the 21st budapest nephrology school 28, 2014 sadayoshi ito division of nephrology, endocrinology and...
TRANSCRIPT

August 28, 2014
Sadayoshi Ito
Division of nephrology, Endocrinology and Vascular Medicine
Tohoku University School of Medicine
Semmelweis University
The Kidney in Heart Failure
The 21st Budapest Nephrology School

Site of acute renal injuries in heart failure
Necrosis
of mTALVasa recta
Lesions seen in the outer medulla
Gl
Vasa recta bundle
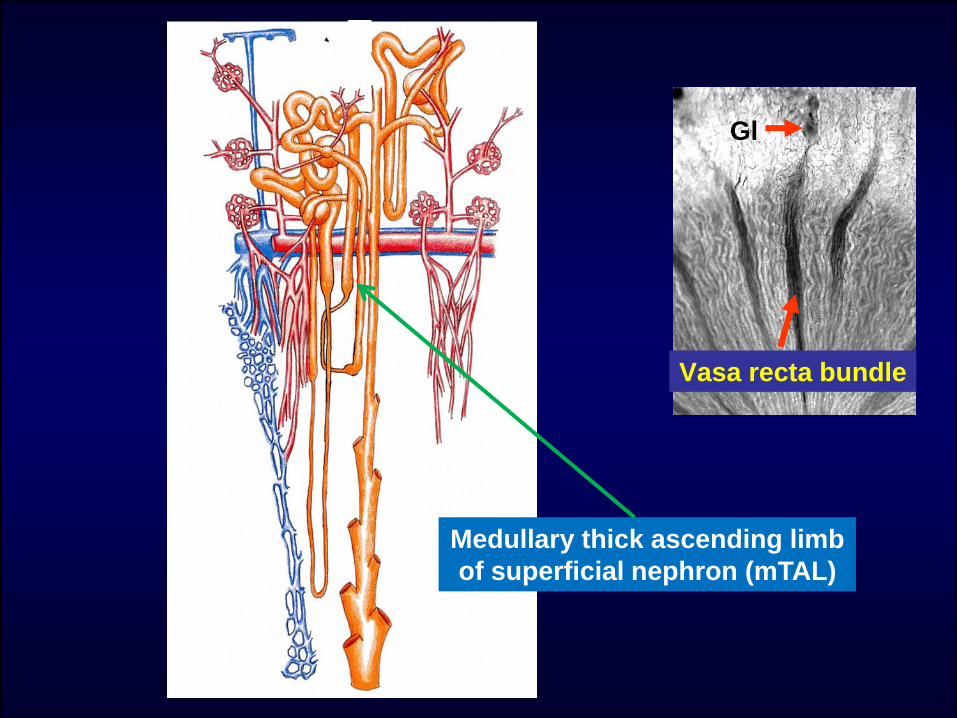
Medullary thick ascending limb
of superficial nephron (mTAL)
Gl
Vasa recta bundle

High Oxygen
Large blood supply
Cortex
Outer medulla
Inner medulla
Vasa recta
Superfcial Gl
Hard work under sever
conditions
Juxtameduulary GL
Large oxygen consumption
(mTAL、PST)
Low oxygen
Small blood supplyNo oxygen consumption
(Thin loop)
Outer medulla: susceptible to ischemic injuries
cortex
Medulla
Hyperglycemia
Acute kidney injury
VR
*

Kidney in Hear Failure
・Alterations in Na handling
・Chronic kidney disease has bad influences
on the prognosis of heart failure;even
microalbuminuria is a predictor of poor
outcomes
• Mechanisms of Na handling in normal and
alterations in heart failure
• Why is microalbuminuria a risk factor?

Responses to salt intake
• Acute and sub-acute responses
• Chronic responses(Adaptations)
-normal-
Repetitions

Medullary BF ↑
Renal response to salt loading (meal)
Sodium homeostasis
Neuro-hormonal changes
(RAS↓, NP↑, PG↑,etc)
GFR↑ Na reabsorption↓
Na excretion↑
Salt intake↑ (meal)
(Ito S, et al: Hypertension
Res 32; 115-121, 2009)
0-90min
Protein intake
90-180min
Pooling in vein,
lymph/tissue

