team-based care in the pcmh - patient-centered primary...
TRANSCRIPT

Team-BasedCareinthePCMHCarlyParry,PhD,MSW,MA(Moderator/Speaker),PCORI
DouglasTynan,PhD,ABPP,APARhoniqueShields-Harris,MD,MHA,FAAP,HealthServicesforChildrenwithSpecialNeeds,Inc.KathrynPhillips,MPH,QualisHealth

Team-Based CarePatient-CenteredPrimaryCareCollaborativeConference
CarlyParry,Ph.D.,MSW,MASeniorProgramOfficer,ImprovingHealthcareSystemsNovember12,2015

• IntroductoryRemarks–Whatdowemeanbyteam-basedcare?– “PatientsontheTeam”
• EnhancingConnectionsbetweenTeams• Panelists:
–W.DouglasTynan,Ph.D.,ABPP–RhoniqueShields-Harris,MD,MHA,FAAP–KathrynE.Phillips,MPH
• Discussion,Q&A
Roadmap

• Teamsaredefinedas:Twoormorepeoplewhointeract“dynamically,interpedently,andadaptivelytoaccomplishasharedgoal”(Taplinetal.,JournalofOncologyPractice,2015)
• ShiftsoccurringincontextofHCdeliveryandpaymentreform– Inter-andMulti-disciplinaryTeamModels–SharedCareModels–Patient-CenteredMedicalHomeModel
• Behavioralhealth/primarycare• OncologyPCMH• Teamsmodelsforcomplexpatients• Oralhealth/primarycare
