the case for comparative effectiveness research - whi whi investigator... · science to improve the...
TRANSCRIPT

Science to Improve the Nation‘s Health Care:
The Case for Comparative Effectiveness
Research
Michael S Lauer, MD, FACC, FAHA
Director, Division of Cardiovascular Sciences
NHLBI/NIH
May 5, 2011

Disclosures
My immediate family and I have NOT
received anything of value related to the
technologies and topics being presented.
I will present my personal views, which are
not necessarily those of NHLBI, NIH, or
DHHS.
I am neither an economist nor a politician.
2
So What is CER?
C = Comparative
Real contest
Existing options
Effectiveness = Outcomes
Clinical outcomes: mortality, morbidity, major
clinical events, costs
Systems outcomes: adherence to guidelines
Research = Science
Observations, experiments, syntheses
3 Mitka M JAMA 2010;304:2229-31
CER Legislation and Health Care Reform
ARRA
Allocation $1.1 billion
Federal Coordinating Council for CER
IOM issued report on priorities June 2009
New Patient-Centered Outcomes Research
Institute (―PCORI‖)
Non-government, non-profit
BOG – 21 members including NIH, AHRQ
Methodology committee
4

5
Screaming Headlines!
―It's hard not to scream when you see how many physicians,
pharmaceutical companies, [and] medical-device
makers…seem to hate science, or at best ignore it. These
days the science that inspires fear and loathing is
‗comparative-effectiveness research.‘‖
Sharon Begley, Newsweek, Feb 28 2009

What‘s Going On?
Scaremongers have morphed effectiveness research into
cost-benefit analysis…Effectiveness research will
―‗threaten…lives‘ as government decides ‗who gets
lifesaving treatment and who doesn't.‘ Sen. Tom
Coburn (a doctor) warned of ‗a Soviet-style Federal
Health Board that will put bureaucrats and politicians in
charge of our nation's health-care system.‘‖
You might attribute Coburn's rant to his small government
ideology, but I say blame his profession—not politics
but medicine. Doctors have long resisted having
science guide their practice.
6 Sharon Begley, Newsweek, Feb 28 2009
What‘s Going On?
―Only a limited amount of evidence is available
about which treatments work best for which
patients and whether the added benefits of
more-effective but more-expensive services
are sufficient to warrant their added costs—
yet current practice tends to adopt more-
expensive treatments even in the absence of
rigorous assessments of their impacts….‖
Peter Orszag
7 Congressional Budget Office 2007

A Story of a Popular Therapy
8 http://explorepahistory.com/cms/pbfiles/Project1/Scheme34/ExplorePAHistory-a0j4x4-a_349.jpg
http://upload.wikimedia.org/wikipedia/commons/0/01/Blood_letting.jpg

Come Down to the Contest…
―Come down to the contest ye Humorists: Let us
take out of the Hospitals or the camps or
elsewhere, 200, or 500 poor People, that have
Fevers etc. Let us divide them in Halfes, let us
cast lots, that one half of them may fall to my
share and the other to yours; I will cure them
without bloodletting…; but do you do as ye
know. We shall see how many Funerals both of
us shall have: But let the reward of the
contention or wager, be 300 Florens, deposited
on both sides: Here your business is decided.‖
9 Van Helmont JA. Oriatrike. London: Lodowick-Loyd, 1662, p.526

The Trial is Reported…
10
―It had been so arranged, that this number was
admitted, alternately, in such a manner that
each of us had one third of the whole. The sick
were indiscriminately received, and were
attended as nearly as possible with the same
care and accommodated with the same
comforts.
Neither Mr Anderson nor I ever once employed
the lancet. He lost two, I four cases; whilst out
of the other third [treated with bloodletting by
the third surgeon] thirty five patients died.”
Milne I and Chalmers I. J Epidemiol Community Health 2002;56:1a
Over 100 Years Later…
11
―During the last
decades we have
certainly bled too
little.‖
William Osler, MD
David Sackett, Gairdner-Wightman Award, March 31, 2009 (www.cebm.net)

Modern Examples of Bloodletting
Thalidomide (birth defects)
Vitamins to prevent cancer/CVD (failed)
PSA for prostate cancer (over-diagnosis)
Anti-arrhythmic drugs (higher death rate)
Hormone replacement (cancer, strokes)
Stents after myocardial infarction
Bone marrow transplantation for breast
cancer (higher death rate)
12 Thank you to Andrew Epstein

