the association pour la santé publique du québec ... - aspq · intake of fat and sugar,...
TRANSCRIPT


The Association pour la santé publique du Québec (ASPQ) is an autonomous non-profit public health
organization, which contributes to the promotion, development and maintenance of the health and
well-being of the Québec population.
Cataloging data previous to publiCation
guidebook aimed at health professionals
lose weight for better not worse
includes bibliographical references
1. obesity 2. Weight control 3. Weight loss methods 4. public health
this guidebook was developed by the association pour la santé publique du Québec in collaboration
with the institut national de santé publique du Québec.
This document’s publication was made possible thanks to the financial contribution of Health Canada
within the prevention and promotion program of the Canadian diabetes strategy. the views herein
expressed do not necessarily reflect Health Canada’s official position.
authors:
• lyne Mongeau, institut national de santé publique du Québec
• Mireille vennes, association pour la santé publique du Québec
• véronique sauriol, association pour la santé publique du Québec
The reading committee significantly contributed to the writing of this guidebook, and the thoughtful
comments of its members improved the text. the following persons were members of the reading
committee:
• diane Côté, dt. p, présidente du Collectif action alternative en obésité
• odette Côté, b.sc., kinésiologie
• Harold Dion, MD CCMF FCMF, Président du conseil d’administration,
Collège québécois des médecins de famille
• Éveline Hudon, MD M. Cl. Sc.
• Marie-Ève turcotte, b. pharm.
• angèle venne, inf. b.sc.
We also wish to thank the following organizations and individuals for their collaboration to
this guidebook:
• Johanne laguë, institut national de santé publique du Québec
• richard Chevalier, Collège de bois-de-boulogne, journal la presse
• Julie trudel, institut national de santé publique du Québec
• valérie blain, association pour la santé publique du Québec
graphic design: studiométrique (www.studiometrique.com)
isbn 2-920202-44-8
legal deposit
bibliothèque nationale du Québec
library and archives Canada
all rights reserved, printed in Canada
© aspQ Éditions
association pour la santé publique du Québec
4126, rue St-Denis, bureau 200, Montréal, Québec, H2W 2M5
Telephone: (514) 528-5811 / Fax: (514) 528-5590
[email protected] / www.aspq.org

Losing weight: for better, not worse
Table of Contents
Introduction 2
Section 1: What you need to know about weight and weight lossWeight and health 3The ABCs of slimming down 6Consequences of various weight-loss methods 8Losing weight is not to be taken lightly 10Learn what it takes to act smart 11
Section 2: A look at weight-loss methodsA look at weight-loss methods: criteria and results 14Five points about weight-loss methods 25
Section 3: A detailed look at weight-loss methodsDescriptions of weight-loss methods 27Conclusion 39
Section 4: Additional informationA quick overview of weight-loss methods 40Ingredients found in weight-loss products 43Costs of weight-loss methods and comparison with a consultation with a health care professional 48Methodology 51Resources 56References 57

IntroductionIt is common knowledge that obesity and excess weight are on the rise in our population and our health is being threatened. However, many people, especially women, do not need to lose weight and are striving to conform to one prescribed notion of beauty.
While some of these people are trying to lose weight for the first time, many have already tried on their own or with the help of available methods. And there is no shortage of weight-loss products, services and methods (WLPSM) available in Québec! To paint a clearer picture of the current situation, in 2003 the Associa-tion pour la santé publique du Québec (ASPQ) and its partners conducted a comprehensive analysis on WLPSMs. For the purpose of this analysis, WLPSMs were defined as products (natural products, over-the-counter medication, meal replacements, etc.), services (weight-loss programs and centres, etc.) and methods (diets, fasting, etc.) designed for weight loss. Medical and nutritional interventions regulated by a professional order, including anorexiants (appetite sup-pressants) prescribed by doctors and personal weight-control practices (watching intake of fat and sugar, exercising, etc.), were not included in the study.
In this analysis, WLPSMs were inventoried, defined in great detail and assessed according to criteria from scientific documents that were validated by a panel of experts from Québec. These established the requirements for several dimensions of healthy weight loss. The general finding from this analysis is that the majority of WLPSMs do not meet many of the weight-loss criteria. Consequently, it is not appropriate to recommend their use for the population in general; however, a few could be used as adjutant to weight control interventions by some individu-als under the supervision of a competent professional. In order to help health care professionals find their way through the maze of WLPSMs, the ASPQ and the Institut national de santé publique du Québec (INSPQ) joined forces to produce this reference guide. It contains helpful, accurate and up-to-date information for professionals so they can help their clients make informed decisions.
Although this guide is not a reference book on how to counsel people controlling their weight, it outlines the basic principles in helping clients make safe and responsible weight-control choices. In addition to the key concepts of weight loss and information on WLPSMs, you’ll find suggestions on further reading and on other resources to shed new light on the choices available to people who are concerned about their weight.
Losing weight: for better, not worse
2

3
SECTION 1 : What you need to know
about w
eight and weight loss
Losing weight: for better, not worse
Weight and healthClearly, weight is a health determinant. A body mass index (BMI) between 18.5 and 24.9 kg/m2 is considered an normal weight. Beside weight, many factors determine a person’s health. The Canadian Guidelines for Body Weight Classifica-tion in Adults1 state that in the individual, the estimation of an individual’s health risk should not be based on measures of body weight and waist measurement alone. Weight is therefore only one part of the picture. When BMI is higher than 25 kg/m2 and waist circumference above the risk threshold losing weight may be beneficial for health. The result shouldn’t, however, be counterproduc-tive, and methods should not be harmful (see The ABCs of losing weight and
Consequences of WLPSMs). Would it not be paradoxical to damage health while trying to improve it?
Because body image is an important part of our culture, many people tend to attach too much importance to weight and forget lifestyle habits and other determinants of health. Losing weight is not the only way to obtain better health: quitting smoking and managing stress are also great ways to become healthier. Eating less fat and starting walking, even in the absence of weight loss have the potential to improve health. Additionally, some studies show that clients aim to lose 20 to 30%3,4 of their initial weight, which is not realistic from metabolic and behavioural standpoints. More importantly, this amount is far more weight than necessary to obtain health improvements. Recent scientific studies show that health can improve as a result of a moderate and maintained weight loss of 5-10% of the initial weight.5 Pursuing unrealistic weight-loss goals has been shown to lead to failure and discouragement6, partly because the weight-loss goal becomes a fixed idea. If clients cannot be persuaded to set realistic weight-loss goals compatible with health improvements, they run the risk of frequently chang-ing diet methods and getting caught in a dieting cycle.
Obviously health improvements will be maintained only if the lost weight is not regained. There is not much point in encouraging weight loss if a professional evaluates that a client will not be able to maintain the new weight. The choice of changes to put into place must take into consideration how long new habits can be maintained. Professionals should also ensure that methods will result in a loss of fat, and not water or muscle mass. In order to avoid these negative consequences, the choice of method is again essential.

4
SECT
ION
1 : W
hat y
ou n
eed
to k
now
ab
out w
eigh
t and
wei
ght l
oss
Losing weight: for better, not worse
Explaining these issues to clients should help reduce their desire to lose weight rapidly and in large amounts. It is essential to clearly explain the relationship between weight and health to clients who come for a weight-loss consul-tation. The following diagram (Figure 1), which is easily explained, can help put things into perspective. Clients will be interested to know that the relationship be-tween changes in diet, being physically active, losing weight and increasing health is not linear. Scientific studies of the last several years have shown that weight is not necessarily the most important element of the lifestyle-weight-health triad.
Lifestyle
Weight
Health
Figure 1 – Lifestyle, weight and health connections
Rethinking old ideas
Firstly, more than a person’s weight, localization of excess fat is a major de-terminant of health risk.1 Thus, many women who have heavier hips, thighs and buttocks wish to slim down to meet certain beauty standards, but this perceived excess weight does not represent a health risk.
Secondly, as shown in Figure 1, lifestyles alone can have a direct impact on health regardless of weight. Recent large-scale cohort studies on men and women have shown that being physically active markedly reduced the risk of seri-ous illness linked to obesity (Type II diabetes, high blood pressure, cardiovascular disease and some cancers), regardless of the BMI.7,8
Along the same lines, a recent meta-analysis came to the following conclusions: 1) regular physical activity markedly reduces health risks associated with excess weight and obesity; 2) obese persons who are physically active can reduce their risk to the extent that their morbidity and mortality rates are lower than that of men of normal weight who are sedentary; 3) a sedentary lifestyle and low cardiorespira-tory fitness are just as important as excess weight and obesity in predicting mortal-ity.9 The hypothesis that a healthy diet also reduces risks associated with obesity has been verified in fewer large-scale studies.

5
SECTION 1 : What you need to know
about w
eight and weight loss
Losing weight: for better, not worse
Ultimately, weight regulation depends on several factors: physiological mechanisms and compensatory behavioural reactions, modification of muscle mass, etc. The reading on the bathroom scale does not always tell the whole story. Viewing weight loss as the only indicator of success can lead to nega-tive effects. For health practitioners, a lack of weight-loss success in clients can reduce work satisfaction and lead to reduced interest in weight control counselling in the long term. For clients who do not experience significant weight loss, efforts made to change their diet and level of physical activity may be seen as sterile, even as a complete failure. From a behavioural and psychological perspective, the absence of results in terms of weight-loss acts as negative reinforcement. Enough for one to be discouraged for a long time.
By focusing on health results, improved quality of life and on the change
process instead of measuring results only in terms of weight lost,
health-care professionals can help people feel better about the investment
they have made in their health. They will be less attracted to WLPSM
and their promises.

6
SECT
ION
1 : W
hat y
ou n
eed
to k
now
ab
out w
eigh
t and
wei
ght l
oss
Losing weight: for better, not worse
The ABCs of weight lossWeight generally remains stable when the following equation is balanced:
amount eaten = energy spent
Weight loss occurs in an energy deficit that can be brought about in
three different ways:
1. Solely by increasing the amount of energy spent while maintaining the amount of food consumed
2. Solely by reducing the amount of food consumed while maintaining the amount of energy spent
3. By using both strategies and reducing the amount of food consumed while increasing the amount of energy spent.
Although the first solution is the best, it is not very realistic for many peo-ple. The amount of physical activity required to lose weight is very high and must be done frequently. This requires a lot of effort and many people cannot keep up. Solution 2 is the most popular, because it is perceived to be easier to restrict food intake. Solution 3 is optimal, because it promotes better maintenance of muscle mass and does not require as stringent a restriction in food intake.
WLPSM promoters look less favourably on solutions 1 and 3 because the concept of effort is harder to sell. They therefore resort to solution 2 or, in order to bring about results in a majority of persons, they rely on various strategies that require significant energy restriction that is not initially apparent. Initially, regardless of its extent, energy restriction will almost always lead to weight loss as glycogen stores are used up. Subsequently, strict energy restriction can also result in significant weight loss, but the body may lose water and muscle mass in addition to the desired loss of fat.10
Other than energy restriction, a balance of macro-nutrients (proteins, carbo-hydrates and fats) in the diet is also very important during weight loss. A low carbohydrate diet is likely to cause higher water and muscle mass loss than other types of WLPSM. This can be explained as follows: some tissue, especially the brain and neurons, need carbohydrates to function. When they are deprived, they use stored carbohydrates, but the body doesn’t store much carbohydrate, and when these have been used up the muscles become a source of carbohy-drates (after undergoing a transformation). Unfortunately (!) fat stores cannot sup-ply much carbohydrate. A professional should always ensure that a moder-ate energy restriction is used and that macro-nutrient intake is balanced.