Team-Based Care: What Do We Mean?
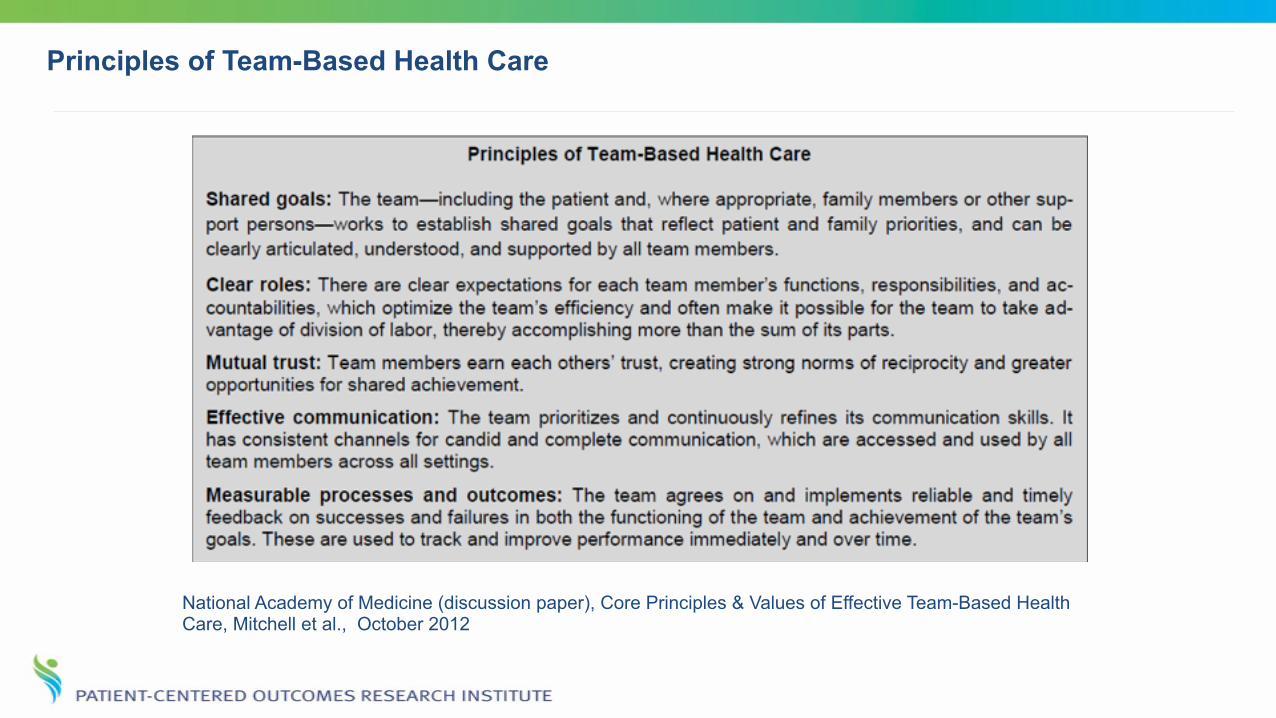
Principles of Team-Based Health Care
National Academy of Medicine (discussion paper), Core Principles & Values of Effective Team-Based Health Care, Mitchell et al., October 2012
• WhatistheRoleofPatientsontheTeam?–Whatistheidealpatientrole?Forwhichpatientsordecision-makingproxies?
–Burdenvs.empowerment?–Appropriatelevelofengagement?–Desiredlevelofengagement–Dopatientsperceiveateam?
Team-Based Care: Patients “on the Team”
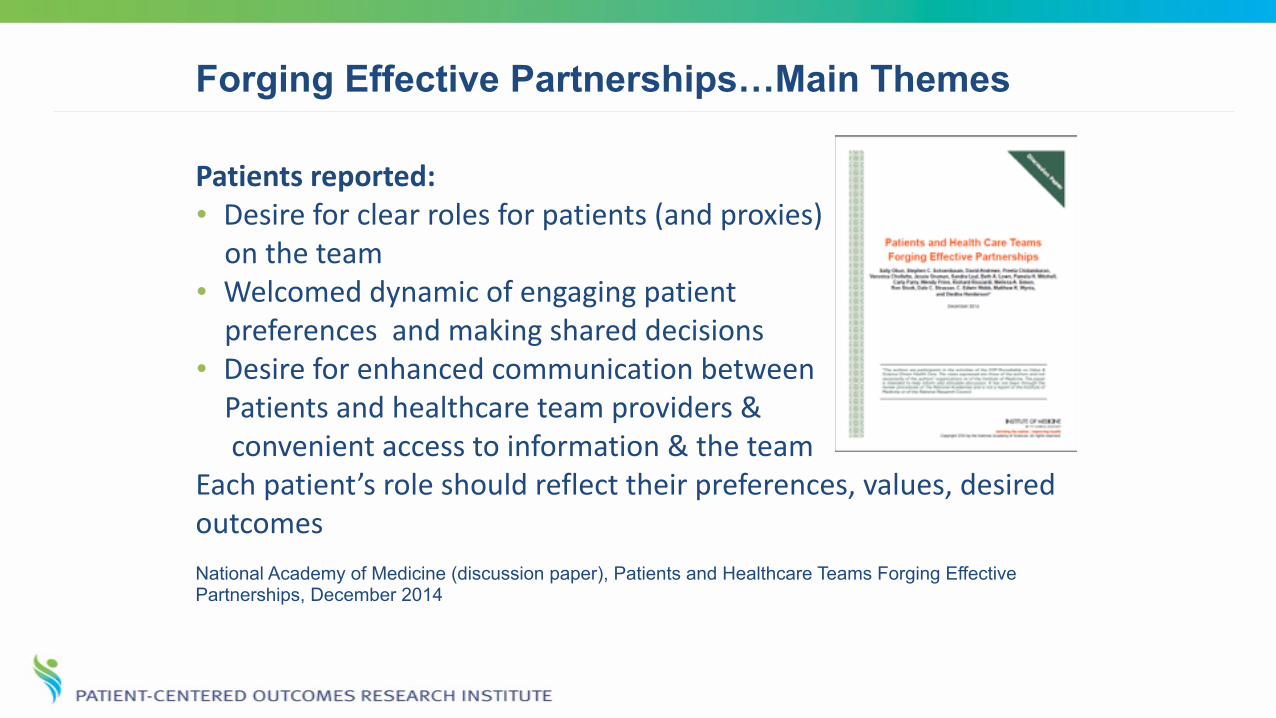
Forging Effective Partnerships…Main Themes
Patientsreported: • Desireforclearrolesforpatients(andproxies) ontheteam • Welcomeddynamicofengagingpatient preferencesandmakingshareddecisions • Desireforenhancedcommunicationbetween Patientsandhealthcareteamproviders& convenientaccesstoinformation&theteam Eachpatient’sroleshouldreflecttheirpreferences,values,desiredoutcomes National Academy of Medicine (discussion paper), Patients and Healthcare Teams Forging Effective Partnerships, December 2014

