the brain and ms
TRANSCRIPT

1
The Brain and MS Text Overview of Video
Dr Suzi Claflin and Prof Bruce Taylor
Suzi: Today we’re going to talk about the brain and multiple sclerosis, so we’ll discuss the different parts of the brain, and how multiple sclerosis affects the brain. Bruce, I think the first thing we’d like to talk about is what are the different parts of the brain, how does it work?
Bruce: Well the brain is a very very complex structure and again I'll use the same model we used in the last thing. The brain is essentially a super computer and it’s made up of lobes, as we’ve discussed before, which look after various functions in the brain.
The frontal lobes are usually thought of as giving people their personality, and also they control the motor aspects of being able to move, you generate your ability to move or use your hand or your eyes, or your tongue for instance, all come from the area here, which we call the motor strip, which is in the frontal lobes. When you come back to the parietal lobes, they're mainly involved with sensation, things such as being able to perceive stimuli, being able to recognise left and right, those sorts of things, are all looked after by the parietal lobes. The occipital lobes, which are right next to the parietal lobes, for very good reasons, look after vision. They process your visual information as it’s coming from the eyes, and they also

2
very very much interact with the parietal lobes, so you can understand the context of what you’re seeing.
Then down the bottom of the brain are the temporal lobes, which look after your memory, but they also provide context to the other lobes. If you experience a sensation, you immediately recognise that is hot, that is cold, that is two stimuli and that feels like, and the reason why you have that is because you remember what stimuli feel like. These lobes interact and connect to each other. Then the rest of the brain, as we mentioned before, is to do with balance and also to connect the brain to the spinal cord.
Suzi: The brain controls the rest of the body, including things that we don’t think it’s controlling maybe, like breathing?
Bruce: Yes, exactly. You don’t have to think to breathe, and that’s really obviously very important. There’s a lot of other housekeeping behaviours that the body has, like regulating your temperature, regulating your blood pressure, your emotions to control your fight or flight reflex, are all done, you don’t have to think about them. They're all just done for you.
They’re controlled by different parts of the brain, and they’re probably the most primitive part of the nervous system, because they’ve evolved from animals, from birds, from dinosaurs even, have had similar means of control. As the species have developed, that’s become more complicated and also become less under our own control, it’s all become automatic.

3
Suzi: What is the brain made of?
Bruce: The brain is made of cells, like every other part of the body, but in the brain there are two major types of cells. One of which is the nerve cells themselves, which we call neurons, which are some of the largest cells in the body and they can have processes which extend out from them, from up to a metre long. The cell bodies of the nerves or the neurons, accumulate in areas which we call grey matter, that’s what gives them the grey colour.
In the white matter, you have the nerve processes, which are the axons or the processes which come out of nerve cells, which connect to other nerve cells and to muscles and to eyes, et cetera. They are sheathed in a protein which is called myelin, and myelin is white, and that’s why we talk about white matter and grey matter.
If we look in our brain model here, we can see that the grey matter tends to be on the outside, you can see the grey, and the white matter which is lighter, it's really darker pink and lighter pink, but the white matter is on the inside. The white matter is really a major switching yard, there are millions of

4
fibres going in all directions, connecting different nerve cells to each other.
Now supporting all your nerve cells, are a whole bunch of other cells, which are called glial cells. Those glial cells provide support for the neurons. If you didn't have them, you’d just have a moosh and it wouldn’t have any structure. The glial cells also produce the myelin which coats the nerves, and they’re called oligodendrocytes and then there’s another type of cells which look after your immune system within the brain.
There are three major types of nerve cells, which we’ll discuss in more detail in the later sections. But the two most important differentiations here are between neurons, which are the nerves themselves and the supporting cells which we call glial cells.
Suzi: When you’re a person who’s living with MS, what is the MS doing in the brain?
Bruce: Well, MS attacks, at least in the first part of the disease, it’ll attack the oligodendrocytes and the myelin, and it’ll strip away that insulation around axons, which the electrical impulses, which control everything in the brain, happen by. If you remove the insulation, it’s the same as removing insulation from a flex connecting your toaster to the wall. It doesn’t work quite as well. Nerve cells like to have that insulation. If you continue to remove it, and continually attack it, the nerve cell itself can die.
That results in loss of nerve cells, and the two ways that is manifest when we see it in people with MS, one is a lesion, or a plaque, which is where the immune system has attacked that particular part of the brain and caused a lesion in that

