temporary cutaneousureterostomy in the … · out at frequent intervals by the nursing staff to...
TRANSCRIPT

Arch. Dis. Childh., 1963, 38, 161.
TEMPORARY CUTANEOUS URETEROSTOMYIN THE MANAGEMENT OF
ADVANCED CONGENITAL URINARY OBSTRUCTION*BY
J. H. JOHNSTONFrom Alder Hey Children's Hospital, Liverpool
The most extreme effects of chronic urinaryobstruction are seen in the child who has suffereda severe lower tract obstruction during foetalexistence. In such cases the renal tract is dilated,sometimes dysplastic and often decompensated, sothat urinary stasis commonly persists after theremoval of the original obstruction. One has todeal with a urinary system which has in manyinstances never been normal and which, in most, isquite incapable of approaching normality. Somecases have insufficient renal tissue to maintain life,but many, if given the chance, have the capacityfor considerable improvement in the function bothof the urinary tract musculature and of the renalparenchyma. The great danger to the patient witha low renal reserve and urinary stasis is complicatinginfection; this is often present at the time of diagnosisor is quickly introduced by instrumentation or byoperation, and if free urinary drainage is notestablished a rapidly fatal pyelonephritis may veryreadily develop.Rickham (1962) has described our unhappy
experience in Liverpool, particularly in infants, withsuprapubic cystostomy in the management ofadvanced lower urinary obstruction. These poorresults are due partly to the presence of the tubewhich perpetuates and aggravates infection, andpartly, I suspect, to hypotonic ureters findingevacuation even more difficult when a very hyper-trophied bladder is empty and contracted. Tubenephrostomy has also, in my experience, beenunsatisfactory with the hydronephrotic kidney;although adequate drainage is obtained, there isagain the great disadvantage of the indwellingcatheter.The ideal method of prolonged decompression in
advanced urinary obstruction should drain theupper tract directly without the use of tubes. Atechnique that fulfils these criteria, and of which
* A paper read at a meeting of the British Association of PaediatricSurgeons in London, September 1962.
I have had experience in 10 patients with severelydamaged urinary tracts from a variety of causes,is that of temporary cutaneous ureterostomy withlater restoration of the normal urinary route afterthe obstruction has been removed. Six of thepatients were infant boys with urethral valves;four of them had bilateral ureterostomy and twounilateral since these each had only one functioningkidney. One of these children died of staphylo-coccal pneumonia; his renal function was extremelypoor, the para-aminohippuric acid (PAH) clearancebeing only 2- 5 %O of normal. An infant girl withbilateral ectopic ureteroceles obstructing all fourduplicated ureters and with only one double kidneyfunctioning had a unilateral double ureterostomy:a girl of 21 months had a unilateral ureterostomyfor an obstructive megaureter affecting a solitary,very poorly functioning kidney: a 3p-year-old boyhad bilateral ureterostomy for a congenital obstruc-tion of the penile urethra, and an infant boy hadbilateral ureterostomy for an undiagnosed temporaryurinary obstruction. In 13 instances in sevenpatients the ureterostomy was of the loop typedescribed by Stephens (F. D. Stephens, 1960,personal communication), the ureter being exposedextraperitoneally through a small high gridironincision, mobilized, brought in continuity to thesurface and opened on its anterior aspect (Fig. 1).The elongated ureter that results from prenatalurinary obstruction can usually be exteriorizedeasily without tension and without endangeringits blood supply. In three instances in three patientsthe ureterostomy was of the terminal type, theureter being divided near the bladder and theproximal end brought to the surface. In two ofthese cases the obstruction lay at the uretero-vesical junction. The ureter reaches the skinsurface much more readily as a terminal stoma,but closure of this type of ureterostomy requiresreimplantation of the ureter to the bladder, andwhen this would not be required in any case for therelief of the original obstruction or for the cure of
161 5B
copyright. on January 2, 2020 by guest. P
rotected byhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.38.198.161 on 1 A
pril 1963. Dow
nloaded from

ARCHIVES OF DISEASE IN CHILDHOOD
FIG. I.-Bilateral loop ureterostomies in infant boy with urethralvalves.
vesico-ureteric reflux, the loop ureterostomy isobviously preferable. With the exception of one
patient who will be described later, local complica-tions with either type of ureterostomy were minimal.Stomal stenosis was not seen in any case; some
FIG. 2.-Intravenous pyelogram of Case 1 before resection ofurethral valves and bilateral ureterostomy closure. Although theright ureterostomy drained urine the kidney did not concentratesufficiently to appear on the radiograph; left hydronephrosis and
hydroureter to site of ureterostomy.
degree of ureteric prolapse occurred with one loopureterostomy.
