the attributable fraction of the lymphatic filariasis ... · lymphatic filariasis (lf) and to...
TRANSCRIPT

The Attributable Fraction of the Lymphatic Filariasis Burden to Water Resource Development and Management
Report prepared for the WHO commissioned study Burden of water-related vector-borne diseases: An analysis of the fraction attributable to components of water resources development and management. Investigators: Tobias E. Erlanger, Jennifer Keiser, Marcel Tanner, Jürg Utzinger
Swiss Tropical Institute, P.O. Box, CH-4002 Basel, Switzerland
Marcia Caldas de Castro, Burton H. Singer
Office of Population Research, Princeton University, Princeton, NJ 08544, USA
Robert Bos, Jamie Bartram and Laurence Haller
Water, Sanitation and Health (WSH/PHE), World Health Organization, Avenue Appia 20,
CH-1211 Geneva 27, Switzerland

2
Contents: Main Objective page 3 Approach page 3 Outcomes page 4 Conclusion page 5 Outlook and Perspectives page 5 Appendix 1 Search strategy and selection criteria for the
comprehensive literature review page 12 Appendix 2 Number of hits for lymphatic filariasis combined with
selected keywords in different electronic databases page 13
Appendix 3 Relevant literature to address the main research objective page 14 Appendix 4 Published review paper American Journal of
Tropical Medicine and Hygiene page 15 Appendix 5 Table summarising geographical distribution of the three
Filaria species, ecology of their vectors and environmental changes leading to increased vector densities page 36
Appendices 6.1–6.14 Key information form of all retrieved publications page 37
3
Main Objective
In order to strengthen the evidence base in support of decision-making on
different intervention options for vector-borne disease prevention and control in the
context of water resources development and management, WHO commissioned
systematic literature reviews on the association between such development and the
burden of four vector-borne diseases.
In accordance with this mandate, the main objective of work reported here was to:
strengthen and expand the current evidence-base of contextual determinants of
lymphatic filariasis (LF) and to assign and quantify attributable fractions of the disease
burden to specific components of water resources development and management.
This implies the need for (i) the definition and characterization of the contextual
determinants of LF; (ii) the compilation of critical LF statistics on a global and regional
scale (stratified according to the 14 WHO sub-regions of the world); (iii) a systematic
literature review; and (iv) preparation of an analytical report, including questions that
remained unanswered and a mapping out of directions for future work.
This report summarises the research approach taken and provides an outlook and
possible perspectives on how to move forward in view of identified research priorities.
The main findings of the systematic review can be found in appendix 4, which contains
the text of the article published in the peer-reviewed literature.
Approach For the sake of the current report, LF is defined as a communicable parasitic
disease caused by Wuchereria bancrofti, Brugia malayi or Brugia timori that can clinically
manifest itself in the form of lymphedema or elephantiasis. Other diseases caused by
Filarioidea (e.g. onchocerciasis and dracunculiasis) are not considered here.
A systematic literature review was carried out to identify all published studies that
examined the effect of water-related environmental changes on the frequency and
transmission dynamics of LF. Special consideration was given to publications that (i)
presented information on the sequential cause-and-effect relationships between water-
related environmental change, abundance of vector populations, entomological
transmission parameters, microfilaria infection prevalence and rates of clinical
4
manifestations, and/or (ii) compared .the epidemiological conditions in sites where
ecosystems had been modified by water resources development with those in
ecologically similar settings without such change. The main findings were synthesised
and formatted into a review paper (Appendix 4).
First, a schematic concept of the contextual determinants of LF was developed.
Next, the fraction of the population at risk of LF was estimated in all 76 countries that are
currently endemic for this disease. At-risk populations in rural and urban areas of all
WHO sub-regions were linked with the most recent burden of disease statistics
expressed in disability adjusted life years (DALYs). We employed the recent
classification, as presented in the appendices of the WHO World Health Report 2004,
which stratifies the world into 14 epidemiological sub-regions. At-risk populations in rural
settings were defined by people living in close proximity to irrigated agro-ecosystems in
those sub-regions where rural LF transmission occurs; in urban settings they were
defined as people lacking access to improved sanitation in those sub-regions where
urban LF transmission occurs. In the context of this report, improved sanitation systems
include facilities which are designed and maintained in a way that they do not favour the
proliferation of LF vectors. The size of the rural population was estimated by multiplying
the average population density in rural areas with the total area under irrigation in the LF
endemic countries. Statistics on urban dwellers lacking access to improved sanitation
were taken from the World Health Report 2004.
Outcomes Appendix 1 summarises the search strategy and selection criteria that we
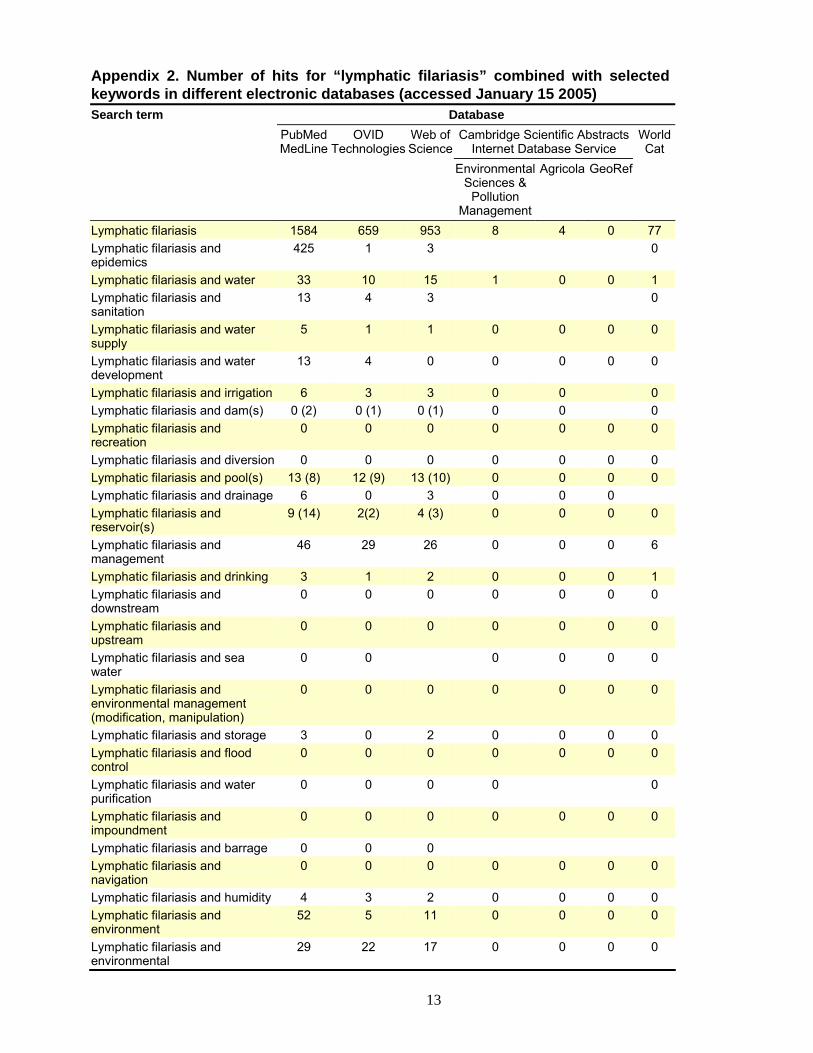
employed to address this objective. Appendix 2 shows the number of hits for different
key words derived from a set of electronically-available databases that are widely used
for literature reviews. PubMed/Medline was found to be the most comprehensive
database, as it comprised most of the literature cited in the other databases that we
screened. Our extensive literature search pertaining to the main objective of this project
yielded only 14 articles, all of which were published in the peer-reviewed literature
(Appendix 3). Two out of these 14 contain descriptive data and were therefore not
included in the systematic review article that was published in the peer reviewed
literature. The review article (Appendix 4) presents a panel that lists the population at risk
in all 76 countries endemic for LF, a figure that summarises the contextual determinants
of LF and four tables that show the main findings of vector abundance, transmission and
clinical manifestation rates. An estimate of the size of the population at higher risk due to

5
irrigation and inadequate sanitation is also presented in the article. As a general
guidance, a table that shows the geographical distribution and ecology of major LF
vectors was compiled (Appendix 5). Finally, from all selected publications, including the
ones with descriptive data, the key information (KIF) was retrieved and summarised in a
standardised format, which is presented in Appendices 6.1–6.14.
Conclusion
The objective of this study was to strengthen and expand the current evidence-
base of contextual determinants of LF, and to assign and quantify attributable fractions of
the disease burden to specific components of water resources development and
management and generally of water-related environmental change. It is part of a larger
investigation examining the effect of water resources development and management on
four vector-borne diseases, the other three being malaria, schistosomiasis and Japanese
encephalitis.
It was intended to quantify the burden of LF attributable to ecosystem change, with
special reference to the changes in local hydrology, through the use of comparative risk
assessment (CRA). Utilising counterfactual analysis, studies were required that examine
alternative scenarios, thereby describing changes in the exposure to risk factors. Hence,
an ideal study would be one that presents data in the initial steady-state (often natural)
environment, e.g. prior to the implementation of a water resources development project.
It would then describe changes that occurred during project implementation and, finally, it
would assess the impact on filarial transmission, prevalence and morbidity several years
after implementation. Unfortunately, not a single study was identified which fulfilled these
criteria. Most studies either simply quantified prevalence rates or entomological
parameters in a specific region (e.g. without differentiating between communities with
and without water resource development) or were carried out after the completion of a
water resource development project. The fact that the majority of publications are lacking
profound environmental, ecological or socio-economic data made it difficult to link
outcome measures with water-related or other risk factors.
It had been suggested that due to scarcity of detailed analyses, the adoption of
indirect methods may be required by calculation of relative risk (RR). Compared with
other diseases (e.g. schistosomiasis), the application of indirect methods to calculate RR
in the case of LF is very delicate. This is explained by the fact that prevalence rates and
morbidity of LF strongly depend on socio-economic, environmental and ecological factors.

6
To date, however, these dynamics have been poorly explored and are far from fully
understood.
A comparison between areas affected by water resources development projects
and areas with similar ecological and epidemiological characteristics but with no water
resource projects might be possible but analysis requires great care. Applying study
results from a specific site to other more distant areas with similar climatic characteristics
is even more arguable, because of small-scale heterogeneities (e.g. prevalence rates
vary between villages while climatic parameters are similar).
In view of the very few high-quality studies and the lack of a good understanding of
basic transmission dynamics of LF in relation to water resources development and
management, we conclude that it is currently not possible to calculate the population
attributable fraction of risk factors or assign and quantify attributable fractions of disease
burdens caused by LF. It was not feasible to derive DALY estimates for the 10 relevant
WHO-designated sub-regions of the world.
Outlook and Perspectives
Undoubtedly, the potential impact of water resources development and
management impact on transmission parameters of LF is considerable, but many critical
questions remain unanswered. Obviously, the dearth of LF-based studies pertaining to
water resources development and management cannot be caught up with within the next
few years.
Here we propose a selection of research priorities in the field of LF, without considering
research pertaining to clinical aspects, drug development, immunology and molecular
parasitology. In our view, some important questions include:
(1) What is the impact of water resources development and management projects on the
frequency and transmission dynamics of LF in different eco-epidemiological settings?
(2) What is the relationship between filaria transmission and infection prevalence or
infection intensity and clinical manifestation rates, particularly in regions with altered
transmission (vector species succession, transmission intensification) due to water
resources projects?
7
(3) What are the specific risk factors, including ecological, epidemiological and socio-
economic, of LF in a certain region?
(4) How big is the impact of rapid urbanisation, accompanied with lack of sufficient
sanitation facilities, water-storage, urban and peri-urban subsistence agriculture or
wastewater mismanagement on the transmission of filariae?
In the following part we further explore these research priorities 1-4 and propose
concrete strategies to tackle these questions.
(1) The fundamental question, whether or not, how and how much water resources
development and management projects impact on the transmission dynamics and
prevalence of LF remains to be answered.
On the basis of our comprehensive literature search and the identification of 14
publications, we were able to carry forward this task. By a meta-analysis of the identified
publications, we reviewed and synthesised the outcomes and produced an article that
has been published in the peer-reviewed literature.
Special attention has been paid to typical agricultural practices currently employed in the
high burden areas of LF and the predicted development of water resources (e.g. irrigated
rice agriculture). The question how water resource development and management
projects impact on LF can, however, only be answered satisfactorily when the
epidemiological parameters in affected communities and control communities are
monitored prior, during and after their implementation. In other words, environmental and
social determinants, transmission indicators and infection and disease prevalences
should be kept under rigorous surveillance for an adequate number of years.
Conceivably, the LF situation could be compared with that of malaria. This is justified on
several grounds: First, in some regions of the world the same vectors transmit both LF
and malaria (e.g. in West Africa Anopheles funestus and Anopheles gambiae). Second,
both diseases depend on similar risk factors, e.g. low socio-economic status, poor
housing conditions, and limited access to health care systems. Third, while the majority
of the global LF disease burden is concentrated in Asia – where the main vectors are
Culex ssp. – the malaria burden is currently concentrated in sub-Saharan Africa.
Importantly, Asia provides suitable environmental conditions for Anopheles species,
harbours more people than any other continent and contains the biggest proportion of
irrigated agriculture. The correct interpretation of this discrepancy will provide further

8
insight into the complex issue of “parasite-vector-environment” relations, both for LF and
malaria.
(2) The relation between transmission, the prevalence of infection and clinical
manifestations, particularly infection intensity (worm load) and LF morbidity is still not
fully understood. In areas where ecological transformations have occurred, e.g. through
the development of irrigation systems, this issue gains in importance. Such
transformations often lead to the creation of breeding sites or they diminish or alter
existing breeding habitats suitable for filaria vectors. As a consequence, the density of
vector populations fluctuates and vector species composition changes. Therefore,
environmental alterations potentially have an impact on filaria transmission. It has to be
assumed that higher filaria transmission gradually increases infection prevalence and the
worm burden. Thus, morbidity and clinical manifestation rates are expected to increase.
In the case of LF, the connection between transmission, infection and morbidity is
complex and often contradictory. Previous studies showed that people with elephantiasis
are often amicrofilaraemic while others have a high grade of infection but show no
clinical signs. The study design already described in (1) could also be applied for
investigating the connection between filaria infection and clinical disease manifestations.
Special attention has to be given to the confounding factors resulting from the fact that
regions with improved water resources facilities attract people. The influx of people from
areas with either low or high LF transmission can bias the outcome of a study.
To tackle these questions, we propose to design a research project of the following kind:
The investigation should be implemented in an area where a water resources
development project is planned. Prior to its implementation, a baseline cross-sectional
survey will assess infection prevalence, clinical manifestation rates and transmission
parameters of all filaria vectors. Further, demographic parameters such as ethnicity,
socio-economic status, and migration patterns of the affected population should be
recorded. At the next phase, designed as a cohort-study, the research will assess
infection prevalence, clinical manifestation rates and transmission parameters of all filaria
vectors during the construction and implementation of the water resources project. After
the project’s completion, the area should be further monitored and all parameters re-
assessed longitudinally for at least another five years. The outcomes of such a study
holds promise to examine and quantify how transmission parameters, infection
prevalence and clinical manifestation rates are interrelated. Further, it will expand the

9
current evidence base of adverse determinants attributable to water resources
development.
Future water resource development should include in-depth assessment of potential
health impacts, including LF. Indeed, institutionalisation of health impact assessments
(HIAs) for development projects quite generally, analogous to environmental impact
assessments, would lead to information requirements that could fill many of the data
gaps described in this review. In addition, mitigation strategies to alleviate potential
negative health impacts – of which LF might be only one component – would also be part
of the process of implementing new water projects. Introduction of monitoring and
surveillance systems proximal to such water projects would facilitate systematic
evaluation of the impact of these ecosystem interventions over time. This, in turn, would
greatly improve our understanding of the role of dams and irrigation systems in either
promoting or reducing LF transmission.
Shedding light on these dynamics is an essential step towards a complete understanding
of the disease. It will also help sustain the achievements of the Global Alliance to
Eliminate Lymphatic Filariasis (GAELF). This initiative aims to reduce filaria infection
prevalence and clinical manifestation rates to nearly zero by wide-spread chemotherapy.
Complete elimination is, however, not feasible and vector populations will be unaffected
by the GAELF. To prevent resurgence and proliferation of LF in the future, the strategy of
GAELF has to be upgraded to include a vector control component. A better
understanding of the disease is the basis for a sustainable control strategy that also
targets the vector population.
(3) For prevention and sustainable control of LF it is crucial to have a clear perception of
its risk factors. To date, the vast majority of studies focused on transmission rates,
infection prevalence or frequencies of clinical symptoms but did not define risk factors
and other determinants of LF. It is of great importance to investigate the major risk
factors for LF in the context of specific areas. As already mentioned under item (1), the
development of water resources potentially creates several new risks and aggravates
common risk factors. Other determinants also alter key parameters of LF. Taking the
construction of irrigation systems as an example, we here describe what kind of risk
factors and determinants have to be considered and how their magnitude can be
estimated:

10
Socio-economic factors
People in irrigated areas benefit from higher agricultural yields and can improve their
socio-economic status. This translates into potentially better access to health services,
increased means to purchase health services and products, and improved nutritional
status. Alleviation of poverty will, therefore, have an impact on LF morbidity. Irrigation
schemes also attract a work force which may have a different socio-economic status. In
the case of LF, studies should always consider the socio-economic status of an affected
population and differentiate groups with different levels of vulnerability, as well as the
evolution of vulnerability over time.
Population density, immigration
Areas in which irrigated agriculture is practiced or where man-made reservoirs are
created attract people and this results in higher population densities. It significantly alters
the demographic structure around water resources development projects. This may lead
to the creation of several new risk factors, including those linked to wastewater
accumulation, waste mismanagement and poor housing conditions. Furthermore,
immigrants may be more susceptible to LF infections if they come from regions with less
filaria transmission. In turn, immigrants from regions where LF is highly endemic will
introduce filariae and thus change transmission intensity in regions where LF
transmission used to be non-existent or low. Studies are needed to elucidate how higher
population densities and human movement, in connection with water resources
development, affect transmission and morbidity of LF.
Artificial breeding-sites and habitat change
Irrigation creates or changes breeding sites that are suitable for filaria vectors. New
plants and animals or the marginalisation of species can lead to shifts in vector species
composition, and can introduce new vector species. As a consequence, vector
transmission parameters change and eventually the frequency and intensity of clinical
manifestation will also change. To investigate these determinants, transmission
parameters, vector species composition, infection prevalence and clinical manifestation
rates have to be investigated prior, during and after the construction of irrigation systems.
As the transmission can vary from year to year it is crucial to monitor those LF
parameters over a period of several years.