5
particular region, and then if you get a number of those over time, you lose nerve cells and then the brain itself will shrink, which we call atrophy.
Suzi: What exactly is a lesion? Is it a mass?
Bruce: No, a lesion is an area of inflammation initially, and it’s an area, we don’t know why this happens, why MS will select that particular part of the brain, spinal cord or optic nerve to attack, and leave all the rest alone.
We don’t know why that is so selective, but it causes a lesion and people often hear you talk about lesions in MS, or plaques in MS, and that’s what multiple sclerosis means, it means multiple sclerotic areas, and sclerosis just means thickening or hardening. That happens after inflammation where the repair system of the brain and the body comes in to action and produces a scar, which is the lesion we see if we look at a brain of someone under the microscope who’s got MS. Or we can see it on an MRI scan.
Suzi: So, a lesion is like a scar that’s left after inflammation?
Bruce: Yeah, you can see the inflammation itself can cause a lesion, but generally what happens is you get a big area of inflammation, and then that gets turned off by the body, then that area will shrink down in size, but is always an area of

6
absolute damage, which we call the plaque of multiple sclerosis.
So, here we have an MRI scan, which is a great way of looking at anatomy and understanding multiple sclerosis and how it affects the brain. This is a slice of someone's brain, going right through the middle, from their nose right through to the back of their head, and this is the back of their head, this is their nose. You can see certain things here in beautiful detail. These are the lips, this is the tongue, this is the top of the spinal cord, and if you remember from our previous thing, we talked about how the spinal cord connected to the brain though the brain stem, and this area here is called the brain stem.
This is the cerebellum. This is the connection between the two hemispheres of the brain, and this is taken right through the middle of the brain, and this is called the corpus callosum, which just means hard area, or corpus means body. That's where a lot of white matter travels, so the two side of the brain can talk to each other. You can see the various sulci, which are the convolutions of the brain, which is why people always say the brain looks a bit like a cauliflower. You can see that this is actually the fat underneath the skin, and this dark area is actually the skull.

7
Suzi: Where on here, I think there’s a lesion that we can see?
Bruce:
We can see several lesions actually, but this is the most obvious lesion. This is a white area, and that’s why we talk about, people talk about plaques and this is actually a plaque of MS, and you can see also, less distinctly but within the corpus callosum, there are several other lesions.
8
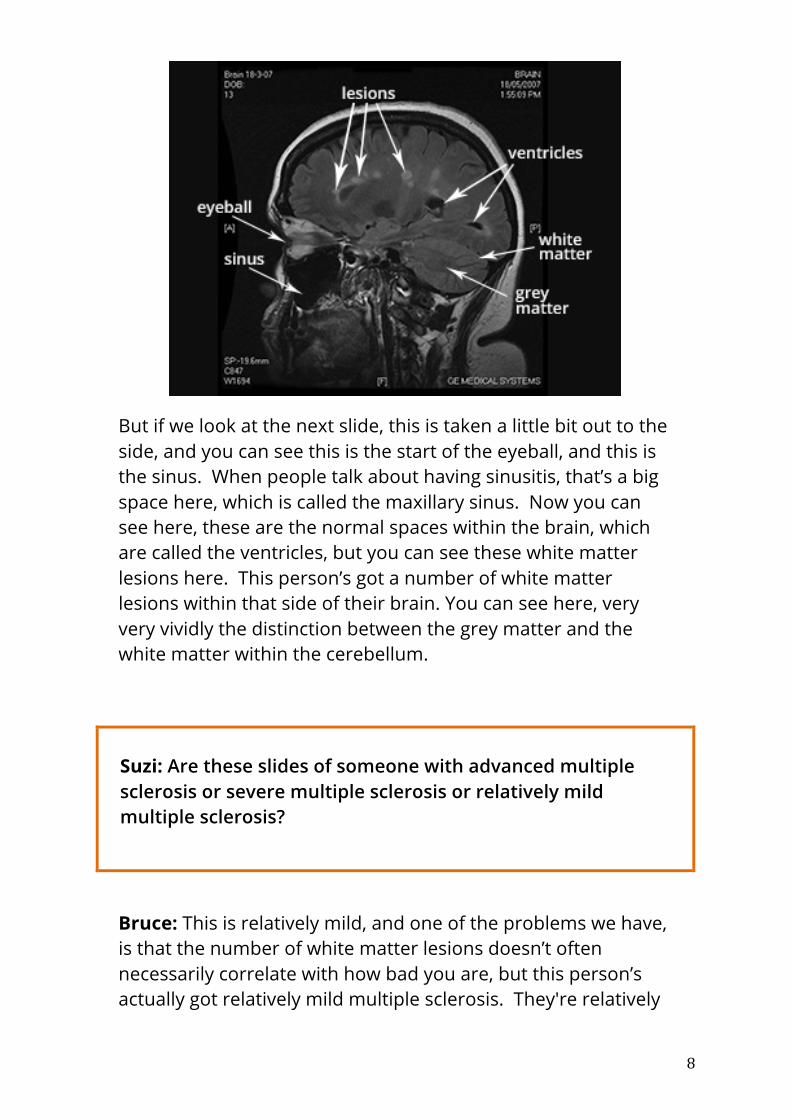
But if we look at the next slide, this is taken a little bit out to the side, and you can see this is the start of the eyeball, and this is the sinus. When people talk about having sinusitis, that’s a big space here, which is called the maxillary sinus. Now you can see here, these are the normal spaces within the brain, which are called the ventricles, but you can see these white matter lesions here. This person’s got a number of white matter lesions within that side of their brain. You can see here, very very vividly the distinction between the grey matter and the white matter within the cerebellum.
Suzi: Are these slides of someone with advanced multiple sclerosis or severe multiple sclerosis or relatively mild multiple sclerosis?
Bruce: This is relatively mild, and one of the problems we have, is that the number of white matter lesions doesn’t often necessarily correlate with how bad you are, but this person’s actually got relatively mild multiple sclerosis. They're relatively