• Inter-teamwork,caretransitions
Enhancing Connections Between Teams

David

The Ideal of Team-Based Care

Wrangling a Hydra

More of this Outcome
❖W.DouglasTynan,Ph.D.,ABPP• ChoosingtheTeam:MentalHealthIntegrationinPrimaryCare
❖RhoniqueShields-Harris,MD,MHA,FAAP• ACareCoordinationModelforAt-RiskChildrenwithDisabilities
❖KathrynE.Phillips,MPH•OralHealthinPrimaryCare:AFrameworkforAction
Our Panelists

–Whatchangesareneededtoensurethathealthprofessionalsgraduatewiththeskillsandexperiencetofunctioninateam-basedmodelandprovideintegratedcareforpatientsandfamilies?
–Patientsandfamilieswerecriticalinchampioningimprovementsinbehavioralhealthcareandcareforchildrenwithspecialneeds.Howcanweencouragepatientandfamilyinvolvementineffortstointegrateoralhealthinprimarycare?
– Isitpossiblefortheindividualreceivingcaretodrivetheteam?Orshouldthepersondeliveringthecaredrivetheteam?
Discussion
Team-BasedCareinthePCMHCarlyParry,PhD,MSW,MA(Moderator/Speaker),PCORI
DouglasTynan,PhD,ABPP,APARhoniqueShields-Harris,MD,MHA,FAAP,HealthServicesforChildrenwithSpecialNeeds,Inc.KathrynPhillips,MPH,QualisHealth
ChoosingtheTeam:MentalHealthIntegrationinPrimaryCare
Dr.W.DouglasTynan,Ph.D.,ABPPDirector,OfficeofIntegratedHealthCare
AssociateDirector,CenterforPsychologyandHealth