11
Exposure
Exposure is a factor that directly influences vectorial capacity. If the human–vector
contact is altered, this affects prevalence rates as well. The factors described above also
influence human exposure to filaria-transmitting mosquitoes. Socio-economic
improvement can result in better housing conditions or an improved capacity to purchase
insecticide-treated mosquito nets. Migration of labour force, e.g. farmers, into areas
where Culex is active, can be expected to result in an increased exposure to vectors.
Vector species composition shifts can promote mosquitoes whose “time of biting activity”
and host preference is different. We suggest these factors be considered integrally in
future investigations.
(4) Currently, the connection between rapid, uncontrolled urbanisation and the
proliferation of LF is not well understood. This topic is, however, of considerable public
health significance and is expected to further gain in importance, particularly in view of
the rapid pace of urbanisation, notably in areas where LF poses high levels of risk (Asia
and sub-Saharan Africa). In shanty towns, for example, the building of small-scale
irrigation systems, the storage of water for household consumption and the lack of
improved sanitation facilities can influence the frequency and transmission dynamics of
LF. Due to rapid environmental transformation and population growth, peri-urban settings
are considered to be particularly challenging for health research and planning. Our
systematic review underscores the need to assess the importance and magnitude of
urban LF and we suggest this had best be achieved by the following study design:
First, infection prevalence and morbidity of LF can be assessed by means of cross-
sectional studies carried out in various urban settings, e.g. in shanty towns, areas with
subsistence agriculture and in inner cities. Second, breeding-sites of filaria vectors
should be defined and the mechanics of their creation described. Third, all important risk
factors and determinants should be assessed.
Tackling these three issues will lead to a better understanding of the dynamics and the
contextual determinants of LF in relation to water resources development and
management, infection, morbidity and urbanisation. Findings from these studies will form
an important basis for the design and implementation of LF-control strategies, more
appropriate planning of water resources development and management projects and the
incorporation of effective health safeguards in urban planning and development.

12
Appendix 1: Search strategy and selection criteria for our comprehensive literature review First, a literature search with special emphasis on research findings published over the past 25 years was carried out using the National Library of Medicine’s PubMed database, OVID Technologies (WebSPIRS 5.02), Cambridge Scientific Abstracts Internet Database Service and Thomson ISI (previously known as Institute for Scientific Information). With special consideration of potential bias of research findings during the DDT era, we also included published work between 1945 and 1975. PubMed/Medline contains citations published mostly from 1966 to the present, whereas Thomson ISI database dates back to 1945. The following keywords were employed to search the above-mentioned databases and websites: “lymphatic filariasis” in combination with “malaria”, “epidemics”, “water”, “sanitation”, “water supply”, “water development”, “irrigation”, “dam(s)”, “recreation”, “diversion”, “pool(s)”, “drainage”, “water reservoir(s)”, “water management”, “drinking water”, “downstream”, “upstream”, “sea water”, “environmental management” (“modification”, “manipulation”), “water storage”, “flood control”, “water purification”, “impoundment”, “barrage”, “navigation”, “humidity”, “environment” and “environmental”. Second, this search was complemented with an iterative proceeding in which we consistently reviewed reference lists of all those publications that were of relevance to address our main objective. The bibliographies of all these recovered manuscripts were retrieved again and the searching strategies repeated until no new information was forthcoming. Third, we also performed computer-aided searches of the websites of the following organisations and institutions: World Health Organisation (WHO), Food and Agriculture Organisation of the United Nations (FAO), World Bank, Centers for Disease Control and Prevention (CDC, Atlanta), online catalogues of the University of Basel and Princeton University. The yields of these searches were found to be meagre. Third, dissertation abstracts and unpublished documents (‘grey literature’) were reviewed. Dissertation abstracts were searched in following databases (accessed on 23.12.2004): - www.google.com - ProQuest Digital Dissertations (http://wwwlib.umi.com/dissertations). - Wageningen Dissertation Abstracts (http://www.agralin.nl/wda/). - Index of Theses. A comprehensive listing of abstracts by universities in Great Britain and Ireland (http://www.theses.com/). - COPAC union online catalogue of the members of the Consortium of University Research Libraries (CURL) (http://www.copac.ac.uk/). - Cambridge Scientific Abstracts Internet Database Service: (http://www.lib.ecu.edu/erdbs/csa.html). - M25 Consortium of Academic Libraries (http://www.m25lib.ac.uk/). - The Unicorn Online Catalogue (WEBCAT) of the London School of Hygiene and Tropical Medicine (http://193.63.251.23/uhtbin/cgisirsi). - IRIS Interdisciplinary Online-Databases (www.libiris1.ict.ac.uk). - Library Online Catalogue IDS Basel/Bern (http://aleph.unibas.ch). - University of Chicago, Center for Research Libraries, Foreign Doctoral Dissertations (http://wwwcrl.uchicago.edu/content.asp). - University of Berkeley Digital Library (http://sunsite.berkeley.edu/Libweb/). For this search we employed the same keywords as described above for the peer-reviewed literature search. Through these databases no useful additional data could be found. The peer-review literature and dissertation abstract search made it clear that in this field of research only a small number of studies were done and even fewer published. Since the “grey literature” is mostly not listed in any database it cannot be retrieved remotely by electronic search-engines.
13
Appendix 2. Number of hits for “lymphatic filariasis” combined with selected keywords in different electronic databases (accessed January 15 2005) Search term Database PubMed
MedLineOVID
TechnologiesWeb of Science
Cambridge Scientific Abstracts Internet Database Service
World Cat
Environmental Sciences &
Pollution Management
Agricola GeoRef
Lymphatic filariasis 1584 659 953 8 4 0 77 Lymphatic filariasis and epidemics
425 1 3 0
Lymphatic filariasis and water 33 10 15 1 0 0 1 Lymphatic filariasis and sanitation
13 4 3 0
Lymphatic filariasis and water supply
5 1 1 0 0 0 0
Lymphatic filariasis and water development
13 4 0 0 0 0 0
Lymphatic filariasis and irrigation 6 3 3 0 0 0 Lymphatic filariasis and dam(s) 0 (2) 0 (1) 0 (1) 0 0 0 Lymphatic filariasis and recreation
0 0 0 0 0 0 0
Lymphatic filariasis and diversion 0 0 0 0 0 0 0 Lymphatic filariasis and pool(s) 13 (8) 12 (9) 13 (10) 0 0 0 0 Lymphatic filariasis and drainage 6 0 3 0 0 0 Lymphatic filariasis and reservoir(s)
9 (14) 2(2) 4 (3) 0 0 0 0
Lymphatic filariasis and management
46 29 26 0 0 0 6
Lymphatic filariasis and drinking 3 1 2 0 0 0 1 Lymphatic filariasis and downstream
0 0 0 0 0 0 0
Lymphatic filariasis and upstream
0 0 0 0 0 0 0
Lymphatic filariasis and sea water
0 0 0 0 0 0
Lymphatic filariasis and environmental management (modification, manipulation)
0 0 0 0 0 0 0
Lymphatic filariasis and storage 3 0 2 0 0 0 0 Lymphatic filariasis and flood control
0 0 0 0 0 0 0
Lymphatic filariasis and water purification
0 0 0 0 0
Lymphatic filariasis and impoundment
0 0 0 0 0 0 0
Lymphatic filariasis and barrage 0 0 0 Lymphatic filariasis and navigation
0 0 0 0 0 0 0
Lymphatic filariasis and humidity 4 3 2 0 0 0 0 Lymphatic filariasis and environment
52 5 11 0 0 0 0
Lymphatic filariasis and environmental
29 22 17 0 0 0 0

14
Appendix 3. Relevant literature to address our main research objective (in inverse chronological order) Smith A. The transmission of bancroftian filariasis on Ukara Island, Tanganyika II. The
distribution bancroftian microfilaraemia compared with the distribution hut-haunting mosquitoes and their breeding-places. Bulletin of Entomology Research. 1955;46:437-444.
Jordan P. Filariasis in the lake province of Tanganyika. East African Journal. 1956
Jun;33(6):237-42. Basu PC. Filariasis in Assam state. Indian Journal of Malariology. 1957;11:293-308. Partono F, Pribadi PW, Soewarta A. Epidemiological and clinical features of Brugia timori in a
newly established village. Karakuak, West Flores, Indonesia. American Journal of Tropical Medicine and Hygiene. 1978;27(5):910-5.
Samarawickrema WA, Kimura E, Spears GF, Penaia L, Sone F, Paulson GS, Cummings RF.
Distribution of vectors, transmission indices and microfilaria rates of subperiodic Wuchereria bancrofti in relation to village ecotypes in Samoa. Transactions of the Royal Society of Tropical Medicine and Hygiene. 1987;81(1):129-35.
Rajagopalan PK, Panocker KN, Das PK. Control of malaria and filariasis vectors in south
India. Parasitology Today. 1987;3(8):233-40. Raccurt CP, Lowrie RC Jr, Katz SP, Duverseau YT. Epidemiology of Wuchereria bancrofti in
Leogane, Haiti. Transactions of the Royal Society of Tropical Medicine and Hygiene. 1988;82(5):721-5.
Amerasinghe FP, Ariyasena TG, 1991. Survey of Adult Mosquitos (Diptera, Culicidae) During
Irrigation Development in the Mahaweli Project, Sri-Lanka. J Med Entomol 28: 387-393. Hunter JM. Elephantiasis: a disease of development in north east Ghana. Social Science and
Medicine. 1992;35(5):627-45; discussion:645-9. Gad AM, Feinsod FM, Soliman BA, Nelson GO, Gibbs PH, Shoukry A. Exposure variables in
bancroftian filariasis in the Nile Delta. Journal of the Egyptian Society of Parasitology. 1994;24(2):439-55.
Appawu MA, Baffoe-Wilmot A, Afari EA, Nkrumah FK, Petrarca V. Species composition and
inversion polymorphism of the Anopheles gambiae complex in some sites of Ghana, west Africa. Acta Trop. 1994 Feb;56(1):15-23.
Dzodzomenyo M, Dunyo SK, Ahorlu CK, Coker WZ, Appawu MA, Pedersen EM, Simonsen
PE (1999). Bancroftian filariasis in an irrigation project community in southern Ghana. Tropical Medicine and International Health. 4(1):13-8.
Appawu MA, Dadzie SK, Baffoe-Wilmot A, Wilson MD. Lymphatic filariasis in Ghana:
entomological investigation of transmission dynamics and intensity in communities served by irrigation systems in the Upper East Region of Ghana. Tropical Medicine and International Health.2001;6(7):511-6.
Supali T, Wibowo H, Ruckert P, Fischer K, Ismid IS, Purnomo, Djuardi Y, Fischer P. High
prevalence of Brugia timori infection in the highland of Alor Island, Indonesia. American Journal of Tropical Medicine and Hygiene. 2002;66(5):560-5.

15
Appendix 4. Review article published in the American Journal of Tropical Medicine and Hygiene 73(3), 2005, pp. 523-533 EFFECT OF WATER RESOURCE DEVELOPMENT AND MANAGEMENT ON LYMPHATIC FILARIASIS, AND ESTIMATES OF POPULATIONS AT RISK TOBIAS E. ERLANGER1, JENNIFER KEISER1, MARCIA CALDAS DE CASTRO2, ROBERT BOS3, BURTON H. SINGER4, MARCEL TANNER1 AND JÜRG UTZINGER1 1 Swiss Tropical Institute, Basel, Switzerland 2 Geography Department, University of South Carolina, Columbia, South Carolina, USA 3 Water, Sanitation and Health, World Health Organization, Geneva, Switzerland 4 Office of Population Research, Princeton University, Princeton, New Jersey, USA
ABSTRACT
Lymphatic filariasis (LF) is a debilitating disease overwhelmingly caused by Wuchereria bancrofti, which is transmitted by various mosquito species. Here, we present a systematic literature review with the following objectives: (i) to establish global and regional estimates of populations at risk of LF with particular consideration of water resource development projects, and (ii) to assess the effects of water resource development and management on the frequency and transmission dynamics of the disease. We estimate that, globally, 2 billion people are at risk of LF. Among them, there are 394.5 million urban dwellers without access to improved sanitation, and 213 million rural dwellers living in close proximity to irrigation. Environmental changes due to water resource development and management consistently led to a shift in vector species composition and generally to a strong proliferation of vector populations. For example, in World Health Organization (WHO) sub-regions 1 and 2 mosquito densities of the Anopheles gambiae complex and An. funestus were up to 25-fold higher in irrigated areas when compared with irrigation-free sites. Although the infection prevalence of LF often increased after the implementation of a water project, there was no clear association with clinical symptoms. Concluding, there is a need to assess and quantify changes of LF transmission parameters and clinical manifestations over the entire course of water resource developments. Where resources allow, integrated vector management should complement mass drug administration, and broad-based monitoring and surveillance of the disease should become an integral part of large-scale waste management and sanitation programs, whose basic rationale lies in a systemic approach to city, district, and regional level health services and disease prevention. INTRODUCTION
People living in tropical and sub-tropical countries have long suffered under the yoke of lymphatic filariasis (LF). This chronic parasitic disease is of great public health and socio-economic significance and is currently endemic in 80 countries/territories of the world.1--3 LF accounts for serious disfiguration and incapacitation of the extremities and the genitals and causes hidden internal damage to lymphatic and renal systems.4--6 Disease, disability, and disfiguration are responsible for a loss of worker productivity, significant treatment costs and social stigma.7,8 At present, the global burden of LF is estimated at 5.78 million disability adjusted life years (DALYs) lost annually.9 Hence, its

16
estimated burden is almost 3.5-fold higher than that of schistosomiasis and approximately one seventh of that of malaria.9 LF is caused by Wuchereria bancrofti, Brugia malayi and B. timori, with > 90% of cases attributable to W. bancrofti.1 Transmission occurs through various mosquito species, primarily Culex (57%), followed by Anopheles (39%), Aedes, Mansonia, and Ochlerotatus. Detailed information on the geographical distribution of the most important LF vectors can be found elsewhere.2 More than 60% of all LF infections are concentrated in Asia and the Pacific region, where Culex is the predominant vector. In Africa, where an estimated 37% of all infections occur, Anopheles is the key vector.2
In 1993, the World Health Organization (WHO) declared LF to be one of six eliminable infectious diseases.10 After several years of preparation and endorsement by the World Health Assembly in 1997, the Global Programme to Eliminate Lymphatic Filariasis (GPELF) was initiated in 1998.11 Large-scale operations were launched in 2000, alongside the forging of a worldwide coalition, the Global Alliance to Eliminate Lymphatic Filariasis, which is a free and non-restrictive partnership forum. WHO serves as its secretariat and is being reinforced by an expert technical advisory group.12--14 GPELF’s goal is to eliminate the disease as a public health problem by 2020. It mainly relies on mass drug administration using albendazole plus either ivermectin or diethylcarbamazine (DEC). At the end of 2003, approximately 70 million people were treated and 36 countries had an active control program in place.14
Sustained political and financial commitment and rigorous monitoring and surveillance are essential elements of the global program, as otherwise LF could re-emerge since a small fraction of the population will continue to carry microfilaria. Furthermore, the vector population is unlikely to be significantly affected by GPELF. Employing a mathematical modeling approach, it was shown that vector control programs, in addition to mass drug administration would substantially increase the chances of meeting GPELF’s ambitious target.15 Indeed, some of the most successful control programs in the past demonstrate that an integrated approach, readily adapted to specific eco-epidemiological settings, was a key factor for controlling and even eliminating LF.16--19
In rural areas undergoing ecological transformations, particularly due to the construction of irrigation schemes and dams, new breeding sites suitable for filaria vectors are created.16,20 As a consequence, the transmission dynamics of LF is expected to change. In Africa, where Anopheles transmit malaria and filaria, the estimated surface area of 12 million ha under irrigation in 1990 is estimated to increase by one third until 2020.21 Rapid and uncoordinated urbanization often leads to new habitats for filaria vectors.22,23 Especially poor design and lack of maintenance of infrastructures for drainage of sewage and storm-water, waste-water management, water storage, and urban subsistence agriculture can facilitate the proliferation of mosquitoes, including those transmitting filaria. Although the proportion of urban dwellers in the least developed countries was only 27% in 1975, it rose to 40% in 2000 and is predicted to further increase. Nearly 50% of the world’s urban population is concentrated in Asia. Currently, the annual growth rate in Asian cities is 2.7%.24 This implies that in the future, an increasing number of habitats with organically polluted water will be available for Culex vectors.
The objectives of the systematic literature review presented in this paper were (i) to assess the current size of the population at risk of LF with particular consideration of water resource development and management, both in rural and urban settings, and (ii)