Ureterostomy may not immediately allowadequate emptying of a severely dilated upper renaltract. The kidney and ureter are, however, easilyevacuated by bimanual compression and massageof the loin, and this manoeuvre should be carriedout at frequent intervals by the nursing staff toprevent urinary accumulation. As the tone of thepelvic and ureteric muscle recovers the residualurine diminishes and one can appreciate improve-ment in ureteric peristalsis and emptying by repeatedimage intensifier observation.The renal function in the children in this series
has shown, in varying degrees of severity, the tubuledefects of chronic back pressure, the most obviousfeatures being uraemia, acidosis and obligatorypolyuria with hyposthenuria. In five kidneys inthree patients clearances of urea, creatinine andPAH were estimated shortly after the performanceof ureterostomy and again, several weeks later,before its closure. In none did the tests show anysignificant change so that there is no objectiveproof that any recovery of renal function occurredin these cases as a result of drainage. That recoverycan and does occur, however, is implied by theclinical improvement that ureterostomy has pro-duced in all patients. This was particularly strikingin three children in whom ureterostomy was per-formed as a secondary procedure when othermethods of drainage had failed to be effective, andthey were extremely ill. In most cases clinicalrecovery appeared shortly after ureterostomydrainage was instituted, but in one it was consider-ably delayed and this case is important in showingthat one must avoid being unduly hasty in diag-nosing irrecoverable renal damage and abandoninghope of survival.
Case Reports
Case 1. A boy with urethral valves was admittedat the age of 6 days with convulsions. His bladder andkidneys were palpably distended. The blood urea was178 mg./l00 ml. and the urine was infected with E. coli.Bilateral loop ureterostomies were performed, but thechild's general condition remained extremely poor. Hewas persistently uraemic and acidaemic and needed a verylarge fluid intake and urinary output to maintain him inanything approaching a reasonable clinical and bio-chemical state; at the age of 5 weeks this fluid exchangeamounted to a daily intake of 1,300 ml. and an outputof 840 ml., nearly tlhree times the normal volumes forhis size. He had repeated attacks of vomiting anddiarrhoea and was quite unable to take orally the copiousintake he required so that intravenous infusions wereneeded almost continually. At the age of 4 months hisweight was still below his birth weight of 7 lb. (3 4 kg.).
162
copyright. on January 2, 2020 by guest. P
rotected byhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.38.198.161 on 1 A
pril 1963. Dow
nloaded from
TEMPORARY CUTANEOUS URETEROSTOMYThen, quite suddenly, he improved, began to gain weightand was able to maintain homeostasis by oral intake alone.His intravenous pyelogram at this time showed that,although the right ureterostomy was draining urine, thekidney did not concentrate the dye; on the left side therewas hydronephrosis and hydroureter (Fig. 2). Theurethral valves were resected by an open, retropubicoperation, and by the age of 6 months the ureterostomieswere closed and the child was micturating normally.He was last seen at the age of 18 months when his clinicalcondition was excellent; his blood urea was 54 mg./100 ml. and his urine was uninfected and free from pus.
Comment. It is likely that part of the clinicalimprovement that occurs in such cases is due notto the recovery of renal function itself but to thedrainage of infection and the relief therefore ofsuch general septic and toxic effects as vomiting,diarrhoea, impaired hepatic function, often withjaundice and depressed marrow activity resultingin anaemia or, as in one of my cases, in severethrombocytopenia with haemorrhages.
Besides its benefit to the upper urinary tract,temporary ureterostomy is of value in restoring thefunction of a chronically distended bladder. Thiswas illustrated by a boy with an unusual type ofurethral obstruction associated with skeletal abnor-malities.