Another Story: Stents After Acute MI
13http://www.circulation.or.kr/info/case/200904/fig1.gif
http://www.indiastudychannel.com/attachments/Resources/82666-221135-Coronary%20Angiogram.jpg

Observational Findings
14 Lamas GA et al. Circulation 1995;92:1101-9
They Ran Into a Problem…
When researchers tried to organize a randomized study of the benefits of angioplasty for patients who had suffered a heart attack three days or more before, they ran into a problem. Many doctors were so convinced of the value of this procedure…that they thought it would be unethicalto assign any patients to the control group, which would get all the best medicines for this condition but not the artery-reopening procedure.
But the researchers persisted, with heavy support from the National Heart, Lung, and Blood Institute. After four years of work examining 2,166 patients, they came to an unexpected conclusion….
15 Boston Globe, December 9, 2006
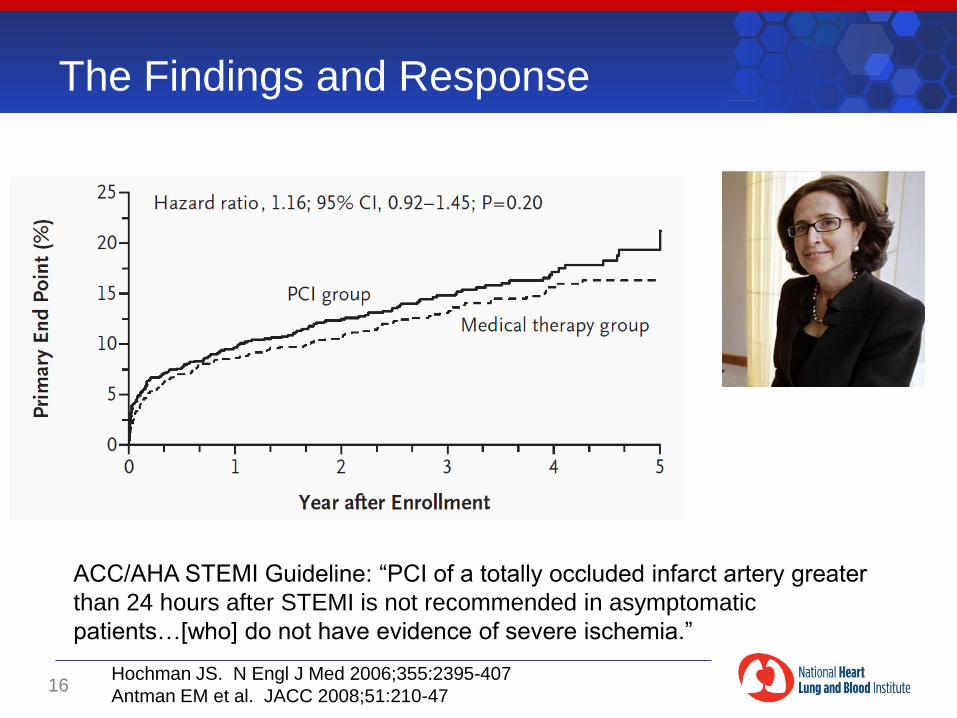
The Findings and Response
16
ACC/AHA STEMI Guideline: ―PCI of a totally occluded infarct artery greater
than 24 hours after STEMI is not recommended in asymptomatic
patients…[who] do not have evidence of severe ischemia.‖
Hochman JS. N Engl J Med 2006;355:2395-407
Antman EM et al. JACC 2008;51:210-47

High-Dose Chemotherapy and ABMT
17
―…We believe that confirmation of these results in a
prospective randomized trial is important before this therapy
can be accepted for widespread use. Many new therapies,
initially promising, fizzle. This treatment should only be
offered at major centers…and, whenever possible, [into]
randomized comparative trials…‖
Peters WP, et al. J Clinical Oncology 1993;11:1132-43

What Actually Happened
18
―… By the time Peters had organized his trial, few women
wanted to participate…[It] meant running the risk of not
getting high-dose chemo, and many had read newspaper
accounts that convinced them that the treatment was their
only chance for survival. Their doctors often agreed. One
transplanter pulled out a copy of Peters' 1993 paper. ‗I don't
see how it's even ethical to do a randomized trial,‘ he said.‖
Brownlee S. Discover Magazine 2002.

