the children’s services role in an integrated care service
TRANSCRIPT

1© 2017. All Rights Reserved.
www.openminds.com163 York Street, Gettysburg, Pennsylvania 17325Phone: 717-334-1329 - Email: [email protected]
The OPEN MINDS Next Generation Forum On Children’s Services#OMChildrens
May 16, 2017 I 2:00 PM ETPresenter: Lori Accardi, LMSW, Executive Director, Encompass Health Home and Catholic Charities of Broome CountyModerator: Howard Shiffman, Senior Associate, OPEN MINDS & OPEN MINDS Next Generation Forum On Children’s Services Co-Chair
The Children’s Services Role In An Integrated Care Service Delivery Model: The Catholic Charities Of Broome County Case Study
2© 2017. All Rights Reserved.
Agenda
I. Impetus For The Movement Toward Integrated Care
II. The Catholic Charities Of Broome County Case Study
III. Discussion & Questions

Impetus For The Movement Toward Integrated CarePresented By: Howard Shiffman, Senior Associate, OPEN MINDS & OPEN MINDS Next Generation Forum On Children’s Services Co-Chair
3
4© 2017. All Rights Reserved.
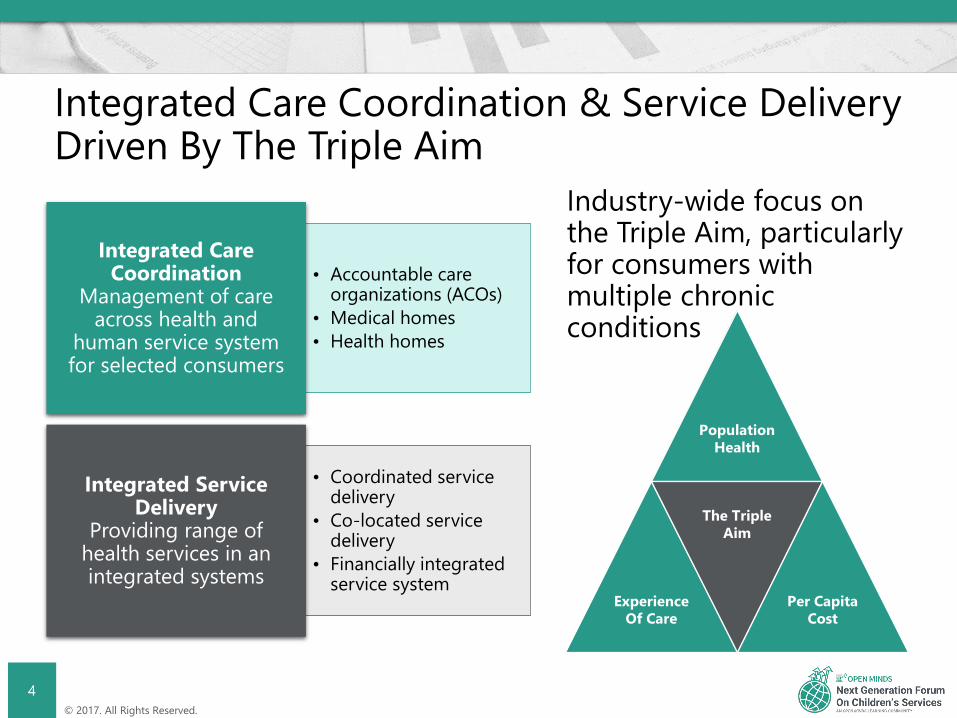
Integrated Care Coordination & Service Delivery Driven By The Triple Aim
Industry-wide focus on the Triple Aim, particularly for consumers with multiple chronic conditions
• Accountable care organizations (ACOs)
• Medical homes • Health homes
Integrated Care Coordination
Management of care across health and
human service system for selected consumers
• Coordinated service delivery
• Co-located service delivery
• Financially integrated service system
Integrated Service Delivery
Providing range of health services in an integrated systems
Population Health
Experience Of Care
The Triple Aim
Per Capita Cost

5© 2017. All Rights Reserved.
Super-Utilizers
The term for people with complex physical health, behavioral health, and social issues who have high rates of utilization
for emergency room (ER) and hospital services
6© 2017. All Rights Reserved.
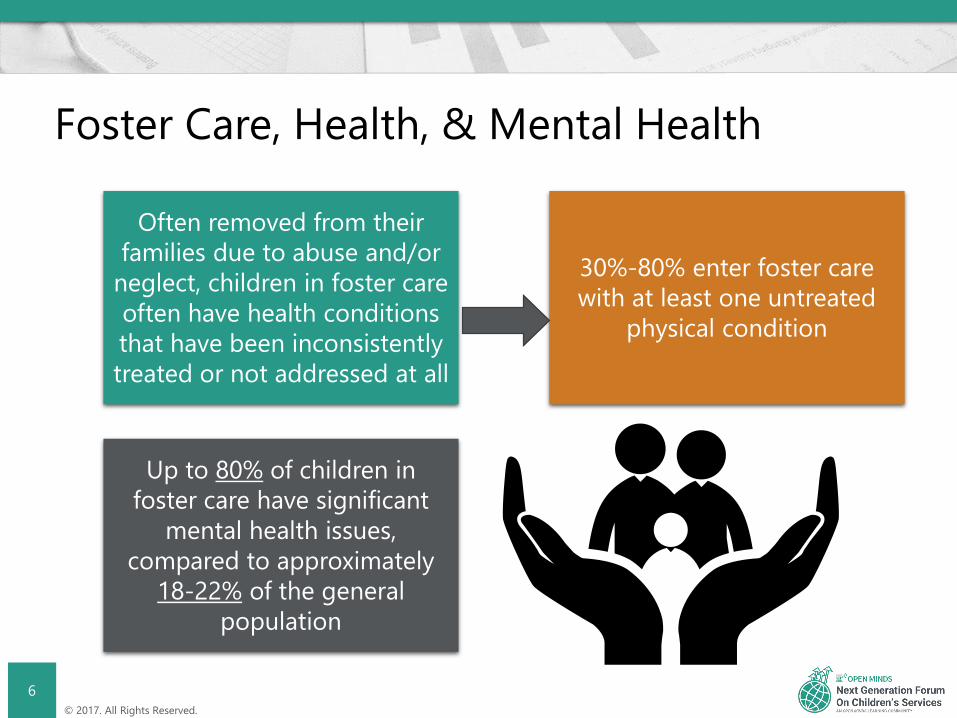
Foster Care, Health, & Mental Health
Often removed from their families due to abuse and/or
neglect, children in foster care often have health conditions that have been inconsistently treated or not addressed at all
30%-80% enter foster care with at least one untreated
physical condition
Up to 80% of children in foster care have significant
mental health issues, compared to approximately
18-22% of the general population