7
SECTION 1 : What you need to know
about w
eight and weight loss
Losing weight: for better, not worse
What is a moderate restriction?
Even if weight loss can benefit some people, the body interprets restriction as a threat, a violation of its homeostasis. The more energy is restricted, the harder the body fights back. Paradoxically, the body protects its fat reserves and uses its muscles as back-up energy. Loss of muscle mass brings about water loss and reduces basal metabolism because muscles burn a lot of energy.10 A diet of fewer than 1000 calories can result in a 20% loss in muscle mass within just a few weeks.11 Even losing just a half kilogram of muscle slows down one’s metabolism.12 Health professionals should steer clear of muscle mass reduction in their clients, because a person with small muscle mass has a higher likelihood of gaining weight later.13,14
To appropriately determine a client’s energy restriction, there is only one method: the starting point must be known, i.e. usual energy intake.15 Such an assessment is the work of a professional, such as a dietician. No WLPSM be-gins with an assessment of a person’s usual food intake – the majority are based on a fixed energy level. Because of this, commercial weight-loss programs deemed acceptable, even recommended by many professionals, may induce a significant energy restriction. For example, a program recommending 1200 kcal/day may seem completely safe. But for a person who usually takes in 2400, this is a 50% reduction that is significant enough to offset the metabolism’s defence mode.
What’s more, consuming 800 to 1200 kcal/day is less than what the majority of healthy adults need16, and this will likely harm normal functioning. Unfortunately, the consequences of differential levels of energy restriction are not fully known, there are also many factors that come into play, and there have not been enough studies to be adequately informed. In any case, it is wise to limit the dif-ference between energy spent and energy consumed to between 500 and 700 kcal/day.17

8
SECT
ION
1 : W
hat y
ou n
eed
to k
now
ab
out w
eigh
t and
wei
ght l
oss
Losing weight: for better, not worse
Consequences of various weight-loss methodsThere are some harmful physical, behavioural and psychological consequences as-sociated with WLPSMs. Instances of short- and long-term physical consequences have been documented, varying from minor impacts to death. Consequences depend on many things, including the length, nature, method and degree of restriction imposed.18 Short-term consequences such as constipation or diarrhea, low blood pressure, headaches, dizziness, intolerance to cold, muscle cramps, hair loss, etc.19,20,21 may be considered minor if the therapy is used oc-casionally and is short term. But when losing weight becomes a lifestyle, as it is for some people, as benign as the physical manifestations may be, they affect productivity.22 Arrhythmia (irregular heartbeat), heart attacks and electrolyte imbal-ances have been associated with very low calorie diets.18 For more than 25 years, death has even been linked to these diets.20 More recently, in the early 1980s, six deaths were reported with the Cambridge liquid diet.20
Weight loss and cognitive restriction23 (replacing eating habits that are regulated by internal bodily needs by ones that are planned and set according to cognitive criteria, or modeled on set diets, or even an overall reduced food intake) are also associated with a reduction of bone mass, which can increase risk of osteoporo-sis.24,25,26 Cognitive restriction has also been linked to the development of men-strual cycle disorders.27,28,29 Gallstone formation is a known risk of restricted diets that result in a weight loss of more than 1.5 kilograms per week.18
Beyond physical consequences, there are numerous psychological barriers linked to a preoccupation with weight that prevent the adoption of healthy lifestyles. Fear of weight gain is just one of the reasons why people choose to continue smoking or keep other negative habits.30 Studies have shown that anxiety about being judged on one’s body can stop people from exercising.31,32,33,34 How-ever, others argue that being preoccupied with one’s weight can be a motivator to control weight, and is therefore beneficial. Some studies have actually shown that people trying to lose weight exhibit a better nutritional profile.35,36 The topic is still rather controversial – although some people benefit from being preoccupied with their weight, when the distress associated with body image increases its tends to bring about negative consequences.37

9
SECTION 1 : What you need to know
about w
eight and weight loss
Losing weight: for better, not worse
Restricting energy intake commands important behavioural modifications. Eating 500 to 700 kcal per day less than usual involves significant changes in a person’s behaviour. If intake is further reduced, greater is food limitation, creating obsessions and associated reactions (depression, irritability, anxiety, anti-social behaviour, mood swings, poor self-image, etc.).38,39,40,41 By paying attention to the body’s outer signals, people can become more and more cognitive eaters which changes their way of seeing food.42 Frequent dieting can lead to the development of eating disorders, especially compulsive eating. 38,39,43,44,45
Finally, users of WLPSMs often have a high chance of regaining weight previously lost and to experience failure. Failing one’s attempt to lose weight over and over again can result in lowered self-esteem, self-confidence and a feel-ing of powerlessness. Health care professionals should not downplay any feelings of shame or guilt in persons who have failed to gain control of their weight.46,47,48,49

10
SECT
ION
1 : W
hat y
ou n
eed
to k
now
ab
out w
eigh
t and
wei
ght l
oss
Losing weight: for better, not worse
Losing weight is not to be taken lightlyThe previous pages clearly show that having a normal and stable weight is a major part of being healthy. But it is also clear that losing weight at any price is not recommended. However, the importance of weight loss is often overlooked as it is often thought of as commonplace. Weight loss is discussed everywhere, with anybody. It doesn’t help that WLPSMs are now so widely accessible and adver-tised at prime time and seen in newspapers and popular magazines, which makes them ubiquitous in people’s lives. Claims of instant weight loss without mention of negative side effects only make them more attractive.
What’s more, without safeguards, recommendations or regulation by authorities and health care professionals, the population is indirectly told that WLPSMs are an easy and effortless way to end obesity and achieve the “perfect” body. As a result, overweight people may feel increasingly guilty and under pressure as WLPSMs are made more accessible, because the misconception will be that they failed to use the apparently easy and available solutions.
The lack of thought given to weight loss, weight-loss products and adver-tising has contributed to making them simple consumer goods, without much consequence other than on one’s wallet. However, when weight loss upsets a body’s balance we are no longer talking about economic consumption. Some people become ill after taking a weight-loss product – this is not something to ignore – and unfortunately side effects of WLPSMs often remain unknown be-cause many people think that they have failed and are uncomfortable talking about it. The fact that no one complains does nothing to help control the weight-loss industry.
Within this context, recommendations on weight loss from health-care profes-sionals can be made too hastily: a reflex suggestion to join a program or go on a popular diet without taking time to spell out the pros and cons. Similarly, a profes-sional who does not dissuade a client who is keen to use a WLPSM can be seen as giving approval.

11
SECTION 1 : What you need to know
about w
eight and weight loss
Losing weight: for better, not worse
Understand to better counselThe effectiveness of weight-loss methods and their possible harmful side effects forces professionals to assess how they can truly help their clients. First, ap-proach the situation with seriousness. Weight issues constitute a very complex and heterogeneous condition. The increase in our population’s weight can be explained by our sedentary lifestyle and poor diets. Although these two factors might explain obesity in a person who consults a professional, they represent only two of the many possible causes. In fact, a clinician who meets an obese or overweight person will make a more complete analysis of the situation by looking at all appropriate causal factors. (Figure 2).
Figure 2- Range of factors causing excess weight and obesity in individualsSource: CAAO 2003
Biologyheredity, glands, illness, taking medication, metabolic upset associated with quitting
smoking and the yoyo syndrome, gender, age and race
Personal aspectsperfectionism, low esteem and self-affirmation, difficulty expressing
oneself, poor body image, anxiety, stress, secondary gainsfrom being obese
Sociocultural aspectsstandards of beauty, environment,
type of employment, socioeconomicstatus, support, encouragement
or pressure
Habits and family lifeeating and exercising habits, familydynamics, parents’ preoccupation
with their weightSelf-
image
Bodyweight
physical activity
eatin
gha
bits
Using this list, the professional and his or her client will together make a more thorough analysis of possible causes. Following this, it is a good idea to divide what can be changed from what cannot, then to establish the importance of each proposed change. When possible, it is better to act on causes of weight gain. For example, a person who gained a lot of weight because of a change in employment would need to recognize what specific changes brought about the weight gain, and then find ways to adapt. This approach has more staying power than a popular diet that does not take any causal factors into consideration.
On the other hand, it would be difficult to act on causes for a weight gain that occurs after quitting smoking, unless it is clearly linked to compensation by eating more. It is basically impossible to find causes in the case of a person with a normal weight who wants to slim down. The intervention could include an explanation of the connection between weight and health, a person’s biology and natural ability to control weight and should try to determine if the person needs help reviewing his or her body image.

12
SECT
ION
1 : W
hat y
ou n
eed
to k
now
ab
out w
eigh
t and
wei
ght l
oss
Losing weight: for better, not worse
Finally, for a person whose causes for weight gain include serious and ingrained psychosocial factors (history of abuse, secondary gains of being obese, emotional deprivation, etc.), the analysis must include the effort necessary to achieve the goals. Simply improving lifestyle and habits without a goal to lose weight may be more realistic and beneficial overall.
Why does your client want to lose weight?
In 1998, 88% of overweight women in Québec stated that their desire to lose weight was to “improve their appearance” versus 82% who “wanted to be health-ier”.50 Aesthetic motivation is dominant for normal weight or underweight women. Besides beauty and health reasons, weight loss can be motivated by a desire to reach other goals, such as improving self-confidence, increasing attrac-tiveness, capacity to affirm yourself, or because a person does not believe him or herself capable of something in particular unless weight loss has been achieved.5 These expectations are fed by the idea we see in the media and in ads whose message is that thin equals youth, success and competency. In general, weight loss alone is not likely to transform anyone. A person will notice this too when they fail to reach their goals. Not getting the expected benefits is another reason why people fail to keep new habits even after reaching weight-loss goals.
It is therefore imperative to understand a client’s real motivations. What does the client really hope to gain by taking this step? Necessary changes should be suggested based on the client’s level of motivation. Making a huge effort for small expected gains can cause the client to give up. With this in mind, both ex-pectations and the actual amount of weight to be lost must be realistic.
Weight-control intervention is clearly quite complex and full of nuances. Practitioners might have to deal with a large range of issues, much more than just eating habits and physical activity. Faced with this challenge, WLPSMs are of little use and remain potentially harmful. However, helping and supporting a person with a weight problem is a real challenge for professionals. When it is done well, the work can be very gratifying.
13
SECTION 1 : What you need to know
about w
eight and weight loss
Losing weight: for better, not worse
What conditions are likely to result in the professional’s and client’s success and satisfaction?
• Set a realistic goal for actual weight lost and weight-loss expectations.• Explain the connection between weight, lifestyle habits and health.• Explain how positive lifestyle changes can occur, even without weight loss. • Ensure the client understands the physiological limits of losing weight: the consequences of using WLPSMs and when severely restricting energy• Adjust changes to be made based on client’s level of motivation.• Ask clients to think about the importance of making long-term changes and how to go about doing so.• Encourage small actions that are more likely to succeed and ensure the process is followed through.• As much as possible, apply only a moderate food restriction and add physical activities.

14
Losing weight: for better, not worse
SECT
ION
2 : A
look
at w
eigh
t-lo
ss
met
hods
A look at weight-loss methods: Criteria and results The analysis of WLPSMs conducted in 2003 by the ASPQ and mentioned in the introduction of this guide was carried out in several steps. First, as many WLPSMs as possible were identified by using different sources of information. Between November 2002 and January 2003, approximately 350 WLPSMs were inventoried from newspapers, magazines, television, Internet, etc. Following this, more than 215 WLPSMs were described in detail and analyzed.
In order to conduct and give the critical analysis a solid basis, the analysis criteria had to be defined for weight-control practices. These criteria, taken from scientific documents and recommendations from organizations interested in the issue of weight, were ratified by a committee of experts.
TYPES OF CRITERIA
The rate of weight lossApproach required for a program or method (including supervision)Dietary intervention Physical activityEffectiveness of the approachSafety of the approach Promotion and advertising surrounding the approachCost of the approach
The following were observed during the critical analysis of the various WLPSMs chosen:
• Many types of WLPSMs are highly accessible and widely advertised;• In general, WLPSMs do not meet the criteria for healthy weight control practices;• Many WLPSMs do not offer solutions adapted to the needs of people who are in a comprehensive change process concerning weight issues;• Using WLPSMs could result in gaining weight back in the short- or long-term or in a failure while attempting to lose weight. This could affect the client’s physical and psychological health;• Not enough is known on the subject to confirm or disprove the effectiveness, danger or harmlessness of many WLPSMs listed.
In the next pages, the analysis criteria of weight control practices are listed, fol-lowed by results of the analysis. The methodology used to identify WLPSMs and how the analysis criteria were developed is described in greater detail on page 49.

15
Losing weight: for better, not worse
SECTION 2 : A look at w
eight-loss m
ethods
The rate of weight lossIf we keep in mind that, when medically indicated, a weight loss of 5-10% of
the initial weight can improve a person’s health, the method used should pro-
mote gradual weight loss, in other words a maximum average loss of 1-2 lbs.
(0.5-1 kg) per week, which translates into a reduction in energy intake of
500-1000 kcal (2000-4000 kJ) per day, and an intake of energy not lower than
1200 kcal (5000 kJ)-1500 kcal (6500 kJ) a day, for women and men respectively.
Ideally, a mixed strategy should be used, in order to promote spending more en-
ergy so the amount of food consumed does not have to be so strictly reduced.
The key ingredient is for weight loss to occur gradually. Only 6% of WLPSMs analyzed meet this criterion and encourage a loss of 2 lbs. or less per week. Conversely, 30% recommend quick weight loss, and some even go as far as to say, “Lose 25 pounds in 30 days.”
Some WLPSMs use a “health discourse,” suggesting gradual weight loss, but at more than 2 lbs. per week.