17
to assess the effect of these ecological transformations on the frequency and transmission dynamics of LF. Our working hypothesis was that environmental changes resulting from water resource development and management adversely affect vector frequencies, filaria transmission, prevalence of infection, and clinical occurrence of LF. These issues are of direct relevance for GPELF and evidence-based policy-making, and for integrated vector management programs and optimal resource allocation for disease control more generally. MATERIALS AND METHODS
Contextual determinants and estimation of population at risk in endemic countries. As a first step, we outlined the contextual determinants of LF transmission in a simplified flow chart (Figure 1). For regional estimates of populations at risk of LF, we used the recent classification set forth in the appendices of the annual World Health Report of WHO, which stratifies the world into 14 epidemiological sub-regions.9 For estimation of population fractions at risk of LF due to water resource development and management, we adopted setting-specific definitions. Hence, for rural areas we considered those people at risk of LF who live in close proximity to irrigated agro-ecosystems, employing data sources from the Food and Agricultural Organization (FAO; http://www.fao.org). We followed a similar approach as in our preceding work with an emphasis on the malaria burden attributable to water resource development and management.25 In fact, the size of the rural irrigation population was estimated by multiplying the average population density in rural areas by the total area currently under irrigation in LF-endemic countries/territories.
In urban settings the size of the population at risk of LF was defined by the proportion that currently lacks access to improved sanitation. Country-specific percentages of urban dwellers without access to improved sanitation were taken from the World Health Report 2004.9 Justification for this indicator is derived from the following experiences. First, there is evidence that, besides common water-borne diseases, lack of access to clean water and improved sanitation increases the risk of acquiring vector-borne diseases.23,26,27 As will be shown in our review and has been noted before, LF transmission is spurred by rapid urbanization in the absence of accompanying waste management and sanitation facility programs.28-32 Second, a large-scale campaign built around chemotherapy and improved sanitation proved successful to control LF in the Shandong province, People’s Republic of China.33 Third, Durrheim and colleagues recently suggested that chronic parasitic diseases, including LF, could be utilized as viable health indicators for monitoring poverty alleviation, as the root ecological causes of these health conditions depend on poor sanitation, inadequate water supply and lack of vector control measures.27
Search strategies and selection criteria. With the aim of identifying all published studies that examined the effect of water resource development and management on the frequency and transmission dynamics of LF, we carried out a systematic literature review. Particular consideration was given to publications that contained specifications on (i) entomological transmission parameters, abundance of vector populations, microfilaria infection prevalence and rates of clinical manifestations as a result of water resource development, and (ii) studies that compared sites where environmental
18
changes occurred with ecologically similar settings where no water resource developments were implemented.
As a first step, we performed computer-aided searches using the National Library of Medicine’s PubMed database, as well as BIOSIS Previews, Cambridge Scientific Abstracts Internet Database Service and ISI Web of Science. We were interested in citations published as far back as 1945. The following keywords (medical subject headings and technical terms) were used: “lymphatic filariasis” in combination with “water”, “water management”, “reservoir(s)”, “irrigation”, “dam(s)”, “pool(s)”, “sanitation”, “ecological transformation”, and “urbanization”. No restrictions were placed on language of publication.
In a next step, the bibliographies of all recovered articles were hand-searched to obtain additional references. In an iterative process, this approach was continued until no new information was forthcoming.
Dissertation abstracts and unpublished documents (‘grey literature’) were also reviewed. Dissertation abstracts were searched in online databases, i.e., ProQuest Digital Dissertations, and the Unicorn Online Catalogue (WEBCAT) of the London School of Hygiene and Tropical Medicine.
Finally, online databases of international organizations and institutions, namely WHO and FAO of the United Nations, and the World Bank, were scrutinized, adhering to the same search strategy and selection criteria explained above. RESULTS
Contextual determinants. The contextual determinants of LF can be subdivided into three broad categories, namely (i) environmental, (ii) biological, and (iii) socio-economic (Figure 1). They act on different temporal and spatial scales, adding to the complexity of the local LF eco-epidemiology.
In the first category, LF transmission is mainly determined by climatic factors and the formation or disappearance of suitable breeding sites for the vector. Breeding sites can be either natural or man-made, and their productivity exhibits strong heterogeneity, even on a small scale, which in turn governs filarial transmission dynamics.
In rural settings, the most prominent man-made breeding sites are water bodies created by irrigation systems and dams. Here, the weight of environmental determinants is strongly associated with biological factors, notably vector and parasite species, and various socio-economic factors such as human migration patterns, access to, and performance of, health systems, and individual protective measures.
In urban areas, artificial breeding sites are often created by waste-water mismanagement, resulting from poor sanitation systems in private dwellings and industrial units, or the absence of them entirely. Here, biological factors shape the epidemiology of LF after environmental changes have occurred, and socio-economic factors strongly interact with the environmental determinants. The local quality of domestic and industrial waste-water management, access to clean water and improved sanitation, and the construction of roads and buildings depend on the socio-economic status of specific sub-populations.

19
Mass-treatment with
filariacides
Poverty alleviation
Figure 1. Contextual determinants of lymphatic filariasis
Environmental changes due to water-resource development and management
Environmental Factors
Urban Industrial waste-water (mis)-management
Domestic water storage
Construction of roads & buildings Local sewerage systems
Rural
Agriculture & irrigation
Large hydroelectric dam construction
Small dams & barrages for agriculture &
domestic use Water supply & sanitation
Biological Factors Socio-economic Factors
Human
Population density
Sex, age, ethnicity & immunity
Exposure
Parasite Population
density
Species & strain
Survival
Mosquito Population
density
Species & strain
Insecticide resistance
Longevity
Poverty
Health systems
Knowledge, attitudes & practices
Immigration & emigration
Intervention Mass-treatment with filariacides
Poverty alleviation
Climate
Integrated vector management
Intervention

20
Endemic countries/territories. Table 1 shows estimates of populations at risk of LF for all the countries/territories where the disease is currently endemic. Only politically independent countries were listed (n = 76). Hence, the populations at risk of French Polynesia, New Caledonia, Réunion, and Wallis and Futuna, which belong to France, and American Samoa, which belongs to the United States of America, were assigned to the geographically closest independent states. Timor-Leste, which recently became independent, is also included. However, no estimates for at-risk populations are currently available for the following LF-endemic countries: Cambodia, Cape Verde, Lao People’s Democratic Republic, Republic of Korea, Solomon Islands, and Sao Tome and Principe. In view of relatively small population sizes living in these countries, neglecting at-risk population of LF there, only marginally influences estimates on regional and global scales. Table 1. Estimates of population at risk in all lymphatic filariasis (LF)-endemic countries/territories of the world, stratified into WHO epidemiological sub-regions (population at risk of LF in thousands. Africa WHO sub-region 1a (24 countries)
Angola (10,423), Benin (6,736), Burkina Faso (12,963)b, Cameroon (9,338), Cape Verde (n.d.), Chad (6,216), Comoros (768)b, Equatorial Guinea (89), Gabon (896), Gambia (1,235), Ghana (6,200)b, Guinea (8,336), Guinea-Bissau (1,253), Liberia (34), Madagascar including Reunionc (15,841), Mali (11,329), Mauritius (12)d, Niger (10,416), Nigeria (121,901), Sao Tome and Principe (n.d.), Senegal (9,247), Seychelles (81), Sierra Leone (890), Togo (1,182)b
WHO sub-region 2a (14 countries) Burundi (1,112), Central African Republic (765), Congo (3,396), Côte d’Ivoire (14,253), Democratic Republic of the Congo (22,481), Ethiopia (3,534), Kenya (10,108), Malawi (11,948), Mozambique (15,336), Rwanda (3,355)e, Uganda (23,399), United Republic of Tanzaniaf (14,421), Zambia (9,980), Zimbabwe (10,816)
The Americas WHO sub-region 4 (6 countries)
Brazilg (3,569)h, Costa Ricag (83)h, Dominican Republic (1,854)h, Guyana (623)h, Surinameg (< 4)i, Trinidad and Tobagog (< 13)h
WHO sub-region 5 (1 country) Haiti (6,078)b
Eastern Mediterranean WHO sub-region 7 (3 countries)
Egyptf (2,446)b, Sudan (8,302)h, Yemen (100)k
South-East Asia WHO sub-region 11 (3 countries)
Indonesia (27,046)h [B. malayi: 27,046, B. timori: 3,900]l, Sri Lanka (9,900)b, Thailandm (10,116)k [B. malayi: 7,791]k
WHO sub-region 12 (6 countries) Bangladesh (93,984)h, India (494,374)h [B. malayi:190,718]h, Maldives (< 3)n, Myanmar (28,000)b, Nepal (1,359)h, Timor-Leste (778)i [B. timori: 778]i
Western-Pacific WHO sub-region 13 (1 country)
Brunei Darussalam (40)o
WHO sub-region 14 (18 countries) Cambodia (n.d.), China (925,979)h [B. malayi: 63,906]h, Cook Islands including French Polynesiac (248)k, Federated States of Micronesia (109)k, Fiji including Wallis and Futunac (854)k, Kiribati (88)k, Lao People’s Democratic Republic (n.d.), Malaysiag (2,736)h [B. malayi: 2,736]h, Niue (2)k, Papua New Guinea (3,000)p, Philippines (23,800)b [B. malayi: 23,800]b, Republic of Korear (n.d.), Samoaf including American Samoac (248)k, Solomon Islandsr (n.d.), Tonga (104)k, Tuvalu (11)k, Vanuatuf including New Caledoniac (422)k, Viet Nam (12,288)h

21
n.d.: no data currently available) a Except Mauritius percentages of the population at risk from Lindsay & Thomas (2000),59 re-calculated with
recent figures from United Nations (2004)60 b Weekly Epidemiological Record (2004)14 c Réunion, French Polynesia, Wallis and Futuna, and New Caledonia belong to France; American Samoa belongs
to the United States of America d WHO (2002)61 e For Rwanda the same “at-risk” percentage as for Burundi was taken f A significant reduction in prevalence and intensity of microfilaria has recently been recorded in the United
Republic of Tanzania, Egypt, Samoa and Vanuatu3 g In Brazil, Costa Rica, Suriname, Trinidad and Tobago, and Malaysia smaller endemic foci have been
eliminated3 h Percentage of people at risk in 1990 taken from Michael et al. (1996),62 re-calculated with recent figures from
United Nations (2004)60 i Pan American Health Organization (2002)63 k Weekly Epidemiological Record (2003)64 l Supali et al. (2002)39 m Thailand has recently eliminated filaria transmission3 n People at risk estimated < 1%13 o It has been assumed that Brunei Darussalam has the same percentage of people at risk as Malaysia in 1995 as
described by Michael et al. (1996)62 p Kazura & Bockarie (2003)65 r Korea and the Solomon Islands using diverse control strategies have eliminated transmission3
People at risk of LF at global and regional scale. We estimate that approximately half of all people currently living in LF-endemic countries are at risk of the disease, which translates to approximately 2 billion. This is considerably higher than the 1-1.2 billion estimates put forth in the literature.1,2,11 The difference is largely explained by at-risk estimates for China. In urban areas, there are 394.5 million at risk of LF due to lack of access to improved sanitation. This is almost twice the estimated size in rural areas, namely 213 million, which is attributed to living in close proximity to irrigated agriculture. The largest percentages in terms of LF burden, as expressed in DALYs lost (52%), people at risk (29%), size of the population at risk due to proximity to irrigated land (69%), and lack of improved sanitation (33%) are in WHO sub-region 12. This sub-region includes Bangladesh, India, Maldives, Myanmar, Nepal and Timor-Leste (Table 2).
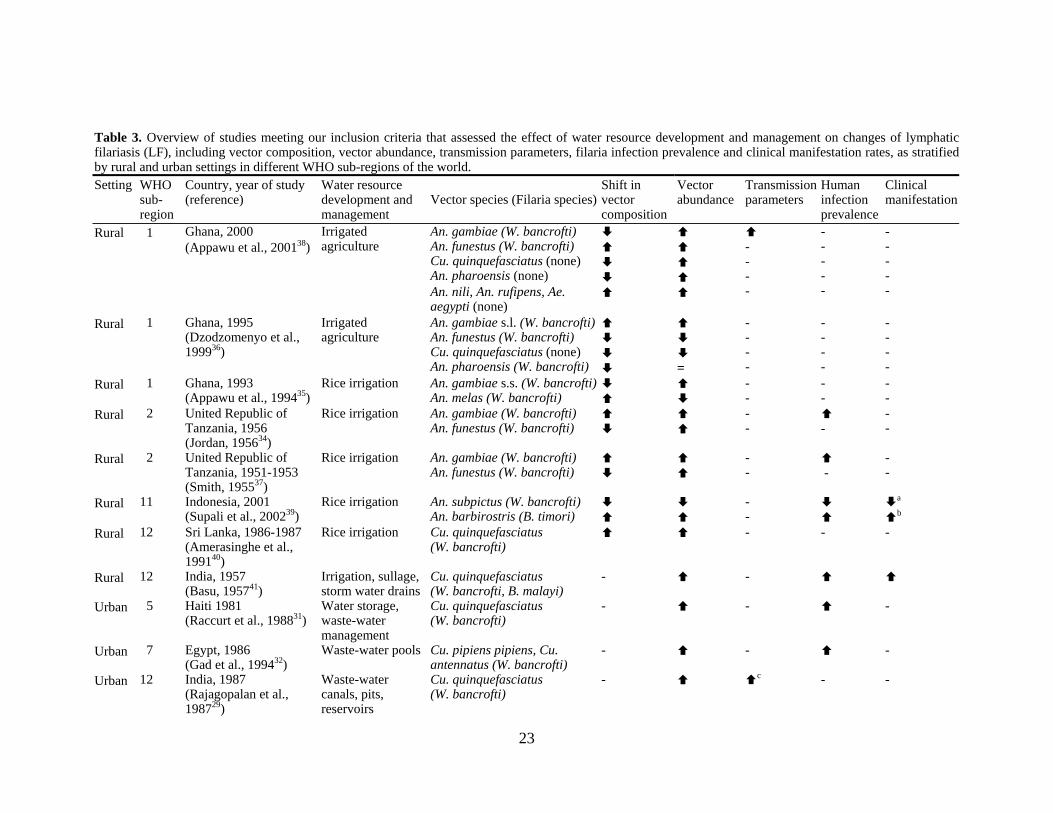
Studies identified and qualitative overview. Overall, 12 studies fulfilled the selection criteria of our literature review. These studies were all published in the peer-reviewed literature, that is, in specialized entomology, parasitology and/or tropical medicine journals. None of the work retrieved from electronic databases other than PubMed or ISI Web of Science was deemed of sufficient quality to justify study inclusion.
Table 3 summarizes the main findings of the selected studies, stratified by rural and urban settings. As a common theme, LF vector composition frequencies shifted in all settings. Water resource developments favored An. gambiae, An. funestus, An. barbirostris, Culex quinquefasciatus, Cu. pipiens pipiens, Cu. antennatus and Aedes polynesiensis, but disfavored An. pharoensis, An. melas, An. subpictus and Ae. samoanus. Transmission parameters were higher in ecosystems altered by water resource projects, and clinical disease manifestation rates often elevated.

