eprints.qut.edu.au the applicability of the precaution adoption process model in understanding older...
TRANSCRIPT

THE APPLICABILITY OF THE PRECAUTION
ADOPTION PROCESS MODEL IN
UNDERSTANDING OLDER ADULTS’ SELF-REGULATORY DRIVING BEHAVIOURS
Heidi Hassan
BDent, MPH, MEpi
Submitted in fulfilment of the requirements for the degree of
Doctor of Philosophy
Centre for Accident Research and Road Safety – Queensland
School of Psychology and Counselling
Faculty of Health
Queensland University of Technology
2017


The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours i
Keywords
Ageing, driving, feedback, latent class analysis, older driver, PAPM, self-awareness,
self-regulation, stages of change.

ii The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Abstract
The number of older Australian drivers is predicted to increase dramatically
in the next decade. Age-related declines in sensory, cognitive and motor abilities can
compromise older adults’ abilities to drive safely. There is a considerable variability
in the way older adults experience ageing and the associated physiological and
pathological declines. Older adults are relatively safe drivers, however, when
compared to young and middle-aged drivers they are more likely to sustain serious
injuries or die if involved in a crash. This over-representation in serious and life-
threatening crashes among older drivers is mainly attributed to their increased
fragility.
For years, mandatory age-based testing has been advocated (and sometimes
implemented) as a strategy to identify unsafe and unfit older drivers. Recently,
research has shown that there are no demonstrable safety benefits associated with
this strategy. Driving cessation is associated with many adverse consequences such
as social isolation and depression. In a society that relies heavily on private cars,
maintaining older adults’ safe mobility is a public health priority.
The transition from driving to non-driving is difficult and older adults should
be a part of the decision-making process. Some older drivers modify their driving
behaviours (e.g. reduction of overall driving and avoidance of challenging driving
situations) in response to perceived changes in their driving abilities. These
behavioural modifications are known as self-regulation of driving. Researchers have
promoted self-regulation as a positive approach that can balance the needs for
mobility and safety. There is however limited understanding pertaining as to why
some older drivers regulate their driving while others don’t. It is still unclear what
works best to promote self-regulation among older drivers. There is growing
evidence that older drivers go through different qualitative stages towards modifying
their driving behaviours. It therefore could be useful to examine the driving self-
regulation process within behaviour change framework. The lack of a theoretically-
informed model of driving self-regulation inhibits our ability to understand and
describe such complex process.

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours iii
This thesis addresses this gap by examining the applicability of a stage-based
theoretical model, the Precaution Adoption Process Model (PAPM), for
understanding why some older drivers adopt self-regulatory (precautionary)
behaviours intended to reduce their road crash risk. The PAPM describes how
individuals move through stages of change towards adoption of health protective
behaviour. The early stages of the PAPM are defined in terms of psychological
states and mindsets of individuals (Weinstein & Sandmand, 2002). The late stages
are mostly governed by factors that can facilitate or hinder the adoption of the
precaution. Individuals progress through seven stages from lack of awareness to
action: unawareness (stage 1); awareness that there is an issue but a lack of personal
engagement with it (stage 2); engagement (“this applies to me”) but indecision (stage
3) about the need to act; either a decision not to act (stage 4) or a decision to act
(stage 5); if the latter, acting by taking the precaution (stage 6) (e.g. self-regulating);
and maintaining the behaviour (stage 7). This thesis aims to develop a conceptual
framework based on the PAPM that profiles older adults into distinctive groups
according to their mindsets towards self-regulatory driving behaviours. By applying
a stage-based approach, the self-regulation process can be broken down into
qualitatively different categories that accommodate the heterogeneity of the older
driver population. This would allow interventions to be customised based on the
individual’s specific need.
The first stage of this research program was qualitative in nature and involved
a study that explored the preliminary fit of the driving regulation process within the
PAPM framework. Five focus groups with a total of 27 participants aged 70 years or
more were conducted. Thematic analysis resulted in the development of five main
themes: the meaning of driving, changes in driving pattern, feedback, the planning
process, and solutions. Driving was perceived as the key to maintaining participants’
mobility and independence. Participants were aware of the impact of ageing on
driving abilities, however, the majority were not aware of any personal changes. The
analysis also resulted in an initial model of driving self-regulation among older
drivers that was informed by the PAPM as the theoretical framework. It identified
several social, personal, and environmental factors that can either facilitate or hinder
older drivers’ transition between the proposed stages of change. The findings from
this study suggest that further examination of the PAPM is needed. The findings

iv The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
informed the development of a questionnaire that was used in the second stage of the
research. In this cross-sectional study, 222 Australian drivers aged 70 years and
more were categorised into five stages of the PAPM based on their intention to
regulate and/or restrict their driving. Participants also completed a self-administered
questionnaire measuring demographic, psychosocial, and environmental factors
related to self-regulation. The analysis of the data collected in study two was divided
in two phases. Phase one investigated the prevalence of the PAPM stages of change
within the sample. Further, the study investigated the psychosocial and
environmental factors associated with different stages of the PAPM and those that
predict the decision to adopt self-regulatory behaviour. Bivariate analyses were
performed to identify the differences between PAPM groups. In addition, logistic
regression was used to determine the predictive variables for adoption of self-
regulatory behaviours. Distribution of the sample across the stages was: unengaged,
n = 104 (46.8%); undecided, n = 24 (10.8%); resisting action, n = 23 (10.4%);
planning to act, n = 22 (9.9%); and acting, n = 49 (22.1%). The significant
predictors in the final model were self-rated driving confidence, family feedback,
self-rated quality of driving and driving relinquishment expectation. The study
indicates that there are significant differences among PAPM stages of change.
Further, several psychosocial variables significantly predicted the adoption of self-
regulatory behaviours among participants.
Phase two employed a bottom-up approach to profile older drivers based on
their mindset towards adopting self-regulatory driving behaviours using Latent Class
Analysis. Latent Class Analysis (LCA) is a person-centred approach used to identify
subgroups with distinctive patterns. The selection of LCA indicators was guided by
the PAPM and involved driving perception, importance of driving, and barriers
towards change. The identified classes were described in terms of socio-
demographic factors, alternative transport use, and self-reported avoidance
behaviour. The analysis identified three classes of self-regulatory behaviours of
older drivers which can be conceptualised to occur through different stages.
Individuals in class 1: willing to change, had the lowest levels of reported driving
confidence, driving comfort, and perceived driving abilities. They were least likely
to agree that giving up driving would restrict their mobility or independence. They
were also least likely to agree that giving up driving would be difficult in terms of

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours v
barriers. Individuals in class 2: the unengaged, had the highest levels of reported
driving ability. They were most likely to agree that driving cessation would restrict
their mobility and independence, and that lifestyle factors were barriers to changing
their driving. Individuals in class 3: the unwilling, had low perceived driving
abilities. They agreed that driving cessation would restrict their independence and
mobility and were most likely to agree that they would be letting other people down
if they stopped driving. This group overall were most likely to agree with statements
about barriers to giving up driving. Based on the findings, the initial model was
refined.
The last stage was experimental and aimed to assess the impact of providing
one-on-one feedback regarding driving performance on stage transition among a
sample of 26 older drivers. This study also investigated the impact of such feedback
on older drivers’ perception of the quality of their driving and their willingness to
modify their driving behaviour. A pre-experimental single group, pre-post design
was employed. No significant changes in participants’ self-rated quality of driving
were found before and after the feedback. However, following the feedback, the
number of participants willing to change their driving behaviour significantly
increased from 4 to 14.
This research program contributes to the theoretical understanding of older
drivers’ self-regulation through the application of the PAPM and the development of
a conceptual model that categorises older adults into different stages of behaviour
change while capturing a wide range of interpersonal, intrapersonal, and
environmental factors that influence self-regulatory driving behaviour. A theory-
based understanding of older drivers’ self-regulatory behaviours and how to
influence them can assist in the development of effective interventions. To the best
of the researcher’s knowledge, this is the first study to develop a comprehensive
model of older drivers’ regulatory behaviour using the stages of change approach.
The model is very flexible and can be customised in different contexts based on the
study population (e.g. women, rural drivers or professional older drivers), the self-
regulatory practice (e.g. tactical, strategic or life-goal) and the desired interventions
(e.g. in-vehicle technologies, educational interventions or health professional
interventions).

vi The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours vii
List of thesis publications and submitted manuscripts
Paper 1* Hassan, H., King, M., & Watt, K. (2015). The perspectives of older
drivers on the impact of feedback on their driving behaviours: a
qualitative study. Transportation Research Part F, 28, pp. 25-39. Q2
Paper 2* Hassan, H., King, M., & Watt, K. (2017). Examination of the
Precaution Adoption Process Model in understanding older drivers’
behaviour: an exploratory study. Transportation Research Part F,
46(A), pp. 111-123. Q2
Paper 3* Hassan, H. & King, M. (under preparation). Older adults’ self-
regulatory driving behaviour: A latent class analysis.
* These papers form chapters of this thesis by publication
Other publications related to the thesis Paper 1 Hassan, H., King, M., and Watt, K. (2015). Older adults’ driving
reduction: Is the gender gap narrowing? (Peer reviewed paper).
Proceedings of the 2015 Australasian Road Safety Conference, 14-16
October 2015, Gold Coast, Australia
Conference presentations relating to this thesis Conference 1 Hassan, H., King, M., & Watt, K. (2014). The applicability of the
Precaution Adoption Process Model for understanding self-regulatory
driving behaviour among older drivers (Poster). In 2014 Australasian
Road Safety Research, Policing and Education Conference, 12-14
November 2014, Grand Hyatt, Melbourne, VIC. Conference 2 Hassan, H., King, M., & Watt, K. (2015). Older adults and driving
reduction: Is the gender gap narrowing? In 2015 Australasian Road
Safety Conference, 14-16 October 2015, Gold Coast, Qld.

viii The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Table of Contents
Keywords .................................................................................................................................. i
Abstract .................................................................................................................................... ii
List of thesis publications and submitted manuscripts ........................................................... vii
Other publications related to the thesis .................................................................................. vii
Conference presentations relating to this thesis ..................................................................... vii
List of Figures ......................................................................................................................... xi
List of Tables .......................................................................................................................... xii
List of Abbreviations ............................................................................................................. xiii
Statement of Original Authorship ......................................................................................... xiv
Acknowledgements ................................................................................................................ xv
Chapter 1: Introduction ...................................................................................... 1
1.1 Introductory comments .................................................................................................. 1
1.2 Background and rationale for the research Program ...................................................... 2
1.3 Research aims .............................................................................................................. 15
1.4 Significance of this study ............................................................................................. 17
1.5 Demarcation of scope of the research program ............................................................ 17
1.6 Thesis outline ............................................................................................................... 17
1.7 Chapter summary ......................................................................................................... 18
Chapter 2: Literature Review ........................................................................... 20
2.1 Introductory comments ................................................................................................ 20
2.2 Growing number of older drivers ................................................................................. 20
2.3 The importance of driving ............................................................................................ 21
2.4 Transportation alternatives ........................................................................................... 22
2.5 Factors enabling driving safety among older drivers ................................................... 23
2.6 Are older drivers a road safety problem compared to other drivers? ........................... 24
2.7 Patterns and characteristics of older drivers’ crashes ................................................... 26
2.8 Current older driver road safety Countermeasures ...................................................... 26
2.9 Chapter summary ......................................................................................................... 47
Chapter 3: Theoretical framework and current models of older adults’ driving behaviour ..................................................................................................... 49
3.1 Introductory comments ................................................................................................ 49
3.2 Descriptive models ....................................................................................................... 49
3.3 Explanatory models ...................................................................................................... 53
3.4 Other models ................................................................................................................ 59
3.5 Limitations with the existing models ........................................................................... 64

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours ix
3.6 The Precaution Adoption Process Model (PAPM) ....................................................... 67
3.7 Chapter summary and implications .............................................................................. 70
Chapter 4: Research Design .............................................................................. 73
4.1 Introductory comments ................................................................................................. 73
4.2 Research questions ....................................................................................................... 73
4.3 Research design and methodology ............................................................................... 75
4.4 Setting, population, and recruitment ............................................................................. 76
4.5 Methods ........................................................................................................................ 77
4.6 Data management and data analysis ............................................................................. 79
4.7 Organisation of papers .................................................................................................. 80
4.8 Ethics Approval ............................................................................................................ 81
Chapter 5: The perspectives of older drivers on the impact of feedback on their driving behaviours: a qualitative study (Study 1) ........................................ 83
5.1 Publication Status ......................................................................................................... 83
5.2 Statement of Contribution............................................................................................. 83
5.3 Abstract ......................................................................................................................... 85
5.4 Introduction .................................................................................................................. 86
5.5 Method .......................................................................................................................... 91
5.6 Analysis ........................................................................................................................ 93
5.7 Results .......................................................................................................................... 93
5.8 Discussion ................................................................................................................... 108
5.9 Limitations .................................................................................................................. 114
5.10 Conclusion .................................................................................................................. 114
Chapter 6: Examination of the Precaution Adoption Process Model in understanding older drivers’ behaviour: an explanatory study (Study 2, Phase 1) 116
6.1 Publication Status ....................................................................................................... 116
6.2 Statement of Contribution........................................................................................... 116
6.3 Abstract ....................................................................................................................... 118
6.4 Introduction ................................................................................................................ 119
6.5 Methods ...................................................................................................................... 122
6.6 Analysis ...................................................................................................................... 126
6.7 Results ........................................................................................................................ 126
6.8 Discussion ................................................................................................................... 133
6.9 Limitations .................................................................................................................. 138
6.10 Conclusion .................................................................................................................. 139
Chapter 7: Older adults’ self-regulatory driving behaviour: A latent class analysis (Study 2, Phase 2) .................................................................................... 140

x The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
7.1 Publication Status ....................................................................................................... 140
7.2 Statement of Contribution .......................................................................................... 140
7.3 Abstract ...................................................................................................................... 141
7.4 Introduction ................................................................................................................ 142
7.5 Method ....................................................................................................................... 145
7.6 Analysis ...................................................................................................................... 147
7.7 Results ........................................................................................................................ 149
7.8 Discussion .................................................................................................................. 152
7.9 Limitations ................................................................................................................. 155
Chapter 8: Feedback and older drivers (Study three) .................................. 157
8.1 Introductory comments .............................................................................................. 157
8.2 Methods ...................................................................................................................... 159
8.3 Analysis ...................................................................................................................... 161
8.4 Results ........................................................................................................................ 161
8.5 discussion ................................................................................................................... 165
8.6 Limitations ................................................................................................................. 167
Chapter 9: Discussion ...................................................................................... 167
9.1 Chapter overview ....................................................................................................... 167
9.2 Overall research findings ........................................................................................... 168
9.3 Contributions to research ........................................................................................... 184
9.4 Practical implications of the research program .......................................................... 186
9.5 Study strengths and limitations .................................................................................. 188
9.6 Future directions ........................................................................................................ 189
9.7 Concluding remarks ................................................................................................... 190
Bibliography ........................................................................................................... 192
Appendices .............................................................................................................. 209

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours xi
List of Figures
Figure 1.1 Annual fatalities: road user type within age groups. .................................. 5
Figure 1.2: Annual number of fatal crashes ................................................................. 6
Figure 1.3: Stages of the Precaution Adoption Process Model .................................. 12
Figure 1.4: Stages of the program of research ........................................................... 16
Figure 1.5: Overview of thesis chapters ..................................................................... 19
Figure 2.1: Multifactorial model of factors enabling safe driving among older drivers .......................................................................................................... 24
Figure 3.1: Driving reduction/cessation framework .................................................. 50
Figure 3.2: Conceptualization of the process of driving behaviour change within the TTM framework ......................................................................... 53
Figure 3.3: Model of the process of driving self-regulation with ageing ................... 55
Figure 3.4: Driving as an Everyday Competence Model for Older Adults .............. 56
Figure 3.5: The Multilevel Older Person’s Transportation and Road Safety Model ........................................................................................................... 58
Figure 3.6: Precede-Proceed model of motor vehicle crashes among older drivers .......................................................................................................... 60
Figure 3.7: Conceptual model of driving cessation process ...................................... 63
Figure 3.8: Challenges in examining older driver behaviour ..................................... 64
Figure 4.1: Flowchart of the research program ......................................................... 77
Figure 4.2: Organisation of the papers ....................................................................... 81
Figure 5.1: Stages of the Precaution Adoption Process Model- Source: (Weinstein & Sandmand, 2002). .................................................................. 89
Figure 5.2: Proposed theoretical model of stage-based driving change involving feedback and self-regulation ...................................................................... 110
Figure 6.1: Preliminary theoretical model of stage-based driving change involving feedback and self-regulation (Hassan et al., 2015) .................... 121
Figure 7.1: Refined model of self-regulatory driving behaviour ............................. 155
Figure 9.1: Refined model of self-regulatory driving behaviour ............................. 184

xii The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
List of Tables
Table 1.1: Adaptation of the PAPM to the older drivers’ regulatory behaviours ...... 14
Table 2.1: Driver Licensing Practice renewal for car drivers (excluding heavy vehicle and motorbikes) in Australia (2016) ................................................ 30
Table 4.1: Precaution Adoption Process Model: Stage Classification Algorithm as applied to self-regulatory driving behaviours among older adults (Adapted from (Weinstein & Sandmand, 2002)) ..................... 78
Table 5.1: Characteristics of Participants ................................................................... 92
Table 6.1: Precaution Adoption Process Model: Stage Classification Algorithm as applied to self-regulatory driving behaviours among older adults (Adapted from Weinstein & Sandmand, 2002) ......................................... 123
Table 6.2: Sample characteristics (n=222) ............................................................... 126
Table 6.3: Most avoided driving situations and reasons for avoidance ................... 128
Table 6.4: Descriptions of the psychometric properties of scales ............................ 129
Table 6.5: PAPM stages .......................................................................................... 129
Table 6.6. Characteristics significantly associated with PAPM stage ..................... 130
Table 6.7: Hierarchical regression analysis (n=199) ................................................ 132
Table 7.1: Sample characteristics (n=222) ............................................................... 147
Table 7.2. Model Fit Statistics ................................................................................. 149
Table 7.3: Item-response probabilities .................................................................... 150
Table 7.4. Significant differences between latent classes ........................................ 151
Table 7.5. Frequencies of LCA classes for PAPM stages obtained by staging algorithm .................................................................................................... 152
Table 8.1: Adaptation of the PAPM to older drivers’ regulatory behaviours .......... 158
Table 8.2: Sample characteristics (n=21) ................................................................. 162
Table 8.3. Fitness to drive ........................................................................................ 163
Table 8.4. Driving errors observed in the driving assessment ................................. 164

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours xiii
List of Abbreviations
ADAS Advanced Driver Assistance System
CDT Clock Drawing Test
DEC Driving as an Everyday Competence Model
KEYS Knowledge Enhances Your Safety
LCA Latent Class Analysis
MOTRS Multilevel Older Person’s Transportation and Road Safety Model
OECD The organisation for Economic Co-operation and Development
PAPM Precaution Adoption Process Model
PDA Perceived Driving Ability
PPM PRECEDE-PROCEED Model
RACQ Royal Automobile Club of Queensland
SPSS Statistical Package for the Social Sciences
TTM Transtheoretical Model
UFOV Useful Field of View

xiv The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Statement of Original Authorship
I declare that this thesis is composed of my original work and that the work
contained in this thesis has not been previously submitted to meet requirements for
an award at this or any other higher education institution. To the best of my
knowledge and belief, the thesis contains no material previously published or written
by another person except where due reference is made. I have clearly stated the
contribution by others to jointly-authored works that I have included in my thesis.
Signature: QUT Verified Signature
Date: 17/01/2018

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours xv
Acknowledgements
When I first started this journey, I didn’t know what to expect. Five years later
and I am forever grateful for everyone who made this possible. This thesis couldn’t
have been completed without the unconditional support I have received from my
supervisors, Dr. Mark King, Dr. Kerrianne Watt, and Emeritus Professor. Mary
Sheehan. Mark, you have taught me that with persistence everything is possible. I
have learnt so much from you and you have always motivated me to go further than I
can! Through the times when I felt that this is not possible, you were there telling me
that I am on the right track. Kerrianne, you have always been there with your
feedback and you have always believed I can do this. Mary, thank you for every
wise and timely input you have provided.
Thank you to all the participants for their time and contribution. This would
have not been possible without them. Thank you to everyone at CARRS-Q for
making this journey easier.
To the three powerful women in my life, my mother, Rania and Marwa, you
have set a high example and you have taught me how to be the woman I am today.
Marwa, this is for you! To my husband, Tamer, you always believed in me! You
have been there by my side from the first day cheering and pushing me. To my boys,
Omar and Ryan, thank you for your patience, for all the times when I could not be
with you and for always welcoming me with smiles and hugs. To my big brother,
my “father” and my role model, Amr, thank you for being there for us when we
needed you the most. My brothers, Ahmed and Mohamed thank you for never losing
faith in me!


The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 1
Chapter 1: Introduction
1.1 INTRODUCTORY COMMENTS
This chapter provides an overview of the research program comprising this
thesis-by-publication. Given the predicted ageing of the driving population in
Australia and the significant over-involvement of older drivers in fatal crashes,
enhancing the safety of older Australian drivers has become a priority. Mandatory
age-based testing has shown no road safety benefits. On the contrary, it can result in
the premature loss of driving and subsequent loss of mobility. Cessation of driving is
linked to many adverse effects such as depression and isolation. It is therefore
important to balance the mobility and safety needs of older adults.
Self-regulation of driving has been promoted as an alternative approach that can
assist older adults in maintaining their driving privilege. It is still unclear why some
older drivers choose to modify their driving behaviours and why others keep driving
when it is no longer safe to do so. Previous studies have identified many
interpersonal, intrapersonal, and environmental factors that impact driving self-
regulation. However, the relative importance and interaction between these factors
and how they affect the driving behaviours among older adults is still not clear. It is
therefore critical to develop a model of driving self-regulation that can guide the
development of interventions. There is growing evidence that older drivers go
through different stages towards modifying their driving behaviours. Therefore, It
would be useful to examine the driving self-regulation process within a behaviour
change framework. Previous studies examining older drivers’ behaviour within
stages of change framework have relied entirely on qualitative findings without
further validation (e.g. (Kowalski, Jeznach, & Tuokko, 2014)) or have been
simplistic and did not add much to our understanding of the driving regulation
process (e.g. (Kostyniuk , Shope, & Molnar, 2001)).
This program of research addressed this significant gap in the older drivers’
literature, the lack of a theoretically-informed model of driving self-regulation that
takes into account the stages of change. The current chapter starts by discussing the
road safety issues related to the older driver and outlines the research background
which inspired this research program (1.2). Section (1.3) presents the aim and

2 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
objectives of the research program. The significance of the study is presented in
section (1.4). Section (1.5) presents the scope of the research and the thesis outline is
presented in section (1.6).
1.2 BACKGROUND AND RATIONALE FOR THE RESEARCH PROGRAM
The older driver
There has been a growing interest in extending the safe mobility of older
adults, given the ageing of our population (Lang, Parkes, & Medina, 2013). Mobility
is critical for the quality of life and well-being of older adults. While mobility can be
achieved through different forms of public and private transportation, driving is the
easiest, most accessible and most common form of transport for people of all ages
(Oxley & Whelan, 2008). Drivers aged 65 years and above are the fastest growing
segment of the driving population in Australia and around 60% of those aged 75
years and above hold a driver license (Bureau of Infrastructure, Transport and
Regional Economics,2014).
The baby boomers (born 1946-64 in a post-war boom in births) rely heavily on their
private cars and driving is their preferred mode of transport (Buys, Snow, Van
Megen, & Miller, 2012). Baby boomers are significantly active, making more trips
than previous generations (Currie & Delbosc, 2010), relying more on their cars and
less on public transport (Alsnih & Hensher, 2003). Over the last decade, older
Australian drivers have increased their annual vehicle kilometres driven by an
estimated 18% (Bureau of Infrastructure, Tranpsort and Regional Economics, 2014).
Older adults view driving as key to their independence and mobility (Adler &
Rottunda, 2006; Musselwhite & Haddad, 2010a). Driving is described by some as a
symbol of identity (Eisenhandler, 1990), independence (Persson, 1993), and security
(Bauer, Kuskowski, Rottunda, & Adler, 2003). The decision to stop driving is one of
the most difficult decisions older adults have to make (Adler & Rottunda, 2006).
Restricting or stopping driving can be associated with feelings of regret and
loneliness (Johnson, 1999), increased risk of depression (Ragland, Satariano, &
MacLeod, 2005), isolation (Fonda, Wallace, & Herzog, 2001), decreased out-of-
home activities (Marottoli, Carlos, Glass, Williams, & et al., 2000), and increased
risk of entering long-term care facilities (Freeman, Gange, Munoz, & West, 2006).

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 3
Stopping driving has also been linked to increased risk of dying (Edwards, Perkins,
Ross, & Reynolds, 2009).
The cessation of driving and subsequent loss of mobility will even have greater
impact in subgroups of the older population such as rural drivers and women. Older
women drivers are over-represented in fatal crashes compared to older men due to
their increased fragility (Oxley, 2010). The future cohort of older women will rely
more on their private cars and may be more reluctant to give up driving compared to
current and past generations (Rosenbloom, 2009). Older women have a higher
disability rate than men of similar age (Alsnih & Hensher, 2003) and may require
more assistance to maintain their mobility needs. With the increasing number of
older women living alone (Siren, 2004), it is expected that cessation of driving
among this age group will have drastic consequences (Siren Hakamies-Blomqvist, &
Lindeman, 2004). As women are starting to resemble men in terms of education and
employment, their driving experience and their attitude towards driving may start to
resemble that of men (Rosenbloom, 2006). Driving will become an integral part of
their identity, and similar to men, it will be the key to their freedom and
independence (Rosenbloom & Herbel, 2009).
Driving is a complex task that requires dynamic interaction between various
cognitive, physical, and sensory functions (Anstey, Wood, Lord, & Walker, 2005).
Ageing is associated with declines in these abilities (Anstey et al, 2005) and
increased prevalence of poorer health and medical conditions that can compromise
driving performance (Marshall, 2008). If unable to compensate for these changes,
older drivers may put themselves and others at risk (Freund, Colgrove, Burke, &
McLeod, 2005; Marottoli & Richardson, 1998). There is great diversity in the way
older adults experience the physiological and pathological declines associated with
ageing and how this affects their driving abilities (Langford & Koppel, 2006). Age
alone is a poor predictor of fitness to drive (Donorfio, D'Ambrosio, Coughlin, &
Mohyde, 2008)). Therefore, chronological age should not be used as a criteria to
restrict people from driving (Yassuda & Wilson, 1997).
As a group, older drivers are relatively safe drivers (De Raedt & Ponjaert-
Kristoffersen, 2000a; Eberhard, 1996). However, when distance driven is taken into
account, older drivers are over-represented in crashes when compared to middle-aged
drivers (King, Soole, Watson, & Schramm, 2011). This could be attributed to the

4 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
low-mileage bias, that is, driving shorter distances is associated with greater crash
risk regardless of age (Janke, 1991). Increased crash risk seen in low-mileage drivers
is often the result of the location of driving (e.g. urban areas with increased incidence
of challenging traffic situations) (Langford et al., 2013). Recent findings from the
Candrive/Ozcandrive study has shown that low- mileage drivers did considerably
poorly on a variety of performance measures compared to other drivers (Langford et
al., 2013). However, the findings should be interpreted with caution given that the
study relied on self-reported measures of driving which fails to provide an accurate
reflection of the actual driving behaviours of older drivers. In fact, the unreliability
of the subjective exposure measures used in majority of previous studies affect the
credibility of the “low-mileage bias” (Staplin, Gish, & Joyce, 2008). In 2015, Coxon
and colleagues examined the association between age, function and driving exposure
using objective measures in a large sample of 380 drivers aged 75 years and above.
The study found that older people with poorer function drove fewer kilometres per
week and took shorter trips closer to home. However, the study was conducted for
one week only, which is a relatively short time to capture usual driving practices (
Coxon et al., 2015). Without objective measures of driving exposure, it is difficult to
determine if increased crash involvement among older drivers reflects low-mileage
drivers.
Older drivers are more likely to be injured or killed if being involved in a
crash compared to younger or middle-aged drivers (King et al., 2011). In fact, the
consistent reduction in the fatalities among younger drivers over the past decade has
not been observed among older drivers in Australia (Fig 1.1) (Bureau of
Infrastructure, Transport and Regional Economics, 2014). On average, 250
Australians aged 65 and above die and another 4000 are hospitalised due to road
crash injuries each year (Bureau of Infrastructure, Transport and Regional
Economics, 2014). Between 2008 and 2013 annual deaths from crashes involving an
older driver increased by an alarming 17 percent (Bureau of Infrastructure, Transport
and Regional Economics, 2014). This over-representation in serious and fatal
crashes is mainly attributed to older adults’ fragility (Meuleners, Harding, Lee, &
Legge, 2006) due to their reduced bone strength and fracture tolerance (Guest,
Boggess, Viljoen, Duke, & Culvern, 2014). In 2003, Li and colleagues examined the
association of frailty (measured as risk of dying in the event of a crash) and increased

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 5
fatal crash involvement among different age groups, with the quantity of exposure to
vehicle travel being controlled for. Their findings showed that fragility was a
substantial determinant of the increased risk per unit of travel among older drivers
(60 years or older) (Li, Braver, & Chen, 2003). Another study conducted in 2008
revealed that when compared to middle-aged drivers, those 85 years and older have
an eight times higher mortality risk per mile travelled but pose only 1.5 mortality risk
to others (Tefft, 2008).
Regardless of the reason for older drivers’ over-representation in fatal
crashes, reducing the personal and societal impact of older drivers’ crashes is a
public health priority.
Figure 1.1 Annual fatalities: road user type within age groups.
Source (Bureau of Infrastructure, Tranpsort and Regional Economics, 2014)

6 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Figure 1.2: Annual number of fatal crashes
Source (Bureau of Infrastructure, Tranpsort and Regional Economics, 2014)
Initiatives to maintain older drivers’ safety
Since driving will continue to be the main source of mobility for older
people, it is important to ensure the safety of older drivers and other road users.
Identifying high-risk older drivers is problematic given that driving is a complex task
that relies on a wide range of abilities. Up until now, there is very limited evidence
to support the use of off-road screening batteries in assessing older adult’s fitness to
drive (Wood, Anstey, Kerr, Lacherez, & Lord, 2008). Much research is needed to
determine the ideal battery of tests to be used that can detect fitness to drive while
ensuring reliability and validity (King et al., 2011). Efforts to monitor older drivers
through age-based mandatory testing have failed to show any safety benefits (Lang et
al., 2013 ; Langford & Koppel, 2006). On the contrary, mandatory age-based testing
may cause older drivers to restrict their driving prematurely with the subsequent
early loss of mobility (Siren & Haustein, 2015; Whelan, Langford, Oxley, Koppel, &
Charlton, 2006).
The adverse consequences associated with driving cessation calls for
strategies that balance older adults’ safety and mobility needs. Further, since older
drivers pose greater risk to themselves than to others, they have the right to play an
active role in the decision-making process (Langford & Koppel, 2006). Considerable

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 7
attention has therefore been directed towards other strategies that can increase older
drivers’ safety without compromising their mobility.
Planning the decision to stop driving can help overcome some of the negative
aspects of driving cessation (Musselwhite, 2013). While uncommon, driving
cessation can occur unexpectedly as a result of sudden illness, involvement in an
accident, or failing a driving test (Dellinger, Sehgal, Sleet, & Barrett-Connor, 2001).
However, driving cessation is more of a gradual and voluntary process whereby the
driver will gradually increase self-imposed restrictions or reduce their driving until
ultimate cessation (Dellinger et al., 2001; Hakamies-Blomqvist & Wahlström, 1998).
These modifications in driving behaviour, prior to driving cessation, are known as
driving self-regulation. Driving cessation is sometimes viewed to be the end result
of the process of self-regulation among older drivers (Dellinger et al., 2001; Lyman,
McGwin Jr, & Sims, 2001).
Self-regulation of driving has been promoted as an alternative positive
approach to keep older adults driving safely for longer (Lang et al., 2013 ). Self-
regulation refers to efforts to modify thoughts, emotions, needs, and actions to reach
higher long-term goals (Ridder & Wit, 2006) . In the context of driving, it refers to
modifying one’s driving behaviours to reduce and/or eliminate crash risk. It is
defined as “the adjustments made by drivers in their driving behaviour that
adequately match changing cognitive, sensory and motor capacities” (Charlton et al.,
2006) which largely depends on the individual’s ability to monitor his/her driving
ability (Anstey et al., 2005). Common examples of self-regulation seen in older
drivers include reducing their overall amount of driving and avoidance of various
driving situations (e.g. avoiding driving at night or peak hours, travelling shorter
distances) (Anstey & Smith, 2003; Baldock, Mathias, McLean, & Berndt, 2006a;
Charlton et al., 2006).
Recently, Molnar and colleagues (2013) have expanded this definition to
include three levels of self-regulation. Strategic self-regulation involves the decisions
made by drivers prior to taking the trip and involves general planning such as
avoiding difficult driving situations or selecting certain driving routes. Tactical self-
regulation involves the decisions made by drivers while they are on the road, such as
gap and headway acceptance, speed choice, and overtaking. Life-goal level of self-
regulation involves the broader decisions made by older drivers in their lives such as

8 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
the choice or what kind of car to drive which can have an indirect but a long-term
impact on their driving future.
Self-regulation and actual crash risk
There are multiple risk factors associated with motor vehicle crashes among
older drivers which makes it difficult to determine if self-regulation is indeed
effective in reducing crashes among this age group (Horswill, Anstey, Hatherly,
Wood, & Pachana, 2011). The relationship between self-regulation and actual crash
risk is still poorly understood. Growing evidence suggests that self-regulation may
show promise in decreasing crash risk among older drivers (Keay et al., 2013).
Anstey et al. (2006) assessed 1446 older drivers aged 70 and above on several visual,
cognitive and functional measures and followed them for five years (1992-1997).
They found that the factors associated with driving cessation were similar to those
associated with increased crash risk in older adults. This could indicate that older
adults with impairments reduce their risk of crash by modifying their driving
behaviour (Anstey, Windsor, Luszcz, & Andrews, 2006). Keay et al., 2013 pointed
out that recent epidemiological results, based on the findings from the North
American Fatality Analysis Rating System, support the use of self-regulation to
increase older drivers’ safety (Keay et al., 2013). Individuals who drive in daylight
and individuals with a history of motor vehicle conviction were less likely to be
injured in a crash probably as these individuals recognise their limitations (Keay et
al., 2013).
Mandatory age-based testings have failed to result in crash reduction among
older drivers. This can be partly explained by the fragility bias discussed before.
Older drivers’ over-representation in fatal crashes is mainly attributed to their
fragility not to their driving abilities or skills (Langford & Koppel, 2006). Age-based
testings are restrictive policies that can result in unnecessary restrictions on older
adults’ mobility. The adverse consequences of driving cessation noted above calls
for strategies that can manage older adults’ safety and mobility needs. Self-
regulation shows promise as an approach that can help older drivers achieve that. It
allows older drivers to be involved in the decision-making process, which can
improve the outcome through better adaptation and planning. In addition, it
accommodates the diversity and heterogeneity of older drivers’ population in terms
of their abilities, resources, and needs. As mentioned before, it is not age perse, but

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 9
rather the associated pathological and psychological declines that compromise the
driving performance. Given that older adults vary considerably in the way they
experience these declines, there is a need for a more “adaptive” strategy that can
accommodate such diversity.
Successful self-regulation
The success of self-regulation, in terms of driving safety, is greatly influenced
by the ability of older drivers to have insight into their declining driving
performance, the accuracy of their insight, their willingness and ability to respond to
this insight, and the effectiveness of their responses (Anstey et al., 2005). Those who
are unaware of limitations in their driving abilities may engage in risky behaviours
that compromise their safety and the safety of others (Marottoli & Richardson,
1998). In addition, older drivers who are aware of declines in their abilities are more
likely to practice self-regulation than those who are less self-aware (Blanchard &
Myers, 2010; Holland & Rabbitt, 1992).
Unfortunately, the changes associated with ageing are usually subtle and older
people may not be aware of how these changes affect their driving abilities. In
addition, driving errors and violations will not necessarily result in crashes or
penalties and drivers may fail to develop an accurate estimation of their abilities
(Dogan, Steg, Delhomme, & Rothengatter, 2012). Should an incident take place, the
driver may not understand why it occurred and how to prevent it in the future (Dogan
et al., 2012). Even if one becomes aware of the need to change, motor vehicle
crashes are rare events, which may not create a sense of urgency, and other health
and life goals may be perceived as more important. Driving self-regulation may in
fact be viewed as a negative behaviour that can impair one’s mobility and
independence. Achieving driving self-regulation for individual older drivers is
therefore complicated and could require extensive deliberation about the pros and
cons and persuasion by influential people such as family members and medical
practitioners. To make matters worse, the strategies and behavioural changes needed
to achieve optimal driving self-regulation, in terms of reducing crashes, are not
clearly defined. It is difficult for older adults to determine which modifications in
their driving behaviours compensate for the loss of certain abilities and subsequently
translate into improved safety. Lack of adequate support and feedback can influence
older people’s ability to make an informed decision about the future of their driving.

10 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
This can result in some older people stopping driving prematurely while other
continues to drive where it is not safe to do so (Berry, 2011).
Gaps in the current literature
For the past forty years or so, a large body of studies have investigated the
process of self-regulation among older drivers. While it is often promoted as a
promising initiative to maintain older drivers’ safe mobility, there are some
significant gaps in the literature related to older drivers’ self-regulation (Molnar et
al., 2015). Driving avoidance and/or reduction is not always related to driving
abilities. Existing evidence indicate that some older adults reduce and/or restrict
their driving for reasons such as retirement, preference, or financial constraints
(Blanchard & Myers, 2010; Meng & Siren, 2012) which should not be regarded as
driving self-regulation.
As it is widely endorsed by road safety researchers as a positive strategy, it is
important to understand the factors that influence some older adults to modify their
driving behaviours. This in turn will assist in the development of interventions that
encourage older drivers to appropriately self-regulate their driving. Previous studies
have identified a large number of factors associated with self-regulation, still, how
these factors come together in the final decision remains unclear. As Molnar and
colleagues (2015) highlight “it is important to extend the current research by trying
to tease out the relationships between self-regulation and the factors for which there
is already considerable evidence” and there is a need “for a more comprehensive,
theoretically-informed, and uniform approach to investigating self-regulation by
older drivers”.
Few studies have attempted to find a theoretical framework to account for the
process of self-regulation in older adults. The challenge in developing a model of
driving self-regulation results from the heterogeneity of the older driver population in
terms of their abilities, needs, and resources. There is a need for a model of self-
regulation that can describe the complexity inherent in diversity of needs, abilities
and resources among older people. Previous studies have pointed out that older
drivers go through different stages of change towards modifying their driving and
ultimately stopping driving (Kostyniuk , Trombley, & Shope, 1998). The stages of
changes theories could be useful in describing and providing a general understanding
of change and planning interventions (Liddle, Carlson, & McKenna, 2004). This

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 11
suggests that older driver interventions might need to be tailored to the specific needs
of each individual (including the stage they are at) and would need to be customised
to move individuals through the stages of change towards adoption of safe driving
behaviour. They would ideally be developed by taking a strategic approach using
both a theory of the change process and existing evidence from previous attempts to
achieve change. However, there has been little development of stage-based theories
applied to driving self-regulation, and hence there is a lack of research on
theoretically-informed interventions that facilitate older drivers’ planning for future
self-regulation and even driving cessation. There is also a lack of consideration of the
role of feedback about behaviour in the stage process, such as responsiveness to
feedback, acceptable sources of feedback, and ability to modify behaviour in relation
to feedback.
Previous studies examining older drivers’ behaviour within stages of change
framework have either relied entirely on qualitative findings without further
validation (e.g. (Kowalski, Jeznach, & Tuokko, 2014)) or have been simplistic and
have therefore not added much to our understanding of the driving regulation process
(e.g. (Kostyniuk , Shope, & Molnar, 2001)). Kowalski and colleagues (2014)
examined older driver behaviour within the Transtheoretical (TTM) framework using
interviews/focus groups with current and former older drivers (Kowalski et al.,
2014). The TTM assumes that health behaviour change involves six stages: pre-
contemplation, contemplation, preparation, action, maintenance, and termination
(Prochaska & Velicer, 1997). A major limitation of the TTM is that it fails to
distinguish between people who are unaware of the risk and those who have decided
not to act. In the TTM as applied to older drivers, it is not clear whether individuals
in the pre-contemplation stage (the non-changers) are aware of their declining
abilities but refuse to modify their driving or are simply unaware. It is likely those
who are aware but refuse to change will not progress through stages of change
similarly to those who are unaware, and therefore that these groups will require
different types of interventions. Older drivers who resist change may not benefit
from traditional behavioural interventions and may be more reluctant to seek
feedback. Furthermore, the focus of the TTM is on changing an existing behaviour
(driving), whereas a focus on driver self-regulation involves an important but subtle

12 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
difference: it is about the adoption of a precaution which is expected to play a role in
later behaviour change.
The literature suggests that self-awareness and insight into driving ability
play a major role in successful driving regulation among older drivers (Anstey et al.,
2005). Therefore, older drivers need to perceive their declining driving abilities as a
threat to their overall safety before they are interested in self-regulation. This
situation is better suited to the application of the Precaution Adoption Process Model
(PAPM) to the self-regulatory behaviours of older drivers, which has been examined
by Kostyniuk et al. (2000). The PAPM (Figure 1.3) describes how individuals move
through stages of change towards adoption of health protective behaviour (Weinstein
& Sandmand, 2002). The early stages of the PAPM are defined in terms of
psychological states and mindset of individuals (Weinstein & Sandmand, 2002). The
later stages are mostly governed by factors that can facilitate or hinder the adoption
of the precaution. Individuals progress through seven stages from lack of awareness
to action: unawareness (stage 1); awareness that there is an issue but a lack of
personal engagement with it (stage 2); engagement (“this applies to me”) but
indecision (stage 3) about the need to act; either a decision not to act (stage 4) or a
decision to act (stage 5); if the latter, acting by taking the precaution (stage 6) (e.g.
self-regulating); and maintaining the behaviour (stage 7). A fuller account is given
in Chapter 3.
Figure 1.3: Stages of the Precaution Adoption Process Model From Health behaviour and health education (p. 127) by Glanz, K. et al., 2008,
Wiley, ProQuest Ebook Central

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 13
The PAPM does not offer explicit details about the barriers and facilitators at
each stage which allows for a more flexible framework that can be adapted to suit
each behaviour uniquely (Weinstein, Sandmand, & Blalock, 2008). Kostyniuk et al.
(2000) hypothesised that predicting problems in one’s driving ability is a key factor
in initiating the driving reduction and cessation process and investigated the impact
of older adults’ anticipation of driving problems on their driving reduction and
cessation by conducting a survey study among 1,053 older drivers and former drivers
over the age of 65. Their findings suggest that the awareness and anticipation of
limitations in driving ability may be the key factor for reducing and/or stopping
driving, which provides further support to the use of PAPM. Unfortunately, their
model failed to recognise the influence of other external and internal factors on the
process of self-regulation. Their model is therefore descriptive and does not provide
a clear idea of the factors that facilitate transition between stages and is not useful in
developing interventions.
Purpose of this study
The applicability of the PAPM to the examination of driving behaviours
among older adults deserves consideration. An attractive feature of this model is that
it deals with both the hazard and the precaution. It claims that for individuals to
consider adopting a precaution they must first perceive the hazard to be of sufficient
personal relevance. The age-related declines in people’s sensory, motor, or cognitive
functions are often subtle and gradual which can make it difficult for older people to
draw the link between these changes and the impact on their driving ability.
Therefore, the early stages of the PAPM emphasise the importance of increasing
people’s awareness about the impact of ageing on their driving ability. While it is
highly likely that older drivers are “generally aware” about the safety issues of older
drivers, they could lack “self-awareness” or insight into their own driving ability.
Once they become personally engaged with the hazard, people are more likely to be
more receptive towards adoption of the precaution and interventions should be
directed towards overcoming barriers of adopting self-regulation, promoting
alternative transport options, and improving the driving cessation outcomes. It also
differentiates between those who are unaware of the hazard and have never thought
about acting and those who have thought about acting and are still undecided (unlike
the TTM which groups them as the pre-contemplators). This differentiation is

14 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
important because those who have thought about acting are more likely to be more
knowledgeable, have different responses to information and are more resistant to
persuasion (Ditto & Lopez, 1992). By adapting the PAPM to address older adults’
self-regulatory driving behaviours, older drivers can be categorised into several
distinctive profiles as shown in Table 1.1. Interventions that promote successful self-
regulatory practice will vary according to the different stages of the PAPM.
Table 1.1: Adaptation of the PAPM to the older drivers’ regulatory behaviours
Stage Profile Characteristics
Stage 1 The
unaware
Generally unaware of the impact of age-related declines
on one’s driving abilities OR unaware of the self-
regulatory practices to reduce one’s risk of crash
Stage 2 The
unengaged
Generally aware of the problem but do not recognise the
changes in their own abilities and/or never thought about
the adoption of self-regulatory practices
Stage 3 The
undecided
Aware of changes in their own abilities but are either
unsure how it impacts their driving or how they should
modify their driving accordingly
Stage 4 The resister Thought about it but refused to either acknowledge the
need to modify their driving behaviours or unable to
modify their behaviours
Stage 5 The planner Thought about it and starting to monitor their driving and
plan to change their driving accordingly
Stage 6 The
regulator
Have started to reduce and/or avoid certain driving
situations in response to their declining abilities
Stage 7 The non-
driver
Have stopped driving altogether in response to their
declining abilities

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 15
1.3 RESEARCH AIMS
This research aims to contribute to the development of a theoretical
framework for a stage-based process leading to self-regulation of driving which
incorporates the role of feedback. This research program builds on the previous work
of Kostyniuk and colleagues (2000) by further examining the applicability of the
PAPM in understanding older adults’ self-regulatory driving behaviour. This aim is
addressed through the following specific objectives:
1. To explore the preliminary fit of older adults’ driving behaviour within the
PAPM framework using qualitative focus groups among current older drivers.
This is an assessment of the in-principle applicability of the PAPM.
2. To develop a conceptual model based on the PAPM that profiles older adults
into distinctive groups based on their mindsets towards self-regulatory driving
behaviours. An operationalisation of the PAPM for older drivers and their
adoption of self-regulation as a precaution.
3. To determine the prevalence of PAPM stages in a sample of older drivers and
identify the socio-demographic and psychosocial characteristics of stages
membership. An exploration of the application of the model stages in a sample
of older drivers.
4. To identify self-regulation profiles among older drivers based on their mindset
towards change using Latent Class Analysis (LCA) and determine the similarity
with the conceptual model. A test of whether the stages identified by the PAPM
reflect the underlying clustering of mindsets.
5. To examine the impact of providing one-on-one feedback regarding driving
performance on stage transition among a sample of older drivers and its impact
older drivers’ perception of the quality of their driving and their willingness to
modify their driving behaviour. A “real world” examination of the potential role
of feedback in contributing to progression through the stages of the PAPM.

16 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
These objectives are addressed through two stages comprised of three studies
with specific research questions (Figure 1.4; details presented in Chapter 4). The
first stage of the research employs an exploratory sequential mixed-method design.
Study 1, a qualitative study which examines the applicability of using the PAPM as a
framework for describing self-regulatory behaviours with a focus on the role of
feedback on the self-regulatory decision-making process. The findings from study 1
inform the development of a preliminary model of self-regulation. Study 2 is a
quantitative study that involves a survey (web-based and paper-based) of older
drivers. The analysis of study 2 is divided into two phases. Phase 1 aims to build on
the previous research by investigating whether a sample of older drivers can
accurately be assigned to the stages of the PAPM and to identify the psychosocial
and environmental factors associated with different stages of the PAPM. Phase 2
utilises a bottom-up approach to profile older drivers based on their mindset towards
adopting self-regulatory driving behaviours using Latent Class Analysis in an
attempt to empirically test the preliminary model. The preliminary model is then
refined and modified based on the findings from the LCA. Stage 2 is comprised of
study 3, an experimental study that assesses the impact of providing participants with
customised feedback on stage transitions and their intention to modify their driving
behaviours accordingly.
Figure 1.4: Stages of the program of research

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 17
1.4 SIGNIFICANCE OF THIS STUDY
The findings from this research program will:
• Contribute to the understanding of the older adults’ driving
experience, and the self-regulatory driving behaviour among older adults,
the decision-making process, and the facilitators and barriers to adopting
self-regulatory behaviours.
• Contribute to the understanding of older drivers’ perceptions and
experiences regarding receiving feedback about their driving abilities. Little
is known about the nature and content of feedback older drivers are
currently receiving about their driving and what type of feedback is
considered important to the older driver. Furthermore, it is still unclear
what would be the most effective way of delivering feedback to older
drivers to encourage them to modify their driving behaviour.
• Contribute to the literature on a theoretical level by developing a
framework of driving self-regulation based on the PAPM.
1.5 DEMARCATION OF SCOPE OF THE RESEARCH PROGRAM
The current research program focuses on the behavioural aspect of adopting
self-regulation and does not investigate the impact of improvements in road
infrastructure, vehicle standards/equipment, or in-vehicle technology on older adults’
safety. Even though Queensland (where respondents were sampled) has specific
licensing requirements for older drivers, this research does not address the
Queensland driver licensing system. Similarly, the research does not examine older
driver crashes or their contributing factors. Instead, it focuses on the psychological
and contextual influences on older driver self-regulation, an issue of common interest
across jurisdictions.
1.6 THESIS OUTLINE
The thesis outline is given in Figure 1.5. Chapter 1 provides an overview of
the research background, rationale, aims and objectives, and outlines the research
program. Chapter 2 reviews the literature on older driver safety and the current

18 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
interventions and strategies employed to address the problem. It identifies gaps in
current knowledge which inform the research questions underpinning the program of
research. Chapter 3 reviews the existing models of older adults’ driving behaviours
and the justification for choosing the PAPM as the underpinning theoretical
framework for this program of research. Chapter 4 provides an overview of the
research design of the thesis and briefly describes the methodology of the three
studies.
This is a thesis by publication, which contains two published journal articles
and a journal article currently under review. Chapter 5 presents the first published
study which describes Study 1 that involved focus groups with current older drivers
and how the findings resulted in the development of a conceptual model that partly
informed the direction of Study 2. Chapter 6 represents the second published article
which describes Phase 1 of Study 2 that involved a quantitative survey of current
older drivers for the investigation and the refinement of the conceptual model.
Chapter 7 represents the third article (on Phase 2 of Study 2) which is currently under
preparation and describes the findings from a Latent Class Analysis. Chapter 8
presents Study 3, an unpublished paper, which examines the usefulness of the model
by investigating the impact of customised feedback on moving people through
stages. Chapter 9 synthesises the results from the three studies and presents a
summary of the findings, discusses the limitations and strengths of this analysis and
provides recommendations for future research and clinical practice.
1.7 CHAPTER SUMMARY
This chapter presented the background to the current research and the specific
aims and research questions that this research program addresses. The expected
increase of the number of older drivers calls for urgent solutions that can maintain
their safe mobility. Previous studies indicate that self-regulation could be a
promising strategy to maintain older adults’ safe driving. However, little attention
has been directed towards developing a model that can enhance our understanding of
this complex process. This program of research adopts a unique approach by
examining the application of the PAPM in improving our understanding of the self-
regulatory driving behaviours among older adults. This improved knowledge can
assist in the developing of customised interventions that can help older drivers

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 19
accurately and successfully regulate their driving (i.e. without imposing unnecessary
restrictions or driving when it is no longer safe to do so).
Figure 1.5: Overview of thesis chapters
Chapter 1
Introduction and study background
Chapter 2
Literature review
Chapter 3
Theoretical approach
Chapter 4
Research design and methodology
Chapter 5
Paper 1 (published paper)
Chapter 6
Paper 2 (published paper)
Chapter 7
Paper 3 (under review)
Chapter 8
Draft research paper
Chapter 9
Synthesised discussion of research findings

20 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Chapter 2: Literature Review
2.1 INTRODUCTORY COMMENTS
This chapter provides a review of the current literature on older drivers’ safety
and mobility issues with a focus on the existing countermeasures that attempt to
maintain older adults’ safe driving. The chapter starts by outlining the road safety
implications of the growing number of older drivers and the need to balance their
safety and mobility. The current approaches to older drivers licensing are discussed.
Next, the chapter provides an overview of the process of self-regulation and the
factors associated with self-regulatory behaviours among older drivers. The current
strategies and challenges of promoting successful self-regulation are also presented.
Finally, the chapter summarises the literature and concludes by identifying the
research gap from which the research questions are derived.
2.2 GROWING NUMBER OF OLDER DRIVERS
The ageing of the baby boomers along with the increased life expectancy of
successive generations will result in major changes in Australia’s demographic (
King et al., 2011). In 2007, 13% of the population were aged 65 years or more
(ABS, 2008). By the year 2030, it is expected that adults aged 65 years and more
will comprise 23% of the Australian’s population (Rakotonirainy, Steinhardt,
Delhomme, Darvell, & Schramm, 2012) and the proportion of adults aged 85 years
or more will rise from 1.6% of the population in 2007 to 7.3% by 2056 (ABS, 2008).
These significant changes in the population structure will provide new
challenges to road safety researchers (Alsnih & Hensher, 2003). First, the proportion
of drivers aged 65 years and above continues to be the fastest growing part of the
driving population (Ball et al., 2006; Wang & Carr, 2004). Second, a larger
percentage of older adults retain their driving license (Hakamies-Blomqvist &
Henriksson, 1999) and continue to drive much longer and for greater distances
compared to previous generations (Braitman & McCartt, 2008; Owsley, McGwin,
Phillips, McNeal, & Stalvey, 2004; Wang & Carr, 2004). Third, the mobility and
transportation needs for the baby boomers are distinctively different to those of
previous generations. Baby boomers are predicted to be significantly active, making

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 21
more trips than previous generations (Currie & Delbosc, 2010), relying more on their
cars and less on public transport (Alsnih & Hensher, 2003). This dependence on the
private automobile will result in unfavourable consequences when it is time to give
up the car keys and retire from driving (Buys, Snow, van Megen, & Miller, 2012).
2.3 THE IMPORTANCE OF DRIVING
Older people now have greater access to cars and their private automobiles are
their principal and favourable form of transport (Molnar & Eby, 2009). The majority
of older drivers view driving as key to their independence and mobility (Adler &
Rottunda, 2006; Musselwhite & Haddad, 2010a). Driving is described by some as a
symbol of identity (Eisenhandler, 1990), independence (Persson, 1993), and security
(Bauer, Kuskowski, et al., 2003), so the decision to stop driving is one of the most
difficult decisions older adults have to make (Adler & Rottunda, 2006).
Qualitative evidence has shown that older adults describe the idea of stopping
driving as traumatizing (Whelan et al., 2006). Driving is convenient and flexible
(Burkhardt, McGavock, & Nelson, 2002) and giving up driving can limit people’s
mobility and leave them feeling socially isolated (Coughlin, 2001; Eisenhandler,
1990). Further, driving is often described as an enjoyable activity by older people
(Burkhardt et al., 2002) and the negative aspects of driving are often attributed to
external factors such as behaviours of other drivers (Burkhardt et al., 2002; Yassuda
& Wilson, 1997) or financial cost associated with driving (Burkhardt et al., 2002).
Restricting or stopping driving can be associated with feelings of regret and
loneliness (Johnson, 1999), increased risk of depression ( Ragland et al., 2005),
isolation (Fonda et al., 2001), decreased out-of-home activities (Marottoli et al.,
2000), and increased risk of entering long-term care facilities (Freeman et al., 2006).
Stopping driving has also been linked to increased risk of dying. In a prospective
cohort study among 660 older adults aged 63 and above, non-drivers had an
increased mortality risk compared to drivers (Edwards et al., 2009). In a larger study
(n = 2,793), risk of dying was 1.68 times higher for non-drivers compared to drivers
(O'Connor, Edwards, Waters, Hudak, & Valdes, 2013), however, health problems
mediated this association (O'Connor et al., 2013).