7© 2017. All Rights Reserved.
Foster Care, Health, & Mental Health Cont.
As a result foster youth are prescribed psychotropic
medications at a much higher rate than non-foster youth,
This costs the state millions of dollars a year
The American Academy of Pediatrics, Healthy Foster Care American Initiative, identifies
mental and behavioral health as:
“The greatest unmet heath need for children and teens in foster
care”
Factors contributing to the mental and behavioral health of children and youth in foster care include:- The history of complex trauma- Frequently changing situations
and transitions- Broken family relationships
- Inconsistent and inadequate access to mental health services
- The over-prescription of psychotropic medications
8© 2017. All Rights Reserved.
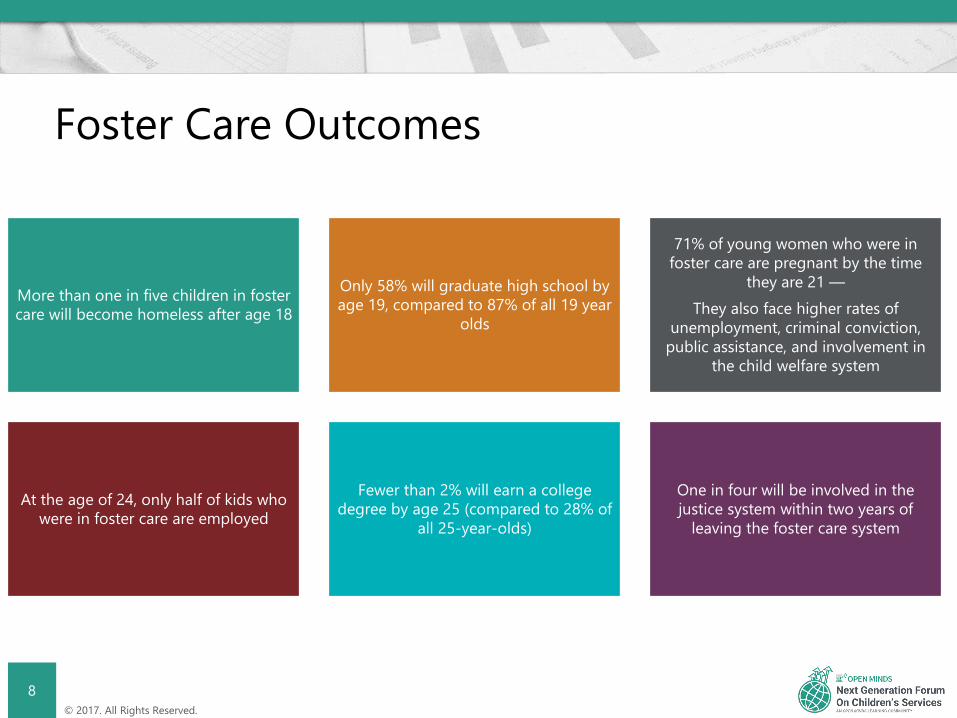
Foster Care Outcomes
More than one in five children in foster care will become homeless after age 18
Only 58% will graduate high school by age 19, compared to 87% of all 19 year
olds
71% of young women who were in foster care are pregnant by the time
they are 21 —They also face higher rates of
unemployment, criminal conviction, public assistance, and involvement in
the child welfare system
At the age of 24, only half of kids who were in foster care are employed
Fewer than 2% will earn a college degree by age 25 (compared to 28% of
all 25-year-olds)
One in four will be involved in the justice system within two years of
leaving the foster care system

9© 2017. All Rights Reserved.
Youth Involved In The Justice System
A multi-site study conducted by the National Center for Mental Health and Juvenile Justice reported that among youth involved in the juvenile justice system:
• 70% met criteria for a mental health disorder• 40% met criteria for a substance use disorder• 90% been exposed to one or more traumatic events
(such as abuse, neglect or witnessing violence)
10© 2017. All Rights Reserved.
Juvenile Justice & Mental Health
Incarcerated youth face disproportionately higher morbidity and higher mortality compared to the general adolescent population
Dental health, reproductive health, and mental health needs are particularly high, likely as a result of lower access to care, engagement in high-risk behaviors, and underlying health disparities
Violence exposure and injury also contribute to the health disparities seen in this population
Juvenile incarceration itself is an important determinant of health, likely correlating with worse health and social functioning across the course of life
11© 2017. All Rights Reserved.
Juvenile Justice Outcomes
Youth who are arrested are two times as likely to not graduate from high school as their non-
arrested peers(the rate increases to four times
that if they are formally processed through the court system)
Young people with disabilities, including mental health and
substance use conditions, are among those at highest risk for
suspension and expulsion, which can be a precursor to juvenile
justice involvement
Children who come into contact with the child welfare system are also at higher risk for subsequent juvenile justice involvement (so-
called “crossover youth”)

12© 2017. All Rights Reserved.
Need For Children’s Services Integration
A more seamless and integrated system would provide shared infrastructure to
identify concerns early and improve access to effective services for all youth in need,
regardless of system involvement
The great challenge is getting all child-serving systems — behavioral health,
juvenile justice, education, child welfare and others — to truly partner with one another in
a way that more efficiently addresses the needs of at-risk youth
13© 2017. All Rights Reserved.
Moving Forward
Systems work best when individuals stop asking “What’s wrong with this child?” and start asking “What happened to this child?”
And the focus begins to shift from legal status, to the clinical profile of the child’s strengths and needs
This shift allows for a better recognition of trauma exposure and symptoms, and higher likelihood of referral to services and supports
II. The Catholic Charities Of Broome County Case Study
Presented By: Lori Accardi, LMSW, Executive Director

A passion for health and compassion for all;Connect with us

MissionCatholic Charities of the Roman Catholic Diocese of Syracuse (Catholic Charities of Broome County) is
dedicated to caring for those in need while promoting human development, collaboration, and the
elimination of poverty and injustice. We strive to empower those served to transform their lives in the
spirit of God's love and compassion.
16
Catholic Charities of Broome County
∗ Established in 1937 as an Area Office of Catholic Charities of the Roman Catholic Diocese of Syracuse NY
∗ Early services included emergency assistance, foster care and adoption and youth services to prevent delinquency
Catholic Charities of Broome County
17
∗ Provides over 40 programs in the areas of behavioral health, intellectual/developmental disabilities, residential services, youth and senior services as well as food pantry and emergency assistance services
∗ Serve over 50,000 people annually through the efforts of over 400 staff and 300 volunteers
∗ Annual budget of $24 million including Encompass Health Home
Catholic Charities of Broome County
18
• Over 100 years of service• Approx. 22,500 employees• Serve 1.3 million people in every NYS county• Estimated total value of services 1.7 Billion• Provide Wide Array of services: ● Mental Health ● HIV/AIDS● Residential ● Foster Care●Developmentally Disabled ● Emergency Svcs● Substance Use Disorders ● Early Intervention
19
NYS Catholic Charities