RAS inhibition promotes natriuresis
(Singer DRJ, et al: Am J Physiol Renal Fluid Electrolyte Physiol 266; F89-F93, 1994)
Uri
nar
y So
do
im E
xcre
tio
n μ
mo
l/m
inPlacebo
600
500
400
300
200
100-120 -60 0 60 120 180 240 300
0.9%saline
2L
**
**
*
*P<0.05
**P<0.01
(min)
angiotensinII
Angiotensin II 0.6pmol/kg/min
Acute Na loading:

160
145
130
115
100
160
140
120
100
80
200
160
120
80
40
0
200
160
120
80
40
0
C1 C2 S1 S2 S3 P1 P2 P3
Na loading
Scramble
Decoy
MA
P (
mm
Hg)
%M
BF
U・
V(m
l/m
in/
g kw
t)U
Na・
V(μ
mo
l/m
in/
g kw
t)
A
B
C
D
(Li N, et al: Circ Res 102; 1101-1108, 2008)
**
** * *
*
**
*
*
*
*
C1 C2 S1 S2 S3 P1 P2 P3
Renal responses to acute sodium loading: medullary blood flow
-HIF1α(regulates NO and PG synthesis)-

Chronic responses to high Na intake
• RAS inhibition and increases in renal
cortical blood flow (superficial cortex)
• Increases in GFR in superficial cortex
• Decreased proximal tubular Na
reabsorption
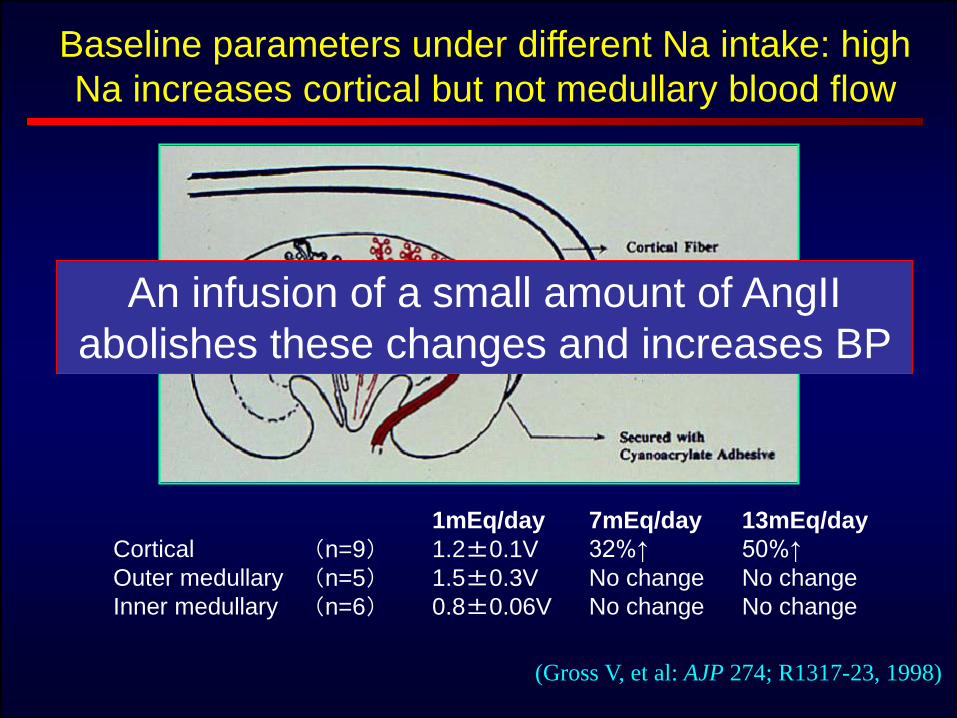
Baseline parameters under different Na intake: high
Na increases cortical but not medullary blood flow
(Gross V, et al: AJP 274; R1317-23, 1998)
Cortical
Outer medullary
Inner medullary
(n=9)(n=5)(n=6)
1mEq/day
1.2±0.1V
1.5±0.3V
0.8±0.06V
7mEq/day
32%↑
No change
No change
13mEq/day
50%↑
No change
No change
An infusion of a small amount of AngII
abolishes these changes and increases BP

Medullary BF ↑
Renal response to salt loading:
Sodium homeostasis
Neuro-hormonal changes
(RAS↓, NP↑, PG↑,etc)
GFR↑ Na reabsorption↓
Na excretion↑
Salt intake↑ (meal)
(Ito S, et al: Hypertension
Res 32; 115-121, 2009)
0-90min
Protein intake
90-180min
Pooling in vein,
lymph/tissue
Low Na diet
GFR↑