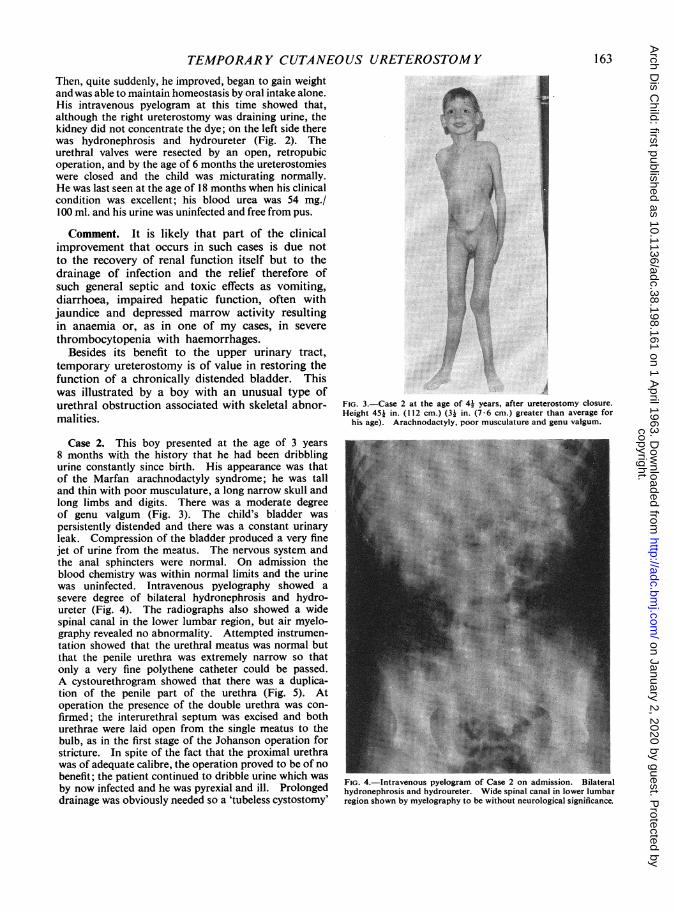
Case 2. This boy presented at the age of 3 years8 months with the history that he had been dribblingurine constantly since birth. His appearance was thatof the Marfan arachnodactyly syndrome; he was talland thin with poor musculature, a long narrow skull andlong limbs and digits. There was a moderate degreeof genu valgum (Fig. 3). The child's bladder waspersistently distended and there was a constant urinaryleak. Compression of the bladder produced a very finejet of urine from the meatus. The nervous system andthe anal sphincters were normal. On admission theblood chemistry was within normal limits and the urinewas uninfected. Intravenous pyelography showed asevere degree of bilateral hydronephrosis and hydro-ureter (Fig. 4). The radiographs also showed a widespinal canal in the lower lumbar region, but air myelo-graphy revealed no abnormality. Attempted instrumen-tation showed that the urethral meatus was normal butthat the penile urethra was extremely narrow so thatonly a very fine polythene catheter could be passed.A cystourethrogram showed that there was a duplica-tion of the penile part of the urethra (Fig. 5). Atoperation the presence of the double urethra was con-firmed; the interurethral septum was excised and bothurethrae were laid open from the single meatus to thebulb, as in the first stage of the Johanson operation forstricture. In spite of the fact that the proximal urethrawas of adequate calibre, the operation proved to be of nobenefit; the patient continued to dribble urine which wasby now infected and he was pyrexial and ill. Prolongeddrainage was obviously needed so a 'tubeless cystostomy'
:.. ---. *S
FIG. 3.-Case 2 at the age of 4? years, after ureterostomy closure.Height 45i in. (112 cm.) (3. in. (7-6 cm.) greater than average for
his age). Arachnodactyly, poor musculature and genu valgum.
FIG. 4.-Intravenous pyelogram of Case 2 on admission. Bilateralhydronephrosis and hydroureter. Wide spinal canal in lower lumbarregion shown by myelography to be without neurological significance.
