technology 1 contrast media and contrast studies jeremy oates michal smolski thiru gunendran
TRANSCRIPT

Technology 1Contrast Media and Contrast studies
Jeremy OatesMichal SmolskiThiru Gunendran
References
• Campbell Walsh
• FRCS Lectures
• Scientific basis of Urology
• Standards for intravascular contrast agent administration to
adult patients. RCR 2010
• Manual on Contrast Media. ACR 2012
• Literature

Technology 1
• Types media and basic structures
• Toxicity of media, Contrast mediated
nephrotoxicity
• Principles of contrast studies (KUB, IVU,
retrograde, angiography)
• How do X-Rays work?
Types media and basic structures
• Radiological (Iodine based, Barium sulfate,
Thorium dioxide – past)
• MR ( Gadolinium )
• Ultrasound (CEUS – Contrast –enhanced
ultrasound – microbubbles )

Why use contrast media• Where considerable difference between the densities of two
organs exists then the outlines of the structures can be visualised on a radiograph due to natural contrast. Similarly, if there is a difference between the average atomic numbers of two tissues, then the outlines of the different structures can be seen by natural contrast.
• However, if the two organs have similar densities and similar average atomic numbers, then it is not possible to distinguish them on a radiograph, because no natural contrast exists. This situation commonly occurs - it is not possible to identify blood vessels within an organ, or to demonstrate the internal structure of the kidney, without artificially altering one of the factors mentioned earlier.

Radiological Contrast media
• CBD
• 55 years of age male presented to
a Urologist with recurrent UTI’s
• CT shows 22 mm mid polar L kidney stone
• Treatment: PCNL
• What type of contrast will you use for CTU
• What contrast will you use for retrograde
pyelogram?
• Explain the choice of CM
Radiological Contrast media• Iodine - provides radio-opacity
(discovered treating syphilis in the 1920’s with sodium iodide)
• Other elements of RCM molecule = carrier• toxicity, solubility of iodine, non-radioopaque
• All IV RCM • Benzene ring• 3 atoms of iodine at C 2,4,6 positions
• Classification• Ionic or non-ionic• High or Low osmolar• Monomeric or Dimeric
Osmolality
• Dependent solely on number of dissociated particles
(not number of molecules).
• The closer the osmolality of RCM to that of plasma the
better the tolerance.
• Osmolality is directly responsible for a number of
clinically important effects. The sensations of heat and
discomfort or even pain from contrast media are
directly related to the osmolality.

Viscosity
• Resistance of a liquid to various forces (and
hence to flow)
• Related to concentration of the Iodine in
a contrast medium
• Inversely related to temperature
• Not related to pressure