22
Table 2. Current global and regional estimates of lymphatic filariasis (LF), including studies identified in our systematic literature review, disability adjusted life years (DALYs), total population, population at risk, population living in proximity to irrigated areas, and urban population without access to improved sanitation (n.d.: no data currently available)
WHO sub-regiona
Studies identified
DALYs in 2004 caused by LF (103)a
Total population in LF-endemic countries (x 103)b
Population at risk of LF (x 103) (from Table 1)
Population in LF-endemic countries living in proximity to irrigated areas (x 103)
Urban population in LF-endemic countries without access to improved sanitation (x 103)a
1 3 976 284,551 235,382c 574g 38,445k
2 2 1,035 312,344 144,903 305 25,956 4 0 9 193,892 6,147 306 25,570l
5 1 1 8,326 6,078 <1 1,561 7 1 122 125,551 10,847 1,646 2,265 9 0 1 n.d. n.d. n.d. n.d. 11 1 242 302,781 47,062d 8,262 31,212 12 3 2,977 1,287,945 618,496d 147,894h 131,157
13 0 0 358 40 <1 n.d. 14 1 411 1,565,246 970,589d, e, f 54,034i 176,791m
Total 12 5,777 4,079,995 2,039,548 213,021 394,511 a Source: World Health Report 20049 b Source: United Nations Urbanization Prospects – The 2003 Revisions60 c Without Cap Verde, and Sao Tome and Principe d In all countries both endemic for W. bancrofti and B. malayi or B. timori “population at risk” from the predominant filaria species was taken e Without Cambodia, Lao People’s Democratic Republic, Republic of Korea, and Solomon Islands f China has considerably reduced LF transmission, therefore those figures are likely to be significantly smaller g Without Equatorial Guinea and Seychelles h Without Maldives and Timor-Leste i Without Cook Islands, Federated States of Micronesia, Kiribati, Niue, Papua New Guinea, Samoa, Solomon Islands, Tonga, Tuvalu, and Vanuatu k Without Liberia, Sao Tome and Principe, and Seychelles l Without Trinidad and Tobago m Without Federated States of Micronesia, Malaysia, Tonga, and Tuvalu
23
Table 3. Overview of studies meeting our inclusion criteria that assessed the effect of water resource development and management on changes of lymphatic filariasis (LF), including vector composition, vector abundance, transmission parameters, filaria infection prevalence and clinical manifestation rates, as stratified by rural and urban settings in different WHO sub-regions of the world. Setting WHO
sub- region
Country, year of study (reference)
Water resource development and management
Vector species (Filaria species)Shift in vector composition
Vector abundance
Transmission parameters
Human infection prevalence
Clinical manifestation
Rural 1 Ghana, 2000 (Appawu et al., 200138)
Irrigated agriculture
An. gambiae (W. bancrofti) An. funestus (W. bancrofti) Cu. quinquefasciatus (none) An. pharoensis (none) An. nili, An. rufipens, Ae. aegypti (none)
- - - -
- - - - -
- - - - -
Rural 1 Ghana, 1995 (Dzodzomenyo et al., 199936)
Irrigated agriculture
An. gambiae s.l. (W. bancrofti)An. funestus (W. bancrofti) Cu. quinquefasciatus (none) An. pharoensis (W. bancrofti)
=
- - - -
- - - -
- - - -
Rural 1 Ghana, 1993 (Appawu et al., 199435)
Rice irrigation An. gambiae s.s. (W. bancrofti)An. melas (W. bancrofti)
- -
- -
- -
Rural 2 United Republic of Tanzania, 1956 (Jordan, 195634)
Rice irrigation An. gambiae (W. bancrofti) An. funestus (W. bancrofti)
- -
-
- -
Rural 2 United Republic of Tanzania, 1951-1953 (Smith, 195537)
Rice irrigation An. gambiae (W. bancrofti) An. funestus (W. bancrofti)
- -
-
- -
Rural 11 Indonesia, 2001 (Supali et al., 200239)
Rice irrigation An. subpictus (W. bancrofti) An. barbirostris (B. timori)
- -
a
b
Rural 12 Sri Lanka, 1986-1987 (Amerasinghe et al., 199140)
Rice irrigation Cu. quinquefasciatus (W. bancrofti)
- - -
Rural 12 India, 1957 (Basu, 195741)
Irrigation, sullage, storm water drains
Cu. quinquefasciatus (W. bancrofti, B. malayi)
- -
Urban 5 Haiti 1981 (Raccurt et al., 198831)
Water storage, waste-water management
Cu. quinquefasciatus (W. bancrofti)
- - -
Urban 7 Egypt, 1986 (Gad et al., 199432)
Waste-water pools Cu. pipiens pipiens, Cu. antennatus (W. bancrofti)
- - -
Urban 12 India, 1987 (Rajagopalan et al., 198729)
Waste-water canals, pits, reservoirs
Cu. quinquefasciatus (W. bancrofti)
- c - -

24
Urban 14 Samoa, 1978-1979 (Samarawickrema et al., 198730)
Man-made breeding sites, water storage
Ae. polynesiensis (W. bancrofti) Ae. samoanus (W. bancrofti)
- -
- -
: increase in sites where water-related change occurred; : decrease in sites where water-related change occurred; =: no change
a Genital lymphedema b Elephantiasis c Except “number of infective larvae per mosquito” which was decreasing Table 4. Absolute and relative change in abundance of different filaria vectors in areas where water resources development and management (WRDM) occurred, compared to similar control sites without WRDM Country, year of study (reference)
Type of change
Vector species Control site WRDM occurred Absolute and relative change in abundance
Number % Number % Number Factor An. gambiae s.l. 756 87.7 1,256/1,831 81.9/73.1 +500/+1,075 1.7/2.4 An. funestus 48 5.6 254/471 16.5/18.8 +206/+423 5.3/9.8 Cu. quinquefasciatusa 51 5.9 0/128 0/5.1 -51/+77 dis./2.5 An. pharoensisa 2 0.2 0/27 0/1.1 -2/+25 dis./13.5
Ghana, 2000 (Appawu et al., 200138)
Irrigated agriculture (site 1/site 2)
An. nilia, An. rufipensa and Ae. aegypti
5 0.6 24/47 1.6/1.9 +19/+42 4.8/9.4
An. gambiae s.l. 15 12 141 77 +126 9.4 An. funestus 101 82 40 22 -61 0.4 Cu. quinquefasciatusa 5 4 0 0 -5 dis.
Ghana, 1995 (Dzodzomenyo et al., 199936)
Irrigated agriculture
An. pharoensis 3 2 3 1 0 1 An. gambiae s.s. 27/17 96/94 50 100 +23/+33 1.9/2.9 Ghana, 1993
(Appawu et al., 199435) Rice irrigation (site 1/site 2) An. melasa 1/1 4/6 0 0 -1/-1 dis.
Cu. quinquefasciatus 209 48.3 467 79.8 +258 2.2 Sri Lanka, 1986-1987 (Amerasinghe et al., 199140)
Rice irrigation Cu. pseudovishnuia 224 51.7 118 20.2 -106 0.5
Ae. polynesiensis – – – – Samoa, 1978-1979 (Samarawickrema et al., 198730)
Man-made breeding sites, water storage
Ae. samoanus – – – –
An. gambiae 29 96.7 714 99.6 +685 24.6 United Republic of Tanzania, 1956 (Jordan, 195634)
Rice irrigation An. funestus 1 3.3 3 0.4 +2 3
An. gambiae 2,057 99.9 3,959 99.7 +1,902 1.9 United Republic of Tanzania, 1951-1953 (Smith, 195537)
Rice irrigation An. funestus 2 0.1 29 0.3 +27 14.5
dis.: disappearance of vector after WRDM; : increase; : decrease a not filaria transmitting

25
Vector densities. In total, seven studies investigated either the shift of LF vector composition frequencies or the change in vector abundance, as shown in Table 4. In two study sites in Ghana and one in the United Republic of Tanzania, composition frequencies of An. gambiae increased in irrigated sites compared to An. funestus.34--36 In turn, the relative dominance of An. gambiae was found to be smaller in irrigated areas in the Upper East region of Ghana and in the United Republic of Tanzania.37,38
In absolute numbers (i.e., mosquito counts), changes manifested themselves more prominently. In all settings where water resource developments were implemented, 1.7--24.6 times more An. gambiae were caught when compared to control sites. Similar numbers were found for An. funestus. Another common LF vector in Africa, namely An. melas, could not maintain itself in irrigated areas. Hence, this species disappeared. Most likely, it was replaced by the strongly proliferating An. gambiae s.s. population.35 In Indonesia, An. subpictus was exclusively found in areas without irrigation and An. barbirostris, a typical rice-field breeder, proliferated in villages with irrigated paddies.39
In urban areas on Upolu Island (Samoa), domestic water-storage and waste accumulation provided suitable breeding sites for Ae. polynesiensis, which in turn became the predominant vector in those areas. On the other hand, Ae. samoanus seemed to favor less populated areas where the relative abundance of Ae. polynesiensis was small.30 High numbers of Culex vectors were found in urban areas dominated by wastewater mismanagement and domestic water storage.29,31,32
Transmission parameters. Table 5 summarizes the five studies that assessed the
impact of water resource development and management on transmission parameters. Three studies were carried out in irrigation schemes,36,38,40 one study evaluated the impact of water mismanagement in the face of urbanization,30 and one study was undertaken after a water management control program had been launched.29 Overall, it was found that irrigation, wastewater mismanagement, water storage, or waste accumulation generally lead to increased biting rates, higher transmission potentials, and a higher proportion of vectors infective or infected with microfilaria.
In east Ghana, the annual biting rate (188 versus 299), the annual infective biting rate (0.5 versus 7.7), the annual transmission potential (0.5 versus 13.8), and the percentage of infective An. gambiae (0.3% versus 2.5-3.3%) were notably higher in irrigated villages compared with control villages.38 This study also found a higher percentage of infective An. funestus (0% versus 1.3%) and a higher worm load per infective vector (1.0 versus 1.8) when compared with the non-irrigated villages. A different study that assessed the prevalence of infective filaria in vectors in irrigated villages in southern Ghana recorded even higher fractions of infective An. gambiae (8%) and An. funestus (2%).36 In Sri Lanka, the geometric mean of female Cu. quinquefasciatus per man-hour was 1.6 times higher after the implementation of a large irrigation system.40
An integrated, community-based bancroftian filariasis and malaria control program was carried out in the first half of the 1980s in urban Pondicherry, India, which aimed at transmission reduction by simultaneous implementation of biological, chemical and physical vector control measures.29 Source reduction by means of environmental management was given high priority. It comprised of draining water-bodies, deweeding, and sealing of tanks and cisterns. Regarding biological control, larvivorous fish were released in permanent water bodies. Larvicides and oil were used as chemical methods, and physical control measures included application of polystyrene expanded

26
beads in wells. Within five years, the annual biting rate for W. bancrofti-transmitting Cu. quinquefasciatus decreased from 26,203 to 3,617, the number of infective bites per person per year decreased from 225 to 22, and the annual transmission potential decreased from 450 to 77. On the other hand, the worm load increased during the program from 2.0 to 3.5.
The effect of urbanization on transmission parameters of LF has been documented in Samoa. In areas affected by ecosystem transformation, the biting density per man per hour (26 versus 8), the fraction of infected (2.2% versus 1.7%) and infective (0.4% versus 0.3%) Ae. polynesiensis were greater than in areas without ecosystem transformation. On the other hand, biting density per man per hour (67 versus 33) and the percentage of infected (0.5% versus 0.2%) and infective (0.2% versus 0.04%) Ae. samoanus were found to be smaller.30 Filarial prevalence and clinical manifestation rates. Infection prevalence and clinical manifestations were assessed in seven and two studies, respectively. Table 6 points out that water resource developments had a strong effect on microfilaria infection prevalence. In six settings, prevalence rates were between 0.5% and 19% higher (median: 7%) compared with control areas.
In 2002, Supali and colleagues39 found that in Indonesian villages with irrigated rice agriculture, An. barbirostris, was responsible for B. timori transmission. The infection prevalence of B. timori among villagers was 6%, while W. bancrofti infections were not found. As many as 7% of all people were diagnosed with leg elephantiasis, which was associated with brugian filariasis. In irrigation-free villages, the main vector was An. subpictus and human filarial infection prevalence was 12%, but both An. barbirostris vectors and B. timori filaria were absent. Clinical symptoms appeared as genital lymphedema in 5% of all people.
The most dramatic impact of a water resource development on LF was found in villages of the United Republic of Tanzania a half-century ago. Microfilaria prevalence in two villages with irrigated rice plantations were 11% and 19% higher compared with two nearby villages where no irrigation systems had been constructed.34
In a north Indian area served by irrigation, infection prevalence for W. bancrofti was found to be 0.5% and disease manifestation 1.5% higher compared with a similar setting without irrigation. Close by, in another irrigated plot, but inhabited by people of a different ethnic origin, microfilaria prevalence was 9% greater. Disease manifestations, on the other hand, were almost at the same level (-0.5%).41
Very high W. bancrofti infection prevalence in the population of Leogane, Haiti (39% and 44%) could be attributed to wastewater discharge by factories located in the city. Infection prevalence in control districts without wastewater pools were much lower (27%).31 High prevalence (17%) in a town in the Egyptian Nile delta was due to sewage ponds of public facilities (prevalence of control site: 12%).32 On Samoa, in contrast, in areas affected by human settlements, the prevalence of W. bancrofti infections was 1.1% smaller than in control areas.30 DISCUSSION Previous studies have shown that the establishment, operation and poor maintenance of water resource development projects and the process of rapid and uncoordinated urbanization have a history of facilitating a change in the frequency and transmission

27
Table 5. Transmission parameters of different filaria vectors in areas where water resource development and management (WRDM) occurred compared to control areas without WRDM Country, year of study (Reference)
Type of change Transmission parameters of different filaria vectors Control site WRDM occurred Relative change
Annual biting rate of An. gambiae and An. funestus 188 299 1.6 Annual infective biting rate of An. gambiae and An. funestus
0.5 7.7 15.4
Worm load of An. gambiae and An. funestus 1.0 1.8 1.8 Annual transmission potential of An. gambiae and An. funestus
0.5 13.8 27.6
Infective An. gambiae 0.3% 3.3%/2.5% 11/8.3
Ghana, 2000 (Appawu et al., 200138)
Irrigated agriculture (site 1/site 2)
Infective An. funestus 0% 0%/1.3% n.a. Infective An. gambiae - 8% - Infective An. funestus - 2% - Infected An. gambiae - 27% -
Ghana, 1995 (Dzodzomenyo et al., 199936)
Irrigated agriculture
Infected An. funestus - 16% - Sri Lanka, 1986-1987 (Amerasinghe et al., 199140)
Rice irrigation Geometric mean female Cu. quinquefasciatus per man-hour
4.6 7.4 1.6
Annual biting rate of Cu. quinquefasciatus 26,203 3,617 0.1 Annual infective biting rate of Cu. quinquefasciatus 225 22 0.1 Worm load of Cu. quinquefasciatus 2.0 3.5 1.8
India, 1979-1985 (Rajagopalan et al., 198729)
Vector control program
Annual transmission potential of Cu. quinquefasciatus 450 77 5.8 Biting density per man hour of Ae. polynesiensis 8 26 3.3 Infected Ae. polynesiensis 1.7% 2.2% 1.3 Infective Ae. polynesiensis 0.3% 0.4% 1.3 Biting density per man hour of Ae. samoanus 67 33 0.5 Infected Ae. samoanus 0.5% 0.2% 0.4
Samoa, 1978-1979 (Samarawickrema et al., 198730)
Man-made breeding sites, water storage
Infective Ae. samoanus 0.2% 0.04% 0.2 n.a. = not applicable

28
Table 6. Filaria prevalence and frequencies of clinical manifestations in areas where water resources development and management (WRDM) occurred compared to similar areas without WRDM Country, year of study (reference) Type of WRDM Filaria vector or clinical
symptoms Control site WRDM occurred Change in absolute
terms W. bancrofti 12% 0% Absence B. timori 0% 6% +6% Genital lymphedema 5% 0% Absence
Indonesia, 2001 (Supali et al., 200239)
Rice irrigation
Elephantiasis 0% 7% +7% Egypt, 1986 (Gad et al., 199432)
Areas around large cesspit / small cesspit
W. bancrofti 12% 17%/7% +5%/-5%
Haiti 1981 (Raccurt et al., 198831)
Wastewater area/area with water storage
W. bancrofti 27% 39%/44% +12%/+17%
Samoa, 1978-1979 (Samarawickrema et al., 198730
Man-made breeding sites, water storage
W. bancrofti 5.3% 4.2% -1.1%
Mixed infection of B. malayi and W. bancrofti (ratio 74:26)
5%/2% 5.5%/12% +0.5%/+9% India, 1957 (Basu, 195741)
Rice irrigation, sullage and storm-water drains in two sites (site 1/site 2) Genital lymphedema and
elephantiasis 3.5%/3% 5%/2.5% +1.5%/-0.5%
United Republic of Tanzania, 1956 (Jordan, 195634)
Rice irrigation W. bancrofti
7% 26% +19%
United Republic of Tanzania, 1951-1953 (Smith, 195537)
Rice irrigation W. bancrofti
12% 23% +11%

29
dynamics of vector-borne diseases.16,20,22,23 However, detailed analyses on the contextual determinants are sparse.42--44 In recent attempts to fill some of these gaps, we systematically reviewed the literature and estimated the current magnitude of urban malaria in Africa45 and examined the effect of irrigation and large dams on the burden of malaria on a global and regional scale.25 Here, we extended our preceding work from malaria to LF, with an emphasis on the effect of water resource development and management, and estimates of at-risk populations.
It is important to note that estimates of populations at risk of LF, as presented in Table 1, differ considerably according to the source of publication. Also, some countries/territories were highly successful in lowering filaria transmission over the past 10-20 years (e.g., China) and therefore care is needed in the interpretation of at-risk population. Our estimate of 2 billion might thus be a significant overestimation.1--3 The term “at-risk” raises problems with its definition, because in most countries where transmission has been interrupted, the population is still likely to face the risk of re-emerging LF epidemics as parasites and vector species continue to be present and environmental conditions are suitable for transmission.
Our population estimates in LF-endemic countries regarding proximity to irrigated areas (i.e., 213 million) are rather conservative. Irrigated areas often attract people and thus the population density is usually disproportionately high. However, depending on the vector species and the practice of irrigation, the risk profile of LF could also be lower when compared to non-irrigated control areas. For transmission of bancroftian filariasis outside of Africa it is less the practice of irrigated agriculture per se, but rather the presence of polluted peridomestic man-made breeding sites that are suitable habitats for LF vectors (mostly Culex).
Care should also be exhibited in the interpretation of our at-risk population estimates in urban settings. We employed access to improved sanitation as the underlying risk factor to derive our estimates. However, the current definition of access to improved sanitation is primarily constructed by an aggregation of different social and infrastructure determinants rather than setting-specific eco-epidemiological features. Arguably, this is an oversimplification, as it fails to capture the complex causal webs of the various levels of disease causality, with outcomes shaped by a combination of distal, proximal, and physiological/pathophysiological causes.46 In fact, settings with access to improved sanitation, as defined by WHO, on the “least improved end” can include highly productive mosquito breeding sites, while mosquito breeding is unlikely to occur in settings on the “most improved end”. Hence, the nature of water resource development and management in urban areas exhibits strong spatio-temporal heterogeneity, often at very small scales. In addition, the fine-grained detail about wastewater management that would be essential for a precise appraisal of potential vector breeding sites is not available on a scale that would sharply reduce uncertainties in the present report. Nevertheless, the estimates in Table 2 do provide a good approximate indication of the magnitude of the problem. Unfortunately, LF is too far down on virtually all disease priority lists to get serious attention and serve as a basis for establishing the financial resources and political will for water-related improvements in urban areas. It is conceivable that endemic countries could get major LF reductions as a by-product of multi-faceted water campaigns that aim to improve overall health in a systemic manner.
The 12 studies we identified through our systematic review can be grouped into two broad categories, namely (i) those that looked at ecosystems influenced by irrigated rural agriculture and (ii) those that investigated urban environments affected by poor

