the beers criteria - c.ymcdn.com€¢ provide a basic understanding of the beers criteria and...
TRANSCRIPT
The Beers CriteriaA Review of Rx Safety Issues in Geriatric Patients
Dane A. Higgins, M.B.A., Pharm.D.
Covington Healthcare Associates, LLC

Objectives
• Address clinical issues involving medication
use in older individuals.
• Provide a basic understanding of the Beers
Criteria and Potentially Inappropriate
Medications (PIMs).
• Identify commonly encountered PIMs and
address lifetime treatment plan issues
involving PIMs.

Aging & Medication Use
• Age-related differences in Rx effectiveness,
sensitivity and toxicity.
• Pharmacokinetic and pharmacodynamic
drug properties change with aging.
• Age-related declines in renal and hepatic
function.
• Increased sensitivity (e.g., anticholinergic
properties of Rxs).
• Rx regimen that is effective, safe and
appropriate in a 45 year old, may be highly
inappropriate in a 65 year old.

What is the Beers Criteria?
• Potentially Inappropriate Medications (PIMs)
• Identifies “High Risk” Drugs in ≥65 YO
• Includes 53 medications or medication
classes and 14 medical conditions/disease
states with caution about using specific
drugs.
• Goal of Criteria to Improve Quality of Care in
Older Individuals.
• Two Primary Purposes:
– Educational Tool
– Quality Measure

Beers Criteria as a Quality Measure
• National Committee for Quality Assurance
(NCQA)
• Healthcare Effectiveness Data and
Information Set (HEDIS)
• Pharmacy Quality Alliance (PQA)
• CMS and Medicare Part D
– Start ratings
– In 2012, “quality bonus payments” (QBPs) linked
to star ratings – 3 stars = 3%, 5 stars = 5%

History of Beers Criteria
• First published by Dr. Beers in 1991
• Updated in 1997, 2003 and 2012
• In 2012, the American Geriatrics Society
(AGS) was responsible for update.
• Interdisciplinary panel of experts in geriatric
care and pharmacotherapy.

Prevalence of PIM Use
• As many as 40% of seniors receive one or
more of the Beers Drugs, depending on care
setting.
– Medicare Part D Plans (2013) ~ 9% used PIMs.
• Adverse Health Effects of PIMs…
– 27% of adverse drug events in primary care are
preventable.
– 42% of adverse drug events in long-term care
are preventable.
– In a 2000/2001 Medical Expenditure Panel
Survey, total estimated healthcare expenditures
related to the use of PIMs was $7.2 billion.

Commonly Used PIMs
PIMs Comments
First-generation antihistamines
(e.g., hydroxyzine, promethazine,
diphenhydramine)
Highly anticholinergic. Avoid.
Antispasmodics (e.g., belladonna,
dicyclomine, hyoscyamine,
scopolamine)
Highly anticholinergic and
uncertain efficacy. Avoid.
Dipyridamole Orthostatic hypotension and more
effective alternatives. Avoid.
Nitrofurantoin Pulmonary toxicity. Not effective
with CrCl <60 mL/min. Avoid
chronic use and CrCl <60 mL/min.
Alpha Blockers (doxazosin,
prazosin, and terazosin)
Orthostatic hypotension. Avoid as
antihypertensive.
Alpha Blockers – Central
(clonidine, methyldopa, etc)
Avoid clonidine as 1st line
antihypertensive. Avoid others.

Commonly Used PIMs
PIMs Comments
Antiarrhythmic (e.g., amiodarone,
propafenone, sotalol)
Rate control better than rhythm
control in geriatrics. Not 1st line.
Digoxin over 0.125 mg/day Higher doses no more effective in
heart failure.
Nifedipine Immediate-release Hypotension. Avoid.
Spironolactone > 25 mg/day High risk of hyperkalemia. Avoid in
heart failure of CrCl < 30 mL/min.
Tertiary Tricyclic Antidepressants
(e.g., amitriptyline, doxepin > 6
mg/day, imipramine)
Highly anticholinergic, sedating,
and can cause orthostatic
hypotension. Secondary TCAs
(nortripytline) are preferred.
Antipsychotics (e.g., quetiapine,
risperidone, olanzapine,
ziprasidone)
Increased risk of stroke and
mortality in people with dementia.
Avoid in dementia.

