that’s unconscionable! - center for bioethics and health law
TRANSCRIPT

Learning Objectives
n Define unconscious (implicit) bias n List types of unconscious bias. n Define Health equity and list common
clinical effects of unconscious bias. n Identify micro-aggressions and micro
validations n Identify three strategies to reduce
unconscious bias in the workplace.

Human mind usage
Source: Journal Psyche
Storage of recent memories. AVAILABLE for quick recall.
Storage of long term memories. NOT AVAILABLE for recall
Ability to focus & differentiate real from what is not real.

Understanding bias
n We rely on mental shortcuts to simplify the world around us.
n These are “schemas” we have accumulated over a lifetime.
n We use these to evaluate people and situations around us.
n Constant and ongoing and at the level of the unconscious mind.

Seminal paper
n “Much of our social behavior is driven by learned stereotypes that operate automatically—and therefore unconsciously—when we interact with other people.”
Greenwald, Anthony G. and M. R. Benaji. Implicit Social Cognition: Attitudes, Self-Esteem and Stereotypes (American Psychological Review, 102.4 (1995): 4-27
Implicit cognition & bias
n Past experiences leave a residual effect that skews perspective and decision making.
n The influential earlier experience is not remembered —that is, it is unavailable to self-report or introspection
n While taking a mental shortcut, we make the wrong turn.
n Even people who very much want to and pride themselves on being impartial can fall prey to these mental detours and arrive at the wrong place.
Measuring implicit bias n The Harvard Implicit Association Test n reveals racial bias by measuring the
amount of time it takes an individual to make an association between two concepts displayed as either words or images.
n might take longer to associate the word “good” with a in-group face than with a out-group face.

Common human errors in implicit cognition that skews patient care

Stereotyping
n An oversimplified, overgeneralized view (usually pejorative) of someone who is from a different group, that do not account for individual differences. – E.g. Sickle cell patients – Homeless patients.

In-group favoritism n We unconsciously and automatically tend to be less
generous to people of a different race than people from our own race.
n White and Black subjects were presented with video clips depicting white, black, and unfamiliar violet-skinned hands being either painfully penetrated by a syringe or being touched by a Q-tip. (Azevedo RT, Human Brain Mapping, 2013)
n fMRI: Autonomic reactivity and anterior insula activity was greater for the pain experienced by own-race compared to that of other-race (Azevedo RT, Human Brain Mapping, 2013)

Fundamental attribution error
n Clinicians may be overly inclined to view the patient’s plight as one brought on by carelessness, foolishness, misbehavior, or naiveté. – “frequent flyers”

Escalation of commitment
n People will make irrational decisions to justify actions they have already taken. – Starting a line of treatment that proves to be
ineffective, but refusing to abandon it.

Confirmation Bias
n The tendency to search for or interpret information and behaviors in a way that confirms what we already believe.
n When they encounter counterevidence, people tend to implicitly counter argue against that evidence, therefore strengthening their favorable feelings toward their belief

Health equity and clinical effects of unconscious
bias.

Lofty Goal of Health Equity
n “To attain the highest level of health for all people” (Healthy People 2020)
1. Requires valuing everyone equally 2. Implementing focused and “ongoing
societal efforts to address avoidable inequalities, historical and contemporary injustices, and the elimination of health and health care disparities.”
Are we there yet?
n Health equity is achieved if we have: 1. Equity of access, 2. Equity of treatments, 3. Equity of outcomes
n Health equity is like the horizon n A sad weakness of the health care system

Clinicians’ perceptions n 4 academic medical centers in Atlanta and Boston; n 287 IM/EM residents randomized to either a black or white
vignette patient for acute coronary syndrome. n Physicians reported no explicit preference for white versus
black patients or differences in perceived cooperativeness. n IATs revealed implicit pro-White preference (mean IAT score
= 0.36, P < .001) n Implicit stereotypes of black Americans as less cooperative
with medical procedures (mean IAT score 0.22, P < .001), and less cooperative generally (mean IAT score 0.30, P < .001).
n As physicians' pro-white implicit bias increased, so did their likelihood of treating white patients and not treating black patients with thrombolysis (P = .009).