30
design and maintenance of infrastructures for drainage of sewage and storm-water. Despite the different nature of these studies, entomological parameters revealed a quite consistent shift in species composition frequencies, and a proliferation of the overall vector population. High abundances were recorded for An. funestus, and especially for An. gambiae, in irrigated agro-ecosystems, particularly in West Africa. Members of the An. gambiae complex are the most anthropophilic filaria vectors.47 In Africa the fraction of irrigated arable land is still small (8.5%) but is expected to increase significantly in the decades to come.48 Consequently, it is conceivable that implementation of irrigation systems in this region increases transmission of W. bancrofti.49 Achieving the GPELF’s ambitious goal could be of a particular challenge in Africa, where the burden of LF could actually increase.
Regarding the observation of higher counts of vector species following water resource developments, these do not automatically translate into a higher LF burden. Due to the complicated nature of LF pathology and the highly complex transmission dynamics, it is possible that after the implementation of an irrigation system in a highly endemic area, the LF burden could level off after a few years.15,43 The entomological studies carried out in Sri Lanka during the development of the Mahaweli irrigation project in the 1980s revealed that several mosquito species proliferated over the course of project implementation. High densities of Cu. quinquefasciatus, which is the main LF vector in Sri Lanka, were documented, however, filaria transmission could not be confirmed.40,50
It is widely acknowledged that vector species shifts dependent on a myriad of factors, i.e., seasonality, temperature, plant succession, irrigation practices, total area under irrigation, water-depth, and water quality.51 In the studies analyzed here, these aspects were not retrievable from the published work. Thus, temporal variations cannot be excluded, rendering study comparison difficult. Future studies should quantify species composition frequencies and vector populations not only between different eco-epidemiological settings, but also during different seasons and according to different irrigation practices within the same setting.
Once a vector species is replaced by another that transmits a different filaria species, clinical manifestation rates are likely to shift. This was observed in rural Indonesia, where bancroftian filariasis transmitting An. subpictus vectors were replaced by timorian filariasis transmitting An. barbirostris, resulting in a shift from genital lymphedema to elephantiasis.39 In Egypt and Senegal a similar phenomenon was observed for schistosomiasis. The construction of large dams led to a shift from Schistosoma haematobium to S. mansoni, most likely because of a shift in intermediate host snails. This was paralleled by a change of clinical manifestation.52,53
Our review only identified two studies that investigated clinical manifestation rates in connection with water projects. Thus, it is difficult to set forth conclusions about whether water resource development projects positively or adversely affect clinical manifestations due to LF. It is delicate to employ results on filaria infection prevalence and transmission parameters as proxies, since microfilaremia and clinical symptoms are not implicitly associated. People with clinical manifestations are often amicrofilaremic, while others who are free of symptoms have microfilariae in their blood.54,55 Currently, there is no clear evidence of acquired or innate immunity to filaria infection. Thus, it is uncertain if lower infection rates and clinical manifestation among the local residents could be, at least partially, explained by acquired immunity or innate immunity genes that govern susceptibility to infection and lymphatic pathology.56,57

31
Another important finding of our systematic literature review is that urbanization, especially in connection with wastewater mismanagement and water storage, resulted in significant shifts in LF transmission parameters, as demonstrated in Haiti, India and Samoa. Reverse shifts in the abundance of Ae. samoanus and Ae. polynesiensis, two vectors with varying infectivity rates, indicated that rapid and uncontrolled urbanization impacts differently on various vector species. Decreased transmission parameters of Ae. samoanus in city centres show that urbanization can also marginalize a vector that fails to adapt to the new condition.
We have estimated that > 70% of urban dwellers in LF-endemic areas are currently located in Asia. Cu. quinquefasciatus, the most important LF vector in this region, prefers polluted waters for breeding. The rapid pace at which urbanization continues to build inroads in Asian (and African) countries, often in the face of declining economies, is paralleled by unprecedented pollutions of open waters and sewage systems beyond organic matters. In fact, industrial pollutants and heavy metals transform these water bodies into hostile environments for the living biota, including LF vectors. Therefore, the issue of uncontrolled urbanization and poor wastewater management as a consequence, gains further importance here.
In urban settings, integrated vector management comprising environmental management (e.g., draining), and biological (e.g., introduction of larvivorous fish), chemical (e.g., application of larvicides) and physical (e.g., use of mosquito nets) control measures can have a significant impact on LF transmission. A prominent example is the community-based integrated control program in Pondicherry, India.29 Despite a somewhat higher worm load five years after the control program was launched, transmission parameters dropped significantly. The reason for the increase of the worm load might be due to larger mosquito populations feeding less exclusively on humans.58 Another example of how an integrated control approach with strong emphasis on environmental management impacts on LF was described by Chernin.28 In Charleston, South Carolina, southern United States, bancroftian filariasis, which was introduced by African slaves, disappeared after the municipal sanitation system had been improved. These measures were initially intended to fight typhoid and related infectious diseases. However, they indirectly reduced polluted domestic waters and therefore reduced the available breeding-sites for filaria transmitting Cu. quinquefasciatus.
To further strengthen and expand the current evidence-base of the contextual determinants of LF, additional investigations are warranted. It would be of particular interest to document qualitatively and quantitatively both transmission and disease parameters, coupled with overall changes in key demographic, health, and socio-economic parameters over the course of major water resource development projects, such as irrigation schemes and large dams. Moreover, it is essential to investigate the role of urban LF, particularly in the light of rapid and uncontrolled urbanization. These investigations are likely to be carried out only if they are incorporated as part of comprehensive waste management and sanitation programs, driven by the need to establish and finance systemic health systems at the city, district, and regional levels. We conclude that integrated vector management, taking into account environmental, biological and socio-economic determinants, should receive more pointed consideration, as it is a promising approach to complement mass drug administration programs that form the backbone of the GPELF. Without an integrated control approach, the ambious goal to eliminate LF as a public health problem by 2020 might remain elusive.

32
REFERENCES 1. WHO, 2001. Lymphatic filariasis. Wkly Epidemiol Rec 76: 149-154. 2. Zagaria N, Savioli L, 2002. Elimination of lymphatic filariasis: a public-health
challenge. Ann Trop Med Parasitol 96 (Suppl. 2): S3-S13. 3. Molyneux D, 2003. Lymphatic filariasis (elephantiasis) elimination: a public health
success and development opportunity. Filaria J 2: 13. 4. Langhammer J, Birk HW, Zahner H, 1997. Renal disease in lymphatic filariasis:
evidence for tubular and glomerular disorders at various stages of the infection. Trop Med Int Health 2: 875-884.
5. Ottesen EA, Duke BO, Karam M, Behbehani K, 1997. Strategies and tools for the control/elimination of lymphatic filariasis. Bull World Health Organ 75: 491-503.
6. Dreyer G, Figueredo-Silva J, Neafie RC, Addiss DG, 1998. Lymphatic filariasis. In: Pathology of Emerging Infections 2.: Washington: American Society for Microbiology.
7. Dreyer G, Noroes J, Addiss D, 1997. The silent burden of sexual disability associated with lymphatic filariasis. Acta Trop 63: 57-60.
8. Ramaiah KD, Das PK, Michael E, Guyatt H, 2000. The economic burden of lymphatic filariasis in India. Parasitol Today 16: 251-253.
9. WHO, 2004. The World Health Report 2004 – Changing History. Geneva: World Health Organization.
10. International Task Force for Disease Eradication, 1993. Recommendations of the International Task Force for Disease Eradication. MMWR Recomm Rep 42: 1-38.
11. Molyneux DH, Bradley M, Hoerauf A, Kyelem D, Taylor MJ, 2003. Mass drug treatment for lymphatic filariasis and onchocerciasis. Trends Parasitol 19: 516-522.
12. Ottesen EA, 2000. The global programme to eliminate lymphatic filariasis. Trop Med Int Health 5: 591-594.
13. WHO, 2000. Preparing and Implementing a National Plan to Eliminate Lymphatic Filariasis: A Guideline for Programme Managers. A guideline for programme managers. Geneva: World Health Organization (WHO/CDS/CPE/CEE/2000.16).
14. WHO, 2004. Report on the mid-term assessment of microfilaraemia reduction in sentinel sites of 13 countries of the Global Programme to Eliminate Lymphatic Filariasis. Wkly Epidemiol Rec 79: 358–365.
15. Michael E, Malecela-Lazaro MN, Simonsen PE, Pedersen EM, Barker G, Kumar A, Kazura JW, 2004. Mathematical modelling and the control of lymphatic filariasis. Lancet Infect Dis 4: 223-234.
16. Harb M, Faris R, Gad AM, Hafez ON, Ramzy R, Buck AA, 1993. The resurgence of lymphatic filariasis in the Nile delta. Bull World Health Organ 71: 49-54.
17. Manga L, 2002. Vector-control synergies, between 'Roll Back Malaria' and the Global Programme to Eliminate Lymphatic Filariasis, in the African region. Ann Trop Med Parasitol 96 (Suppl. 2): S129-S132.
18. Prasittisuk C, 2002. Vector-control synergies, between 'Roll Back Malaria' and the Global Programme to Eliminate Lymphatic Filariasis, in South-east Asia. Ann Trop Med Parasitol 96 (Suppl. 2): S133-S137.
19. Burkot T, Bockarie M, 2004. Vectors. Am J Trop Med Hyg 71 (Suppl.): 24-26. 20. Hunter JM, 1992. Elephantiasis: a disease of development in north east Ghana.
Soc Sci Med 35: 627-645.

33
21. Rosengrant MW, Perez ND, 1997. Water Resource Development in Africa: A Review and Synthesis of Issues, Potentials and Strategies for the Future. International Food Policy Research Institute, EPTD Discussion Paper No. 28.
22. Mott KE, Desjeux P, Moncayo A, Ranque P, de Raadt P, 1990. Parasitic diseases and urban development. Bull World Health Organ 68: 691-698.
23. Knudsen AB, Slooff R, 1992. Vector-borne disease problems in rapid urbanization: new approaches to vector control. Bull World Health Organ 70: 1-6.
24. United Nations, 2004. Nations Human Settlements Programme. Washington, DC: United Nations.
25. Keiser J, Castro MC, Maltese MF, Bos R, Tanner M, Singer BH, Utzinger J, 2005. Effect of irrigation and large dams on the burden of malaria on a global and regional scale. Am J Trop Med Hyg 72: (in press).
26. Fontes G, Rocha EM, Brito AC, Antunes CM, 1998. Lymphatic filariasis in Brazilian urban area (Maceio, Alagoas). Mem Inst Oswaldo Cruz 93: 705-710.
27. Durrheim DN, Wynd S, Liese B, Gyapong JO, 2004. Lymphatic filariasis endemicity - an indicator of poverty? Trop Med Int Health 9: 843-845.
28. Chernin E, 1987. The disappearance of bancroftian filariasis from Charleston, South Carolina. Am J Trop Med Hyg 37: 111-114.
29. Rajagopalan PK, Panicker KN, Das PK, 1987. Control of malaria and filariasis vectors in South India. Parasitol Today 3: 233-241.
30. Samarawickrema WA, Kimura E, Spears GF, Penaia L, Sone F, Paulson GS, Cumm ings RF, 1987. Distribution of vectors, transmission indices and microfilaria rates of subperiodic Wuchereria bancrofti in relation to village ecotypes in Samoa. Trans R Soc Trop Med Hyg 81: 129-135.
31. Raccurt CP, Lowrie RC, Jr., Katz SP, Duverseau YT, 1988. Epidemiology of Wuchereria bancrofti in Leogane, Haiti. Trans R Soc Trop Med Hyg 82: 721-725.
32. Gad AM, Feinsod FM, Soliman BA, Nelson GO, Gibbs PH, Shoukry A, 1994. Exposure variables in bancroftian filariasis in the Nile Delta. J Egypt Soc Parasitol 24: 439-455.
33. Cao WC, Van der Ploeg CPB, Ren ZX, Habbema JDF, 1997. Success against lymphatic filariasis. World Health Forum 18: 17-20.
34. Jordan P, 1956. Filariasis in the Lake Province of Tanganyika. East Afr Med J 33: 237-242.
35. Appawu MA, Baffoe-Wilmot A, Afari EA, Nkrumah FK, Petrarca V, 1994. Species composition and inversion polymorphism of the Anopheles gambiae complex in some sites of Ghana, West Africa. Acta Trop 56: 15-23.
36. Dzodzomenyo M, Dunyo SK, Ahorlu CK, Coker WZ, Appawu MA, Pedersen EM, Simonsen PE, 1999. Bancroftian filariasis in an irrigation project community in southern Ghana. Trop Med Int Health 4: 13-18.
37. Smith A, 1955. The transmission of bancroftian filariasis on Ukara Island, Tanganyika II. The distribution bancroftian microfilaraemia compared with the distribution hut-haunting mosquitoes and their breeding-places. Bull Entomol Res 46: 437-444.
38. Appawu MA, Dadzie SK, Baffoe-Wilmot A, Wilson MD, 2001. Lymphatic filariasis in Ghana: entomological investigation of transmission dynamics and intensity in communities served by irrigation systems in the Upper East Region of Ghana. Trop Med Int Health 6: 511-516.
34
39. Supali T, Wibowo H, Rückert P, Fischer K, Ismid IS, Purnomo, Djuardi Y, Fischer P, 2002. High prevalence of Brugia timori infection in the highland of Alor Island, Indonesia. Am J Trop Med Hyg 66: 560-565.
40. Amerasinghe FP, Ariyasena TG, 1991. Survey of adult mosquitoes (Diptera: Culicidae) during irrigation development in the Mahaweli Project, Sri Lanka. J Med Entomol 28: 387-393.
41. Basu PC, 1957. Filariasis in Assam State. Indian J Malariol 11: 293-308. 42. Patz JA, Graczyk TK, Geller N, Vittor AY, 2000. Effects of environmental change
on emerging parasitic diseases. Int J Parasitol 30: 1395-1405. 43. Amerasinghe FP, 2003. Irrigation and mosquito-borne diseases. J Parasitol 89
(Suppl.): S14-S22. 44. Molyneux DH, 2003. Common themes in changing vector-borne disease
scenarios. Trans R Soc Trop Med Hyg 97: 129-132. 45. Keiser J, Utzinger J, Castro MC, Smith TA, Tanner M, Singer BH, 2004.
Urbanization in sub-saharan Africa and implication for malaria control. Am J Trop Med Hyg 71 (2 Suppl.): 118-127.
46. Ezzati M, Utzinger J, Cairncross S, Cohen AJ, Singer BH, 2005. Environmental risks in the developing world: exposure indicators for evaluating interventions, programmes, and policies. J Epidemiol Community Health 59: 15-22.
47. Costantini C, Sagnon N, della Torre A, Coluzzi M, 1999. Mosquito behavioural aspects of vector-human interactions in the Anopheles gambiae complex. Parassitologia 41: 209-217.
48. Keiser J, Utzinger J, Singer BH, 2002. The potential of intermittent irrigation for increasing rice yields, lowering water consumption, reducing methane emissions, and controlling malaria in African rice fields. J Am Mosq Control Assoc 18: 329-340.
49. Surtees G, 1970. Effects of irrigation on mosquito populations and mosquito-borne diseases in man, with particular reference to ricefield extension. Int J Environ Stud 1: 35-42.
50. Amerasinghe FP, Munasingha NB, 1988. A predevelopment mosquito survey in the Mahaweli Development Project area, Sri Lanka: adults. J Med Entomol 25: 276-285.
51. Service MW, 1984. Problems of vector-borne disease and irrigation projects. Ins Sci Appl 5: 227-231.
52. Abdel-Wahab MF, Strickland GT, El-Sahly A, El-Kady N, Zakaria S, Ahmed L, 1979. Changing pattern of schistosomiasis in Egypt 1935-79. Lancet 314: 242-244.
53. Southgate VR, 1997. Schistosomiasis in the Senegal River Basin: before and after the construction of the dams at Diama, Senegal and Manantali, Mali and future prospects. J Helminthol 71: 125-132.
54. Kar SK, Mania J, Kar PK, 1993. Humoral immune response during filarial fever in Bancroftian filariasis. Trans R Soc Trop Med Hyg 87: 230-233.
55. Ravindran B, 2003. Aping Jane Goodall: insights into human lymphatic filariasis. Trends Parasitol 19: 105-109.
56. Hise AG, Hazlett FE, Bockarie MJ, Zimmerman PA, Tisch DJ, Kazura JW, 2003. Polymorphisms of innate immunity genes and susceptibility to lymphatic filariasis. Genes Immun 4: 524-527.