Commonly Used PIMs
PIMs Comments
Barbiturates (e.g., butalbital,
phenobarbital)
High rate of physical dependence,
tolerance and risk of overdose at
low doses. Avoid.
Benzodiazepines (e.g., alprazolam,
lorazepam, temazepam, diazepam)
Increased sensitivity and slower
metabolism to long-acting agents.
Avoid for insomnia, agitation or
delirium. May be used in seizure
disorder, severe anxiety, etc.
Non-benzodiazepine Hypnotics
(Lunesta®, Ambien®, Sonata®)
Adverse events similar to
benzodiazepines (delirium, falls,
fractures). Minimal improvement in
sleep latency or duration.
Androgens (testosterone) Potential for cardiac problems.
Estrogens +/- Progestin Carcinogenic potential (e.g.,
endometrium, breast) and other
risks.
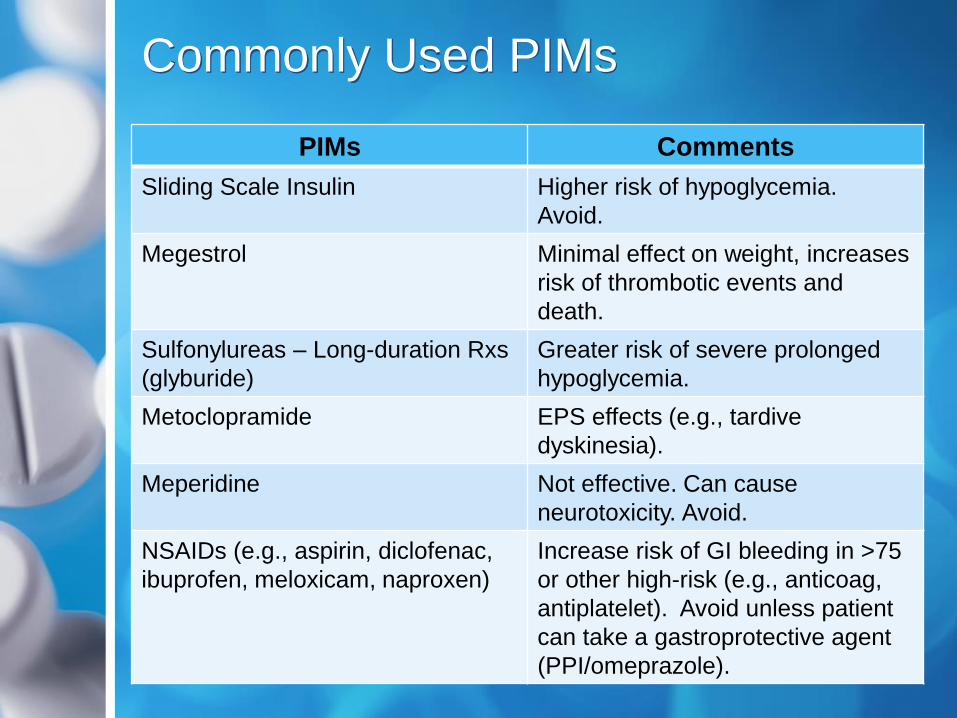
Commonly Used PIMs
PIMs Comments
Sliding Scale Insulin Higher risk of hypoglycemia.
Avoid.
Megestrol Minimal effect on weight, increases
risk of thrombotic events and
death.
Sulfonylureas – Long-duration Rxs
(glyburide)
Greater risk of severe prolonged
hypoglycemia.
Metoclopramide EPS effects (e.g., tardive
dyskinesia).
Meperidine Not effective. Can cause
neurotoxicity. Avoid.
NSAIDs (e.g., aspirin, diclofenac,
ibuprofen, meloxicam, naproxen)
Increase risk of GI bleeding in >75
or other high-risk (e.g., anticoag,
antiplatelet). Avoid unless patient
can take a gastroprotective agent
(PPI/omeprazole).

