the basics of child abuse and neglect · child maltreatment is an abusive action (commission) or...
TRANSCRIPT
THE BASICS OF CHILD ABUSE AND
NEGLECT
SARAH PASSMORE, DO

OBJECTIVES
• Understand of the incidence of abuse
• Understand of when to suspect abuse
• Understand when a report needs to be made

REPORTING
• Medical professionals are mandated reporters of suspected abuse or neglect
• A report is not a diagnosis, it is a request for further investigation based on SUSPICION
• Done “in good faith,” now presumed in Oklahoma

DEFINITION
• Child maltreatment is an abusive action (commission) or lack of action (omission) that results in morbidity or death
• Physical, Sexual
• Emotional/Psychological
• Failure to Thrive
• Neglect
• Medical Child Abuse (Munchausen Syndrome by Proxy)
• Prenatal maternal drug and alcohol abuse.

EPIDEMIOLOGY/NCANDS
2013
Child Population of reporting states 64,780,672
3,016,794 referrals (47.1 per 1,000 children)
1,837,326 screened in
Oklahoma is 63.1 per 1,000 children
OK DHS 2014 ANNUAL REPORT
67,670 children involved in investigations
14,172 confirmed victims of abuse
11,538 children in out-of-home care
1,269 adopted out of foster care system
3,823 reunited with families
CHILDREN’S DEFENSE FUND 2012
922,098 children live in Oklahoma
A child is abused or neglected every hour
A child dies before his or her first birthday every 22 hours
226,679 (24.7%) in poverty
98,058 in extreme poverty (10.7 %)
38.4 % of 2 year olds are not fully immunized
49th in per pupil expenditures

EPIDEMIOLOGY
• 62% of perpetrators are female
• Males are more common perpetrators of sexual abuse
• 10-40% of abusive parents were abused as children
• Parents who abuse have been reported from ALL ethnic, geographic, religious, educational, occupational and socioeconomic groups

CHILD PARENT
RISK FACTORS
• Colicky babies
• Developmentally delayed children
• Premature infants
• Children with learning and/or behavior problems
• Substance abuse
• Lack of education about child development
• Teenage parents
• Single parents
• Family crisis such as job loss
• Marital troubles
• Death of sibling
• Exhaustion
• Physical or mental illness in the parent

RED FLAGS
• No explanation for injury
• Multiple explanations for injury
• Implausible explanation for injury/Injury does not meet developmental stage of the child
• Delay in seeking treatment
• Unexplained apnea
• Repeated drug or toxin exposure
• Serious noncompliance with medical care
• Cold injury
• Injury resulting from discipline
• Bilateral, symmetric injuries
BEHAVIORAL CHARACTERISTICS OF ABUSED CHILDREN
• Child maltreatment can negatively impact a child’s behavior well beyond any specific event that occurs.
• These children may:
• act out, be disruptive, have “behavior problems”
• act out violently towards others, get in fights
• have sleep difficulties
• have low self esteem
• be withdrawn

BRUISES
PHYSICAL ABUSE
• Most common manifestation of PAB
• Bruising is expected in mobile kids on shins, forehead, boney prominences
• It is NOT possible to date bruises