16
Losing weight: for better, not worse
SECT
ION
2 : A
look
at w
eigh
t-lo
ss
met
hods
The approach used (including supervision)Weight loss should be handled using a global approach (incorporate eating
habits, physical activity and behaviour modification), and yet be personalized
(based on the client’s bio-psychosocial assessment and age).
In a global approach to weight loss, no product, food supplement or device
should be required to accompany eating and physical activity plans.
Supervision during weight loss should be provided by a health-care profession-
al, such as a doctor, nurse, dietician or kinesiologist and ideally by a multidisci-
plinary team of health-care professionals.
Those who develop the method should be or should include health-care profes-
sionals, such as doctors, nurses, dieticians and kinesiologists who hold rec-
ognized credentials or have in addition received training in one of the following
fields: nutrition, metabolism, physiology or related fields. These people should
also be part of a multidisciplinary team.
The approach
In general, a global approach is not promoted by the WLPSM industry. Less than 1% of WLPSMs analyzed use this approach. For some, complementary products are suggested but no additional products should be necessary when using a global approach to weight loss. Some WLPSMs even have their own definition of “global» and promote so-called complementary or essential products and/or new technologies.
Some advertisements featuring WLPSMs are contradictory. Even though a global approach is promoted, client testimonials feature people who are thrilled to be able to keep eating the way they used to, as long as they respect the caloric limit proposed in the WLPSM. It is therefore difficult to qualify these WLPSMs as using a global approach.
Less than 1% of WLPSMs could qualify as using a personalized approach, but since this officially also incorporates a thorough bio-psychosocial assessment, no WLPSM analyzed meets this criterion.
Some claim to use a personalized approach, especially weight-loss programs and centres. However, it is wise to make a visit to be sure that their claims are valid.
When investigating franchises, one must check that a personalized approach is used in every location. In many cases the personalized approach turns out to be supplying clients with a range of products, claiming to be adapted to the consumer while no global assessment of his or her real needs has been made.

17
Losing weight: for better, not worse
SECTION 2 : A look at w
eight-loss m
ethods
Supervision
Supervision available during weight loss is rarely through a qualified person. Less than 5% of WLPSMs – essentially weight-loss programs and centres – claim to of-fer supervision by health-care professionals, such as doctors, nurses, dieticians or kinesiologists. At best, a dietician would work as a program or method supervisor but does not offer adapted services directly to the client. Thus, there is no multidis-ciplinary expertise readily available.
Rather than offering organized supervision, some WLPSM developers and promot-ers are now offering supervision and guidance through the Internet. Some provide their clientele with on-line monitoring, which might include a BMI calculation, reci-pes and helpful tips, discussion groups, etc. In some cases, on-line consultations with professionals are available, but it is nevertheless difficult to establish their suitability.
Lastly, less than 5% of WLPSMs are developed by health-care professionals, for example, physicians in the case of popular diets. In one case, the approach and proposed products were said to have been examined by a multidisciplinary team acting as advisors. Some natural products are developed by pharmaceutical labo-ratories, and others are developed by naturopaths or independent herbalists.

18
Losing weight: for better, not worse
SECT
ION
2 : A
look
at w
eigh
t-lo
ss
met
hods
Dietary interventionThe weight-loss approach should promote healthy eating based on a varied
diet from the four food groups described in Canada’s Food Guide to Healthy
Eating (CFGHE)51, according to Canada’s Guidelines for Healthy Eating.51 In a
personalized approach, weight loss should be combined with dietary recom-
mendations based on an assessment of the individual’s eating habits.
Without a doubt, a healthy diet is essential to good general health. However, less than half of WLPSMs (40%) suggest following a healthy, balanced diet and 38% do not even refer to it. In other cases, the concept of healthy eating is used by WLPSMs to claim the enhancement of the effectiveness of the approach.
Approximately 10% of WLPSMs go as far as minimizing the importance of diet, stressing their approach requires no effort, no deprivation, and no changes in eating habits.
What’s more, 12% of WLPSMs fail to meet healthy eating principles because:
• They promote a diet too low in energy;
• The distribution of macro-nutrients is very different from what is suggested in Nutrition Recommendations for Canadians;52
• They lack variety, a basic principle of Canada’s Guidelines for Healthy Eating (ex.: unbalanced diet, eating only one food, too many restrictions, using meal-replacement products).
For less than 2% of WLPSMs, personalized eating plans are allegedly offered, but in many cases healthy eating is proposed only as a complement to the products.
Lastly, less than 5% of WLPSMs directly refer to Canada’s Food Guide to Healthy
Eating, which should serve as the basis for food interventions proposed in the programs.

19
Losing weight: for better, not worse
SECTION 2 : A look at w
eight-loss m
ethods
Physical activityThe approach used to lose weight should promote regular physical activity
(ideally 30 minutes a day), and this should be introduced gradually based on
the client’s age and existing physical activity habits.
We already know that playing sports or being active regularly benefits health. According to scientific documents53, physical activity is the main factor in keeping weight off. Interestingly, 58% of WLPSMs analyzed make no reference to physical activity and some of them go as far as downplaying its importance, stressing their approach requires no effort, no exercise, and no lifestyle changes.
Within the range of available WLPSMs, only 34% encourage physical activity. Most contain general statements explaining that physical activity can benefit health. Once again the notion is used to enhance the perception of effectiveness.
There is generally little information provided on the frequency and duration of physical activity. However, 11% of WLPSMs give instructions and promote regular exercise, sometimes including an activity list.
With the exception of training centres that usually offer exercise programs adapted to clients’ needs, there exists practically no personalized and progressive plan based on a needs assessment.

20
Losing weight: for better, not worse
SECT
ION
2 : A
look
at w
eigh
t-lo
ss
met
hods
Effectiveness of the approachThe weight-loss approach should be based on well-founded scientific prin-
ciples, including evidence-based data. Its long-term effectiveness (1 year
minimum) should also be assessed.
Effectiveness is interpreted differently from one WLPSM to another and it usually implies the short-term. If we consider a definition of weight-loss maintained over 1, 3 and 5 years, very few weight-loss methods qualify. Additionally, keeping in mind that an approach’s effectiveness and safety is based on different criteria (global and personalized approach, gradual weight loss, professional supervision), no WLPSMs analyzed can qualify.
During analysis, one way to verify the effectiveness and safety of a natural product claiming therapeutic properties is to see if it bears a DIN (Drug Identification Num-ber). A DIN guarantees that a product’s safety, effectiveness and quality have been examined by the Therapeutic Products Directorate (TPD).54 In the future, natural products will need to be labelled with a product number (NPN)55 to be marketable.
At the time of analysis, less than 6% of WLPSMs listed in categories that required their products to bear DINs had such a number. Meal replacements are not subject to this requirement, but are governed by specific regulations.56
Of all the WLPSMs analyzed, excluding those with a DIN:
• Just over 1% figure in statistics and less than 3% are mentioned in reliable and thorough studies able to demonstrate their effective weight-loss properties. In two cases, some active ingredients were rigorously studied, but not the entire product;
• At least 3% were part of rigorous studies that showed they were not effective for weight loss or were recognized as being ineffective. More than half of these are devices or machines, while the others supposedly bring about substantial weight loss by transdermal means.
While all WLPSMs analyzed claim they are effective for weight loss, more than one third contain one or several ingredients found on lists of weight-loss ingredi-ents banned by the Food and Drug Administration (FDA)57 because they were not shown to be effective.

21
Losing weight: for better, not worse
SECTION 2 : A look at w
eight-loss m
ethods
Safety of the approachThe weight-loss approach used must be safe, meaning that there should not be
doubt as to its safety.
There are very few thorough studies that demonstrate the safety of WLPSMs. Yet, in their documentation and advertising, they make safety claims, such as “no side effects” and “no risk.”
It is possible that ingredients found in some products are not dangerous on their own, but they could increase health risks if a global approach requiring a significant energy restriction is followed (ex.: consuming only a liquid formula over a span of several days).
Analysis shows that at least 34% of WLPSMs come with warnings, either on the label, in the accompanying documents or in advertisements. Most commonly, these warnings are general in nature and address children, pregnant women and women who are nursing. They are sometimes presented in the form of recom-mendations to consult a doctor before starting any weight-loss method or using a particular WLPSM (something that products from the United States are required to mention in their advertisements).
There are also warnings that accompany devices and machines that may affect people who have pacemakers or other medical devices (ex.: medical pumps). In certain cases, the warnings are not found on the packaging, but rather on the ac-companying documents inside.
Many products contain ingredients (ex.: cascara buckthorn, milk thistle, high mal-low, psyllium, senna, etc.) with known side effects, yet no warning appears on the label. Out of 215 WLPSMs analyzed (where the list of ingredients was available), 49 contained ingredients known to have side effects, contraindications or possible interactions with foods or medications (see the chart of natural products on page 41). The majority of these products do not come with any warning. In other cases, warnings are often general and do not address the problematic ingredient.
At least 6% of WLPSMs are presented as harmless, without side effects, but one of them contains high levels of bladderwrack and the resulting high level of iodine increases the risk of hyperthyroidism58. Its use is therefore contraindicated.57
Finally, in some cases it is not possible to confirm the safety of a product because the list of ingredients (mostly for mail-order products) is not accessible.

22
Losing weight: for better, not worse
SECT
ION
2 : A
look
at w
eigh
t-lo
ss
met
hods
Promoting and advertising the approachThe claims of a weight-loss approach should respect current laws and regula-
tions. They should make realistic affirmations and contain correct and complete
information.
Analysis of WLPSM promotion and advertising shows there are significant differ-ences between their alleged benefits and healthy weight-control practices. Various marketing strategies for WLPSMs are shown in the following list.
Main strategies used in advertising (not mutually exclusive)
• Natural• Scientifically proven/clinical study/approved by an MD• Health discourse• Impressive photos• Testimonials• Guarantee• Permanent weight loss• Effortless (no need to eat less and/or no exercising)• Before and after photo shots
The popular “health discourse” marketing strategy includes statistics on over-weight and obesity in commercials and the various ways these conditions affect health. The consumer is fooled thinking he or she is dealing with a weight-loss specialist. Once trust is gained, the consumer uses a product that seems harmless and believes it to be the solution to weight loss.
For several of the WLPSMs analyzed, dubious marketing strategies were employed (experience weight loss while sleeping, permanent, substantial in little time and sensational testimonials). These marketing strategies were revealed after a major study59 was published by the Federal Trade Commission (FTC) covering 300 WLPSMs available in the United States.
In the analysis, 30% of medications sold without a prescription, food supplements, creams, body-wrapping techniques, patches, devices and appliances were recog-nized as using implausible allegations in advertisements according to experts at a FTC meeting.60
23
Losing weight: for better, not worse
SECTION 2 : A look at w
eight-loss m
ethods
Claims deemed as implausible:
• Everyone will experience substantial weight loss • Lose weight permanently• Lose a substantial amount of weight and still eat unlimited amounts of calorie-rich food • Lose a substantial amount of weight by blocking fat or calorie absorption• Lose a substantial amount of weight by using a particular transdermal product• Lose a substantial amount of weight without reducing energy intake or increasing physical activity• Safe weight loss of more than 3 lbs. per week for more than four weeks.
Several WLPSMs products are presented as useful adjuncts in treating obesity or even diabetes. Article 3 of the Canadian Food and Drugs Act says, “No person shall advertise any food, drug, cosmetic or device to the general public as a treat-ment, preventative or cure for any of the diseases, disorders or abnormal physical states referred to in Schedule A.”61 Obesity is a disease listed in Schedule A.
During this analysis, it was not possible to verify if the labelling and allegations of all products sold as meal replacements respected the Food and Drugs Act, in terms of foods used in special diets.
Similarly, the Québec magazine Protégez-Vous conducted a study in March 199862, on meal replacements in an effort to reveal problems with labelling and erroneous claims. This study showed several infractions of Canadian regulations B.24.202 and B.24.204 of the Food and Drugs Act and the Guide to Food Label-
ling and Advertising. It also revealed a number of important elements that did not conform to the Guide.

24
Losing weight: for better, not worse
SECT
ION
2 : A
look
at w
eigh
t-lo
ss
met
hods
Costs of the approachWeight-loss products and methods should come with complete information
on the total potential cost of the weight-loss approach (including all its
components).
Weight-loss services should offer complete information on the total potential
cost of the weight-loss approach (including all components and follow-up) as
well as instalment payment methods.
Using WLPSMs in a weight-loss approach can be expensive. There are often addi-tional costs that arise from purchasing products or services suggested to enhance results. The chart on page 46 illustrates the potential costs of a weight-loss ap-proach that uses WLPSMs and compares it to the cost of consulting a health-care professional.
The fact that WLPSMs are very prevalent and visible detracts from concern about their high cost. Out of 215 WLPSMs evaluated, at least 60 were available in pharmacies, 88 in health-food stores and almost all were available on the Internet. Accessibility will probably increase because pharmacies and health-food stores are popping up in larger supermarkets or department stores and the topic of obesity is very present in the media.