Commonly Used PIMs
PIMs Comments
Ketorolac Major increase in GI bleeding risk.
Avoid.
Pentazocine More CNS adverse events
(confusion and hallucinations) than
other opioids. Avoid.
Skeletal Muscle Relaxants (e.g.,
carisoprodol, chlorzoxazone,
cyclobenzaprine, metaxalone,
methocarbamol, orphenadrine)
Poorly tolerated and efficacy is
questionable (particularly with
chronic use). Avoid.
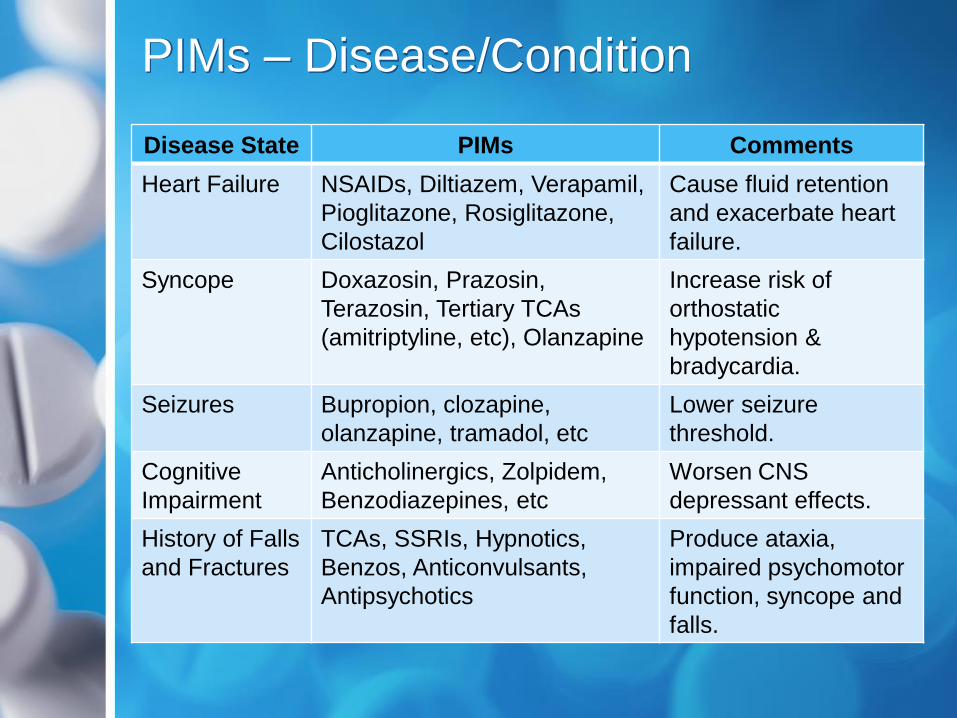
PIMs – Disease/Condition
Disease State PIMs Comments
Heart Failure NSAIDs, Diltiazem, Verapamil,
Pioglitazone, Rosiglitazone,
Cilostazol
Cause fluid retention
and exacerbate heart
failure.
Syncope Doxazosin, Prazosin,
Terazosin, Tertiary TCAs
(amitriptyline, etc), Olanzapine
Increase risk of
orthostatic
hypotension &
bradycardia.
Seizures Bupropion, clozapine,
olanzapine, tramadol, etc
Lower seizure
threshold.
Cognitive
Impairment
Anticholinergics, Zolpidem,
Benzodiazepines, etc
Worsen CNS
depressant effects.
History of Falls
and Fractures
TCAs, SSRIs, Hypnotics,
Benzos, Anticonvulsants,
Antipsychotics
Produce ataxia,
impaired psychomotor
function, syncope and
falls.

PIMs – Disease/Condition
Disease State PIMs Comments
Insomnia Pseudoephedrine,
Phenylephrine, Stimulants
Worsen insomnia.
Constipation Anticholinergics, Urinary
Incontinence Rxs, Diltiazem,
Verapamil, etc
Worsen constipation.
Avoid.
History of GI/
Duodenal
Ulcers
Aspirin (>325 mg/day) or
NSAIDs
May exacerbate or
cause ulcers.
Kidney
Disease
(Stage IV or V)
NSAIDs, Triamterene Kidney injury. Avoid.
Urinary
Incontinence
Estrogens May aggravate
incontinence.