•Catholic Charities is a well established, respected and often sought after social service agency throughout NYS.
• Many are existing Office of Mental Health, HIV/AIDS/ Targeted Case Management, Voluntary Foster Care, Early Intervention and related types of providers.
• Highly skilled, knowledgeable and compassionate staff already accustomed to care management requirements.
•Well connected and long standing established relationships with community providers.
20
The Encompass Advantage
∗ Section 2703 of the Affordable Care Act establishes authority for states to develop and receive federal reimbursement for their Medicaid populations with chronic illness. Health Home services support the provision of coordinated, comprehensive medical and behavioral health care through care coordination and integration.
∗ Requirement that Hospitals refer Medicaid Recipients who are eligible to Health Homes
Health Homes and Impact on Service Integration
21

•Care management service model•All professionals involved in a member’s care communicate
with one another•Care Manager oversees and coordinates access to all
services•Health Home services are provided through partnerships
between: • Health Care Providers • Health Plans • Community Based Organizations
Collectively, WE are the Health Home.22
What is a Health home?
∗ Reduce avoidable hospital admissions and readmissions
∗ Reduce avoidable emergency room service∗ Provide timely follow up care∗ Reduction in health care costs∗ Less reliance on long term care facilities ∗ Improved experience of care and quality care
outcomes from the individual
23
Goals of a Health Home

1. Comprehensive Care Management
2. Care Coordination and Health Promotion
3. Comprehensive Transitional Care
4. Individual and Family Support
5. Referral to Community and Social Support
Services
6. Use of Health Information Technology24
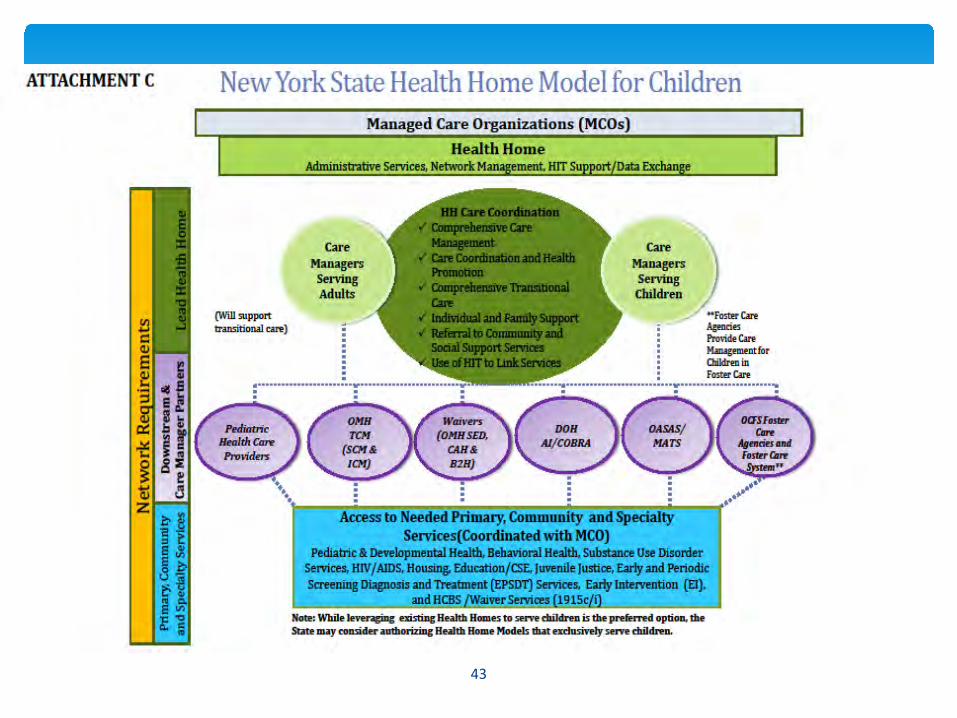
Health Homes 101: Six Core Services
1) Comprehensive Care Management-Completing a comprehensive assessment using CANS-NY -Completing and updating with child and family the child’s plan of care, that is person-centered and family focused, to identify needs/goals-Utilizing multi-disciplinary teams to include family members and social supports
2) Care Coordination and Health Promotion- Coordinating with service providers to ensure necessary care- Coordinating with clinicians to assure all health conditions are addressed- Coordinating case reviews- Providing crisis response, being available 24/7- Coordinating crisis intervention
3) Comprehensive Transitional Care- Transitional planning from one Health Home to another- Movement to and from other counties- Effective linkage/referral and enrollment to care management prior to discharges- Follow-up on admission to and discharge planning from hospitals, ER’s, residential and rehabilitative settings- Overlay/connection of care management services as needed; flexibility to vary intensity of services at transition points
25
SIX CORE SERVICES –EXAMPLES for children and families

4) Individual and Family Support- Referring child and family to peer supports, support groups, social services and entitlement programs as needed - Consulting with and educating child/family/caretaker on advanced directives- Facilitating interpreter services as needed
5) Referral to Community and Social Support Services- Referring and linking individuals to community services and social supports that they have identified having an interest in and are a part of their care plan- Tracking and following up on all referrals made - Collaborating and coordinating with community based providers to support effective utilization
6) Use of Health Information Technology- Care management agency adopting HIT systems and practices as implemented by designated health homes - Medicaid Analytics Performance Portal (MAPP)- Regional Health Information Organizations (RHIO)
26
SIX CORE SERVICES –EXAMPLES for children and families
• Person must be Eligible for Medicaid and have:• Two or more chronic conditions or• One single qualifying condition of
• HIV/AIDS,• Serious Mental Illness (SMI) / Serious Emotional Disturbance (SED), OR• Complex Trauma ( children)
• Chronic Conditions Include:• Alcohol and Substance Abuse• Mental Health Condition• Cardiovascular Disease (e.g., Hypertension)• Metabolic Disease (e.g., Diabetes)• Respiratory Disease (e.g., Asthma)• Obesity BMI >25 (BMI at/or above 25 for adults, and at or above 85thpercentile for children)• Other chronic conditions (see DOH website for list of chronic conditions)
http://www.health.ny.gov/health_care/medicaid/program/medicaid_health_homes/docs/09-23-2014_eligibility_criteria_hh_services.pdf
27
Eligibility