22 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
2.4 TRANSPORTATION ALTERNATIVES
The availability of other transport options (Coughlin, 2001) and the cost of
public transport (Corpuz, 2007) have been identified as important factors in the
decision to give up driving among older adults. In fact, some older drivers may
continue to drive despite being aware of their declining ability to avoid the use of
alternative transports (Atkin, 2001). In a recent study conducted by Buys et al.
(2012), among a sample of 24 older adults in Queensland, the private automobile was
considered to be the most convenient mode of transport among participants
regardless of the availability of public transportation (Buys et al., 2012). As Buys et
al. (2012) points out, the convenience and ease offered by the car may act as an
important barrier to the use of alternative transport options among older drivers. In
addition, psychological barriers (e.g. feeling a burden, fear for safety) (Taylor &
Tripodes, 2001), geographical barriers (e.g. availability of alternative transport or
social support) (Musselwhite & Haddad, 2010b), and lack of knowledge (Peel,
Westmoreland, & Steinberg, 2002) can affect the usage of these alternatives.
Overall, older drivers often view public transportation to be costly, unreliable,
unsafe, and difficult to access (Allan & McGee, 2003; Gardezi et al., 2006). Older
adults often view taxis as an expensive form of transportation and report concern
over their personal safety (Oxley, Charlton, & Fildes, 2003). Qualitative evidence
suggests that former drivers prefer rides from others for their transportation and
mobility needs (Burkhardt et al., 2002) as it gives them a sense of closeness with
their family (Musselwhite & Shergold, 2013). However, they often express concerns
about the fear of becoming a burden (Bonnel, 1999). This is supported by the
research conducted by Bauer et al. (2003), where many of the women who
participated in the study used formal transit services regularly to maintain their
independence and freedom (Bauer, Rottunda, & Adler, 2003). Although transit
services did not provide them with the same freedom or flexibility they had when
driving, they valued the sense of “selectivity and decision-making involved in using
them” (Bauer, Rottunda, et al., 2003).
Shifting to a new transportation option requires active planning (Shergold,
Parkhurst, & Musselwhite, 2012) and people are not very keen on obtaining
information about alternative transport options (Nordfjærn, Şimşekoğlu, & Rundmo,
2014) especially if they do not consider they need such information (Shergold et al.,

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 23
2012). An interesting solution provided by Musselwhite & Shergold (2013)
emphasises the need to promote the use of alternative modes of transport throughout
life or at least from a much younger age. This gradual introduction of alternative
transport options might help eliminate the psychological barriers associated with
their use (Musselwhite & Shergold, 2013).
2.5 FACTORS ENABLING DRIVING SAFETY AMONG OLDER DRIVERS
Safe driving requires a dynamic interaction between different sensory,
cognitive and motor abilities. As people start to age, they may experience decline in
these abilities (Holland & Rabbitt, 1992). This is often caused by the increased
prevalence of health problems with ageing and the medications used to treat these
conditions but can also be seen with normal ageing (Anstey et al., 2005). If unable to
compensate for these changes, older drivers may put themselves and others at risk
(Freund et al., 2005). There is an extensive body of research that explains the link
between age-related declines among older drivers and higher risk of at-fault crash
involvement (Staplin, Lococo, Martell, & Stutts, 2012).
Anstey, Wood, Lord, and Walker (2005) presented a model of driving safety
in older adults (Figure 2-1) which consists of two main factors: driving capacity and
self-monitoring and beliefs about driving. Driving capacity is determined by
cognition, sensory, and physical function (Anstey et al., 2005). Self-monitoring
beliefs refers to the ability to evaluate one’s driving ability, and adapt driving
behaviours accordingly (Anstey et al., 2005). Therefore, older drivers’ insight into
their driving skill is crucial for accurate evaluation of their ability and accordingly
successful self-regulation behaviours. However, up until now, the relationship
between reduced fitness to drive and increased risk of crash is not fully understood.
The inconsistency in the measures used to assess the functional and cognitive
abilities among older drivers and the diversity in the driving outcome measures used
in previous studies makes it rather difficult to establish a clear and a consistent link
between a certain functional ability, driving performance and increased crash risk.

24 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Driving Behaviour
Self-monitoring and beliefs about driving
capacity Capacity to drive safely
Cognition Vision Physical function
Figure 2.1: Multifactorial model of factors enabling safe driving among older drivers
From “Cognitive, sensory and physical factors enabling driving safety in older
adults” by Anstey et al, 2005, Clinical Psychology Review 25, p. 60.
2.6 ARE OLDER DRIVERS A ROAD SAFETY PROBLEM COMPARED TO OTHER DRIVERS?
In Queensland, drivers aged 60 years and above are over-represented in fatal
and life-threatening crashes and their involvement increases steadily with age
(Rakotonirainy et al., 2012). Furthermore, drivers aged 80 years and above are most
likely to be at fault for injury or death-related crashes (Rakotonirainy et al., 2012).
However, the association between age and crash risk is highly complex (Cheung &
McCartt, 2011) and there is an ongoing debate about the risks older drivers carry to
themselves and to other road users in terms of crash involvement. Still, age is often
used as the basis of strict licensing conditions and assessment and it is therefore
important to determine if older drivers have an elevated crash involvement. As a
group, older drivers are relatively safe drivers and account for far fewer crashes
compared to other drivers (De Raedt & Ponjaert-Kristoffersen, 2000a; Eberhard,
1996). However, when distance driven is taken into account, older drivers are over-
represented in crashes compared to middle-aged drivers (King et al., 2011). Older

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 25
drivers are also more likely to be injured or killed if being involved in a crash
compared to younger or middle-aged drivers (King et al., 2011). Researchers debate
that methodological biases are the reason for this overestimation of older drivers’
involvement in crashes; particularly the fragility and the low-mileage biases.
The fragility bias
Due to their frailty, older drivers are over-represented in serious and life-
threatening motor vehicle crashes (Meuleners et al., 2006) and this involvement
increases steadily with age (Bédard, Guyatt, Stones, & Hirdes, 2001). This can be
attributed to reduced bone strength and fracture tolerance (Guest et al., 2014). Since
crash data mostly relies on reported incidents (Hauer, 2006), the increased likelihood
of being seriously injured or dying in a crash among older drivers may result in
increased rates of incident (Hauer, 2006). In 2003, Li and colleagues examined the
association of frailty (measured as risk of dying in the event of a crash) and increased
fatal crash involvement among different age groups, with the quantity of exposure to
vehicle travel being controlled for. Their findings showed that fragility was a
substantial determinant of the increased risk per unit of travel among older drivers
(60 years or older) (Li et al., 2003). Another study conducted in 2008 revealed that
when compared to middle-aged drivers, those 85 years and older have an eight times
higher mortality risk per mile travelled but pose only 1.5 mortality risk to others
(Tefft, 2008).
The low-mileage bias
Driving shorter distances is associated with greater crash risk regardless of age
(Janke, 1991). Therefore, the increased crash rate among older drivers could be
exaggerated due to the lower mileage driver (Hakamies-Blomqvist, Raitanen, &
O’Neill, 2002). Increased crash risk seen in low mileage drivers is often the result of
the location of driving (e.g. urban areas with increased incidence of challenging
traffic situations) (Langford et al., 2013). Recent findings from the
Candrive/Ozcandrive study has confirmed the association between low mileage and
increased crash risk among older drivers where low mileage drivers did considerably
more poorly on a variety of performance measures (Langford et al., 2013). However,
this study relied on self-reported measures of driving which does not provide an
accurate reflection of the actual driving behaviours of older drivers. In 2015, Coxon
and colleagues examined the association between age, function and driving exposure

26 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
using objective measures in a large sample of 380 drivers aged 75 years and above.
They found that older people with poorer function drove fewer kilometres per week
and took shorter trips closer to home (Coxon et al., 2015) However, the study was
conducted for one week which may be relatively short to capture usual driving
practices.
2.7 PATTERNS AND CHARACTERISTICS OF OLDER DRIVERS’ CRASHES
Older drivers have distinctive crash patterns compared to other age groups.
They are often responsible for their crashes (King et al., 2011; Stutts, 1998) and the
most common causes of their crashes are failure to see other road users, sudden
illness, or lack of awareness to traffic signal (King et al., 2011). The large part of
their crashes involves collisions with another vehicle (Langford, Andrea, Fildes,
Williams, & Hull, 2005) and is more likely to occur at intersections (Boufous, Finch,
Hayen, & Williamson, 2008). A recent study analysing Queensland crash data over
9 years period has revealed that drivers aged 60 and above are over-represented in
fatal and serious crashes and failure to give way crashes (Rakotonirainy et al., 2012).
The impact to the vehicle’s side commonly seen in intersection crashes coupled with
older adults’ fragility have been attributed to the more serious injury or greater death
rates among older drivers in intersection crashes (Morris, Welsh, Frampton,
Charlton, & Fildes, 2003). Older drivers have a small share of speed-related or
alcohol-related crashes (OECD, 2001) and their crashes rarely occur at night
(Langford et al., 2005), on weekends, in peak hour traffic, or in adverse weather
(OECD, 2001).
Interestingly, recent studies indicate that older drivers’ crashes are decreasing.
Cheung & McCartt (2011) analysed crash rates in the United States and revealed that
older drivers’ fatal crash risk has declined through with the greatest decline observed
among those aged 70 years or above (Cheung & McCartt, 2011).
2.8 CURRENT OLDER DRIVER ROAD SAFETY COUNTERMEASURES
The significant over-involvement of older adults in fatal and life-threatening
crashes has prompted the development and implementation of a variety of
countermeasures to promote their safe mobility. These countermeasures aim to

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 27
maintain safer older drivers on our road systems and to manage the mobility needs of
older drivers; they include:
1) Identifying high-risk older drivers and referring them to licensing
authorities for additional assessment (Langford & Koppel, 2006). The main
aim should be to manage their limitations and improve their skills so that they
can maintain their driving for as long as they can safely (Langford & Koppel,
2006). However, if considered unsafe and unfit to drive, resources should be
directed to improve their cessation of driving experience.
2) Encouraging the older drivers to self-monitor their driving and
self-regulate accordingly and to seek feedback regarding their driving
abilities and performance regularly (Berry, 2011).
3) Encouraging older drivers to plan their driving cessation from
early age to minimise the negative consequences associated with driving
cessation (Musselwhite & Shergold, 2013).
2.8.1 Identifying high-risk older drivers
The major challenge faced by road safety researchers is the identification of
“high-risk” older drivers (Dobbs, Heller, & Schopflocher, 1998) who would benefit
from variety of interventions that intend to keep them driving safely and for longer
(Langford, Bohensky, Koppel, & Newstead, 2008). Throughout the literature, there
is inconsistency in the definition of “older driver” with no clear rationale that
explains the choice of a certain age limit above which one becomes an “older driver”
(Lang et al., 2013 ). Chronological age is a weak predictor of crash risk (Dickerson
et al., 2007) and it should not be used as a criteria to restrict people from driving
(Yassuda & Wilson, 1997). Using a single cut-point to define the older driver is
inadequate as it assumes that those over a certain age are a homogenous group and
crossing this age will shift the risk of crash from low to high (Newgard, 2008) and
ignores the fact that aging patterns vary widely among people (King et al., 2011).
Older drivers are often divided into two broad groups, those with medical
conditions that require reporting to a transportation authority and those who are
relatively healthy (Rudman, Friedland, Chipman, & Sciortino, 2006b). Certain
health conditions and medications are often associated with an increased risk of

28 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
crashes (Dobbs, 2008) and ageing is often accompanied with an increased incidence
of such conditions. Some researchers suggest that policies should be targeted
towards identifying medically-at-risk older drivers and to provide them with
individualized assessments (Dobbs, 2008). This strategy would mean that physicians
will play a greater role in the older drivers’ licensing policies. However, while
previous research has indicated that older adults trust and respect their physician’s
opinions regarding their driving (Coughlin, Mohyde, D'Ambrosio, & Gilbert, 2004),
there are various problems that could arise if the licensing system becomes overly
medically-regulated. Physicians often lack knowledge regarding the relationship
between medical conditions and driving (Dobbs, 2008), and they often express
concerns about compromising their patient’s trust (Betz, Jones, Petroff, & Schwartz,
2013). Another major concern is that a medically-regulated licensing system may
divert people away from disclosing and discussing changes in their driving abilities
with their physicians (Berry, 2011). They can also become more reliant on their
physicians to assess their driving abilities, and therefore do not monitor their driving
or regulate it in response to age-related declines that are not a part of medical illness
(Berry, 2011).
Driving is a complex task that requires dynamic interaction between various
cognitive, physical, and sensory functions (Anstey et al., 2005). Some medical
conditions may affect driving abilities and can assist healthcare professionals in
identifying older adults who may require further assessment (Marshall, 2008).
However, the diversity of ways a disease may affect two individuals, the severity of
the disease, the effect of treatment on crash risk, and the presence of multiple
medical conditions make it difficult to generalise the association between a medical
condition and fitness to drive (Marshall, 2008). Further, while medical conditions
have an effect on older drivers’ fitness to drive, the crash risk is only slightly-to-
moderately increased (Marshall, 2008) and driver retraining or other interventions
may have the potential to reduce crash risk (Marshall, 2008).
There is also a great discrepancy between the relatively healthy older adults
in terms of how they are experiencing non-pathological declines in their driving
abilities, the types of these declines, and how these declines could impact their
driving performance. In the absence of a medical condition that clearly affects
driving abilities, it may be difficult to identify older drivers who are suffering from

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 29
subtle and progressive age-related changes in their functional abilities and regulation
and/or restriction of driving is in many of these cases a voluntary act by the driver.
Still, policy makers view older drivers as a homogenous group and neglect the fact
that there is a considerable variation in driving performance and health measures
among older adults which is seen even at older ages (Langford & Koppel, 2006).
Overall, identifying high-risk group of older drivers is still problematic since
driving is a complex activity that relies on a wide range of sensory, motor, and
cognitive abilities. Up until now, there is very limited evidence to support the use of
off-road screening batteries in assessing older adult’s fitness to drive (Wood et al.,
2008) and there are contradicting evidence in regards to which abilities are crucial
for safe driving (Marshall, 2008). A recent systematic review has revealed that the
“use of a single tool measuring cognition, vision, perception or physical ability is not
sufficient to determine fitness to drive” (Dickerson, Meuel, Ridenour, & Cooper,
2014). Much research is needed to determine the ideal battery of tests to be used that
can detect fitness to drive while ensuring reliability and validity (King et al., 2011).
Attempts have been directed towards identifying older drivers through
measures of medical screening and on-road tests. The effectiveness of these
measures is discussed in the following section.
Age-Based Licensing Interventions
Age-based assessments have been proposed as a strategy that can help
identify older drivers at increased crash risk. There is a wide variation in the
assessment procedure and age requirements for licensing renewal in Australia as
shown in Table 2.1.
Still, despite its widespread use, age-based mandatory testing has not shown
any safety benefits in term of reduction of crash risks (Mitchell, 2010) and has not
been shown to be effective in identifying older drivers with increased crash risk due
to functional declines (Oxley & Whelan, 2008) .
Previous studies which compared the rate of crashes of older drivers between
areas with mandatory age-based testing and areas with no age-based renewal
requirements found no difference in the rate of crashes among older drivers
(Hakamies-Blomqvist & Peters, 2000). In 1986, Torpey conducted a study where he
compared older drivers’ fatality crash rates across different licensing jurisdictions in

30 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Australia (with the exception of Victoria, all states had some form of mandatory age-
based assessment) (Torpey, 1986). Interestingly, the Victorian crash rate was lower
than crash rates for Queensland, Western Australia, and Tasmania and was closely
similar to those in South Australia and New South Wales (Torpey, 1986).
Table 2.1: Driver Licensing Practice renewal for car drivers (excluding heavy
vehicle and motorbikes) in Australia (2016)
State Age-requirement
for re-license
Medical Examination On-road Practical Test
ACT 75 Annual medical certificate from
the age of 75
When reported
New South
Wales
75 Annual medical certificate from
the age of 75
Biannual on-road test
from the age of 85
Not required for
conditional licences
Northern
Territory
- When reported When reported
Queensland 75 Annual medical certificate from
the age of 75
When reported
South
Australia
- When reported When reported
Tasmania 75 Annual medical assessment When reported
Victoria -
When reported When reported
Western
Australia
80 Annual medical examination
required from the age of 80 to
assess fitness to drive
Annual practical driving
assessment if
recommended by health
professional from the age
of 85

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 31
A similar study was conducted by Langford et al. in 2004 which determined
that mandatory assessment programs do not offer any noticeable safety benefits
(Langford, Fitzharris, Koppel, & Newstead, 2004).
Further, older drivers in states that employ some form of mandatory
assessment may choose to surrender their driving license while those in states with
no mandatory assessment may keep their license even after they stop their driving
(Langford, Fitzharris, Koppel, et al., 2004). To overcome the limitation associated
with previous study, Langford and colleagues compared the rates of fatal crash
among drivers aged 80 years and over in Melbourne which has no mandatory driving
assessment and Sydney where medical and on-road assessment is mandatory, using
population, number of licences held, total distance driven, and time spent driving as
exposure measures, while controlling for possible differences in driving activity
across the states (Langford, Fitzharris, Newstead, & Koppel, 2004). There was no
difference in crash risk based on population between Melbourne and Sydney. Per
licensed driver and per time spent driving, Sydney had statistically higher rates of
fatal crash involvement than older drivers in Melbourne (Langford, Fitzharris,
Newstead, et al., 2004).
In addition, a recent study by Ross et al. (2011) reported that drivers from
Victoria where no age-based testing is required are between 2 and 5 times more
likely to be driving than those from states with age-based testing (New South Wales
and South Australia) (Ross, Browning, Luszcz, Mitchell, & Anstey, 2011).
Interestingly, the percentage of older drivers suffering from cognitive impairments
(as measured by Mini Mental State Examination) and visual impairments (static
visual acuity) was similar between these three states (Ross et al., 2011).
In 2012, Tay examined the association between licensing requirements and
crash rates for older drivers in five Canadian provinces. There was a positive
association between the strictness of the licensing system and the mean crash rates.
The author concluded that since policies should be developed based on scientific
evidence, age-based testing is not recommended as they have no demonstrable safety
benefits (Tay, 2012). In New Zealand, older drivers aged 80 years and above were
subjected to a licence test through the period from 1999 to the end of 2006 which
involved an on road test of around 20 minutes that was suspended in 2006 (Keall &
Woodbury, 2014). Analysis of New Zealand Travel Survey data, licensing data, and

32 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
police-reported crash data failed to demonstrate any changes in the levels of road
injury involving drivers aged 80 and above (Keall & Woodbury, 2014). The study
provided further support to the ineffectiveness of on-road testing as an assessment
strategy for older drivers (Keall & Woodbury, 2014).
To conclude, attempts to address the older drivers’ safety problem through
mandatory testing offer no safety benefit (Lang et al., 2013 ). On the contrary, they
can compromise the mobility and safety of older adults and prompt premature
cessation of driving (Hakamies-Blomqvist & Wahlström, 1998). Premature
restriction of driving can cause older adults to use alternative riskier modes of
transportation such as walking or cycling (Langford et al., 2008; Oxley & Whelan,
2008). Older adults are at greater risk as vulnerable road users than when using a car
(Oxley & Whelan, 2008). Further, older drivers’ skills and performance can
sometimes be enhanced to satisfactory levels through a number of countermeasures
such as education, physical rehabilitation, self-regulation, and/or regulation by
licensing authorities ( Eby, Molnar, Shope, Vivoda, & Fordyce, 2003)
Langford and Koppel raise an interesting point about older drivers’ right to
choose to continue or stop driving (Langford & Koppel, 2006) as their over-
involvement in serious and fatal crashes is caused by their increased fragility and
they do not represent an increased risk to other road users (Langford & Koppel,
2006).
Licence Restrictions
In Australia, drivers with diagnosed medical conditions and disabilities that
impair their driving abilities could be subjected to licence restrictions. According to
Langford & Koppel (2011) licence restrictions attempt to:
● enhance fitness to drive – (e.g. wearing corrective lenses);
● create safer vehicles – (e.g. using automatic transmission); and
● avoid challenging driving situations- (e.g. night driving).
There are few studies that have attempted to examine the effectiveness of
restricted licenses on the crash risk of older drivers. A recent study using provincial
insurance claim data from all drivers aged 66 years or over for the years 1999-2006

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 33
in British Columbia compared crashes caused by drivers with restricted versus
unrestricted licenses (Nasvadi & Wister, 2009). Restricted licence holders were more
likely to be older, men, and with a history of at-fault crashes (Nasvadi & Wister,
2009). The results showed that drivers were involved in fewer crashes after
restrictions were placed on their licences (Nasvadi & Wister, 2009). Further,
compared to unrestricted drivers, restricted licence holders continued to drive crash
free for longer and their risk of causing a crash was 87% that of unrestricted drivers
after controlling for age and gender (Nasvadi & Wister, 2009).
Recently, Langford & Koppel examined the extent of use of restricted
licences and their safety benefits in the state of Victoria (Langford & Koppel, 2011).
Less than 10% of older drivers had a licence restriction (Langford & Koppel, 2011).
Majority of licence restrictions (95%) involved wearing corrective lenses when
driving followed by (2%) of driving a vehicle with automatic transmission (Langford
& Koppel, 2011). The findings indicate that restrictions associated with wearing
corrective lenses while driving, restricting travel to a specified distance from one’s
home and preventing night-time driving were associated with lower crash rates
(Langford & Koppel, 2011). License restrictions were associated with decreased
crash rates and the increased crash risk of restricted drivers relative to drivers with no
licence restrictions was small and within an acceptable level (Langford & Koppel,
2011). However, the small number of older drivers with licence restrictions makes it
difficult to reach a definite conclusion of the safety benefits (Langford & Koppel,
2011).
Older drivers view licence restriction policy favourably if it does not
negatively impact their mobility (King et al., 2011). Given that licence restrictions
can impose unnecessary limitations on older drivers’ mobility, further research is
needed before it can be widely employed as a strategy to manage older driver safety
and to determine those who are most likely to benefit from them (Langford &
Koppel, 2011).
2.8.2 Encouraging older drivers to self-monitor their driving and self-regulate accordingly
The process of self-regulation starts by recognising the decline in certain
driving abilities and the need to appropriately compensate for such decline. The
majority of older drivers’ studies view self-regulation strategies as either avoidance

34 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
behaviours or driving reduction. Recently, Molnar and colleagues have introduced a
new and a broader definition of self-regulation where they classify self-regulatory
behaviours into three levels; strategic, tactical and life-goal (Molnar et al., 2013).
Strategic self-regulation involves the decisions made by drivers prior to taking the
trip and involve general planning such as avoiding difficult driving situations or
selecting certain driving routes. Tactical self-regulation involves the decisions made
by drivers while they are on the road, such as gap and headway acceptance, speed
choice, and overtaking, avoiding potentially distracting secondary activities in the
vehicle while driving. Life-goal level of self-regulation involves the broader
decisions made by older drivers in their lives such as the choice or what kind of car
to drive, with safety often being an important consideration in the vehicle purchase
decision. Interventions to promote successful self-regulatory behaviours will vary
for each level. On the strategic level; interventions enhancing self-awareness of
limitations in driving abilities would be beneficial. On the tactical level, older
drivers would benefit from in-vehicle technologies that can assist them in making
safer decisions on roads. On the life-goal level, strategies should promote use of
alternative transport options, moving close to public transport, and planning retiring
from driving. Most of the previous studies investigating the process of self-
regulation have focused on strategic self-regulation. The following discussion will
focus on strategic self-regulation as there are very few studies that have examined the
tactical and life-goal self-regulatory behaviours among older drivers.
Factors associated with self-regulation
Socio-demographic factors
Age: Older age has been associated with mileage reduction (Marottoli et al.,
1993) and subsequent driving cessation (Freeman et al., 2006). However, some
studies failed to show a significant association between increasing age and self-
regulation (Blanchard & Myers, 2010). These mixed findings could be the result of
differences on how self-regulation is defined between studies or due to differences in
the sample (e.g. different age groups, prevalence of medical illnesses, and health
status).
Gender: Older women are more likely to self-regulate their driving than
older men (Anstey et al., 2006). When compared to males, older female drivers are
more likely to avoid driving at night, in bad weather, in rush hour and on highways

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 35
(Baldock et al., 2006a). They also make fewer trips, drive fewer days and fewer
miles/kilometres, and drive closer to home compared to older men (Rosenbloom &
Herbel, 2009). Men, on the other hand, make less radical changes to their driving
behaviours (Evans, 1991) and they are very reluctant to give up driving (Kostyniuk
et al., 1998). Further, compared to men, women are more likely to acknowledge
their declining abilities (McNamara, Chen, George, Walker, & Ratcliffe, 2013),
while men tend to associate their decision to giving up driving to external reasons
(e.g. medical conditions) rather than declining abilities (McNamara et al., 2013).
Older women are also more likely to stop driving before older men (Anstey et al.,
2006) and some could be even giving up driving prematurely (Siren & Meng, 2013).
A Finnish study indicated that women who surrendered their driving license at the
age of 70 (n=1476) had lesser overall health ratings than those women who
maintained their driving license (n=1494) (Siren, Hakamies-Blomqvist, & Lindeman,
2004). Interestingly, those health conditions affected that overall health and mobility
of former drivers but were not necessarily affecting their fitness to drive which
indicates that some women may be stopping driving too early when they are still fit
to drive (Siren et al., 2004).
But why do women give up driving earlier than men? This could be
attributed to how women view the role and the importance of driving. For women,
driving is an essential means to meet their daily practical needs (e.g. family
commitments, employment, social activities, etc.) while for men it is key to their
identity, independence and freedom (Musselwhite & Haddad, 2010b). In addition,
women often indicate that loss of confidence is the reason they stopped driving
(McNamara et al., 2013). Older women lack confidence in their driving as they often
have less driving experience when compared to men (Marottoli et al., 1993).
Another explanation is that their male partners often discourage them from driving
and criticise their driving performance (Siren & Hakamies-Blomqvist, 2005).
As women are starting to resemble men in terms of education and
employment, their driving experience and their attitude towards driving may start to
resemble that of men (Rosenbloom, 2006). Driving will become an integral part of
their identity, and like men, it will be the key to their freedom and independence. It
is therefore predicted that the future cohort of female drivers will be driving for
longer (Rosenbloom & Herbel, 2009).

36 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Income and household composition: Qualitative evidence has shown that
financial comfort could impact older drivers’ decision to stop driving (Adler &
Rottunda, 2006). Some studies showed an association between lower annual
household income and self-regulation (Naumann, Dellinger, & Kresnow, 2011;
Ragland, 2004), higher income and driving cessation (Unsworth, Wells, Browning,
Thomas, & Kendig, 2007), and others have shown no association (West et al., 2003).
Charlton et al. (2006) reported that those who were not the major driver of the
household were more likely to report adoption of self-regulation. On the other hand,
Ragland et al. (2004) reported that household arrangements had no impact on self-
regulation. Braitman and McCartt (2008) reported that those who were single,
divorced or widowed were 53% more likely to self-regulate than those who were
married.
Experience of a crash
In a study conducted by Charlton et al. (2006), drivers with a history of self-
reported crash in the last two years were 1.5 times more likely to self-regulate their
driving compared to those who were not involved in a crash. Ball et al. (1998) also
reported more avoidance among older drivers with a history of at-fault crashes in the
prior five years as obtained from state records.
Health, medical conditions, and age-related decline
There is an association between a large number of health and physical
functioning measures and cessation of driving as evident in longitudinal studies
(Anstey & Smith, 2003). However, not all those suffering from serious health issues
regulate or stop their driving. A study by Stewart et al. (1993) revealed that an
alarming 68% of older drivers who suffered from a short-term vision loss continued
to drive (Stewart, Moore, Marks, May, & Hale, 1993). Similar findings were seen
among older women, where 38% of those with a self-reported condition or symptom
that may affect driving ability continued to drive (Siren et al., 2004). This could be
due to the fact that older drivers’ perceptions of their health conditions and how they
impact their driving are far more important factor than their objective health
condition (Anstey et al., 2005). In addition, individuals suffering from some types of
cognitive impairments may lack insight into their declining abilities and therefore
will not regulate accordingly (Ackerman et al., 2011). Recent findings have shown
that older drivers have high ratings of their driving ability regardless of their

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 37
cognitive ability assessed by the Clock Drawing Test (CDT) (Wong, Smith, &
Sullivan, 2012). Further those who failed the CDT were less likely to report driving
avoidance and were less interested in participating in driving programs (Wong et al.,
2012).
Knowledge and health literacy
A recent study among 322 Australian drivers aged 65 years and over
investigated the association between health literacy and self-regulation of driving
(Sargent-Cox, Windsor, Walker, & Anstey, 2011). Around 86% of participants
demonstrated good knowledge about health conditions and driving safety but around
50% lacked knowledge about the impact of certain medications on driving abilities
(Sargent-Cox et al., 2011). The findings also show that health knowledge is far less
significant for predicting driving behaviour than actual health experience (Sargent-
Cox et al., 2011).
Confidence
Numerous studies point to the significant association between self-reported
driving confidence/comfort and driving behaviour (Blanchard & Myers, 2010). Self-
regulation as a result of lack of confidence may be a cause for concern (Moták,
Gabaude, Bougeant, & Huet, 2014) rather than an indication of successful self-
regulation. Self-regulation of driving as a response to the discomfort older adults
experience in stressful driving conditions rather than intentional monitoring of their
driving ability (Meng & Siren, 2012) represents a failure of self-regulation rather
than a success. These drivers may attribute their feelings of discomfort to external
reasons (i.e. glare from other cars’ headlights on their glasses, changes in the road
systems) rather than possible declines in their own driving abilities. On the other
hand, drivers may impose unnecessary driving restrictions on their driving (Meng &
Siren, 2012), despite being able to safely drive in these situations if they adopted
other coping strategies such as pre-journey planning or vehicle modifications
(Gwyther & Holland, 2014).
Self-awareness
In the multifactorial model for enabling driving safety, factors of cognition,
sensory function and physical function predict an individual’s driving capacity;
however, accurate insight into one’s driving capacity is crucial for safe driving
38 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
behaviour (Anstey et al., 2005). In driving, not only it is important to recognise that
a specific ability has declined but also to understand the implication of that decline
on the driving performance (Charlton, Oxley, Fildes, & Les, 2001). Those who are
unaware of limitations in their driving abilities may engage in behaviours that
jeopardise their safety and the safety of others (Marottoli & Richardson, 1998). In
addition, older drivers who are aware of declines in their abilities are more likely to
practice self-regulation than those who are less self-aware (Blanchard & Myers,
2010; Holland & Rabbitt, 1992; Molnar & Eby, 2008). Whether older drivers are
aware of their functional abilities or not remains questionable. A study conducted
among older drivers (n=257) has shown that those with existing visual and/or
attentional impairments reported more avoidance than those free of impairments
(Ball et al., 1998). Further, a five-year longitudinal study showed that older drivers
at increased crash risk determined by Useful Field of View (UFOV) test reduced
their driving exposure and increased driving avoidance over time compared with
those at low risk of crash (Ross et al., 2009).
On the other hand, several studies have reported that older drivers overrate
their driving abilities and performance. For instance, Holland and Rabbitt (1992)
demonstrated that drivers in their 70s rated their sensory abilities to be similar to
those in their 50s. Freund et al. (2005) found that among drivers aged 65 years and
above who were referred to driving evaluation, 65% of the participants estimated
they will perform better and 31.9% estimated they will perform the same on the
driving test as others their own age. In addition, higher self-rating of skill was
significantly associated with increased risk of driving difficulty assessed by driving
simulation (Freund et al., 2005).
Further, some researchers point out that self-regulation of driving is actually
an automatic process performed by the driver to minimise the mental load associated
with the functional declines brought by ageing rather than to enhance their safety (De
Raedt & Ponjaert-Kristoffersen, 2000a) . Therefore, drivers may not be aware that
they are compensating for functional loss. Their self-regulation of driving may be
merely a response to the discomfort they experience in challenging driving
conditions rather than intentional monitoring of their driving ability (Meng & Siren,
2012).

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 39
Limitations of self-regulation literature
The discrepancies in the findings of previous studies on self-regulation can be
attributed to methodological problems (Molnar et al., 2015). To start with, the way
self-regulation is defined varies considerably between studies. The majority of these
studies have examined self-regulation in terms of avoidance of difficult situations,
e.g. driving at night, adverse conditions (Baldock et al., 2006a; Charlton et al., 2006).
Self-regulation of driving involves any decision drivers make to enhance their overall
driving safety by overcoming limitations in their driving. This involves a variety of
behaviours such as planning trips, reducing the overall amount of driving, restricting
driving, taking a passenger to assist with navigation and broader life decisions that
can impact their overall driving (e.g. relocating to a senior’s house, vehicle
adaptation) (Molnar et al., 2013). For example, recent findings suggest that the
reasons behind reducing driving are different from avoiding challenging situations
(Meng & Siren, 2012). Reducing the overall amount of driving is often attributed to
lifestyle factors and the reduced need for mobility (e.g. retirement, relocation) (Meng
& Siren, 2012). On the other hand, driving avoidance is often triggered by negative
feelings associated with driving situations (Meng & Siren, 2012). Latest findings
that younger drivers also avoid some driving situations (Naumann et al., 2011)
suggest that driving avoidance is not always the result of age-related declines in
driving abilities. In their study, Naumann et al. (2011) reported that around 25% of
drivers aged 18-24 avoided driving at night, 50% avoided driving in bad weather,
and almost 20% avoided driving on highways and high-speed roads. Reduced
driving has been linked to number of factors such as retirement (Burson, Larrick, &
Klayman, 2006) or changes in lifestyle (Blanchard & Myers, 2010). Up until now,
few studies have investigated the reasons for avoidance or reducing driving among
older drivers. Motivations to reduce driving and to avoid driving situations for
reason other than awareness of impaired abilities should not be regarded as self-
regulation. Future studies should examine the specific reasons older drivers choose
to modify their driving patterns before classifying it as self-regulation.
Second, most of these studies have relied on self-report measures. Recent
findings suggest that self-report measures of driving behaviours do not match
objective measures of real-world driving (e.g. older drivers can not accurately
estimate their driving distances (Huebner, Porter, & Marshall, 2006) and they tend to

40 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
drive more frequently in challenging situations than they actually report (Blanchard
& Myers, 2010).
Third, up until now, the majority of previous studies focused on the
association between self-regulation and specific impairments and medical conditions
among older adults (Rudman et al., 2006). Recently, attention has been diverted into
understanding the psychosocial factors that affect self-regulatory driving behaviours.
However, due to the differences in the way drivers’ perceptions are measured and
defined, it is difficult to compare the findings (Blanchard & Myers, 2010).
Fourth, majority of studies rely on convenience sample of older drivers which
can limit the generalisation of the findings. Previous studies vary considerably
regarding participants’ characteristics, their driving patterns, and their cultural and
social context (Molnar et al., 2015).
Finally, driving cessation is more of a gradual and voluntary process
whereby the driver will gradually increase self-imposed restrictions (Dellinger et al.,
2001). As suggested by previous research, the driving cessation process may occur
through stages and older adults’ response to feedback may vary depending on which
stage they are at. Without longitudinal studies that follow older drivers through the
process of self-regulation it will be difficult to conclude which and how certain
factors influence older drivers’ decision to change and/or stop their driving. The
majority of the studies examining the factors associated with self-regulation has been
cross-sectional (Ackerman, Edwards, Ross, Ball, & Lunsman, 2008).
Is self-regulation effective in eliminating crash risk?
The large number of factors and countermeasures that contribute to the crash
risk among older drivers and the methodological limitations outlined above make it
difficult to determine if self-regulation is effective in eliminating increases in crash
risk caused by age-related declines (Horswill et al., 2011). However, some evidence
suggests that the self-regulation may be a promising strategy in reducing crash risk
among older drivers. A study by Anstey et al. (2006) assessed 1446 older drivers
aged 70 and above at baseline on several visual, cognitive and functional measures
and followed them for a five years’ period (1992-1997). The authors found that the
variables associated with driving cessation to be similar to those associated with
increased crash risk in older adults, which suggests that older adults with cognitive or

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 41
visual impairments reduce their risk of crash by modifying their driving behaviour
(Anstey et al., 2006). Further, analysis of fatal crashes from the Fatality Analysis
Reporting System between 1997 and 2008, indicated that the licensing rate for
people 70 and older increased from 73 to 78 percent, but fatal passenger vehicle
crashes per licensed drivers in this age group fell 37 percent, in comparison to a 23
percent decrease for drivers ages 35 to 54 (Cheung & McCartt, 2011). The decline
was greatest (47%) among drivers 80 and older. While the reasons are not fully
understood, self-regulation may be playing a role (Braitman & Williams, 2011).
Keay et al., 2013 pointed out that recent epidemiological results, based on the
findings from the North American Fatality Analysis Rating System, support the use
of self-regulation to increase older drivers’ safety (Keay et al., 2013). Individuals
who drive in daylight and individuals with a history of motor vehicle conviction were
less likely to be injured in a crash probably as these individuals recognise their
limitations (Keay et al., 2013).
The impact of feedback on self-regulation among older drivers
To date, research that focuses on the impact of feedback on older drivers’
self-awareness and subsequent self-regulatory behaviours is limited. The changes
associated with ageing are usually subtle and older people may not be aware of how
these changes impact their driving abilities. In addition, driving errors and violations
will not necessarily result in crashes or penalties and drivers may fail to develop an
accurate estimation of their abilities (Dogan et al., 2012). If an incident takes place,
the driver may not understand why it occurred and how to prevent it in the future
(Dogan et al., 2012). Therefore, feedback can help drivers calibrate their perceptions
of their own performance with their actual performance (Donmez, Boyle, & Lee,
2007). Little is known about the factors that can influence the effectiveness of such
feedback, specifically in terms of timing and content.
Few studies suggest that feedback may lead older adults to make informed
decisions about their driving behaviour (Owsley, Stalvey, & Phillips, 2003). In a
study conducted by Holland and Rabbitt (1992), two thirds of participants (n=80)
reported making compensatory changes in their driving behaviours in response to
feedback about their sensory abilities. Eby et al. (2003) reported that 14% of older
adults, who completed a workbook that raised issues regarding health, cognition,
vision, and driving behaviour, discovered changes in their abilities, with 25%

42 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
reporting their intention to adjust their driving behaviour accordingly ( Eby et al.,
2003). In another study 129 older adults received feedback about their eligibility to
receive an insurance discount following the result of a UFOV test and those who
failed to qualify were more likely to increase driving avoidance over 3 months period
(Ackerman et al., 2011).
The following section will discuss existing interventions which are used to
provide older adults with feedback and promote driving self-regulation.
Self-screening tools
Self-screening tools can be used as first-tier assessment, pointing drivers to
the presence of adverse health problems and encouraging them to seek further
assessment and evaluation. They are available in both paper-based format and web-
based format. There are several advantages associated with the use of self-screening
tools. First they are relatively easy and cheap to dispense which makes them highly
accessible (Eby et al., 2003). They can also be completed in the driver’s house,
which is a friendly non-threatening environment (Eby et al., 2003). Further, previous
qualitative studies have indicated that such tools can promote early discussion of
driving future with family members and subsequently assist in the early identification
of driving-related problems which in turn may facilitate timely action to prolong safe
mobility (Eby et al., 2003). On the other hand, self-screening tools can only be
completed by cognitively intact individuals in order to understand the feedback and
act appropriately on it (Eby et al., 2003). In addition, individuals who choose to
complete self-screening are more likely to be more safety-oriented and older adults
with existing driving-related problems and limitations may be reluctant to use these
tools (Dunn, 2011). Self-screening tools are liable to self-enhancement bias which
can create a false sense of safety by providing inaccurate positive feedback on
driving abilities (Lang et al., 2013 ). Furthermore, the degree to which older drivers
can access information on age related changes and how these changes may affect
driving is still unknown (Siren & Haustein, 2015).
Family members and healthcare professionals
Older people are more likely to value the advice of those who have direct
knowledge about their driving abilities and those who are concerned about their best
interests (Coughlin et al., 2004). Generally, family members may be the first to

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 43
express their worries about an older adults’ ability to drive (Gillins, 1990). However,
the sensitivity of the topic may make it difficult to initiate such sensitive
conversation. Family members are often aware of the importance of driving in the
older person’s life and how it affects independence and wellbeing. In fact, some
family members may avoid being involved in this discussion altogether (Rudman et
al., 2006) to avoid creating problems (Connell, Harmon, Janevic, & Kostyniuk,
2013). This could also be complicated by existing difficulties or poor
communication (Connell et al., 2013). In a recent qualitative study, adult children
reported adopting a passive attitude towards their parents’ declining abilities such as
refusing to take rides with parents or discussing driving concerns with other family
members but not the parents (Connell et al., 2013). The loss of a driver’s license can
cause additional burden to families’ already busy lives (Johnson, 1999) and some
children would even tone down the risks associated with their parents’ declining
driving abilities to avoid being their carer (Connell et al., 2013). Therefore, family
members tend to ask the physicians to initiate the conversation (Persson, 1993).
In Queensland, drivers aged 75 years and above are required to hold a
current medical certificate that indicates their fitness to drive, regardless of whether
they have a medical condition or not. Therefore, physicians have the opportunity to
prevent and/or minimise the morbidity and mortality associated with traffic injury
among their patients and the general public (Molnar, Byszewski, Marshall, & Man-
Son-Hing, 2005). While many older drivers will give up driving based on their
physicians’ recommendations (Coughlin et al., 2004; D'Ambrosio, Coughlin,
Donorfio, Mohyde, & Meyer, 2008), there are number of barriers that can limit the
physician’s role in the decision-making process. To start with, physicians often
report that they lack the training and the confidence (Jang et al., 2007) necessary to
determine older adults’ fitness to drive. Further, none of the tools used in doctor’s
offices to assess the fitness-to-drive have been scientifically validated. Physicians
may also lack the knowledge regarding licensing policies and medical restrictions for
specific medical conditions (Bogner, Straton, Gallo, Rebok, & Keyl, 2004; Brooke &
Southward, 2006). Qualitative findings indicate that physicians may also be unaware
if their patients are still driving or not as some clinicians reported that they do not
routinely ask about driving (Bédard et al., 2001). In a recent study among 322
Australian drivers aged 65 years and more, an alarming 85.7% drivers indicated that

44 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
they did not receive any advice from their physician about the impact of their
medical condition on their driving abilities (Sargent-Cox et al., 2011).
Physicians often report feeling uncomfortable assuming an active role in
maintaining seniors’ mobility (Rudman et al., 2006b) as it may have a negative
impact on the physician-patient relationship (Jang et al., 2007). In fact, some older
drivers seek the input of another physician if the first one deem them unfit to drive
(Staplin & Freund, 2013).
Physicians can play an important role in the management of the older drivers’
safety issues if these gaps are addressed. In addition, normalising and discussing
fitness to drive from an early time can overcome the sensitivity associated with the
topic (Bédard et al., 2001).
In-vehicle technology
In- vehicle devices designed to prevent crashes are becoming technically
feasible and affordable (Walker, Stanton, & Young, 2001). These devices may have
the potential to improve road safety (Coughlin, 2005) and potentially maintain older
drivers’ mobility for longer (Rakotonirainy & Steinhardt, 2009). There has also been
a focus on the development of Advanced Driver Assistance Systems (ADAS), which
are electronic systems designed to help the driver manoeuvre through challenging
traffic circumstances (Lindgren, Chen, Jordan, & Zhang, 2008). Advanced Driver
Assistance Systems can improve driving safety by enhancing driver’s behaviour,
cognition, and perception. These systems can provide the driver with timely
feedback which can increase driver awareness about immediate environmental
changes (Zhao & Wu, 2012). However, little is known about the impact ADAS has
on older drivers’ insight into the impact of age-related declines on their driving
performance. It can be argued that ADAS can point out specific limitations in the
older adults’ driving. A blind spot detection and a lane change assist system, for
example, can improve older drivers’ awareness of existing motor and visual
limitations (difficulty in turning head and reduced peripheral vision) and assist them
in merging and lane changes. It can allow the driver to be aware of the difficulties
involved with the driving task, the actions (or the avoidance of actions), and whether
they have the necessary abilities to cope. But this form of feedback may not
communicate the information necessary to alter the driver’s behaviour (Donmez et
al., 2007). Combined feedback (i.e., immediate and retrospective), on the other

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 45
hand, may offer additional benefits. Retrospective feedback can refresh older
drivers’ memory and help them evaluate the driving errors and incidents which the
immediate feedback has highlighted during the drive (Donmez et al., 2007). A
recent review of the effect of a number of in-vehicle technologies has determined
that ADAS can in fact assist older drivers with their everyday performance, reduce
their possibility of being involved in a crash, and reduce the severity of the crash for
both drivers and occupants (Eby et al., 2015). Recent qualitative evidence suggests
that older drivers don’t seek ADAS for age-related reasons, however, they perceived
such technologies to be useful in terms of compensating for age-related changes,
enhancing their safety, and improving their overall driving performance (Gish,
Vrkljan, Grenier, & Van Miltenburg).
Educational interventions
A common shortfall among the majority of educational interventions
targeting older drivers is that they are not based on theoretical knowledge of
behavioural change (Tuokko, Rhodes, et al., 2014). In addition, the majority of
educational interventions have been designed to improve older drivers’ knowledge
which can only lead to crash reduction if it causes changes in behaviour (Stalvey &
Owsley, 2003). A promising program is The Knowledge Enhances Your Safety
(KEYS), which was developed for older drivers with visual impairments to enhance
their awareness about visual impairments and promote adoption of self-regulatory
behaviours. It can be delivered in a clinical setting in a one-on-one format in order to
facilitate the tailoring of the intervention to the requirements of each person (Stalvey
& Owsley, 2003). The intervention was based on the Social Cognitive Theory to
promote the adoption of self-regulatory behaviour and is based on four components
a) motivational conditions, (b) self-regulatory skills, (c) confidence in one’s ability to
perform the behaviour, and (d) prerequisite knowledge and skills (Stalvey & Owsley,
2003).
In a study conducted by Stalvey and Owsley (2003), 365 older drivers, aged
60 years and over with visual limitations were allocated to one of two groups. The
intervention group (i.e. those who received the educational intervention in addition to
a comprehensive eye examination) were significantly more likely to recognise their
visual limitations; report more difficulty with challenging driving situations; avoid
challenging situation and reduce their driving exposure compared to the control

46 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
group (i.e. those who received the eye examination) (Stalvey & Owsley, 2003). In
2004, Owsley et al. conducted a similar study among 403, 60 years and above older
drivers with visual impairments and followed participants every six months for two
years. Those who received the intervention reported more avoidance of challenging
driving situations and self-regulatory behaviours than the control group, however,
there were no differences in the crash outcome (Owsley et al., 2004). They explain
how the risk of being involved in a crash is determined by a large number of factors
(e.g. vehicle condition, environmental conditions, drivers’ abilities) and it might be
simplistic to assume that educational programs alone would affect crash rate (Owsley
et al., 2004). In addition, driving is a habitual skill which makes it difficult to change
driver attitudes and practices (Owsley et al., 2004). In addition, while educational
interventions can enhance older adults’ awareness of the limitations in their driving
ability they may not be enough to assist them in overcoming the barriers toward
changing their behaviour.
2.8.3 Encouraging older drivers to plan their driving cessation from an earlier age
Driving cessation is usually a gradual process where people start to reduce
and/or restrict their driving until complete cessation (Dellinger et al., 2001). Older
drivers may be unwilling to plan their driving retirement due to their awareness of
the potentially negative consequences of driving cessation (King et al., 2011).
However, planning retiring from driving can make the experience easier and less
traumatic (Gilhooly, Hamilton, O’Neill, & al., 2003) and can improve the outcomes
through better ongoing preparation and maintenance of control (Buys et al., 2012).
Having an early conversation about one’s driving future can allow for more time for
professional skill assessment, potential driver rehabilitation, and even family
adjustment to a new transportation support role (Coughlin, 2004). Musselwhite and
Shergold (2013) followed 21 older drivers in the United Kingdom over a period of
ten months through five waves of data collection (focus group, three interviews, and
a travel behaviour diary). Those who planned their cessation reported a relatively
higher quality of life after stopping driving as opposed to those who did not plan
their driving retirement (Musselwhite & Shergold, 2013). The planners went through
an experimental period; trying new transport options and new travel modes which
provided them with a sense of achievement and control (Musselwhite & Shergold,
2013). On the other hand, the non-planners found it very difficult to adjust without

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 47
their car and blamed external factors for the lack of transport options (Musselwhite &
Shergold, 2013).
Previous research indicates that the vast majority of older drivers do not plan
the transition to non-driving state, even those who suffer from medical conditions
that can impair their driving (Adler & Rottunda, 2006).
In a 2006 study among 656 older Victorian drivers aged 55 years and above,
83% of those aged 75 years and more had thought about stopping driving but only
17% of these had made plans for it (Charlton et al., 2006). In Australian Capital
Territory, a study by Oxley et al. (2010) among older women drivers (n=673) and
former drivers (n=53) aged 60 years and over showed that current drivers had not
made plans about giving up driving; however, those who experienced health
concerns (e.g. vision problems) were more likely to think about not driving in the
future compared to those with no problems. Around 58% of former drivers reported
that they stopped driving suddenly but the majority (66%) reported that it was not a
difficult decision (Oxley, Charlton, Scully, & Koppel, 2010). In another study
conducted by Bauer et al. (2003), women who made the decision to stop driving
without the interference of others were more likely to adjust to their new lifestyle. In
addition, when the decision to give up driving is gradual, women had more time to
plan ahead (e.g. relocation, gathering information about alternative transports) and
reported better adaptation compared to those who were forced to stop suddenly
(Bauer, Rottunda, et al., 2003).
2.9 CHAPTER SUMMARY
This chapter has presented the implications of the ageing population in
regards to road safety and mobility needs. Attempts to manage the older drivers’
problems can be broadly categorised into three groups: 1). Identifying high-risk older
drivers, 2). Encouraging older drivers to self-monitor and self-regulate their driving
behaviours, and 3). Encouraging older drivers to plan their driving retirement from
an earlier age. Self-regulation is a favourable approach that can help older drivers
maintain their active lifestyle without compromising their safety and the safety of
others. However, as outlined above, there is still a gap in our knowledge of how to
promote successful self-regulation and the need for a model that can help us clearly
explain and describe this process is much needed. As discussed before, the

48 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
heterogeneity among the older drivers’ population has not been addressed with the
existing interventions which are mostly designed as one-size-fits-all. The lack of a
theoretically-informed model of driving self-regulation inhibits our ability to
understand and describe such complex process. There is growing evidence that older
drivers go through different qualitative stages towards modifying their driving
behaviours. It therefore could be useful to examine the driving self-regulation
process within behaviour change framework. The following chapter discusses the
existing models of driving self-regulation and explains the potential use of PAPM in
understanding such complex process.