Pocket List From AGS

Beyond Beers Criteria
• STOPP
– Screening Tool of Older Persons’ potentially
inappropriate Prescriptions
• START
– Screening Tool to Alert doctors to the Right
Treatment
– Beers Criteria focuses on prescribing drugs that
should be avoided, while START focuses on
under prescribing in the elderly (failure to use
statin in atherosclerotic disease, ACE inhibitor in
heart failure, etc)
– Study found one or more Rx omissions in 57.9%
of patients at time of hospital admission.

Beers Drugs and Life Care Plans
• Published reviews on the Beers Criteria by
nurses have suggested that practicing
nurses should use the AGS pocket list (see
previous slides) to help identify high-risk
drug use in their patients. (Fick DM. 2012 Beers Criteria Update –
How Should Practicing Nurses Use the Criteria? J Gerontological Nursing. 2012)
• Beers Criteria could be employed when
conducting a Life Care Plan….
• First Step is Identifying “PIMs”
• Modify Treatment Plan Due to PIMs
• Modification will vary based on PIM and
patient-specific medical considerations…

Beers Drugs and Life Care Plans
• Discontinue PIM/Not for Lifetime Use
– Muscle relaxants (carisoprodol, cyclobenz-
aprine, etc) – Not effective with chronic use and
major safety concerns.
– Benzos (alprazolam, diazepam, etc) – Efficacy
with chronic use is questionable. Numerous
safety concerns.
– Hypnotics (zolpidem, etc) – Chronic use
produced minimal improvement in sleep latency
and duration.
– NSAIDs: While NSAIDs are reasonable for pain
management in younger patients, risk is far
greater in older individuals.

Beers Drugs and Life Care Plans
• Convert PIM to Safer Alternative
– Amitriptyline Nortriptyline
– Long-Acting Benzo (diazepam, flurazepam)
Short-Acting Benzo (lorazepam, temazepam)
• Still risk with short-acting agents
– Meperidine Morphine, Oxycodone, etc
– Glyburide Glipizide or Glimepiride

Beers Drugs and Life Care Plans
• Dose Adjustments for PIMs
– Digoxin – If over 0.125 mg/day
– Spironolactone – If over 25 mg/day
– TCAs (e.g., amitriptyline) – If continued, a dose
reduction is often advisable on a trial basis.
– Virtually any CNS depressant from Beers could
be a target for weaning: benzos, antipsychotics
(except schizophrenia), hypnotics, muscle
relaxants, etc.
• In many cases (e.g., zolpidem, cyclobenz-
aprine), efficacy is not reduced at lower dose,
but risk of side effects are reduced.

Beers Drugs and Life Care Plans
• Add Medications
– In some instances medications may need to be
added to the treatment plan to address safety
concerns…
– NSAIDs: If chronic NSAIDs are employed in
older individuals, a proton-pump-inhibitor
(omeprazole, pantoprazole, etc) may need to be
added. Over-the-counter (OTC) PPIs can be
purchased for about $20/month.

Beers Drugs and Life Care Plans
• No Rx Change to PIM
– Beers Criteria is a Guideline, Not a Requirement
– Prescribing decisions must consider multiple
factors/issues in individual patients.
– Disagreement over some drugs. For example,
some clinicians feel that low-dose amitriptyline is
reasonable in neuropathic-related pain
management, alpha blockers are reasonable in
hypertension with co-morbid BPH, etc.
– In some cases (e.g., amitriptyline, doxazosin), if
the patient is tolerating the drug without side-
effects, a wait and see approach is reasonable (if
closely monitored and doses are low).

Dane A. Higgins, M.B.A., Pharm. D.
Covington Healthcare Associates, LLC
3800 Colonnade Pkwy, Suite 110
Birmingham, AL 35243
205-970-3939