∗ The term complex trauma incorporates at least:∗ Infants/children/or adolescents’ exposure to multiple traumatic events, often of an invasive, interpersonal nature, and∗ the wide-ranging, long-term impact of this exposure.
∗ Nature of the traumatic events:∗ often is severe and pervasive, such as abuse or profound neglect;∗ usually begins early in life;∗ can be disruptive of the child’s development and the formation of a healthy sense of self (with self-regulatory, executive
functioning, self-perceptions, etc.);∗ often occur in the context of the child’s relationship with a caregiver; and∗ can interfere with the child’s ability to form a secure attachment bond, which is considered a prerequisite for healthy social-
emotional functioning.
∗ Many aspects of a child’s healthy physical and mental development rely on this secure attachment, a primary source of safety and stability.
∗ Wide-ranging, long-term adverse effects can include impairments in:∗ physiological responses and related neurodevelopment,∗ emotional responses,∗ cognitive processes including the ability to think, learn, and concentrate,∗ impulse control and other self-regulating behavior,∗ self-image, and∗ relationships with others.
28
Complex trauma
Appropriateness Criteria: • Individuals meeting the Health Home eligibility criteria must be appropriate for
Health Home care management. Assessing whether an individual is appropriate for Health Homes includes determining if the person is:
• At risk for an adverse event (e.g., death, disability, inpatient or nursing home admission, mandated preventive services, or out of home placement)
• Has inadequate social/family/housing support, or serious disruptions in family relationships;
• Has inadequate connectivity with healthcare system;• Does not adhere to treatments or has difficulty managing medications;• Has recently been released from incarceration, placement, detention, or psychiatric
hospitalization;• Has deficits in activities of daily living, learning or cognition issues, or• Is concurrently eligible or enrolled, along with either their child or caregiver, in a
Health Home.
29
Appropriateness

∗ Medicaid Analytics Performance Portal ∗ CANS-NY Assessment tool is integrated into MAPP∗ Billing, rate information and CANS-NY algorithms (High,
Medium, Low)∗ Referral portal
∗ Community referrals by LGU/SPOAs, LDSS and eventually others, for Assignment
∗ Direct Referrals by Health Homes, Managed Care Plans, Care Managers for Assignment
∗ Will assist with managing consent to refer, enroll, and share information
30
MAPP Functionality for Children
∗ As a member of a Health Home there is one person, a care manager, who coordinates all care and services for the child
∗ The care manager will help families and children understand how to manage their health care and social needs
∗ The care manager will make sure there is access to needed services: ∗ Access to healthcare providers such as doctors, nurses, nutritionist,
counselors, mental health providers, substance abuse providers, etc. ∗ Access to medication ∗ A Safe place to live∗ Insurance to pay for care and services∗ Access to transportation for appointments
31
Advantages of being in a Health Home
•Best Practices•Strengths-Based•Family and Youth Driven•Peer Support•Tailoring Services to the Unique Needs
of Children•Coordinating Services by Partnering•Quality Care
32
Our Core Values

∗ Outreach and Engagement Activities∗ Outreach and Engagement refers to all the activities involved in
obtaining consent, gathering eligibility documentation, engaging the family and youth in the assessment process and educating enrollee on how the HH will benefit them.
∗ Currently the period allowed is up to three months and must demonstrate ongoing and progressive efforts to enroll the person including welcome letters, outreach visits and calls and meetings with collaterals
33
Outreach and Engagement
∗ Strategies to engage potentially eligible persons include: ∗ Educating community providers and referral sources∗ Facilitating meetings with Care Management Agencies to share ideas and
gather provider input. ∗ Increasing community presence ∗ Adding innovative technologies
∗ Referrals from website and on-call line∗ Help Desk (Giva)∗ Social Media and Mobile Apps
∗ Co-locating at services that target populations use∗ Food pantries∗ Hospitals
34
Outreach and Engagement Strategies
• We promote strengths based, person centered care management.
• We promote hands on and direct contact with people in their home and community.
• We work to meet most basic needs first so they can focus on other areas as well.
• We value and have experience with peer services and staff.
• Nurse CMs are available to address complex medical issues.
35
Care Management Model
∗ Principles of Family Wraparound Process:∗ Voice & Choice; Planning is grounded in family members’ perspective∗ Team Based; Agreed upon by family and service relationships∗ Natural Supports; Participation of family’s network of interpersonal and community
relationships∗ Collaboration; All team members work cooperatively and share responsibility∗ Community Based; Strategies that are responsive, accessible and promote family
integration into home and community∗ Culturally Competent; Respects and builds on the values, preferences, beliefs, culture
and identity of the child and family∗ Individualized; Customized set of strategies, supports and services to achieve identified
goals∗ Strengths Based; Process identifies and builds on the capabilities, knowledge, skills and
assets of the child/family∗ Persistence; Team persists in working toward goals ∗ Outcome Based; Team monitors progress towards goals, and Care Manager updates
POC accordingly
Standards for Care Management
36
∗ Policy #6-Plan of Care (POC)∗ Initiated during the first Interdisciplinary Team Meeting, and based on CANS-NY assessment∗ Includes input from all providers/Team members
∗ Anyone not able to be present, will be asked to provide input into the POC∗ Alternate methods of participation e.g. phone/video conferencing is recommended
∗ Is Youth/Family driven∗ Includes those identified by the Child/Family as an important source of support
∗ Every effort is made to include the parent/legal guardian and/or medical consenter∗ Plans will not be finalized without their consent
∗ Includes all 10 elements, and will be developed in Netsmart∗ Completed within 30 days of the CANS-NY assessment, and updated as needed in
conjunction with quarterly reviews and CAN-NY re-assessment∗ Signed by Child, Parent/Consenter - Shared with the Team
Standards for Care Management
37