BRUISES
• Often the result of excessive discipline
• Those that don’t cruise, don’t bruise
BRUISES
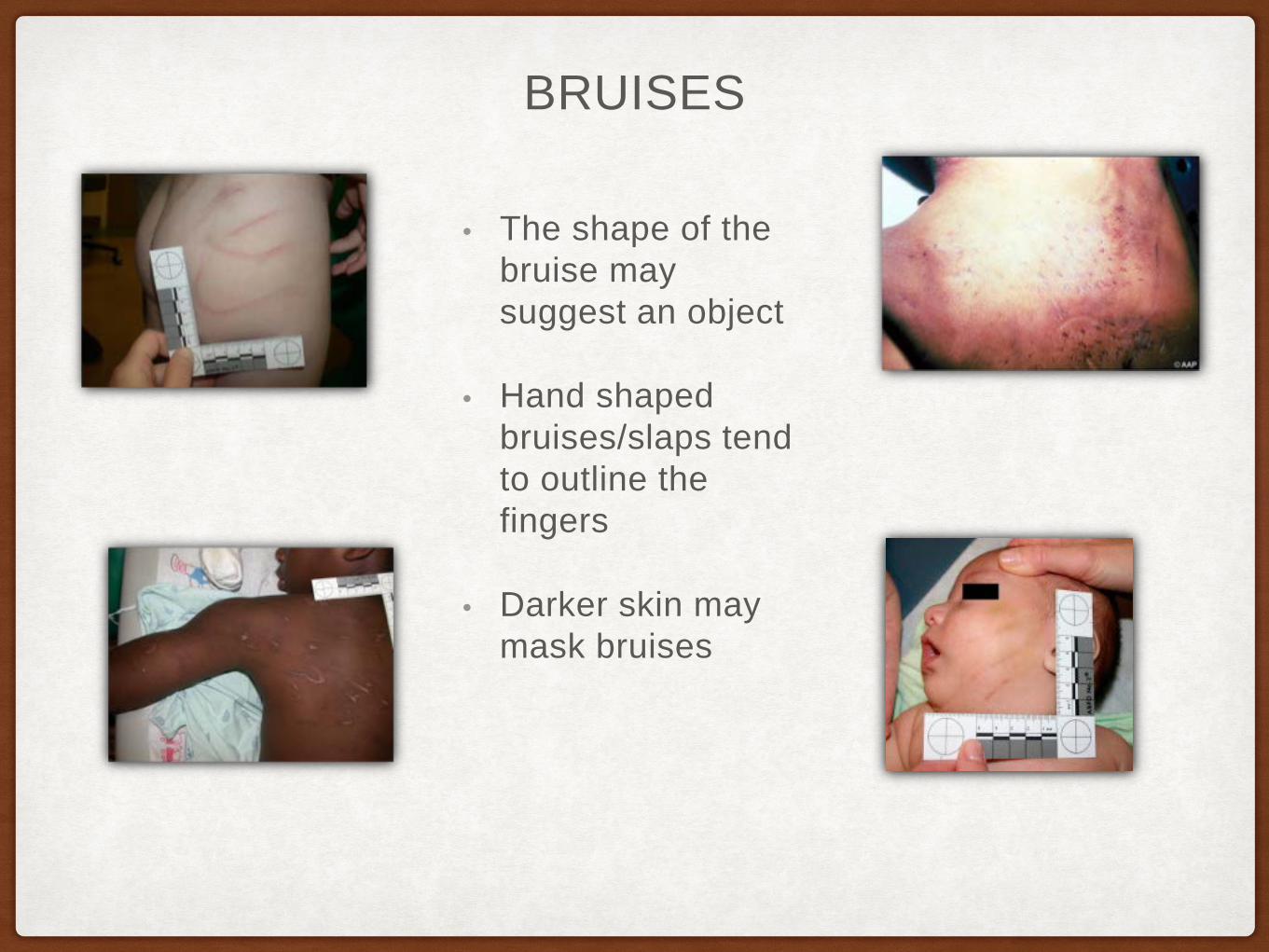
• The shape of the bruise may suggest an object
• Hand shaped bruises/slaps tend to outline the fingers
• Darker skin may mask bruises