35
57. Stolk WA, Ramaiah KD, van Oortmarssen GJ, Das PK, Habbema JDF, de Vlas SJ, 2004. Meta-analysis of age-prevalence patterns in lymphatic filariasis: no decline in microfilaraemia prevalence in older age groups as predicted by models with acquired immunity. Parasitology 129: 605-612.
58. Samuel PP, Arunachalam N, Hiriyan J, Thenmozhi V, Gajanana A, Satyanarayana K, 2004. Host-feeding pattern of Culex quinquefasciatus Say and Mansonia annulifera (Theobald) (Diptera: Culicidae), the major vectors of filariasis in a rural area of south India. J Med Entomol 41: 442-446.
59. Lindsay SW, Thomas CJ, 2000. Mapping and estimating the population at risk from lymphatic filariasis in Africa. Trans R Soc Trop Med Hyg 94: 37-45.
60. United Nations, 2004. World Urbanization Prospects. The 2003 Revisions. New York: Department of Economic and Social Affairs; Population Division of the United Nations (ESA/P/WP.190).
61. WHO, 2002. Defining the Roles of Vector Control and Xenomonitoring in the Global Programme to Eliminate Lymphatic Filariasis. Report of the Informal Consultation. Geneva: World Health Organization (WHO/CDS/CPE/PVC/2002.3).
62. Michael E, Bundy DAP, Grenfell BT, 1996. Re-assessing the global prevalence and distribution of lymphatic filariasis. Parasitology 112: 409-428.
63. WHO, 2002. Lymphatic filariasis elimination in the Americas. Report of the regional program-manager's meeting. Port-au-Prince, Haiti: Pan American Health Organization.
64. WHO, 2003. Lymphatic filariasis. Wkly Epidemiol Rec 78: 171-179. 65. Kazura JW, Bockarie MJ, 2003. Lymphatic filariasis in Papua New Guinea:
interdisciplinary research on a national health problem. Trends Parasitol 19: 260-263.
Acknowledgments: We thank Dr Felix P. Amerashinge, Prof. David H. Molyneux, Dr Will Parks, Dr Erling Pedersen, and Dr Christopher A. Scott for valuable comments on the manuscript. We also thank Jacqueline V. Druery and her team from Stokes library at Princeton University for help in obtaining a large body of relevant literature. Financial support: This investigation received financial support from the Water, Sanitation and Health unit in the Protection of the Human Environment Department (WSH/PHE) at the World Health Organization (WHO ref Reg. file: E5/445/15). The research of J. Keiser and J. Utzinger is supported by the Swiss National Science Foundation (Projects No. PMPDB--106221 and PPOOB--102883, respectively). M. C. Castro is financially supported by the Office of Population Research and the Centre for Health and Wellbeing at Princeton University. Authors’ addresses: Tobias E. Erlanger, Jennifer Keiser, Marcel Tanner, Jürg Utzinger, Swiss Tropical Institute, P.O. Box, CH–4002 Basel, Switzerland; Marcia Caldas de Castro, Geography Department, University of South Carolina, Callcott Room 125, Columbia, SC 29208; Robert Bos, Department of Protection of the Human Environment, World Health Organization; 20 Avenue Appia, CH–1211 Geneva 27, Switzerland; Burton H. Singer, Office of Population Research, Princeton University, 245 Wallace Hall, Princeton, NJ 08544.

36
Appendix 5. Table summarising geographical distribution of the three LF species, the ecology of their vectors and environmental changes leading to increased vector densities
Filaria type
Endemic region Major vector species
Natural ecology
Environmental change leading to increased LF vector densities
Brugia timori
Alor, Flores and Timor islands
Anopheles barbirostris Fresh water Dams and irrigation, fresh water collection, flood control
Brugia malayi
South Asia Anopheles barbirostris Anopheles campestris Anopheles donaldi
Fresh water Dams and irrigation, fresh water collection, flood control
Mansonia uniformis Mansonia bonneae Mansonia dives Mansonia annulata Mansonia annulifera
Fresh water with aquatic weeds
Man-made reservoirs, drainage canals of irrigation schemes, aquatic weed growth
Culex quinquefasciatus Organically polluted water
Inadequate waste-water treatment due to rapid urbanisation, organic pollution of fresh water
Wuchereria bancrofti
Americas Culex quinquefasciatus Organically polluted water
Inadequate waste-water treatment due to rapid urbanisation, organic pollution of fresh water
Afrotropical Anopheles funestus Anopheles gambiae
Fresh water Dams and irrigation, fresh water collections, flood control
Culex quinquefasciatus Organically polluted water
Inadequate waste-water treatment due to rapid urbanisation, organic pollution of fresh water
Middle East Culex pipiens molestus Culex quinquefasciatus
Organically polluted water
Inadequate waste-water treatment due to rapid urbanisation, organic pollution of fresh water
Far East Culex quinquefasciatus Organically polluted water
Inadequate waste-water treatment due to rapid urbanisation, organic pollution of fresh water
Papuan Anopheles farauti Anopheles koliensis Anopheles punctulatus
Fresh water Dams and irrigation, fresh water collection, flood control
Nicobar, Thailand
Ochlerotatus niveus Ochlerotatus harinasutai
Fresh water with moderate organic pollution
Domestic water collections, rain water canals
Polynesia Aedes polynesiensis Aedes samoanus
Small fresh water collections
Lack of solid and organic waste management, inadequate drinking water supply
Source: Zagaria & Savioli (2002), Annals of Tropical Medicine and Parasitology, 96(Suppl.):3-13.

37
Appendix 6.1. Key information form (Smith-1955-Bull Ent Res) WHO sub-region 1 Disease Lymphatic filariasis Author Smith A. Title The Transmission of Bancroftial Filariasis on Ukara Island Tanganyika. II.
The Distribution of Bancroftial Microfilaraemia Compared with the Distribution of Hut-Haunting Mosquitoes and their Breeding Places.
Reference Bulletin of Entomology Research. 1955;46:437-444. Language English Country, year of study
Tanganyika [Tanzania], 1951-53
Village, district, region
Ukara Island
Geographical coordinates
Lo: 33° 00’ E / La: 01° 50’ S
WHO sub-region {1-14}
1
Abstract
Key information
- Microfilaraemia prevalence rate - Number of female Anopheles gambiae and Anopheles funestus
caught Water resource development and management project
Gravitational irrigation
Type Rice irrigation Year of inception
-

38
Outcome measures (e.g. prevalence, incidence, # of cases, parasites density exposed population, etc.)
Irrigated areas
Villages Microfilariae prevalence (%)
No. of An. gambiae caught
No. of An. funestus caught
Chifule 30 3622 25
Bukungu 20 3891 31
Bwisya 24 - -
Chigara 23 - -
Buyembe 26 - -
Mbule 20 - -
Bubanja 26 7143 27
Katende 24 1084 33
Nyanguja 16 - -
Isiba 22 4050 8
Chamhunda 23 - -
Buyanja 24 3726 30
Bukiko 23 - -
Nyamanga 25 4194 51
Mean 23.3 3959 29
Non-irrigated areas
Villages Microfilariae prevalence (%)
No. of An. gambiae caught
No. of An. funestus caught
Kome 11 1714 3
Buyombe 7 - - Huna 15 3386 3
Bulabi 16 - - Lubonwe 9 1277 1
Busere 10 - - Bumiro 13 1852 1
Masaka 17 - -
Mean 12 2057 2 Relative changes, risk (RR)
Additional notes

39
Appendix 6.2. Key information form (Jordan-1956-East Afr Med Jou) WHO sub-region 1 Disease Lymphatic filariasis Author Jordan P. Title Filariasis in the lake Province of Tanganyika Reference East African Medical Journal. 1956 Jun;33(6):233-6. Language English Country, year of study Tanganyika (Tanzania), 1956 Village, district, region Babanja, Boyombe Geographical coordinates Lo: 33° 02’ E / La: 01° 50’ S WHO sub-region {1-14} 1 Abstract
Key information - Microfilaraemia in two villages - Mosquito-catches (An. gambiae, An. funestus) in two villages
Water resource development and management project
- Rice cultivation - Pits for grass for cattle fodder
Type - Irrigation Year of inception Outcome measures (e.g. prevalence, incidence, # of cases, parasites density exposed population, etc.)
Showing catches of A. gambiae and A. funestus per hut in two villages, 3 miles apart, with differents microfilaraema rates
Flit catches per hut Village %
microfilaraemia An. gambiaeMay July
An. funestusMay July
Babanja Boyombe
26 7
714 29
16 6.1
2.7 0.1
3.8 0.1
Before
During After
Relative changes, risk (RR) Additional notes

40
Appendix 6.3. Key information form (Basu-1954-Ind Jou Malarol) WHO sub-region 11 Disease Lymphatic filariasis Author Basu PC. Title Filariasis in Assam state. Reference Indian Journal of Malariology. 1957 Jun;11(3):293-308. Language English Country, year of study
India, 1957
Village, district, region
Bakakhat area, Chabua area:, Assam state, India
Geographical coordinates
Bakakhat: La: 93° 36’ E / Lo: 26° 38’ N; Chabua area: La: 95° 11E / Lo: 27° 29’ N
WHO sub-region {1-14}
12
Abstract
Key information
Clinical data, infection rates and entomological data of tea garden and non-tea garden dwellers: - Climatic data - Clinical data, disease rates, prevalence, filariaemia rates of different villages and tea gardens in two regions of Assam - Age distribution of disease and infection - Mosquito density, dissection, rates of infection - Endemecity rates of different categories of persons
Water resource development and management project
Irrigation in tea gardens
Type Irrigation Year of inception

41
Outcome measures (e.g. prevalence, incidence, # of cases, parasites density exposed population, etc.)

42
Before During After
Relative changes, risk (RR)
Additional notes

43
Appendix 6.4. Key information form (Partono-1978-Am Jou Trop Med) WHO sub-region 11 Disease Lymphatic filariasis Author Partono F, Pribadi PW, Soewarta A. Title Epidemiological and clinical features of Brugia timori in a newly established village,
Karakuak, West Flores, Indonesia. Reference American Journal of Tropical Medicine and Hygiene. 1978 Sep;27(5):910-5. Language English Country, year of study
Indonesia, 1977
Village, district, region
Village Karakuak, West Flores, Indonesia
Geographical coordinates
Lo: 8° 18’ S / La: 120° 28’ E
WHO sub-region {1-14}
11
Abstract The epidemiological and clinical features of Brugia timori filariasis in a newly established village, Karakuak, West Flores, is described. The microfilarial rate by finger stick and Nuclepore filtration was 24% and 30%, respectively, and the disease rate 64%. Infected persons were found in every family and household with no predominant age or sex preference. Development of elephantiasis in the population was associated with residence in the new village of Karakuak, where extensive rice field cultivation was initiated soon after arrival. The irrigated fields provided excellent breeding sites for the vector, Anopheles barbirostris. People with no previous exposure to the parasite developed elephantiasis earlier and more frequently than those originating from other endemic areas.
Key information
- Microfilaremia (smear and membrane filtration method) age and sex distributed - Comparison of number (%) of people with microfilaremia, scar and elephantiasis among endemic and non-endemic filarial areas - Number (%) of persons with clinical signs and symptoms of Timorian filariasis - Indoor and outdoor collection of various potential filaria-transmitting mosquitoes
Water resource development and management project
Rice Irrigation
Type Rice
Year of inception
1962

44
Outcome measures (e.g. prevalence, incidence, # of cases, parasites density exposed population, etc.)
The detection of microfilaremia by blood smear and membrane filtration; age and sex distribution
Age group Males Females Total
20µl Nucleopore 20µl Nucleopore
0-4 10/0 (0)* - 10/2 (20) - 20/2 (10)
5-9 13/1 (8) 5/0 (0) 16/2 (13) 6/1 (17) 29/4 (14)
10-19 32/7 (22) 22/5 (23) 22/3 (14) 23/3 (13) 54/10 (19)
20-29 14/3 (21) - 14/1 (7) - 28/4 (14)
30-39 13/6 (46) 13/6 (46) 13/4 (31) 16/5 (31) 26/10 (38)
40-49 13/6 (46) - 9/2 (22) - 22/8 (36)
50+ 9/7 (78) 7/7 (100) 12/4 (33) 4/2 (50) 21/12 (57)
Total 104/30 (29) 47/18 (38) 96/18 (19) 49/11 (22) 200/50 (25)
* number examined / number positive (%)
Comparison of number (%) of people with microfilaremia, scar and elephantiasis
among people from endemic and non-endemic filarial areas Non-endemic Endemic Age at
exp-osure
No exam-ined
Mf positive Scars
Elephant-iasis
No exam-ined
Mf positive Scars
Elephant- iasis
0-10 19 3 (16) 6 (32) 4 (21) 19 4 (21) 10 (53) 2 (11)
11+ 32 9 (28) 18 (56) 11 (34) 38 13 (34) 21 (55) 5 (13)
Total 51 21 (24) 24 (47) 15 (29) 57 17 (30) 31 (54) 7 (12)

45
Number (%) of persons with clinical signs and symptoms of Timorian filariasis
Males Females
Age group
No examined
Adeno-lymph-angitis
Scars Elephant-iasis
Total filarial
diseases
No examined
Adeno-lymph-angitis
Scars Elephant-iasis
Total filarial
diseases
0-4 11 2 (18)* 0 (8) 0 2 (18) 10 1 (10) 0 0 1 (10)
5-9 13 6 (46) 3 (23) 1 (8) 7 (54) 16 3 (19) 5 (31) 1 (6) 7 (44)
10-19 32 16 (50) 17 (53) 3 (13) 23 (72) 22 12 (55) 12
(55) 6 (27) 21 (95)
20-29 14 10 (71) 5 (36) 5 (36) 13 (93) 14 5 (36) 4 (29) 7 (50) 9 (64)
30-39 13 11 (85) 12 (92) 1 (8) 12 (92) 13 8 (62) 5 (38) 3 (23) 9 (69)
40-49 13 7 (54) 7 (54) 2 (15) 9 (69) 9 3 (33) 3 (33) 2 (22) 5 (55)
50 9 5 (56) 2 (22) 2 (22) 5 (56) 13 4 (31) 6 (46) 1 (8) 7 (54)
Total 105 57 (54) 46 (44) 15 (14) 71 (68) 97 36 (37) 35
(36) 20 (21) 59 (61)
Mosquito collection Indoor human bait
Day 1 Day 2
Indoor resting day 3
Outdoor human bait day
3 Species
8pm-10pm
10pm-5am
8pm-10pm
10pm-12pm
12pm-3am
3am-6am
2am-4am
8pm-9pm
Total
Anopheles barbirostris 3 75 12 18 41 15 250 13 427
Anopheles sundaicus 31 52 6 20 4 5 6 6 130
Anopheles aconitus 4 11 0 4 9 2 0 2 30
Anopheles vagus 7 13 4 7 7 3 14 3 58
Anopheles subpictus 16 47 2 8 0 2 0 6 81
Anopheles annularis 4 0 4 4 4 6 0 4 26
Mansonia uniformis 0 0 0 0 0 0 0 1 1
Culex fusco-cephalus 0 0 0 0 0 0 0 4 4
Culex pipiens fatigas 0 0 0 1 0 0 0 0 1
Culex 0 0 0 0 0 0 0 1 1
46
Before During After
Relative changes, risk (RR)
Additional notes
Further publications from island of Flores: - Partono F.-Trans R Soc Trop Med Hyg. 1989 Nov-Dec;83(6):821-6 - Partono F.-Trans R Soc Trop Med Hyg. 1984;78(3):370-2. - Hoedojo-Southeast Asian J Trop Med Public Health. 1980 Sep;11(3):399-404. - Partono F.-Southeast Asian J Trop Med Public Health. 1978 Sep;9(3):338-43. - Partono F.-J Parasitol. 1977 Jun;63(3):540-6. - Atmosoedjono S.-J Med Entomol. 1977 Jan 31;13(4-5):611-3. - Dennis D.T.-Am J Trop Med Hyg. 1976 Nov;25(6):797-802. - Partono F.-Trans R Soc Trop Med Hyg. 1976;70(4):354-5.