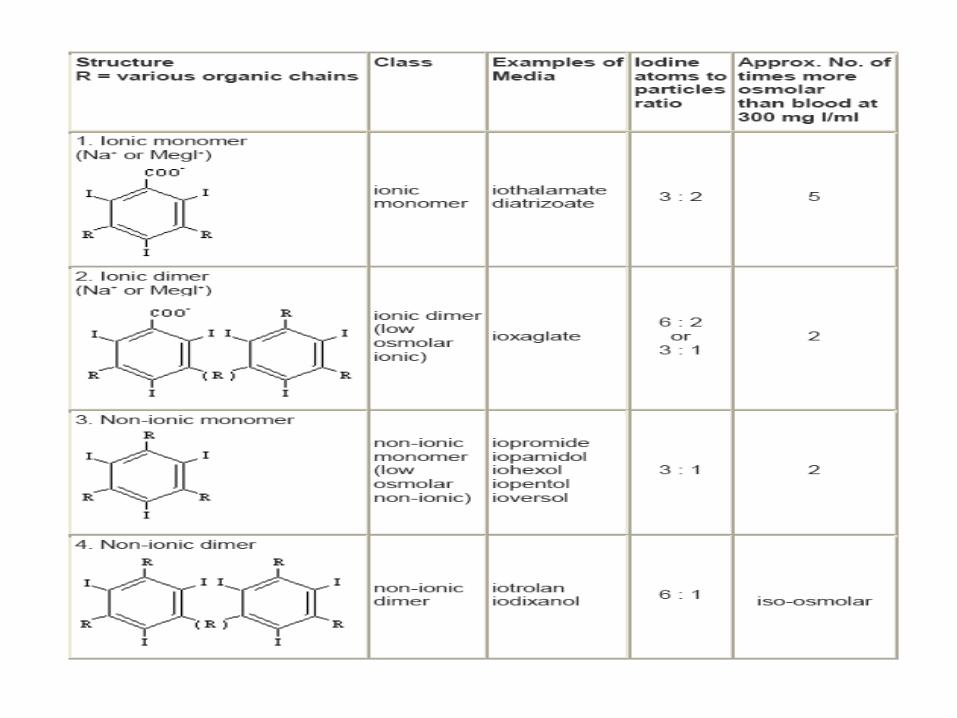
Radiological Contrast Media• 4 types RCM
• Ionic monomer = high osmolar • Ionic dimer = low osmolar• Non-ionic monomer = low osmolar • Non-ionic dimer = iso-osmolar
• Distribution• Hydrophilic• Capillary permeability throughout extracellular compartment.• Filtered unchanged in glomerulus.
• Excreted - 90% by glomerular filtration in 12 hrs
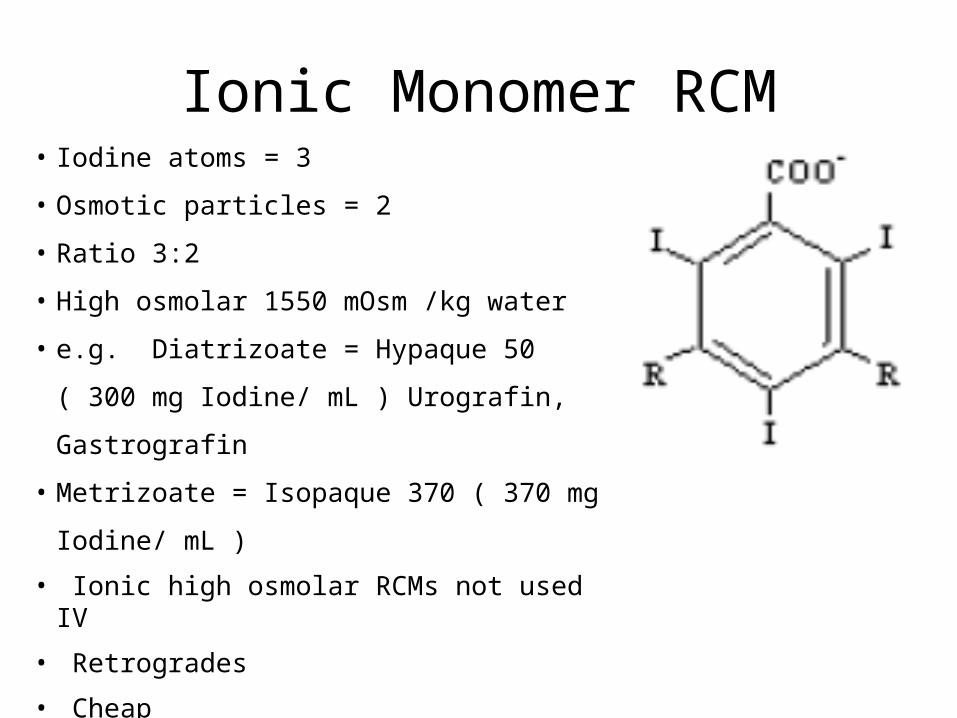
Ionic Monomer RCM• Iodine atoms = 3
• Osmotic particles = 2
• Ratio 3:2
• High osmolar 1550 mOsm /kg water
• e.g. Diatrizoate = Hypaque 50 ( 300 mg Iodine/ mL )
Urografin, Gastrografin
• Metrizoate = Isopaque 370 ( 370 mg Iodine/ mL )
• Ionic high osmolar RCMs not used IV
• Retrogrades
• Cheap
• Side effects 10x non-ionic
• Also used to treat tape worms
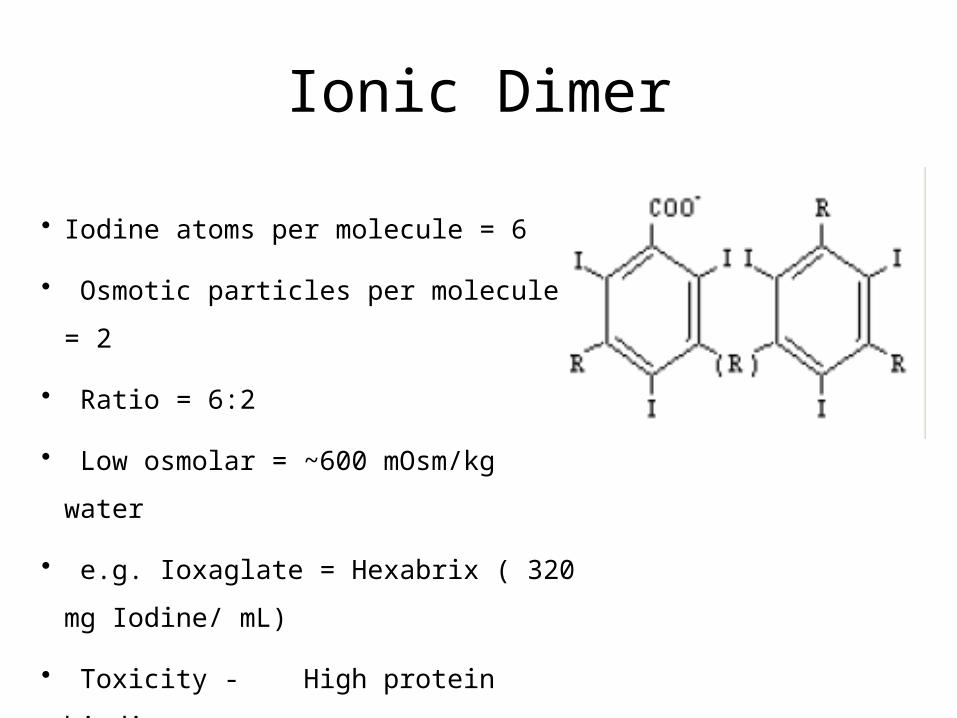
Ionic Dimer
• Iodine atoms per molecule = 6
• Osmotic particles per molecule = 2
• Ratio = 6:2
• Low osmolar = ~600 mOsm/kg water
• e.g. Ioxaglate = Hexabrix ( 320 mg Iodine/ mL)
• Toxicity - High protein binding
Electrical charge
Non-Ionic RCM
• Cation replaced by non-dissociating organic chain
• Tri-iodinated non-ionising compounds• Fewer particles per iodine atom• Lower osmolality• Fewer side effects• More expensive
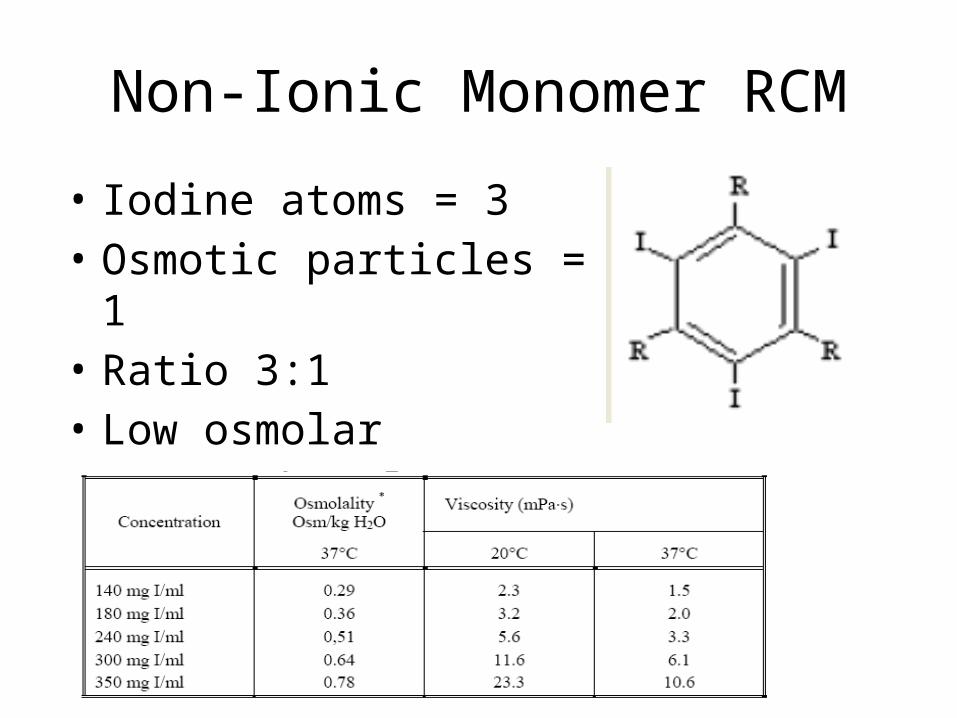
Non-Ionic Monomer RCM
• Iodine atoms = 3• Osmotic particles = 1• Ratio 3:1• Low osmolar• e.g. Iohexol = Omnipaque