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 49
Chapter 3: Theoretical framework and current models of older adults’ driving behaviour
3.1 INTRODUCTORY COMMENTS
This section reviews the existing models of older adults’ driving behaviour
and summarises the key determinants identified by each model that influence older
adults’ driving behaviour. The limitations of each model will also be discussed.
Finally, this section concludes by justifying the selection of the PAPM as the
theoretical base for this program of research.
The theories and models included in this review are presented according to
their level of sophistication. The search identified six models which are specific to
the older drivers’ behaviour which varied greatly in terms of their theoretical
development and their level of sophistication, the models were grouped into:
1. Descriptive models which specify determinants of driving behaviours
without a clear indication of how these factors interact.
2. Explanatory models which describe and explain how the determinants of
self-regulatory behaviours interact to initiate change.
3.2 DESCRIPTIVE MODELS
Kostyniuk, Shope & Molnar (2000): The Precaution Adoption Process Model
Kostyniuk and colleagues (2000) were the first to highlight the need to
develop a comprehensive model of the driving reduction and cessation process using
behaviour change theories. They hypothesised that predicting problems in one’s
driving ability is a key factor in initiating the driving reduction and cessation process.
They examined the applicability of the Precaution Adoption Process Model (PAPM)
as the framework to look at how older drivers cope with the age-related declines and
their willingness to make changes in response to these declines (Kostyniuk et al.,
2001). The PAPM is a stage-based theoretical model which assumes that people
need to be aware of the risk associated with their behaviour before they are
susceptible to behavioural change (Weinstein & Sandmand, 2002). It characterises

50 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
seven stages along the path from lack of awareness to action (unaware, unengaged,
undecided, decided not to act, decided to act, planning, acting and maintaining).
They conducted a survey study among 1,053 older drivers and former drivers over
the age of 65 where they investigated the impact of older adults’ anticipation of
driving problems on their driving reduction and cessation. Their findings suggest
that the awareness and anticipation of limitations in driving ability may be the key
factor for reducing and/or stopping driving, which provides an initial support to the
use of PAPM.
Figure 3.1: Driving reduction/cessation framework
From “Driving reduction/cessation among older drivers: toward a behavioural
framework” by Kostyniuk, L., Shope, J. & Molnar, L., 2000, 9th International
Asscoiation for Travel Behaviour Conference, Gold Coast, Australia, . 17
Key determinant: anticipation of problems in older adults’ driving and awareness of
change in their driving abilities.
Limitations: the model doesn’t recognise the influence of other external and internal
factors on older adults’ decision to modify and/or reduce their driving. The model is
rather descriptive and does not provide a clear idea of the factors that facilitate
transition between stages and is not useful in developing interventions.

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 51
Anstey et al. (2005): Multifactorial model of factors enabling driving safety among older drivers
This model was developed based on a literature review of 13 empirical
studies examining the relationship between many cognitive, sensory, and physical
factors and either self-reported crashes, state crash records or on-road driving
measures by Anstey and colleagues in 2005. It consists of two main factors; driving
capacity and self-monitoring and beliefs about driving (Figure 2.1). Driving capacity
is determined by cognition, sensory, and physical function (Anstey et al., 2005).
Self-monitoring beliefs refers to the ability to evaluate one’s driving ability and adapt
driving behaviours accordingly (Anstey et al., 2005). This model suggests that older
drivers’ insight into their driving skill is crucial for accurate evaluation of their
ability and accordingly successful self-regulatory behaviours. In fact, perceptions
about one’s ability may be a stronger determinant to reduce and/or restrict driving
than actual ability (Anstey et al., 2005). The strength of this model is that it is based
on an exhaustive review of recent literature on the impact of ageing and health on
driving abilities among older adults. It also emphasises the impact of insight and
self-monitoring abilities on adoption of safe driving behaviour while incorporating
the objective determinants of driving capacity. However, this model fails to account
for the contextual factors relevant to older adults driving behaviours (e.g.
environmental, intrapersonal, and interpersonal).
Key determinants: driving capacity as a function of interaction of cognitive,
visual, and physical function and self-monitoring beliefs and insight into driving
capacity.
Limitations: while the model describes how these two determinants interact
to affect the driving behaviour, it is very simplistic and does not incorporate the
impact of other interpersonal, intrapersonal, and environmental factors on older
adults’ behaviour.
Kowalski, Jeznach, Tuokko: Transtheoretical Model (TTM) (2014)
In 2014, Kowalski and colleagues examined the older driver behaviour within
the TTM framework using interviews/focus groups with 32 drivers and 19 former
drivers (Kowalski et al., 2014). Their model describes how older drivers go through
different stages of the TTM towards changing or stopping their driving. Pre-

52 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
contemplation is viewed as the period where people drive without imposing any
changes to their driving. It is not clear if those in the pre-contemplation stage are
unaware of the need to change their driving behaviour or if they are aware but refuse
to change. In the contemplation stage people start to think about changing their
driving in the future. These two phases include the “non-changers”, those who did
not change their driving. In the preparation stage individuals are planning to change
their driving behaviour in the near future. The action stage involves the period where
drivers start to impose self-restriction on their driving and avoid challenging
situation. Maintenance stage involves the phase where the driving behaviour change
has been successfully attained and is being maintained. They also added a sixth
stage of termination where older adults stop driving altogether.
The model emphasises the role of self-awareness of limitations in driving
abilities on the driving behaviour among older adults. It is also the first model to
highlight that older drivers could be divided into “gradual restrictors”, imposing
certain restrictions on their driving as they move from pre-contemplation to action or
maintenance or “consistent restrictors”, those who have always imposed restrictions
on their driving which may reflect a specific personality type (e.g.,
conscientiousness), or other external factors (i.e., reduced need to drive due to
relocation) rather than an awareness of declining abilities.
Key determinants: awareness of the need to change, pros and cons of
driving and external factors.
Limitations: a limitation of the TTM is that it fails to distinguish between
people who are unaware of the risk and those who have decided not to act. As
shown in this model, it is not clear whether individuals in the pre-contemplation
stage (the non-changers) are aware of the declining abilities but refuse to modify
their driving or simply unaware. It is therefore logical to assume that the resisters
will not progress through stages of change similarly to those who are unaware and
that they will require different types of interventions. Older drivers who resist change
may not benefit from traditional behavioural interventions and may be more reluctant
to seek feedback.

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 53
Figure 3.2: Conceptualization of the process of driving behaviour change within the TTM framework
From “Stages of driving behaviour change within the Transtheoretical Model (TM)" by Kowalski, K., Jeznach, A. & Tuokko, H.A., 2014, Journal of Safety Research, 50,
p 19.
3.3 EXPLANATORY MODELS
Rudman’s model of self-regulation (2006)
This model was developed based on the result of qualitative findings from
focus groups with 29 pre-senior drivers, 24 senior drivers, and 26 retired senior
drivers. The model highlights the impact of interpersonal, intrapersonal and
environmental factors, on the ability of older adults to self-monitor and adjust their
driving. It also highlights the impact of older drivers’ level of comfort on their
driving behaviour.

54 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Key determinants: this model (Figure 3.3) is the first comprehensive model
of self-regulatory driving behaviour among older drivers accounting for many
environmental, intrapersonal and interpersonal factors that affect older adults’
decision and ability to adopt safe driving behaviours. The influence and role of
feedback on older drivers’ decision-making process is highlighted in this model, an
area that is under researched in the older drivers’ literature.
Limitations: the model fails to account for the impact of driving capacity on
older adults’ driving behaviour. In addition, the model suggests that driving comfort
influenced by a number of interpersonal, intrapersonal, and environmental factors
acts as a key determinant of self-regulation (Rudman et al., 2006b). If older drivers
avoid certain driving situations because they feel uncomfortable then their self-
regulation of driving may be a response to the discomfort they experience in
challenging driving conditions rather than intentional monitoring of their driving
ability (Meng & Siren, 2012). This means that if participants’ discomfort was indeed
caused by factors unrelated to declines in their driving ability, it may have led to
unnecessary driving restrictions (Meng & Siren, 2012). Modifications in driving
behaviour for factors other than declines in the driving abilities (e.g. financial
reasons, lifestyle factors, affective factors) should not be regarded as self-regulation
as they do not necessarily result in improvement in safety. On the contrary, they
could cause the opposite effect.

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 55
Figure 3.3: Model of the process of driving self-regulation with ageing
From “Holding on and letting go: the perspectives of pre-seniors and seniors on driving self-regulation in later life” by Rudman, D., Friedland, J., Chipman, M. &
Sciortino, P., 2006a, Canadian Journal on aging, 25, p72.

56 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Driving as an Everyday Competence model for older adults (DEC) (2010)
This model (Figure 3.4) was developed by Lindstrom et al. (2010) through a
review of the literature on driving models and on models of everyday competence to
explain older adults’ level of competency and level of performance for driving. The
DEC model incorporates elements from Willis’s model of everyday competence,
Michon’s hierarchical model of driving, and Anstey’s model. Driving competence
refers to what an individual is “capable of given the dynamic interaction within and
between the individual and the environment” and it is not directly measurable
(Lindstrom-Forneri, Tuokko, Garrett, & Molnar, 2010). The model suggests that the
level of driving competence is determined by the interaction between the individual
and the environment and is moderated by beliefs and awareness. Further, awareness,
beliefs, and self-monitoring can have an impact on the strategic level driving process
which would be expected to impact driving performance. The model includes
various sociocultural factors (e.g. availability of alternative transportation options)
and psychosocial factors (e.g. beliefs about driving). Further, it demonstrates how
driving competence (what one is capable of) leads to driving performance (what one
does).
Figure 3.4: Driving as an Everyday Competence Model for Older Adults
From “Driving as an everyday competence: a model of driving competence and behaviour” by Lindstrom-Forneri, W., Tuokko, H., Garrett, D. & Molnar, F., 2010,
Clinical Gerontologist, 33(4), p. 284

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 57
Key determinants: the DEC model proposes that the interaction within and
between the individual and environmental factors at the global and specific
contextual levels determine the individual’s level of driving competence. Driving
performance is what the older driver does on road and is measurable. Driving
performance is the subsequent action resulting from interactions of the global factors,
specific contextual factors, and moderators and involves decisions made at the
strategic, tactical, and operational levels.
Limitations: the DEC model contributes to our understanding of the dynamic
individual-environment interaction associated with driving competence and driving
performance among older drivers. While the DEC incorporates many factors, it
lacks specificity about how these factors interact together (Wong, Smith, Sullivan, &
Allan, 2014).
Multilevel Older Persons Transportation and Road Safety model (MOTRS) (Wong et al., 2014)
The model was developed by Wong et al. (2014) through a systematic review
of 29 empirical studies which examines self-regulation of driving among older
adults. The model consists of four levels: socio-demographic variables at both
individual level (e.g. age, gender, health condition) and environmental level (e.g.
urban density, driving specific policies), driving specific variables at both individual
level (e.g. insight, driving experience, availability of driving partners) and
environmental level (e.g. availability of alternative transport options, road
conditions), psychosocial variables (driving confidence, perceived behavioural
control, perceived barriers, normative influence), and self-regulatory driving
behaviours. The MOTRS model proposes that socio-demographic and driving
specific factors predict older adults’ adoption of driving-related self-regulation
through their psychosocial influences.
The MOTRS model (Figure 3-5) adopts a connectionist framework and
assumes that the adoption of self-regulation is determined by a combination of
excitatory and inhibitory activation received in parallel from various socio-
demographic and driving specific factors through their collective influence on their
psychosocial variables. The MOTRS model accounts for the process of learning
through the use of bidirectional causal pathways, particularly at the level between
self-regulatory behaviours the psychosocial factors. These bi-directional pathways

58 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
allow learning to occur whenever error responses (e.g. a near-miss) are noted and
sent back through the network, a process called back propagation. In addition to
explaining the changes of attitudes and beliefs using back propagation, the MOTRS
model also accounts for the incremental process of such changes. In a connectionist
network, the recency and frequency with which a pattern has been activated
influence the ease and speed of subsequent activation when elicited by similar cues.
When a stimulus is introduced, learning changes weight of related activation
pathways, making the current and similar pathways easier to reproduce in the future,
sometimes at the expense of other unrelated pathways.
Key determinants: this model is rather comprehensive, incorporating many
factors that could influence self-regulation and allowing for them to interact in many
ways.
Limitations: the model does not specify detailed theoretical relationships
between these variables. It also views driving self-regulation as a unidirectional
process and therefore does not clearly describe the decision-making process. In
addition, the model was developed based on a systematic review of quantitative
studies examining the driving self-regulation process. Excluding qualitative
evidence, may have to capture important factors that have not been explored
previously in quantitative studies.
Figure 3.5: The Multilevel Older Person’s Transportation and Road Safety Model
From “Toward the multilevel older person’s transportation and road safety model: a new perspective on the role of demographic, functional, and psychosocial factors” by
Wong, I.Y., Smith, S., Sullivan, K. & Allan, A., 2014, Journals of Gerontology: Psychological Sciences, 71(1), p. 82

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 59
3.4 OTHER MODELS
These models are concerned with the driving cessation process among older
drivers rather than self-regulatory driving behaviours but will be presented here
briefly.
Classen et al. (2007): Precede-Proceed model
Classen et al. (2007) argue that the answer to the older driver safety issue can
be achieved through the adoption of an ecological approach to health promotion. An
ecological approach recognises that all aspects of a person’s environment are
considered as potential intervention targets, as well as the person’s own cognitions,
skills, and behaviour (Crosby & Noar, 2011). Therefore, they propose the use of the
PRECEDE-PROCEED model (PPM) as a framework within which various
individual and community theories can be utilised so that the most effective
intervention strategies can be implemented. The PRECEDE-PROCEED model is not
intended to predict or explain the relationship between predictors of certain
behaviour but to provide a framework for applying theories for planning and
evaluating health behaviour change programs (Glanz, Rimer, & Viswanath, 2008)
The model (Figure 3.6) has two separate components, the PRECEDE and the
PROCEED. The PRECEDE phase (Predisposing, Reinforcing, and Enabling
Constructs in Educational Diagnosis and Evaluation) constitutes the diagnostic and
assessment component of the model and provides a framework for systematically
assessing the social epidemiological, educational and ecological, and administrative
and policy aspects of a topic under study. The PROCEED (Policy, Regulatory and
Organisational Constructs in Educational and Environmental Development) or
intervention phase, recognises the impact of improved environmental and
organizational resources and services in improving health. Overall, the model has
eight phases, with the PRECEDE component comprising four phases and the
PROCEED component comprising four phases.
Classen and colleagues utilised a mixed-method approach to examine the main
epidemiological factors within the social context of older drivers in the United States.
Their first study employed a cross-sectional design where they analysed the 2003
Fatality Analysis Rating System dataset. This was followed by a metasynthesis

60 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
based on inductive and deductive analyses, of six qualitative studies. By integrating
the quantitative and qualitative findings, they identified 11 multi-causal factors for
safe driving among older drivers (previous motor vehicle convictions, passengers,
registered vehicle owners, principal impact, hour of the day, relation to junction,
traffic control device, vehicle manoeuvre, gender, road surface condition, state
policies) (Classen et al., 2007). Their health promotion intervention plan has two
intermediate outcomes (3 months-1 years); increased insight on risk and protective
factors and application of protective strategies. It also has three long-term outcomes
(1-5 years); decreased risk of crash and injuries, driving safer for longer, and use of
alternative transport options which can be achieved through behaviour change, policy
change, and creating safer roads and safer vehicles.
Figure 3.6: Precede-Proceed model of motor vehicle crashes among older drivers
From “Population-based health promotion perspective for older driver safety: conceptual framework to intervention plan” by Classen, S. et al., 2007, Clinical
Interventions in Aging 2(4), p. 691

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 61
This model can serve as a framework to assist researchers in choosing
theories that support the development of older drivers’ interventions. A great
advantage of the PPM is that it utilises both quantitative and qualitative data to
identify priorities and to establish the multiple factors related to the problem (Crosby
& Noar, 2011). Further it assumes that efforts to effect health behaviour change
must be similarly multidimensional in nature (Tramm, McCarthy, & Yates, 2012).
In this model, the improvement in the older drivers’ safety can be achieved through
changes in the driver behaviour, physical environment, social environment and
policies. The findings from this study highlights the importance of the physical and
social environment on older drivers’ safety, however, little attention is directed
towards the intrapersonal (e.g. confidence, self-awareness, perceptions) and
interpersonal (e.g. feedback and social norms) predictors of driving behaviours.
Further, age-based licensing systems are viewed as enabling factors in this model
that can influence older drivers’ safety (Classen et al., 2007). However, current
evidence points out that age-based testing is not recommended as they have no
demonstrable safety benefits (Tay, 2012). In addition, the model is rather exhaustive
and broad and it may be extensive, expensive, and unrealistic to identify
theoretically-consistent interventions to achieve changes in all of these outcomes
(Tramm et al., 2012). The complexity of the model and the complex nature of the
proposed outcome (crash reduction) might also make it difficult to evaluate
effectiveness. In other words, if crash reduction is to occur, it will be difficult to
conclude if the improvement of physical environment or the adoption of self-
regulatory behaviours was the reason.
Stress-coping framework: Model of interpersonal health behaviour (2012)
Choi and colleagues (2012) examined the process of driving cessation within
the stress-coping framework. Stress-coping models of health propose that the
individual’s ability to cope with stressors can affect the outcome and consequences
of stressful events (Choi, Adams, & Mezuk, 2012). Individuals vary widely in their
abilities to adapt to major life challenges and in the available resources that can assist
them to cope with this change. Therefore, the authors argue that the application of
the stress paradigm to the topic of the driving cessation process can help understand
the psychosocial and physical well-being of older adults in relation to their
environment. This can assist in the development of interventions based on personal,

62 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
environmental and social resources to minimise the negative impact of driving
cessation.
Their model (Figure 3.7) was derived from reviewing the literature on older
drivers and their driving behaviours. In their model, the primary stressors mainly
refer to health and functional declines, which involves cognitive impairment, visual
impairment, and functional impairment. Secondary stressors, on the other hand,
could be internal such as subjective discomfort or anxiety about driving or external
such as pressures on older drivers to stop driving. Older adults who experience any
of these stresses can adopt either an emotion-focused coping (e.g. denial or
avoidance) or problem-focused coping strategy. Emotion-focused coping can be
effective (e.g. acceptance of the need to stop driving or denial of the importance of
driving) or ineffective if it causes older drivers to assume they can drive safely
despite suffering from cognitive and/or visual impairments. Problem-solving coping
strategies involve making informed decisions (e.g. self-regulation of driving, use of
alternative transport or attending a refresher course). Personal, environmental, and
social resources can act as buffers between stressors and health and well-being. The
driving cessation process takes place within spatial (e.g., residential environment,
living arrangements) and temporal (e.g. transportation policy) contexts. In addition,
the driving cessation process can be influenced by various socio-demographic factors
such as age, gender, or marital status.

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 63
Figure 3.7: Conceptual model of driving cessation process
From “Examining the aging process through the stress-coping framework: application to driving cessation in later life” by Choi, M., Adams, K.B. & Mezuk, B.,
2011, Aging and Mental Health, 16(1), p. 78
This model offers a comprehensive framework of the driving cessation process
among older drivers. It recognises the heterogeneity of the older drivers and that the
driving cessation process may vary among different socio-demographic groups.
Older drivers, who are mainly influenced by internal stressors may be more likely to
voluntarily give up their car keys. On the other hand, the decision to stop driving
may be more involuntary among those more affected by external stressors.
Therefore, interventions could be perceived and accepted differently by the two
groups. The secondary internal stressors in this model refer to experiencing
difficulty due to lack of confidence and fails to identify the role of insight and self-

64 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
awareness in adopting self-regulatory driving behaviours. Therefore, this model
does not allow the examination of the impact of targeted interventions that can
provide older drivers with feedback to enhance their awareness. It therefore fails to
acknowledge the important role of health professionals, in-vehicle technology, self-
assessment tools and other resources that can help promote safe driving among older
adults. In addition, self-regulatory driving is viewed in this model as a coping
strategy to deal with the stresses associated with declining health among older
drivers. However, self-regulation is a broad and a multifactorial process that is not
yet completely understood. This model is therefore useful in assisting to develop
interventions targeted towards promoting the well-being and quality of life of retired
drivers rather than examining the driving regulation/cessation process.
3.5 LIMITATIONS WITH THE EXISTING MODELS
Figure 3.8: Challenges in examining older driver behaviour
Examining older drivers’ decision-making process towards the adoption of
self-regulation within a behaviour change theory is difficult given the uniqueness of
the driving behaviour (Fig. 3.8). For baby boomers, driving is the most reliable and
convenient mode of transport. It is a big part of their identity and offers them
freedom of mobility and independence. The declines in driving abilities are usually
gradual or subtle and it is very hard for older drivers to draw the impact of such
declines on their abilities. Even when they start noticing some changes, older drivers
may be reluctant to discuss their driving as they fear it may result in losing their
64

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 65
driving privelges (Betz et al., 2016). In addition, driving is a habitual process
(Caragata, 2017) that is not viewed as a harmful or risky behaviour (Kostyniuk et al.,
2000). The harms associated with driving are often attributed to “risky driving
behaviours” such as driving under the influence, speeding, or distraction. It might
be difficult for older adults to recognise how the declines in certain abilities affect
their driving and increase their risk of being involved in a crash. Older adults often
have mixed feelings of denial and disbelief about the need to change their driving
behaviour (Betz et al., 2016). Their lack of control over the decision-making (Liddle
et al., 2008) can create a peroid of uncertanity full of unexpected information and
charged emotion. It is crucial that in this early phase older adults receive feedback
about their driving abilities that increase their self-awareness and create a state of
“personal engagment”. Feedback in this phase should help them to accurately
calibrate their perceived abilities with their actual abilities. Accurate perception of
one’s driving abilities can help older adults to adopt efficient regulatory behaviour to
minimise their risk (Horswill et al., 2013). Previous studies suggest that insight into
declining functional abilities may be the trigger for self-regulation among older
drivers (Anstey et al., 2005; Blanchard and Myers, 2010; Charlton et al., 2006;
Molnar and Eby, 2008). Few studies have demonstrated that those who are aware of
declines in their abilities may practice self-regulation (Holland and Rabbitt, 1992;
MacDonald et al., 2008).
Once engaged, older drivers start weighing the pros and cons of modifying
their driving behaviours. Prioritising driving self-regulation is very difficult. Unlike
the motivation associated with other behaviour changes (e.g. improved health, losing
weight, etc.), there are no tangible or immediate benefits to adopting self-regulation
(other than perceived reduced risk of crash and perceived increased comfort). In
addition, the decision to stop driving usually has implications on other people not the
driver alone (e.g. becoming a burden, loss of the prinicpal driver). Previous studies
suggest that older drivers’ experiences, needs, facilitators and barriers of change are
entirely different and can change with time. Therefore, interventions should provide
older drivers with customised feedback based on their individual circumstances and
should incorporate the environmental and social factors that impact older drivers’
ability to modify their driving. Previous studies indicate that customised feedback is
effective in improving safe driving habits of older drivers (Lavalliere et al., 2012).

66 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
The longevity of the process may cause older drivers to become discouraged and
relapse back to their old driving behaviours particularly in the lack of feedback.
There have been several attempts to develop a model that can explain the
driving modification and/or cessation process among older adults. The existing
models vary considerably in regards to their development, determinants, and utilities.
Collectively, they identify several environmental, interpersonal, and intrapersonal
determinants that influence older adults’ driving behaviours. However, the
interaction between these factors and how and when they can induce the change is
not always clear. A major drawback of the existing models is failing to acknowledge
the heterogeneity of the older driver population in regards to their driving abilities,
their attitudes toward driving, their perception of their driving abilities, and their
surrounding environment. They also fail to recognise that older drivers go through
different stages of change and their experiences, needs, facilitators, and barriers to
change are entirely different and can change with time. Therefore, the target
participants (e.g., baseline stage of participants) and the desired outcomes would
influence the content and the strategies used to implement the intervention (Tuokko,
Rhodes, et al., 2014).
The stages of changes theories could be useful in describing and providing a
general understanding of change and planning interventions (Liddle et al., 2004). A
model developed by taking a strategic approach using both a theory of the change
process and existing evidence from previous attempts to achieve change is much
needed to help designing interventions for older drivers that are customised, based on
the individual (the baseline stage) and the anticipated outcome (increased awareness,
enhance self-monitoring, adoption of self-regulation, or planning cessation), and
flexible to move individuals through the stages of change towards adoption of safe
driving behaviour (Tuokko, Jouk, et al., 2014). However, there has been little
development of stage-based theories applied to driving self-regulation, and a lack of
research on theoretically-informed interventions that facilitate older drivers’ planning
for future self-regulation and even driving. Previous studies examining older
drivers’ behaviour within stages of change framework have either relied entirely on
qualitative findings without further validation (e.g. Kowalski et al., 2014) or have
been simplistic and have therefore not added much to our understanding of the
driving regulation process (e.g. Kostyniuk et al., 2001). There is a need for a model

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 67
that does not limit its focus to changes in driving exposure (driving restriction and/or
avoidance) but emphasises how older drivers cope with declining abilities by
adopting precautionary behaviours. The PAPM is a preventative decision-making
framework constructed around the goal of preventing or minimising future harm
ideal when dealing with complex behaviours which fits well with driving self-
regulation.
3.6 THE PRECAUTION ADOPTION PROCESS MODEL (PAPM)
Stages of change theories suggest that behaviour change is a dynamic and a
temporal process (Prochaska & Velicer, 1997) where individuals progress through a
number of stages towards action (Weinstein & Sandmand, 2002). The progression of
stages is determined by certain variables. People in similar stages face common
barriers to change and those in different stages face different barriers to change
(Weinstein & Sandmand, 2002). The progression through stages does not necessarily
terminate in action and people can relapse and regress through stages (Weinstein &
Sandmand, 2002). All stage theories share the same main elements outlined by
Weinstein (1998): 1). A classification system to define the stages, 2). An ordering of
the stages, 3). Common barriers to change facing people in the same stage, and 4).
Different barriers to change facing people in different stages.
Structure of the PAPM
The Precaution Adoption Process Model describes how individuals move
through stages of changes towards adoption of health protective behaviour
(Weinstein & Sandmand, 2002). The early stages of the PAPM are defined in terms
of psychological states and mindset of individuals (Weinstein & Sandmand, 2002).
The late stages are mostly governed by factors that can facilitate or hinder the
adoption of the precaution. Individuals progress through seven stages from lack of
awareness to action: unawareness (stage 1); awareness that there is an issue but a
lack of personal engagement with it (stage 2); engagement (“this applies to me”) but
indecision (stage 3) about the need to act; either a decision not to act (stage 4) or a
decision to act (stage 5); if the latter, acting by taking the precaution (stage 6) (e.g.
self-regulating); and maintaining the behaviour (stage 7). The unique feature of the
PAPM is that it deals with both the hazard and the precaution arguing that

68 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
individuals must first perceive a hazard of sufficient personal relevance before they
are ready to hear messages about adopting a precaution.
The PAPM does not offer explicit details about the barriers and facilitators at
each stage which allows for a more flexible framework that could be adapted to suit
each behaviour uniquely (Weinstein et al., 2008). Weinstein and colleagues provide
some suggestions about possible factors that can determine progression between
stages. For instance, the early stages of the PAPM is concerned about enhancing
people’s awareness and achieving personal engagement. This can be achieved by
providing information about the health issue and the protective behaviour,
communication from reliable individuals, and personal experience with the hazard.
In the third stage, perceived significance of the hazard, beliefs about the likelihood of
the health hazard, and fear may influence one’s decision about adopting the
protective behaviour. To facilitate the decision-making process, it is crucial that
individuals are aware about their susceptibility to the hazard and the effectiveness of
the suggested precaution. In the final stages, it is important to address the barriers
towards adopting the behaviour. Individuals may regress to an earlier stage,
however, they can never go back to stage 2 as they have acquired a certain level of
awareness and engagement (Weinstein & Sandmand, 2002).
Application of the PAPM in the older driver settings
The PAPM appears to be an attractive model for studying older adults’ self-
regulatory driving behaviour for the following reasons:
1.) It emphasises that self-awareness of risk (e.g. compromised safety due to
driving limitations) is the first step to initiate change among individuals.
As outlined before, there is a considerable support that self-awareness is the
key towards modifying behaviour.
2.) It differentiates between those who are unaware about the hazard and never
thought about acting and those who have thought about acting and are still
undecided (unlike the TTM which groups them as the pre-contemplators).
This differentiation is important because those who have thought about
acting are more likely to be more knowledgeable, have different responses
to information and are more resistant to persuasion (Ditto & Lopez, 1992).
In the context of driving, information regarding declining driving abilities

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 69
which could subsequently require cessation of driving or modifying one’s
driving behaviour would often be viewed as undesirable information. If
someone has already formed an opinion about their driving abilities they
will have a greater tendency to adhere to their opinion; what is known as
“confirmation bias,” or “perseverance of beliefs” (Weinstein et al., 2008).
3.) The early stages of the PAPM deal with the attitudes and beliefs people
hold about the hazard and precaution while the later stages deal with
addressing barriers; whether internal or external, towards adoption of
change. This differentiation is important because while some people may
be aware and willing to change they may be unable to change their
behaviours.
4.) It offers a flexible framework with no clear information on what determines
transition between stages and therefore could be adapted to suit each
behaviour uniquely.
5.) It is concerned with the adoption of precaution or cessation of risky
behaviour which requires deliberate planning. Self-regulation of driving
refers to the driving behaviour modifications one adopts in attempt to
improve their safety. It is therefore a conscious process that requires active
planning. Modifications of driving behaviours for reasons other than
improving one safety (e.g. affective coping or lifestyle factors) is not
considered as self-regulation.
As discussed before, there has been limited application of the PAPM within
the older driver population. Kostyniuk and colleagues (2000) were the first to
highlight the potential use of the PAPM in understanding the older adults’ driving
behaviour. Their study was the initial step towards developing a behavioural
framework of driving reduction and cessation among older drivers where they
investigated the impact of drivers’ perception of their driving abilities on their
driving reduction and cessation. Their findings suggest that anticipation of problems
in driving ability may be the trigger for driving reduction which satisfies the initial
condition of the PAPM (Kostyniuk et al., 2000). The adaptation of the PAPM in their
study was not fully described, and was based mostly on older adults’ awareness of
their declining abilities but failed to recognise the influence of other external and
internal factors on the process of self-regulation.

70 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Coxon and colleagues (2017) conducted a randomised controlled trial among
366 older drivers aged 75 years and above where intervention group participated in
an individualized, one-on-one safe-transportation program adapted from the
Knowledge Enhances Your Safety curriculum delivered in two sessions held
approximately 1 month apart. Further, the education messages were customised to
the behavioural change of each participant using the PAPM (Coxon et al., 2017).
Participants were followed for over 12 months where distance driven measured using
in-vehicle monitoring was examined. Secondary outcomes for driving exposure
included night driving, farthest radial distance driven from home, and self-reported
driving space. While intervention group participants showed greater readiness to
engage in self-regulatory driving practices, distance driven per week, use of
alternative transport and community engagement were similar between the two
groups (Coxon et al., 2016).
This could be attributed to the nature of the intervention provided.
Educational interventions can raise older drivers’ knowledge about existing issues
and problems but it may be difficult to translate into well-formulated instructions.
They often lack the practical component and training necessary to assist older drivers
in recognising the actual problems they face on the road. The intervention will vary
not only on the participant’s stage, but the desired outcome and their surrounding
environment. The content of the education intervention was tailored based on the
PAPM stage of the participants. However, an educational intervention may not be
the best type of strategy to promote the change for all of the participants or
participants may have not perceived it as useful. Second, the intervention did not
translate into reduced mileage or changes in driving exposures using objective
measures of driving. Driving reduction is not an indication of self-regulation, but
mostly reflect lifestyle choices. Participants may have engaged in different
regulatory behaviours that were not measured in this study (e.g. self-monitoring,
restriction and avoidance, and life goal changes).
3.7 CHAPTER SUMMARY AND IMPLICATIONS
This chapter summarises the existing models of older adults’ driving
behaviour. While the PAPM has been gaining recent attention in the older drivers’
literature, there is still considerable gaps in our understanding of how (if possible) it
can explain older drivers’ regulatory behaviour.

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 71


The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 73
Chapter 4: Research Design
4.1 INTRODUCTORY COMMENTS
This chapter summaries the research design and methodology adopted to obtain
the aims and objectives outlined in Chapter 1. The chapter’s structure is as follow:
section 4.2 describes the specific research questions that will be examined in the
studies, section 4.3 discusses the mixed method research design implemented,
section 4.4 presents the recruitment strategies and participants’ characteristics;
section 4.5 describes the instruments used in the study; section 4.6 outlines the data
management and data analysis; section 4.7 presents the organisation of the papers
and, finally section 4.8 discusses the ethical considerations of the research
4.2 RESEARCH QUESTIONS
This program of research aims to examine the applicability of the Precaution
Adoption Process Model in understanding older adults’ self-regulatory driving
behaviour, specifically, to develop a comprehensive model that explains and
describes the process of driving self-regulation guided by the PAPM. A novel
approach using Latent Class Analysis (LCA) is employed to empirically validate or
reject the developed model. The research aim is addressed through four research
questions.
Research Question 1
Can older drivers be grouped into different stages of PAPM based on their
qualitative differences (e.g. attitudes, awareness, and perceptions) and patterns of
change?
The first research question is addressed in Study 1 presented in Chapter 5. The
PAPM has been explored previously in relation to driving behaviours among older
adults; however, this description has been very simplistic. This research question
provides the opportunity to obtain in-depth understanding of the process of driving
self-regulation among older adults by exploring their perceptions and experiences of
self-regulation. In addition, this research question constitutes the basis of this
program of research by exploring the preliminary fit of older adults’ driving
behaviour within the PAPM framework using qualitative focus groups among current

74 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
older drivers. The process of driving self-regulation starts by older drivers’
awareness of the need to change. This is followed by a decision-making process
where individuals weigh the pros and cons of modifying their driving. Once a
decision is reached, environmental and psychological barriers influence older adults’
ability to adopt such change. The findings from the study guided the development of
a preliminary model of older drivers’ self-regulatory behaviour. The choice of the
PAPM as the theoretical underpinning of this research has been discussed before.
The conceptual model served as a framework for the quantitative study. The
findings also informed the development of the questionnaire used in study 2.
Research Question 2
What is the prevalence of the stages of the PAPM in the study population and what
are the psychosocial and environmental factors associated with stages of the PAPM?
This research question is addressed in the second study presented in Chapter 6.
Participants were assigned into different stages of the PAPM based on a commonly
used stage algorithm. The aim of study 2 was to investigate the prevalence of PAPM
stages within a sample of older drivers. Further, the study aimed to identify the
psychosocial and environmental factors associated with different stages of the PAPM
and those that predict the decision to adopt self-regulatory behaviour which may be
worthy for further investigation.
Research Question 3
Would groups, identified utilising Latent Class Analysis (LCA), match those in the
conceptual model?
This research question investigated whether older adults’ self-regulatory driving
behaviour is truly a reflection of the stages of change described by the PAPM. To
achieve this, a bottom-up approach to profile older drivers based on their mindset
towards adopting self-regulatory driving behaviours using Latent Class analysis was
employed. Latent Class Analysis is a person-centred approach used to identify
subgroups with distinctive patterns. The selection of LCA indicators was guided by
the PAPM and involved driving perception, importance of driving, and barriers
towards change. The identified classes were described in terms of socio-
demographic factors, alternative transport use, and self-reported avoidance
behaviour. Findings from the LCA will assist in validating, refining, or rejecting the

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 75
conceptual model. There are three possible outcomes from conducting the LCA.
The sample may not contain different groups of driving behaviour, based on the
selected indicators. This outcome will therefore reject the hypothesis that PAPM can
describe older adults’ driving behaviour. The sample may contain subgroups of
older drivers that corresponds with the PAPM stages of change and therefore would
support the use of the PAPM. Finally, the sample may contain subgroups of older
drivers but does not correspond to the PAPM; which could indicate that there are
alternative ways to group older drivers.
Research Question 4
Can providing older adults with customised and evaluative feedback assist in
stage transition and modify their willingness to change their driving
behaviour?
This research question was addressed in study 3 where older drivers received
evaluative and customised feedback from a driving instructor. The literature
suggests that providing older drivers with feedback from someone they trust can help
enhance their awareness about limitations in their driving. The impact of such
feedback on participants’ insight and willingness to change was examined along with
participants’ opinions in regards to the usefulness of this feedback.
4.3 RESEARCH DESIGN AND METHODOLOGY
The research program used a mixed method approach comprised of two studies
that follows an exploratory sequential process. This was followed with a third
experimental study that assessed the impact of feedback on PAPM stage transition.
This design was chosen as the newness and complexity of the topic meant it is best to
explore the theory first qualitatively and to follow up with a quantitative study to
confirm the findings (Creswell & Plano, 2011). Further, mixing qualitative and
quantitative methods can help provide a more comprehensive understanding of the
research topic (Hesse-Biber, 2010) and can overcome the limitations of each
individual method, “producing richer and more rigorous understandings” of the
topic being studied (Creswell & Plano, 2011). Prior to conducting the first study, a
thorough review of the existing models of older drivers’ behaviour was conducted to
gain a better understanding of the various factors that affect the older adults’
regulatory behaviours. This later assisted in the developing of the conceptual model

76 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
along with the findings from study one. Study one involved qualitative focus groups
among older drivers to explore the applicability of the PAPM and to explore specific
aspects of their driving behaviour. The findings assisted in the development of the
questionnaire used for the quantitative survey. The second study was quantitative in
nature and further examined whether older drivers can be categorised within PAPM
stages and the sociodemographic and psychosocial factors associated with each
stage. The findings from study two are intended to provide further support for the
use of PAPM and to assist in refining the conceptual model. Study three was
experimental in nature and attempted to identify the impact of providing customised
feedback on the progression of stages of the PAPM. A flowchart of the research
program is presented in Figure 4.1.
4.4 SETTING, POPULATION, AND RECRUITMENT
The study was conducted in Queensland, Australia. The population of interest
for this research program were adults aged 70 or over who were still driving. A
convenience sampling technique was used to recruit potential participants. For the
focus group study and the quantitative survey, participants were required to be
English-speaking adults aged 70 years or over who hold a current valid driving
license. Various recruitment strategies were employed to ensure sample variability
including flyers posted in seniors’ clubs, geriatric clinics, and local shopping centres
and through social media. However, this strategy did not prove successful, so an
advertisement was placed in a Sunshine Coast seniors’ newspaper where people
interested in participating were encouraged to contact the research team. For the
experimental study, participants were drivers aged 70 or above who were either self-
referred or referred to the Royal Automobile Club of Queensland (RACQ) by their
doctor for an on-road driving assessment.

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 77
Figure 4.1: Flowchart of the research program
4.5 METHODS
Qualitative study
The qualitative data were collected through focus groups. A semi-structured
discussion guide was developed based on current literature on older drivers and the
research questions informed by the PAPM. Detailed description of the method is
provided in Chapter 5.
Literature Review of the
existing models of older
drivers’ behaviour
Qualitative Research
Focus group discussions
among current older drivers
Combine findings from the qualitative research and the literature review to:
-Develop a conceptual model of older drivers’ behaviour based on the PAPM
-Develop the questionnaire for the quantitative study
Quantitative Research
Online and paper-based survey
among current older drivers
Latent Class Analysis
-To identify subgroups of older drivers and determine whether they match those identified
by the PAPM
Refining the model
Experimental study
-To determine the impact of providing customised feedback on the progression of
stages of the PAPM.

78 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Quantitative survey
Participants completed a questionnaire online or in a paper-based form with a
paid return envelope. Both questionnaires included an information sheet describing
the nature of the study and completing the questionnaire was considered evidence of
consent to participate. The questionnaire design was based on the qualitative study
findings and the literature review and collected information on socio-demographics
(age, gender, education, employment, etc.), self-rated health, crash history, driving
experience, current driving patterns, driving perceptions, feedback about driving and
transport options of older drivers. In addition, participants’ driving reduction and
avoidance behaviours were collected. Participants were classified into PAPM stages
based on their responses using an algorithm developed along similar lines to the one
used by Weinstein and Sandman (2002) (Table 4-1). Detailed description of the
questionnaire items is provided in Chapter 6.
Table 4.1: Precaution Adoption Process Model: Stage Classification Algorithm as
applied to self-regulatory driving behaviours among older adults (Adapted from
(Weinstein & Sandmand, 2002)) PAPM Stage Algorithm
Stage 2
Unengaged
Some other older drivers need to change their driving, but I believe that I
am a safe driver and have never thought about the need to change my
driving
Stage 3
Undecided
I am at the point where I am not sure if I should start thinking about ways
to avoid certain driving situation or reduce my driving
Stage 4
Resisting action Avoiding certain driving situations would be pointless to me
Stage 5
Planning to act I am planning to avoid certain driving situations and reducing my driving
Stage 6
Acting
I have just recently started to avoid challenging driving situations or drive
less
Experimental study
Prior to the assessment session, the driving instructor handed eligible
participants an information sheet describing the nature of the study. Participants
were then asked to complete a pre-test questionnaire that collect information on the
socio-demographics (age, gender, education, employment, etc.), self-rated health,

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 79
crash history, driving experience, current driving patterns, driving perceptions,
feedback about driving and transport options of older drivers. In addition,
participants’ driving reduction was measured by asking participants to rate the
overall amount of their driving compared to ten years ago on a 4-point scale from
“much less” to “more”. The driving assessment takes around 50 minutes to
complete. The driver instructor gives participants clear instructions as they start
driving in their familiar surroundings. If deemed safe, they start progressing to
busier and heavy traffic. The driving instructor assess participants based on a range
of driving skills. After the driving assessment, participants completed a post-test
questionnaire which collected information regarding the impact of receiving
feedback on changes in their perception and willingness to modify or change their
driving behaviour. Information regarding the usefulness of this type of feedback was
also collected.
4.6 DATA MANAGEMENT AND DATA ANALYSIS
For the qualitative focus group, thematic analysis was conducted following the
process outlined by Braun and Clarke (2013) to identify, analyse and report themes
within the data. Transcripts were read through carefully to gain familiarity with the
data content and to detect meaningful topics across the transcripts. Small sections of
the transcripts were initially coded, followed by an initial identification of themes
and collation of similar codes within themes (Braun & Clarke, 2013). The
supervisors independently conducted analyses of a sample of the transcripts.
The quantitative survey data were coded, entered and checked. Data coding for
each question, missing values and invalid answers were recorded in a code book.
Data were entered in the SPSS software version 20. Data checking was conducted by
checking for outliers, identifying genuine missing data, and assessing the distribution
of the data. Checks were performed by conducting descriptive statistics for
continuous and categorical variables. For continuous variables, the mean, standard
deviation, median, minimum, maximum, and skewness were calculated. For the
categorical variables, checks were performed by studying the proportion of cases in
each category. Normality of the continuous variables was examined by assessing
whether the mean values were within ± 10% of the median values and if the Z-score
obtained by dividing the skewness by its standard error was ≥-3 or ≤ 3, and
histogram was used as a measure of visual assessment. If data were normally

80 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
distributed, then bivariate analyses were conducted using parametric tests such as the
independent samples t-test and Pearson’s correlation. When data were not normally
distributed, non-parametric tests such as the Mann-Whitney U test were used. For
categorical variables, bivariate analyses were conducted by performing Pearson's chi-
squared test. For multivariable regression analyses, checks for multicollinearity were
performed by screening Pearson’s correlation matrices and/or computing variance
inflation factor. Multicollinearity was assumed to not be an issue if the variance
inflation factor for all variables were below 10. Latent class analysis is a person-
oriented statistical procedure that identifies unobservable subgroups within a
population based on certain pattern of observed responses (Hagenaars, McCutcheon,
& ebrary, 2002). For this study, LCA was exploratory and no assumption of specific
number of classes was made. The selection of the appropriate number of classes
depends on a number of fit indices. The procedure starts by running model with the
lower number of classes and gradually increasing number of classes while comparing
the fit indices (Geiser, 2013). Lower values of Bayesian Information Criteria (BIC),
the Akaike Information Criteria (AIC), and the sample size adjusted BIC indicate
better fit (Geiser, 2013). However, the BIC is regarded as a more reliable indicator
of model fit (Nylund, Asparouhov, & Muthén, 2007). Entropy is an index from zero
to one that is used to evaluate the precision of assigning latent class membership;
with a value of one indicating the individuals are perfectly classified into their latent
classes (Geiser, 2013). Further, the Vuong-Lo-Mendell-Rubin Likelihood Ratio Test
(VLMR LRT) is another indicator of model fit that provides a p value of the model
strength over a model with one fewer class (Geiser, 2013). Significant p values on
the VLMR LRT indicate that the current model is a significantly better fit for the
data than a model with one fewer class (Nylund et al., 2007). Given the nature of the
research, the theoretical implications guided decisions regarding the most appropriate
number of classes. Statistical analysis was conducted using SPSS and MPLUS 7.
4.7 ORGANISATION OF PAPERS
The papers are organised according to the four research questions of the
research program (Fig 4.2). Study one is presented in Chapter 5 as taken from Paper
1. Papers 2 and 3 relate to study two of the research program and are presented in
Chapter 6 and Chapter 7 respectively. Chapter 8 presents study three which is under
review.

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 81
Study 1 – Chapter 5 R.Q.1 Can older drivers be grouped into different stages of PAPM based on their qualitative differences (e.g. attitudes, awareness, and perceptions) and patterns of change? Published paper full title: The perspectives of older drivers on the impact of feedback on their driving behaviours: a qualitative study Sample: N=27 current Australian drivers aged 70 years and more Design and Method: Qualitative focus groups Analysis: Thematic analysis
Study 2- Chapter 6 First phase R.Q. 2 What is the prevalence of the stages of the PAPM in the study population and what are the psychosocial and environmental factors associated with stages of the PAPM? Published paper full title: Examination of the Precaution Adoption Process Model in understanding older drivers’ behaviour: an exploratory study Sample: N=222 Australian drivers aged 70 years and more Design and Method: Quantitative survey Analysis: Logistic regression
Study 2 – Chapter 7 Second phase R.Q.3 Would groups, identified utilising Latent Class Analysis (LCA), match those in the conceptual model and those of the staging algorithm? Submitted paper full title: Older adults’ self-regulatory driving behaviour: Results of a latent class analysis Sample: N=222 current Australian drivers aged 70 years and more Design and Method: Quantitative survey Analysis: Latent Class Analysis
Study 3 – Chapter 8
R.Q.4 Can providing older adults with customised and evaluative feedback modify their willingness to change their driving behaviour? Unpublished chapter Sample: N=21 drivers
Design and Method: pre-post-test design
Figure 4.2: Organisation of the papers
4.8 ETHICS APPROVAL
Ethical clearance to conduct the study was obtained from the Queensland
University of Technology Human Research and Ethics Committee (Approval number
1200000501). Consent for participation was obtained from eligible participants who
were instructed that their participation is entirely voluntary and withdrawal from the
study will not result in any penalty. If requested, all information provided by the
withdrawn participant would be completely destroyed. Participants were also
guaranteed that their confidentiality would be maintained and findings of the
research were reported anonymously. For the survey and final experimental study,

82 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
completion of the questionnaire was evidence of consent. The collected data were
treated with the confidentiality and were reported upon in an aggregate way to mask
the identity of the individual participants. In addition, the research materials were
stored locked, in the office of the researcher. The computer data were stored and
password protection, while backup copies were kept on a USB drive in locked filing
cabinets. As required by the Queensland University of Technology, the
questionnaires and coded information were, and will be, kept under strict security, at
all times, by the researcher, being stored for the required period of five years, and
then destroyed.

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 83
Chapter 5: The perspectives of older drivers on the impact of feedback on their driving behaviours: a qualitative study (Study 1)
5.1 PUBLICATION STATUS
This chapter comprises Paper 1 as taken from:
Hassan, H., King, M., & Watt, K. (2015). The perspectives of older drivers on the
impact of feedback on their driving behaviours: a qualitative study. Transportation
Research Part F, 28, pp. 25-39.
5.2 STATEMENT OF CONTRIBUTION
The candidate, as first author, accepts the overall responsibility for this
publication. The candidate was responsible for all aspects of the manuscript
preparation, including reviewing the literature, formulating the research question,
conducting and supervising data collection, analysing and interpreting the results and
writing and submitting the final manuscript. All co-authors meet the criteria for
authorship and take responsibility for their role in delivering the publication. All of
the co-authors of this paper are members of the candidate’s supervisory team and
their contribution to this paper was supervisory in nature. Written permission was
provided from each to include the publication as part of this thesis and its publication
on the QUT ePrints database.
The authors listed below have certified that:
1. they meet the criteria for authorship in that they have participated in the
conception, execution, or interpretation, of at least that part of the publication in their
field of expertise;
2. they take public responsibility for their part of the publication, except for the
responsible author who accepts overall responsibility of the publication;
3. there are no other authors of the publication according to these criteria;

84 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
4. potential conflicts of interest have been disclosed to granting bodies, the
editor or publisher of journals or other publications, and the head of the responsible
academic unit, and
5. they agree to the use of the publication in the student’s thesis and its
publication on the QUT’s ePrint site consistent with any limitations set by publisher
requirements.
Principal Supervisor Confirmation
I have sighted email or other correspondence from all Co-authors verifying their
authorship
Dr Mark King QUT Verified Signature 30 Aug 2017
------------------------- ----------------------------------- ------------
Name Signature Date

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 85
The perspectives of older drivers on the impact of feedback on their
driving behaviours: A qualitative study
Heidy Hassan a, Mark King b, Kerrianne Watt c
a The Centre for Accident Research and Road Safety – Queensland (CARRS-Q), GPO Box 2434, Brisbane, Queensland, Australia. Corresponding author. Tel: +61731387727. Email: [email protected] b The Centre for Accident Research and Road Safety – Queensland (CARRS-Q), GPO Box 2434, Brisbane, Queensland, Australia c School of Public Health, Tropical Medicine and Rehabilitation Sciences- James Cook University, Townsville, Queensland, Australia Highlights
• Focus group sessions were conducted with older drivers. • We explored older drivers’ perceptions and experiences of self-regulation,
using the Precaution Adoption Process Model as a framework. • We also investigated the possible impact of feedback on their decision-
making process. • Relevant issues that should be further investigated are discussed
5.3 ABSTRACT
Self-regulation is a coping strategy that allows older drivers to drive safely for
longer. Self-regulation depends largely on the ability of drivers to evaluate their own
driving. Therefore, the success of self-regulation, in terms of driving safety, is
influenced by the ability of older drivers to have insight into their declining driving
performance. In addition, previous studies suggest that providing feedback to older
adults regarding their driving skills may lead them to change their driving behaviour.
However, little is currently known about the impact of feedback on older drivers’
self-awareness and their subsequent driving regulatory behaviour. This study
explored the process of self-regulation and driving cessation among older drivers
using the PAPM as a framework. It also investigated older adults’ perceptions and
opinions about receiving feedback in regards to their driving abilities. Qualitative
focus groups with 27 participants aged 70 years or more were conducted. Thematic
analysis resulted in the development of five main themes; the meaning of driving,
changes in driving pattern, feedback, the planning process, and solutions. The
analysis also resulted in an initial model of driving self-regulation among older
drivers that is informed by the current research and the Precaution Adoption Process

86 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Model as the theoretical framework. It identifies a number of social, personal, and
environmental factors that can either facilitate or hinder people’s transition between
stages of change. The findings from this study suggest that further elaboration of the
PAPM is needed to take into account the role of insight and feedback on the process
of self-regulation among older drivers.
Keywords Older drivers; Feedback; Self-regulation; Awareness; PAPM; Behaviour; Perception
5.4 INTRODUCTION
In Australia, it is estimated that the proportion of people aged 65 years and
more will increase from 13% in 2007 to approximately 25% in 2056 (ABS, 2008).
As the population ages, there will be an increased number of older licensed drivers
on our road system (King et al., 2011). Moreover, as the baby boomers age, they
will be driving more than previous generations (Wang & Carr, 2004). In
Queensland, drivers aged 60 years and above are over-represented in fatal and life-
threatening crashes and their involvement increases steadily with age (Rakotonirainy
et al., 2012). Furthermore, drivers aged 80 years and above are most likely to be at a
fault for injury or death-related crashes (Rakotonirainy et al., 2012). As a result, the
safety of older drivers has been receiving more attention from road safety researchers
in recent years.
Ageing is associated with non-pathological changes in the sensory, motor,
and cognitive functions that can impair people’s ability to safely operate a motor
vehicle (Molnar, Eby, St. Louis, & Neumeyer, 2007). Nevertheless, there is a
considerable variation in how individuals experience these declines (Eby, Trombley,
Molnar, & Shope, 1998) and the impact of such declines on actual crash risk is not
always fully known (Whelan et al., 2006). Further, older adults consider driving to
be key to their independence and mobility (Molnar et al., 2007). Restricting or
stopping driving can be associated with increased risk of depression (Ragland et al.,
2005), isolation (Fonda et al., 2001), and entering long-term care facilities (Freeman
et al., 2006).