47
Appendix 6.5. Key information form (Rajagopalan-1987-Paras Today) WHO sub-region 12 Disease Lymphatic filariasis Author Rajagopalan PK, Panocker KN, Das PK.
Title Control of malaria and filariasis vectors in south India. Reference Parasitology Today. 1987; 3(8):233-40. Language English Country, year of study
India, 1987
Village, district, region
Pondicherry town
Geographical coordinates
La: 11° 56’ N / Lo: 79° 50’ E
WHO sub-region {1-14}
12
Abstract
Key information - Evaluation of a malaria and filariasis control programme
- Annual Transmission Index for Wuchereria bancrofti Water resource development and management project
- Vector control programme of the “Vector control Research Centre in Pondicherry”
Type - Cesspits, cisterns, wells, water drains, storm channels, other water bodiesYear of inception 1981 Outcome measures (e.g. prevalence, incidence, # of cases, parasites density exposed population, etc.)
- Including measures of the mosquito control programme: physical, chemical, biological strategies and environmental management

48
Annual transmission index for Wuchereria bancrofti in Pondicherry during the 5 years of the VCRC vectors control project
1979-80
(pre-control)
1981 1982 1983 1984 1985
Estimated no. of
mosquitoes biting a man in one year
(a)
26 203 8238 3181 3222 1662 3617
Proportion of
mosquitoes infective
(from biting collections only) (b)
0.0086 0.006 0.004 0.0066 0.0079 0.0061
Estimated no. of
infective bites a man receives in
a year
225 49 13 21 13 22
Number of infective
larvae per infective
mosquito (c)
2.0 4.0 2.6 2.9 3.72 3.50
Annual transmission
index (a x b x c)
450 197 33 62 49 77
Before During After
Relative changes, risk (RR)
Additional notes

49
Appendix 6.6. Key information form (Samawrickrema- Trans Roy Soc Trop Med Int Health-1987) WHO sub-region 5 Disease Lymphatic filariasis Author Samawrickrema WA, Kimura E, Spears, GFS, Penaia L, Fola Sone, Paulson GS,
Cummings RF. Title Distribution of vectors, tansmission indices and microfilaria rates of subperiodic
Wuchereria bancrofti in relation to village ecotypes in Samoa Reference Transactions of the Royal Society of Tropical Medicine and International
Health. 1987;81, 129-135. Language English Country, year of study
Samoa, 1978-79
Village, district, region
Upulu and Savaii islands
Geographical coordinates
Lo: 13° 48’ S / La: 172° 08’ W
WHO sub-region {1-14}
5
Abstract Aedes polynesiensis and Ae. samoanus biting densities and Wuchereria bancrofti infection and infective rates were studied in 47 villages throughout the islands of Samoa Upolu, Manono and Savaii during 1978-79, and microfilaria (mf) rates were surveyed in 28 of the villages. The mf rate was correlated with both infection and infective rates of Ae. polynesiensis in Upolu, but not of Ae. samoanus. In Upolu, Ae. polynesiensis was apparently the major vector. It was relatively more abundant in more cultivated and populated areas, along the northern coast of Upolu, except Apia town area. In Savaii, Ae. samoanus predominated over Ae. polynesiensis except in "plantation" villages. Relatively high biting densities and rates of infection and infectivity indicated that Ae. samoanus was not less important than Ae. polynesiensis as a vector in Savaii. Ae. samoanus preferred natural vegetation, in contrast to Ae. polynesiensis which was found near human habitations in cultivated land. There was no difference between the biting densities of Ae. polynesiensis in "coastal" and "inland" villages, indicating that crab holes (numerous only in some coastal villages) may not influence the density of Ae. polynesiensis. Higher mf rates were associated with villages where Ae. polynesiensis, rather than Ae. samoanus, was dominant, indicating that Ae. polynesiensis was generally a more efficient vector. In the former villages, the difference in mf rates between males and females was smaller than in the latter, probably reflecting a difference in biting habits of the vectors. Ae. polynesiensis infections were recorded in plantations over 2 km from any village, suggesting that both habitats were foci of transmission.
Key information
- Microfilaremia prevalence rates of humans, biting densities, infection and infective rates of Aedes species on Upolu and Savaii island - Biting frequencies depending on different village ecotypes
Water resource development and management project
Higher human population, urbanization, domestic water storage, accumulation of junk
Type Various artificial water bodies

50
Year of inception
Outcome measures (e.g. prevalence, incidence, # of cases, parasites density exposed population, etc.)

51
Before During After
Relative changes, risk (RR)
Additional notes

52
Appendix 6.7. Key information form (Raccurt-1988-Trans Roy Soc Trop Med Hyg) WHO sub-region 5 Disease Lymphatic filariasis Author Raccurt CP, Lowrie RC Jr, Katz SP, Duverseau YT. Title Epidemiology of Wuchereria bancrofti in Leogane, Haiti. Reference Transactions of the Royal Society of Tropical Medicine and Hygiene.
1988;82(5):721-5. Language English Country, year of study
Haiti, 1981
Village, district, region
Leogane
Geographical coordinates
La: 18° 31’ N / Lo: 72° 38’ W
WHO sub-region {1-14}
5
Abstract A survey for Wuchereria bancrofti in Leogane, Haiti, revealed that 140 of 421 individuals (33%) had a patent infection, of which 40% lived in the suburban outskirts of the city. The median microfilaria density was 19.1 per 20 mm3 of blood for suburban dwellers compared with only 8.8 for those living in the city. The vector, Culex quinquefasciatus (Say), breeds mostly in and around numerous rum distilleries, located exclusively around the periphery of the city, and this undoubtedly accounts for the higher prevalence and intensity of infection among suburban dwellers.
Key information
- Microfilariae (Mf) rates and Mf densities of 4 spots in and around Leogane. - Positive regression lines of cumulative frequency distribution of Wuchereria bancrofti microfilaria-positive cases.
Water resource development and management project
- Leogane inner city (low risk) - Dampus suburban area: sugar cane fields and crushing factories (high risk) - Chassange: distilleries: sugar waste water discharge in ditches and pits; water storage in concrete vats (very high risk) - Ca-Ira: Mangrove swamps; vector Culicoides furens transmits Mansonella ozzardi (medium to high risk)
Type Sugarcane Year of inception
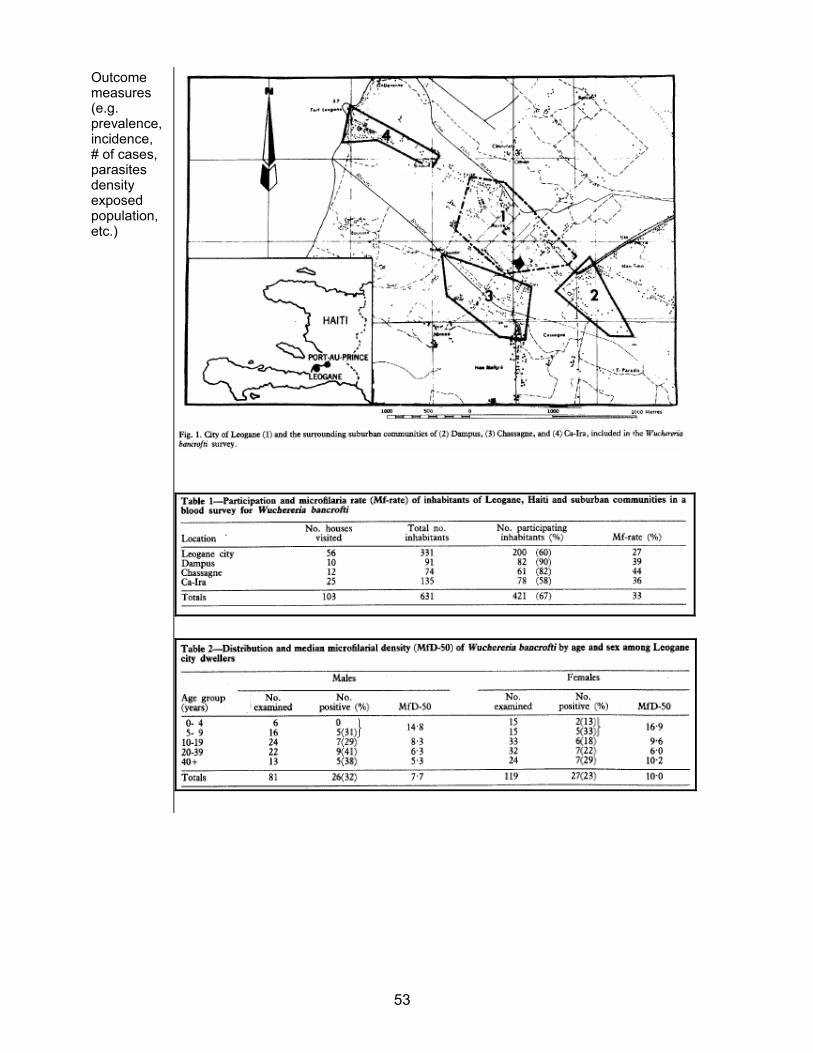
53
Outcome measures (e.g. prevalence, incidence, # of cases, parasites density exposed population, etc.)

54
Microfilaria (Mf)-rate of Wuchereria bancrofti of 421 participants Location Mf-rate in %
Leogane city 27 Dampus 39
Chassange 44
Ca-Ira 36
- Larvae of Culex quinquefaciatus collected around the distilleries; ~2000 larvae per dip (475 ml). - After 5-17d 47% of Culex quinquefaciatus had third stage larvae.
Before During After
Relative changes, risk (RR)
Additional notes

55
Appendix 6.8. Key information form (Amerasinghe-1991-Jou Med Entom) WHO sub-region 12 Disease Lymphatic filariasis Author Amerasinghe F.P. Title Survey of adult mosquitoes (Diptera: Culicidae) during irrigation development in the
Mahaweli Project, Sri Lanka Reference Journal of Medical Entomology. 1991 May; 28(3):387-393.
Language English Country, year of study
Sri Lanka, 1986-1987
Village, district, region
Block 6, Zone 4, Mahaweli System C, Eastern Sri Lanka
Geographical coordinates
La: 07°20’N / Lo: 81°04’E
WHO sub-region {1-14}
12
Abstract
Key information
- Entomological survey before during and after an irrigation project. - 71 mosquito-species collected - Shift in vector composition and abundance - Cx. qinquefasciatus counts increased 2.2 times during the completion of the project- The geometric mean female Cu. quinquefasciatus per man-hour rose from 4.6 to 7.4 (factor: 1.6) during the completion of the project
Water resource development and management project
Canals, medium and small dams, pumps and resettlement of people
Type Rice irrigation Year of inception
1988

56
Outcome measures (e.g. prevalence, incidence, of cases, parasites density exposed population, etc.)

57
Appendix 6.9. Key information form (Hunter-1992-Soc Sci Med) WHO sub-region 1 Disease Lymphatic filariasis Author
Hunter JM. Title Elephantiasis: a disease of development in north east Ghana. Reference
Social Science and Medicine. 1992 Sep;35(5):627-45; discussion 645-9.
Language English Country, year of study Ghana, 1989 Village, district, region 41 chiefdoms in north east Ghana Geographical coordinates La: 10° 30’ – 11° 00’ N / Lo: 0° 00’ – 1° 30’ W WHO sub-region {1-14} 1 Abstract A reconnaissance survey for the presence of lymphatic filariasis is
made in 41 chiefdoms of north east Ghana. Four disease levels are identified culminating in hyperendemic disease foci associated with two government-introduced rice irrigation projects. Attention is also drawn to the disease effects of small village dams. Multiple concurrent infections are noted. Within the most stricken irrigation villages, aspects of concealment, stigma and marriage are considered. Failure to control lymphatic filariasis has led to hospital avoidance and neglect of the disease jointly by patients, physicians and nurses. Culpability rests with the irrigation authority and government health services. An outline is given of possible measures for disease control. A multisectoral policy of 'prevention before development' is strongly advocated.
Key information - Observation of clinical symptoms of LF and the spatial relation to irrigation and water storage projects - Different aspects dealing with (water) development projects in northern Ghana - No data available: reconnaissance survey, descriptive
Water resource development and management project
- Small dams and irrigation systems in northern Ghana - Especially the Vea and Tono irrigation project
Type - Rice, shorgum, millet, vegetables - Water for livestock
Year of inception - Vea: 1965 (start) – 1984 (completion) - Tono: 1975 (start) – 1985 (completion) - Construction of various little dams 1958 -1964
Outcome measures (e.g. prevalence, incidence, of cases, parasites density exposed population, etc.)
Descriptive: - Distinctive higher prevalence of clinical symptoms in villages within 2 km range of irrigation systems and dams - Higher prevalence of clinical symptoms in women than in men - Absence or low prevalence of clinical symptoms in villages > 2 km from major irrigation systems and dams
Before - Village chiefs reported an increase both of LF-symptomatic cases and insect nuisance
During After
58
Relative changes, risk (RR) Estimated by author (!) to be > 1 in villages within the flight range of Anopheles gambiae + funestus.(~2 km).
Additional notes

59
Appendix 6.10. Key information form (Gad-1994-Jou Egypt Soc Paras) WHO-region 7 Disease Lymphatic filariasis Author Gad AM, Feinsod FM, Soliman BA, Nelson GO, Gibbs PH, Shoukry A. Title Exposure variables in bancroftian filariasis in the Nile Delta Reference Journal of the Egyptian Society of Parasitology. 1994 Aug;24(2):439-55. Language English Country, year of study
Egypt, 1986
Village, district, region
El Kashish, Qalubyia District
Geographical coordinates
La: 30° 13’ N / Lo: 31° 18’ E
WHO sub-region {1-14}
7
Abstract To demonstrate focality of filariasis within endemic rural areas and to define exposure variables which may influence this phenomenon, the population of an agrarian endemic village, of 12,500 individuals, in the Nile Delta of Egypt was censused. A sequential sample of individuals residing in every fifth house was tested for microfilaremia (239 households with 8.6 +/- 3.5 individuals per household (HHD). Three areas of the village were tested simultaneously and a questionnaire was filled out for each sampled HHD with special emphasis given to the entomological and environmental factors that might affect filarial infection. One area (area A) had a higher intensity of larvae and biting adults of the main filarial vector, Culex pipiens, than the other two areas (areas B and C). Of the 1488 persons who agreed to be tested in the three areas 181 (12.2%) were microfilaremic. Microfilaremia prevalences were the same in males and females and microfilariae were present in all age groups. Filarial infection was most prevalent in area "A" (1.16 +/- 0.14 infected people per HHD) than in area "B" (0.44 +/- 0.11) or "C" (0.72 +/- 0.10) (ANOVA; p = 0.0003). several possible predictor variables were analyzed by logistic regression with the presence of infection as the response variable. Among individuals residing around the main Culex pipiens development sites, those living in houses facing vacant land are exposed to more mosquito bites and had a greater chance of having filarial infection (relative risk [RR] = 1.5; logistic regression, P = 0.0089). People residing in large households had a reduced chance of having filarial infection (RR = 0.87; logistic regression, p = 0.0015). These data show that the distribution of microfilaremic individuals is uneven within the study village and suggest that small HHD and houses that bordered open areas containing mosquito development sites are potential risk factors for acquiring filarial infection.

60
Key information - Microfilaremia prevalence in the study population according to age and sex - Comparison of microfilaremia prevalence among individuals - Variance in prevalence of microfilaremia within households (HHD) - Comparison of microfilaria prevalence and household (HHD) prevalence between the 3 study areas A, B and C - Risk factors associated with microfilaremia
Water resource development and management project
- Cesspits and cesspools
Type - Wastewater Year of inception
-
Outcome measures (e.g. prevalence, incidence, # of cases, parasites density exposed population, etc.)

61
Microfilaremia prevalence in the study population according to age and sex
Microfilaremia prevalence Male Female Total
Age group (years)
N % N % N %
<10 227 6 239 7 466 6.65 >10≤20 209 16 141 13 350 14.57 >20≤30 108 7 105 15 213 10.80 >30≤40 83 13 99 18 182 15.93 >40≤50 54 13 55 20 109 16.50 >50≤60 53 19 42 24 95 21.05
>60 41 15 32 9 73 12.33 total 775 11 713 13 1488 12.16
Comparison of microfilaremia prevalence among overall individuals
P-values
Area N Prevalence±SE Area A Area B Area C
A 399 0.17±0.019 0.001 0.030
B 326 0.07±0.015 0.024
C 763 0.12±0.012
A: area with a large open cesspool (10mx6m) “very high risk” B: area with a closed cesspool (1mx1m) “high risk” C: remainder of the whole study-site (village) “normal risk” Variance in prevalence of microfilaremia within households (HHD)
P-values
Area HHD prevalence Variance
area A Area B Area C
A 0.19 0.0324 0.006 0.707
B 0.07 0.0144 0.001
C 0.12 0.0361

62
Comparison of microfilaria prevalence and household (HHD) prevalence between the 3 study areas A, B and C
No. of people with microfilaria
HHD prevalence
ANOVA Tukey’s MC test
ANOVA Tukey’s MC test
Area No Mean/HHD±SE P-value A B C Mean/HHD±SE P-value A B C
A 57 1.16±0.14 0.0003 - * * 0.19±0.024 0.0006 - * *
B 54 0.44±0.11 - NS 0.07±0.017 NS
C 127 0.72±0.10 - 0.12±0.017
-
- significant (p<0.05)
Risk factors associated with microfilaremia Vacant space HHD size Distance
Area p-value Rel.risk p-value Rel.risk p-value Rel.risk A 0.0089** 1.50 0.0016** 0.87 0.6656 0.99 B 0.5543 1.15 0.4425 1.05 0.0973 0.95 C 0.0555 1.25 0.2772 0.96 0.0141** 1.00
* RR=exp (regression coefficient) with risk increased or decreased as the magnitude relative to 1 (no change of risk) ** significant (p<0.05)
Before During After
Relative changes, risk (RR)
Other prevalence studies in the same region: - Harb M-Bull World Health Organ. 1993;71(1):49-54.
Additional notes

63
Appendix 6.11. Key information form (Appawu-1994-Acta Tropica) WHO sub-Region 1 Disease Lymphatic filariasis Author Appawu MA, Baffoe-Wilmot A, Afari EA, Nkrumah FK, Petrarca V.
Title Species composition and inversion polymorphism of the Anopheles gambiae complex in some sites of Ghana, west Africa.
Reference Acta Tropica. 1994 Feb;56(1):15-23. Language English Country, year of study Ghana, 1993 Village, district, region North-south transect through Ghana Geographical coordinates - WHO sub-region {1-14} 1 Abstract Samples of Anopheles gambiae s.l. were collected from eight
localities belonging to four of the five main ecological strata of Ghana. Analysis of ovarian polytene chromosomes revealed the presence of An. gambiae s.s. in all the sites studied, while An. arabiensis was detected only in the extreme northern locality of Navrongo and An. melas in some southern sites. Anopheles arabiensis showed a degree of inversion polymorphism comparable to the one observed in other West African countries. The analysis of the chromosomal polymorphism of An. gambiae s.s. showed the presence of the FOREST form in the rain forest localities and the SAVANNA form in the coastal savanna sites. The MOPTI form occurred sympatrically with the SAVANNA form in the northernmost locality. The possible influence of the presence of various taxa of the An. gambiae complex and of their intra-specific variants on malaria vectorial system is discussed.
Key information - Species composition (Anopheles gambiae, Anopheles arabiensis, Anopheles melas) through a transsect in Ghana. Some places have irrigation. Various ecological zones are represented.
Water resource development and management project
- Irrigation in Navrongo, Tachekope and Dawhenya
Type Rice-irrigation Year of inception Outcome measures (e.g. prevalence, incidence, # of cases, parasites density exposed population, etc.)