Non-Ionic Dimer RCM
• Iodine atoms = 6• Osmotic particles = 1• Ratio 6:1• Iso-osmolar ~ 300 mOsm• eg Iodixanol = Visipaque
Points to Remember for RCM
• Radio-opacity• Iodine conc. of solution• No. of iodine atoms per molecule• Conc. of molecules in solution
• Osmolality• No. of particles
– Ionic vs. Non-ionic• Low osmolality
– Fewer side effects / reactions – pain of injection
• High osmolality– Greater risk reactions– Causes osmotic diuresis
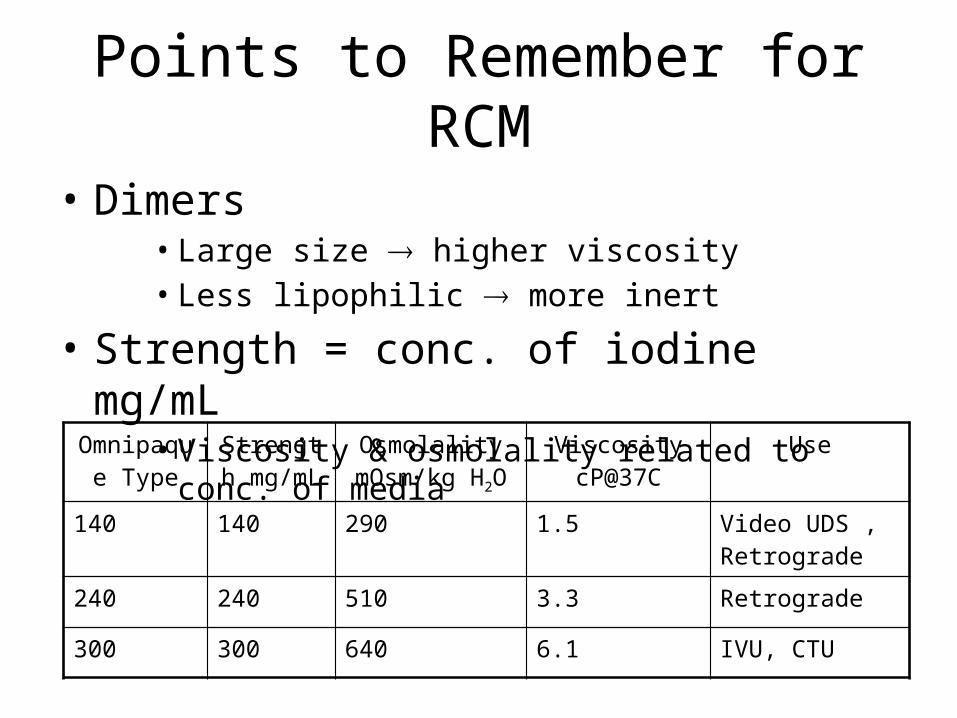
Points to Remember for RCM
• Dimers• Large size higher viscosity• Less lipophilic more inert
• Strength = conc. of iodine mg/mL• Viscosity & osmolality related to conc. of media
Omnipaque Type
Strength mg/mL
Osmolality mOsm/kg H2O
Viscosity cP@37C
Use
140 140 290 1.5 Video UDS , Retrograde
240 240 510 3.3 Retrograde
300 300 640 6.1 IVU, CTU
MCQ Types media and basic structures
• Which is an ionic CM ?
a. Iohexol
b. Iopamidol
c. Ioxaglate
d. Iodixanol

MCQ Types media and basic structures
• Which is a non-ionic CM?
a. Ioxaglate
b. Iohexol
c. Iothalamate
d. Diatriozoate
MCQ Types media and basic structures
• Omnipaque is used primarily for:
a. Contrast CT
b. Video UDS
c. Retrograde
d. All the above
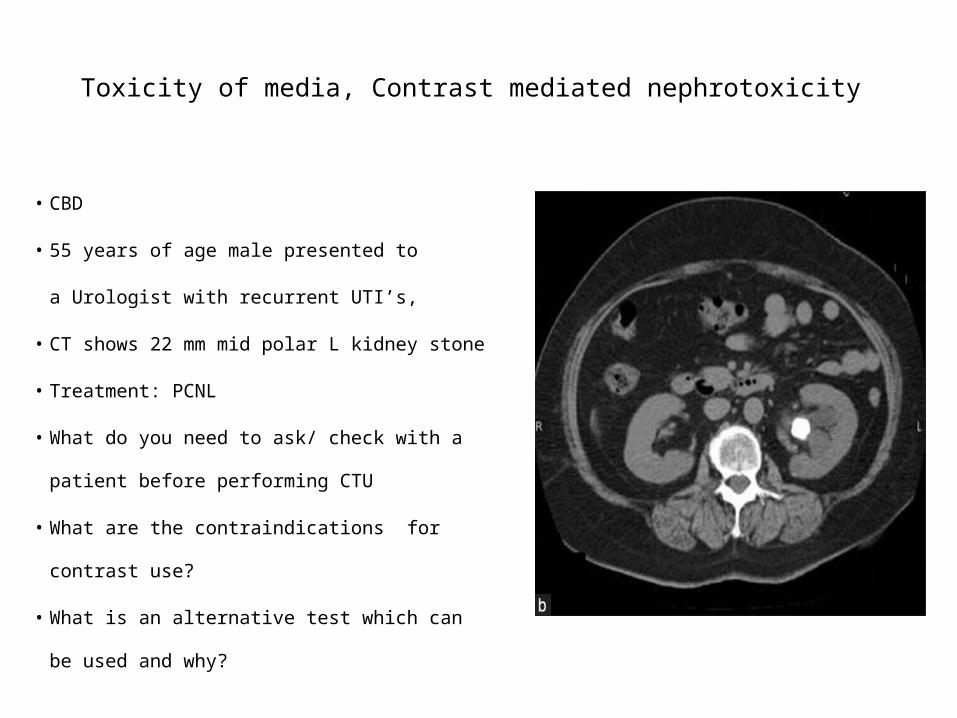
Toxicity of media, Contrast mediated nephrotoxicity
• CBD
• 55 years of age male presented to
a Urologist with recurrent UTI’s,
• CT shows 22 mm mid polar L kidney stone
• Treatment: PCNL
• What do you need to ask/ check with a
patient before performing CTU
• What are the contraindications for contrast
use?
• What is an alternative test which can be
used and why?
Toxicity of media• Osmolality
• Ionic vs. Non-ionic• Dimer vs. Monomer
• Electrical charge
• Lipophilicity• Correlates with the toxicity of ionic contrast media. Non-ionic contrast media
very hydrophilic, properties other than lipophilicity (e.g. hydrogen bonding) are responsible for interactions with biological molecules and membranes.
• Protein binding
• Protein receptors• Membranes
• Mediator release