163
copyright. on January 2, 2020 by guest. P
rotected byhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.38.198.161 on 1 A
pril 1963. Dow
nloaded from

1ARCHIVES OF DISEASE IN CHILDHOOD
FIG. 5.-Cystourethrogram of Case 2. Obstructive duplication ofpenile urethra.
was c*rried out. It proved, however, to be extremelydifficult to bring the thick-walled bladder to the surfacewithout tension and because of subsequent retractionand stenosis of the stoma with inadequate drainage itbecame necessary to insert a suprapubic catheter.Repeated attempts were made to induce micturition, butwhen the catheter was removed the patient again dribbledfrom the urethra and leaked suprapubically, and hisgeneral condition became progressively worse. Fourteenweeks after his admission bilateral loop ureterostomieswere performed. This led to an almost immediateclinical improvement and the child went home threeweeks later wearing a collecting appliance. The uretero-stomies were closed after 13 weeks when he was able tomicturate quite well on demand, although he leakedurine between voidings. Gradually, his control improvedso that now, 11 months after the ureterostomy closure,he is quite dry by day but often wet at night. Theurine is now uninfected. He has yet to have the secondstage urethral reconstruction operation.
Comment. Persistent bladder dysfunction afterthe removal of a congenital urinary obstructionoccurs, as in the above patient, particularly in thecase in which the diagnosis has been delayed. It isprobably partly due to diminished vesical toneresulting fi-om prolonged overdistension, as is seenwith the atonic obstructed bladder of adults, but
another, possibly more important, factor in itscausation is such a child's complete lack of experi-ence of the normal sensations associated withbladder filling and emptying so that he may needa long period of self-education of the neural arcsconcerned before normal micturition and urinarycontrol is possible. A period of ureterostomydrainage serves the dual purpose of helping torestore normal bladder activity and of protectingthe upper urinary tract during the process.
In the case of acquired urinary disease the uretersdo not come safely to the surface as loops andfailure to diagnose what was probably an exampleof this rare cause of urinary obstruction in infancyled to local ureterostomy complications.
Case 3. A boy aged 6 weeks was admitted to hospitalin an almost moribund state with convulsions and deepjaundice. The bladder was tensely distended above theumbilicus and both kidneys were enlarged. The bloodurea was 150 mg./100 ml. and the serum bilirubin28 mg./100 ml. The urine obtained by catheterizationwas macroscopically purulent and grew E. coli on culture.I thought that the child must have urethral valves anddecided to perform bilateral ureterostomies. Cystoscopyand cystography were omitted. When the ureters wereexposed they were found to be quite dilated, but thinwalled and straight. Loop ureterostomies were done,but although the ureters could be brought to the surfacewithout tension, the mobilization led to necrosis of partof each ureter adjacent to the ureterostomy; the child'spoor general condition undoubtedly contributed to thedevelopment of this complication. Later investigationsshowed that the renal enlargement was due to severebilateral acute pyelonephritis with only moderate hydro-nephrosis and that the bladder was slightly trabeculated,with bullous cystitis, but failed to demonstrate anyresidual urinary obstruction whatever. A left nephrec-tomy was required later because of septic destructionof the kidney, but the child ultimately recovered andleft hospital micturating normally. In retrospect, itappears likely that the obstruction in this case was purelyinflammatory, due to a prostatitis or a basal cystitis.