25
Losing weight: for better, not worse
SECTION 2 : A look at w
eight-loss m
ethods
Five points about weight-loss methods 1. Industry legislation
• In Québec and Canada there is no legislation pertaining to the WLPSM industry.• A lack of resources prevents the thorough application of regulations on certain components of WLPSMs, most notably public fraud, contracts governed by the Consumer Protection Act and the Food and Drugs Act.• In many cases, government does not intervene until a complaint has been made. Unfortunately, people who put weight back on rarely complain, especially because they consider themselves as responsible for failing.
2. Effectiveness• Few thorough studies support affirmations of WLPSMs’ long-term safety and effectiveness.• Repeated failures, due to lower mid- and long-term effectiveness of WLPSMs, can hinder the healthy control of one’s weight.
3. SafetyA WLPSM may be dangerous:
• Because it causes overly rapid weight loss, which results in a loss of muscle mass, resulting in a slower metabolism;• Because it denies or neglects the importance of lifestyle changes and it is the maintenance of a lower weight over the long term that really matters for health;• Because it can cause minor undesirable side effects (fatigue, constipation, nausea and diarrhea) that reduce a person’s general productivity and well-being;• Because it can cause major undesirable side effects (arrhythmia, electrolyte imbalances, development of eating disorders, formation of gall stones, decrease in bone density and death).
4. Supervision• Pretention of supervision that responds to specific individual need is common.• Supervision offered through programs and commercial weight-loss centres is not generally provided by health-care professionals, despite promoters’ confusing claims regarding specialties and titles.
5. Natural does not necessarily mean safe• The erroneous belief that natural products are safe and do not have undesirable side effects is widespread and would explain in part the interest in these products and the tendency among some to self-medicate.

26
Losing weight: for better, not worse
SECT
ION
2 : A
look
at w
eigh
t-lo
ss
met
hods
• Whether intentionally or not, individuals usually fail to inform health-care professionals that they are taking natural products.• Several adverse side effects are due to the significant variation in the quality and quantity of ingredients found in natural products.• The complete list of ingredients, their amounts and known side effects are not always mentioned on the label.
WLPSMs are increasingly part of the problem rather than the solution because they can act as significant obstacles to the adoption of a healthy approach to a weight problem or body-image problem.

27
Losing weight: for better, not worse
SECTION 3 : A detailed look at
weight-loss m
ethods
Weight-loss centres(ex. : Centre de santé minceur, Centre de la diète, Infraslim centre minceur, etc.)
Manufacturers’ claims• Personalized• Quick, permanent and significant weight loss
Alleged means of action• Variety of technologies• Consultations• Diets based on reduced food intake, food combinations, products and meal replacements, etc.
Manufacturers’ warnings/contraindications• Generally none
Results of analysis• Despite promoters’ confusing claims regarding specialties and titles, supervision is not necessarily provided by health-care professionals.• Suggested weight loss is quick and significant.• The approach proposed by centres does not always include an eating or exercise program.• Few thorough studies support the effectiveness and safety of products or technologies recommended by centres.• Statistics on the effectiveness of the approaches proposed by centres are rarely known.• Affirmations of permanent weight loss, very common in centres, are not backed by scientific literature.• Centres often propose an approach based on health, but their practices tend to focus more on aesthetics (ex.: reshaping, body sculpting, etc.).• Treatment is usually offered on a one-time basis and is not necessarily part of a global approach.
Argument
Weight-loss centres suggest using technologies or products whose effectiveness has not necessarily been shown in thorough studies. They rely, rather, on sensa-tional testimonials from “satisfied clients” to support their claims.
The economic aspect must be considered. These centres are often company franchises looking to make a profit. If the first attempt to lose weight does not bear fruit, a “higher performing” product or technology will be offered to eliminate extra pounds.
Finally, despite the fact that the word “health” appears in many company names, supervision proposed in centres is not necessarily offered by a health-care professional.

28
Losing weight: for better, not worse
SECT
ION
3 : A
det
aile
d lo
ok a
t w
eigh
t-lo
ss m
etho
ds
Weight-loss programs(ex. : Weight Watchers, Minçavi, Herbalife etc.)
Developers’ claims• Guaranteed weight loss• Personalized approach• Balanced program
Operating procedures• Hypocaloric diets with or without exercise and/or products• Weekly group meetings
Developers’ warnings/contraindications• Generally none
Results of the analysis• On average, the suggested energy intake varies between 1000 - 1500 calories.• There is a contradiction between what is promoted officially, what is advertised and what is practised: for example, scientific recommendations suggest a weight-loss goal of 5%, but the method or approach suggests a higher weight loss; claims are made that the program follows Canada’s Food
Guide to Healthy Eating, but it does not respect a balance of macro-nutrients; claims are made that the program promotes a healthy and balanced eating program, but in fact it works with a calorie point system.• Supervision is not necessarily provided by health-care professionals and is not necessarily based on individuals’ needs.• The weight-loss approach is not necessarily based on an individual assessment, even if self-assessment is sometimes recommended at the start of the program.• The weight-loss approach sometimes requires food supplements and suggests consuming foods prepared and marketed by the programs.
Notes from the scientific literature• Few evaluation studies on weight-loss maintenance or program effectiveness are available63.• Even when weight loss is not necessary, people adopt a weight-loss approach64.

29
Losing weight: for better, not worse
SECTION 3 : A detailed look at
weight-loss m
ethods
Argument
Weight-loss programs often do not include an initial individual needs assessment, qualified supervision or training of professionals. Programs do not always take into account an individual’s environment, history or psychosocial condition.
What’s more, competition can arise among people in the program, despite the promotion of co-operation and mutual support, and the program’s success or failure depends essentially on the individual. Some people can deprive themselves of food before they are weighed, but eat right after, often impulsively. They there-fore eat based on an external locus of control rather than on their real physio- logical needs.
Lastly, it is not by counting calories or points that a person will learn anything of lasting value concerning food and healthy eating habits.

30
Losing weight: for better, not worse
SECT
ION
3 : A
det
aile
d lo
ok a
t w
eigh
t-lo
ss m
etho
ds
Meal replacements(ex. : Slim Fast, Nutribar, Scan Diet, etc.)
Manufacturers’ claims • Reduces weight by 1-2 lbs. per week• Allows for long-term weight-loss maintenance• Modifies eating habits in the short- and long-term• Reduces risk of illness• Contains all nutrients found in a balanced meal
Directions for use• Replace one or two meals a day with a suggested weekly menu for 8-12 weeks• To keep lost weight off, continue to substitute one meal a day• Replace all daily meals (based on one of the listed products)
Nutritional value
Ex: a bar- 230 to 260 calories- 56% carbohydrates- 23% fats- 21% proteins
Recommended diet of 1200 calories per day, as prescribed in the regulation
Manufacturers’ warnings/contraindications• No adverse side effects listed. • For those under 18, pregnant women or women who are nursing, and people with health problems, the manufacturer recommends consulting a doctor be-fore starting any diet for weight loss.
Results of the analysis• The approach is not personalized and does not lead to a behaviour modification approach, based on a previous assessment of an individual’s lifestyle and state of health.• By suggesting meal replacements, some manufacturers do not respect current regulations.65
• Using meal replacements does not promote a varied diet, as recommended in Canada’s Food Guide to Healthy Eating.• Meal substitutes are not particularly tasty or mouth-watering.66
• A meal replacement diet is monotonous.

31
Losing weight: for better, not worse
SECTION 3 : A detailed look at
weight-loss m
ethods
Notes from the scientific literature• By replacing all meals with a meal substitute, as recommended by the manufacturer, there is a risk of developing nutritional deficiencies.16
• Consuming meal substitutes does not encourage learning about or adopting long-term healthy eating habits.16
• A person who chooses not to consume meal substitutes and whose complementary meal is not nutritionally sound would tend to follow a diet with very few calories, which can be dangerous without medical supervision.16
• Research on the effectiveness of meal substitutes for weight loss or maintenance is financed in whole or in part by manufacturers of these products. This creates the potential for a research bias.
Argument
Meal substitutes are an unnatural way to eat and do not lead to learning the basics to ensure long-term weight-loss maintenance. Additionally, to keep weight off, it is suggested to continue integrating the product in daily meal planning. Is it possible to eat meal substitutes for life?
Using meal substitutes means consuming less food than is recommended by Canada’s Food Guide to Healthy Eating. Their consumption also develops a taste for sugar. Not only are these people depriving themselves of other flavours and tastes, but they are also avoiding sugary foods that taste better!
In general, people do not have all the necessary information to be able to compare a meal’s energy content with that of a meal substitute. For example, a sandwich (approximately 300 calories) nearly matches the energy content of a meal substi-tute, but it is a much better choice because it will often include a serving from each food group.
Lastly, the level of food restriction imposed by following a diet of just 1200 calories per day is certainly not suitable for everyone.

32
Losing weight: for better, not worse
SECT
ION
3 : A
det
aile
d lo
ok a
t w
eigh
t-lo
ss m
etho
ds
Diets• Hypocaloric (ex.: Scarsdale)
• High protein (ex.: Atkins)
• Based on the glycemic index (ex.: Montignac)
• Dissociation and prohibition of certain foods (ex.: Fit for Life, Montignac)
• Based on Ayurvedic type (ex.: Rainbow diet)
• Based on blood groups (ex.: D’Adamo), etc.
Some diets have a determined duration, while others require long-term lifestyle
changes.
Developers’ claims• Guaranteed permanent weight loss• Balanced• No deprivation• Prevent cardiovascular problems and obesity
Nutritional value• Exclusion of certain macro-nutrients (ex.: carbohydrates, fats)• An average of 800 to 1800 calories per day
Developers’ warnings/contraindications• Generally none.• Sometimes a time limit is suggested for very low energy diets.• Sometimes the diet is not recommended for pregnant women or children.
Results of the analysis• Several diets contain less than 1200 calories per day and suggest weight loss at a rate of one kilogram (approximately 2 lbs.) per week.• Not all of the diets suggest a global approach which should include physical activity.• No personalized supervision is offered.• Food variety is often limited.• Food supplements or products are frequently suggested.
Notes from the scientific literature• The diets adopt the same basic principle: weight loss varies according to the amount of food restricted. Hypocaloric diets result in short-term weight loss, but in 90 to 95% of cases weight is put back on within five years after the program or diet ends.67
• Various physical symptoms are associated with hypocaloric diets: fatigue, constipation, nausea, diarrhea.19 Depending on the degree to which calories are restricted, side effects can include arrhythmia, electrolyte imbalance21, reduction of bone mass23,26, and iron deficiencies.68
• Certain diets provoke nutritional deficiencies, especially in vitamins A and E, magnesium, zinc, fibre, potassium and calcium.69

33
Losing weight: for better, not worse
SECTION 3 : A detailed look at
weight-loss m
ethods
• Psychosocial effects, notably loss of self-esteem, self-confidence and satisfaction with one’s body, were noticed following frequent dieting.46
• There is a strong connection between frequent dieting and eating disorders.45
Argument
Popular diets are not effective or safe in the long run because they do not incorpo-rate a global and personalized approach. A popular diet is not for everyone: THE one-size-fits-all diet does not exist.
Some diets even recommend eliminating or reducing the consumption of foods that are recommended by Canada’s Food Guide to Healthy Eating. Doing this may result in significant nutritional deficiencies and physical or psychological symptoms.
Lastly, a diet might become so complicated and restrictive that a person simply does not eat. The resulting reduction in energy intake will induce weight loss.

34
Losing weight: for better, not worse
SECT
ION
3 : A
det
aile
d lo
ok a
t w
eigh
t-lo
ss m
etho
ds
Natural/over-the-counter/ homeopathic products(ex. : Chitosol, Crave free, Triolax, Xenadrine, etc.)
Manufacturers’ claims• Quick weight loss, effortless, localized, permanent, sometimes sensational• Used in conjunction with treatment for obesity• Reduced production of LDL cholesterol and triglycerides • Help troubles with metabolism due to obesity• Burn or absorb fats and sugars• Block absorption of carbohydrates and fats• Appetite suppressant or regulator• Raise basal metabolism• Help to stabilize weight
Manufacturers’ warnings/contraindications• Often none• Generally, the product claims to be safe, non-toxic and have no side effects.• Generally, the product is not recommended for pregnant or nursing women. A general warning from an organization like the FDA or Health Canada might be included. For example, there could be a warning that the product is in no way designed for diagnosing, treating, curing or preventing illness.
List of common ingredients (non-exhaustive list) • Algae• Caffeine• Cascara buckthorn
• Chitosane• Chromium
Results of the analysis• In most cases, the therapeutic product has no identifying number (DIN). In the future, natural products will have to bear a product number (NPN).• Ingredients often have different designations and their quantity is not always indicated.• In several cases, serious potential side effects are often ignored.• Truthful and complete product information, especially on real contents is not always accessible.• Few studies confirm the effectiveness and/or safety of products.• Several ingredients are laxatives and/or strong diuretics.• General information is given on eating habits and physical activity or it is absent from the product’s accompanying literature.• No supervision or follow-up is offered.• Some herbs are thought to be effective and/or risk free simply because of their country of origin or that they have been used for generations (ex.: the Orient).
• Fruit enzymes• Ephedra or Ma Huang• Garcinia cambodgia
• Guarana• Guar gum
• St. John’s Wort• Senna• Green tea• Cider vinegar• Yerba mate

35
Losing weight: for better, not worse
SECTION 3 : A detailed look at
weight-loss m
ethods
Notes from the scientific literature• Some natural products are likely to cause adverse side effects which can be attributed to ingredient substitution, too low or too high a dose, medicinal herbs or supplements of mediocre quality, poorly identified ingredients (wrong species), variability of component elements, heavy metal contamination, adulteration by prescribed medication, fortification and enrichment70, interactions with prescription medication71 and allergic reactions.72 Some products may also contain ingredients derived from herbs that are naturally toxic.73
• The use of some ingredients found in natural weight-loss products have already been questioned by Health Canada and the American FDA, including Ephedra74, birthwort75 and St. John’s Wort.76
• Studies have proven that other compounds like chromium77, chitosan78, bladderwrack57, psyllium as well as guar gum79 have proven ineffective in weight loss and were noted for their potential side effects.• Other ingredients regularly found in natural weight-loss products, such as cassia or senna and cascara buckthorn, have a laxative and/or diuretic effect. These products can result in serious electrolyte imbalances, damage to the kidneys, gastro-intestinal complications, and arrhythmia.80
• Natural health products are popular because more than 50% of Canadians use them.81
• In general, people seem to believe these products are safe because they come from natural plants.73
• In a prospective study82, half of patients who were asked about their use of diet supplements did not inform their doctors. Considering the possible interactions between medication and natural products, we should worry about the risk to consumers.
Argument
By simply listing so-called effective ingredients, natural products perpetuate the
idea that excess weight will miraculously disappear and melt away.
But more importantly, using these products to lose weight can be risky – some of them even result in serious health problems or death. Therefore, the principle of caution always has to be applied, and not use natural products whose safety and
effectiveness for weight loss have not been proven scientifically.