Toxicity of media
• Major life threatening contrast reaction is rare
– Non-ionic agents– Severe 0.04%– Very serious reactions 0.004%– Deaths 0.001%
Katayama et al, Radiology 1990

Toxicity of media
• Classification of adverse reactions– Idiosyncratic anaphylactoid reactions
• Not dose related
– Non-idiosyncratic chemotoxic reactions• Dose dependent• Molecular toxicity• Physiological characteristics• Mechanisms
– Chemotoxic– Hyperosmolar
IdiosyncraticNot dose related
Mild Intermediate Severe
Mild urticaria Extensive urticaria
Cardiopulmonary collapse
Angio-oedema Pulmonary oedema
Bronchospasm Bronchospasm
Layngospasm Laryngospasm
Hypotension Hypotension

Non-idiosyncraticDose dependent
Minor Intermediate Severe
Tachy/brady Oliguria/anuria VT/VF
Azotaemia MI
Myocardial ischaemia
Arrhythmia
Bronchospasm

Adverse Drug Reactions - RCM
Ionic HOCM Patients Nonionic LOCM
169,284 Total No. 163,363
12.7% Total ADR 3.13%
0.22% Severe ADR 0.04%
(1) Deaths (1)
Katayama et al, Radiology 1990

ADR - Symptoms ExperiencedIonic HOCM %
Symptom Nonionic LOCM %
4.58 Nausea 1.042.29 Heat 0.922.97 Vomiting 0.453.16 Urticaria 0.471.12 Flushing 0.160.4 Venous pain 0.050.58 Coughing 0.150.17 Dyspnoea 0.04

Severe ADR to RCMIonic HOCM ADR% Clinical history Non-ionic LOCM ADR
%
0.18 No Hx of allergy 0.03
0.53 Hx of allergy 0.10
0.13 No previous ADR to RCM
0.03
0.73 Previous ADR to RCM
0.18
1.88 Asthma 0.23
0.49 Atopy 0.11
0.53 Heart disease 0.10
0.20 Renal disease 0.04
0.22 Diabetes 0.05
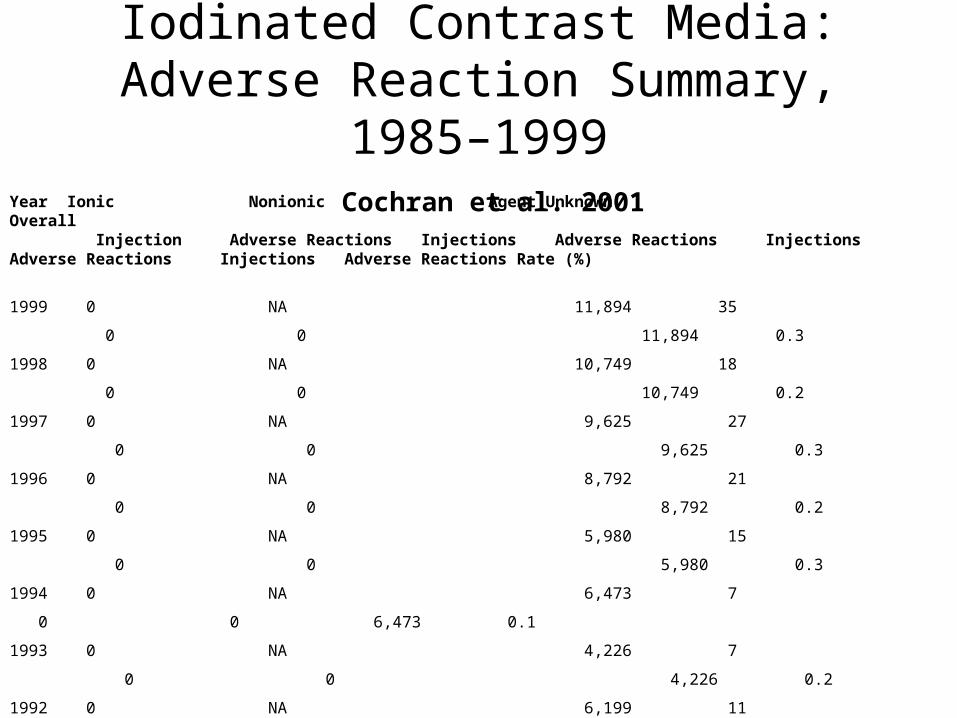
Iodinated Contrast Media: Adverse Reaction Summary, 1985–1999
Cochran et al. 2001Year Ionic Nonionic Agent Unknown Overall Injection Adverse Reactions Injections Adverse Reactions Injections Adverse Reactions Injections Adverse Reactions Rate (%)
1999 0 NA 11,894 35 0 0 11,894 0.3
1998 0 NA 10,749 18 0 0 10,749 0.2
1997 0 NA 9,625 27 0 0 9,625 0.3
1996 0 NA 8,792 21 0 0 8,792 0.2
1995 0 NA 5,980 15 0 0 5,980 0.3
1994 0 NA 6,473 7 0 0 6,473 0.1
1993 0 NA 4,226 7 0 0 4,226 0.2
1992 0 NA 6,199 11 0 0 6,199 0.2
1991 0 NA 4,763 14 0 0 4,763 0.3
1990 2,460 18 2,540 21 0 0 5,000 0.8
1989 7,191 23 1,398 2 1,134 16 9,723 0.4
1988 1,812 28 400 6 2,514 9 4,726 0.9
1987 0 NA 0 NA 870 12 870 1.4
1986 702 55 0 0 0 0 702 7.8
1985 751 46 0 0 0 0 751 6.1
Total 12,916 170 73,039 184 4,518 37 90,473 0.43
Iodinated Contrast Media: Adverse Reaction Summary, 1985–1999
Cochran et al. 2001
• Mild and moderate adverse events more common with ionic contrast material than with non-ionic
• Severe reactions are seen equally with ionic and non-ionic contrast material but differ in type:– Ionic – allergic-like – Non - ionic cario-pulmonary decompensation