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 87
Previous studies have indicated that some older adults adopt strategies to
reduce their crash risk while maintaining their driving, a process known as self-
regulation. Self-regulation has been defined as “the adjustments made by drivers in
their driving behaviour that adequately match changing cognitive, sensory and motor
capacities” (Charlton et al., 2006) which largely depends on the individual’s ability
to monitor his/her driving ability (Anstey et al., 2005). Common examples of self-
regulation seen in older drivers include reducing their overall amount of driving and
avoidance of various driving situations (e.g. avoiding driving at night or peak hours,
travelling shorter distances) (Anstey & Smith, 2003; Baldock et al., 2006a; Charlton
et al., 2006). Driving cessation is sometimes viewed to be the end result of the
process of self-regulation among older drivers (Dellinger et al., 2001; Lyman et al.,
2001). While uncommon, driving cessation can occur unexpectedly as a result of
sudden illness, involvement in an accident, or failing a driving test (Dellinger et al.,
2001). However, driving cessation is more of a gradual and voluntary process
whereby the driver will gradually increase self-imposed restrictions until ultimate
cessation (Dellinger et al., 2001; Hakamies-Blomqvist & Wahlström, 1998).
The question remains as to whether older drivers can accurately adjust their
driving in response to their age-related declines. The literature suggests that self-
awareness and insight into driving ability play a major role in successful driving
regulation among older drivers (Anstey et al., 2005). It is argued that individuals
who lack awareness of their abilities and limitations may engage in behaviours that
compromise their safety and the safety of those around them (Marottoli &
Richardson, 1998). In addition, older drivers who are aware of declines in their
abilities are more likely to practice self-regulation than those who are less self-aware
(Blanchard & Myers, 2010; Holland & Rabbitt, 1992). Lack of adequate support and
feedback can impact older people’s ability to make an informed decision about the
future of their driving. This can result in some older people stopping driving
prematurely while other continues to drive where it is not safe to do so (Berry, 2011).
Feedback may assist older drivers to appropriately monitor their driving and thus
results in proper adjustments in their driving behaviours.
Furthermore, the driving cessation process may occur through stages, and
interventions and feedback may be perceived differently at each stage (Kostyniuk et
al., 1998). This suggests that older driver interventions should be tailored to the

88 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
specific needs of each individual (including the stage they are at) and recognizes that
older adults should not be treated as a homogenous group. Such interventions would
therefore need to be customised to move individuals through the stages of change
towards adoption of safe driving behaviour. They would be developed by taking a
strategic approach using both a theory of the change process and existing evidence
from previous attempts to achieve change. However, there has been little
development of stage-based theories applied to driving self-regulation, and hence a
lack of research on theoretically-informed interventions that facilitate older drivers’
planning for future self-regulation and even driving cessation. There is also a lack of
consideration about the role of feedback about behaviour in the stage process, such
as responsiveness to feedback, acceptable sources of feedback, and ability to modify
behaviour in relation to feedback. This research aims to contribute to the
development of a theoretical framework for a stage-based process leading to self-
regulation of driving which incorporates the role of feedback, with the intention of
testing the theoretical approach in future research with older drivers.
The research approach builds on existing theory rather than starting from a
blank slate. The stage-based theoretical model used as the basis for the study is the
Precaution Adoption Process Model, or PAPM (Weinstein et al., 2008), which
provides a framework for understanding why older drivers adopt self-regulatory
(precautionary) behaviours intended to reduce their road crash risk. The PAPM
assumes that people need to be aware of the risk associated with their behaviour
before they are susceptible to behavioural change, and that awareness of the risk is
not necessarily enough to lead them to change their risk behaviour. It characterises
seven stages along the path from lack of awareness to action (Figure 5.1):
unawareness; awareness that there is an issue but a lack of personal engagement with
it; engagement (“this applies to me”) but indecision about the need to act; either a
decision not to act or a decision to act; if the latter, acting by taking the precaution
(e.g. self-regulating); and maintaining the behaviour. In each stage the types of
information and interventions needed to move people closer to action vary. The
greatest advantage of such a stage theory is that messages or other interventions can
be tailored for people at different stages. Interventions targeted at increased
awareness of risk and precaution effectiveness can move people between early stages

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 89
while later stages require interventions that address barriers to adoption of the
precaution.
Figure 5.1: Stages of the Precaution Adoption Process Model- Source: (Weinstein & Sandmand, 2002).
The PAPM has been used previously to study adoption of behaviours related
to osteoporosis prevention (Mauck et al., 2002), disaster preparedness (Glik,
Eisenman, Zhou, Tseng, & Asch, 2014), epilepsy (Elliott, Seals, & Jacobson, 2007),
colorectal cancer screening (Costanza et al., 2005), fruit intake (De Vet, De Nooijer,
Oenema, De Vries, & Brug, 2008), coping with premenstrual syndrome (Delara et
al., 2012), and home radon testing (Weinstein, Lyon, Sandmand, & Cuite, 1998).
In relation to driving, the PAPM has been explored by Kostyniuk et al., 2000
in which they argue that the use of the PAPM is a productive way to look at how
older drivers cope with age-related declines and their willingness to make changes in
response to these declines. Their description of the process of driving self-regulation
begins with driver acknowledgement of potential future problems with driving
ability, followed by awareness of their experience of increasing difficulties with
driving, and eventual avoidance of difficult driving situations (Kostyniuk et al.,
2001). Unfortunately, the adaptation of the PAPM in this study was not fully
described, and was based mostly on older adults’ awareness of their declining
abilities, i.e. it failed to recognize the influence of other external and internal factors
on the process of self-regulation. For example, external factors such as a lack of
alternative transport, and internal factors such as self-efficacy with respect to the
precautionary behaviour (“can I successfully regulate my driving?”) may interfere
with adoption of self-regulation in spite of awareness of the problem.

90 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Nevertheless, the applicability of the PAPM to examine the driving
behaviours among older adults deserves further consideration. An attractive feature
of this model is that it deals with both the hazard and the precaution. It claims that
for individuals to consider adopting a precaution they must first perceive the hazard
to be of sufficient personal relevance. The age-related declines in people’s sensory,
motor, or cognitive functions are often subtle and gradual which can make it difficult
for older people to draw the link between these changes and the impact on their
driving ability. Interventions should encourage people to adequately regulate their
driving without imposing unnecessary restrictions or stopping driving prematurely.
Therefore, the early stages of the PAPM emphasize the importance of increasing
people’s awareness about the impact of ageing on their driving ability. While it is
highly likely that older adults are “generally aware” about the safety issues of older
drivers, they could lack “self-awareness” or insight into their own driving ability.
Once they become personally engaged with the hazard, people are more likely to be
more receptive towards adoption of the precaution.
Therefore, the main aim of this study was to further understand the process of
driving self-regulation among older adults by exploring their perceptions and
experiences of self-regulation, using the PAPM as a framework, and in particular to
investigate the possible impact of feedback on their driving on their decision-making
process. Further aims were: to determine the applicability of the PAPM to the self-
regulatory behaviour of older drivers and how it could be elaborated; to identify
barriers and facilitators to the progression of drivers between stages; and to identify
the current limitations and problems with the feedback older drivers are currently
receiving. The intention was not to support or reject the PAPM, but to use it as a
starting point for theory development.
A qualitative study design using focus groups was chosen to explore
participants’ perceptions of driving cessation and the impact of feedback on their
decision-making process. Qualitative research is appropriate given the theoretical
issues raised above. There has been limited application of stage-based approaches
such as the PAPM to older driver self-regulation and there is a consequent need to
pursue an exploratory approach, especially in regard to the role of feedback. Focus
groups are useful in exploring under-researched areas as they do not require any
prior empirical knowledge about the issue (Braun & Clarke, 2013). In addition,

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 91
focus groups can elicit a wide range of views, perspectives, or understanding of an
issue (Braun & Clarke, 2013).
5.5 METHOD
Recruitment
The research was conducted in the Brisbane and Sunshine Coast areas of the
state of Queensland, Australia. The estimated population of Queensland in 2012 is
4.5 million with 13.1 % of Queenslanders aged 65 years and over. In 2011, females
outnumbered males in the 75 years and above age groups (ABS, 2011). Females
were also more likely to be living alone with 33.8% of women aged 65 years and
over living alone compared with 18.4% of older men (ABS, 2011). Driving is the
preferred mode of transport in this area (Liddle, Turpin, Carlson, & McKenna, 2008)
and the licensing authority is Queensland Transport and Main Roads. Drivers aged
75 years and above are required to carry a valid medical certificate obtained from
their doctor. Participants were required to be English-speaking adults aged 70 years
or over. Initially recruitment was aimed at former drivers as well as current drivers
because of the importance of their perspective on the driving cessation process and
the feedback they received during this process. However, only one former driver
contacted the research team, probably due to the sensitive nature of the topic and/or
the difficulty in getting to the sessions, so only current drivers were used. Various
recruitment strategies were employed to ensure sample variability including flyers
posted in seniors’ clubs, geriatric clinics, and local shopping centres and through
social media. However, this strategy did not prove successful. The first author was
interviewed on local radio (on the Sunshine Coast) to promote the study and to solicit
older drivers, however only four participants responded. Finally, an advertisement
was placed in a Sunshine Coast senior’s newspaper where people interested in
participating were encouraged to contact the research team. This led to recruitment
of further 23 participants to give a total sample of 27, all of whom were current
drivers with 10 or more years of experience. Because only three participants resided
in Brisbane and the remaining participants were from the Sunshine Coast area, one
focus group session of four participants took place in Brisbane and the remaining
four sessions took place in Caloundra, a city on the Sunshine Coast.

92 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Participants
Twenty-seven older drivers participated in the study. A summary of the
demographic characteristics of the participants is given in Table 5.1.
Table 5.1: Characteristics of Participants Characteristics Descriptive statistics (N=27)
Gender 17 (63%) Female
10 (37%) Male
Age Median=74 (range 74-90)
Education 2 (7.4%) Primary school
13 (48.1%) Secondary school
8 (29.6%) Certificate/Diploma
2 (7.4%) Bachelor degree
2 (7.4%) Postgraduate qualification
Type of Residence 18 (66.7%) Private home
9 (33.3%) Retirement home
Living situation 15 (55.6%) Living with spouse or partner
12 (44.4%) Living alone
Employment 18 (66.7%) Unemployed
7 (25.9%) Part-time work
1 (3.7%) Full-time work
Self-rated Health 9 (33.3%) Excellent
15 (55.6%) Very good
3 (11.1%) Fair
Procedure
A semi-structured discussion guide was developed based on current literature
on older drivers and the research questions informed by the PAPM. In particular, it
explored: (1) the importance of driving and the impact of driving cessation, (2)
changes of driving behaviour among older drivers, (3) awareness of changes in
driving abilities; (4) perceived indications of the need to give up driving, (5) their
future plans for stopping driving, and (6) impact of feedback on their planning and
decision making process. A total of five sessions were conducted from February
The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 93
2014 to March 2014. Sessions were held in a private room where the moderator
explained the study goals and obtained signed consent from the participants. The
sessions lasted 60-90 minutes each and the number of participants varied between
two to eight. Sessions were audio-recorded and then transcribed verbatim for
subsequent coding and analysis. Participants completed a background questionnaire
to collect basic demographics and driving status. Each participant received a $40 gift
voucher at the end of the session for their time and travel. The study had full ethics
approval from the Research Ethics Unit at the Queensland University of Technology
(Approval number 1200000501).
5.6 ANALYSIS
Thematic analysis was conducted following the process outlined by Braun and
Clarke (2006) to identify, analyse and report themes within the data. Transcripts
were read through carefully to gain familiarity with the data content and to detect
meaningful topics across the transcripts. Small sections of the transcripts were
initially coded, following which the first author conducted an initial identification of
themes and collation of similar codes within themes (Braun & Clarke, 2006). The
other authors independently conducted analyses of a sample of the transcripts, as a
result of which the themes were refined. This process resulted in the development of
the five themes discussed below.
5.7 RESULTS
The analysis resulted in the development of five main themes. The themes were:
• The meaning of driving
• Changes in driving patterns
• Feedback
• The planning process
• Solutions
Under most of the main themes there were sub-themes. Each of the themes and sub-
themes is elaborated below, and quotes from the transcripts are used to provide
examples of the comments made.

94 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Theme one, the meaning of driving
In order to capture what driving meant to the participants, they were asked
about the negative aspects or issues associated with driving at their age along with
the importance of driving. Participants discussed how driving enabled them to be
functional and independent, and how it provided them with a sense of enjoyment.
Driving was essential to maintain participants’ independence and social
inclusion: “Very important. I work part-time. I also play bowls a lot, and I go to
different clubs and things for that. You can't possibly lead a really independent life
relying on public transport. It's too difficult. It takes a whole day to do one thing, and
I don't have time to do that. It is very important to me, and I think for most older
people, it is part of their independence. Giving up driving is a really hard move, I've
discovered, with other people. They feel as if they've lost their independence. Even if
they're only driving to the local shops and back, they feel as though they've still got
their independence if they can drive. It's very important” (Female, 70)
Driving also enabled participants to stay connected with their family: “But we
have family that live good distance apart. And to get to see them in public transport,
well, there isn’t” (Female, unknown)
For those who lived in communities outside the main urban area, driving was
a necessity as alternative transport options were very limited: “The community that I
live in is very small community ……. if you can drive it’s fine, it’s 20-25 km to the
nearest supermarket shopping complex, the mall and all the rest of it. You need to
have a car to get in and out of the place. The elderly folk who don’t have a car have
to rely on neighbours, a once a week bus, of if they are sick at night they have to call
the ambulance……….. I’ve seen a couple of elderly folk absolutely go to pieces when
they got very sick and couldn’t drive anymore” (Female, 71)
Moreover, driving was something that they enjoyed doing: “I thoroughly
enjoy driving. I think it’s wonderful” (Female, 76)
Interestingly, the negative aspects of driving were mostly related to external
factors other than difficulties they encounter in their own driving. Other drivers’
behaviour and lack of courtesy was a major issue noted by the majority of the
participants: “Other drivers are appalling, especially young males. They tailgate
you, they've got to get past you. Bit of road rage there. There's all those things that

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 95
weren't there in my youth, when I was driving. I have to be aware of all those sorts of
things, as well” (Female, 70)
Safety was another issue mentioned by the participants. They did not view
the roads to be as safe as it used to be when they were younger: “When we learned to
drive, there weren't the drunks and addicts on the road. The roads were a lot safer
than they are now” (Female, 76)
Changes in the road systems and the lack of signage that meets the
participants’ needs was also raised by several participants: “There should be a street
sign on every corner so you know what road you’re on and what road you want to go
to and it would help a lot” (Female, 70)
Another issue was how they have become unfamiliar with the constant
changes in the road rules: “I find one of the negative things amongst our age group is
that a lot of older people aren't cognizant with the road rules that have changed. I've
actually got a copy of the latest road rules and went through it and there are a lot of
things that have changed. And a lot of new rules that I wasn't aware with” (Female,
72).
Theme two, changes in driving patterns
When asked about any changes in their driving behaviours as they aged, the
majority of participants noted that they are generally driving less for various reasons
such as retirement, relocation, changes in their family responsibilities, or a mere
preference, for example:
“I don't have to work anymore. I drove four hours to and from work, which I don't
do now” (Female, 76)
“I would drive a lot less nowadays only because I’m living in the metropolis of
Sippy Downs (a suburb of the Sunshine Coast, Queensland) - before I lived in the
country” (Female, 84)
“I drive a lot less though because all our grandchildren are all grown up, they've all
found their own ways. We don't need to meet them at school or take them to sports
events and things like that” (Male, 90)
“I'd rather stay at home, and play on my computer” (Male, 71)
However, a few female participants noted that they drive more now due to
death of their husbands: “I think I do drive more. My husband’s passed away, he

96 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
used to do the driving. So, you've got to do it yourself” (Female, 74). Others noted
driving more due to lifestyle changes: “I certainly drive more than when I was
working. Because we’ve got all this time on our hands!” (Female, 78)
Participants also noted that they plan their trips quite often now: “I find that I
tend to plan my journeys ahead a little bit more. If I'm going somewhere where I'm
not quite so familiar, I get the map out and I make sure that I've written down what
streets I'm [?], what roads I'm going” (Female, 72). However, they attributed this to
the constant changes in the road system: “I think that's because there's a lot more
roads and different angle, you know, they keep on changing roads and such, so we've
got to be more aware of it, haven't we? That's why we do it more now than we ever
used to, because it was only ever one road to take, wasn't there?” (Female, 70) and
for safety reasons as well: “You were safer to get out of your car and ask directions
as well. Now, I wouldn't dream of going up to somebody's door at night and saying,
I'm lost, can you help me. I would have, when I was young.” (Female, 76)
Night time driving was problematic for some of the participants:
“I find driving at night time. I don't drive at night-time if I can avoid it. If I'm down
to see my family, I always try and get home before dark. I can drive at night time, I
have to wear glasses at night time. I have intraocular lens in my eyes I wear, so I
don't need glasses so much, but at night time I really need them to get the clarity of
the lights” (Female, 75)
“I think I've changed my driving. Since I got these (points to his glasses), I don't drive
anywhere near as much in the night time…. Yeah, where it never used to worry me,
headlights or anything like that. Now, I'd rather not drive in the night time if I can
avoid it… That's right. No problems with the confidence, about handling the vehicle,
or avoiding an accident. It's just the sight” (Male, 84)
Another issue was neck turning and merging:
“The neck's a bit, looking over the shoulder. I use the mirrors an awful lot” (Female,
79)
“I did find even coming on the Sunshine Motorway from where we live, you had to
merge. Okay. I’m used to mirrors, but you still have to turn around and sometimes
there’s a bit of pain there and you can get a – What do they call it...Monocular
vision, that doesn’t give you the depth of perception so that was just one physical
angle that” (Male, 71)

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 97
Some participants find it difficult to read road signs as they drive: “I'm pretty
confident, but it's just if I know where I'm going. If you tell me to go such and such,
that lane, that street, do that, fine. But it's when I've got to read signs…. There
weren’t so many signs when we were younger.” (Female, 78)
Participants also noted that they don’t drive very long distances, they are
slower, and more cautious.
Theme three, feedback
We asked the participants if they have sought information about their driving
ability before. Doctor’s advice, a driving instructor, refresher courses, and the
internet were mentioned in several discussions:
“Oh, he knows (refers to his doctor). I've talked to him. He's just said, “If
that's the way you feel, don't drive. It's up to you.” (Male, 70)
“We did an advanced driving course many years ago, and then down here at
the university before it was at a university …anyway, it was very good, excellent! It
was run by two ex-policemen” (Female, Unknown)
“I went on the Internet about it, and downloaded a lot of information from
overseas. I don't know where they get the results for some of their studies from,
because it doesn't make any sense to me……. Some of the stuff you can download is
really hilarious. A lot of it's pretty right” (Male, 84)
“I felt I was getting a bit dicky driving so I rang the NRMA and asked them,
“Could I do a driving test?” And he said, “Well, we don't really do that.” He said,
“But I’ll get someone to come down and go with you.” So, they sort of came from
“?” and took me around where I usually shop and about two hours later, we got
back and I hadn’t hit anything. So anyway, he said – So I said, “How did I go?” He
said, “Well, only two things,” he said, “I could find.” He said, “You drive too fast
and you drive too close to the vehicle in front.” And do you know what? That has
helped my driving so much, just to be told that. You probably know you’re driving
too fast and you know you’re getting there, but just to be told by someone in
authority, it – And because up here, you get on the highway and it says travel three
chevrons behind, which is a wonderful indication because it hits you in your mind
and you just need a reminder about it” (Female, 71)

98 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
For the majority of participants, feedback about regulating or stopping
driving had to come from someone they trust and respect, and be evidence-based:
“It’s got to be from somebody that you trust and respect” (Male, 76)
“and people pay more attention to professional people rather than...it's tough
for you, you know… It carries more weight. They've got the evidence. They'll say,
well, you tick some of the boxes, but you don't tick some of the others” (Female, 71)
The majority of participants thought that they would listen to their physician:
“At this stage, I'm not going to discuss it with my medical people, but when
the time comes, I would certainly respect a professional giving me clues as which
way to go” (Male, 71)
Some even noted that it is the doctor’s responsibility to raise the issue and
they should be the first source of feedback:
“I think the main thing is you're seeing a doctor, the doctor knows what your
physical capacity is, if you know him well enough. He should be able to say...if
you're suffering from a particular disease or perhaps it is asthma, maybe a heart
attack. That's the time the doctor should at least say you're in an area where you
should not be driving, and should advise that” (Male, 70)
However, there were several grey areas and uncertainties identified about
receiving feedback from a physician, for example the fact that some physicians are
very busy was raised by one participant who had to get her medical certificate from
another doctor: “He's never said anything to me, my doctor. I go to the doctor late in
the afternoon, because I generally have to wait, and he's that busy that he just wants
to get rid of me, if you know what I mean” (Female, 79)
Another issue raised was the reliability of the criteria doctors use to assess
their patients for fitness to drive, especially related cognitive impairments and the
concept of differential ageing, for example:
“It's very hard for a doctor to say if somebody has a heart attack, they
shouldn't drive. There's a lot of people driving around that's got pacemakers, and
they've got no trouble driving, and yet, another person can be driving down the road,
never had a heart attack, never had anything wrong, and suffer a heart attack and
die at the wheel” (Female, 74)

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 99
“I know of several other people, one woman, who at 92 is still driving. She
had the beginnings of dementia. Physically, she was okay, eyesight fine. But she
should not have been driving, and she was. And it very much depends on what they
write on file” (Female, 70)
“It's a difficult thing. This is where it comes back to the medical profession, I
think (refers to another participant), he’s 86, he looks pretty fit for me, being able to
still drive at that age is phenomenal. Here I am, a little younger and I don't feel as
though I should be. It does come back to that, perhaps it's the medical profession
again. Have to say, this man's fit, or he's not.” (Male, 70)
The negative impact on the physician-patient relationship associated with
telling older adults not to drive was also noted by participants for example:
“But, as I say I know two other people whose doctors told them and it did not
happen very nicely. In fact, one gentleman went to another and got a tick on his…
And he continued to drive” (Female, 71)
Also, the fact that some doctors are very familiar with their patient, could
make it harder for them to notify authorities if they are unfit to drive:
“But your doctor signs...it's a certificate. And if you've been in the company
of elderly people like we have, it's only a matter of waltzing up to the doctor and say,
I need a certificate to get my license again, okay thank you very much, no problem at
all” (Male, 71)
“I think there needs to be some kind of interim body to make these sorts of
decisions, because doctors themselves are too familiar with patients. As we said
earlier, you might have been going to see that same doctor for many years. They're
reluctant to make those sorts of decisions” (Female, 70)
Interestingly, participants were not very open to receiving feedback from
their family members:
“I mean, there's been a lot of talk about children trying to persuade parents
that it's time to hang up the car keys, very difficult. I think it's probably the wrong
person telling them, you need one further away, a dispassionate person who's not
actually family to say this” (Female, 71)

100 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
And some noted that their children don’t understand their worries and
concerns:
“I tell my kids that I don't feel comfortable driving. Part of it is my age, and
they say, “Dad, you're mad. You're silly.” They can't see the fact that I feel
uncomfortable. I don't think that they've been in an accident where they've seen the
results of what can happen in a car” (Male, 70)
When asked about other sources of feedback that they think could raise
awareness of the older drivers, participants mentioned several options:
“So, should it be coming from TV announcements in a nice gentle kind of
way, should it be coming in the media, in the newspaper…” (Female, 70)
“The fact that you can get a brochure that says, how old are you? These are
the statistics of vehicle accidents that are occurring in this particular range, or this
medical area. There's a lot more people having heart attacks at the wheel…There’s
that, and I don't know, perhaps they've got to open up courses, so you can come and
say, “Look, how do you think you're driving? Are you one of those good 70-year-old
drivers? Come and we'll tell you why you are not” (Male, 70)
Theme four, the planning process
Majority of the participants did not plan or think about the possibility of
stopping driving in the future. There were five main areas explored under this
theme.
Reactions to giving up driving and expectations
Participants’ reactions to the possibility of giving up driving was very
emotional: “I hope by the time I can't drive, I'll be dead or I'll be making my plan to
go somewhere where I don't have to drive” (Female, 71). Stopping driving is a hard
decision: “It’s a big dilemma, because we're all aware of the fact that the day will
come, of course. But not yet. And you know, we have to drive” (Female, 71) and there
is a lot of uncertainty about what the future holds, not just in regard to their abilities
to drive but in the advances in technology as well: “I can't predict what I'm going to
be doing in 10 years' time, because partly…. the technology will change. Partly, I
don't know how I'm going to feel” (Female, 70)

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 101
Interestingly, some participants were more accepting of the idea and started
thinking about alternative options throughout the discussion: “I’d just go to other
places and I don't mind public transport…..It’s not as – You can’t get anywhere quite
as quick, but you can do it and I reckon if they – I got – Lost my license, I’d get one
of those mobility scooters and get around and use public transport and I don't think
I’d let it stop me getting out and about” (Female, 74)
Some participants drew their expectations from other older drivers’
experiences, which often meant driving less and to their local destinations: “Well, I
think you just be driving less, you know, like people do as they get older, they just
drive to church, to the big shopping centre, you know to the library, they don’t…
Like my daughter… you rely on the family to come and visit you” (Female, 72)
Others indicated that they are not planning to renew their licence in the near
future, which is mainly due to medical conditions or getting older:
“I probably won't renew my license next year…. I tear tendons and
shoulders. My neck is not getting any better. Occasionally, if I get up too quickly, I
get giddy. The doctor says it's up to you, but my recommendation is, when your
license is due next year, forget it. If you last that long” (Male, 84)
“I think in another three years or four I won’t be driving a lot, because I’m
getting too old.” (Male, 86)
Few participants indicated that they have thought about the possibility of
giving up driving one day, even though they are still fairly active and enjoy driving.
They have noted that they made some major changes in their lifestyle that would
facilitate their transition to a non-driving state one day:
“The place that I live in is not that far from where my daughter and her
family live and that was a consideration when I took the unit, and I can walk to the
shops and I can walk to church” (Female, 70)
“I've recently moved into a retirement village, and I've been very careful to
choose one where there's a very good bus service there. I'm quite prepared that when
the time comes where I feel I'm not good enough to drive, I will give it up, but it's
really important to me. It was one of the things that I looked at” (Female, 72)
Indications for giving up driving

102 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Loss of confidence and nervousness was an important reason for giving up
driving as noted by some participants: “I’ll see at the moment, if I start to get nervy,
that, that is a big thing, if you’re getting nervous” (Female, 72)
Changes in their health condition and abilities was also perceived as an
important reason to give up driving: “I think it just depends very much on health”
(Female, 71)
For some, age did not seem to be an important factor per se, partly because
people age differently and start experiencing changes and declines in different way.
But also, because majority of the participants were in their 70s and the fact that
people are driving for longer now, meant that they believed they had 20 years or
more to still be actively driving:
“See, I’ve got friends who are 92 and they still drive. So, I’m thinking, well,
you know, I’ve got a way to go yet but that’s sort of – so it doesn’t sort of bother me”
(Female, 74)
“He’s said that to me a few times. And I say to him, “Why do you feel like
that?” and the only answer I get is “Because I’m, getting old,” but surely, that’s not
the criteria. And that’s why I’ve been trying to question him if he has any other
feelings that might be prompting that thought…. It doesn’t matter. The age doesn’t
come in to it. It’s just your mental attitude” (Female, Unknown)
Being involved in a crash was not considered by the participants as an enough
reason for stopping which could be due to the severity of the crash and the fact that
they did not view themselves to be at fault: “I had my first crash a few years ago, not
my fault, of course. <Laughs> But that’s about all…. And when I had this crash, I
thought that was a thing to say that I better give up driving. I lasted three days. It
was terrible” (Female, 84)
Loss of comfort was also another indication for giving up driving as noted by
one participant who had already reduced the amount of his driving in the past years:
“Perhaps that's one of the...I don't feel comfortable on the road. If someone else
would drive me, I'd do it, but that's why I walk, and that's why I cycle” (Male, 70)

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 103
Household composition was an important factor. Some participants indicated
that they will be relying on their spouses for driving in the near future. On the
contrary, female drivers who lost their husbands were doing more driving now as
opposed to the past:
“If I lose my license, I’ve lost my independence. I’ve got to get on a bus, but
I mean I’ve got (refers to his wife) anyway so she can drive and she’s a good driver”
(Male, 75)
“It’s very important to have a car for myself because I live by myself and
same thing goes” (Female, 76)
“I enjoy driving, I must admit it. I had a very sick husband for the last seven
years of his life so hence I was the designated driver” (Female, 71)
Advice and feedback from others was also seen as a reason for regulating or
giving up driving altogether:
“It wouldn't bother me if the doctor said to me, “Don't drive.” I would take
his advice” (Male, 70)
“We used to drive to Brisbane, but the reason we don't drive to Brisbane is
because we have a family problem there, as far as a family concern about not driving
long distances anymore” (Male, 86)
For others, it was more of a self-monitoring process, where people start to
notice changes in their driving as they age. Drawing from other people’s
experiences, they viewed that people were more accepting of giving up driving when
they made the decision:
“If you are a driver and I'm very grateful that I can and do, I think you
probably would be aware of what could or could not happen and hopefully take
steps” (Female, 71)
“I, I know of one lady who, voluntarily handed in her license said I don’t
think I can drive anymore, and she then accepted that quite well. But, as I say I know
two other people whose doctors told them and it did not happen very nicely. In fact,
one gentleman went to another and got a tick on his… And he continued to drive”
(Female, 71)
Abilities for safe driving and awareness of changes

104 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Participants mentioned numerous sensory, physical and cognitive abilities
that they perceived critical for safe driving:
“Eyesight, for one” (Male, 76)
“And also, now your good physical health” (Female, 71)
“I think that your cognitive ability when your driving is one where also to
be… focused and be concentrating on the task at hand and try to take in as many
things as possible” (Female, 70)
“Be aware of your surroundings, for one thing” (Male, 90)
“Focus on your driving, when you're driving. Don't get distracted by other
things. You've got to concentrate. All these distractions, people don't concentrate
enough, and your reaction time gets longer as you get older.” (Female, 76)
The major changes in their abilities, were slower reaction time, being more
cautious, changes in their eyesight, and being more patient
“Yes. I find that I'm not as quick as I used to be, so in my youth, where I'd be
able to drive, a simple thing like that, look left and right. My mind would say
everything's clear, now I find I've got to look twice. I'm far more careful. I'm slower”
(Male, 70)
“I think one of the other issues could be sort of eyesight as well. I think now
there’s such a plethora of the road signs around that it’s probably quite easy to miss
one particularly because in my situation like a little bit in the distance, where before
you would have seen it but probably now you’re thinking “Is it or isn’t it.” (Male,
71)
However, the majority of participants did not report changes in their abilities
and even noted that their driving ability is much the same: “As far as our own
abilities are concerned, I don't think...there hasn't been a lot of change in the last 20
years, for me” (Female, 70)
One interesting point raised by several participants is that driving is a habitual
process that you should be able to maintain doing over time: “I think because in our
declining years, we're creatures of habit, if they've always been a good driver, why
would it change? Unless there are other forces at work like, you lose your hearing or

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 105
your eyesight isn't so good anymore, or your concentration. But it's difficult to break
the habit of years.” (Female, 71)
Barriers and facilitators for giving up driving
As noted above household composition was an important consideration in the
decision-making process. It appeared that having a spouse or family to rely on could
facilitate the transition to a non-driving state. On the contrary, having family relying
on their driving or living alone could mean that it is essential for older adults to drive
for longer.
Living arrangements and location was another important factor. It appeared
that participants who lived in retirement villages where everything is walking
distance found it easier to give up driving one day. Others who lived in communities
far from urban areas reported that giving up driving could mean isolation for them.
Participants’ opinions regarding the use of in-vehicle technology were highly
variable. Some viewed technology as a wonderful possibility that could help them
overcome some limitations they encounter in their driving, such as reverse parking,
merging, and driving in unfamiliar places:
“Automatic parking will be a dream” (Female, 76)
“I use cruise control a fair bit when I’m out on the highway. But you’ve only got to
touch the brake and then it goes off” (Male, 75)
“I think some of those are wonderful, my daughter’s got one that you know; she can
see what’s be-behind… See on the driveway behind her. Ahh, just wonderful, I
wouldn’t have to worry about my neck, now would I?” (Female, 72)
Others mentioned some issues associated with the use of in-vehicle
technology such as being user-friendly, affordability, and its impact on their
concentration and safety:
“I’m not interested in having them on my car. I can’t even work the microwave so
how am I able to work that?” (Female, 71)
“I’m never gonna be able to afford a car with all those things in it” (Female, 74)
“I wouldn't say the latest technology is a wrong thing, but when they get back to the
concentration of the drivers, concentrating on going wherever, the more modern
technologies now installed, the less the driver is concentrating. And it's
concentration that causes most of the accidents” (Male, 71)

106 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
“GPS. I think they're a menace. Because you've got to look at it or listen to it, and
you're taking your eyes off the road, and it only takes a second and you're at a crash”
(Male, 90)
Alternative transport option is an important factor as well. Issues concerning
availability, accessibility, convenience, and acceptance were raised. The majority of
participants held strong opinions against the public transportation system:
“Because I hate public transportation. Non-existent, at our end of the world”
(Female, 79)
They viewed it as time-consuming: “I find it useful having a car because you
pop into your car, you get A to B without going all around neighbourhoods that day.
That's probably a drive that's going to take you 20 minutes, it takes a bus an hour
and a half” (Female, 74), inconvenient: “If I had to give up driving, I'd be lost. I'd
have to ride on taxis, and I think the bus service is every hour at the least. So, it's
very important for me to keep on driving” (Male, 90), inaccessible: “I can walk
down to a bus stop, but I couldn't possibly walk up the hill climbing with my
shopping” (Female, 72), restricting: “So your evenings, you're confined. It's not so
bad in the day when there is public transport around, but at night, you can't go out
without your car. You can't go out to dinner” (Female, 76), difficult to plan: “I can’t
remember the last time I used public transport so that in itself is a little bit of a nervy
thing about finding out which bus goes where and timetables and everything”
(Female, 78), and unsafe: “and then you’re quite likely to get bashed on the bus.”
(Male, 71)
Other older adults’ experiences about giving up driving seemed to have left an
impact on some participants about how their life would look like without driving.
This may make it difficult for them to come to terms with the decision to give up
driving: “So it is extremely important that you drive, and I’ve seen a couple of
elderly folk absolutely go to pieces when they got very sick and couldn’t drive
anymore……. You have got to hand your license, they just, they just melt…it’s very
scary” (Female, 71)
Theme five, solutions
Participants expressed their opinions about possible sources of feedback
about older adults’ driving abilities.
On-road testing

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 107
Opinions varied regarding the introduction of age-based on-road testing.
Some were very accepting of the idea and saw it as “common sense” (Female, 74).
Others thought it should only be required if a medical condition is present: “It might
be even if you’re on medication or if you had the shakes or something like that, I take
great exception to that at 72” (Female, 72) and that it would need to be gradually
introduced from an early age: “I think it should be spread over all ages. The new
drivers, after they're off their P-plates, the last lot. The year after that, they should go
for another test” (Male, 84)
Medical examination
Overall, participants viewed the medical examination positively. However,
they thought it should incorporate a physical component as well and need to be more
strictly enforced:
“I really do agree with that examination, because I’ve had my eyes fixed
annually, you know, and they noticed any deterioration, and you've got to trust your
doctor” (Male, 76)
“I thought it would be good idea though that you could go and have a
physical test sometime” (Male, 71)
“But then it's a matter of being enforced, isn't it? This chap, it wasn't
obvious. But he was elderly, and the fact that he had a medical condition and was
still driving, it was dangerous” (Male, 70)
Driving courses and driving schools
Participants who attended driving courses viewed them positively and noted
that they helped raise their awareness about limitations in their driving:
“One thing that – We were at a lecture the other day with the national seniors
group and the person was talking physio care for elderly people and one of the
things he did mention was ability to turn your neck around, and he was saying
particularly in the bottom area and I did find even coming on the Sunshine
Motorway from where we live, you had to merge. Okay. I’m used to mirrors, but
you still have to turn around and sometimes there’s a bit of pain there and you can
get a – What do they call it?......Monocular vision, that doesn’t give you the depth of
perception so that was just one physical angle that” (Male, 71)

108 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
“And you could go on a refresher course and improve your...I think that is an
RACQ course for drivers. They pick up your faults and advise you how to adapt your
driving” (Female, 76)
“I think it would be a very good idea, and I'd be quite prepared if someone
came with me for half an hour, or an hour. Whether they be a driving instructor or
somebody else and just pick up any bad habits that I might have, or give me
feedback. I think that would be a great thing to do. My sister has just done it. She
almost had a very bad high speed accident because she misjudged the speed of the
car coming towards her, so she got someone from a driving school to take her for a
lesson and it was quite helpful” (Female, 72)
“That one I had with the NRMA, that only cost me about $75 and they’re
absolutely worth every penny. What he – the information and the feedback he gave
me and the feeling I had when I was doing it” (Female, 71)
5.8 DISCUSSION
This study used the PAPM as a framework for understanding older drivers’
transition from a state of unawareness about declines in their driving abilities to
adopting self-regulatory driving behaviours. Overall, participants were conscious of
the fact that driving abilities change with age, despite not being personally engaged
or aware of the effect ageing might have had on their own abilities. It also seemed
that some older drivers engage in what appears to be self-regulatory driving
behaviour, such as driving less, but for reasons other than compensating for age-
related declines. As suggested by previous studies (Ball et al., 1998; Blanchard &
Myers, 2010) , it appeared that changes in their lifestyle (such as retirement,
household composition, relocation) played a major role in the changes in their
driving patterns. Similar to previous research on older drivers, the most challenging
driving situations identified by the participants were night time driving (Ball et al.,
1998; Charlton, Oxley, Fildes, Oxley, & Newstead, 2003) and neck turning (Staplin,
Gish, Decina, Lococo, & McKnight, 1998a). Building upon previous research and
the findings of the current study, we have developed an initial model of driving self-
regulation among older drivers (Figure 5.2). It can be seen that Stage 1 of the PAPM
(unawareness that driving may change with age) has been omitted and that the
additional construct of insight has been inserted, while actual capacity to drive safely

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 109
(with its cognitive, physical and vision aspects) has been separated from the stages.
It is important to note that this model shares a lot of similarity with Rudman et al.’s
(2006) model of driving comfort. However, our model is consistent with the PAPM
in that it identifies awareness and insight into declining ability as the first step
towards self-monitoring and self-regulatory driving behaviours. Rudman et al.’s
model suggests that driving comfort influenced by a number of interpersonal,
intrapersonal, and environmental factors acts as a key determinant of self-regulation
(Rudman, Friedland, Chipman, & Sciortino, 2006). If older drivers avoid certain
driving situations because they feel uncomfortable and without being aware of
possible declines in their abilities, then their self-regulatory behaviour could be seen
as an automatic process to minimise the mental load associated with the functional
declines brought by ageing rather than enhance their safety (De Raedt & Ponjaert-
Kristoffersen, 2000b). Their self-regulation of driving may be a response to the
discomfort they experience in challenging driving conditions rather than intentional
monitoring of their driving ability (Meng & Siren, 2012). It is interesting that even
though some participants in our study noted that they encountered certain difficulties
and felt discomfort in some driving situations (such as night time driving or driving
in unfamiliar places) they attributed this discomfort to external reasons (i.e. glare
from other cars’ headlights on their glasses, changes in the road systems) and did not
increase their awareness about possible declines in their driving abilities. If
participants’ discomfort was indeed caused by factors unrelated to declines in their
driving ability, it may have led to unnecessary driving restrictions (Meng & Siren,
2012). To be effective, self-regulation should result in decreased exposure to
challenging situations and conditions. Therefore, drivers need to be conscious and
aware of deficits in their driving abilities and how they can compromise their safety.
Furthermore, self-imposed restrictions on driving due to lack of confidence can be
worrying (Moták et al., 2014) as highlighted by a recent study which found that
drivers who are not confident or moderately confident of being a safe driver are up to
1.94 times more likely to be involved in a crash than drivers who are very confident
of being safe drivers (Oxley et al., 2010).

110 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Figure 5.2: Proposed theoretical model of stage-based driving change involving feedback and self-
regulation
For people to move from stage 2 to stage 3, they need to perceive the hazard
or precaution to be of personal relevance to them which requires people to have
insight into the impact of age-related declines on their driving ability. As suggested
by (Weinstein et al., 2008) persuading people to think about an issue can be
accomplished by personally experiencing the hazard (i.e. being involved in a crash)
and/or communications from significant others (i.e. feedback from family, friends, or
health professionals). Previous research has shown that an individual’s perceived
susceptibility of being involved in a crash can be an important factor in stopping
driving (Lafont, Laumon, Helmer, Dartigues, & Fabrigoule, 2008). However, some
studies have indicated that history of crashes was not a major influence in the older
adult’s decision to stop driving (Dellinger et al., 2001; Persson, 1993) which is
consistent with our findings. Still, further research is needed to determine whether
the severity of the crash, the recency of the crash, and the perception of being at fault
might have an impact on the individual decision to modify or stop driving. Providing
feedback regarding age-related declines and their impact on older adults’ driving
performance can lead to appropriate adjustments in their driving behaviours
(Ackerman et al., 2011). In a study conducted by Holland and Rabbitt (1992), two
thirds of participants reported making compensatory changes in their driving

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 111
behaviours in response to feedback about their sensory abilities. Eby et al. (2003)
reported that 14% of older adults, who completed a workbook which raised issues
regarding health, cognition, vision, and driving behaviour, discovered overlooked
changes in their abilities, with 25% reporting their intention to adjust their driving
behaviour accordingly. Older drivers can receive feedback from various sources.
The content, timing, and effectiveness of such feedback, however, may vary. It
appeared that participants are open to receiving feedback from their doctor which is
consistent with previous studies (Coughlin et al., 2004). However, physicians have
reported that there are barriers toward discussing the issue of driving cessation with
their patients such as unawareness about reporting requirements, negative reactions
from their patients (Betz et al., 2013), and lack of confidence and skill (Marshall,
Demmings, Woolnough, Salim, & Man-Son-Hing, 2012).
Furthermore, health literacy related to driving safety can increase older
adult’s awareness of the effects of age-related declines on their driving ability ( Eby
et al., 2003; Owsley et al., 2003) and might have an influence on the self-regulation
of driving behaviours in older adults (Sargent-Cox et al., 2011).
There are number of factors identified by Weinstein et al. (2008) that can
determine people’s transition from stage 3 to stage 5 which we have included in our
model. While we have not explored all of these factors in our study, we explored
participants’ beliefs and expectations of their driving future. It appeared that some
participants drew their expectations from other older people’s experiences which for
them meant driving less and in local areas. In addition, participants were aware of the
importance of driving in maintaining their independence and quality of life as they
have seen with other older people who stopped driving. It seemed that participants
were looking forward to continue driving for longer as more and more people are
driving in their 90s now. We also explored the pros and cons of driving among
participants. The results also suggest that driving is vital to participants’ identity and
well-being and not just a mean of getting around. Consistent with previous studies,
participants viewed driving to be the key to their independence and the principal
form of their transportation (Rakotonirainy & Steinhardt, 2009). It enabled them to
stay connected in their community (Eisenhandler, 1990) and provided them with
feelings of enjoyment (Coughlin, 2001). There were few negative aspects associated
with driving among participants which were mainly related to external factors such

112 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
as other drivers’ behaviours and constant changes in road systems. Interestingly, it
appeared that loss of confidence or comfort is an important determinant in the
decision-making process among some participants. Decreased confidence among
older adults has been identified as an important factor to giving up driving
(Ackerman et al., 2011; Meng & Siren, 2012; Ross, Dodson, Edwards, Ackerman, &
Ball, 2012). Two studies that asked older adults to rate their confidence level in
several driving conditions found that confidence was significantly related to self-
reported avoidance of difficult driving situations (Baldock et al., 2006a; Marottoli &
Richardson, 1998). Parker et al. (2001) also found that drivers with higher ratings of
nervousness reported more driving problems, lower mileage and less frequent driving
(Parker, MacDonald, Sutcliffe, & Rabbitt, 2001)
Having decided to modify or stop their driving, older adults need to start
dealing with barriers associated with giving up their driving. In our study, we have
identified some barriers and facilitators that can impact older adults’ decision to
modify or stop driving. The issues and problems with alternative transport raised in
this study were consistent with previous literature. The availability of other transport
options (Coughlin, 2001) and the cost of public transport (Corpuz, 2007) have been
identified as an important factor in the decision to give up driving among older
adults. Older drivers often view public transportation to be inaccessible, expensive,
inconvenient, unsafe, and unreliable which may affect their decisions regarding their
driving behaviours (Allan & McGee, 2003; Gardezi et al., 2006). Older adults often
view taxis as an expensive form of transportation and report concern over their
personal safety (Oxley et al., 2003). On the other hand, buses and trains are viewed
to be inconvenient and inaccessible due to a number of factors such as difficulty
getting on and out of the bus, having to walk to and from stops, and lack of
experience with public transport options (Oxley et al., 2003). An interesting solution
provided by Musselwhite & Shergold (2013) emphasizes the need to promote the use
of alternative modes of transport throughout life or at least from a much younger age.
This gradual introduction of alternative transport options might help eliminate the
psychological barriers associated with their use (Musselwhite & Shergold, 2013). It
appeared also that household composition is an important factor in the decision-
making process. Having family relying on their driving or living alone, could make
it difficult for some older adults to give up driving. There are inconsistent findings

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 113
among the literature in regards to living arrangements and self-regulation. While
some studies have reported that those who were not the principal driver of the
household were more likely to adopt self-regulation (Charlton et al., 2006; Donorfio,
D'Ambrosio, Coughlin, & Mohyde, 2009) other studies have reported that living
conditions have no impact on adoption of self-regulation (Ragland, Satariano, &
MacLeod, 2004) and those who are living alone are more likely to self-regulate than
those who are living with a spouse (Braitman & McCartt, 2008). The finding also
indicates that technology could play an important in prolonging older drivers’ safe
mobility by compensating for limitations in their driving ability. For example, a
blind spot detection and a lane change assist system can compensate for existing
motor and visual limitations (difficulty in turning head and reduced peripheral
vision) and assist them in merging and lane changes. While most participants
viewed such in-vehicle systems positively, there were number of barriers identified
in this study to the adoption of technology among older drivers (e.g. complexity,
safety and reliance issues, and affordability). Emerging studies suggest that in-
vehicle technology can assist older drivers by augmenting their driving ability
(Coughlin, 2005; Guo, Brennan, Edwards, & Blythe, 2012). It thus carries the
promise of allowing older adults to drive for longer without compromising their
safety (Rakotonirainy & Steinhardt, 2009). However, these technologies should be
centred around older adults’ needs and opinions (Musselwhite & Haddad, 2008).
Another important issue raised in this study is the way older adults cope with
driving cessation. Some older adults are able to cope well with the challenges of
later life than others (Hamarat, Thompson, Steele, Matheny, & Simons, 2002), an
aspect essential to successful ageing (Fiksenbaum, Greenglass, & Eaton, 2006).
Planning to stop driving could be difficult, partly because of what driving means to a
person’s identity and well-being, but also because of the uncertainty surrounding the
issue in terms of when, why, and how one would or should give up driving. Planning
can make it easier for people to come to terms with giving up driving as it gives them
a sense of control over the decision making process (Musselwhite & Shergold,
2013). Coping with driving cessation has mainly been viewed as reactive though it
can also involve a proactive approach. The available interventions mainly assist
older adults in reacting effectively to cessation of driving. However, it may be
equally important to assist older adults in coping proactively with giving up driving.

114 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
A recent study conducted by Musselwhite & Shergold (2013) which followed 21
individuals over a period of 10 months through the process of driving cessation
revealed that people who plan their driving cessation ahead are more likely to have a
better quality of life after stopping driving. Further research is needed to explore the
possibility of designing an intervention that can help older adults take steps toward
this planning process, similar to those programs that assist with major life transitions
(e.g. retirement). Furthermore, we need to raise people’s awareness that self-
regulatory behaviours are not solely linked to health deterioration. Older people can
suffer from subtle and deceptive changes in their abilities (decreased reaction time,
joint stiffness) that can affect their driving behaviour.
5.9 LIMITATIONS
The study participants were volunteers, of good health, and leading an active
lifestyle. The findings may have differed for participants with poorer health and a
less active lifestyle. Furthermore, the majority of participants resided in the
Sunshine Coast area which is different from urban locations such as Brisbane
particularly in terms of a relative lack of public transportation options and a high
proportion of retirees in the population. The qualitative nature of the study meant
that participants’ responses could be subject to social desirability, although as the
quotes demonstrate the comments were wide-ranging and participants reported
behaviours that were not necessarily desirable. In addition, due to the nature of the
study, the results are not generalizable to all older drivers and do not permit
statistical inference. Our aim was to gain in-depth data about older drivers’
perceptions and opinions about the changes in their driving behaviours over time and
it was not the aim of this study to collect data that are generalizable. Nevertheless,
the exploratory nature of this study allowed us to gain significant insight into the
issue being studied and can therefore help define specific research questions that
should be tested with quantitative data from questionnaire surveys.
5.10 CONCLUSION
This study explored the process of self-regulation and driving cessation
among older drivers using the PAPM as a framework. It also investigated older
adults’ perceptions and opinions about receiving feedback in regards to their driving
abilities. The findings from this study suggest that further elaboration of the PAPM

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 115
is needed to take into account the role of insight and feedback on the process of self-
regulation among older drivers. Since the driving cessation process occurs over
time, it would be beneficial to conduct a study that follows a larger sample through
the decision-making process.
Acknowledgment
The Australian Postgraduate Award Scheme provided funds for the PhD
research program of the first author. We also gratefully thank Amy Williamson from
the Centre for Accident Research and Road Safety-Queensland for assisting in
conducting the focus group sessions.

116 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Chapter 6: Examination of the Precaution Adoption Process Model in understanding older drivers’ behaviour: an explanatory study (Study 2, Phase 1)
6.1 PUBLICATION STATUS
This chapter comprises Paper 2 as taken from:
Hassan, H., King, M., & Watt, K. (2017). Examination of the Precaution Adoption
Process Model in understanding older drivers’ behaviour: an explanatory study.
Transportation Research Part F, 46(A):111-123.
6.2 STATEMENT OF CONTRIBUTION
The candidate, as first author, accepts the overall responsibility for this
publication. The candidate was responsible for all aspects of the manuscript
preparation, including reviewing the literature, formulating the research question,
conducting and supervising data collection, analysing and interpreting the results and
writing and submitting the final manuscript. All co-authors meet the criteria for
authorship and take responsibility for their role in delivering the publication. All of
the co-authors of this paper are members of the candidate’s supervisory team and
their contribution to this paper was supervisory in nature. Written permission was
provided from each to include the publication as part of this thesis and its publication
on the QUT ePrints database.
The authors listed below have certified that:
1. they meet the criteria for authorship in that they have participated in the
conception, execution, or interpretation, of at least that part of the publication in their
field of expertise;
2. they take public responsibility for their part of the publication, except for the
responsible author who accepts overall responsibility of the publication;
3. there are no other authors of the publication according to these criteria;

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 117
4. potential conflicts of interest have been disclosed to granting bodies, the
editor or publisher of journals or other publications, and the head of the responsible
academic unit, and
5. they agree to the use of the publication in the student’s thesis and its
publication on the QUT’s ePrint site consistent with any limitations set by publisher
requirements.
Principal Supervisor Confirmation
I have sighted email or other correspondence from all Co-authors verifying their
authorship
Dr Mark King QUT Verified Signature 30 Aug 2017
------------------------- ----------------------------------- ------------
Name Signature Date
Examination of the Precaution Adoption Process Model in understanding older
drivers’ behaviour: an explanatory study

118 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Heidy Hassan a, Mark King b, Kerrianne Watt c
a The Centre for Accident Research and Road Safety – Queensland (CARRS-Q), GPO Box 2434, Brisbane, Queensland, Australia. Corresponding author. Tel: +61731387727. Email: [email protected] b The Centre for Accident Research and Road Safety – Queensland (CARRS-Q), GPO Box 2434, Brisbane, Queensland, Australia c School of Public Health, Tropical Medicine and Rehabilitation Sciences- James Cook University, Townsville, Queensland, Australia
6.3 ABSTRACT
Self-regulation of driving has been proposed as an effective strategy to keep
older adults driving safely for longer. Little is known of what influence older adults’
decision to adopt self-regulatory driving behaviours. Hassan and colleagues (2015)
developed an initial model of self-regulation using the Precaution Adoption Process
Model (PAPM) as a theoretical framework. The present study aims to build on the
previous research by investigating whether a sample of older drivers can accurately
be assigned to the PAPM stages of change. Further, the study aims to identify the
psychosocial and environmental factors associated with different stages of the PAPM
and those that predict the decision to adopt self-regulatory behaviour. Logistic
regression analysis indicated that self-rated driving confidence, family feedback,
self-rated quality of driving and driving relinquishment expectation were significant
predictors of PAPM stages. Findings from this research have practical and theoretical
applications for improving our understanding of the self-regulatory behaviours of
older drivers.
Keywords
Awareness; Behaviour; Older drivers; Perception; PAPM; Self-regulation

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 119
6.4 INTRODUCTION
There has been a growing interest in understanding the risk factors for motor
vehicle crashes among older adults, given the ageing population and the predicted
increase in the number of older drivers (King, Soole, Watson, & Schramm, 2011).
Driving provides people with a sense of independence and freedom which improves
their quality of life (Liddle et al., 2014). Stopping driving has been associated with a
large number of negative outcomes such as decreased out-of-home activities,
increased dependency, and increased depression (Fonda et al., 2001; Marottoli et al.,
2000).
However, ageing is often accompanied by declines in the sensory, cognitive
and motor abilities considered necessary for safe driving (Anstey et al., 2005). If
unable to compensate for these changes, older drivers may put themselves and others
at risk (Freund et al., 2005; Marottoli & Richardson, 1998). In addition, due to their
increased fragility, older drivers are overrepresented in serious and fatal crashes (Li
et al., 2003).
Previous studies have shown that some older adults modify their driving (e.g.
driving reduction and/or driving restriction) in response to declines in their abilities,
a process known as self-regulation (Hassan, King, & Watt, 2015). While often
viewed as an effective strategy to maintain older adults’ safe mobility, the process of
self-regulation is still not completely understood, particularly in terms of the factors
that influence older drivers’ decision to restrict and/or reduce their driving. The
majority of previous research has focused on examining the association between self-
regulation and specific impairments and medical conditions among older adults
(Rudman et al., 2006). However, recent findings that younger drivers also avoid
some driving situations (Naumann et al., 2011) suggest that driving avoidance can be
the result of factors other than declining abilities. In fact, up until now, it is still
unclear whether older drivers adopt self-regulatory behaviour to compensate for their
age-related declines or whether it is simply a lifestyle choice (Siren & Kjær, 2011).
In addition, the success of self-regulation in terms of maintaining older drivers’ safe
mobility depends largely on their awareness of limitations in their driving abilities,
rather than their actual abilities (Anstey et al., 2005). Therefore, a strong emphasis
has been placed on identifying the impact of self-awareness on self-regulation among
older drivers, and recently growing attention has been directed towards

120 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
understanding the psychosocial factors that affect the self-regulatory driving
behaviours. However, the inconsistencies in the way drivers’ perceptions are
measured and defined, make it difficult to compare the findings (Blanchard & Myers,
2010).
Given the large number of factors influencing older drivers’ behaviour, it is
essential that research in this area is well grounded, both theoretically and
practically. Theories and models of driver behaviour can help us describe, explain,
predict and change behaviours through the development of appropriate intervention
programs (Crosby & Noar, 2011). The driving cessation process can be
conceptualised as occurring in stages (Kostyniuk et al., 1998). Interventions for
older drivers should therefore be customised, based on the individual (the baseline
stage and the personal, social, and environmental circumstances) and the anticipated
outcome (increased awareness, enhanced self-monitoring, adoption of self-
regulation, or planning cessation), and be sufficiently flexible to move individuals
through the stages of change towards adoption of safe driving behaviour (Tuokko,
Jouk, et al., 2014). However, there has been little development of stage-based
theories applied to driving self-regulation, and hence a lack of research on
theoretically-informed interventions that facilitate older drivers’ planning for future
self-regulation and even driving (Hassan et al., 2015).
Hassan et al. (2015) examined the applicability of the stage-based Precaution
Adoption Process Model (PAPM) in understanding older adults’ self-regulatory
driving behaviour. Building upon the relevant literature and on findings from a
series of qualitative focus groups among 27 Australian older drivers, the authors
developed a preliminary model of driving self-regulation among older drivers
(Figure 6.1). It can be seen that Stage 1 of the PAPM (unaware about the issue) has
been omitted as previous studies clearly demonstrate that older drivers are generally
aware about the impact of medical or functional impairments on driving abilities
(Sargent-Cox et al., 2011), however, they sometimes lack insight into their own
driving ability and are therefore not receptive towards adoption of self-regulation.
The model identifies self-awareness and insight into declining ability as the
first step towards self-monitoring and self-regulatory driving behaviours. It
incorporates both personal and environmental factors that have been found to impact

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 121
older adults’ driving behaviours and delineates suggested strategies to help people
move through stages.
Figure 6.1: Preliminary theoretical model of stage-based driving change involving feedback and self-regulation (Hassan et al., 2015)
The present study aims to build on the previous research by investigating
whether a sample of older drivers can accurately be assigned to the stages of the
PAPM. Further, the study aims to identify the psychosocial and environmental
factors associated with different stages of the PAPM and those that predict the
decision to adopt self-regulatory behaviour which may be worthy for further
investigation. However, predictors of stage transitions can only be identified through
prospective longitudinal research (Weinstein & Sandmand, 2002).
Specifically, this study will answer the following questions:

122 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
1. To what extent are the PAPM stages observed in our study
population?
2. What are the psychosocial and environmental factors
associated with stages of the PAPM?
3. What are the differences between those who have adopted
self-regulatory driving behaviours and those who did not think about
regulating their driving or resisted changing?
6.5 METHODS
Participants and recruitment
A total of 247 Australian drivers took part in this cross-sectional study. This
study took place in the Brisbane and Sunshine Coast areas of the state of Queensland,
Australia. In 2015, the estimated resident population of Queensland was 4.8 million
and the proportion of those aged 65 years and over in Queensland has increased by
4% from June 2014 to June 2015 (ABS, 2015). In 2011, females outnumbered males
in the 75 years and above age groups (ABS, 2011) with around 33.8% of women
aged 65 years and over living alone compared to 18.4% of older men (Australian
Bureau of Statistics, 2011). The licensing authority is Queensland Transport and
Main Roads and drivers aged 75 years and over are required to carry a valid medical
certificate obtained from their doctor. Participants were recruited through various
recruitment strategies to ensure sample variability such as flyers posted and
distributed in seniors’ clubs, geriatric clinics, and local shopping centres,
advertisements in local newspapers and through social media. A web-based version
of the questionnaire was also developed to gain access to a wider range of older
drivers. Eligible participants were current drivers aged 70 years and older. The
study was conducted between May 2014 and October 2014. Participants completed
the questionnaire online or in a paper-based form with a paid return envelope to the
principal researcher. Both questionnaires included an information sheet describing
the nature of the study and completing the questionnaire was considered evidence of
consent to participate. All participants received the chance to enter a draw to win
one of ten $50 shopping vouchers. All procedures were approved by the Human
Research Ethics Committee of Queensland University of Technology.