64
Appendix 6.12. Key information form (Dzodzomenyo-1999-Trop Med Int Health) WHO sub-Region 1 Disease Lymphatic filariasis Author Dzodzomenyo M, Dunyo SK, Ahorlu CK, Coker WZ, Appawu
MA, Pedersen EM, Simonsen PE. Title Bancroftian filariasis in an irrigation project community in southern
Ghana. Reference Tropical Medicine & International Health. 1999 Jan;4(1):13-8. Language English Country, year of study Ghana, 1995 Village, district, region Gomoa Okyereko Geographical coordinates La: 5° 25’ N / Lo: 0° 37’ W WHO sub-region {1-14} 1 Abstract An epidemiological study to document the endemicity and
transmission characteristics of bancroftian filariasis was conducted in an irrigation project community in southern Ghana. In a 50% random sample of the population, the prevalence of microfilaraemia was 26.4% and the geometric mean microfilarial intensity among positives was 819 microfilariae/ml of blood. Hydrocoele was found in 13.8% of the males aged > or =18 years, and 1.4% of the residents examined, all females, had lymphoedema/elephantiasis. Detailed monitoring of the microfilarial intensity in 8 individuals over a 24-h period confirmed its nocturnal periodicity with a peak at approximately 0100 hours. The most important vector was Anopheles gambiae s.l., followed by Anopheles funestus. The abundance of these mosquitoes and their relative importance as vectors varied considerably between the wet and the dry season. Opening of the irrigation canals late in the dry season resulted in a remarkable increase in the population of Anopheles gambiae (8.3% of which carried infective filarial larvae) to levels comparable to those seen during the wet season, suggesting that the irrigation project is responsible for increased transmission of lymphatic filariasis in the community.
Key information - Microfilaremia and clinical manifestations (hydrocele + elephantiasis) - Microfilaria periodicity in peripheral blood - No. (%) of vector species before and after opening of canals - No. (%) of infected and infective vectors during opened canals
Water resource development and management project
Irrigation Okyereko Irrigation Project (OIP)
Type Rice Year of inception 1974 Outcome measures (e.g. prevalence, incidence, # of cases, parasites density exposed population, etc.)
- Microfilariae periodicity peak at 2.00 am (8 persons observed)

65
No. mosquitoes caught by human landing catch during the late dry season (canals opened)
Species No. collected (no.
dissected)
No. infected (% infection
rate)
No. infective (% infectivity
rate) Anopheles
gambiae s.l. 169 (168) 45 (26.8) 14 (8.3)
Anopheles funestus
53 (50) 8 (16.0) 1 (2.0)
Anopheles pharoensis
3 (3) 2 (66.7) 1 (33.3)
Culex quinquefasciatus
18 (18) 1 (5.6) 0 (0.0)
Mansonella spec.
17 (17) 1 (5.9) 0 (0.0)
Total 260 (256) 57 (22.3) 16 (6.3) Wuchereria bancrofti microfilaraemia and clinical manifestations
Age group
No. examined
No. with mf (%)
Geometric Mean
Intensity in mf/ml
No. males with
hydrocoele (%)
No. of individuals
with elephantiasis
(%) 1-9 87 6
(6.9) 696 0 (0.0) 0 (0.0)
10-19 68 15 (22.1)
1288 2 (4.8) 1 (1.5)
20-39 68 24 (35.3)
999 2 (9.1) 0 (0.0)
40-59 37 19 (51.4)
506 3 (16.7) 3 (8.1)
≤ 60 36 14 (38.9)
737 1 (16.7) 0 (0.0)
Total 296 78 (26.4)
819 8 (5.7) 4 (1.4)

66
Distribution of indoor resting mosquitoes / 1 houses No. door resting mosquitoes collected (% of
total collected for period Species Wet season /
canal closed Early dry season /
canal closed
Late dry season canal
open Anopheles
gambiae s.l. 113 (61.1) 15 (12.1) 141 (76.6)
Anopheles funestus
56 (30.3) 101 (81.5) 40 (21.7)
Anopheles pharoensis
10 (5.4) 3 (2.4) 3 (1.7)
Culex quinquefasciatus
6 (3.2) 5 (4.0) 0 (0.0)
Mansonella spec.
0 (0.0) 0 (0.0) 0 (0.0)
Total 185 (100) 124 (100) 184 (100.0) Before During After
Relative changes, risk (RR)
Additional notes

67
Appendix 6.13. Key information form (Appawu-2001-Trop Med Int Health) WHO sub-region 1 Disease Lymphatic filariasis Author Appawu MA, Dadzie SK, Baffoe-Wilmot A, Wilson MD. Title Lymphatic filariasis in Ghana: entomological investigation of transmission dynamics
and intensity in communities served by irrigation systems in the Upper East Region of Ghana.
Reference Tropical Medicine & International Health. 2001 Jul;6(7):511-6. Language English Country, year of study
Ghana, 2000
Village, district, region
Districts: Kassena Nankana, Bolgatanga, Bawku
Geographical coordinates
Wuru (Kassena Nankana District) La:10° 59’ N / Lo: 1° 34’ W Vea (Bolgatanga District) La: 10° 52’ N / Lo: 0° 51’ W Kongo (Bolgatanga District) La: 10° 50’ N / Lo: 0° 42’ W
WHO sub-region {1-14}
1
Abstract We conducted an entomological study to document the effect of irrigation on the vectors and transmission dynamics of lymphatic filariasis in the Upper East Region of Ghana. Mosquitoes were collected by indoor spraying of houses in a cluster of communities located around irrigation projects (Tono and Vea) and others withoutreservoirs (Azoka). Anopheles gambiae s.s. was the dominant species and major vector, followed by Anopheles funestus. Anopheles arabiensis constituted 9-14% of the Anopheles gambiae complex but none were infective. Culex quinquefasciatuswas also not infective in these communities. Chromosomal examinations showed that >60% (n=280-386) of the Anopheles gambiae s.s. in irrigated communities were Mopti forms whilst 73% (n=224) in the non-irrigated area were Savannah forms. Infectivity rates (2.3-2.8 vs. 0.25), worm load (1.62-2.04 vs. 1.0), annual bites per person (6.50-8.83 vs. 0.47) and annual transmission potential (13.26-14.30 vs. 0.47) were significantly higher in irrigated communities.
Key information
- No. of different vectors in irrigated and non-irrigated regions - No. and distribution of sibling species of the Anopheles gambiae complex in irrigated and non-irrigated regions - Frequencies of Mopti and Savannah chromosomal population forms of Anopheles gambiae s.s. irrigated communities (Tono and Vea) and without irrigation (Azoka) - Entomological parameters for the transmission of bancroftian filariasis in irrigated communities (Tono and Vea) and without irrigation (Azoka)
Water resource development and management project
Kassena Nankana: Tono irrigation project Bolgatana: Vea reservoir
Type Irrigation canals, water storage for livestock Year of inception

68
Outcome measures (e.g. prevalence, incidence, # of cases, parasites density exposed population, etc.)
Mosquitoes collected from irrigated communities (Tono and Vea) and without irrigation (Azoka)
Tono Vea Azoka
Species no. % no. % no. %
Anopheles gambiae 1256 81.9 1831 73.1 756 87.7
Anopheles funestus 254 16.6 471 18.8 48 5.6
Anopheles pharoensis 0 0 27 1.1 2 0.23
Anopheles nili 0 0 14 0.6 0 0
Anopheles rufipens 24 1.6 0 0 0 0
Culex quinquefasciatus 0 0 128 5.1 51 5.9
Aedes aegypti 0 0 33 1.3 5 0.6
Total 1534 2504 862
Distribution of sibling species of Anopheles gambiae complex in irrigated
communities (Tono and Vea) and without irrigation (Azoka)
Localitiy No. examined No. of Anopheles gambiae s.s. (%)
No. of Anopheles arabiensis (%)
Tono 464 402 (86.6) 62 (13.4)
Vea 618 562 (90.9) 56 (9.06)
Azoka 356 306 (85.9) 50 (14.0)
Total 1438 1270 (88.3) 168 (11.7)
Frequencies of Mopti and Savannah chromosomal population forms of Anopheles gambiae s.s. irrigated communities (Tono and Vea) and without irrigated (Azoka)
Locality No. examined No. of Mopti No. of Savannah
Tono 464 280 (69.79 122 (30.4)
Vea 618 386 (62.5) 176 (37.5)
Azoka 356 82 (26.8) 224 (73.2)
Total 1438 748 320

69
Entomological parameters for the transmission of bancroftian filariasis in irrigated communities (Tono and Vea) and without irrigated (Azoka)
Locality Species No. dissected
No. with L3
Infective (%)
Total of L3 ABR AIBR Worm
load ATP
Anopheles gambiae
s.l. 1256 42 3.34 68
Anopheles funestus 254 0 0 0
Tono
Total 1510 42 2.80 68 315 8.83 1.62 14.30Anopheles gambiae
s.l. 1831 46 2.51 94
Anopheles funestus 471 6 1.27 12
Vea
Total 2302 52 2.30 106 283 6.50 2.04 13.26Anopheles gambiae
s.l. 756 2 0.26 2
Anopheles funestus 48 0 0 0
Azoka
Total 804 2 0.25 2 188 0.47 1.0 0.47 L3: infective third stag larvae of Wuchereria bancrofti; ABR: annual biting rate; AIBR: annual infective biting rate; ATP: annual transmission potential.
Before During After
Relative changes, risk (RR)
Additional notes
For prevalence rates of this region see: - Dunyo S.K.-Trans R Soc Trop Med Hyg. 1996 Nov-Dec; 90(6): 634-8. - Hunter J.M.-1992;35(5):627-45; discussion:645-9.

70
Appendix 6.14: key information form (Supali-2002-Am J Trop Med Hyg) WHO sub-region 11 Disease Lymphatic filariasis Author Supali T, Wibowo H, Ruckert P, Fischer K, Ismid IS, Purnomo, Djuardi Y, Fischer
P. Title High prevalence of Brugia timori infection in the highland of Alor Island, Indonesia.
Reference American Journal of Tropical Medicine and Hygiene. 2002 May;66(5):560-5. Language English Country, year of study
Indonesia, 2001
Village, district, region
Alor Island
Geographical coordinates
Lo: 124° 30’ E / La: 8° 20’ S
WHO sub-region {1-14}
11
Abstract To identify areas endemic for Brugia timori infection, a field survey was carried out in 2001 on Alor, East Nusa Tenggara Timor, Indonesia. Elephantiasis was reported on this island by villagers as a major health problem. Bancroftian filariasis was detected in four villages in the coastal area, whereas Brugia timoriwas identified in four rice-farming villages. No mixed infections with both species were found. In the highland village Mainang (elevation = 880 m), 586 individuals were examined for Brugia timori infection and 157 (27%) microfilaria carriers were detected. The prevalence of microfilaremic individuals standardized by sex and age was 25%. The geometric mean microfilarial density of microfilaremic individuals was 138 microfilariae/ml. Among teenagers and adults, males tended to have a higher microfilarial prevalence than females. Microfilaria prevalence increased with age and a maximum was observed in the fifth decade of life. In infected individuals, the microfilarial density increased rapidly and high levels were observed in those individuals 11-20 years old. The highest microfilaria density was found in a 27-year-old woman (6,028 microfilariae/ml). Brugia timori on Alor was nocturnally periodic, but in patients with high parasite loads, a small number of microfilariae was also detected in the day blood. The disease rate was high and many persons reported a history of acute filarial attacks. Seventy-seven (13%) individuals showed lymphedema of the leg that occasionally presented severe elephantiasis. No hydrocele or genital lymphedema were observed. This study showed that Brugia timori infection is not restricted to the lowland and indicated that it might have a wider distribution in the lesser Sunda archipelago than previously assumed.
Key information
- Prevalence of Wuchereria bancrofti, Brugia malayi and Brugia timori infections - Predominance of Wuchereria bancrofti, Brugia timori and Brugia malayi vectors (Anopheles subpictus complex and Anopheles barbirostris respectively)
Water resource development and management project
Normal agriculture
Type Rice

71
Year of inception
Outcome measures (e.g. prevalence, incidence, # of cases, parasites density exposed population, etc.)
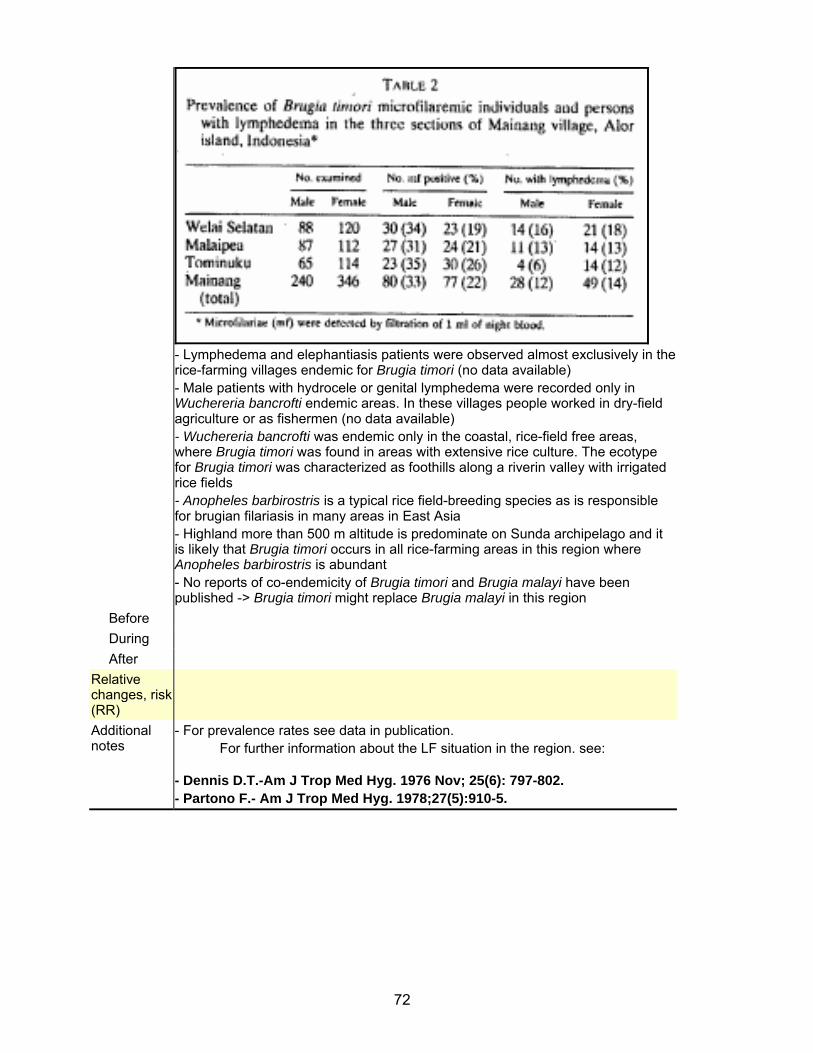
72
- Lymphedema and elephantiasis patients were observed almost exclusively in the rice-farming villages endemic for Brugia timori (no data available) - Male patients with hydrocele or genital lymphedema were recorded only in Wuchereria bancrofti endemic areas. In these villages people worked in dry-field agriculture or as fishermen (no data available) - Wuchereria bancrofti was endemic only in the coastal, rice-field free areas, where Brugia timori was found in areas with extensive rice culture. The ecotype for Brugia timori was characterized as foothills along a riverin valley with irrigated rice fields - Anopheles barbirostris is a typical rice field-breeding species as is responsible for brugian filariasis in many areas in East Asia - Highland more than 500 m altitude is predominate on Sunda archipelago and it is likely that Brugia timori occurs in all rice-farming areas in this region where Anopheles barbirostris is abundant - No reports of co-endemicity of Brugia timori and Brugia malayi have been published -> Brugia timori might replace Brugia malayi in this region
Before During After
Relative changes, risk (RR)
Additional notes
- For prevalence rates see data in publication. For further information about the LF situation in the region. see:
- Dennis D.T.-Am J Trop Med Hyg. 1976 Nov; 25(6): 797-802. - Partono F.- Am J Trop Med Hyg. 1978;27(5):910-5.