• Establishing strong relationships/partnerships• Coordinating between Children and Adult Health Home • Training care managers on medical conditions, early intervention, and
Transition age youth (TAY), in order to serve a broader children’s population
• CANS-NY training/certification (incl. supervisors)• Wraparound family planning process/Interdisciplinary Team• Committee on Special Education (CSE) meetings participation• Discharge planning meeting• Hospital team meeting• Support groups, peer support, family support• Participate in ongoing webinars• In addition to minimum requirements, do whatever is necessary!
38
BEST PRACTICES
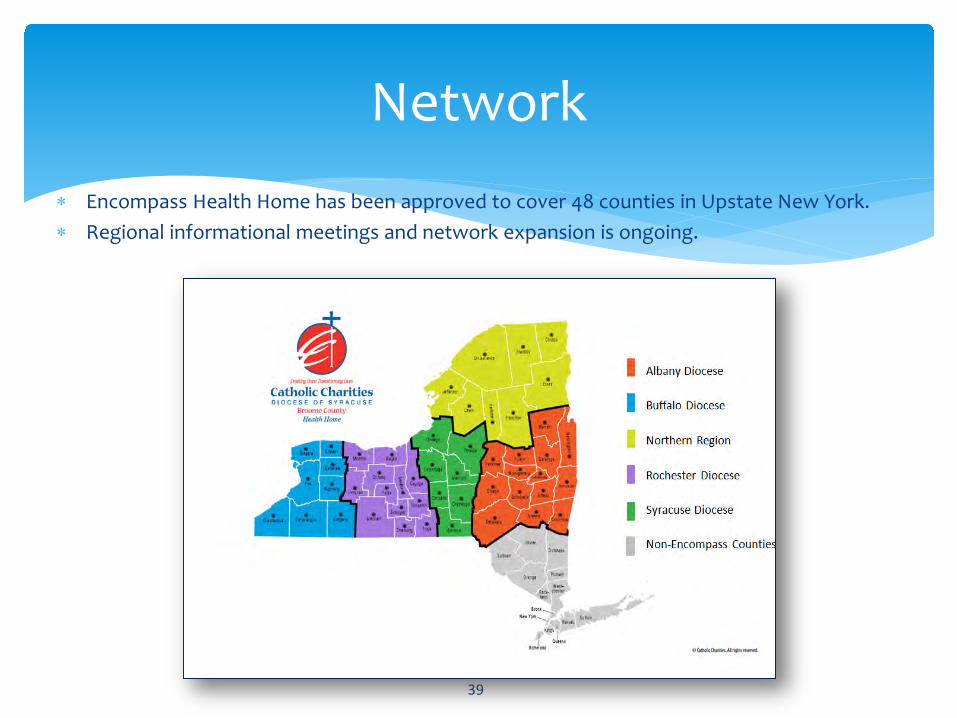
∗ Encompass Health Home has been approved to cover 48 counties in Upstate New York. ∗ Regional informational meetings and network expansion is ongoing.
39
Network

Establish partnerships w/ various systems:•Office of Mental Health•Office of Substance Abuse Services•Office of Child and Family Services•Local Departments of Social Services/County Mental Health•Single Points Of Accountability (SPOA)•Voluntary Foster Care Agencies(VFCA)•Juvenile Justice•Pediatric Health Care and Specialty Providers•Education – Preschool and Committee on Special Ed•Early Intervention
40
Children’s Health HomeRequirements

∗ Regional Support Coordinators to coordinate with systems of care such as Single Points of Accountability and Local Departments of Social Services
∗ 65 Agencies serving families and children contracted to provide Care Management Services including Targeted Case Management and Voluntary Foster Care Providers
∗ 22 Agencies actively serving high need children in outreach and enrollment
∗ 10 Managed Care Organizations
∗ Providers in primary care, medical specialty care, behavioral health, human services and other community organizations that support families
41
The Encompass Network
42
43
Participation in ongoing collaborative efforts:
•Erie County Family Voices and Renssalaer County to pilot High Fidelity Wraparound Model•County Single Points of Accountability Provider Groups•Early Intervention Provider Groups•NYS Health Home Coalition and Subgroups on CMA Performance and Monitoring; Billing and Reimbursement and Incident Review•Education for community providers on the role of the Care Manager and the Health Home. •NYS Health Home Learning Collaborative•NYS Coalition for Children’s Behavioral Health•Health Home Managed Care Organization Workgroup
44
Collaborations
• Contracts with Care Management Agencies
• Contracts with Managed Care Organizations
• Contracts with Regional Health Information Organizations in each region
• Data Exchange Agreement s with other Lead Health Homes
• Numerous Memorandums of Understanding with Community providers
• Contracts with Managed Long Term Care Service Organizations
45
Contractual Relationships
46

• Health Homes, LDSS, LGU, CMAs and MCOs should prioritize the enrollment of based on the following:• Children enrolled in OMH TCM CM programs that will convert to HH• Children on OMH Waiver list (already Medicaid eligible), within 30 days of discharge from inpatient/residential/day
treatment settings to participate in discharge planning • Children on TCM waitlist• Children who are on the Bridges to Health Wait list. • Children in licensed congregate care• Children that are within 3 months of foster care discharge• Children enrolled in LDSS prevention services where foster care placement in imminent• Children prescribed 3 or more psychotropic medications• Children who are within 30 days of discharge from inpatient, residential or detox setting • Medically fragile children with multiple chronic conditions that have had an inpatient stay within the last 30 days• Children who have an ER referral but are not admitted for inpatient services; or are discharged with a
recommendation for community follow-up• Children with multiple system involvement
• Children in Early Intervention (EI) target date to be enrolled later in 2017. 47
Targeted Populations for Roll-out of Health Homes Serving Children:
December 2016