BRUISES

BURNS
• Approximately 10% PAB involves burns
BURNS
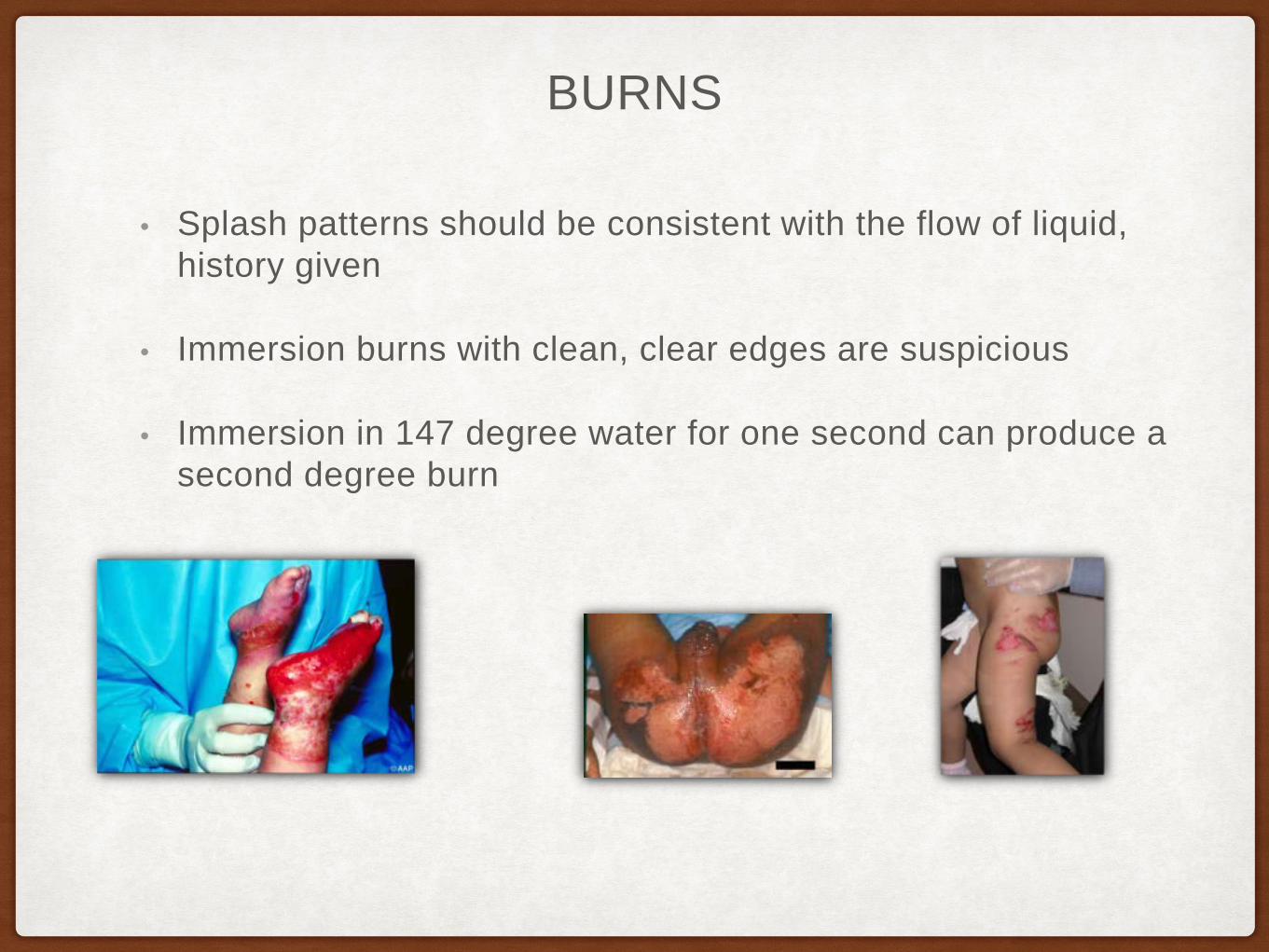
• Splash patterns should be consistent with the flow of liquid, history given
• Immersion burns with clean, clear edges are suspicious
• Immersion in 147 degree water for one second can produce a second degree burn

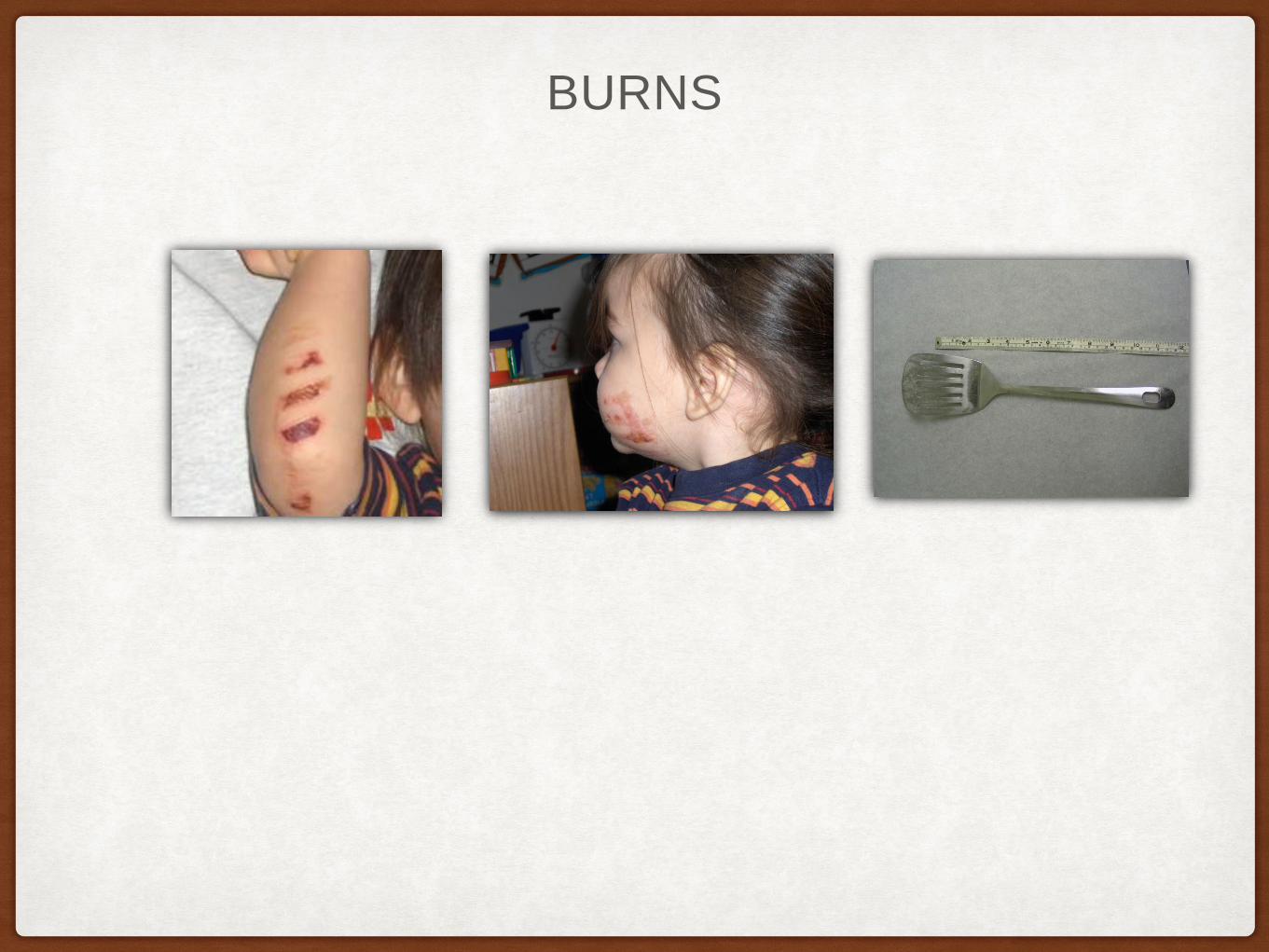
• Cigarette burns are hard to identify
• Diaper area burns, burns to back of hand are suspicious
BURNS