Risk factors for adverse intravenous contrast media reactions
• Previous reaction to CM – 5 x increased risk
• True allergies – 2 x
• Asthma – 6 x iso-, non-ionic, 10 x – HOCM
• Renal problems – risk proportional to the pre-existing impairment
• Metformin therapy
• Miscellaneous Risk Factors:
Multiple myeloma and HOCM, B-blocker, sickle cell trait,
pheochromocytoma and HOCM, thyroid cancer, cardiac status, anxiety,
pregnancy
Previous reaction to CM
• Exact nature of ADR
• Agent used
• Re-examine need for RCM study• Risk/benefit ratio
• Alternative - non-contrast, USS, MRI
• If RCM necessary• Use different RCM
• LOCM / iso-osmolar CM
• Prophlactic steroids - no conclusive evidence

Other known allergies - Atopy and CM
• Increased risk – 2 x
• Confirm previous type of allergic reaction
• Re-examine need for RCM study
• Risk/benefit ratio
• Alternative - non-contrast, USS, MRI
• If RCM necessary
• Use different RCM
• LOCM / iso-osmolar CM
Asthma and CM
• Risk severe ADR• LOCM x6, HOCM x10
• Confirm diagnosis
• Determine if well controlled
• Defer if exacerbation or poor control
• Rx as per previous reaction
Metformin therapy
• Excreted exclusively via kidneys
• Can cause/exacerbate lactic acidosis
• Normal Cr range of eGFR – don’t stop
• If out of range consult stopping for 48 hrs with
referring clinic
Standards for intravascular contrast agent administration to adult patients. RCR 2010
Risk factors for adverse intravenous contrast media reactions
• Use a non-ionic low or iso-osmolar agent
• Maintain close medical supervision
• Leave the cannula in place and observe the patient for 30 minutes
• Be ready to treat promptly any adverse reaction and ensure that
emergency drugs and equipment are available
Standards for intravascular contrast agent administration to adult
patients. RCR 2010

MCQWhat is the incidence of CMN in patients with normal renal function?
a. Less than 1%
b. 2 – 3%
c. 5%
d. Up to 10 %

MCQWhat is the incidence of CMN in patients with severe renal impairment?
a. 20%
b. 30%
c. 40%
d. 50%
MCQ
What is the concentration of CM in urine comparing to concentration in plasma?
a. 5 x
b. 10 x
c. 20 x
d. 50-100 x
MCQ
When does Cr peak in CMN?
a. 1-2 days
b. 3-5 days
c. 5-7 days
d. 8-10 days
MCQWhen does Cr value normalises in CMN?
a. 3-5 days
b. 5-7 days
c. 7-10 days
d. 10-14 days
Incidence• 3-5% inpatients develop ARF• No strict definition of CMN
– 25-100% increase in 24-72hr (50% seems best)
• Occurs in 0.1-0.5% with normal renal function• Risk factors
– Renal impairment (creat>140, GFR<70ml/min)– DM– Volume depletion– Heart failure– High doses, repeated doses– AGE– NSAIDS, gentamicin, chemotherapeutic agents (eg cisplatin)
– Mild/mod renal impairment: 5-10% CMN+DM : 10-40%
– Severe renal impairment: 50%

Renal processing of contrast• >99% excreted by kidneys
– Half life (with normal function) : approx 2 hours– Freely filtered, osmotic force results in diuresis– Concentration in urine 50-100 x that of plasma
– Elimination by intestine and biliary tree may increase• But accumulation also occurs with normal function
– Plasma concentration: bi-exponential decay curve1. Mixing of contrast into interstitial space2. (after 2 hours); as excreted in normal function
– Inhibition of Na and water reabsorption in proximal tubule• Increased flow rates• Increased perfusion of distal portion of loop• Decrease in GFR (tubuloglomerular feedback- TGF)
Pathophysiology– Incompletely understood– Animal studies
• Transient increase in renal perfusion• Abrupt prolonged decrease
– Seems 2 main mechanisms1. Hypoperfusion
– Contrast and osmotic stress– Endothelin, prostoglandins, NO reduced: vasoconstriction– High osmolar : TGF response;
» vasoconstriction afferent arterioles» Decrease in GFR, increase in renal vascular resistance
– Cannot be only mechanism as failure of vasodilators2. Direct toxicity to tubular cells
– Cytotoxic reactive oxygen species– Rationale for anti-oxidant (N-acetyl cysteine)
– Structural effects: vacuolization proximal tubules, DNA fragmentation, necrosis of thick ascending limb of L of H
– Long term affects unknown (glomerulosclerosis?)

Diagnosis CMN• Form of ATN
• Differential;
– Ischaemic ATN
– Atheroembolic disease
• GFR ideal, but difficult
• Mild proteinuria and oliguria may occur
• Contrast media can affect protein assays
• Granular casts (muddy brown)
• Persistent nephrogram
• Most resolve in 1-2 weeks, peak creat at 3-5 days
• Recent study 1826 patients coronary angiography
– 14% CMN, mortality 7%
– Odds ratio for mortality of approx. 5
Prevention of CMN• Volume expansion
– Solomon et al.1. 0.45% saline 12 hrs before and after2. (1. + frusemide)3. (1. + manitol)
• Advantage in group 1 and 3 same. • Frusemide group worse
• Isotonic saline best• Sodium bicarbonate may be better than NaClN-acetylcysteine
• Conflicting reports• Meta analysis shows mixed benefits• 600mg BD day before and day of contrast
• Others suggested; ANP, dopamine • NSAIDS; discontinue 24hr before and after
Ultrasound CM & CEUS• Alters echo amplitude in ultrasonography
• Changes in absorption, reflection & refraction• Encapsulated microbubbles <10µm diameter• Confined to vascular space• Increase echo strength up to 300 fold
• Can use targeting ligands to bind to endothelial receptors (integrins & growth facor receptors) enableing microbubble complex to accumultae in area of interest.
• Can derive measures of tumor blood flow and blood volume by employing high mechanical index ultrasonography to destroy micro bubbles in a given region and then determining the rate at which they reappear; a process termed replenishment kinetics
• Increased sensitivity of TRUSS guided prostate biopsy (38-54% vs. 65-93%)• Eg: Levovist, Sonovist• Complications very rare
MRI Contrast MediaGadolinium (paramagnetic agent)
• T1 - This tissue-specific time constant for protons, is a measure of the time taken to realign with the external magnetic field.
• Gadolinium decreases T1 relaxation time.• Enhanced tissues and fluids appear extremely bright on T1-
weighted images. • Provides high sensitivity for detection of vascular tissues (e.g.
tumors). • Dynamic Contrast Enhanced MRI more sensitive than T2W images
for prostate cancer localization (50% vs 21%; p = 0.006) and similarly specific (85% vs 81%; p = 0.593).Jackson et. al B J Radiol. 2009