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 123
Materials
A questionnaire was designed to collect information on the socio-
demographics (age, gender, education, employment, etc.), self-rated health, crash
history, driving experience, current driving patterns, driving perceptions, feedback
about driving and transport options of older drivers. In addition, participants’ driving
reduction was measured by asking participants to rate the overall amount of their
driving compared to ten years ago, on a 4-point scale from “much less” to “more”.
Participants’ self-restriction and avoidance behaviour was measured by asking
participants to rate the extent to which they would avoid driving under 18 various
challenging driving conditions (e.g. driving at night-time, driving alone, driving on
high traffic roads, etc.) on a five point Likert type scale from “not at all” (0) to
“avoid completely” (4). These situations have been reported consistently in previous
studies (Sullivan, Smith, Horswill, & Lurie-Beck, 2011) and were considered to be
relevant to our study population (i.e. we did not include driving in snow even though
it has been reported before because there is no snow in Queensland). A driving
restriction score was calculated based on the average score of responses to the 18
items with higher scores indicating increased avoidance.
Outcome variable
Participants were classified into stages of the PAPM based on their responses
using an algorithm that was developed along similar lines to the one used by
Weinstein and Sandman (2002). We omitted stage 1 (general unawareness that
driving may change with age) because people are generally aware of the problems
associated with ageing and driving through the media. We also omitted stage 7
(maintenance) as we interpreted it as driving cessation and we did not include former
drivers in our sample. We asked participants to indicate which of the statements
presented in Table 6.1 better describe them. Based on their answers, participants
could then be categorised into stages of the PAPM (stage 2 to stage 6).
Table 6.1: Precaution Adoption Process Model: Stage Classification Algorithm as
applied to self-regulatory driving behaviours among older adults (Adapted from
Weinstein & Sandmand, 2002) PAPM stage Algorithm
Stage 2
Unengaged
Some other older drivers need to change their driving, but I believe that I
am a safe driver and have never thought about the need to change my

124 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
driving
Stage 3
Undecided
I am at the point where I am not sure if I should start thinking about ways
to avoid certain driving situation or reduce my driving
Stage 4
Resisting action Avoiding certain driving situations would be pointless to me
Stage 5
Planning to act I am planning to avoid certain driving situations and reducing my driving
Stage 6
Self-regulating
I have just recently started to avoid challenging driving situations or drive
less
Independent variables
Socio-demographics, self-rated health and driving experience
The questionnaire collected data about participants’ demographics.
Participants’ self-rated health was assessed by a single question asking respondents
to rate their health as “very poor”, “poor”, “fair”, “very good”, and “excellent”.
Driving experience was measured using two questions, the length of possession of an
open driving license and annual kilometres driven.
Feedback
Participants were also asked whether they received feedback about their
driving from their doctor, family, or friends.
Alternative transport, living conditions and life-goal changes
Data about participants’ use of alternative transport options and barriers
towards use were measured. Participants’ life goal decisions (e.g. moving to a senior
home, moving closer to public transport, or moving closer to common destinations),
in-vehicle technology use, living conditions and whether they were the principal
driver were also assessed.
Psychosocial variables
Participants’ driving confidence was measured by a single question
“compared to ten years ago, do you still feel confident that you can safely drive to
places you need to go” with answers ranging from “much less”, “a little less”, “the
same”, and “more”. For the purpose of analysis, participants were grouped into two
categories, reduced confidence (much less, a little less), or not reduced (the same,
more).

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 125
Participants’ overall self-rated quality of driving was measured by a single
question “How would you rate the quality of your driving” with answers ranging
from “excellent”, “good”, “average”, “fair”, and “poor”.
Perception of crash risk was measured using three different questions: “how
likely is it for you to have a car crash compared to other people your age”, “how
likely is it for you to have a car crash compared to yourself ten years ago”, and “how
likely is it for you to be injured if you are involved in a car crash” with answers
ranging from “extremely likely”, “somewhat likely”, and “not at all likely”.
Regulatory self-efficacy was measured by asking participants to rate how
easy it would be for them to avoid driving in the 18 challenging driving situations,
similar to the items used for assessing self-regulation of driving by avoidance, on a
three-point scale ranging from very hard (0) to not hard at all (2). An index was
calculated based on the average score of the responses to the 18 items.
The perceived driving ability scale (PDA) is a previously validated 15-item
scale (MacDonald, Myers, & Blanchard, 2008) used to measure participants’ current
perceived driving abilities (e.g., to see road signs at a distance, to see vehicles
coming up alongside, to make an over the shoulder check) along a 4-point scale
(‘‘poor’’, ‘‘fair’’, ‘‘good’’, ‘‘very good”). A mean scale score was computed with
higher scores indicating more positive perceptions.
A driving stress scale similar to the one used by Hakamies-Blomqvist
(1994a), was used to measure participants’ experienced stress in a number of driving
situations on a 4 point scale ranging from 0 (heavy stress) to 3 (no stress) and a total
“Driving Stress” score was calculated (Hakamies-Blomqvist, 1994a)
A driving relinquishment scale was developed to assess participants’ views
about the importance of driving and barriers toward giving up driving and was
measured by asking participants to indicate their agreement with eight statements
about the importance of driving and barriers to giving up driving (e.g. giving up
driving will simplify my life, giving up driving is not possible because of my
lifestyle). A mean scale score was computed with higher scores indicating a more
positive attitude towards giving up driving.

126 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
6.6 ANALYSIS
Before conducting the analysis, data screening was performed to check for
missing data. Six cases were missing responses on the dependent variable and
therefore were excluded from the analysis. One case was missing responses on the
dependent variable and therefore was excluded from the analysis. One case was
missing a response on gender and was excluded. Another 16 cases were missing
responses on important psychosocial predictors and were excluded. A total of 222
cases were included in the final analyses. Missing values on psychosocial scales
were replaced with the series mean to compute the average score. Several variables
were collapsed into two or three alternatives in order to obtain meaningful categories
with respect to the purposes of the study. Descriptive statistics and bivariate analysis
were conducted for all five PAPM stages. However, for the purpose of the binomial
regression analysis and due to the small number of participants in some of the PAPM
stages, we decided to combine participants into two stages. The Pre-decision stage
(stage 2 and stage 3) includes participants who are still actively driving without any
changes to their driving. Participants in this stage may have never thought about the
need to change their driving (stage 2) or may start to wonder about the need to
modify their driving but have not made a decision yet (stage 3). The Decision stage
(stage 5 and stage 6) includes participants who are planning to or have started to
reduce and/or restrict their driving. Participants in stage 4 (resisting action) are
omitted from the regression analysis as they may be over-confident and resistant to
conventional interventions. Data were analysed in SPSS version 20.0 (IBM
Corporation, Armonk, NY).
6.7 RESULTS
Table 6.2: Sample characteristics (n=222) Mean age in years (SD) 75.5 (5.1) Gender Male Female
135 (60.8%) 87 (39.2%)
Principal driver Yes No
154 (69.4%) 68 (30.6%)
Education Primary school Secondary school Certificate Bachelor degree Postgraduate degree
13 (5.9%) 90 (40.5%) 55 (24.8%) 39 (17.6%) 25 (11.3%)
Dwelling A private home A retirement home or seniors’ complex
172 (77.5%) 50 (22.5%)
Living condition

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 127
Alone With spouse or partner Other
74 (33.3%) 136 (61.3%) 12 (5.4%)
Employment Yes No
66 (29.7%) 156 (70.3%)
Driving environment City Suburb Rural
28 (12.6%) 160 (72.1%) 15 (6.8%)
Trip length Less than 15 minutes 15-30 minutes More than 30 minutes
22 (9.9%) 125 (56.3%) 75 (33.8%)
Driving experience, years open driving license (mean and standard deviation) 55.4 (6.3%) Annual km driven Less than 5,000 km/year 5,000-10,000 km/year More than 10,000 km/year
52 (23.4%) 89 (40.1%) 81 (36.5%)
Driving reduction Much less A little less The same More
88 (39.6%) 70 (31.5%) 52 (23.4%) 12 (5.4%)
Self-rated health Excellent Very good Fair Poor
39 (17.6%) 132 (59.5%) 48 (21.6%) 3 (1.4%)
Self-rated quality of driving Excellent Good Average
53 (23.9%) 136 (61.3%) 33 (14.9%)
Perception of crash compared to ten years ago Somewhat likely Not likely
52 (23.4%) 170 (76.6%)
Perception of crash risk compared to others same age Extremely likely Somewhat likely Not likely
2 (0.9%) 37 (16.7%) 183 (82.4%)
Perception of risk of injury if involved in a crash Extremely likely Somewhat likely Not likely
12 (5.4%) 141 (63.5%) 69 (31.1%)
Driving confidence Much less A little less The same More
1 (0.5%) 51 (23%) 167 (75.2%) 3 (1.4%)
Sample characteristics
The sample ranged in age from 70 to 94 years (M= 75.5, SD ± 5.1), and
included 87 females (39.2 %) and 135 males (60.8%) (Table 6.2). By comparison,
official data shows that 46% of drivers aged 70 and above are female (Department of
Transport and Main Roads, 2015), which indicates that this sample has a lower
proportion of females. As noted in the Results section, gender was not a significant
factor in the regression analyses. Around 23% of participants rated their health to be
fair, 59.5% to be very good, and 17.6% to be excellent. The majority of participants
(71%) indicated that they have reduced their overall driving compared to ten years
ago. Responses to the questions on the most frequently avoided driving situations

128 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
are presented in Table 6.3. Driving at night in the rain was the most commonly
avoided situation (41%) followed by peak hour driving (35.6%), driving at night
(31.1%), and long distance driving (29.7%). The most stressful situation was
fatigued driving (65.8%) followed by driving on slippery roads (58.1%), driving in
unfamiliar areas (46.4%), and night-time driving (44.6%).
Table 6.3: Most avoided driving situations and reasons for avoidance Driving situation Avoidance (n, %) Reasons for avoidance
At night in the rain 91 (41%)
No need (n=31) Not comfortable (n=26)
Not confident (n=19) Other (n=5)
Peak hour
79 (35.6%)
No need (n=24) Not comfortable (n=29)
Not confident (n=7) Other (n=4)
At night
69 (31.1%)
No need (n=15) Not comfortable (n=27)
Not confident (n=14)Long distance driving
66 (29.7%)
No need (n=30)
Not comfortable (n=12) Not confident (n=6)
Other (n=3)Glare
49 (22.1%)
No need (n=11)
Not comfortable (n=16) Not confident (n=5)
Other (n=4)
Feedback
Participants preferred to receive feedback about their driving from their
doctor (30.6%), their partner (30.2%), their family members (14%), or from a person
of authority (12.2%). Around 82% of the participants indicated that a medical or a
vision problem could be a reason to stop or modify their driving with 75.5% of
participants indicating that they would stop driving if advised by their doctor. Only
five (2.3%) participants indicated that they had been involved in a crash in the past
year and only four (1.8%) had received suggestions to stop or modify their driving.
Around 44.6% of participants reported being involved in a conversation about their
driving with their doctor recently, followed by 43.2% with their family members, and
21.2% with a friend.
Alternative transport, living conditions and life-goal changes
Around 64% of participants in our study indicated that they rarely or never
use public transport. Most of these participants reported that they did not use public
transport because they did not need to (73.4%), while specific barriers were

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 129
inconvenience (40.6%), and having the nearest bus stop located too far from home
(25.9%). Around 92% of participants indicated that they rarely or never use taxis.
Again, most reported that this was because they did not need to (80.4%), while cost
was also identified as a specific barrier (43.6%). Finally, 50% of participants
indicated that they rarely or never rely on their family for transport. Around 25.2%
of participants have moved to a new place closer to their common destinations,
22.1% of participants have moved to a place with better transportation options, and
14.9% of participants have moved to a seniors’ home. Around 61.3% of participants
were living with a spouse/partner and 69.4% were the principal drivers in their
households.
Psychosocial variables
Psychometric properties of all scales used in this study are shown in Table
6.4, together with means and standard deviations.
Table 6.4: Descriptions of the psychometric properties of scales
Scale Number of
items Mean SD Scale actual range
Scale sample range
Cronbach’s alpha
Driving avoidance scale 18 0.7 0.6 0-4 (4 greatest avoidance) 0-2.8 0.91Self-regulatory scale 18 1.5 0.6 0-2 (2 higher self-efficacy) 0-2 0.96
PDA scale 15 2.3 0.5 0-3 (3 higher ratings) 0-3 0.93Driving stress scale 16 1.96 0.6 0-3 (3 less stress) 0-3 0.94
Driving relinquishment scale 8 1.3 0.5 0-3 (3 indicates more positive attitude) 0-2.6 0.8
PAPM stages
Participants’ PAPM stages for regulating driving are presented in Table 6.5.
Almost half of participants (46.8%) belonged to stage 2, 10.8% were categorised into
stage 3, 10.4% were in stage 4, 9.9% were in stage 5, and 22.1% of participants were
in stage 6.
Table 6.5: PAPM stages PAPM stage N (%)
Stage 2 (Unengaged) Stage 3 (Undecided)
Stage 4 (Resisting action) Stage 5 (Planning to act) Stage 6 (Self-regulating)
104 (46.8%) 24 (10.8%) 23 (10.4%) 22 (9.9%)
49 (22.1%)

130 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Characteristics associated with PAPM stages
Several characteristics varied as a function of PAPM stages (Table 6.6;
associations which were not significant are not shown).
Table 6.6. Characteristics significantly associated with PAPM stage Variable Stage 2 Stage 3 Stage 4 Stage 5 Stage 6Annual km driven Less than 5,000 km/year 5,000-10,000 km/year More than 10,000 km/year
20 (19.2%) 46 (44.2%) 38 (36.5%)
6 (25%) 6 (25%)
12 (50%)
1 (4.3%) 9 (39.1%) 13 (56.5%)
9 (40.9%) 6 (27.3%) 7 (31.8%)
16 (32.7%) 22 (44.9%) 11 (22.4%)
Driving reduction Reduced Not reduced
64 (61.5%) 40 (38.5%)
18 (75%) 6 (25%)
14 (60.9%) 9 (39.1%)
18 (81.8%) 4 (18.2%)
44 (89.8%) 5 (10.2%)
Driving confidence Reduced Not reduced
10 (9.6%)
94 (90.4%)
8 (33.3%)
16 (66.7%)
2 (8.7%)
21 (91.3%)
7 (31.8%)
15 (68.2%)
25 (51%) 24 (49%)
Self-rated quality of driving Excellent Good Average
39 (37.5%) 59 (56.7%)
6 (5.8%)
3 (12.5%)
13 (54.2%) 8 (33.3%)
7 (30.4%) 12 (52.2%) 4 (17.4%)
1 (4.5%)
18 (81.8%) 3 (13.6%)
3 (6.1%)
34 (69.4%) 12 (24.5%)
Perception of crash compared to self, ten years ago Not likely Somewhat likely
89 (85.6%) 15 (14.4%)
14 (58.3%) 10 (41.7%)
16 (69.6%) 7 (30.4%)
15 (68.2%) 7 (31.8%)
36 (73.5%) 13 (26.5%)
Public transport use Frequently or sometimes Never or rarely
29 (27.9%) 75 (72.1%)
8 (33.3%)
16 (66.7%)
8 (34.8%) 15 (65.2%)
14 (63.3%) 8 (36.4%)
20 (40.8%) 29 (59.2%)
Family discussion Yes No
32 (30.8%) 72 (69.2%)
11 (45.8%) 13 (54.2%)
8 (34.8%) 15 (65.2%)
14 (63.6%) 8 (36.4%)
31 (63.3%) 18 (36.7%)
Mean (±SD) Mean (±SD) Mean (±SD) Mean (±SD) Mean (±SD) Age 74.88(4.57) 74.33 (3.35) 74.04 (5.56) 77.68 (6.08) 77.20 (5.64)Driving experience 55.13 (5.88) 52 (6.79) 54.13 (4.65) 56.95 (6.28) 57.58 (6.74)Driving Avoidance Scale 0.49 (0.54) 0.59 (0.50) 0.39 (0.53) 1.04 (0.46) 1.07 (0.60)PDA scale 2.45 (0.45) 2.02(0.61) 2.41 (0.48) 1.98(0.43) 2.04 (0.44)Driving stress scale 2.11 (0.54) 1.78 (0.67) 2.21 (0.64) 1.77 (0.51) 1.69 (0.51)Driving relinquishment scale 1.17 (0.59) 1.33 (0.54) 1.08 (0.51) 1.54 (0.33) 1.41 (0.47)
Annual kilometres driven differed significantly between PAPM groups (χ2(8)
= 18.539, p = 0.018). Around 40.9% of participants in stage 5 (Planning to act) and
32.7% of participants in stage 6 (Self-regulating) reported driving less than 5,000
km/year compared to 4.3% of those in stage 4 (Resisting action) and 19.2% of those
in stage 2 (Unengaged). Reduction of driving compared to ten years ago differed
significantly between PAPM groups (χ2(4) = 15.564, p = 0.004). Around 81.8% of
participants in stage 5 (Planning to act) and 89.9% of participants in stage 6 (Self-
regulating) reported driving less compared to 60.9% of those in stage 4 (Resisting
action) and 61.5% of those in stage 2 (Unengaged). Self-rated confidence differed
significantly between PAPM groups (χ2(4) = 36.820, p <0.001). Around 31.8% of
participants in stage 5 (Planning to act), 33.3% of those in stage 3 (Undecided) and
51% of participants in stage 6 (Self-regulating) reported less confidence compared to
8.7% of those in stage 4 (Resisting action) and 9.6% of those in stage 2 (Unengaged).

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 131
Perception of the likelihood of being involved in a crash compared to ten years ago
differed significantly between PAPM groups (χ2(4) = 10.908, p = 0.028).
Interestingly, around 41.7% of participants in stage 3 (Undecided) reported greater
likelihood of being involved in a crash compared to 31.8% of participants in stage 5
(Planning to act), 30.4% of those in stage 4 (Resisting action), 26.5% of participants
in stage 6 (Self-regulating) and 14.4% of those in stage 2 (Unengaged). Public
transport use differed significantly between PAPM groups (χ2(4) = 10.887, p
=0.028). The majority of participants (63.6%) in stage 5 (Planning to act) reported
using public transport frequently/sometimes compared to 40.8% of those in stage 6
(Self-regulating), 34.8% of those in stage 4 (Resisting action), 33.3% of those in
stage 3 (Undecided) and 27.9% of those in stage 2 (Unengaged). Being involved in a
family discussion differed significantly between PAPM groups (χ2(4) = 19.061, p
<0.001). Around 63.6% of participants in stage 5 (Planning to act) and 63.3% of
participants in stage 6 (Self-regulating) reported having a family discussion
regarding their driving compared to 45.8% of those in stage 3 (Undecided), 34.8% of
those in stage 4 (Resisting action), and 30.8% of those in stage 2 (Unengaged).
Driving avoidance differed by PAPM stage (F(4,217)=13.69, p<0.001). Post
hoc tests revealed that the driving avoidance scale scores were higher for those in
stage 6 (Self-regulating) than in stage 4 (Resisting action) (0.682, 95% CI (0303 to
1.06), p <0.001), stage 3 (Undecided) (0.474, 95% CI (0.100 to 0.847), p=0.005), and
stage 2 (Unengaged) (0.581, 95% CI (0.322 to 0.841), p<0.001). Driving
relinquishment scale scores also varied by PAPM stage (F(4,217)= 3.86; p=0.005)
and the mean scale scores were statistically significantly lower for those in stage 2
(Unengaged) than those in stage 5 (Planning to act) (0.37, 95% CI (0.024 to 0.714), p
=0.030), and participants in stage 4 (Resisting action) scored significantly lower than
those in stage 5 (Planning to act) (0.46, 95% CI (0.02 to 0.89), p=0.035). Driving
Stress scores differed by PAPM stage (F(4,217) =7.02; p<0.001). Mean driving
stress scale score were higher for those in stage 6 (Self-regulating) compared to stage
2 (Unengaged) (0.411, 95% CI (0.145 to 0.676, p <0.001), and stage 4 (Resisting
action) (0.512, 95% CI (0.125 to 0.900), p <0.05). Mean PDA scores varied with
PAPM stage (F(4,217) =10.78; p<0.001) and were higher for those in stage 2
(Unengaged) compared to stage 3 (Undecided) (0.422, 95% CI (0.0127 to 0.718), p
<0.001), stage 5 (Planning to act) (0.474, 95% CI (0.169 to 0.781), p <0.001), and

132 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
stage 6 (Self-regulating) (0.407, 95% CI (0.181 to 0.633), p<0.001). In addition,
PDA scores were higher for those in stage 4 (Resisting action) compared to stage 3
(Undecided) (0.38, 95% CI (0.0062 to 0.767), p =0.004), stage 5 (Planning to act)
(0.43, 95% CI (0.0498 to 0.8276), p =0.018), and stage 6 (Self-regulating) (0.37,
95% CI (0.0413 to 0.7006), p=0.019).
Predictors of PAPM stages
Binary logistic regression modelling was used to determine the characteristics
of those who plan and adopt changes in their driving in comparison to those who
have decided not to change. Intercorrelations between predictor variables showed no
excessive multicollinearity. A hierarchical regression model was developed, where
we controlled for the effect of socio-demographics, driving experience, and self-rated
health as these variables have been commonly used within the older driver literature
as predictors of self-regulatory behaviours. Our analysis therefore focused on the
effect of modifiable psychosocial and environmental factors. Relevant independent
variables were included in the analysis with a p-value cut-off point of 0.25. Stepwise
logistic regression was conducted and variables were retained in the model at p<0.05.
Binomial regression analysis was conducted to compare the characteristics only of
those in the “Pre-decision” versus “Decision” phases. Table 6.7 presents the result of
the hierarchical logistic regression.
At step 1 of the regression analysis, socio-demographic, self-rated health, and
driving experience variables significantly predicted group membership (F (7,199)
=20.066, p<0.001) and accounted for 13.2% of the variance in decision to change
driving.
Table 6.7: Hierarchical regression analysis (n=199) Step Variable B Wald Exp(B) R2 R2 change F 1
Age Gender (reference Female) Annual Km/driven (reference >10,000 km/yr.) 5,001-10,000 km/yr. Less than 5000 km/yr. Self-rated health (reference Excellent) Very good
0.066 -0.139 0.268 0.734 0.534
2.680 0.160 0.510 3.026 1.235
1.069 0.870 1.307 2.083 1.706
0.132* 20.066*

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 133
Average Licensed year
0.972 0.034
3.354 1.006
2.643 1.035
2 Age Gender (reference Female) Annual Km/driven (reference >10,000 km/yr.) 5,001-10,000 km/yr. Less than 5000 km/yr. Self-rated health (reference Excellent) Very good Average Licensed year Self-rated quality of driving (reference excellent) Good Average Family discussion Yes Driving relinquishment scale Confidence Reduced
0.032 -1.22 0.419 0.797 0.076 0.310 0.076 1.879 2.141 1.151 1.020 1.065
0.438 0.090 0.954 2.384 0.017 0.238 3.575 9.445* 8.248* 8.623* 7.959* 6.841*
1.032 0.885 1.521 2.218 1.078 1.363 1.079 6.548* 8.505* 3.165* 2.772* 2.902*
0.412 0.28 71.014*
N=199, *p<0.05,
After controlling for the effect of socio-demographic factors and driving
experience, the psychosocial and environmental factors in the model accounted for
an extra 28% of the variability. In the final model, age, gender, self-rated health, and
driving experience were not significant predictors of group membership. The
significant predictors in the final model were self-rated driving confidence (β =
1.065, p <0.01), family feedback (β = 1.152, p <0.01), overall self-rated quality of
driving (β = 1.879 and 2.141, p <0.01) and driving relinquishment scale (β = 1.020, p
<0.01).
6.8 DISCUSSION
The purpose of this study was to further examine the applicability of the
Precaution Adoption Process Model in understanding self-regulatory driving
behaviours among older adults. A major concern regarding the older driver literature

134 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
is the scarcity of theoretically-based research. To the authors’ knowledge, few
studies have attempted to develop a model of self-regulatory driving behaviours
among older adults based on the stages of change theory.
The findings from this study indicate that older drivers can be categorised into
stages of the PAPM (Table 5) with the majority of participants (46.8%) in stage 2
(Unengaged). This may indicate that older drivers, while aware of the impact of
ageing on driving abilities, are not personally engaged. Only 22.1% of participants
belonged to stage 6 (Self-regulating) of the PAPM, despite over two thirds of
participants indicating they have reduced their driving compared to ten years ago.
Driving reduction could be a reflection of individual’s lifestyle preference and not
related to the declining abilities associated with ageing. This is partly supported by
the emerging evidence that, similar to older drivers, younger drivers also avoid some
driving situations (Blanchard & Myers, 2010; Naumann et al., 2011)
Of interest in this study are the characteristics associated with stages of PAPM.
It is postulated that awareness of risk and precaution effectiveness can influence
people’s movement between early stages of the PAPM (Weinstein & Sandmand,
2002). In our sample, participants in stage 2 (Unengaged) and stage 4 (Resisting
action) scored significantly higher on the PDA scale, which indicates higher self-
ratings of driving ability, compared to those in the other stages. The role of insight
and self-awareness in driving self-regulation has been identified by several authors
(Anstey et al., 2005). Whether older drivers are aware of their functional abilities or
not remains questionable. According to Ball et al. (1998) older drivers are aware of
their declining driving abilities and regulate their driving accordingly (Ball et al.,
1998). On the other hand, a number of studies have reported that older drivers tend to
overrate their driving abilities and performance. For instance, Holland and Rabbitt
(1992) revealed that drivers in their 70s rated their sensory abilities to be similar to
those in their 50s (Holland & Rabbitt, 1992). Freund et al. (2005) demonstrated a
significant association between higher self-rating of skills and increased risk of
driving difficulty (Freund et al., 2005).
The importance of driving is another significant factor that can impact older
drivers’ decision to regulate and/or stop driving. The majority of older drivers view
driving to be key to their independence and mobility (Adler & Rottunda, 2006;
Musselwhite & Haddad, 2010a). Described by some as a symbol of identity
(Eisenhandler, 1990), independence (Persson, 1993), and security (Bauer,

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 135
Kuskowski, et al., 2003), it is no wonder that the decision to stop driving is one of
the most difficult decisions that older adults have to make (Adler & Rottunda, 2006).
In our study, participants viewed driving to be extremely important. There was a
statistically significant association between PAPM stages and driving relinquishment
scale. Participants in stage 5 (Planning to act) reported significantly higher scores on
the driving relinquishment scale (which indicates more positive attitude towards
giving up driving) compared to those in stage 2 (Unengaged) and stage 4 (Resisting
action).
Previous studies point to the important role of confidence as a mediator
between declining abilities and self-regulation (Parker et al., 2001; Rudman et al.,
2006), with a large number of studies reporting significant association between self-
reported driving confidence/comfort and driving behaviour (Baldock et al., 2006a;
Marottoli & Richardson, 1998; Parker et al., 2001). Older drivers avoid situations
where they lack confidence (e.g. driving at night or at night in the rain) (Baldock et
al., 2006; Charlton et al., 2006). In our sample, confidence was significantly
associated with PAPM groups and higher scores (which indicate greater confidence)
were seen among those in stage 4 (Resisting action) and stage 2 (Unengaged).
However as pointed out by Motak et al. (2014) self-regulation as a result of lack of
confidence may be cause for concern (Moták et al., 2014) rather than an indication of
successful self-regulation. Therefore, the success of self-regulation in terms of
enhancing safety depends largely whether it is based on awareness and resulting
compensation, or lack of confidence. Self-regulation of driving as a response to the
discomfort older adults experience in stressful driving conditions rather than
intentional monitoring of their driving ability (Meng & Siren, 2012) may therefore
represent a failure of self-regulation rather than a success. These drivers may
attribute their feelings of discomfort to external reasons (i.e. glare from other cars’
headlights on their glasses, changes in the road systems) rather than possible declines
in their own driving abilities (Hassan et al., 2015). However, this effect of
discomfort can also have the opposite effect, with drivers indulging in unnecessary
driving restrictions (Meng & Siren, 2012). Drivers who impose unnecessary
restrictions on their driving due to lack of confidence may be able to safely drive in
these situations if they adopted other coping strategies such as pre-journey planning
or vehicle modifications (Gwyther & Holland, 2014).

136 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Providing feedback regarding driving-related abilities may assist older adults in
making better and informed decisions regarding their driving (Holland & Rabbitt,
1992; Owsley et al., 2003). In our study, 44.6% of participants had discussed their
driving with their doctors, 43.2% with their family, and 21.2% with their friends.
Being involved in a family discussion about driving in the past year differed
significantly between PAPM stages. Qualitative research indicates that older drivers
prefer to receive feedback from someone who has direct knowledge and
understanding with their driving (Coughlin et al., 2004). Generally, family members
may be the first to express their concerns over an older adult’s driving ability
(Gillins, 1990). Feedback can also be given by healthcare professionals and many
older drivers will give up driving if advised to do so by their physician (Coughlin et
al., 2004; D'Ambrosio et al., 2008).
The later stages of the PAPM deal with barriers towards adoption of the
precaution. In our study, participants in stage 5 (Planning to act) were significantly
more likely to report more use of public transport. These findings are consistent with
previous research which indicates that the availability of other transport options
(Coughlin, 2001) and the cost of public transport (Corpuz, 2007) are important
factors in the decision to give up driving among older adults. Unfortunately, older
drivers often view public transportation to be inaccessible, expensive, inconvenient,
unsafe, and unreliable (Allan & McGee, 2003; Gardezi et al., 2006) and often view
taxis as an expensive form of transportation and report concerns over their personal
safety (Oxley et al., 2003). A number of psychological barriers (e.g. feeling they are
a burden, fear for safety) (Taylor & Tripodes, 2001) and geographical barriers (e.g.
availability of alternative transport or social support) (Musselwhite & Haddad,
2010b) can also affect the usage of these alternatives. Shifting to a new
transportation option requires active planning (Shergold et al., 2012) and people are
less keen to obtain information about alternative transport options (Nordfjærn et al.,
2014) especially if they do not consider they need such information (Shergold et al.,
2012).
Planning retiring from driving can make the experience less traumatic and
improve the outcomes through gradual preparation and feeling of control (Buys et
al., 2012; Liddle, Gustafsson, Bartlett, & McKenna, 2012). In line with previous
research conducted by Molnar et al. (2013), we investigated participants’ life goal

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 137
decisions and whether they impact their driving behaviour and decision making
process. Around 25.2% of participants indicated that they had moved to a new place
closer to their common destinations, 22.1% had moved to a place with better public
transport options, and 14.9% had moved to a seniors’ home. While not significantly
different among PAPM groups, moving to a seniors’ home was significantly
associated with driving reduction with 87.9% of those living in seniors’ homes
indicating that they have reduced their driving compared to 68.3% of those who are
still living at home. Unfortunately, previous research indicates that the vast majority
of older drivers do not plan the transition to a non-driving state, even those who
suffer from medical conditions that can impair their driving (Adler & Rottunda,
2006; Peel et al., 2002). Older drivers may be reluctant to engage in planning due to
their awareness of the potentially negative outcomes of driving cessation ( King et
al., 2011).
A hierarchical regression analysis was conducted after controlling for the effect
of age, gender, self-rated health, and driving experience to examine the impact of the
psychosocial and environmental factors on PAPM stages. Given the small sample
size, participants were grouped into two groups based on their decision to self-
regulate their driving. Those in stages 2 and 3 were collapsed into one group, the
Pre-decision group, while those in stages 5 and 6 were collapsed into the Decision
group. The significant predictors in the final model were self-rated driving
confidence, family feedback, overall self-rated quality of driving and driving
relinquishment scale. The cross-sectional nature of the study makes it impossible to
determine if these variables predict transitions between stages of PAPM. However,
the previous older drivers’ literature point out the role each of these variables plays
in the decision-making process among older drivers. It is therefore crucial to
investigate the role of these factors as predictors for PAPM stages transition by
conducting longitudinal studies that follow older drivers through stages of change.
It is also important to note that stage theories have been criticised for
oversimplifying complex human behaviour and imposing artificial stages (Littell &
Girvin, 2002). While uncommon, driving cessation can occur unexpectedly as a
result of sudden illness, involvement in a crash, or failing a driving test (Dellinger et
al., 2001). Driving cessation is usually more of a gradual and voluntary process
(Dellinger et al., 2001; Hakamies-Blomqvist & Wahlström, 1998) and there is

138 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
evidence that the driving cessation process may occur through stages (Hassan et al.,
2015; Kostyniuk et al., 1998; Kowalski et al., 2014). This suggests that older driver
interventions should be tailored to the specific needs of each individual (including
the stage they are at) and recognises that older adults should not be treated as a
homogenous group (Hassan et al., 2015). Further, the determinants of driving-
regulation are a mixture of environmental, psychological, and social factors.
Theorizing self-regulatory driving behaviour is therefore important to enhance our
understanding of this process. Stages of change theories can assist in providing a
generalized description and a means of planning interventions (Liddle et al., 2004).
The PAPM has been used previously to study adoption of behaviours related to
osteoporosis prevention (Mauck et al., 2002), disaster preparedness (Glik et al.,
2014), epilepsy (Elliott et al., 2007), colorectal cancer screening (Costanza et al.,
2005), fruit intake (de Vet et al., 2008), coping with premenstrual syndrome (Delara
et al., 2012), and home radon testing (Weinstein et al., 1998). In relation to driving,
the PAPM has been explored by Kostyniuk et al. (2000), however the adaptation of
the PAPM in their study was not fully described, and was based mostly on older
adults’ awareness of their declining abilities, i.e. it failed to recognize the influence
of other external and internal factors on the process of self-regulation (Kostyniuk et
al., 2000).
To the authors’ knowledge, this study is the first to attempt to examine the
association between psychosocial and environmental variables and PAPM stages of
change among older drivers. This study provides further support for the proposition
that self-regulatory driving behaviour among older drivers can be examined using the
PAPM. Further experimental research is planned to investigate the impact of
evaluative feedback on participants’ self-awareness of their driving ability and
subsequent stage transition. However, there is a need for a prospective study where
older drivers are followed through the stages of change as they occur, to better
determine which variables predict the adoption of self-regulatory driving behaviours
among older adults.
6.9 LIMITATIONS
The recruitment strategy may have attracted active and healthier drivers who
are more interested in driving and more safety-oriented. This may have resulted in
fewer participants in stage 4 (Resisting action). The findings are based on a small

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 139
sample of Brisbane and Sunshine Coast drivers and the extent to which the results
can be generalised to other Australian states is unclear. Cognitive functioning was
not assessed in this study. This is an important factor in the ability to self-regulate
driving. Very few participants reported that they were involved in a crash recently
which made it difficult to explore this variable. Self-report measures were used to
assess driving pattern and health status, and may be subject to recall bias. This study
also employed a cross-sectional design and without longitudinal studies that follow
older drivers through the process of self-regulation it will be difficult to conclude
which and how certain factors influence older drivers’ decision to change and/or stop
their driving. This study used a staging algorithm adopted from previous studies,
however, with limited validity and reliability. This may have resulted in participants
being misclassified into the wrong stages. Future studies should attempt to overcome
this limitation by employing reliable and valid tools for classification.
6.10 CONCLUSION
A theory-based understanding of the process of self-regulation among older
drivers will support the development of effective interventions to promote safe
driving or improve outcomes of driving cessation. By applying a stage-based
approach, the self-regulation process can be broken down into qualitatively different
categories that accommodate the heterogeneity of the older driver population. This
would allow interventions to be customised based on the individual’s specific need.
Successful self-regulation relies on accurate insight into one’s driving ability and the
PAPM identifies awareness and personal engagement as the initial step towards
behaviour change. Further, the PAPM differentiates between those who are not
engaged by the issue and those who are resistant to change. Older drivers who are
reluctant to modify their driving may benefit from interventions targeted towards
creating safer vehicles and safer road networks. Our study indicates that there are
significant differences among PAPM stages of change. Further, a number of
psychosocial variables significantly predicted the adoption of self-regulatory
behaviours among participants.
Acknowledgment
The Australian Postgraduate Award Scheme provided funds for the PhD
research program of the first author.

140 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Chapter 7: Older adults’ self-regulatory driving behaviour: A latent class analysis (Study 2, Phase 2)
7.1 PUBLICATION STATUS
This chapter comprises Paper 3 as taken from: Hassan, H. & King, M. (Under
preparation). Older adults’ self-regulatory driving behaviour: A latent class analysis.
7.2 STATEMENT OF CONTRIBUTION
The candidate, as first author, accepts the overall responsibility for this
publication. The candidate was responsible for all aspects of the manuscript
preparation, including reviewing the literature, formulating the research question,
conducting and supervising data collection, analysing and interpreting the results and
writing and submitting the final manuscript. All co-authors meet the criteria for
authorship and take responsibility for their role in delivering the publication. All of
the co-authors of this paper are members of the candidate’s supervisory team and
their contribution to this paper was supervisory in nature. Written permission was
provided from each to include the publication as part of this thesis and its publication
on the QUT ePrints database.
Principal Supervisor Confirmation
I have sighted email or other correspondence from all Co-authors verifying their
authorship
Dr Mark King QUT Verified Signature 30 Aug 2017
------------------------- ----------------------------------- ------------
Name Signature Date

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 141
Older adults’ self-regulatory driving behaviour: A latent class analysis
7.3 ABSTRACT
Self-regulation of driving has been proposed as an effective strategy to keep
older adults driving safely for longer. Little is known of what influence older adults’
decision to adopt self-regulatory driving behaviours. Previous studies have shown
that older drivers go through different stages towards adopting self-regulation.
Interventions that address factors relevant to each stage can therefore be more
effective than “one-size-fits-all” strategies. Hassan and colleagues (2015)
developed an initial model of self-regulation using the Precaution Adoption Process
Model (PAPM) as a theoretical framework. The present study aims to build on the
previous research by investigating whether there are distinct profiles of older adults
based on their mindsets towards adopting self-regulatory driving behaviour which
match those in the PAPM model. We used latent class analysis to identify driving
self-regulatory profiles of 222 older adults based on their driving perceptions,
importance of driving, and perceived barriers towards giving up driving. Latent class
analysis identified three classes of older drivers. Class 1 (n=104) consisted of those
who had the lowest levels of reported driving confidence, driving comfort, and
perceived driving abilities. They were least likely to agree that giving up driving
would restrict their mobility or independence. Class 2 (n=66) consisted of those who
had the highest levels of reported perceived driving ability. They were most likely to
agree that driving cessation would restrict their mobility and independence, and that
lifestyle factors were barriers to changing their driving. Class 3 (n= 52) consisted of
those who had low perceived driving abilities and were most likely to agree that they
would be letting other people down if they stop driving. The latent class analysis
categories differed in terms of the kinds of intervention that appear likely to address
them. It is recommended that interventions be customised to meet the need of each
class.
Keywords
Mobility, Precaution Adoption Process Model, Safety

142 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
7.4 INTRODUCTION
The proportion of older drivers in Australia is predicted to increase due to a
combination of population ageing and increased licensure of successive age cohort
(King & Scott-Parker, 2016). This in turn will present some major challenges in
terms of maintaining their safety and mobility. Driving is essential to older people’s
independence and well-being and driving cessation has been linked to many negative
outcomes (Liddle, Carlson, & McKenna, 2004). As people age, they start
experiencing declines in the sensory, motor, and cognitive abilities necessary for safe
driving (Anstey, Wood, Lord, & Walker, 2005). As a group, older adults are
relatively safe drivers, however due to their increased fragility, they are over-
represented in serious and fatal crashes (Li, Braver, & Chen, 2003). Considerable
attention has been directed towards strategies that can ensure road users’ safety
without compromising older adults’ mobility. Self-regulation of driving has been
promoted as an alternative positive approach to keep older adults driving safely for
longer (Lang, Parkes, & Medina, 2013 ).
Previous studies have identified several factors associated with self-regulation, still,
how these factors come together in the final decision remains unclear. As Molnar
and colleagues (2015) highlight “it is important to extend the current research by
trying to tease out the relationships between self-regulation and the factors for which
there is already considerable evidence” and there is a need “for a more
comprehensive, theoretically-informed, and uniform approach to investigating self-
regulation by older drivers”. Few studies have attempted to find a theoretical
framework to account for the process of self-regulation in older adults. The
challenge in developing a model of driving self-regulation results from the
heterogeneity of the older driver population in terms of their abilities, needs, and
resources. Previous studies have pointed out that older drivers go through different
stages of change towards modifying their driving and ultimately stopping driving
(Kostyniuk et al., 1998; Liddle et al, 2004). The stages of changes theories could be
useful in describing and providing a general understanding of change and planning
interventions (Liddle et al., 2004). This suggests that older driver interventions
might need to be tailored to the specific needs of each individual (including the stage
they are at) and would need to be customised to move individuals through the stages
of change towards adoption of safe driving behaviour. They would ideally be

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 143
developed by taking a strategic approach using both a theory of the change process
and existing evidence from previous attempts to achieve change. However, there has
been little development of stage-based theories applied to driving self-regulation, and
hence there is a lack of research on theoretically-informed interventions that facilitate
older drivers’ planning for future self-regulation and even driving cessation.
The literature suggests that self-awareness and insight into driving ability play a
major role in successful driving regulation among older drivers (Anstey et al., 2005).
Therefore, older drivers need to perceive their declining driving abilities as a threat
to their overall safety before they are interested in self-regulation. This situation is
suited to the application of the Precaution Adoption Process Model (PAPM) to the
self-regulatory behaviours of older drivers, which has been examined by Kostyniuk
et al. (2000). The PAPM describes how individuals move through stages of change
towards adoption of health protective behaviour (Weinstein & Sandmand, 2002).
The early stages of the PAPM are defined in terms of psychological states and
mindset of individuals (Weinstein & Sandmand, 2002). The later stages are mostly
governed by factors that can facilitate or hinder the adoption of the precaution.
Individuals progress through seven stages from lack of awareness to action:
unawareness (stage 1); awareness that there is an issue but a lack of personal
engagement with it (stage 2); engagement (“this applies to me”) but indecision (stage
3) about the need to act; either a decision not to act (stage 4) or a decision to act
(stage 5); if the latter, acting by taking the precaution (stage 6) (e.g. self-regulating);
and maintaining the behaviour (stage 7). Hassan et al. (2015) examined the
applicability of the PAPM in understanding older adults’ self-regulatory driving
behaviours (Hassan, King, & Watt, 2015). Subsequently, they applied these stages to
a survey sample of older drivers, demonstrating the utility of the approach. However,
the question remains whether older adults’ self-regulatory driving behaviour is a
reflection of the stages of change described by the PAPM. This study, therefore,
builds on the research reported in Hassan et al. (2017) by utilising a bottom-up
approach to profile older drivers based on their mindset towards adopting self-
regulatory driving behaviours using Latent Class Analysis. Latent Class Analysis
(LCA) is a person-centred approach commonly used to identify subgroups with
distinctive patterns. Unlike cluster analysis which identifies groups based on some

144 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
measure of similarity, LCA classifies objects according to their probabilities of the
values of all observed variables (Elliott, Jacobsohn, Winston, & Ginsburg, 2012).
Graver and colleagues (2008) states that “latent class regression analysis allows the
researcher to build, identify, and test a regression model that is relevant for each
latent, unobservable segment of the population. Specifically, latent class regression
analysis forms segments of subjects (employees, customers, suppliers) that possess
similar beta coefficients from multiple regression analysis. The technique is relevant
for both academic researchers and practitioners, and can be valuable to theoretical
development”. LCA has been used previously in the transport literature (De Oña,
López, Mujalli, & Calvo, 2013; Elliott et al., 2012) and with older drivers (Choi,
DiNitto, & Marti, 2015). A recent study in 2017 described three latent classes of
driving self-regulation among 729 older drivers based on their self-reported driving
frequency and avoidance behaviour (Bergen, West, Luo, Bird, et al., 2017).
The PAPM explain how people reach decisions to act and how they translate
that decision into actions. The early stages (from stage 1 to stage 5) describe the
decision-making process, while the late stages (stages 6 and 7) describe the acting
process. All the stages prior to action are defined in terms of mental states rather
than in terms of factors external to the person. Our study attempted to investigate
whether there are distinct profiles of older drivers based on their mindsets towards
self-regulating their driving behaviours rather than their actions which correspond to
the early stages of the PAPM (stages 1-5).
We hypothesised that there are three possible outcomes to the LCA
1. Our sample is homogenous and does not contain different groups of
driving behaviour.
2. Our sample is heterogeneous and contains subgroups of older drivers that
correspond with the PAPM stages of change.
3. Our sample is heterogeneous and contains subgroups of older drivers
that do not correspond to the PAPM stages of change.