FocusonHealthBehaviors
3ModelsforSelectingMHProviders
• Conveniencemodel– Selectingproviderswhoarelocal,currentemployees,referralsources
• Economicmodel– Selectingthelowestcostprovidersofmentalhealth
• PatientNeedsmodel– Determineneedsofpatientpopulation.
• Pediatric,geriatric,healthyadults–whichpatientsserved&theirneeds.– Matchprovidersandskillstothoseneeds
• Specificskillsneededforthedefinedpatientpopulation.
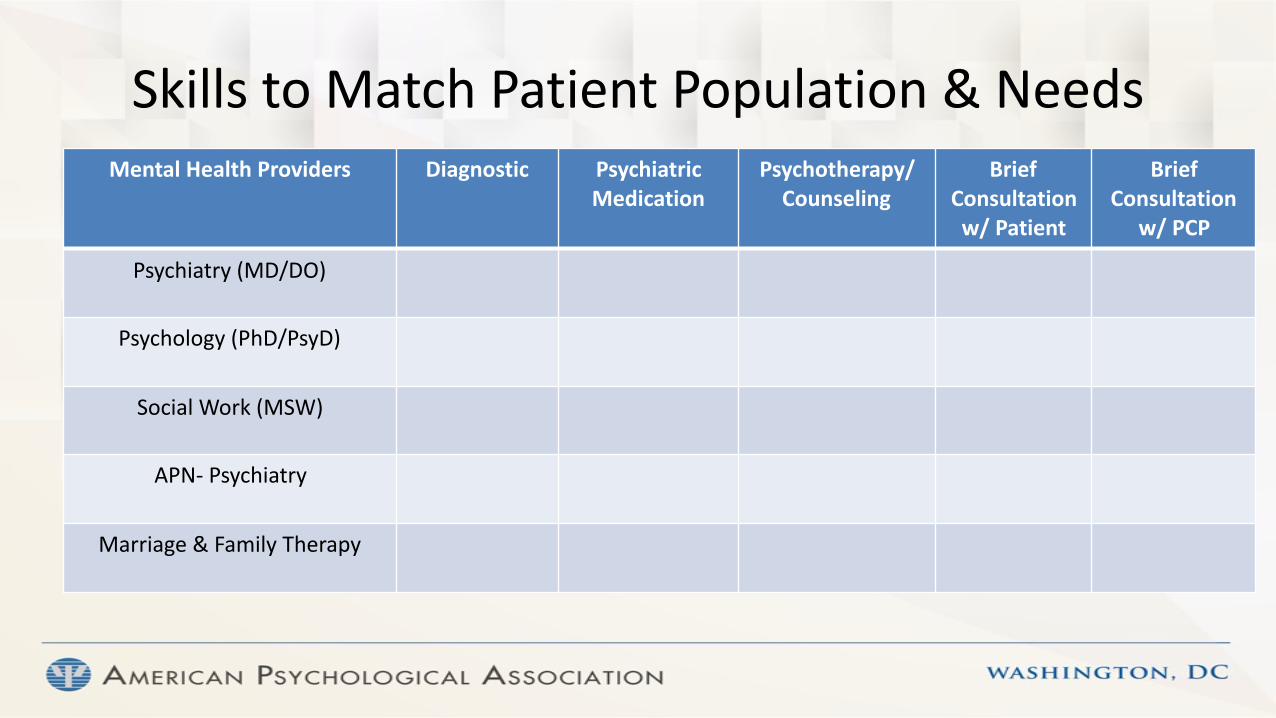
SkillstoMatchPatientPopulation&NeedsMentalHealthProviders Diagnostic Psychiatric
MedicationPsychotherapy/Counseling
BriefConsultationw/Patient
BriefConsultation
w/PCP
Psychiatry(MD/DO)
Psychology(PhD/PsyD)
SocialWork(MSW)
APN-Psychiatry
Marriage&FamilyTherapy
Team-BasedCareinthePCMHCarlyParry,PhD,MSW,MA(Moderator/Speaker),PCORI
DouglasTynan,PhD,ABPP,APARhoniqueShields-Harris,MD,MHA,FAAP,HealthServicesforChildrenwithSpecialNeeds,Inc.KathrynPhillips,MPH,QualisHealth

Oral Health in Primary Care: A Framework for Action
Patient-Centered Primary Care Collaborative Annual Conference Kathryn E. Phillips, MPH
November 12, 2015

23
Who we are…
Qualis Health is one of the nation's leading population healthcare management organizations. We work with public and private sector clients to advance the quality, efficiency,
and value of healthcare.
We help primary care practices adopt new models of care delivery to achieve the Triple Aim: Better care, better health,
lower per capita costs.