Reserve of GFR and RBF (after amino acids infusion)
(RuILope LM, et al: Kidney Int 31:992-2, 1987)
ERPF: effective renal plasma flow、 AA: amino acid
Normal Na diet Low Na diet
160
140
120
100
80
GF
R [m
l/m
in]
700
600
500
400
300
ER
PF
[m
l/m
in]
basekline
*
*
baselineAA
180
200
900
800
AA

Medullary BF ↑
Renal response to salt loading (meal)
Sodium homeostasis
Neuro-hormonal changes
(RAS↓, NP↑, PG↑,etc)
GFR↑ Na reabsorption↓
Na excretion↑
Salt intake↑ (meal)
(Ito S, et al: Hypertension
Res 32; 115-121, 2009)
0-90min
Protein intake
90-180min
Pooling in vein,
lymph/tissue BP

211
Renal perfusion pressure (mmHg)
RBF, GFR and pressure natriuresis
GFR
RBF
0 40 80 120 160 200 240 280
natriuresis

Pressure natriuresis and renal hemodynamics
(Cowley AW Jr.: Physiol. Rev 72(1); 231-300, 1992)
140
100
60
50 75 100 125 150 50 75 100 125 150
50
30
10
12
8
4
50 75 100 125 150
AP
140
100
60
50 75 100 125 150 50 75 100 125 150
20
12
4
50 75 100 125 150
12
8
4
50
30
10
0 2 4 6 8
cortex
medulla
AP
RENAL BLOOD FLOW
(%control)
RENAL BLOOD FLOW
(% control)VASA RECTA PRESSURE
(mmHg)
INTERSTITIAL PRESSURE
(mmHg) ∆INGERSTITIAL PRESSURE
(mmHg)
∆UNaV
(μEq/min/gkwt)
INTERSTITSAL PRESSURE
(mmHg)
PTC PRESSURE
(mmHg)
AP AP
AP AP AP

Medullary BF ↑
Renal response to salt loading (meal)
Sodium homeostasis
Neuro-hormonal changes
(RAS↓, NP↑, PG↑,etc)
GFR↑ Na reabsorption↓
Na excretion↑
Salt intake↑ (meal)
(Ito S, et al: Hypertension
Res 32; 115-121, 2009)
0-90min
Protein intake
90-180min
Pooling in vein,
lymph/tissue BP
Pressure natriuresis as
a goalkeeper of Na
homeostasis

Medullary BF ↑
Renal response to salt loading:
Sodium homeostasis
Neuro-hormonal changes
(RAS↓, NP↑, PG↑,etc)
GFR↑ Na reabsorption↓
Na excretion↑
Salt intake↑ (meal)
(Ito S, et al: Hypertension
Res 32; 115-121, 2009)
0-90min
Protein intake
90-180min
Pooling in vein,
lymph/tissue
Heart failure
GFR↑
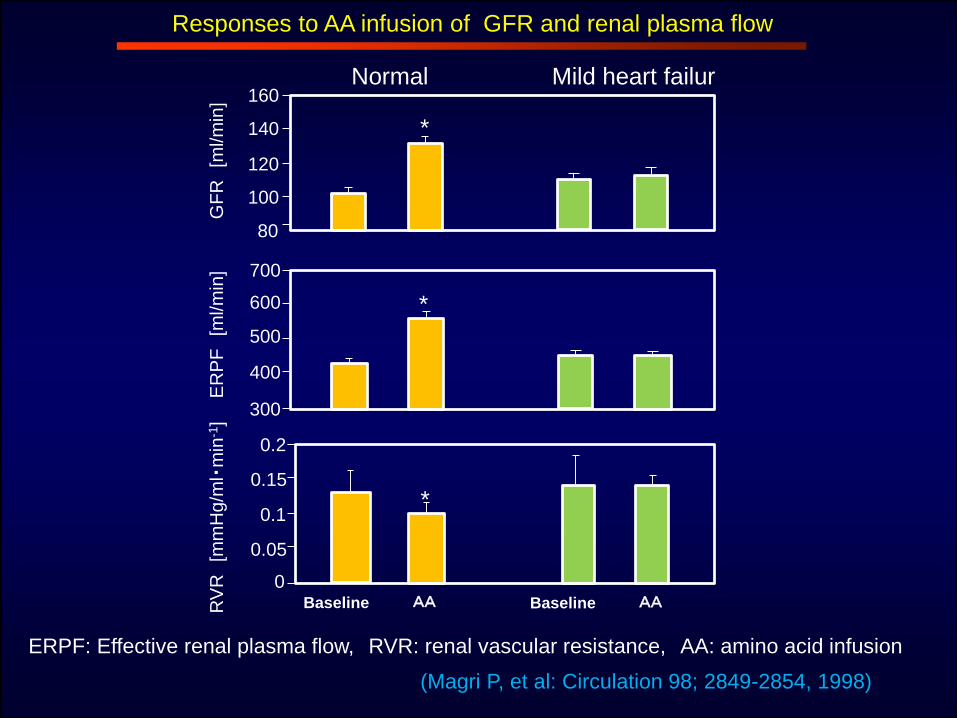
Responses to AA infusion of GFR and renal plasma flow
(Magri P, et al: Circulation 98; 2849-2854, 1998)
Normal Mild heart failur160
140
120
100
80G
FR
[ml/m
in]
700
600
500
400
300
0.2
0.15
0.1
0.05
0
ER
PF
[ml/m
in]
RV
R[m
mH
g/m
l・m
in-1
]
Baseline AA
*
*
*
Baseline AA
ERPF: Effective renal plasma flow, RVR: renal vascular resistance, AA: amino acid infusion