FRACTURES
• Multiple fractures healing at different stages indicate abuse, especially in non mobile children
• Posterior rib fractures obtained by squeezing
• Uncommon fractures without a history of trauma (i.e. vertebrae, sternum, pelvis, scapulae)

HEAD TRAUMA
• The most common cause of death from abuse is due to head trauma
• More than 95% of serious intracranial injuries in the first year are nonaccidental
• Symptoms may be vague
• A large subdural without a history of significant trauma is suspicious
• Retinal hemorrhages in 50-80%, often unilateral
• Catastrophic injury explained by simple fall is suspicious
• Can have long term sequelae

ABUSIVE HEAD TRAUMA
SEXUAL ABUSE
• How do we know? Disclosure of abuse by a child
• Normal is normal
• Significant trauma may need surgical repair
• Never use speculum on prepubertal child

WHAT TO DO IF YOU SUSPECT ABUSE
• Avoid interviewing extensively It’s OK to ask ‘how did you get your owie.’
• Treat appropriately for injury (i.e. splint, dress burn, refer)
• Make DHS referral. This can be done through hospital or clinic social worker or by calling directly
• Police may need to be involved, especially if child is not safe to go home
• If alleged SAB <72 hrs prior, needs SANE exam (forensic exam.)
PHYSICIANS ARE MANDATED REPORTERS

What we recognize as common disorders in adult medicine and psychiatry are likely the result of what
we fail to recognize or address in childhood.Dr. Vincent Felitti
Adverse Childhood Experiences and
HopeMichael Baxter, DO
Assistant Professor (Clinical)Department of Pediatrics
OU-School of Community Medicine-TU
Updates in Child and Adolescent Psychiatry The Children’s Hospital at Saint Francis
March 4th, 2016
678,932
“Abused children need Hope.”
- Me, Today.
27
Adverse childhood experiences and hope
3.8 Million

Dr. C. R. Snyder
“Hope is defined as the perceived capability to derive pathways to desired goals, and motivate
oneself via agency thinking to use those pathways.”
29
Snyder, C.R. 2002. Hope Theory: Rainbows in the Mind. Psychological Inquiry Vol 13. No 4, 249-275
Adverse childhood experiences and hope
Snyder, C. R., Harris, C., Anderson, J. R., Holleran, S. A., Irving, L. M., Sigmon, S. T., et al.(1991). The will and the ways: Development
and validation of an individual-differences measure of hope. Journal of Personality and
Social Psychology, 60, 570-585.
Hope Theory
30
Snyder, C.R. 2002. Hope Theory: Rainbows in the Mind. Psychological Inquiry Vol 13. No 4, 249-275
Adverse childhood experiences and hope

Hope Theory
31
Snyder, C.R. 2002. Hope Theory: Rainbows in the Mind. Psychological Inquiry Vol 13. No 4, 249-275
Adverse childhood experiences and hope

