalityvariables3. Communication behavior
Perceived Characteristicsof the Innovation1. Relative Advantage2. Compatibility3. Complexity4. Trialability5. Observability
1. Adoption Continued AdoptionLater Adoption
2. RejectionDiscontinuanceContinued Rejection
Source: “Communication and Community Development for Health Information: Constructs and Models for Evaluation” by John E. Bowes, Review prepared for the National Network of Libraries of Medicine, Pacific Northwest Region, Seattle, December 1997. [email protected]
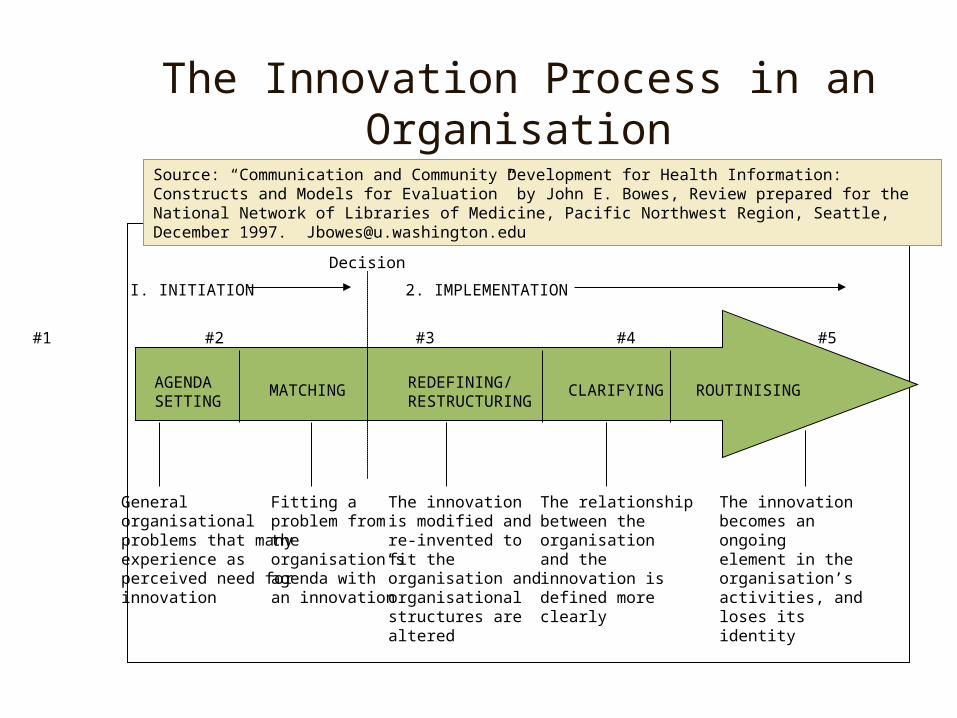
The Innovation Process in an Organisation
AGENDASETTING
MATCHING REDEFINING/RESTRUCTURING
CLARIFYING ROUTINISING
#1 #2 #3 #4 #5
Decision
I. INITIATION 2. IMPLEMENTATION
Generalorganisationalproblems that manyexperience as perceived need forinnovation
Fitting aproblem fromtheorganisation’sagenda withan innovation
The innovationis modified andre-invented tofit theorganisation and organisational structures arealtered
The relationshipbetween theorganisationand theinnovation isdefined moreclearly
The innovationbecomes anongoingelement in theorganisation’sactivities, and loses itsidentity
Source: “Communication and Community Development for Health Information: Constructs and Models for Evaluation” by John E. Bowes, Review prepared for the National Network of Libraries of Medicine, Pacific Northwest Region, Seattle, December 1997. [email protected]

Co-orientation Model
Client Perception of Practice
Client Estimate ofProvider’s Perception
Health Provider’sPerception of Practice
Provider’s Estimate ofClient’s Perception
AGREEMENT PERCEIVED
AGREEMENT
ACCURACY AGREEMENT PERCEIVED
Source: “Communication and Community Development for Health Information: Constructs and Models for Evaluation” by John E. Bowes, Review prepared for the National Network of Libraries of Medicine, Pacific Northwest Region, Seattle, December 1997. [email protected]
[NB: Accuracy measures the extent to which each party’s estimate coincides with the other’s described position or perception. Agreement perceived suggests the level of descrepancy or congruence with the other.]

The Stanford Process
Process Model 1. Creationof CampaignComponents
2. PotentialExposure
TREATMENT VARIABLES Categories ofVariables
RelevantEvaluationLevel Project Evaluation
VariablesMeasured
MeasurementMethods andStudies
1 2. 3. 4. & 5. 6. & 7. 8.
Project Broadcast-organisation -amount-administration -schedule-effort Distribution-cost -print materials
-ORT packetsTraining
1. & 2.Staff interviews, project records, policy maker, interviews, cost effectiveness
study, administrative history
COGNITIVE & ATTITUDINALOUTCOMES
3. ActualExposure
4. KnowledgeChange
5. AttitudeChange
BEHAVIORALOUTCOMES
HEALTHSTATUSOUTCOMES
6. Trial of Behavior
7. Adoption ofBehavior
8. Change inHealth Status
Impact Evaluation
Media UseComponent-specific exposure Access to &use of healthcare facilitiesInformation seeking& advice sources
Prior status & changes in traditionalbeliefs; Message specific recall & recognition, e.g.,measurement of diarrhealdisease, nutrition of thechild, water supply,sanitation food & personal hygiene
Prior status & changes in: Response to diarrhea, breast-feeding & other feeding questions; domestic water & waste disposal; personal hygiene; food preparation hygiene; use of health care resources
MorbidityMortalityNutritionalstatus
3. thru 8.Panel Study, using interviews, observation, anthropometric
measurement. Ethnographic Study, using interviews & ethnographic techniques. Pre-post Study, using interviews &
observations. Mortality Study, using interviews. Health Worker Study, using interviews.
Source: “Communication and Community Development for Health Information: Constructs and Models for Evaluation” by John E. Bowes, Review prepared for the National Network of Libraries of Medicine, Pacific Northwest Region, Seattle, December 1997. [email protected]

The Soul City Thoughts on Behaviour Change
Source: Print Publication - Soul City: Thoughts on Behaviour Change
Advocacy
Social & Political Environment
Community
IndividualLocus of ControlKnowledge
Approval
Attitude
Intention Practice
Barriers
Diffusion of Innovation
Social Influence