Cumulative Na balance during sodium loading
(Volpe M et al.Hypertension 30: 168-76, 1997)
Sodiu
m
Inta
ke(m
mol)
Base day0
100
200
300
1 2 3 4 5 6 7 8
Normal(n=10)
Mild heart failure, untreated(n=10)
Mild heart failure, ACEI(n=6)
0
100
200
300
400

Effects of Na loading on GFR and tubular function
(Volpe M et al: Hypertension 30: 168-76, 1997)
Normal Mild heart failure
GFR(m
l/m
in)
250100250100
150
130
110
90
GFR
FE
K(%
)
4
12
8
*
*
∆
100 250 200 250
(mmol/day)
Reflects proximal tubular reabsorption
(under maximal water diuresis)
Heart failure・not simple impairment of
sodium excretion
・some Na-retaining mechanism
is activated by sodium load
Salt toxicity

Superficial nephron
Midcortical nephron
Juxtamedullary nephron
Outer stripe
Inner stripe
CHF
cortex
Outer
medulla
Inner medulla
Whole GFR
15% decrease
35% decrease
Increase in GFR
Reabsorption by mTAL
(O2 consumption)

Measurement of NO/ROS in
microperfused mTAL
tip
High Na Low Na
Laser beam
fluorescence
Exchange

Increased Na reabsorption enhances
O2-, but reduces NO activity in mTAL
(Abe M, et al: Am J Physiol Renal Physiol 291; F350-357, 2006)
O2- NO

Measurement of NO/ROS in tissue strip
kidney
.
500 mm
OMDVR
GlmCX
OM
500mm
V Recta
GlCX
OM
.
OMDVR
mTAL
100 mm
V Recta
mTAL
100mm
mTAL
50mmV Recta
(Mori T et al. Hypertension 2002
Dickhout JG, Mori T et al. Circ Research 2002
Mori T et al. Hypertension 2003
Cowley AW,Jr, Mori T et al. Am J Physiol. 2003
Mori T et al. Hypertension 2004)
A single layer of
mTAL and vasa recta

Tubulo-Vascular Crosstalk
Descending
Vasa recta Ang II
Ang II
Ang II
Ang II
Ang II Ang II
mTAL
[NO]i
NOS
X
[O2-]i
NAD(P)H
X[NO]i
(Dickhout JG et al. Circ Research 2002
Mori T et al. Hypertension 2003)
NOS
[NO]i
[O2-]i
NAD(P)H
[O2-]i
X
NaCl

S Ml
0
10
20
30
40
Cotex
Myocardial infarctSham‐operated
Outer medulla
NKCC2 in mTAL increases in heart failure
mRNA Immunoblots
(Nogae S et al: Kidney Int. 57; 2055-2063, 2000)
130kD
BS
C1 m
RN
A,
am
ol/μ
g R
NA
ACEi no effect