Complications
• Minimal nephrotoxicity• Allergy rare• Nephrogenic systemic fibrosis
– Severe delayed fibrotic reaction of tissues (from day of exposure up to 2-3 months)
– Can be progressive & fatal in around 5%– Starts with red, itchy painful swelling on limbs progressing
to muscle weakness and contractures.– Risk with GFR <60 (Highest if <30)– Not reported GRF >60
RCR 2007
Lymphotropic Superparamagnetic Nanoparticles
Particles are taken up by macrophages of the reticuloendothelial system and accumulate in lymph nodes. Passive, cell-specific targeting of the iron oxide nanoparticles to lymph nodes.
Differential cellular content of benign versus malignantly infiltrated nodes make this method suitable for cancer staging.
Lymphotropic nanoparticle enhanced MRI, differences in benign versus malignant infiltration of lymph nodes can be visualised, which adds accuracy to standard MRI beyond criteria based solely upon the size and shape of lymph nodes.
• LN staging CaPSens 91% vs 35%, Spec 98% vs 90% - compared to standard MRIMukesh et al NEJM, June 2003
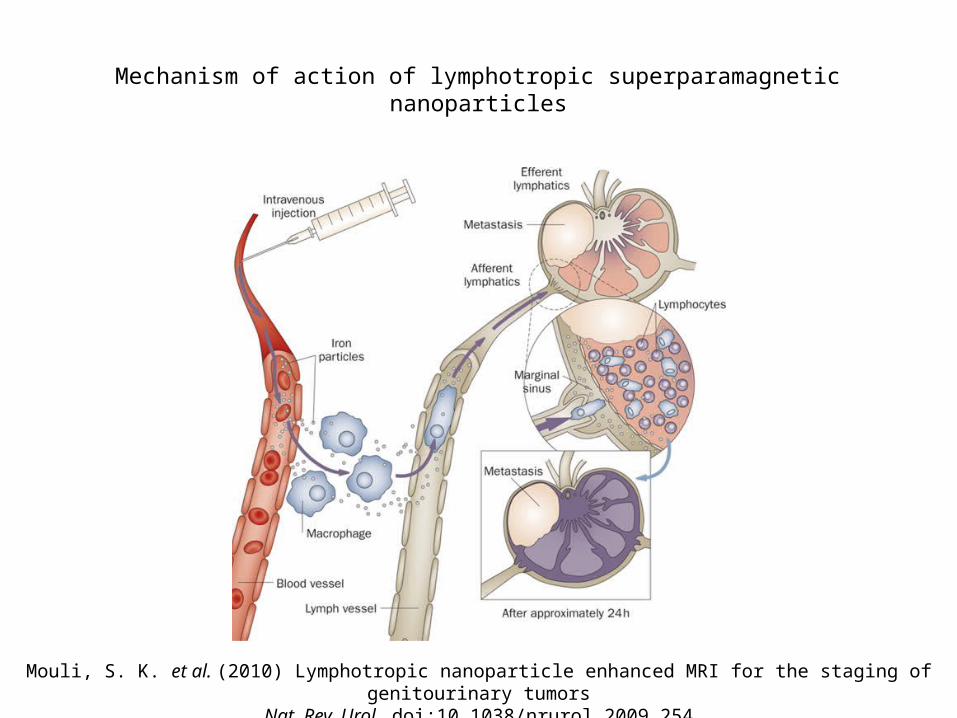
Mechanism of action of lymphotropic superparamagnetic nanoparticles
Mouli, S. K. et al. (2010) Lymphotropic nanoparticle enhanced MRI for the staging of genitourinary tumorsNat. Rev. Urol. doi:10.1038/nrurol.2009.254
PET
• Detects pairs of gamma rays emitted indirectly by positron (anti-particle of electron) emitting radionucleotide.
• Combined with CT or MRI.• Carbon-11, Nitrogen-13, Fluorine-18 attached
to glucose, water or a specific ligand.
• Commonest agent: Fluorine 18 fluorodeoxyglucose (FDG)
X-Rays - the unknown quantity
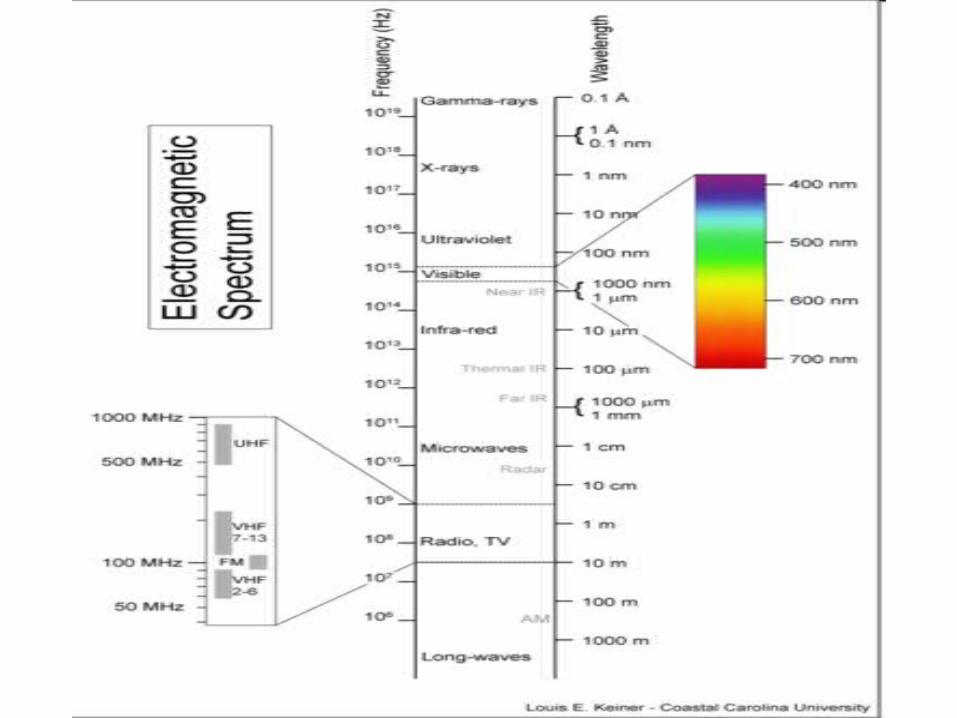
• Wilhelm Conrad Roentgen 1896• Electromagnetic radiation
• Photon energies between -rays and UV radiation
• Basis for medical use• Differential attenuation of x-rays interacting with tissues• Transmitted x-ray ‘flux’ depends on attenuation of beam along
path• Superimposed shadow of internal anatomy• X-ray sensitive detector captures transmitted fraction• X-rays converted to visible projection image
X-Ray Production
• Conversion of kinetic energy attained by electrons accelerated under a potential difference
• X-ray generator• Provides voltage to energise tube
• X-ray tube• Environment = vacuum• Cathode - filament • Separate filament circuit• Anode - tungsten target• Collimators - define x-ray beam shape incident on patient