36
Losing weight: for better, not worse
SECT
ION
3 : A
det
aile
d lo
ok a
t w
eigh
t-lo
ss m
etho
ds
Transdermal products: creams, patches, wraps, sprays and gels(ex. : Patch Minceur, Cellimine Zones rebelles, Élancyl Chrono-actif, etc. )
Manufacturers’ claims• Weight loss• Cellulite treatment• Firms and tones body• Appetite control• Reduced fat and sugar absorption• Excess cutaneous fatty tissue disappears• Based on algotherapy
Main ingredients listed• Algae• Caffeine• Fruit enzymes• Garcinia cambogia• Green tea
Manufacturers’ warnings/contraindications• Generally none.• Sometimes the product is contraindicated for pregnant women and/or people with health problems.
Results of analysis• No eating or physical activity program is offered.• No thorough study supports claims for effective weight loss.• At an FTC meeting, a group of experts found allegations of substantial weight loss through transdermal products to be implausible, based on current scientific findings.60
Argument
Products are presented as being miraculous, but is it really possible to lose weight
or make “fat melt away” by wrapping yourself in plastic? Seriously, there is no
over-the-counter transdermal product available recognized for its effectiveness
in weight loss.

37
Losing weight: for better, not worse
SECTION 3 : A detailed look at
weight-loss m
ethods
Machines, devices and techniques(ex. : Press Point, Bracelet minceur, Gaine Lanaforme, Pantashort amincissant, etc.)
Manufacturers’ claims• Weight loss, weight-loss maintained• Stimulate and firm muscles effortlessly• Tone thighs, flatten stomach• Reduce excess subcutaneous fatty tissue• Curb appetite, reduce snacking
Alleged means• Acupressure• Electrical stimulation• Electrical acupuncture • Magnets/magnetic field
Manufacturers’ warnings/contraindications• Generally none.• No side effects.• Not recommended for pregnant women or people with pacemakers.
Results of analysis• Weight loss of more than 1-2 pounds per week is often suggested.• The role of food and exercise is often minimized.• The approach is neither personalized nor global.• Weight-loss affirmations are not backed by any conclusive research.• At an FTC meeting, a group of experts found allegations of substantial weight loss through products used on the exterior of the body to be implausible, based on current scientific findings.60
Argument
Promised results often seem marvellous, but is it really possible to control your ap-
petite with a (programmable!) bracelet or to fight unsightly cellulite just by wearing
a special pair of shorts? No machine, device or technique has been recognized on
its own as effective for weight loss. And if some machines result in weight loss that
is measurable, they would be affecting water weight loss, not fat.


ConclusionObesity and excess weight are on the rise. Consequently, health risks in the popu-lation are also increasing. Concurrently, having a thin and young body perseveres as the popular dream. As a result, trying to lose weight is as popular for individuals with excess weight that is harmful for their health as for individuals who have aes-thetic objectives.
A multitude of products, services and methods to lose weight (WLPSMs) is being offered in response to this demand. This market is constantly growing in an environ-ment that lacks proper regulation. To complicate matters further, myths and mis-taken ideas surround WLPSMs: that weight can be lost without making any effort or changing long-term habits, that a healthy weight must be achieved to reap health benefits and that strenuous exercise is required to be healthy. Finally, weight loss is often considered as an ultimate goal and answer to many problems, rather than an improvement to one’s overall health.
With so few resources, our health-care system responds poorly to those requiring healthy and safe weight controls. With such important needs, competent resources that are financially accessible are severely lacking.
With an increasing focus on obesity, health-care professionals will be more and more in demand to guide people through weight management, answer questions related to weight loss, and intervene when individuals try dangerous quick fixes.
This reference guide does not cover all possible weight-related issues, but is de-signed to give health-care professionals the major elements involved in providing effective care: the basic principles of healthy weight management, the key facts on WLPSMs, and their limitations and risks associated with their use.
Above all, this guide aims to destroy the myth of a one-size-fits-all solution for weight loss. As is often the case, the individual approach is the best one!
39
Losing weight: for better, not worse

40
Losing weight: for better, not worse
SECT
ION
4 : A
dditi
onal
info
rmat
ion
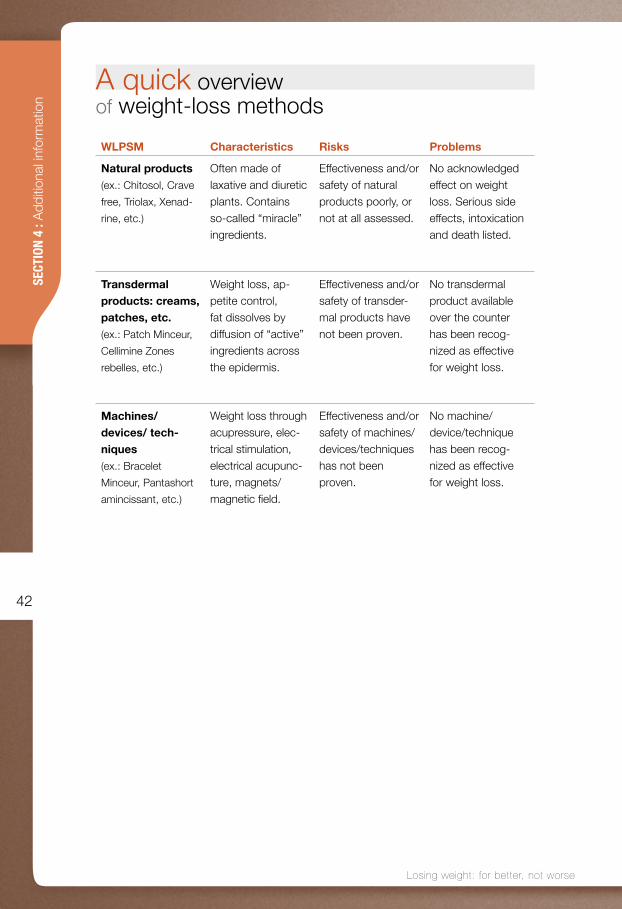
A quick overview of weight-loss methods
WLPSM Characteristics Risks Problems
Die
ts
Hypocaloric diets(ex. : Scarsdale)
Strict and mo-notonous menus.
Deficiency in calcium and some fatty acids. Fatigue, constipa-tion, nausea.
Very restricted diet and lost weight is regained quickly.
High protein(ex.: Atkins)
Consumption of starchy food, le-gumes, fruits and sugar is prohib-ited. No restriction of foods rich in fat and protein.
Deficiency of vitamins, fibers and mineral salts. Fatigue, con-stipation, high cholesterol.
Serious health consequences, especially cardio-vascular prob-lems.
Hypoglycemic(ex.:
Montignac)
Exclusion of foods with a high glyce-mic index (white flour, potatoes, cooked carrots, etc.). Don’t mix fat and carbohy-drates.
Nutritional defi-ciency due to an insufficient con-sumption of some food categories.
Deprivation of foods recommend-ed by CFGHE. 83
Diet is difficult to understand. The hypothesis that foods low on the glycemic index promote weight loss is not scien-tifically demon-strated.
Dissoci-ated food or single food(ex.: Fit for life,
Montignac)
Consumption of one food category at a time.
Deficiency in calci-um, vitamins and minerals, possibly in protein too.
Complex eating guidelines, depri-vation of foods recommended by CFGHE.
Based on blood types(ex.: D’Adamo)
Some foods are incompatible with our blood type.
Does not promote the consumption of a variety of foods as rec-ommended by CFGHE.
Diet leads to a de-privation of foods recommended by CFGHE. Basics of the diet are not sci-entifically validated.

41
Losing weight: for better, not worse
SECTION 4 : Additional inform
ation
A quick overview of weight-loss methods
WLPSM Characteristics Risks Problems
Commercial weight- loss pro-grams (ex.: Weight Watch-
ers, Minçavi, etc.)
Restricted diet.Generally group meetings for sup-port and motivation.
Weight frequently gained back when ending the program. Approach is not necessarily personalized.
Possibly no prior individual needs as-sessment, qualified supervision or pro-fessional training.
Weight-loss centres (ex.: Centre
de santé minceur,
Centre de la diète,
Infraslim centre min-
ceur, etc.)
Use of slimming techniques, natural products and inner cleansing treat-ments (purges). Food combining.
Nutritional deficien-cy. Proposed rate of weight loss is too high.
Inherent risks in taking numerous natural products.
Supervision not necessarily assured by health-care pro-fessionals. Claims of product and tech-nique effectiveness not supported by thorough studies.
Meal substitutes(ex.: Slim Fast, Nutri-
bar, Scan Diet, etc.)
Low-calorie diet. Replace one or two meals by substitutes.
Lack of dietary variety. Incorrect use may cause en-ergy and nutritional deficits. Might result in too rapid weight loss.
Denatured relation-ship with food. Consumption of fewer food choices recommended by CFGHE.
42
Losing weight: for better, not worse
SECT
ION
4 : A
dditi
onal
info
rmat
ion
WLPSM Characteristics Risks Problems
Natural products(ex.: Chitosol, Crave
free, Triolax, Xenad-
rine, etc.)
Often made of laxative and diuretic plants. Contains so-called “miracle” ingredients.
Effectiveness and/or safety of natural products poorly, or not at all assessed.
No acknowledged effect on weight loss. Serious side effects, intoxication and death listed.
Transdermal products: creams, patches, etc.(ex.: Patch Minceur,
Cellimine Zones
rebelles, etc.)
Weight loss, ap-petite control, fat dissolves by diffusion of “active” ingredients across the epidermis.
Effectiveness and/or safety of transder-mal products have not been proven.
No transdermal product available over the counter has been recog-nized as effective for weight loss.
Machines/devices/ tech-niques(ex.: Bracelet
Minceur, Pantashort
amincissant, etc.)
Weight loss through acupressure, elec-trical stimulation, electrical acupunc-ture, magnets/magnetic field.
Effectiveness and/or safety of machines/devices/techniques has not been proven.
No machine/ device/technique has been recog-nized as effective for weight loss.
A quick overview of weight-loss methods

43
Losing weight: for better, not worse
SECTION 4 : Additional inform
ation
Ingredients in weight-loss products(non-exhaustive list)
Ingredients Effectiveness for weight loss
Safety/adverse side effects
Possible inter-actions with medications and contraindications
Citric acid Fruit enzymesEx.: bromeline (from pineapples), papain
One of 111 ingredients found in weight loss products which the American FDA has banned for its unfounded claims of effectiveness.57
Not documented. Bromeline: interac-tions with anticoag-ulants and inhibitors of thrombocytic aggregation.84 Papain: interac-tions with Warfarin, a medication used to prevent blood clots.84
Usnic acid Commercial prod-uct (Lipokinetix) containing usnic acid, taken off the market by the FDA in 2001 due to side effects.
Severe liver toxicity, Hepatitis, acute liver failure requiring transplants.85
Not documented.
Marine algae Ascophyllum bladderwrack
Lack of proof of efficacy.57
Some types of algae are toxic and can store heavy metals and other toxic substances .62 The high level of iodine in blad-derwrack may increase the risk of hyperthyroidism. Its use is therefore not recommended.57
Prolonged ingestion of bladderwrack can reduce iron, sodium and potas-sium absorption. May interfere with thyroid treatment, to be avoided by those suffering from acne. Some people might easily overdose on iodine.62