What Actually Happened; Large RCT
19
―… From the moment Peters first administered high-dose chemotherapy
until the first clinical trials were concluded, nearly 20 years passed.
During that time, hundreds of physicians practiced the unproven
treatment. An estimated 30,000 breast cancer patients suffered through
high-dose chemotherapy, only a fraction of them as part of a clinical
trial. All told, the nation spent around $3 billion paying for it, while an
estimated 4,000 to 9,000 women died not from their cancer but from the
treatment…‖
Brownlee S. Discover Magazine 2002.
Peters WP et al. J Clinical Oncology 2005;23:2191-2200

Let‘s Look at These Stories
Bloodletting
Made sense, strong professional interest
Observational impressions failed
Stakeholders favored evidence-free medicine
Long time to do a trial, long time to change
Stents after MI and HDC with BMT
Made sense, strong professional interest
Observational data failed
Stakeholders favored evidence-free medicine
Long time to do a trial, short time to change
20

Upbeat Story of Collaboration: NETT
Lung reduction surgery in emphysema (N=1218)
21 National Emphysema Treatment Trial Research Group. N Engl J Med. 2003;348:2059-73
―The National Marfan Foundation does not recommend switching from a
beta blocker to losartan as a way to manage Marfan syndrome until the trial
is completed. This is because we do not know whether losartan is clearly
better than atenolol for taking care of people with Marfan syndrome. Also, we
do not know if people with Marfan syndrome will have unwanted side effects
when they take losartan.‖
Upbeat Story of Collaboration: Marfan Syndrome
http://www.marfan.org/marfan/2408/Atenolol-vs.-Losartan-Clinical-Trial

Success Story: Prevention of MI
23 Yeh RW, et al. N Engl J Med 2010;362:2155-65

Evidence-Based Medicine Works!
24
Better hypertension control
Better cholesterol control
Selby J et al Med Care 2010;48:133-9
Contemporary Challenges…
Criteria for priorities
Public health
Scientific opportunity
Stakeholder interests: may collide
How will do affordable pragmatic trials?
When can we trust observational data?
Implementation: Will knowledge help?
What about personalized medicine?
25 Lauer MS, Collins FS. JAMA 2010;303:2182-3

Stakeholder Interests May Collide
―It is difficult to get a man to
understand something when
his salary depends upon his
not understanding it.‖
Upton Sinclair
26 I, Candidate for Governor: And How I Got Licked (1935), ISBN 0-520-08198-6; repr. University of California Press, 1994, p. 109.

So What is a Practical Trial?
―The hypothesis and study design are
developed specifically to answer the
questions faced by decision makers‖
Decision makers = patients, clinicians,
payers, policy makers
27 Tunis S, Stryer D, Clancy C. JAMA 2003;290:1624-32

What‘s the Lesion?
―Neither of the major sources of funding for
clinical research in the United States—the
NIH and the medical products industry—
has as a primary mission the goal of
ensuring that studies are performed to
address clinical questions important to
decision makers.‖
Sean Tunis, Daniel Stryer, and Carolyn Clancy
28 Tunis S, Stryer D, Clancy C. JAMA 2003;290:1624-32

An Inspiring Story
29
“It started with no funding and skepticism in some quarters
but today GISSI is recognized as an Italian achievement that
has changed cardiology treatment worldwide.”
http://eurheartj.oxfordjournals.org/content/31/9/1023.full