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 145
7.5 METHOD
Participants and procedure
The detailed method for collection of the survey data on which this study is
based has been published previously (in press). Briefly, we recruited a total of 247
Australian drivers through various recruitment strategies to ensure sample variability.
Eligible participants were current drivers aged 70 years and older who resided in the
Brisbane and Sunshine Coast areas of Queensland, Australia. The study was
conducted between May 2014 and October 2014. Participants completed the
questionnaire online or in a paper-based form with a paid return envelope to the
principal researcher. Both questionnaires included an information sheet describing
the nature of the study and completing the questionnaire was considered evidence of
consent to participate. All participants received the chance to enter a draw to win
one of ten $50 shopping vouchers. All procedures were approved by the Human
Research Ethics Committee of Queensland University of Technology.
Material
The questionnaire collected information on the socio-demographics (age,
gender, education, employment, etc.), self-rated health, crash history, driving
experience, current driving patterns, driving perceptions, driving feedback
experiences and transport options of older drivers.
Indicators of willingness to regulate and/or stop driving latent class membership
The selection of the latent class analysis indicators was guided by the PAPM
and the literature on older drivers’ safety. The PAPM offers a flexible framework
and the factors influencing stage transitions are not clearly defined. The early stages
of the PAPM reflect individuals’ mindsets towards adopting the change and are
affected by individuals’ perceptions and perceived barriers towards adopting the
change. Perceptions about one’s ability is a strong determinant to reduce and/or
restrict driving (Anstey et al., 2005). Numerous studies point to the significant
association between self-reported driving confidence/comfort and driving behaviour
(Blanchard & Myers, 2010). The importance of driving is another significant factor
that can impact older drivers’ decision to regulate and/or stop driving (Adler &
Rottunda, 2006; Musselwhite & Haddad, 2010a). In addition, perceived barriers

146 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
(e.g. maintenance of independence and lifestyle) can affect adoption of self-
regulation (Gwyther and Holland, 2012).
Assuming that these predictors comprise the most relevant factors for
explaining behaviour change, it should be possible to characterise individuals in
different mindsets. For instance, those in the early stages of the PAPM will have
lower perception of risk and greater perceived barriers to change.
Driving perception
Driving confidence was measured by a single question “compared to ten
years ago, do you still feel confident that you can safely drive to places you need to
go” with answers ranging through “much less”, “a little less”, “the same”, and
“more”. For analysis, participants were grouped into two categories, reduced
confidence (much less, a little less), or not reduced (the same, more). In addition,
participants’ self-reported driving stress was measured using a scale developed by
Hakamies-Blomqvist (1994a) that measures participants’ experienced stress in a
number of driving situations on a 4-point scale ranging from 0 (heavy stress) to 3 (no
stress) and a total “Driving Stress” score was calculated (Hakamies-Blomqvist,
1994a).
Perception of crash risk was measured using three different questions: “how
likely is it for you to have a car crash compared to other people your age”, “how
likely is it for you to have a car crash compared to yourself ten years ago”, and “how
likely is it for you to be injured if you are involved in a car crash” with answers
ranging from “extremely likely”, “somewhat likely”, and “not at all likely”.
The perceived driving ability scale (PDA), a previously validated 15-item
scale (MacDonald, Myers, & Blanchard, 2008), was used to measure participants’
current perceived driving abilities (e.g., to see road signs at a distance, to see vehicles
coming up alongside, to make an over the shoulder check) along a 4-point scale
(‘‘poor’’, ‘‘fair’’, ‘‘good’’, ‘‘very good”). A mean scale score was computed with
higher scores indicating more positive perceptions.
Importance of driving
Participants’ views about the importance of driving were measured by asking
participants to indicate their agreement with two statements (“giving up driving will
restrict my mobility” and “giving up driving will restrict my independence”) along a

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 147
5-point scale (“Strongly disagree”, “disagree”, “neither disagree or agree”, “agree”,
“Strongly agree”)
Barriers towards giving up driving
Participants’ views about the barriers toward giving up driving were measured
by asking participants to indicate their agreement with five statements (“giving up
driving will let other people down”, “changing my driving is not possible because of
my lifestyle”, “changing my driving is not possible because others rely on me”,
“changing my driving is not possible because public transportation is not available
for me”, and “changing my driving is not possible because I can’t rely on others”)
along a 5-point scale (“Strongly disagree”, “disagree”, “neither disagree or agree”,
“agree”, “Strongly agree”)
7.6 ANALYSIS
Before conducting the analysis, data screening was performed to check for
missing data. A total of 222 cases were included in the final analysis. Missing
values on psychosocial scales were replaced with the series mean to compute the
average score. Several variables were collapsed into two or three alternatives to
obtain meaningful categories with respect to the purposes of the study. Scales were
dichotomised on the median for ease of interpretation of the latent classes. We
performed LCA using MPlus Version 7.1. The number of latent classes was
determined based on the findings from several statistical fit indices: the Akaike
information criterion (AIC), the Bayesian information criterion (BIC), the sample-
size-adjusted BIC (SSABIC), the Vuong-Lo-Mendell-Rubin adjusted likelihood ratio
test (LMR), and the entropy values. Lower values on the AIC, BIC, and SSABIC
indicate better fitting models, with the BIC being the most reliable of these fit indices
(Nylund, Asparouhov, & Muthén, 2007) . Higher entropy values indicate clearer
classification (Ramaswamy, Desarbo, Reibstein, & Robinson, 1993).
Table 7.1: Sample characteristics (n=222) Mean age in years (SD) 75.5 (5.1) Gender Male Female
135 (60.8%) 87 (39.2%)
Principal driver

148 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Yes No
154 (69.4%) 68 (30.6%)
Education Primary school Secondary school Certificate Bachelor degree Postgraduate degree
13 (5.9%) 90 (40.5%) 55 (24.8%) 39 (17.6%) 25 (11.3%)
Dwelling A private home A retirement home or seniors’ complex
172 (77.5%) 50 (22.5%)
Living condition Alone With spouse or partner Other
74 (33.3%) 136 (61.3%) 12 (5.4%)
Employment Yes No
66 (29.7%) 156 (70.3%)
Driving environment City Suburb Rural
28 (12.6%) 160 (72.1%) 15 (6.8%)
Trip length Less than 15 minutes 15-30 minutes More than 30 minutes
22 (9.9%) 125 (56.3%) 75 (33.8%)
Driving experience, years open driving license (mean and standard deviation)
55.4 (6.3%)
Annual km driven Less than 5,000 km/year 5,000-10,000 km/year More than 10,000 km/year
52 (23.4%) 89 (40.1%) 81 (36.5%)
Driving reduction Much less A little less The same More
88 (39.6%) 70 (31.5%) 52 (23.4%) 12 (5.4%)
Self-rated health Excellent Very good Fair Poor
39 (17.6%) 132 (59.5%) 48 (21.6%) 3 (1.4%)
Self-rated quality of driving Excellent Good Average
53 (23.9%) 136 (61.3%) 33 (14.9%)
Perception of crash compared to ten years ago Somewhat likely Not likely
52 (23.4%) 170 (76.6%)
Driving confidence Much less A little less The same More
1 (0.5%) 51 (23%) 167 (75.2%) 3 (1.4%)

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 149
7.7 RESULTS
Sample Characteristics
The sample ranged in age from 70 to 94 years (M= 75.5, SD ± 5.1), and
included 87 females (39.2 %) and 135 males (60.8%) (Table 7.1). Around 23% of
participants rated their health to be fair, 59.5% to be very good, and 17.6% to be
excellent.
Determination of number of classes
Latent class solutions containing 2 through 5 classes were fitted to the data.
Based on the LMR test value, the three-class solution was the best fitting model
(Table 7.2). Specifically, the LMRT value did not indicate that the four-class
solution was a better fit than the three-class solution, despite having lower values on
other fit indices. In addition, the addition of the fourth class did not add
substantively to the meaning of the latent classes and was formed of only a small
number of cases. Model fit should always be judged based on substantive meaning
(i.e., the classes should be distinct and meaningful) (Nylund et al., 2007).
Table 7.2. Model Fit Statistics
Number of classes 2 3 4 5 AIC 2718.747 2681.277 2648.596 2636.819BIC 2797.009 2800.371 2808.522 2837.577BIC adjusted 2724.120 2689.453 2659.575 2650.601Entropy 0.805 0.814 0.804 0.846 Vuong-Lo-Mendell-Rubin Likelihood ratio test
-1461.798 (p<0.0001)
-1336.374 (p<0.02)
-1305.639 (p=0.2774)
0.2947
Class indicators and interpretation of classes
The average latent class assignment probabilities for individuals assigned to
each class is presented in Table 7.3. Overall, values close to 1 indicate a high
precision or reliability of the classification; with values of 0.8 or larger indicating a
good class solution (Celeux & Soromenho, 1996). We obtained high class
assignment probabilities for the three classes (0.96, 0.89, 0.89). As shown in Table
7.3, participants in class 1 and class 3 were more likely to report lower ratings of
their driving abilities and higher ratings of driving stress compared to those in class
2. Participants in class 2 and class 3 were more likely to report greater barriers to
stopping driving compared to those in class 1. For those in class 3, letting others

150 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
down and having people relying on their driving appeared to be a greater barrier
compared to the other two classes.
Table 7.3: Item-response probabilities
Class homogeneity Class separation
Variable Class 1 N=104
Class 2 N=66
Class 3 N=52
Class 1 vs. 2
Class 1 vs. 3
Class 2 vs. 3
Stress (high) 0.7 0.1 0.6 0.04 0.64 15.8 PDA (poor) 0.7 0.05 0.7 0.02 0.9 45.39
Letting others down
0.3 0.8 1 9.65 1 1
Lifestyle is a barrier
0.2 0.8 0.8 21.98 21.13 0.96
Others rely on me
0.03 0.6 0.9 51.17 325.9 6.38
(Class homogeneity individuals within a given class are similar to each other with respect to item responses (above 0.7 or below 0.3) and class separation individuals across two classes are dissimilar with respect to item responses. (>5 or <0.2))
Class 1 N= 104
Class 2 N=66
Class 3 N=52
Confidence Reduced Not reduced
0.354 0.646
0.053 0.947
0.218 0.782
Perception compared to others Somewhat likely Not likely
0.205 0.795
0.000 1.000
0.332 0.668
Giving up driving will restrict my mobility Agree Disagree
0.737 0.263
0.922 0.078
0.935 0.065
Giving up driving will restrict my independence Agree Disagree
0.772 0.228
0.982 0.018
0.944 0.056
Giving up driving will let other people down Agree Disagree
0.312 0.688
0.814 0.186
1.000 0.000
Changing my driving is not possible because of my lifestyle Agree Disagree
0.216 0.784
0.858 0.142
0.853 0.147
Changing my driving is not possible because others rely on me Agree Disagree
0.032 0.968
0.627 0.373
0.915 0.085
Changing my driving is not possible because public transportation is not available Agree Disagree
0.217 0.783
0.376 0.624
0.608 0.392

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 151
Changing my driving is not possible as I can’t rely on others Agree Disagree
0.297 0.703
0.571 0.429
0.816 0.184
Stress High stress Low stress
0.738 0.262
0.104 0.896
0.646 0.354
PDA Low perception High perception
0.751 0.249
0.057 0.943
0.733 0.267
The LCA identified 3 classes; 104 of the participants were classified into
class 1, 66 were classified into class 2, and 52 were classified into class 3. Table 7.4
presents the characteristics of the classes where significant differences were found;
they related primarily to travel and driving patterns, and feelings regarding fitness to
drive. It can be seen there are distinct differences which are discussed further below.
Almost all participants of class 3 were principal drivers opposed to two third of
participants in class 1 and class 2. Participants in class 2 reported greater use of in-
vehicle technology and limited use of public transport compared to those in the other
two classes. They were also more likely to driver for greater distances and longer
durations. Participants in class 1 were more likely to report feeling unfit to drive
compared to the other two classes.
Table 7.4. Significant differences between latent classes
Class 1 Class 2 Class 3 Age (Mean, SD) 76.2 (5.2) 74 (3.5) 76.1 (6.3)Annual Km Less than 5,000 km/year 5,001 to 10,000 km/year More than 10,001 km/year
33 (31.7%) 41 (39.4%) 30 (28.8%)
7 (10.6%) 29 (43.9%) 30 (45.5%)
12 (23.1%) 19 (36.5%) 21 (40.4%)
Trip Length Less than 15 minutes 15-30 minutes More than 30 minutes
11 (10.6%) 58 (55.8%) 35 (33.7%)
1 (1.5%) 41 (62.1%) 24 (36.4%)
10 (19.2%) 26 (50%) 16 (30.8%)
In-vehicle technology use Yes No
47 (45.2%) 57 (54.8%)
48 (72.7%) 18 (27.3%)
29 (55.8%) 23 (44.2%)
Public Transport use Sometimes Never/Rarely
50 (48.1%) 54 (51.9%)
13 (19.7%) 53 (80.3%)
16 (30.8%) 36 (69.2%)
Principal driver Yes No
66 (63.5%) 38 (36.5%)
41 (62.1%) 25 (37.9%)
47 (90.4%) 5 (9.6%)
Motivation to change driving Feeling unfit to drive
76 (73.1%)
37 (56.1%)
28 (53.8%)
Avoid driving at night in the rain Avoid completely Very often
21 (20.2%) 14 (13.5%)
1 (1.5%) 3 (4.5%)
6 (11.5%) 9 (17.3%)

152 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Reasonably often Not often Not at all
20 (19.2%) 26 (25%) 23 (22.1%)
6 (9.1%) 21 (31.8%) 35 (53%)
11 (21.2%) 13 (25%) 13 (25%)
Table 7.5. Frequencies of LCA classes for PAPM stages obtained by staging algorithm
Stages obtained by PAPM algorithm Latent Class 1 Latent Class 2 Latent Class 3
Stage 2 (unengaged) 33 43 28
Stage 3 (Undecided) 12 6 6
Stage 4 (Decided not to act) 8 11 4
Stage 5 (Decided to act) 19 0 3
Stage 6 (Acting) 32 6 11
Total 104 66 52
Table 7.5 demonstrates the frequencies of LCA classes for PAPM stages obtained by
the staging algorithm adopted from Weinstein et al. (2008) (χ2(8) = 37.596, p <
0.0001). The latent classes consisted mainly of participants in stage 2 the
unengaged, with the majority seen in class 2. Almost half of the participants in stage
5 and 6 of the PAPM belonged to class 1.
7.8 DISCUSSION
This study aimed to identify distinct self-regulatory driving profiles of older
drivers based on their mindset towards change. Using LCA, we identified three
unique classes. Individuals in class 1, which we have labelled as “willing to
change”, had high levels of stress and poor perception of their driving abilities.
Driving was still important in terms of their mobility and independence; however,
they identified fewer barriers in regard to changing their driving. This class
resembles stage 5 (decided to act / the planner) in the PAPM where individuals
acknowledge the limitations in their driving and the need to modify their driving
behaviour accordingly. While driving is still important, participants are more open
towards change and are relying more on the public transport system. Participants in
this class reported greater use of alternative transport which could indicate that they
are looking and testing alternative options to driving. Individuals in this class would
benefit best from support in overcoming barriers toward modifying their driving (e.g.
social support, alternative transport options, enhances self-efficacy).

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 153
Individuals in class 3, labelled “the unwilling” also had high levels of stress and
poor perception of their driving abilities. However, they differ from participants in
class 1 in that they perceive greater barriers in regard to giving up driving
particularly in letting others down and having others relying on them. This
resembles stage 4 of the PAPM where drivers have been made aware of limitations
in their driving abilities however, they are unwilling or unable to change.
It is notable that 90% of participants in this class were principal drivers, compared to
almost 60% in the other two classes. It is possible that the drivers in this class are
expressing an inability to self-regulate because of external factors, such as the
expectations of others, an unvarying mobility need and a lack of alternatives. This
implies that they perceive self-regulation as impossible given these (supposedly)
external factors. In practice, these factors may not be as impossible to change as
these drivers believe. For example, they may not be aware of some alternative
options, and the people who rely on them to drive may understand the issues faced
by these drivers and can find their own alternatives. It is also possible that
individuals in this class, despite being aware of limitations in their driving, cannot
see the impact of such decline on their safety. Motor vehicle crashes are rare events
so that possibility of increased crash risk may not create a sense of urgency, and
other health and life goals may be perceived as more important. On the contrary,
driving self-regulation may be viewed as a negative behaviour that can impair one’s
mobility and independence. Prioritising driving self-regulation is therefore a
complicated task that could require extensive deliberation and persuasion. To make
matters worse, the strategies and behavioural changes needed to achieve optimal
driving self-regulation, in terms of reducing crashes, are not clearly defined. It is
difficult for older adults to determine which modifications in their driving behaviours
can translate into improved safety. Individuals in this class may not respond well to
feedback and could benefit from passive interventions (e.g. in-vehicle technology,
improvements in road infrastructure).
Individuals in class 2 were labelled as “the unaware”, and had positive perceptions
about their driving abilities. This group also had the highest probability of
identifying lifestyle factors as a barrier to changing their driving. This class is
similar to stage 2 of the PAPM (unengaged) which is comprised of older adults who
are either not experiencing declines in their abilities that necessitate changes in their

154 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
driving behaviour or who are unaware of such declines. It represents a stage prior to
the decision-making process, where individuals have not thought about the need to
change. Interestingly, participants in this class reported greater use of in-vehicle
technology compared to the other two classes. It could be possible that the use of
such technology enables the driver to compensate for some limitations and to
maintain safe driving, an area that deserves more attention. Individuals in this class
would benefit from interventions that enhance their awareness of limitations in their
driving abilities (e.g. customised feedback, on-road assessments).
It is notable that the LCA did not identify all the stages that comprise the
PAPM. To some extent this is an artefact of the study design; for example, the
recruitment material and participant information sheets suggest that age-related
declines in driving exist, so it is unlikely that a participant could claim to be
“unaware” of the issue and therefore in stage 1 of the PAPM. It has been noted in
other research on stages of change approaches that some stages are passed through
very rapidly (Lenio, 2006), which means that the probability of selecting participants
while they are in this stage is low; the non-identification of a class similar to stage 3
the undecided may be an example of this. Nevertheless, examining the self-
regulatory driving behaviour within a health behaviour framework is challenging.
Health behaviour theories deal with behaviours considered “harmful” to the
individual (e.g. smoking, lack of physical activities). As noted by Kostyniuk et al.
(2000) driving in itself is not a harmful behaviour, it is only when certain abilities are
compromised that the risk of crash might increase. The PAPM is a preventative
decision-making framework constructed around the goal of preventing or minimising
future harm, ideal when dealing with complex behaviours, which fits perfectly with
driving self-regulation.
The findings suggest that the driving self-regulation of older adults can be
conceptualised within the PAPM. However, some modifications to the PAPM
framework are needed given the unique nature of driving. The refined model
consists of self-regulatory profiles of older drivers identified from the LCA which
represents certain stages of the PAPM.
Another important finding is that the latent classes and the stages obtained by
the staging algorithm adopted from Weinstein et al. (2008) do not correspond well.

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 155
The use of such staging algorithm without further validation can increase the risk of
misclassification.
Figure 7.1: Refined model of self-regulatory driving behaviour
7.9 LIMITATIONS
The recruitment strategy may have attracted active and healthier drivers who
are more interested in driving and more safety-oriented. The findings are based on a
small sample of Brisbane and Sunshine Coast drivers and the extent to which the
results can be generalised to other Australian states is unclear. Self-report measures
were used to assess driving pattern and health status, and may be subject to recall
bias. This study also employed a cross-sectional design and without longitudinal
studies that follow older drivers through the process of self-regulation it will be
difficult to conclude which and how certain factors influence older drivers’ decision
to change and/or stop their driving.
Conclusion
This study provides further support that older drivers are heterogeneous
group and interventions should be customised to meet individuals’ needs. The
findings also indicate that older adults’ self-regulatory driving behaviour could be
classified within the PAPM framework, although there are differences in latent
classes associated with awareness of decline and perceived ability or opportunity to

156 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
address it. Therefore, it is implied that interventions should be designed to cater for
each distinct class. However, future studies incorporating larger samples are needed
to validate this finding and to identify the social factors and explanatory mechanisms
that are linked with membership in each profile In addition, future research should
be directed toward prospectively examining self-regulatory profiles of older drivers.
Acknowledgment
The Australian Postgraduate Award Scheme provided funds for the PhD
research program of the first author.
The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 157
Chapter 8: Feedback and older drivers (Study three)
8.1 INTRODUCTORY COMMENTS
As discussed in the previous chapters, older drivers hold different attitudes and
beliefs towards driving. Older drivers go through different stages of behavioural
change towards modifying their driving. Distinctive profiles of older drivers can
represent different stages of the PAPM and would correspond to different
interventions (Table 8.1). As Weinstein et al (2008) state “the PAPM is a conceptual
framework or a skeleton that needs to be fleshed out for each behaviour with
information about how stage transitions occur”. Older adults driving behaviour has
not been examined before within the PAPM framework. Therefore, the interventions
proposed in Table 8.1 are guided by the recommendations provided by Weinstein et
al (2008), previous literature on older drivers, and the results of the qualitative study.
Feedback can play a major role in promoting stage transition. The transition
between stage 2 (unengaged) to stage 3 (engaged but undecided) can be facilitated by
feedback that comes from trusted individual (e.g. health professionals or family
members). This feedback would allow older drivers to start wondering about their
own abilities and whether it has changed as they aged. It could be the starting point
for them to seek more customised feedback that can help them evaluate their own
skills and bridge the gap between their perceived and actual driving abilities. It will
therefore enhance older adults’ awareness about their driving limitations and could
initiate the decision-making process (the later stages of the model).
Kruger and Dunning (1999) states that inaccurate self-evaluation of one’s skills
and abilities can be caused by four feedback-related reasons; lack of feedback,
attributing failure to other causes than lack of skill, not understanding why failure
occurred, and not receiving self-corrective information (Dogan, Steg, Delhomme &
Rothengatter, 2012). As driving is a habitual process, older drivers hardly receive
any evaluative feedback about their driving and therefore fail to accurately evaluate
their driving skills and abilities. Few participants in study one indicated that they
sought feedback from professional driving instructors which they viewed positively.
Driving instructors can objectively assess older adults’ actual driving performance.

158 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
They can provide them with driving-specific feedback on how to improve their skills.
As noted by Di Stefano and Lovell (2006) “Driving instructors have a major role in
assisting older drivers to maintain their driving skills and retain their licences in
both ‘refresher’ and ‘rehabilitation’ contexts”. This pilot study aimed to assess the
acceptability of providing one-on-one feedback regarding driving performance to a
sample of older drivers. The study also investigated the impact of such feedback on
older drivers’ perception of the quality of their driving and their willingness to
modify their driving behaviour.
Table 8.1: Adaptation of the PAPM to older drivers’ regulatory behaviours Stage Profile Characteristics Interventions
Stage 1 The unaware Generally unaware of the impact of
age-related declines on one’s
driving abilities OR unaware of the
self-regulatory practices to reduce
one’s risk of crash
Unaware Uninformed
(general)
This stage is not relevant to
the older drivers because
older drivers are generally
aware that driving changes
as they age. However,
individuals may benefit from
media campaigns that help
eliminate the negative
stereotyping of the older
drivers, encourage them to
seek feedback and promote
self-regulation.
Stage 2 The unengaged Generally aware of the problem but
do not recognise the changes in their
own abilities and/or never thought
about the adoption of self-regulatory
practices
Unaware uninformed
(personal)
Individuals in this stage will
correspond well to
interventions that provide a
personal message relevant to
their situation. Feedback
should be personalised and
delivered from trusted
person.
Stage 3 The undecided Aware of changes in their own
abilities but are either unsure of how
it impacts their driving or how they
should modify their driving
accordingly
Undecided
Individuals in this stage are
often reluctant to change and
weighing the pros and cons.
Interventions should
persuade drivers-at-risk of
modifying their driving
behaviours and inform them
about the benefit of adopting
self-regulation
Stage 4 The resister Thought about it but refused to
either acknowledge the need to
modify their driving behaviours or
Individuals in this stage are
very difficult to change
because they have informed

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 159
unable to modify their behaviours
Unwilling or discouraged decisions about the topic.
They may benefit well from
passive interventions (e.g.
improvement in road
environments, ADAS).
Continuous persuasion and
encouragement is needed.
Stage 5 The planner Thought about it and starting to
monitor their driving and plan to
change their driving accordingly
Willing or encouraged
Individuals in this stage are
planning to change but they
may lack the needed
resources or the detailed
direction of how to adopt the
change. Interventions should
remove the surrounding
barriers and provide them
with detailed instructions on
how to adopt the change.
Stage 6 The regulator Have started to reduce and/or avoid
certain driving situations in
response to their declining abilities
Reinforcement
Stage 7 The non-driver Have stopped driving altogether in
response to their declining abilities
Reinforcement
8.2 METHODS
Participants and recruitment
A total of 26 Australian drivers were recruited through the Royal Automobile
Club of Queensland (RACQ) which is a motoring club and mutual organisation,
providing roadside assistance, insurance, travel, finance and other services to its
Queensland members. They are involved in running a number of older driver
programs in Queensland that aims to improve the safety of senior drivers. They run
a 50-minute, one-on-one Driver Assessment program which covers; driving skills
and behaviours, application of road rules in traffic conditions and hazards that drivers
may come across in their everyday driving. As will be explained below, a much
higher number of participants had been anticipated, based on advice from RACQ
about the rates of referral in previous years. Eligible participants were current
drivers, English speaking, aged 65 years and older. All procedures were approved by
the Human Research Ethics Committee of Queensland University of Technology.

160 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Procedure
Most of the participants were referred to RACQ by their physician to assess their
fitness to drive. The remaining participants took part in the RACQ one-on-one
Driver Assessment Program to get their driving skills evaluated. The study was
conducted between March 2015 and November 2015. The driver instructor met the
participants at their home either in the morning or the afternoons. Participants
received an information sheet describing the nature of the study (Appendix H). The
drive was conducted in an RACQ vehicle which is dual-controlled, 4-cylinder
automatic car. The drive occurred in a light-to-moderate traffic density in fine
weather conditions and took approximately 50 minutes to complete. The drive
included variety of locations such as roundabouts, lane-changing and merging,
narrow suburban roadways, intersections, Stop and Give way situations, and self-
navigation exercises. Participants completed a pre-test questionnaire prior to their
on-road assessment (Appendix I). After the drive, participants received customised
feedback in regard to their driving and were asked to complete the post-test
questionnaire (Appendix J). The feedback was customised one-on-one which
involved:
• Driving skills and behaviours
• Application of road rules in traffic conditions
• Hazards that drivers may come across in their everyday driving.
The feedback provided the driver with a clear idea about their driving performance,
their driving errors, and how to continue to drive safely (Appendix K).
Materials
A questionnaire was designed to collect information on the socio-
demographics, self-rated health, crash history, driving experience, current driving
patterns, driving perceptions, feedback about driving and transport options of older
drivers. In addition, participants’ driving reduction was measured by asking
participants to rate the overall amount of their driving compared to ten years ago, on
a 4-point scale from “much less” to “more”. Participants’ self-restriction and
avoidance behaviour was measured by asking participants to rate the extent to which
they would avoid driving under 18 various challenging driving conditions (e.g.
driving at night-time, driving alone, driving on high traffic roads, etc.) on a 5-point
Likert type scale from “not at all” (0) to “avoid completely” (4). A driving

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 161
restriction score was calculated based on the average score of responses to the 18
items with higher scores indicating increased avoidance.
Outcome variables:
Participants’ self-rated quality of driving was assessed by asking participant
“how would you rate your quality of driving?” with possible answers ranging from
poor, fair, average, good, excellent prior to and after the drive.
Participants’ willingness to change was assessed by asking “now that you have
received the driver instructor’s feedback which statement better describe you?” with
possible answers ranging from I will not change my driving, as I believe I am a safe
driver and my driving abilities has not changed, I intend to start monitoring my
driving abilities and changing my driving accordingly, I intend to start avoiding some
challenging driving situations, I intend to consider giving up driving altogether. This
was compared to their PAPM stage.
8.3 ANALYSIS
Before conducting the analysis, data screening was performed to check for
missing data. A total of 21 cases were included in the final analyses. Missing values
on psychosocial scales were replaced with the series mean to compute the average
score. Several variables were collapsed into two or three alternatives to obtain
meaningful categories with respect to the purposes of the study. Participants’
characteristics were described with median and range for continuous variables or
frequencies and percentages for categorical variables. Exploratory non-parametric
tests were chosen given the small sample size and the violations of the assumption of
normality (Wilcoxon signed-rank test and McNemar’s test). The alpha level for
significance was adjusted to a value p < 0.025. Data were analysed in SPSS version
20.0 (IBM Corporation, Armonk, NY).
8.4 RESULTS
Sample characteristics
The sample ranged in age from 71 to 88 years (Median= 80.5, Range= 17), and
included 6 females (28.6 %) and 15 males (71.4%) (Table 8.2). Nine participants
rated their health to be fair, nine to be very good, and three to be excellent. Most
participants (57.1%) rated their driving to be good. The majority of participants
(57.1%) indicated that they have reduced their overall driving compared to ten years

162 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
ago. Participants preferred to receive feedback about their driving from their doctor
(71.4%), their family members (9.5%), or from a person of authority (19%). All the
participants indicated that a medical problem could be a reason to stop or modify
their driving with 71.4% of participants indicating that they would stop driving if
advised by their doctor. Six participants received recommendations to stop driving,
two of them ignored the advice, two requested their driving to be formally assessed,
one restricted driving, and one has stopped driving. Around 66% of participants in
our study indicated that they rarely or never use public transport. Around 90% of
participants indicated that they rarely or never use taxis. Finally, 52% of participants
indicated that they rarely or never rely on their family for transport. Psychometric
properties of all scales used in this study are shown in Table 4, together with means
and standard deviations.
PAPM stages
Around 33% of participants belonged to stage 2, 14.3% were categorised into
stage 3, 33.3% were in stage 4, 14.3% were in stage 5, and 4.8% of participants were
in stage 6. For the analyses, participants were combined into two groups; those who
did not change their driving behaviour comprising stages 2, 3 and 4 (81%); and those
who changed their driving behaviour or intend to do so comprising stages 5 and 6
(19%).
Table 8.2: Sample characteristics (n=21)
Age (Median and range) 80.5 (17) Gender Male Female
15 (71.4%) 6 (28.6%)
Principal driver Yes No
17 (81%) 4 (19%)
Education Primary school Secondary school Certificate Bachelor degree Postgraduate degree
3 (14.3%) 12 (57.1%) 4 (19%) 1 (4.8%) 1 (4.8%)
Living condition Alone With spouse or partner Other
6 (28.6%) 13 (61.9%) 2 (9.5%)
Employment Yes No
3 (14.3%) 18 (85.7%)
Driving reduction Reduced Not reduced
12 (57.1%) 9 (42.9%)
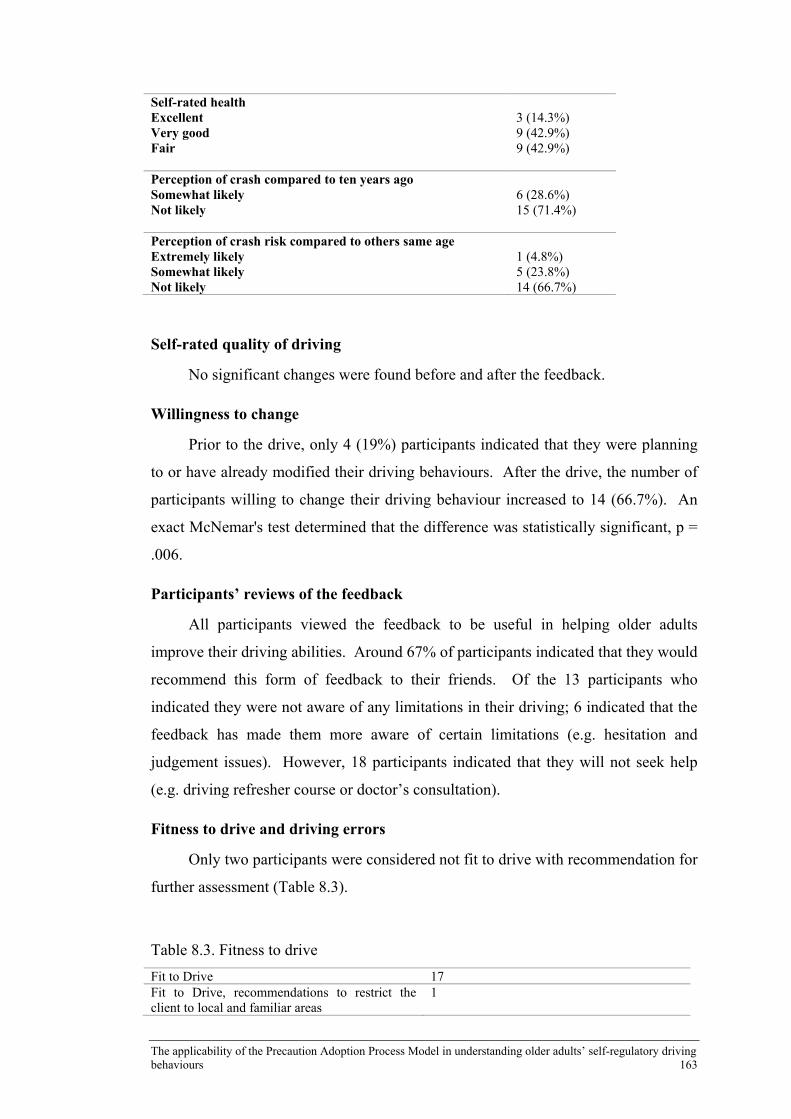
The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 163
Self-rated health Excellent Very good Fair
3 (14.3%) 9 (42.9%) 9 (42.9%)
Perception of crash compared to ten years ago Somewhat likely Not likely
6 (28.6%) 15 (71.4%)
Perception of crash risk compared to others same age Extremely likely Somewhat likely Not likely
1 (4.8%) 5 (23.8%) 14 (66.7%)
Self-rated quality of driving
No significant changes were found before and after the feedback.
Willingness to change
Prior to the drive, only 4 (19%) participants indicated that they were planning
to or have already modified their driving behaviours. After the drive, the number of
participants willing to change their driving behaviour increased to 14 (66.7%). An
exact McNemar's test determined that the difference was statistically significant, p =
.006.
Participants’ reviews of the feedback
All participants viewed the feedback to be useful in helping older adults
improve their driving abilities. Around 67% of participants indicated that they would
recommend this form of feedback to their friends. Of the 13 participants who
indicated they were not aware of any limitations in their driving; 6 indicated that the
feedback has made them more aware of certain limitations (e.g. hesitation and
judgement issues). However, 18 participants indicated that they will not seek help
(e.g. driving refresher course or doctor’s consultation).
Fitness to drive and driving errors
Only two participants were considered not fit to drive with recommendation for
further assessment (Table 8.3).
Table 8.3. Fitness to drive
Fit to Drive 17 Fit to Drive, recommendations to restrict the client to local and familiar areas
1

164 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Fit to drive but with recommendations to enhance skills and confidence
1
Not fit to drive 2
The first participant displayed on several occasions his complete lack of
mirror and shoulder check for vehicles potentially hidden in his blindspot. He also
had problems with road positioning prior to turning as he turned from the centre of a
wide single lane road to the right with minimal indication. The driving instructor
commented that “although the client drives with confidence and is not
inappropriately overcautious, he does not display forward planning and I was not
satisfied with their ability to predict and avoid conflicts”. The second participant
displayed on several occasion his complete lack of mirror and shoulder check (e.g.
changing lane while another vehicle is beside him, wandering into an adjacent lane
and turning across an intersection too slowly). His vehicle operation skills were not
always appropriate, such as slowing down to almost a complete stop when turning
into side streets. The participant’s concentration seemed to waver at some times and
he caused an unsafe situation to eventuate and as a result the driving instructor was
required to verbally and physically intervene during the assessment. The driving
instructor commented that “Even though the client appeared to drive with a high
degree of self-confidence, I did not feel entirely safe as a passenger and was not
totally satisfied with their ability to predict and avoid all traffic conflicts. My main
concern is the driver’s lack of awareness at times of his surrounding and what he
perceives to be a safe speed in some situations. On the day, the only reason the
client was not involved in an incident was due to my intervention and the evasive
action of other drivers. I am not convinced that he will act upon the advice given”.
Driving errors were classified into legal or safety errors (Table 8.4). There
was a total of eight errors and nineteen errors that fell under the legal and safety
categories respectively.
Table 8.4. Driving errors observed in the driving assessment
Legal errors Indication at Roundabout-Incorrect Technique Inconsistent indication at roundabouts Line and lane markings were crossed on multilane roads/roundabouts Crossing lane line markings at intersections Failure to give way to other vehicles/pedestrians at intersections Failure to indicate when turning and when merging Speeding
1 6 2 1 1 2 3

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 165
Failure to stop at Stop sign 2 Safety errors Generally insufficient use of rear-view mirrors Insufficient/Absence blind spot observation when merging or changing lanes Not cancelling indicators at times Not keeping up with traffic at times Insufficient safe space when stopped in traffic Inadequate lateral scanning Failure to observe traffic signs, lane/road markings Insufficient safe space when driving Inappropriate speed Occasional issues with holding a safe lane position Generally poor forward observation In car conversation caused a loss of concentration at times Reversing errors Very late indication and incorrect road position for a turn Late braking Seating position too reclined Gap selection when merging Lane changing process too slow Slow to proceed when turning at intersections
9 8 1 1 5 8 7 7 7 2 3 4 4 1 1 1 1 1 1
8.5 DISCUSSION
Before discussing the findings from the study, it is important to note that
recruitment of participants proved to be very difficult and the small sample size
makes it difficult to reach significant findings. The driving instructors indicated that
the number of referrals made by health professionals (on which the planning for this
study was based) had significantly decreased compared to previous years. Many
eligible participants refused to take part in the study. The sensitivity of the topic and
the anxiety associated with the whole assessment procedure may have contributed to
this. The recruitment difficulty highlights important issues that deserve further
exploration in future studies. First, it is important to examine the perceptions of both
physicians and older drivers on the physician referral system and how this impacts on
the patient-doctor relationship. Second, it is important to “normalise” the topic of
driving assessment and cessation among the older population. The introduction of
this topic from early stages may make it easier to discuss it later (Betz, Jones,
Petroff, & Schwartz, 2013). Third, the stereotyping of the older drivers as timid and
dangerous may add to the sensitivity of the topic and refusal to participate. Lastly, it
is important that the driving assessment programs are more readily available,
appropriately tailored, and promoted.
Nevertheless, the findings from this study add to our understanding of the
acceptability of providing feedback to older drivers and its impact on their self-rated

166 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
quality of driving and willingness to change. Overall, majority of participants were
in stage 2 or stage 4 of the PAPM. These findings are consistent with previous
research (Freund et al., 2005) which demonstrated that older drivers assign high
ratings to their driving skill even when being referred for assessment. This could
indicate that discussion with physicians about possible problems in their driving and
being referred for further evaluation did not increase their self-awareness.
Participants may have truly viewed their driving abilities to be unchanged and did
not feel the need to change. It could also reflect a state of conscious denial
complicated by the importance of driving on their independence and mobility
(Freund et al., 2005). This is interesting because around 71% of participants
indicated that they would stop driving if advised by their doctor. It could be possible
that the discussion with their physicians lacked the depth needed to persuade them
about the need to monitor and/or modify their driving. The feedback received from
their doctor could have been non-evaluative and incomprehensive which failed to
increase their awareness. Another possibility is that participants may have been
referred by doctors who are not their regular physicians. Therefore, they may have
lacked the trust in the advice given.
Another interesting finding is the limited use of public transportation and
taxis among our sample. This could be because the majority of participants were the
principal drivers in the household and others may have relied on their driving.
Few participants were considered unfit to drive as they displayed on several
occasions their lack of safe driving skills. Consistent with previous studies, the
majority of driving errors were related to visual scanning and signalling and
indication (Koppel et al., 2016). Emerging studies indicate that older drivers’ skills
can improve with evaluative feedback and driving training programs (Romoser,
2012). In regards to feedback, all participants viewed the feedback to be useful in
helping older adults improve their driving abilities and the majority indicated that
they would recommend this form of feedback to their friends. Of the 13 participants
who indicated they were not aware of any limitations in their driving; 6 indicated that
the feedback has made them more aware of certain limitations (e.g. hesitation and
judgement issues). However, 18 participants indicated that they will not seek help
(e.g. driving refresher course or doctor’s consultation). The feedback had no impact
on participants’ ratings of their driving ability. Still, the majority of the participants

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 167
indicated that they are now planning to modify their driving behaviours. It could be
possible that the short-time frame did not give the participants enough time to reflect
on the content of the feedback.
8.6 LIMITATIONS
The study used a very small sample, the findings can’t be generalised to wider
population. The study did not include a control group and feedback was provided by
different instructors and may not be standardised. Participants were referred by their
doctors, social desirability bias and conscious denial may have affected their
answers. Participants’ cognitive abilities were not assessed.
Chapter 9: Discussion
9.1 CHAPTER OVERVIEW
Self-regulation of driving is a promising approach that can assist older adults to
maintain their driving privilege. Still, there is a lack of a comprehensive theoretical
model that positions the process of self-regulation within a framework of behaviour
change. By enhancing our understanding of the process of driving self-regulation,
we can develop effective interventions that can assist in addressing the mobility
needs of the older driver population. The overarching aim of this research program
was to examine the process of self-regulation among older drivers using the PAPM
as a framework in an attempt to develop a comprehensive theoretical model of
driving self-regulation. By doing so, interventions can be adapted to the individual’s
needs and the desired outcome. The previous chapters have documented the research
program which addressed the following objectives:

168 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Objective 1: Explore the preliminary fit of older adults’ driving behaviour
within the PAPM framework using qualitative focus groups among current
older drivers.
Objective 2: Develop a conceptual model based on the PAPM that profiles
older adults into distinctive groups based on their mindset towards adopting
self-regulatory driving behaviours.
Objective 3: Determine the prevalence of PAPM stages in a sample of older
drivers and identify the sociodemographic and psychosocial characteristics of
stages membership.
Objective 4: Identify self-regulatory driving profiles among older drivers
based on their mindset towards change using Latent Class Analysis (LCA)
and determine whether they are similar to those in the conceptual model.
Objective 5: Examine the impact of providing one-on-one feedback
regarding driving performance on stage transition among a sample of older
drivers and its impact older drivers’ perception of the quality of their driving
and their willingness to modify their driving behaviour.
This chapter presents a synthesis of the main findings of the research and
discusses the strength and limitations of the research. The chapter is organised
according to the research questions and concludes with recommendations for future
research.
9.2 OVERALL RESEARCH FINDINGS
Research Question 1
Study One: Can older drivers be grouped into different stages of PAPM based
on their qualitative differences (e.g. attitudes, awareness, and perceptions) and
patterns of change?
Consistent with previous findings (Adler & Rottunda, 2006; Musselwhite &
Haddad, 2010a), participants viewed driving to be key to their independence and
mobility. Most participants, despite being aware of the impact of ageing on driving

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 169
abilities, indicated that their abilities have not changed. Participants indicated that
they have reduced their driving over the years. However, by delving into the
motivations behind such behaviours, it appeared that reasons other than declining
abilities played the biggest role in the decision-making (e.g. retirement and
preference). This is consistent with previous studies (Ball et al., 1998; Blanchard &
Myers, 2010) which have shown that lifestyle factors play a major role in the
changes of older adults’ driving patterns. Without delving deep into the motivations
behind such behaviour, it is impossible to conclude that these behaviours are self-
regulatory in nature. As highlighted by Molnar et al. (2015), this is a major
limitation in most of the previous studies. Another form of strategic self-regulation
that was highly adopted by participants was journey planning which participants
attributed to the constant changes in the roads and for safety reasons. In regards to
driving avoidance, night-time driving and merging were problematic for some
participants which is consistent with previous studies (Ball et al., 1998; Charlton,
Oxley, Fildes, oxley, & Newstead, 2003 & Staplin, Gish, Decina, Lococo, &
McKnight, 1998a).
There is a paucity of research investigating the impact of feedback on older
drivers’ self-awareness and subsequent self-regulatory behaviours. Participants were
asked if they have sought information about their driving ability. Doctor’s advice, a
driving instructor, refresher courses, and the internet were mentioned in several
discussions. For most participants, feedback about regulating or stopping driving had
to come from someone they trust and respect.
This study was also unique in terms of investigating the impact of life-goal
decisions on older adults’ driving patterns. It appeared that participants who lived in
retirement villages where everything is walking distance found it easier to be
prepared to give up driving one day. Others who lived in communities far from
urban areas reported that giving up driving could mean isolation for them.
Participants’ opinions regarding the use of in-vehicle technology were highly
variable. Some viewed technology as a wonderful possibility that could help them
overcome some limitations they encounter in their driving, such as reverse parking,
merging, and driving in unfamiliar places. Alternative transport option is an
important factor as well. In fact, some older drivers may continue to drive despite
being aware of their declining ability to avoid the use of alternative transports (Atkin,

170 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
2001). Issues concerning availability, accessibility, convenience, and acceptance
were raised which is consistent with previous findings (Allan & McGee, 2003;
Gardezi et al., 2006).
The findings from the first study resonate with existing literature on older
driver. However, it was unique because it conceptualised older adults’ driving
behaviour within the stages of the PAPM. It is important to note that the intention
was not to support or reject the PAPM, but to use it as a starting point for the
development of the model.
The first stage of the PAPM was omitted because older adults are generally
aware of the age-related declines in driving abilities. The unengaged which matches
stage 2 of the PAPM is comprised of participants who were aware that ageing can
have impact on people’s driving ability and that older drivers adapt to these changes
by restricting and reducing the amount of their driving. However, participants in this
stage were confident about their driving and did not feel the need to change their
driving or seek feedback regarding their driving ability. Some of the drivers in this
stage indicated that they have not changed the amount of driving “I think I'm still
driving around about as much as we used to, because we're still young enough to get
out and about and we firmly believe that you do what when you can.” Those who
have changed the amount of their driving have attributed the changes to merely
preference or lifestyle changes “I drive less than I did, but that's partly because
driving was part of my career, my work career, and I'm only working part-time now.
I don't have to go out on the road.”
Interestingly, participants in this stage pointed out that age per se is not an
indication to start monitoring or restricting one’s driving “He’s said that to me a few
times. And I say to him, “Why do you feel like that?” and the only answer I get is
“Because I’m, getting old,” but surely, that’s not the criteria. And that’s why I’ve
been trying to question him if he has any other feelings that might be prompting that
thought. It doesn’t matter. The age doesn’t come in to it. It’s just your mental
attitude”. People are driving for longer now and people in their 70s view themselves
capable of driving for the next 20 years or so “It’s never an easy thing when
somebody has to stop driving, I’m not looking forward to it, I’m 70. I just talked to a
friend of mine the other day; her mother stopped driving at 91. I said 91; she goes

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 171
“oh! But Gloria she is a perfectionist she could not drive unless she knew she was
doing it right”.
It also appears that participants in this stage were unable to draw the link
between the impact of the decline of certain ability on their driving performance and
some of them were highly overconfident “My ability is much the same as it always
has been, because when I retired from the workplace, I didn't stop driving. I kept
going, and I've kept going, and I do still drive a lot. Maybe I've slowed down a little,
last time I ever had a speeding ticket in my life. But, I do now tend to be much more
aware of my surroundings. But my ability to drive I think hasn't changed all that
greatly”. However, later in the conversation the same participant admitted to
changes in his vision which had an impact on their driving “I can speak on that for
myself. At Christmas time...I have an eye problem, which has never been a real
problem. But, I went for a check-up two week before Christmas and the specialist
said, do you require glasses to drive, and I said no. I used to have them for reading,
close-up reading. He said, “I have to be honest, if you were here today for a driver's
test, I would have to fail you.” I've gotten used to seeing things the way they are, or
the way they are now, not how they used to be. I went to the eye optometrist and got
a pair of glasses for driving, and yes, it did make a heck of a difference, to see more
clearly when I'm driving”. Participants in this stage did not appear to think about the
future of their driving or plan their retiring from driving “We are travelling now as
much as we can while we can. Because, ahead in the future, who knows. Who knows
about tomorrow, who knows in 10 years' time? But I am very confident in saying that
when I realise, I will give up driving”. They also did not feel the need to seek
feedback about their driving abilities “At this stage, I'm not going to discuss it with
my medical people, but when the time comes, I would certainly respect a professional
giving me clues as which way to go”. Participants in this stage viewed giving up
driving as an emotional and an overwhelming step “Giving up driving is a really
hard move, I've discovered, with other people. They feel as if they've lost their
independence. Even if they're only driving to the local shops and back, they feel as
though they've still got their independence if they can drive. It's very important”.
Driving allowed them to stay connected and was essential for their wellbeing “Very
important. I work part-time. I also play bowls a lot, and I go to different clubs and
things for that. You can't possibly lead a really independent life relying on public

172 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
transport. It's too difficult. It takes a whole day to do one thing, and I don't have time
to do that. It is very important to me, and I think for most older people, it is part of
their independence”. They also held strong opinions against public transport options
“You can't possibly lead a really independent life relying on public transport. It's too
difficult. It takes a whole day to do one thing, and I don't have time to do that.”
The undecided stage matches stage 3 of the PAPM. In this stage, participants
have started to notice changes in their driving ability and are starting to think about
the future of their driving “I think in another three years or four I won’t be driving a
lot, because I’m getting too old”. Driving is still key to their independence; however,
they are starting to consider alternative options such as relying on their partners to
drive them “If I lose my license, I’ve lost my independence. I’ve got to get on a bus,
but I mean I’ve got Maureen anyway so she can drive and she’s a good driver”, or
on public transport “I don't mind public transport. I lived – I’ve – Up when I was in
the country, we had one bus a day and that was a school bus which was pretty hectic,
but if you went out of the school bus, you didn’t get to town. But up here where I
live, there’re lots of buses and there’s trains”. Crash involvement appears to be a
reason to seek advice or consider their driving ability. A female participant who had
been involved in a crash that affected her confidence attempted to seek professional
feedback about her driving ability “I felt I was getting a bit dicky driving so I rang
the NRMA and asked them, “Could I do a driving test?” And he said, “Well, we
don't really do that.” He said, “But I’ll get someone to come down and go with
you.” So, they sort of came from Goldman and took me around where I usually shop
and about two hours later, we got back and I hadn’t hit anything. So anyway, he
said – So I said, “How did I go?” He said, “Well, only two things,” he said, “I
could find.” He said, “You drive too fast and you drive too close to the vehicle in
front.” And do you know what? That has helped my driving so much, just to be told
that. You probably know you’re driving too fast and you know you’re getting there,
but just to be told by someone in authority, it – And because up here, you get on the
highway and it says travel three Chevrons behind, which is a wonderful indication
because it hits you in your mind and you just need a reminder about it” and this
feedback helped her to continue driving and regain her confidence for the time being
“That one I had with the NRMA, that only cost me about $75 and they’re absolutely

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 173
worth every penny. What he – the information and the feedback he gave me and the
feeling I had when I was doing it”.
In the resistant stage, which matches stage 4 of the PAPM, participants have
experienced a situation in which their driving ability has been questioned but it did
not seem as a strong indication for them to change or stop their driving. A female
participant was involved in a crash few years ago that made her questioned whether
she should continue to drive or not “I had my first crash a few years ago, not my
fault, of course. <Laughs> But that’s about all. When I had this crash, I thought
that was a thing to say that I better give up driving. I lasted three days. It was
terrible”. However, few years later she still has not noticed any changes in her
abilities “I think my ability is still the same, but one thing, I think I do notice now,
that I’m a little bit more cautious”. Driving for her is fairly important “I’m more or
less echoing those, yes, independence and lack of public transport. I have family
fairly close by, but I’m the one who goes to see them”. Another participant, who had
recently had her medical certificate issued by the doctor, believes that the doctor had
made a mistake “That was the doctor I went to have it all filled out, and she filled it
out that I always have to wear spectacles, as they call them. Fine. She ticked some
box in it which meant that I had a medical condition. I just had to see her, because I
wanted this form filled out, and I didn't see my usual doctor in the clinic. They kicked
up a fuss down at the registration part, made me fill out acres of forms. I said what's
all this about? They said, medical, medical. I said, I've got to wear glasses, which
are all I consider it. They all looked at me…. Yes. My doctor said she shouldn't have
ticked that. That means if you've got epilepsy or some medical condition that will
interfere with your driving. That now is stuck on my license”. For her, public
transportation is not an option and giving up her driving would have a devastating
impact on her mobility “Because I hate public transportation. Non-existent, at our
end of the world”.
Participants in the planner stage recognise the need to monitor one’s ability
and regulate their driving accordingly “I feel it needs to be self-limiting but feel that,
for me, anyway, there comes to a stage where I will be putting other people on the
road at risk. No matter how much I wanted to keep driving, I wouldn't do it. So, that's
my criteria”. They have made life goal changes to facilitate giving up driving in the
future “I've recently moved into a retirement village, and I've been very careful to

174 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
choose one where there's a very good bus service there. I'm quite prepared that when
the time comes where I feel I'm not good enough to drive, I will give it up, but it's
really important to me. It was one of the things that I looked at” and are more
knowledgeable and acceptable of alternative transport options “The village where I
live, they run a bus to all the shopping centres twice a week, and on the way home,
they'll actually deliver you to your door if you've got shopping. So, that's a wonderful
solution for people. You've got to plan for that”. They are aware that they need to
keep informed about that constant changes around them “I find one of the negative
things amongst our age group is that a lot of older people aren't cognizant with the
road rules that have changed. I've actually got a copy of the latest road rules and
went through it and there are a lot of things that have changed and a lot of new rules
that I wasn't aware with, and I think that the older drivers don't have the experience.
There are road rules that we don't necessarily know. Whereas the younger ones do
and they take their right of way”.
“I think it would be a very good idea, and I'd be quite prepared if someone
came with me for half an hour, or an hour. Whether they are a driving instructor or
somebody else and just pick up any bad habits that I might have, or give me
feedback. I think that would be a great thing to do. My sister has just done it. She
almost had a very bad high-speed accident because she misjudged the speed of the
car coming towards her, so she got someone from a driving school to take her for a
lesson and it was quite helpful”
The last stage which matches stage 6 of the PAPM, the regulator is comprised
of participants who have started to restrict their driving or avoid certain challenges
situations in response to changes in their driving abilities “I think I've changed my
driving. Since I got these (point to his glasses), I don't drive anywhere near as much
in the night-time…. Yeah, where it never used to worry me, headlights or anything
like that. Now, I'd rather not drive in the night-time if I can avoid it… That's right.
No problems with the confidence, about handling the vehicle, or avoiding an
accident. It's just the sight”. They are aware of the changes in their abilities and have
sought feedback from a health professional “I probably won't renew my license next
year. My sight is growing together, it's not calcifying. It's the opposite. My bone
density is over the top of the scale. As a result, I tear tendons and shoulders. My neck
is not getting any better. Occasionally, if I get up too quickly, I get giddy. The doctor

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 175
says it's up to you, but my recommendation is, when your license is due next year,
forget it if you last that long”. They have made plans that would make giving up
driving easier in the future “It's the best move we made. We'd shifted from the Coast
down to the Glass House. We were out there for eight years. Half-acre block was
getting a bit too much for me to manage. My wife was still working, she ran the
Lifeline shops. I was talking to the dog all day and weeding” “We're not going out as
much as what we did. We live in a retirement village, and we're the type of people
that are happy with each other's company. We can sit down and listen to some music,
or watch a DVD, or watch the television, and talk about various things that don't
need to go out. When we were younger, we seemed to always be visiting friends. Our
friends now are within a 50-metre radius, you just walk across the way”. Still, they
are aware that in the future technology can assist to overcome some of the limitations
they are experiencing and promote their mobility for longer “Things have changed,
because technology, you can drive a car now, and it can park itself. Before long,
they're also, as I mentioned earlier, they've got technology where they're thinking
about getting a car from here to there. You jump in your car and say, “I want to go
to...” and it'll happen. Under those circumstances, I would be using those sort of
facilities, and if need be, purchase a car that would be able to do that. There might
be others that would not be able to afford the technology, part of the cost now. They
can't afford an up-to-date car now. I think down in the future, I can see that it will be
happening”.
The findings also informed the development of a conceptual model of self-
regulation, based on the PAPM that provided a description of the factors that can
promote the transition between each stage. By addressing these factors, it appears
possible to design interventions that are specific for individuals’ needs. The model
was based on the stages of the PAPM and provided suggestion of some factors that
can facilitate the transition between the stages towards adoption of change. The
model is described in Chapter 5. It emphasises the role of self-awareness and insight
into one’s driving abilities in moving people from being unengaged (stage 2) to the
pre-decision stage (stage 3). This can be achieved by providing individuals with
customised feedback from trusted sources. Interventions at this stage should aim to
enhance older adults’ awareness and increase their knowledge about the impact of

176 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
ageing on driving (e.g. educational interventions, feedback from health professionals,
or self-assessment tools).
Once engaged, the decision-making process start by examining one’s risk of being
involved in a crash compared to their younger self or compared to others in the same
age. This is the main factor that impact people’s transition to stage 4 or stage 5 of
the PAPM. Individuals who don’t perceive themselves at risk of crash will move to
stage 4 and they may benefit from passive interventions (e.g. in-vehicle technologies,
improvements in road designs, and vehicle modifications) and persuasion. On the
other hand, if older adults perceive themselves to be at risk of crash they will
progress to the stage 5, self-monitoring. In this stage, individuals start to actively
monitor their driving and to determine if they are encountering difficulties or
problems while driving. Individuals also start to seek additional feedback from
various sources (e.g. family, friends, health professionals, or driving instructor).
Based on the content of the feedback and the suggested modifications to one’s
driving, individuals start to weigh the pros and cons of such change. The presence of
environmental barriers such as lack of alternative transport options or being the
principal driver in the household can greatly hinder the progression to stage 6.
Interventions at this stage should aim at addressing barriers towards changing or
modifying behaviours. The final stage represents the stage where drivers are
continuously modifying and regulating their driving in response to declines in their
abilities until they stop driving altogether. It is important that interventions in this
stage reinforce the messages provided in stage 5.
Research Question 2
Study 2, Phase 1: What is the prevalence of the stages of the PAPM in the
study population? What are the psychosocial and environmental factors associated
with stages of the PAPM?
This study aimed to further examine the applicability of the PAPM in
understanding self-regulatory driving behaviours among older adults. Participants
were classified into different stages of PAPM using a stage algorithm adapted from
Weinstein et al. (2002). The majority of participants were in the unengaged stage
(46.8%) followed by stage 6 (22.1%), stage 3 (10.8%), stage 4 (10.4%), and stage 5
(9.9%). The first stage of the PAPM was omitted because older drivers are generally
aware of the impact of ageing on the driving abilities. The last stage of the PAPM

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 177
was also omitted because it was postulated as driving cessation and the study did not
include former drivers. These findings indicate that a significant proportion of
Australian older drivers don’t regulate their driving. Despite around 70% of
participants indicating that they have reduced their driving compared to ten years
ago, only 22% indicated that they are regulating their driving. This is consistent with
the first qualitative study which suggests that older drivers may appear to engage in
self-regulatory driving behaviours such as reducing their overall amount of driving or
avoiding certain challenging situations. However, this reduction or avoidance
behaviour could be the result of lifestyle changes and mere preferences rather than an
actual decline in one’s driving ability.
This study investigated the psychosocial characteristics associated with PAPM
stages. The early stages of the PAPM deal with individual’s mindset, perceptions,
and awareness. There was a significant association between psychosocial factors and
PAPM stages membership. In particular, perceived driving abilities, driving
confidence, and attitudes towards giving up driving were significantly associated
with PAPM stages. The findings indicated that participants in stages 2 and 4 of the
PAPM assign higher self-ratings to their driving abilities, have more negative
attitude towards giving up driving, and have higher driving confidence compared to
those in stages 5 and 6. Successful self-regulation depends largely on individual’s
awareness of limitations in driving abilities rather than the actual abilities (Anstey et
al., 2005). This suggests that individuals in the early stages of the PAPM could
benefit from interventions targeted toward enhancing their self-awareness about their
driving abilities. The late stages of the PAPM deal with barriers towards adoption of
the precaution. Participants in stage 5 (Planning to act) were significantly more
likely to report more use of public transport. These findings are consistent with
previous research which indicates that the availability of other transport options
(Coughlin, 2001) and the costs of public transport (Corpuz, 2007) are important
factors in the decision to give up driving among older adults. Planning retiring from
driving can make the experience less traumatic and improve the outcomes through
gradual preparation and feeling of control (Buys et al., 2012; Liddle, Gustafsson,
Bartlett, & McKenna, 2012). In line with previous research conducted by Molnar et
al. (2013), this study investigated participants’ life goal decisions and whether they
impact their driving behaviour and decision-making process. Around 25.2% of
178 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
participants indicated that they had moved to a new place closer to their common
destinations, 22.1% had moved to a place with better public transport options, and
14.9% had moved to a seniors’ home. While not significantly different among
PAPM groups, moving to a seniors’ home was significantly associated with driving
reduction with 87.9% of those living in seniors’ homes indicating that they have
reduced their driving compared to 68.3% of those who are still living at home.
Unfortunately, previous research indicates that the vast majority of older drivers do
not plan the transition to a non-driving state, even those who suffer from medical
conditions that can impair their driving (Adler & Rottunda, 2006; Peel et al., 2002).
Older drivers may be reluctant to engage in planning due to their awareness of the
potentially negative outcomes of driving cessation (King et al., 2011). Of interest in
this study was the impact of feedback on stage membership. Providing feedback
regarding driving-related abilities may assist older adults in making better and
informed decisions regarding their driving (Holland & Rabbitt, 1992; Owsley et al.,
2003). 44.6% of participants had discussed their driving with their doctors, 43.2%
with their family, and 21.2% with their friends. Being involved in a family
discussion about driving in the past year differed significantly between PAPM
stages. Qualitative research indicates that older drivers prefer to receive feedback
from someone who has direct knowledge and understanding with their driving
(Coughlin et al., 2004). Generally, family members may be the first to express their
concerns over an older adult’s driving ability (Gillins, 1990). A hierarchical
regression analysis was conducted after controlling for the effect of age, gender, self-
rated health, and driving experience to examine the impact of the psychosocial and
environmental factors on PAPM stages. Given the small sample size, participants
were grouped into two groups based on their decision to self-regulate their driving.
Those in stages 2 and 3 were collapsed into one group, the Pre-decision group, while
those in stages 5 and 6 were collapsed into the Decision group. The significant
predictors in the final model were self-rated driving confidence, family feedback,
overall self-rated quality of driving and driving relinquishment scale.
This study provided further support for the proposition that self-regulatory
driving behaviour among older drivers can be examined using the PAPM. Ideally,
the next step would be to conduct a prospective study where older drivers are
followed through the stages of change as they occur, to better determine which

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 179
variables predict the adoption of self-regulatory driving behaviours among older
adults. However, this was not feasible both in regards to time and financial
constraints. To overcome these limitations and test the applicability of the model,
the second phase of study 2 adopted a novel approach. Latent Class Analysis was
employed to determine if distinct self-regulatory driving profiles of older drivers
based on their mindset towards change can be identified from the sample. These
emerging profiles (if any) would then be compared to the stages of the PAPM. The
selection of the indicators was guided by the findings from the first phase of study 2
and the significant characteristics associated with the PAPM stages.
Research Question 3
Study 2, Phase 2: Would groups, identified utilising Latent Class Analysis (LCA),
match those in the conceptual PAPM and those assigned by the stage algorithm?
The LCA identified three unique classes that may be targeted using
intervention programs. Individuals in class 1, which have been labelled as “willing
to change”, had the poorest perception about their driving abilities. Driving was still
important in terms of their mobility and independence, however, they identified
fewer barriers in regards to changing their driving. This class resembles stage 5
(decided to act / the planner) in the PAPM where individuals acknowledge the
limitations in their driving and the need to modify their driving behaviour
accordingly. While driving is still important, participants are more open towards
change and are relying more on the public transport system. Individuals in this class
would benefit best from support in overcoming barriers toward modifying their
driving (e.g. social supports, alternative transport options, enhance self-efficacy).
Individuals in class 2 were labelled as “the unaware”, and had positive perceptions
about their driving abilities. This group also had the highest probability of
identifying lifestyle factors as a barrier to changing their driving. This class is
similar to stage 2 of the PAPM (unengaged) which is comprised of older adults who
are either not experiencing declines in their abilities that necessitate changes in their
driving behaviour or who are unaware of such declines. It represents a stage prior to
the decision-making process, where individuals have not thought about the need to
change. Participants in this class reported greater use of in-vehicle technology
compared to the other two classes. It could be possible that the use of such
technology enables the driver to compensate for some limitations and to maintain

180 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
safe driving, an area that deserves more attention. Individuals in this class would
benefit from interventions that enhance their awareness of limitations in their driving
abilities (e.g. customised feedback, on-road assessments).
Individuals in class 3, labelled “the resisters” as for stage 4 of the PAPM (although
they differ in some respects), are those who have identified weakness in their driving
but are unable or unwilling to change their driving. It appears that having others
relying on their driving and unavailability of other transportation options prevents
them from changing their driving. It is possible that the drivers in this class are
expressing an inability to self-regulate because of external factors, such as the
expectations of others, an unvarying mobility need and a lack of alternatives. This
implies that they perceive self-regulation as impossible given these (supposedly)
external factors. In practice these factors may not be as impossible to change as these
drivers believe. For example, they may not be aware of some alternative options,
and the people who rely on them to drive may understand the issues faced by these
drivers and can find their own alternatives. It is also possible that individuals in this
class, despite being aware of limitations in their driving, cannot see the impact of
such decline on their safety. Motor vehicle crashes are rare events so that possibility
of increased crash risk may not create a sense of urgency, and other health and life
goals may be perceived as more important. On the contrary, driving self-regulation
may be viewed as a negative behaviour that can impair one’s mobility and
independence. Prioritising driving self-regulation is therefore a complicated task that
could require extensive deliberation and persuasion. To make matters worse, the
strategies and behavioural changes needed to achieve optimal driving self-regulation,
in terms of reducing crashes, are not clearly defined. It is difficult for older adults to
determine which modifications in their driving behaviours can translate into
improved safety. Individuals in this class may not respond well to feedback and
could benefit from passive interventions (e.g. in-vehicle technology, improvements
in road infrastructure).
Research Question 4
Study 3: Can providing older adults with customised and evaluative feedback assist
in stage transition and modify their willingness to change their driving behaviour?