44
Losing weight: for better, not worse
SECT
ION
4 : A
dditi
onal
info
rmat
ion
Ingredients Effectiveness for weight loss
Safety/adverse side effects
Possible inter-actions with medications and contraindications
Aristolochia Not documented for weight loss.
Substitution of S. tetandra (han fang ji) in a weight- loss product by Aristolochia west-landii (guan fang ji).
100 documented cases of nephropa-thy, 30 of which resulted in terminal kidney failure requir-ing transplants.75,86
Not documented.
Cascara buck-thornPowerful laxative
Weight loss due to the laxative effect.
May cause recur-rent diarrhea.62 The use of laxatives over long periods of time can create a depen-dence.87,88
Losing high amounts of liquid can result in low levels of potassium. This deficiency may possibly cause heart problems.84,87
ChitineSubstance extract-ed from the shell of crustaceansChitosaneGlucosamine poly-mere produced with chitine57
Effectiveness not proven: no effect on weight loss shown in humans.62
Scientific data contests effective-ness for weight loss in humans.89
Some fats could block the absorp-tion of fat-soluble vitamins; risk of short- and long-term deficiency.62
Gastro-intestinal symptoms.89
Dangerous for people with seafood allergies.62
Ingredients in weight-loss products(non-exhaustive list)

45
Losing weight: for better, not worse
SECTION 4 : Additional inform
ation
Ingredients in weight-loss products(non-exhaustive list)
Ingredients Effectiveness for weight loss
Safety/adverse side effects
Possible inter-actions with medications and contraindications
Chromium (Cr)Chromium Pico-linate
The FTC has con-cluded that there is insufficient scientific proof to support al-legations in ads for chromium-based products.57
Recent studies show that high doses can be dan-gerous.57
Reports of severe muscle injury (rhab-domiolisys) and kidney damage.90
Not documented.
EphedraEphedrineMa-HuangHerbal ecstasyMahuangMahuanggenMa huang root
Often combined with caffeine or guarana
Modest short-term weight loss.89
Palpitations, psy-chiatric symptoms, gastro-intestinal symptoms, shaking, insomnia, 16 000 reports of adverse side effects, includ-ing 17 deaths, 15 myocardial infarc-tions and 24 cardiac, cerebro-vascular and neurological ac-cidents, 11 strokes and 16 psychiatric symptoms.74,91
Persons suffer-ing from coronary thrombosis, diabe-tes, glaucoma, hy-pertension, thyroid, cardiac or prostate problems.74,88
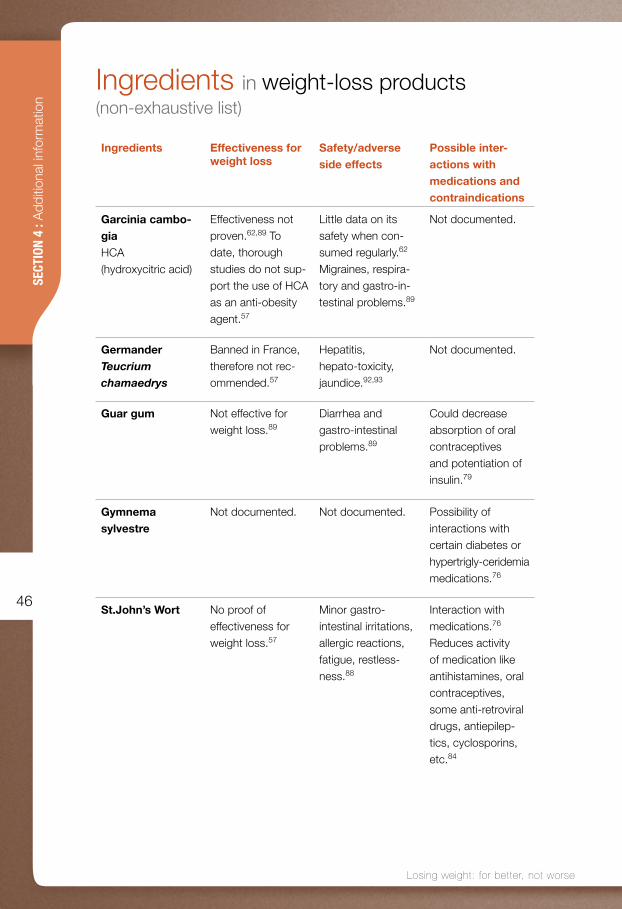
46
Losing weight: for better, not worse
SECT
ION
4 : A
dditi
onal
info
rmat
ion
Ingredients in weight-loss products(non-exhaustive list)
Ingredients Effectiveness for weight loss
Safety/adverse side effects
Possible inter-actions with medications and contraindications
Garcinia cambo-giaHCA (hydroxycitric acid)
Effectiveness not proven.62,89 To date, thorough studies do not sup-port the use of HCA as an anti-obesity agent.57
Little data on its safety when con-sumed regularly.62
Migraines, respira-tory and gastro-in-testinal problems.89
Not documented.
GermanderTeucrium chamaedrys
Banned in France, therefore not rec-ommended.57
Hepatitis, hepato-toxicity, jaundice.92,93
Not documented.
Guar gum Not effective for weight loss.89
Diarrhea and gastro-intestinal problems.89
Could decrease absorption of oral contraceptives and potentiation of insulin.79
Gymnema sylvestre
Not documented. Not documented. Possibility of interactions with certain diabetes or hypertrigly-ceridemia medications.76
St.John’s Wort No proof of effectiveness for weight loss.57
Minor gastro- intestinal irritations, allergic reactions, fatigue, restless-ness.88
Interaction with medications.76
Reduces activity of medication like antihistamines, oral contraceptives, some anti-retroviral drugs, antiepilep-tics, cyclosporins, etc.84

47
Losing weight: for better, not worse
SECTION 4 : Additional inform
ation
Ingredients in weight-loss products(non-exhaustive list)
Ingredients Effectiveness for weight loss
Safety/adverse side effects
Possible inter-actions with medications and contraindications
Common plantain or Psyllium (Plantago major)
May reduce short-term food intake, but the only ran-domized test did not reveal any effect on body weight.57,89
When taken in large quantities may cause gastro- intestinal problems.57,88
May potentially affect or slow absorption and the mechanism of certain medications taken at the same time, particularly derivatives of cou-marin and cardiac glycoside, vitamins and minerals (calcium, iron and zinc).57,84,88
Senna or cassia Depends on the quantity in the product; several products contain insufficient quanti-ties of laxative substances to bring about the desired effect.62
The use of laxatives over long periods of time can create dependence and cause recurrent diarrhea.88
Losing high amounts of liquid can result in low levels of potassium. This deficiency may possibly cause heart problems.62 The increased intestinal move-ment may reduce absorption of some orally administered medication.84,88

48
Losing weight: for better, not worse
SECT
ION
4 : A
dditi
onal
info
rmat
ion
Length/Type of WLPSM
Costs/General rates/Initial costs
3 months 6 months 1 year
Weight Watchers
Enrollment: $22 Weekly fees: $14 First visit: $36Following weeks: $14 5- or 12- week package: $69 or $154Semi-annual or annual membership: $299 or $529
$210 (including enrollment, first visit and 12-week package)
$360 (including enrollment, first visit and semi-annual member-ship)
$590 (including enrollment, first visit and annual member-ship)
Minçavi Enrollment: $30 Re-enrollment (with or without weigh-in journal): $16 or $23 New eating program: $5Adult weigh-in: $8 Students: $5 Every 2 weeks: $14 On-line consultation: $40 and +
$170(including enrollment, new eating program, 1 virtual consulta-tion and 1 weigh-in per week for 12 weeks)
$310 (including enrollment, new eating program, 2 virtual consulta-tions and 1 weigh-in per week for 24 weeks)
$610 (including enrollment, new eating program, 4 virtual consulta-tions and 1 weigh-in per week for 52 weeks)
Slim Fast Bar: $11 for 6Powder: $12 for 530 gSoup: $12 for 6 Packages: $2/package
$330 (60 products/ month for 3 months)
$500 (180 prod-ucts the first 3 months then 30 products/month the following 3 months)
$830 (60 products/month the first 3 months then 30 products/month the following 9 months)
Cost of weight-loss methods compared to consulting a health-care professional (2004)

49
Losing weight: for better, not worse
SECTION 4 : Additional inform
ation
Length/Type of WLPSM
Costs/General rates/Initial costs
3 months 6 months 1 year
Lypozic(Leblanc
Natural prod-
ucts)
$60 for 4 products (Slim Gel, Diu Slim, Taille Mince, Coupe Fringale)30 days
$180 (taking 4 products together as recom-mended)
$360 (taking 4 products together as recom-mended)
$720 (taking 4 products together as recom-mended)
Greens +(Natural
products)
Abs+$35 for 90 capsulesWeight loss: 6 capsules per dayWeight maintenance: 3 capsules per dayLean+$30 for 60 capsules$55 for 120 capsules2-4 capsules per dayShape+$33 for 120 capsules4 capsules per day
$475 (taking 3 products together as recom-mended in a publicity brochure)
$950 (taking 3 products together as recom-mended in a publicity brochure)
$1895 (taking 3 products together as recom-mended in a publicity brochure)
Kilo Cardio(Energy Car-
dio program)
8-week program, 3x/week $23/sessionOpening a file: $60
$610 (including opening a file and 24 sessions)
$1010 (annual subscrip-tion and program costs)
Cost of weight-loss methods compared to consulting a health-care professional (2004)

50
Losing weight: for better, not worse
SECT
ION
4 : A
dditi
onal
info
rmat
ion
Length/Type of WLPSM
Costs/General rates/Initial costs
3 months 6 months 1 year
Dietician Fee suggested by theOPDQ 94: $75/hourFee suggested by a group of dieticians in a private practice and according to number of visits: $29 to $43
From $215 to $375 (average cost for ap-proximately 5 visits)
From $495 to $855 (average cost for ap-proximately 15 visits)
From $870 to $1500 (average cost for ap-proximately 30 visits)
Kinesiologist Between $50 and $60/hour (fee variable depending on the professional/no fee suggested by the FKQ 95)Supervised and adapted program: from $20 to $35/hour
From $200 to $300 (average cost for ap-proximately 4 visits)
From $300 to $360 (average cost for ap-proximately 6 visits)
From $600 to $720 (average cost for ap-proximately 12 visits)
Cost of weight-loss methods compared to consulting a health-care professional (2004)
Note: None of the above-mentioned costs includes taxes.

51
Losing weight: for better, not worse
SECTION 4 : Additional inform
ation
Methodology The ASPQ education project (Éducation aux saines pratiques de contrôle du poids comme stratégie de promotion d’un mode de vie sain) for healthy weight-control practices was designed to promote healthy lifestyles and counter-act unhealthy weight-control practices to prevent obesity and diabetes and related health complications. This project was funded by Health Canada through its Cana-dian Diabetes Strategy – prevention and promotion contribution program.
The first part of this project was a critical analysis of weight-control practices of-fered by the private industry. Various products, services and weight-loss methods (WLPSM) available in Québec were identified and documented in order to examine the differences between these WLPSMs and the criteria of healthy weight-control practices found in scientific literature and approved by a committee of experts.
In the second part, two educational guides were produced — one for adolescents, “What’s up, Jennifer?” and another for adult women called “Lose weight…or be yourself?” These two guides were distributed in women’s magazines in February 2004. Then in May of the same year, the Ministère de la Santé and des Services sociaux came out with a second distribution of the guide for adolescents through the CLSC network and Directions de santé publique du Québec. Both guides can now be ordered from the ASPQ (www.aspq.org).
1. Identifying WLPSMs available in QuébecThe first step was to find different sources of information that would identify the greatest number of WLPSMs available in Québec. The sources that were found, which had to cover a large range of WLPSMs and be available in Québec, are listed in the following table.
Information sources to identify WLPSMs
Daily newspapers and regional weeklies
Magazines and journals
Television
Pharmacies
Natural food stores
Advertising (leaflets, flyers, etc.)
Books
Internet
% of WLPSMs present (not mutually exclusive)
16 %
19 %
7 %
29 %
42 %
40 %
7 %
82 %

52
Losing weight: for better, not worse
SECT
ION
4 : A
dditi
onal
info
rmat
ion
The original plan was to make an exhaustive inventory of WLPSMs available in Québec. However, their number and quantity is always changing, so it was de-cided to select some WLPSMs in a given window of time, from November 2002 to January 2003 inclusive. Personal weight-control practices (monitoring fat or sugar consumption, exercising, etc.) were not included in the study. Products sold by prescription, medical treatments, medical weight-loss clinics and dietician clinics were also excluded, most notably because they fall under a field of practice regu-lated by a professional order.
In the end, more than 350 WLPSMs were selected from the various sourc-es consulted. Because of their wide variety and to make the analysis easier, WLPSMs were classified into eight categories. Some of the WLPSMs listed were not described or analyzed because:
• There was not enough information on the given WLPSM to be able to perform an adequate analysis;
• Some products were very similar, as with slimming creams, which were numerous and more often designed to treat cellulite than weight loss;
• Sometimes one product was marketed under different names, for example in the United States and in Canada;
• The WLPSM was not easily or not at all available in Québec (ex.: Jenny Craig).
Subsequently, 215 WLPSMs were described based on information available in ads from different sources: the media, Internet sites, pamphlets, sales outlets, etc. These were the WLPSMs chosen for analysis. The following table shows the breakdown of the selected WLPSMs, as well as those document-ed and analyzed, according to category. The WLPSMs chosen for analysis were described on health and safety data sheets. Observations were compiled in a database for statistical purposes.