The GISSI Story
Trial (topic) Patients Cost (Euro millions ) Cost/Pt* (E K)
Thrombolysis 12,000 0.4 0.03
Thrombolysis and
sc heparin
13,000 4 0.2
ACE after MI 19,000 6 0.3
PUFA and Vit E 11,000 4 0.2
Statin in HF 7,000 20 3
30
*Per trial, as some were factorial designs
―Logistical Aspects‖
• All Italian cardiologists are invited to participate
• Enrollment of a broad spectrum of patients
• Clinical procedures which mimic clinical practice
• Low costs
• Immediate transfer to clinical practice (investigators see patients)
Tavazzi L et al. Am Heart J 2004;148:222-9
Practical Trial Design Tool
31 Thorpe KE et al. CMAJ 2009;180:E47
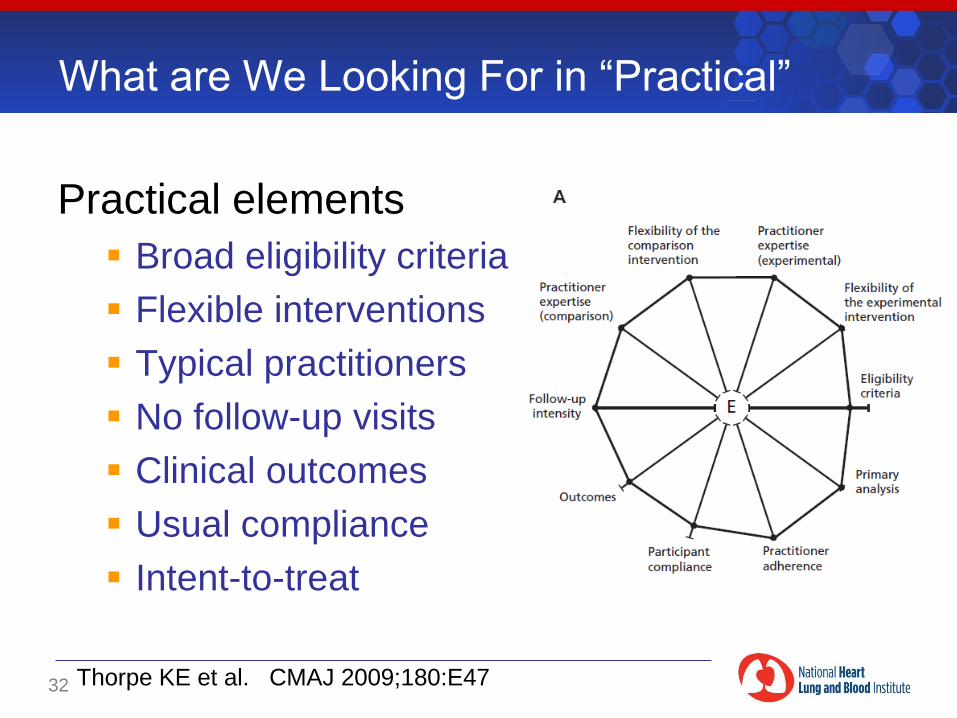
What are We Looking For in ―Practical‖
Practical elements
Broad eligibility criteria
Flexible interventions
Typical practitioners
No follow-up visits
Clinical outcomes
Usual compliance
Intent-to-treat
32 Thorpe KE et al. CMAJ 2009;180:E47
An Ongoing Example
33

How Can We Simplify and Improve Trials?
Sites and Coordinating Centers
Fit trials into practice and clinical IT
Limit case report form length
Apply metrics for performance
Operations
Decrease monitoring, use statistical analyses
Research and evaluate processes
Central IRB and standardized contracts
Design: factorial, adaptive, cluster
34 Eisenstein EL, Califf RM. Clinical Trials 2008;5:75. Menikoff J. NEJM 2010;363:1951
Back to Basics: Beware Inferior CER
35
―It was because they were brilliant
observers of humans, not
experimenters upon them, and
observation by itself provides
insufficient evidence of the value of
a treatment.‖
David Sackett
―The principle of science, the
definition, almost, is the following:
The test of all knowledge is the
experiment. Experiment is the
sole judge of truth.‖
Richard Feynman
Inferior CER: Observational data, small trials, surrogates
With thanks to Robert Califf and David Sackett
Back to Basics: Beware Inferior CER
36
―The smaller the studies, the less likely the research
findings are to be true. (Inadequate power)
The greater the financial interests and prejudices, the less
likely the research findings are to be true. (Excess bias) ‖
Ioannidis JPA. PLoS Medicine 2005;2:e124

Likelihood of Truth
37
Design Likelihood of Truth
Large, adequately powered RCT with little
bias and 1:1 pre-study odds
85%
Meta-analysis of small trials 41%
Small, well-performed phase II trial 23%
Large epidemiological study 20%
Discovery-oriented exploratory research 0.1%
Ioannidis JPA. PLoS Medicine 2005;2:e124
How Can You Support National CER?
Do the right thing! Embrace science…
That means:
Do large, simple pragmatic trials
Target evidence-free medicine
If it‘s ―unethical‖ it may be most ethical
Beware of real conflicts of interests
Create a culture in which enrollment in large,
simple trials is the norm, not the exception
Science guides medical practice
38