• Administrative Services• Efficiently and effectively process referrals• Assign eligible individuals to CMAs based upon experience and defined member characteristics• Assure required data is submitted to the state through the MAPP, i.e. tracking information, CMART,
CANS-NY• Responsible for billing processed, FFS and MCOs and reconciling all payment to downstream providers• Maintain a structured quality management process that incudes quality planning, control and
improvement that seeks to improve services and outcomes through on-going refinement in response to data and continuous feedback
• Assure care managers have access to other pertinent administrative data that may not be available in MAPP to inform outreach and engagement efforts
• Maintain DEAAs, BAAs and other security• Share information about training opportunities • Marketing of HH care management services• Promotion of evidence based best practices • Support of engagement with families• Develop policies and procedures to satisfy state standards
48
Providing Support to our Network/our Role
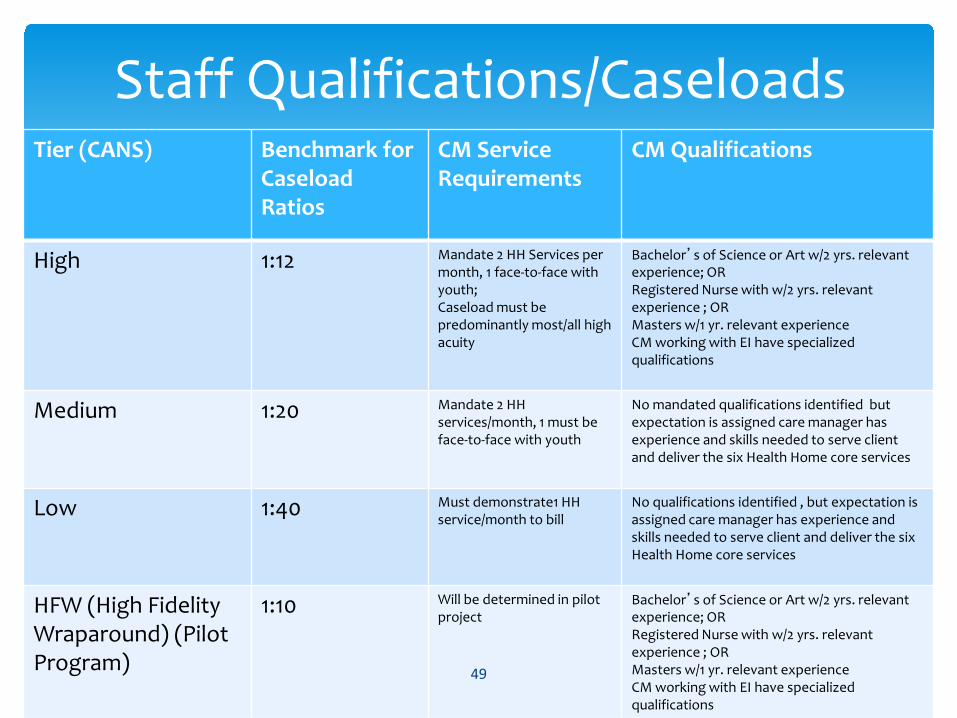
Tier (CANS) Benchmark for Caseload Ratios
CM Service Requirements
CM Qualifications
High 1:12 Mandate 2 HH Services per month, 1 face-to-face with youth;Caseload must be predominantly most/all high acuity
Bachelor’s of Science or Art w/2 yrs. relevant experience; ORRegistered Nurse with w/2 yrs. relevant experience ; ORMasters w/1 yr. relevant experienceCM working with EI have specialized qualifications
Medium 1:20 Mandate 2 HH services/month, 1 must be face-to-face with youth
No mandated qualifications identified but expectation is assigned care manager has experience and skills needed to serve client and deliver the six Health Home core services
Low 1:40 Must demonstrate1 HH service/month to bill
No qualifications identified , but expectation is assigned care manager has experience and skills needed to serve client and deliver the six Health Home core services
HFW (High Fidelity Wraparound) (Pilot Program)
1:10 Will be determined in pilot project
Bachelor’s of Science or Art w/2 yrs. relevant experience; ORRegistered Nurse with w/2 yrs. relevant experience ; ORMasters w/1 yr. relevant experienceCM working with EI have specialized qualifications
49
Staff Qualifications/Caseloads
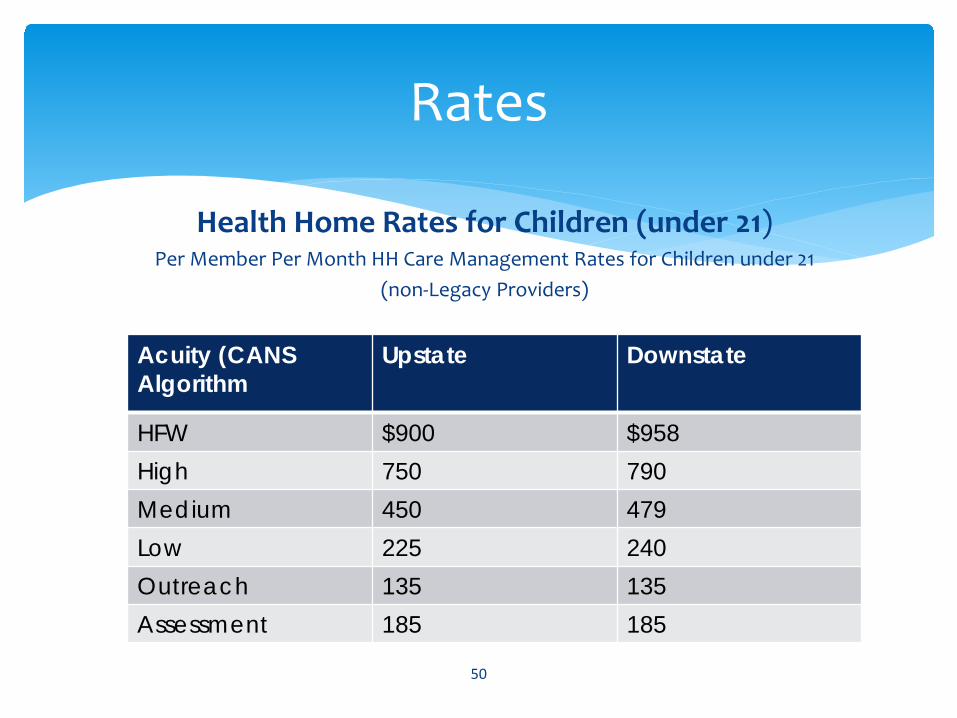
Health Home Rates for Children (under 21)Per Member Per Month HH Care Management Rates for Children under 21
(non-Legacy Providers)
50
Rates
Acuity (CANS Algorithm
Upstate Downstate
HFW $900 $958High 750 790Medium 450 479Low 225 240Outreach 135 135Assessment 185 185
• PSYCKES (Psychiatric Services and Clinical Knowledge Enhancement System) PSYCKES is a HIPAA-compliant, web-based application that provides access to Medicaid claims data for the behavioral health population.
• Best Practice Decision-making Tool• Improve client outcomes by providing immediate access to comprehensive, user
friendly information across providers over time• Support clinical decision making• Support intake assessment and treatment planning• Facilitate care coordination, discharge planning
51
Health Information Technology (HIT)
• RHIOs (Regional Health Information Organizations)• CMAs are requested to contract with their local RHIOs to enhance their
services and quality of care. • The RHIOs in the Encompass HH coverage area are:
• HealthlinkNY (Southern Tier and Hudson Valley)• HEALTHeLINK (Western NY)• Rochester RHIO (Rochester Region)• HealtheConnections (Syracuse Region) • Hixny (Albany and Norther Region)
• Netsmart CareManager/Milllinpro• Electronic Health Record and Billing Software
52
HIT continued

• We apply the best practice standards to ourselves and determine an acceptable standard prior to requiring them of other CMAs.
• We work with the CMAs on areas of compliance and growth.
• We are working to develop audit tools to assist CMAs with quality, outreach and billing compliance.
• We share data from MCOs with the CMAs to assist their assessment of service quality.
53
Quality Assurance Measures
Specific Quality Measures for Children
• Well-Child Visits and Preventive Care• Immunization Status • Annual Dental Visit • Weight Assessment and Counseling for Nutrition and Physical
Activity for Children/Adolescents: Body Mass Index • Follow-up After Hospitalization for Psychiatric Reasons • Lead Testing • Follow Up Care for children Prescribed ADHD Medication:
Initiation and Continuation • Medication Management/Monitoring: Asthma; Antipsychotics• Appropriate Treatment for Children with Pharyngitis
54
54
Guides to Quality/Sources of Data
• Healthcare Effectiveness Data & Information Set (HEDIS-Updated every year) http://www.ncqa.org/hedis-quality-measurement• State Plan Amendment (SPA) Outcomes• Center for Medicare and Medicaid Services (CMS) Measures• MCO Gap in Care Reports
• Medicaid Analytics Performance Portal (MAPP)-Dashboards• Encompass Policies & Procedures• CMART3-Care Management Assessment Reporting Tool• Netsmart Reports• PSYCKES/RHIO• Internal Case File Audits and External Surveys• Participant Surveys• Complaints and Incidents• Other documents and input from Providers, supports and
Participants/Families55
55