Pathway and
Agency
32
Goal
Adverse childhood experiences and hope
Dr. Rob Anda
“If we can predict it, we can prevent it.”
33Adverse childhood experiences and hope
Relationship of Childhood Abuse and Household Dysfunction to Many of the Leading Causes of Death in Adults Felitti, Vincent J et al.American Journal of Preventive Medicine , Volume 14 , Issue 4 , 245 - 258
http://www.childabuseqc.org/#!adverse-childhood-experiences/c12xo

Psychological Abuse
34
http://acestudy.org
Adverse childhood experiences and hope







The higher the ACEs, the higher the risks
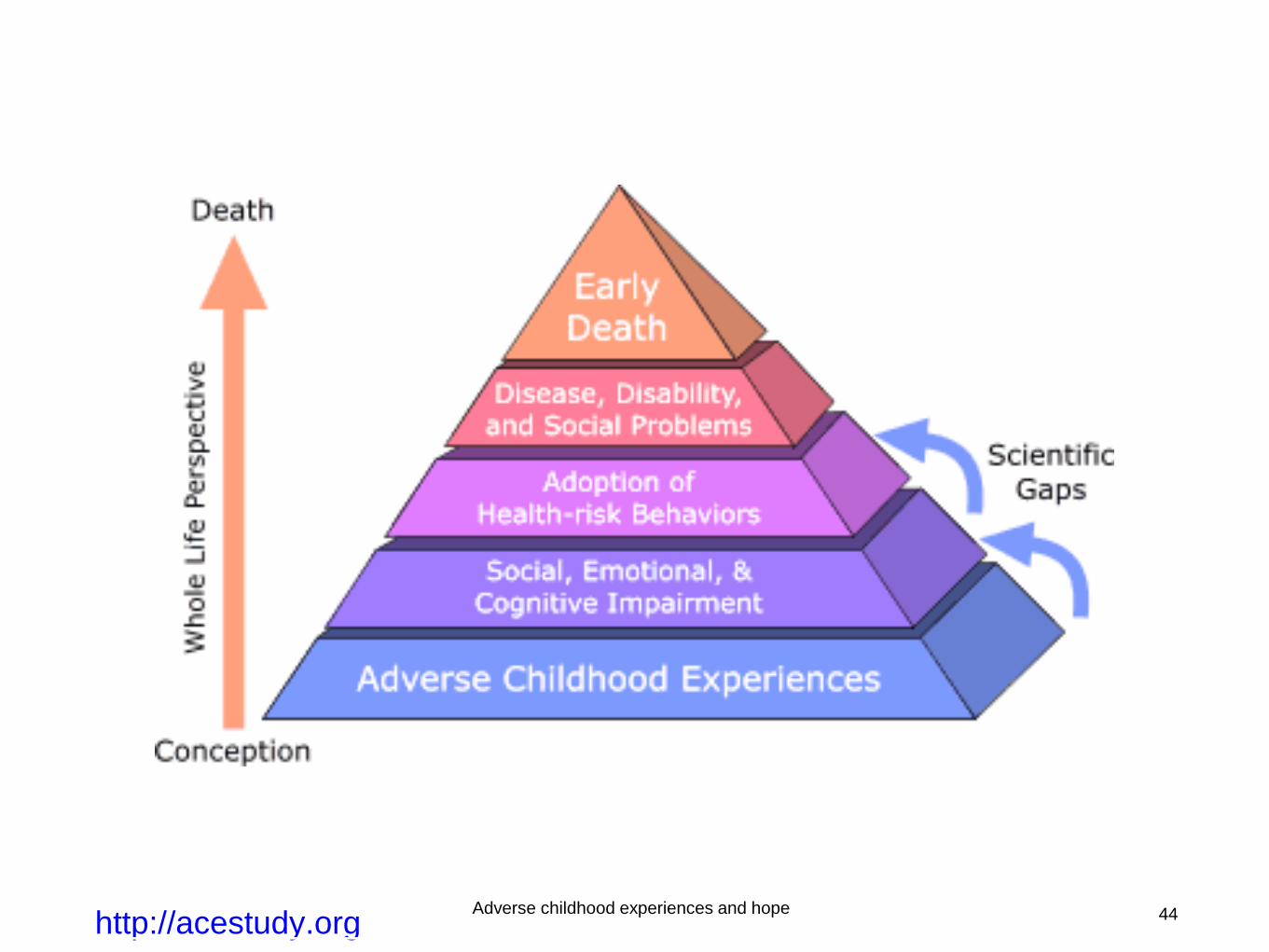

45

–Dr. C. Henry Kempe
“Our children’s future and the world’s future are one.”
46Adverse childhood experiences and hope