DiscussionClosure of the terminal ureterostomy requires
reimplantation of the ureter to the bladder and it isdifficult, in my experience, to reimplant a verydilated, thick-walled ureter and avoid with certaintyand permanently subsequent vesico-ureteric refluxwith its consequences of persistent infection andprogressive renal deterioration. The best chance ofachieving a competent valve with such a ureter lies,I believe, in performing a direct anastomosis of theureter to the bladder high on its posterior wall andsupplementing the stoma with a long Bischoff
164
copyright. on January 2, 2020 by guest. P
rotected byhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.38.198.161 on 1 A
pril 1963. Dow
nloaded from

TEMPORARY CUTANEOUS URETEROSTOMYostioplasty. I am not, however, in a position toquote long-term results of this technique. In thecase of the Ioop ureterostomy, the exteriorizedureter becomes oedematous and thickened, but onemust resist, during the closure operation, thetemptation to make things easier and neater byresecting this part of the ureter and performing anend-to-end anastomosis. One usually finds thatthe ureter below the ureterostomy is appreciablysmaller than the portion above, and in two casesin which the ureterostomies were resected, intra-venous pyelography several months after the closureoperation showed that this luminal disparity per-sisted with, in one of them, increased dilatation ofthe kidney and the upper part of the ureter. In thiscase, where resection of the ureter was unavoidablesince part of it underwent necrosis, retrogradepyelography of the sole remaining kidney six monthsafter ureterostomy closure showed considerabledelay in emptying of the ureter above the anas-tomosis. After one and a half hours very littleof the dye injected into the renal pelvis had passedinto the lower ureter and bladder (Fig. 6). Underthe image intensifier one could see vigorous peri-stalsis to the site of the anastomosis, but no dyewas seen to pass through within half an hour of theinjection; one also had the impression of reversedperistalsis from this point. The delay at theanastomosis is due, I believe, not to any localnarrowing, which cannot be significant with adilated ureter, but to a failure of transmission of theperistaltic wave consequent on ureteric resection,a phenomenon that Murnaghan (1959) found tooccur on occasion after complete division andreanastomosis of the ureter in the dog. Thisfunctional obstruction at the site of ureterostomyclosure should be avoidable by retaining continuityof the ureteric musculature and this proved to beso in Case 2. This boy's ureterostomies wereclosed by mobilization of the ureter and transversesuture of the stoma, leaving the posterior wall intact.An intravenous pyelogram 10 months later showedthat there was still severe dilatation of both kidneysand ureters, but no obstruction above the uretericclosures which were visible as linear-filling defects(Fig. 7).
Timing of Closure. If the child survives andthrives there must never, I believe, be any questionof not closing the ureterostomies; when the patient'sgeneral condition is good, he is gaining weight andthe ureterostomies are draining freely with minimalresidue in the upper renal tract, the urinary obstruc-tion can be removed if this has not already beendone. The ability of the bladder to empty must
FIG. 6.-Retrograde pyelogram of Case 3. six months after closureof ureterostomy with resection of part of the ureter. Marked delayin emptying of kidney and ureter above ureteric anastomosis. Radio-graph taken one and a half hours after injection of contrast medium.
FIG. 7.-Intravenous pyelogram of Case 2, 10 months after bilateralureterostomy closure, retaining continuity of ureteric musculature.No stasis above sites of closure, which are visible as linear filling
defects.
165
copyright. on January 2, 2020 by guest. P
rotected byhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.38.198.161 on 1 A
pril 1963. Dow
nloaded from

166 ARCHIVES OF DISEASE IN CHILDHOOD
then be assessed, and this is particularly easy whenthere are loop ureterostomies; a catheter is passedinto the ureter below the ureterostomy and saline isinjected through it to the bladder. By connectingan intravenous drip set to the catheter the patient'scapacity to micturate can be trained and observedfor weeks if necessary and its adequacy confirmedradiologically. If these precautions are taken, andthey are needed especially in the child with anatonic neurally dissociated bladder, one can readilyjudge when ureterostomy closure is safe.
The technique of temporary ureterostomy carriesits own problems, although the complications I havedescribed are undoubtedly avoidable. The methodis obviously not required for every child with con-genital urinary obstruction. Its great use, either
as a primary elective procedure or as a method ofresort when other drainage techniques have failed,is in the really ill child with a dilated, infecteddecompensated urinary tract which needs prolongeddecompression. In such cases, and these are, ofcourse, the patients with the most severely damagedrenal tracts who are most precariously situated,I have found temporary ureterostomy a mostvaluable, even a life-saving, method of management.
I am indebted to Miss Isabella Forshall for allowingme to undertake radiological and biochemical investiga-tions on two of her patients included in the series.
REFERENCESMurnaghan, G. F. (1959). Experimental aspects of hydronephrosis.
Brit. J. Urol., 31, 370.Rickham, P. P. (1962). Advanced lower urinary obstruction in
childhood. Arch. Dis. Childh.. 37, 122.
copyright. on January 2, 2020 by guest. P
rotected byhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.38.198.161 on 1 A
pril 1963. Dow
nloaded from