53
Losing weight: for better, not worse
SECTION 4 : Additional inform
ation
WLPSM CATEGORY WLPSM chosen
WLPSM analyzed
n % n %
Non-prescription medication and
natural products (ex.: appetite suppres-
sants, fat burners, laxatives, diuretics)
203 57.8 152 70.7
Meal substitutes
and food products23 6.6 13 6.0
Weight-loss programs 11 3.1 8 3.7
Weight-loss centres 20 5.7 9 4.2
Diets 35 10.0 18 8.4
Patches, creams, sprays, wraps 31 8.8 7 3.3
Machines and devices (ex.: electrical
stimulation, acupressure, pressure
therapy, etc.)
21 6.0 7 3.3
Alternative methods (ex.: hypnosis,
aromatherapy, acupuncture, fasting)7 2.0 1 0.5
Total 351 100 215 100
54
Losing weight: for better, not worse
SECT
ION
4 : A
dditi
onal
info
rmat
ion
2. Establishing analysis criteria for weight-control practices To properly conduct the critical analysis of the various WLPSMs listed, the analysis criteria of weight-control practices had to be defined. These criteria, taken from scientific literature and recommendations from organizations interested in weight issues were approved by a committee of experts. The eight members of the committee had different expertise on the subjet of weight (nutrition, obesity, public health, kinesiology, pharmacology and toxicology, health sociology and consumer rights):
Martin Brochu, assistant professor in the kinesiology administrative unit at the Université de Montréal;
Dr. Véronique Déry, specialist in public health and scientific director at the Agence d’évaluation des technologies et des modes d’intervention en santé;
Lise Dubois, nutritionist, health sociologist and professor in the department of social and preventative medicine at the Université Laval;
Dr. Dominique Garrel, endocrinologist and director of the nutrition department at the Université de Montréal;
Simone Lemieux, nutritionist, professor in the department of food sciences and nutrition at the Université Laval and part of the Obesity Research Chair team;
Lyne Mongeau, nutritionist, scientific advisor to the Institut national de santé pub-lique du Québec, the Direction Développement des individus and des communau-tés, Lifestyles unit, and member of the Association pour la santé publique du Québec’s Council of Governors;
Gilles Morissette, senior officer in competition law, in the Canadian Competition Bureau;
Dr. Albert Nantel, specialist in pharmacology and toxicology and scientific advisor to the Institut national de santé publique du Québec, and the Biological, Environ-mental and Occupational Risks Branch, Health and Environment Unit.

55
Losing weight: for better, not worse
SECTION 4 : Additional inform
ation
Summary of the main guidelines that exist for healthy weight-control practices
• Health Canada• Canadian non-government organizations• National Heart, Lung, and Blood Institute (National Institutes of Health)• Partnership for Healthy Weight Management• Michigan Task Force to Establish Weight Loss Guidelines• American Heart Association• NHS - National Health Services• World Health Organization
In light of comments and suggestions from committee members, the criteria have been revised and measurement indicators or elements have been identified. This was a necessary distinction. In fact, owing to the diversity of WLPSMs and the limits of current regulation, it was difficult to establish criteria directly applicable to WLPSM analysis.
WLPSM effectiveness and safety criteria are a good example. Although current regulation does not require most WLPSMs to prove claims of effectiveness or safety, consumers still need this type of information to make an informed decision about weight loss.
A new set of criteria was proposed to the committee members. Comments from the committee were then integrated into a series of final proposals approved by all committee members. The criteria refer to a weight-loss approach in the widest sense and are divided into eight categories:
CRITERIA CATEGORIES
The rate of weight lossApproach required for a program or method (including supervision)Dietary intervention Physical activityEffectiveness of the approachSafety of the approach Promotion and advertising surrounding the approachCost of the approach

56
Losing weight: for better, not worse
SECT
ION
4 : A
dditi
onal
info
rmat
ion
Books
• Apfeldorfer G (1997). Maigrir, c’est dans la tête, Paris, Éditions Odile Jacob, 348 p.• Apfeldorfer G (2000). Maigrir, c’est fou!, Paris, Éditions Odile Jacob, 304 p.• Berg FM (2001). Children and Teens Afraid to Eat. Helping Youth in Today’s Weight-Obsessed World, Hettinger, Healthy Weight Network, 339 p.• Berg FM (2000). Women Afraid to Eat. Breaking Free in Today’s Weight-Obsessed World, Hettinger, Healthy Weight Network, 384 p.• Cash TF (1997). The Body Image Workbook: An 8-step program for learning to like your looks, Oakland, New Harbinger Publications, 221 p.• Fairburn CG, Brownell KD (2002). Eating Disorders and Obesity. A Comprehensive Handbook, 2nd ed., New York, The Guilford Press, 633 p.• Fischler C (2001). L’Homnivore, Paris, Édi-tions Odile Jacob, 440 p.• Foster GD, Nonas CA (2004). Managing Obesity: A Clinical Guide, Chicago, American Dietetic Association, 247 p.• Kirby J (for The American Dietetic Associa-tion) (1999). Maigrir pour les nuls, Alameda, Sybex, 374 p. • Kratina K, King NL, Hayes D (1996). Moving Away from Diets, Lake Dallas, Helm Seminars Pub, 174 p.• OPDQ (2000). Manuel de nutrition clinique, Montreal, Ordre professionnel des diététistes du Québec.• Wadden TA, Stunkard AJ (2002). Handbook of Obesity Treatment, New York, The Guilford Press, 624 p.• Waterhouse D (1994). Mince alors… Finis les régimes!, Montreal, Éditions de l’Homme, 258 p.• Wilson TG (1996). Acceptance and Change in the Treatment of Eating Disorders and Obe-sity. Behavior Therapy, 27:417-439.• Zermati JP (2002). Maigrir sans régime, Paris, Éditions Odile Jacob, 416 p.
Web sites
• Québec-Ossg. Bariatric surgery support group, [On line], May 9, 2004. http://ossg.ca (May 21, 2004).• FTC (Federal Trade Commission). “Weight Loss Advertising: An Analysis of Current Trends.” A Federal Trade Commission Staff Report, [On line], September 2002. [http://www3.ftc.gov/bcp/reports/weightloss.pdf] (August 1, 2003).• NHLBI (National Heart, Lung, and Blood Institute). “Clinical Guidelines on the Identifica-tion, Evaluation, and Treatment of Overweight and Obesity in Adults,” [Summary], [On line], 1998. [http://www.nhlbi.nih.gov/nhlbi/] (Sep-tember 18, 2000).• Health Canada. “The VITALITY Approach – a Guide for Leaders,” Ottawa, Department of Public Works and Governement Services. Health Canada publications service, cat. no H39-525/2000F, [On line], 2000. [http://www.hc-sc.gc.ca/hpfb-dgpsa/onpp-bppn/vitality_approach_f.pdf] (September 7, 2003).
Training
Le Collectif action alternative en obésité (CAAO). Small-group training seminars. Telephone: (514) 270-3779, e-mail address: [email protected] Web site: www.caao.qc.ca
ResourcesHealth-care professionals who wish to have more information on the topics discussed in this reference guide may consult this list of related resources.