Decision Making ToolsRHIO: Regional Health Information Exchange Organization:• A “clinical biography” or “episodes of care” for Participants:
• Lab reports & Radiology reports and images• Medical Diagnosis• Hospital discharge summaries• Clinical documents and reports on healthcare visits• Admission/Discharge notification• Emergency Department reports• Emergency Medical Services (EMS) reports• Patient demographics• Prescriptions/Medications• Immunizations• Allergies
5656
Decision-Making Tools
PSYCKES: Psychiatric Services & Clinical Knowledge Enhancement System (OMH)∗ A web-based portfolio of quality indicators, updated weekly, designed
to support quality improvement and clinical decision-making in the New York State (NYS) Medicaid population
∗ Behavioral Health QARR (Quality Assurance Reporting Requirements)o Behavioral Health Diagnosiso Mental Health Services Datao Psychotropic Medications
5757

Managed Care Audits & Gap in Care Reports
∗ Focuses on Care Management standards and protocols, HEDIS and the gaps in care that are found when looking at claims data
∗ Reports sent to Health Home, and distributed to CMAs∗ CMAs provide appropriate follow-up and report back to Health
Home, who report back to MCO∗ CMAs document all efforts to address HEDIS in Netsmart
5858
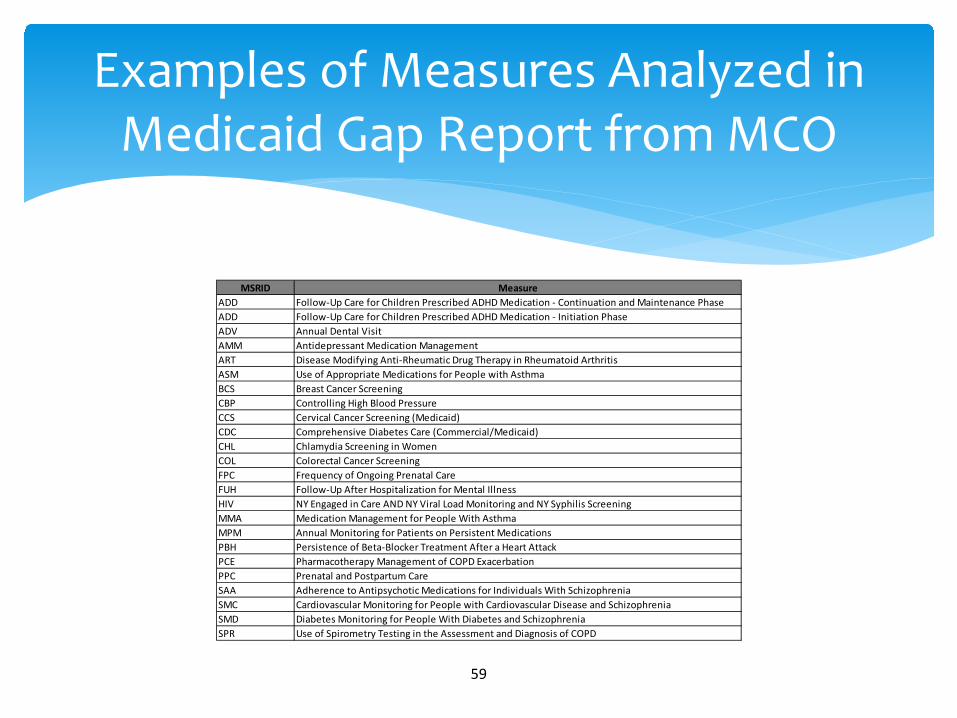
MSRID MeasureADD Follow-Up Care for Children Prescribed ADHD Medication - Continuation and Maintenance PhaseADD Follow-Up Care for Children Prescribed ADHD Medication - Initiation PhaseADV Annual Dental VisitAMM Antidepressant Medication ManagementART Disease Modifying Anti-Rheumatic Drug Therapy in Rheumatoid ArthritisASM Use of Appropriate Medications for People with AsthmaBCS Breast Cancer ScreeningCBP Controlling High Blood PressureCCS Cervical Cancer Screening (Medicaid)CDC Comprehensive Diabetes Care (Commercial/Medicaid)CHL Chlamydia Screening in WomenCOL Colorectal Cancer ScreeningFPC Frequency of Ongoing Prenatal CareFUH Follow-Up After Hospitalization for Mental IllnessHIV NY Engaged in Care AND NY Viral Load Monitoring and NY Syphilis Screening MMA Medication Management for People With AsthmaMPM Annual Monitoring for Patients on Persistent MedicationsPBH Persistence of Beta-Blocker Treatment After a Heart AttackPCE Pharmacotherapy Management of COPD ExacerbationPPC Prenatal and Postpartum CareSAA Adherence to Antipsychotic Medications for Individuals With SchizophreniaSMC Cardiovascular Monitoring for People with Cardiovascular Disease and SchizophreniaSMD Diabetes Monitoring for People With Diabetes and SchizophreniaSPR Use of Spirometry Testing in the Assessment and Diagnosis of COPD
59
Examples of Measures Analyzed in Medicaid Gap Report from MCO