X-Ray Production
Rotating Anode X-ray generator:A = AnodeC = Cathode E = Envelope (Vacuum)R = RotorS = Stator windingsT = Target W = X-ray window
X-Ray Production• Cathode filament
• Filament circuit activated• Intense heating• Thermionic emission electrons released
• X-ray generator• Applies high voltage to cathode & anode• Electrons accelerated to +ve anode
• Anode• Highly energised electrons interact with target• Target = tungsten - high atomic no. & high Tm (3653 K)
• Interactions x-ray photon generation• Bremsstrahlung effect = braking radiation• Deceleration of electrons due to +ve nucleus• Kinetic energy lost converted to UV x-ray photons• Characteristic radiation - displaced orbital electron
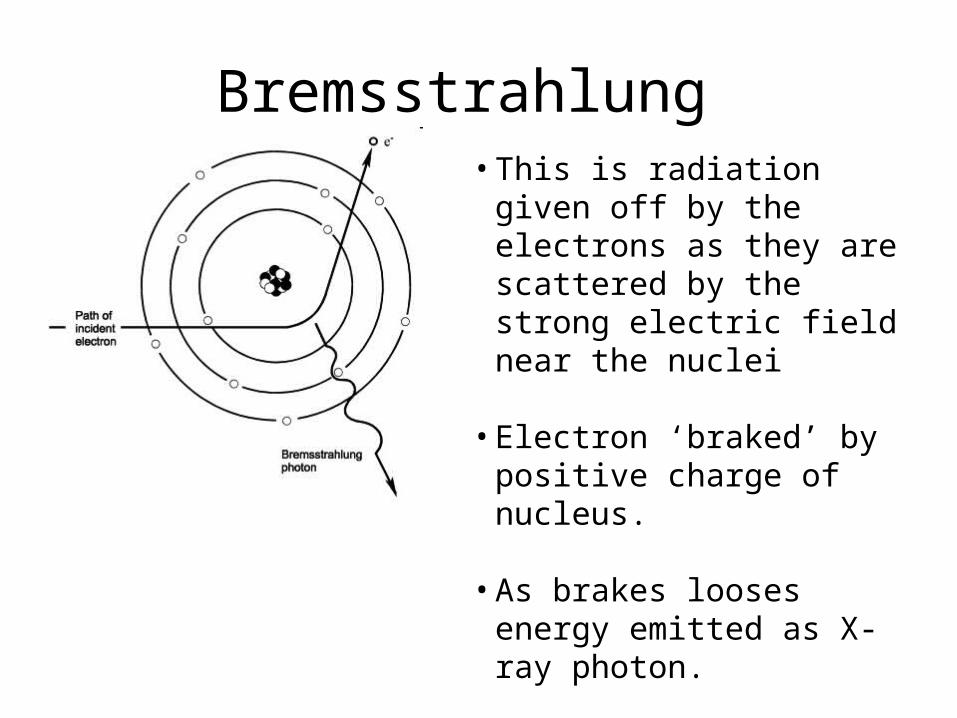
Bremsstrahlung • This is radiation given off by the
electrons as they are scattered by the strong electric field near the nuclei
• Electron ‘braked’ by positive charge of nucleus.
• As brakes looses energy emitted as X-ray photon.

Characteristic radiation
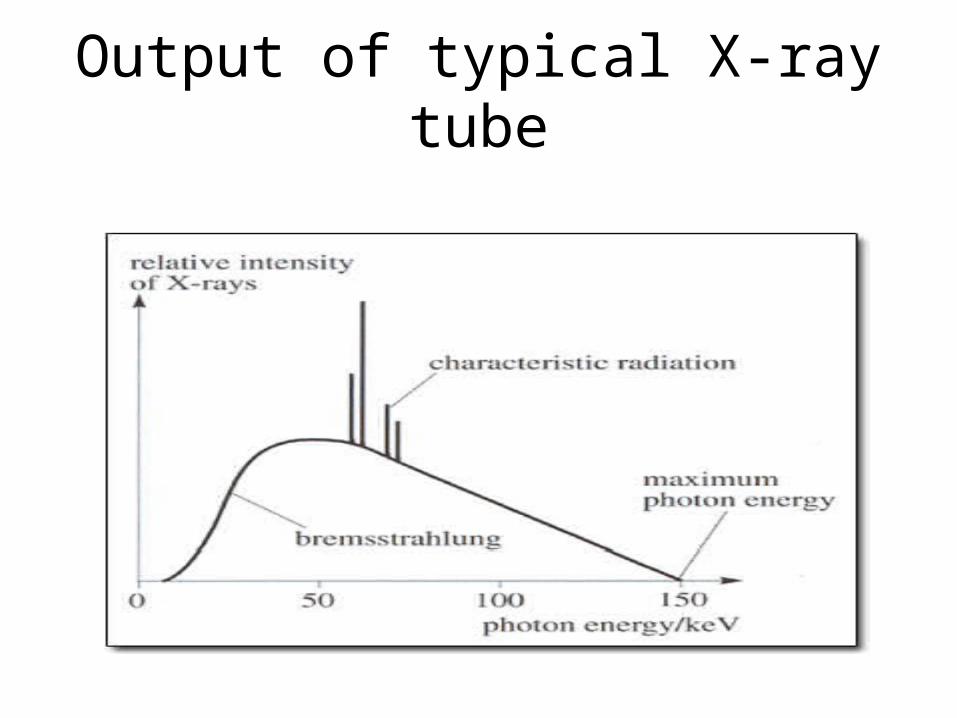
Output of typical X-ray tube