• Attenuated pressure natriuresis and Na
retention
• In heart failure, medullary blood flow does
not increases by acute sodium loading
• α-hANP increases medullary blood flow in
addition to other effects
Importance of Medullary Blood
flow in heart failure

4
3
2
1
0
Fra
ction o
f S
ham
Sham CHF
1.5
1.0
0.5
0.0
Fra
ction o
f C
HF
CHF DNX-CHF
*
#
SHAM CHF CHF DNX-CHF1 2 3 4 5 6 1 2 3 4 5 6 1 2 3 4 5 6 1 2 3 4 5 6
(Torp M, et al: Acta Physiol 204; 451-459, 2012)
Values are mean ± SE. n = 6 in all groups.*P < 0.05 (vs. SHAM). #P < 0.05 (vs. CHF).
Renal denervation inhibits NKCC2 overexpression in CHF

8
6
4
2
060 100 140 180
8
6
4
2
060 100 140 180
% H
2O
Excre
tion
% N
a E
xcre
tion
RPP mmHg RPP mmHg
*
* P<.05
Denervated, N=7
Innervated, N=6
*
*
Pressure natriuresis and renal SNS
(Roman RJ, et al: Am J Physiol Renal Physiol 248; F190-F198, 1985)

Decreased cardiac out put
Ang II
Water and Na retention
ADH
SFN-GFR JMN-GFR
NKCC2 (mTAL)
PT reabsorptionMBF
DT, CD reabsorption
SNS RAAS RBF
(TVC)
Renal functional alterations in heart failure
ROS
aldosterone
SFN, superficial
JMN, jutamedullarury
TVC, tubulo-vascular crosstalk

Kidney in Hear Failure
・Alterations in Na handling
・Chronic kidney disease has bad influences
on the prognosis of heart failure;even
microalbuminuria is a predictor of poor
outcomes
• Mechanisms of Na handling in normal and
alterations in heart failure
• Why is microalbuminuria a risk factor?

Kralik PM. Am J Pathol 175:500-5009, 2009
Albuminuria originates only from a small fraction of nephrons
Albumin immunohistochemistry

Perforating arties
Arteriolar damages
Albumin leakage
Strain vessels
・High pressure
・Pulsatile pressure
・High vascular tone
Arcuate artery
albumin(-)
Microalbuminuria
JMN

50 mmHg
Albumin leakage
Albuminuria: impaired medullary circulation
Glomerular HT
Vasa recta controlling
medullary blood flow
Pressure natriuresis
Na retention

Albuminuria
• Impaired medullary circulation, and
pressure natriuresis: Na retention
• Worse outcomes in heart failure:

Perspectives
• Na restriction
• Improve cardiac function
• Renal artery stenosis
• RAAS inhibition: starting low dose, watch BP
• Inhibition of proximal tubular reabsorption:αhANP, increase RBF, NEP inhibitor, adenosine A1 antagonist
• Improve medullary circulation:αhANP, some Ca antagonists (?), NEP inhibition, etc
• Improvement of anemia: Hb 10-11(12)g/dl

急性圧利尿曲線
2.0
腎灌流圧
1.0
0.5
0
コントロール
Na排泄量
尿中
(伊藤貞嘉: Hypertension Frontier 7, 2004)
単離灌流腎In vitro

慢性的食塩摂取量と血圧の関係(慢性圧利尿曲線)
300
200
100
Na排泄量(摂取量)
尿中
50 100 150 200
健常者食塩非感受性高血圧
食塩感受性高血圧
平均血圧(mmHg)
(mmol/日)

急性圧利尿曲線とそれに及ぼすRASとNP系の影響
2.0
血圧
1.0
0.5
0
NP(+)
コントロール
AⅡ(+)
AⅡ(++)
Na排泄量
尿中
(伊藤貞嘉: Hypertension Frontier 7, 2004)
糸球体濾過開始
尿細管による再吸収抑制

急性圧利尿曲線から慢性圧利尿曲線(食塩摂取と血圧)
A
2.0
血圧
1.0
0.5
0
B
C´C
D
NP(+)
コントロール
AⅡ(+)
AⅡ(++)
Na排泄量
尿中
(伊藤貞嘉: Hypertension Frontier 7, 2004)
食塩感受性が大なほど揺れ幅が大きい