Unconscious bias ! Health disparities
n In CKD patients, African American patients had 71% lower odds of receiving a prescription of oxycodone than white patients (P < .001). (Meghani SH, JCO, 2014)
n Metastatic cancer patients: found that only 35% of racial minority patients received the appropriate prescriptions—as established by the World Health Organization guidelines—compared with 50% of nonminority patients --Cleeland CS, et al Ann Intern Med. 1997
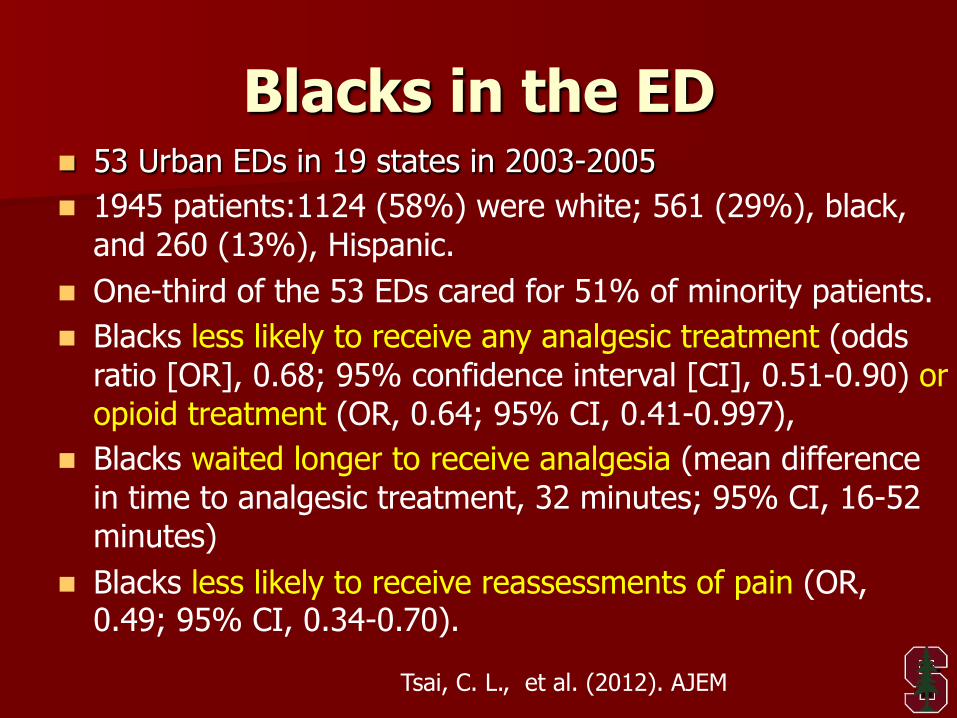
Blacks in the ED n 53 Urban EDs in 19 states in 2003-2005 n 1945 patients:1124 (58%) were white; 561 (29%), black,
and 260 (13%), Hispanic. n One-third of the 53 EDs cared for 51% of minority patients. n Blacks less likely to receive any analgesic treatment (odds
ratio [OR], 0.68; 95% confidence interval [CI], 0.51-0.90) or opioid treatment (OR, 0.64; 95% CI, 0.41-0.997),
n Blacks waited longer to receive analgesia (mean difference in time to analgesic treatment, 32 minutes; 95% CI, 16-52 minutes)
n Blacks less likely to receive reassessments of pain (OR, 0.49; 95% CI, 0.34-0.70).
Tsai, C. L., et al. (2012). AJEM

Pain care disparities.
n Black Americans are systematically undertreated for pain relative to White Americans.
n PNAS Study by Hoffman et al n Lay white people strongly endorsed false beliefs about
biological differences reported lower pain ratings for a black (vs. white) target.
n Half of a sample of white medical students and residents endorsed these beliefs.
n Doctors who endorsed these beliefs rated the black (vs. white) patient's pain as lower and made less accurate treatment recommendations
Hoffman KM. PNAS, Apr2016.

Identify micro-
aggressions and micro validations
Science of Micro-Communication n In an encounter: Small packets of
interaction occur like a tennis volley – Transfer of information – Micro-aggressions – Micro-validations
n The micro-validations and micro-aggressions moderate how patients process the information and act upon it.
n The ratio is important.

Micro-aggression
A subtle but offensive comment or action that is often unintentional or unconsciously reinforces a stereotype

Micro-validations
n Micro-validations are the anti-dote for micro-aggressions.
n Small verbal and non-verbal responses that indicate understanding and support of the other persons plight.

Thought exercise 3
We are going to view several micro-interactions. Your task: Diagnose each clip: Is it a micro-aggression or a micro-validation? Shout it out.

Micro-communication exercise (30 seconds)

Micro-communication exercise (11 seconds)

Micro-communication exercise (27 seconds)
Micro-communication exercise (24 seconds)

Micro-communication exercise (9 seconds)

Micro-communication exercise (16 seconds)

Micro-communication exercise (22 seconds)

Micro-communication exercise (31 seconds)

Micro-communication exercise (25 seconds)

Micro-communication exercise (22 seconds)

Micro-communication exercise (25 seconds)

Micro-communication exercise (19 seconds)

Micro-communication exercise (19 seconds)

Individual strategies
n Gain knowledge n Self-assessment of attitudes: present state
and desired future state n Feedback from a trusted source.

Perspective-taking n Perspective-taking is the cognitive, analytic process by
which an individual views a situation from another's point-of-view.
n Empathy is “affective perspective-taking”: is the capacity to feel or understand the emotions of another person from within the other being's frame of reference – Consideration of an out-group member increases identification
with out-group members – Reduces stereotype bias in the moment – Increases willingness to interact with out-group members

Cloaking exercises
n Checking decisions for bias by imagining how we would evaluate the stigmatized person if he or she belonged to a different, non-stigmatized social group.
Organizational strategies
n Regular diversity self-assessment n Routine patient diversity data capture and
review regularly for patterns and gaps n Diversity recruitment n Careful on-boarding. *** n Trainings– immersive small group
exercises. n Beware of burdensome training mandates.

Final thought exercise Practice a micro-validation: What to do? 1. Turn to a neighbor 2. Ask a question to them (their work, commute, office
space, clinical load, research projects, upcoming deadline etc.)
3. When they answer, respond with a micro-validation
Remember: A micro validation should be subtle, very short, genuine. Avoid personal comments about physical attributes.