Characteristic radiation varies with type of anode
X-Ray Interactions
• Relative transparency of body to x-rays• Attenuation
• Removal of x-rays by absorption & scattering• Attenuation by patient volume pattern detected
• Mechanisms• Photoelectric absorption• Compton scatter• Rayleigh scatter• Pair production• Combine to attenuate incident photon beam• Removal of photons as beam passes through matter

X-Ray Detection
• Film - analogue• Silver bromide• Pattern of X-ray beam incident on film• Lots of photons opaque silver specks = black• Fixation - unaffected silver bromide crystals removed
• Photostimulable luminescence• Photostimulable storage phosphor• Analogue to digital conversion• Digital signal converted to output e.g. video• Rapid sampling of digital image matrix real time imaging
Digital Radiography
• Flat Panel Detectors (FPD) in place of X-ray film (Two types)
– Indirect FPD's – Amorphous silicone (a-Si) is the most frequent type of FPD
sold in the medical imaging industry today. Combining a-Si detectors with a
scintillator in the detector’s outer layer, which is made from Cesium Iodide,
or Gadolinium Oxysulfide, converts X-ray to light. Because the X-ray energy
is converted to light, the a-Si detector is considered an indirect image
capture technology.
– Direct FPD's – Amorphous selenium (a-Se) are known as “direct” detectors
because X-ray photons are converted directly to charge.

EMQ
a. Bremsstrahlung
b. Characteristic radiation
c. Cathode
d. Anode
e. Filament
f. Photostimulable luminescence
g. Direct FPD
Identify matching term for each of the following statements:
1. Relies on stimulation with visible light to produce a signal.
2. Heating element responsible for thermionic emission.
3. Negatively charged diode.
4. Radiation of deceleration.
5. Replacement of inner electrons by another electron with effecting in
photon emission.
6. Positively charged diode.
7. Converts x-ray to light signal.
Principle of IVU• To obtain clinically useful information about the upper tract & related
structures• Adequate dose of contrast• Radiograph
– Control– Nephrogram– Pyelocalyceal phase– Sequence to assess dynamics of urine formation & propulsion
• Adequate distention of opacified collecting system• Tomography• Use of oblique, prone, upright positions• Minimise risk to patient• How to - viva question• Metformin and - viva question

How to perform IVU?
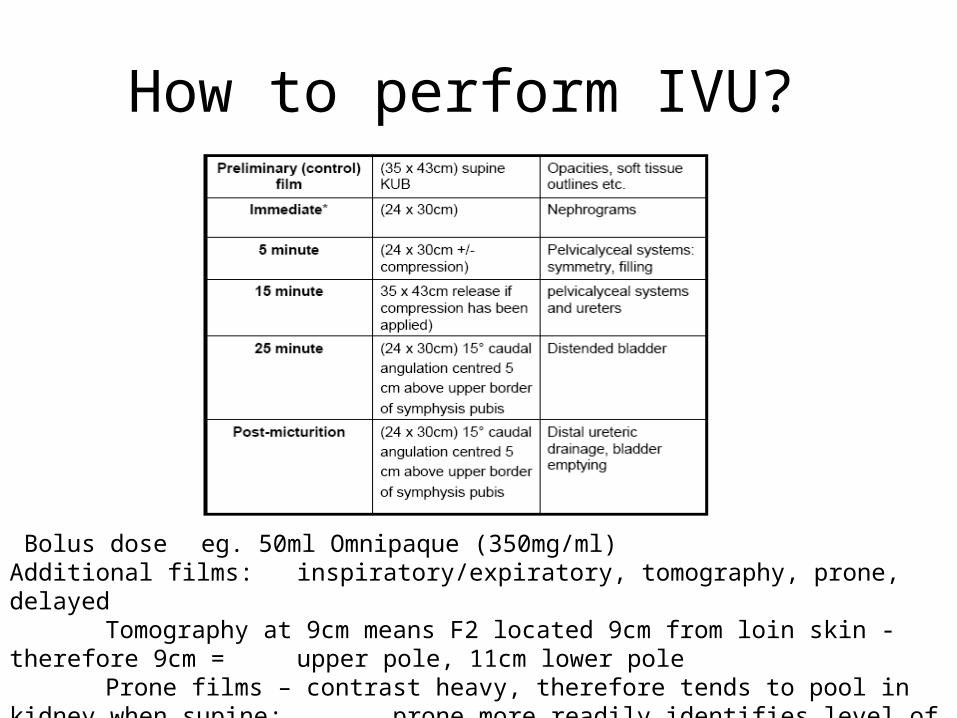
How to perform IVU?
Bolus dose eg. 50ml Omnipaque (350mg/ml) Additional films: inspiratory/expiratory, tomography, prone, delayed
Tomography at 9cm means F2 located 9cm from loin skin - therefore 9cm = upper pole, 11cm lower pole Prone films – contrast heavy, therefore tends to pool in kidney when supine; prone more readily identifies level of obstruction
Principle of Retrograde
• Detailed image of upper tract anatomy & pathology• Not functional - independent of renal function• 5 to 7ch ureteric catheter• 5-10 ml warm omnipaque - use minimum• Strength 140-240mg/ml
• Avoid obscuring subtle details
• Slow injection - avoid high pressure• Overdistention• Rupture• Backflow - pain, obscures findings
Indications for Retrograde
• Non-visualisation of upper tract on IVU• Inconclusive or suspicious IVU / CT• Incomplete IVU• Previous RCM adverse reaction• Part of other procedure
• PCNL• Pyeloplasty• URS
Principle of DSA
• Indications for angiography• Investigation renovascular hypertension• Trauma - view to embolise• Transplant
– Pre-op donors– Post – occlusion / stenosis anastamosis, acute thrombosis
• Suspected renal artery disease• Vascular anatomy - complex surgery
MR angiography and CT angiography superseding in certain situations

Principle of DSA
• Technique• Seldinger - needle, wire, catheter• Aortogram locate renal artery L1/L2 screen• Mask image• Contrast - fast infusion - 10mls in1.5 secs• Images – 4 per sec for 2 sec, then 2 per sec for 6 sec
• Digital subtraction • Optimises images • Enhances electronically the contrast• Minimum contrast, dose 30-50%• Removes background