the association between cognitive function and subsequent
TRANSCRIPT

The association between cognitive function andsubsequent depression a systematic review andmeta-analysis
M A Scult1 A R Paulli1 E S Mazure2 T E Moffitt1 A R Hariri1dagger and T J Strauman1dagger
1Department of Psychology amp Neuroscience Duke University Durham NC USA2Duke University Medical Center Library amp Archives Duke University Medical Center Durham NC USA
Despite a growing interest in understanding the cognitive deficits associated with major depressive disorder (MDD) it islargely unknown whether such deficits exist before disorder onset or how they might influence the severity of subse-quent illness The purpose of the present study was to conduct a systematic review and meta-analysis of longitudinaldatasets to determine whether cognitive function acts as a predictor of later MDD diagnosis or change in depressionsymptoms Eligible studies included longitudinal designs with baseline measures of cognitive functioning and later uni-polar MDD diagnosis or symptom assessment The systematic review identified 29 publications representing 34 uniquesamples and 121 749 participants that met the inclusionexclusion criteria Quantitative meta-analysis demonstrated thathigher cognitive function was associated with decreased levels of subsequent depression (r =minus0088 95 confidenceinterval minus0121 to minus0054 p lt 0001) However sensitivity analyses revealed that this association is likely driven by con-current depression symptoms at the time of cognitive assessment Our review and meta-analysis indicate that the asso-ciation between lower cognitive function and later depression is confounded by the presence of contemporaneousdepression symptoms at the time of cognitive assessment Thus cognitive deficits predicting MDD likely represent dele-terious effects of subclinical depression symptoms on performance rather than premorbid risk factors for disorder
Received 9 May 2016 Revised 21 July 2016 Accepted 26 July 2016
Key words Cognitive function depression intelligence longitudinal premorbid risk
Introduction
A growing literature has found that depression is asso-ciated with impaired cognitive functioning (Snyder2013) For example broad deficits in neuropsychologic-al functioning have been demonstrated in a number ofreviews and meta-analyses on depression (Christensenet al 1997 Rogers et al 2004 Snyder 2013 Rock et al2014) and cognitive deficits have been found to correl-ate with symptom severity (McDermott amp Ebmeier2009) Theoretical models have been proposed suggest-ing that cognitive dysfunction could either be a riskfactor for later depression or that cognitive functionmay be impaired as a result of depression (Stern2003 Barnett et al 2006) In support of the latter hy-pothesis two recent meta-analyses concluded that thedeficits in cognitive function persist after remissionfrom depression (Bora et al 2013 Rock et al 2014)However evidence showing that deficits in cognitive
function persist after remission from depressionwhich are primarily derived from cross-sectional stud-ies does not rule out the possibility that poor cognitivefunction preceded the onset of depression The presentreview and meta-analysis sought to comprehensivelysummarize the state of the research on cognitive func-tion and its association with future depressive symp-toms using data from longitudinal studies
While the clinical diagnosis of depression is relative-ly codified according to DSM and ICD criteria and de-pression symptoms are readily measured with anumber of validated instruments (Lewinsohn et al2000 Cuijpers et al 2004) a similar canonical approachto measuring cognitive function is not present Thus itis important to specify a working definition of cogni-tive function before examining its possible associationwith depression Empirical work has reinforced theconcept of a single construct of cognitive functionthrough high correlations in performance among dis-parate cognitive tasks (Spearman 1904) This has ledto the derivation of a single factor representing generalcognitive function or ability known as lsquogrsquo (Johnson et al2004) The lsquogrsquo factor is commonly determined byadministering a wide range of tasks and using factoranalysis to determine the shared variance across
Address for correspondence Dr M A Scult Department ofPsychology amp Neuroscience Duke University Durham NC 27708USA
(Email matthewscultdukeedu)dagger Co-equal authorship
Psychological Medicine Page 1 of 17 copy Cambridge University Press 2016doi101017S0033291716002075
REVIEW ARTICLE
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
these tasks (Ree amp Earles 1991) Even in cases when lsquogrsquois not calculated as such there are other customaryways of capturing this general factor by combingacross cognitive tasks eg by creating an index of ex-ecutive functions (Miyake et al 2000) or measuringthe intelligence quotient (Gottfredson 1997)
Although executive functions and intelligence areoften considered independently evidence has sug-gested that they may best be characterized by an inte-grated framework based on a common neural network(Barbey et al 2012) supporting the idea that theyreflect a shared general factor of cognitive ability Inlight of these findings and the observation that indivi-duals with depression commonly exhibit deficits acrossa range of cognitive tasks our review used the broad-est measure of cognitive function that was available ina given study When a higher-order construct was notavailable results from individual measures were usedWe restricted analyses to prospective cohort studieswith depression assessment before age 65 in order tominimize potential influences of age-related cognitivedecline
We follow our literature review with a quantitativemeta-analysis to (1) determine whether cognitive func-tion predicts later depression (2) evaluate whether dif-ferences in the measurement of depression (categoricalv continuous) influence observed associations and (3)examine whether sex or age of participants may mod-erate effects and (4) whether effects are confounded bydepression symptoms at baseline
Methods
We followed the Meta-Analyses of ObservationalStudies in Epidemiology (MOOSE) guidelines (Stroupet al 2000) (Supplementary Table S1) and the literaturesearch strategies suggested by Atkinson et al (2014)
Search process
Systematic searches were conducted in February 2015and updated in December 2015 in three electronic data-bases PubMed EMBASE and PsycINFO Searcheswere conducted by a research librarian EM and over-seen by MS The search syntax was adapted for eachdatabase and designed to capture the participants pre-dictors comparisons and outcomes described belowaccording to the PICOS framework (Moher amp Liberati2009) The Boolean operator lsquoORrsquo was used within cat-egories and the operator lsquoANDrsquo was used betweencategories The complete search strategy is describedin the Search Strategy in the Supplementary MaterialHand searches were conducted of the reference listsof included articles
Eligibility criteria
The review included English language studies of em-pirical studies investigating the longitudinal associ-ation of cognitive function (IQ neuropsychologicaltests executive functions) with unipolar depressiondiagnosis or symptoms Detailed inclusionexclusioncriteria were as follows
Participant characteristics
Eligible studies included children adolescents andadults under the age of 65 This age range was spe-cified because of the possible impact of cognitive de-cline in older populations Articles examining ahighly specific population (eg with a particular med-ical diagnosis) were excluded so as to not limit the gen-eralizability of results Studies that required MDDdiagnosis hospitalization or admission to a treatmentcenter as part of the inclusion criteria at baselinewere also excluded from the review so as to permitconclusions about depression onset This was to ensurethat a majority of study participants did not have de-pression at baseline However cohort studies wereincluded even if they did not measure depression atbaseline assuming that these samples would have de-pression prevalence rates that were comparable topopulation norms Subgroup analyses were subse-quently performed on the studies that specificallyexcluded for any history of depression If there wereseveral papers about one cohort the paper with largersample size or better study quality was included
Predictor type
Eligible studies included a measure of cognitive execu-tive or neuropsychological function The studyincluded a range of cognitive predictors given thatprevious studies have found broad deficits in cognitivefunction in depression (Christensen et al 1997 Rogerset al 2004 Snyder 2013 Rock et al 2014) Whenmore than one cognitive predictor was reported as anoutcome in a study the broadest measure of cognitivefunctioning was used If no measure captured broadcognitive functioning the measure that was mostclosely aligned with constructs on a standard IQ test(working memory processing speed verbal compre-hension or perceptual reasoning) was used in themeta-analysis
Studies were excluded if cognitive function wasassessed via educational achievement given thatthese measures can be more easily influenced by learn-ing disabilities than by general cognitive functioning(Siegel 1999) Self-report descriptive measures of cog-nitive functioning were also excluded in favor ofmore objective measures Last since this study sought
2 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Table 1 Characteristics of included studies
StudyName ofcohort Type of cohort
Samplesize Comorbidity
Howdepressionassessed
Mean IQatbaseline
Name ofcognitivemeasure
Type of cognitivemeasure
Name ofdepressionoutcome
Type ofdepressionoutcome
Covariatesincluded inmeta-analysisa
Percentfemale Raceethnicity Continent
Meanage atbaseline
Timebetweenassessments(years)
Year ofinitialassessment
Baer et al(2013)
ConcordiaLongitudinalRetirementProject
Retirees 333 NR Studyassessment
NR MontrealCognitiveAssessment
VerbalComprehensionPerceptualReasoning WorkingMemory
Center forEpidemiologicalStudiesDepression Scale(CES-D)
Continuous Depressionsymptoms atTime 1
NR (bothmaleandfemale)
NR NorthAmerica
5906 4 sim2005
Beaujeanet al (2013)
NationalLongitudinalStudy ofAdolescentHealth (AddHealth)
Communitysample
14 322 NR Studyassessment
10061 Add HealthPictureVocabularyTest (AHPVT)ndash an abridgedversion of thePPVT-R
VerbalComprehension
Created for thisstudy
Continuous Depressionsymptoms atTime 1
50 7631 White1674Black 422Asian 25AmericanIndian1183Hispanic005 MixedRace
NorthAmerica
1598 7 1994
Belsky et al(2012)
EnvironmentalRiskLongitudinalTwin Study(E-Risk)
Birth cohort 2123 Conductdisorderanxietypsychosisborderlinepersonalitydisorder
Studyassessment
100 WechslerPreschool andPrimary Scaleof Intelligence(WPPSI)
General IntelligenceVerbalComprehensionPerceptualReasoning
ChildrenrsquosDepressionInventory (CDI)
Continuous None 51 sim90 White Europe 5 7 1999
Betts et al(2016)
MaterUniversityStudy ofPregnancy(MUSP)
Pre-birthcohort
1934 PsychosisMania
Studyassessment
NR PeabodyPictureVocabularyTest-Revised(PPVT-R)
VerbalComprehension
CompositeInternationalDiagnosticInterview(CIDI-Auto)
Continuous(latentfactor)
None NR NR Australia 5 16 1989
Canals et al(2002)(females)
NR Communitysample
99 NR Studyassessment
NR Academicaptitude test(AAT)
General IntelligenceVerbalComprehensionPerceptualReasoning
Schedules forClinicalAssessment inNeuropsychiatry
Categorical None 100 NR Europe sim11 6 NR
Canals et al(2002)(males)
NR Communitysample
100 NR Studyassessment
NR Academicaptitude test(AAT)
General IntelligenceVerbalComprehensionPerceptualReasoning
Schedules forClinicalAssessment inNeuropsychiatry
Categorical None 0 NR Europe sim12 6 NR
Connollyet al (2014)
TempleUniversityAdolescentCognitionand Emotion(ACE) Project
Communitysample
200 NR Studyassessment
NR Digit Span fromWechslerIntelligenceScale forChildren(WISC)
Working Memory ChildrenrsquosDepressionInventory (CDI)
Continuous Depressionsymptoms atTime 1
565 452 White513 Black
NorthAmerica
1241 1 NR
Association
between
cognitivefunction
andsubsequent
depression3
httpdxdoiorg101017S0033291716002075D
ownloaded from
httpww
wcam
bridgeorgcore Duke U
niversity Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core term
s of use available at httpww
wcam
bridgeorgcoreterms
Table 1 (cont)
StudyName ofcohort Type of cohort
Samplesize Comorbidity
Howdepressionassessed
Mean IQatbaseline
Name ofcognitivemeasure
Type of cognitivemeasure
Name ofdepressionoutcome
Type ofdepressionoutcome
Covariatesincluded inmeta-analysisa
Percentfemale Raceethnicity Continent
Meanage atbaseline
Timebetweenassessments(years)
Year ofinitialassessment
Der et al(2009)
US NationalLongitudinalSurvey ofYouth 1979
Communitysample
7458 Noted a rangeof healthconditions
Studyassessment
NR Armed ServicesVocationalAptitudeBattery(ASVAB)Armed ForcesQualificationTest (AFQT)
General IntelligenceVerbalComprehension
Center forEpidemiologicalStudiesDepression Scale(CES-D)
Continuous Depressionsymptoms atTime 1
52 31 Black19Hispanic
NorthAmerica
179 sim22 1979
Dubow et al(2008)(females)
ColumbiaCountyLongitudinalStudy(CCLS)
SchoolChildrenGrade 3
215 NR Studyassessment
sim104 CaliforniaShort-FormTest of MentalMaturity
General Intellignce MinnesotaMultiphasicPersonalityInventory(MMPI) Scale 2
Continuous None 100 90 White3 Blacklt1Asianlt1Hispanic
NorthAmerica
8 11 1960
Dubow et al(2008)(males)
ColumbiaCountyLongitudinalStudy(CCLS)
SchoolChildrenGrade 3
211 NR Studyassessment
sim104 CaliforniaShort-FormTest of MentalMaturity
General Intelligence MinnesotaMultiphasicPersonalityInventory(MMPI) Scale 2
Continuous None 0 90 White3 Blacklt1Asianlt1Hispanic
NorthAmerica
8 11 1960
Evans et al(2015)
NR SchoolChildrenGrades 5ndash9
192 Some withADHD
Studyassessment
111 WechslerAbbreviatedScale ofIntelligence(WASI)
General IntelligenceVerbalComprehensionPerceptualReasoning WorkingMemorySet-Shifting
ChildrenrsquosDepressionInventory (CDI)
Continuous Depressionsymptoms atTime 1
521 714 White182 Black26 Asian36Hispanic42 MixedRace
NorthAmerica
1236 03 sim2000s
Franz et al(2011)
Vietnam EraTwin Studyof Aging
Military cohort 1231 NR Studyassessment
NR Armed ForcesQualificationTest (AFQTForm 7A)
General IntelligencePerceptualReasoning WorkingMemory ProcessingSpeed Set-ShiftingInhibition
Center forEpidemiologicalStudiesDepression Scale(CES-D)
Continuous None 0 86 White NorthAmerica
20 35 sim1970
Gale et al(2008)
VietnamExperienceStudy (VES)
Military cohort 3258 Mix Studyassessment
100 Generaltechnicalsection of theArmyClassificationBattery
General IntelligenceVerbalComprehensionArithmeticreasoning
DiagnosticInterviewSchedule (DIS)
Categorical SocioeconomicStatusEthnicity Placeof service
0 808 White127 Black
NorthAmerica
204 sim17 sim1964
Gale et al(2009)(1958Cohort)
1958 NationalChildDevelopmentSurvey
Birth cohort 6369 NR Studyassessment
1028 General abilitytest devisedby theNationalFoundationforEducationalResearch inEngland andWales
General Intelligence Rutterrsquos MalaiseInventory
Continuous None NR (bothmaleandfemale)
NR Europe 11 22 1969
4MA
Scultet
al
httpdxdoiorg101017S0033291716002075D
ownloaded from
httpww
wcam
bridgeorgcore Duke U
niversity Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core term
s of use available at httpww
wcam
bridgeorgcoreterms
Gale et al(2009)(1970Cohort)
1970 BritishCohort Study
Birth cohort 6074 NR Studyassessment
1018 British abilityScale
General Intelligence Rutterrsquos MalaiseInventory
Continuous None NR (bothmaleandfemale)
NR Europe 10 20 1980
Gjerde(1995)(females)
NR Recruited froma nurseryschool
51 NR Studyassessment
1187 Wechsler AdultIntelligenceScale (WAIS)
General Intelligence General BehaviorInventory (GBI)Depression scale
Continuous None 100 sim66 Whitesim25Blacksim005Asian
NorthAmerica
18 5 1983
Gjerde et al(1995)(males)
NR Recruited froma nurseryschool
45 NR Studyassessment
11112 Wechsler AdultIntelligenceScale (WAIS)
General Intelligence General BehaviorInventory (GBI)Depression scale
Continuous None 0 sim66 Whitesim25 Blacksim005Asian
NorthAmerica
18 5 1983
Hatch et al(2007)
1946 BritishCohort Study
Birth cohort 957 NR Studyassessment
NR NationalFoundationforEducationalResearch Test
General IntelligenceVerbalComprehensionPerceptualReasoning
General HealthQuestionnaire(GHQ-28)-severedepressionsubscale
Continuous None 51 NR Europe 8 45 1954
Hipwellet al (2011)
PittsburghGirls Study(PGS)
Communitysample
195 NR Studyassessment
9954 WechslerIntelligenceScale forChildren(WISC) III-R
VerbalComprehension
Schedule forAffectiveDisorders forSchool-AgeChildren-Present andLifetime Version(K-SADS-PL)
Continuous Depressionsymptoms atTime 1
100 70 Black ormultiracial
NorthAmerica
1154 1 1998
Horowitz ampGarber(2003)
NR Elementaryschool cohort
196 NR Studyassessment
10461 WechslerIntelligenceScale forChildren(WISC) -R
General IntelligenceVerbalComprehensionPerceptualReasoning
Schedule forAffectiveDisorders forSchool-AgeChildren-EpidemiologicalVersion(K-SADS-E)
Categorical Depressionsymptoms atTime 1
542 89 White147 Black33 Other
NorthAmerica
1186 6 sim1980
Koenenet al (2009)
DunedinCohort
Birth cohort 730 None Studyassessment
NR WechslerIntelligenceScale forChildren(WISC)
General IntelligenceVerbalComprehensionPerceptualReasoning WorkingMemory ProcessingSpeed
DiagnosticInterviewAssessment (forDSM-IV)
Categorical SexSocioeconomicStatusPhysicalHealthchildhoodmaltreatment
48 lsquoPrimarilyWhitersquo
NewZealand
9 23 1981
McCord ampEnsminger(1997)(females)
WoodlawnCohort
Elementaryschool cohort
346 Some withalcoholism
Studyassessment
NR (13 Unspecified IQof sample had scoresover 110)
General Intelligence CompositeInternationalInterviewSchedule(according toDSM-III-R)
Categorical None 100 100 Black NorthAmerica
sim6 27 1966
McCord ampEnsminger(1997)(males)
WoodlawnCohort
Elementaryschool cohort
313 Some withalcoholism
Studyassessment
NR (11 Unspecified IQof sample had scoresover 110)
General Intelligence CompositeInternationalInterviewSchedule(according toDSM-III-R)
Categorical None 0 100 Black NorthAmerica
sim6 27 1966
Meyer et al(2004)
NR Risk sample 86 NR Studyassessment
sim118 WISC General IntelligenceVerbalComprehensionPerceptualReasoning
SCID Categorical None 63 90 White9 Black 1Hispanic
NorthAmerica
11 13 1989
Association
between
cognitivefunction
andsubsequent
depression5
httpdxdoiorg101017S0033291716002075D
ownloaded from
httpww
wcam
bridgeorgcore Duke U
niversity Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core term
s of use available at httpww
wcam
bridgeorgcoreterms
Table 1 (cont)
StudyName ofcohort Type of cohort
Samplesize Comorbidity
Howdepressionassessed
Mean IQatbaseline
Name ofcognitivemeasure
Type of cognitivemeasure
Name ofdepressionoutcome
Type ofdepressionoutcome
Covariatesincluded inmeta-analysisa
Percentfemale Raceethnicity Continent
Meanage atbaseline
Timebetweenassessments(years)
Year ofinitialassessment
Papmeyeret al (2015)
ScottishBipolarFamily Study
Risk sample 111 NR Studyassessment
Controls108Patients107
National AdultReading Test(NART)
VerbalComprehension
Structured ClinicalInterview forDSM Disorders(SCID)symptoms
Categorical None 52 NR Europe 21 2 NR
Pine et al(1997)
NR Communitysample
644 NR Studyassessment
1007 UnspecifiedlsquoIQrsquo
General Intelligence Based onDiagnosticInterviewSchedule forChildren
Continuous Depressionsymptoms atTime 1
52 91 White NorthAmerica
138 9 1983
Quinn ampJoormann(2015)
NR Undergraduatestudents
43 NR Studyassessment
NR n-back Working Memory Beck DepressionInventory II(BDI-II)
Continuous Depressionsymptoms atTime 1
63 58 White30Hispanic orLatino 19Asian 2AfricanAmerican2AmericanIndian 2NativeHawaiian2 Indian
NorthAmerica
19 014 NR
Rawal ampRice (2012)
EarlyPrediction ofAdolescentDepressionstudy
Risk sample 230 None Studyassessment
9746 WechslerIntelligenceScale forChildren(WISC)
General IntelligenceVerbalComprehensionPerceptualReasoning WorkingMemory ProcessingSpeed
Child andAdolescentPsychiatricAssessment(CAPA)
Both Depressionsymptoms atTime 1 AgeOvergeneralityto negativecues
596 NR Europe 1371 1 NR
Sharp et al(2008)
The ChildBehaviourStudy
Communitysample
439 NR Studyassessment
105 WechslerIntelligenceScale forChildren(WISC)
General IntelligenceVerbalComprehensionPerceptualReasoning
The Mood andFeelingsQuestionnaire
Continuous Depressionsymptoms atTime 1
52 97 White05 Black25 Asian
Europe 94 1 NR
Simons et al(2009)
East FlandersProspectiveTwin Survey
Twin registry 444 NR Studyassessment
NR Principalcomponentfrom StroopConceptShifting Testand LetterDigitSubstitutionTest
Processing SpeedSet-ShiftingInhibition
Structured ClinicalInterview forDSM Disorders(SCID)symptoms
Continuous Depressionsymptoms atTime 1
100 NR Europe 28 2 NR
6MA
Scultet
al
httpdxdoiorg101017S0033291716002075D
ownloaded from
httpww
wcam
bridgeorgcore Duke U
niversity Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core term
s of use available at httpww
wcam
bridgeorgcoreterms
Slykermanet al (2015)
AucklandBirthweightCollaborativeStudy
Birth cohortrisk sample
609 NR Studyassessment
NR Stanford-BinetIntelligenceScale 4th Ed
General IntelligenceFluid ReasoningKnowledgeQunatitativeReasoningVisual-SpatialProcessingWorking Memory
Center forEpidemiologicalStudiesDepression Scale(CES-D)
Categorical(cut-point)
None 49 NR NewZealand
35 75 sim2000
Soslashrensenet al (2012)
DanishDraft-BoardStudy
Military cohort 21 914 NR Psychiatricregistry
Controls100Patients96ndash98
Boslashrge PriensProslashve (BPP)
General IntelligenceVerbalComprehensionPerceptualReasoning
DanishInternationalClassification ofdiseases (ICD) 8amp 10
Categorical None 0 NR Europe 195 sim36 1968ndash1989
Vinberget al (2013)
NR High-risktwins
224 Bipolardisorderanxietysubstanceabuse other
Studyassessmentpsychiatricregistry
NR CambridgeCognitiveAssessment(CAMCOG)
GeneralNeuropsychologicalFunctionOrientationLanugage MemoryAttention AbstractThinking VisualPerception
Beck DepressionInventory (BDI)
Continuous Depressionsymptoms atTime 1
65 NR Europe 439 7 2003
Zammitet al (2004)
SwedishConscripts(1969ndash1970)
Military cohort 50 053 None Hospitallinkage
NR UnspecifiedlsquoIQrsquo
General IntelligenceVerbalComprehensionPerceptualReasoning GeneralKnowledgeMechanicalKnowledge
InternationalClassification ofdiseases (ICD)hospitalpsychiatricadmissions
Categorical Diagnosis atbaselinedisturbedbehavior druguse raised in acity
0 NR Europe sim19 27 1969
Sample size is the number of subjects included in reported analyses of interest NR not reportedsim indicates only a range was reporteda This column notes covariates included in the meta-analysis We focused on controlling for depressive symptoms at T1 but some studies reported effect sizes that also included controlling
for other variables ndash when the zero-order correlations were unavailable these estimates were used
Association
between
cognitivefunction
andsubsequent
depression7
httpdxdoiorg101017S0033291716002075D
ownloaded from
httpww
wcam
bridgeorgcore Duke U
niversity Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core term
s of use available at httpww
wcam
bridgeorgcoreterms
to investigate general information processing abilitiesrather than cognitive attributional style studies withcognitive attribution measures as the sole cognitivemeasure were excluded
Comparisons
Search terms used to indicate the possible associationbetween cognitive function and depression includedrisk premorbid prodromal onset predict and association(for a full list see search terms in the SupplementaryMaterial) When data were reported from multipletime-points the analysis accounting for the longesttime between assessments was used
Outcomes
Eligible studies reported depression diagnosis orsymptoms determined by investigator or self-reportPresence of comorbidity was permitted given that de-pression has been found to be highly comorbid withother disorders (Melartin et al 2002 Kessler et al2003) Articles not adequately specifying how depres-sion was assessed or articles that did not uniquelymeasure depression [ie only had an index of lsquomentaldisordersrsquo or the category of lsquomood disordersrsquo lumpedtogether (Gale et al 2010)] were excluded if no uniquemeasure of depression could be obtained from studyauthors This is because although comorbidity waspermitted these could have represented instances ofpure anxiety disorders with few or no depressivesymptoms or instances of bipolar disorder
Study design
Eligible study search terms included cohort studies lon-gitudinal epidemiological prospective retrospective follow-up or case-control studies Studies not following a longi-tudinal design were excluded during full-text reviewAdditionally studies where cognitive function wasassessed only concurrently with or after depressionwere excluded given that the purpose of the reviewwas to investigate whether cognitive function pre-dicted later depression
Studies were included regardless of whether theywere reported in peer-review journals in order to ac-count for potentially biased reporting of resultsReview articles were included in the search terms tofind additional relevant references but were notincluded in the meta-analysis Baseline and protocolstudies without follow-up data were excluded
Study selection
A flow diagram of the process of study selection showsthe overall procedures (Fig 1) Records identified fromthe search processes were combined in EndNote
software version X7 and duplicates were removedTitles and abstracts were reviewed independently bytwo reviewers (MS and AP) according to the eligibil-ity criteria described above and marked as either po-tentially eligible or not eligible If either authormarked an article as potentially eligible it wasincluded in the full-text review for closer examinationby MS and AP who used an electronic form to indi-cate if an article should be included or excluded in thefinal selection When an article was excluded the rea-son for exclusion was selected from a hierarchical listof exclusion criteria presented in Fig 1 Both MSand AP were initially blinded to the otherrsquos decisionsAfter both MS and AP completed their reviews dis-crepancies about whether a study should be includedor excluded were resolved via discussion and consen-sus amongst MS AP TM AH and TS
Data extraction
Study information was extracted independently byMS and AP using an electronic form created forthis study Information was collected and codedbased on report characteristics participant characteris-tics study setting predictors outcome measures andquality assessment (Cooper 2010) Any discrepancies(approximately 3 of data points) were resolved viaconsensus
For studies with categorical depression diagnoses ef-fect sizes were generally presented as odds ratios Forthese studies the odds ratio plus the upper and lowerbound of the confidence interval were recorded Twoof the studies (Zammit et al 2004 Gale et al 2008)reported odds ratios greater than one to indicate thatlower IQ was associated with greater risk of depressionThe other studies reported odds ratios in the reverseleading to odds ratios less than one for the same direc-tion of the effect Therefore the odds ratios from the firsttwo studies were recalculated by dividing (1oddsratio) Another study (McCord amp Ensminger 1997)reported results from chi-squared tests Additional stud-ies reported mean premorbid IQ scores rather than oddsratios in which case the means sample sizes andor pvalues and number of tails of the t test were utilizedto calculate the effect size
For studies in which depression was measured as acontinuous variable effect sizes were presented as cor-relation coefficients The direction of the effect (posi-tive or negative) and the sample size were alsoextracted to be used in the meta-analysis Two studiesreported only beta weights (Simons et al 2009 Rawalamp Rice 2012) and we were not able to obtain zero-order correlations from the authors Given that previ-ous reports have suggested that beta weights can beused as an estimate of correlation coefficients in
8 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
meta-analysis (Peterson amp Brown 2005) the betaweights were used instead and analyses were runboth including and excluding these data points
When insufficient information was presented in thearticle authors were contacted requesting further de-tail An additional six studies were included at thispoint One study (Hatch et al 2007) included effectsizes for the female half of the cohort and did not pro-vide statistics for the males but did indicate a null ef-fect Only women from this study were included in themeta-analyses but imputing a score of 0 for the malesyielded similar overall results
Follow-up analyses directly compared studies thatreported zero-order correlations between IQ at time
1 depression at time 1 and depression at time 2(additional details described in the SupplementaryMethods)
Statistical methods
Data were analyzed using Comprehensive Meta-Analysis software version 30 (Biostat Inc USA) Arandom-effects model was used for expected hetero-geneity across studies A random-effects model alsoallows for broader generalization of results to thepopulation at large Heterogeneity of effects was calcu-lated using the Q statistic where a significant p valueindicates that true effect varies across studies The I2
Fig 1 Flow diagram of the search process
Association between cognitive function and subsequent depression 9
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
statistic was used to calculate the ratio of the true het-erogeneity to total variation acting as an index of sig-nal-to-noise ratio When I2 is large it is has beenrecommended to consider subgroup analysis or meta-regression to account for the variance (Borensteinet al 2011)
Subgroup analyses were conducted using a mixed-effects analysis in which a random effects model wasused to combine studies within each subgroup and afixed effect model was used to combine subgroupsand yield the overall effect (the study-to-study vari-ance is not assumed to be the same for all subgroups)Subgroup analyses were conducted comparing type ofoutcome (continuous v categorical) broad v specificcognitive measures and outcomes that were adjustedv unadjusted for baseline depression symptoms
Meta-regression was performed using the followingvariables on unadjusted analyses age at baseline ageat follow-up time between assessments IQ percentwhite year of cognitive assessment year of follow-upassessment percent female and study quality score
Study quality and publication bias
Study quality was evaluated independently by MSand AP using a checklist adapted from Luppino ampWit (Luppino et al 2010) The checklist contained 12items and studies were rated with a lsquo+rsquo if it met criteriafor that item a lsquominusrsquo if it did not meet criteria for an itemand a rsquorsquo if unclear lsquo+rsquo were coded as a score of 1 andminus were coded as a score of 0 Total scores and percen-tages were calculated Articles with total scores of 0ndash3were considered to be of low quality scores of 4ndash7were considered a medium quality and scores of 8ndash12 were considered to be of high quality Any discrep-ancies (approximately 3 of data points) wereresolved via consensus
Publication bias was assessed using a funnel plotwhich presents study size on the vertical axis (as stand-ard error in this case) as a function of effect size on thex-axis When no publication bias exists the studiesshould be distributed symmetrically about the com-bined effect size (Borenstein et al 2011) If evidenceof publication bias was observed Duval amp Tweediersquostrim-and-fill method was used (Duval amp Tweedie2000) which recalculates effects based on imputingdata from studies that are likely to be missing Lastthe Fail-safe N was calculated (Cooper 1979) whichindicates the number of missing studies that wouldneed to exist to nullify the observed effect
Results
A flow diagram of the search process is shown inFig 1 The search identified 2773 records through
PubMed 2158 through EMBASE and 1345 throughPsycINFO for a total of 6276 records Duplicaterecords (1709) were removed in EndNote resulting in4567 unique records After title and abstracts werereviewed 329 records were identified as potentially eli-gible for the meta-analysis These 329 records werereviewed in full and 300 articles were excluded hier-archically if they were a review baseline or protocolpaper (n = 6) if the sample had a mean age over 65at the depression assessment (n = 41) if the samplehad a specific medical illness (n = 23) if the studywas not a longitudinal design (n = 19) if MDD diagno-sis hospitalization or admission to treatment centerwas part of the inclusion criteria of the study (n = 18)if cognitive function was assessed only concurrentlywith or after depression (n = 36) if cognitive functionwas assessed by educational achievement or self-report(n = 26) if cognitive function was assessed by attribu-tion style rather than neuropsychological measure (n= 7) if there was no measure of cognitive function (n= 18) or no uniquely measured depression outcome(n = 24) Furthermore if articles reported on the samesample as another article with higher quality or moreinformation the duplicate articles were excluded (n =8) Last a number of studies appeared to measureboth cognitive function and depression but did not re-port enough information to be included in the meta-analysis and did not respond to requests for additionalinformation (n = 74 approximately 59 unique samples)In total 29 publication were included in the meta-ana-lysis comprising 34 samples (one study included twoseparate birth cohorts and another four reported dataseparately for men and women)
Study characteristics
The characteristics of included samples are detailed inTable 1 Sample sizes ranged from 43 to 50 053 with amedian of 3395 The most common types of sampleswere school samples (934) community samples (834) and birth cohorts (734) The samples were major-ity white with two samples having exclusively blackparticipants Additionally eight samples were menonly six samples were women only and the restreported combined effect sizes Mean age of partici-pants at baseline ranged from 35 to 59 years with amedian of 12 years Most samples did not reportwhether comorbid diagnoses were present (2334)
Of the 74 papers excluded for having insufficient in-formation (representing 60 unique samples) the me-dian number of subjects was not statistically differentbetween those studies and the studies included in themeta-analysis (n = 288 and n = 3395 respectively p =019) nor did the average age of study participants atbaseline statistically differ (median across studies = 11
10 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
v 12 respectively p = 057) The types of cognitivemeasures used were also similar across the excludedand included studies with the most common measurebeing IQ (2860 and 2029) followed by VerbalComprehension (860 and 529)
Meta-analysis
The overall analysis yielded a significant associationbetween cognitive function and subsequent depressionoutcomes [r =minus0088 95 confidence interval (CI)minus0121 to minus0054 p lt 0001 Fig 2] Results were similarwhen excluding the two studies that used beta-weights(r =minus0071 95 CI minus0100 to minus0042 p lt 0001) orwhen using episodic memory in place of processingspeed in a study reporting both outcomes (r =minus008595 CI minus0118 to minus0051 p lt 0001) Follow-up ana-lyses were conducted in the sample of studies report-ing educational attainment and self-report outcomes(Supplementary Table S2) Heterogeneity across sam-ples was significant (Q = 80154 p lt 0001) suggestingsubstantial variation across the individual samplesThe ratio of the true heterogeneity to total variationwas large (I2 = 9588) I2 is on a relative scale andvalues close to 100 indicate that most of the observedvariance is real rather than spurious and suggeststhat subgroup analyses or meta-regression may helpto explain this variability (Borenstein et al 2011)
Subgroup analyses and meta-regression
A significant difference was found between categoricaland continuous effect sizes (p lt 0001) The studiesassessing continuous outcomes were found to have alarger effect (r =minus0121 95 CI minus0168 to minus0073 p lt0001 n = 22) than studies assessing categorical out-comes (r =minus0035 95 CI minus0054 to minus0017 p lt 0001n = 12) No differences were observed between studiesutilizing broad v specific cognitive measures (p = 057)
Outcomes were also compared adjusting for baselinedepression symptoms at the time of cognitive assess-ment Nine studies provided enough detail to calculatethe partial correlation coefficients adjusting for base-line depression symptoms Using the partial correl-ation coefficients led to a null result (r =minus0032 95CI minus0078 to 0014 p = 0169 n = 9 Fig 3) The nullresult does not seem to be due to a lack of power be-cause using the unadjusted correlation coefficients forthe same nine studies still led to a significant result(r =minus0120 95 CI minus0169 to minus0070 p lt 0001 n = 9Fig 3) As a follow-up the difference in effect sizes be-tween the adjusted and unadjusted values for these 9studies were tested (r = 0082 95 CI 0069ndash0095 p lt0001 n = 9) suggesting that the effects are significantlydifferent when directly comparing the values that doand do not control for baseline depression symptoms
Expanding the subgroup analyses to include studiesthat controlled for baseline depression plus other co-variates (Zammit et al 2004 Simons et al 2009 Rawalamp Rice 2012) and studies that explicitly excluded fora history of depression diagnosis (Gale et al 2008Vinberg et al 2013 Papmeyer et al 2015) did notchange the null result (r =minus0027 95 CI minus0058 to0005 p = 0097 n = 15)
None of the meta-regression analyses were signifi-cant indicating that the between-study variance wasnot attributable to age at baseline IQ percent of sam-ple that was female percent of the sample that waswhite age at follow-up time between assessmentsyear of cognitive assessment year of follow-up assess-ment or study quality score
Study quality and publication bias
Multiple samples within a study were combined forthe purposes of quality assessment given that studieswithin the same publication were found to employthe same methodology Of the 29 publications reviewed12 were rated as high quality and 17 were rated as me-dium quality Details are provided in SupplementaryTable S1 Comparable results to the overall findingswere obtained when just using high quality studies (r=minus0085 95 CI minus0141 to minus0029 p = 0003)
Inspection of the funnel plot (Fig 4) found no evi-dence for publication bias to support the hypothesisIn fact imputation of negative correlations suggestedthat additional studies favoring the hypothesis maybe missing While the calculated effect size is minus0088(95 CI minus0121 to minus0054) using Duval amp Tweediersquostrim-and-fill method the imputed effect size estimateis larger at minus0137 (95 CI minus0176 to minus0099 imputedstudies n = 11) Last the Fail-safe N procedure foundthat 3583 null studies would need to be located forthe combined two-tailed p value to exceed 005 Thissuggests that significant results are not likely to be con-founded by publication bias and may even underesti-mate true effect sizes
Discussion
The present systematic review and meta-analysis of 29longitudinal publications including 1 21 749 partici-pants revealed that after accounting for baseline depres-sion symptoms variability in cognitive function did notpredict subsequent depression Consistent with priorreports there was a significant contemporaneous associ-ation between higher depression symptoms and lowercognitive function These patterns have implications forunderstanding the association between cognitive func-tion and depression and may be important for advan-cing etiologic and treatment research
Association between cognitive function and subsequent depression 11
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
First our findings reinforce models positing thatcognitive function tracks with depression severity(McDermott amp Ebmeier 2009) One possible explan-ation for this contemporaneous association is that de-pression symptoms interfere with the capacity tocomplete cognitive assessments possibly through thegeneral lack of motivation that is one hallmark of thedisorder While this explanation represents an experi-mental confound for studies focused on assessmentof cognitive function it likewise represents an oppor-tunity for studies to focus more comprehensively onthe assessment of both depression and mood disordersymptoms since performance on cognitive tests maybe a sensitive measure of motivational state thatcould augment self-reported symptoms Alternativelythe co-occurrence of cognitive deficits and depressionsymptoms may reflect shared genetic etiology (Hagen-aars et al 2016) and dysfunction of neural circuits
supporting both cognitive and emotional processes(Scult et al 2016) In particular dysfunction of prefront-al and striatal circuits have been associated with bothdepression and cognitive function (Keedwell et al2005 Aarts et al 2011)
Second our findings suggest that prior studies oflinks between cognitive function and depression thatdid not assess baseline symptoms may have overesti-mated the potential protective role of higher cognitivefunction While the importance of accounting for sub-clinical symptoms is not novel the implementation ofsuch accounting is often neglected in psychiatric epi-demiology given the current categorical threshold-based diagnostic system In our meta-analysis largereffects were observed for continuous as compared tocategorical outcomes which aligns with growing em-phasis on dimensional measures of psychopathology(Cuthbert amp Kozak 2013)
Fig 2 Meta-analysis of the association between cognitive function and subsequent depression A forest plot for all studiesthat investigated associations between cognition and later depression Results are reported as correlation coefficients denotedby squares and 95 confidence intervals (CI) indicated by lines (effect sizes are converted to correlation coefficients ifreported as odds ratios) Meta-analysis results are displayed as the diamond The overall analysis found a significant effect ofcognition on depression (r =minus0088 95 CI minus0121 to minus0054 p lt 0001)
12 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Fig 4 Trim-and-fill funnel plots for all samples Fisherrsquos Z a measure of effect size is plotted on the x-axis and the standarderror is plotted on the y-axis Larger studies appear toward the top of the graph and smaller studies towards the bottom Inthe absence of publication bias the studies are symmetrically distributed around the mean Actual studies are shown in opencircles and imputed studies would be shown in black circles No additional studies would be expected in the oppositedirection (to the right) of the observed effect but an additional 11 studies are imputed to the left of the mean effect sizeWhile the calculated effect size is minus0088 [95 confidence interval (CI) minus0121 to minus0054] using Duval amp Tweediersquos trim-and-fill method the imputed effect size estimate is larger at minus0137 (95 CI minus0176 to minus0099 imputed studies n = 11)
Fig 3 Meta-analysis comparing values adjusted for baseline depression symptoms v unadjusted A forest plot for analysiscomparing results from a subset of the same set of studies reported in Fig 2 when using unadjusted values compared tousing values that are adjusted for baseline depression Effects are significant for unadjusted values [r =minus0120 95 confidenceinterval (CI) minus0169 to minus0070 p lt 0001] but not for adjusted values (r =minus0032 95 CI minus0078 to 0014 p = 0169) Results arereported as correlation coefficients denoted by squares and 95 CIs indicated by lines Meta-analysis results are displayed asdiamonds
Association between cognitive function and subsequent depression 13
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Third the associations between cognitive functionand either current or later depression were not moder-ated by data quality or participant age sex and raceHowever there are a number of additional potentialmoderators that could not be addressed in the currentreview and meta-analysis For example the numberand type of comorbid conditions with depressionwere often not reported in the included studies butcould represent an important moderator of theobserved effects Modeling the effects of comorbid ill-ness is an important avenue for future research
One limitation of the current literature is that only ahandful of studies reviewed explicitly excluded for de-pression diagnosis at baseline (Gale et al 2008 Vinberget al 2013 Papmeyer et al 2015) however consistentwith the finding that controlling for baseline depres-sion symptoms led to a null association between cogni-tion and subsequent depression there was no effectobserved when including these studies in the sub-group analyses further suggesting that the associationbetween cognitive function and depression is likelycontemporaneous It will be important to follow-upthese analyses with individual studies that includerigorous assessment of baseline depression symptomsand other potentially confounding factors to furtherclarify this relationship
An open question that remains for future research iswhether deficits in cognitive function are likely to pre-dict the development of more sever or recurrent de-pression later in life Only one of the included studies(Koenen et al 2009) specifically investigated recurrentdepression and found that lower IQ was associatedwith greater persistence of disorder
A final consideration is that while our review andmeta-analysis focused on general cognitive functionmainly assessed via IQ there may be specific subtypesof cognitive function that are more predictive of laterdepression For example a lack of cognitive flexibilitymay more closely match with the ruminative stylecharacteristic of depression and therefore tasks specifi-cally measuring this component of cognitive functionmight have some predictive utility While our reviewdid not find differences between broad and specificmeasures of cognitive function there were not enoughstudies identified to allow for precise consideration ofdifferences between individual cognitive domains
A limitation of the meta-analysis is that while thepresent study followed standard guidelines (Stroupet al 2000 Atkinson et al 2014) decisions aboutstudy selection data extraction and quality assess-ment include a number of decision points that neces-sarily involve a level of subjectivity Reliability wasascertained by using independent raters however dif-ferent inclusionexclusion criteria or a different ap-proach to the evaluation of those criteria could result
in a different set of studies being includedUltimately the quality of the meta-analysis is depend-ent upon the underlying studies that are analyzedFurthermore although studies with insufficient infor-mation to be included in the meta-analysis were notfound to differ based on basic study data from thosestudies included in the meta-analysis nonetheless itis unknown how if at all data from these studiescould change the overall results
Acknowledging these limitations our present reviewand meta-analysis found that while an association is evi-dent between cognitive function and later depressiongeneral cognitive function does not appear to be a riskfactor for depression but rather is more likely relatedto performance decrements associated with concurrentdepressive symptoms Our results suggest that low cog-nitive function is therefore probably not a causal factorof depression and that clinical practice may benefitmore from a focus on how decreased cognitive functionin the depressed state is likely to influence treatment out-comes (Gyurak et al 2015) Our findings have importantimplications for better understanding depression and forthe design of future studies in highlighting the need tocontrol for subthreshold depression symptoms when in-vestigating risk factors for mental illness as well as whenassessing cognitive function more generally
Supplementary material
The supplementary material for this article can befound at httpdxdoiorg101017S0033291716002075
Acknowledgements
MAS is supported by an National Science Foundation(NSF) Graduate Research Fellowship ARH is sup-ported by National Institutes of Health (NIH) grantsRO1DA033369 amp R01AG049789 TEM is supportedby National Institutes of Health (NIH) grantsR01AG049789 We would like to thank HarrisCooper PhD at Duke University who provided invalu-able insight into conducting the meta-analysis Wethank all of the authors of studies who provided add-itional information for this meta-analysis
Declaration of Interest
None
References
Aarts E van Holstein M Cools R (2011) Striatal dopamineand the interface between motivation and cognitionFrontiers in Psychology 2 163
14 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Atkinson KM Koenka AC Sanchez CE Moshontz HCooper H (2014) Reporting standards for literaturesearches and report inclusion criteria making researchsyntheses more transparent and easy to replicate ResearchSynthesis Methods 6 87ndash95
Baer LH Tabri N Blair M Bye D Li KZH Pushkar D(2013) Longitudinal associations of need for cognitioncognitive activity and depressive symptomatology withcognitive function in recent retirees Journals of GerontologySeries B Psychological Sciences and Social Sciences 68 655ndash664
Barbey AK Colom R Solomon J Krueger F Forbes CGrafman J (2012) An integrative architecture for generalintelligence and executive function revealed by lesionmapping Brain 135 1154ndash1164
Barnett JH Salmond CH Jones PB Sahakian BJ (2006)Cognitive reserve in neuropsychiatry Psychological Medicine36 1053ndash1064
Beaujean AA Parker S Qiu X (2013) The relationshipbetween cognitive ability and depression a longitudinaldata analysis Social Psychiatry and Psychiatric Epidemiology48 1983ndash1992
Belsky DW Caspi A Arseneault L Bleidorn W Fonagy PGoodman M Houts R Moffitt TE (2012) Etiologicalfeatures of borderline personality related characteristics in abirth cohort of 12-year-old children Development andPsychopathology 24 251ndash265
Betts KS Williams GM Najman JM Alati R (2016)Predicting spectrums of adult mania psychosis anddepression by prospectively ascertained childhoodneurodevelopment Journal of Psychiatric Research 72 22ndash29
Bora E Harrison BJ Yuumlcel M Pantelis C (2013) Cognitiveimpairment in euthymic major depressive disorder a meta-analysis Psychological Medicine 43 2017ndash2026
Borenstein M Hedges LV Higgins JPT Rothstein HR(2011) Introduction to Meta-Analysis John Wiley amp SonsWest Sussex UK
Canals J Domegravenech-Llaberia E Fernaacutendez-Ballart J Martiacute-Henneberg C (2002) Predictors of depression at eighteenA 7-year follow-up study in a Spanish nonclinicalpopulation European Child amp Adolescent Psychiatry 11226ndash233
Christensen H Griffiths K Mackinnon A (1997) Aquantitative review of cognitive deficits in depression andAlzheimer-type dementia Selection of Studies 3 631ndash651
Connolly SL Wagner Ca Shapero BG Pendergast LLAbramson LY Alloy LB (2014) Rumination prospectivelypredicts executive functioning impairments in adolescentsJournal of Behavior Therapy and Experimental Psychiatry 4546ndash56
Cooper HM (1979) Statistically combining independentstudies a meta-analysis of sex differences in conformityresearch Journal of Personality and Social Psychology 37131ndash146
Cooper HM (2010) Research Synthesis and Meta-Analysis AStep-by-Step Approach 4th edn SAGE PublicationsWashington (DC) USA
Cuijpers P de Graaf R van Dorsselaer S (2004) Minordepression risk profiles functional disability health careuse and risk of developing major depression Journal ofAffective Disorders 79 71ndash79
Cuthbert BN Kozak MJ (2013) Constructing constructs forpsychopathology the NIMH research domain criteriaJournal of Abnormal Psychology 122 928ndash937
Der G Batty GD Deary IJ (2009) The association between IQin adolescence and a range of health outcomes at 40 in the1979 US National Longitudinal Study of Youth Intelligence37 573ndash580
Dubow EF Boxer P Huesmann LR (2008) Childhood andadolescent predictors of early and middle adulthoodalcohol use and problem drinking the Columbia CountyLongitudinal Study Addiction 103 36ndash47
Duval S Tweedie R (2000) Trim and fill a simple funnel-plot-based method of testing and adjusting for publicationbias in meta-analysis Biometrics 56 455ndash463
Evans LD Kouros CD Samanez-Larkin S Garber J (2015)Concurrent and short-term prospective relations amongneurocognitive functioning coping and depressivesymptoms in youth Journal of Clinical Child and AdolescentPsychology 53 1ndash15
Franz CE Lyons MJ OrsquoBrien R Panizzon MS Kim K BhatR Grant MD Toomey R Eisen S Xian H Kremen WS(2011) A 35-year longitudinal assessment of cognition andmidlife depression symptoms the Vietnam Era Twin Studyof Aging American Association for Geriatric PsychiatryAmerican Journal of Geriatric Psychiatry 19 559ndash570
Gale CR Batty GD Tynelius P Deary IJ Rasmussen F(2010) Intelligence in early adulthood and subsequenthospitalization for mental disorders Epidemiology 2170ndash77
Gale CR Deary IJ Boyle SH Barefoot J Mortensen LHBatty GD (2008) Cognitive ability in early adulthood andrisk of 5 specific psychiatric disorders in middle age theVietnam experience study Archives of General Psychiatry 651410ndash1418
Gale CR Hatch SL Batty GD Deary IJ (2009) Intelligence inchildhood and risk of psychological distress in adulthoodthe 1958 National Child Development Survey and the 1970British Cohort Study Intelligence 37 592ndash599
Gjerde PF (1995) Alternative pathways to chronicdepressive symptoms in young adults gender differencesin developmental trajectories Child Development 661277ndash1300
Gottfredson LS (1997) Mainstream science on intelligence aneditorial with 52 signatories history and bibliographyIntelligence 24 13ndash23
Guyer AE Choate VR Grimm KJ Pine DS Keenan K(2011) Emerging depression is associated with facememory deficits in adolescent girls Elsevier Inc Journal ofthe American Academy of Child and Adolescent Psychiatry 50180ndash190
Gyurak A Patenaude B Korgaonkar MS Grieve SMWilliams LM Etkin A (2015) Frontoparietal activationduring response inhibition predicts remission toantidepressants in patients with major depression BiologicalPsychiatry 79 1ndash8
Hagenaars SP Harris SE Davies G Hill WD LiewaldDCM Ritchie SJ Marioni RE Fawns-Ritchie C Cullen BMalik R METASTROKE Consortium IC for BPGSpiroMeta Consortium CHARGE ConsortiumPulmonary Group CCA and LG Worrall BB Sudlow
Association between cognitive function and subsequent depression 15
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
CLM Wardlaw JM Gallacher J Pell J McIntosh AMSmith DJ Gale CR Deary IJ (2016) Shared geneticaetiology between cognitive functions and physical andmental health in UK Biobank (N = 112 151) and 24 GWASconsortiaMolecular Psychiatry Published online 26 January2016 doi101038mp2015225
Hatch SL Jones PB Kuh D Hardy R Wadsworth MEJRichards M (2007) Childhood cognitive ability and adultmental health in the British 1946 birth cohort Social Scienceamp Medicine (1982) 64 2285ndash2296
Hipwell AE Sapotichne B Klostermann S Battista DKeenan K (2011) Autobiographical memory as a predictorof depression vulnerability in girls Journal of Clinical Childand Adolescent Psychology 40 254ndash265
Horowitz JL Garber J (2003) Relation of intelligence andreligiosity to depressive disorders in offspring of depressedand nondepressed mothers The American Academy ofChild and Adolescent Psychiatry Journal of the AmericanAcademy of Child and Adolescent Psychiatry 42 578ndash586
Johnson W Bouchard TJ Krueger RF McGue MGottesman II (2004) Just one g consistent results fromthree test batteries Intelligence 32 95ndash107
Keedwell PA Andrew C Williams SCR Brammer MJPhillips ML (2005) The neural correlates of anhedoniain major depressive disorder Biological Psychiatry 58843ndash853
Kessler RC Berglund P Demler O Jin R Koretz DMerikangas KR Rush AJ Walters EE Wang PS (2003)The epidemiology of major depressive disorder resultsfrom the National Comorbidity Survey Replication(NCS-R) Journal of the American Medical Association 2893095ndash3105
Koenen KC Moffitt TE Roberts AL Martin LT KubzanskyL Harrington H Poulton R Caspi A (2009) Childhood IQand adult mental disorders a test of the cognitive reservehypothesis American Journal of Psychiatry 166 50ndash57
Lewinsohn PM Solomon A Seeley JR Zeiss A (2000)Clinical implications of lsquosubthresholdrsquo depressivesymptoms Journal of Abnormal Psychology 109 345ndash351
Luppino FS de Wit LM Bouvy PF Stijnen T Cuijpers PPenninx BWJH Zitman FG (2010) Overweight obesityand depression a systematic review and meta-analysisof longitudinal studies Archives of General Psychiatry 67220ndash229
McCord J Ensminger ME (1997) Multiple risks andcomorbidity in an African-American population CriminalBehaviour and Mental Health 7 339ndash352
McDermott LM Ebmeier KP (2009) A meta-analysis ofdepression severity and cognitive function Elsevier BVJournal of Affective Disorders 119 1ndash8
Melartin TK Rytsaumllauml HJ Leskelauml US Lestelauml-Mielonen PSSokero TP Isometsauml ET (2002) Current comorbidity ofpsychiatric disorders among DSM-IV major depressivedisorder patients in psychiatric care in the VantaaDepression Study Journal of Clinical Psychiatry 63 126ndash134
Meyer SE Carlson GA Wiggs EA Martinez PE RonsavilleDS KlimesndashDougan B Gold PW RadkendashYarrow M(2004) A prospective study of the association amongimpaired executive functioning childhood attentional
problems and the development of bipolar disorderDevelopment and Psychopathology 16 461ndash476
MiyakeA FriedmanNP EmersonMJWitzki aHHowerter AWager TD (2000) The unity and diversity of executivefunctions and their contributions to complex lsquoFrontal Lobersquotasks a latentvariable analysisCognitive Psychology41 49ndash100
Moher D Liberati A (2009) Preferred reporting items forsystematic reviews and meta-analyses the PRISMAstatement Annals of Internal Medicine 151 264ndash269
Papmeyer M Sussmann JE Hall J McKirdy J Peel AMacdonald A Lawrie SM Whalley HC McIntosh AM(2015) Neurocognition in individuals at high familial riskof mood disorders with or without subsequent onset ofdepression Psychological Medicine 45 1ndash11
Peterson RA Brown SP (2005) On the use of betacoefficients in meta-analysis Journal of Applied Psychology90 175ndash181
Pine DS Cohen P Brook J Coplan JD (1997) Psychiatricsymptoms in adolescence as predictors of obesity in earlyadulthood a longitudinal study American Journal of PublicHealth 87 1303ndash1310
Quinn ME Joormann J (2015) Control when it countschange in executive control under stress predicts depressionsymptoms Emotion Junio 22 1ndash10
Rawal A Rice F (2012) Examining overgeneralautobiographical memory as a risk factor for adolescentdepression Elsevier Inc Journal of the American Academy ofChild and Adolescent Psychiatry 51 518ndash527
Ree MJ Earles JA (1991) The stability of g across differentmethods of estimation Intelligence 15 271ndash278
Rock PL Roiser JP Riedel WJ Blackwell AD (2014)Cognitive impairment in depression a systematic reviewand meta-analysis Psychological Medicine 44 2029ndash2040
Rogers MA Kasai K Koji M Fukuda R Iwanami ANakagome K Fukuda M Kato N (2004) Executive andprefrontal dysfunction in unipolar depression a review ofneuropsychological and imaging evidence NeuroscienceResearch 50 1ndash11
Scult MA Knodt AR Swartz JR Brigidi BD Hariri AR(2016) Thinking and feeling individual differences inhabitual emotion regulation and stress-related mood areassociated with prefrontal executive control ClinicalPsychological Science doi1011772167702616654688
Sharp C Petersen N Goodyer I (2008) Emotional reactivityand the emergence of conduct problems and emotionalsymptoms in 7- to 11-year-olds a 1-year follow-up studyJournal of the American Academy of Child and AdolescentPsychiatry 47 565ndash573
Siegel LS (1999) Issues in the definition and diagnosis oflearning disabilities a perspective on Guckenberger vBoston University Journal of Learning Disabilities 32 304ndash319
Simons CJP Jacobs N Derom C Thiery E Jolles J van Os JKrabbendam L (2009) Cognition as predictor of currentand follow-up depressive symptoms in the generalpopulation Acta Psychiatrica Scandinavica 120 45ndash52
Slykerman RF Thompson J Waldie K Murphy R Wall CMitchell EA (2015) Maternal stress during pregnancy isassociated with moderate to severe depression in 11-year-old children Acta Paediatrica 104 68ndash74
16 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Snyder HR (2013) Major depressive disorder is associatedwith broad impairments on neuropsychological measuresof executive function a meta-analysis and reviewPsychological Bulletin 139 81ndash132
Soslashrensen HJ Saeligbye D Urfer-Parnas A Mortensen ELParnas J (2012) Premorbid intelligence and educationallevel in bipolar and unipolar disorders a Danish draftboard study Journal of Affective Disorders 136 1188ndash1191
SpearmanC (1904) lsquoGeneral intelligencersquoobjectivelydeterminedandmeasuredAmerican Journal of Psychology 15 201
Stern Y (2003) The concept of cognitive reserve a catalyst forresearch Journal of Clinical and Experimental Neuropsychology(Neuropsychology Development and Cognition Section A) 25589ndash593
Stroup D Berlin J Morton S Olkin I Williamson GDRennie D Moher D Becker BJ Sipe TA Thacker SB(2000) Meta-analysis of Observational Studies inEpidemiology a proposal for reporting Journal of theAmerican Medical Association 283 2008
Vinberg M Miskowiak KW Kessing LV (2013) Impairmentof executive function and attention predicts onset ofaffective disorder in healthy high-risk twins Journal ofClinical Psychiatry 74 e747ndashe753
Zammit S Allebeck P David AS Dalman C HemmingssonT Lundberg I Lewis G (2004) A longitudinal study ofpremorbid IQ Score and risk of developing schizophreniabipolar disorder severe depression and other nonaffectivepsychoses Archives of General Psychiatry 61 354ndash360
Association between cognitive function and subsequent depression 17
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms

these tasks (Ree amp Earles 1991) Even in cases when lsquogrsquois not calculated as such there are other customaryways of capturing this general factor by combingacross cognitive tasks eg by creating an index of ex-ecutive functions (Miyake et al 2000) or measuringthe intelligence quotient (Gottfredson 1997)
Although executive functions and intelligence areoften considered independently evidence has sug-gested that they may best be characterized by an inte-grated framework based on a common neural network(Barbey et al 2012) supporting the idea that theyreflect a shared general factor of cognitive ability Inlight of these findings and the observation that indivi-duals with depression commonly exhibit deficits acrossa range of cognitive tasks our review used the broad-est measure of cognitive function that was available ina given study When a higher-order construct was notavailable results from individual measures were usedWe restricted analyses to prospective cohort studieswith depression assessment before age 65 in order tominimize potential influences of age-related cognitivedecline
We follow our literature review with a quantitativemeta-analysis to (1) determine whether cognitive func-tion predicts later depression (2) evaluate whether dif-ferences in the measurement of depression (categoricalv continuous) influence observed associations and (3)examine whether sex or age of participants may mod-erate effects and (4) whether effects are confounded bydepression symptoms at baseline
Methods
We followed the Meta-Analyses of ObservationalStudies in Epidemiology (MOOSE) guidelines (Stroupet al 2000) (Supplementary Table S1) and the literaturesearch strategies suggested by Atkinson et al (2014)
Search process
Systematic searches were conducted in February 2015and updated in December 2015 in three electronic data-bases PubMed EMBASE and PsycINFO Searcheswere conducted by a research librarian EM and over-seen by MS The search syntax was adapted for eachdatabase and designed to capture the participants pre-dictors comparisons and outcomes described belowaccording to the PICOS framework (Moher amp Liberati2009) The Boolean operator lsquoORrsquo was used within cat-egories and the operator lsquoANDrsquo was used betweencategories The complete search strategy is describedin the Search Strategy in the Supplementary MaterialHand searches were conducted of the reference listsof included articles
Eligibility criteria
The review included English language studies of em-pirical studies investigating the longitudinal associ-ation of cognitive function (IQ neuropsychologicaltests executive functions) with unipolar depressiondiagnosis or symptoms Detailed inclusionexclusioncriteria were as follows
Participant characteristics
Eligible studies included children adolescents andadults under the age of 65 This age range was spe-cified because of the possible impact of cognitive de-cline in older populations Articles examining ahighly specific population (eg with a particular med-ical diagnosis) were excluded so as to not limit the gen-eralizability of results Studies that required MDDdiagnosis hospitalization or admission to a treatmentcenter as part of the inclusion criteria at baselinewere also excluded from the review so as to permitconclusions about depression onset This was to ensurethat a majority of study participants did not have de-pression at baseline However cohort studies wereincluded even if they did not measure depression atbaseline assuming that these samples would have de-pression prevalence rates that were comparable topopulation norms Subgroup analyses were subse-quently performed on the studies that specificallyexcluded for any history of depression If there wereseveral papers about one cohort the paper with largersample size or better study quality was included
Predictor type
Eligible studies included a measure of cognitive execu-tive or neuropsychological function The studyincluded a range of cognitive predictors given thatprevious studies have found broad deficits in cognitivefunction in depression (Christensen et al 1997 Rogerset al 2004 Snyder 2013 Rock et al 2014) Whenmore than one cognitive predictor was reported as anoutcome in a study the broadest measure of cognitivefunctioning was used If no measure captured broadcognitive functioning the measure that was mostclosely aligned with constructs on a standard IQ test(working memory processing speed verbal compre-hension or perceptual reasoning) was used in themeta-analysis
Studies were excluded if cognitive function wasassessed via educational achievement given thatthese measures can be more easily influenced by learn-ing disabilities than by general cognitive functioning(Siegel 1999) Self-report descriptive measures of cog-nitive functioning were also excluded in favor ofmore objective measures Last since this study sought
2 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Table 1 Characteristics of included studies
StudyName ofcohort Type of cohort
Samplesize Comorbidity
Howdepressionassessed
Mean IQatbaseline
Name ofcognitivemeasure
Type of cognitivemeasure
Name ofdepressionoutcome
Type ofdepressionoutcome
Covariatesincluded inmeta-analysisa
Percentfemale Raceethnicity Continent
Meanage atbaseline
Timebetweenassessments(years)
Year ofinitialassessment
Baer et al(2013)
ConcordiaLongitudinalRetirementProject
Retirees 333 NR Studyassessment
NR MontrealCognitiveAssessment
VerbalComprehensionPerceptualReasoning WorkingMemory
Center forEpidemiologicalStudiesDepression Scale(CES-D)
Continuous Depressionsymptoms atTime 1
NR (bothmaleandfemale)
NR NorthAmerica
5906 4 sim2005
Beaujeanet al (2013)
NationalLongitudinalStudy ofAdolescentHealth (AddHealth)
Communitysample
14 322 NR Studyassessment
10061 Add HealthPictureVocabularyTest (AHPVT)ndash an abridgedversion of thePPVT-R
VerbalComprehension
Created for thisstudy
Continuous Depressionsymptoms atTime 1
50 7631 White1674Black 422Asian 25AmericanIndian1183Hispanic005 MixedRace
NorthAmerica
1598 7 1994
Belsky et al(2012)
EnvironmentalRiskLongitudinalTwin Study(E-Risk)
Birth cohort 2123 Conductdisorderanxietypsychosisborderlinepersonalitydisorder
Studyassessment
100 WechslerPreschool andPrimary Scaleof Intelligence(WPPSI)
General IntelligenceVerbalComprehensionPerceptualReasoning
ChildrenrsquosDepressionInventory (CDI)
Continuous None 51 sim90 White Europe 5 7 1999
Betts et al(2016)
MaterUniversityStudy ofPregnancy(MUSP)
Pre-birthcohort
1934 PsychosisMania
Studyassessment
NR PeabodyPictureVocabularyTest-Revised(PPVT-R)
VerbalComprehension
CompositeInternationalDiagnosticInterview(CIDI-Auto)
Continuous(latentfactor)
None NR NR Australia 5 16 1989
Canals et al(2002)(females)
NR Communitysample
99 NR Studyassessment
NR Academicaptitude test(AAT)
General IntelligenceVerbalComprehensionPerceptualReasoning
Schedules forClinicalAssessment inNeuropsychiatry
Categorical None 100 NR Europe sim11 6 NR
Canals et al(2002)(males)
NR Communitysample
100 NR Studyassessment
NR Academicaptitude test(AAT)
General IntelligenceVerbalComprehensionPerceptualReasoning
Schedules forClinicalAssessment inNeuropsychiatry
Categorical None 0 NR Europe sim12 6 NR
Connollyet al (2014)
TempleUniversityAdolescentCognitionand Emotion(ACE) Project
Communitysample
200 NR Studyassessment
NR Digit Span fromWechslerIntelligenceScale forChildren(WISC)
Working Memory ChildrenrsquosDepressionInventory (CDI)
Continuous Depressionsymptoms atTime 1
565 452 White513 Black
NorthAmerica
1241 1 NR
Association
between
cognitivefunction
andsubsequent
depression3
httpdxdoiorg101017S0033291716002075D
ownloaded from
httpww
wcam
bridgeorgcore Duke U
niversity Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core term
s of use available at httpww
wcam
bridgeorgcoreterms
Table 1 (cont)
StudyName ofcohort Type of cohort
Samplesize Comorbidity
Howdepressionassessed
Mean IQatbaseline
Name ofcognitivemeasure
Type of cognitivemeasure
Name ofdepressionoutcome
Type ofdepressionoutcome
Covariatesincluded inmeta-analysisa
Percentfemale Raceethnicity Continent
Meanage atbaseline
Timebetweenassessments(years)
Year ofinitialassessment
Der et al(2009)
US NationalLongitudinalSurvey ofYouth 1979
Communitysample
7458 Noted a rangeof healthconditions
Studyassessment
NR Armed ServicesVocationalAptitudeBattery(ASVAB)Armed ForcesQualificationTest (AFQT)
General IntelligenceVerbalComprehension
Center forEpidemiologicalStudiesDepression Scale(CES-D)
Continuous Depressionsymptoms atTime 1
52 31 Black19Hispanic
NorthAmerica
179 sim22 1979
Dubow et al(2008)(females)
ColumbiaCountyLongitudinalStudy(CCLS)
SchoolChildrenGrade 3
215 NR Studyassessment
sim104 CaliforniaShort-FormTest of MentalMaturity
General Intellignce MinnesotaMultiphasicPersonalityInventory(MMPI) Scale 2
Continuous None 100 90 White3 Blacklt1Asianlt1Hispanic
NorthAmerica
8 11 1960
Dubow et al(2008)(males)
ColumbiaCountyLongitudinalStudy(CCLS)
SchoolChildrenGrade 3
211 NR Studyassessment
sim104 CaliforniaShort-FormTest of MentalMaturity
General Intelligence MinnesotaMultiphasicPersonalityInventory(MMPI) Scale 2
Continuous None 0 90 White3 Blacklt1Asianlt1Hispanic
NorthAmerica
8 11 1960
Evans et al(2015)
NR SchoolChildrenGrades 5ndash9
192 Some withADHD
Studyassessment
111 WechslerAbbreviatedScale ofIntelligence(WASI)
General IntelligenceVerbalComprehensionPerceptualReasoning WorkingMemorySet-Shifting
ChildrenrsquosDepressionInventory (CDI)
Continuous Depressionsymptoms atTime 1
521 714 White182 Black26 Asian36Hispanic42 MixedRace
NorthAmerica
1236 03 sim2000s
Franz et al(2011)
Vietnam EraTwin Studyof Aging
Military cohort 1231 NR Studyassessment
NR Armed ForcesQualificationTest (AFQTForm 7A)
General IntelligencePerceptualReasoning WorkingMemory ProcessingSpeed Set-ShiftingInhibition
Center forEpidemiologicalStudiesDepression Scale(CES-D)
Continuous None 0 86 White NorthAmerica
20 35 sim1970
Gale et al(2008)
VietnamExperienceStudy (VES)
Military cohort 3258 Mix Studyassessment
100 Generaltechnicalsection of theArmyClassificationBattery
General IntelligenceVerbalComprehensionArithmeticreasoning
DiagnosticInterviewSchedule (DIS)
Categorical SocioeconomicStatusEthnicity Placeof service
0 808 White127 Black
NorthAmerica
204 sim17 sim1964
Gale et al(2009)(1958Cohort)
1958 NationalChildDevelopmentSurvey
Birth cohort 6369 NR Studyassessment
1028 General abilitytest devisedby theNationalFoundationforEducationalResearch inEngland andWales
General Intelligence Rutterrsquos MalaiseInventory
Continuous None NR (bothmaleandfemale)
NR Europe 11 22 1969
4MA
Scultet
al
httpdxdoiorg101017S0033291716002075D
ownloaded from
httpww
wcam
bridgeorgcore Duke U
niversity Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core term
s of use available at httpww
wcam
bridgeorgcoreterms
Gale et al(2009)(1970Cohort)
1970 BritishCohort Study
Birth cohort 6074 NR Studyassessment
1018 British abilityScale
General Intelligence Rutterrsquos MalaiseInventory
Continuous None NR (bothmaleandfemale)
NR Europe 10 20 1980
Gjerde(1995)(females)
NR Recruited froma nurseryschool
51 NR Studyassessment
1187 Wechsler AdultIntelligenceScale (WAIS)
General Intelligence General BehaviorInventory (GBI)Depression scale
Continuous None 100 sim66 Whitesim25Blacksim005Asian
NorthAmerica
18 5 1983
Gjerde et al(1995)(males)
NR Recruited froma nurseryschool
45 NR Studyassessment
11112 Wechsler AdultIntelligenceScale (WAIS)
General Intelligence General BehaviorInventory (GBI)Depression scale
Continuous None 0 sim66 Whitesim25 Blacksim005Asian
NorthAmerica
18 5 1983
Hatch et al(2007)
1946 BritishCohort Study
Birth cohort 957 NR Studyassessment
NR NationalFoundationforEducationalResearch Test
General IntelligenceVerbalComprehensionPerceptualReasoning
General HealthQuestionnaire(GHQ-28)-severedepressionsubscale
Continuous None 51 NR Europe 8 45 1954
Hipwellet al (2011)
PittsburghGirls Study(PGS)
Communitysample
195 NR Studyassessment
9954 WechslerIntelligenceScale forChildren(WISC) III-R
VerbalComprehension
Schedule forAffectiveDisorders forSchool-AgeChildren-Present andLifetime Version(K-SADS-PL)
Continuous Depressionsymptoms atTime 1
100 70 Black ormultiracial
NorthAmerica
1154 1 1998
Horowitz ampGarber(2003)
NR Elementaryschool cohort
196 NR Studyassessment
10461 WechslerIntelligenceScale forChildren(WISC) -R
General IntelligenceVerbalComprehensionPerceptualReasoning
Schedule forAffectiveDisorders forSchool-AgeChildren-EpidemiologicalVersion(K-SADS-E)
Categorical Depressionsymptoms atTime 1
542 89 White147 Black33 Other
NorthAmerica
1186 6 sim1980
Koenenet al (2009)
DunedinCohort
Birth cohort 730 None Studyassessment
NR WechslerIntelligenceScale forChildren(WISC)
General IntelligenceVerbalComprehensionPerceptualReasoning WorkingMemory ProcessingSpeed
DiagnosticInterviewAssessment (forDSM-IV)
Categorical SexSocioeconomicStatusPhysicalHealthchildhoodmaltreatment
48 lsquoPrimarilyWhitersquo
NewZealand
9 23 1981
McCord ampEnsminger(1997)(females)
WoodlawnCohort
Elementaryschool cohort
346 Some withalcoholism
Studyassessment
NR (13 Unspecified IQof sample had scoresover 110)
General Intelligence CompositeInternationalInterviewSchedule(according toDSM-III-R)
Categorical None 100 100 Black NorthAmerica
sim6 27 1966
McCord ampEnsminger(1997)(males)
WoodlawnCohort
Elementaryschool cohort
313 Some withalcoholism
Studyassessment
NR (11 Unspecified IQof sample had scoresover 110)
General Intelligence CompositeInternationalInterviewSchedule(according toDSM-III-R)
Categorical None 0 100 Black NorthAmerica
sim6 27 1966
Meyer et al(2004)
NR Risk sample 86 NR Studyassessment
sim118 WISC General IntelligenceVerbalComprehensionPerceptualReasoning
SCID Categorical None 63 90 White9 Black 1Hispanic
NorthAmerica
11 13 1989
Association
between
cognitivefunction
andsubsequent
depression5
httpdxdoiorg101017S0033291716002075D
ownloaded from
httpww
wcam
bridgeorgcore Duke U
niversity Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core term
s of use available at httpww
wcam
bridgeorgcoreterms
Table 1 (cont)
StudyName ofcohort Type of cohort
Samplesize Comorbidity
Howdepressionassessed
Mean IQatbaseline
Name ofcognitivemeasure
Type of cognitivemeasure
Name ofdepressionoutcome
Type ofdepressionoutcome
Covariatesincluded inmeta-analysisa
Percentfemale Raceethnicity Continent
Meanage atbaseline
Timebetweenassessments(years)
Year ofinitialassessment
Papmeyeret al (2015)
ScottishBipolarFamily Study
Risk sample 111 NR Studyassessment
Controls108Patients107
National AdultReading Test(NART)
VerbalComprehension
Structured ClinicalInterview forDSM Disorders(SCID)symptoms
Categorical None 52 NR Europe 21 2 NR
Pine et al(1997)
NR Communitysample
644 NR Studyassessment
1007 UnspecifiedlsquoIQrsquo
General Intelligence Based onDiagnosticInterviewSchedule forChildren
Continuous Depressionsymptoms atTime 1
52 91 White NorthAmerica
138 9 1983
Quinn ampJoormann(2015)
NR Undergraduatestudents
43 NR Studyassessment
NR n-back Working Memory Beck DepressionInventory II(BDI-II)
Continuous Depressionsymptoms atTime 1
63 58 White30Hispanic orLatino 19Asian 2AfricanAmerican2AmericanIndian 2NativeHawaiian2 Indian
NorthAmerica
19 014 NR
Rawal ampRice (2012)
EarlyPrediction ofAdolescentDepressionstudy
Risk sample 230 None Studyassessment
9746 WechslerIntelligenceScale forChildren(WISC)
General IntelligenceVerbalComprehensionPerceptualReasoning WorkingMemory ProcessingSpeed
Child andAdolescentPsychiatricAssessment(CAPA)
Both Depressionsymptoms atTime 1 AgeOvergeneralityto negativecues
596 NR Europe 1371 1 NR
Sharp et al(2008)
The ChildBehaviourStudy
Communitysample
439 NR Studyassessment
105 WechslerIntelligenceScale forChildren(WISC)
General IntelligenceVerbalComprehensionPerceptualReasoning
The Mood andFeelingsQuestionnaire
Continuous Depressionsymptoms atTime 1
52 97 White05 Black25 Asian
Europe 94 1 NR
Simons et al(2009)
East FlandersProspectiveTwin Survey
Twin registry 444 NR Studyassessment
NR Principalcomponentfrom StroopConceptShifting Testand LetterDigitSubstitutionTest
Processing SpeedSet-ShiftingInhibition
Structured ClinicalInterview forDSM Disorders(SCID)symptoms
Continuous Depressionsymptoms atTime 1
100 NR Europe 28 2 NR
6MA
Scultet
al
httpdxdoiorg101017S0033291716002075D
ownloaded from
httpww
wcam
bridgeorgcore Duke U
niversity Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core term
s of use available at httpww
wcam
bridgeorgcoreterms
Slykermanet al (2015)
AucklandBirthweightCollaborativeStudy
Birth cohortrisk sample
609 NR Studyassessment
NR Stanford-BinetIntelligenceScale 4th Ed
General IntelligenceFluid ReasoningKnowledgeQunatitativeReasoningVisual-SpatialProcessingWorking Memory
Center forEpidemiologicalStudiesDepression Scale(CES-D)
Categorical(cut-point)
None 49 NR NewZealand
35 75 sim2000
Soslashrensenet al (2012)
DanishDraft-BoardStudy
Military cohort 21 914 NR Psychiatricregistry
Controls100Patients96ndash98
Boslashrge PriensProslashve (BPP)
General IntelligenceVerbalComprehensionPerceptualReasoning
DanishInternationalClassification ofdiseases (ICD) 8amp 10
Categorical None 0 NR Europe 195 sim36 1968ndash1989
Vinberget al (2013)
NR High-risktwins
224 Bipolardisorderanxietysubstanceabuse other
Studyassessmentpsychiatricregistry
NR CambridgeCognitiveAssessment(CAMCOG)
GeneralNeuropsychologicalFunctionOrientationLanugage MemoryAttention AbstractThinking VisualPerception
Beck DepressionInventory (BDI)
Continuous Depressionsymptoms atTime 1
65 NR Europe 439 7 2003
Zammitet al (2004)
SwedishConscripts(1969ndash1970)
Military cohort 50 053 None Hospitallinkage
NR UnspecifiedlsquoIQrsquo
General IntelligenceVerbalComprehensionPerceptualReasoning GeneralKnowledgeMechanicalKnowledge
InternationalClassification ofdiseases (ICD)hospitalpsychiatricadmissions
Categorical Diagnosis atbaselinedisturbedbehavior druguse raised in acity
0 NR Europe sim19 27 1969
Sample size is the number of subjects included in reported analyses of interest NR not reportedsim indicates only a range was reporteda This column notes covariates included in the meta-analysis We focused on controlling for depressive symptoms at T1 but some studies reported effect sizes that also included controlling
for other variables ndash when the zero-order correlations were unavailable these estimates were used
Association
between
cognitivefunction
andsubsequent
depression7
httpdxdoiorg101017S0033291716002075D
ownloaded from
httpww
wcam
bridgeorgcore Duke U
niversity Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core term
s of use available at httpww
wcam
bridgeorgcoreterms
to investigate general information processing abilitiesrather than cognitive attributional style studies withcognitive attribution measures as the sole cognitivemeasure were excluded
Comparisons
Search terms used to indicate the possible associationbetween cognitive function and depression includedrisk premorbid prodromal onset predict and association(for a full list see search terms in the SupplementaryMaterial) When data were reported from multipletime-points the analysis accounting for the longesttime between assessments was used
Outcomes
Eligible studies reported depression diagnosis orsymptoms determined by investigator or self-reportPresence of comorbidity was permitted given that de-pression has been found to be highly comorbid withother disorders (Melartin et al 2002 Kessler et al2003) Articles not adequately specifying how depres-sion was assessed or articles that did not uniquelymeasure depression [ie only had an index of lsquomentaldisordersrsquo or the category of lsquomood disordersrsquo lumpedtogether (Gale et al 2010)] were excluded if no uniquemeasure of depression could be obtained from studyauthors This is because although comorbidity waspermitted these could have represented instances ofpure anxiety disorders with few or no depressivesymptoms or instances of bipolar disorder
Study design
Eligible study search terms included cohort studies lon-gitudinal epidemiological prospective retrospective follow-up or case-control studies Studies not following a longi-tudinal design were excluded during full-text reviewAdditionally studies where cognitive function wasassessed only concurrently with or after depressionwere excluded given that the purpose of the reviewwas to investigate whether cognitive function pre-dicted later depression
Studies were included regardless of whether theywere reported in peer-review journals in order to ac-count for potentially biased reporting of resultsReview articles were included in the search terms tofind additional relevant references but were notincluded in the meta-analysis Baseline and protocolstudies without follow-up data were excluded
Study selection
A flow diagram of the process of study selection showsthe overall procedures (Fig 1) Records identified fromthe search processes were combined in EndNote
software version X7 and duplicates were removedTitles and abstracts were reviewed independently bytwo reviewers (MS and AP) according to the eligibil-ity criteria described above and marked as either po-tentially eligible or not eligible If either authormarked an article as potentially eligible it wasincluded in the full-text review for closer examinationby MS and AP who used an electronic form to indi-cate if an article should be included or excluded in thefinal selection When an article was excluded the rea-son for exclusion was selected from a hierarchical listof exclusion criteria presented in Fig 1 Both MSand AP were initially blinded to the otherrsquos decisionsAfter both MS and AP completed their reviews dis-crepancies about whether a study should be includedor excluded were resolved via discussion and consen-sus amongst MS AP TM AH and TS
Data extraction
Study information was extracted independently byMS and AP using an electronic form created forthis study Information was collected and codedbased on report characteristics participant characteris-tics study setting predictors outcome measures andquality assessment (Cooper 2010) Any discrepancies(approximately 3 of data points) were resolved viaconsensus
For studies with categorical depression diagnoses ef-fect sizes were generally presented as odds ratios Forthese studies the odds ratio plus the upper and lowerbound of the confidence interval were recorded Twoof the studies (Zammit et al 2004 Gale et al 2008)reported odds ratios greater than one to indicate thatlower IQ was associated with greater risk of depressionThe other studies reported odds ratios in the reverseleading to odds ratios less than one for the same direc-tion of the effect Therefore the odds ratios from the firsttwo studies were recalculated by dividing (1oddsratio) Another study (McCord amp Ensminger 1997)reported results from chi-squared tests Additional stud-ies reported mean premorbid IQ scores rather than oddsratios in which case the means sample sizes andor pvalues and number of tails of the t test were utilizedto calculate the effect size
For studies in which depression was measured as acontinuous variable effect sizes were presented as cor-relation coefficients The direction of the effect (posi-tive or negative) and the sample size were alsoextracted to be used in the meta-analysis Two studiesreported only beta weights (Simons et al 2009 Rawalamp Rice 2012) and we were not able to obtain zero-order correlations from the authors Given that previ-ous reports have suggested that beta weights can beused as an estimate of correlation coefficients in
8 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
meta-analysis (Peterson amp Brown 2005) the betaweights were used instead and analyses were runboth including and excluding these data points
When insufficient information was presented in thearticle authors were contacted requesting further de-tail An additional six studies were included at thispoint One study (Hatch et al 2007) included effectsizes for the female half of the cohort and did not pro-vide statistics for the males but did indicate a null ef-fect Only women from this study were included in themeta-analyses but imputing a score of 0 for the malesyielded similar overall results
Follow-up analyses directly compared studies thatreported zero-order correlations between IQ at time
1 depression at time 1 and depression at time 2(additional details described in the SupplementaryMethods)
Statistical methods
Data were analyzed using Comprehensive Meta-Analysis software version 30 (Biostat Inc USA) Arandom-effects model was used for expected hetero-geneity across studies A random-effects model alsoallows for broader generalization of results to thepopulation at large Heterogeneity of effects was calcu-lated using the Q statistic where a significant p valueindicates that true effect varies across studies The I2
Fig 1 Flow diagram of the search process
Association between cognitive function and subsequent depression 9
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
statistic was used to calculate the ratio of the true het-erogeneity to total variation acting as an index of sig-nal-to-noise ratio When I2 is large it is has beenrecommended to consider subgroup analysis or meta-regression to account for the variance (Borensteinet al 2011)
Subgroup analyses were conducted using a mixed-effects analysis in which a random effects model wasused to combine studies within each subgroup and afixed effect model was used to combine subgroupsand yield the overall effect (the study-to-study vari-ance is not assumed to be the same for all subgroups)Subgroup analyses were conducted comparing type ofoutcome (continuous v categorical) broad v specificcognitive measures and outcomes that were adjustedv unadjusted for baseline depression symptoms
Meta-regression was performed using the followingvariables on unadjusted analyses age at baseline ageat follow-up time between assessments IQ percentwhite year of cognitive assessment year of follow-upassessment percent female and study quality score
Study quality and publication bias
Study quality was evaluated independently by MSand AP using a checklist adapted from Luppino ampWit (Luppino et al 2010) The checklist contained 12items and studies were rated with a lsquo+rsquo if it met criteriafor that item a lsquominusrsquo if it did not meet criteria for an itemand a rsquorsquo if unclear lsquo+rsquo were coded as a score of 1 andminus were coded as a score of 0 Total scores and percen-tages were calculated Articles with total scores of 0ndash3were considered to be of low quality scores of 4ndash7were considered a medium quality and scores of 8ndash12 were considered to be of high quality Any discrep-ancies (approximately 3 of data points) wereresolved via consensus
Publication bias was assessed using a funnel plotwhich presents study size on the vertical axis (as stand-ard error in this case) as a function of effect size on thex-axis When no publication bias exists the studiesshould be distributed symmetrically about the com-bined effect size (Borenstein et al 2011) If evidenceof publication bias was observed Duval amp Tweediersquostrim-and-fill method was used (Duval amp Tweedie2000) which recalculates effects based on imputingdata from studies that are likely to be missing Lastthe Fail-safe N was calculated (Cooper 1979) whichindicates the number of missing studies that wouldneed to exist to nullify the observed effect
Results
A flow diagram of the search process is shown inFig 1 The search identified 2773 records through
PubMed 2158 through EMBASE and 1345 throughPsycINFO for a total of 6276 records Duplicaterecords (1709) were removed in EndNote resulting in4567 unique records After title and abstracts werereviewed 329 records were identified as potentially eli-gible for the meta-analysis These 329 records werereviewed in full and 300 articles were excluded hier-archically if they were a review baseline or protocolpaper (n = 6) if the sample had a mean age over 65at the depression assessment (n = 41) if the samplehad a specific medical illness (n = 23) if the studywas not a longitudinal design (n = 19) if MDD diagno-sis hospitalization or admission to treatment centerwas part of the inclusion criteria of the study (n = 18)if cognitive function was assessed only concurrentlywith or after depression (n = 36) if cognitive functionwas assessed by educational achievement or self-report(n = 26) if cognitive function was assessed by attribu-tion style rather than neuropsychological measure (n= 7) if there was no measure of cognitive function (n= 18) or no uniquely measured depression outcome(n = 24) Furthermore if articles reported on the samesample as another article with higher quality or moreinformation the duplicate articles were excluded (n =8) Last a number of studies appeared to measureboth cognitive function and depression but did not re-port enough information to be included in the meta-analysis and did not respond to requests for additionalinformation (n = 74 approximately 59 unique samples)In total 29 publication were included in the meta-ana-lysis comprising 34 samples (one study included twoseparate birth cohorts and another four reported dataseparately for men and women)
Study characteristics
The characteristics of included samples are detailed inTable 1 Sample sizes ranged from 43 to 50 053 with amedian of 3395 The most common types of sampleswere school samples (934) community samples (834) and birth cohorts (734) The samples were major-ity white with two samples having exclusively blackparticipants Additionally eight samples were menonly six samples were women only and the restreported combined effect sizes Mean age of partici-pants at baseline ranged from 35 to 59 years with amedian of 12 years Most samples did not reportwhether comorbid diagnoses were present (2334)
Of the 74 papers excluded for having insufficient in-formation (representing 60 unique samples) the me-dian number of subjects was not statistically differentbetween those studies and the studies included in themeta-analysis (n = 288 and n = 3395 respectively p =019) nor did the average age of study participants atbaseline statistically differ (median across studies = 11
10 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
v 12 respectively p = 057) The types of cognitivemeasures used were also similar across the excludedand included studies with the most common measurebeing IQ (2860 and 2029) followed by VerbalComprehension (860 and 529)
Meta-analysis
The overall analysis yielded a significant associationbetween cognitive function and subsequent depressionoutcomes [r =minus0088 95 confidence interval (CI)minus0121 to minus0054 p lt 0001 Fig 2] Results were similarwhen excluding the two studies that used beta-weights(r =minus0071 95 CI minus0100 to minus0042 p lt 0001) orwhen using episodic memory in place of processingspeed in a study reporting both outcomes (r =minus008595 CI minus0118 to minus0051 p lt 0001) Follow-up ana-lyses were conducted in the sample of studies report-ing educational attainment and self-report outcomes(Supplementary Table S2) Heterogeneity across sam-ples was significant (Q = 80154 p lt 0001) suggestingsubstantial variation across the individual samplesThe ratio of the true heterogeneity to total variationwas large (I2 = 9588) I2 is on a relative scale andvalues close to 100 indicate that most of the observedvariance is real rather than spurious and suggeststhat subgroup analyses or meta-regression may helpto explain this variability (Borenstein et al 2011)
Subgroup analyses and meta-regression
A significant difference was found between categoricaland continuous effect sizes (p lt 0001) The studiesassessing continuous outcomes were found to have alarger effect (r =minus0121 95 CI minus0168 to minus0073 p lt0001 n = 22) than studies assessing categorical out-comes (r =minus0035 95 CI minus0054 to minus0017 p lt 0001n = 12) No differences were observed between studiesutilizing broad v specific cognitive measures (p = 057)
Outcomes were also compared adjusting for baselinedepression symptoms at the time of cognitive assess-ment Nine studies provided enough detail to calculatethe partial correlation coefficients adjusting for base-line depression symptoms Using the partial correl-ation coefficients led to a null result (r =minus0032 95CI minus0078 to 0014 p = 0169 n = 9 Fig 3) The nullresult does not seem to be due to a lack of power be-cause using the unadjusted correlation coefficients forthe same nine studies still led to a significant result(r =minus0120 95 CI minus0169 to minus0070 p lt 0001 n = 9Fig 3) As a follow-up the difference in effect sizes be-tween the adjusted and unadjusted values for these 9studies were tested (r = 0082 95 CI 0069ndash0095 p lt0001 n = 9) suggesting that the effects are significantlydifferent when directly comparing the values that doand do not control for baseline depression symptoms
Expanding the subgroup analyses to include studiesthat controlled for baseline depression plus other co-variates (Zammit et al 2004 Simons et al 2009 Rawalamp Rice 2012) and studies that explicitly excluded fora history of depression diagnosis (Gale et al 2008Vinberg et al 2013 Papmeyer et al 2015) did notchange the null result (r =minus0027 95 CI minus0058 to0005 p = 0097 n = 15)
None of the meta-regression analyses were signifi-cant indicating that the between-study variance wasnot attributable to age at baseline IQ percent of sam-ple that was female percent of the sample that waswhite age at follow-up time between assessmentsyear of cognitive assessment year of follow-up assess-ment or study quality score
Study quality and publication bias
Multiple samples within a study were combined forthe purposes of quality assessment given that studieswithin the same publication were found to employthe same methodology Of the 29 publications reviewed12 were rated as high quality and 17 were rated as me-dium quality Details are provided in SupplementaryTable S1 Comparable results to the overall findingswere obtained when just using high quality studies (r=minus0085 95 CI minus0141 to minus0029 p = 0003)
Inspection of the funnel plot (Fig 4) found no evi-dence for publication bias to support the hypothesisIn fact imputation of negative correlations suggestedthat additional studies favoring the hypothesis maybe missing While the calculated effect size is minus0088(95 CI minus0121 to minus0054) using Duval amp Tweediersquostrim-and-fill method the imputed effect size estimateis larger at minus0137 (95 CI minus0176 to minus0099 imputedstudies n = 11) Last the Fail-safe N procedure foundthat 3583 null studies would need to be located forthe combined two-tailed p value to exceed 005 Thissuggests that significant results are not likely to be con-founded by publication bias and may even underesti-mate true effect sizes
Discussion
The present systematic review and meta-analysis of 29longitudinal publications including 1 21 749 partici-pants revealed that after accounting for baseline depres-sion symptoms variability in cognitive function did notpredict subsequent depression Consistent with priorreports there was a significant contemporaneous associ-ation between higher depression symptoms and lowercognitive function These patterns have implications forunderstanding the association between cognitive func-tion and depression and may be important for advan-cing etiologic and treatment research
Association between cognitive function and subsequent depression 11
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
First our findings reinforce models positing thatcognitive function tracks with depression severity(McDermott amp Ebmeier 2009) One possible explan-ation for this contemporaneous association is that de-pression symptoms interfere with the capacity tocomplete cognitive assessments possibly through thegeneral lack of motivation that is one hallmark of thedisorder While this explanation represents an experi-mental confound for studies focused on assessmentof cognitive function it likewise represents an oppor-tunity for studies to focus more comprehensively onthe assessment of both depression and mood disordersymptoms since performance on cognitive tests maybe a sensitive measure of motivational state thatcould augment self-reported symptoms Alternativelythe co-occurrence of cognitive deficits and depressionsymptoms may reflect shared genetic etiology (Hagen-aars et al 2016) and dysfunction of neural circuits
supporting both cognitive and emotional processes(Scult et al 2016) In particular dysfunction of prefront-al and striatal circuits have been associated with bothdepression and cognitive function (Keedwell et al2005 Aarts et al 2011)
Second our findings suggest that prior studies oflinks between cognitive function and depression thatdid not assess baseline symptoms may have overesti-mated the potential protective role of higher cognitivefunction While the importance of accounting for sub-clinical symptoms is not novel the implementation ofsuch accounting is often neglected in psychiatric epi-demiology given the current categorical threshold-based diagnostic system In our meta-analysis largereffects were observed for continuous as compared tocategorical outcomes which aligns with growing em-phasis on dimensional measures of psychopathology(Cuthbert amp Kozak 2013)
Fig 2 Meta-analysis of the association between cognitive function and subsequent depression A forest plot for all studiesthat investigated associations between cognition and later depression Results are reported as correlation coefficients denotedby squares and 95 confidence intervals (CI) indicated by lines (effect sizes are converted to correlation coefficients ifreported as odds ratios) Meta-analysis results are displayed as the diamond The overall analysis found a significant effect ofcognition on depression (r =minus0088 95 CI minus0121 to minus0054 p lt 0001)
12 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Fig 4 Trim-and-fill funnel plots for all samples Fisherrsquos Z a measure of effect size is plotted on the x-axis and the standarderror is plotted on the y-axis Larger studies appear toward the top of the graph and smaller studies towards the bottom Inthe absence of publication bias the studies are symmetrically distributed around the mean Actual studies are shown in opencircles and imputed studies would be shown in black circles No additional studies would be expected in the oppositedirection (to the right) of the observed effect but an additional 11 studies are imputed to the left of the mean effect sizeWhile the calculated effect size is minus0088 [95 confidence interval (CI) minus0121 to minus0054] using Duval amp Tweediersquos trim-and-fill method the imputed effect size estimate is larger at minus0137 (95 CI minus0176 to minus0099 imputed studies n = 11)
Fig 3 Meta-analysis comparing values adjusted for baseline depression symptoms v unadjusted A forest plot for analysiscomparing results from a subset of the same set of studies reported in Fig 2 when using unadjusted values compared tousing values that are adjusted for baseline depression Effects are significant for unadjusted values [r =minus0120 95 confidenceinterval (CI) minus0169 to minus0070 p lt 0001] but not for adjusted values (r =minus0032 95 CI minus0078 to 0014 p = 0169) Results arereported as correlation coefficients denoted by squares and 95 CIs indicated by lines Meta-analysis results are displayed asdiamonds
Association between cognitive function and subsequent depression 13
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Third the associations between cognitive functionand either current or later depression were not moder-ated by data quality or participant age sex and raceHowever there are a number of additional potentialmoderators that could not be addressed in the currentreview and meta-analysis For example the numberand type of comorbid conditions with depressionwere often not reported in the included studies butcould represent an important moderator of theobserved effects Modeling the effects of comorbid ill-ness is an important avenue for future research
One limitation of the current literature is that only ahandful of studies reviewed explicitly excluded for de-pression diagnosis at baseline (Gale et al 2008 Vinberget al 2013 Papmeyer et al 2015) however consistentwith the finding that controlling for baseline depres-sion symptoms led to a null association between cogni-tion and subsequent depression there was no effectobserved when including these studies in the sub-group analyses further suggesting that the associationbetween cognitive function and depression is likelycontemporaneous It will be important to follow-upthese analyses with individual studies that includerigorous assessment of baseline depression symptomsand other potentially confounding factors to furtherclarify this relationship
An open question that remains for future research iswhether deficits in cognitive function are likely to pre-dict the development of more sever or recurrent de-pression later in life Only one of the included studies(Koenen et al 2009) specifically investigated recurrentdepression and found that lower IQ was associatedwith greater persistence of disorder
A final consideration is that while our review andmeta-analysis focused on general cognitive functionmainly assessed via IQ there may be specific subtypesof cognitive function that are more predictive of laterdepression For example a lack of cognitive flexibilitymay more closely match with the ruminative stylecharacteristic of depression and therefore tasks specifi-cally measuring this component of cognitive functionmight have some predictive utility While our reviewdid not find differences between broad and specificmeasures of cognitive function there were not enoughstudies identified to allow for precise consideration ofdifferences between individual cognitive domains
A limitation of the meta-analysis is that while thepresent study followed standard guidelines (Stroupet al 2000 Atkinson et al 2014) decisions aboutstudy selection data extraction and quality assess-ment include a number of decision points that neces-sarily involve a level of subjectivity Reliability wasascertained by using independent raters however dif-ferent inclusionexclusion criteria or a different ap-proach to the evaluation of those criteria could result
in a different set of studies being includedUltimately the quality of the meta-analysis is depend-ent upon the underlying studies that are analyzedFurthermore although studies with insufficient infor-mation to be included in the meta-analysis were notfound to differ based on basic study data from thosestudies included in the meta-analysis nonetheless itis unknown how if at all data from these studiescould change the overall results
Acknowledging these limitations our present reviewand meta-analysis found that while an association is evi-dent between cognitive function and later depressiongeneral cognitive function does not appear to be a riskfactor for depression but rather is more likely relatedto performance decrements associated with concurrentdepressive symptoms Our results suggest that low cog-nitive function is therefore probably not a causal factorof depression and that clinical practice may benefitmore from a focus on how decreased cognitive functionin the depressed state is likely to influence treatment out-comes (Gyurak et al 2015) Our findings have importantimplications for better understanding depression and forthe design of future studies in highlighting the need tocontrol for subthreshold depression symptoms when in-vestigating risk factors for mental illness as well as whenassessing cognitive function more generally
Supplementary material
The supplementary material for this article can befound at httpdxdoiorg101017S0033291716002075
Acknowledgements
MAS is supported by an National Science Foundation(NSF) Graduate Research Fellowship ARH is sup-ported by National Institutes of Health (NIH) grantsRO1DA033369 amp R01AG049789 TEM is supportedby National Institutes of Health (NIH) grantsR01AG049789 We would like to thank HarrisCooper PhD at Duke University who provided invalu-able insight into conducting the meta-analysis Wethank all of the authors of studies who provided add-itional information for this meta-analysis
Declaration of Interest
None
References
Aarts E van Holstein M Cools R (2011) Striatal dopamineand the interface between motivation and cognitionFrontiers in Psychology 2 163
14 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Atkinson KM Koenka AC Sanchez CE Moshontz HCooper H (2014) Reporting standards for literaturesearches and report inclusion criteria making researchsyntheses more transparent and easy to replicate ResearchSynthesis Methods 6 87ndash95
Baer LH Tabri N Blair M Bye D Li KZH Pushkar D(2013) Longitudinal associations of need for cognitioncognitive activity and depressive symptomatology withcognitive function in recent retirees Journals of GerontologySeries B Psychological Sciences and Social Sciences 68 655ndash664
Barbey AK Colom R Solomon J Krueger F Forbes CGrafman J (2012) An integrative architecture for generalintelligence and executive function revealed by lesionmapping Brain 135 1154ndash1164
Barnett JH Salmond CH Jones PB Sahakian BJ (2006)Cognitive reserve in neuropsychiatry Psychological Medicine36 1053ndash1064
Beaujean AA Parker S Qiu X (2013) The relationshipbetween cognitive ability and depression a longitudinaldata analysis Social Psychiatry and Psychiatric Epidemiology48 1983ndash1992
Belsky DW Caspi A Arseneault L Bleidorn W Fonagy PGoodman M Houts R Moffitt TE (2012) Etiologicalfeatures of borderline personality related characteristics in abirth cohort of 12-year-old children Development andPsychopathology 24 251ndash265
Betts KS Williams GM Najman JM Alati R (2016)Predicting spectrums of adult mania psychosis anddepression by prospectively ascertained childhoodneurodevelopment Journal of Psychiatric Research 72 22ndash29
Bora E Harrison BJ Yuumlcel M Pantelis C (2013) Cognitiveimpairment in euthymic major depressive disorder a meta-analysis Psychological Medicine 43 2017ndash2026
Borenstein M Hedges LV Higgins JPT Rothstein HR(2011) Introduction to Meta-Analysis John Wiley amp SonsWest Sussex UK
Canals J Domegravenech-Llaberia E Fernaacutendez-Ballart J Martiacute-Henneberg C (2002) Predictors of depression at eighteenA 7-year follow-up study in a Spanish nonclinicalpopulation European Child amp Adolescent Psychiatry 11226ndash233
Christensen H Griffiths K Mackinnon A (1997) Aquantitative review of cognitive deficits in depression andAlzheimer-type dementia Selection of Studies 3 631ndash651
Connolly SL Wagner Ca Shapero BG Pendergast LLAbramson LY Alloy LB (2014) Rumination prospectivelypredicts executive functioning impairments in adolescentsJournal of Behavior Therapy and Experimental Psychiatry 4546ndash56
Cooper HM (1979) Statistically combining independentstudies a meta-analysis of sex differences in conformityresearch Journal of Personality and Social Psychology 37131ndash146
Cooper HM (2010) Research Synthesis and Meta-Analysis AStep-by-Step Approach 4th edn SAGE PublicationsWashington (DC) USA
Cuijpers P de Graaf R van Dorsselaer S (2004) Minordepression risk profiles functional disability health careuse and risk of developing major depression Journal ofAffective Disorders 79 71ndash79
Cuthbert BN Kozak MJ (2013) Constructing constructs forpsychopathology the NIMH research domain criteriaJournal of Abnormal Psychology 122 928ndash937
Der G Batty GD Deary IJ (2009) The association between IQin adolescence and a range of health outcomes at 40 in the1979 US National Longitudinal Study of Youth Intelligence37 573ndash580
Dubow EF Boxer P Huesmann LR (2008) Childhood andadolescent predictors of early and middle adulthoodalcohol use and problem drinking the Columbia CountyLongitudinal Study Addiction 103 36ndash47
Duval S Tweedie R (2000) Trim and fill a simple funnel-plot-based method of testing and adjusting for publicationbias in meta-analysis Biometrics 56 455ndash463
Evans LD Kouros CD Samanez-Larkin S Garber J (2015)Concurrent and short-term prospective relations amongneurocognitive functioning coping and depressivesymptoms in youth Journal of Clinical Child and AdolescentPsychology 53 1ndash15
Franz CE Lyons MJ OrsquoBrien R Panizzon MS Kim K BhatR Grant MD Toomey R Eisen S Xian H Kremen WS(2011) A 35-year longitudinal assessment of cognition andmidlife depression symptoms the Vietnam Era Twin Studyof Aging American Association for Geriatric PsychiatryAmerican Journal of Geriatric Psychiatry 19 559ndash570
Gale CR Batty GD Tynelius P Deary IJ Rasmussen F(2010) Intelligence in early adulthood and subsequenthospitalization for mental disorders Epidemiology 2170ndash77
Gale CR Deary IJ Boyle SH Barefoot J Mortensen LHBatty GD (2008) Cognitive ability in early adulthood andrisk of 5 specific psychiatric disorders in middle age theVietnam experience study Archives of General Psychiatry 651410ndash1418
Gale CR Hatch SL Batty GD Deary IJ (2009) Intelligence inchildhood and risk of psychological distress in adulthoodthe 1958 National Child Development Survey and the 1970British Cohort Study Intelligence 37 592ndash599
Gjerde PF (1995) Alternative pathways to chronicdepressive symptoms in young adults gender differencesin developmental trajectories Child Development 661277ndash1300
Gottfredson LS (1997) Mainstream science on intelligence aneditorial with 52 signatories history and bibliographyIntelligence 24 13ndash23
Guyer AE Choate VR Grimm KJ Pine DS Keenan K(2011) Emerging depression is associated with facememory deficits in adolescent girls Elsevier Inc Journal ofthe American Academy of Child and Adolescent Psychiatry 50180ndash190
Gyurak A Patenaude B Korgaonkar MS Grieve SMWilliams LM Etkin A (2015) Frontoparietal activationduring response inhibition predicts remission toantidepressants in patients with major depression BiologicalPsychiatry 79 1ndash8
Hagenaars SP Harris SE Davies G Hill WD LiewaldDCM Ritchie SJ Marioni RE Fawns-Ritchie C Cullen BMalik R METASTROKE Consortium IC for BPGSpiroMeta Consortium CHARGE ConsortiumPulmonary Group CCA and LG Worrall BB Sudlow
Association between cognitive function and subsequent depression 15
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
CLM Wardlaw JM Gallacher J Pell J McIntosh AMSmith DJ Gale CR Deary IJ (2016) Shared geneticaetiology between cognitive functions and physical andmental health in UK Biobank (N = 112 151) and 24 GWASconsortiaMolecular Psychiatry Published online 26 January2016 doi101038mp2015225
Hatch SL Jones PB Kuh D Hardy R Wadsworth MEJRichards M (2007) Childhood cognitive ability and adultmental health in the British 1946 birth cohort Social Scienceamp Medicine (1982) 64 2285ndash2296
Hipwell AE Sapotichne B Klostermann S Battista DKeenan K (2011) Autobiographical memory as a predictorof depression vulnerability in girls Journal of Clinical Childand Adolescent Psychology 40 254ndash265
Horowitz JL Garber J (2003) Relation of intelligence andreligiosity to depressive disorders in offspring of depressedand nondepressed mothers The American Academy ofChild and Adolescent Psychiatry Journal of the AmericanAcademy of Child and Adolescent Psychiatry 42 578ndash586
Johnson W Bouchard TJ Krueger RF McGue MGottesman II (2004) Just one g consistent results fromthree test batteries Intelligence 32 95ndash107
Keedwell PA Andrew C Williams SCR Brammer MJPhillips ML (2005) The neural correlates of anhedoniain major depressive disorder Biological Psychiatry 58843ndash853
Kessler RC Berglund P Demler O Jin R Koretz DMerikangas KR Rush AJ Walters EE Wang PS (2003)The epidemiology of major depressive disorder resultsfrom the National Comorbidity Survey Replication(NCS-R) Journal of the American Medical Association 2893095ndash3105
Koenen KC Moffitt TE Roberts AL Martin LT KubzanskyL Harrington H Poulton R Caspi A (2009) Childhood IQand adult mental disorders a test of the cognitive reservehypothesis American Journal of Psychiatry 166 50ndash57
Lewinsohn PM Solomon A Seeley JR Zeiss A (2000)Clinical implications of lsquosubthresholdrsquo depressivesymptoms Journal of Abnormal Psychology 109 345ndash351
Luppino FS de Wit LM Bouvy PF Stijnen T Cuijpers PPenninx BWJH Zitman FG (2010) Overweight obesityand depression a systematic review and meta-analysisof longitudinal studies Archives of General Psychiatry 67220ndash229
McCord J Ensminger ME (1997) Multiple risks andcomorbidity in an African-American population CriminalBehaviour and Mental Health 7 339ndash352
McDermott LM Ebmeier KP (2009) A meta-analysis ofdepression severity and cognitive function Elsevier BVJournal of Affective Disorders 119 1ndash8
Melartin TK Rytsaumllauml HJ Leskelauml US Lestelauml-Mielonen PSSokero TP Isometsauml ET (2002) Current comorbidity ofpsychiatric disorders among DSM-IV major depressivedisorder patients in psychiatric care in the VantaaDepression Study Journal of Clinical Psychiatry 63 126ndash134
Meyer SE Carlson GA Wiggs EA Martinez PE RonsavilleDS KlimesndashDougan B Gold PW RadkendashYarrow M(2004) A prospective study of the association amongimpaired executive functioning childhood attentional
problems and the development of bipolar disorderDevelopment and Psychopathology 16 461ndash476
MiyakeA FriedmanNP EmersonMJWitzki aHHowerter AWager TD (2000) The unity and diversity of executivefunctions and their contributions to complex lsquoFrontal Lobersquotasks a latentvariable analysisCognitive Psychology41 49ndash100
Moher D Liberati A (2009) Preferred reporting items forsystematic reviews and meta-analyses the PRISMAstatement Annals of Internal Medicine 151 264ndash269
Papmeyer M Sussmann JE Hall J McKirdy J Peel AMacdonald A Lawrie SM Whalley HC McIntosh AM(2015) Neurocognition in individuals at high familial riskof mood disorders with or without subsequent onset ofdepression Psychological Medicine 45 1ndash11
Peterson RA Brown SP (2005) On the use of betacoefficients in meta-analysis Journal of Applied Psychology90 175ndash181
Pine DS Cohen P Brook J Coplan JD (1997) Psychiatricsymptoms in adolescence as predictors of obesity in earlyadulthood a longitudinal study American Journal of PublicHealth 87 1303ndash1310
Quinn ME Joormann J (2015) Control when it countschange in executive control under stress predicts depressionsymptoms Emotion Junio 22 1ndash10
Rawal A Rice F (2012) Examining overgeneralautobiographical memory as a risk factor for adolescentdepression Elsevier Inc Journal of the American Academy ofChild and Adolescent Psychiatry 51 518ndash527
Ree MJ Earles JA (1991) The stability of g across differentmethods of estimation Intelligence 15 271ndash278
Rock PL Roiser JP Riedel WJ Blackwell AD (2014)Cognitive impairment in depression a systematic reviewand meta-analysis Psychological Medicine 44 2029ndash2040
Rogers MA Kasai K Koji M Fukuda R Iwanami ANakagome K Fukuda M Kato N (2004) Executive andprefrontal dysfunction in unipolar depression a review ofneuropsychological and imaging evidence NeuroscienceResearch 50 1ndash11
Scult MA Knodt AR Swartz JR Brigidi BD Hariri AR(2016) Thinking and feeling individual differences inhabitual emotion regulation and stress-related mood areassociated with prefrontal executive control ClinicalPsychological Science doi1011772167702616654688
Sharp C Petersen N Goodyer I (2008) Emotional reactivityand the emergence of conduct problems and emotionalsymptoms in 7- to 11-year-olds a 1-year follow-up studyJournal of the American Academy of Child and AdolescentPsychiatry 47 565ndash573
Siegel LS (1999) Issues in the definition and diagnosis oflearning disabilities a perspective on Guckenberger vBoston University Journal of Learning Disabilities 32 304ndash319
Simons CJP Jacobs N Derom C Thiery E Jolles J van Os JKrabbendam L (2009) Cognition as predictor of currentand follow-up depressive symptoms in the generalpopulation Acta Psychiatrica Scandinavica 120 45ndash52
Slykerman RF Thompson J Waldie K Murphy R Wall CMitchell EA (2015) Maternal stress during pregnancy isassociated with moderate to severe depression in 11-year-old children Acta Paediatrica 104 68ndash74
16 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Snyder HR (2013) Major depressive disorder is associatedwith broad impairments on neuropsychological measuresof executive function a meta-analysis and reviewPsychological Bulletin 139 81ndash132
Soslashrensen HJ Saeligbye D Urfer-Parnas A Mortensen ELParnas J (2012) Premorbid intelligence and educationallevel in bipolar and unipolar disorders a Danish draftboard study Journal of Affective Disorders 136 1188ndash1191
SpearmanC (1904) lsquoGeneral intelligencersquoobjectivelydeterminedandmeasuredAmerican Journal of Psychology 15 201
Stern Y (2003) The concept of cognitive reserve a catalyst forresearch Journal of Clinical and Experimental Neuropsychology(Neuropsychology Development and Cognition Section A) 25589ndash593
Stroup D Berlin J Morton S Olkin I Williamson GDRennie D Moher D Becker BJ Sipe TA Thacker SB(2000) Meta-analysis of Observational Studies inEpidemiology a proposal for reporting Journal of theAmerican Medical Association 283 2008
Vinberg M Miskowiak KW Kessing LV (2013) Impairmentof executive function and attention predicts onset ofaffective disorder in healthy high-risk twins Journal ofClinical Psychiatry 74 e747ndashe753
Zammit S Allebeck P David AS Dalman C HemmingssonT Lundberg I Lewis G (2004) A longitudinal study ofpremorbid IQ Score and risk of developing schizophreniabipolar disorder severe depression and other nonaffectivepsychoses Archives of General Psychiatry 61 354ndash360
Association between cognitive function and subsequent depression 17
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
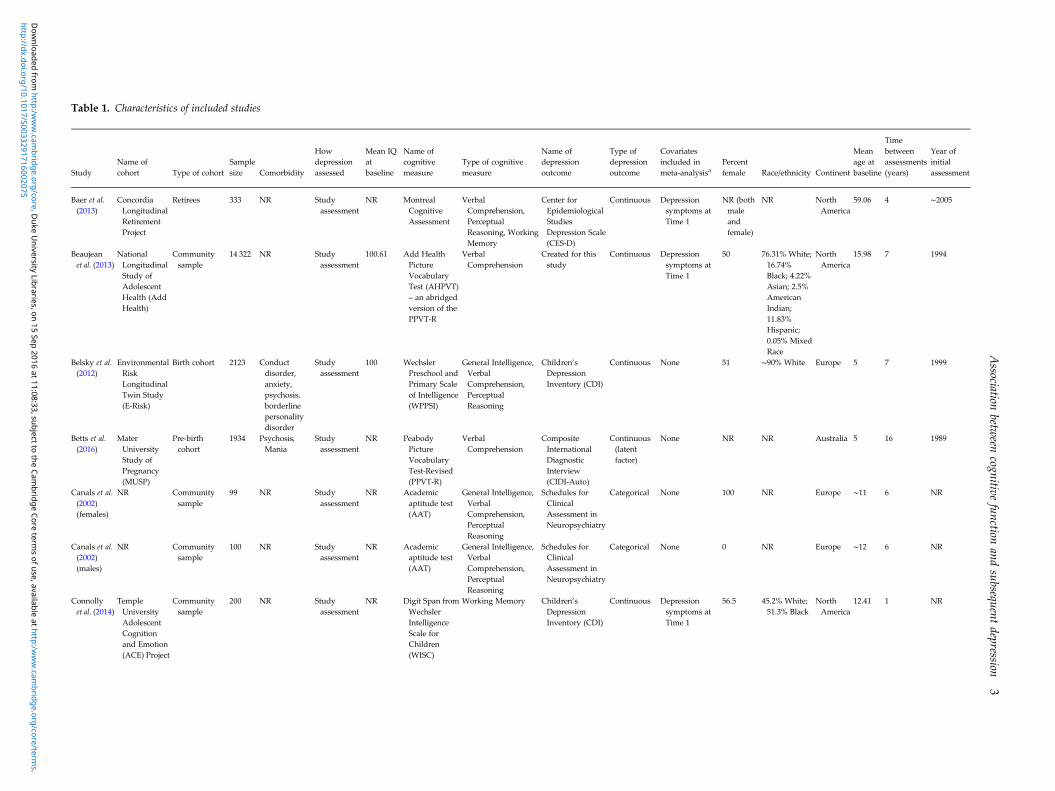
Table 1 Characteristics of included studies
StudyName ofcohort Type of cohort
Samplesize Comorbidity
Howdepressionassessed
Mean IQatbaseline
Name ofcognitivemeasure
Type of cognitivemeasure
Name ofdepressionoutcome
Type ofdepressionoutcome
Covariatesincluded inmeta-analysisa
Percentfemale Raceethnicity Continent
Meanage atbaseline
Timebetweenassessments(years)
Year ofinitialassessment
Baer et al(2013)
ConcordiaLongitudinalRetirementProject
Retirees 333 NR Studyassessment
NR MontrealCognitiveAssessment
VerbalComprehensionPerceptualReasoning WorkingMemory
Center forEpidemiologicalStudiesDepression Scale(CES-D)
Continuous Depressionsymptoms atTime 1
NR (bothmaleandfemale)
NR NorthAmerica
5906 4 sim2005
Beaujeanet al (2013)
NationalLongitudinalStudy ofAdolescentHealth (AddHealth)
Communitysample
14 322 NR Studyassessment
10061 Add HealthPictureVocabularyTest (AHPVT)ndash an abridgedversion of thePPVT-R
VerbalComprehension
Created for thisstudy
Continuous Depressionsymptoms atTime 1
50 7631 White1674Black 422Asian 25AmericanIndian1183Hispanic005 MixedRace
NorthAmerica
1598 7 1994
Belsky et al(2012)
EnvironmentalRiskLongitudinalTwin Study(E-Risk)
Birth cohort 2123 Conductdisorderanxietypsychosisborderlinepersonalitydisorder
Studyassessment
100 WechslerPreschool andPrimary Scaleof Intelligence(WPPSI)
General IntelligenceVerbalComprehensionPerceptualReasoning
ChildrenrsquosDepressionInventory (CDI)
Continuous None 51 sim90 White Europe 5 7 1999
Betts et al(2016)
MaterUniversityStudy ofPregnancy(MUSP)
Pre-birthcohort
1934 PsychosisMania
Studyassessment
NR PeabodyPictureVocabularyTest-Revised(PPVT-R)
VerbalComprehension
CompositeInternationalDiagnosticInterview(CIDI-Auto)
Continuous(latentfactor)
None NR NR Australia 5 16 1989
Canals et al(2002)(females)
NR Communitysample
99 NR Studyassessment
NR Academicaptitude test(AAT)
General IntelligenceVerbalComprehensionPerceptualReasoning
Schedules forClinicalAssessment inNeuropsychiatry
Categorical None 100 NR Europe sim11 6 NR
Canals et al(2002)(males)
NR Communitysample
100 NR Studyassessment
NR Academicaptitude test(AAT)
General IntelligenceVerbalComprehensionPerceptualReasoning
Schedules forClinicalAssessment inNeuropsychiatry
Categorical None 0 NR Europe sim12 6 NR
Connollyet al (2014)
TempleUniversityAdolescentCognitionand Emotion(ACE) Project
Communitysample
200 NR Studyassessment
NR Digit Span fromWechslerIntelligenceScale forChildren(WISC)
Working Memory ChildrenrsquosDepressionInventory (CDI)
Continuous Depressionsymptoms atTime 1
565 452 White513 Black
NorthAmerica
1241 1 NR
Association
between
cognitivefunction
andsubsequent
depression3
httpdxdoiorg101017S0033291716002075D
ownloaded from
httpww
wcam
bridgeorgcore Duke U
niversity Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core term
s of use available at httpww
wcam
bridgeorgcoreterms
Table 1 (cont)
StudyName ofcohort Type of cohort
Samplesize Comorbidity
Howdepressionassessed
Mean IQatbaseline
Name ofcognitivemeasure
Type of cognitivemeasure
Name ofdepressionoutcome
Type ofdepressionoutcome
Covariatesincluded inmeta-analysisa
Percentfemale Raceethnicity Continent
Meanage atbaseline
Timebetweenassessments(years)
Year ofinitialassessment
Der et al(2009)
US NationalLongitudinalSurvey ofYouth 1979
Communitysample
7458 Noted a rangeof healthconditions
Studyassessment
NR Armed ServicesVocationalAptitudeBattery(ASVAB)Armed ForcesQualificationTest (AFQT)
General IntelligenceVerbalComprehension
Center forEpidemiologicalStudiesDepression Scale(CES-D)
Continuous Depressionsymptoms atTime 1
52 31 Black19Hispanic
NorthAmerica
179 sim22 1979
Dubow et al(2008)(females)
ColumbiaCountyLongitudinalStudy(CCLS)
SchoolChildrenGrade 3
215 NR Studyassessment
sim104 CaliforniaShort-FormTest of MentalMaturity
General Intellignce MinnesotaMultiphasicPersonalityInventory(MMPI) Scale 2
Continuous None 100 90 White3 Blacklt1Asianlt1Hispanic
NorthAmerica
8 11 1960
Dubow et al(2008)(males)
ColumbiaCountyLongitudinalStudy(CCLS)
SchoolChildrenGrade 3
211 NR Studyassessment
sim104 CaliforniaShort-FormTest of MentalMaturity
General Intelligence MinnesotaMultiphasicPersonalityInventory(MMPI) Scale 2
Continuous None 0 90 White3 Blacklt1Asianlt1Hispanic
NorthAmerica
8 11 1960
Evans et al(2015)
NR SchoolChildrenGrades 5ndash9
192 Some withADHD
Studyassessment
111 WechslerAbbreviatedScale ofIntelligence(WASI)
General IntelligenceVerbalComprehensionPerceptualReasoning WorkingMemorySet-Shifting
ChildrenrsquosDepressionInventory (CDI)
Continuous Depressionsymptoms atTime 1
521 714 White182 Black26 Asian36Hispanic42 MixedRace
NorthAmerica
1236 03 sim2000s
Franz et al(2011)
Vietnam EraTwin Studyof Aging
Military cohort 1231 NR Studyassessment
NR Armed ForcesQualificationTest (AFQTForm 7A)
General IntelligencePerceptualReasoning WorkingMemory ProcessingSpeed Set-ShiftingInhibition
Center forEpidemiologicalStudiesDepression Scale(CES-D)
Continuous None 0 86 White NorthAmerica
20 35 sim1970
Gale et al(2008)
VietnamExperienceStudy (VES)
Military cohort 3258 Mix Studyassessment
100 Generaltechnicalsection of theArmyClassificationBattery
General IntelligenceVerbalComprehensionArithmeticreasoning
DiagnosticInterviewSchedule (DIS)
Categorical SocioeconomicStatusEthnicity Placeof service
0 808 White127 Black
NorthAmerica
204 sim17 sim1964
Gale et al(2009)(1958Cohort)
1958 NationalChildDevelopmentSurvey
Birth cohort 6369 NR Studyassessment
1028 General abilitytest devisedby theNationalFoundationforEducationalResearch inEngland andWales
General Intelligence Rutterrsquos MalaiseInventory
Continuous None NR (bothmaleandfemale)
NR Europe 11 22 1969
4MA
Scultet
al
httpdxdoiorg101017S0033291716002075D
ownloaded from
httpww
wcam
bridgeorgcore Duke U
niversity Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core term
s of use available at httpww
wcam
bridgeorgcoreterms
Gale et al(2009)(1970Cohort)
1970 BritishCohort Study
Birth cohort 6074 NR Studyassessment
1018 British abilityScale
General Intelligence Rutterrsquos MalaiseInventory
Continuous None NR (bothmaleandfemale)
NR Europe 10 20 1980
Gjerde(1995)(females)
NR Recruited froma nurseryschool
51 NR Studyassessment
1187 Wechsler AdultIntelligenceScale (WAIS)
General Intelligence General BehaviorInventory (GBI)Depression scale
Continuous None 100 sim66 Whitesim25Blacksim005Asian
NorthAmerica
18 5 1983
Gjerde et al(1995)(males)
NR Recruited froma nurseryschool
45 NR Studyassessment
11112 Wechsler AdultIntelligenceScale (WAIS)
General Intelligence General BehaviorInventory (GBI)Depression scale
Continuous None 0 sim66 Whitesim25 Blacksim005Asian
NorthAmerica
18 5 1983
Hatch et al(2007)
1946 BritishCohort Study
Birth cohort 957 NR Studyassessment
NR NationalFoundationforEducationalResearch Test
General IntelligenceVerbalComprehensionPerceptualReasoning
General HealthQuestionnaire(GHQ-28)-severedepressionsubscale
Continuous None 51 NR Europe 8 45 1954
Hipwellet al (2011)
PittsburghGirls Study(PGS)
Communitysample
195 NR Studyassessment
9954 WechslerIntelligenceScale forChildren(WISC) III-R
VerbalComprehension
Schedule forAffectiveDisorders forSchool-AgeChildren-Present andLifetime Version(K-SADS-PL)
Continuous Depressionsymptoms atTime 1
100 70 Black ormultiracial
NorthAmerica
1154 1 1998
Horowitz ampGarber(2003)
NR Elementaryschool cohort
196 NR Studyassessment
10461 WechslerIntelligenceScale forChildren(WISC) -R
General IntelligenceVerbalComprehensionPerceptualReasoning
Schedule forAffectiveDisorders forSchool-AgeChildren-EpidemiologicalVersion(K-SADS-E)
Categorical Depressionsymptoms atTime 1
542 89 White147 Black33 Other
NorthAmerica
1186 6 sim1980
Koenenet al (2009)
DunedinCohort
Birth cohort 730 None Studyassessment
NR WechslerIntelligenceScale forChildren(WISC)
General IntelligenceVerbalComprehensionPerceptualReasoning WorkingMemory ProcessingSpeed
DiagnosticInterviewAssessment (forDSM-IV)
Categorical SexSocioeconomicStatusPhysicalHealthchildhoodmaltreatment
48 lsquoPrimarilyWhitersquo
NewZealand
9 23 1981
McCord ampEnsminger(1997)(females)
WoodlawnCohort
Elementaryschool cohort
346 Some withalcoholism
Studyassessment
NR (13 Unspecified IQof sample had scoresover 110)
General Intelligence CompositeInternationalInterviewSchedule(according toDSM-III-R)
Categorical None 100 100 Black NorthAmerica
sim6 27 1966
McCord ampEnsminger(1997)(males)
WoodlawnCohort
Elementaryschool cohort
313 Some withalcoholism
Studyassessment
NR (11 Unspecified IQof sample had scoresover 110)
General Intelligence CompositeInternationalInterviewSchedule(according toDSM-III-R)
Categorical None 0 100 Black NorthAmerica
sim6 27 1966
Meyer et al(2004)
NR Risk sample 86 NR Studyassessment
sim118 WISC General IntelligenceVerbalComprehensionPerceptualReasoning
SCID Categorical None 63 90 White9 Black 1Hispanic
NorthAmerica
11 13 1989
Association
between
cognitivefunction
andsubsequent
depression5
httpdxdoiorg101017S0033291716002075D
ownloaded from
httpww
wcam
bridgeorgcore Duke U
niversity Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core term
s of use available at httpww
wcam
bridgeorgcoreterms
Table 1 (cont)
StudyName ofcohort Type of cohort
Samplesize Comorbidity
Howdepressionassessed
Mean IQatbaseline
Name ofcognitivemeasure
Type of cognitivemeasure
Name ofdepressionoutcome
Type ofdepressionoutcome
Covariatesincluded inmeta-analysisa
Percentfemale Raceethnicity Continent
Meanage atbaseline
Timebetweenassessments(years)
Year ofinitialassessment
Papmeyeret al (2015)
ScottishBipolarFamily Study
Risk sample 111 NR Studyassessment
Controls108Patients107
National AdultReading Test(NART)
VerbalComprehension
Structured ClinicalInterview forDSM Disorders(SCID)symptoms
Categorical None 52 NR Europe 21 2 NR
Pine et al(1997)
NR Communitysample
644 NR Studyassessment
1007 UnspecifiedlsquoIQrsquo
General Intelligence Based onDiagnosticInterviewSchedule forChildren
Continuous Depressionsymptoms atTime 1
52 91 White NorthAmerica
138 9 1983
Quinn ampJoormann(2015)
NR Undergraduatestudents
43 NR Studyassessment
NR n-back Working Memory Beck DepressionInventory II(BDI-II)
Continuous Depressionsymptoms atTime 1
63 58 White30Hispanic orLatino 19Asian 2AfricanAmerican2AmericanIndian 2NativeHawaiian2 Indian
NorthAmerica
19 014 NR
Rawal ampRice (2012)
EarlyPrediction ofAdolescentDepressionstudy
Risk sample 230 None Studyassessment
9746 WechslerIntelligenceScale forChildren(WISC)
General IntelligenceVerbalComprehensionPerceptualReasoning WorkingMemory ProcessingSpeed
Child andAdolescentPsychiatricAssessment(CAPA)
Both Depressionsymptoms atTime 1 AgeOvergeneralityto negativecues
596 NR Europe 1371 1 NR
Sharp et al(2008)
The ChildBehaviourStudy
Communitysample
439 NR Studyassessment
105 WechslerIntelligenceScale forChildren(WISC)
General IntelligenceVerbalComprehensionPerceptualReasoning
The Mood andFeelingsQuestionnaire
Continuous Depressionsymptoms atTime 1
52 97 White05 Black25 Asian
Europe 94 1 NR
Simons et al(2009)
East FlandersProspectiveTwin Survey
Twin registry 444 NR Studyassessment
NR Principalcomponentfrom StroopConceptShifting Testand LetterDigitSubstitutionTest
Processing SpeedSet-ShiftingInhibition
Structured ClinicalInterview forDSM Disorders(SCID)symptoms
Continuous Depressionsymptoms atTime 1
100 NR Europe 28 2 NR
6MA
Scultet
al
httpdxdoiorg101017S0033291716002075D
ownloaded from
httpww
wcam
bridgeorgcore Duke U
niversity Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core term
s of use available at httpww
wcam
bridgeorgcoreterms
Slykermanet al (2015)
AucklandBirthweightCollaborativeStudy
Birth cohortrisk sample
609 NR Studyassessment
NR Stanford-BinetIntelligenceScale 4th Ed
General IntelligenceFluid ReasoningKnowledgeQunatitativeReasoningVisual-SpatialProcessingWorking Memory
Center forEpidemiologicalStudiesDepression Scale(CES-D)
Categorical(cut-point)
None 49 NR NewZealand
35 75 sim2000
Soslashrensenet al (2012)
DanishDraft-BoardStudy
Military cohort 21 914 NR Psychiatricregistry
Controls100Patients96ndash98
Boslashrge PriensProslashve (BPP)
General IntelligenceVerbalComprehensionPerceptualReasoning
DanishInternationalClassification ofdiseases (ICD) 8amp 10
Categorical None 0 NR Europe 195 sim36 1968ndash1989
Vinberget al (2013)
NR High-risktwins
224 Bipolardisorderanxietysubstanceabuse other
Studyassessmentpsychiatricregistry
NR CambridgeCognitiveAssessment(CAMCOG)
GeneralNeuropsychologicalFunctionOrientationLanugage MemoryAttention AbstractThinking VisualPerception
Beck DepressionInventory (BDI)
Continuous Depressionsymptoms atTime 1
65 NR Europe 439 7 2003
Zammitet al (2004)
SwedishConscripts(1969ndash1970)
Military cohort 50 053 None Hospitallinkage
NR UnspecifiedlsquoIQrsquo
General IntelligenceVerbalComprehensionPerceptualReasoning GeneralKnowledgeMechanicalKnowledge
InternationalClassification ofdiseases (ICD)hospitalpsychiatricadmissions
Categorical Diagnosis atbaselinedisturbedbehavior druguse raised in acity
0 NR Europe sim19 27 1969
Sample size is the number of subjects included in reported analyses of interest NR not reportedsim indicates only a range was reporteda This column notes covariates included in the meta-analysis We focused on controlling for depressive symptoms at T1 but some studies reported effect sizes that also included controlling
for other variables ndash when the zero-order correlations were unavailable these estimates were used
Association
between
cognitivefunction
andsubsequent
depression7
httpdxdoiorg101017S0033291716002075D
ownloaded from
httpww
wcam
bridgeorgcore Duke U
niversity Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core term
s of use available at httpww
wcam
bridgeorgcoreterms
to investigate general information processing abilitiesrather than cognitive attributional style studies withcognitive attribution measures as the sole cognitivemeasure were excluded
Comparisons
Search terms used to indicate the possible associationbetween cognitive function and depression includedrisk premorbid prodromal onset predict and association(for a full list see search terms in the SupplementaryMaterial) When data were reported from multipletime-points the analysis accounting for the longesttime between assessments was used
Outcomes
Eligible studies reported depression diagnosis orsymptoms determined by investigator or self-reportPresence of comorbidity was permitted given that de-pression has been found to be highly comorbid withother disorders (Melartin et al 2002 Kessler et al2003) Articles not adequately specifying how depres-sion was assessed or articles that did not uniquelymeasure depression [ie only had an index of lsquomentaldisordersrsquo or the category of lsquomood disordersrsquo lumpedtogether (Gale et al 2010)] were excluded if no uniquemeasure of depression could be obtained from studyauthors This is because although comorbidity waspermitted these could have represented instances ofpure anxiety disorders with few or no depressivesymptoms or instances of bipolar disorder
Study design
Eligible study search terms included cohort studies lon-gitudinal epidemiological prospective retrospective follow-up or case-control studies Studies not following a longi-tudinal design were excluded during full-text reviewAdditionally studies where cognitive function wasassessed only concurrently with or after depressionwere excluded given that the purpose of the reviewwas to investigate whether cognitive function pre-dicted later depression
Studies were included regardless of whether theywere reported in peer-review journals in order to ac-count for potentially biased reporting of resultsReview articles were included in the search terms tofind additional relevant references but were notincluded in the meta-analysis Baseline and protocolstudies without follow-up data were excluded
Study selection
A flow diagram of the process of study selection showsthe overall procedures (Fig 1) Records identified fromthe search processes were combined in EndNote
software version X7 and duplicates were removedTitles and abstracts were reviewed independently bytwo reviewers (MS and AP) according to the eligibil-ity criteria described above and marked as either po-tentially eligible or not eligible If either authormarked an article as potentially eligible it wasincluded in the full-text review for closer examinationby MS and AP who used an electronic form to indi-cate if an article should be included or excluded in thefinal selection When an article was excluded the rea-son for exclusion was selected from a hierarchical listof exclusion criteria presented in Fig 1 Both MSand AP were initially blinded to the otherrsquos decisionsAfter both MS and AP completed their reviews dis-crepancies about whether a study should be includedor excluded were resolved via discussion and consen-sus amongst MS AP TM AH and TS
Data extraction
Study information was extracted independently byMS and AP using an electronic form created forthis study Information was collected and codedbased on report characteristics participant characteris-tics study setting predictors outcome measures andquality assessment (Cooper 2010) Any discrepancies(approximately 3 of data points) were resolved viaconsensus
For studies with categorical depression diagnoses ef-fect sizes were generally presented as odds ratios Forthese studies the odds ratio plus the upper and lowerbound of the confidence interval were recorded Twoof the studies (Zammit et al 2004 Gale et al 2008)reported odds ratios greater than one to indicate thatlower IQ was associated with greater risk of depressionThe other studies reported odds ratios in the reverseleading to odds ratios less than one for the same direc-tion of the effect Therefore the odds ratios from the firsttwo studies were recalculated by dividing (1oddsratio) Another study (McCord amp Ensminger 1997)reported results from chi-squared tests Additional stud-ies reported mean premorbid IQ scores rather than oddsratios in which case the means sample sizes andor pvalues and number of tails of the t test were utilizedto calculate the effect size
For studies in which depression was measured as acontinuous variable effect sizes were presented as cor-relation coefficients The direction of the effect (posi-tive or negative) and the sample size were alsoextracted to be used in the meta-analysis Two studiesreported only beta weights (Simons et al 2009 Rawalamp Rice 2012) and we were not able to obtain zero-order correlations from the authors Given that previ-ous reports have suggested that beta weights can beused as an estimate of correlation coefficients in
8 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
meta-analysis (Peterson amp Brown 2005) the betaweights were used instead and analyses were runboth including and excluding these data points
When insufficient information was presented in thearticle authors were contacted requesting further de-tail An additional six studies were included at thispoint One study (Hatch et al 2007) included effectsizes for the female half of the cohort and did not pro-vide statistics for the males but did indicate a null ef-fect Only women from this study were included in themeta-analyses but imputing a score of 0 for the malesyielded similar overall results
Follow-up analyses directly compared studies thatreported zero-order correlations between IQ at time
1 depression at time 1 and depression at time 2(additional details described in the SupplementaryMethods)
Statistical methods
Data were analyzed using Comprehensive Meta-Analysis software version 30 (Biostat Inc USA) Arandom-effects model was used for expected hetero-geneity across studies A random-effects model alsoallows for broader generalization of results to thepopulation at large Heterogeneity of effects was calcu-lated using the Q statistic where a significant p valueindicates that true effect varies across studies The I2
Fig 1 Flow diagram of the search process
Association between cognitive function and subsequent depression 9
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
statistic was used to calculate the ratio of the true het-erogeneity to total variation acting as an index of sig-nal-to-noise ratio When I2 is large it is has beenrecommended to consider subgroup analysis or meta-regression to account for the variance (Borensteinet al 2011)
Subgroup analyses were conducted using a mixed-effects analysis in which a random effects model wasused to combine studies within each subgroup and afixed effect model was used to combine subgroupsand yield the overall effect (the study-to-study vari-ance is not assumed to be the same for all subgroups)Subgroup analyses were conducted comparing type ofoutcome (continuous v categorical) broad v specificcognitive measures and outcomes that were adjustedv unadjusted for baseline depression symptoms
Meta-regression was performed using the followingvariables on unadjusted analyses age at baseline ageat follow-up time between assessments IQ percentwhite year of cognitive assessment year of follow-upassessment percent female and study quality score
Study quality and publication bias
Study quality was evaluated independently by MSand AP using a checklist adapted from Luppino ampWit (Luppino et al 2010) The checklist contained 12items and studies were rated with a lsquo+rsquo if it met criteriafor that item a lsquominusrsquo if it did not meet criteria for an itemand a rsquorsquo if unclear lsquo+rsquo were coded as a score of 1 andminus were coded as a score of 0 Total scores and percen-tages were calculated Articles with total scores of 0ndash3were considered to be of low quality scores of 4ndash7were considered a medium quality and scores of 8ndash12 were considered to be of high quality Any discrep-ancies (approximately 3 of data points) wereresolved via consensus
Publication bias was assessed using a funnel plotwhich presents study size on the vertical axis (as stand-ard error in this case) as a function of effect size on thex-axis When no publication bias exists the studiesshould be distributed symmetrically about the com-bined effect size (Borenstein et al 2011) If evidenceof publication bias was observed Duval amp Tweediersquostrim-and-fill method was used (Duval amp Tweedie2000) which recalculates effects based on imputingdata from studies that are likely to be missing Lastthe Fail-safe N was calculated (Cooper 1979) whichindicates the number of missing studies that wouldneed to exist to nullify the observed effect
Results
A flow diagram of the search process is shown inFig 1 The search identified 2773 records through
PubMed 2158 through EMBASE and 1345 throughPsycINFO for a total of 6276 records Duplicaterecords (1709) were removed in EndNote resulting in4567 unique records After title and abstracts werereviewed 329 records were identified as potentially eli-gible for the meta-analysis These 329 records werereviewed in full and 300 articles were excluded hier-archically if they were a review baseline or protocolpaper (n = 6) if the sample had a mean age over 65at the depression assessment (n = 41) if the samplehad a specific medical illness (n = 23) if the studywas not a longitudinal design (n = 19) if MDD diagno-sis hospitalization or admission to treatment centerwas part of the inclusion criteria of the study (n = 18)if cognitive function was assessed only concurrentlywith or after depression (n = 36) if cognitive functionwas assessed by educational achievement or self-report(n = 26) if cognitive function was assessed by attribu-tion style rather than neuropsychological measure (n= 7) if there was no measure of cognitive function (n= 18) or no uniquely measured depression outcome(n = 24) Furthermore if articles reported on the samesample as another article with higher quality or moreinformation the duplicate articles were excluded (n =8) Last a number of studies appeared to measureboth cognitive function and depression but did not re-port enough information to be included in the meta-analysis and did not respond to requests for additionalinformation (n = 74 approximately 59 unique samples)In total 29 publication were included in the meta-ana-lysis comprising 34 samples (one study included twoseparate birth cohorts and another four reported dataseparately for men and women)
Study characteristics
The characteristics of included samples are detailed inTable 1 Sample sizes ranged from 43 to 50 053 with amedian of 3395 The most common types of sampleswere school samples (934) community samples (834) and birth cohorts (734) The samples were major-ity white with two samples having exclusively blackparticipants Additionally eight samples were menonly six samples were women only and the restreported combined effect sizes Mean age of partici-pants at baseline ranged from 35 to 59 years with amedian of 12 years Most samples did not reportwhether comorbid diagnoses were present (2334)
Of the 74 papers excluded for having insufficient in-formation (representing 60 unique samples) the me-dian number of subjects was not statistically differentbetween those studies and the studies included in themeta-analysis (n = 288 and n = 3395 respectively p =019) nor did the average age of study participants atbaseline statistically differ (median across studies = 11
10 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
v 12 respectively p = 057) The types of cognitivemeasures used were also similar across the excludedand included studies with the most common measurebeing IQ (2860 and 2029) followed by VerbalComprehension (860 and 529)
Meta-analysis
The overall analysis yielded a significant associationbetween cognitive function and subsequent depressionoutcomes [r =minus0088 95 confidence interval (CI)minus0121 to minus0054 p lt 0001 Fig 2] Results were similarwhen excluding the two studies that used beta-weights(r =minus0071 95 CI minus0100 to minus0042 p lt 0001) orwhen using episodic memory in place of processingspeed in a study reporting both outcomes (r =minus008595 CI minus0118 to minus0051 p lt 0001) Follow-up ana-lyses were conducted in the sample of studies report-ing educational attainment and self-report outcomes(Supplementary Table S2) Heterogeneity across sam-ples was significant (Q = 80154 p lt 0001) suggestingsubstantial variation across the individual samplesThe ratio of the true heterogeneity to total variationwas large (I2 = 9588) I2 is on a relative scale andvalues close to 100 indicate that most of the observedvariance is real rather than spurious and suggeststhat subgroup analyses or meta-regression may helpto explain this variability (Borenstein et al 2011)
Subgroup analyses and meta-regression
A significant difference was found between categoricaland continuous effect sizes (p lt 0001) The studiesassessing continuous outcomes were found to have alarger effect (r =minus0121 95 CI minus0168 to minus0073 p lt0001 n = 22) than studies assessing categorical out-comes (r =minus0035 95 CI minus0054 to minus0017 p lt 0001n = 12) No differences were observed between studiesutilizing broad v specific cognitive measures (p = 057)
Outcomes were also compared adjusting for baselinedepression symptoms at the time of cognitive assess-ment Nine studies provided enough detail to calculatethe partial correlation coefficients adjusting for base-line depression symptoms Using the partial correl-ation coefficients led to a null result (r =minus0032 95CI minus0078 to 0014 p = 0169 n = 9 Fig 3) The nullresult does not seem to be due to a lack of power be-cause using the unadjusted correlation coefficients forthe same nine studies still led to a significant result(r =minus0120 95 CI minus0169 to minus0070 p lt 0001 n = 9Fig 3) As a follow-up the difference in effect sizes be-tween the adjusted and unadjusted values for these 9studies were tested (r = 0082 95 CI 0069ndash0095 p lt0001 n = 9) suggesting that the effects are significantlydifferent when directly comparing the values that doand do not control for baseline depression symptoms
Expanding the subgroup analyses to include studiesthat controlled for baseline depression plus other co-variates (Zammit et al 2004 Simons et al 2009 Rawalamp Rice 2012) and studies that explicitly excluded fora history of depression diagnosis (Gale et al 2008Vinberg et al 2013 Papmeyer et al 2015) did notchange the null result (r =minus0027 95 CI minus0058 to0005 p = 0097 n = 15)
None of the meta-regression analyses were signifi-cant indicating that the between-study variance wasnot attributable to age at baseline IQ percent of sam-ple that was female percent of the sample that waswhite age at follow-up time between assessmentsyear of cognitive assessment year of follow-up assess-ment or study quality score
Study quality and publication bias
Multiple samples within a study were combined forthe purposes of quality assessment given that studieswithin the same publication were found to employthe same methodology Of the 29 publications reviewed12 were rated as high quality and 17 were rated as me-dium quality Details are provided in SupplementaryTable S1 Comparable results to the overall findingswere obtained when just using high quality studies (r=minus0085 95 CI minus0141 to minus0029 p = 0003)
Inspection of the funnel plot (Fig 4) found no evi-dence for publication bias to support the hypothesisIn fact imputation of negative correlations suggestedthat additional studies favoring the hypothesis maybe missing While the calculated effect size is minus0088(95 CI minus0121 to minus0054) using Duval amp Tweediersquostrim-and-fill method the imputed effect size estimateis larger at minus0137 (95 CI minus0176 to minus0099 imputedstudies n = 11) Last the Fail-safe N procedure foundthat 3583 null studies would need to be located forthe combined two-tailed p value to exceed 005 Thissuggests that significant results are not likely to be con-founded by publication bias and may even underesti-mate true effect sizes
Discussion
The present systematic review and meta-analysis of 29longitudinal publications including 1 21 749 partici-pants revealed that after accounting for baseline depres-sion symptoms variability in cognitive function did notpredict subsequent depression Consistent with priorreports there was a significant contemporaneous associ-ation between higher depression symptoms and lowercognitive function These patterns have implications forunderstanding the association between cognitive func-tion and depression and may be important for advan-cing etiologic and treatment research
Association between cognitive function and subsequent depression 11
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
First our findings reinforce models positing thatcognitive function tracks with depression severity(McDermott amp Ebmeier 2009) One possible explan-ation for this contemporaneous association is that de-pression symptoms interfere with the capacity tocomplete cognitive assessments possibly through thegeneral lack of motivation that is one hallmark of thedisorder While this explanation represents an experi-mental confound for studies focused on assessmentof cognitive function it likewise represents an oppor-tunity for studies to focus more comprehensively onthe assessment of both depression and mood disordersymptoms since performance on cognitive tests maybe a sensitive measure of motivational state thatcould augment self-reported symptoms Alternativelythe co-occurrence of cognitive deficits and depressionsymptoms may reflect shared genetic etiology (Hagen-aars et al 2016) and dysfunction of neural circuits
supporting both cognitive and emotional processes(Scult et al 2016) In particular dysfunction of prefront-al and striatal circuits have been associated with bothdepression and cognitive function (Keedwell et al2005 Aarts et al 2011)
Second our findings suggest that prior studies oflinks between cognitive function and depression thatdid not assess baseline symptoms may have overesti-mated the potential protective role of higher cognitivefunction While the importance of accounting for sub-clinical symptoms is not novel the implementation ofsuch accounting is often neglected in psychiatric epi-demiology given the current categorical threshold-based diagnostic system In our meta-analysis largereffects were observed for continuous as compared tocategorical outcomes which aligns with growing em-phasis on dimensional measures of psychopathology(Cuthbert amp Kozak 2013)
Fig 2 Meta-analysis of the association between cognitive function and subsequent depression A forest plot for all studiesthat investigated associations between cognition and later depression Results are reported as correlation coefficients denotedby squares and 95 confidence intervals (CI) indicated by lines (effect sizes are converted to correlation coefficients ifreported as odds ratios) Meta-analysis results are displayed as the diamond The overall analysis found a significant effect ofcognition on depression (r =minus0088 95 CI minus0121 to minus0054 p lt 0001)
12 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Fig 4 Trim-and-fill funnel plots for all samples Fisherrsquos Z a measure of effect size is plotted on the x-axis and the standarderror is plotted on the y-axis Larger studies appear toward the top of the graph and smaller studies towards the bottom Inthe absence of publication bias the studies are symmetrically distributed around the mean Actual studies are shown in opencircles and imputed studies would be shown in black circles No additional studies would be expected in the oppositedirection (to the right) of the observed effect but an additional 11 studies are imputed to the left of the mean effect sizeWhile the calculated effect size is minus0088 [95 confidence interval (CI) minus0121 to minus0054] using Duval amp Tweediersquos trim-and-fill method the imputed effect size estimate is larger at minus0137 (95 CI minus0176 to minus0099 imputed studies n = 11)
Fig 3 Meta-analysis comparing values adjusted for baseline depression symptoms v unadjusted A forest plot for analysiscomparing results from a subset of the same set of studies reported in Fig 2 when using unadjusted values compared tousing values that are adjusted for baseline depression Effects are significant for unadjusted values [r =minus0120 95 confidenceinterval (CI) minus0169 to minus0070 p lt 0001] but not for adjusted values (r =minus0032 95 CI minus0078 to 0014 p = 0169) Results arereported as correlation coefficients denoted by squares and 95 CIs indicated by lines Meta-analysis results are displayed asdiamonds
Association between cognitive function and subsequent depression 13
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Third the associations between cognitive functionand either current or later depression were not moder-ated by data quality or participant age sex and raceHowever there are a number of additional potentialmoderators that could not be addressed in the currentreview and meta-analysis For example the numberand type of comorbid conditions with depressionwere often not reported in the included studies butcould represent an important moderator of theobserved effects Modeling the effects of comorbid ill-ness is an important avenue for future research
One limitation of the current literature is that only ahandful of studies reviewed explicitly excluded for de-pression diagnosis at baseline (Gale et al 2008 Vinberget al 2013 Papmeyer et al 2015) however consistentwith the finding that controlling for baseline depres-sion symptoms led to a null association between cogni-tion and subsequent depression there was no effectobserved when including these studies in the sub-group analyses further suggesting that the associationbetween cognitive function and depression is likelycontemporaneous It will be important to follow-upthese analyses with individual studies that includerigorous assessment of baseline depression symptomsand other potentially confounding factors to furtherclarify this relationship
An open question that remains for future research iswhether deficits in cognitive function are likely to pre-dict the development of more sever or recurrent de-pression later in life Only one of the included studies(Koenen et al 2009) specifically investigated recurrentdepression and found that lower IQ was associatedwith greater persistence of disorder
A final consideration is that while our review andmeta-analysis focused on general cognitive functionmainly assessed via IQ there may be specific subtypesof cognitive function that are more predictive of laterdepression For example a lack of cognitive flexibilitymay more closely match with the ruminative stylecharacteristic of depression and therefore tasks specifi-cally measuring this component of cognitive functionmight have some predictive utility While our reviewdid not find differences between broad and specificmeasures of cognitive function there were not enoughstudies identified to allow for precise consideration ofdifferences between individual cognitive domains
A limitation of the meta-analysis is that while thepresent study followed standard guidelines (Stroupet al 2000 Atkinson et al 2014) decisions aboutstudy selection data extraction and quality assess-ment include a number of decision points that neces-sarily involve a level of subjectivity Reliability wasascertained by using independent raters however dif-ferent inclusionexclusion criteria or a different ap-proach to the evaluation of those criteria could result
in a different set of studies being includedUltimately the quality of the meta-analysis is depend-ent upon the underlying studies that are analyzedFurthermore although studies with insufficient infor-mation to be included in the meta-analysis were notfound to differ based on basic study data from thosestudies included in the meta-analysis nonetheless itis unknown how if at all data from these studiescould change the overall results
Acknowledging these limitations our present reviewand meta-analysis found that while an association is evi-dent between cognitive function and later depressiongeneral cognitive function does not appear to be a riskfactor for depression but rather is more likely relatedto performance decrements associated with concurrentdepressive symptoms Our results suggest that low cog-nitive function is therefore probably not a causal factorof depression and that clinical practice may benefitmore from a focus on how decreased cognitive functionin the depressed state is likely to influence treatment out-comes (Gyurak et al 2015) Our findings have importantimplications for better understanding depression and forthe design of future studies in highlighting the need tocontrol for subthreshold depression symptoms when in-vestigating risk factors for mental illness as well as whenassessing cognitive function more generally
Supplementary material
The supplementary material for this article can befound at httpdxdoiorg101017S0033291716002075
Acknowledgements
MAS is supported by an National Science Foundation(NSF) Graduate Research Fellowship ARH is sup-ported by National Institutes of Health (NIH) grantsRO1DA033369 amp R01AG049789 TEM is supportedby National Institutes of Health (NIH) grantsR01AG049789 We would like to thank HarrisCooper PhD at Duke University who provided invalu-able insight into conducting the meta-analysis Wethank all of the authors of studies who provided add-itional information for this meta-analysis
Declaration of Interest
None
References
Aarts E van Holstein M Cools R (2011) Striatal dopamineand the interface between motivation and cognitionFrontiers in Psychology 2 163
14 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Atkinson KM Koenka AC Sanchez CE Moshontz HCooper H (2014) Reporting standards for literaturesearches and report inclusion criteria making researchsyntheses more transparent and easy to replicate ResearchSynthesis Methods 6 87ndash95
Baer LH Tabri N Blair M Bye D Li KZH Pushkar D(2013) Longitudinal associations of need for cognitioncognitive activity and depressive symptomatology withcognitive function in recent retirees Journals of GerontologySeries B Psychological Sciences and Social Sciences 68 655ndash664
Barbey AK Colom R Solomon J Krueger F Forbes CGrafman J (2012) An integrative architecture for generalintelligence and executive function revealed by lesionmapping Brain 135 1154ndash1164
Barnett JH Salmond CH Jones PB Sahakian BJ (2006)Cognitive reserve in neuropsychiatry Psychological Medicine36 1053ndash1064
Beaujean AA Parker S Qiu X (2013) The relationshipbetween cognitive ability and depression a longitudinaldata analysis Social Psychiatry and Psychiatric Epidemiology48 1983ndash1992
Belsky DW Caspi A Arseneault L Bleidorn W Fonagy PGoodman M Houts R Moffitt TE (2012) Etiologicalfeatures of borderline personality related characteristics in abirth cohort of 12-year-old children Development andPsychopathology 24 251ndash265
Betts KS Williams GM Najman JM Alati R (2016)Predicting spectrums of adult mania psychosis anddepression by prospectively ascertained childhoodneurodevelopment Journal of Psychiatric Research 72 22ndash29
Bora E Harrison BJ Yuumlcel M Pantelis C (2013) Cognitiveimpairment in euthymic major depressive disorder a meta-analysis Psychological Medicine 43 2017ndash2026
Borenstein M Hedges LV Higgins JPT Rothstein HR(2011) Introduction to Meta-Analysis John Wiley amp SonsWest Sussex UK
Canals J Domegravenech-Llaberia E Fernaacutendez-Ballart J Martiacute-Henneberg C (2002) Predictors of depression at eighteenA 7-year follow-up study in a Spanish nonclinicalpopulation European Child amp Adolescent Psychiatry 11226ndash233
Christensen H Griffiths K Mackinnon A (1997) Aquantitative review of cognitive deficits in depression andAlzheimer-type dementia Selection of Studies 3 631ndash651
Connolly SL Wagner Ca Shapero BG Pendergast LLAbramson LY Alloy LB (2014) Rumination prospectivelypredicts executive functioning impairments in adolescentsJournal of Behavior Therapy and Experimental Psychiatry 4546ndash56
Cooper HM (1979) Statistically combining independentstudies a meta-analysis of sex differences in conformityresearch Journal of Personality and Social Psychology 37131ndash146
Cooper HM (2010) Research Synthesis and Meta-Analysis AStep-by-Step Approach 4th edn SAGE PublicationsWashington (DC) USA
Cuijpers P de Graaf R van Dorsselaer S (2004) Minordepression risk profiles functional disability health careuse and risk of developing major depression Journal ofAffective Disorders 79 71ndash79
Cuthbert BN Kozak MJ (2013) Constructing constructs forpsychopathology the NIMH research domain criteriaJournal of Abnormal Psychology 122 928ndash937
Der G Batty GD Deary IJ (2009) The association between IQin adolescence and a range of health outcomes at 40 in the1979 US National Longitudinal Study of Youth Intelligence37 573ndash580
Dubow EF Boxer P Huesmann LR (2008) Childhood andadolescent predictors of early and middle adulthoodalcohol use and problem drinking the Columbia CountyLongitudinal Study Addiction 103 36ndash47
Duval S Tweedie R (2000) Trim and fill a simple funnel-plot-based method of testing and adjusting for publicationbias in meta-analysis Biometrics 56 455ndash463
Evans LD Kouros CD Samanez-Larkin S Garber J (2015)Concurrent and short-term prospective relations amongneurocognitive functioning coping and depressivesymptoms in youth Journal of Clinical Child and AdolescentPsychology 53 1ndash15
Franz CE Lyons MJ OrsquoBrien R Panizzon MS Kim K BhatR Grant MD Toomey R Eisen S Xian H Kremen WS(2011) A 35-year longitudinal assessment of cognition andmidlife depression symptoms the Vietnam Era Twin Studyof Aging American Association for Geriatric PsychiatryAmerican Journal of Geriatric Psychiatry 19 559ndash570
Gale CR Batty GD Tynelius P Deary IJ Rasmussen F(2010) Intelligence in early adulthood and subsequenthospitalization for mental disorders Epidemiology 2170ndash77
Gale CR Deary IJ Boyle SH Barefoot J Mortensen LHBatty GD (2008) Cognitive ability in early adulthood andrisk of 5 specific psychiatric disorders in middle age theVietnam experience study Archives of General Psychiatry 651410ndash1418
Gale CR Hatch SL Batty GD Deary IJ (2009) Intelligence inchildhood and risk of psychological distress in adulthoodthe 1958 National Child Development Survey and the 1970British Cohort Study Intelligence 37 592ndash599
Gjerde PF (1995) Alternative pathways to chronicdepressive symptoms in young adults gender differencesin developmental trajectories Child Development 661277ndash1300
Gottfredson LS (1997) Mainstream science on intelligence aneditorial with 52 signatories history and bibliographyIntelligence 24 13ndash23
Guyer AE Choate VR Grimm KJ Pine DS Keenan K(2011) Emerging depression is associated with facememory deficits in adolescent girls Elsevier Inc Journal ofthe American Academy of Child and Adolescent Psychiatry 50180ndash190
Gyurak A Patenaude B Korgaonkar MS Grieve SMWilliams LM Etkin A (2015) Frontoparietal activationduring response inhibition predicts remission toantidepressants in patients with major depression BiologicalPsychiatry 79 1ndash8
Hagenaars SP Harris SE Davies G Hill WD LiewaldDCM Ritchie SJ Marioni RE Fawns-Ritchie C Cullen BMalik R METASTROKE Consortium IC for BPGSpiroMeta Consortium CHARGE ConsortiumPulmonary Group CCA and LG Worrall BB Sudlow
Association between cognitive function and subsequent depression 15
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
CLM Wardlaw JM Gallacher J Pell J McIntosh AMSmith DJ Gale CR Deary IJ (2016) Shared geneticaetiology between cognitive functions and physical andmental health in UK Biobank (N = 112 151) and 24 GWASconsortiaMolecular Psychiatry Published online 26 January2016 doi101038mp2015225
Hatch SL Jones PB Kuh D Hardy R Wadsworth MEJRichards M (2007) Childhood cognitive ability and adultmental health in the British 1946 birth cohort Social Scienceamp Medicine (1982) 64 2285ndash2296
Hipwell AE Sapotichne B Klostermann S Battista DKeenan K (2011) Autobiographical memory as a predictorof depression vulnerability in girls Journal of Clinical Childand Adolescent Psychology 40 254ndash265
Horowitz JL Garber J (2003) Relation of intelligence andreligiosity to depressive disorders in offspring of depressedand nondepressed mothers The American Academy ofChild and Adolescent Psychiatry Journal of the AmericanAcademy of Child and Adolescent Psychiatry 42 578ndash586
Johnson W Bouchard TJ Krueger RF McGue MGottesman II (2004) Just one g consistent results fromthree test batteries Intelligence 32 95ndash107
Keedwell PA Andrew C Williams SCR Brammer MJPhillips ML (2005) The neural correlates of anhedoniain major depressive disorder Biological Psychiatry 58843ndash853
Kessler RC Berglund P Demler O Jin R Koretz DMerikangas KR Rush AJ Walters EE Wang PS (2003)The epidemiology of major depressive disorder resultsfrom the National Comorbidity Survey Replication(NCS-R) Journal of the American Medical Association 2893095ndash3105
Koenen KC Moffitt TE Roberts AL Martin LT KubzanskyL Harrington H Poulton R Caspi A (2009) Childhood IQand adult mental disorders a test of the cognitive reservehypothesis American Journal of Psychiatry 166 50ndash57
Lewinsohn PM Solomon A Seeley JR Zeiss A (2000)Clinical implications of lsquosubthresholdrsquo depressivesymptoms Journal of Abnormal Psychology 109 345ndash351
Luppino FS de Wit LM Bouvy PF Stijnen T Cuijpers PPenninx BWJH Zitman FG (2010) Overweight obesityand depression a systematic review and meta-analysisof longitudinal studies Archives of General Psychiatry 67220ndash229
McCord J Ensminger ME (1997) Multiple risks andcomorbidity in an African-American population CriminalBehaviour and Mental Health 7 339ndash352
McDermott LM Ebmeier KP (2009) A meta-analysis ofdepression severity and cognitive function Elsevier BVJournal of Affective Disorders 119 1ndash8
Melartin TK Rytsaumllauml HJ Leskelauml US Lestelauml-Mielonen PSSokero TP Isometsauml ET (2002) Current comorbidity ofpsychiatric disorders among DSM-IV major depressivedisorder patients in psychiatric care in the VantaaDepression Study Journal of Clinical Psychiatry 63 126ndash134
Meyer SE Carlson GA Wiggs EA Martinez PE RonsavilleDS KlimesndashDougan B Gold PW RadkendashYarrow M(2004) A prospective study of the association amongimpaired executive functioning childhood attentional
problems and the development of bipolar disorderDevelopment and Psychopathology 16 461ndash476
MiyakeA FriedmanNP EmersonMJWitzki aHHowerter AWager TD (2000) The unity and diversity of executivefunctions and their contributions to complex lsquoFrontal Lobersquotasks a latentvariable analysisCognitive Psychology41 49ndash100
Moher D Liberati A (2009) Preferred reporting items forsystematic reviews and meta-analyses the PRISMAstatement Annals of Internal Medicine 151 264ndash269
Papmeyer M Sussmann JE Hall J McKirdy J Peel AMacdonald A Lawrie SM Whalley HC McIntosh AM(2015) Neurocognition in individuals at high familial riskof mood disorders with or without subsequent onset ofdepression Psychological Medicine 45 1ndash11
Peterson RA Brown SP (2005) On the use of betacoefficients in meta-analysis Journal of Applied Psychology90 175ndash181
Pine DS Cohen P Brook J Coplan JD (1997) Psychiatricsymptoms in adolescence as predictors of obesity in earlyadulthood a longitudinal study American Journal of PublicHealth 87 1303ndash1310
Quinn ME Joormann J (2015) Control when it countschange in executive control under stress predicts depressionsymptoms Emotion Junio 22 1ndash10
Rawal A Rice F (2012) Examining overgeneralautobiographical memory as a risk factor for adolescentdepression Elsevier Inc Journal of the American Academy ofChild and Adolescent Psychiatry 51 518ndash527
Ree MJ Earles JA (1991) The stability of g across differentmethods of estimation Intelligence 15 271ndash278
Rock PL Roiser JP Riedel WJ Blackwell AD (2014)Cognitive impairment in depression a systematic reviewand meta-analysis Psychological Medicine 44 2029ndash2040
Rogers MA Kasai K Koji M Fukuda R Iwanami ANakagome K Fukuda M Kato N (2004) Executive andprefrontal dysfunction in unipolar depression a review ofneuropsychological and imaging evidence NeuroscienceResearch 50 1ndash11
Scult MA Knodt AR Swartz JR Brigidi BD Hariri AR(2016) Thinking and feeling individual differences inhabitual emotion regulation and stress-related mood areassociated with prefrontal executive control ClinicalPsychological Science doi1011772167702616654688
Sharp C Petersen N Goodyer I (2008) Emotional reactivityand the emergence of conduct problems and emotionalsymptoms in 7- to 11-year-olds a 1-year follow-up studyJournal of the American Academy of Child and AdolescentPsychiatry 47 565ndash573
Siegel LS (1999) Issues in the definition and diagnosis oflearning disabilities a perspective on Guckenberger vBoston University Journal of Learning Disabilities 32 304ndash319
Simons CJP Jacobs N Derom C Thiery E Jolles J van Os JKrabbendam L (2009) Cognition as predictor of currentand follow-up depressive symptoms in the generalpopulation Acta Psychiatrica Scandinavica 120 45ndash52
Slykerman RF Thompson J Waldie K Murphy R Wall CMitchell EA (2015) Maternal stress during pregnancy isassociated with moderate to severe depression in 11-year-old children Acta Paediatrica 104 68ndash74
16 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Snyder HR (2013) Major depressive disorder is associatedwith broad impairments on neuropsychological measuresof executive function a meta-analysis and reviewPsychological Bulletin 139 81ndash132
Soslashrensen HJ Saeligbye D Urfer-Parnas A Mortensen ELParnas J (2012) Premorbid intelligence and educationallevel in bipolar and unipolar disorders a Danish draftboard study Journal of Affective Disorders 136 1188ndash1191
SpearmanC (1904) lsquoGeneral intelligencersquoobjectivelydeterminedandmeasuredAmerican Journal of Psychology 15 201
Stern Y (2003) The concept of cognitive reserve a catalyst forresearch Journal of Clinical and Experimental Neuropsychology(Neuropsychology Development and Cognition Section A) 25589ndash593
Stroup D Berlin J Morton S Olkin I Williamson GDRennie D Moher D Becker BJ Sipe TA Thacker SB(2000) Meta-analysis of Observational Studies inEpidemiology a proposal for reporting Journal of theAmerican Medical Association 283 2008
Vinberg M Miskowiak KW Kessing LV (2013) Impairmentof executive function and attention predicts onset ofaffective disorder in healthy high-risk twins Journal ofClinical Psychiatry 74 e747ndashe753
Zammit S Allebeck P David AS Dalman C HemmingssonT Lundberg I Lewis G (2004) A longitudinal study ofpremorbid IQ Score and risk of developing schizophreniabipolar disorder severe depression and other nonaffectivepsychoses Archives of General Psychiatry 61 354ndash360
Association between cognitive function and subsequent depression 17
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms

Table 1 (cont)
StudyName ofcohort Type of cohort
Samplesize Comorbidity
Howdepressionassessed
Mean IQatbaseline
Name ofcognitivemeasure
Type of cognitivemeasure
Name ofdepressionoutcome
Type ofdepressionoutcome
Covariatesincluded inmeta-analysisa
Percentfemale Raceethnicity Continent
Meanage atbaseline
Timebetweenassessments(years)
Year ofinitialassessment
Der et al(2009)
US NationalLongitudinalSurvey ofYouth 1979
Communitysample
7458 Noted a rangeof healthconditions
Studyassessment
NR Armed ServicesVocationalAptitudeBattery(ASVAB)Armed ForcesQualificationTest (AFQT)
General IntelligenceVerbalComprehension
Center forEpidemiologicalStudiesDepression Scale(CES-D)
Continuous Depressionsymptoms atTime 1
52 31 Black19Hispanic
NorthAmerica
179 sim22 1979
Dubow et al(2008)(females)
ColumbiaCountyLongitudinalStudy(CCLS)
SchoolChildrenGrade 3
215 NR Studyassessment
sim104 CaliforniaShort-FormTest of MentalMaturity
General Intellignce MinnesotaMultiphasicPersonalityInventory(MMPI) Scale 2
Continuous None 100 90 White3 Blacklt1Asianlt1Hispanic
NorthAmerica
8 11 1960
Dubow et al(2008)(males)
ColumbiaCountyLongitudinalStudy(CCLS)
SchoolChildrenGrade 3
211 NR Studyassessment
sim104 CaliforniaShort-FormTest of MentalMaturity
General Intelligence MinnesotaMultiphasicPersonalityInventory(MMPI) Scale 2
Continuous None 0 90 White3 Blacklt1Asianlt1Hispanic
NorthAmerica
8 11 1960
Evans et al(2015)
NR SchoolChildrenGrades 5ndash9
192 Some withADHD
Studyassessment
111 WechslerAbbreviatedScale ofIntelligence(WASI)
General IntelligenceVerbalComprehensionPerceptualReasoning WorkingMemorySet-Shifting
ChildrenrsquosDepressionInventory (CDI)
Continuous Depressionsymptoms atTime 1
521 714 White182 Black26 Asian36Hispanic42 MixedRace
NorthAmerica
1236 03 sim2000s
Franz et al(2011)
Vietnam EraTwin Studyof Aging
Military cohort 1231 NR Studyassessment
NR Armed ForcesQualificationTest (AFQTForm 7A)
General IntelligencePerceptualReasoning WorkingMemory ProcessingSpeed Set-ShiftingInhibition
Center forEpidemiologicalStudiesDepression Scale(CES-D)
Continuous None 0 86 White NorthAmerica
20 35 sim1970
Gale et al(2008)
VietnamExperienceStudy (VES)
Military cohort 3258 Mix Studyassessment
100 Generaltechnicalsection of theArmyClassificationBattery
General IntelligenceVerbalComprehensionArithmeticreasoning
DiagnosticInterviewSchedule (DIS)
Categorical SocioeconomicStatusEthnicity Placeof service
0 808 White127 Black
NorthAmerica
204 sim17 sim1964
Gale et al(2009)(1958Cohort)
1958 NationalChildDevelopmentSurvey
Birth cohort 6369 NR Studyassessment
1028 General abilitytest devisedby theNationalFoundationforEducationalResearch inEngland andWales
General Intelligence Rutterrsquos MalaiseInventory
Continuous None NR (bothmaleandfemale)
NR Europe 11 22 1969
4MA
Scultet
al
httpdxdoiorg101017S0033291716002075D
ownloaded from
httpww
wcam
bridgeorgcore Duke U
niversity Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core term
s of use available at httpww
wcam
bridgeorgcoreterms
Gale et al(2009)(1970Cohort)
1970 BritishCohort Study
Birth cohort 6074 NR Studyassessment
1018 British abilityScale
General Intelligence Rutterrsquos MalaiseInventory
Continuous None NR (bothmaleandfemale)
NR Europe 10 20 1980
Gjerde(1995)(females)
NR Recruited froma nurseryschool
51 NR Studyassessment
1187 Wechsler AdultIntelligenceScale (WAIS)
General Intelligence General BehaviorInventory (GBI)Depression scale
Continuous None 100 sim66 Whitesim25Blacksim005Asian
NorthAmerica
18 5 1983
Gjerde et al(1995)(males)
NR Recruited froma nurseryschool
45 NR Studyassessment
11112 Wechsler AdultIntelligenceScale (WAIS)
General Intelligence General BehaviorInventory (GBI)Depression scale
Continuous None 0 sim66 Whitesim25 Blacksim005Asian
NorthAmerica
18 5 1983
Hatch et al(2007)
1946 BritishCohort Study
Birth cohort 957 NR Studyassessment
NR NationalFoundationforEducationalResearch Test
General IntelligenceVerbalComprehensionPerceptualReasoning
General HealthQuestionnaire(GHQ-28)-severedepressionsubscale
Continuous None 51 NR Europe 8 45 1954
Hipwellet al (2011)
PittsburghGirls Study(PGS)
Communitysample
195 NR Studyassessment
9954 WechslerIntelligenceScale forChildren(WISC) III-R
VerbalComprehension
Schedule forAffectiveDisorders forSchool-AgeChildren-Present andLifetime Version(K-SADS-PL)
Continuous Depressionsymptoms atTime 1
100 70 Black ormultiracial
NorthAmerica
1154 1 1998
Horowitz ampGarber(2003)
NR Elementaryschool cohort
196 NR Studyassessment
10461 WechslerIntelligenceScale forChildren(WISC) -R
General IntelligenceVerbalComprehensionPerceptualReasoning
Schedule forAffectiveDisorders forSchool-AgeChildren-EpidemiologicalVersion(K-SADS-E)
Categorical Depressionsymptoms atTime 1
542 89 White147 Black33 Other
NorthAmerica
1186 6 sim1980
Koenenet al (2009)
DunedinCohort
Birth cohort 730 None Studyassessment
NR WechslerIntelligenceScale forChildren(WISC)
General IntelligenceVerbalComprehensionPerceptualReasoning WorkingMemory ProcessingSpeed
DiagnosticInterviewAssessment (forDSM-IV)
Categorical SexSocioeconomicStatusPhysicalHealthchildhoodmaltreatment
48 lsquoPrimarilyWhitersquo
NewZealand
9 23 1981
McCord ampEnsminger(1997)(females)
WoodlawnCohort
Elementaryschool cohort
346 Some withalcoholism
Studyassessment
NR (13 Unspecified IQof sample had scoresover 110)
General Intelligence CompositeInternationalInterviewSchedule(according toDSM-III-R)
Categorical None 100 100 Black NorthAmerica
sim6 27 1966
McCord ampEnsminger(1997)(males)
WoodlawnCohort
Elementaryschool cohort
313 Some withalcoholism
Studyassessment
NR (11 Unspecified IQof sample had scoresover 110)
General Intelligence CompositeInternationalInterviewSchedule(according toDSM-III-R)
Categorical None 0 100 Black NorthAmerica
sim6 27 1966
Meyer et al(2004)
NR Risk sample 86 NR Studyassessment
sim118 WISC General IntelligenceVerbalComprehensionPerceptualReasoning
SCID Categorical None 63 90 White9 Black 1Hispanic
NorthAmerica
11 13 1989
Association
between
cognitivefunction
andsubsequent
depression5
httpdxdoiorg101017S0033291716002075D
ownloaded from
httpww
wcam
bridgeorgcore Duke U
niversity Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core term
s of use available at httpww
wcam
bridgeorgcoreterms
Table 1 (cont)
StudyName ofcohort Type of cohort
Samplesize Comorbidity
Howdepressionassessed
Mean IQatbaseline
Name ofcognitivemeasure
Type of cognitivemeasure
Name ofdepressionoutcome
Type ofdepressionoutcome
Covariatesincluded inmeta-analysisa
Percentfemale Raceethnicity Continent
Meanage atbaseline
Timebetweenassessments(years)
Year ofinitialassessment
Papmeyeret al (2015)
ScottishBipolarFamily Study
Risk sample 111 NR Studyassessment
Controls108Patients107
National AdultReading Test(NART)
VerbalComprehension
Structured ClinicalInterview forDSM Disorders(SCID)symptoms
Categorical None 52 NR Europe 21 2 NR
Pine et al(1997)
NR Communitysample
644 NR Studyassessment
1007 UnspecifiedlsquoIQrsquo
General Intelligence Based onDiagnosticInterviewSchedule forChildren
Continuous Depressionsymptoms atTime 1
52 91 White NorthAmerica
138 9 1983
Quinn ampJoormann(2015)
NR Undergraduatestudents
43 NR Studyassessment
NR n-back Working Memory Beck DepressionInventory II(BDI-II)
Continuous Depressionsymptoms atTime 1
63 58 White30Hispanic orLatino 19Asian 2AfricanAmerican2AmericanIndian 2NativeHawaiian2 Indian
NorthAmerica
19 014 NR
Rawal ampRice (2012)
EarlyPrediction ofAdolescentDepressionstudy
Risk sample 230 None Studyassessment
9746 WechslerIntelligenceScale forChildren(WISC)
General IntelligenceVerbalComprehensionPerceptualReasoning WorkingMemory ProcessingSpeed
Child andAdolescentPsychiatricAssessment(CAPA)
Both Depressionsymptoms atTime 1 AgeOvergeneralityto negativecues
596 NR Europe 1371 1 NR
Sharp et al(2008)
The ChildBehaviourStudy
Communitysample
439 NR Studyassessment
105 WechslerIntelligenceScale forChildren(WISC)
General IntelligenceVerbalComprehensionPerceptualReasoning
The Mood andFeelingsQuestionnaire
Continuous Depressionsymptoms atTime 1
52 97 White05 Black25 Asian
Europe 94 1 NR
Simons et al(2009)
East FlandersProspectiveTwin Survey
Twin registry 444 NR Studyassessment
NR Principalcomponentfrom StroopConceptShifting Testand LetterDigitSubstitutionTest
Processing SpeedSet-ShiftingInhibition
Structured ClinicalInterview forDSM Disorders(SCID)symptoms
Continuous Depressionsymptoms atTime 1
100 NR Europe 28 2 NR
6MA
Scultet
al
httpdxdoiorg101017S0033291716002075D
ownloaded from
httpww
wcam
bridgeorgcore Duke U
niversity Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core term
s of use available at httpww
wcam
bridgeorgcoreterms
Slykermanet al (2015)
AucklandBirthweightCollaborativeStudy
Birth cohortrisk sample
609 NR Studyassessment
NR Stanford-BinetIntelligenceScale 4th Ed
General IntelligenceFluid ReasoningKnowledgeQunatitativeReasoningVisual-SpatialProcessingWorking Memory
Center forEpidemiologicalStudiesDepression Scale(CES-D)
Categorical(cut-point)
None 49 NR NewZealand
35 75 sim2000
Soslashrensenet al (2012)
DanishDraft-BoardStudy
Military cohort 21 914 NR Psychiatricregistry
Controls100Patients96ndash98
Boslashrge PriensProslashve (BPP)
General IntelligenceVerbalComprehensionPerceptualReasoning
DanishInternationalClassification ofdiseases (ICD) 8amp 10
Categorical None 0 NR Europe 195 sim36 1968ndash1989
Vinberget al (2013)
NR High-risktwins
224 Bipolardisorderanxietysubstanceabuse other
Studyassessmentpsychiatricregistry
NR CambridgeCognitiveAssessment(CAMCOG)
GeneralNeuropsychologicalFunctionOrientationLanugage MemoryAttention AbstractThinking VisualPerception
Beck DepressionInventory (BDI)
Continuous Depressionsymptoms atTime 1
65 NR Europe 439 7 2003
Zammitet al (2004)
SwedishConscripts(1969ndash1970)
Military cohort 50 053 None Hospitallinkage
NR UnspecifiedlsquoIQrsquo
General IntelligenceVerbalComprehensionPerceptualReasoning GeneralKnowledgeMechanicalKnowledge
InternationalClassification ofdiseases (ICD)hospitalpsychiatricadmissions
Categorical Diagnosis atbaselinedisturbedbehavior druguse raised in acity
0 NR Europe sim19 27 1969
Sample size is the number of subjects included in reported analyses of interest NR not reportedsim indicates only a range was reporteda This column notes covariates included in the meta-analysis We focused on controlling for depressive symptoms at T1 but some studies reported effect sizes that also included controlling
for other variables ndash when the zero-order correlations were unavailable these estimates were used
Association
between
cognitivefunction
andsubsequent
depression7
httpdxdoiorg101017S0033291716002075D
ownloaded from
httpww
wcam
bridgeorgcore Duke U
niversity Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core term
s of use available at httpww
wcam
bridgeorgcoreterms
to investigate general information processing abilitiesrather than cognitive attributional style studies withcognitive attribution measures as the sole cognitivemeasure were excluded
Comparisons
Search terms used to indicate the possible associationbetween cognitive function and depression includedrisk premorbid prodromal onset predict and association(for a full list see search terms in the SupplementaryMaterial) When data were reported from multipletime-points the analysis accounting for the longesttime between assessments was used
Outcomes
Eligible studies reported depression diagnosis orsymptoms determined by investigator or self-reportPresence of comorbidity was permitted given that de-pression has been found to be highly comorbid withother disorders (Melartin et al 2002 Kessler et al2003) Articles not adequately specifying how depres-sion was assessed or articles that did not uniquelymeasure depression [ie only had an index of lsquomentaldisordersrsquo or the category of lsquomood disordersrsquo lumpedtogether (Gale et al 2010)] were excluded if no uniquemeasure of depression could be obtained from studyauthors This is because although comorbidity waspermitted these could have represented instances ofpure anxiety disorders with few or no depressivesymptoms or instances of bipolar disorder
Study design
Eligible study search terms included cohort studies lon-gitudinal epidemiological prospective retrospective follow-up or case-control studies Studies not following a longi-tudinal design were excluded during full-text reviewAdditionally studies where cognitive function wasassessed only concurrently with or after depressionwere excluded given that the purpose of the reviewwas to investigate whether cognitive function pre-dicted later depression
Studies were included regardless of whether theywere reported in peer-review journals in order to ac-count for potentially biased reporting of resultsReview articles were included in the search terms tofind additional relevant references but were notincluded in the meta-analysis Baseline and protocolstudies without follow-up data were excluded
Study selection
A flow diagram of the process of study selection showsthe overall procedures (Fig 1) Records identified fromthe search processes were combined in EndNote
software version X7 and duplicates were removedTitles and abstracts were reviewed independently bytwo reviewers (MS and AP) according to the eligibil-ity criteria described above and marked as either po-tentially eligible or not eligible If either authormarked an article as potentially eligible it wasincluded in the full-text review for closer examinationby MS and AP who used an electronic form to indi-cate if an article should be included or excluded in thefinal selection When an article was excluded the rea-son for exclusion was selected from a hierarchical listof exclusion criteria presented in Fig 1 Both MSand AP were initially blinded to the otherrsquos decisionsAfter both MS and AP completed their reviews dis-crepancies about whether a study should be includedor excluded were resolved via discussion and consen-sus amongst MS AP TM AH and TS
Data extraction
Study information was extracted independently byMS and AP using an electronic form created forthis study Information was collected and codedbased on report characteristics participant characteris-tics study setting predictors outcome measures andquality assessment (Cooper 2010) Any discrepancies(approximately 3 of data points) were resolved viaconsensus
For studies with categorical depression diagnoses ef-fect sizes were generally presented as odds ratios Forthese studies the odds ratio plus the upper and lowerbound of the confidence interval were recorded Twoof the studies (Zammit et al 2004 Gale et al 2008)reported odds ratios greater than one to indicate thatlower IQ was associated with greater risk of depressionThe other studies reported odds ratios in the reverseleading to odds ratios less than one for the same direc-tion of the effect Therefore the odds ratios from the firsttwo studies were recalculated by dividing (1oddsratio) Another study (McCord amp Ensminger 1997)reported results from chi-squared tests Additional stud-ies reported mean premorbid IQ scores rather than oddsratios in which case the means sample sizes andor pvalues and number of tails of the t test were utilizedto calculate the effect size
For studies in which depression was measured as acontinuous variable effect sizes were presented as cor-relation coefficients The direction of the effect (posi-tive or negative) and the sample size were alsoextracted to be used in the meta-analysis Two studiesreported only beta weights (Simons et al 2009 Rawalamp Rice 2012) and we were not able to obtain zero-order correlations from the authors Given that previ-ous reports have suggested that beta weights can beused as an estimate of correlation coefficients in
8 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
meta-analysis (Peterson amp Brown 2005) the betaweights were used instead and analyses were runboth including and excluding these data points
When insufficient information was presented in thearticle authors were contacted requesting further de-tail An additional six studies were included at thispoint One study (Hatch et al 2007) included effectsizes for the female half of the cohort and did not pro-vide statistics for the males but did indicate a null ef-fect Only women from this study were included in themeta-analyses but imputing a score of 0 for the malesyielded similar overall results
Follow-up analyses directly compared studies thatreported zero-order correlations between IQ at time
1 depression at time 1 and depression at time 2(additional details described in the SupplementaryMethods)
Statistical methods
Data were analyzed using Comprehensive Meta-Analysis software version 30 (Biostat Inc USA) Arandom-effects model was used for expected hetero-geneity across studies A random-effects model alsoallows for broader generalization of results to thepopulation at large Heterogeneity of effects was calcu-lated using the Q statistic where a significant p valueindicates that true effect varies across studies The I2
Fig 1 Flow diagram of the search process
Association between cognitive function and subsequent depression 9
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
statistic was used to calculate the ratio of the true het-erogeneity to total variation acting as an index of sig-nal-to-noise ratio When I2 is large it is has beenrecommended to consider subgroup analysis or meta-regression to account for the variance (Borensteinet al 2011)
Subgroup analyses were conducted using a mixed-effects analysis in which a random effects model wasused to combine studies within each subgroup and afixed effect model was used to combine subgroupsand yield the overall effect (the study-to-study vari-ance is not assumed to be the same for all subgroups)Subgroup analyses were conducted comparing type ofoutcome (continuous v categorical) broad v specificcognitive measures and outcomes that were adjustedv unadjusted for baseline depression symptoms
Meta-regression was performed using the followingvariables on unadjusted analyses age at baseline ageat follow-up time between assessments IQ percentwhite year of cognitive assessment year of follow-upassessment percent female and study quality score
Study quality and publication bias
Study quality was evaluated independently by MSand AP using a checklist adapted from Luppino ampWit (Luppino et al 2010) The checklist contained 12items and studies were rated with a lsquo+rsquo if it met criteriafor that item a lsquominusrsquo if it did not meet criteria for an itemand a rsquorsquo if unclear lsquo+rsquo were coded as a score of 1 andminus were coded as a score of 0 Total scores and percen-tages were calculated Articles with total scores of 0ndash3were considered to be of low quality scores of 4ndash7were considered a medium quality and scores of 8ndash12 were considered to be of high quality Any discrep-ancies (approximately 3 of data points) wereresolved via consensus
Publication bias was assessed using a funnel plotwhich presents study size on the vertical axis (as stand-ard error in this case) as a function of effect size on thex-axis When no publication bias exists the studiesshould be distributed symmetrically about the com-bined effect size (Borenstein et al 2011) If evidenceof publication bias was observed Duval amp Tweediersquostrim-and-fill method was used (Duval amp Tweedie2000) which recalculates effects based on imputingdata from studies that are likely to be missing Lastthe Fail-safe N was calculated (Cooper 1979) whichindicates the number of missing studies that wouldneed to exist to nullify the observed effect
Results
A flow diagram of the search process is shown inFig 1 The search identified 2773 records through
PubMed 2158 through EMBASE and 1345 throughPsycINFO for a total of 6276 records Duplicaterecords (1709) were removed in EndNote resulting in4567 unique records After title and abstracts werereviewed 329 records were identified as potentially eli-gible for the meta-analysis These 329 records werereviewed in full and 300 articles were excluded hier-archically if they were a review baseline or protocolpaper (n = 6) if the sample had a mean age over 65at the depression assessment (n = 41) if the samplehad a specific medical illness (n = 23) if the studywas not a longitudinal design (n = 19) if MDD diagno-sis hospitalization or admission to treatment centerwas part of the inclusion criteria of the study (n = 18)if cognitive function was assessed only concurrentlywith or after depression (n = 36) if cognitive functionwas assessed by educational achievement or self-report(n = 26) if cognitive function was assessed by attribu-tion style rather than neuropsychological measure (n= 7) if there was no measure of cognitive function (n= 18) or no uniquely measured depression outcome(n = 24) Furthermore if articles reported on the samesample as another article with higher quality or moreinformation the duplicate articles were excluded (n =8) Last a number of studies appeared to measureboth cognitive function and depression but did not re-port enough information to be included in the meta-analysis and did not respond to requests for additionalinformation (n = 74 approximately 59 unique samples)In total 29 publication were included in the meta-ana-lysis comprising 34 samples (one study included twoseparate birth cohorts and another four reported dataseparately for men and women)
Study characteristics
The characteristics of included samples are detailed inTable 1 Sample sizes ranged from 43 to 50 053 with amedian of 3395 The most common types of sampleswere school samples (934) community samples (834) and birth cohorts (734) The samples were major-ity white with two samples having exclusively blackparticipants Additionally eight samples were menonly six samples were women only and the restreported combined effect sizes Mean age of partici-pants at baseline ranged from 35 to 59 years with amedian of 12 years Most samples did not reportwhether comorbid diagnoses were present (2334)
Of the 74 papers excluded for having insufficient in-formation (representing 60 unique samples) the me-dian number of subjects was not statistically differentbetween those studies and the studies included in themeta-analysis (n = 288 and n = 3395 respectively p =019) nor did the average age of study participants atbaseline statistically differ (median across studies = 11
10 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
v 12 respectively p = 057) The types of cognitivemeasures used were also similar across the excludedand included studies with the most common measurebeing IQ (2860 and 2029) followed by VerbalComprehension (860 and 529)
Meta-analysis
The overall analysis yielded a significant associationbetween cognitive function and subsequent depressionoutcomes [r =minus0088 95 confidence interval (CI)minus0121 to minus0054 p lt 0001 Fig 2] Results were similarwhen excluding the two studies that used beta-weights(r =minus0071 95 CI minus0100 to minus0042 p lt 0001) orwhen using episodic memory in place of processingspeed in a study reporting both outcomes (r =minus008595 CI minus0118 to minus0051 p lt 0001) Follow-up ana-lyses were conducted in the sample of studies report-ing educational attainment and self-report outcomes(Supplementary Table S2) Heterogeneity across sam-ples was significant (Q = 80154 p lt 0001) suggestingsubstantial variation across the individual samplesThe ratio of the true heterogeneity to total variationwas large (I2 = 9588) I2 is on a relative scale andvalues close to 100 indicate that most of the observedvariance is real rather than spurious and suggeststhat subgroup analyses or meta-regression may helpto explain this variability (Borenstein et al 2011)
Subgroup analyses and meta-regression
A significant difference was found between categoricaland continuous effect sizes (p lt 0001) The studiesassessing continuous outcomes were found to have alarger effect (r =minus0121 95 CI minus0168 to minus0073 p lt0001 n = 22) than studies assessing categorical out-comes (r =minus0035 95 CI minus0054 to minus0017 p lt 0001n = 12) No differences were observed between studiesutilizing broad v specific cognitive measures (p = 057)
Outcomes were also compared adjusting for baselinedepression symptoms at the time of cognitive assess-ment Nine studies provided enough detail to calculatethe partial correlation coefficients adjusting for base-line depression symptoms Using the partial correl-ation coefficients led to a null result (r =minus0032 95CI minus0078 to 0014 p = 0169 n = 9 Fig 3) The nullresult does not seem to be due to a lack of power be-cause using the unadjusted correlation coefficients forthe same nine studies still led to a significant result(r =minus0120 95 CI minus0169 to minus0070 p lt 0001 n = 9Fig 3) As a follow-up the difference in effect sizes be-tween the adjusted and unadjusted values for these 9studies were tested (r = 0082 95 CI 0069ndash0095 p lt0001 n = 9) suggesting that the effects are significantlydifferent when directly comparing the values that doand do not control for baseline depression symptoms
Expanding the subgroup analyses to include studiesthat controlled for baseline depression plus other co-variates (Zammit et al 2004 Simons et al 2009 Rawalamp Rice 2012) and studies that explicitly excluded fora history of depression diagnosis (Gale et al 2008Vinberg et al 2013 Papmeyer et al 2015) did notchange the null result (r =minus0027 95 CI minus0058 to0005 p = 0097 n = 15)
None of the meta-regression analyses were signifi-cant indicating that the between-study variance wasnot attributable to age at baseline IQ percent of sam-ple that was female percent of the sample that waswhite age at follow-up time between assessmentsyear of cognitive assessment year of follow-up assess-ment or study quality score
Study quality and publication bias
Multiple samples within a study were combined forthe purposes of quality assessment given that studieswithin the same publication were found to employthe same methodology Of the 29 publications reviewed12 were rated as high quality and 17 were rated as me-dium quality Details are provided in SupplementaryTable S1 Comparable results to the overall findingswere obtained when just using high quality studies (r=minus0085 95 CI minus0141 to minus0029 p = 0003)
Inspection of the funnel plot (Fig 4) found no evi-dence for publication bias to support the hypothesisIn fact imputation of negative correlations suggestedthat additional studies favoring the hypothesis maybe missing While the calculated effect size is minus0088(95 CI minus0121 to minus0054) using Duval amp Tweediersquostrim-and-fill method the imputed effect size estimateis larger at minus0137 (95 CI minus0176 to minus0099 imputedstudies n = 11) Last the Fail-safe N procedure foundthat 3583 null studies would need to be located forthe combined two-tailed p value to exceed 005 Thissuggests that significant results are not likely to be con-founded by publication bias and may even underesti-mate true effect sizes
Discussion
The present systematic review and meta-analysis of 29longitudinal publications including 1 21 749 partici-pants revealed that after accounting for baseline depres-sion symptoms variability in cognitive function did notpredict subsequent depression Consistent with priorreports there was a significant contemporaneous associ-ation between higher depression symptoms and lowercognitive function These patterns have implications forunderstanding the association between cognitive func-tion and depression and may be important for advan-cing etiologic and treatment research
Association between cognitive function and subsequent depression 11
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
First our findings reinforce models positing thatcognitive function tracks with depression severity(McDermott amp Ebmeier 2009) One possible explan-ation for this contemporaneous association is that de-pression symptoms interfere with the capacity tocomplete cognitive assessments possibly through thegeneral lack of motivation that is one hallmark of thedisorder While this explanation represents an experi-mental confound for studies focused on assessmentof cognitive function it likewise represents an oppor-tunity for studies to focus more comprehensively onthe assessment of both depression and mood disordersymptoms since performance on cognitive tests maybe a sensitive measure of motivational state thatcould augment self-reported symptoms Alternativelythe co-occurrence of cognitive deficits and depressionsymptoms may reflect shared genetic etiology (Hagen-aars et al 2016) and dysfunction of neural circuits
supporting both cognitive and emotional processes(Scult et al 2016) In particular dysfunction of prefront-al and striatal circuits have been associated with bothdepression and cognitive function (Keedwell et al2005 Aarts et al 2011)
Second our findings suggest that prior studies oflinks between cognitive function and depression thatdid not assess baseline symptoms may have overesti-mated the potential protective role of higher cognitivefunction While the importance of accounting for sub-clinical symptoms is not novel the implementation ofsuch accounting is often neglected in psychiatric epi-demiology given the current categorical threshold-based diagnostic system In our meta-analysis largereffects were observed for continuous as compared tocategorical outcomes which aligns with growing em-phasis on dimensional measures of psychopathology(Cuthbert amp Kozak 2013)
Fig 2 Meta-analysis of the association between cognitive function and subsequent depression A forest plot for all studiesthat investigated associations between cognition and later depression Results are reported as correlation coefficients denotedby squares and 95 confidence intervals (CI) indicated by lines (effect sizes are converted to correlation coefficients ifreported as odds ratios) Meta-analysis results are displayed as the diamond The overall analysis found a significant effect ofcognition on depression (r =minus0088 95 CI minus0121 to minus0054 p lt 0001)
12 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Fig 4 Trim-and-fill funnel plots for all samples Fisherrsquos Z a measure of effect size is plotted on the x-axis and the standarderror is plotted on the y-axis Larger studies appear toward the top of the graph and smaller studies towards the bottom Inthe absence of publication bias the studies are symmetrically distributed around the mean Actual studies are shown in opencircles and imputed studies would be shown in black circles No additional studies would be expected in the oppositedirection (to the right) of the observed effect but an additional 11 studies are imputed to the left of the mean effect sizeWhile the calculated effect size is minus0088 [95 confidence interval (CI) minus0121 to minus0054] using Duval amp Tweediersquos trim-and-fill method the imputed effect size estimate is larger at minus0137 (95 CI minus0176 to minus0099 imputed studies n = 11)
Fig 3 Meta-analysis comparing values adjusted for baseline depression symptoms v unadjusted A forest plot for analysiscomparing results from a subset of the same set of studies reported in Fig 2 when using unadjusted values compared tousing values that are adjusted for baseline depression Effects are significant for unadjusted values [r =minus0120 95 confidenceinterval (CI) minus0169 to minus0070 p lt 0001] but not for adjusted values (r =minus0032 95 CI minus0078 to 0014 p = 0169) Results arereported as correlation coefficients denoted by squares and 95 CIs indicated by lines Meta-analysis results are displayed asdiamonds
Association between cognitive function and subsequent depression 13
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Third the associations between cognitive functionand either current or later depression were not moder-ated by data quality or participant age sex and raceHowever there are a number of additional potentialmoderators that could not be addressed in the currentreview and meta-analysis For example the numberand type of comorbid conditions with depressionwere often not reported in the included studies butcould represent an important moderator of theobserved effects Modeling the effects of comorbid ill-ness is an important avenue for future research
One limitation of the current literature is that only ahandful of studies reviewed explicitly excluded for de-pression diagnosis at baseline (Gale et al 2008 Vinberget al 2013 Papmeyer et al 2015) however consistentwith the finding that controlling for baseline depres-sion symptoms led to a null association between cogni-tion and subsequent depression there was no effectobserved when including these studies in the sub-group analyses further suggesting that the associationbetween cognitive function and depression is likelycontemporaneous It will be important to follow-upthese analyses with individual studies that includerigorous assessment of baseline depression symptomsand other potentially confounding factors to furtherclarify this relationship
An open question that remains for future research iswhether deficits in cognitive function are likely to pre-dict the development of more sever or recurrent de-pression later in life Only one of the included studies(Koenen et al 2009) specifically investigated recurrentdepression and found that lower IQ was associatedwith greater persistence of disorder
A final consideration is that while our review andmeta-analysis focused on general cognitive functionmainly assessed via IQ there may be specific subtypesof cognitive function that are more predictive of laterdepression For example a lack of cognitive flexibilitymay more closely match with the ruminative stylecharacteristic of depression and therefore tasks specifi-cally measuring this component of cognitive functionmight have some predictive utility While our reviewdid not find differences between broad and specificmeasures of cognitive function there were not enoughstudies identified to allow for precise consideration ofdifferences between individual cognitive domains
A limitation of the meta-analysis is that while thepresent study followed standard guidelines (Stroupet al 2000 Atkinson et al 2014) decisions aboutstudy selection data extraction and quality assess-ment include a number of decision points that neces-sarily involve a level of subjectivity Reliability wasascertained by using independent raters however dif-ferent inclusionexclusion criteria or a different ap-proach to the evaluation of those criteria could result
in a different set of studies being includedUltimately the quality of the meta-analysis is depend-ent upon the underlying studies that are analyzedFurthermore although studies with insufficient infor-mation to be included in the meta-analysis were notfound to differ based on basic study data from thosestudies included in the meta-analysis nonetheless itis unknown how if at all data from these studiescould change the overall results
Acknowledging these limitations our present reviewand meta-analysis found that while an association is evi-dent between cognitive function and later depressiongeneral cognitive function does not appear to be a riskfactor for depression but rather is more likely relatedto performance decrements associated with concurrentdepressive symptoms Our results suggest that low cog-nitive function is therefore probably not a causal factorof depression and that clinical practice may benefitmore from a focus on how decreased cognitive functionin the depressed state is likely to influence treatment out-comes (Gyurak et al 2015) Our findings have importantimplications for better understanding depression and forthe design of future studies in highlighting the need tocontrol for subthreshold depression symptoms when in-vestigating risk factors for mental illness as well as whenassessing cognitive function more generally
Supplementary material
The supplementary material for this article can befound at httpdxdoiorg101017S0033291716002075
Acknowledgements
MAS is supported by an National Science Foundation(NSF) Graduate Research Fellowship ARH is sup-ported by National Institutes of Health (NIH) grantsRO1DA033369 amp R01AG049789 TEM is supportedby National Institutes of Health (NIH) grantsR01AG049789 We would like to thank HarrisCooper PhD at Duke University who provided invalu-able insight into conducting the meta-analysis Wethank all of the authors of studies who provided add-itional information for this meta-analysis
Declaration of Interest
None
References
Aarts E van Holstein M Cools R (2011) Striatal dopamineand the interface between motivation and cognitionFrontiers in Psychology 2 163
14 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Atkinson KM Koenka AC Sanchez CE Moshontz HCooper H (2014) Reporting standards for literaturesearches and report inclusion criteria making researchsyntheses more transparent and easy to replicate ResearchSynthesis Methods 6 87ndash95
Baer LH Tabri N Blair M Bye D Li KZH Pushkar D(2013) Longitudinal associations of need for cognitioncognitive activity and depressive symptomatology withcognitive function in recent retirees Journals of GerontologySeries B Psychological Sciences and Social Sciences 68 655ndash664
Barbey AK Colom R Solomon J Krueger F Forbes CGrafman J (2012) An integrative architecture for generalintelligence and executive function revealed by lesionmapping Brain 135 1154ndash1164
Barnett JH Salmond CH Jones PB Sahakian BJ (2006)Cognitive reserve in neuropsychiatry Psychological Medicine36 1053ndash1064
Beaujean AA Parker S Qiu X (2013) The relationshipbetween cognitive ability and depression a longitudinaldata analysis Social Psychiatry and Psychiatric Epidemiology48 1983ndash1992
Belsky DW Caspi A Arseneault L Bleidorn W Fonagy PGoodman M Houts R Moffitt TE (2012) Etiologicalfeatures of borderline personality related characteristics in abirth cohort of 12-year-old children Development andPsychopathology 24 251ndash265
Betts KS Williams GM Najman JM Alati R (2016)Predicting spectrums of adult mania psychosis anddepression by prospectively ascertained childhoodneurodevelopment Journal of Psychiatric Research 72 22ndash29
Bora E Harrison BJ Yuumlcel M Pantelis C (2013) Cognitiveimpairment in euthymic major depressive disorder a meta-analysis Psychological Medicine 43 2017ndash2026
Borenstein M Hedges LV Higgins JPT Rothstein HR(2011) Introduction to Meta-Analysis John Wiley amp SonsWest Sussex UK
Canals J Domegravenech-Llaberia E Fernaacutendez-Ballart J Martiacute-Henneberg C (2002) Predictors of depression at eighteenA 7-year follow-up study in a Spanish nonclinicalpopulation European Child amp Adolescent Psychiatry 11226ndash233
Christensen H Griffiths K Mackinnon A (1997) Aquantitative review of cognitive deficits in depression andAlzheimer-type dementia Selection of Studies 3 631ndash651
Connolly SL Wagner Ca Shapero BG Pendergast LLAbramson LY Alloy LB (2014) Rumination prospectivelypredicts executive functioning impairments in adolescentsJournal of Behavior Therapy and Experimental Psychiatry 4546ndash56
Cooper HM (1979) Statistically combining independentstudies a meta-analysis of sex differences in conformityresearch Journal of Personality and Social Psychology 37131ndash146
Cooper HM (2010) Research Synthesis and Meta-Analysis AStep-by-Step Approach 4th edn SAGE PublicationsWashington (DC) USA
Cuijpers P de Graaf R van Dorsselaer S (2004) Minordepression risk profiles functional disability health careuse and risk of developing major depression Journal ofAffective Disorders 79 71ndash79
Cuthbert BN Kozak MJ (2013) Constructing constructs forpsychopathology the NIMH research domain criteriaJournal of Abnormal Psychology 122 928ndash937
Der G Batty GD Deary IJ (2009) The association between IQin adolescence and a range of health outcomes at 40 in the1979 US National Longitudinal Study of Youth Intelligence37 573ndash580
Dubow EF Boxer P Huesmann LR (2008) Childhood andadolescent predictors of early and middle adulthoodalcohol use and problem drinking the Columbia CountyLongitudinal Study Addiction 103 36ndash47
Duval S Tweedie R (2000) Trim and fill a simple funnel-plot-based method of testing and adjusting for publicationbias in meta-analysis Biometrics 56 455ndash463
Evans LD Kouros CD Samanez-Larkin S Garber J (2015)Concurrent and short-term prospective relations amongneurocognitive functioning coping and depressivesymptoms in youth Journal of Clinical Child and AdolescentPsychology 53 1ndash15
Franz CE Lyons MJ OrsquoBrien R Panizzon MS Kim K BhatR Grant MD Toomey R Eisen S Xian H Kremen WS(2011) A 35-year longitudinal assessment of cognition andmidlife depression symptoms the Vietnam Era Twin Studyof Aging American Association for Geriatric PsychiatryAmerican Journal of Geriatric Psychiatry 19 559ndash570
Gale CR Batty GD Tynelius P Deary IJ Rasmussen F(2010) Intelligence in early adulthood and subsequenthospitalization for mental disorders Epidemiology 2170ndash77
Gale CR Deary IJ Boyle SH Barefoot J Mortensen LHBatty GD (2008) Cognitive ability in early adulthood andrisk of 5 specific psychiatric disorders in middle age theVietnam experience study Archives of General Psychiatry 651410ndash1418
Gale CR Hatch SL Batty GD Deary IJ (2009) Intelligence inchildhood and risk of psychological distress in adulthoodthe 1958 National Child Development Survey and the 1970British Cohort Study Intelligence 37 592ndash599
Gjerde PF (1995) Alternative pathways to chronicdepressive symptoms in young adults gender differencesin developmental trajectories Child Development 661277ndash1300
Gottfredson LS (1997) Mainstream science on intelligence aneditorial with 52 signatories history and bibliographyIntelligence 24 13ndash23
Guyer AE Choate VR Grimm KJ Pine DS Keenan K(2011) Emerging depression is associated with facememory deficits in adolescent girls Elsevier Inc Journal ofthe American Academy of Child and Adolescent Psychiatry 50180ndash190
Gyurak A Patenaude B Korgaonkar MS Grieve SMWilliams LM Etkin A (2015) Frontoparietal activationduring response inhibition predicts remission toantidepressants in patients with major depression BiologicalPsychiatry 79 1ndash8
Hagenaars SP Harris SE Davies G Hill WD LiewaldDCM Ritchie SJ Marioni RE Fawns-Ritchie C Cullen BMalik R METASTROKE Consortium IC for BPGSpiroMeta Consortium CHARGE ConsortiumPulmonary Group CCA and LG Worrall BB Sudlow
Association between cognitive function and subsequent depression 15
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
CLM Wardlaw JM Gallacher J Pell J McIntosh AMSmith DJ Gale CR Deary IJ (2016) Shared geneticaetiology between cognitive functions and physical andmental health in UK Biobank (N = 112 151) and 24 GWASconsortiaMolecular Psychiatry Published online 26 January2016 doi101038mp2015225
Hatch SL Jones PB Kuh D Hardy R Wadsworth MEJRichards M (2007) Childhood cognitive ability and adultmental health in the British 1946 birth cohort Social Scienceamp Medicine (1982) 64 2285ndash2296
Hipwell AE Sapotichne B Klostermann S Battista DKeenan K (2011) Autobiographical memory as a predictorof depression vulnerability in girls Journal of Clinical Childand Adolescent Psychology 40 254ndash265
Horowitz JL Garber J (2003) Relation of intelligence andreligiosity to depressive disorders in offspring of depressedand nondepressed mothers The American Academy ofChild and Adolescent Psychiatry Journal of the AmericanAcademy of Child and Adolescent Psychiatry 42 578ndash586
Johnson W Bouchard TJ Krueger RF McGue MGottesman II (2004) Just one g consistent results fromthree test batteries Intelligence 32 95ndash107
Keedwell PA Andrew C Williams SCR Brammer MJPhillips ML (2005) The neural correlates of anhedoniain major depressive disorder Biological Psychiatry 58843ndash853
Kessler RC Berglund P Demler O Jin R Koretz DMerikangas KR Rush AJ Walters EE Wang PS (2003)The epidemiology of major depressive disorder resultsfrom the National Comorbidity Survey Replication(NCS-R) Journal of the American Medical Association 2893095ndash3105
Koenen KC Moffitt TE Roberts AL Martin LT KubzanskyL Harrington H Poulton R Caspi A (2009) Childhood IQand adult mental disorders a test of the cognitive reservehypothesis American Journal of Psychiatry 166 50ndash57
Lewinsohn PM Solomon A Seeley JR Zeiss A (2000)Clinical implications of lsquosubthresholdrsquo depressivesymptoms Journal of Abnormal Psychology 109 345ndash351
Luppino FS de Wit LM Bouvy PF Stijnen T Cuijpers PPenninx BWJH Zitman FG (2010) Overweight obesityand depression a systematic review and meta-analysisof longitudinal studies Archives of General Psychiatry 67220ndash229
McCord J Ensminger ME (1997) Multiple risks andcomorbidity in an African-American population CriminalBehaviour and Mental Health 7 339ndash352
McDermott LM Ebmeier KP (2009) A meta-analysis ofdepression severity and cognitive function Elsevier BVJournal of Affective Disorders 119 1ndash8
Melartin TK Rytsaumllauml HJ Leskelauml US Lestelauml-Mielonen PSSokero TP Isometsauml ET (2002) Current comorbidity ofpsychiatric disorders among DSM-IV major depressivedisorder patients in psychiatric care in the VantaaDepression Study Journal of Clinical Psychiatry 63 126ndash134
Meyer SE Carlson GA Wiggs EA Martinez PE RonsavilleDS KlimesndashDougan B Gold PW RadkendashYarrow M(2004) A prospective study of the association amongimpaired executive functioning childhood attentional
problems and the development of bipolar disorderDevelopment and Psychopathology 16 461ndash476
MiyakeA FriedmanNP EmersonMJWitzki aHHowerter AWager TD (2000) The unity and diversity of executivefunctions and their contributions to complex lsquoFrontal Lobersquotasks a latentvariable analysisCognitive Psychology41 49ndash100
Moher D Liberati A (2009) Preferred reporting items forsystematic reviews and meta-analyses the PRISMAstatement Annals of Internal Medicine 151 264ndash269
Papmeyer M Sussmann JE Hall J McKirdy J Peel AMacdonald A Lawrie SM Whalley HC McIntosh AM(2015) Neurocognition in individuals at high familial riskof mood disorders with or without subsequent onset ofdepression Psychological Medicine 45 1ndash11
Peterson RA Brown SP (2005) On the use of betacoefficients in meta-analysis Journal of Applied Psychology90 175ndash181
Pine DS Cohen P Brook J Coplan JD (1997) Psychiatricsymptoms in adolescence as predictors of obesity in earlyadulthood a longitudinal study American Journal of PublicHealth 87 1303ndash1310
Quinn ME Joormann J (2015) Control when it countschange in executive control under stress predicts depressionsymptoms Emotion Junio 22 1ndash10
Rawal A Rice F (2012) Examining overgeneralautobiographical memory as a risk factor for adolescentdepression Elsevier Inc Journal of the American Academy ofChild and Adolescent Psychiatry 51 518ndash527
Ree MJ Earles JA (1991) The stability of g across differentmethods of estimation Intelligence 15 271ndash278
Rock PL Roiser JP Riedel WJ Blackwell AD (2014)Cognitive impairment in depression a systematic reviewand meta-analysis Psychological Medicine 44 2029ndash2040
Rogers MA Kasai K Koji M Fukuda R Iwanami ANakagome K Fukuda M Kato N (2004) Executive andprefrontal dysfunction in unipolar depression a review ofneuropsychological and imaging evidence NeuroscienceResearch 50 1ndash11
Scult MA Knodt AR Swartz JR Brigidi BD Hariri AR(2016) Thinking and feeling individual differences inhabitual emotion regulation and stress-related mood areassociated with prefrontal executive control ClinicalPsychological Science doi1011772167702616654688
Sharp C Petersen N Goodyer I (2008) Emotional reactivityand the emergence of conduct problems and emotionalsymptoms in 7- to 11-year-olds a 1-year follow-up studyJournal of the American Academy of Child and AdolescentPsychiatry 47 565ndash573
Siegel LS (1999) Issues in the definition and diagnosis oflearning disabilities a perspective on Guckenberger vBoston University Journal of Learning Disabilities 32 304ndash319
Simons CJP Jacobs N Derom C Thiery E Jolles J van Os JKrabbendam L (2009) Cognition as predictor of currentand follow-up depressive symptoms in the generalpopulation Acta Psychiatrica Scandinavica 120 45ndash52
Slykerman RF Thompson J Waldie K Murphy R Wall CMitchell EA (2015) Maternal stress during pregnancy isassociated with moderate to severe depression in 11-year-old children Acta Paediatrica 104 68ndash74
16 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Snyder HR (2013) Major depressive disorder is associatedwith broad impairments on neuropsychological measuresof executive function a meta-analysis and reviewPsychological Bulletin 139 81ndash132
Soslashrensen HJ Saeligbye D Urfer-Parnas A Mortensen ELParnas J (2012) Premorbid intelligence and educationallevel in bipolar and unipolar disorders a Danish draftboard study Journal of Affective Disorders 136 1188ndash1191
SpearmanC (1904) lsquoGeneral intelligencersquoobjectivelydeterminedandmeasuredAmerican Journal of Psychology 15 201
Stern Y (2003) The concept of cognitive reserve a catalyst forresearch Journal of Clinical and Experimental Neuropsychology(Neuropsychology Development and Cognition Section A) 25589ndash593
Stroup D Berlin J Morton S Olkin I Williamson GDRennie D Moher D Becker BJ Sipe TA Thacker SB(2000) Meta-analysis of Observational Studies inEpidemiology a proposal for reporting Journal of theAmerican Medical Association 283 2008
Vinberg M Miskowiak KW Kessing LV (2013) Impairmentof executive function and attention predicts onset ofaffective disorder in healthy high-risk twins Journal ofClinical Psychiatry 74 e747ndashe753
Zammit S Allebeck P David AS Dalman C HemmingssonT Lundberg I Lewis G (2004) A longitudinal study ofpremorbid IQ Score and risk of developing schizophreniabipolar disorder severe depression and other nonaffectivepsychoses Archives of General Psychiatry 61 354ndash360
Association between cognitive function and subsequent depression 17
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms

Gale et al(2009)(1970Cohort)
1970 BritishCohort Study
Birth cohort 6074 NR Studyassessment
1018 British abilityScale
General Intelligence Rutterrsquos MalaiseInventory
Continuous None NR (bothmaleandfemale)
NR Europe 10 20 1980
Gjerde(1995)(females)
NR Recruited froma nurseryschool
51 NR Studyassessment
1187 Wechsler AdultIntelligenceScale (WAIS)
General Intelligence General BehaviorInventory (GBI)Depression scale
Continuous None 100 sim66 Whitesim25Blacksim005Asian
NorthAmerica
18 5 1983
Gjerde et al(1995)(males)
NR Recruited froma nurseryschool
45 NR Studyassessment
11112 Wechsler AdultIntelligenceScale (WAIS)
General Intelligence General BehaviorInventory (GBI)Depression scale
Continuous None 0 sim66 Whitesim25 Blacksim005Asian
NorthAmerica
18 5 1983
Hatch et al(2007)
1946 BritishCohort Study
Birth cohort 957 NR Studyassessment
NR NationalFoundationforEducationalResearch Test
General IntelligenceVerbalComprehensionPerceptualReasoning
General HealthQuestionnaire(GHQ-28)-severedepressionsubscale
Continuous None 51 NR Europe 8 45 1954
Hipwellet al (2011)
PittsburghGirls Study(PGS)
Communitysample
195 NR Studyassessment
9954 WechslerIntelligenceScale forChildren(WISC) III-R
VerbalComprehension
Schedule forAffectiveDisorders forSchool-AgeChildren-Present andLifetime Version(K-SADS-PL)
Continuous Depressionsymptoms atTime 1
100 70 Black ormultiracial
NorthAmerica
1154 1 1998
Horowitz ampGarber(2003)
NR Elementaryschool cohort
196 NR Studyassessment
10461 WechslerIntelligenceScale forChildren(WISC) -R
General IntelligenceVerbalComprehensionPerceptualReasoning
Schedule forAffectiveDisorders forSchool-AgeChildren-EpidemiologicalVersion(K-SADS-E)
Categorical Depressionsymptoms atTime 1
542 89 White147 Black33 Other
NorthAmerica
1186 6 sim1980
Koenenet al (2009)
DunedinCohort
Birth cohort 730 None Studyassessment
NR WechslerIntelligenceScale forChildren(WISC)
General IntelligenceVerbalComprehensionPerceptualReasoning WorkingMemory ProcessingSpeed
DiagnosticInterviewAssessment (forDSM-IV)
Categorical SexSocioeconomicStatusPhysicalHealthchildhoodmaltreatment
48 lsquoPrimarilyWhitersquo
NewZealand
9 23 1981
McCord ampEnsminger(1997)(females)
WoodlawnCohort
Elementaryschool cohort
346 Some withalcoholism
Studyassessment
NR (13 Unspecified IQof sample had scoresover 110)
General Intelligence CompositeInternationalInterviewSchedule(according toDSM-III-R)
Categorical None 100 100 Black NorthAmerica
sim6 27 1966
McCord ampEnsminger(1997)(males)
WoodlawnCohort
Elementaryschool cohort
313 Some withalcoholism
Studyassessment
NR (11 Unspecified IQof sample had scoresover 110)
General Intelligence CompositeInternationalInterviewSchedule(according toDSM-III-R)
Categorical None 0 100 Black NorthAmerica
sim6 27 1966
Meyer et al(2004)
NR Risk sample 86 NR Studyassessment
sim118 WISC General IntelligenceVerbalComprehensionPerceptualReasoning
SCID Categorical None 63 90 White9 Black 1Hispanic
NorthAmerica
11 13 1989
Association
between
cognitivefunction
andsubsequent
depression5
httpdxdoiorg101017S0033291716002075D
ownloaded from
httpww
wcam
bridgeorgcore Duke U
niversity Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core term
s of use available at httpww
wcam
bridgeorgcoreterms
Table 1 (cont)
StudyName ofcohort Type of cohort
Samplesize Comorbidity
Howdepressionassessed
Mean IQatbaseline
Name ofcognitivemeasure
Type of cognitivemeasure
Name ofdepressionoutcome
Type ofdepressionoutcome
Covariatesincluded inmeta-analysisa
Percentfemale Raceethnicity Continent
Meanage atbaseline
Timebetweenassessments(years)
Year ofinitialassessment
Papmeyeret al (2015)
ScottishBipolarFamily Study
Risk sample 111 NR Studyassessment
Controls108Patients107
National AdultReading Test(NART)
VerbalComprehension
Structured ClinicalInterview forDSM Disorders(SCID)symptoms
Categorical None 52 NR Europe 21 2 NR
Pine et al(1997)
NR Communitysample
644 NR Studyassessment
1007 UnspecifiedlsquoIQrsquo
General Intelligence Based onDiagnosticInterviewSchedule forChildren
Continuous Depressionsymptoms atTime 1
52 91 White NorthAmerica
138 9 1983
Quinn ampJoormann(2015)
NR Undergraduatestudents
43 NR Studyassessment
NR n-back Working Memory Beck DepressionInventory II(BDI-II)
Continuous Depressionsymptoms atTime 1
63 58 White30Hispanic orLatino 19Asian 2AfricanAmerican2AmericanIndian 2NativeHawaiian2 Indian
NorthAmerica
19 014 NR
Rawal ampRice (2012)
EarlyPrediction ofAdolescentDepressionstudy
Risk sample 230 None Studyassessment
9746 WechslerIntelligenceScale forChildren(WISC)
General IntelligenceVerbalComprehensionPerceptualReasoning WorkingMemory ProcessingSpeed
Child andAdolescentPsychiatricAssessment(CAPA)
Both Depressionsymptoms atTime 1 AgeOvergeneralityto negativecues
596 NR Europe 1371 1 NR
Sharp et al(2008)
The ChildBehaviourStudy
Communitysample
439 NR Studyassessment
105 WechslerIntelligenceScale forChildren(WISC)
General IntelligenceVerbalComprehensionPerceptualReasoning
The Mood andFeelingsQuestionnaire
Continuous Depressionsymptoms atTime 1
52 97 White05 Black25 Asian
Europe 94 1 NR
Simons et al(2009)
East FlandersProspectiveTwin Survey
Twin registry 444 NR Studyassessment
NR Principalcomponentfrom StroopConceptShifting Testand LetterDigitSubstitutionTest
Processing SpeedSet-ShiftingInhibition
Structured ClinicalInterview forDSM Disorders(SCID)symptoms
Continuous Depressionsymptoms atTime 1
100 NR Europe 28 2 NR
6MA
Scultet
al
httpdxdoiorg101017S0033291716002075D
ownloaded from
httpww
wcam
bridgeorgcore Duke U
niversity Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core term
s of use available at httpww
wcam
bridgeorgcoreterms
Slykermanet al (2015)
AucklandBirthweightCollaborativeStudy
Birth cohortrisk sample
609 NR Studyassessment
NR Stanford-BinetIntelligenceScale 4th Ed
General IntelligenceFluid ReasoningKnowledgeQunatitativeReasoningVisual-SpatialProcessingWorking Memory
Center forEpidemiologicalStudiesDepression Scale(CES-D)
Categorical(cut-point)
None 49 NR NewZealand
35 75 sim2000
Soslashrensenet al (2012)
DanishDraft-BoardStudy
Military cohort 21 914 NR Psychiatricregistry
Controls100Patients96ndash98
Boslashrge PriensProslashve (BPP)
General IntelligenceVerbalComprehensionPerceptualReasoning
DanishInternationalClassification ofdiseases (ICD) 8amp 10
Categorical None 0 NR Europe 195 sim36 1968ndash1989
Vinberget al (2013)
NR High-risktwins
224 Bipolardisorderanxietysubstanceabuse other
Studyassessmentpsychiatricregistry
NR CambridgeCognitiveAssessment(CAMCOG)
GeneralNeuropsychologicalFunctionOrientationLanugage MemoryAttention AbstractThinking VisualPerception
Beck DepressionInventory (BDI)
Continuous Depressionsymptoms atTime 1
65 NR Europe 439 7 2003
Zammitet al (2004)
SwedishConscripts(1969ndash1970)
Military cohort 50 053 None Hospitallinkage
NR UnspecifiedlsquoIQrsquo
General IntelligenceVerbalComprehensionPerceptualReasoning GeneralKnowledgeMechanicalKnowledge
InternationalClassification ofdiseases (ICD)hospitalpsychiatricadmissions
Categorical Diagnosis atbaselinedisturbedbehavior druguse raised in acity
0 NR Europe sim19 27 1969
Sample size is the number of subjects included in reported analyses of interest NR not reportedsim indicates only a range was reporteda This column notes covariates included in the meta-analysis We focused on controlling for depressive symptoms at T1 but some studies reported effect sizes that also included controlling
for other variables ndash when the zero-order correlations were unavailable these estimates were used
Association
between
cognitivefunction
andsubsequent
depression7
httpdxdoiorg101017S0033291716002075D
ownloaded from
httpww
wcam
bridgeorgcore Duke U
niversity Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core term
s of use available at httpww
wcam
bridgeorgcoreterms
to investigate general information processing abilitiesrather than cognitive attributional style studies withcognitive attribution measures as the sole cognitivemeasure were excluded
Comparisons
Search terms used to indicate the possible associationbetween cognitive function and depression includedrisk premorbid prodromal onset predict and association(for a full list see search terms in the SupplementaryMaterial) When data were reported from multipletime-points the analysis accounting for the longesttime between assessments was used
Outcomes
Eligible studies reported depression diagnosis orsymptoms determined by investigator or self-reportPresence of comorbidity was permitted given that de-pression has been found to be highly comorbid withother disorders (Melartin et al 2002 Kessler et al2003) Articles not adequately specifying how depres-sion was assessed or articles that did not uniquelymeasure depression [ie only had an index of lsquomentaldisordersrsquo or the category of lsquomood disordersrsquo lumpedtogether (Gale et al 2010)] were excluded if no uniquemeasure of depression could be obtained from studyauthors This is because although comorbidity waspermitted these could have represented instances ofpure anxiety disorders with few or no depressivesymptoms or instances of bipolar disorder
Study design
Eligible study search terms included cohort studies lon-gitudinal epidemiological prospective retrospective follow-up or case-control studies Studies not following a longi-tudinal design were excluded during full-text reviewAdditionally studies where cognitive function wasassessed only concurrently with or after depressionwere excluded given that the purpose of the reviewwas to investigate whether cognitive function pre-dicted later depression
Studies were included regardless of whether theywere reported in peer-review journals in order to ac-count for potentially biased reporting of resultsReview articles were included in the search terms tofind additional relevant references but were notincluded in the meta-analysis Baseline and protocolstudies without follow-up data were excluded
Study selection
A flow diagram of the process of study selection showsthe overall procedures (Fig 1) Records identified fromthe search processes were combined in EndNote
software version X7 and duplicates were removedTitles and abstracts were reviewed independently bytwo reviewers (MS and AP) according to the eligibil-ity criteria described above and marked as either po-tentially eligible or not eligible If either authormarked an article as potentially eligible it wasincluded in the full-text review for closer examinationby MS and AP who used an electronic form to indi-cate if an article should be included or excluded in thefinal selection When an article was excluded the rea-son for exclusion was selected from a hierarchical listof exclusion criteria presented in Fig 1 Both MSand AP were initially blinded to the otherrsquos decisionsAfter both MS and AP completed their reviews dis-crepancies about whether a study should be includedor excluded were resolved via discussion and consen-sus amongst MS AP TM AH and TS
Data extraction
Study information was extracted independently byMS and AP using an electronic form created forthis study Information was collected and codedbased on report characteristics participant characteris-tics study setting predictors outcome measures andquality assessment (Cooper 2010) Any discrepancies(approximately 3 of data points) were resolved viaconsensus
For studies with categorical depression diagnoses ef-fect sizes were generally presented as odds ratios Forthese studies the odds ratio plus the upper and lowerbound of the confidence interval were recorded Twoof the studies (Zammit et al 2004 Gale et al 2008)reported odds ratios greater than one to indicate thatlower IQ was associated with greater risk of depressionThe other studies reported odds ratios in the reverseleading to odds ratios less than one for the same direc-tion of the effect Therefore the odds ratios from the firsttwo studies were recalculated by dividing (1oddsratio) Another study (McCord amp Ensminger 1997)reported results from chi-squared tests Additional stud-ies reported mean premorbid IQ scores rather than oddsratios in which case the means sample sizes andor pvalues and number of tails of the t test were utilizedto calculate the effect size
For studies in which depression was measured as acontinuous variable effect sizes were presented as cor-relation coefficients The direction of the effect (posi-tive or negative) and the sample size were alsoextracted to be used in the meta-analysis Two studiesreported only beta weights (Simons et al 2009 Rawalamp Rice 2012) and we were not able to obtain zero-order correlations from the authors Given that previ-ous reports have suggested that beta weights can beused as an estimate of correlation coefficients in
8 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
meta-analysis (Peterson amp Brown 2005) the betaweights were used instead and analyses were runboth including and excluding these data points
When insufficient information was presented in thearticle authors were contacted requesting further de-tail An additional six studies were included at thispoint One study (Hatch et al 2007) included effectsizes for the female half of the cohort and did not pro-vide statistics for the males but did indicate a null ef-fect Only women from this study were included in themeta-analyses but imputing a score of 0 for the malesyielded similar overall results
Follow-up analyses directly compared studies thatreported zero-order correlations between IQ at time
1 depression at time 1 and depression at time 2(additional details described in the SupplementaryMethods)
Statistical methods
Data were analyzed using Comprehensive Meta-Analysis software version 30 (Biostat Inc USA) Arandom-effects model was used for expected hetero-geneity across studies A random-effects model alsoallows for broader generalization of results to thepopulation at large Heterogeneity of effects was calcu-lated using the Q statistic where a significant p valueindicates that true effect varies across studies The I2
Fig 1 Flow diagram of the search process
Association between cognitive function and subsequent depression 9
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
statistic was used to calculate the ratio of the true het-erogeneity to total variation acting as an index of sig-nal-to-noise ratio When I2 is large it is has beenrecommended to consider subgroup analysis or meta-regression to account for the variance (Borensteinet al 2011)
Subgroup analyses were conducted using a mixed-effects analysis in which a random effects model wasused to combine studies within each subgroup and afixed effect model was used to combine subgroupsand yield the overall effect (the study-to-study vari-ance is not assumed to be the same for all subgroups)Subgroup analyses were conducted comparing type ofoutcome (continuous v categorical) broad v specificcognitive measures and outcomes that were adjustedv unadjusted for baseline depression symptoms
Meta-regression was performed using the followingvariables on unadjusted analyses age at baseline ageat follow-up time between assessments IQ percentwhite year of cognitive assessment year of follow-upassessment percent female and study quality score
Study quality and publication bias
Study quality was evaluated independently by MSand AP using a checklist adapted from Luppino ampWit (Luppino et al 2010) The checklist contained 12items and studies were rated with a lsquo+rsquo if it met criteriafor that item a lsquominusrsquo if it did not meet criteria for an itemand a rsquorsquo if unclear lsquo+rsquo were coded as a score of 1 andminus were coded as a score of 0 Total scores and percen-tages were calculated Articles with total scores of 0ndash3were considered to be of low quality scores of 4ndash7were considered a medium quality and scores of 8ndash12 were considered to be of high quality Any discrep-ancies (approximately 3 of data points) wereresolved via consensus
Publication bias was assessed using a funnel plotwhich presents study size on the vertical axis (as stand-ard error in this case) as a function of effect size on thex-axis When no publication bias exists the studiesshould be distributed symmetrically about the com-bined effect size (Borenstein et al 2011) If evidenceof publication bias was observed Duval amp Tweediersquostrim-and-fill method was used (Duval amp Tweedie2000) which recalculates effects based on imputingdata from studies that are likely to be missing Lastthe Fail-safe N was calculated (Cooper 1979) whichindicates the number of missing studies that wouldneed to exist to nullify the observed effect
Results
A flow diagram of the search process is shown inFig 1 The search identified 2773 records through
PubMed 2158 through EMBASE and 1345 throughPsycINFO for a total of 6276 records Duplicaterecords (1709) were removed in EndNote resulting in4567 unique records After title and abstracts werereviewed 329 records were identified as potentially eli-gible for the meta-analysis These 329 records werereviewed in full and 300 articles were excluded hier-archically if they were a review baseline or protocolpaper (n = 6) if the sample had a mean age over 65at the depression assessment (n = 41) if the samplehad a specific medical illness (n = 23) if the studywas not a longitudinal design (n = 19) if MDD diagno-sis hospitalization or admission to treatment centerwas part of the inclusion criteria of the study (n = 18)if cognitive function was assessed only concurrentlywith or after depression (n = 36) if cognitive functionwas assessed by educational achievement or self-report(n = 26) if cognitive function was assessed by attribu-tion style rather than neuropsychological measure (n= 7) if there was no measure of cognitive function (n= 18) or no uniquely measured depression outcome(n = 24) Furthermore if articles reported on the samesample as another article with higher quality or moreinformation the duplicate articles were excluded (n =8) Last a number of studies appeared to measureboth cognitive function and depression but did not re-port enough information to be included in the meta-analysis and did not respond to requests for additionalinformation (n = 74 approximately 59 unique samples)In total 29 publication were included in the meta-ana-lysis comprising 34 samples (one study included twoseparate birth cohorts and another four reported dataseparately for men and women)
Study characteristics
The characteristics of included samples are detailed inTable 1 Sample sizes ranged from 43 to 50 053 with amedian of 3395 The most common types of sampleswere school samples (934) community samples (834) and birth cohorts (734) The samples were major-ity white with two samples having exclusively blackparticipants Additionally eight samples were menonly six samples were women only and the restreported combined effect sizes Mean age of partici-pants at baseline ranged from 35 to 59 years with amedian of 12 years Most samples did not reportwhether comorbid diagnoses were present (2334)
Of the 74 papers excluded for having insufficient in-formation (representing 60 unique samples) the me-dian number of subjects was not statistically differentbetween those studies and the studies included in themeta-analysis (n = 288 and n = 3395 respectively p =019) nor did the average age of study participants atbaseline statistically differ (median across studies = 11
10 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
v 12 respectively p = 057) The types of cognitivemeasures used were also similar across the excludedand included studies with the most common measurebeing IQ (2860 and 2029) followed by VerbalComprehension (860 and 529)
Meta-analysis
The overall analysis yielded a significant associationbetween cognitive function and subsequent depressionoutcomes [r =minus0088 95 confidence interval (CI)minus0121 to minus0054 p lt 0001 Fig 2] Results were similarwhen excluding the two studies that used beta-weights(r =minus0071 95 CI minus0100 to minus0042 p lt 0001) orwhen using episodic memory in place of processingspeed in a study reporting both outcomes (r =minus008595 CI minus0118 to minus0051 p lt 0001) Follow-up ana-lyses were conducted in the sample of studies report-ing educational attainment and self-report outcomes(Supplementary Table S2) Heterogeneity across sam-ples was significant (Q = 80154 p lt 0001) suggestingsubstantial variation across the individual samplesThe ratio of the true heterogeneity to total variationwas large (I2 = 9588) I2 is on a relative scale andvalues close to 100 indicate that most of the observedvariance is real rather than spurious and suggeststhat subgroup analyses or meta-regression may helpto explain this variability (Borenstein et al 2011)
Subgroup analyses and meta-regression
A significant difference was found between categoricaland continuous effect sizes (p lt 0001) The studiesassessing continuous outcomes were found to have alarger effect (r =minus0121 95 CI minus0168 to minus0073 p lt0001 n = 22) than studies assessing categorical out-comes (r =minus0035 95 CI minus0054 to minus0017 p lt 0001n = 12) No differences were observed between studiesutilizing broad v specific cognitive measures (p = 057)
Outcomes were also compared adjusting for baselinedepression symptoms at the time of cognitive assess-ment Nine studies provided enough detail to calculatethe partial correlation coefficients adjusting for base-line depression symptoms Using the partial correl-ation coefficients led to a null result (r =minus0032 95CI minus0078 to 0014 p = 0169 n = 9 Fig 3) The nullresult does not seem to be due to a lack of power be-cause using the unadjusted correlation coefficients forthe same nine studies still led to a significant result(r =minus0120 95 CI minus0169 to minus0070 p lt 0001 n = 9Fig 3) As a follow-up the difference in effect sizes be-tween the adjusted and unadjusted values for these 9studies were tested (r = 0082 95 CI 0069ndash0095 p lt0001 n = 9) suggesting that the effects are significantlydifferent when directly comparing the values that doand do not control for baseline depression symptoms
Expanding the subgroup analyses to include studiesthat controlled for baseline depression plus other co-variates (Zammit et al 2004 Simons et al 2009 Rawalamp Rice 2012) and studies that explicitly excluded fora history of depression diagnosis (Gale et al 2008Vinberg et al 2013 Papmeyer et al 2015) did notchange the null result (r =minus0027 95 CI minus0058 to0005 p = 0097 n = 15)
None of the meta-regression analyses were signifi-cant indicating that the between-study variance wasnot attributable to age at baseline IQ percent of sam-ple that was female percent of the sample that waswhite age at follow-up time between assessmentsyear of cognitive assessment year of follow-up assess-ment or study quality score
Study quality and publication bias
Multiple samples within a study were combined forthe purposes of quality assessment given that studieswithin the same publication were found to employthe same methodology Of the 29 publications reviewed12 were rated as high quality and 17 were rated as me-dium quality Details are provided in SupplementaryTable S1 Comparable results to the overall findingswere obtained when just using high quality studies (r=minus0085 95 CI minus0141 to minus0029 p = 0003)
Inspection of the funnel plot (Fig 4) found no evi-dence for publication bias to support the hypothesisIn fact imputation of negative correlations suggestedthat additional studies favoring the hypothesis maybe missing While the calculated effect size is minus0088(95 CI minus0121 to minus0054) using Duval amp Tweediersquostrim-and-fill method the imputed effect size estimateis larger at minus0137 (95 CI minus0176 to minus0099 imputedstudies n = 11) Last the Fail-safe N procedure foundthat 3583 null studies would need to be located forthe combined two-tailed p value to exceed 005 Thissuggests that significant results are not likely to be con-founded by publication bias and may even underesti-mate true effect sizes
Discussion
The present systematic review and meta-analysis of 29longitudinal publications including 1 21 749 partici-pants revealed that after accounting for baseline depres-sion symptoms variability in cognitive function did notpredict subsequent depression Consistent with priorreports there was a significant contemporaneous associ-ation between higher depression symptoms and lowercognitive function These patterns have implications forunderstanding the association between cognitive func-tion and depression and may be important for advan-cing etiologic and treatment research
Association between cognitive function and subsequent depression 11
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
First our findings reinforce models positing thatcognitive function tracks with depression severity(McDermott amp Ebmeier 2009) One possible explan-ation for this contemporaneous association is that de-pression symptoms interfere with the capacity tocomplete cognitive assessments possibly through thegeneral lack of motivation that is one hallmark of thedisorder While this explanation represents an experi-mental confound for studies focused on assessmentof cognitive function it likewise represents an oppor-tunity for studies to focus more comprehensively onthe assessment of both depression and mood disordersymptoms since performance on cognitive tests maybe a sensitive measure of motivational state thatcould augment self-reported symptoms Alternativelythe co-occurrence of cognitive deficits and depressionsymptoms may reflect shared genetic etiology (Hagen-aars et al 2016) and dysfunction of neural circuits
supporting both cognitive and emotional processes(Scult et al 2016) In particular dysfunction of prefront-al and striatal circuits have been associated with bothdepression and cognitive function (Keedwell et al2005 Aarts et al 2011)
Second our findings suggest that prior studies oflinks between cognitive function and depression thatdid not assess baseline symptoms may have overesti-mated the potential protective role of higher cognitivefunction While the importance of accounting for sub-clinical symptoms is not novel the implementation ofsuch accounting is often neglected in psychiatric epi-demiology given the current categorical threshold-based diagnostic system In our meta-analysis largereffects were observed for continuous as compared tocategorical outcomes which aligns with growing em-phasis on dimensional measures of psychopathology(Cuthbert amp Kozak 2013)
Fig 2 Meta-analysis of the association between cognitive function and subsequent depression A forest plot for all studiesthat investigated associations between cognition and later depression Results are reported as correlation coefficients denotedby squares and 95 confidence intervals (CI) indicated by lines (effect sizes are converted to correlation coefficients ifreported as odds ratios) Meta-analysis results are displayed as the diamond The overall analysis found a significant effect ofcognition on depression (r =minus0088 95 CI minus0121 to minus0054 p lt 0001)
12 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Fig 4 Trim-and-fill funnel plots for all samples Fisherrsquos Z a measure of effect size is plotted on the x-axis and the standarderror is plotted on the y-axis Larger studies appear toward the top of the graph and smaller studies towards the bottom Inthe absence of publication bias the studies are symmetrically distributed around the mean Actual studies are shown in opencircles and imputed studies would be shown in black circles No additional studies would be expected in the oppositedirection (to the right) of the observed effect but an additional 11 studies are imputed to the left of the mean effect sizeWhile the calculated effect size is minus0088 [95 confidence interval (CI) minus0121 to minus0054] using Duval amp Tweediersquos trim-and-fill method the imputed effect size estimate is larger at minus0137 (95 CI minus0176 to minus0099 imputed studies n = 11)
Fig 3 Meta-analysis comparing values adjusted for baseline depression symptoms v unadjusted A forest plot for analysiscomparing results from a subset of the same set of studies reported in Fig 2 when using unadjusted values compared tousing values that are adjusted for baseline depression Effects are significant for unadjusted values [r =minus0120 95 confidenceinterval (CI) minus0169 to minus0070 p lt 0001] but not for adjusted values (r =minus0032 95 CI minus0078 to 0014 p = 0169) Results arereported as correlation coefficients denoted by squares and 95 CIs indicated by lines Meta-analysis results are displayed asdiamonds
Association between cognitive function and subsequent depression 13
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Third the associations between cognitive functionand either current or later depression were not moder-ated by data quality or participant age sex and raceHowever there are a number of additional potentialmoderators that could not be addressed in the currentreview and meta-analysis For example the numberand type of comorbid conditions with depressionwere often not reported in the included studies butcould represent an important moderator of theobserved effects Modeling the effects of comorbid ill-ness is an important avenue for future research
One limitation of the current literature is that only ahandful of studies reviewed explicitly excluded for de-pression diagnosis at baseline (Gale et al 2008 Vinberget al 2013 Papmeyer et al 2015) however consistentwith the finding that controlling for baseline depres-sion symptoms led to a null association between cogni-tion and subsequent depression there was no effectobserved when including these studies in the sub-group analyses further suggesting that the associationbetween cognitive function and depression is likelycontemporaneous It will be important to follow-upthese analyses with individual studies that includerigorous assessment of baseline depression symptomsand other potentially confounding factors to furtherclarify this relationship
An open question that remains for future research iswhether deficits in cognitive function are likely to pre-dict the development of more sever or recurrent de-pression later in life Only one of the included studies(Koenen et al 2009) specifically investigated recurrentdepression and found that lower IQ was associatedwith greater persistence of disorder
A final consideration is that while our review andmeta-analysis focused on general cognitive functionmainly assessed via IQ there may be specific subtypesof cognitive function that are more predictive of laterdepression For example a lack of cognitive flexibilitymay more closely match with the ruminative stylecharacteristic of depression and therefore tasks specifi-cally measuring this component of cognitive functionmight have some predictive utility While our reviewdid not find differences between broad and specificmeasures of cognitive function there were not enoughstudies identified to allow for precise consideration ofdifferences between individual cognitive domains
A limitation of the meta-analysis is that while thepresent study followed standard guidelines (Stroupet al 2000 Atkinson et al 2014) decisions aboutstudy selection data extraction and quality assess-ment include a number of decision points that neces-sarily involve a level of subjectivity Reliability wasascertained by using independent raters however dif-ferent inclusionexclusion criteria or a different ap-proach to the evaluation of those criteria could result
in a different set of studies being includedUltimately the quality of the meta-analysis is depend-ent upon the underlying studies that are analyzedFurthermore although studies with insufficient infor-mation to be included in the meta-analysis were notfound to differ based on basic study data from thosestudies included in the meta-analysis nonetheless itis unknown how if at all data from these studiescould change the overall results
Acknowledging these limitations our present reviewand meta-analysis found that while an association is evi-dent between cognitive function and later depressiongeneral cognitive function does not appear to be a riskfactor for depression but rather is more likely relatedto performance decrements associated with concurrentdepressive symptoms Our results suggest that low cog-nitive function is therefore probably not a causal factorof depression and that clinical practice may benefitmore from a focus on how decreased cognitive functionin the depressed state is likely to influence treatment out-comes (Gyurak et al 2015) Our findings have importantimplications for better understanding depression and forthe design of future studies in highlighting the need tocontrol for subthreshold depression symptoms when in-vestigating risk factors for mental illness as well as whenassessing cognitive function more generally
Supplementary material
The supplementary material for this article can befound at httpdxdoiorg101017S0033291716002075
Acknowledgements
MAS is supported by an National Science Foundation(NSF) Graduate Research Fellowship ARH is sup-ported by National Institutes of Health (NIH) grantsRO1DA033369 amp R01AG049789 TEM is supportedby National Institutes of Health (NIH) grantsR01AG049789 We would like to thank HarrisCooper PhD at Duke University who provided invalu-able insight into conducting the meta-analysis Wethank all of the authors of studies who provided add-itional information for this meta-analysis
Declaration of Interest
None
References
Aarts E van Holstein M Cools R (2011) Striatal dopamineand the interface between motivation and cognitionFrontiers in Psychology 2 163
14 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Atkinson KM Koenka AC Sanchez CE Moshontz HCooper H (2014) Reporting standards for literaturesearches and report inclusion criteria making researchsyntheses more transparent and easy to replicate ResearchSynthesis Methods 6 87ndash95
Baer LH Tabri N Blair M Bye D Li KZH Pushkar D(2013) Longitudinal associations of need for cognitioncognitive activity and depressive symptomatology withcognitive function in recent retirees Journals of GerontologySeries B Psychological Sciences and Social Sciences 68 655ndash664
Barbey AK Colom R Solomon J Krueger F Forbes CGrafman J (2012) An integrative architecture for generalintelligence and executive function revealed by lesionmapping Brain 135 1154ndash1164
Barnett JH Salmond CH Jones PB Sahakian BJ (2006)Cognitive reserve in neuropsychiatry Psychological Medicine36 1053ndash1064
Beaujean AA Parker S Qiu X (2013) The relationshipbetween cognitive ability and depression a longitudinaldata analysis Social Psychiatry and Psychiatric Epidemiology48 1983ndash1992
Belsky DW Caspi A Arseneault L Bleidorn W Fonagy PGoodman M Houts R Moffitt TE (2012) Etiologicalfeatures of borderline personality related characteristics in abirth cohort of 12-year-old children Development andPsychopathology 24 251ndash265
Betts KS Williams GM Najman JM Alati R (2016)Predicting spectrums of adult mania psychosis anddepression by prospectively ascertained childhoodneurodevelopment Journal of Psychiatric Research 72 22ndash29
Bora E Harrison BJ Yuumlcel M Pantelis C (2013) Cognitiveimpairment in euthymic major depressive disorder a meta-analysis Psychological Medicine 43 2017ndash2026
Borenstein M Hedges LV Higgins JPT Rothstein HR(2011) Introduction to Meta-Analysis John Wiley amp SonsWest Sussex UK
Canals J Domegravenech-Llaberia E Fernaacutendez-Ballart J Martiacute-Henneberg C (2002) Predictors of depression at eighteenA 7-year follow-up study in a Spanish nonclinicalpopulation European Child amp Adolescent Psychiatry 11226ndash233
Christensen H Griffiths K Mackinnon A (1997) Aquantitative review of cognitive deficits in depression andAlzheimer-type dementia Selection of Studies 3 631ndash651
Connolly SL Wagner Ca Shapero BG Pendergast LLAbramson LY Alloy LB (2014) Rumination prospectivelypredicts executive functioning impairments in adolescentsJournal of Behavior Therapy and Experimental Psychiatry 4546ndash56
Cooper HM (1979) Statistically combining independentstudies a meta-analysis of sex differences in conformityresearch Journal of Personality and Social Psychology 37131ndash146
Cooper HM (2010) Research Synthesis and Meta-Analysis AStep-by-Step Approach 4th edn SAGE PublicationsWashington (DC) USA
Cuijpers P de Graaf R van Dorsselaer S (2004) Minordepression risk profiles functional disability health careuse and risk of developing major depression Journal ofAffective Disorders 79 71ndash79
Cuthbert BN Kozak MJ (2013) Constructing constructs forpsychopathology the NIMH research domain criteriaJournal of Abnormal Psychology 122 928ndash937
Der G Batty GD Deary IJ (2009) The association between IQin adolescence and a range of health outcomes at 40 in the1979 US National Longitudinal Study of Youth Intelligence37 573ndash580
Dubow EF Boxer P Huesmann LR (2008) Childhood andadolescent predictors of early and middle adulthoodalcohol use and problem drinking the Columbia CountyLongitudinal Study Addiction 103 36ndash47
Duval S Tweedie R (2000) Trim and fill a simple funnel-plot-based method of testing and adjusting for publicationbias in meta-analysis Biometrics 56 455ndash463
Evans LD Kouros CD Samanez-Larkin S Garber J (2015)Concurrent and short-term prospective relations amongneurocognitive functioning coping and depressivesymptoms in youth Journal of Clinical Child and AdolescentPsychology 53 1ndash15
Franz CE Lyons MJ OrsquoBrien R Panizzon MS Kim K BhatR Grant MD Toomey R Eisen S Xian H Kremen WS(2011) A 35-year longitudinal assessment of cognition andmidlife depression symptoms the Vietnam Era Twin Studyof Aging American Association for Geriatric PsychiatryAmerican Journal of Geriatric Psychiatry 19 559ndash570
Gale CR Batty GD Tynelius P Deary IJ Rasmussen F(2010) Intelligence in early adulthood and subsequenthospitalization for mental disorders Epidemiology 2170ndash77
Gale CR Deary IJ Boyle SH Barefoot J Mortensen LHBatty GD (2008) Cognitive ability in early adulthood andrisk of 5 specific psychiatric disorders in middle age theVietnam experience study Archives of General Psychiatry 651410ndash1418
Gale CR Hatch SL Batty GD Deary IJ (2009) Intelligence inchildhood and risk of psychological distress in adulthoodthe 1958 National Child Development Survey and the 1970British Cohort Study Intelligence 37 592ndash599
Gjerde PF (1995) Alternative pathways to chronicdepressive symptoms in young adults gender differencesin developmental trajectories Child Development 661277ndash1300
Gottfredson LS (1997) Mainstream science on intelligence aneditorial with 52 signatories history and bibliographyIntelligence 24 13ndash23
Guyer AE Choate VR Grimm KJ Pine DS Keenan K(2011) Emerging depression is associated with facememory deficits in adolescent girls Elsevier Inc Journal ofthe American Academy of Child and Adolescent Psychiatry 50180ndash190
Gyurak A Patenaude B Korgaonkar MS Grieve SMWilliams LM Etkin A (2015) Frontoparietal activationduring response inhibition predicts remission toantidepressants in patients with major depression BiologicalPsychiatry 79 1ndash8
Hagenaars SP Harris SE Davies G Hill WD LiewaldDCM Ritchie SJ Marioni RE Fawns-Ritchie C Cullen BMalik R METASTROKE Consortium IC for BPGSpiroMeta Consortium CHARGE ConsortiumPulmonary Group CCA and LG Worrall BB Sudlow
Association between cognitive function and subsequent depression 15
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
CLM Wardlaw JM Gallacher J Pell J McIntosh AMSmith DJ Gale CR Deary IJ (2016) Shared geneticaetiology between cognitive functions and physical andmental health in UK Biobank (N = 112 151) and 24 GWASconsortiaMolecular Psychiatry Published online 26 January2016 doi101038mp2015225
Hatch SL Jones PB Kuh D Hardy R Wadsworth MEJRichards M (2007) Childhood cognitive ability and adultmental health in the British 1946 birth cohort Social Scienceamp Medicine (1982) 64 2285ndash2296
Hipwell AE Sapotichne B Klostermann S Battista DKeenan K (2011) Autobiographical memory as a predictorof depression vulnerability in girls Journal of Clinical Childand Adolescent Psychology 40 254ndash265
Horowitz JL Garber J (2003) Relation of intelligence andreligiosity to depressive disorders in offspring of depressedand nondepressed mothers The American Academy ofChild and Adolescent Psychiatry Journal of the AmericanAcademy of Child and Adolescent Psychiatry 42 578ndash586
Johnson W Bouchard TJ Krueger RF McGue MGottesman II (2004) Just one g consistent results fromthree test batteries Intelligence 32 95ndash107
Keedwell PA Andrew C Williams SCR Brammer MJPhillips ML (2005) The neural correlates of anhedoniain major depressive disorder Biological Psychiatry 58843ndash853
Kessler RC Berglund P Demler O Jin R Koretz DMerikangas KR Rush AJ Walters EE Wang PS (2003)The epidemiology of major depressive disorder resultsfrom the National Comorbidity Survey Replication(NCS-R) Journal of the American Medical Association 2893095ndash3105
Koenen KC Moffitt TE Roberts AL Martin LT KubzanskyL Harrington H Poulton R Caspi A (2009) Childhood IQand adult mental disorders a test of the cognitive reservehypothesis American Journal of Psychiatry 166 50ndash57
Lewinsohn PM Solomon A Seeley JR Zeiss A (2000)Clinical implications of lsquosubthresholdrsquo depressivesymptoms Journal of Abnormal Psychology 109 345ndash351
Luppino FS de Wit LM Bouvy PF Stijnen T Cuijpers PPenninx BWJH Zitman FG (2010) Overweight obesityand depression a systematic review and meta-analysisof longitudinal studies Archives of General Psychiatry 67220ndash229
McCord J Ensminger ME (1997) Multiple risks andcomorbidity in an African-American population CriminalBehaviour and Mental Health 7 339ndash352
McDermott LM Ebmeier KP (2009) A meta-analysis ofdepression severity and cognitive function Elsevier BVJournal of Affective Disorders 119 1ndash8
Melartin TK Rytsaumllauml HJ Leskelauml US Lestelauml-Mielonen PSSokero TP Isometsauml ET (2002) Current comorbidity ofpsychiatric disorders among DSM-IV major depressivedisorder patients in psychiatric care in the VantaaDepression Study Journal of Clinical Psychiatry 63 126ndash134
Meyer SE Carlson GA Wiggs EA Martinez PE RonsavilleDS KlimesndashDougan B Gold PW RadkendashYarrow M(2004) A prospective study of the association amongimpaired executive functioning childhood attentional
problems and the development of bipolar disorderDevelopment and Psychopathology 16 461ndash476
MiyakeA FriedmanNP EmersonMJWitzki aHHowerter AWager TD (2000) The unity and diversity of executivefunctions and their contributions to complex lsquoFrontal Lobersquotasks a latentvariable analysisCognitive Psychology41 49ndash100
Moher D Liberati A (2009) Preferred reporting items forsystematic reviews and meta-analyses the PRISMAstatement Annals of Internal Medicine 151 264ndash269
Papmeyer M Sussmann JE Hall J McKirdy J Peel AMacdonald A Lawrie SM Whalley HC McIntosh AM(2015) Neurocognition in individuals at high familial riskof mood disorders with or without subsequent onset ofdepression Psychological Medicine 45 1ndash11
Peterson RA Brown SP (2005) On the use of betacoefficients in meta-analysis Journal of Applied Psychology90 175ndash181
Pine DS Cohen P Brook J Coplan JD (1997) Psychiatricsymptoms in adolescence as predictors of obesity in earlyadulthood a longitudinal study American Journal of PublicHealth 87 1303ndash1310
Quinn ME Joormann J (2015) Control when it countschange in executive control under stress predicts depressionsymptoms Emotion Junio 22 1ndash10
Rawal A Rice F (2012) Examining overgeneralautobiographical memory as a risk factor for adolescentdepression Elsevier Inc Journal of the American Academy ofChild and Adolescent Psychiatry 51 518ndash527
Ree MJ Earles JA (1991) The stability of g across differentmethods of estimation Intelligence 15 271ndash278
Rock PL Roiser JP Riedel WJ Blackwell AD (2014)Cognitive impairment in depression a systematic reviewand meta-analysis Psychological Medicine 44 2029ndash2040
Rogers MA Kasai K Koji M Fukuda R Iwanami ANakagome K Fukuda M Kato N (2004) Executive andprefrontal dysfunction in unipolar depression a review ofneuropsychological and imaging evidence NeuroscienceResearch 50 1ndash11
Scult MA Knodt AR Swartz JR Brigidi BD Hariri AR(2016) Thinking and feeling individual differences inhabitual emotion regulation and stress-related mood areassociated with prefrontal executive control ClinicalPsychological Science doi1011772167702616654688
Sharp C Petersen N Goodyer I (2008) Emotional reactivityand the emergence of conduct problems and emotionalsymptoms in 7- to 11-year-olds a 1-year follow-up studyJournal of the American Academy of Child and AdolescentPsychiatry 47 565ndash573
Siegel LS (1999) Issues in the definition and diagnosis oflearning disabilities a perspective on Guckenberger vBoston University Journal of Learning Disabilities 32 304ndash319
Simons CJP Jacobs N Derom C Thiery E Jolles J van Os JKrabbendam L (2009) Cognition as predictor of currentand follow-up depressive symptoms in the generalpopulation Acta Psychiatrica Scandinavica 120 45ndash52
Slykerman RF Thompson J Waldie K Murphy R Wall CMitchell EA (2015) Maternal stress during pregnancy isassociated with moderate to severe depression in 11-year-old children Acta Paediatrica 104 68ndash74
16 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Snyder HR (2013) Major depressive disorder is associatedwith broad impairments on neuropsychological measuresof executive function a meta-analysis and reviewPsychological Bulletin 139 81ndash132
Soslashrensen HJ Saeligbye D Urfer-Parnas A Mortensen ELParnas J (2012) Premorbid intelligence and educationallevel in bipolar and unipolar disorders a Danish draftboard study Journal of Affective Disorders 136 1188ndash1191
SpearmanC (1904) lsquoGeneral intelligencersquoobjectivelydeterminedandmeasuredAmerican Journal of Psychology 15 201
Stern Y (2003) The concept of cognitive reserve a catalyst forresearch Journal of Clinical and Experimental Neuropsychology(Neuropsychology Development and Cognition Section A) 25589ndash593
Stroup D Berlin J Morton S Olkin I Williamson GDRennie D Moher D Becker BJ Sipe TA Thacker SB(2000) Meta-analysis of Observational Studies inEpidemiology a proposal for reporting Journal of theAmerican Medical Association 283 2008
Vinberg M Miskowiak KW Kessing LV (2013) Impairmentof executive function and attention predicts onset ofaffective disorder in healthy high-risk twins Journal ofClinical Psychiatry 74 e747ndashe753
Zammit S Allebeck P David AS Dalman C HemmingssonT Lundberg I Lewis G (2004) A longitudinal study ofpremorbid IQ Score and risk of developing schizophreniabipolar disorder severe depression and other nonaffectivepsychoses Archives of General Psychiatry 61 354ndash360
Association between cognitive function and subsequent depression 17
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms

Table 1 (cont)
StudyName ofcohort Type of cohort
Samplesize Comorbidity
Howdepressionassessed
Mean IQatbaseline
Name ofcognitivemeasure
Type of cognitivemeasure
Name ofdepressionoutcome
Type ofdepressionoutcome
Covariatesincluded inmeta-analysisa
Percentfemale Raceethnicity Continent
Meanage atbaseline
Timebetweenassessments(years)
Year ofinitialassessment
Papmeyeret al (2015)
ScottishBipolarFamily Study
Risk sample 111 NR Studyassessment
Controls108Patients107
National AdultReading Test(NART)
VerbalComprehension
Structured ClinicalInterview forDSM Disorders(SCID)symptoms
Categorical None 52 NR Europe 21 2 NR
Pine et al(1997)
NR Communitysample
644 NR Studyassessment
1007 UnspecifiedlsquoIQrsquo
General Intelligence Based onDiagnosticInterviewSchedule forChildren
Continuous Depressionsymptoms atTime 1
52 91 White NorthAmerica
138 9 1983
Quinn ampJoormann(2015)
NR Undergraduatestudents
43 NR Studyassessment
NR n-back Working Memory Beck DepressionInventory II(BDI-II)
Continuous Depressionsymptoms atTime 1
63 58 White30Hispanic orLatino 19Asian 2AfricanAmerican2AmericanIndian 2NativeHawaiian2 Indian
NorthAmerica
19 014 NR
Rawal ampRice (2012)
EarlyPrediction ofAdolescentDepressionstudy
Risk sample 230 None Studyassessment
9746 WechslerIntelligenceScale forChildren(WISC)
General IntelligenceVerbalComprehensionPerceptualReasoning WorkingMemory ProcessingSpeed
Child andAdolescentPsychiatricAssessment(CAPA)
Both Depressionsymptoms atTime 1 AgeOvergeneralityto negativecues
596 NR Europe 1371 1 NR
Sharp et al(2008)
The ChildBehaviourStudy
Communitysample
439 NR Studyassessment
105 WechslerIntelligenceScale forChildren(WISC)
General IntelligenceVerbalComprehensionPerceptualReasoning
The Mood andFeelingsQuestionnaire
Continuous Depressionsymptoms atTime 1
52 97 White05 Black25 Asian
Europe 94 1 NR
Simons et al(2009)
East FlandersProspectiveTwin Survey
Twin registry 444 NR Studyassessment
NR Principalcomponentfrom StroopConceptShifting Testand LetterDigitSubstitutionTest
Processing SpeedSet-ShiftingInhibition
Structured ClinicalInterview forDSM Disorders(SCID)symptoms
Continuous Depressionsymptoms atTime 1
100 NR Europe 28 2 NR
6MA
Scultet
al
httpdxdoiorg101017S0033291716002075D
ownloaded from
httpww
wcam
bridgeorgcore Duke U
niversity Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core term
s of use available at httpww
wcam
bridgeorgcoreterms
Slykermanet al (2015)
AucklandBirthweightCollaborativeStudy
Birth cohortrisk sample
609 NR Studyassessment
NR Stanford-BinetIntelligenceScale 4th Ed
General IntelligenceFluid ReasoningKnowledgeQunatitativeReasoningVisual-SpatialProcessingWorking Memory
Center forEpidemiologicalStudiesDepression Scale(CES-D)
Categorical(cut-point)
None 49 NR NewZealand
35 75 sim2000
Soslashrensenet al (2012)
DanishDraft-BoardStudy
Military cohort 21 914 NR Psychiatricregistry
Controls100Patients96ndash98
Boslashrge PriensProslashve (BPP)
General IntelligenceVerbalComprehensionPerceptualReasoning
DanishInternationalClassification ofdiseases (ICD) 8amp 10
Categorical None 0 NR Europe 195 sim36 1968ndash1989
Vinberget al (2013)
NR High-risktwins
224 Bipolardisorderanxietysubstanceabuse other
Studyassessmentpsychiatricregistry
NR CambridgeCognitiveAssessment(CAMCOG)
GeneralNeuropsychologicalFunctionOrientationLanugage MemoryAttention AbstractThinking VisualPerception
Beck DepressionInventory (BDI)
Continuous Depressionsymptoms atTime 1
65 NR Europe 439 7 2003
Zammitet al (2004)
SwedishConscripts(1969ndash1970)
Military cohort 50 053 None Hospitallinkage
NR UnspecifiedlsquoIQrsquo
General IntelligenceVerbalComprehensionPerceptualReasoning GeneralKnowledgeMechanicalKnowledge
InternationalClassification ofdiseases (ICD)hospitalpsychiatricadmissions
Categorical Diagnosis atbaselinedisturbedbehavior druguse raised in acity
0 NR Europe sim19 27 1969
Sample size is the number of subjects included in reported analyses of interest NR not reportedsim indicates only a range was reporteda This column notes covariates included in the meta-analysis We focused on controlling for depressive symptoms at T1 but some studies reported effect sizes that also included controlling
for other variables ndash when the zero-order correlations were unavailable these estimates were used
Association
between
cognitivefunction
andsubsequent
depression7
httpdxdoiorg101017S0033291716002075D
ownloaded from
httpww
wcam
bridgeorgcore Duke U
niversity Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core term
s of use available at httpww
wcam
bridgeorgcoreterms
to investigate general information processing abilitiesrather than cognitive attributional style studies withcognitive attribution measures as the sole cognitivemeasure were excluded
Comparisons
Search terms used to indicate the possible associationbetween cognitive function and depression includedrisk premorbid prodromal onset predict and association(for a full list see search terms in the SupplementaryMaterial) When data were reported from multipletime-points the analysis accounting for the longesttime between assessments was used
Outcomes
Eligible studies reported depression diagnosis orsymptoms determined by investigator or self-reportPresence of comorbidity was permitted given that de-pression has been found to be highly comorbid withother disorders (Melartin et al 2002 Kessler et al2003) Articles not adequately specifying how depres-sion was assessed or articles that did not uniquelymeasure depression [ie only had an index of lsquomentaldisordersrsquo or the category of lsquomood disordersrsquo lumpedtogether (Gale et al 2010)] were excluded if no uniquemeasure of depression could be obtained from studyauthors This is because although comorbidity waspermitted these could have represented instances ofpure anxiety disorders with few or no depressivesymptoms or instances of bipolar disorder
Study design
Eligible study search terms included cohort studies lon-gitudinal epidemiological prospective retrospective follow-up or case-control studies Studies not following a longi-tudinal design were excluded during full-text reviewAdditionally studies where cognitive function wasassessed only concurrently with or after depressionwere excluded given that the purpose of the reviewwas to investigate whether cognitive function pre-dicted later depression
Studies were included regardless of whether theywere reported in peer-review journals in order to ac-count for potentially biased reporting of resultsReview articles were included in the search terms tofind additional relevant references but were notincluded in the meta-analysis Baseline and protocolstudies without follow-up data were excluded
Study selection
A flow diagram of the process of study selection showsthe overall procedures (Fig 1) Records identified fromthe search processes were combined in EndNote
software version X7 and duplicates were removedTitles and abstracts were reviewed independently bytwo reviewers (MS and AP) according to the eligibil-ity criteria described above and marked as either po-tentially eligible or not eligible If either authormarked an article as potentially eligible it wasincluded in the full-text review for closer examinationby MS and AP who used an electronic form to indi-cate if an article should be included or excluded in thefinal selection When an article was excluded the rea-son for exclusion was selected from a hierarchical listof exclusion criteria presented in Fig 1 Both MSand AP were initially blinded to the otherrsquos decisionsAfter both MS and AP completed their reviews dis-crepancies about whether a study should be includedor excluded were resolved via discussion and consen-sus amongst MS AP TM AH and TS
Data extraction
Study information was extracted independently byMS and AP using an electronic form created forthis study Information was collected and codedbased on report characteristics participant characteris-tics study setting predictors outcome measures andquality assessment (Cooper 2010) Any discrepancies(approximately 3 of data points) were resolved viaconsensus
For studies with categorical depression diagnoses ef-fect sizes were generally presented as odds ratios Forthese studies the odds ratio plus the upper and lowerbound of the confidence interval were recorded Twoof the studies (Zammit et al 2004 Gale et al 2008)reported odds ratios greater than one to indicate thatlower IQ was associated with greater risk of depressionThe other studies reported odds ratios in the reverseleading to odds ratios less than one for the same direc-tion of the effect Therefore the odds ratios from the firsttwo studies were recalculated by dividing (1oddsratio) Another study (McCord amp Ensminger 1997)reported results from chi-squared tests Additional stud-ies reported mean premorbid IQ scores rather than oddsratios in which case the means sample sizes andor pvalues and number of tails of the t test were utilizedto calculate the effect size
For studies in which depression was measured as acontinuous variable effect sizes were presented as cor-relation coefficients The direction of the effect (posi-tive or negative) and the sample size were alsoextracted to be used in the meta-analysis Two studiesreported only beta weights (Simons et al 2009 Rawalamp Rice 2012) and we were not able to obtain zero-order correlations from the authors Given that previ-ous reports have suggested that beta weights can beused as an estimate of correlation coefficients in
8 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
meta-analysis (Peterson amp Brown 2005) the betaweights were used instead and analyses were runboth including and excluding these data points
When insufficient information was presented in thearticle authors were contacted requesting further de-tail An additional six studies were included at thispoint One study (Hatch et al 2007) included effectsizes for the female half of the cohort and did not pro-vide statistics for the males but did indicate a null ef-fect Only women from this study were included in themeta-analyses but imputing a score of 0 for the malesyielded similar overall results
Follow-up analyses directly compared studies thatreported zero-order correlations between IQ at time
1 depression at time 1 and depression at time 2(additional details described in the SupplementaryMethods)
Statistical methods
Data were analyzed using Comprehensive Meta-Analysis software version 30 (Biostat Inc USA) Arandom-effects model was used for expected hetero-geneity across studies A random-effects model alsoallows for broader generalization of results to thepopulation at large Heterogeneity of effects was calcu-lated using the Q statistic where a significant p valueindicates that true effect varies across studies The I2
Fig 1 Flow diagram of the search process
Association between cognitive function and subsequent depression 9
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
statistic was used to calculate the ratio of the true het-erogeneity to total variation acting as an index of sig-nal-to-noise ratio When I2 is large it is has beenrecommended to consider subgroup analysis or meta-regression to account for the variance (Borensteinet al 2011)
Subgroup analyses were conducted using a mixed-effects analysis in which a random effects model wasused to combine studies within each subgroup and afixed effect model was used to combine subgroupsand yield the overall effect (the study-to-study vari-ance is not assumed to be the same for all subgroups)Subgroup analyses were conducted comparing type ofoutcome (continuous v categorical) broad v specificcognitive measures and outcomes that were adjustedv unadjusted for baseline depression symptoms
Meta-regression was performed using the followingvariables on unadjusted analyses age at baseline ageat follow-up time between assessments IQ percentwhite year of cognitive assessment year of follow-upassessment percent female and study quality score
Study quality and publication bias
Study quality was evaluated independently by MSand AP using a checklist adapted from Luppino ampWit (Luppino et al 2010) The checklist contained 12items and studies were rated with a lsquo+rsquo if it met criteriafor that item a lsquominusrsquo if it did not meet criteria for an itemand a rsquorsquo if unclear lsquo+rsquo were coded as a score of 1 andminus were coded as a score of 0 Total scores and percen-tages were calculated Articles with total scores of 0ndash3were considered to be of low quality scores of 4ndash7were considered a medium quality and scores of 8ndash12 were considered to be of high quality Any discrep-ancies (approximately 3 of data points) wereresolved via consensus
Publication bias was assessed using a funnel plotwhich presents study size on the vertical axis (as stand-ard error in this case) as a function of effect size on thex-axis When no publication bias exists the studiesshould be distributed symmetrically about the com-bined effect size (Borenstein et al 2011) If evidenceof publication bias was observed Duval amp Tweediersquostrim-and-fill method was used (Duval amp Tweedie2000) which recalculates effects based on imputingdata from studies that are likely to be missing Lastthe Fail-safe N was calculated (Cooper 1979) whichindicates the number of missing studies that wouldneed to exist to nullify the observed effect
Results
A flow diagram of the search process is shown inFig 1 The search identified 2773 records through
PubMed 2158 through EMBASE and 1345 throughPsycINFO for a total of 6276 records Duplicaterecords (1709) were removed in EndNote resulting in4567 unique records After title and abstracts werereviewed 329 records were identified as potentially eli-gible for the meta-analysis These 329 records werereviewed in full and 300 articles were excluded hier-archically if they were a review baseline or protocolpaper (n = 6) if the sample had a mean age over 65at the depression assessment (n = 41) if the samplehad a specific medical illness (n = 23) if the studywas not a longitudinal design (n = 19) if MDD diagno-sis hospitalization or admission to treatment centerwas part of the inclusion criteria of the study (n = 18)if cognitive function was assessed only concurrentlywith or after depression (n = 36) if cognitive functionwas assessed by educational achievement or self-report(n = 26) if cognitive function was assessed by attribu-tion style rather than neuropsychological measure (n= 7) if there was no measure of cognitive function (n= 18) or no uniquely measured depression outcome(n = 24) Furthermore if articles reported on the samesample as another article with higher quality or moreinformation the duplicate articles were excluded (n =8) Last a number of studies appeared to measureboth cognitive function and depression but did not re-port enough information to be included in the meta-analysis and did not respond to requests for additionalinformation (n = 74 approximately 59 unique samples)In total 29 publication were included in the meta-ana-lysis comprising 34 samples (one study included twoseparate birth cohorts and another four reported dataseparately for men and women)
Study characteristics
The characteristics of included samples are detailed inTable 1 Sample sizes ranged from 43 to 50 053 with amedian of 3395 The most common types of sampleswere school samples (934) community samples (834) and birth cohorts (734) The samples were major-ity white with two samples having exclusively blackparticipants Additionally eight samples were menonly six samples were women only and the restreported combined effect sizes Mean age of partici-pants at baseline ranged from 35 to 59 years with amedian of 12 years Most samples did not reportwhether comorbid diagnoses were present (2334)
Of the 74 papers excluded for having insufficient in-formation (representing 60 unique samples) the me-dian number of subjects was not statistically differentbetween those studies and the studies included in themeta-analysis (n = 288 and n = 3395 respectively p =019) nor did the average age of study participants atbaseline statistically differ (median across studies = 11
10 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
v 12 respectively p = 057) The types of cognitivemeasures used were also similar across the excludedand included studies with the most common measurebeing IQ (2860 and 2029) followed by VerbalComprehension (860 and 529)
Meta-analysis
The overall analysis yielded a significant associationbetween cognitive function and subsequent depressionoutcomes [r =minus0088 95 confidence interval (CI)minus0121 to minus0054 p lt 0001 Fig 2] Results were similarwhen excluding the two studies that used beta-weights(r =minus0071 95 CI minus0100 to minus0042 p lt 0001) orwhen using episodic memory in place of processingspeed in a study reporting both outcomes (r =minus008595 CI minus0118 to minus0051 p lt 0001) Follow-up ana-lyses were conducted in the sample of studies report-ing educational attainment and self-report outcomes(Supplementary Table S2) Heterogeneity across sam-ples was significant (Q = 80154 p lt 0001) suggestingsubstantial variation across the individual samplesThe ratio of the true heterogeneity to total variationwas large (I2 = 9588) I2 is on a relative scale andvalues close to 100 indicate that most of the observedvariance is real rather than spurious and suggeststhat subgroup analyses or meta-regression may helpto explain this variability (Borenstein et al 2011)
Subgroup analyses and meta-regression
A significant difference was found between categoricaland continuous effect sizes (p lt 0001) The studiesassessing continuous outcomes were found to have alarger effect (r =minus0121 95 CI minus0168 to minus0073 p lt0001 n = 22) than studies assessing categorical out-comes (r =minus0035 95 CI minus0054 to minus0017 p lt 0001n = 12) No differences were observed between studiesutilizing broad v specific cognitive measures (p = 057)
Outcomes were also compared adjusting for baselinedepression symptoms at the time of cognitive assess-ment Nine studies provided enough detail to calculatethe partial correlation coefficients adjusting for base-line depression symptoms Using the partial correl-ation coefficients led to a null result (r =minus0032 95CI minus0078 to 0014 p = 0169 n = 9 Fig 3) The nullresult does not seem to be due to a lack of power be-cause using the unadjusted correlation coefficients forthe same nine studies still led to a significant result(r =minus0120 95 CI minus0169 to minus0070 p lt 0001 n = 9Fig 3) As a follow-up the difference in effect sizes be-tween the adjusted and unadjusted values for these 9studies were tested (r = 0082 95 CI 0069ndash0095 p lt0001 n = 9) suggesting that the effects are significantlydifferent when directly comparing the values that doand do not control for baseline depression symptoms
Expanding the subgroup analyses to include studiesthat controlled for baseline depression plus other co-variates (Zammit et al 2004 Simons et al 2009 Rawalamp Rice 2012) and studies that explicitly excluded fora history of depression diagnosis (Gale et al 2008Vinberg et al 2013 Papmeyer et al 2015) did notchange the null result (r =minus0027 95 CI minus0058 to0005 p = 0097 n = 15)
None of the meta-regression analyses were signifi-cant indicating that the between-study variance wasnot attributable to age at baseline IQ percent of sam-ple that was female percent of the sample that waswhite age at follow-up time between assessmentsyear of cognitive assessment year of follow-up assess-ment or study quality score
Study quality and publication bias
Multiple samples within a study were combined forthe purposes of quality assessment given that studieswithin the same publication were found to employthe same methodology Of the 29 publications reviewed12 were rated as high quality and 17 were rated as me-dium quality Details are provided in SupplementaryTable S1 Comparable results to the overall findingswere obtained when just using high quality studies (r=minus0085 95 CI minus0141 to minus0029 p = 0003)
Inspection of the funnel plot (Fig 4) found no evi-dence for publication bias to support the hypothesisIn fact imputation of negative correlations suggestedthat additional studies favoring the hypothesis maybe missing While the calculated effect size is minus0088(95 CI minus0121 to minus0054) using Duval amp Tweediersquostrim-and-fill method the imputed effect size estimateis larger at minus0137 (95 CI minus0176 to minus0099 imputedstudies n = 11) Last the Fail-safe N procedure foundthat 3583 null studies would need to be located forthe combined two-tailed p value to exceed 005 Thissuggests that significant results are not likely to be con-founded by publication bias and may even underesti-mate true effect sizes
Discussion
The present systematic review and meta-analysis of 29longitudinal publications including 1 21 749 partici-pants revealed that after accounting for baseline depres-sion symptoms variability in cognitive function did notpredict subsequent depression Consistent with priorreports there was a significant contemporaneous associ-ation between higher depression symptoms and lowercognitive function These patterns have implications forunderstanding the association between cognitive func-tion and depression and may be important for advan-cing etiologic and treatment research
Association between cognitive function and subsequent depression 11
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
First our findings reinforce models positing thatcognitive function tracks with depression severity(McDermott amp Ebmeier 2009) One possible explan-ation for this contemporaneous association is that de-pression symptoms interfere with the capacity tocomplete cognitive assessments possibly through thegeneral lack of motivation that is one hallmark of thedisorder While this explanation represents an experi-mental confound for studies focused on assessmentof cognitive function it likewise represents an oppor-tunity for studies to focus more comprehensively onthe assessment of both depression and mood disordersymptoms since performance on cognitive tests maybe a sensitive measure of motivational state thatcould augment self-reported symptoms Alternativelythe co-occurrence of cognitive deficits and depressionsymptoms may reflect shared genetic etiology (Hagen-aars et al 2016) and dysfunction of neural circuits
supporting both cognitive and emotional processes(Scult et al 2016) In particular dysfunction of prefront-al and striatal circuits have been associated with bothdepression and cognitive function (Keedwell et al2005 Aarts et al 2011)
Second our findings suggest that prior studies oflinks between cognitive function and depression thatdid not assess baseline symptoms may have overesti-mated the potential protective role of higher cognitivefunction While the importance of accounting for sub-clinical symptoms is not novel the implementation ofsuch accounting is often neglected in psychiatric epi-demiology given the current categorical threshold-based diagnostic system In our meta-analysis largereffects were observed for continuous as compared tocategorical outcomes which aligns with growing em-phasis on dimensional measures of psychopathology(Cuthbert amp Kozak 2013)
Fig 2 Meta-analysis of the association between cognitive function and subsequent depression A forest plot for all studiesthat investigated associations between cognition and later depression Results are reported as correlation coefficients denotedby squares and 95 confidence intervals (CI) indicated by lines (effect sizes are converted to correlation coefficients ifreported as odds ratios) Meta-analysis results are displayed as the diamond The overall analysis found a significant effect ofcognition on depression (r =minus0088 95 CI minus0121 to minus0054 p lt 0001)
12 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Fig 4 Trim-and-fill funnel plots for all samples Fisherrsquos Z a measure of effect size is plotted on the x-axis and the standarderror is plotted on the y-axis Larger studies appear toward the top of the graph and smaller studies towards the bottom Inthe absence of publication bias the studies are symmetrically distributed around the mean Actual studies are shown in opencircles and imputed studies would be shown in black circles No additional studies would be expected in the oppositedirection (to the right) of the observed effect but an additional 11 studies are imputed to the left of the mean effect sizeWhile the calculated effect size is minus0088 [95 confidence interval (CI) minus0121 to minus0054] using Duval amp Tweediersquos trim-and-fill method the imputed effect size estimate is larger at minus0137 (95 CI minus0176 to minus0099 imputed studies n = 11)
Fig 3 Meta-analysis comparing values adjusted for baseline depression symptoms v unadjusted A forest plot for analysiscomparing results from a subset of the same set of studies reported in Fig 2 when using unadjusted values compared tousing values that are adjusted for baseline depression Effects are significant for unadjusted values [r =minus0120 95 confidenceinterval (CI) minus0169 to minus0070 p lt 0001] but not for adjusted values (r =minus0032 95 CI minus0078 to 0014 p = 0169) Results arereported as correlation coefficients denoted by squares and 95 CIs indicated by lines Meta-analysis results are displayed asdiamonds
Association between cognitive function and subsequent depression 13
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Third the associations between cognitive functionand either current or later depression were not moder-ated by data quality or participant age sex and raceHowever there are a number of additional potentialmoderators that could not be addressed in the currentreview and meta-analysis For example the numberand type of comorbid conditions with depressionwere often not reported in the included studies butcould represent an important moderator of theobserved effects Modeling the effects of comorbid ill-ness is an important avenue for future research
One limitation of the current literature is that only ahandful of studies reviewed explicitly excluded for de-pression diagnosis at baseline (Gale et al 2008 Vinberget al 2013 Papmeyer et al 2015) however consistentwith the finding that controlling for baseline depres-sion symptoms led to a null association between cogni-tion and subsequent depression there was no effectobserved when including these studies in the sub-group analyses further suggesting that the associationbetween cognitive function and depression is likelycontemporaneous It will be important to follow-upthese analyses with individual studies that includerigorous assessment of baseline depression symptomsand other potentially confounding factors to furtherclarify this relationship
An open question that remains for future research iswhether deficits in cognitive function are likely to pre-dict the development of more sever or recurrent de-pression later in life Only one of the included studies(Koenen et al 2009) specifically investigated recurrentdepression and found that lower IQ was associatedwith greater persistence of disorder
A final consideration is that while our review andmeta-analysis focused on general cognitive functionmainly assessed via IQ there may be specific subtypesof cognitive function that are more predictive of laterdepression For example a lack of cognitive flexibilitymay more closely match with the ruminative stylecharacteristic of depression and therefore tasks specifi-cally measuring this component of cognitive functionmight have some predictive utility While our reviewdid not find differences between broad and specificmeasures of cognitive function there were not enoughstudies identified to allow for precise consideration ofdifferences between individual cognitive domains
A limitation of the meta-analysis is that while thepresent study followed standard guidelines (Stroupet al 2000 Atkinson et al 2014) decisions aboutstudy selection data extraction and quality assess-ment include a number of decision points that neces-sarily involve a level of subjectivity Reliability wasascertained by using independent raters however dif-ferent inclusionexclusion criteria or a different ap-proach to the evaluation of those criteria could result
in a different set of studies being includedUltimately the quality of the meta-analysis is depend-ent upon the underlying studies that are analyzedFurthermore although studies with insufficient infor-mation to be included in the meta-analysis were notfound to differ based on basic study data from thosestudies included in the meta-analysis nonetheless itis unknown how if at all data from these studiescould change the overall results
Acknowledging these limitations our present reviewand meta-analysis found that while an association is evi-dent between cognitive function and later depressiongeneral cognitive function does not appear to be a riskfactor for depression but rather is more likely relatedto performance decrements associated with concurrentdepressive symptoms Our results suggest that low cog-nitive function is therefore probably not a causal factorof depression and that clinical practice may benefitmore from a focus on how decreased cognitive functionin the depressed state is likely to influence treatment out-comes (Gyurak et al 2015) Our findings have importantimplications for better understanding depression and forthe design of future studies in highlighting the need tocontrol for subthreshold depression symptoms when in-vestigating risk factors for mental illness as well as whenassessing cognitive function more generally
Supplementary material
The supplementary material for this article can befound at httpdxdoiorg101017S0033291716002075
Acknowledgements
MAS is supported by an National Science Foundation(NSF) Graduate Research Fellowship ARH is sup-ported by National Institutes of Health (NIH) grantsRO1DA033369 amp R01AG049789 TEM is supportedby National Institutes of Health (NIH) grantsR01AG049789 We would like to thank HarrisCooper PhD at Duke University who provided invalu-able insight into conducting the meta-analysis Wethank all of the authors of studies who provided add-itional information for this meta-analysis
Declaration of Interest
None
References
Aarts E van Holstein M Cools R (2011) Striatal dopamineand the interface between motivation and cognitionFrontiers in Psychology 2 163
14 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Atkinson KM Koenka AC Sanchez CE Moshontz HCooper H (2014) Reporting standards for literaturesearches and report inclusion criteria making researchsyntheses more transparent and easy to replicate ResearchSynthesis Methods 6 87ndash95
Baer LH Tabri N Blair M Bye D Li KZH Pushkar D(2013) Longitudinal associations of need for cognitioncognitive activity and depressive symptomatology withcognitive function in recent retirees Journals of GerontologySeries B Psychological Sciences and Social Sciences 68 655ndash664
Barbey AK Colom R Solomon J Krueger F Forbes CGrafman J (2012) An integrative architecture for generalintelligence and executive function revealed by lesionmapping Brain 135 1154ndash1164
Barnett JH Salmond CH Jones PB Sahakian BJ (2006)Cognitive reserve in neuropsychiatry Psychological Medicine36 1053ndash1064
Beaujean AA Parker S Qiu X (2013) The relationshipbetween cognitive ability and depression a longitudinaldata analysis Social Psychiatry and Psychiatric Epidemiology48 1983ndash1992
Belsky DW Caspi A Arseneault L Bleidorn W Fonagy PGoodman M Houts R Moffitt TE (2012) Etiologicalfeatures of borderline personality related characteristics in abirth cohort of 12-year-old children Development andPsychopathology 24 251ndash265
Betts KS Williams GM Najman JM Alati R (2016)Predicting spectrums of adult mania psychosis anddepression by prospectively ascertained childhoodneurodevelopment Journal of Psychiatric Research 72 22ndash29
Bora E Harrison BJ Yuumlcel M Pantelis C (2013) Cognitiveimpairment in euthymic major depressive disorder a meta-analysis Psychological Medicine 43 2017ndash2026
Borenstein M Hedges LV Higgins JPT Rothstein HR(2011) Introduction to Meta-Analysis John Wiley amp SonsWest Sussex UK
Canals J Domegravenech-Llaberia E Fernaacutendez-Ballart J Martiacute-Henneberg C (2002) Predictors of depression at eighteenA 7-year follow-up study in a Spanish nonclinicalpopulation European Child amp Adolescent Psychiatry 11226ndash233
Christensen H Griffiths K Mackinnon A (1997) Aquantitative review of cognitive deficits in depression andAlzheimer-type dementia Selection of Studies 3 631ndash651
Connolly SL Wagner Ca Shapero BG Pendergast LLAbramson LY Alloy LB (2014) Rumination prospectivelypredicts executive functioning impairments in adolescentsJournal of Behavior Therapy and Experimental Psychiatry 4546ndash56
Cooper HM (1979) Statistically combining independentstudies a meta-analysis of sex differences in conformityresearch Journal of Personality and Social Psychology 37131ndash146
Cooper HM (2010) Research Synthesis and Meta-Analysis AStep-by-Step Approach 4th edn SAGE PublicationsWashington (DC) USA
Cuijpers P de Graaf R van Dorsselaer S (2004) Minordepression risk profiles functional disability health careuse and risk of developing major depression Journal ofAffective Disorders 79 71ndash79
Cuthbert BN Kozak MJ (2013) Constructing constructs forpsychopathology the NIMH research domain criteriaJournal of Abnormal Psychology 122 928ndash937
Der G Batty GD Deary IJ (2009) The association between IQin adolescence and a range of health outcomes at 40 in the1979 US National Longitudinal Study of Youth Intelligence37 573ndash580
Dubow EF Boxer P Huesmann LR (2008) Childhood andadolescent predictors of early and middle adulthoodalcohol use and problem drinking the Columbia CountyLongitudinal Study Addiction 103 36ndash47
Duval S Tweedie R (2000) Trim and fill a simple funnel-plot-based method of testing and adjusting for publicationbias in meta-analysis Biometrics 56 455ndash463
Evans LD Kouros CD Samanez-Larkin S Garber J (2015)Concurrent and short-term prospective relations amongneurocognitive functioning coping and depressivesymptoms in youth Journal of Clinical Child and AdolescentPsychology 53 1ndash15
Franz CE Lyons MJ OrsquoBrien R Panizzon MS Kim K BhatR Grant MD Toomey R Eisen S Xian H Kremen WS(2011) A 35-year longitudinal assessment of cognition andmidlife depression symptoms the Vietnam Era Twin Studyof Aging American Association for Geriatric PsychiatryAmerican Journal of Geriatric Psychiatry 19 559ndash570
Gale CR Batty GD Tynelius P Deary IJ Rasmussen F(2010) Intelligence in early adulthood and subsequenthospitalization for mental disorders Epidemiology 2170ndash77
Gale CR Deary IJ Boyle SH Barefoot J Mortensen LHBatty GD (2008) Cognitive ability in early adulthood andrisk of 5 specific psychiatric disorders in middle age theVietnam experience study Archives of General Psychiatry 651410ndash1418
Gale CR Hatch SL Batty GD Deary IJ (2009) Intelligence inchildhood and risk of psychological distress in adulthoodthe 1958 National Child Development Survey and the 1970British Cohort Study Intelligence 37 592ndash599
Gjerde PF (1995) Alternative pathways to chronicdepressive symptoms in young adults gender differencesin developmental trajectories Child Development 661277ndash1300
Gottfredson LS (1997) Mainstream science on intelligence aneditorial with 52 signatories history and bibliographyIntelligence 24 13ndash23
Guyer AE Choate VR Grimm KJ Pine DS Keenan K(2011) Emerging depression is associated with facememory deficits in adolescent girls Elsevier Inc Journal ofthe American Academy of Child and Adolescent Psychiatry 50180ndash190
Gyurak A Patenaude B Korgaonkar MS Grieve SMWilliams LM Etkin A (2015) Frontoparietal activationduring response inhibition predicts remission toantidepressants in patients with major depression BiologicalPsychiatry 79 1ndash8
Hagenaars SP Harris SE Davies G Hill WD LiewaldDCM Ritchie SJ Marioni RE Fawns-Ritchie C Cullen BMalik R METASTROKE Consortium IC for BPGSpiroMeta Consortium CHARGE ConsortiumPulmonary Group CCA and LG Worrall BB Sudlow
Association between cognitive function and subsequent depression 15
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
CLM Wardlaw JM Gallacher J Pell J McIntosh AMSmith DJ Gale CR Deary IJ (2016) Shared geneticaetiology between cognitive functions and physical andmental health in UK Biobank (N = 112 151) and 24 GWASconsortiaMolecular Psychiatry Published online 26 January2016 doi101038mp2015225
Hatch SL Jones PB Kuh D Hardy R Wadsworth MEJRichards M (2007) Childhood cognitive ability and adultmental health in the British 1946 birth cohort Social Scienceamp Medicine (1982) 64 2285ndash2296
Hipwell AE Sapotichne B Klostermann S Battista DKeenan K (2011) Autobiographical memory as a predictorof depression vulnerability in girls Journal of Clinical Childand Adolescent Psychology 40 254ndash265
Horowitz JL Garber J (2003) Relation of intelligence andreligiosity to depressive disorders in offspring of depressedand nondepressed mothers The American Academy ofChild and Adolescent Psychiatry Journal of the AmericanAcademy of Child and Adolescent Psychiatry 42 578ndash586
Johnson W Bouchard TJ Krueger RF McGue MGottesman II (2004) Just one g consistent results fromthree test batteries Intelligence 32 95ndash107
Keedwell PA Andrew C Williams SCR Brammer MJPhillips ML (2005) The neural correlates of anhedoniain major depressive disorder Biological Psychiatry 58843ndash853
Kessler RC Berglund P Demler O Jin R Koretz DMerikangas KR Rush AJ Walters EE Wang PS (2003)The epidemiology of major depressive disorder resultsfrom the National Comorbidity Survey Replication(NCS-R) Journal of the American Medical Association 2893095ndash3105
Koenen KC Moffitt TE Roberts AL Martin LT KubzanskyL Harrington H Poulton R Caspi A (2009) Childhood IQand adult mental disorders a test of the cognitive reservehypothesis American Journal of Psychiatry 166 50ndash57
Lewinsohn PM Solomon A Seeley JR Zeiss A (2000)Clinical implications of lsquosubthresholdrsquo depressivesymptoms Journal of Abnormal Psychology 109 345ndash351
Luppino FS de Wit LM Bouvy PF Stijnen T Cuijpers PPenninx BWJH Zitman FG (2010) Overweight obesityand depression a systematic review and meta-analysisof longitudinal studies Archives of General Psychiatry 67220ndash229
McCord J Ensminger ME (1997) Multiple risks andcomorbidity in an African-American population CriminalBehaviour and Mental Health 7 339ndash352
McDermott LM Ebmeier KP (2009) A meta-analysis ofdepression severity and cognitive function Elsevier BVJournal of Affective Disorders 119 1ndash8
Melartin TK Rytsaumllauml HJ Leskelauml US Lestelauml-Mielonen PSSokero TP Isometsauml ET (2002) Current comorbidity ofpsychiatric disorders among DSM-IV major depressivedisorder patients in psychiatric care in the VantaaDepression Study Journal of Clinical Psychiatry 63 126ndash134
Meyer SE Carlson GA Wiggs EA Martinez PE RonsavilleDS KlimesndashDougan B Gold PW RadkendashYarrow M(2004) A prospective study of the association amongimpaired executive functioning childhood attentional
problems and the development of bipolar disorderDevelopment and Psychopathology 16 461ndash476
MiyakeA FriedmanNP EmersonMJWitzki aHHowerter AWager TD (2000) The unity and diversity of executivefunctions and their contributions to complex lsquoFrontal Lobersquotasks a latentvariable analysisCognitive Psychology41 49ndash100
Moher D Liberati A (2009) Preferred reporting items forsystematic reviews and meta-analyses the PRISMAstatement Annals of Internal Medicine 151 264ndash269
Papmeyer M Sussmann JE Hall J McKirdy J Peel AMacdonald A Lawrie SM Whalley HC McIntosh AM(2015) Neurocognition in individuals at high familial riskof mood disorders with or without subsequent onset ofdepression Psychological Medicine 45 1ndash11
Peterson RA Brown SP (2005) On the use of betacoefficients in meta-analysis Journal of Applied Psychology90 175ndash181
Pine DS Cohen P Brook J Coplan JD (1997) Psychiatricsymptoms in adolescence as predictors of obesity in earlyadulthood a longitudinal study American Journal of PublicHealth 87 1303ndash1310
Quinn ME Joormann J (2015) Control when it countschange in executive control under stress predicts depressionsymptoms Emotion Junio 22 1ndash10
Rawal A Rice F (2012) Examining overgeneralautobiographical memory as a risk factor for adolescentdepression Elsevier Inc Journal of the American Academy ofChild and Adolescent Psychiatry 51 518ndash527
Ree MJ Earles JA (1991) The stability of g across differentmethods of estimation Intelligence 15 271ndash278
Rock PL Roiser JP Riedel WJ Blackwell AD (2014)Cognitive impairment in depression a systematic reviewand meta-analysis Psychological Medicine 44 2029ndash2040
Rogers MA Kasai K Koji M Fukuda R Iwanami ANakagome K Fukuda M Kato N (2004) Executive andprefrontal dysfunction in unipolar depression a review ofneuropsychological and imaging evidence NeuroscienceResearch 50 1ndash11
Scult MA Knodt AR Swartz JR Brigidi BD Hariri AR(2016) Thinking and feeling individual differences inhabitual emotion regulation and stress-related mood areassociated with prefrontal executive control ClinicalPsychological Science doi1011772167702616654688
Sharp C Petersen N Goodyer I (2008) Emotional reactivityand the emergence of conduct problems and emotionalsymptoms in 7- to 11-year-olds a 1-year follow-up studyJournal of the American Academy of Child and AdolescentPsychiatry 47 565ndash573
Siegel LS (1999) Issues in the definition and diagnosis oflearning disabilities a perspective on Guckenberger vBoston University Journal of Learning Disabilities 32 304ndash319
Simons CJP Jacobs N Derom C Thiery E Jolles J van Os JKrabbendam L (2009) Cognition as predictor of currentand follow-up depressive symptoms in the generalpopulation Acta Psychiatrica Scandinavica 120 45ndash52
Slykerman RF Thompson J Waldie K Murphy R Wall CMitchell EA (2015) Maternal stress during pregnancy isassociated with moderate to severe depression in 11-year-old children Acta Paediatrica 104 68ndash74
16 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Snyder HR (2013) Major depressive disorder is associatedwith broad impairments on neuropsychological measuresof executive function a meta-analysis and reviewPsychological Bulletin 139 81ndash132
Soslashrensen HJ Saeligbye D Urfer-Parnas A Mortensen ELParnas J (2012) Premorbid intelligence and educationallevel in bipolar and unipolar disorders a Danish draftboard study Journal of Affective Disorders 136 1188ndash1191
SpearmanC (1904) lsquoGeneral intelligencersquoobjectivelydeterminedandmeasuredAmerican Journal of Psychology 15 201
Stern Y (2003) The concept of cognitive reserve a catalyst forresearch Journal of Clinical and Experimental Neuropsychology(Neuropsychology Development and Cognition Section A) 25589ndash593
Stroup D Berlin J Morton S Olkin I Williamson GDRennie D Moher D Becker BJ Sipe TA Thacker SB(2000) Meta-analysis of Observational Studies inEpidemiology a proposal for reporting Journal of theAmerican Medical Association 283 2008
Vinberg M Miskowiak KW Kessing LV (2013) Impairmentof executive function and attention predicts onset ofaffective disorder in healthy high-risk twins Journal ofClinical Psychiatry 74 e747ndashe753
Zammit S Allebeck P David AS Dalman C HemmingssonT Lundberg I Lewis G (2004) A longitudinal study ofpremorbid IQ Score and risk of developing schizophreniabipolar disorder severe depression and other nonaffectivepsychoses Archives of General Psychiatry 61 354ndash360
Association between cognitive function and subsequent depression 17
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms

Slykermanet al (2015)
AucklandBirthweightCollaborativeStudy
Birth cohortrisk sample
609 NR Studyassessment
NR Stanford-BinetIntelligenceScale 4th Ed
General IntelligenceFluid ReasoningKnowledgeQunatitativeReasoningVisual-SpatialProcessingWorking Memory
Center forEpidemiologicalStudiesDepression Scale(CES-D)
Categorical(cut-point)
None 49 NR NewZealand
35 75 sim2000
Soslashrensenet al (2012)
DanishDraft-BoardStudy
Military cohort 21 914 NR Psychiatricregistry
Controls100Patients96ndash98
Boslashrge PriensProslashve (BPP)
General IntelligenceVerbalComprehensionPerceptualReasoning
DanishInternationalClassification ofdiseases (ICD) 8amp 10
Categorical None 0 NR Europe 195 sim36 1968ndash1989
Vinberget al (2013)
NR High-risktwins
224 Bipolardisorderanxietysubstanceabuse other
Studyassessmentpsychiatricregistry
NR CambridgeCognitiveAssessment(CAMCOG)
GeneralNeuropsychologicalFunctionOrientationLanugage MemoryAttention AbstractThinking VisualPerception
Beck DepressionInventory (BDI)
Continuous Depressionsymptoms atTime 1
65 NR Europe 439 7 2003
Zammitet al (2004)
SwedishConscripts(1969ndash1970)
Military cohort 50 053 None Hospitallinkage
NR UnspecifiedlsquoIQrsquo
General IntelligenceVerbalComprehensionPerceptualReasoning GeneralKnowledgeMechanicalKnowledge
InternationalClassification ofdiseases (ICD)hospitalpsychiatricadmissions
Categorical Diagnosis atbaselinedisturbedbehavior druguse raised in acity
0 NR Europe sim19 27 1969
Sample size is the number of subjects included in reported analyses of interest NR not reportedsim indicates only a range was reporteda This column notes covariates included in the meta-analysis We focused on controlling for depressive symptoms at T1 but some studies reported effect sizes that also included controlling
for other variables ndash when the zero-order correlations were unavailable these estimates were used
Association
between
cognitivefunction
andsubsequent
depression7
httpdxdoiorg101017S0033291716002075D
ownloaded from
httpww
wcam
bridgeorgcore Duke U
niversity Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core term
s of use available at httpww
wcam
bridgeorgcoreterms
to investigate general information processing abilitiesrather than cognitive attributional style studies withcognitive attribution measures as the sole cognitivemeasure were excluded
Comparisons
Search terms used to indicate the possible associationbetween cognitive function and depression includedrisk premorbid prodromal onset predict and association(for a full list see search terms in the SupplementaryMaterial) When data were reported from multipletime-points the analysis accounting for the longesttime between assessments was used
Outcomes
Eligible studies reported depression diagnosis orsymptoms determined by investigator or self-reportPresence of comorbidity was permitted given that de-pression has been found to be highly comorbid withother disorders (Melartin et al 2002 Kessler et al2003) Articles not adequately specifying how depres-sion was assessed or articles that did not uniquelymeasure depression [ie only had an index of lsquomentaldisordersrsquo or the category of lsquomood disordersrsquo lumpedtogether (Gale et al 2010)] were excluded if no uniquemeasure of depression could be obtained from studyauthors This is because although comorbidity waspermitted these could have represented instances ofpure anxiety disorders with few or no depressivesymptoms or instances of bipolar disorder
Study design
Eligible study search terms included cohort studies lon-gitudinal epidemiological prospective retrospective follow-up or case-control studies Studies not following a longi-tudinal design were excluded during full-text reviewAdditionally studies where cognitive function wasassessed only concurrently with or after depressionwere excluded given that the purpose of the reviewwas to investigate whether cognitive function pre-dicted later depression
Studies were included regardless of whether theywere reported in peer-review journals in order to ac-count for potentially biased reporting of resultsReview articles were included in the search terms tofind additional relevant references but were notincluded in the meta-analysis Baseline and protocolstudies without follow-up data were excluded
Study selection
A flow diagram of the process of study selection showsthe overall procedures (Fig 1) Records identified fromthe search processes were combined in EndNote
software version X7 and duplicates were removedTitles and abstracts were reviewed independently bytwo reviewers (MS and AP) according to the eligibil-ity criteria described above and marked as either po-tentially eligible or not eligible If either authormarked an article as potentially eligible it wasincluded in the full-text review for closer examinationby MS and AP who used an electronic form to indi-cate if an article should be included or excluded in thefinal selection When an article was excluded the rea-son for exclusion was selected from a hierarchical listof exclusion criteria presented in Fig 1 Both MSand AP were initially blinded to the otherrsquos decisionsAfter both MS and AP completed their reviews dis-crepancies about whether a study should be includedor excluded were resolved via discussion and consen-sus amongst MS AP TM AH and TS
Data extraction
Study information was extracted independently byMS and AP using an electronic form created forthis study Information was collected and codedbased on report characteristics participant characteris-tics study setting predictors outcome measures andquality assessment (Cooper 2010) Any discrepancies(approximately 3 of data points) were resolved viaconsensus
For studies with categorical depression diagnoses ef-fect sizes were generally presented as odds ratios Forthese studies the odds ratio plus the upper and lowerbound of the confidence interval were recorded Twoof the studies (Zammit et al 2004 Gale et al 2008)reported odds ratios greater than one to indicate thatlower IQ was associated with greater risk of depressionThe other studies reported odds ratios in the reverseleading to odds ratios less than one for the same direc-tion of the effect Therefore the odds ratios from the firsttwo studies were recalculated by dividing (1oddsratio) Another study (McCord amp Ensminger 1997)reported results from chi-squared tests Additional stud-ies reported mean premorbid IQ scores rather than oddsratios in which case the means sample sizes andor pvalues and number of tails of the t test were utilizedto calculate the effect size
For studies in which depression was measured as acontinuous variable effect sizes were presented as cor-relation coefficients The direction of the effect (posi-tive or negative) and the sample size were alsoextracted to be used in the meta-analysis Two studiesreported only beta weights (Simons et al 2009 Rawalamp Rice 2012) and we were not able to obtain zero-order correlations from the authors Given that previ-ous reports have suggested that beta weights can beused as an estimate of correlation coefficients in
8 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
meta-analysis (Peterson amp Brown 2005) the betaweights were used instead and analyses were runboth including and excluding these data points
When insufficient information was presented in thearticle authors were contacted requesting further de-tail An additional six studies were included at thispoint One study (Hatch et al 2007) included effectsizes for the female half of the cohort and did not pro-vide statistics for the males but did indicate a null ef-fect Only women from this study were included in themeta-analyses but imputing a score of 0 for the malesyielded similar overall results
Follow-up analyses directly compared studies thatreported zero-order correlations between IQ at time
1 depression at time 1 and depression at time 2(additional details described in the SupplementaryMethods)
Statistical methods
Data were analyzed using Comprehensive Meta-Analysis software version 30 (Biostat Inc USA) Arandom-effects model was used for expected hetero-geneity across studies A random-effects model alsoallows for broader generalization of results to thepopulation at large Heterogeneity of effects was calcu-lated using the Q statistic where a significant p valueindicates that true effect varies across studies The I2
Fig 1 Flow diagram of the search process
Association between cognitive function and subsequent depression 9
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
statistic was used to calculate the ratio of the true het-erogeneity to total variation acting as an index of sig-nal-to-noise ratio When I2 is large it is has beenrecommended to consider subgroup analysis or meta-regression to account for the variance (Borensteinet al 2011)
Subgroup analyses were conducted using a mixed-effects analysis in which a random effects model wasused to combine studies within each subgroup and afixed effect model was used to combine subgroupsand yield the overall effect (the study-to-study vari-ance is not assumed to be the same for all subgroups)Subgroup analyses were conducted comparing type ofoutcome (continuous v categorical) broad v specificcognitive measures and outcomes that were adjustedv unadjusted for baseline depression symptoms
Meta-regression was performed using the followingvariables on unadjusted analyses age at baseline ageat follow-up time between assessments IQ percentwhite year of cognitive assessment year of follow-upassessment percent female and study quality score
Study quality and publication bias
Study quality was evaluated independently by MSand AP using a checklist adapted from Luppino ampWit (Luppino et al 2010) The checklist contained 12items and studies were rated with a lsquo+rsquo if it met criteriafor that item a lsquominusrsquo if it did not meet criteria for an itemand a rsquorsquo if unclear lsquo+rsquo were coded as a score of 1 andminus were coded as a score of 0 Total scores and percen-tages were calculated Articles with total scores of 0ndash3were considered to be of low quality scores of 4ndash7were considered a medium quality and scores of 8ndash12 were considered to be of high quality Any discrep-ancies (approximately 3 of data points) wereresolved via consensus
Publication bias was assessed using a funnel plotwhich presents study size on the vertical axis (as stand-ard error in this case) as a function of effect size on thex-axis When no publication bias exists the studiesshould be distributed symmetrically about the com-bined effect size (Borenstein et al 2011) If evidenceof publication bias was observed Duval amp Tweediersquostrim-and-fill method was used (Duval amp Tweedie2000) which recalculates effects based on imputingdata from studies that are likely to be missing Lastthe Fail-safe N was calculated (Cooper 1979) whichindicates the number of missing studies that wouldneed to exist to nullify the observed effect
Results
A flow diagram of the search process is shown inFig 1 The search identified 2773 records through
PubMed 2158 through EMBASE and 1345 throughPsycINFO for a total of 6276 records Duplicaterecords (1709) were removed in EndNote resulting in4567 unique records After title and abstracts werereviewed 329 records were identified as potentially eli-gible for the meta-analysis These 329 records werereviewed in full and 300 articles were excluded hier-archically if they were a review baseline or protocolpaper (n = 6) if the sample had a mean age over 65at the depression assessment (n = 41) if the samplehad a specific medical illness (n = 23) if the studywas not a longitudinal design (n = 19) if MDD diagno-sis hospitalization or admission to treatment centerwas part of the inclusion criteria of the study (n = 18)if cognitive function was assessed only concurrentlywith or after depression (n = 36) if cognitive functionwas assessed by educational achievement or self-report(n = 26) if cognitive function was assessed by attribu-tion style rather than neuropsychological measure (n= 7) if there was no measure of cognitive function (n= 18) or no uniquely measured depression outcome(n = 24) Furthermore if articles reported on the samesample as another article with higher quality or moreinformation the duplicate articles were excluded (n =8) Last a number of studies appeared to measureboth cognitive function and depression but did not re-port enough information to be included in the meta-analysis and did not respond to requests for additionalinformation (n = 74 approximately 59 unique samples)In total 29 publication were included in the meta-ana-lysis comprising 34 samples (one study included twoseparate birth cohorts and another four reported dataseparately for men and women)
Study characteristics
The characteristics of included samples are detailed inTable 1 Sample sizes ranged from 43 to 50 053 with amedian of 3395 The most common types of sampleswere school samples (934) community samples (834) and birth cohorts (734) The samples were major-ity white with two samples having exclusively blackparticipants Additionally eight samples were menonly six samples were women only and the restreported combined effect sizes Mean age of partici-pants at baseline ranged from 35 to 59 years with amedian of 12 years Most samples did not reportwhether comorbid diagnoses were present (2334)
Of the 74 papers excluded for having insufficient in-formation (representing 60 unique samples) the me-dian number of subjects was not statistically differentbetween those studies and the studies included in themeta-analysis (n = 288 and n = 3395 respectively p =019) nor did the average age of study participants atbaseline statistically differ (median across studies = 11
10 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
v 12 respectively p = 057) The types of cognitivemeasures used were also similar across the excludedand included studies with the most common measurebeing IQ (2860 and 2029) followed by VerbalComprehension (860 and 529)
Meta-analysis
The overall analysis yielded a significant associationbetween cognitive function and subsequent depressionoutcomes [r =minus0088 95 confidence interval (CI)minus0121 to minus0054 p lt 0001 Fig 2] Results were similarwhen excluding the two studies that used beta-weights(r =minus0071 95 CI minus0100 to minus0042 p lt 0001) orwhen using episodic memory in place of processingspeed in a study reporting both outcomes (r =minus008595 CI minus0118 to minus0051 p lt 0001) Follow-up ana-lyses were conducted in the sample of studies report-ing educational attainment and self-report outcomes(Supplementary Table S2) Heterogeneity across sam-ples was significant (Q = 80154 p lt 0001) suggestingsubstantial variation across the individual samplesThe ratio of the true heterogeneity to total variationwas large (I2 = 9588) I2 is on a relative scale andvalues close to 100 indicate that most of the observedvariance is real rather than spurious and suggeststhat subgroup analyses or meta-regression may helpto explain this variability (Borenstein et al 2011)
Subgroup analyses and meta-regression
A significant difference was found between categoricaland continuous effect sizes (p lt 0001) The studiesassessing continuous outcomes were found to have alarger effect (r =minus0121 95 CI minus0168 to minus0073 p lt0001 n = 22) than studies assessing categorical out-comes (r =minus0035 95 CI minus0054 to minus0017 p lt 0001n = 12) No differences were observed between studiesutilizing broad v specific cognitive measures (p = 057)
Outcomes were also compared adjusting for baselinedepression symptoms at the time of cognitive assess-ment Nine studies provided enough detail to calculatethe partial correlation coefficients adjusting for base-line depression symptoms Using the partial correl-ation coefficients led to a null result (r =minus0032 95CI minus0078 to 0014 p = 0169 n = 9 Fig 3) The nullresult does not seem to be due to a lack of power be-cause using the unadjusted correlation coefficients forthe same nine studies still led to a significant result(r =minus0120 95 CI minus0169 to minus0070 p lt 0001 n = 9Fig 3) As a follow-up the difference in effect sizes be-tween the adjusted and unadjusted values for these 9studies were tested (r = 0082 95 CI 0069ndash0095 p lt0001 n = 9) suggesting that the effects are significantlydifferent when directly comparing the values that doand do not control for baseline depression symptoms
Expanding the subgroup analyses to include studiesthat controlled for baseline depression plus other co-variates (Zammit et al 2004 Simons et al 2009 Rawalamp Rice 2012) and studies that explicitly excluded fora history of depression diagnosis (Gale et al 2008Vinberg et al 2013 Papmeyer et al 2015) did notchange the null result (r =minus0027 95 CI minus0058 to0005 p = 0097 n = 15)
None of the meta-regression analyses were signifi-cant indicating that the between-study variance wasnot attributable to age at baseline IQ percent of sam-ple that was female percent of the sample that waswhite age at follow-up time between assessmentsyear of cognitive assessment year of follow-up assess-ment or study quality score
Study quality and publication bias
Multiple samples within a study were combined forthe purposes of quality assessment given that studieswithin the same publication were found to employthe same methodology Of the 29 publications reviewed12 were rated as high quality and 17 were rated as me-dium quality Details are provided in SupplementaryTable S1 Comparable results to the overall findingswere obtained when just using high quality studies (r=minus0085 95 CI minus0141 to minus0029 p = 0003)
Inspection of the funnel plot (Fig 4) found no evi-dence for publication bias to support the hypothesisIn fact imputation of negative correlations suggestedthat additional studies favoring the hypothesis maybe missing While the calculated effect size is minus0088(95 CI minus0121 to minus0054) using Duval amp Tweediersquostrim-and-fill method the imputed effect size estimateis larger at minus0137 (95 CI minus0176 to minus0099 imputedstudies n = 11) Last the Fail-safe N procedure foundthat 3583 null studies would need to be located forthe combined two-tailed p value to exceed 005 Thissuggests that significant results are not likely to be con-founded by publication bias and may even underesti-mate true effect sizes
Discussion
The present systematic review and meta-analysis of 29longitudinal publications including 1 21 749 partici-pants revealed that after accounting for baseline depres-sion symptoms variability in cognitive function did notpredict subsequent depression Consistent with priorreports there was a significant contemporaneous associ-ation between higher depression symptoms and lowercognitive function These patterns have implications forunderstanding the association between cognitive func-tion and depression and may be important for advan-cing etiologic and treatment research
Association between cognitive function and subsequent depression 11
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
First our findings reinforce models positing thatcognitive function tracks with depression severity(McDermott amp Ebmeier 2009) One possible explan-ation for this contemporaneous association is that de-pression symptoms interfere with the capacity tocomplete cognitive assessments possibly through thegeneral lack of motivation that is one hallmark of thedisorder While this explanation represents an experi-mental confound for studies focused on assessmentof cognitive function it likewise represents an oppor-tunity for studies to focus more comprehensively onthe assessment of both depression and mood disordersymptoms since performance on cognitive tests maybe a sensitive measure of motivational state thatcould augment self-reported symptoms Alternativelythe co-occurrence of cognitive deficits and depressionsymptoms may reflect shared genetic etiology (Hagen-aars et al 2016) and dysfunction of neural circuits
supporting both cognitive and emotional processes(Scult et al 2016) In particular dysfunction of prefront-al and striatal circuits have been associated with bothdepression and cognitive function (Keedwell et al2005 Aarts et al 2011)
Second our findings suggest that prior studies oflinks between cognitive function and depression thatdid not assess baseline symptoms may have overesti-mated the potential protective role of higher cognitivefunction While the importance of accounting for sub-clinical symptoms is not novel the implementation ofsuch accounting is often neglected in psychiatric epi-demiology given the current categorical threshold-based diagnostic system In our meta-analysis largereffects were observed for continuous as compared tocategorical outcomes which aligns with growing em-phasis on dimensional measures of psychopathology(Cuthbert amp Kozak 2013)
Fig 2 Meta-analysis of the association between cognitive function and subsequent depression A forest plot for all studiesthat investigated associations between cognition and later depression Results are reported as correlation coefficients denotedby squares and 95 confidence intervals (CI) indicated by lines (effect sizes are converted to correlation coefficients ifreported as odds ratios) Meta-analysis results are displayed as the diamond The overall analysis found a significant effect ofcognition on depression (r =minus0088 95 CI minus0121 to minus0054 p lt 0001)
12 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Fig 4 Trim-and-fill funnel plots for all samples Fisherrsquos Z a measure of effect size is plotted on the x-axis and the standarderror is plotted on the y-axis Larger studies appear toward the top of the graph and smaller studies towards the bottom Inthe absence of publication bias the studies are symmetrically distributed around the mean Actual studies are shown in opencircles and imputed studies would be shown in black circles No additional studies would be expected in the oppositedirection (to the right) of the observed effect but an additional 11 studies are imputed to the left of the mean effect sizeWhile the calculated effect size is minus0088 [95 confidence interval (CI) minus0121 to minus0054] using Duval amp Tweediersquos trim-and-fill method the imputed effect size estimate is larger at minus0137 (95 CI minus0176 to minus0099 imputed studies n = 11)
Fig 3 Meta-analysis comparing values adjusted for baseline depression symptoms v unadjusted A forest plot for analysiscomparing results from a subset of the same set of studies reported in Fig 2 when using unadjusted values compared tousing values that are adjusted for baseline depression Effects are significant for unadjusted values [r =minus0120 95 confidenceinterval (CI) minus0169 to minus0070 p lt 0001] but not for adjusted values (r =minus0032 95 CI minus0078 to 0014 p = 0169) Results arereported as correlation coefficients denoted by squares and 95 CIs indicated by lines Meta-analysis results are displayed asdiamonds
Association between cognitive function and subsequent depression 13
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Third the associations between cognitive functionand either current or later depression were not moder-ated by data quality or participant age sex and raceHowever there are a number of additional potentialmoderators that could not be addressed in the currentreview and meta-analysis For example the numberand type of comorbid conditions with depressionwere often not reported in the included studies butcould represent an important moderator of theobserved effects Modeling the effects of comorbid ill-ness is an important avenue for future research
One limitation of the current literature is that only ahandful of studies reviewed explicitly excluded for de-pression diagnosis at baseline (Gale et al 2008 Vinberget al 2013 Papmeyer et al 2015) however consistentwith the finding that controlling for baseline depres-sion symptoms led to a null association between cogni-tion and subsequent depression there was no effectobserved when including these studies in the sub-group analyses further suggesting that the associationbetween cognitive function and depression is likelycontemporaneous It will be important to follow-upthese analyses with individual studies that includerigorous assessment of baseline depression symptomsand other potentially confounding factors to furtherclarify this relationship
An open question that remains for future research iswhether deficits in cognitive function are likely to pre-dict the development of more sever or recurrent de-pression later in life Only one of the included studies(Koenen et al 2009) specifically investigated recurrentdepression and found that lower IQ was associatedwith greater persistence of disorder
A final consideration is that while our review andmeta-analysis focused on general cognitive functionmainly assessed via IQ there may be specific subtypesof cognitive function that are more predictive of laterdepression For example a lack of cognitive flexibilitymay more closely match with the ruminative stylecharacteristic of depression and therefore tasks specifi-cally measuring this component of cognitive functionmight have some predictive utility While our reviewdid not find differences between broad and specificmeasures of cognitive function there were not enoughstudies identified to allow for precise consideration ofdifferences between individual cognitive domains
A limitation of the meta-analysis is that while thepresent study followed standard guidelines (Stroupet al 2000 Atkinson et al 2014) decisions aboutstudy selection data extraction and quality assess-ment include a number of decision points that neces-sarily involve a level of subjectivity Reliability wasascertained by using independent raters however dif-ferent inclusionexclusion criteria or a different ap-proach to the evaluation of those criteria could result
in a different set of studies being includedUltimately the quality of the meta-analysis is depend-ent upon the underlying studies that are analyzedFurthermore although studies with insufficient infor-mation to be included in the meta-analysis were notfound to differ based on basic study data from thosestudies included in the meta-analysis nonetheless itis unknown how if at all data from these studiescould change the overall results
Acknowledging these limitations our present reviewand meta-analysis found that while an association is evi-dent between cognitive function and later depressiongeneral cognitive function does not appear to be a riskfactor for depression but rather is more likely relatedto performance decrements associated with concurrentdepressive symptoms Our results suggest that low cog-nitive function is therefore probably not a causal factorof depression and that clinical practice may benefitmore from a focus on how decreased cognitive functionin the depressed state is likely to influence treatment out-comes (Gyurak et al 2015) Our findings have importantimplications for better understanding depression and forthe design of future studies in highlighting the need tocontrol for subthreshold depression symptoms when in-vestigating risk factors for mental illness as well as whenassessing cognitive function more generally
Supplementary material
The supplementary material for this article can befound at httpdxdoiorg101017S0033291716002075
Acknowledgements
MAS is supported by an National Science Foundation(NSF) Graduate Research Fellowship ARH is sup-ported by National Institutes of Health (NIH) grantsRO1DA033369 amp R01AG049789 TEM is supportedby National Institutes of Health (NIH) grantsR01AG049789 We would like to thank HarrisCooper PhD at Duke University who provided invalu-able insight into conducting the meta-analysis Wethank all of the authors of studies who provided add-itional information for this meta-analysis
Declaration of Interest
None
References
Aarts E van Holstein M Cools R (2011) Striatal dopamineand the interface between motivation and cognitionFrontiers in Psychology 2 163
14 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Atkinson KM Koenka AC Sanchez CE Moshontz HCooper H (2014) Reporting standards for literaturesearches and report inclusion criteria making researchsyntheses more transparent and easy to replicate ResearchSynthesis Methods 6 87ndash95
Baer LH Tabri N Blair M Bye D Li KZH Pushkar D(2013) Longitudinal associations of need for cognitioncognitive activity and depressive symptomatology withcognitive function in recent retirees Journals of GerontologySeries B Psychological Sciences and Social Sciences 68 655ndash664
Barbey AK Colom R Solomon J Krueger F Forbes CGrafman J (2012) An integrative architecture for generalintelligence and executive function revealed by lesionmapping Brain 135 1154ndash1164
Barnett JH Salmond CH Jones PB Sahakian BJ (2006)Cognitive reserve in neuropsychiatry Psychological Medicine36 1053ndash1064
Beaujean AA Parker S Qiu X (2013) The relationshipbetween cognitive ability and depression a longitudinaldata analysis Social Psychiatry and Psychiatric Epidemiology48 1983ndash1992
Belsky DW Caspi A Arseneault L Bleidorn W Fonagy PGoodman M Houts R Moffitt TE (2012) Etiologicalfeatures of borderline personality related characteristics in abirth cohort of 12-year-old children Development andPsychopathology 24 251ndash265
Betts KS Williams GM Najman JM Alati R (2016)Predicting spectrums of adult mania psychosis anddepression by prospectively ascertained childhoodneurodevelopment Journal of Psychiatric Research 72 22ndash29
Bora E Harrison BJ Yuumlcel M Pantelis C (2013) Cognitiveimpairment in euthymic major depressive disorder a meta-analysis Psychological Medicine 43 2017ndash2026
Borenstein M Hedges LV Higgins JPT Rothstein HR(2011) Introduction to Meta-Analysis John Wiley amp SonsWest Sussex UK
Canals J Domegravenech-Llaberia E Fernaacutendez-Ballart J Martiacute-Henneberg C (2002) Predictors of depression at eighteenA 7-year follow-up study in a Spanish nonclinicalpopulation European Child amp Adolescent Psychiatry 11226ndash233
Christensen H Griffiths K Mackinnon A (1997) Aquantitative review of cognitive deficits in depression andAlzheimer-type dementia Selection of Studies 3 631ndash651
Connolly SL Wagner Ca Shapero BG Pendergast LLAbramson LY Alloy LB (2014) Rumination prospectivelypredicts executive functioning impairments in adolescentsJournal of Behavior Therapy and Experimental Psychiatry 4546ndash56
Cooper HM (1979) Statistically combining independentstudies a meta-analysis of sex differences in conformityresearch Journal of Personality and Social Psychology 37131ndash146
Cooper HM (2010) Research Synthesis and Meta-Analysis AStep-by-Step Approach 4th edn SAGE PublicationsWashington (DC) USA
Cuijpers P de Graaf R van Dorsselaer S (2004) Minordepression risk profiles functional disability health careuse and risk of developing major depression Journal ofAffective Disorders 79 71ndash79
Cuthbert BN Kozak MJ (2013) Constructing constructs forpsychopathology the NIMH research domain criteriaJournal of Abnormal Psychology 122 928ndash937
Der G Batty GD Deary IJ (2009) The association between IQin adolescence and a range of health outcomes at 40 in the1979 US National Longitudinal Study of Youth Intelligence37 573ndash580
Dubow EF Boxer P Huesmann LR (2008) Childhood andadolescent predictors of early and middle adulthoodalcohol use and problem drinking the Columbia CountyLongitudinal Study Addiction 103 36ndash47
Duval S Tweedie R (2000) Trim and fill a simple funnel-plot-based method of testing and adjusting for publicationbias in meta-analysis Biometrics 56 455ndash463
Evans LD Kouros CD Samanez-Larkin S Garber J (2015)Concurrent and short-term prospective relations amongneurocognitive functioning coping and depressivesymptoms in youth Journal of Clinical Child and AdolescentPsychology 53 1ndash15
Franz CE Lyons MJ OrsquoBrien R Panizzon MS Kim K BhatR Grant MD Toomey R Eisen S Xian H Kremen WS(2011) A 35-year longitudinal assessment of cognition andmidlife depression symptoms the Vietnam Era Twin Studyof Aging American Association for Geriatric PsychiatryAmerican Journal of Geriatric Psychiatry 19 559ndash570
Gale CR Batty GD Tynelius P Deary IJ Rasmussen F(2010) Intelligence in early adulthood and subsequenthospitalization for mental disorders Epidemiology 2170ndash77
Gale CR Deary IJ Boyle SH Barefoot J Mortensen LHBatty GD (2008) Cognitive ability in early adulthood andrisk of 5 specific psychiatric disorders in middle age theVietnam experience study Archives of General Psychiatry 651410ndash1418
Gale CR Hatch SL Batty GD Deary IJ (2009) Intelligence inchildhood and risk of psychological distress in adulthoodthe 1958 National Child Development Survey and the 1970British Cohort Study Intelligence 37 592ndash599
Gjerde PF (1995) Alternative pathways to chronicdepressive symptoms in young adults gender differencesin developmental trajectories Child Development 661277ndash1300
Gottfredson LS (1997) Mainstream science on intelligence aneditorial with 52 signatories history and bibliographyIntelligence 24 13ndash23
Guyer AE Choate VR Grimm KJ Pine DS Keenan K(2011) Emerging depression is associated with facememory deficits in adolescent girls Elsevier Inc Journal ofthe American Academy of Child and Adolescent Psychiatry 50180ndash190
Gyurak A Patenaude B Korgaonkar MS Grieve SMWilliams LM Etkin A (2015) Frontoparietal activationduring response inhibition predicts remission toantidepressants in patients with major depression BiologicalPsychiatry 79 1ndash8
Hagenaars SP Harris SE Davies G Hill WD LiewaldDCM Ritchie SJ Marioni RE Fawns-Ritchie C Cullen BMalik R METASTROKE Consortium IC for BPGSpiroMeta Consortium CHARGE ConsortiumPulmonary Group CCA and LG Worrall BB Sudlow
Association between cognitive function and subsequent depression 15
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
CLM Wardlaw JM Gallacher J Pell J McIntosh AMSmith DJ Gale CR Deary IJ (2016) Shared geneticaetiology between cognitive functions and physical andmental health in UK Biobank (N = 112 151) and 24 GWASconsortiaMolecular Psychiatry Published online 26 January2016 doi101038mp2015225
Hatch SL Jones PB Kuh D Hardy R Wadsworth MEJRichards M (2007) Childhood cognitive ability and adultmental health in the British 1946 birth cohort Social Scienceamp Medicine (1982) 64 2285ndash2296
Hipwell AE Sapotichne B Klostermann S Battista DKeenan K (2011) Autobiographical memory as a predictorof depression vulnerability in girls Journal of Clinical Childand Adolescent Psychology 40 254ndash265
Horowitz JL Garber J (2003) Relation of intelligence andreligiosity to depressive disorders in offspring of depressedand nondepressed mothers The American Academy ofChild and Adolescent Psychiatry Journal of the AmericanAcademy of Child and Adolescent Psychiatry 42 578ndash586
Johnson W Bouchard TJ Krueger RF McGue MGottesman II (2004) Just one g consistent results fromthree test batteries Intelligence 32 95ndash107
Keedwell PA Andrew C Williams SCR Brammer MJPhillips ML (2005) The neural correlates of anhedoniain major depressive disorder Biological Psychiatry 58843ndash853
Kessler RC Berglund P Demler O Jin R Koretz DMerikangas KR Rush AJ Walters EE Wang PS (2003)The epidemiology of major depressive disorder resultsfrom the National Comorbidity Survey Replication(NCS-R) Journal of the American Medical Association 2893095ndash3105
Koenen KC Moffitt TE Roberts AL Martin LT KubzanskyL Harrington H Poulton R Caspi A (2009) Childhood IQand adult mental disorders a test of the cognitive reservehypothesis American Journal of Psychiatry 166 50ndash57
Lewinsohn PM Solomon A Seeley JR Zeiss A (2000)Clinical implications of lsquosubthresholdrsquo depressivesymptoms Journal of Abnormal Psychology 109 345ndash351
Luppino FS de Wit LM Bouvy PF Stijnen T Cuijpers PPenninx BWJH Zitman FG (2010) Overweight obesityand depression a systematic review and meta-analysisof longitudinal studies Archives of General Psychiatry 67220ndash229
McCord J Ensminger ME (1997) Multiple risks andcomorbidity in an African-American population CriminalBehaviour and Mental Health 7 339ndash352
McDermott LM Ebmeier KP (2009) A meta-analysis ofdepression severity and cognitive function Elsevier BVJournal of Affective Disorders 119 1ndash8
Melartin TK Rytsaumllauml HJ Leskelauml US Lestelauml-Mielonen PSSokero TP Isometsauml ET (2002) Current comorbidity ofpsychiatric disorders among DSM-IV major depressivedisorder patients in psychiatric care in the VantaaDepression Study Journal of Clinical Psychiatry 63 126ndash134
Meyer SE Carlson GA Wiggs EA Martinez PE RonsavilleDS KlimesndashDougan B Gold PW RadkendashYarrow M(2004) A prospective study of the association amongimpaired executive functioning childhood attentional
problems and the development of bipolar disorderDevelopment and Psychopathology 16 461ndash476
MiyakeA FriedmanNP EmersonMJWitzki aHHowerter AWager TD (2000) The unity and diversity of executivefunctions and their contributions to complex lsquoFrontal Lobersquotasks a latentvariable analysisCognitive Psychology41 49ndash100
Moher D Liberati A (2009) Preferred reporting items forsystematic reviews and meta-analyses the PRISMAstatement Annals of Internal Medicine 151 264ndash269
Papmeyer M Sussmann JE Hall J McKirdy J Peel AMacdonald A Lawrie SM Whalley HC McIntosh AM(2015) Neurocognition in individuals at high familial riskof mood disorders with or without subsequent onset ofdepression Psychological Medicine 45 1ndash11
Peterson RA Brown SP (2005) On the use of betacoefficients in meta-analysis Journal of Applied Psychology90 175ndash181
Pine DS Cohen P Brook J Coplan JD (1997) Psychiatricsymptoms in adolescence as predictors of obesity in earlyadulthood a longitudinal study American Journal of PublicHealth 87 1303ndash1310
Quinn ME Joormann J (2015) Control when it countschange in executive control under stress predicts depressionsymptoms Emotion Junio 22 1ndash10
Rawal A Rice F (2012) Examining overgeneralautobiographical memory as a risk factor for adolescentdepression Elsevier Inc Journal of the American Academy ofChild and Adolescent Psychiatry 51 518ndash527
Ree MJ Earles JA (1991) The stability of g across differentmethods of estimation Intelligence 15 271ndash278
Rock PL Roiser JP Riedel WJ Blackwell AD (2014)Cognitive impairment in depression a systematic reviewand meta-analysis Psychological Medicine 44 2029ndash2040
Rogers MA Kasai K Koji M Fukuda R Iwanami ANakagome K Fukuda M Kato N (2004) Executive andprefrontal dysfunction in unipolar depression a review ofneuropsychological and imaging evidence NeuroscienceResearch 50 1ndash11
Scult MA Knodt AR Swartz JR Brigidi BD Hariri AR(2016) Thinking and feeling individual differences inhabitual emotion regulation and stress-related mood areassociated with prefrontal executive control ClinicalPsychological Science doi1011772167702616654688
Sharp C Petersen N Goodyer I (2008) Emotional reactivityand the emergence of conduct problems and emotionalsymptoms in 7- to 11-year-olds a 1-year follow-up studyJournal of the American Academy of Child and AdolescentPsychiatry 47 565ndash573
Siegel LS (1999) Issues in the definition and diagnosis oflearning disabilities a perspective on Guckenberger vBoston University Journal of Learning Disabilities 32 304ndash319
Simons CJP Jacobs N Derom C Thiery E Jolles J van Os JKrabbendam L (2009) Cognition as predictor of currentand follow-up depressive symptoms in the generalpopulation Acta Psychiatrica Scandinavica 120 45ndash52
Slykerman RF Thompson J Waldie K Murphy R Wall CMitchell EA (2015) Maternal stress during pregnancy isassociated with moderate to severe depression in 11-year-old children Acta Paediatrica 104 68ndash74
16 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Snyder HR (2013) Major depressive disorder is associatedwith broad impairments on neuropsychological measuresof executive function a meta-analysis and reviewPsychological Bulletin 139 81ndash132
Soslashrensen HJ Saeligbye D Urfer-Parnas A Mortensen ELParnas J (2012) Premorbid intelligence and educationallevel in bipolar and unipolar disorders a Danish draftboard study Journal of Affective Disorders 136 1188ndash1191
SpearmanC (1904) lsquoGeneral intelligencersquoobjectivelydeterminedandmeasuredAmerican Journal of Psychology 15 201
Stern Y (2003) The concept of cognitive reserve a catalyst forresearch Journal of Clinical and Experimental Neuropsychology(Neuropsychology Development and Cognition Section A) 25589ndash593
Stroup D Berlin J Morton S Olkin I Williamson GDRennie D Moher D Becker BJ Sipe TA Thacker SB(2000) Meta-analysis of Observational Studies inEpidemiology a proposal for reporting Journal of theAmerican Medical Association 283 2008
Vinberg M Miskowiak KW Kessing LV (2013) Impairmentof executive function and attention predicts onset ofaffective disorder in healthy high-risk twins Journal ofClinical Psychiatry 74 e747ndashe753
Zammit S Allebeck P David AS Dalman C HemmingssonT Lundberg I Lewis G (2004) A longitudinal study ofpremorbid IQ Score and risk of developing schizophreniabipolar disorder severe depression and other nonaffectivepsychoses Archives of General Psychiatry 61 354ndash360
Association between cognitive function and subsequent depression 17
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms

to investigate general information processing abilitiesrather than cognitive attributional style studies withcognitive attribution measures as the sole cognitivemeasure were excluded
Comparisons
Search terms used to indicate the possible associationbetween cognitive function and depression includedrisk premorbid prodromal onset predict and association(for a full list see search terms in the SupplementaryMaterial) When data were reported from multipletime-points the analysis accounting for the longesttime between assessments was used
Outcomes
Eligible studies reported depression diagnosis orsymptoms determined by investigator or self-reportPresence of comorbidity was permitted given that de-pression has been found to be highly comorbid withother disorders (Melartin et al 2002 Kessler et al2003) Articles not adequately specifying how depres-sion was assessed or articles that did not uniquelymeasure depression [ie only had an index of lsquomentaldisordersrsquo or the category of lsquomood disordersrsquo lumpedtogether (Gale et al 2010)] were excluded if no uniquemeasure of depression could be obtained from studyauthors This is because although comorbidity waspermitted these could have represented instances ofpure anxiety disorders with few or no depressivesymptoms or instances of bipolar disorder
Study design
Eligible study search terms included cohort studies lon-gitudinal epidemiological prospective retrospective follow-up or case-control studies Studies not following a longi-tudinal design were excluded during full-text reviewAdditionally studies where cognitive function wasassessed only concurrently with or after depressionwere excluded given that the purpose of the reviewwas to investigate whether cognitive function pre-dicted later depression
Studies were included regardless of whether theywere reported in peer-review journals in order to ac-count for potentially biased reporting of resultsReview articles were included in the search terms tofind additional relevant references but were notincluded in the meta-analysis Baseline and protocolstudies without follow-up data were excluded
Study selection
A flow diagram of the process of study selection showsthe overall procedures (Fig 1) Records identified fromthe search processes were combined in EndNote
software version X7 and duplicates were removedTitles and abstracts were reviewed independently bytwo reviewers (MS and AP) according to the eligibil-ity criteria described above and marked as either po-tentially eligible or not eligible If either authormarked an article as potentially eligible it wasincluded in the full-text review for closer examinationby MS and AP who used an electronic form to indi-cate if an article should be included or excluded in thefinal selection When an article was excluded the rea-son for exclusion was selected from a hierarchical listof exclusion criteria presented in Fig 1 Both MSand AP were initially blinded to the otherrsquos decisionsAfter both MS and AP completed their reviews dis-crepancies about whether a study should be includedor excluded were resolved via discussion and consen-sus amongst MS AP TM AH and TS
Data extraction
Study information was extracted independently byMS and AP using an electronic form created forthis study Information was collected and codedbased on report characteristics participant characteris-tics study setting predictors outcome measures andquality assessment (Cooper 2010) Any discrepancies(approximately 3 of data points) were resolved viaconsensus
For studies with categorical depression diagnoses ef-fect sizes were generally presented as odds ratios Forthese studies the odds ratio plus the upper and lowerbound of the confidence interval were recorded Twoof the studies (Zammit et al 2004 Gale et al 2008)reported odds ratios greater than one to indicate thatlower IQ was associated with greater risk of depressionThe other studies reported odds ratios in the reverseleading to odds ratios less than one for the same direc-tion of the effect Therefore the odds ratios from the firsttwo studies were recalculated by dividing (1oddsratio) Another study (McCord amp Ensminger 1997)reported results from chi-squared tests Additional stud-ies reported mean premorbid IQ scores rather than oddsratios in which case the means sample sizes andor pvalues and number of tails of the t test were utilizedto calculate the effect size
For studies in which depression was measured as acontinuous variable effect sizes were presented as cor-relation coefficients The direction of the effect (posi-tive or negative) and the sample size were alsoextracted to be used in the meta-analysis Two studiesreported only beta weights (Simons et al 2009 Rawalamp Rice 2012) and we were not able to obtain zero-order correlations from the authors Given that previ-ous reports have suggested that beta weights can beused as an estimate of correlation coefficients in
8 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
meta-analysis (Peterson amp Brown 2005) the betaweights were used instead and analyses were runboth including and excluding these data points
When insufficient information was presented in thearticle authors were contacted requesting further de-tail An additional six studies were included at thispoint One study (Hatch et al 2007) included effectsizes for the female half of the cohort and did not pro-vide statistics for the males but did indicate a null ef-fect Only women from this study were included in themeta-analyses but imputing a score of 0 for the malesyielded similar overall results
Follow-up analyses directly compared studies thatreported zero-order correlations between IQ at time
1 depression at time 1 and depression at time 2(additional details described in the SupplementaryMethods)
Statistical methods
Data were analyzed using Comprehensive Meta-Analysis software version 30 (Biostat Inc USA) Arandom-effects model was used for expected hetero-geneity across studies A random-effects model alsoallows for broader generalization of results to thepopulation at large Heterogeneity of effects was calcu-lated using the Q statistic where a significant p valueindicates that true effect varies across studies The I2
Fig 1 Flow diagram of the search process
Association between cognitive function and subsequent depression 9
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
statistic was used to calculate the ratio of the true het-erogeneity to total variation acting as an index of sig-nal-to-noise ratio When I2 is large it is has beenrecommended to consider subgroup analysis or meta-regression to account for the variance (Borensteinet al 2011)
Subgroup analyses were conducted using a mixed-effects analysis in which a random effects model wasused to combine studies within each subgroup and afixed effect model was used to combine subgroupsand yield the overall effect (the study-to-study vari-ance is not assumed to be the same for all subgroups)Subgroup analyses were conducted comparing type ofoutcome (continuous v categorical) broad v specificcognitive measures and outcomes that were adjustedv unadjusted for baseline depression symptoms
Meta-regression was performed using the followingvariables on unadjusted analyses age at baseline ageat follow-up time between assessments IQ percentwhite year of cognitive assessment year of follow-upassessment percent female and study quality score
Study quality and publication bias
Study quality was evaluated independently by MSand AP using a checklist adapted from Luppino ampWit (Luppino et al 2010) The checklist contained 12items and studies were rated with a lsquo+rsquo if it met criteriafor that item a lsquominusrsquo if it did not meet criteria for an itemand a rsquorsquo if unclear lsquo+rsquo were coded as a score of 1 andminus were coded as a score of 0 Total scores and percen-tages were calculated Articles with total scores of 0ndash3were considered to be of low quality scores of 4ndash7were considered a medium quality and scores of 8ndash12 were considered to be of high quality Any discrep-ancies (approximately 3 of data points) wereresolved via consensus
Publication bias was assessed using a funnel plotwhich presents study size on the vertical axis (as stand-ard error in this case) as a function of effect size on thex-axis When no publication bias exists the studiesshould be distributed symmetrically about the com-bined effect size (Borenstein et al 2011) If evidenceof publication bias was observed Duval amp Tweediersquostrim-and-fill method was used (Duval amp Tweedie2000) which recalculates effects based on imputingdata from studies that are likely to be missing Lastthe Fail-safe N was calculated (Cooper 1979) whichindicates the number of missing studies that wouldneed to exist to nullify the observed effect
Results
A flow diagram of the search process is shown inFig 1 The search identified 2773 records through
PubMed 2158 through EMBASE and 1345 throughPsycINFO for a total of 6276 records Duplicaterecords (1709) were removed in EndNote resulting in4567 unique records After title and abstracts werereviewed 329 records were identified as potentially eli-gible for the meta-analysis These 329 records werereviewed in full and 300 articles were excluded hier-archically if they were a review baseline or protocolpaper (n = 6) if the sample had a mean age over 65at the depression assessment (n = 41) if the samplehad a specific medical illness (n = 23) if the studywas not a longitudinal design (n = 19) if MDD diagno-sis hospitalization or admission to treatment centerwas part of the inclusion criteria of the study (n = 18)if cognitive function was assessed only concurrentlywith or after depression (n = 36) if cognitive functionwas assessed by educational achievement or self-report(n = 26) if cognitive function was assessed by attribu-tion style rather than neuropsychological measure (n= 7) if there was no measure of cognitive function (n= 18) or no uniquely measured depression outcome(n = 24) Furthermore if articles reported on the samesample as another article with higher quality or moreinformation the duplicate articles were excluded (n =8) Last a number of studies appeared to measureboth cognitive function and depression but did not re-port enough information to be included in the meta-analysis and did not respond to requests for additionalinformation (n = 74 approximately 59 unique samples)In total 29 publication were included in the meta-ana-lysis comprising 34 samples (one study included twoseparate birth cohorts and another four reported dataseparately for men and women)
Study characteristics
The characteristics of included samples are detailed inTable 1 Sample sizes ranged from 43 to 50 053 with amedian of 3395 The most common types of sampleswere school samples (934) community samples (834) and birth cohorts (734) The samples were major-ity white with two samples having exclusively blackparticipants Additionally eight samples were menonly six samples were women only and the restreported combined effect sizes Mean age of partici-pants at baseline ranged from 35 to 59 years with amedian of 12 years Most samples did not reportwhether comorbid diagnoses were present (2334)
Of the 74 papers excluded for having insufficient in-formation (representing 60 unique samples) the me-dian number of subjects was not statistically differentbetween those studies and the studies included in themeta-analysis (n = 288 and n = 3395 respectively p =019) nor did the average age of study participants atbaseline statistically differ (median across studies = 11
10 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
v 12 respectively p = 057) The types of cognitivemeasures used were also similar across the excludedand included studies with the most common measurebeing IQ (2860 and 2029) followed by VerbalComprehension (860 and 529)
Meta-analysis
The overall analysis yielded a significant associationbetween cognitive function and subsequent depressionoutcomes [r =minus0088 95 confidence interval (CI)minus0121 to minus0054 p lt 0001 Fig 2] Results were similarwhen excluding the two studies that used beta-weights(r =minus0071 95 CI minus0100 to minus0042 p lt 0001) orwhen using episodic memory in place of processingspeed in a study reporting both outcomes (r =minus008595 CI minus0118 to minus0051 p lt 0001) Follow-up ana-lyses were conducted in the sample of studies report-ing educational attainment and self-report outcomes(Supplementary Table S2) Heterogeneity across sam-ples was significant (Q = 80154 p lt 0001) suggestingsubstantial variation across the individual samplesThe ratio of the true heterogeneity to total variationwas large (I2 = 9588) I2 is on a relative scale andvalues close to 100 indicate that most of the observedvariance is real rather than spurious and suggeststhat subgroup analyses or meta-regression may helpto explain this variability (Borenstein et al 2011)
Subgroup analyses and meta-regression
A significant difference was found between categoricaland continuous effect sizes (p lt 0001) The studiesassessing continuous outcomes were found to have alarger effect (r =minus0121 95 CI minus0168 to minus0073 p lt0001 n = 22) than studies assessing categorical out-comes (r =minus0035 95 CI minus0054 to minus0017 p lt 0001n = 12) No differences were observed between studiesutilizing broad v specific cognitive measures (p = 057)
Outcomes were also compared adjusting for baselinedepression symptoms at the time of cognitive assess-ment Nine studies provided enough detail to calculatethe partial correlation coefficients adjusting for base-line depression symptoms Using the partial correl-ation coefficients led to a null result (r =minus0032 95CI minus0078 to 0014 p = 0169 n = 9 Fig 3) The nullresult does not seem to be due to a lack of power be-cause using the unadjusted correlation coefficients forthe same nine studies still led to a significant result(r =minus0120 95 CI minus0169 to minus0070 p lt 0001 n = 9Fig 3) As a follow-up the difference in effect sizes be-tween the adjusted and unadjusted values for these 9studies were tested (r = 0082 95 CI 0069ndash0095 p lt0001 n = 9) suggesting that the effects are significantlydifferent when directly comparing the values that doand do not control for baseline depression symptoms
Expanding the subgroup analyses to include studiesthat controlled for baseline depression plus other co-variates (Zammit et al 2004 Simons et al 2009 Rawalamp Rice 2012) and studies that explicitly excluded fora history of depression diagnosis (Gale et al 2008Vinberg et al 2013 Papmeyer et al 2015) did notchange the null result (r =minus0027 95 CI minus0058 to0005 p = 0097 n = 15)
None of the meta-regression analyses were signifi-cant indicating that the between-study variance wasnot attributable to age at baseline IQ percent of sam-ple that was female percent of the sample that waswhite age at follow-up time between assessmentsyear of cognitive assessment year of follow-up assess-ment or study quality score
Study quality and publication bias
Multiple samples within a study were combined forthe purposes of quality assessment given that studieswithin the same publication were found to employthe same methodology Of the 29 publications reviewed12 were rated as high quality and 17 were rated as me-dium quality Details are provided in SupplementaryTable S1 Comparable results to the overall findingswere obtained when just using high quality studies (r=minus0085 95 CI minus0141 to minus0029 p = 0003)
Inspection of the funnel plot (Fig 4) found no evi-dence for publication bias to support the hypothesisIn fact imputation of negative correlations suggestedthat additional studies favoring the hypothesis maybe missing While the calculated effect size is minus0088(95 CI minus0121 to minus0054) using Duval amp Tweediersquostrim-and-fill method the imputed effect size estimateis larger at minus0137 (95 CI minus0176 to minus0099 imputedstudies n = 11) Last the Fail-safe N procedure foundthat 3583 null studies would need to be located forthe combined two-tailed p value to exceed 005 Thissuggests that significant results are not likely to be con-founded by publication bias and may even underesti-mate true effect sizes
Discussion
The present systematic review and meta-analysis of 29longitudinal publications including 1 21 749 partici-pants revealed that after accounting for baseline depres-sion symptoms variability in cognitive function did notpredict subsequent depression Consistent with priorreports there was a significant contemporaneous associ-ation between higher depression symptoms and lowercognitive function These patterns have implications forunderstanding the association between cognitive func-tion and depression and may be important for advan-cing etiologic and treatment research
Association between cognitive function and subsequent depression 11
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
First our findings reinforce models positing thatcognitive function tracks with depression severity(McDermott amp Ebmeier 2009) One possible explan-ation for this contemporaneous association is that de-pression symptoms interfere with the capacity tocomplete cognitive assessments possibly through thegeneral lack of motivation that is one hallmark of thedisorder While this explanation represents an experi-mental confound for studies focused on assessmentof cognitive function it likewise represents an oppor-tunity for studies to focus more comprehensively onthe assessment of both depression and mood disordersymptoms since performance on cognitive tests maybe a sensitive measure of motivational state thatcould augment self-reported symptoms Alternativelythe co-occurrence of cognitive deficits and depressionsymptoms may reflect shared genetic etiology (Hagen-aars et al 2016) and dysfunction of neural circuits
supporting both cognitive and emotional processes(Scult et al 2016) In particular dysfunction of prefront-al and striatal circuits have been associated with bothdepression and cognitive function (Keedwell et al2005 Aarts et al 2011)
Second our findings suggest that prior studies oflinks between cognitive function and depression thatdid not assess baseline symptoms may have overesti-mated the potential protective role of higher cognitivefunction While the importance of accounting for sub-clinical symptoms is not novel the implementation ofsuch accounting is often neglected in psychiatric epi-demiology given the current categorical threshold-based diagnostic system In our meta-analysis largereffects were observed for continuous as compared tocategorical outcomes which aligns with growing em-phasis on dimensional measures of psychopathology(Cuthbert amp Kozak 2013)
Fig 2 Meta-analysis of the association between cognitive function and subsequent depression A forest plot for all studiesthat investigated associations between cognition and later depression Results are reported as correlation coefficients denotedby squares and 95 confidence intervals (CI) indicated by lines (effect sizes are converted to correlation coefficients ifreported as odds ratios) Meta-analysis results are displayed as the diamond The overall analysis found a significant effect ofcognition on depression (r =minus0088 95 CI minus0121 to minus0054 p lt 0001)
12 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Fig 4 Trim-and-fill funnel plots for all samples Fisherrsquos Z a measure of effect size is plotted on the x-axis and the standarderror is plotted on the y-axis Larger studies appear toward the top of the graph and smaller studies towards the bottom Inthe absence of publication bias the studies are symmetrically distributed around the mean Actual studies are shown in opencircles and imputed studies would be shown in black circles No additional studies would be expected in the oppositedirection (to the right) of the observed effect but an additional 11 studies are imputed to the left of the mean effect sizeWhile the calculated effect size is minus0088 [95 confidence interval (CI) minus0121 to minus0054] using Duval amp Tweediersquos trim-and-fill method the imputed effect size estimate is larger at minus0137 (95 CI minus0176 to minus0099 imputed studies n = 11)
Fig 3 Meta-analysis comparing values adjusted for baseline depression symptoms v unadjusted A forest plot for analysiscomparing results from a subset of the same set of studies reported in Fig 2 when using unadjusted values compared tousing values that are adjusted for baseline depression Effects are significant for unadjusted values [r =minus0120 95 confidenceinterval (CI) minus0169 to minus0070 p lt 0001] but not for adjusted values (r =minus0032 95 CI minus0078 to 0014 p = 0169) Results arereported as correlation coefficients denoted by squares and 95 CIs indicated by lines Meta-analysis results are displayed asdiamonds
Association between cognitive function and subsequent depression 13
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Third the associations between cognitive functionand either current or later depression were not moder-ated by data quality or participant age sex and raceHowever there are a number of additional potentialmoderators that could not be addressed in the currentreview and meta-analysis For example the numberand type of comorbid conditions with depressionwere often not reported in the included studies butcould represent an important moderator of theobserved effects Modeling the effects of comorbid ill-ness is an important avenue for future research
One limitation of the current literature is that only ahandful of studies reviewed explicitly excluded for de-pression diagnosis at baseline (Gale et al 2008 Vinberget al 2013 Papmeyer et al 2015) however consistentwith the finding that controlling for baseline depres-sion symptoms led to a null association between cogni-tion and subsequent depression there was no effectobserved when including these studies in the sub-group analyses further suggesting that the associationbetween cognitive function and depression is likelycontemporaneous It will be important to follow-upthese analyses with individual studies that includerigorous assessment of baseline depression symptomsand other potentially confounding factors to furtherclarify this relationship
An open question that remains for future research iswhether deficits in cognitive function are likely to pre-dict the development of more sever or recurrent de-pression later in life Only one of the included studies(Koenen et al 2009) specifically investigated recurrentdepression and found that lower IQ was associatedwith greater persistence of disorder
A final consideration is that while our review andmeta-analysis focused on general cognitive functionmainly assessed via IQ there may be specific subtypesof cognitive function that are more predictive of laterdepression For example a lack of cognitive flexibilitymay more closely match with the ruminative stylecharacteristic of depression and therefore tasks specifi-cally measuring this component of cognitive functionmight have some predictive utility While our reviewdid not find differences between broad and specificmeasures of cognitive function there were not enoughstudies identified to allow for precise consideration ofdifferences between individual cognitive domains
A limitation of the meta-analysis is that while thepresent study followed standard guidelines (Stroupet al 2000 Atkinson et al 2014) decisions aboutstudy selection data extraction and quality assess-ment include a number of decision points that neces-sarily involve a level of subjectivity Reliability wasascertained by using independent raters however dif-ferent inclusionexclusion criteria or a different ap-proach to the evaluation of those criteria could result
in a different set of studies being includedUltimately the quality of the meta-analysis is depend-ent upon the underlying studies that are analyzedFurthermore although studies with insufficient infor-mation to be included in the meta-analysis were notfound to differ based on basic study data from thosestudies included in the meta-analysis nonetheless itis unknown how if at all data from these studiescould change the overall results
Acknowledging these limitations our present reviewand meta-analysis found that while an association is evi-dent between cognitive function and later depressiongeneral cognitive function does not appear to be a riskfactor for depression but rather is more likely relatedto performance decrements associated with concurrentdepressive symptoms Our results suggest that low cog-nitive function is therefore probably not a causal factorof depression and that clinical practice may benefitmore from a focus on how decreased cognitive functionin the depressed state is likely to influence treatment out-comes (Gyurak et al 2015) Our findings have importantimplications for better understanding depression and forthe design of future studies in highlighting the need tocontrol for subthreshold depression symptoms when in-vestigating risk factors for mental illness as well as whenassessing cognitive function more generally
Supplementary material
The supplementary material for this article can befound at httpdxdoiorg101017S0033291716002075
Acknowledgements
MAS is supported by an National Science Foundation(NSF) Graduate Research Fellowship ARH is sup-ported by National Institutes of Health (NIH) grantsRO1DA033369 amp R01AG049789 TEM is supportedby National Institutes of Health (NIH) grantsR01AG049789 We would like to thank HarrisCooper PhD at Duke University who provided invalu-able insight into conducting the meta-analysis Wethank all of the authors of studies who provided add-itional information for this meta-analysis
Declaration of Interest
None
References
Aarts E van Holstein M Cools R (2011) Striatal dopamineand the interface between motivation and cognitionFrontiers in Psychology 2 163
14 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Atkinson KM Koenka AC Sanchez CE Moshontz HCooper H (2014) Reporting standards for literaturesearches and report inclusion criteria making researchsyntheses more transparent and easy to replicate ResearchSynthesis Methods 6 87ndash95
Baer LH Tabri N Blair M Bye D Li KZH Pushkar D(2013) Longitudinal associations of need for cognitioncognitive activity and depressive symptomatology withcognitive function in recent retirees Journals of GerontologySeries B Psychological Sciences and Social Sciences 68 655ndash664
Barbey AK Colom R Solomon J Krueger F Forbes CGrafman J (2012) An integrative architecture for generalintelligence and executive function revealed by lesionmapping Brain 135 1154ndash1164
Barnett JH Salmond CH Jones PB Sahakian BJ (2006)Cognitive reserve in neuropsychiatry Psychological Medicine36 1053ndash1064
Beaujean AA Parker S Qiu X (2013) The relationshipbetween cognitive ability and depression a longitudinaldata analysis Social Psychiatry and Psychiatric Epidemiology48 1983ndash1992
Belsky DW Caspi A Arseneault L Bleidorn W Fonagy PGoodman M Houts R Moffitt TE (2012) Etiologicalfeatures of borderline personality related characteristics in abirth cohort of 12-year-old children Development andPsychopathology 24 251ndash265
Betts KS Williams GM Najman JM Alati R (2016)Predicting spectrums of adult mania psychosis anddepression by prospectively ascertained childhoodneurodevelopment Journal of Psychiatric Research 72 22ndash29
Bora E Harrison BJ Yuumlcel M Pantelis C (2013) Cognitiveimpairment in euthymic major depressive disorder a meta-analysis Psychological Medicine 43 2017ndash2026
Borenstein M Hedges LV Higgins JPT Rothstein HR(2011) Introduction to Meta-Analysis John Wiley amp SonsWest Sussex UK
Canals J Domegravenech-Llaberia E Fernaacutendez-Ballart J Martiacute-Henneberg C (2002) Predictors of depression at eighteenA 7-year follow-up study in a Spanish nonclinicalpopulation European Child amp Adolescent Psychiatry 11226ndash233
Christensen H Griffiths K Mackinnon A (1997) Aquantitative review of cognitive deficits in depression andAlzheimer-type dementia Selection of Studies 3 631ndash651
Connolly SL Wagner Ca Shapero BG Pendergast LLAbramson LY Alloy LB (2014) Rumination prospectivelypredicts executive functioning impairments in adolescentsJournal of Behavior Therapy and Experimental Psychiatry 4546ndash56
Cooper HM (1979) Statistically combining independentstudies a meta-analysis of sex differences in conformityresearch Journal of Personality and Social Psychology 37131ndash146
Cooper HM (2010) Research Synthesis and Meta-Analysis AStep-by-Step Approach 4th edn SAGE PublicationsWashington (DC) USA
Cuijpers P de Graaf R van Dorsselaer S (2004) Minordepression risk profiles functional disability health careuse and risk of developing major depression Journal ofAffective Disorders 79 71ndash79
Cuthbert BN Kozak MJ (2013) Constructing constructs forpsychopathology the NIMH research domain criteriaJournal of Abnormal Psychology 122 928ndash937
Der G Batty GD Deary IJ (2009) The association between IQin adolescence and a range of health outcomes at 40 in the1979 US National Longitudinal Study of Youth Intelligence37 573ndash580
Dubow EF Boxer P Huesmann LR (2008) Childhood andadolescent predictors of early and middle adulthoodalcohol use and problem drinking the Columbia CountyLongitudinal Study Addiction 103 36ndash47
Duval S Tweedie R (2000) Trim and fill a simple funnel-plot-based method of testing and adjusting for publicationbias in meta-analysis Biometrics 56 455ndash463
Evans LD Kouros CD Samanez-Larkin S Garber J (2015)Concurrent and short-term prospective relations amongneurocognitive functioning coping and depressivesymptoms in youth Journal of Clinical Child and AdolescentPsychology 53 1ndash15
Franz CE Lyons MJ OrsquoBrien R Panizzon MS Kim K BhatR Grant MD Toomey R Eisen S Xian H Kremen WS(2011) A 35-year longitudinal assessment of cognition andmidlife depression symptoms the Vietnam Era Twin Studyof Aging American Association for Geriatric PsychiatryAmerican Journal of Geriatric Psychiatry 19 559ndash570
Gale CR Batty GD Tynelius P Deary IJ Rasmussen F(2010) Intelligence in early adulthood and subsequenthospitalization for mental disorders Epidemiology 2170ndash77
Gale CR Deary IJ Boyle SH Barefoot J Mortensen LHBatty GD (2008) Cognitive ability in early adulthood andrisk of 5 specific psychiatric disorders in middle age theVietnam experience study Archives of General Psychiatry 651410ndash1418
Gale CR Hatch SL Batty GD Deary IJ (2009) Intelligence inchildhood and risk of psychological distress in adulthoodthe 1958 National Child Development Survey and the 1970British Cohort Study Intelligence 37 592ndash599
Gjerde PF (1995) Alternative pathways to chronicdepressive symptoms in young adults gender differencesin developmental trajectories Child Development 661277ndash1300
Gottfredson LS (1997) Mainstream science on intelligence aneditorial with 52 signatories history and bibliographyIntelligence 24 13ndash23
Guyer AE Choate VR Grimm KJ Pine DS Keenan K(2011) Emerging depression is associated with facememory deficits in adolescent girls Elsevier Inc Journal ofthe American Academy of Child and Adolescent Psychiatry 50180ndash190
Gyurak A Patenaude B Korgaonkar MS Grieve SMWilliams LM Etkin A (2015) Frontoparietal activationduring response inhibition predicts remission toantidepressants in patients with major depression BiologicalPsychiatry 79 1ndash8
Hagenaars SP Harris SE Davies G Hill WD LiewaldDCM Ritchie SJ Marioni RE Fawns-Ritchie C Cullen BMalik R METASTROKE Consortium IC for BPGSpiroMeta Consortium CHARGE ConsortiumPulmonary Group CCA and LG Worrall BB Sudlow
Association between cognitive function and subsequent depression 15
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
CLM Wardlaw JM Gallacher J Pell J McIntosh AMSmith DJ Gale CR Deary IJ (2016) Shared geneticaetiology between cognitive functions and physical andmental health in UK Biobank (N = 112 151) and 24 GWASconsortiaMolecular Psychiatry Published online 26 January2016 doi101038mp2015225
Hatch SL Jones PB Kuh D Hardy R Wadsworth MEJRichards M (2007) Childhood cognitive ability and adultmental health in the British 1946 birth cohort Social Scienceamp Medicine (1982) 64 2285ndash2296
Hipwell AE Sapotichne B Klostermann S Battista DKeenan K (2011) Autobiographical memory as a predictorof depression vulnerability in girls Journal of Clinical Childand Adolescent Psychology 40 254ndash265
Horowitz JL Garber J (2003) Relation of intelligence andreligiosity to depressive disorders in offspring of depressedand nondepressed mothers The American Academy ofChild and Adolescent Psychiatry Journal of the AmericanAcademy of Child and Adolescent Psychiatry 42 578ndash586
Johnson W Bouchard TJ Krueger RF McGue MGottesman II (2004) Just one g consistent results fromthree test batteries Intelligence 32 95ndash107
Keedwell PA Andrew C Williams SCR Brammer MJPhillips ML (2005) The neural correlates of anhedoniain major depressive disorder Biological Psychiatry 58843ndash853
Kessler RC Berglund P Demler O Jin R Koretz DMerikangas KR Rush AJ Walters EE Wang PS (2003)The epidemiology of major depressive disorder resultsfrom the National Comorbidity Survey Replication(NCS-R) Journal of the American Medical Association 2893095ndash3105
Koenen KC Moffitt TE Roberts AL Martin LT KubzanskyL Harrington H Poulton R Caspi A (2009) Childhood IQand adult mental disorders a test of the cognitive reservehypothesis American Journal of Psychiatry 166 50ndash57
Lewinsohn PM Solomon A Seeley JR Zeiss A (2000)Clinical implications of lsquosubthresholdrsquo depressivesymptoms Journal of Abnormal Psychology 109 345ndash351
Luppino FS de Wit LM Bouvy PF Stijnen T Cuijpers PPenninx BWJH Zitman FG (2010) Overweight obesityand depression a systematic review and meta-analysisof longitudinal studies Archives of General Psychiatry 67220ndash229
McCord J Ensminger ME (1997) Multiple risks andcomorbidity in an African-American population CriminalBehaviour and Mental Health 7 339ndash352
McDermott LM Ebmeier KP (2009) A meta-analysis ofdepression severity and cognitive function Elsevier BVJournal of Affective Disorders 119 1ndash8
Melartin TK Rytsaumllauml HJ Leskelauml US Lestelauml-Mielonen PSSokero TP Isometsauml ET (2002) Current comorbidity ofpsychiatric disorders among DSM-IV major depressivedisorder patients in psychiatric care in the VantaaDepression Study Journal of Clinical Psychiatry 63 126ndash134
Meyer SE Carlson GA Wiggs EA Martinez PE RonsavilleDS KlimesndashDougan B Gold PW RadkendashYarrow M(2004) A prospective study of the association amongimpaired executive functioning childhood attentional
problems and the development of bipolar disorderDevelopment and Psychopathology 16 461ndash476
MiyakeA FriedmanNP EmersonMJWitzki aHHowerter AWager TD (2000) The unity and diversity of executivefunctions and their contributions to complex lsquoFrontal Lobersquotasks a latentvariable analysisCognitive Psychology41 49ndash100
Moher D Liberati A (2009) Preferred reporting items forsystematic reviews and meta-analyses the PRISMAstatement Annals of Internal Medicine 151 264ndash269
Papmeyer M Sussmann JE Hall J McKirdy J Peel AMacdonald A Lawrie SM Whalley HC McIntosh AM(2015) Neurocognition in individuals at high familial riskof mood disorders with or without subsequent onset ofdepression Psychological Medicine 45 1ndash11
Peterson RA Brown SP (2005) On the use of betacoefficients in meta-analysis Journal of Applied Psychology90 175ndash181
Pine DS Cohen P Brook J Coplan JD (1997) Psychiatricsymptoms in adolescence as predictors of obesity in earlyadulthood a longitudinal study American Journal of PublicHealth 87 1303ndash1310
Quinn ME Joormann J (2015) Control when it countschange in executive control under stress predicts depressionsymptoms Emotion Junio 22 1ndash10
Rawal A Rice F (2012) Examining overgeneralautobiographical memory as a risk factor for adolescentdepression Elsevier Inc Journal of the American Academy ofChild and Adolescent Psychiatry 51 518ndash527
Ree MJ Earles JA (1991) The stability of g across differentmethods of estimation Intelligence 15 271ndash278
Rock PL Roiser JP Riedel WJ Blackwell AD (2014)Cognitive impairment in depression a systematic reviewand meta-analysis Psychological Medicine 44 2029ndash2040
Rogers MA Kasai K Koji M Fukuda R Iwanami ANakagome K Fukuda M Kato N (2004) Executive andprefrontal dysfunction in unipolar depression a review ofneuropsychological and imaging evidence NeuroscienceResearch 50 1ndash11
Scult MA Knodt AR Swartz JR Brigidi BD Hariri AR(2016) Thinking and feeling individual differences inhabitual emotion regulation and stress-related mood areassociated with prefrontal executive control ClinicalPsychological Science doi1011772167702616654688
Sharp C Petersen N Goodyer I (2008) Emotional reactivityand the emergence of conduct problems and emotionalsymptoms in 7- to 11-year-olds a 1-year follow-up studyJournal of the American Academy of Child and AdolescentPsychiatry 47 565ndash573
Siegel LS (1999) Issues in the definition and diagnosis oflearning disabilities a perspective on Guckenberger vBoston University Journal of Learning Disabilities 32 304ndash319
Simons CJP Jacobs N Derom C Thiery E Jolles J van Os JKrabbendam L (2009) Cognition as predictor of currentand follow-up depressive symptoms in the generalpopulation Acta Psychiatrica Scandinavica 120 45ndash52
Slykerman RF Thompson J Waldie K Murphy R Wall CMitchell EA (2015) Maternal stress during pregnancy isassociated with moderate to severe depression in 11-year-old children Acta Paediatrica 104 68ndash74
16 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Snyder HR (2013) Major depressive disorder is associatedwith broad impairments on neuropsychological measuresof executive function a meta-analysis and reviewPsychological Bulletin 139 81ndash132
Soslashrensen HJ Saeligbye D Urfer-Parnas A Mortensen ELParnas J (2012) Premorbid intelligence and educationallevel in bipolar and unipolar disorders a Danish draftboard study Journal of Affective Disorders 136 1188ndash1191
SpearmanC (1904) lsquoGeneral intelligencersquoobjectivelydeterminedandmeasuredAmerican Journal of Psychology 15 201
Stern Y (2003) The concept of cognitive reserve a catalyst forresearch Journal of Clinical and Experimental Neuropsychology(Neuropsychology Development and Cognition Section A) 25589ndash593
Stroup D Berlin J Morton S Olkin I Williamson GDRennie D Moher D Becker BJ Sipe TA Thacker SB(2000) Meta-analysis of Observational Studies inEpidemiology a proposal for reporting Journal of theAmerican Medical Association 283 2008
Vinberg M Miskowiak KW Kessing LV (2013) Impairmentof executive function and attention predicts onset ofaffective disorder in healthy high-risk twins Journal ofClinical Psychiatry 74 e747ndashe753
Zammit S Allebeck P David AS Dalman C HemmingssonT Lundberg I Lewis G (2004) A longitudinal study ofpremorbid IQ Score and risk of developing schizophreniabipolar disorder severe depression and other nonaffectivepsychoses Archives of General Psychiatry 61 354ndash360
Association between cognitive function and subsequent depression 17
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms

meta-analysis (Peterson amp Brown 2005) the betaweights were used instead and analyses were runboth including and excluding these data points
When insufficient information was presented in thearticle authors were contacted requesting further de-tail An additional six studies were included at thispoint One study (Hatch et al 2007) included effectsizes for the female half of the cohort and did not pro-vide statistics for the males but did indicate a null ef-fect Only women from this study were included in themeta-analyses but imputing a score of 0 for the malesyielded similar overall results
Follow-up analyses directly compared studies thatreported zero-order correlations between IQ at time
1 depression at time 1 and depression at time 2(additional details described in the SupplementaryMethods)
Statistical methods
Data were analyzed using Comprehensive Meta-Analysis software version 30 (Biostat Inc USA) Arandom-effects model was used for expected hetero-geneity across studies A random-effects model alsoallows for broader generalization of results to thepopulation at large Heterogeneity of effects was calcu-lated using the Q statistic where a significant p valueindicates that true effect varies across studies The I2
Fig 1 Flow diagram of the search process
Association between cognitive function and subsequent depression 9
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
statistic was used to calculate the ratio of the true het-erogeneity to total variation acting as an index of sig-nal-to-noise ratio When I2 is large it is has beenrecommended to consider subgroup analysis or meta-regression to account for the variance (Borensteinet al 2011)
Subgroup analyses were conducted using a mixed-effects analysis in which a random effects model wasused to combine studies within each subgroup and afixed effect model was used to combine subgroupsand yield the overall effect (the study-to-study vari-ance is not assumed to be the same for all subgroups)Subgroup analyses were conducted comparing type ofoutcome (continuous v categorical) broad v specificcognitive measures and outcomes that were adjustedv unadjusted for baseline depression symptoms
Meta-regression was performed using the followingvariables on unadjusted analyses age at baseline ageat follow-up time between assessments IQ percentwhite year of cognitive assessment year of follow-upassessment percent female and study quality score
Study quality and publication bias
Study quality was evaluated independently by MSand AP using a checklist adapted from Luppino ampWit (Luppino et al 2010) The checklist contained 12items and studies were rated with a lsquo+rsquo if it met criteriafor that item a lsquominusrsquo if it did not meet criteria for an itemand a rsquorsquo if unclear lsquo+rsquo were coded as a score of 1 andminus were coded as a score of 0 Total scores and percen-tages were calculated Articles with total scores of 0ndash3were considered to be of low quality scores of 4ndash7were considered a medium quality and scores of 8ndash12 were considered to be of high quality Any discrep-ancies (approximately 3 of data points) wereresolved via consensus
Publication bias was assessed using a funnel plotwhich presents study size on the vertical axis (as stand-ard error in this case) as a function of effect size on thex-axis When no publication bias exists the studiesshould be distributed symmetrically about the com-bined effect size (Borenstein et al 2011) If evidenceof publication bias was observed Duval amp Tweediersquostrim-and-fill method was used (Duval amp Tweedie2000) which recalculates effects based on imputingdata from studies that are likely to be missing Lastthe Fail-safe N was calculated (Cooper 1979) whichindicates the number of missing studies that wouldneed to exist to nullify the observed effect
Results
A flow diagram of the search process is shown inFig 1 The search identified 2773 records through
PubMed 2158 through EMBASE and 1345 throughPsycINFO for a total of 6276 records Duplicaterecords (1709) were removed in EndNote resulting in4567 unique records After title and abstracts werereviewed 329 records were identified as potentially eli-gible for the meta-analysis These 329 records werereviewed in full and 300 articles were excluded hier-archically if they were a review baseline or protocolpaper (n = 6) if the sample had a mean age over 65at the depression assessment (n = 41) if the samplehad a specific medical illness (n = 23) if the studywas not a longitudinal design (n = 19) if MDD diagno-sis hospitalization or admission to treatment centerwas part of the inclusion criteria of the study (n = 18)if cognitive function was assessed only concurrentlywith or after depression (n = 36) if cognitive functionwas assessed by educational achievement or self-report(n = 26) if cognitive function was assessed by attribu-tion style rather than neuropsychological measure (n= 7) if there was no measure of cognitive function (n= 18) or no uniquely measured depression outcome(n = 24) Furthermore if articles reported on the samesample as another article with higher quality or moreinformation the duplicate articles were excluded (n =8) Last a number of studies appeared to measureboth cognitive function and depression but did not re-port enough information to be included in the meta-analysis and did not respond to requests for additionalinformation (n = 74 approximately 59 unique samples)In total 29 publication were included in the meta-ana-lysis comprising 34 samples (one study included twoseparate birth cohorts and another four reported dataseparately for men and women)
Study characteristics
The characteristics of included samples are detailed inTable 1 Sample sizes ranged from 43 to 50 053 with amedian of 3395 The most common types of sampleswere school samples (934) community samples (834) and birth cohorts (734) The samples were major-ity white with two samples having exclusively blackparticipants Additionally eight samples were menonly six samples were women only and the restreported combined effect sizes Mean age of partici-pants at baseline ranged from 35 to 59 years with amedian of 12 years Most samples did not reportwhether comorbid diagnoses were present (2334)
Of the 74 papers excluded for having insufficient in-formation (representing 60 unique samples) the me-dian number of subjects was not statistically differentbetween those studies and the studies included in themeta-analysis (n = 288 and n = 3395 respectively p =019) nor did the average age of study participants atbaseline statistically differ (median across studies = 11
10 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
v 12 respectively p = 057) The types of cognitivemeasures used were also similar across the excludedand included studies with the most common measurebeing IQ (2860 and 2029) followed by VerbalComprehension (860 and 529)
Meta-analysis
The overall analysis yielded a significant associationbetween cognitive function and subsequent depressionoutcomes [r =minus0088 95 confidence interval (CI)minus0121 to minus0054 p lt 0001 Fig 2] Results were similarwhen excluding the two studies that used beta-weights(r =minus0071 95 CI minus0100 to minus0042 p lt 0001) orwhen using episodic memory in place of processingspeed in a study reporting both outcomes (r =minus008595 CI minus0118 to minus0051 p lt 0001) Follow-up ana-lyses were conducted in the sample of studies report-ing educational attainment and self-report outcomes(Supplementary Table S2) Heterogeneity across sam-ples was significant (Q = 80154 p lt 0001) suggestingsubstantial variation across the individual samplesThe ratio of the true heterogeneity to total variationwas large (I2 = 9588) I2 is on a relative scale andvalues close to 100 indicate that most of the observedvariance is real rather than spurious and suggeststhat subgroup analyses or meta-regression may helpto explain this variability (Borenstein et al 2011)
Subgroup analyses and meta-regression
A significant difference was found between categoricaland continuous effect sizes (p lt 0001) The studiesassessing continuous outcomes were found to have alarger effect (r =minus0121 95 CI minus0168 to minus0073 p lt0001 n = 22) than studies assessing categorical out-comes (r =minus0035 95 CI minus0054 to minus0017 p lt 0001n = 12) No differences were observed between studiesutilizing broad v specific cognitive measures (p = 057)
Outcomes were also compared adjusting for baselinedepression symptoms at the time of cognitive assess-ment Nine studies provided enough detail to calculatethe partial correlation coefficients adjusting for base-line depression symptoms Using the partial correl-ation coefficients led to a null result (r =minus0032 95CI minus0078 to 0014 p = 0169 n = 9 Fig 3) The nullresult does not seem to be due to a lack of power be-cause using the unadjusted correlation coefficients forthe same nine studies still led to a significant result(r =minus0120 95 CI minus0169 to minus0070 p lt 0001 n = 9Fig 3) As a follow-up the difference in effect sizes be-tween the adjusted and unadjusted values for these 9studies were tested (r = 0082 95 CI 0069ndash0095 p lt0001 n = 9) suggesting that the effects are significantlydifferent when directly comparing the values that doand do not control for baseline depression symptoms
Expanding the subgroup analyses to include studiesthat controlled for baseline depression plus other co-variates (Zammit et al 2004 Simons et al 2009 Rawalamp Rice 2012) and studies that explicitly excluded fora history of depression diagnosis (Gale et al 2008Vinberg et al 2013 Papmeyer et al 2015) did notchange the null result (r =minus0027 95 CI minus0058 to0005 p = 0097 n = 15)
None of the meta-regression analyses were signifi-cant indicating that the between-study variance wasnot attributable to age at baseline IQ percent of sam-ple that was female percent of the sample that waswhite age at follow-up time between assessmentsyear of cognitive assessment year of follow-up assess-ment or study quality score
Study quality and publication bias
Multiple samples within a study were combined forthe purposes of quality assessment given that studieswithin the same publication were found to employthe same methodology Of the 29 publications reviewed12 were rated as high quality and 17 were rated as me-dium quality Details are provided in SupplementaryTable S1 Comparable results to the overall findingswere obtained when just using high quality studies (r=minus0085 95 CI minus0141 to minus0029 p = 0003)
Inspection of the funnel plot (Fig 4) found no evi-dence for publication bias to support the hypothesisIn fact imputation of negative correlations suggestedthat additional studies favoring the hypothesis maybe missing While the calculated effect size is minus0088(95 CI minus0121 to minus0054) using Duval amp Tweediersquostrim-and-fill method the imputed effect size estimateis larger at minus0137 (95 CI minus0176 to minus0099 imputedstudies n = 11) Last the Fail-safe N procedure foundthat 3583 null studies would need to be located forthe combined two-tailed p value to exceed 005 Thissuggests that significant results are not likely to be con-founded by publication bias and may even underesti-mate true effect sizes
Discussion
The present systematic review and meta-analysis of 29longitudinal publications including 1 21 749 partici-pants revealed that after accounting for baseline depres-sion symptoms variability in cognitive function did notpredict subsequent depression Consistent with priorreports there was a significant contemporaneous associ-ation between higher depression symptoms and lowercognitive function These patterns have implications forunderstanding the association between cognitive func-tion and depression and may be important for advan-cing etiologic and treatment research
Association between cognitive function and subsequent depression 11
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
First our findings reinforce models positing thatcognitive function tracks with depression severity(McDermott amp Ebmeier 2009) One possible explan-ation for this contemporaneous association is that de-pression symptoms interfere with the capacity tocomplete cognitive assessments possibly through thegeneral lack of motivation that is one hallmark of thedisorder While this explanation represents an experi-mental confound for studies focused on assessmentof cognitive function it likewise represents an oppor-tunity for studies to focus more comprehensively onthe assessment of both depression and mood disordersymptoms since performance on cognitive tests maybe a sensitive measure of motivational state thatcould augment self-reported symptoms Alternativelythe co-occurrence of cognitive deficits and depressionsymptoms may reflect shared genetic etiology (Hagen-aars et al 2016) and dysfunction of neural circuits
supporting both cognitive and emotional processes(Scult et al 2016) In particular dysfunction of prefront-al and striatal circuits have been associated with bothdepression and cognitive function (Keedwell et al2005 Aarts et al 2011)
Second our findings suggest that prior studies oflinks between cognitive function and depression thatdid not assess baseline symptoms may have overesti-mated the potential protective role of higher cognitivefunction While the importance of accounting for sub-clinical symptoms is not novel the implementation ofsuch accounting is often neglected in psychiatric epi-demiology given the current categorical threshold-based diagnostic system In our meta-analysis largereffects were observed for continuous as compared tocategorical outcomes which aligns with growing em-phasis on dimensional measures of psychopathology(Cuthbert amp Kozak 2013)
Fig 2 Meta-analysis of the association between cognitive function and subsequent depression A forest plot for all studiesthat investigated associations between cognition and later depression Results are reported as correlation coefficients denotedby squares and 95 confidence intervals (CI) indicated by lines (effect sizes are converted to correlation coefficients ifreported as odds ratios) Meta-analysis results are displayed as the diamond The overall analysis found a significant effect ofcognition on depression (r =minus0088 95 CI minus0121 to minus0054 p lt 0001)
12 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Fig 4 Trim-and-fill funnel plots for all samples Fisherrsquos Z a measure of effect size is plotted on the x-axis and the standarderror is plotted on the y-axis Larger studies appear toward the top of the graph and smaller studies towards the bottom Inthe absence of publication bias the studies are symmetrically distributed around the mean Actual studies are shown in opencircles and imputed studies would be shown in black circles No additional studies would be expected in the oppositedirection (to the right) of the observed effect but an additional 11 studies are imputed to the left of the mean effect sizeWhile the calculated effect size is minus0088 [95 confidence interval (CI) minus0121 to minus0054] using Duval amp Tweediersquos trim-and-fill method the imputed effect size estimate is larger at minus0137 (95 CI minus0176 to minus0099 imputed studies n = 11)
Fig 3 Meta-analysis comparing values adjusted for baseline depression symptoms v unadjusted A forest plot for analysiscomparing results from a subset of the same set of studies reported in Fig 2 when using unadjusted values compared tousing values that are adjusted for baseline depression Effects are significant for unadjusted values [r =minus0120 95 confidenceinterval (CI) minus0169 to minus0070 p lt 0001] but not for adjusted values (r =minus0032 95 CI minus0078 to 0014 p = 0169) Results arereported as correlation coefficients denoted by squares and 95 CIs indicated by lines Meta-analysis results are displayed asdiamonds
Association between cognitive function and subsequent depression 13
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Third the associations between cognitive functionand either current or later depression were not moder-ated by data quality or participant age sex and raceHowever there are a number of additional potentialmoderators that could not be addressed in the currentreview and meta-analysis For example the numberand type of comorbid conditions with depressionwere often not reported in the included studies butcould represent an important moderator of theobserved effects Modeling the effects of comorbid ill-ness is an important avenue for future research
One limitation of the current literature is that only ahandful of studies reviewed explicitly excluded for de-pression diagnosis at baseline (Gale et al 2008 Vinberget al 2013 Papmeyer et al 2015) however consistentwith the finding that controlling for baseline depres-sion symptoms led to a null association between cogni-tion and subsequent depression there was no effectobserved when including these studies in the sub-group analyses further suggesting that the associationbetween cognitive function and depression is likelycontemporaneous It will be important to follow-upthese analyses with individual studies that includerigorous assessment of baseline depression symptomsand other potentially confounding factors to furtherclarify this relationship
An open question that remains for future research iswhether deficits in cognitive function are likely to pre-dict the development of more sever or recurrent de-pression later in life Only one of the included studies(Koenen et al 2009) specifically investigated recurrentdepression and found that lower IQ was associatedwith greater persistence of disorder
A final consideration is that while our review andmeta-analysis focused on general cognitive functionmainly assessed via IQ there may be specific subtypesof cognitive function that are more predictive of laterdepression For example a lack of cognitive flexibilitymay more closely match with the ruminative stylecharacteristic of depression and therefore tasks specifi-cally measuring this component of cognitive functionmight have some predictive utility While our reviewdid not find differences between broad and specificmeasures of cognitive function there were not enoughstudies identified to allow for precise consideration ofdifferences between individual cognitive domains
A limitation of the meta-analysis is that while thepresent study followed standard guidelines (Stroupet al 2000 Atkinson et al 2014) decisions aboutstudy selection data extraction and quality assess-ment include a number of decision points that neces-sarily involve a level of subjectivity Reliability wasascertained by using independent raters however dif-ferent inclusionexclusion criteria or a different ap-proach to the evaluation of those criteria could result
in a different set of studies being includedUltimately the quality of the meta-analysis is depend-ent upon the underlying studies that are analyzedFurthermore although studies with insufficient infor-mation to be included in the meta-analysis were notfound to differ based on basic study data from thosestudies included in the meta-analysis nonetheless itis unknown how if at all data from these studiescould change the overall results
Acknowledging these limitations our present reviewand meta-analysis found that while an association is evi-dent between cognitive function and later depressiongeneral cognitive function does not appear to be a riskfactor for depression but rather is more likely relatedto performance decrements associated with concurrentdepressive symptoms Our results suggest that low cog-nitive function is therefore probably not a causal factorof depression and that clinical practice may benefitmore from a focus on how decreased cognitive functionin the depressed state is likely to influence treatment out-comes (Gyurak et al 2015) Our findings have importantimplications for better understanding depression and forthe design of future studies in highlighting the need tocontrol for subthreshold depression symptoms when in-vestigating risk factors for mental illness as well as whenassessing cognitive function more generally
Supplementary material
The supplementary material for this article can befound at httpdxdoiorg101017S0033291716002075
Acknowledgements
MAS is supported by an National Science Foundation(NSF) Graduate Research Fellowship ARH is sup-ported by National Institutes of Health (NIH) grantsRO1DA033369 amp R01AG049789 TEM is supportedby National Institutes of Health (NIH) grantsR01AG049789 We would like to thank HarrisCooper PhD at Duke University who provided invalu-able insight into conducting the meta-analysis Wethank all of the authors of studies who provided add-itional information for this meta-analysis
Declaration of Interest
None
References
Aarts E van Holstein M Cools R (2011) Striatal dopamineand the interface between motivation and cognitionFrontiers in Psychology 2 163
14 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Atkinson KM Koenka AC Sanchez CE Moshontz HCooper H (2014) Reporting standards for literaturesearches and report inclusion criteria making researchsyntheses more transparent and easy to replicate ResearchSynthesis Methods 6 87ndash95
Baer LH Tabri N Blair M Bye D Li KZH Pushkar D(2013) Longitudinal associations of need for cognitioncognitive activity and depressive symptomatology withcognitive function in recent retirees Journals of GerontologySeries B Psychological Sciences and Social Sciences 68 655ndash664
Barbey AK Colom R Solomon J Krueger F Forbes CGrafman J (2012) An integrative architecture for generalintelligence and executive function revealed by lesionmapping Brain 135 1154ndash1164
Barnett JH Salmond CH Jones PB Sahakian BJ (2006)Cognitive reserve in neuropsychiatry Psychological Medicine36 1053ndash1064
Beaujean AA Parker S Qiu X (2013) The relationshipbetween cognitive ability and depression a longitudinaldata analysis Social Psychiatry and Psychiatric Epidemiology48 1983ndash1992
Belsky DW Caspi A Arseneault L Bleidorn W Fonagy PGoodman M Houts R Moffitt TE (2012) Etiologicalfeatures of borderline personality related characteristics in abirth cohort of 12-year-old children Development andPsychopathology 24 251ndash265
Betts KS Williams GM Najman JM Alati R (2016)Predicting spectrums of adult mania psychosis anddepression by prospectively ascertained childhoodneurodevelopment Journal of Psychiatric Research 72 22ndash29
Bora E Harrison BJ Yuumlcel M Pantelis C (2013) Cognitiveimpairment in euthymic major depressive disorder a meta-analysis Psychological Medicine 43 2017ndash2026
Borenstein M Hedges LV Higgins JPT Rothstein HR(2011) Introduction to Meta-Analysis John Wiley amp SonsWest Sussex UK
Canals J Domegravenech-Llaberia E Fernaacutendez-Ballart J Martiacute-Henneberg C (2002) Predictors of depression at eighteenA 7-year follow-up study in a Spanish nonclinicalpopulation European Child amp Adolescent Psychiatry 11226ndash233
Christensen H Griffiths K Mackinnon A (1997) Aquantitative review of cognitive deficits in depression andAlzheimer-type dementia Selection of Studies 3 631ndash651
Connolly SL Wagner Ca Shapero BG Pendergast LLAbramson LY Alloy LB (2014) Rumination prospectivelypredicts executive functioning impairments in adolescentsJournal of Behavior Therapy and Experimental Psychiatry 4546ndash56
Cooper HM (1979) Statistically combining independentstudies a meta-analysis of sex differences in conformityresearch Journal of Personality and Social Psychology 37131ndash146
Cooper HM (2010) Research Synthesis and Meta-Analysis AStep-by-Step Approach 4th edn SAGE PublicationsWashington (DC) USA
Cuijpers P de Graaf R van Dorsselaer S (2004) Minordepression risk profiles functional disability health careuse and risk of developing major depression Journal ofAffective Disorders 79 71ndash79
Cuthbert BN Kozak MJ (2013) Constructing constructs forpsychopathology the NIMH research domain criteriaJournal of Abnormal Psychology 122 928ndash937
Der G Batty GD Deary IJ (2009) The association between IQin adolescence and a range of health outcomes at 40 in the1979 US National Longitudinal Study of Youth Intelligence37 573ndash580
Dubow EF Boxer P Huesmann LR (2008) Childhood andadolescent predictors of early and middle adulthoodalcohol use and problem drinking the Columbia CountyLongitudinal Study Addiction 103 36ndash47
Duval S Tweedie R (2000) Trim and fill a simple funnel-plot-based method of testing and adjusting for publicationbias in meta-analysis Biometrics 56 455ndash463
Evans LD Kouros CD Samanez-Larkin S Garber J (2015)Concurrent and short-term prospective relations amongneurocognitive functioning coping and depressivesymptoms in youth Journal of Clinical Child and AdolescentPsychology 53 1ndash15
Franz CE Lyons MJ OrsquoBrien R Panizzon MS Kim K BhatR Grant MD Toomey R Eisen S Xian H Kremen WS(2011) A 35-year longitudinal assessment of cognition andmidlife depression symptoms the Vietnam Era Twin Studyof Aging American Association for Geriatric PsychiatryAmerican Journal of Geriatric Psychiatry 19 559ndash570
Gale CR Batty GD Tynelius P Deary IJ Rasmussen F(2010) Intelligence in early adulthood and subsequenthospitalization for mental disorders Epidemiology 2170ndash77
Gale CR Deary IJ Boyle SH Barefoot J Mortensen LHBatty GD (2008) Cognitive ability in early adulthood andrisk of 5 specific psychiatric disorders in middle age theVietnam experience study Archives of General Psychiatry 651410ndash1418
Gale CR Hatch SL Batty GD Deary IJ (2009) Intelligence inchildhood and risk of psychological distress in adulthoodthe 1958 National Child Development Survey and the 1970British Cohort Study Intelligence 37 592ndash599
Gjerde PF (1995) Alternative pathways to chronicdepressive symptoms in young adults gender differencesin developmental trajectories Child Development 661277ndash1300
Gottfredson LS (1997) Mainstream science on intelligence aneditorial with 52 signatories history and bibliographyIntelligence 24 13ndash23
Guyer AE Choate VR Grimm KJ Pine DS Keenan K(2011) Emerging depression is associated with facememory deficits in adolescent girls Elsevier Inc Journal ofthe American Academy of Child and Adolescent Psychiatry 50180ndash190
Gyurak A Patenaude B Korgaonkar MS Grieve SMWilliams LM Etkin A (2015) Frontoparietal activationduring response inhibition predicts remission toantidepressants in patients with major depression BiologicalPsychiatry 79 1ndash8
Hagenaars SP Harris SE Davies G Hill WD LiewaldDCM Ritchie SJ Marioni RE Fawns-Ritchie C Cullen BMalik R METASTROKE Consortium IC for BPGSpiroMeta Consortium CHARGE ConsortiumPulmonary Group CCA and LG Worrall BB Sudlow
Association between cognitive function and subsequent depression 15
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
CLM Wardlaw JM Gallacher J Pell J McIntosh AMSmith DJ Gale CR Deary IJ (2016) Shared geneticaetiology between cognitive functions and physical andmental health in UK Biobank (N = 112 151) and 24 GWASconsortiaMolecular Psychiatry Published online 26 January2016 doi101038mp2015225
Hatch SL Jones PB Kuh D Hardy R Wadsworth MEJRichards M (2007) Childhood cognitive ability and adultmental health in the British 1946 birth cohort Social Scienceamp Medicine (1982) 64 2285ndash2296
Hipwell AE Sapotichne B Klostermann S Battista DKeenan K (2011) Autobiographical memory as a predictorof depression vulnerability in girls Journal of Clinical Childand Adolescent Psychology 40 254ndash265
Horowitz JL Garber J (2003) Relation of intelligence andreligiosity to depressive disorders in offspring of depressedand nondepressed mothers The American Academy ofChild and Adolescent Psychiatry Journal of the AmericanAcademy of Child and Adolescent Psychiatry 42 578ndash586
Johnson W Bouchard TJ Krueger RF McGue MGottesman II (2004) Just one g consistent results fromthree test batteries Intelligence 32 95ndash107
Keedwell PA Andrew C Williams SCR Brammer MJPhillips ML (2005) The neural correlates of anhedoniain major depressive disorder Biological Psychiatry 58843ndash853
Kessler RC Berglund P Demler O Jin R Koretz DMerikangas KR Rush AJ Walters EE Wang PS (2003)The epidemiology of major depressive disorder resultsfrom the National Comorbidity Survey Replication(NCS-R) Journal of the American Medical Association 2893095ndash3105
Koenen KC Moffitt TE Roberts AL Martin LT KubzanskyL Harrington H Poulton R Caspi A (2009) Childhood IQand adult mental disorders a test of the cognitive reservehypothesis American Journal of Psychiatry 166 50ndash57
Lewinsohn PM Solomon A Seeley JR Zeiss A (2000)Clinical implications of lsquosubthresholdrsquo depressivesymptoms Journal of Abnormal Psychology 109 345ndash351
Luppino FS de Wit LM Bouvy PF Stijnen T Cuijpers PPenninx BWJH Zitman FG (2010) Overweight obesityand depression a systematic review and meta-analysisof longitudinal studies Archives of General Psychiatry 67220ndash229
McCord J Ensminger ME (1997) Multiple risks andcomorbidity in an African-American population CriminalBehaviour and Mental Health 7 339ndash352
McDermott LM Ebmeier KP (2009) A meta-analysis ofdepression severity and cognitive function Elsevier BVJournal of Affective Disorders 119 1ndash8
Melartin TK Rytsaumllauml HJ Leskelauml US Lestelauml-Mielonen PSSokero TP Isometsauml ET (2002) Current comorbidity ofpsychiatric disorders among DSM-IV major depressivedisorder patients in psychiatric care in the VantaaDepression Study Journal of Clinical Psychiatry 63 126ndash134
Meyer SE Carlson GA Wiggs EA Martinez PE RonsavilleDS KlimesndashDougan B Gold PW RadkendashYarrow M(2004) A prospective study of the association amongimpaired executive functioning childhood attentional
problems and the development of bipolar disorderDevelopment and Psychopathology 16 461ndash476
MiyakeA FriedmanNP EmersonMJWitzki aHHowerter AWager TD (2000) The unity and diversity of executivefunctions and their contributions to complex lsquoFrontal Lobersquotasks a latentvariable analysisCognitive Psychology41 49ndash100
Moher D Liberati A (2009) Preferred reporting items forsystematic reviews and meta-analyses the PRISMAstatement Annals of Internal Medicine 151 264ndash269
Papmeyer M Sussmann JE Hall J McKirdy J Peel AMacdonald A Lawrie SM Whalley HC McIntosh AM(2015) Neurocognition in individuals at high familial riskof mood disorders with or without subsequent onset ofdepression Psychological Medicine 45 1ndash11
Peterson RA Brown SP (2005) On the use of betacoefficients in meta-analysis Journal of Applied Psychology90 175ndash181
Pine DS Cohen P Brook J Coplan JD (1997) Psychiatricsymptoms in adolescence as predictors of obesity in earlyadulthood a longitudinal study American Journal of PublicHealth 87 1303ndash1310
Quinn ME Joormann J (2015) Control when it countschange in executive control under stress predicts depressionsymptoms Emotion Junio 22 1ndash10
Rawal A Rice F (2012) Examining overgeneralautobiographical memory as a risk factor for adolescentdepression Elsevier Inc Journal of the American Academy ofChild and Adolescent Psychiatry 51 518ndash527
Ree MJ Earles JA (1991) The stability of g across differentmethods of estimation Intelligence 15 271ndash278
Rock PL Roiser JP Riedel WJ Blackwell AD (2014)Cognitive impairment in depression a systematic reviewand meta-analysis Psychological Medicine 44 2029ndash2040
Rogers MA Kasai K Koji M Fukuda R Iwanami ANakagome K Fukuda M Kato N (2004) Executive andprefrontal dysfunction in unipolar depression a review ofneuropsychological and imaging evidence NeuroscienceResearch 50 1ndash11
Scult MA Knodt AR Swartz JR Brigidi BD Hariri AR(2016) Thinking and feeling individual differences inhabitual emotion regulation and stress-related mood areassociated with prefrontal executive control ClinicalPsychological Science doi1011772167702616654688
Sharp C Petersen N Goodyer I (2008) Emotional reactivityand the emergence of conduct problems and emotionalsymptoms in 7- to 11-year-olds a 1-year follow-up studyJournal of the American Academy of Child and AdolescentPsychiatry 47 565ndash573
Siegel LS (1999) Issues in the definition and diagnosis oflearning disabilities a perspective on Guckenberger vBoston University Journal of Learning Disabilities 32 304ndash319
Simons CJP Jacobs N Derom C Thiery E Jolles J van Os JKrabbendam L (2009) Cognition as predictor of currentand follow-up depressive symptoms in the generalpopulation Acta Psychiatrica Scandinavica 120 45ndash52
Slykerman RF Thompson J Waldie K Murphy R Wall CMitchell EA (2015) Maternal stress during pregnancy isassociated with moderate to severe depression in 11-year-old children Acta Paediatrica 104 68ndash74
16 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Snyder HR (2013) Major depressive disorder is associatedwith broad impairments on neuropsychological measuresof executive function a meta-analysis and reviewPsychological Bulletin 139 81ndash132
Soslashrensen HJ Saeligbye D Urfer-Parnas A Mortensen ELParnas J (2012) Premorbid intelligence and educationallevel in bipolar and unipolar disorders a Danish draftboard study Journal of Affective Disorders 136 1188ndash1191
SpearmanC (1904) lsquoGeneral intelligencersquoobjectivelydeterminedandmeasuredAmerican Journal of Psychology 15 201
Stern Y (2003) The concept of cognitive reserve a catalyst forresearch Journal of Clinical and Experimental Neuropsychology(Neuropsychology Development and Cognition Section A) 25589ndash593
Stroup D Berlin J Morton S Olkin I Williamson GDRennie D Moher D Becker BJ Sipe TA Thacker SB(2000) Meta-analysis of Observational Studies inEpidemiology a proposal for reporting Journal of theAmerican Medical Association 283 2008
Vinberg M Miskowiak KW Kessing LV (2013) Impairmentof executive function and attention predicts onset ofaffective disorder in healthy high-risk twins Journal ofClinical Psychiatry 74 e747ndashe753
Zammit S Allebeck P David AS Dalman C HemmingssonT Lundberg I Lewis G (2004) A longitudinal study ofpremorbid IQ Score and risk of developing schizophreniabipolar disorder severe depression and other nonaffectivepsychoses Archives of General Psychiatry 61 354ndash360
Association between cognitive function and subsequent depression 17
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms

statistic was used to calculate the ratio of the true het-erogeneity to total variation acting as an index of sig-nal-to-noise ratio When I2 is large it is has beenrecommended to consider subgroup analysis or meta-regression to account for the variance (Borensteinet al 2011)
Subgroup analyses were conducted using a mixed-effects analysis in which a random effects model wasused to combine studies within each subgroup and afixed effect model was used to combine subgroupsand yield the overall effect (the study-to-study vari-ance is not assumed to be the same for all subgroups)Subgroup analyses were conducted comparing type ofoutcome (continuous v categorical) broad v specificcognitive measures and outcomes that were adjustedv unadjusted for baseline depression symptoms
Meta-regression was performed using the followingvariables on unadjusted analyses age at baseline ageat follow-up time between assessments IQ percentwhite year of cognitive assessment year of follow-upassessment percent female and study quality score
Study quality and publication bias
Study quality was evaluated independently by MSand AP using a checklist adapted from Luppino ampWit (Luppino et al 2010) The checklist contained 12items and studies were rated with a lsquo+rsquo if it met criteriafor that item a lsquominusrsquo if it did not meet criteria for an itemand a rsquorsquo if unclear lsquo+rsquo were coded as a score of 1 andminus were coded as a score of 0 Total scores and percen-tages were calculated Articles with total scores of 0ndash3were considered to be of low quality scores of 4ndash7were considered a medium quality and scores of 8ndash12 were considered to be of high quality Any discrep-ancies (approximately 3 of data points) wereresolved via consensus
Publication bias was assessed using a funnel plotwhich presents study size on the vertical axis (as stand-ard error in this case) as a function of effect size on thex-axis When no publication bias exists the studiesshould be distributed symmetrically about the com-bined effect size (Borenstein et al 2011) If evidenceof publication bias was observed Duval amp Tweediersquostrim-and-fill method was used (Duval amp Tweedie2000) which recalculates effects based on imputingdata from studies that are likely to be missing Lastthe Fail-safe N was calculated (Cooper 1979) whichindicates the number of missing studies that wouldneed to exist to nullify the observed effect
Results
A flow diagram of the search process is shown inFig 1 The search identified 2773 records through
PubMed 2158 through EMBASE and 1345 throughPsycINFO for a total of 6276 records Duplicaterecords (1709) were removed in EndNote resulting in4567 unique records After title and abstracts werereviewed 329 records were identified as potentially eli-gible for the meta-analysis These 329 records werereviewed in full and 300 articles were excluded hier-archically if they were a review baseline or protocolpaper (n = 6) if the sample had a mean age over 65at the depression assessment (n = 41) if the samplehad a specific medical illness (n = 23) if the studywas not a longitudinal design (n = 19) if MDD diagno-sis hospitalization or admission to treatment centerwas part of the inclusion criteria of the study (n = 18)if cognitive function was assessed only concurrentlywith or after depression (n = 36) if cognitive functionwas assessed by educational achievement or self-report(n = 26) if cognitive function was assessed by attribu-tion style rather than neuropsychological measure (n= 7) if there was no measure of cognitive function (n= 18) or no uniquely measured depression outcome(n = 24) Furthermore if articles reported on the samesample as another article with higher quality or moreinformation the duplicate articles were excluded (n =8) Last a number of studies appeared to measureboth cognitive function and depression but did not re-port enough information to be included in the meta-analysis and did not respond to requests for additionalinformation (n = 74 approximately 59 unique samples)In total 29 publication were included in the meta-ana-lysis comprising 34 samples (one study included twoseparate birth cohorts and another four reported dataseparately for men and women)
Study characteristics
The characteristics of included samples are detailed inTable 1 Sample sizes ranged from 43 to 50 053 with amedian of 3395 The most common types of sampleswere school samples (934) community samples (834) and birth cohorts (734) The samples were major-ity white with two samples having exclusively blackparticipants Additionally eight samples were menonly six samples were women only and the restreported combined effect sizes Mean age of partici-pants at baseline ranged from 35 to 59 years with amedian of 12 years Most samples did not reportwhether comorbid diagnoses were present (2334)
Of the 74 papers excluded for having insufficient in-formation (representing 60 unique samples) the me-dian number of subjects was not statistically differentbetween those studies and the studies included in themeta-analysis (n = 288 and n = 3395 respectively p =019) nor did the average age of study participants atbaseline statistically differ (median across studies = 11
10 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
v 12 respectively p = 057) The types of cognitivemeasures used were also similar across the excludedand included studies with the most common measurebeing IQ (2860 and 2029) followed by VerbalComprehension (860 and 529)
Meta-analysis
The overall analysis yielded a significant associationbetween cognitive function and subsequent depressionoutcomes [r =minus0088 95 confidence interval (CI)minus0121 to minus0054 p lt 0001 Fig 2] Results were similarwhen excluding the two studies that used beta-weights(r =minus0071 95 CI minus0100 to minus0042 p lt 0001) orwhen using episodic memory in place of processingspeed in a study reporting both outcomes (r =minus008595 CI minus0118 to minus0051 p lt 0001) Follow-up ana-lyses were conducted in the sample of studies report-ing educational attainment and self-report outcomes(Supplementary Table S2) Heterogeneity across sam-ples was significant (Q = 80154 p lt 0001) suggestingsubstantial variation across the individual samplesThe ratio of the true heterogeneity to total variationwas large (I2 = 9588) I2 is on a relative scale andvalues close to 100 indicate that most of the observedvariance is real rather than spurious and suggeststhat subgroup analyses or meta-regression may helpto explain this variability (Borenstein et al 2011)
Subgroup analyses and meta-regression
A significant difference was found between categoricaland continuous effect sizes (p lt 0001) The studiesassessing continuous outcomes were found to have alarger effect (r =minus0121 95 CI minus0168 to minus0073 p lt0001 n = 22) than studies assessing categorical out-comes (r =minus0035 95 CI minus0054 to minus0017 p lt 0001n = 12) No differences were observed between studiesutilizing broad v specific cognitive measures (p = 057)
Outcomes were also compared adjusting for baselinedepression symptoms at the time of cognitive assess-ment Nine studies provided enough detail to calculatethe partial correlation coefficients adjusting for base-line depression symptoms Using the partial correl-ation coefficients led to a null result (r =minus0032 95CI minus0078 to 0014 p = 0169 n = 9 Fig 3) The nullresult does not seem to be due to a lack of power be-cause using the unadjusted correlation coefficients forthe same nine studies still led to a significant result(r =minus0120 95 CI minus0169 to minus0070 p lt 0001 n = 9Fig 3) As a follow-up the difference in effect sizes be-tween the adjusted and unadjusted values for these 9studies were tested (r = 0082 95 CI 0069ndash0095 p lt0001 n = 9) suggesting that the effects are significantlydifferent when directly comparing the values that doand do not control for baseline depression symptoms
Expanding the subgroup analyses to include studiesthat controlled for baseline depression plus other co-variates (Zammit et al 2004 Simons et al 2009 Rawalamp Rice 2012) and studies that explicitly excluded fora history of depression diagnosis (Gale et al 2008Vinberg et al 2013 Papmeyer et al 2015) did notchange the null result (r =minus0027 95 CI minus0058 to0005 p = 0097 n = 15)
None of the meta-regression analyses were signifi-cant indicating that the between-study variance wasnot attributable to age at baseline IQ percent of sam-ple that was female percent of the sample that waswhite age at follow-up time between assessmentsyear of cognitive assessment year of follow-up assess-ment or study quality score
Study quality and publication bias
Multiple samples within a study were combined forthe purposes of quality assessment given that studieswithin the same publication were found to employthe same methodology Of the 29 publications reviewed12 were rated as high quality and 17 were rated as me-dium quality Details are provided in SupplementaryTable S1 Comparable results to the overall findingswere obtained when just using high quality studies (r=minus0085 95 CI minus0141 to minus0029 p = 0003)
Inspection of the funnel plot (Fig 4) found no evi-dence for publication bias to support the hypothesisIn fact imputation of negative correlations suggestedthat additional studies favoring the hypothesis maybe missing While the calculated effect size is minus0088(95 CI minus0121 to minus0054) using Duval amp Tweediersquostrim-and-fill method the imputed effect size estimateis larger at minus0137 (95 CI minus0176 to minus0099 imputedstudies n = 11) Last the Fail-safe N procedure foundthat 3583 null studies would need to be located forthe combined two-tailed p value to exceed 005 Thissuggests that significant results are not likely to be con-founded by publication bias and may even underesti-mate true effect sizes
Discussion
The present systematic review and meta-analysis of 29longitudinal publications including 1 21 749 partici-pants revealed that after accounting for baseline depres-sion symptoms variability in cognitive function did notpredict subsequent depression Consistent with priorreports there was a significant contemporaneous associ-ation between higher depression symptoms and lowercognitive function These patterns have implications forunderstanding the association between cognitive func-tion and depression and may be important for advan-cing etiologic and treatment research
Association between cognitive function and subsequent depression 11
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
First our findings reinforce models positing thatcognitive function tracks with depression severity(McDermott amp Ebmeier 2009) One possible explan-ation for this contemporaneous association is that de-pression symptoms interfere with the capacity tocomplete cognitive assessments possibly through thegeneral lack of motivation that is one hallmark of thedisorder While this explanation represents an experi-mental confound for studies focused on assessmentof cognitive function it likewise represents an oppor-tunity for studies to focus more comprehensively onthe assessment of both depression and mood disordersymptoms since performance on cognitive tests maybe a sensitive measure of motivational state thatcould augment self-reported symptoms Alternativelythe co-occurrence of cognitive deficits and depressionsymptoms may reflect shared genetic etiology (Hagen-aars et al 2016) and dysfunction of neural circuits
supporting both cognitive and emotional processes(Scult et al 2016) In particular dysfunction of prefront-al and striatal circuits have been associated with bothdepression and cognitive function (Keedwell et al2005 Aarts et al 2011)
Second our findings suggest that prior studies oflinks between cognitive function and depression thatdid not assess baseline symptoms may have overesti-mated the potential protective role of higher cognitivefunction While the importance of accounting for sub-clinical symptoms is not novel the implementation ofsuch accounting is often neglected in psychiatric epi-demiology given the current categorical threshold-based diagnostic system In our meta-analysis largereffects were observed for continuous as compared tocategorical outcomes which aligns with growing em-phasis on dimensional measures of psychopathology(Cuthbert amp Kozak 2013)
Fig 2 Meta-analysis of the association between cognitive function and subsequent depression A forest plot for all studiesthat investigated associations between cognition and later depression Results are reported as correlation coefficients denotedby squares and 95 confidence intervals (CI) indicated by lines (effect sizes are converted to correlation coefficients ifreported as odds ratios) Meta-analysis results are displayed as the diamond The overall analysis found a significant effect ofcognition on depression (r =minus0088 95 CI minus0121 to minus0054 p lt 0001)
12 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Fig 4 Trim-and-fill funnel plots for all samples Fisherrsquos Z a measure of effect size is plotted on the x-axis and the standarderror is plotted on the y-axis Larger studies appear toward the top of the graph and smaller studies towards the bottom Inthe absence of publication bias the studies are symmetrically distributed around the mean Actual studies are shown in opencircles and imputed studies would be shown in black circles No additional studies would be expected in the oppositedirection (to the right) of the observed effect but an additional 11 studies are imputed to the left of the mean effect sizeWhile the calculated effect size is minus0088 [95 confidence interval (CI) minus0121 to minus0054] using Duval amp Tweediersquos trim-and-fill method the imputed effect size estimate is larger at minus0137 (95 CI minus0176 to minus0099 imputed studies n = 11)
Fig 3 Meta-analysis comparing values adjusted for baseline depression symptoms v unadjusted A forest plot for analysiscomparing results from a subset of the same set of studies reported in Fig 2 when using unadjusted values compared tousing values that are adjusted for baseline depression Effects are significant for unadjusted values [r =minus0120 95 confidenceinterval (CI) minus0169 to minus0070 p lt 0001] but not for adjusted values (r =minus0032 95 CI minus0078 to 0014 p = 0169) Results arereported as correlation coefficients denoted by squares and 95 CIs indicated by lines Meta-analysis results are displayed asdiamonds
Association between cognitive function and subsequent depression 13
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Third the associations between cognitive functionand either current or later depression were not moder-ated by data quality or participant age sex and raceHowever there are a number of additional potentialmoderators that could not be addressed in the currentreview and meta-analysis For example the numberand type of comorbid conditions with depressionwere often not reported in the included studies butcould represent an important moderator of theobserved effects Modeling the effects of comorbid ill-ness is an important avenue for future research
One limitation of the current literature is that only ahandful of studies reviewed explicitly excluded for de-pression diagnosis at baseline (Gale et al 2008 Vinberget al 2013 Papmeyer et al 2015) however consistentwith the finding that controlling for baseline depres-sion symptoms led to a null association between cogni-tion and subsequent depression there was no effectobserved when including these studies in the sub-group analyses further suggesting that the associationbetween cognitive function and depression is likelycontemporaneous It will be important to follow-upthese analyses with individual studies that includerigorous assessment of baseline depression symptomsand other potentially confounding factors to furtherclarify this relationship
An open question that remains for future research iswhether deficits in cognitive function are likely to pre-dict the development of more sever or recurrent de-pression later in life Only one of the included studies(Koenen et al 2009) specifically investigated recurrentdepression and found that lower IQ was associatedwith greater persistence of disorder
A final consideration is that while our review andmeta-analysis focused on general cognitive functionmainly assessed via IQ there may be specific subtypesof cognitive function that are more predictive of laterdepression For example a lack of cognitive flexibilitymay more closely match with the ruminative stylecharacteristic of depression and therefore tasks specifi-cally measuring this component of cognitive functionmight have some predictive utility While our reviewdid not find differences between broad and specificmeasures of cognitive function there were not enoughstudies identified to allow for precise consideration ofdifferences between individual cognitive domains
A limitation of the meta-analysis is that while thepresent study followed standard guidelines (Stroupet al 2000 Atkinson et al 2014) decisions aboutstudy selection data extraction and quality assess-ment include a number of decision points that neces-sarily involve a level of subjectivity Reliability wasascertained by using independent raters however dif-ferent inclusionexclusion criteria or a different ap-proach to the evaluation of those criteria could result
in a different set of studies being includedUltimately the quality of the meta-analysis is depend-ent upon the underlying studies that are analyzedFurthermore although studies with insufficient infor-mation to be included in the meta-analysis were notfound to differ based on basic study data from thosestudies included in the meta-analysis nonetheless itis unknown how if at all data from these studiescould change the overall results
Acknowledging these limitations our present reviewand meta-analysis found that while an association is evi-dent between cognitive function and later depressiongeneral cognitive function does not appear to be a riskfactor for depression but rather is more likely relatedto performance decrements associated with concurrentdepressive symptoms Our results suggest that low cog-nitive function is therefore probably not a causal factorof depression and that clinical practice may benefitmore from a focus on how decreased cognitive functionin the depressed state is likely to influence treatment out-comes (Gyurak et al 2015) Our findings have importantimplications for better understanding depression and forthe design of future studies in highlighting the need tocontrol for subthreshold depression symptoms when in-vestigating risk factors for mental illness as well as whenassessing cognitive function more generally
Supplementary material
The supplementary material for this article can befound at httpdxdoiorg101017S0033291716002075
Acknowledgements
MAS is supported by an National Science Foundation(NSF) Graduate Research Fellowship ARH is sup-ported by National Institutes of Health (NIH) grantsRO1DA033369 amp R01AG049789 TEM is supportedby National Institutes of Health (NIH) grantsR01AG049789 We would like to thank HarrisCooper PhD at Duke University who provided invalu-able insight into conducting the meta-analysis Wethank all of the authors of studies who provided add-itional information for this meta-analysis
Declaration of Interest
None
References
Aarts E van Holstein M Cools R (2011) Striatal dopamineand the interface between motivation and cognitionFrontiers in Psychology 2 163
14 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Atkinson KM Koenka AC Sanchez CE Moshontz HCooper H (2014) Reporting standards for literaturesearches and report inclusion criteria making researchsyntheses more transparent and easy to replicate ResearchSynthesis Methods 6 87ndash95
Baer LH Tabri N Blair M Bye D Li KZH Pushkar D(2013) Longitudinal associations of need for cognitioncognitive activity and depressive symptomatology withcognitive function in recent retirees Journals of GerontologySeries B Psychological Sciences and Social Sciences 68 655ndash664
Barbey AK Colom R Solomon J Krueger F Forbes CGrafman J (2012) An integrative architecture for generalintelligence and executive function revealed by lesionmapping Brain 135 1154ndash1164
Barnett JH Salmond CH Jones PB Sahakian BJ (2006)Cognitive reserve in neuropsychiatry Psychological Medicine36 1053ndash1064
Beaujean AA Parker S Qiu X (2013) The relationshipbetween cognitive ability and depression a longitudinaldata analysis Social Psychiatry and Psychiatric Epidemiology48 1983ndash1992
Belsky DW Caspi A Arseneault L Bleidorn W Fonagy PGoodman M Houts R Moffitt TE (2012) Etiologicalfeatures of borderline personality related characteristics in abirth cohort of 12-year-old children Development andPsychopathology 24 251ndash265
Betts KS Williams GM Najman JM Alati R (2016)Predicting spectrums of adult mania psychosis anddepression by prospectively ascertained childhoodneurodevelopment Journal of Psychiatric Research 72 22ndash29
Bora E Harrison BJ Yuumlcel M Pantelis C (2013) Cognitiveimpairment in euthymic major depressive disorder a meta-analysis Psychological Medicine 43 2017ndash2026
Borenstein M Hedges LV Higgins JPT Rothstein HR(2011) Introduction to Meta-Analysis John Wiley amp SonsWest Sussex UK
Canals J Domegravenech-Llaberia E Fernaacutendez-Ballart J Martiacute-Henneberg C (2002) Predictors of depression at eighteenA 7-year follow-up study in a Spanish nonclinicalpopulation European Child amp Adolescent Psychiatry 11226ndash233
Christensen H Griffiths K Mackinnon A (1997) Aquantitative review of cognitive deficits in depression andAlzheimer-type dementia Selection of Studies 3 631ndash651
Connolly SL Wagner Ca Shapero BG Pendergast LLAbramson LY Alloy LB (2014) Rumination prospectivelypredicts executive functioning impairments in adolescentsJournal of Behavior Therapy and Experimental Psychiatry 4546ndash56
Cooper HM (1979) Statistically combining independentstudies a meta-analysis of sex differences in conformityresearch Journal of Personality and Social Psychology 37131ndash146
Cooper HM (2010) Research Synthesis and Meta-Analysis AStep-by-Step Approach 4th edn SAGE PublicationsWashington (DC) USA
Cuijpers P de Graaf R van Dorsselaer S (2004) Minordepression risk profiles functional disability health careuse and risk of developing major depression Journal ofAffective Disorders 79 71ndash79
Cuthbert BN Kozak MJ (2013) Constructing constructs forpsychopathology the NIMH research domain criteriaJournal of Abnormal Psychology 122 928ndash937
Der G Batty GD Deary IJ (2009) The association between IQin adolescence and a range of health outcomes at 40 in the1979 US National Longitudinal Study of Youth Intelligence37 573ndash580
Dubow EF Boxer P Huesmann LR (2008) Childhood andadolescent predictors of early and middle adulthoodalcohol use and problem drinking the Columbia CountyLongitudinal Study Addiction 103 36ndash47
Duval S Tweedie R (2000) Trim and fill a simple funnel-plot-based method of testing and adjusting for publicationbias in meta-analysis Biometrics 56 455ndash463
Evans LD Kouros CD Samanez-Larkin S Garber J (2015)Concurrent and short-term prospective relations amongneurocognitive functioning coping and depressivesymptoms in youth Journal of Clinical Child and AdolescentPsychology 53 1ndash15
Franz CE Lyons MJ OrsquoBrien R Panizzon MS Kim K BhatR Grant MD Toomey R Eisen S Xian H Kremen WS(2011) A 35-year longitudinal assessment of cognition andmidlife depression symptoms the Vietnam Era Twin Studyof Aging American Association for Geriatric PsychiatryAmerican Journal of Geriatric Psychiatry 19 559ndash570
Gale CR Batty GD Tynelius P Deary IJ Rasmussen F(2010) Intelligence in early adulthood and subsequenthospitalization for mental disorders Epidemiology 2170ndash77
Gale CR Deary IJ Boyle SH Barefoot J Mortensen LHBatty GD (2008) Cognitive ability in early adulthood andrisk of 5 specific psychiatric disorders in middle age theVietnam experience study Archives of General Psychiatry 651410ndash1418
Gale CR Hatch SL Batty GD Deary IJ (2009) Intelligence inchildhood and risk of psychological distress in adulthoodthe 1958 National Child Development Survey and the 1970British Cohort Study Intelligence 37 592ndash599
Gjerde PF (1995) Alternative pathways to chronicdepressive symptoms in young adults gender differencesin developmental trajectories Child Development 661277ndash1300
Gottfredson LS (1997) Mainstream science on intelligence aneditorial with 52 signatories history and bibliographyIntelligence 24 13ndash23
Guyer AE Choate VR Grimm KJ Pine DS Keenan K(2011) Emerging depression is associated with facememory deficits in adolescent girls Elsevier Inc Journal ofthe American Academy of Child and Adolescent Psychiatry 50180ndash190
Gyurak A Patenaude B Korgaonkar MS Grieve SMWilliams LM Etkin A (2015) Frontoparietal activationduring response inhibition predicts remission toantidepressants in patients with major depression BiologicalPsychiatry 79 1ndash8
Hagenaars SP Harris SE Davies G Hill WD LiewaldDCM Ritchie SJ Marioni RE Fawns-Ritchie C Cullen BMalik R METASTROKE Consortium IC for BPGSpiroMeta Consortium CHARGE ConsortiumPulmonary Group CCA and LG Worrall BB Sudlow
Association between cognitive function and subsequent depression 15
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
CLM Wardlaw JM Gallacher J Pell J McIntosh AMSmith DJ Gale CR Deary IJ (2016) Shared geneticaetiology between cognitive functions and physical andmental health in UK Biobank (N = 112 151) and 24 GWASconsortiaMolecular Psychiatry Published online 26 January2016 doi101038mp2015225
Hatch SL Jones PB Kuh D Hardy R Wadsworth MEJRichards M (2007) Childhood cognitive ability and adultmental health in the British 1946 birth cohort Social Scienceamp Medicine (1982) 64 2285ndash2296
Hipwell AE Sapotichne B Klostermann S Battista DKeenan K (2011) Autobiographical memory as a predictorof depression vulnerability in girls Journal of Clinical Childand Adolescent Psychology 40 254ndash265
Horowitz JL Garber J (2003) Relation of intelligence andreligiosity to depressive disorders in offspring of depressedand nondepressed mothers The American Academy ofChild and Adolescent Psychiatry Journal of the AmericanAcademy of Child and Adolescent Psychiatry 42 578ndash586
Johnson W Bouchard TJ Krueger RF McGue MGottesman II (2004) Just one g consistent results fromthree test batteries Intelligence 32 95ndash107
Keedwell PA Andrew C Williams SCR Brammer MJPhillips ML (2005) The neural correlates of anhedoniain major depressive disorder Biological Psychiatry 58843ndash853
Kessler RC Berglund P Demler O Jin R Koretz DMerikangas KR Rush AJ Walters EE Wang PS (2003)The epidemiology of major depressive disorder resultsfrom the National Comorbidity Survey Replication(NCS-R) Journal of the American Medical Association 2893095ndash3105
Koenen KC Moffitt TE Roberts AL Martin LT KubzanskyL Harrington H Poulton R Caspi A (2009) Childhood IQand adult mental disorders a test of the cognitive reservehypothesis American Journal of Psychiatry 166 50ndash57
Lewinsohn PM Solomon A Seeley JR Zeiss A (2000)Clinical implications of lsquosubthresholdrsquo depressivesymptoms Journal of Abnormal Psychology 109 345ndash351
Luppino FS de Wit LM Bouvy PF Stijnen T Cuijpers PPenninx BWJH Zitman FG (2010) Overweight obesityand depression a systematic review and meta-analysisof longitudinal studies Archives of General Psychiatry 67220ndash229
McCord J Ensminger ME (1997) Multiple risks andcomorbidity in an African-American population CriminalBehaviour and Mental Health 7 339ndash352
McDermott LM Ebmeier KP (2009) A meta-analysis ofdepression severity and cognitive function Elsevier BVJournal of Affective Disorders 119 1ndash8
Melartin TK Rytsaumllauml HJ Leskelauml US Lestelauml-Mielonen PSSokero TP Isometsauml ET (2002) Current comorbidity ofpsychiatric disorders among DSM-IV major depressivedisorder patients in psychiatric care in the VantaaDepression Study Journal of Clinical Psychiatry 63 126ndash134
Meyer SE Carlson GA Wiggs EA Martinez PE RonsavilleDS KlimesndashDougan B Gold PW RadkendashYarrow M(2004) A prospective study of the association amongimpaired executive functioning childhood attentional
problems and the development of bipolar disorderDevelopment and Psychopathology 16 461ndash476
MiyakeA FriedmanNP EmersonMJWitzki aHHowerter AWager TD (2000) The unity and diversity of executivefunctions and their contributions to complex lsquoFrontal Lobersquotasks a latentvariable analysisCognitive Psychology41 49ndash100
Moher D Liberati A (2009) Preferred reporting items forsystematic reviews and meta-analyses the PRISMAstatement Annals of Internal Medicine 151 264ndash269
Papmeyer M Sussmann JE Hall J McKirdy J Peel AMacdonald A Lawrie SM Whalley HC McIntosh AM(2015) Neurocognition in individuals at high familial riskof mood disorders with or without subsequent onset ofdepression Psychological Medicine 45 1ndash11
Peterson RA Brown SP (2005) On the use of betacoefficients in meta-analysis Journal of Applied Psychology90 175ndash181
Pine DS Cohen P Brook J Coplan JD (1997) Psychiatricsymptoms in adolescence as predictors of obesity in earlyadulthood a longitudinal study American Journal of PublicHealth 87 1303ndash1310
Quinn ME Joormann J (2015) Control when it countschange in executive control under stress predicts depressionsymptoms Emotion Junio 22 1ndash10
Rawal A Rice F (2012) Examining overgeneralautobiographical memory as a risk factor for adolescentdepression Elsevier Inc Journal of the American Academy ofChild and Adolescent Psychiatry 51 518ndash527
Ree MJ Earles JA (1991) The stability of g across differentmethods of estimation Intelligence 15 271ndash278
Rock PL Roiser JP Riedel WJ Blackwell AD (2014)Cognitive impairment in depression a systematic reviewand meta-analysis Psychological Medicine 44 2029ndash2040
Rogers MA Kasai K Koji M Fukuda R Iwanami ANakagome K Fukuda M Kato N (2004) Executive andprefrontal dysfunction in unipolar depression a review ofneuropsychological and imaging evidence NeuroscienceResearch 50 1ndash11
Scult MA Knodt AR Swartz JR Brigidi BD Hariri AR(2016) Thinking and feeling individual differences inhabitual emotion regulation and stress-related mood areassociated with prefrontal executive control ClinicalPsychological Science doi1011772167702616654688
Sharp C Petersen N Goodyer I (2008) Emotional reactivityand the emergence of conduct problems and emotionalsymptoms in 7- to 11-year-olds a 1-year follow-up studyJournal of the American Academy of Child and AdolescentPsychiatry 47 565ndash573
Siegel LS (1999) Issues in the definition and diagnosis oflearning disabilities a perspective on Guckenberger vBoston University Journal of Learning Disabilities 32 304ndash319
Simons CJP Jacobs N Derom C Thiery E Jolles J van Os JKrabbendam L (2009) Cognition as predictor of currentand follow-up depressive symptoms in the generalpopulation Acta Psychiatrica Scandinavica 120 45ndash52
Slykerman RF Thompson J Waldie K Murphy R Wall CMitchell EA (2015) Maternal stress during pregnancy isassociated with moderate to severe depression in 11-year-old children Acta Paediatrica 104 68ndash74
16 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Snyder HR (2013) Major depressive disorder is associatedwith broad impairments on neuropsychological measuresof executive function a meta-analysis and reviewPsychological Bulletin 139 81ndash132
Soslashrensen HJ Saeligbye D Urfer-Parnas A Mortensen ELParnas J (2012) Premorbid intelligence and educationallevel in bipolar and unipolar disorders a Danish draftboard study Journal of Affective Disorders 136 1188ndash1191
SpearmanC (1904) lsquoGeneral intelligencersquoobjectivelydeterminedandmeasuredAmerican Journal of Psychology 15 201
Stern Y (2003) The concept of cognitive reserve a catalyst forresearch Journal of Clinical and Experimental Neuropsychology(Neuropsychology Development and Cognition Section A) 25589ndash593
Stroup D Berlin J Morton S Olkin I Williamson GDRennie D Moher D Becker BJ Sipe TA Thacker SB(2000) Meta-analysis of Observational Studies inEpidemiology a proposal for reporting Journal of theAmerican Medical Association 283 2008
Vinberg M Miskowiak KW Kessing LV (2013) Impairmentof executive function and attention predicts onset ofaffective disorder in healthy high-risk twins Journal ofClinical Psychiatry 74 e747ndashe753
Zammit S Allebeck P David AS Dalman C HemmingssonT Lundberg I Lewis G (2004) A longitudinal study ofpremorbid IQ Score and risk of developing schizophreniabipolar disorder severe depression and other nonaffectivepsychoses Archives of General Psychiatry 61 354ndash360
Association between cognitive function and subsequent depression 17
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms

v 12 respectively p = 057) The types of cognitivemeasures used were also similar across the excludedand included studies with the most common measurebeing IQ (2860 and 2029) followed by VerbalComprehension (860 and 529)
Meta-analysis
The overall analysis yielded a significant associationbetween cognitive function and subsequent depressionoutcomes [r =minus0088 95 confidence interval (CI)minus0121 to minus0054 p lt 0001 Fig 2] Results were similarwhen excluding the two studies that used beta-weights(r =minus0071 95 CI minus0100 to minus0042 p lt 0001) orwhen using episodic memory in place of processingspeed in a study reporting both outcomes (r =minus008595 CI minus0118 to minus0051 p lt 0001) Follow-up ana-lyses were conducted in the sample of studies report-ing educational attainment and self-report outcomes(Supplementary Table S2) Heterogeneity across sam-ples was significant (Q = 80154 p lt 0001) suggestingsubstantial variation across the individual samplesThe ratio of the true heterogeneity to total variationwas large (I2 = 9588) I2 is on a relative scale andvalues close to 100 indicate that most of the observedvariance is real rather than spurious and suggeststhat subgroup analyses or meta-regression may helpto explain this variability (Borenstein et al 2011)
Subgroup analyses and meta-regression
A significant difference was found between categoricaland continuous effect sizes (p lt 0001) The studiesassessing continuous outcomes were found to have alarger effect (r =minus0121 95 CI minus0168 to minus0073 p lt0001 n = 22) than studies assessing categorical out-comes (r =minus0035 95 CI minus0054 to minus0017 p lt 0001n = 12) No differences were observed between studiesutilizing broad v specific cognitive measures (p = 057)
Outcomes were also compared adjusting for baselinedepression symptoms at the time of cognitive assess-ment Nine studies provided enough detail to calculatethe partial correlation coefficients adjusting for base-line depression symptoms Using the partial correl-ation coefficients led to a null result (r =minus0032 95CI minus0078 to 0014 p = 0169 n = 9 Fig 3) The nullresult does not seem to be due to a lack of power be-cause using the unadjusted correlation coefficients forthe same nine studies still led to a significant result(r =minus0120 95 CI minus0169 to minus0070 p lt 0001 n = 9Fig 3) As a follow-up the difference in effect sizes be-tween the adjusted and unadjusted values for these 9studies were tested (r = 0082 95 CI 0069ndash0095 p lt0001 n = 9) suggesting that the effects are significantlydifferent when directly comparing the values that doand do not control for baseline depression symptoms
Expanding the subgroup analyses to include studiesthat controlled for baseline depression plus other co-variates (Zammit et al 2004 Simons et al 2009 Rawalamp Rice 2012) and studies that explicitly excluded fora history of depression diagnosis (Gale et al 2008Vinberg et al 2013 Papmeyer et al 2015) did notchange the null result (r =minus0027 95 CI minus0058 to0005 p = 0097 n = 15)
None of the meta-regression analyses were signifi-cant indicating that the between-study variance wasnot attributable to age at baseline IQ percent of sam-ple that was female percent of the sample that waswhite age at follow-up time between assessmentsyear of cognitive assessment year of follow-up assess-ment or study quality score
Study quality and publication bias
Multiple samples within a study were combined forthe purposes of quality assessment given that studieswithin the same publication were found to employthe same methodology Of the 29 publications reviewed12 were rated as high quality and 17 were rated as me-dium quality Details are provided in SupplementaryTable S1 Comparable results to the overall findingswere obtained when just using high quality studies (r=minus0085 95 CI minus0141 to minus0029 p = 0003)
Inspection of the funnel plot (Fig 4) found no evi-dence for publication bias to support the hypothesisIn fact imputation of negative correlations suggestedthat additional studies favoring the hypothesis maybe missing While the calculated effect size is minus0088(95 CI minus0121 to minus0054) using Duval amp Tweediersquostrim-and-fill method the imputed effect size estimateis larger at minus0137 (95 CI minus0176 to minus0099 imputedstudies n = 11) Last the Fail-safe N procedure foundthat 3583 null studies would need to be located forthe combined two-tailed p value to exceed 005 Thissuggests that significant results are not likely to be con-founded by publication bias and may even underesti-mate true effect sizes
Discussion
The present systematic review and meta-analysis of 29longitudinal publications including 1 21 749 partici-pants revealed that after accounting for baseline depres-sion symptoms variability in cognitive function did notpredict subsequent depression Consistent with priorreports there was a significant contemporaneous associ-ation between higher depression symptoms and lowercognitive function These patterns have implications forunderstanding the association between cognitive func-tion and depression and may be important for advan-cing etiologic and treatment research
Association between cognitive function and subsequent depression 11
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
First our findings reinforce models positing thatcognitive function tracks with depression severity(McDermott amp Ebmeier 2009) One possible explan-ation for this contemporaneous association is that de-pression symptoms interfere with the capacity tocomplete cognitive assessments possibly through thegeneral lack of motivation that is one hallmark of thedisorder While this explanation represents an experi-mental confound for studies focused on assessmentof cognitive function it likewise represents an oppor-tunity for studies to focus more comprehensively onthe assessment of both depression and mood disordersymptoms since performance on cognitive tests maybe a sensitive measure of motivational state thatcould augment self-reported symptoms Alternativelythe co-occurrence of cognitive deficits and depressionsymptoms may reflect shared genetic etiology (Hagen-aars et al 2016) and dysfunction of neural circuits
supporting both cognitive and emotional processes(Scult et al 2016) In particular dysfunction of prefront-al and striatal circuits have been associated with bothdepression and cognitive function (Keedwell et al2005 Aarts et al 2011)
Second our findings suggest that prior studies oflinks between cognitive function and depression thatdid not assess baseline symptoms may have overesti-mated the potential protective role of higher cognitivefunction While the importance of accounting for sub-clinical symptoms is not novel the implementation ofsuch accounting is often neglected in psychiatric epi-demiology given the current categorical threshold-based diagnostic system In our meta-analysis largereffects were observed for continuous as compared tocategorical outcomes which aligns with growing em-phasis on dimensional measures of psychopathology(Cuthbert amp Kozak 2013)
Fig 2 Meta-analysis of the association between cognitive function and subsequent depression A forest plot for all studiesthat investigated associations between cognition and later depression Results are reported as correlation coefficients denotedby squares and 95 confidence intervals (CI) indicated by lines (effect sizes are converted to correlation coefficients ifreported as odds ratios) Meta-analysis results are displayed as the diamond The overall analysis found a significant effect ofcognition on depression (r =minus0088 95 CI minus0121 to minus0054 p lt 0001)
12 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Fig 4 Trim-and-fill funnel plots for all samples Fisherrsquos Z a measure of effect size is plotted on the x-axis and the standarderror is plotted on the y-axis Larger studies appear toward the top of the graph and smaller studies towards the bottom Inthe absence of publication bias the studies are symmetrically distributed around the mean Actual studies are shown in opencircles and imputed studies would be shown in black circles No additional studies would be expected in the oppositedirection (to the right) of the observed effect but an additional 11 studies are imputed to the left of the mean effect sizeWhile the calculated effect size is minus0088 [95 confidence interval (CI) minus0121 to minus0054] using Duval amp Tweediersquos trim-and-fill method the imputed effect size estimate is larger at minus0137 (95 CI minus0176 to minus0099 imputed studies n = 11)
Fig 3 Meta-analysis comparing values adjusted for baseline depression symptoms v unadjusted A forest plot for analysiscomparing results from a subset of the same set of studies reported in Fig 2 when using unadjusted values compared tousing values that are adjusted for baseline depression Effects are significant for unadjusted values [r =minus0120 95 confidenceinterval (CI) minus0169 to minus0070 p lt 0001] but not for adjusted values (r =minus0032 95 CI minus0078 to 0014 p = 0169) Results arereported as correlation coefficients denoted by squares and 95 CIs indicated by lines Meta-analysis results are displayed asdiamonds
Association between cognitive function and subsequent depression 13
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Third the associations between cognitive functionand either current or later depression were not moder-ated by data quality or participant age sex and raceHowever there are a number of additional potentialmoderators that could not be addressed in the currentreview and meta-analysis For example the numberand type of comorbid conditions with depressionwere often not reported in the included studies butcould represent an important moderator of theobserved effects Modeling the effects of comorbid ill-ness is an important avenue for future research
One limitation of the current literature is that only ahandful of studies reviewed explicitly excluded for de-pression diagnosis at baseline (Gale et al 2008 Vinberget al 2013 Papmeyer et al 2015) however consistentwith the finding that controlling for baseline depres-sion symptoms led to a null association between cogni-tion and subsequent depression there was no effectobserved when including these studies in the sub-group analyses further suggesting that the associationbetween cognitive function and depression is likelycontemporaneous It will be important to follow-upthese analyses with individual studies that includerigorous assessment of baseline depression symptomsand other potentially confounding factors to furtherclarify this relationship
An open question that remains for future research iswhether deficits in cognitive function are likely to pre-dict the development of more sever or recurrent de-pression later in life Only one of the included studies(Koenen et al 2009) specifically investigated recurrentdepression and found that lower IQ was associatedwith greater persistence of disorder
A final consideration is that while our review andmeta-analysis focused on general cognitive functionmainly assessed via IQ there may be specific subtypesof cognitive function that are more predictive of laterdepression For example a lack of cognitive flexibilitymay more closely match with the ruminative stylecharacteristic of depression and therefore tasks specifi-cally measuring this component of cognitive functionmight have some predictive utility While our reviewdid not find differences between broad and specificmeasures of cognitive function there were not enoughstudies identified to allow for precise consideration ofdifferences between individual cognitive domains
A limitation of the meta-analysis is that while thepresent study followed standard guidelines (Stroupet al 2000 Atkinson et al 2014) decisions aboutstudy selection data extraction and quality assess-ment include a number of decision points that neces-sarily involve a level of subjectivity Reliability wasascertained by using independent raters however dif-ferent inclusionexclusion criteria or a different ap-proach to the evaluation of those criteria could result
in a different set of studies being includedUltimately the quality of the meta-analysis is depend-ent upon the underlying studies that are analyzedFurthermore although studies with insufficient infor-mation to be included in the meta-analysis were notfound to differ based on basic study data from thosestudies included in the meta-analysis nonetheless itis unknown how if at all data from these studiescould change the overall results
Acknowledging these limitations our present reviewand meta-analysis found that while an association is evi-dent between cognitive function and later depressiongeneral cognitive function does not appear to be a riskfactor for depression but rather is more likely relatedto performance decrements associated with concurrentdepressive symptoms Our results suggest that low cog-nitive function is therefore probably not a causal factorof depression and that clinical practice may benefitmore from a focus on how decreased cognitive functionin the depressed state is likely to influence treatment out-comes (Gyurak et al 2015) Our findings have importantimplications for better understanding depression and forthe design of future studies in highlighting the need tocontrol for subthreshold depression symptoms when in-vestigating risk factors for mental illness as well as whenassessing cognitive function more generally
Supplementary material
The supplementary material for this article can befound at httpdxdoiorg101017S0033291716002075
Acknowledgements
MAS is supported by an National Science Foundation(NSF) Graduate Research Fellowship ARH is sup-ported by National Institutes of Health (NIH) grantsRO1DA033369 amp R01AG049789 TEM is supportedby National Institutes of Health (NIH) grantsR01AG049789 We would like to thank HarrisCooper PhD at Duke University who provided invalu-able insight into conducting the meta-analysis Wethank all of the authors of studies who provided add-itional information for this meta-analysis
Declaration of Interest
None
References
Aarts E van Holstein M Cools R (2011) Striatal dopamineand the interface between motivation and cognitionFrontiers in Psychology 2 163
14 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Atkinson KM Koenka AC Sanchez CE Moshontz HCooper H (2014) Reporting standards for literaturesearches and report inclusion criteria making researchsyntheses more transparent and easy to replicate ResearchSynthesis Methods 6 87ndash95
Baer LH Tabri N Blair M Bye D Li KZH Pushkar D(2013) Longitudinal associations of need for cognitioncognitive activity and depressive symptomatology withcognitive function in recent retirees Journals of GerontologySeries B Psychological Sciences and Social Sciences 68 655ndash664
Barbey AK Colom R Solomon J Krueger F Forbes CGrafman J (2012) An integrative architecture for generalintelligence and executive function revealed by lesionmapping Brain 135 1154ndash1164
Barnett JH Salmond CH Jones PB Sahakian BJ (2006)Cognitive reserve in neuropsychiatry Psychological Medicine36 1053ndash1064
Beaujean AA Parker S Qiu X (2013) The relationshipbetween cognitive ability and depression a longitudinaldata analysis Social Psychiatry and Psychiatric Epidemiology48 1983ndash1992
Belsky DW Caspi A Arseneault L Bleidorn W Fonagy PGoodman M Houts R Moffitt TE (2012) Etiologicalfeatures of borderline personality related characteristics in abirth cohort of 12-year-old children Development andPsychopathology 24 251ndash265
Betts KS Williams GM Najman JM Alati R (2016)Predicting spectrums of adult mania psychosis anddepression by prospectively ascertained childhoodneurodevelopment Journal of Psychiatric Research 72 22ndash29
Bora E Harrison BJ Yuumlcel M Pantelis C (2013) Cognitiveimpairment in euthymic major depressive disorder a meta-analysis Psychological Medicine 43 2017ndash2026
Borenstein M Hedges LV Higgins JPT Rothstein HR(2011) Introduction to Meta-Analysis John Wiley amp SonsWest Sussex UK
Canals J Domegravenech-Llaberia E Fernaacutendez-Ballart J Martiacute-Henneberg C (2002) Predictors of depression at eighteenA 7-year follow-up study in a Spanish nonclinicalpopulation European Child amp Adolescent Psychiatry 11226ndash233
Christensen H Griffiths K Mackinnon A (1997) Aquantitative review of cognitive deficits in depression andAlzheimer-type dementia Selection of Studies 3 631ndash651
Connolly SL Wagner Ca Shapero BG Pendergast LLAbramson LY Alloy LB (2014) Rumination prospectivelypredicts executive functioning impairments in adolescentsJournal of Behavior Therapy and Experimental Psychiatry 4546ndash56
Cooper HM (1979) Statistically combining independentstudies a meta-analysis of sex differences in conformityresearch Journal of Personality and Social Psychology 37131ndash146
Cooper HM (2010) Research Synthesis and Meta-Analysis AStep-by-Step Approach 4th edn SAGE PublicationsWashington (DC) USA
Cuijpers P de Graaf R van Dorsselaer S (2004) Minordepression risk profiles functional disability health careuse and risk of developing major depression Journal ofAffective Disorders 79 71ndash79
Cuthbert BN Kozak MJ (2013) Constructing constructs forpsychopathology the NIMH research domain criteriaJournal of Abnormal Psychology 122 928ndash937
Der G Batty GD Deary IJ (2009) The association between IQin adolescence and a range of health outcomes at 40 in the1979 US National Longitudinal Study of Youth Intelligence37 573ndash580
Dubow EF Boxer P Huesmann LR (2008) Childhood andadolescent predictors of early and middle adulthoodalcohol use and problem drinking the Columbia CountyLongitudinal Study Addiction 103 36ndash47
Duval S Tweedie R (2000) Trim and fill a simple funnel-plot-based method of testing and adjusting for publicationbias in meta-analysis Biometrics 56 455ndash463
Evans LD Kouros CD Samanez-Larkin S Garber J (2015)Concurrent and short-term prospective relations amongneurocognitive functioning coping and depressivesymptoms in youth Journal of Clinical Child and AdolescentPsychology 53 1ndash15
Franz CE Lyons MJ OrsquoBrien R Panizzon MS Kim K BhatR Grant MD Toomey R Eisen S Xian H Kremen WS(2011) A 35-year longitudinal assessment of cognition andmidlife depression symptoms the Vietnam Era Twin Studyof Aging American Association for Geriatric PsychiatryAmerican Journal of Geriatric Psychiatry 19 559ndash570
Gale CR Batty GD Tynelius P Deary IJ Rasmussen F(2010) Intelligence in early adulthood and subsequenthospitalization for mental disorders Epidemiology 2170ndash77
Gale CR Deary IJ Boyle SH Barefoot J Mortensen LHBatty GD (2008) Cognitive ability in early adulthood andrisk of 5 specific psychiatric disorders in middle age theVietnam experience study Archives of General Psychiatry 651410ndash1418
Gale CR Hatch SL Batty GD Deary IJ (2009) Intelligence inchildhood and risk of psychological distress in adulthoodthe 1958 National Child Development Survey and the 1970British Cohort Study Intelligence 37 592ndash599
Gjerde PF (1995) Alternative pathways to chronicdepressive symptoms in young adults gender differencesin developmental trajectories Child Development 661277ndash1300
Gottfredson LS (1997) Mainstream science on intelligence aneditorial with 52 signatories history and bibliographyIntelligence 24 13ndash23
Guyer AE Choate VR Grimm KJ Pine DS Keenan K(2011) Emerging depression is associated with facememory deficits in adolescent girls Elsevier Inc Journal ofthe American Academy of Child and Adolescent Psychiatry 50180ndash190
Gyurak A Patenaude B Korgaonkar MS Grieve SMWilliams LM Etkin A (2015) Frontoparietal activationduring response inhibition predicts remission toantidepressants in patients with major depression BiologicalPsychiatry 79 1ndash8
Hagenaars SP Harris SE Davies G Hill WD LiewaldDCM Ritchie SJ Marioni RE Fawns-Ritchie C Cullen BMalik R METASTROKE Consortium IC for BPGSpiroMeta Consortium CHARGE ConsortiumPulmonary Group CCA and LG Worrall BB Sudlow
Association between cognitive function and subsequent depression 15
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
CLM Wardlaw JM Gallacher J Pell J McIntosh AMSmith DJ Gale CR Deary IJ (2016) Shared geneticaetiology between cognitive functions and physical andmental health in UK Biobank (N = 112 151) and 24 GWASconsortiaMolecular Psychiatry Published online 26 January2016 doi101038mp2015225
Hatch SL Jones PB Kuh D Hardy R Wadsworth MEJRichards M (2007) Childhood cognitive ability and adultmental health in the British 1946 birth cohort Social Scienceamp Medicine (1982) 64 2285ndash2296
Hipwell AE Sapotichne B Klostermann S Battista DKeenan K (2011) Autobiographical memory as a predictorof depression vulnerability in girls Journal of Clinical Childand Adolescent Psychology 40 254ndash265
Horowitz JL Garber J (2003) Relation of intelligence andreligiosity to depressive disorders in offspring of depressedand nondepressed mothers The American Academy ofChild and Adolescent Psychiatry Journal of the AmericanAcademy of Child and Adolescent Psychiatry 42 578ndash586
Johnson W Bouchard TJ Krueger RF McGue MGottesman II (2004) Just one g consistent results fromthree test batteries Intelligence 32 95ndash107
Keedwell PA Andrew C Williams SCR Brammer MJPhillips ML (2005) The neural correlates of anhedoniain major depressive disorder Biological Psychiatry 58843ndash853
Kessler RC Berglund P Demler O Jin R Koretz DMerikangas KR Rush AJ Walters EE Wang PS (2003)The epidemiology of major depressive disorder resultsfrom the National Comorbidity Survey Replication(NCS-R) Journal of the American Medical Association 2893095ndash3105
Koenen KC Moffitt TE Roberts AL Martin LT KubzanskyL Harrington H Poulton R Caspi A (2009) Childhood IQand adult mental disorders a test of the cognitive reservehypothesis American Journal of Psychiatry 166 50ndash57
Lewinsohn PM Solomon A Seeley JR Zeiss A (2000)Clinical implications of lsquosubthresholdrsquo depressivesymptoms Journal of Abnormal Psychology 109 345ndash351
Luppino FS de Wit LM Bouvy PF Stijnen T Cuijpers PPenninx BWJH Zitman FG (2010) Overweight obesityand depression a systematic review and meta-analysisof longitudinal studies Archives of General Psychiatry 67220ndash229
McCord J Ensminger ME (1997) Multiple risks andcomorbidity in an African-American population CriminalBehaviour and Mental Health 7 339ndash352
McDermott LM Ebmeier KP (2009) A meta-analysis ofdepression severity and cognitive function Elsevier BVJournal of Affective Disorders 119 1ndash8
Melartin TK Rytsaumllauml HJ Leskelauml US Lestelauml-Mielonen PSSokero TP Isometsauml ET (2002) Current comorbidity ofpsychiatric disorders among DSM-IV major depressivedisorder patients in psychiatric care in the VantaaDepression Study Journal of Clinical Psychiatry 63 126ndash134
Meyer SE Carlson GA Wiggs EA Martinez PE RonsavilleDS KlimesndashDougan B Gold PW RadkendashYarrow M(2004) A prospective study of the association amongimpaired executive functioning childhood attentional
problems and the development of bipolar disorderDevelopment and Psychopathology 16 461ndash476
MiyakeA FriedmanNP EmersonMJWitzki aHHowerter AWager TD (2000) The unity and diversity of executivefunctions and their contributions to complex lsquoFrontal Lobersquotasks a latentvariable analysisCognitive Psychology41 49ndash100
Moher D Liberati A (2009) Preferred reporting items forsystematic reviews and meta-analyses the PRISMAstatement Annals of Internal Medicine 151 264ndash269
Papmeyer M Sussmann JE Hall J McKirdy J Peel AMacdonald A Lawrie SM Whalley HC McIntosh AM(2015) Neurocognition in individuals at high familial riskof mood disorders with or without subsequent onset ofdepression Psychological Medicine 45 1ndash11
Peterson RA Brown SP (2005) On the use of betacoefficients in meta-analysis Journal of Applied Psychology90 175ndash181
Pine DS Cohen P Brook J Coplan JD (1997) Psychiatricsymptoms in adolescence as predictors of obesity in earlyadulthood a longitudinal study American Journal of PublicHealth 87 1303ndash1310
Quinn ME Joormann J (2015) Control when it countschange in executive control under stress predicts depressionsymptoms Emotion Junio 22 1ndash10
Rawal A Rice F (2012) Examining overgeneralautobiographical memory as a risk factor for adolescentdepression Elsevier Inc Journal of the American Academy ofChild and Adolescent Psychiatry 51 518ndash527
Ree MJ Earles JA (1991) The stability of g across differentmethods of estimation Intelligence 15 271ndash278
Rock PL Roiser JP Riedel WJ Blackwell AD (2014)Cognitive impairment in depression a systematic reviewand meta-analysis Psychological Medicine 44 2029ndash2040
Rogers MA Kasai K Koji M Fukuda R Iwanami ANakagome K Fukuda M Kato N (2004) Executive andprefrontal dysfunction in unipolar depression a review ofneuropsychological and imaging evidence NeuroscienceResearch 50 1ndash11
Scult MA Knodt AR Swartz JR Brigidi BD Hariri AR(2016) Thinking and feeling individual differences inhabitual emotion regulation and stress-related mood areassociated with prefrontal executive control ClinicalPsychological Science doi1011772167702616654688
Sharp C Petersen N Goodyer I (2008) Emotional reactivityand the emergence of conduct problems and emotionalsymptoms in 7- to 11-year-olds a 1-year follow-up studyJournal of the American Academy of Child and AdolescentPsychiatry 47 565ndash573
Siegel LS (1999) Issues in the definition and diagnosis oflearning disabilities a perspective on Guckenberger vBoston University Journal of Learning Disabilities 32 304ndash319
Simons CJP Jacobs N Derom C Thiery E Jolles J van Os JKrabbendam L (2009) Cognition as predictor of currentand follow-up depressive symptoms in the generalpopulation Acta Psychiatrica Scandinavica 120 45ndash52
Slykerman RF Thompson J Waldie K Murphy R Wall CMitchell EA (2015) Maternal stress during pregnancy isassociated with moderate to severe depression in 11-year-old children Acta Paediatrica 104 68ndash74
16 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Snyder HR (2013) Major depressive disorder is associatedwith broad impairments on neuropsychological measuresof executive function a meta-analysis and reviewPsychological Bulletin 139 81ndash132
Soslashrensen HJ Saeligbye D Urfer-Parnas A Mortensen ELParnas J (2012) Premorbid intelligence and educationallevel in bipolar and unipolar disorders a Danish draftboard study Journal of Affective Disorders 136 1188ndash1191
SpearmanC (1904) lsquoGeneral intelligencersquoobjectivelydeterminedandmeasuredAmerican Journal of Psychology 15 201
Stern Y (2003) The concept of cognitive reserve a catalyst forresearch Journal of Clinical and Experimental Neuropsychology(Neuropsychology Development and Cognition Section A) 25589ndash593
Stroup D Berlin J Morton S Olkin I Williamson GDRennie D Moher D Becker BJ Sipe TA Thacker SB(2000) Meta-analysis of Observational Studies inEpidemiology a proposal for reporting Journal of theAmerican Medical Association 283 2008
Vinberg M Miskowiak KW Kessing LV (2013) Impairmentof executive function and attention predicts onset ofaffective disorder in healthy high-risk twins Journal ofClinical Psychiatry 74 e747ndashe753
Zammit S Allebeck P David AS Dalman C HemmingssonT Lundberg I Lewis G (2004) A longitudinal study ofpremorbid IQ Score and risk of developing schizophreniabipolar disorder severe depression and other nonaffectivepsychoses Archives of General Psychiatry 61 354ndash360
Association between cognitive function and subsequent depression 17
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms

First our findings reinforce models positing thatcognitive function tracks with depression severity(McDermott amp Ebmeier 2009) One possible explan-ation for this contemporaneous association is that de-pression symptoms interfere with the capacity tocomplete cognitive assessments possibly through thegeneral lack of motivation that is one hallmark of thedisorder While this explanation represents an experi-mental confound for studies focused on assessmentof cognitive function it likewise represents an oppor-tunity for studies to focus more comprehensively onthe assessment of both depression and mood disordersymptoms since performance on cognitive tests maybe a sensitive measure of motivational state thatcould augment self-reported symptoms Alternativelythe co-occurrence of cognitive deficits and depressionsymptoms may reflect shared genetic etiology (Hagen-aars et al 2016) and dysfunction of neural circuits
supporting both cognitive and emotional processes(Scult et al 2016) In particular dysfunction of prefront-al and striatal circuits have been associated with bothdepression and cognitive function (Keedwell et al2005 Aarts et al 2011)
Second our findings suggest that prior studies oflinks between cognitive function and depression thatdid not assess baseline symptoms may have overesti-mated the potential protective role of higher cognitivefunction While the importance of accounting for sub-clinical symptoms is not novel the implementation ofsuch accounting is often neglected in psychiatric epi-demiology given the current categorical threshold-based diagnostic system In our meta-analysis largereffects were observed for continuous as compared tocategorical outcomes which aligns with growing em-phasis on dimensional measures of psychopathology(Cuthbert amp Kozak 2013)
Fig 2 Meta-analysis of the association between cognitive function and subsequent depression A forest plot for all studiesthat investigated associations between cognition and later depression Results are reported as correlation coefficients denotedby squares and 95 confidence intervals (CI) indicated by lines (effect sizes are converted to correlation coefficients ifreported as odds ratios) Meta-analysis results are displayed as the diamond The overall analysis found a significant effect ofcognition on depression (r =minus0088 95 CI minus0121 to minus0054 p lt 0001)
12 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Fig 4 Trim-and-fill funnel plots for all samples Fisherrsquos Z a measure of effect size is plotted on the x-axis and the standarderror is plotted on the y-axis Larger studies appear toward the top of the graph and smaller studies towards the bottom Inthe absence of publication bias the studies are symmetrically distributed around the mean Actual studies are shown in opencircles and imputed studies would be shown in black circles No additional studies would be expected in the oppositedirection (to the right) of the observed effect but an additional 11 studies are imputed to the left of the mean effect sizeWhile the calculated effect size is minus0088 [95 confidence interval (CI) minus0121 to minus0054] using Duval amp Tweediersquos trim-and-fill method the imputed effect size estimate is larger at minus0137 (95 CI minus0176 to minus0099 imputed studies n = 11)
Fig 3 Meta-analysis comparing values adjusted for baseline depression symptoms v unadjusted A forest plot for analysiscomparing results from a subset of the same set of studies reported in Fig 2 when using unadjusted values compared tousing values that are adjusted for baseline depression Effects are significant for unadjusted values [r =minus0120 95 confidenceinterval (CI) minus0169 to minus0070 p lt 0001] but not for adjusted values (r =minus0032 95 CI minus0078 to 0014 p = 0169) Results arereported as correlation coefficients denoted by squares and 95 CIs indicated by lines Meta-analysis results are displayed asdiamonds
Association between cognitive function and subsequent depression 13
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Third the associations between cognitive functionand either current or later depression were not moder-ated by data quality or participant age sex and raceHowever there are a number of additional potentialmoderators that could not be addressed in the currentreview and meta-analysis For example the numberand type of comorbid conditions with depressionwere often not reported in the included studies butcould represent an important moderator of theobserved effects Modeling the effects of comorbid ill-ness is an important avenue for future research
One limitation of the current literature is that only ahandful of studies reviewed explicitly excluded for de-pression diagnosis at baseline (Gale et al 2008 Vinberget al 2013 Papmeyer et al 2015) however consistentwith the finding that controlling for baseline depres-sion symptoms led to a null association between cogni-tion and subsequent depression there was no effectobserved when including these studies in the sub-group analyses further suggesting that the associationbetween cognitive function and depression is likelycontemporaneous It will be important to follow-upthese analyses with individual studies that includerigorous assessment of baseline depression symptomsand other potentially confounding factors to furtherclarify this relationship
An open question that remains for future research iswhether deficits in cognitive function are likely to pre-dict the development of more sever or recurrent de-pression later in life Only one of the included studies(Koenen et al 2009) specifically investigated recurrentdepression and found that lower IQ was associatedwith greater persistence of disorder
A final consideration is that while our review andmeta-analysis focused on general cognitive functionmainly assessed via IQ there may be specific subtypesof cognitive function that are more predictive of laterdepression For example a lack of cognitive flexibilitymay more closely match with the ruminative stylecharacteristic of depression and therefore tasks specifi-cally measuring this component of cognitive functionmight have some predictive utility While our reviewdid not find differences between broad and specificmeasures of cognitive function there were not enoughstudies identified to allow for precise consideration ofdifferences between individual cognitive domains
A limitation of the meta-analysis is that while thepresent study followed standard guidelines (Stroupet al 2000 Atkinson et al 2014) decisions aboutstudy selection data extraction and quality assess-ment include a number of decision points that neces-sarily involve a level of subjectivity Reliability wasascertained by using independent raters however dif-ferent inclusionexclusion criteria or a different ap-proach to the evaluation of those criteria could result
in a different set of studies being includedUltimately the quality of the meta-analysis is depend-ent upon the underlying studies that are analyzedFurthermore although studies with insufficient infor-mation to be included in the meta-analysis were notfound to differ based on basic study data from thosestudies included in the meta-analysis nonetheless itis unknown how if at all data from these studiescould change the overall results
Acknowledging these limitations our present reviewand meta-analysis found that while an association is evi-dent between cognitive function and later depressiongeneral cognitive function does not appear to be a riskfactor for depression but rather is more likely relatedto performance decrements associated with concurrentdepressive symptoms Our results suggest that low cog-nitive function is therefore probably not a causal factorof depression and that clinical practice may benefitmore from a focus on how decreased cognitive functionin the depressed state is likely to influence treatment out-comes (Gyurak et al 2015) Our findings have importantimplications for better understanding depression and forthe design of future studies in highlighting the need tocontrol for subthreshold depression symptoms when in-vestigating risk factors for mental illness as well as whenassessing cognitive function more generally
Supplementary material
The supplementary material for this article can befound at httpdxdoiorg101017S0033291716002075
Acknowledgements
MAS is supported by an National Science Foundation(NSF) Graduate Research Fellowship ARH is sup-ported by National Institutes of Health (NIH) grantsRO1DA033369 amp R01AG049789 TEM is supportedby National Institutes of Health (NIH) grantsR01AG049789 We would like to thank HarrisCooper PhD at Duke University who provided invalu-able insight into conducting the meta-analysis Wethank all of the authors of studies who provided add-itional information for this meta-analysis
Declaration of Interest
None
References
Aarts E van Holstein M Cools R (2011) Striatal dopamineand the interface between motivation and cognitionFrontiers in Psychology 2 163
14 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Atkinson KM Koenka AC Sanchez CE Moshontz HCooper H (2014) Reporting standards for literaturesearches and report inclusion criteria making researchsyntheses more transparent and easy to replicate ResearchSynthesis Methods 6 87ndash95
Baer LH Tabri N Blair M Bye D Li KZH Pushkar D(2013) Longitudinal associations of need for cognitioncognitive activity and depressive symptomatology withcognitive function in recent retirees Journals of GerontologySeries B Psychological Sciences and Social Sciences 68 655ndash664
Barbey AK Colom R Solomon J Krueger F Forbes CGrafman J (2012) An integrative architecture for generalintelligence and executive function revealed by lesionmapping Brain 135 1154ndash1164
Barnett JH Salmond CH Jones PB Sahakian BJ (2006)Cognitive reserve in neuropsychiatry Psychological Medicine36 1053ndash1064
Beaujean AA Parker S Qiu X (2013) The relationshipbetween cognitive ability and depression a longitudinaldata analysis Social Psychiatry and Psychiatric Epidemiology48 1983ndash1992
Belsky DW Caspi A Arseneault L Bleidorn W Fonagy PGoodman M Houts R Moffitt TE (2012) Etiologicalfeatures of borderline personality related characteristics in abirth cohort of 12-year-old children Development andPsychopathology 24 251ndash265
Betts KS Williams GM Najman JM Alati R (2016)Predicting spectrums of adult mania psychosis anddepression by prospectively ascertained childhoodneurodevelopment Journal of Psychiatric Research 72 22ndash29
Bora E Harrison BJ Yuumlcel M Pantelis C (2013) Cognitiveimpairment in euthymic major depressive disorder a meta-analysis Psychological Medicine 43 2017ndash2026
Borenstein M Hedges LV Higgins JPT Rothstein HR(2011) Introduction to Meta-Analysis John Wiley amp SonsWest Sussex UK
Canals J Domegravenech-Llaberia E Fernaacutendez-Ballart J Martiacute-Henneberg C (2002) Predictors of depression at eighteenA 7-year follow-up study in a Spanish nonclinicalpopulation European Child amp Adolescent Psychiatry 11226ndash233
Christensen H Griffiths K Mackinnon A (1997) Aquantitative review of cognitive deficits in depression andAlzheimer-type dementia Selection of Studies 3 631ndash651
Connolly SL Wagner Ca Shapero BG Pendergast LLAbramson LY Alloy LB (2014) Rumination prospectivelypredicts executive functioning impairments in adolescentsJournal of Behavior Therapy and Experimental Psychiatry 4546ndash56
Cooper HM (1979) Statistically combining independentstudies a meta-analysis of sex differences in conformityresearch Journal of Personality and Social Psychology 37131ndash146
Cooper HM (2010) Research Synthesis and Meta-Analysis AStep-by-Step Approach 4th edn SAGE PublicationsWashington (DC) USA
Cuijpers P de Graaf R van Dorsselaer S (2004) Minordepression risk profiles functional disability health careuse and risk of developing major depression Journal ofAffective Disorders 79 71ndash79
Cuthbert BN Kozak MJ (2013) Constructing constructs forpsychopathology the NIMH research domain criteriaJournal of Abnormal Psychology 122 928ndash937
Der G Batty GD Deary IJ (2009) The association between IQin adolescence and a range of health outcomes at 40 in the1979 US National Longitudinal Study of Youth Intelligence37 573ndash580
Dubow EF Boxer P Huesmann LR (2008) Childhood andadolescent predictors of early and middle adulthoodalcohol use and problem drinking the Columbia CountyLongitudinal Study Addiction 103 36ndash47
Duval S Tweedie R (2000) Trim and fill a simple funnel-plot-based method of testing and adjusting for publicationbias in meta-analysis Biometrics 56 455ndash463
Evans LD Kouros CD Samanez-Larkin S Garber J (2015)Concurrent and short-term prospective relations amongneurocognitive functioning coping and depressivesymptoms in youth Journal of Clinical Child and AdolescentPsychology 53 1ndash15
Franz CE Lyons MJ OrsquoBrien R Panizzon MS Kim K BhatR Grant MD Toomey R Eisen S Xian H Kremen WS(2011) A 35-year longitudinal assessment of cognition andmidlife depression symptoms the Vietnam Era Twin Studyof Aging American Association for Geriatric PsychiatryAmerican Journal of Geriatric Psychiatry 19 559ndash570
Gale CR Batty GD Tynelius P Deary IJ Rasmussen F(2010) Intelligence in early adulthood and subsequenthospitalization for mental disorders Epidemiology 2170ndash77
Gale CR Deary IJ Boyle SH Barefoot J Mortensen LHBatty GD (2008) Cognitive ability in early adulthood andrisk of 5 specific psychiatric disorders in middle age theVietnam experience study Archives of General Psychiatry 651410ndash1418
Gale CR Hatch SL Batty GD Deary IJ (2009) Intelligence inchildhood and risk of psychological distress in adulthoodthe 1958 National Child Development Survey and the 1970British Cohort Study Intelligence 37 592ndash599
Gjerde PF (1995) Alternative pathways to chronicdepressive symptoms in young adults gender differencesin developmental trajectories Child Development 661277ndash1300
Gottfredson LS (1997) Mainstream science on intelligence aneditorial with 52 signatories history and bibliographyIntelligence 24 13ndash23
Guyer AE Choate VR Grimm KJ Pine DS Keenan K(2011) Emerging depression is associated with facememory deficits in adolescent girls Elsevier Inc Journal ofthe American Academy of Child and Adolescent Psychiatry 50180ndash190
Gyurak A Patenaude B Korgaonkar MS Grieve SMWilliams LM Etkin A (2015) Frontoparietal activationduring response inhibition predicts remission toantidepressants in patients with major depression BiologicalPsychiatry 79 1ndash8
Hagenaars SP Harris SE Davies G Hill WD LiewaldDCM Ritchie SJ Marioni RE Fawns-Ritchie C Cullen BMalik R METASTROKE Consortium IC for BPGSpiroMeta Consortium CHARGE ConsortiumPulmonary Group CCA and LG Worrall BB Sudlow
Association between cognitive function and subsequent depression 15
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
CLM Wardlaw JM Gallacher J Pell J McIntosh AMSmith DJ Gale CR Deary IJ (2016) Shared geneticaetiology between cognitive functions and physical andmental health in UK Biobank (N = 112 151) and 24 GWASconsortiaMolecular Psychiatry Published online 26 January2016 doi101038mp2015225
Hatch SL Jones PB Kuh D Hardy R Wadsworth MEJRichards M (2007) Childhood cognitive ability and adultmental health in the British 1946 birth cohort Social Scienceamp Medicine (1982) 64 2285ndash2296
Hipwell AE Sapotichne B Klostermann S Battista DKeenan K (2011) Autobiographical memory as a predictorof depression vulnerability in girls Journal of Clinical Childand Adolescent Psychology 40 254ndash265
Horowitz JL Garber J (2003) Relation of intelligence andreligiosity to depressive disorders in offspring of depressedand nondepressed mothers The American Academy ofChild and Adolescent Psychiatry Journal of the AmericanAcademy of Child and Adolescent Psychiatry 42 578ndash586
Johnson W Bouchard TJ Krueger RF McGue MGottesman II (2004) Just one g consistent results fromthree test batteries Intelligence 32 95ndash107
Keedwell PA Andrew C Williams SCR Brammer MJPhillips ML (2005) The neural correlates of anhedoniain major depressive disorder Biological Psychiatry 58843ndash853
Kessler RC Berglund P Demler O Jin R Koretz DMerikangas KR Rush AJ Walters EE Wang PS (2003)The epidemiology of major depressive disorder resultsfrom the National Comorbidity Survey Replication(NCS-R) Journal of the American Medical Association 2893095ndash3105
Koenen KC Moffitt TE Roberts AL Martin LT KubzanskyL Harrington H Poulton R Caspi A (2009) Childhood IQand adult mental disorders a test of the cognitive reservehypothesis American Journal of Psychiatry 166 50ndash57
Lewinsohn PM Solomon A Seeley JR Zeiss A (2000)Clinical implications of lsquosubthresholdrsquo depressivesymptoms Journal of Abnormal Psychology 109 345ndash351
Luppino FS de Wit LM Bouvy PF Stijnen T Cuijpers PPenninx BWJH Zitman FG (2010) Overweight obesityand depression a systematic review and meta-analysisof longitudinal studies Archives of General Psychiatry 67220ndash229
McCord J Ensminger ME (1997) Multiple risks andcomorbidity in an African-American population CriminalBehaviour and Mental Health 7 339ndash352
McDermott LM Ebmeier KP (2009) A meta-analysis ofdepression severity and cognitive function Elsevier BVJournal of Affective Disorders 119 1ndash8
Melartin TK Rytsaumllauml HJ Leskelauml US Lestelauml-Mielonen PSSokero TP Isometsauml ET (2002) Current comorbidity ofpsychiatric disorders among DSM-IV major depressivedisorder patients in psychiatric care in the VantaaDepression Study Journal of Clinical Psychiatry 63 126ndash134
Meyer SE Carlson GA Wiggs EA Martinez PE RonsavilleDS KlimesndashDougan B Gold PW RadkendashYarrow M(2004) A prospective study of the association amongimpaired executive functioning childhood attentional
problems and the development of bipolar disorderDevelopment and Psychopathology 16 461ndash476
MiyakeA FriedmanNP EmersonMJWitzki aHHowerter AWager TD (2000) The unity and diversity of executivefunctions and their contributions to complex lsquoFrontal Lobersquotasks a latentvariable analysisCognitive Psychology41 49ndash100
Moher D Liberati A (2009) Preferred reporting items forsystematic reviews and meta-analyses the PRISMAstatement Annals of Internal Medicine 151 264ndash269
Papmeyer M Sussmann JE Hall J McKirdy J Peel AMacdonald A Lawrie SM Whalley HC McIntosh AM(2015) Neurocognition in individuals at high familial riskof mood disorders with or without subsequent onset ofdepression Psychological Medicine 45 1ndash11
Peterson RA Brown SP (2005) On the use of betacoefficients in meta-analysis Journal of Applied Psychology90 175ndash181
Pine DS Cohen P Brook J Coplan JD (1997) Psychiatricsymptoms in adolescence as predictors of obesity in earlyadulthood a longitudinal study American Journal of PublicHealth 87 1303ndash1310
Quinn ME Joormann J (2015) Control when it countschange in executive control under stress predicts depressionsymptoms Emotion Junio 22 1ndash10
Rawal A Rice F (2012) Examining overgeneralautobiographical memory as a risk factor for adolescentdepression Elsevier Inc Journal of the American Academy ofChild and Adolescent Psychiatry 51 518ndash527
Ree MJ Earles JA (1991) The stability of g across differentmethods of estimation Intelligence 15 271ndash278
Rock PL Roiser JP Riedel WJ Blackwell AD (2014)Cognitive impairment in depression a systematic reviewand meta-analysis Psychological Medicine 44 2029ndash2040
Rogers MA Kasai K Koji M Fukuda R Iwanami ANakagome K Fukuda M Kato N (2004) Executive andprefrontal dysfunction in unipolar depression a review ofneuropsychological and imaging evidence NeuroscienceResearch 50 1ndash11
Scult MA Knodt AR Swartz JR Brigidi BD Hariri AR(2016) Thinking and feeling individual differences inhabitual emotion regulation and stress-related mood areassociated with prefrontal executive control ClinicalPsychological Science doi1011772167702616654688
Sharp C Petersen N Goodyer I (2008) Emotional reactivityand the emergence of conduct problems and emotionalsymptoms in 7- to 11-year-olds a 1-year follow-up studyJournal of the American Academy of Child and AdolescentPsychiatry 47 565ndash573
Siegel LS (1999) Issues in the definition and diagnosis oflearning disabilities a perspective on Guckenberger vBoston University Journal of Learning Disabilities 32 304ndash319
Simons CJP Jacobs N Derom C Thiery E Jolles J van Os JKrabbendam L (2009) Cognition as predictor of currentand follow-up depressive symptoms in the generalpopulation Acta Psychiatrica Scandinavica 120 45ndash52
Slykerman RF Thompson J Waldie K Murphy R Wall CMitchell EA (2015) Maternal stress during pregnancy isassociated with moderate to severe depression in 11-year-old children Acta Paediatrica 104 68ndash74
16 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Snyder HR (2013) Major depressive disorder is associatedwith broad impairments on neuropsychological measuresof executive function a meta-analysis and reviewPsychological Bulletin 139 81ndash132
Soslashrensen HJ Saeligbye D Urfer-Parnas A Mortensen ELParnas J (2012) Premorbid intelligence and educationallevel in bipolar and unipolar disorders a Danish draftboard study Journal of Affective Disorders 136 1188ndash1191
SpearmanC (1904) lsquoGeneral intelligencersquoobjectivelydeterminedandmeasuredAmerican Journal of Psychology 15 201
Stern Y (2003) The concept of cognitive reserve a catalyst forresearch Journal of Clinical and Experimental Neuropsychology(Neuropsychology Development and Cognition Section A) 25589ndash593
Stroup D Berlin J Morton S Olkin I Williamson GDRennie D Moher D Becker BJ Sipe TA Thacker SB(2000) Meta-analysis of Observational Studies inEpidemiology a proposal for reporting Journal of theAmerican Medical Association 283 2008
Vinberg M Miskowiak KW Kessing LV (2013) Impairmentof executive function and attention predicts onset ofaffective disorder in healthy high-risk twins Journal ofClinical Psychiatry 74 e747ndashe753
Zammit S Allebeck P David AS Dalman C HemmingssonT Lundberg I Lewis G (2004) A longitudinal study ofpremorbid IQ Score and risk of developing schizophreniabipolar disorder severe depression and other nonaffectivepsychoses Archives of General Psychiatry 61 354ndash360
Association between cognitive function and subsequent depression 17
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms

Fig 4 Trim-and-fill funnel plots for all samples Fisherrsquos Z a measure of effect size is plotted on the x-axis and the standarderror is plotted on the y-axis Larger studies appear toward the top of the graph and smaller studies towards the bottom Inthe absence of publication bias the studies are symmetrically distributed around the mean Actual studies are shown in opencircles and imputed studies would be shown in black circles No additional studies would be expected in the oppositedirection (to the right) of the observed effect but an additional 11 studies are imputed to the left of the mean effect sizeWhile the calculated effect size is minus0088 [95 confidence interval (CI) minus0121 to minus0054] using Duval amp Tweediersquos trim-and-fill method the imputed effect size estimate is larger at minus0137 (95 CI minus0176 to minus0099 imputed studies n = 11)
Fig 3 Meta-analysis comparing values adjusted for baseline depression symptoms v unadjusted A forest plot for analysiscomparing results from a subset of the same set of studies reported in Fig 2 when using unadjusted values compared tousing values that are adjusted for baseline depression Effects are significant for unadjusted values [r =minus0120 95 confidenceinterval (CI) minus0169 to minus0070 p lt 0001] but not for adjusted values (r =minus0032 95 CI minus0078 to 0014 p = 0169) Results arereported as correlation coefficients denoted by squares and 95 CIs indicated by lines Meta-analysis results are displayed asdiamonds
Association between cognitive function and subsequent depression 13
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Third the associations between cognitive functionand either current or later depression were not moder-ated by data quality or participant age sex and raceHowever there are a number of additional potentialmoderators that could not be addressed in the currentreview and meta-analysis For example the numberand type of comorbid conditions with depressionwere often not reported in the included studies butcould represent an important moderator of theobserved effects Modeling the effects of comorbid ill-ness is an important avenue for future research
One limitation of the current literature is that only ahandful of studies reviewed explicitly excluded for de-pression diagnosis at baseline (Gale et al 2008 Vinberget al 2013 Papmeyer et al 2015) however consistentwith the finding that controlling for baseline depres-sion symptoms led to a null association between cogni-tion and subsequent depression there was no effectobserved when including these studies in the sub-group analyses further suggesting that the associationbetween cognitive function and depression is likelycontemporaneous It will be important to follow-upthese analyses with individual studies that includerigorous assessment of baseline depression symptomsand other potentially confounding factors to furtherclarify this relationship
An open question that remains for future research iswhether deficits in cognitive function are likely to pre-dict the development of more sever or recurrent de-pression later in life Only one of the included studies(Koenen et al 2009) specifically investigated recurrentdepression and found that lower IQ was associatedwith greater persistence of disorder
A final consideration is that while our review andmeta-analysis focused on general cognitive functionmainly assessed via IQ there may be specific subtypesof cognitive function that are more predictive of laterdepression For example a lack of cognitive flexibilitymay more closely match with the ruminative stylecharacteristic of depression and therefore tasks specifi-cally measuring this component of cognitive functionmight have some predictive utility While our reviewdid not find differences between broad and specificmeasures of cognitive function there were not enoughstudies identified to allow for precise consideration ofdifferences between individual cognitive domains
A limitation of the meta-analysis is that while thepresent study followed standard guidelines (Stroupet al 2000 Atkinson et al 2014) decisions aboutstudy selection data extraction and quality assess-ment include a number of decision points that neces-sarily involve a level of subjectivity Reliability wasascertained by using independent raters however dif-ferent inclusionexclusion criteria or a different ap-proach to the evaluation of those criteria could result
in a different set of studies being includedUltimately the quality of the meta-analysis is depend-ent upon the underlying studies that are analyzedFurthermore although studies with insufficient infor-mation to be included in the meta-analysis were notfound to differ based on basic study data from thosestudies included in the meta-analysis nonetheless itis unknown how if at all data from these studiescould change the overall results
Acknowledging these limitations our present reviewand meta-analysis found that while an association is evi-dent between cognitive function and later depressiongeneral cognitive function does not appear to be a riskfactor for depression but rather is more likely relatedto performance decrements associated with concurrentdepressive symptoms Our results suggest that low cog-nitive function is therefore probably not a causal factorof depression and that clinical practice may benefitmore from a focus on how decreased cognitive functionin the depressed state is likely to influence treatment out-comes (Gyurak et al 2015) Our findings have importantimplications for better understanding depression and forthe design of future studies in highlighting the need tocontrol for subthreshold depression symptoms when in-vestigating risk factors for mental illness as well as whenassessing cognitive function more generally
Supplementary material
The supplementary material for this article can befound at httpdxdoiorg101017S0033291716002075
Acknowledgements
MAS is supported by an National Science Foundation(NSF) Graduate Research Fellowship ARH is sup-ported by National Institutes of Health (NIH) grantsRO1DA033369 amp R01AG049789 TEM is supportedby National Institutes of Health (NIH) grantsR01AG049789 We would like to thank HarrisCooper PhD at Duke University who provided invalu-able insight into conducting the meta-analysis Wethank all of the authors of studies who provided add-itional information for this meta-analysis
Declaration of Interest
None
References
Aarts E van Holstein M Cools R (2011) Striatal dopamineand the interface between motivation and cognitionFrontiers in Psychology 2 163
14 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Atkinson KM Koenka AC Sanchez CE Moshontz HCooper H (2014) Reporting standards for literaturesearches and report inclusion criteria making researchsyntheses more transparent and easy to replicate ResearchSynthesis Methods 6 87ndash95
Baer LH Tabri N Blair M Bye D Li KZH Pushkar D(2013) Longitudinal associations of need for cognitioncognitive activity and depressive symptomatology withcognitive function in recent retirees Journals of GerontologySeries B Psychological Sciences and Social Sciences 68 655ndash664
Barbey AK Colom R Solomon J Krueger F Forbes CGrafman J (2012) An integrative architecture for generalintelligence and executive function revealed by lesionmapping Brain 135 1154ndash1164
Barnett JH Salmond CH Jones PB Sahakian BJ (2006)Cognitive reserve in neuropsychiatry Psychological Medicine36 1053ndash1064
Beaujean AA Parker S Qiu X (2013) The relationshipbetween cognitive ability and depression a longitudinaldata analysis Social Psychiatry and Psychiatric Epidemiology48 1983ndash1992
Belsky DW Caspi A Arseneault L Bleidorn W Fonagy PGoodman M Houts R Moffitt TE (2012) Etiologicalfeatures of borderline personality related characteristics in abirth cohort of 12-year-old children Development andPsychopathology 24 251ndash265
Betts KS Williams GM Najman JM Alati R (2016)Predicting spectrums of adult mania psychosis anddepression by prospectively ascertained childhoodneurodevelopment Journal of Psychiatric Research 72 22ndash29
Bora E Harrison BJ Yuumlcel M Pantelis C (2013) Cognitiveimpairment in euthymic major depressive disorder a meta-analysis Psychological Medicine 43 2017ndash2026
Borenstein M Hedges LV Higgins JPT Rothstein HR(2011) Introduction to Meta-Analysis John Wiley amp SonsWest Sussex UK
Canals J Domegravenech-Llaberia E Fernaacutendez-Ballart J Martiacute-Henneberg C (2002) Predictors of depression at eighteenA 7-year follow-up study in a Spanish nonclinicalpopulation European Child amp Adolescent Psychiatry 11226ndash233
Christensen H Griffiths K Mackinnon A (1997) Aquantitative review of cognitive deficits in depression andAlzheimer-type dementia Selection of Studies 3 631ndash651
Connolly SL Wagner Ca Shapero BG Pendergast LLAbramson LY Alloy LB (2014) Rumination prospectivelypredicts executive functioning impairments in adolescentsJournal of Behavior Therapy and Experimental Psychiatry 4546ndash56
Cooper HM (1979) Statistically combining independentstudies a meta-analysis of sex differences in conformityresearch Journal of Personality and Social Psychology 37131ndash146
Cooper HM (2010) Research Synthesis and Meta-Analysis AStep-by-Step Approach 4th edn SAGE PublicationsWashington (DC) USA
Cuijpers P de Graaf R van Dorsselaer S (2004) Minordepression risk profiles functional disability health careuse and risk of developing major depression Journal ofAffective Disorders 79 71ndash79
Cuthbert BN Kozak MJ (2013) Constructing constructs forpsychopathology the NIMH research domain criteriaJournal of Abnormal Psychology 122 928ndash937
Der G Batty GD Deary IJ (2009) The association between IQin adolescence and a range of health outcomes at 40 in the1979 US National Longitudinal Study of Youth Intelligence37 573ndash580
Dubow EF Boxer P Huesmann LR (2008) Childhood andadolescent predictors of early and middle adulthoodalcohol use and problem drinking the Columbia CountyLongitudinal Study Addiction 103 36ndash47
Duval S Tweedie R (2000) Trim and fill a simple funnel-plot-based method of testing and adjusting for publicationbias in meta-analysis Biometrics 56 455ndash463
Evans LD Kouros CD Samanez-Larkin S Garber J (2015)Concurrent and short-term prospective relations amongneurocognitive functioning coping and depressivesymptoms in youth Journal of Clinical Child and AdolescentPsychology 53 1ndash15
Franz CE Lyons MJ OrsquoBrien R Panizzon MS Kim K BhatR Grant MD Toomey R Eisen S Xian H Kremen WS(2011) A 35-year longitudinal assessment of cognition andmidlife depression symptoms the Vietnam Era Twin Studyof Aging American Association for Geriatric PsychiatryAmerican Journal of Geriatric Psychiatry 19 559ndash570
Gale CR Batty GD Tynelius P Deary IJ Rasmussen F(2010) Intelligence in early adulthood and subsequenthospitalization for mental disorders Epidemiology 2170ndash77
Gale CR Deary IJ Boyle SH Barefoot J Mortensen LHBatty GD (2008) Cognitive ability in early adulthood andrisk of 5 specific psychiatric disorders in middle age theVietnam experience study Archives of General Psychiatry 651410ndash1418
Gale CR Hatch SL Batty GD Deary IJ (2009) Intelligence inchildhood and risk of psychological distress in adulthoodthe 1958 National Child Development Survey and the 1970British Cohort Study Intelligence 37 592ndash599
Gjerde PF (1995) Alternative pathways to chronicdepressive symptoms in young adults gender differencesin developmental trajectories Child Development 661277ndash1300
Gottfredson LS (1997) Mainstream science on intelligence aneditorial with 52 signatories history and bibliographyIntelligence 24 13ndash23
Guyer AE Choate VR Grimm KJ Pine DS Keenan K(2011) Emerging depression is associated with facememory deficits in adolescent girls Elsevier Inc Journal ofthe American Academy of Child and Adolescent Psychiatry 50180ndash190
Gyurak A Patenaude B Korgaonkar MS Grieve SMWilliams LM Etkin A (2015) Frontoparietal activationduring response inhibition predicts remission toantidepressants in patients with major depression BiologicalPsychiatry 79 1ndash8
Hagenaars SP Harris SE Davies G Hill WD LiewaldDCM Ritchie SJ Marioni RE Fawns-Ritchie C Cullen BMalik R METASTROKE Consortium IC for BPGSpiroMeta Consortium CHARGE ConsortiumPulmonary Group CCA and LG Worrall BB Sudlow
Association between cognitive function and subsequent depression 15
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
CLM Wardlaw JM Gallacher J Pell J McIntosh AMSmith DJ Gale CR Deary IJ (2016) Shared geneticaetiology between cognitive functions and physical andmental health in UK Biobank (N = 112 151) and 24 GWASconsortiaMolecular Psychiatry Published online 26 January2016 doi101038mp2015225
Hatch SL Jones PB Kuh D Hardy R Wadsworth MEJRichards M (2007) Childhood cognitive ability and adultmental health in the British 1946 birth cohort Social Scienceamp Medicine (1982) 64 2285ndash2296
Hipwell AE Sapotichne B Klostermann S Battista DKeenan K (2011) Autobiographical memory as a predictorof depression vulnerability in girls Journal of Clinical Childand Adolescent Psychology 40 254ndash265
Horowitz JL Garber J (2003) Relation of intelligence andreligiosity to depressive disorders in offspring of depressedand nondepressed mothers The American Academy ofChild and Adolescent Psychiatry Journal of the AmericanAcademy of Child and Adolescent Psychiatry 42 578ndash586
Johnson W Bouchard TJ Krueger RF McGue MGottesman II (2004) Just one g consistent results fromthree test batteries Intelligence 32 95ndash107
Keedwell PA Andrew C Williams SCR Brammer MJPhillips ML (2005) The neural correlates of anhedoniain major depressive disorder Biological Psychiatry 58843ndash853
Kessler RC Berglund P Demler O Jin R Koretz DMerikangas KR Rush AJ Walters EE Wang PS (2003)The epidemiology of major depressive disorder resultsfrom the National Comorbidity Survey Replication(NCS-R) Journal of the American Medical Association 2893095ndash3105
Koenen KC Moffitt TE Roberts AL Martin LT KubzanskyL Harrington H Poulton R Caspi A (2009) Childhood IQand adult mental disorders a test of the cognitive reservehypothesis American Journal of Psychiatry 166 50ndash57
Lewinsohn PM Solomon A Seeley JR Zeiss A (2000)Clinical implications of lsquosubthresholdrsquo depressivesymptoms Journal of Abnormal Psychology 109 345ndash351
Luppino FS de Wit LM Bouvy PF Stijnen T Cuijpers PPenninx BWJH Zitman FG (2010) Overweight obesityand depression a systematic review and meta-analysisof longitudinal studies Archives of General Psychiatry 67220ndash229
McCord J Ensminger ME (1997) Multiple risks andcomorbidity in an African-American population CriminalBehaviour and Mental Health 7 339ndash352
McDermott LM Ebmeier KP (2009) A meta-analysis ofdepression severity and cognitive function Elsevier BVJournal of Affective Disorders 119 1ndash8
Melartin TK Rytsaumllauml HJ Leskelauml US Lestelauml-Mielonen PSSokero TP Isometsauml ET (2002) Current comorbidity ofpsychiatric disorders among DSM-IV major depressivedisorder patients in psychiatric care in the VantaaDepression Study Journal of Clinical Psychiatry 63 126ndash134
Meyer SE Carlson GA Wiggs EA Martinez PE RonsavilleDS KlimesndashDougan B Gold PW RadkendashYarrow M(2004) A prospective study of the association amongimpaired executive functioning childhood attentional
problems and the development of bipolar disorderDevelopment and Psychopathology 16 461ndash476
MiyakeA FriedmanNP EmersonMJWitzki aHHowerter AWager TD (2000) The unity and diversity of executivefunctions and their contributions to complex lsquoFrontal Lobersquotasks a latentvariable analysisCognitive Psychology41 49ndash100
Moher D Liberati A (2009) Preferred reporting items forsystematic reviews and meta-analyses the PRISMAstatement Annals of Internal Medicine 151 264ndash269
Papmeyer M Sussmann JE Hall J McKirdy J Peel AMacdonald A Lawrie SM Whalley HC McIntosh AM(2015) Neurocognition in individuals at high familial riskof mood disorders with or without subsequent onset ofdepression Psychological Medicine 45 1ndash11
Peterson RA Brown SP (2005) On the use of betacoefficients in meta-analysis Journal of Applied Psychology90 175ndash181
Pine DS Cohen P Brook J Coplan JD (1997) Psychiatricsymptoms in adolescence as predictors of obesity in earlyadulthood a longitudinal study American Journal of PublicHealth 87 1303ndash1310
Quinn ME Joormann J (2015) Control when it countschange in executive control under stress predicts depressionsymptoms Emotion Junio 22 1ndash10
Rawal A Rice F (2012) Examining overgeneralautobiographical memory as a risk factor for adolescentdepression Elsevier Inc Journal of the American Academy ofChild and Adolescent Psychiatry 51 518ndash527
Ree MJ Earles JA (1991) The stability of g across differentmethods of estimation Intelligence 15 271ndash278
Rock PL Roiser JP Riedel WJ Blackwell AD (2014)Cognitive impairment in depression a systematic reviewand meta-analysis Psychological Medicine 44 2029ndash2040
Rogers MA Kasai K Koji M Fukuda R Iwanami ANakagome K Fukuda M Kato N (2004) Executive andprefrontal dysfunction in unipolar depression a review ofneuropsychological and imaging evidence NeuroscienceResearch 50 1ndash11
Scult MA Knodt AR Swartz JR Brigidi BD Hariri AR(2016) Thinking and feeling individual differences inhabitual emotion regulation and stress-related mood areassociated with prefrontal executive control ClinicalPsychological Science doi1011772167702616654688
Sharp C Petersen N Goodyer I (2008) Emotional reactivityand the emergence of conduct problems and emotionalsymptoms in 7- to 11-year-olds a 1-year follow-up studyJournal of the American Academy of Child and AdolescentPsychiatry 47 565ndash573
Siegel LS (1999) Issues in the definition and diagnosis oflearning disabilities a perspective on Guckenberger vBoston University Journal of Learning Disabilities 32 304ndash319
Simons CJP Jacobs N Derom C Thiery E Jolles J van Os JKrabbendam L (2009) Cognition as predictor of currentand follow-up depressive symptoms in the generalpopulation Acta Psychiatrica Scandinavica 120 45ndash52
Slykerman RF Thompson J Waldie K Murphy R Wall CMitchell EA (2015) Maternal stress during pregnancy isassociated with moderate to severe depression in 11-year-old children Acta Paediatrica 104 68ndash74
16 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Snyder HR (2013) Major depressive disorder is associatedwith broad impairments on neuropsychological measuresof executive function a meta-analysis and reviewPsychological Bulletin 139 81ndash132
Soslashrensen HJ Saeligbye D Urfer-Parnas A Mortensen ELParnas J (2012) Premorbid intelligence and educationallevel in bipolar and unipolar disorders a Danish draftboard study Journal of Affective Disorders 136 1188ndash1191
SpearmanC (1904) lsquoGeneral intelligencersquoobjectivelydeterminedandmeasuredAmerican Journal of Psychology 15 201
Stern Y (2003) The concept of cognitive reserve a catalyst forresearch Journal of Clinical and Experimental Neuropsychology(Neuropsychology Development and Cognition Section A) 25589ndash593
Stroup D Berlin J Morton S Olkin I Williamson GDRennie D Moher D Becker BJ Sipe TA Thacker SB(2000) Meta-analysis of Observational Studies inEpidemiology a proposal for reporting Journal of theAmerican Medical Association 283 2008
Vinberg M Miskowiak KW Kessing LV (2013) Impairmentof executive function and attention predicts onset ofaffective disorder in healthy high-risk twins Journal ofClinical Psychiatry 74 e747ndashe753
Zammit S Allebeck P David AS Dalman C HemmingssonT Lundberg I Lewis G (2004) A longitudinal study ofpremorbid IQ Score and risk of developing schizophreniabipolar disorder severe depression and other nonaffectivepsychoses Archives of General Psychiatry 61 354ndash360
Association between cognitive function and subsequent depression 17
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms

Third the associations between cognitive functionand either current or later depression were not moder-ated by data quality or participant age sex and raceHowever there are a number of additional potentialmoderators that could not be addressed in the currentreview and meta-analysis For example the numberand type of comorbid conditions with depressionwere often not reported in the included studies butcould represent an important moderator of theobserved effects Modeling the effects of comorbid ill-ness is an important avenue for future research
One limitation of the current literature is that only ahandful of studies reviewed explicitly excluded for de-pression diagnosis at baseline (Gale et al 2008 Vinberget al 2013 Papmeyer et al 2015) however consistentwith the finding that controlling for baseline depres-sion symptoms led to a null association between cogni-tion and subsequent depression there was no effectobserved when including these studies in the sub-group analyses further suggesting that the associationbetween cognitive function and depression is likelycontemporaneous It will be important to follow-upthese analyses with individual studies that includerigorous assessment of baseline depression symptomsand other potentially confounding factors to furtherclarify this relationship
An open question that remains for future research iswhether deficits in cognitive function are likely to pre-dict the development of more sever or recurrent de-pression later in life Only one of the included studies(Koenen et al 2009) specifically investigated recurrentdepression and found that lower IQ was associatedwith greater persistence of disorder
A final consideration is that while our review andmeta-analysis focused on general cognitive functionmainly assessed via IQ there may be specific subtypesof cognitive function that are more predictive of laterdepression For example a lack of cognitive flexibilitymay more closely match with the ruminative stylecharacteristic of depression and therefore tasks specifi-cally measuring this component of cognitive functionmight have some predictive utility While our reviewdid not find differences between broad and specificmeasures of cognitive function there were not enoughstudies identified to allow for precise consideration ofdifferences between individual cognitive domains
A limitation of the meta-analysis is that while thepresent study followed standard guidelines (Stroupet al 2000 Atkinson et al 2014) decisions aboutstudy selection data extraction and quality assess-ment include a number of decision points that neces-sarily involve a level of subjectivity Reliability wasascertained by using independent raters however dif-ferent inclusionexclusion criteria or a different ap-proach to the evaluation of those criteria could result
in a different set of studies being includedUltimately the quality of the meta-analysis is depend-ent upon the underlying studies that are analyzedFurthermore although studies with insufficient infor-mation to be included in the meta-analysis were notfound to differ based on basic study data from thosestudies included in the meta-analysis nonetheless itis unknown how if at all data from these studiescould change the overall results
Acknowledging these limitations our present reviewand meta-analysis found that while an association is evi-dent between cognitive function and later depressiongeneral cognitive function does not appear to be a riskfactor for depression but rather is more likely relatedto performance decrements associated with concurrentdepressive symptoms Our results suggest that low cog-nitive function is therefore probably not a causal factorof depression and that clinical practice may benefitmore from a focus on how decreased cognitive functionin the depressed state is likely to influence treatment out-comes (Gyurak et al 2015) Our findings have importantimplications for better understanding depression and forthe design of future studies in highlighting the need tocontrol for subthreshold depression symptoms when in-vestigating risk factors for mental illness as well as whenassessing cognitive function more generally
Supplementary material
The supplementary material for this article can befound at httpdxdoiorg101017S0033291716002075
Acknowledgements
MAS is supported by an National Science Foundation(NSF) Graduate Research Fellowship ARH is sup-ported by National Institutes of Health (NIH) grantsRO1DA033369 amp R01AG049789 TEM is supportedby National Institutes of Health (NIH) grantsR01AG049789 We would like to thank HarrisCooper PhD at Duke University who provided invalu-able insight into conducting the meta-analysis Wethank all of the authors of studies who provided add-itional information for this meta-analysis
Declaration of Interest
None
References
Aarts E van Holstein M Cools R (2011) Striatal dopamineand the interface between motivation and cognitionFrontiers in Psychology 2 163
14 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Atkinson KM Koenka AC Sanchez CE Moshontz HCooper H (2014) Reporting standards for literaturesearches and report inclusion criteria making researchsyntheses more transparent and easy to replicate ResearchSynthesis Methods 6 87ndash95
Baer LH Tabri N Blair M Bye D Li KZH Pushkar D(2013) Longitudinal associations of need for cognitioncognitive activity and depressive symptomatology withcognitive function in recent retirees Journals of GerontologySeries B Psychological Sciences and Social Sciences 68 655ndash664
Barbey AK Colom R Solomon J Krueger F Forbes CGrafman J (2012) An integrative architecture for generalintelligence and executive function revealed by lesionmapping Brain 135 1154ndash1164
Barnett JH Salmond CH Jones PB Sahakian BJ (2006)Cognitive reserve in neuropsychiatry Psychological Medicine36 1053ndash1064
Beaujean AA Parker S Qiu X (2013) The relationshipbetween cognitive ability and depression a longitudinaldata analysis Social Psychiatry and Psychiatric Epidemiology48 1983ndash1992
Belsky DW Caspi A Arseneault L Bleidorn W Fonagy PGoodman M Houts R Moffitt TE (2012) Etiologicalfeatures of borderline personality related characteristics in abirth cohort of 12-year-old children Development andPsychopathology 24 251ndash265
Betts KS Williams GM Najman JM Alati R (2016)Predicting spectrums of adult mania psychosis anddepression by prospectively ascertained childhoodneurodevelopment Journal of Psychiatric Research 72 22ndash29
Bora E Harrison BJ Yuumlcel M Pantelis C (2013) Cognitiveimpairment in euthymic major depressive disorder a meta-analysis Psychological Medicine 43 2017ndash2026
Borenstein M Hedges LV Higgins JPT Rothstein HR(2011) Introduction to Meta-Analysis John Wiley amp SonsWest Sussex UK
Canals J Domegravenech-Llaberia E Fernaacutendez-Ballart J Martiacute-Henneberg C (2002) Predictors of depression at eighteenA 7-year follow-up study in a Spanish nonclinicalpopulation European Child amp Adolescent Psychiatry 11226ndash233
Christensen H Griffiths K Mackinnon A (1997) Aquantitative review of cognitive deficits in depression andAlzheimer-type dementia Selection of Studies 3 631ndash651
Connolly SL Wagner Ca Shapero BG Pendergast LLAbramson LY Alloy LB (2014) Rumination prospectivelypredicts executive functioning impairments in adolescentsJournal of Behavior Therapy and Experimental Psychiatry 4546ndash56
Cooper HM (1979) Statistically combining independentstudies a meta-analysis of sex differences in conformityresearch Journal of Personality and Social Psychology 37131ndash146
Cooper HM (2010) Research Synthesis and Meta-Analysis AStep-by-Step Approach 4th edn SAGE PublicationsWashington (DC) USA
Cuijpers P de Graaf R van Dorsselaer S (2004) Minordepression risk profiles functional disability health careuse and risk of developing major depression Journal ofAffective Disorders 79 71ndash79
Cuthbert BN Kozak MJ (2013) Constructing constructs forpsychopathology the NIMH research domain criteriaJournal of Abnormal Psychology 122 928ndash937
Der G Batty GD Deary IJ (2009) The association between IQin adolescence and a range of health outcomes at 40 in the1979 US National Longitudinal Study of Youth Intelligence37 573ndash580
Dubow EF Boxer P Huesmann LR (2008) Childhood andadolescent predictors of early and middle adulthoodalcohol use and problem drinking the Columbia CountyLongitudinal Study Addiction 103 36ndash47
Duval S Tweedie R (2000) Trim and fill a simple funnel-plot-based method of testing and adjusting for publicationbias in meta-analysis Biometrics 56 455ndash463
Evans LD Kouros CD Samanez-Larkin S Garber J (2015)Concurrent and short-term prospective relations amongneurocognitive functioning coping and depressivesymptoms in youth Journal of Clinical Child and AdolescentPsychology 53 1ndash15
Franz CE Lyons MJ OrsquoBrien R Panizzon MS Kim K BhatR Grant MD Toomey R Eisen S Xian H Kremen WS(2011) A 35-year longitudinal assessment of cognition andmidlife depression symptoms the Vietnam Era Twin Studyof Aging American Association for Geriatric PsychiatryAmerican Journal of Geriatric Psychiatry 19 559ndash570
Gale CR Batty GD Tynelius P Deary IJ Rasmussen F(2010) Intelligence in early adulthood and subsequenthospitalization for mental disorders Epidemiology 2170ndash77
Gale CR Deary IJ Boyle SH Barefoot J Mortensen LHBatty GD (2008) Cognitive ability in early adulthood andrisk of 5 specific psychiatric disorders in middle age theVietnam experience study Archives of General Psychiatry 651410ndash1418
Gale CR Hatch SL Batty GD Deary IJ (2009) Intelligence inchildhood and risk of psychological distress in adulthoodthe 1958 National Child Development Survey and the 1970British Cohort Study Intelligence 37 592ndash599
Gjerde PF (1995) Alternative pathways to chronicdepressive symptoms in young adults gender differencesin developmental trajectories Child Development 661277ndash1300
Gottfredson LS (1997) Mainstream science on intelligence aneditorial with 52 signatories history and bibliographyIntelligence 24 13ndash23
Guyer AE Choate VR Grimm KJ Pine DS Keenan K(2011) Emerging depression is associated with facememory deficits in adolescent girls Elsevier Inc Journal ofthe American Academy of Child and Adolescent Psychiatry 50180ndash190
Gyurak A Patenaude B Korgaonkar MS Grieve SMWilliams LM Etkin A (2015) Frontoparietal activationduring response inhibition predicts remission toantidepressants in patients with major depression BiologicalPsychiatry 79 1ndash8
Hagenaars SP Harris SE Davies G Hill WD LiewaldDCM Ritchie SJ Marioni RE Fawns-Ritchie C Cullen BMalik R METASTROKE Consortium IC for BPGSpiroMeta Consortium CHARGE ConsortiumPulmonary Group CCA and LG Worrall BB Sudlow
Association between cognitive function and subsequent depression 15
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
CLM Wardlaw JM Gallacher J Pell J McIntosh AMSmith DJ Gale CR Deary IJ (2016) Shared geneticaetiology between cognitive functions and physical andmental health in UK Biobank (N = 112 151) and 24 GWASconsortiaMolecular Psychiatry Published online 26 January2016 doi101038mp2015225
Hatch SL Jones PB Kuh D Hardy R Wadsworth MEJRichards M (2007) Childhood cognitive ability and adultmental health in the British 1946 birth cohort Social Scienceamp Medicine (1982) 64 2285ndash2296
Hipwell AE Sapotichne B Klostermann S Battista DKeenan K (2011) Autobiographical memory as a predictorof depression vulnerability in girls Journal of Clinical Childand Adolescent Psychology 40 254ndash265
Horowitz JL Garber J (2003) Relation of intelligence andreligiosity to depressive disorders in offspring of depressedand nondepressed mothers The American Academy ofChild and Adolescent Psychiatry Journal of the AmericanAcademy of Child and Adolescent Psychiatry 42 578ndash586
Johnson W Bouchard TJ Krueger RF McGue MGottesman II (2004) Just one g consistent results fromthree test batteries Intelligence 32 95ndash107
Keedwell PA Andrew C Williams SCR Brammer MJPhillips ML (2005) The neural correlates of anhedoniain major depressive disorder Biological Psychiatry 58843ndash853
Kessler RC Berglund P Demler O Jin R Koretz DMerikangas KR Rush AJ Walters EE Wang PS (2003)The epidemiology of major depressive disorder resultsfrom the National Comorbidity Survey Replication(NCS-R) Journal of the American Medical Association 2893095ndash3105
Koenen KC Moffitt TE Roberts AL Martin LT KubzanskyL Harrington H Poulton R Caspi A (2009) Childhood IQand adult mental disorders a test of the cognitive reservehypothesis American Journal of Psychiatry 166 50ndash57
Lewinsohn PM Solomon A Seeley JR Zeiss A (2000)Clinical implications of lsquosubthresholdrsquo depressivesymptoms Journal of Abnormal Psychology 109 345ndash351
Luppino FS de Wit LM Bouvy PF Stijnen T Cuijpers PPenninx BWJH Zitman FG (2010) Overweight obesityand depression a systematic review and meta-analysisof longitudinal studies Archives of General Psychiatry 67220ndash229
McCord J Ensminger ME (1997) Multiple risks andcomorbidity in an African-American population CriminalBehaviour and Mental Health 7 339ndash352
McDermott LM Ebmeier KP (2009) A meta-analysis ofdepression severity and cognitive function Elsevier BVJournal of Affective Disorders 119 1ndash8
Melartin TK Rytsaumllauml HJ Leskelauml US Lestelauml-Mielonen PSSokero TP Isometsauml ET (2002) Current comorbidity ofpsychiatric disorders among DSM-IV major depressivedisorder patients in psychiatric care in the VantaaDepression Study Journal of Clinical Psychiatry 63 126ndash134
Meyer SE Carlson GA Wiggs EA Martinez PE RonsavilleDS KlimesndashDougan B Gold PW RadkendashYarrow M(2004) A prospective study of the association amongimpaired executive functioning childhood attentional
problems and the development of bipolar disorderDevelopment and Psychopathology 16 461ndash476
MiyakeA FriedmanNP EmersonMJWitzki aHHowerter AWager TD (2000) The unity and diversity of executivefunctions and their contributions to complex lsquoFrontal Lobersquotasks a latentvariable analysisCognitive Psychology41 49ndash100
Moher D Liberati A (2009) Preferred reporting items forsystematic reviews and meta-analyses the PRISMAstatement Annals of Internal Medicine 151 264ndash269
Papmeyer M Sussmann JE Hall J McKirdy J Peel AMacdonald A Lawrie SM Whalley HC McIntosh AM(2015) Neurocognition in individuals at high familial riskof mood disorders with or without subsequent onset ofdepression Psychological Medicine 45 1ndash11
Peterson RA Brown SP (2005) On the use of betacoefficients in meta-analysis Journal of Applied Psychology90 175ndash181
Pine DS Cohen P Brook J Coplan JD (1997) Psychiatricsymptoms in adolescence as predictors of obesity in earlyadulthood a longitudinal study American Journal of PublicHealth 87 1303ndash1310
Quinn ME Joormann J (2015) Control when it countschange in executive control under stress predicts depressionsymptoms Emotion Junio 22 1ndash10
Rawal A Rice F (2012) Examining overgeneralautobiographical memory as a risk factor for adolescentdepression Elsevier Inc Journal of the American Academy ofChild and Adolescent Psychiatry 51 518ndash527
Ree MJ Earles JA (1991) The stability of g across differentmethods of estimation Intelligence 15 271ndash278
Rock PL Roiser JP Riedel WJ Blackwell AD (2014)Cognitive impairment in depression a systematic reviewand meta-analysis Psychological Medicine 44 2029ndash2040
Rogers MA Kasai K Koji M Fukuda R Iwanami ANakagome K Fukuda M Kato N (2004) Executive andprefrontal dysfunction in unipolar depression a review ofneuropsychological and imaging evidence NeuroscienceResearch 50 1ndash11
Scult MA Knodt AR Swartz JR Brigidi BD Hariri AR(2016) Thinking and feeling individual differences inhabitual emotion regulation and stress-related mood areassociated with prefrontal executive control ClinicalPsychological Science doi1011772167702616654688
Sharp C Petersen N Goodyer I (2008) Emotional reactivityand the emergence of conduct problems and emotionalsymptoms in 7- to 11-year-olds a 1-year follow-up studyJournal of the American Academy of Child and AdolescentPsychiatry 47 565ndash573
Siegel LS (1999) Issues in the definition and diagnosis oflearning disabilities a perspective on Guckenberger vBoston University Journal of Learning Disabilities 32 304ndash319
Simons CJP Jacobs N Derom C Thiery E Jolles J van Os JKrabbendam L (2009) Cognition as predictor of currentand follow-up depressive symptoms in the generalpopulation Acta Psychiatrica Scandinavica 120 45ndash52
Slykerman RF Thompson J Waldie K Murphy R Wall CMitchell EA (2015) Maternal stress during pregnancy isassociated with moderate to severe depression in 11-year-old children Acta Paediatrica 104 68ndash74
16 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Snyder HR (2013) Major depressive disorder is associatedwith broad impairments on neuropsychological measuresof executive function a meta-analysis and reviewPsychological Bulletin 139 81ndash132
Soslashrensen HJ Saeligbye D Urfer-Parnas A Mortensen ELParnas J (2012) Premorbid intelligence and educationallevel in bipolar and unipolar disorders a Danish draftboard study Journal of Affective Disorders 136 1188ndash1191
SpearmanC (1904) lsquoGeneral intelligencersquoobjectivelydeterminedandmeasuredAmerican Journal of Psychology 15 201
Stern Y (2003) The concept of cognitive reserve a catalyst forresearch Journal of Clinical and Experimental Neuropsychology(Neuropsychology Development and Cognition Section A) 25589ndash593
Stroup D Berlin J Morton S Olkin I Williamson GDRennie D Moher D Becker BJ Sipe TA Thacker SB(2000) Meta-analysis of Observational Studies inEpidemiology a proposal for reporting Journal of theAmerican Medical Association 283 2008
Vinberg M Miskowiak KW Kessing LV (2013) Impairmentof executive function and attention predicts onset ofaffective disorder in healthy high-risk twins Journal ofClinical Psychiatry 74 e747ndashe753
Zammit S Allebeck P David AS Dalman C HemmingssonT Lundberg I Lewis G (2004) A longitudinal study ofpremorbid IQ Score and risk of developing schizophreniabipolar disorder severe depression and other nonaffectivepsychoses Archives of General Psychiatry 61 354ndash360
Association between cognitive function and subsequent depression 17
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms

Atkinson KM Koenka AC Sanchez CE Moshontz HCooper H (2014) Reporting standards for literaturesearches and report inclusion criteria making researchsyntheses more transparent and easy to replicate ResearchSynthesis Methods 6 87ndash95
Baer LH Tabri N Blair M Bye D Li KZH Pushkar D(2013) Longitudinal associations of need for cognitioncognitive activity and depressive symptomatology withcognitive function in recent retirees Journals of GerontologySeries B Psychological Sciences and Social Sciences 68 655ndash664
Barbey AK Colom R Solomon J Krueger F Forbes CGrafman J (2012) An integrative architecture for generalintelligence and executive function revealed by lesionmapping Brain 135 1154ndash1164
Barnett JH Salmond CH Jones PB Sahakian BJ (2006)Cognitive reserve in neuropsychiatry Psychological Medicine36 1053ndash1064
Beaujean AA Parker S Qiu X (2013) The relationshipbetween cognitive ability and depression a longitudinaldata analysis Social Psychiatry and Psychiatric Epidemiology48 1983ndash1992
Belsky DW Caspi A Arseneault L Bleidorn W Fonagy PGoodman M Houts R Moffitt TE (2012) Etiologicalfeatures of borderline personality related characteristics in abirth cohort of 12-year-old children Development andPsychopathology 24 251ndash265
Betts KS Williams GM Najman JM Alati R (2016)Predicting spectrums of adult mania psychosis anddepression by prospectively ascertained childhoodneurodevelopment Journal of Psychiatric Research 72 22ndash29
Bora E Harrison BJ Yuumlcel M Pantelis C (2013) Cognitiveimpairment in euthymic major depressive disorder a meta-analysis Psychological Medicine 43 2017ndash2026
Borenstein M Hedges LV Higgins JPT Rothstein HR(2011) Introduction to Meta-Analysis John Wiley amp SonsWest Sussex UK
Canals J Domegravenech-Llaberia E Fernaacutendez-Ballart J Martiacute-Henneberg C (2002) Predictors of depression at eighteenA 7-year follow-up study in a Spanish nonclinicalpopulation European Child amp Adolescent Psychiatry 11226ndash233
Christensen H Griffiths K Mackinnon A (1997) Aquantitative review of cognitive deficits in depression andAlzheimer-type dementia Selection of Studies 3 631ndash651
Connolly SL Wagner Ca Shapero BG Pendergast LLAbramson LY Alloy LB (2014) Rumination prospectivelypredicts executive functioning impairments in adolescentsJournal of Behavior Therapy and Experimental Psychiatry 4546ndash56
Cooper HM (1979) Statistically combining independentstudies a meta-analysis of sex differences in conformityresearch Journal of Personality and Social Psychology 37131ndash146
Cooper HM (2010) Research Synthesis and Meta-Analysis AStep-by-Step Approach 4th edn SAGE PublicationsWashington (DC) USA
Cuijpers P de Graaf R van Dorsselaer S (2004) Minordepression risk profiles functional disability health careuse and risk of developing major depression Journal ofAffective Disorders 79 71ndash79
Cuthbert BN Kozak MJ (2013) Constructing constructs forpsychopathology the NIMH research domain criteriaJournal of Abnormal Psychology 122 928ndash937
Der G Batty GD Deary IJ (2009) The association between IQin adolescence and a range of health outcomes at 40 in the1979 US National Longitudinal Study of Youth Intelligence37 573ndash580
Dubow EF Boxer P Huesmann LR (2008) Childhood andadolescent predictors of early and middle adulthoodalcohol use and problem drinking the Columbia CountyLongitudinal Study Addiction 103 36ndash47
Duval S Tweedie R (2000) Trim and fill a simple funnel-plot-based method of testing and adjusting for publicationbias in meta-analysis Biometrics 56 455ndash463
Evans LD Kouros CD Samanez-Larkin S Garber J (2015)Concurrent and short-term prospective relations amongneurocognitive functioning coping and depressivesymptoms in youth Journal of Clinical Child and AdolescentPsychology 53 1ndash15
Franz CE Lyons MJ OrsquoBrien R Panizzon MS Kim K BhatR Grant MD Toomey R Eisen S Xian H Kremen WS(2011) A 35-year longitudinal assessment of cognition andmidlife depression symptoms the Vietnam Era Twin Studyof Aging American Association for Geriatric PsychiatryAmerican Journal of Geriatric Psychiatry 19 559ndash570
Gale CR Batty GD Tynelius P Deary IJ Rasmussen F(2010) Intelligence in early adulthood and subsequenthospitalization for mental disorders Epidemiology 2170ndash77
Gale CR Deary IJ Boyle SH Barefoot J Mortensen LHBatty GD (2008) Cognitive ability in early adulthood andrisk of 5 specific psychiatric disorders in middle age theVietnam experience study Archives of General Psychiatry 651410ndash1418
Gale CR Hatch SL Batty GD Deary IJ (2009) Intelligence inchildhood and risk of psychological distress in adulthoodthe 1958 National Child Development Survey and the 1970British Cohort Study Intelligence 37 592ndash599
Gjerde PF (1995) Alternative pathways to chronicdepressive symptoms in young adults gender differencesin developmental trajectories Child Development 661277ndash1300
Gottfredson LS (1997) Mainstream science on intelligence aneditorial with 52 signatories history and bibliographyIntelligence 24 13ndash23
Guyer AE Choate VR Grimm KJ Pine DS Keenan K(2011) Emerging depression is associated with facememory deficits in adolescent girls Elsevier Inc Journal ofthe American Academy of Child and Adolescent Psychiatry 50180ndash190
Gyurak A Patenaude B Korgaonkar MS Grieve SMWilliams LM Etkin A (2015) Frontoparietal activationduring response inhibition predicts remission toantidepressants in patients with major depression BiologicalPsychiatry 79 1ndash8
Hagenaars SP Harris SE Davies G Hill WD LiewaldDCM Ritchie SJ Marioni RE Fawns-Ritchie C Cullen BMalik R METASTROKE Consortium IC for BPGSpiroMeta Consortium CHARGE ConsortiumPulmonary Group CCA and LG Worrall BB Sudlow
Association between cognitive function and subsequent depression 15
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
CLM Wardlaw JM Gallacher J Pell J McIntosh AMSmith DJ Gale CR Deary IJ (2016) Shared geneticaetiology between cognitive functions and physical andmental health in UK Biobank (N = 112 151) and 24 GWASconsortiaMolecular Psychiatry Published online 26 January2016 doi101038mp2015225
Hatch SL Jones PB Kuh D Hardy R Wadsworth MEJRichards M (2007) Childhood cognitive ability and adultmental health in the British 1946 birth cohort Social Scienceamp Medicine (1982) 64 2285ndash2296
Hipwell AE Sapotichne B Klostermann S Battista DKeenan K (2011) Autobiographical memory as a predictorof depression vulnerability in girls Journal of Clinical Childand Adolescent Psychology 40 254ndash265
Horowitz JL Garber J (2003) Relation of intelligence andreligiosity to depressive disorders in offspring of depressedand nondepressed mothers The American Academy ofChild and Adolescent Psychiatry Journal of the AmericanAcademy of Child and Adolescent Psychiatry 42 578ndash586
Johnson W Bouchard TJ Krueger RF McGue MGottesman II (2004) Just one g consistent results fromthree test batteries Intelligence 32 95ndash107
Keedwell PA Andrew C Williams SCR Brammer MJPhillips ML (2005) The neural correlates of anhedoniain major depressive disorder Biological Psychiatry 58843ndash853
Kessler RC Berglund P Demler O Jin R Koretz DMerikangas KR Rush AJ Walters EE Wang PS (2003)The epidemiology of major depressive disorder resultsfrom the National Comorbidity Survey Replication(NCS-R) Journal of the American Medical Association 2893095ndash3105
Koenen KC Moffitt TE Roberts AL Martin LT KubzanskyL Harrington H Poulton R Caspi A (2009) Childhood IQand adult mental disorders a test of the cognitive reservehypothesis American Journal of Psychiatry 166 50ndash57
Lewinsohn PM Solomon A Seeley JR Zeiss A (2000)Clinical implications of lsquosubthresholdrsquo depressivesymptoms Journal of Abnormal Psychology 109 345ndash351
Luppino FS de Wit LM Bouvy PF Stijnen T Cuijpers PPenninx BWJH Zitman FG (2010) Overweight obesityand depression a systematic review and meta-analysisof longitudinal studies Archives of General Psychiatry 67220ndash229
McCord J Ensminger ME (1997) Multiple risks andcomorbidity in an African-American population CriminalBehaviour and Mental Health 7 339ndash352
McDermott LM Ebmeier KP (2009) A meta-analysis ofdepression severity and cognitive function Elsevier BVJournal of Affective Disorders 119 1ndash8
Melartin TK Rytsaumllauml HJ Leskelauml US Lestelauml-Mielonen PSSokero TP Isometsauml ET (2002) Current comorbidity ofpsychiatric disorders among DSM-IV major depressivedisorder patients in psychiatric care in the VantaaDepression Study Journal of Clinical Psychiatry 63 126ndash134
Meyer SE Carlson GA Wiggs EA Martinez PE RonsavilleDS KlimesndashDougan B Gold PW RadkendashYarrow M(2004) A prospective study of the association amongimpaired executive functioning childhood attentional
problems and the development of bipolar disorderDevelopment and Psychopathology 16 461ndash476
MiyakeA FriedmanNP EmersonMJWitzki aHHowerter AWager TD (2000) The unity and diversity of executivefunctions and their contributions to complex lsquoFrontal Lobersquotasks a latentvariable analysisCognitive Psychology41 49ndash100
Moher D Liberati A (2009) Preferred reporting items forsystematic reviews and meta-analyses the PRISMAstatement Annals of Internal Medicine 151 264ndash269
Papmeyer M Sussmann JE Hall J McKirdy J Peel AMacdonald A Lawrie SM Whalley HC McIntosh AM(2015) Neurocognition in individuals at high familial riskof mood disorders with or without subsequent onset ofdepression Psychological Medicine 45 1ndash11
Peterson RA Brown SP (2005) On the use of betacoefficients in meta-analysis Journal of Applied Psychology90 175ndash181
Pine DS Cohen P Brook J Coplan JD (1997) Psychiatricsymptoms in adolescence as predictors of obesity in earlyadulthood a longitudinal study American Journal of PublicHealth 87 1303ndash1310
Quinn ME Joormann J (2015) Control when it countschange in executive control under stress predicts depressionsymptoms Emotion Junio 22 1ndash10
Rawal A Rice F (2012) Examining overgeneralautobiographical memory as a risk factor for adolescentdepression Elsevier Inc Journal of the American Academy ofChild and Adolescent Psychiatry 51 518ndash527
Ree MJ Earles JA (1991) The stability of g across differentmethods of estimation Intelligence 15 271ndash278
Rock PL Roiser JP Riedel WJ Blackwell AD (2014)Cognitive impairment in depression a systematic reviewand meta-analysis Psychological Medicine 44 2029ndash2040
Rogers MA Kasai K Koji M Fukuda R Iwanami ANakagome K Fukuda M Kato N (2004) Executive andprefrontal dysfunction in unipolar depression a review ofneuropsychological and imaging evidence NeuroscienceResearch 50 1ndash11
Scult MA Knodt AR Swartz JR Brigidi BD Hariri AR(2016) Thinking and feeling individual differences inhabitual emotion regulation and stress-related mood areassociated with prefrontal executive control ClinicalPsychological Science doi1011772167702616654688
Sharp C Petersen N Goodyer I (2008) Emotional reactivityand the emergence of conduct problems and emotionalsymptoms in 7- to 11-year-olds a 1-year follow-up studyJournal of the American Academy of Child and AdolescentPsychiatry 47 565ndash573
Siegel LS (1999) Issues in the definition and diagnosis oflearning disabilities a perspective on Guckenberger vBoston University Journal of Learning Disabilities 32 304ndash319
Simons CJP Jacobs N Derom C Thiery E Jolles J van Os JKrabbendam L (2009) Cognition as predictor of currentand follow-up depressive symptoms in the generalpopulation Acta Psychiatrica Scandinavica 120 45ndash52
Slykerman RF Thompson J Waldie K Murphy R Wall CMitchell EA (2015) Maternal stress during pregnancy isassociated with moderate to severe depression in 11-year-old children Acta Paediatrica 104 68ndash74
16 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Snyder HR (2013) Major depressive disorder is associatedwith broad impairments on neuropsychological measuresof executive function a meta-analysis and reviewPsychological Bulletin 139 81ndash132
Soslashrensen HJ Saeligbye D Urfer-Parnas A Mortensen ELParnas J (2012) Premorbid intelligence and educationallevel in bipolar and unipolar disorders a Danish draftboard study Journal of Affective Disorders 136 1188ndash1191
SpearmanC (1904) lsquoGeneral intelligencersquoobjectivelydeterminedandmeasuredAmerican Journal of Psychology 15 201
Stern Y (2003) The concept of cognitive reserve a catalyst forresearch Journal of Clinical and Experimental Neuropsychology(Neuropsychology Development and Cognition Section A) 25589ndash593
Stroup D Berlin J Morton S Olkin I Williamson GDRennie D Moher D Becker BJ Sipe TA Thacker SB(2000) Meta-analysis of Observational Studies inEpidemiology a proposal for reporting Journal of theAmerican Medical Association 283 2008
Vinberg M Miskowiak KW Kessing LV (2013) Impairmentof executive function and attention predicts onset ofaffective disorder in healthy high-risk twins Journal ofClinical Psychiatry 74 e747ndashe753
Zammit S Allebeck P David AS Dalman C HemmingssonT Lundberg I Lewis G (2004) A longitudinal study ofpremorbid IQ Score and risk of developing schizophreniabipolar disorder severe depression and other nonaffectivepsychoses Archives of General Psychiatry 61 354ndash360
Association between cognitive function and subsequent depression 17
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms

CLM Wardlaw JM Gallacher J Pell J McIntosh AMSmith DJ Gale CR Deary IJ (2016) Shared geneticaetiology between cognitive functions and physical andmental health in UK Biobank (N = 112 151) and 24 GWASconsortiaMolecular Psychiatry Published online 26 January2016 doi101038mp2015225
Hatch SL Jones PB Kuh D Hardy R Wadsworth MEJRichards M (2007) Childhood cognitive ability and adultmental health in the British 1946 birth cohort Social Scienceamp Medicine (1982) 64 2285ndash2296
Hipwell AE Sapotichne B Klostermann S Battista DKeenan K (2011) Autobiographical memory as a predictorof depression vulnerability in girls Journal of Clinical Childand Adolescent Psychology 40 254ndash265
Horowitz JL Garber J (2003) Relation of intelligence andreligiosity to depressive disorders in offspring of depressedand nondepressed mothers The American Academy ofChild and Adolescent Psychiatry Journal of the AmericanAcademy of Child and Adolescent Psychiatry 42 578ndash586
Johnson W Bouchard TJ Krueger RF McGue MGottesman II (2004) Just one g consistent results fromthree test batteries Intelligence 32 95ndash107
Keedwell PA Andrew C Williams SCR Brammer MJPhillips ML (2005) The neural correlates of anhedoniain major depressive disorder Biological Psychiatry 58843ndash853
Kessler RC Berglund P Demler O Jin R Koretz DMerikangas KR Rush AJ Walters EE Wang PS (2003)The epidemiology of major depressive disorder resultsfrom the National Comorbidity Survey Replication(NCS-R) Journal of the American Medical Association 2893095ndash3105
Koenen KC Moffitt TE Roberts AL Martin LT KubzanskyL Harrington H Poulton R Caspi A (2009) Childhood IQand adult mental disorders a test of the cognitive reservehypothesis American Journal of Psychiatry 166 50ndash57
Lewinsohn PM Solomon A Seeley JR Zeiss A (2000)Clinical implications of lsquosubthresholdrsquo depressivesymptoms Journal of Abnormal Psychology 109 345ndash351
Luppino FS de Wit LM Bouvy PF Stijnen T Cuijpers PPenninx BWJH Zitman FG (2010) Overweight obesityand depression a systematic review and meta-analysisof longitudinal studies Archives of General Psychiatry 67220ndash229
McCord J Ensminger ME (1997) Multiple risks andcomorbidity in an African-American population CriminalBehaviour and Mental Health 7 339ndash352
McDermott LM Ebmeier KP (2009) A meta-analysis ofdepression severity and cognitive function Elsevier BVJournal of Affective Disorders 119 1ndash8
Melartin TK Rytsaumllauml HJ Leskelauml US Lestelauml-Mielonen PSSokero TP Isometsauml ET (2002) Current comorbidity ofpsychiatric disorders among DSM-IV major depressivedisorder patients in psychiatric care in the VantaaDepression Study Journal of Clinical Psychiatry 63 126ndash134
Meyer SE Carlson GA Wiggs EA Martinez PE RonsavilleDS KlimesndashDougan B Gold PW RadkendashYarrow M(2004) A prospective study of the association amongimpaired executive functioning childhood attentional
problems and the development of bipolar disorderDevelopment and Psychopathology 16 461ndash476
MiyakeA FriedmanNP EmersonMJWitzki aHHowerter AWager TD (2000) The unity and diversity of executivefunctions and their contributions to complex lsquoFrontal Lobersquotasks a latentvariable analysisCognitive Psychology41 49ndash100
Moher D Liberati A (2009) Preferred reporting items forsystematic reviews and meta-analyses the PRISMAstatement Annals of Internal Medicine 151 264ndash269
Papmeyer M Sussmann JE Hall J McKirdy J Peel AMacdonald A Lawrie SM Whalley HC McIntosh AM(2015) Neurocognition in individuals at high familial riskof mood disorders with or without subsequent onset ofdepression Psychological Medicine 45 1ndash11
Peterson RA Brown SP (2005) On the use of betacoefficients in meta-analysis Journal of Applied Psychology90 175ndash181
Pine DS Cohen P Brook J Coplan JD (1997) Psychiatricsymptoms in adolescence as predictors of obesity in earlyadulthood a longitudinal study American Journal of PublicHealth 87 1303ndash1310
Quinn ME Joormann J (2015) Control when it countschange in executive control under stress predicts depressionsymptoms Emotion Junio 22 1ndash10
Rawal A Rice F (2012) Examining overgeneralautobiographical memory as a risk factor for adolescentdepression Elsevier Inc Journal of the American Academy ofChild and Adolescent Psychiatry 51 518ndash527
Ree MJ Earles JA (1991) The stability of g across differentmethods of estimation Intelligence 15 271ndash278
Rock PL Roiser JP Riedel WJ Blackwell AD (2014)Cognitive impairment in depression a systematic reviewand meta-analysis Psychological Medicine 44 2029ndash2040
Rogers MA Kasai K Koji M Fukuda R Iwanami ANakagome K Fukuda M Kato N (2004) Executive andprefrontal dysfunction in unipolar depression a review ofneuropsychological and imaging evidence NeuroscienceResearch 50 1ndash11
Scult MA Knodt AR Swartz JR Brigidi BD Hariri AR(2016) Thinking and feeling individual differences inhabitual emotion regulation and stress-related mood areassociated with prefrontal executive control ClinicalPsychological Science doi1011772167702616654688
Sharp C Petersen N Goodyer I (2008) Emotional reactivityand the emergence of conduct problems and emotionalsymptoms in 7- to 11-year-olds a 1-year follow-up studyJournal of the American Academy of Child and AdolescentPsychiatry 47 565ndash573
Siegel LS (1999) Issues in the definition and diagnosis oflearning disabilities a perspective on Guckenberger vBoston University Journal of Learning Disabilities 32 304ndash319
Simons CJP Jacobs N Derom C Thiery E Jolles J van Os JKrabbendam L (2009) Cognition as predictor of currentand follow-up depressive symptoms in the generalpopulation Acta Psychiatrica Scandinavica 120 45ndash52
Slykerman RF Thompson J Waldie K Murphy R Wall CMitchell EA (2015) Maternal stress during pregnancy isassociated with moderate to severe depression in 11-year-old children Acta Paediatrica 104 68ndash74
16 M A Scult et al
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms
Snyder HR (2013) Major depressive disorder is associatedwith broad impairments on neuropsychological measuresof executive function a meta-analysis and reviewPsychological Bulletin 139 81ndash132
Soslashrensen HJ Saeligbye D Urfer-Parnas A Mortensen ELParnas J (2012) Premorbid intelligence and educationallevel in bipolar and unipolar disorders a Danish draftboard study Journal of Affective Disorders 136 1188ndash1191
SpearmanC (1904) lsquoGeneral intelligencersquoobjectivelydeterminedandmeasuredAmerican Journal of Psychology 15 201
Stern Y (2003) The concept of cognitive reserve a catalyst forresearch Journal of Clinical and Experimental Neuropsychology(Neuropsychology Development and Cognition Section A) 25589ndash593
Stroup D Berlin J Morton S Olkin I Williamson GDRennie D Moher D Becker BJ Sipe TA Thacker SB(2000) Meta-analysis of Observational Studies inEpidemiology a proposal for reporting Journal of theAmerican Medical Association 283 2008
Vinberg M Miskowiak KW Kessing LV (2013) Impairmentof executive function and attention predicts onset ofaffective disorder in healthy high-risk twins Journal ofClinical Psychiatry 74 e747ndashe753
Zammit S Allebeck P David AS Dalman C HemmingssonT Lundberg I Lewis G (2004) A longitudinal study ofpremorbid IQ Score and risk of developing schizophreniabipolar disorder severe depression and other nonaffectivepsychoses Archives of General Psychiatry 61 354ndash360
Association between cognitive function and subsequent depression 17
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms

Snyder HR (2013) Major depressive disorder is associatedwith broad impairments on neuropsychological measuresof executive function a meta-analysis and reviewPsychological Bulletin 139 81ndash132
Soslashrensen HJ Saeligbye D Urfer-Parnas A Mortensen ELParnas J (2012) Premorbid intelligence and educationallevel in bipolar and unipolar disorders a Danish draftboard study Journal of Affective Disorders 136 1188ndash1191
SpearmanC (1904) lsquoGeneral intelligencersquoobjectivelydeterminedandmeasuredAmerican Journal of Psychology 15 201
Stern Y (2003) The concept of cognitive reserve a catalyst forresearch Journal of Clinical and Experimental Neuropsychology(Neuropsychology Development and Cognition Section A) 25589ndash593
Stroup D Berlin J Morton S Olkin I Williamson GDRennie D Moher D Becker BJ Sipe TA Thacker SB(2000) Meta-analysis of Observational Studies inEpidemiology a proposal for reporting Journal of theAmerican Medical Association 283 2008
Vinberg M Miskowiak KW Kessing LV (2013) Impairmentof executive function and attention predicts onset ofaffective disorder in healthy high-risk twins Journal ofClinical Psychiatry 74 e747ndashe753
Zammit S Allebeck P David AS Dalman C HemmingssonT Lundberg I Lewis G (2004) A longitudinal study ofpremorbid IQ Score and risk of developing schizophreniabipolar disorder severe depression and other nonaffectivepsychoses Archives of General Psychiatry 61 354ndash360
Association between cognitive function and subsequent depression 17
httpdxdoiorg101017S0033291716002075Downloaded from httpwwwcambridgeorgcore Duke University Libraries on 15 Sep 2016 at 110833 subject to the Cambridge Core terms of use available at httpwwwcambridgeorgcoreterms