57
Losing weight: for better, not worse
SECTION 4 : Additional inform
ation
Reference1 Health Canada 2003). Canadian Guidelines for Body Weight Classification in Adults, Ot-tawa, Office of Nutrition Policy and Promotion. Health Canada publications service, Cat no. H49-179/2003F, p. 9.2 Consult the previous reference for full infor-mation on levels of risk.3 Foster GD, Wadden TA, Vogt RA, Brewer G (1997). What is a reasonable weight loss? Pa-tient’s expectations and evaluations of obesity treatment outcomes. Journal of Consulting and Clinical Psychology. 65:79-85.4 Jeffery RW, Wing RR, Mayer RR (1998). “Are smaller weight losses or more achievable weight-loss goals better in the long-term for obese?” Journal of Consulting and Clinical Psychology. 66:641-645.5 NHLBI (National Heart, Lung, and Blood Institute) (1998). “Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults,” [Summa-ry], [On line], [http://www.nhlbi.nih.gov/nhlbi/] (18 septembre 2000).6 Cooper Z, Fairburn CG (2001). “A new co-gnitive behavioural approach to the treatment of obesity.” Behaviour Research and Therapy. 39:499-511.7 Lee CD, Blair SN, Jackson AS (1999). “Car-dio respiratory fitness, body composition, and all-cause and cardiovascular disease mortality in men.” American Journal of Clinical Nutrition. 69:373-380.8 Farrell SW, Braun L, Barlow CE, Cheng YJ, Blair SN (2002). “The relation of body mass index, cardio respiratory fitness, and all-cause mortality in women.” Obesity Research. 10:417-423.9 Blair SN, Brodney S (1999). “Effects of physical inactivity and obesity on morbidity and mortality: current evidence and research issues.” Medicine and Science in Sports Exer-cise. 31:S646-S662.10 Ravussin E (2002). “Energy expenditure and body weight.” Eating Disorders and Obe-sity. A Comprehensive Handbook. Fairburn CG, Brownell KD, 2nd ed., New York, The Guilford Press, Chap. 10, pp. 55-61.11 Pavlou KN, Steffee WP, Lerman RH, Bur-rows V (1985). “Effects of dieting and exer-cise on lean body mass, oxygen uptake, and strength.” Medicine and Science in Sports and Exercise. 17:466-471.12 Cunningham JJ (1982). “Body composition and resting metabolic rate; the myth of femi-nine metabolism.” American Journal of Clinical Nutrition. 36:721.13 Astrup A, Gøtzsche PC, Van de Werken K, Ranneries C, Toubro S, Raben A, Buemann B (1999). “Meta-analysis of resting metabolic rate in formerly obese subjects.” American Journal of Clinical Nutrition. 69:1117-22.14 Leibel RL, Rosenbaum M, Hirsch J (1995). “Changes in energy expenditure resulting from
altered body weight.” New England Journal of Medicine. 332(10):621-628.15 Wadden TA, Berkowitz RI (2002). “Very-Low-Calorie Diets.” Eating Disorders and Obesity. A Comprehensive Handbook. Fair-burn CG, Brownell KD (ed.), 2nd ed., New York, The Guilford Press, Chap. 96, pp. 534-538.16 Melanson K, Dwyer J (2002). “Popular diets for treatment of overweight and obesity.” Handbook of Obesity Treatment. Wadden TA, Stunkard AJ (ed.), New York, The Guilford Press, Chap. 12, pp. 249-282.17 Calloway W (1988). “Biologic adaptations to starvation and semi-starvation.” Obesity and Weight Control. Frankle RT and Yang MI, New York, Aspen Publication, pp.97-108.18 Gregg EW, Williamson DF (2002). “The relationship of intentional weight loss to di-sease incidence and mortality.” Handbook of Obesity Treatment. Wadden TA, Stunkard AJ (ed.), New York, The Guilford Press, Chap. 7, pp. 125-143. 19 Valdez R, Gregg EW, Williamson DF (2002). “Effects of weight loss on morbidity and mortality.” Eating Disorders and Obesity. A Comprehensive Handbook. Brownell KD, CG Fairburn (ed.), New York, The Guilford Press, Chap. 88, pp. 490-494.20 Berg FM (1999). “Health risks associa-ted with weight loss and obesity treatment programs.” Journal of Social Issues. 55(2): 277-297.21 Rasio E (1970). “Répercussions métaboli-ques du jeûne.” Revue Médicale de Bruxelles. 26(10):569-579.22 Petersmark and Smith (1989). Toward safe weight-loss recommendations for adult weight-loss programs in Michigan. Michigan Health Council, Lansing MI, Michigan Depart-ment of Public Health.23 Apfeldorfer G, Zermati J-P (2001). “La restriction cognitive face à l’obésité, histoire des idées, description clinique.” La Presse médicale. 30 (32): 1575-1580.24 Van Loan MD, Keim NL (2000). “Influence of cognitive eating restraint on total-body measurements of bone mineral density and bone mineral content in pre menopausal wo-men aged 18-45 y: a cross-sectional study.” American Journal of Clinical Nutrition. 72(3):837-43.25 Langlois JA, Mussolino ME, Visser M, Loo-ker AC, Harris T, Madans J (2001). “Weight loss from maximum body weight among mid-dle-aged and older white women and the risk of hip fracture: the NHANES I epidemiologic follow-up study.” Osteoporosis International. 12(9):763-8.26 Felson DT, Zhang Y, Hannan MT, Anderson JJ (1993). “Effects of weight and body mass index on bone mineral density in men and wo-men: the Framingham study.” Journal of Bone and Mineral Research. 8(5):567-73.27 Schweiger U, Tuschl RJ, Platte P, Broocks A, Laessle RG, Pirke KM (1992). “Everyday
58
Losing weight: for better, not worse
SECT
ION
4 : A
dditi
onal
info
rmat
ion
eating behavior and menstrual function in young women.” Fertility and Sterility. 57(4):771-5.28 Barr SI, Prior JC, Vigna YM (1994). “Res-trained eating and ovulatory disturbances: possible implications for bone health.” Ameri-can Journal of Clinical Nutrition. 59(1):92-7.29 Selzer R, Caust J, Hibbert M, Bowes G, Patton G (1996). “The association between secondary amenorrhoea and common eating disordered weight control practices in an ado-lescent population.” Journal of Adolescent Health. 19(1): 56-61.30 King TK, Matacin M, Marcus BH, Bock BC, Tripolone J (2000). “Body image evaluations in women smokers.” Addictive Behaviors. 25(4):613-8.31 Hart EA, Leary MR, Rejeski WJ (1989). “The measurement of social anxiety.” Jour-nal of Sports and Exercise Psychology. 11:94-104.32 Ransdell LB, Wells CL, Manore MM, Swan PD, Corbin CB (1998). “Social physique an-xiety in post menopausal women.” Journal of Women Aging. 10:19-39.33 Frederick CM, Morrison CS (1996). “Social physique anxiety: personality constructs, mo-tivations, exercise attitudes, and behaviors.” Perceptual and Motor Skills. 82(3, 1st part):963-72.34 McAuley E, Bane SM, Rudolph DL, Lox CL (1995). “Physique anxiety and exercise in middle-aged adults.” Journal of Gerontology Series B: Psychological Sciences and Social Sciences. 50(5): P229-35.35 Lowry R, Galuska DA, Fulton JE, Wechsler H, Kann L, Collins JL (2000). “Physical activity, food choice, and weight management goals and practices among US college students.” American Journal of Preventive Medicine. 18(1):18-27.36 Wardle J, Griffith J, Johnson F, Rapoport L (2000). “Intentional weight control and food choice habits in a national representative sam-ple of adults in the UK.” International Journal of Obesity. 24: 534-540.37 Schwartz, M.B., & Brownell, K.D. (2004). “Obesity and Body Image.” Body Image. 1, 43-56.38 Keys A, Brozek J, Henschel A, Mickelsen F, Taylor HF (1950). The Biology of Human Star-vation, Minneapolis, University of Minnesota Press, 1385 p.39 McFarlane T, Polivy J, McCabe RE (1999). “Help, not harm: psychological foundation for a non-dieting approach toward health.” Jour-nal of Social Issues. 55:261-276.40 Parham H (1996). “Is there a new weight paradigm? “ Nutrition Today. 31(4):155-161.41 Garner DM, Wooley SC (1991). “Con-fronting the failure of behavioural and dietary treatments for obesity.” Clinical Psychology Review. 11:729-780.42 Apfeldorfer G, Zermati J-P (2001). “La restriction cognitive face à l’obésité, histoire
des idées, description clinique.” La Presse Médicale. 30(32):1575-1580.43 Robison JI (1997). “Weight Management: shifting the paradigm.” Journal of Health Edu-cation. 28(1):28-34.44 Hawks SR, Richins P (1994). “Toward a new paradigm for the management of obesity. Journal of Health Education.” 25:147-53.45 Polivy J, Herman CP (1985). “Dieting and Binging: a causal analysis.” American Psycho-logy. 40:193-201.46 Wadden TA, Womble LG, Stunkard AJ, An-derson DA (2002). “Psychosocial consequen-ces of obesity and weight loss.” Handbook of Obesity Treatment. Wadden TA, Stunkard AJ (réd.), New York, The Guilford Press, Chap. 8, pp. 144-172.47 WHO (2000). “Obesity, Preventing and Managing the Global Epidemic.” Report of a WHO Consultation, Technical Report Series No 894, Geneva, World Health Organisation , 252 p.48 Polivy J, Herman CP (1999). “Distress and eating: why do dieters overeat?” International Journal of Eating Disorders. 26(2):153-154.49 Foreyt JP, Goodrick GK (1993). “Evidence for success of behaviour modification in wei-ght loss and control.” Annual International Medicine. 119:698-701.50 Total is more than 100% because the women could choose more than one resonse. Ledoux M, Rivard M (2000). “Poids corporel. “ Enquête sociale et de santé 1998. Institut de la statistique du Québec, Gouvernement du Québec, Chap. 8, pp. 185-199.51 Health and Welfare Canada (1992). Using the Food Guide, Minister of Supply and Servi-ces Canada.52 Health and Welfare Canada (1990). Nutri-tion Recommendations for Canadians. Report from the scientific review committee. Ottawa, Minister of Supply and Services Canada.53 Pronk NP, Wing RR (1994). “Physical activity and long-term maintenance of weight loss.” Obesity Research. 2:587-599; Klem ML, Wing RR, McGuire MT, Seagle HM, Hill JO (1997). “A descriptive study of individuals successful at long-term maintenance of substantial weight loss.” American Journal of Clinical Nutrition. 6:239-246.54 Health Canada, August revision (2001). How Drugs are Reviewed in Canada, Ottawa, Therapeutic Products Directorate.55 Health Canada (2003). Natural Health Products Regulations. Canada Gazette, Part II, volume 137 No 13, Article 8. SOR/DORS 2003-196.56 Health Canada (2002). The Food and Drugs Act, Ottawa, Health Products and Food Branch, Article B.24.200.57 Allison DB, Fontaine KR, Heshka S, Men-tore JL, Heymsfield SB (2001). “Alternative treatments for weight loss: a critical review.” Critical Reviews in Food Science and Nutri-tion. 41(1):1-28.

59
Losing weight: for better, not worse
SECTION 4 : Additional inform
ation
58 “PDR for Herbal Medicines (1998). 1st ed.”, Medical Economics, 1244 p.59 Federal Trade Commission (2002). “Wei-ght-loss advertising: an analysis of current trends.” Federal Trade Commission Staff Report.60 Federal Trade Commission (2003). “De-ception in weight-loss advertising workshop: seizing opportunities and building par-tnerships to stop weight-loss fraud.” Federal Trade Commission Staff Report.61 Health Canada (2003). The Food and Drugs Act, Ottawa, Health Products and Food Branch, Schedule A, Article 3, guidance document.62 Dionne I (1999). “Grosses Promesses, pe-tits résultats…” Protégez-vous. May: 3-9.63 Van Gaal LF (1998). “Dietary treatment of obesity.” Handbook of Obesity. Bray GA, Bou-chard C, James WPT (ed.), New York, Marcel Dekker Inc, Chap. 43, pp. 875-890.64 Canada Task Force. (1991). Report of the task force on the treatment of obesity. Ottawa: Health Services and Promotion Branch, Health and Welfare Canada.65 Health Canada (2002). Food and Drugs Act, Ottawa, Health Products and Food Branch, Article B.24.200.66 Apfeldorfer G (1994). Traité de l’alimenta-tion du corps, Paris, Flammarion, p. 695.67 Wooley SC, Garner DM (1994). “Dietary treatments for obesity are ineffective.” British Medical Journal. 309:655-656.68 Pinhas-Hamiel O, Newfield RS, Koren I, Agmon A, Lilos P, Philip M (2003). “Greater prevalence of iron deficiency in overweight and obese children and adolescents.” Inter-national Journal of Obesity. 27:417-418.69 Freedman MR, King J, Kennedy E (2001). “Popular diets: a scientific review.” Obesity Research, Vol. 9 Suppl. 1, pp. 1S-40S.70 McCutcheon AR (2002). Exploration des questions d’actualités liées à la qualité des plantes et des produits botaniques: document de travail. Perspectives on Natural Health Pro-ducts, Ottawa, Health Canada, pp. 55-95.71 Boon H, Jurgens T, (2001). Drug Inte-ractions with Natural Health Products: work document. Perspectives on Natural Health Products, Ottawa, Health Canada, pp. 1-27.72 Bielory L (2002). “Adverse reactions to complementary and alternatives medicine: radweed’s cousin, the coneflower (Echinacea), is a problem more than a sneeze.” Annual of Allergy, Asthma and Immunology. 88:7-9.73 Barnes J, Anderson LA, Philipson JD (2002). Herbal Medicines, 2nd ed., London, Pharmaceutical Press, 530 p.74 Food and Drug Administration (FDA) (2004). “FDA issues regulation prohibiting sale of dietary supplements containing ephedrine alkaloids and reiterates its advice that consu-mers stop using these products.” FDA News PO4-17. U.S. Food and Drug Administration; FDA (2003). “FDA announces plans to prohibit
sales of dietary supplements containing Ephe-dra.” U.S. Department of Health and Human Services; Health Canada (2001). Advisory not to use products containing Ephedra or ephe-drine. No 2001-67; Health Canada (2003). Health Canada reminds Canadians of the dangers of Ephedra or ephedrine. 75 FDA (2001). “FDA warns consumers to dis-continue use of botanical products that con-tains aristolochic acid.” Consumers Advisory, Centre for Food Safety and Applied Nutritions. U.S. Food and Drug Administration; Health Canada (2001) Health Canada advising not to use products labelled to contain Aristolochia. No 2001-91.76 Health Canada (2000). Potentially harmful drug interaction with St. John’s Wort and prescription drugs. No 2000-36.77 Pittler MH, Stevinson C, Ernst E (2003). “Chromium picolinate for reducing body weight: meta-analysis of randomized trials.” International Journal of Obesity. 27:522-529.78 Pittler MH, Abbot NC, Harkness EF, Ernst E (1999). “Randomized, double-blind trial of chi-tosan for body weight reduction.” European Journal of Clinical Nutrition. 53:379-381.79 Pittler MH, Ernst E (2001). “Guar gum for body weight reduction: meta-analysis of randomized trials.” American Journal of Medi-cine. 110(9):724-730.80 Berg FM (1999). “Health risks associa-ted with weight loss and obesity treatment programs.” Journal of Social Issues. 55(2):277-297.81 Health Canada (2002). Canadian Adverse Reaction Newsletter.82 Hensrud DD, Engle DD, Scheitel SM (1999). “Underreporting the use of dietary supplements and non prescription medica-tions among patients undergoing a periodic health examination.” Mayo Clinic Proceedings 74(5):443-447 [see comments pp. 531-532].83 Health Canada (2002). Canada’s Food Guide to Healthy Eating.84 Blumenthal M (2000). “Interactions between herbs and conventional drugs: Introductory considerations.” Herbal Gram. 49:52-63.85 Favreau JT, Ryu LR, Braunstein G, Or-chansky G, Park SS, Coody GL, Love LA, Fong TL (2002). “Severe hepatotoxicity associated with the dietary supplement Lipo-Kinetix.” Annals of Internal Medicine. 136(8): 590-595.86 Chen J (2000). “Nephrotoxicity associated with the use of Aristolochic.” Herbal Gram. 48: 48-49.87 Mayo Foundation for Medical Education and Research (2002), Herbal diet pills, Web-site: www.mayoclinic.com 88 WHO (1999). WHO monographs on selec-ted medicinal plants. World Health Organiza-tion. Volume 1.89 Pittler MH, Ernst E (2004). “Dietary supple-ments for body-weight reduction: a systema-

60
Losing weight: for better, not worse
SECT
ION
4 : A
dditi
onal
info
rmat
ion
tic review.” American Journal of Clinical Nursing. 79: 529-536.90 Pittler MH, Stevinson C, Ernst E (2003). “Chromium picolinate for reducing body weight: meta-analysis of randomized trials.” International Journal of Obesity. 27: 522-529.91 Shekelle PG, Hardy ML, Morton SC, Maglione M, Mojica WA, Suttorp MJ, Rhodes SL, Jungvig L, Gagné J (2003). “Efficacy and safety of Ephedra and Ephedrine for weight loss and athletic performance.” Journal of American Medical Association. 289(12):1537-1545.92 De Berardinis V, Moulis C, Maurice M, Beaune P, Pessatre D, Pompon D, Loeper J (2000). “Human Microsomal Epoxide Hydrolase is the target of germander-induced auto antibodies on the surface of human hepatocytes.” Molecular Pharmacology. 58: 542-551.93 Laliberté L, Villeneuve J-P (1996). “Hepatitis after the use of Germander, a herbal remedy.” Canadian Medical Association Journal. 154:1689-1692.94 Ordre professionnel des diététistes du Québec95 Fédération des kinésiologues du Québec