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 181
To answer this question, a study was conducted where participants were
provided with customised one-on-one feedback in regards to their driving skills and
driving abilities. The feedback was provided by a driving instructor; which was
identified in focus group as a trustworthy and useful form of feedback.
Unfortunately, even though the recruitment lasted for around 9 months, only 22
participants were included in the final study. Therefore, the results should be
interpreted with caution and can’t be generalised to the population. All participants
viewed the feedback to be useful in helping older adults improve their driving
abilities. Around 67% of participants indicated that they would recommend this
form of feedback to their friends. Of the 13 participants who indicated they were not
aware of any limitations in their driving; 6 indicated that the feedback has made them
more aware of certain limitations (e.g. hesitation and judgement issues). However,
18 participants indicated that they will not seek help (e.g. driving refresher course or
doctor’s consultation). No significant changes were found before and after the
feedback in participants’ self-rated quality of driving. Prior to the drive, only 4
(19%) participants indicated that they are planning to or modified their driving
behaviours. After the drive, the number of those who were willing to change their
driving behaviour has significantly increased to 14 (66.7%).
Refining the initial model
Examining the self-regulatory driving behaviour within a health behaviour
framework is challenging. To start with, health behaviour theories deal with
behaviours considered “harmful” to the individual (e.g. smoking, lack of physical
activities). As noted by Kostyniuk et al. (2000) driving is not a harmful behaviour, it
is only when certain abilities are compromised that the risk of crash might increase.
Further, crashes are rare events and modifying one’s driving behaviour can be
limiting and inconvenient. Therefore, older adults may not perceive self-regulation
as a priority and could even perceive it as a negative behaviour. It is also important
to note that unlike other behaviours, there are no tangible or immediate benefits to
adopting self-regulation (other than perceived reduced risk of crash and perceived
increased comfort). The longevity of the process may cause older drivers to become
discouraged and relapse back to their old driving behaviours. Second, modifying
one’s driving can have implications on other people such as family members. Older
drivers may be reluctant to modify their driving behaviours because of having family

182 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
members who rely on their driving or because they want to avoid being a burden on
other family members. In other risky behaviours investigated previously within
behaviour change theories, minimising or stopping the behaviours can have no or
positive impact on other people.
The PAPM is a preventative decision-making framework constructed around
the goal of preventing or minimising future harm, ideal when dealing with complex
behaviours, which fits perfectly with driving self-regulation. First, it starts with
one’s awareness of risk and the need to adopt the precautionary behaviour. As
discussed in previous chapters, self-awareness is key to adopting self-regulation. In
fact, modification in driving behaviours for reasons others than increased insight into
limitations of driving abilities should not be regarded as self-regulation. Second, it
differentiates between those who are unaware and those who are resistant to change.
This is particularly useful because having different interventions for each stage is
rather useful. Third, the stages account for the qualitative differences in behaviours
and motivators among older drivers.
Overall, this research program suggests that the driving self-regulation of
older adults can be conceptualised within the PAPM. However, some modifications
to the PAPM framework are needed given the unique nature of driving. The refined
model consists of self-regulatory profiles of older drivers identified from the LCA
which represents certain stages of the PAPM.
As discussed before, stage 1 of the PAPM in the preliminary model was
omitted because it is most likely that older drivers are generally aware of the impact
of ageing on driving abilities. In addition, actual capacity to drive safely adapted
from Anstey et al. (2005) (with its cognitive, physical and vision aspects) has been
included but separated from the stages. The first stage in the model represents the
“unaware driver” which is comprised of individuals who lack personal engagement
about the impact of ageing on their driving abilities. This lack of insight is due to
lack of feedback or experience with the hazard (e.g. being involved in a crash). This
study found no significant association between crash involvement and PAPM stages.
However, only few participants were involved in a crash which made it difficult to
test for any significant association. Future studies should investigate the impact of
being involved in a crash and crash characteristic (e.g. severity, recency, outcome,
and being at fault) on self-awareness. This is a stage prior to the decision-making

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 183
process where older drivers have not thought about the future of their driving. As
suggested from the qualitative findings, older adults’ attitudes and perceptions
towards driving self-regulation are the result of the information within their family
and community. At this stage, individuals benefit most from interventions that can
increase their self-awareness and encourage them to think about precautionary
behaviours (i.e. driving self-regulation) to overcome any driving limitations.
Feedback at this stage should be provided from a trustworthy person, be evidence-
based, and allow the driver to accurately assess their driving ability. As previous
studies suggest, family members and healthcare professionals often initiate such
discussion with the older driver.
Once engaged, the decision-making process starts and individuals start to estimate
their risk of crashing and their risk of being injured. In addition, individuals weigh
the pros and cons of modifying their driving behaviour. This stage, the undecided, is
critical because individuals start to acquire and manage new information, assess their
surrounding environments and resources, and evaluate the immediate and long-term
outcome of their decision. It is very important at this stage to provide individuals
with objective and evaluative feedback of their driving abilities. Equally important is
recommendations on how to overcome barriers associated with adopting self-
regulation (e.g. lack of transport options, relying on family members). Some older
drivers perceive their risk of crash to be minimal and view self-regulation to be
unnecessary or inconvenient. The “resister” is very difficult to change since he/she
has already formed an opinion about the precaution. Individuals in this stage will
benefit from reinforcing the message and persuasion. They could also benefit from
passive interventions (e.g. in-vehicle technology or improvements in road structure).
The “planner” on the other hand represents those who have decided to modify their
driving behaviour. In this stage individuals start to monitor their behaviour and
assess their need to change. This can be difficult within the driving context for
several reasons. First, it may be difficult for older drivers to draw the link between
the decline in certain driving ability and impairment in their performance. Second, it
may be difficult to determine which modifications are needed to overcome such
limitation and improve their safety. Third, there is a possibility that some drivers
may become more anxious and their discomfort may cause unnecessary restrictions.
It is therefore crucial at this stage that participants receive accurate, objective,

184 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
evaluative, and exhaustive feedback. It is also important to reinforce the
recommendations on overcoming barriers toward adopting self-regulation.
The final stage is the regulator driver. In this stage, individuals are constantly
monitoring and regulating their driving according to their driving abilities. In line
with Molnar et al. (2013), self-regulation should be divided into strategic, tactical
and life-goal. These terms have described previously in chapter two. To encourage
life-goal changes, individuals can benefit from interventions aimed at planning
driving retirement, use of alternative transport options, and modifying their living
arrangements. To encourage strategic self-regulation, individuals could benefit from
education interventions, similar to KEYS that encourage older drivers to reduce
and/or restrict their driving according to their driving abilities. Finally, tactical self-
regulation could be achieved through driving retraining programs on-road or in the
simulator to enhance the driver skills and performance.
Figure 9.1: Refined model of self-regulatory driving behaviour
9.3 CONTRIBUTIONS TO RESEARCH
This research program contributes to the theoretical understanding of older
drivers’ self-regulation through the application of the PAPM and the development of
a conceptual model that categorises older adults into different stages of behaviour
change while capturing a wide range of interpersonal, intrapersonal, and
environmental factors that influence self-regulatory driving behaviour among the

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 185
older drivers. A theory-based understanding of older drivers’ self-regulatory
behaviours and how to influence them can assist in the development of effective
interventions. To my knowledge, this is the first study to develop a comprehensive
model of older drivers’ regulatory behaviour using the stages of change theories.
The model includes a large number of interpersonal, intrapersonal, and
environmental factors associated with driving self-regulation and identified
previously in the literature. Still, the model is very flexible and can be customised in
different contexts based on the study population (e.g. women, rural drivers or
professional older drivers), the self-regulatory practice (e.g. tactical, strategic or life-
goal) and the desired interventions (e.g. In-vehicle technologies, educational
interventions or health professional interventions). The model can also be applied to
a large number of “precautionary behaviours” adopted by the older population. The
findings from the LCA have provided empirical support to the use of the model
through the identification of classes of older drivers that match to a degree those in
the conceptual model.
This program of research adds to our understanding of the impact of feedback
on older adults’ self-regulatory driving behaviour. The findings from the qualitative
study indicate that some older adults seek feedback in regards to their driving
abilities. The problems often encountered are the lack of trusted and evidence-based
source of such feedback. The study identified numerous sources that can provide
older adults with different form of feedback about ageing and driving. It is important
to emphasise that the content and source of feedback will vary greatly based on
individual’s stage in the conceptual model. For instance, participants identified the
lack of readily-available printed materials that contains facts and statistics about the
older driver. These materials can be made readily available in physicians’ offices or
seniors club with the aim of enhancing older adults’ knowledge about the problems
encountered with ageing on their driving abilities.
Finally, this program of research investigated the impact of life-goal decisions
on older adults’ self-regulatory driving behaviour, an area that deserves further
exploration. The qualitative findings indicated that those who were living in seniors’
villages or in areas with better public transport options had thought about the future
of their driving. The quantitative findings indicated that 25.2% of participants had
moved to a new place closer to their common destinations, 22.1% had moved to a

186 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
place with better public transport options, and 14.9% had moved to a seniors’ home.
While not significantly different among PAPM groups, moving to a seniors’ home
was significantly associated with driving reduction with 87.9% of those living in
seniors’ homes indicating that they have reduced their driving compared to 68.3% of
those who are still living at home.
9.4 PRACTICAL IMPLICATIONS OF THE RESEARCH PROGRAM
Findings from this research program have implications for the management of
the older drivers’ safety issues. The conceptual model can act as a framework for
further investigating the older adults’ driving behaviours. It can also assist in
designing interventions that encourage older drivers to self-monitor and
appropriately self-regulate their driving while taking into accounts the needs and
expectations of the older driver and assist them in making informed decisions about
the future of their driving. Previous studies have shown that involving older drivers
in the decision making provides them with sense of control which can ease the
transition to the non-driving state in the future. The practical implications of this
study correspond to the stages proposed by the conceptual model. Interventions will
vary in their source, content, and timing based on each stage. Interventions would
only work if they are customised based on individual’s baseline and the anticipated
outcome. Older drivers are generally aware of the impact of ageing on one’s driving
ability. Still, older drivers are overall safe drivers, despite being portrayed in the
media as a heightened crash risk. This stereotyping, could be adding to the
sensitivity of the topic and the difficulty of initiating discussion with older drivers.
The media need to stop stereotyping the older driver as timid and dangerous.
Accurate information about older drivers’ crash statistics and impact of ageing on
driving abilities should be made readily available and accessible to the public. For
stage 2, the unengaged, it is important to increase self-awareness of the impact of
age-related declines on older adults’ driving. Previous literature suggest that older
drivers are generally aware of the impact of ageing on driving. However, due to the
complexity of the driving behaviour and the subtle nature of the declines associated
with ageing, older drivers may find it difficult to draw the link between the two. It is
therefore important to design interventions that can enhance older drivers’ self-
awareness. As noted in study 1 and study 2, the majority of participants did not feel
the need to modify their driving, which could reflect lack of insight. Findings from

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 187
qualitative focus groups indicated that participants are open to receiving feedback
about their driving, provided that it comes from a person they trust. Older drivers
would benefit from one-to-one discussions with their healthcare professionals who
can accurately assess if they have a medical or non-pathological condition that
impact their driving. Future studies should address the barriers associated with
providing feedback to older drivers in healthcare setting (e.g. compromising patient-
doctor relationship, lack of training to medical professionals, and sensitivity of the
topic). In addition, interventions should also incorporate the family and carers of
older drivers who can play a role in enhancing their awareness but may lack the
understanding and knowledge of how to do that. For stage 3, individuals would
benefit from interventions that accurately reflect their risk of crash and encourage
seeking feedback accordingly. Assessment of driving in a friendly environment can
provide older drivers with objective measure of their driving skill and performance.
This study suggests that driving instructors could play an important role. Future
work should develop a battery of test that can assess older drivers’ skills with high
reliability and sensitivity. Some individuals however may choose to make their
own assessment and refuse the feedback. Older drivers who were made of aware of
limitations in their driving but refuse to change will progress to stage 4. Individuals
in this stage are the most difficult to tackle because they have made their opinions
and will not be respond well to conventional interventions. They can benefit best
from passive interventions. Others who believe they are at risk of crash will move to
stage 5 where they will start to actively observe their driving and seek further
feedback. In this stage, individuals can benefit from more detailed information of
how to adopt the change and how to overcome the barriers towards such change.
This research identified a large number of barriers towards change that should be
addressed in designing older drivers’ interventions. Lack of alternative transports is
a common barrier which could even be a greater issue for rural older drivers. In
addition, interventions that can assist older drivers plan their driving retirement may
be beneficial. To improve mobility and road safety for older drivers, interventions
must consider modifiable (i.e., different than age or gender) facilitators and barriers
to the use of adaptive strategies, as well as the needs of older drivers. These
interventions must be personalised, proactive and planned on a continuum to
promote safe and responsible driving according to the abilities of older drivers, but
also considering their personal and environmental factors, as well as their social

188 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
participation. In fact, many personal factors such as openness, perceptions,
knowledge and abilities must be considered, but also environmental factors such as
support, cost and the proximity of resources
9.5 STUDY STRENGTHS AND LIMITATIONS
The strengths and limitations of this research program have been presented
in previous chapters. Overall, it has a number of strengths. This study was unique in
its attempt to utilise a bottom-up approach; through Latent Class Analysis, in
identifying self-regulatory driving behaviour profiles among older adults based on
their mindset towards changing their driving behaviour. In addition, the study used a
robust theoretical model, PAPM. The present study utilised an exploratory
sequential mixed method design which resulted in enhancing our understanding of
the self-regulatory process among older drivers. Another methodological strength is
the inclusion of large number of interpersonal, intrapersonal, and environmental
factors associated with the process of self-regulation.
The study had several limitations. Overall, recruitment has proven difficult
for the three studies despite utilising various recruitment strategies. This can be due
to transportation difficulties, health problems common at this age group, sensitivity
of the topic, lack of interest, or not understanding the potential benefits of the
research. For the qualitative study, it was extremely difficult to recruit former
drivers and the study failed to capture the experiences of driving-regulation and
driving cessation among this group. For the quantitative study and the pre-post
study, the sample was relatively small in number which limited the power for some
of the group analyses and may have increased the risk of Type II error. This in turn
may affect the generalisability of the results to the broader population.
Second, the sampling method may have introduced some biases. The study
relied on convenience sample and therefore may have attracted participants who are
more safety-oriented; more motivated to continue driving, and have higher awareness
of their driving abilities. In addition, the findings are based on a small sample of
Brisbane and Sunshine Coast drivers and the extent to which the results can be
generalised to other Australian states is unclear.
Third, the study relied on self-report and participants were required to think
back retrospectively and report on their reasons and patterns of driving restriction.

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 189
This self-report may have been biased or subject to forgetting. The self-rating
questionnaires used did not measure response bias and therefore it is uncertain if
participants answered the questions in a forthright manner. In addition, participants
may have scored themselves higher than average introducing social desirability bias.
In this study, standard scales were used to measure the psychosocial variables.
While their use is common, it is possible that they do not capture the variables
related to the older drivers.
Fourth, this study did not assess the cognitive skills of the participants and
findings may be different for cognitively impaired drivers.
In addition, the staging algorithm used in this study was similar to the one
recommended by Weinstein et al. (2008). There is limited research that examines
the validity and reliability of such staging algorithm despite being used before in the
transport literature (Coxon et al., 2015). This may have resulted in participants being
misclassified into the wrong stages. Future studies should attempt to overcome this
limitation by employing reliable and valid tools for classification.
The study was cross-sectional in nature and therefore causality cannot be
established.
9.6 FUTURE DIRECTIONS
This exploratory research program provided reasonable support for the use of
PAPM as a framework in investigating driving regulation and/or cessation among
older adults. Future research should attempt to employ a larger prospective design
that initially stage older drivers in the PAPM and follow them through their driving
regulation and cessation process. This will assist in the identification of the factors
and the critical events that help stage progression. The process of self-regulation is
highly complex and it is important to expand the way we define and measure self-
regulation to include any behaviours that the driver embark upon to enhance their
safety. Majority of previous studies have focused on driving restriction and
avoidance of challenging situation. There is also paucity of research regarding
tactical self-regulation among older drivers.

190 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
While there is an increased shift towards using objective measures of driving
abilities; more attention is still needed in developing reliable and valid measures of
older drivers’ perception. As discussed before, older adults’ perception of their
driving ability rather than their actual driving is what motivate them to change. A
major drawback of previous studies is that there is inconsistency in the way older
drivers’ perceptions are measured and defined. Further, the majority of these
measures have no information about their reliability and validity.
While this research program attempted to examine the impact of feedback on
older drivers’ intention to change; the small sample size made it difficult to reach a
significant result. Future research should attempt to examine the impact of
customised feedback on moving older drivers through stages of change using a large
sample size and control groups.
In future research, it is useful to conceptualise self-regulation using stages of
change theories. This will accommodate for the heterogeneity of the older drivers’
population in terms of their mindset towards change (e.g. perceptions and self-
efficacy) and barriers towards adopting the change (e.g. presence of alternative
transport options and household composition). By knowing the stage of change
where the individual is at, interventions could be customised to move them towards
the desired outcome. The barriers identified in the qualitative study serve as
appropriate targets for future interventions. On the other hand, older drivers’
willingness to seek feedback and to rely on in-vehicle technology could be seen as
avenues to promote safe mobility. Future research should also be directed towards
the use of in-vehicle technology and their role in maintaining older drivers’ mobility
by overcoming limitations in their driving abilities.
9.7 CONCLUDING REMARKS
This program of research has enhanced our understanding of the process of
self-regulation among older drivers. First, this research program presented a
comprehensive theoretically-based model of older adults’ driving self-regulation.
The model was based on the PAPM which identifies various stages of change that
start by unawareness to modifying one driving. The model included a large number
of interpersonal, intrapersonal and environmental factors that influence stage
transition. It can assist in designing, implementing, and evaluating interventions that

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 191
can assist older adults regulate their driving successfully. Second, a novel approach
using LCA has identified three class of self-regulatory driving behaviours similar to
those identified by the model providing further empirical support to the model.
192 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Bibliography
Ackerman, M. L., Crowe, M., Vance, D. E., Wadley, V. G., Owsley, C., & Ball, K. K. (2011). The impact of feedback on self-rated driving ability and driving self-regulation among older adults. Gerontologist, 51(3), 367-378. doi: 10.1093/geront/gnq082
Ackerman, M. L., Edwards, J. D., Ross, L. A., Ball, K. K., & Lunsman, M. (2008). Examination of cognitive and instrumental functional performance as indicators for driving cessation risk across 3 years. The Gerontologist, 48(6), 802-810.
Adler, G., & Rottunda, S. (2006). Older adults' perspectives on driving cessation. Journal of Aging Studies, 20(3), 227-235. doi: http://dx.doi.org/10.1016/j.jaging.2005.09.003
Allan, D. E., & McGee, P. (2003). Accessible transportation for all in the capital regional district: where are we now, where should we be going? Final report for BC Transit, Capital Region District and Vancouver Island Health Authority
Alsnih, R., & Hensher, D. A. (2003). The mobility and accessability expectations of seniors in an ageing population. Transportation Research Part A: Policy and Practice, 37, 903-916.
Anstey, K. J., & Smith, G. A. (2003). Associations of biomarkers, cognition and self-reports of sensory function with self-reported driving behaviour and confidence. Gerontology, 49(3), 196-202.
Anstey, K. J., Windsor, T. D., Luszcz, M. A., & Andrews, G. R. (2006). Predicting driving cessation over 5 years in older adults: psychological wellbeing and cognitive competence are stronger predictors than physical health. Journal of American Geriatric Society, 54(1), 121-126. doi: 10.1111/j.1532-5415.2005.00471.x
Anstey, K. J., Wood, J., Lord, S., & Walker, J. G. (2005). Cognitive, sensory and physical factors enabling driving safety in older adults. Clinical Psychology Review, 25(1), 45-65. doi: 10.1016/j.cpr.2004.07.008
Atkin, C. (2001). Impact of public service advertising: Research evidence and effective strategies. Kaiser Family Foundation, Menlo Park, CA.
Australian Bureau of Staistics. (2008). Population Projections, Australia, 2006 to 2101. Canberra, Australia. Retrieved from http://www.abs.gov.au/AUSSTATS/[email protected]/DetailsPage/3222.02006%20to%202101
Australian Bureau of Staistics. (2011). Census of Population and Housing 2011. Canberra, Australia. Retrieved from http://www.abs.gov.au/websitedbs/censushome.nsf/home/2011information?opendocument&navpos=310
Australian Bureau of Staistics. (2015). Australian Demographic Statistics, Jun 2015. Canberra, Australia. Retrived from http://www.abs.gov.au/ausstats/[email protected]/mf/3101.0
Baldock, M. R. J., Mathias, J. L., McLean, J., & Berndt, A. (2006a). Self-regulation of driving and older drivers' functional abilities. Clinical Gerontologist, 30(1), 53-70. doi: 10.1300/J018v30n01_05

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 193
Ball, K. K., Owsley, C., Stalvey, B., Roenker, D. L., Sloane, M. E., & Graves, M. (1998). Driving avoidance and functional impairment in older drivers. Accident Analysis & Prevention, 30(3), 313-322. doi: http://dx.doi.org/10.1016/S0001-4575(97)00102-4
Ball, K. K., Roenker, D. L., Wadley, V. G., Edwards, J. D., Roth, D. L., McGwin Jr, G., et al. (2006). Can high-risk older drivers be identified through performance-based measurements in a Department of Motor Vehicles setting. Journal of American Geriatric Society, 54(1), 77-84.
Bauer, M., Kuskowski, M., Rottunda, S., & Adler, G. (2003). The influence of age and gender on the driving patterns of older adults. Journal of women & aging, 15(4), 3-16. doi: 10.1300/J074v15n04_02
Bauer, M., Rottunda, S., & Adler, G. (2003). Older women and driving cessation. Qualitative Social Work, 2(3), 309-325. doi: 10.1177/14733250030023006
Bédard, M., Guyatt, G. H., Stones, M. J., & Hirdes, J. P. (2001). The independent contribution of driver, crash, and vehicle characteristics to driver fatalities. Accident Analysis & Prevention, 34(6), 717-727. doi: http://dx.doi.org/10.1016/S0001-4575(01)00072-0
Bergen, G., West, B. A., Luo, F., Bird, D. C., Freund, K., Fortinsky, R. H., & Staplin, L. (2017). How do older adult drivers self-regulate? Characteristics of self-regulation classes defined by latent class analysis. Journal of Safety Research, 61, 205-210. doi: http://dx.doi.org/10.1016/j.jsr.2017.01.002
Berry, C. (2011). Can older drivers be nudged? How the public and private sectors can influence older drivers’ self-regulation. RAC Foundation, London
Betz, M., Jones, J., Petroff, E., & Schwartz, R. (2013). “I wish we could normalize driving health": a qualitative study of clinician discussions with older drivers. Journal of General Internal Medicine, 28(12), 1573-1580. doi: 10.1007/s11606-013-2498-x
Betz, M., Kanani, H., Juarez-Colunga, E., & Schawrtz, R. (2016). Discussions about driving between older adults and primary care providers. Journal of American Geriatric Society, 64(4), 1318-1323.
Blanchard, R. A., & Myers, A. M. (2010). Examination of driving comfort and self-regulatory practices in older adults using in-vehicle devices to assess natural driving patterns. Accident Analaysis and Prevention, 42(4), 1213-1219. doi: 10.1016/j.aap.2010.01.013
Bogner, H. R., Straton, J. B., Gallo, J. J., Rebok, G. W., & Keyl, P. M. (2004). The role of physicians in assessing older drivers: barriers, opportunities, and strategies. The Journal of the American Board of Family Practice, 17(1), 38-43. doi: 10.3122/jabfm.17.1.38
Bonnel, W. B. (1999). Giving up the car: Older women's lossses and experiences. Journal of Psychosocial Nursing & Mental Health Services, 37(5), 10-15.
Boufous, S., Finch, C., Hayen, A., & Williamson, A. (2008). The impact of environmental, vehicle and driver characteristics on injury severity in older drivers hospitalized as a result of a traffic crash. Journal of Safety Research, 39(1), 65-72. doi: http://dx.doi.org/10.1016/j.jsr.2007.10.010
Braitman, K. A., & McCartt, A. T. (2008). Characteristics of older drivers who self-limit their driving. Annals of Advances in Automotive Medicine, 52, 245-254.
Braitman, K. A., & Williams, A. F. (2011). Changes in self-regulatory driving among older drivers over time. Traffic Injury Prevention, 12(6), 568-575. doi: 10.1080/15389588.2011.616249

194 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Braun, V., & Clarke, V. (2013). Successful Qualitative Research: A practical guide for beginners. London: Sage.
Brooke, B. T., & Southward, R. D. (2006). An audit of advice on fitness to drive during accident and emergency department attendance. Emergency Medicine Journal, 23(2), 103-104. doi: 10.1136/emj.2004.020776
Bureau of Infrastructure, Transport and Regional Economics. (2014). Road safety of older Australians. Canberra, Australian Government
Burkhardt, J. E., McGavock, A. T., & Nelson, C. A. (2002). Improving public transit options for older persons. Washington DC.
Burson, K. A., Larrick, R. P., & Klayman, J. (2006). Skilled or unskilled, but still unaware of it: how perceptions of difficulty drive miscalibration in relative comparisons. Journal of Personality and Social Psychology, 90(1), 60-77. doi: 10.1037/0022-3514.90.1.60
Buys, L., Snow, S., van Megen, K., & Miller, E. (2012). Transportation behaviours of older adults: An investigation into car dependency in urban Australia. Australasian Journal on Ageing, 31(3), 181-186. doi: http://dx.doi.org/10.1111/j.1741-6612.2011.00567.x
Caragata, GE. (2017). Model development and exploration into the driving decisions of older adults. Avaliable from file:///C:/Users/heidi/Downloads/etd9976_GCaragata%20(1).pdf
Carr DB, Schwartzberg JG, Manning L, & J., S. Physician’s guide to assessing and counseling older driver 2nd editions. (2010). U.S. Department of Transportation, National Highway Traffic Safety Administration, Washington.
Celeux, G., & Soromenho, G. (1996). An entropy criterion for assessing the number of clusters in a mixture model. Journal of Classification, 13(2), 195-212. doi: 10.1007/bf01246098
Charlton, J., Oxley, J., Fildes, B., & Les, M. (2001). Self-regulatory behaviour of older drivers. Paper presented at the 2001 Road Safety, Research, Policing and Education Conference, Melbourne, Australia.
Charlton, J., Oxley, J., Fildes, B., Oxley, P., Newstead, S., Koppel, S., & O’Hare, M. (2006). Characteristics of older drivers who adopt self-regulatory driving behaviours. Transportation Research Part F: Traffic Psychology and Behaviour, 9(5), 363-373. doi: http://dx.doi.org/10.1016/j.trf.2006.06.006
Cheung, I., & McCartt, A. T. (2011). Declines in fatal crashes of older drivers: changes in crash risk and survivability. Accident Analysis & Prevention, 43(3), 666-674. doi: 10.1016/j.aap.2010.10.010
Choi, M., Adams, K. B., & Mezuk, B. (2012). Examining the aging process through the stress-coping framework: application to driving cessation in later life. Aging Mental Health, 16(1), 75-83. doi: 10.1080/13607863.2011.583633
Choi, N. G., DiNitto, D. M., & Marti, C. N. (2015). Older adults who are at risk of driving under the influence: A latent class analysis. Psychology of Addictive Behaviors, 29(3), 725-732. doi: 10.1037/adb0000055
Classen, S., Lopez, E. D. S., Winter, S., Awadzi, K. D., Ferree, N., & Garvan, C. W. (2007). Population-based health promotion perspective for older driver safety: conceptual framework to intervention plan. Clinical Interventions in Aging, 2(4), 677-693.
Connell, C. M., Harmon, A., Janevic, M. R., & Kostyniuk, L. P. (2013). Older adults’ driving reduction and cessation: perspectives of adult children.

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 195
Journal of Applied Gerontology, 32(8), 975-996. doi: 10.1177/0733464812448962
Corpuz, G. (2007). Public transport or private vehicle: factors that impact on mode choice. Paper presented at the 30th Australasian Transport Research Forum.
Costanza, M. E., Luckmann, R., Stoddard, A. M., Avrunin, J. S., White, M. J., Stark, J. R., Rosal, M. C. (2005). Applying a stage model of behavior change to colon cancer screening. Preventive Medicine, 41(3–4), 707-719. doi: http://dx.doi.org/10.1016/j.ypmed.2004.12.013
Coughlin, J. (2001). Transportation and older persons: Perceptions and preferences. Washington DC: AARP Public Policy Institute.
Coughlin, J. (2005). Not your father’s auto industry? Aging, the automobile, and the drive for product innovation. Generations, 28(4), 38-44.
Coughlin, J., Mohyde, M., D'Ambrosio, L. A., & Gilbert, J. (2004). Who drives older driver decisions? MIT AgeLab.
Coxon, K., Chevalier, A., Brown, J., Clarke, E., Billot, L., Boufous, S., . . . Keay, L. (2017). Effects of a safe transportation educational program for older drivers on driving exposure and community participation: a randomized controlled trial. Journal of American Geriatric Society, 65(3), 540-549. doi: 10.1111/jgs.14550
Coxon, K., Chevalier, A., Lo, S., Ivers, R., Brown, J., & Keay, L. (2015). Behind the wheel: predictors of driving exposure in older drivers. Journal of American Geriatric Society, 63(6), 1137-1145. doi: 10.1111/jgs.13440
Coxon, K., & Keay, L. (2015). Behind the wheel: community consultation informs adaptation of safe-transport program for older drivers. BMC Research Notes, 8(1), 764. doi: 10.1186/s13104-015-1745-0
Creswell, J. W., & Plano, C. V. L. (2011). Creswell, J. W., & Plano, C. V. L. (2011). Designing and conducting mixed methods research. . Los Angeles: SAGE Publications.
Crosby, R., & Noar, S. M. (2011). What is a planning model? An introduction to PRECEDE‐PROCEED. Journal of Public Health Dentistry, 71, S7-S15. doi: 10.1111/j.1752-7325.2011.00235.x
Currie, G., & Delbosc, A. (2010). Exploring public transport usage trends in an ageing population. . Transportation, 37, 151–164.
D'Ambrosio, L., Coughlin, J., Donorfio, L., Mohyde, M., & Meyer, J. (2008). Gender Differences in self-regulation patterns and attitudes toward driving among older adults. Journal of Women & Aging, 20(3), 265-282. doi: 10.1080/08952840801984758
De Oña, J., López, G., Mujalli, R., & Calvo, F. J. (2013). Analysis of traffic accidents on rural highways using Latent Class Clustering and Bayesian Networks. Accident Analysis and Prevention, 51, 1-10. doi: 10.1016/j.aap.2012.10.016
De Raedt, R., & Ponjaert-Kristoffersen, I. (2000a). Can strategic and tactical compensation reduce crash risk in older drivers? Age and Ageing, 29(6), 517-521. doi: 10.1093/ageing/29.6.517
De Raedt, R., & Ponjaert-Kristoffersen, I. (2000b). The relationship between cognitive/neuropsychological factors and car driving performance in older adults. Journal of American Geriatric Society, 48(12), 1664-1668.
de Vet, E., de Nooijer, J., Oenema, A., de Vries, N. K., & Brug, J. (2008). Predictors of stage transitions in the precaution adoption process model. American Journal of Health Promotion, 22(4), 282-290. doi: 10.4278/060829120R2.1

196 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Delara, M., Ghofranipour, F., Fallah, P. A., Tavafian, S. S., Kazemnejad, A., Montazeri, A., . . . Kooshki, M. (2012). Coping strategy in adolescents with premenstrual syndrome: Application of the Construal Level Theory and the Precaution Adoption Process Model. Psychology, Health & Medicine, 18(2), 203-212. doi: 10.1080/13548506.2012.701752
Dellinger, A. M., Sehgal, M., Sleet, D. A., & Barrett-Connor, E. (2001). Driving cessation: what older former drivers tell us. Journal of American Geriatric Society, 49(4), 431-435.
Department of Transport and Main Roads. (2015). Current Queensland Driver Licences, June, 2015. Obtained from http://www.tmr.qld.gov.au/safety/transport-and-road-statistics/licensing-statistics.aspx
Di Stefano, M. & Lovell, R.K. (2006). Using a participatory research method to develop a handbook for driving instructors to assist with teaching older drivers. Australian Occupational Therapy Journal 53, 132-135
Dickerson, A. E., Meuel, D. B., Ridenour, C. D., & Cooper, K. (2014). Assessment tools predicting fitness to drive in older adults: a systematic review. American Journal of Occupational Therapist 68(6), 670-680. doi: 10.5014/ajot.2014.011833
Dickerson, A. E., Molnar, L. J., Eby, D. W., Adler, G., Bedard, M., Berg-Weger, M., . . . Trujillo, L. (2007). Transportation and aging: A research agenda for advancing safe mobility. The Gerontologist, 47(5), 578-590. doi: 10.1093/geront/47.5.578
Ditto, P. H., & Lopez, D. F. (1992). Motivated Skepticism: use of differential decision criteria for preferred and nonpreferred conclusions. Journal of Personality and Social Psychology, 63(4), 568-584. doi: 10.1037//0022-3514.63.4.568
Dobbs, A. R., Heller, R. B., & Schopflocher, D. (1998). A comparative approach to identify unsafe older drivers. Accident Analysis & Prevention, 30(3), 363-370. doi: http://dx.doi.org/10.1016/S0001-4575(97)00110-3
Dobbs, B. M. (2008). Aging baby boomers—a blessing or challenge for driver licensing authorities. Traffic Injury Prevention, 9(4), 379-386. doi: 10.1080/15389580802045823
Dogan, E., Steg, L., Delhomme, P., & Rothengatter, T. (2012). The effects of non-evaluative feedback on drivers' self-evaluation and performance. Accident Analysis and Prevention, 45, 522-528. doi: 10.1016/j.aap.2011.09.004
Donmez, B., Boyle, L. N., & Lee, J. D. (2007). Safety implications of providing real-time feedback to distracted drivers. Accident Analysis & Prevention, 39(3), 581-590. doi: http://dx.doi.org/10.1016/j.aap.2006.10.003
Donorfio, L. K., D'Ambrosio, L. A., Coughlin, J. F., & Mohyde, M. (2009). To drive or not to drive, that isn't the question-the meaning of self-regulation among older drivers. Journal of Safety Research, 40(3), 221-226. doi: 10.1016/j.jsr.2009.04.002
Dunn, V. (2011). Evaluating the effectiveness of Devon County Council’s “Driving Safer For Longer” schemes. Plymouth: University of Plymouth. Retrieved online from http://www.devon.gov.uk/evaluationdrivingsaferforlonger.pdf.
Eberhard, J. (1996). Safe mobility of senior citizens. Journal of International Association of Traffic and Safety Science, 20(1), 29-37.
Eby, D. W., Molnar, L., Liang, Z., St. Louis, R. M., Zanier, N., & Lidia, P. (2015). Keeping Older Adults Driving Safely: A Research Synthesis of Advanced In-

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 197
Vehicle Technologies. AAA Foundation for Traffic Safety, Washington, DC. Retrieved from: https://www.aaafoundation.org/sites/default/files/SeniorsAndTechnologyReport.pdf.
Eby, D. W., Molnar, L. J., Shope, J. T., Vivoda, J. M., & Fordyce, T. A. (2003). Improving older driver knowledge and self-awareness through self-assessment: the driving decisions workbook. Journal of Safety Research, 34(4), 371-381.
Eby, D. W., Trombley, D., Molnar, L. J., & Shope, J. T. (1998). The assessment of older driver capabilities: a review of the literature. UMTRI-98-24.
Edwards, J. D., Perkins, M., Ross, L. A., & Reynolds, S. L. (2009). Driving status and three-year mortality among community-dwelling older adults. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences, 64A(2), 300-305. doi: 10.1093/gerona/gln019
Eisenhandler, S. A. (1990). The asphalt identikit: old age and the driver's license. Internation Journal of Aging and Human Development, 30(1), 1-14.
Elliott, J. O., Seals, B. F., & Jacobson, M. P. (2007). Use of the Precaution Adoption Process Model to examine predictors of osteoprotective behavior in epilepsy. Seizure, 16(5), 424-437. doi: http://dx.doi.org/10.1016/j.seizure.2007.02.016
Elliott, M. R., Jacobsohn, L., Winston, F. K., & Ginsburg, K. R. (2012). Determining subgroups of teens for targeted driving injury prevention strategies: a latent class analysis approach. Traffic Injury Prevention, 13(3), 258-264. doi: 10.1080/15389588.2011.648289
Evans, L. (1991). Traffic Safety and the Driver. New York: Van Nostrand Reinhold. Retrieved from https://books.google.com.au/books?hl=en&lr=&id=OyuGJJ6rKQ0C&oi=fnd&pg=PR13&ots=ztdceeokCG&sig=aLsea-e_4IwVO-Aq9SktTaQeA3M&redir_esc=y#v=onepage&q&f=false
Fiksenbaum, L. M., Greenglass, E. R., & Eaton, J. (2006). Perceived social support, hassles, and coping among the elderly. Journal of Applied Gerontology, 25(1), 17-30. doi: 10.1177/0733464805281908
Fonda, S. J., Wallace, R. B., & Herzog, A. R. (2001). Changes in driving patterns and worsening depressive symptoms among older adults. Journal of Gerontological B psychology, 56(6), S343-351.
Freeman, E. E., Gange, S. J., Munoz, B., & West, S. K. (2006). Driving status and risk of entry into long-term care in older adults. American Journal of Public Health, 96(7), 1254-1259. doi: 10.2105/ajph.2005.069146
Freund, B., Colgrove, L. A., Burke, B. L., & McLeod, R. (2005). Self-rated driving performance among elderly drivers referred for driving evaluation. Accident Analysis & Prevention, 37(4), 613-618. doi: http://dx.doi.org/10.1016/j.aap.2005.03.002
Gardezi, F., Wilson, K. G., Man-Son-Hing, M., Marshall, S. C., Molnar, F. J., Dobbs, B. M., & Tuokko, H. A. (2006). Qualitative research on older drivers. Clinical Gerontologist, 30(1), 5-22. doi: 10.1300/J018v30n01_02
Garver, M.S, Williams, Z., Taylor, G.S. (2008). Employing latnet class regression analysis to examine logistics theory: An application of truck driver retention. Journal of Buisness Logistics, 29(2), 233-IX.
Geiser, C. (2013). Data analysis with Mplus (Vol. 1). New York: The Guilford Press. Gilhooly, M., Hamilton, K., O’Neill, M., & al., e. (2003). Transport and ageing:
extending quality of life via public and private transport. Swindon, Wiltshire:

198 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
ESRC Research Findings from the Growing Older Programme 16, Economic and Social Research Council.
Gillins, L. (1990). Yielding to age: when the elderly can no longer drive. Journal of Gerontological Nursing, 16(11), 12-15.
Gish, J., Vrkljan, B., Grenier, A., & Van Miltenburg, B. (2016). Driving with advanced vehicle technology: A qualitative investigation of older drivers’ perceptions and motivations for use. Accident Analysis & Prevention. doi: http://dx.doi.org/10.1016/j.aap.2016.06.027
Glanz, K., Rimer, B. K., & Viswanath, K. (2008). Health behavior and health education: theory, research, and practice. San Francisco: Jossey-Bass.
Glik, D. C., Eisenman, D. P., Zhou, Q., Tseng, C.-H., & Asch, S. M. (2014). Using the Precaution Adoption Process model to describe a disaster preparedness intervention among low-income Latinos. Health Education Research, 29(2), 272-283. doi: 10.1093/her/cyt109
Guest, M., Boggess, M. M., Viljoen, D. A., Duke, J. M., & Culvern, C. N. (2014). Age-related injury and compensation claim rates in heavy industry. Occupational Medicine, 64(2), 95-103. doi: 10.1093/occmed/kqt166
Guo, A. W., Brennan, D., Edwards, S. J. F., & Blythe, P. T. (2012). Driving on: Using in vehicle systems to help older people stay on the road. Paper presented at the 19th ITS World Congress, Vienna, Austria.
Gwyther, H., & Holland, C. (2014). Feelings of vulnerability and effects on driving behaviour – A qualitative study. Transportation Research Part F: Traffic Psychology and Behaviour, 24, 50-59. doi: 10.1016/j.trf.2014.03.001
Hagenaars, J. A., & McCutcheon, A. L., (2002). Applied latent class analysis. Cambridge;New York; U6 - ctx_ver=Z39.88-2004&ctx_enc=info%3Aofi%2Fenc%3AUTF-8&rfr_id=info%3Asid%2Fsummon.serialssolutions.com&rft_val_fmt=info%3Aofi%2Ffmt%3Akev%3Amtx%3Abook&rft.genre=book&rft.title=Applied+latent+class+analysis&rft.au=Hagenaars%2C+Jacques+A&rft.au=McCutcheon%2C+Allan+L&rft.date=2002-01-01&rft.pub=Cambridge+University+Press&rft.externalDocID=b36848888¶mdict=en-US U7 - eBook: Cambridge University Press.
Hakamies-Blomqvist, L. (1994a). Mental workload and compensation in older drivers. In K. Johansson & C. Lundberg (Eds.), Aging and Driving (pp. 59–65). Stockholm: Karolinska Institute
Hakamies-Blomqvist, L., & Henriksson, P. (1999). Cohort effects in older drivers' accident type distribution: are older drivers as old as they used to be? Transportation Research Part F: Traffic Psychology and Behaviour, 2(3), 131-138. doi: http://dx.doi.org/10.1016/S1369-8478(99)00009-1
Hakamies-Blomqvist, L., & Peters, B. (2000). Recent European research on older drivers. Accident Analysis & Prevention, 32(4), 601-607. doi: http://dx.doi.org/10.1016/S0001-4575(99)00073-1
Hakamies-Blomqvist, L., Raitanen, T., & O’Neill, D. (2002). Driver ageing does not cause higher accident rates per km. Transportation Research Part F: Traffic Psychology and Behaviour, 5(4), 271-274. doi: http://dx.doi.org/10.1016/S1369-8478(03)00005-6
Hakamies-Blomqvist, L., & Wahlström, B. (1998). Why do older drivers give up driving? Accident Analysis & Prevention, 30(3), 305-312. doi: http://dx.doi.org/10.1016/S0001-4575(97)00106-1

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 199
Hamarat, E., Thompson, D., Steele, D., Matheny, K., & Simons, C. (2002). Age differences in coping resources and satisfaction with life among middle-aged, young-old, and oldest-old adults. The Journal of Genetic Psychology, 163(3), 360-367.
Hassan, H., King, M., & Watt, K. (2015). The perspectives of older drivers on the impact of feedback on their driving behaviours: A qualitative study. Transportation Research Part F: Traffic Psychology and Behaviour, 28, 25-39. doi: 10.1016/j.trf.2014.11.003
Hauer, E. (2006). The frequency-severity indeterminacy. Accident Analysis & Prevention, 38, 78-83.
Hesse-Biber, S. (2010). Qualitative Approaches to Mixed Methods Practice. Qualitative Inquiry, 16(6), 455-468. doi: 10.1177/1077800410364611
Holland, C. A., & Rabbitt, P. M. A. (1992). People's awareness of their age-related sensory and cognitive deficits and the implications for road safety. Applied Cognitive Psychology, 6(3), 217-231. doi: 10.1002/acp.2350060304
Horswill, M. S., Anstey, K. J., Hatherly, C., Wood, J. M., & Pachana, N. A. (2011). Older drivers’ insight into their hazard perception ability. Accident Analysis & Prevention, 43(6), 2121-2127. doi: http://dx.doi.org/10.1016/j.aap.2011.05.035
Hu, P. S., Jones, W. D., Reuscher, T., Schmoyer, R. S., Truett, L. F., & . (2000). Projecting fatalities in crashes involving older drivers, 2000–2025. Oak Ridge National laboratory, U.S. Department of Energy. (Report ORNL-6963).
Huebner, K. D., Porter, M. M., & Marshall, S. C. (2006). Validation of an electronic device for measuring driving exposure. Traffic Injury Prevention, 7(1), 76-80. doi: 10.1080/15389580500413067
Jang, R., Man-Son-Hing, M., Molnar, F., Hogan, D., Marshall, S., Auger, J., . . . Naglie, G. (2007). Family physicians’ attitudes and practices regarding assessments of medical fitness to drive in older persons. Journal of General Internal Medicine, 22(4), 531-543. doi: 10.1007/s11606-006-0043-x
Janke, M. K. (1991). Accidents, mileage, and the exaggeration of risk. Accident Analysis & Prevention, 23(2–3), 183-188. doi: http://dx.doi.org/10.1016/0001-4575(91)90048-A
Johnson, J. E. (1999). Urban Older Adults and the Forfeiture of a Driver’s License. Journal of Gerontological Nursing, 25(12), 12-18.
Keall, M. D., & Woodbury, E. (2014). An analysis of changes in mobility and safety of older drivers associated with a specific older driver on-road licensing test: a population study. BMC Public Health, 14(1), 165-165. doi: 10.1186/1471-2458-14-165
Keay, L., Coxon, K., Brown, J., Clarke, E., Boufous, S., Bundy, A., . . . Ivers, R. (2013). A randomized trial to evaluate the effectiveness of an individual, education-based safe transport program for drivers aged 75 years and older. BMC Public Health, 13, 106. doi: 10.1016/j.aap.2007.07.012 http://dx.doi.org/10.1186/1471-2458-13-106
King, M., Soole, D., Watson, A., & Schramm, A. (2011). Older driver safety advisory committee – supporting research and consultation. Report to Department of Transport and Main Roads
King, M. J., & Scott-Parker, B. J. (2016). Older male and female drivers in car-dependent settings: how much do they use other modes, and do they compensate for reduced driving to maintain mobility? Ageing and Society, 1-19. doi: 10.1017/S0144686X15001555