Care MART3
Health Homes are required to provide NYS DOH with the following information submitted via the Health Home Care Management Assessment Reporting Tool (HH-CMART3). All data is extracted from Netsmart:
• Interventionso The submission will contain data regarding Care Management Core
Services provided to Health Home members during the reporting period.
• Assessmentso The submission contains data regarding Participant assessments
performed during the reporting period (excluding CANS-NY).• Plans of Care
o The submission will contain data regarding Plans of Care developed during the reporting period.
Encompass will provide feedback to CMAs regarding performance standards in these areas.6060
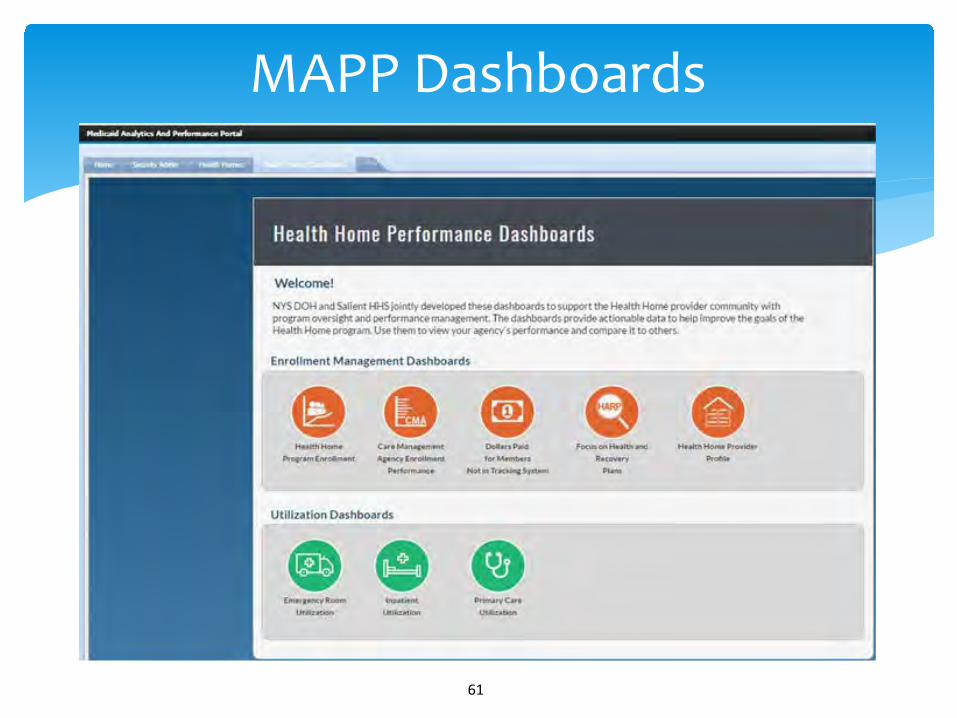
MAPP Dashboards
6161

Case File Audits
∗ Encompass will review quarterly submissions; provide feedback/assistance with developing corrective action plans that may be required for areas that do not meet minimal standards.
∗ Encompass will provide follow up with the CMA after the corrections have been made to assure understanding of the needed corrections and to offer feedback for sustaining performance.
∗ Additional corrective action measures and support regarding CMA performance will be formally developed as needed. o CMA performance may impact additional participant assignments until
identified improvements occur and are sustained.
6262
CMA Monitoring Responsibilities
∗ Supervision of Care Managers and appropriate Care Management standards
∗ Develop Policies and Procedures that address standards and quality processes
∗ Managing and reporting of Complaints/Incidents and barriers to Care Management to Health Home
∗ Regular monitoring of data to drive Care Management activities∗ Initiating corrective action processes to improve care∗ Establishing relationships with Providers, MCOs and Health Home
for guidance
6363

• Adults (designated 7/12)Outreach 924Enrolled 1,350Total 2,274
Children (designated 12/16)Outreach 137Enrolled 317Total 454
Grand Total 2,728
64
Current Outreach and Enrollment (as of May 12, 2017)
Growing from one county to 48 counties has been described by one of our leaders as an “audacious” initiative. So why did we do it ?
•Successful experience serving high need adults and expertise in serving persons with a serious mental illness•After being approached by other groups, we chose to partner with other Catholic Charities dioceses and agencies based on shared values and mission•We had strong statewide leadership and longstanding collegial relationships•Diversity of services including social determinants •Decades of expertise in high need children’s services •Respected reputation and strong local relationships with county and state government
65
REFLECTIONS OF A HEALTH HOME

Health Homes are very complex and challenging to implement:
• Care management agencies that are at different levels of experience
• A marketplace or competition for market share versus a mission driven mentality
• Unanticipated Consequences: The other local adult lead HH in our county has not passed the re-designation process and all adults in outreach must now be referred to Encompass and its network
• Challenged to communicate and differentiate ourselves from other Children’s Health Homes: emphasis on in person communication and customer service, focus on mission and on working in the community versus telephonically
66
REFLECTIONS OF A HEALTH HOME

Use of Health Information Technology is a blessing and a challenge:
• HH name is incorrect in places• Misalignment with MCOs and Care Management Agencies• Lack of understanding by Care Managers on how to answer questions
on assessment tools• Misalignment between our HH IT platform and MAPP• Continual training needed for CMAs • Collaboration of State Partner Agencies with Department of
Health• Breaks down the old silos of care to promote integration• Each State agency incorporates its own requirements of the HH:
complex assessment and planning process to incorporate all the specialized tools
67
REFLECTIONS OF A HEALTH HOME

∗ The Health Home model has the potential to break down the old silos of care for high need children and to provide services in a holistic family strengths based way
∗ Care Managers have the opportunity to become skilled generalists that can assess with expertise in a range of areas including mental health, substance use, HIV/AIDS, and chronic disease
∗ The Health Home model holds the potential to intervene early to offer evidenced based models to address service needs and promote health
68
REFLECTIONS OF A HEALTH HOME

• Identifying ways to generate ground up referrals for populations in need or underserved: rural , LGBTQ, refugee, homeless populations
• Identifying new agencies with similar expertise in case management to provide services
• Promoting Encompass with providers and populations to be served in balance with bringing new Care Management agencies into operation
• Recruiting and retaining a qualified work force in a marketplace where Care Managers are in demand
• Estimating needed Administrative capacity
• Streamlining referral and data processing systems and incorporating predictor models into the Health Home
• Enrolling parents of high need children and developing a Family Care Management model
69
Challenges and Future Development

∗ Creating systems of oversight for corporate compliance, case auditing and complaint and incident investigations.
∗ Creating collegial consultation committees to address clinical, ethical, IT , billing and other cross system issues.
∗ Developing Regional Advisory Boards to include Care Management agencies and key stakeholders
70
Challenges and Future Development
• Providers should assess the populations that they already have relationships with who are in need of these services and build their base on this group
• Ability to recruit and retain staff who can be supported to learn new technology and provide holistic assessment and care management services
• Financial forecasting ability to identify staff resources, supervision structures and administrative oversight
• Methods to offload processes to relieve care management staff and assist in managing caseloads
71
Considerations in Getting Involved in Health Homes
• Ability to build on collaborative relationships
• Willingness to go the extra mile to meet governmental requirements and expectations
• Developing a Family Care Management Model that will address separate individual needs as well as family system needs
A passion for the mission!
www.encompasshealthhome.org
72
Considerations in Getting Involved in Health Homes
Thank youQUESTIONS?
73

III. Discussion & Questions