9
young, they don’t have any specific, a lot of atrophy, so they haven’t had a lot of damage, and this is a relatively mild MS brain.
This is now taking a different way, and when you look at a scan, you look at it in multiple different ways. This is again a scan that goes through this way. This is the back and this is the front, and these are the normal spaces in the brain where the spinal fluid is made, and they’re called the ventricles. You can see those white matter lesions again, here, all around through this area. The reason why they tend to crop around here, is because there's a lot of white matter here. These are what we call periventricular lesions. They're particularly here, and they abut on to the ventricles, and that’s a very very common sight to see in MS.

10
Again, when we talk about atrophy, now this is a series of brain scans which were first taken in 1995, and the last scan was taken in 2005. Again you can see this is a slightly different way we’ve done these scans. You can see the white matter lesions, these bright white dots, and you can see these ventricles here, and the grey and white matter of the brain, again front and back.
Then we do the scan again two years later, and that lesion is less intense, it's become smaller, and it’s developing into a scar. If you come along a little bit later, this person’s got a new lesion here, a new lesion here, they've got active MS. But the thing to note here is, if you look at how big the ventricles are here and how big they are here, they're expanding. This person, because of all this inflammation they're having, is losing brain tissue.
Again, you come here, and this lesion looks bigger, there’s new lesions here, and again the ventricles look bigger. Even more so 10 years after the start of this disease, in this person you can see there is a lot of white matter damage, this is now getting subcortical change, and you can see that we’re now getting significant atrophy. Some of these lesions have turned into holes. There’s a hole there, you can see it here, that has developed because of this big lesion here, which has developed

11
since the start. That’s an area of what we call gliosis or it’s actually a hole in the brain, this person’s lost brain tissue here. You can see this is progression of MS with time.
Suzi: When we say that the ventricles have expanded, that is an example of brain atrophy?
Bruce: That’s correct. Now the other way we look for atrophy, is it’s not quite as obvious, but if you look here. The sulci or the spaces between the convolutions of the brain, you can see this is the sulcus, these are getting wider, which means the brain is shrinking down in size.
Suzi: These lesions, if a person has a lesion, do they necessarily experience symptoms from that lesion?
Bruce: No, they don’t often, and that’s one of the reasons why, when we're looking after people with multiple sclerosis we talk to them, examine them, but we’ll also do MRI scans. Because this is a great bit switching area, and the brain doesn’t necessarily experience symptoms by having lesions in that area. If you have a lesion in your optic nerve, you will lose vision generally. If you have lesion in your spinal cord, you’ll usually get problems below the level of that lesion. But often within the brain itself, you may not have any symptoms that you’ve had progression or new lesions of your multiple sclerosis. Some of these lesions here, particularly in the frontal lobe, could be totally asymptomatic.

12
Suzi: But where lesions are, does that have any impact on what your symptoms are?
Bruce: Absolutely, if you have lesions, not so much in this area, but if you have lesions within the brain stem as we were talking about here, we can very specifically tell where that lesion is, because someone might get numbness or get weakness on the side of their face. They might get double vision. We can actually very very accurately pinpoint there, because we know they've got clear manifestations.
Similarly, if you have lesions in the cerebellum, that’ll often cause ataxia, or difficulty with movement. If you get lesions within the optic nerve, it could obviously cause optic neuritis, and loss of vision, and the spinal cord can cause weakness and numbness below the level of the lesion. But up here in the brain, you can get lesions which cause symptoms, but it’s less common.
Suzi: Well I think that’s great, thank you Bruce for talking to me about it today. In this video, we talked about the brain and how it functions, and how MS impacts the brain. In the next video, we're going to delve into some of the things that Bruce talked about today, nerve cells and glial cells, how they function and how they're affected by MS.