200 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Koppel, S., Charlton, J.L., Langford, J., Di Stefano, M., MacDonald, W., Vlahodimitrakou, Z., Mazer, B.L., Gelinas, I., Vrkljan, B., Eliasz, K., Myers, A., Tuokko, H.A., & Marshall, S.C. (2016). Driving task: how older drivers' on-road driving performance relates to abilities, perceptions, and restrictions. Canadian Journal of Aging, 35(1), 15-31. doi: 10.1017/S0714980816000015
Kostyniuk , L. P., Shope, J. T., & Molnar, L. J. (2000). Driving reduction/cessation among older drivers: toward a behavioral framework. In Travel Behaviour Research: The Leading Edge (Hensher, D, Ed.) (2000), p. 783-795. .
Kostyniuk , L. P., Trombley, D. A., & Shope, J. T. (1998). Reduction and cessation of driving among older drivers: a review of the literature. UMTRI-98-23.
Kowalski, K., Jeznach, A., & Tuokko, H. A. (2014). Stages of driving behavior change within the Transtheoretical Model (TM). Journal of Safety Research, 50(0), 17-25. doi: http://dx.doi.org/10.1016/j.jsr.2014.01.002
Lafont, S., Laumon, B., Helmer, C., Dartigues, J.-F., & Fabrigoule, C. (2008). Driving Cessation and self-reported car crashes in older drivers: the impact of cognitive impairment and dementia in a population-based study. Journal of Geriatric Psychiatry and Neurology, 21(3), 171-182. doi: 10.1177/0891988708316861
Lang, B., Parkes, A., & Medina, K. F. (2013 ). Driving choices for the older motorist :the role of self-assessment tools.
Langford, J., Andrea, D., Fildes, B., Williams, T., & Hull, M. (2005). Assessing responsibility for older drivers' crashes, Austroads, AP-R265/05.
Langford, J., Bohensky, M., Koppel, S., & Newstead, S. (2008). Do age-based mandatory assessments reduce older drivers’ risk to other road users? Accident Analysis & Prevention, 40(6), 1913-1918. doi: http://dx.doi.org/10.1016/j.aap.2008.08.010
Langford, J., Charlton, J. L., Koppel, S., Myers, A., Tuokko, H., Marshall, S., . . . Macdonald, W. (2013). Findings from the Candrive/Ozcandrive study: Low mileage older drivers, crash risk and reduced fitness to drive. Accident Analysis and Prevention, 61, 304.
Langford, J., Fitzharris, M., Koppel, S., & Newstead, S. (2004). Effectiveness of Mandatory License Testing for Older Drivers in Reducing Crash Risk Among Urban Older Australian Drivers. Traffic Injury Prevention, 5(4), 326-335. doi: 10.1080/15389580490509464
Langford, J., Fitzharris, M., Newstead, S., & Koppel, S. (2004). Some consequences of different older driver licensing procedures in Australia. Accident Analysis & Prevention, 36(6), 993-1001. doi: http://dx.doi.org/10.1016/j.aap.2003.11.003
Langford, J., & Koppel, S. (2006). The case for and against mandatory age-based assessment of older drivers. Transportation Research Part F: Traffic Psychology and Behaviour, 9(5), 353-362. doi: http://dx.doi.org/10.1016/j.trf.2006.06.009
Langford, J., & Koppel, S. (2011). Licence restrictions as an under-used strategy in managing older driver safety. Accident Analysis and Prevention, 43(1), 487-493. doi: 10.1016/j.aap.2010.09.005
Lenio, J.A. (2006) Analysis of the Transtheoretical model of behaviour change. Journal of Student Research University of Wisconsin-Stout. Retreived online from https://minds.wisconsin.edu/bitstream/handle/1793/52717/14Lenio.pdf?sequence=1

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 201
Li, G., Braver, E. R., & Chen, L.-H. (2003). Fragility versus excessive crash involvement as determinants of high death rates per vehicle-mile of travel among older drivers. Accident Analysis & Prevention, 35(2), 227-235. doi: http://dx.doi.org/10.1016/S0001-4575(01)00107-5
Liddle, J., Carlson, G., & McKenna, K. (2004). Using a Matrix in Life Transition Research. Qualitative Health Research, 14(10), 1396-1417. doi: 10.1177/1049732304268793
Liddle, J., Gustafsson, L., Bartlett, H., & McKenna, K. (2012). Time use, role participation and life satisfaction of older people: Impact of driving status. Australian Occupational Therapy Journal, 59(5), 384-392. doi: 10.1111/j.1440-1630.2011.00956.x
Liddle, J., Haynes, M., Pachana, N. A., Mitchell, G., McKenna, K., & Gustafsson, L. (2014). Effect of a Group Intervention to Promote Older Adults’ Adjustment to Driving Cessation on Community Mobility: A Randomized Controlled Trial. The Gerontologist, 54(3), 409-422. doi: 10.1093/geront/gnt019
Liddle, J., Turpin, M., Carlson, G., & McKenna, K. (2008). The needs and experiences related to driving cessation for older people. British Journal of Occupational Therapy, 71, 379+.
Lindgren, A. M., Chen, F., Jordan, P. W., & Zhang, H. (2008). Requirements for the Design of Advanced Driver Assistance Systems – The Differences between Swedish and Chinese Drivers.
Lindstrom-Forneri, W., Tuokko, H. A., Garrett, D., & Molnar, F. (2010). Driving as an Everyday Competence: A Model of Driving Competence and Behavior. Clinical Gerontologist, 33(4), 283-297. doi: 10.1080/07317115.2010.502106
Littell, J. H., & Girvin, H. (2002). Stages of change. A critique. Behav Modif, 26(2), 223-273.
Lyman, J. M., McGwin Jr, G., & Sims, R. V. (2001). Factors related to driving difficulty and habits in older drivers. Accident Analysis & Prevention, 33(3), 413-421. doi: http://dx.doi.org/10.1016/S0001-4575(00)00055-5
MacDonald, L., Myers, A. M., & Blanchard, R. A. (2008). Correspondence among older drivers' perceptions, abilities, and behaviors. Topics in Geriatric Rehabilitation, 24(3), 239.
Marottoli, R. A., Carlos, F. M. d. L., Glass, T. A., Williams, C. S., & et al. (2000). Consequences of driving cessation: Decreased out-of-home activity levels. The Journals of Gerontology, 55B(6), S334-340.
Marottoli, R. A., Ostfeld, A. M., Merrill, S. S., Perlman, G. D., Foley, D. J., & Cooney, L. M., Jr. (1993). Driving cessation and changes in mileage driven among elderly individuals. Journal of Gerontology, 48(5), S255-260.
Marottoli, R. A., & Richardson, E. D. (1998). Confidence in, and self-rating of, driving ability among older drivers. Accident Analaysis and Prevention, 30(3), 331-336.
Marshall, S. C. (2008). The Role of Reduced Fitness to Drive Due to Medical Impairments in Explaining Crashes Involving Older Drivers. Traffic Injury Prevention, 9(4), 291-298. doi: 10.1080/15389580801895244
Marshall, S. J., & Biddle, S. J. H. (2001). The transtheoretical model of behavior change: a meta-analysis of applications to physical activity and exercise. Annals of Behavioral Medicine, 23(4), 229-246. doi: 10.1207/s15324796abm2304_2
Marshall, S. M. D. M. F., Demmings, E. M. M. D. M., Woolnough, A. M., Salim, D. B., & Man-Son-Hing, M. M. D. M. F. (2012). Determining Fitness to Drive

202 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
in Older Persons: A Survey of Medical and Surgical Specialists. Canadian Geriatrics Journal, 15(4), 101-119.
Mauck, K. F., Cuddihy, M. T., Trousdale, R. T., Pond, G. R., Pankratz, V. S., & Melton Iii, L. J. (2002). The Decision to Accept Treatment for Osteoporosis Following Hip Fracture: Exploring the Woman’s Perspective Using a Stage-of-Change Model. Osteoporosis International, 13(7), 560-564. doi: 10.1007/s001980200073
McNamara, A., Chen, G., George, S., Walker, R., & Ratcliffe, J. (2013). What factors influence older people in the decision to relinquish their driver's licence? A discrete choice experiment. Accid Anal Prev, 55, 178.
Meng, A., & Siren, A. (2012). Cognitive problems, self-rated changes in driving skills, driving-related discomfort and self-regulation of driving in old drivers. Accident Analysis & Prevention, 49(0), 322-329. doi: http://dx.doi.org/10.1016/j.aap.2012.01.023
Meuleners, L. B., Harding, A., Lee, A. H., & Legge, M. (2006). Fragility and crash over-representation among older drivers in Western Australia. Accident Analysis & Prevention, 38(5), 1006-1010. doi: http://dx.doi.org/10.1016/j.aap.2006.04.005
Mitchell, K. (2010). Older drivers: a review. In E. Box, J. Gandolfi and K. Mitchell, Maintaining Safe Mobility for the Ageing Population, London: RAC Foundation.
Molnar, L. J., Byszewski, A. M., Marshall, S. C., & Man-Son-Hing, M. (2005). In-office evaluation of medical fitness to drive: practical approaches for assessing older people. Can Fam Physician, 51, 372-379.
Molnar, L. J., & Eby, D. W. (2008). The Relationship between Self-Regulation and Driving-Related Abilities in Older Drivers: An Exploratory Study. Traffic Injury Prevention, 9(4), 314-319. doi: 10.1080/15389580801895319
Molnar, L. J., & Eby, D. W. (2009). Getting around: Meeting the boomers' mobility needs. In Boomer bust? economic and political issues of the graying society., ed. R. Houston, vol. 2, Praeger Publishing.
Molnar, L. J., Eby, D. W., Langford, J., Charlton, J. L., St. Louis, R. M., & Roberts, J. S. (2013). Tactical, strategic, and life-goal self-regulation of driving by older adults: Development and testing of a questionnaire. Journal of Safety Research, 46(0), 107-117. doi: http://dx.doi.org/10.1016/j.jsr.2013.05.001
Molnar, L. J., Eby, D. W., St. Louis, R. M., & Neumeyer, A. L. (2007). Promising approaches for promoting lifelong community mobility.
Molnar, L. J., Eby, D. W., Zhang, L., Zanier, N., St. Louis, R. M., & Kostyniuk , L. P. (2015). Self-regulation of driving by older adults: A Synthesis of the Literature and Framework for Future Research.: AAA Foundation for Traffic Safety.
Morris, A., Welsh, R., Frampton, R., Charlton, J., & Fildes, B. (2003). Vehicle crashworthiness and the older motorist. Ageing and Society, 23(04), 395-409.
Moták, L., Gabaude, C., Bougeant, J.-C., & Huet, N. (2014). Comparison of driving avoidance and self-regulatory patterns in younger and older drivers. Transportation Research Part F: Traffic Psychology and Behaviour, 26, 18-27. doi: 10.1016/j.trf.2014.06.007
Musselwhite, C., & Haddad, H. (2008). Prolonging safe driving through technology. Final Report. UWE research report.

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 203
Musselwhite, C., & Haddad, H. (2010a). Exploring older drivers’ perceptions of driving. European Journal of Ageing, 7(3), 181-188. doi: 10.1007/s10433-010-0147-3
Musselwhite, C., & Haddad, H. (2010b). Mobility, accessibility and quality of later life. Quality in Ageing and Older Adults, 11(1), 25-37.
Musselwhite, C., & Shergold, I. (2013). Examining the process of driving cessation in later life. European Journal of Ageing, 10(2), 89-100. doi: 10.1007/s10433-012-0252-6
Nasvadi, G. E., & Wister, A. (2009). Do restricted driver's licenses lower crash risk among older drivers? A survival analysis of insurance data from British Columbia. The Gerontologist, 49(4), 474-484. doi: 10.1093/geront/gnp039
Naumann, R. B., Dellinger, A. M., & Kresnow, M.-j. (2011). Driving self-restriction in high-risk conditions: How do older drivers compare to others? Journal of Safety Research, 42(1), 67-71. doi: http://dx.doi.org/10.1016/j.jsr.2010.12.001
Newgard, C. D. (2008). Defining the “older” crash victim: The relationship between age and serious injury in motor vehicle crashes. Accident Analysis and Prevention, 40(4), 1498-1505. doi: 10.1016/j.aap.2008.03.010
Nordfjærn, T., Şimşekoğlu, Ö., & Rundmo, T. (2014). The role of deliberate planning, car habit and resistance to change in public transportation mode use. Transportation Research Part F: Traffic Psychology and Behaviour, 27, 90-98. doi: 10.1016/j.trf.2014.09.010
Nylund, K. L., Asparouhov, T., & Muthén, B. O. (2007). Deciding on the Number of Classes in Latent Class Analysis and Growth Mixture Modeling: A Monte Carlo Simulation Study. Structural Equation Modeling: A Multidisciplinary Journal, 14(4), 535-569. doi: 10.1080/10705510701575396
O'Connor, M. L., Edwards, J. D., Waters, M. P., Hudak, E. M., & Valdes, E. G. (2013). Mediators of the association between driving cessation and mortality among older adults. J Aging Health, 25(8 Suppl), 249S-269S. doi: 10.1177/0898264313497796
OECD. (2001). Ageing and Transport. Mobility Needs and Safety Issues. OECD Publications, Paris.
Owsley, C., McGwin, G., Phillips, J. M., McNeal, S. F., & Stalvey, B. T. (2004). Impact of an educational program on the safety of high-risk, visually impaired, older drivers. American Journal of Preventive Medicine, 26(3), 222-229. doi: 10.1016/j.amepre.2003.12.005
Owsley, C., Stalvey, B. T., & Phillips, J. M. (2003). The efficacy of an educational intervention in promoting self-regulation among high-risk older drivers. Accident Analysis & Prevention, 35(3), 393-400. doi: http://dx.doi.org/10.1016/S0001-4575(02)00016-7
Oxley, J., Charlton, J., & Fildes, B. (2003). Self Regulation of Older Drivers: A Review of the Literature. (Report AP-R221-03). Sydney, Australia.
Oxley, J., Charlton, J., Scully, J., & Koppel, S. (2010). Older female drivers: An emerging transport safety and mobility issue in Australia. Accident Analysis & Prevention, 42(2), 515-522. doi: http://dx.doi.org/10.1016/j.aap.2009.09.017
Oxley, J., & Whelan, M. (2008). It Cannot Be All about Safety: The Benefits of Prolonged Mobility. Traffic Injury Prevention, 9(4), 367-378. doi: 10.1080/15389580801895285

204 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Parker, D., MacDonald, L., Sutcliffe, P., & Rabbitt, P. (2001). Confidence and the older driver. Ageing & Society, 21(02), 169-182. doi: doi:10.1017/S0144686X01008133
Peel, N., Westmoreland, J., & Steinberg, M. (2002). Transport safety for older people: a study of their experiences, perceptions and management needs. Inj Control Saf Promot, 9(1), 19-24. doi: 10.1076/icsp.9.1.19.3327
Persson, D. (1993). The elderly driver: Deciding when to stop. The Gerontologist, 33(1), 88-88. doi: 10.1093/geront/33.1.88
Prochaska, J. O., & Velicer, W. F. (1997). The transtheoretical model of health behavior change. Am J Health Promot, 12(1), 38-48.
Ragland, D. R., Satariano, W. A., & MacLeod, K. E. (2004). Reasons given by older people for limitation or avoidance of driving. Gerontologist, 44(2), 237-244.
Ragland, D. R., Satariano, W. A., & MacLeod, K. E. (2005). Driving Cessation and Increased Depressive Symptoms. The Journals of Gerontology, 60A(3), 399-403.
Rakotonirainy, A., & Steinhardt, D. (2009). In-vehicle technology functional requirements for older drivers. Paper presented at the Proceedings of the 1st International Conference on Automotive User Interfaces and Interactive Vehicular Applications, Essen, Germany.
Rakotonirainy, A., Steinhardt, D., Delhomme, P., Darvell, M., & Schramm, A. (2012). Older drivers’ crashes in Queensland, Australia. Accident Analysis & Prevention, 48(0), 423-429. doi: http://dx.doi.org/10.1016/j.aap.2012.02.016
Ramaswamy, V., Desarbo, W. S., Reibstein, D. J., & Robinson, W. T. (1993). An Empirical Pooling Approach for Estimating Marketing Mix Elasticities with PIMS Data. Marketing Science, 12(1), 103-124. doi: 10.1287/mksc.12.1.103
Ridder, D. T. D. d., Wit, J. B. F. d., & Wiley, I. (2006). Self-regulation in health behavior (Vol. 1. Aufl.;1;). Hoboken, NJ;Chichester, England;: John Wiley & Sons.
Rosenbloom, S. (2006). Is the Driving Experience of Older Women Changing? Safety and Mobility Consequences over Time. Transportation Research Record: Journal of the Transportation Research Board, 1956(-1), 127-132. doi: 10.3141/1956-16
Rosenbloom, S., & Herbel, S. (2009). The Safety and Mobility Patterns of Older Women: Do Current Patterns Foretell the Future? Public Works Management & Policy, 13(4), 338-353.
Ross, L. A., Browning, C., Luszcz, M. A., Mitchell, P., & Anstey, K. J. (2011). Age-Based Testing for Driver's License Renewal: Potential Implications for Older Australians. J Am Geriatr Soc, 59(2), 281-285. doi: 10.1111/j.1532-5415.2010.03241.x
Ross, L. A., Clay, O. J., Edwards, J. D., Ball, K. K., Wadley, V. G., Vance, D. E., . . . Joyce, J. J. (2009). Do Older Drivers At-Risk for Crashes Modify Their Driving Over Time? Journals of Gerontology: Series B, 64B(2), 163-170. doi: 10.1093/geronb/gbn034
Ross, L. A., Dodson, J. E., Edwards, J. D., Ackerman, M. L., & Ball, K. (2012). Self-rated driving and driving safety in older adults. Accident Analysis & Prevention, 48(0), 523-527. doi: http://dx.doi.org/10.1016/j.aap.2012.02.015
Rudman, D. L., Friedland, J., Chipman, M., & Sciortino, P. (2006a). Holding on and letting go: the perspectives of pre-seniors and seniors on driving self-regulation in later life. Canadian Journal on Aging, 25(1), 65-76.

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 205
Rudman, D. L., Friedland, J., Chipman, M., & Sciortino, P. (2006b). Holding on and letting go: the perspectives of pre-seniors and seniors on driving self-regulation in later life. Can J Aging, 25(1), 65-76.
Sargent-Cox, K. A., Windsor, T., Walker, J., & Anstey, K. J. (2011). Health literacy of older drivers and the importance of health experience for self-regulation of driving behaviour. Accident Analysis & Prevention, 43(3), 898-905. doi: http://dx.doi.org/10.1016/j.aap.2010.11.012
Shergold, I., Parkhurst, G., & Musselwhite, C. (2012). Rural car dependence:an emerging barrier to community activity for older people. Transport Planning and Technology, 35(1), 69-85.
Siren, A., & Hakamies-Blomqvist, L. (2005). Sense and sensibility. A narrative study of older women’s car driving. Transportation Research Part F: Traffic Psychology and Behaviour, 8(3), 213-228. doi: http://dx.doi.org/10.1016/j.trf.2005.04.008
Siren, A., Hakamies-Blomqvist, L., & Lindeman, M. (2004). Driving Cessation and Health in Older Women. Journal of Applied Gerontology, 23(1), 58-69. doi: 10.1177/0733464804263129
Siren, A., & Haustein, S. (2015). Driving licences and medical screening in old age: Review of literature and European licensing policies. Journal of Transport & Health, 2(1), 68-78. doi: http://dx.doi.org/10.1016/j.jth.2014.09.003
Siren, A., & Kjær, M. R. (2011). How is the older road users’ perception of risk constructed? Transportation Research Part F: Traffic Psychology and Behaviour, 14(3), 222-228. doi: http://dx.doi.org/10.1016/j.trf.2011.01.002
Siren, A., & Meng, A. (2013). Older drivers’ self-assessed driving skills, driving-related stress and self-regulation in traffic. Transportation Research Part F: Traffic Psychology and Behaviour, 17, 88-97. doi: 10.1016/j.trf.2012.10.004
Stalvey, B. T., & Owsley, C. (2003). The Development and Efficacy of a Theory-Based Educational Curriculum to Promote Self-Regulation Among High-Risk Older Drivers. Health Promotion Practice, 4(2), 109-119. doi: 10.1177/1524839902250757
Staplin, L., & Freund, K. (2013). Policy prescriptions to preserve mobility for seniors--A dose of realism. Accident Analysis and Prevention, 61, 212. doi: 10.1016/j.aap.2013.01.014
Staplin, L., GIsh, K. W., Decina, L. E., Lococo, K., & McKnight, A. S. (1998a). Intersection negotiation problems of older drivers volume 2: Background synthesis ((Report No. 1446/FR). ).
Staplin, L., Lococo, K., Martell, C., & Stutts, J. (2012). Taxonomy of older driver behaviours and crash risk. United States Department of Transportation Report No. DOT HS 811 468A. Washington, DC:NHTSA.
Stewart, R. B., Moore, M. T., Marks, R. G., May, F. E., & Hale, W. E. (1993). Driving cessation and accidents in the elderly: an analysis of symptoms, diseases, congnitive dysfunction and medications.
Stutts, J. (1998). Do older drivers with visual and cognitive impairments drive less? Journal of American Geriatric Society, 46, 854-861.
Sullivan, K. A., Smith, S. S., Horswill, M. S., & Lurie-Beck, J. K. (2011). Older adults’ safety perceptions of driving situations: Towards a new driving self-regulation scale. Accident Analysis and Prevention, 43(3), 1003-1009. doi: 10.1016/j.aap.2010.11.031
Tay, R. (2012). Ageing driver licensing requirements and traffic safety. Ageing and Society, 32(4), 655-672. doi: http://dx.doi.org/10.1017/S0144686X11000535

206 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Taylor, B. D., & Tripodes, S. (2001). The effects of driving cessation on the elderly with dementia and their caregivers. Accident Analysis & Prevention, 33(4), 519-528.
Tefft, B. C. (2008). Risks older drivers pose to themselves and to other road users. Journal of Safety Research, 39(6), 577-582. doi: http://dx.doi.org/10.1016/j.jsr.2008.10.002
Torpey, S. (1986). Licence re-testing of older drivers. Melbourne: Road Traffic Authority.
Tramm, R., McCarthy, A., & Yates, P. (2012). Using the Precede–Proceed Model of Health Program Planning in breast cancer nursing research. Journal of advanced nursing, 68(8), 1870-1880. doi: 10.1111/j.1365-2648.2011.05888.x
Tuokko, H., McGee, P., Gabriel, G., & Rhodes, R. E. (2007). Perception, attitudes and beliefs, and openness to change: Implications for older driver education. Accident Analysis & Prevention, 39(4), 812-817. doi: http://dx.doi.org/10.1016/j.aap.2006.12.002
Tuokko, H., Jouk, A., Myers, A., Marshall, S., Man-Son-Hing, M., Porter, M. M., . . . Vrkljan, B. (2014). A re-examination of driving-related attitudes and readiness to change driving behavior in older adults. Physical & Occupational Therapy in Geriatrics, 32(3), 210-227. doi: 10.3109/02703181.2014.931503
Tuokko, H., Rhodes, R., Love, J., Cloutier, D., Jouk, A., & Schoklitsch, A. (2015). Just the facts: changes in older driver attitudes after exposure to educational interventions. Traffic Injury Prevention, 16(6), 558-564. doi: 10.1080/15389588.2014.992067
Unsworth, C. A., Wells, Y., Browning, C., Thomas, S. A., & Kendig, H. (2007). To continue, modify or relinquish driving: findings from a longitudinal study of healthy ageing. Gerontology, 53(6), 423-431. doi: 10.1159/000111489
Walker, G. H., Stanton, N. A., & Young, M. S. (2001). Where is computing driving cars? International Journal of Human–Computer Interaction, 13(2), 203-229. doi: 10.1207/S15327590IJHC1302_7
Wang, C. C., & Carr, D. B. (2004). Older driver safety: a report from the older drivers project. Journal of American Geriatric Society, 52(1), 143-149.
Weinstein, N. D., Lyon, J. E., Sandmand, P. M., & Cuite, C. L. (1998). Experimental evidence for stages of health behavior change: the Precaution Adoption Process Model applied to home radon testing. Health Psychology, 17(5), 445-453.
Weinstein, N. D., & Sandmand, P. M. (2002). The Precaution Adoption Process Model. In K. Glanz, B.K. Rimer, F.M. Lewis (Eds.), Health behavior and health education: theory, research and practice (3rd ed) (pp. 121–143), Jossey-Bass, San Francisco.
Weinstein, N. D., Sandmand, P. M., & Blalock, S. J. (2008). The Precaution Adoption Process Model. In K. Glanz, B. k. Rimer & K. Viswanath (Eds.), Health Behaviour and Health Education, 4th ed. (pp. 123-147). San Franciso: Jossey-Bass.
West, C. G., Gildengorin, G., Haegerstrom-Portnoy, G., Lott, L. A., Schneck, M. E., & Brabyn, J. A. (2003). Vision and driving self-restriction in older adults. Journal of American Geriatric Society, 51(10), 1348-1355.
Whelan, M., Langford, J., Oxley, J., Koppel, S., & Charlton, J. (2006). The elderly and mobility: a review of the literature, Monash University Accident Research Centre, Report No. 255.

The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours 207
Wong, I. Y., Smith, S. S., & Sullivan, K. A. (2012). The relationship between cognitive ability, insight and self-regulatory behaviors: findings from the older driver population. Accident Analysis and Prevention, 49, 316-321.
Wong, I. Y., Smith, S. S., Sullivan, K. A., & Allan, A. C. (2016). Toward the Multilevel older person's transportation and road safety model: a new perspective on the role of demographic, functional, and psychosocial factors. Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 71(1), 71-86. doi: 10.1093/geronb/gbu099
Wood, J. M., Anstey, K. J., Kerr, G. K., Lacherez, P. F., & Lord, S. (2008). A multidomain approach for predicting older driver safety under in-traffic road conditions. Journal of American Geriatric Society, 56(6), 986-993. doi: 10.1111/j.1532-5415.2008.01709.x
Wood, J. M., Horswill, M. S., Lacherez, P. F., & Anstey, K. J. (2013). Evaluation of screening tests for predicting older driver performance and safety assessed by an on-road test. Accident Analysis and Prevention, 50, 1161-1168. doi: 10.1016/j.aap.2012.09.009
Yassuda, M. S., & Wilson, J. J. (1997). Driving cesssation: The perspective of senior drivers. Educational Gerontology, 23(6), 525-538.
Zhao, G., & Wu, C. (2012). The effects of driver identity on driving safety in a retrospective feedback system. Accident Analysis & Prevention, 45(0), 354-365.


Chapter 10: 209
Appendices
Appendix A
Recruitment Flyer for Focus Groups

210 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Appendix B
Newspaper advertisement for Focus Groups
We are inviting individuals aged 70 years or more who are either former drivers or current drivers to participate in a study on driving. This project is being conducted by researchers at Queensland University of Technology (QUT) to explore your beliefs and attitudes regarding receiving feedback about driving. Your participation will involve completing a background questionnaire and attending a 90-minute focus group session. All participants will receive $40 Coles and Myer gift voucher. Please email [email protected] or phone 0416 779 400 for further information. Thank you for your interest and feel free to tell your friends about the study. Participation is confidential and all responses and information will be stored securely and remain confidential. This project has been approved by QUT's Human Research Ethics Committee (Ref No. 1200000501).

Chapter 10: 211
Appendix C
Focus Group Protocol and Discussion Guide Preparation: 1. Confirm room booking. 2. Call to confirm location, date, and time with participants. 3. Check materials; tape recorder, batteries, pens, name tags, participant information sheet and consent forms, background questionnaires, incentives and refreshments. On the day: 1. Welcome participants, invite them to help themselves with the refreshments. Make sure you check if they want to go to the bathroom and they know where the bathroom is. Once everyone is seated provide them with name tags. 2. Introduce yourself and hand each person the participant information sheet, the consent form, and the background questionnaire to fill in. 3. Once collect them, ask them if they have any questions. 4. Introduce the Ground Rules: - Introduce yourself and your role again and the reason for this discussion. -Please try and speak one at a time, so that we will not miss important information. - There are no right or wrong answers, all comments are important. - It is okay for people to disagree or express different opinions. Turn on tape recorder Ice-breaker: okay everyone, let’s start today by introducing ourselves, tell us how long you have been driving. Would you say driving is important for you? If so, can you tell us why? Rationale: Importance of driving Perceived advantages of driving Reasons for driving (e.g. other relying on driving)
Probes: Independence, convenience, enjoyment, sense of control, identity, social inclusion, other relying on your driving.
Would you say that now at your age, there are negative aspects associated with driving? Rationale: Perceived disadvantages of driving (Intrapersonal factor) Levels of comfort Level of confidence
Probes: Expense and cost, fear and anxiety, discomfort, behaviour of other drivers and pressure from others to stop driving.
Do you think there are differences now versus say ten or twenty years ago in your driving ability? If so can you tell us how?

212 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Rationale: Perceived changes in driving ability Self-efficacy Confidence
Probes: physical changes (vision, hearing, reflexes, head and neck mobility, fatigue) Psychological changes (confidence, enjoyment, and ability to be in stressful situation while feeling safe) What abilities do they think are important for safe driving?
Have you changed your driving over the last ten years or so? If yes, can you tell us how? Rationale: change process Probes: Drive less, adopt certain strategies, and avoid certain driving
situations What made you aware that you need to adopt strategies to continue driving? Rationale: Interpersonal influence Insight Knowledge and health literacy Self-efficacy Feedback Probes: family, friends, health professional, refreshing course, self-
assessment tool In ten or twenty years from now, do you think your driving will be changed, would you say you will be doing things differently? Rationale: Beliefs about likelihood and personal susceptibility to impaired driving Self-enhancement bias Level of confidence Probes: avoid certain driving situation; drive less, use alternative transportation options more or stop driving altogether Have you ever thought about the possibility of stopping driving someday? How will you know it is about time to stop? What will influence your decision to stop driving? Have you ever sought information about the effect of ageing on your driving ability? If yes, then why? Have you ever discussed with someone your driving concerns or worries, say your doctor or your family? Would you say it is helpful if you receive feedback about your driving ability? If so can you suggest how and from whom? In your opinion, what would you be looking forward in your discussion with your physician?

Chapter 10: 213
Is there anything else that comes to your mind?
Appendix D
Consent Form for Focus Groups

214 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours

Chapter 10: 215
Appendix E
Background Questionnaire- Focus Group Study
QUESTIONNAIRE
Feedback and Older Driver Study
This questionnaire booklet contains questions about you and your driving practices. All information received will be treated confidentially. Please respond carefully to all questions and remember there are no right
or wrong answers.
Centre for Accident Research and Road Safety – Queensland (CARRS-Q) Queensland University of Technology
130 Victoria Park Road, Kelvin Grove, Queensland 4059 Australia Email [email protected] Web www.carrsq.qut.edu.au
CRICOS No. 00213J
Thank you for your assistance

216 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Background questionnaire
1. Are you (please tick) □ Male
□ Female
2. Your age (Years) ________________
3. What is your postcode? ________________
4. What is your highest education level?
□Primary School
□Secondary
□Certificate/Diploma
□Bachelor degree
□Postgraduate
5. Is English your native language?
□Yes
□No
6. Do you live in?
□A private home
□A retirement home or seniors’ complex
□Other, please specify________________
7. Do you live:
□Alone
□With spouse or partner
□With family members
□With friend(s)
□With paid caregiver
□Other, please specify ________________
8. Do you work (paid or voluntary) at the moment?
□Yes, full-time
□Yes, part-time
□No
9. Are you still driving? □Yes
□No

Chapter 10: 217
10. Do you hold a current open driver’s licence?
□Yes
□No
□Other, please specify________________
11. For approximately how many years you have had your open driver’s licence?
12. What is your annual number of kilometres driven?
□Less than 5000 km/yr.
□5,000-10,000 km/yr.
□10,001-20,000 km/yr.
□20,001-30,000 km/yr.
□More than 30,000 km/yr.
13. Overall would you say your health is?
□Excellent
□Very good
□Fair
□Poor
□Very poor
14. Are you currently taking any prescribed medications?
□No
□Yes, please specify and how many ________________ ________________ ________________
End of questionnaire Thank you very much for your participation in this study

218 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Appendix F
Participant Information Sheet-Survey

Chapter 10: 219
Appendix G
Study Two Questionnaire
SURVEY Feedback and Older Driver Study
This survey booklet contains questions about you and your driving practices. All information received will be treated confidentially. Please respond carefully to all questions and remember there are no right or wrong answers.
Thank you for your assistance Centre for Accident Research and Road Safety – Queensland (CARRS-Q) Queensland University of Technology (QUT) 130 Victoria Park Road Kelvin Grove Queensland 4059 Australia Email [email protected] Web www.carrsq.qut.edu.au CRICOS No. 00213J

220 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Gender Male Female
Your age (Years) _____________________
What is your postcode? _____________________
What is your highest education level?
Primary School
Secondary
Certificate/Diploma
Bachelor degree
Postgraduate
Is English your native language?
Yes
No
Do you live in?
A private home
A retirement home or seniors’ complex
Other, please specify_______________________________________
Do you live:
Alone
With spouse or partner
With family members
With friend(s)
With paid caregiver
Other, please specify _______________________________________
Do you work (paid or voluntary) at the moment?
Yes, full-time
Yes, part-time
No
Overall would you say your health is?
Excellent
Very good
Fair
Poor
Very poor
Are you still driving?

Chapter 10: 221
Yes
No
Are you the main driver in your household?
Yes
No
Shared equally
For approximately how many years you have had your open driver’s licence?
______________________________________
What is your annual number of kilometres driven?
Less than 5000 km/yr.
5,000-10,000 km/yr.
10,001-20,000 km/yr.
20,001-30,000 km/yr.
More than 30,000 km/yr.
Have you taken any driving courses?
No
Yes
Do you remember who offered the course? _______________________________________
In the past ten years or so, have you ever taken (please tick all that applies):
Vision test
Rules test
Road test
In an average week, how many days per week do you normally drive? _________________________________
Where do you generally drive
City
Rural
Suburb
How long are most of your driving trips (each way)?
Less than 15 minutes
15-30 minutes
30-60 minutes
Over 60 minutes
Which way do you prefer to get around?
Drive yourself
Have someone drive you

222 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Use public transportation or taxi
Other, please explain ________________________________
If you had to go somewhere and did not want to drive yourself, what would you do?
Ask a friend or relative to drive you
Call a taxi or take a bus or other public transport
Drive yourself regardless of how you feel
Cancel or postpone your plans and stay home
Other, please specify ________________________________
Please think for a moment about all the places you drive in a typical week. You can tick more than one.
Shop
Church (or other place of worship)
Work
Relative’s house
Friend’s house
Out to eat
Appointments (hair, doctor)
Other, please specify_______________________________________
How would you rate the quality of your driving? Would you say it was?
Excellent
Good
Average
Fair
Poor
In the past year, have you had any crashes when you were the driver?
(Please include minor scrapes and bumps)?
No
Yes
If yes, please specify the number of all the crashes and whether or not you were at fault. _________________________________
Compared to ten years ago, would you say that you drive
Much less
A little less
The same
More
Compared to ten years ago, do you still feel confident that you can safely drive to places you need to go
Much less

Chapter 10: 223
A little less
The same
More
How likely is it for you to have a car crash, compared to other people your age?
Not likely
Somewhat likely
Extremely likely
How likely is it for you to have a car crash, compared to yourself ten years ago?
Not likely
Somewhat likely
Extremely likely
How likely is it for you to be injured if you are involved in a crash?
Not likely
Somewhat likely
Extremely likely
How often do you use public transport?
Always
Frequently
Sometimes
Rarely
Never
If you use public transport rarely, can you tell us why (you can tick more than once)
Don’t need to
Don’t know enough about it
Inconvenient
Time-consuming
Don’t feel safe
Cost too much
Unreliable
Bus stop far from home
Other _______________________________________
How often do you use taxis?
Always
Frequently
Sometimes
Rarely
Never

224 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
If you use taxis rarely, can you tell us why (you can tick more than once) Don’t need to
Don’t know enough about it
Inconvenient
Time-consuming
Don’t feel safe
Cost too much
Unreliable
Other _______________________________________
How often do you take rides from family or friends? Always
Frequently
Sometimes
Rarely
Never
In general, how comfortable are you asking family or friends for rides? Very comfortable
Somewhat comfortable
Somewhat uncomfortable
Very uncomfortable
How important is it for you to continue to drive? Extremely important
Very important
Moderately important
Somewhat important
Not that important
Have you moved to a new place closer to your common destinations (shops, family, church, etc.)?
Yes
No
If you ticked no, is this something that you would consider in future? Yes
No
Did not think about it
Have you moved to a senior community that provides transportation? Yes
No
If you ticked no, is this something that you would consider in future? Yes

Chapter 10: 225
No
Did not think about it
Have you moved to a new place with better options for public transportation? Yes
No
If you ticked no, is this something that you would consider in future? Yes
No
Did not think about it
Do you use in-vehicle technology to make your driving easier? (e.g. navigation system, cruise control, blind spot detection)
Yes
No
If you ticked no, is this something that you would consider in future? Yes
No
Did not think about it
In the past year, have you talked about your driving with any of the following? You can tick more than one.
Your doctor
Family members
Friends
Other, please specify ___________________________________
Has anyone suggested over the past year that you limit or stop your driving? No
Yes
If you ticked yes, please indicate all that apply Family member
Friend
Your doctor
An eye care professional
Other, please specify ____________________________________
What did you do in response to their suggestion? Ignored it
Made own assessment of ability and decided no action was required
Restricted my driving, please specify _______________________________________
Other, please specify
_______________________________________
Whose suggestion regarding change in driving status would you most likely

226 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
listen to? Partner
Other family members
Doctor
Friend
Person of authority (e.g. police)
Which of the following could make you consider changing your current driving? (Please tick all that apply)
Medical condition
Vision problem
Feeling unfit to drive
Feeling nervous when driving
Feeling uncomfortable when driving
If I have a crash
If advised by my family
If advised by my doctor
If my license is revoked
Other _______________________________________
Which of the following statements better describe you?
I am at the point where I am not sure if I should start thinking about ways to avoid certain driving situation or reduce my driving
Avoiding certain driving situations would be pointless to me
Some other older drivers need to change their driving, but I believe that I am a safe driver and have never thought about the need to change my driving
I am planning to avoid certain driving situations and reducing my driving
I have just recently started to avoid challenging driving situations or drive less
To what extent do you avoid driving under the following conditions?
Not
at a
ll
Not
oft
en
Reas
onab
ly o
ften
Very
oft
en
Avoi
d co
mpl
etel
y
At night in the rain 1 2 3 4 5 In the rain 1 2 3 4 5 When alone 1 2 3 4 5 With distracting passengers 1 2 3 4 5 Parallel parking 1 2 3 4 5

Chapter 10: 227
Not
at a
ll
Not
oft
en
Reas
onab
ly o
ften
Very
oft
en
Avoi
d co
mpl
etel
y
Familiar roads 1 2 3 4 5 Unfamiliar roads 1 2 3 4 5 Freeways 1 2 3 4 5 High traffic roads 1 2 3 4 5 Peak hour 1 2 3 4 5 At the start/end of school time 1 2 3 4 5 At night 1 2 3 4 5 When there is roadworks 1 2 3 4 5 Long distance driving 1 2 3 4 5 Lane changes 1 2 3 4 5 Right turns 1 2 3 4 5 When sun in my eyes 1 2 3 4 5 Roundabouts 1 2 3 4 5

228 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
If you ticked any of the situations above, why do you avoid driving at this situation(s)?
Not
con
fiden
t
Not
com
fort
able
No
need
Oth
er p
leas
e sp
ecify
At night in the rain □ □ □ _________________
In the rain □ □ □ _________________
When alone □ □ □ _________________
With distracting passengers □ □ □ _________________
Parallel parking □ □ □ _________________
Familiar roads □ □ □ _________________
Unfamiliar roads □ □ □ _________________
Freeways □ □ □ _________________
High traffic roads □ □ □ _________________
Peak hour □ □ □ _________________
At the start/end of school time □ □ □ _________________
At night □ □ □ _________________
When there is roadworks □ □ □ _________________
Long distance driving □ □ □ _________________
Lane changes □ □ □ _________________
Right turns □ □ □ _________________
When sun in my eyes □ □ □ _________________
Roundabouts □ □ □ _________________

Chapter 10: 229
If you want to, how easy will it be for you to avoid driving at the following conditions?
Very
har
d
Som
ewha
t har
d
Not
har
d at
all
At night in the rain 1 2 3 In the rain 1 2 3 When alone 1 2 3 With distracting passengers 1 2 3 Parallel parking 1 2 3 Familiar roads 1 2 3 Unfamiliar roads 1 2 3 Freeways 1 2 3 High traffic roads 1 2 3 Peak hour 1 2 3 At the start/end of school time 1 2 3 At night 1 2 3 When there is roadworks 1 2 3 Long distance driving 1 2 3 Lane changes 1 2 3 Right turns 1 2 3 When sun in my eyes 1 2 3 Roundabouts 1 2 3

230 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Please rate your current ability in the following conditions (assume daytime driving unless specified otherwise).
Ver
y go
od
Goo
d
Fai
r
Poo
r
To see road signs at a distance 1 2 3 4
To see road signs at a distance (night) 1 2 3 4
To see your speedometer and control 1 2 3 4
To see pavement lines (at night) 1 2 3 4
Avoid hitting curbs or medians 1 2 3 4
See vehicle coming up beside you 1 2 3 4
See object on the road (at night) with glare from light or wet roads
1 2 3 4
Quickly spot pedestrian stepping out from between parked cars 1 2 3 4
Move your foot quickly from the gas to the brake pedal 1 2 3 4
Make an over the shoulder check 1 2 3 4
Quickly find a street or exit in an unfamiliar area or heavy traffic 1 2 3 4
Get in and out of your car 1 2 3 4
Reverse or back up 1 2 3 4
Make quick driving decisions 1 2 3 4
Drive safely (avoid crashes) 1 2 3 4
Please indicate your agreement or disagreement with the following statements.

Chapter 10: 231
Stro
ngly
agr
ee
Agre
e
Disa
gree
Stro
ngly
dis
agre
e
Most of my friends do not drive 1 2 3 4
People who are important to me think I should change my driving behaviours
1 2 3 4
People who are important to me approve of my driving behaviour 1 2 3 4
Giving up driving will save me money 1 2 3 4
Giving up driving will simplify my life 1 2 3 4
Giving up driving will restrict my mobility 1 2 3 4
Giving up driving will restrict my independence 1 2 3 4
Giving up driving will relieve me of unwanted responsibilities 1 2 3 4
Giving up driving will mean letting down people who rely on me 1 2 3 4
Changing my driving is not possible because of my lifestyle 1 2 3 4
Changing my driving is not possible because other people rely on me 1 2 3 4
Changing my driving is not possible because public transportation is not available to me
1 2 3 4
Changing my driving is not possible because I don’t want to use public transportation
1 2 3 4
Changing my driving is not possible because I can’t rely on others to drive me
1 2 3 4

232 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Please rate the experienced stress connected to the following traffic conditions. (Please assume your general everyday driving.)
Heav
y st
ress
Mod
erat
e st
ress
Neg
ligib
le st
ress
No
stre
ss
Driving on slippery road 1 2 3 4
Driving when tired 1 2 3 4 Night driving 1 2 3 4 Coping with competitiveness of other drivers 1 2 3 4
Driving in rush hours 1 2 3 4
Driving in unfamiliar surroundings 1 2 3 4
Driving long distance 1 2 3 4
Coping with carefulness of others 1 2 3 4
Overtaking 1 2 3 4
Parking or reversing 1 2 3 4
Driving in crossings 1 2 3 4 Adjusting to traffic flow 1 2 3 4 Switching lanes 1 2 3 4 Observing traffic signs 1 2 3 4
Driving on highways 1 2 3 4
Merging from side roads 1 2 3 4
Thank you for completing the survey.
Chapter 10: 233
Appendix H
Study 3 Participant Information Sheet

234 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Appendix I
Questionnaire (1)
Feedback and Older Driver Study This survey booklet contains questions about you and your driving practices. All information received will be treated confidentially. Please respond carefully to all questions and remember there are no right or wrong answers. Please tick only one answer unless otherwise specified.
Thank you for your assistance Centre for Accident Research and Road Safety – Queensland (CARRS-Q) Queensland University of Technology (QUT) 130 Victoria Park Road Kelvin Grove Queensland 4059 Australia Email [email protected] Web www.carrsq.qut.edu.au CRICOS No. 00213J

Chapter 10: 235
Office Only IDENTIFICATION NUMBER ___________________ Please answer the following questions (tick only one answer unless otherwise specified) Gender Male Female Your age (Years) _____________________
What is your highest education level? Primary School Secondary Certificate/Diploma Bachelor degree Postgraduate
Is English your native language? Yes No
Do you live: Alone With spouse or partner With family members With friend(s) With paid caregiver Other, please specify
_______________________________________ Do you work (paid or voluntary) at the moment?
Yes, full-time Yes, part-time No
Overall would you say your health is? Excellent Very good Fair Poor Very poor

236 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Are you the main driver in your household? Yes No Shared equally
For approximately how many years you have had your open driver’s licence? _______________________________________
How would you rate the quality of your driving? Would you say it was? Excellent Good Average Fair Poor
Compared to ten years ago, would you say that you drive Much less A little less The same More
How likely is it for you to have a car crash, compared to other people your age? Not likely Somewhat likely Extremely likely
How likely is it for you to have a car crash, compared to yourself ten years ago? Not likely Somewhat likely Extremely likely
How often do you use public transport? Always Frequently Sometimes Rarely Never
How often do you use taxis? Always Frequently Sometimes Rarely

Chapter 10: 237
Never How often do you take rides from family or friends?
Always Frequently Sometimes Rarely Never
How important is it for you to continue to drive? Extremely important Very important Moderately important Somewhat important Not that important
In the past year, have you talked about your driving with any of the following? You can tick more than one.
Your doctor Family members Friends Other, please specify
_______________________________________ Has anyone suggested over the past year that you limit or stop your driving?
No Yes
If you ticked yes, please indicate all that apply Family member Friend Your doctor An eye care professional Other, please specify
_______________________________________ What did you do in response to their suggestion?
Ignored it Made own assessment of ability and decided no action was required Restricted my driving, please specify
_______________________________________
Other, please specify ______________________________________

238 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
_ Whose suggestion regarding change in driving status would you most likely listen to? Please tick only one option
Partner Other family members Doctor Friend Person of authority (e.g. police)
Which of the following could make you consider changing your current driving? (Please tick all that apply)
Medical condition Vision problem Feeling unfit to drive Feeling nervous when driving Feeling uncomfortable when driving If I have a crash If advised by my family If advised by my doctor If my license is revoked Other
_______________________________________ Which of the following statements better describe you?
I am at the point where I am not sure if I should start thinking about ways to avoid certain driving situation or reduce my driving
Avoiding certain driving situations would be pointless to me Some other older drivers need to change their driving, but I believe that I am a safe
driver and have never thought about the need to change my driving I am planning to avoid certain driving situations and reducing my driving I have just recently started to avoid challenging driving situations or drive less

Chapter 10: 239
To what extent do you avoid driving under the following conditions?
Nev
er
Rare
ly
Som
etim
es
Oft
en
Alw
ays
At night in the rain 1 2 3 4 5 In the rain 1 2 3 4 5 When alone 1 2 3 4 5 Parallel parking 1 2 3 4 5 Freeways 1 2 3 4 5 High traffic roads 1 2 3 4 5Peak hour 1 2 3 4 5 At night 1 2 3 4 5 Right turns 1 2 3 4 5 How confident are you in your ability to drive under the following conditions?
Not
at a
ll
Not
ver
y co
nfid
ent
Reas
onab
ly
conf
iden
t
Very
con
fiden
t
Com
plet
ely
Conf
iden
t At night in the rain 1 2 3 4 5 In the rain 1 2 3 4 5 When alone 1 2 3 4 5 Parallel parking 1 2 3 4 5 Freeways 1 2 3 4 5 High traffic roads 1 2 3 4 5Peak hour 1 2 3 4 5 At night 1 2 3 4 5 Right turns 1 2 3 4 5

240 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
How hard would it be for you?
Very
har
d
Som
ewha
t har
d
Not
har
d at
all
To avoid driving in the rain 1 2 3 To avoid driving alone 1 2 3 To avoid reverse parallel parking 1 2 3 To avoid right turns 1 2 3 To avoid driving on freeways 1 2 3 To avoid high traffic roads 1 2 3 To avoid driving in peak hour 1 2 3 To avoid driving at night 1 2 3 To avoid driving at night in the rain 1 2 3
Please rate your current ability in the following conditions (assume daytime driving unless specified otherwise).
V
ery
good
Goo
d
Fai
r
Poo
r
To see road signs at a distance 1 2 3 4
To see road signs at a distance (night) 1 2 3 4
To see your speedometer and control 1 2 3 4
To see pavement lines (at night) 1 2 3 4
Avoid hitting curbs or medians 1 2 3 4
See vehicle coming up beside you 1 2 3 4
See object on the road (at night) with glare from light or wet roads
1 2 3 4
Quickly spot pedestrian stepping out from between parked cars 1 2 3 4
Move your foot quickly from the gas to the brake pedal 1 2 3 4
Make an over the shoulder check 1 2 3 4
Quickly find a street or exit in an unfamiliar area or heavy traffic 1 2 3 4
Get in and out of your car 1 2 3 4
Reverse or back up 1 2 3 4

Chapter 10: 241
Ver
y go
od
Goo
d
Fai
r
Poo
r
Make quick driving decisions 1 2 3 4
Drive safely (avoid crashes) 1 2 3 4
Please indicate your agreement or disagreement with the following statements.
Stro
ngly
dis
agre
e
Disa
gree
Nei
ther
ag
ree
or
disa
gree
Agre
e
Driving a vehicle is pleasurable 1 2 3 4
I am experiencing increasing apprehension about driving 1 2 3 4
I am becoming more concerned about the unsafe behaviours of older drivers
1 2 3 4
Being able to drive is important to me 1 2 3 4
Driving is necessary to my life to give me the flexibility I desire 1 2 3 4
Driving is central to my independence 1 2 3 4
Some people think I should stop driving 1 2 3 4
People close to me disapprove of my driving 1 2 3 4
My friends drive their vehicle regularly 1 2 3 4
The physical demands of driving a vehicle (e.g. turning my head to shoulder check) are becoming a challenge
1 2 3 4
The financial cost of driving and maintaining a vehicle is an increasing concern of mine
1 2 3 4
Parking is becoming more difficult to me 1 2 3 4
I plan to continue driving in the foreseeable future 1 2 3 4
I intend to keep driving when I want to in the near future 1 2 3 4
Giving up driving will simplify my life 1 2 3 4

242 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Giving up driving will restrict my mobility 1 2 3 4 5
Giving up driving will restrict my independence 1 2 3 4 5
Giving up driving will relieve me of unwanted responsibilities 1 2 3 4 5
Giving up driving will mean letting down people who rely on me 1 2 3 4 5
Changing my driving is not possible because of my lifestyle 1 2 3 4 5
Changing my driving is not possible because other people rely on me 1 2 3 4 5
Changing my driving is not possible because public transportation is not available to me
1 2 3 4 5
Changing my driving is not possible because I don’t want to use public transportation
1 2 3 4 5
Changing my driving is not possible because I can’t rely on others to drive me
1 2 3 4 5
Thank you for completing the survey.

Chapter 10: 243
Appendix J
Questionnaire (2)
Feedback and Older Driver Study
Thank you for your assistance
Centre for Accident Research and Road Safety – Queensland (CARRS-Q) Queensland University of Technology (QUT)
130 Victoria Park Road Kelvin Grove Queensland 4059 Australia
Email [email protected] Web www.carrsq.qut.edu.au
CRICOS No. 00213J

244 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
Office Only IDENTIFICATION NUMBER ___________________ Before the drive, were you aware of some of the limitations in your driving (if any) that has been pointed out by the driving instructor?
No Yes, please explain
__________________________________________________________________________________ After the drive, are you more aware of changes in your abilities that could be affecting your driving?
No Yes, please explain
__________________________________________________________________________________ Before the drive, did you think that you need to modify or adjust your driving behaviours?
No Yes, please explain
__________________________________________________________________________________ After the drive, do you think that you need to modify or adjust your driving behaviours?
No Yes, please explain
__________________________________________________________________________________ Before the drive, did you have any concerns in regards to your driving?
No Yes, please explain
__________________________________________________________________________________ Did the feedback you received answered some of these concerns?
No Yes, please explain
__________________________________________________________________________________

Chapter 10: 245
After the drive, how would you rate the quality of your driving? Would you say it was? Excellent Good Average Fair Poor
Would you say that now you will consider seeking more help in regards to your driving (e.g. a driving refresher course, doctor’s consultation)
No Yes Don’t know yet
Now that you have received the driver instructor’s feedback, which statement better describe you?
I will not change my driving, as I believe I am a safe driver and my driving abilities has
not changed. I intend to start monitoring my driving abilities and changing my driving accordingly I intend to start avoiding some challenging driving situations I intend to consider giving up driving altogether
If you want to how hard will it be to reduce or give up driving? Very hard Somewhat hard Not hard at all
If you think giving up driving is not possible, would you say it is because I don’t want to rely on public transportation It will limit my mobility and independence I don’t have family members to rely on to drive me Other family members rely on me Other
________________________________________________________________________

246 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours
In the near future, will you consider? Moving to a senior home or a retirement village,
Yes No
Moving to a place with a better transportation options, Yes No
Depending on other family members and relative to drive you, Yes No
Do you think that this form of feedback could be useful for helping older adults improve their driving abilities?
No Yes
Would you recommend this to any of your friends? No Yes
How can this form of feedback be improved in your opinion? ______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ Overall how would you rate the usefulness of this feedback?
Very useful Somewhat useful A little useful Not at all useful
Thank you for completing the survey.

Chapter 10: 247
Appendix K
Feedback provided by driving instructor

248 The applicability of the Precaution Adoption Process Model in understanding older adults’ self-regulatory driving behaviours