24
What is the problem we are trying to solve? A Prevention Gap
• Caries and periodontal disease are preventable chronic infectious diseases
• Unacceptably high burden of disease nationwide • The healthcare system, as currently configured, fails to reach
the populations with the highest burden of disease resulting in pervasive health disparities and wasteful spending
• Dental care is the most common unmet health need
25
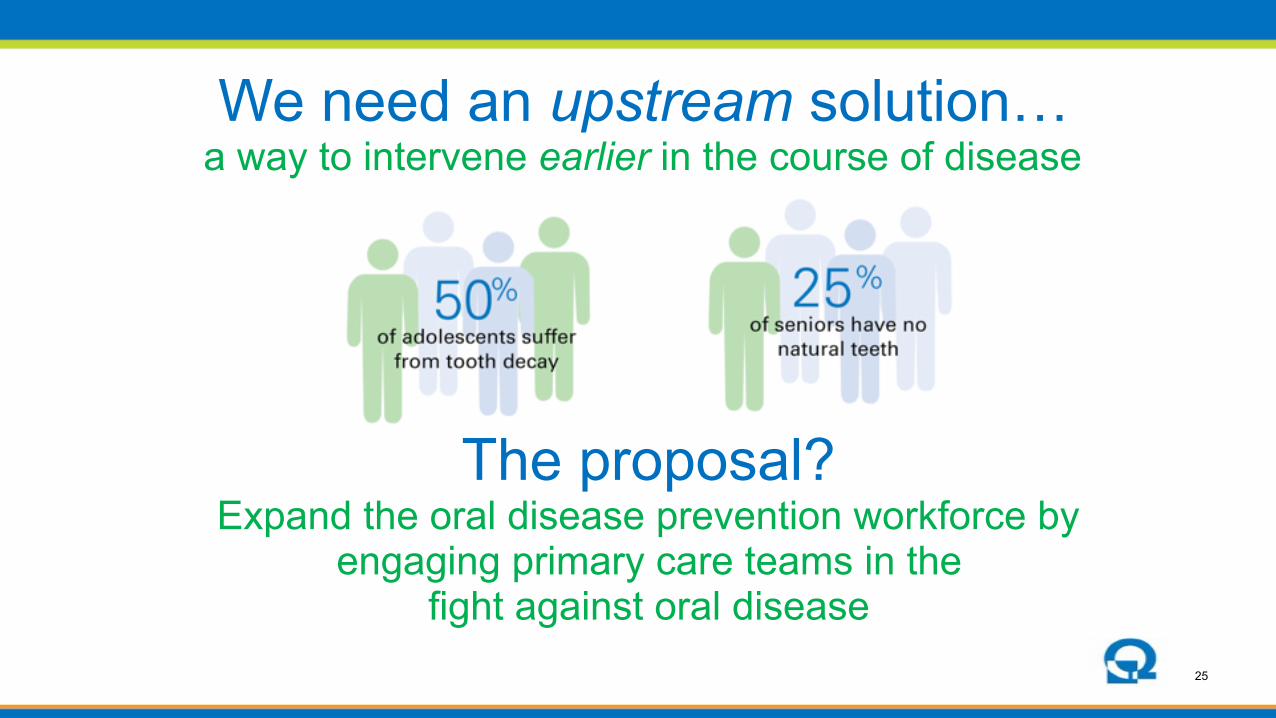
We need an upstream solution…
a way to intervene earlier in the course of disease
The proposal?
Expand the oral disease prevention workforce by engaging primary care teams in the
fight against oral disease

26
Why enlist primary care teams?
Access: Frequent contact with high-risk groups: Children, pregnant women, adults with diabetes
Skills: • Disease prevention • Risk assessment, screening, case-finding • Help patients navigate the healthcare system • Engage patients in behavior change:
Goal setting & self-management support

27
Partnership for Prevention

28
• Ms. G is a 69 year-old woman suffering from diabetes, depression, and asthma.
• Her medical care is managed in a primary care clinic. Her care team monitors her blood sugar and PHQ-9 score every 3 months, and adjusts her medications accordingly.
• Mrs. G’s asthma severity is briefly assessed at each visit, and every autumn (before influenza season) her care team reviews her lung function, adjusts her medications if necessary, and makes sure she receives her flu shot.
• At a yearly visit, special attention is given to testing for kidney disease and loss of sensation in her feet. She is seen by an optometrist for an eye exam.
A New Vision: Care for Ms. G

29
• A year ago, her care team began screening for oral disease while assessing her eyes, feet, and kidney function.
• An initial oral health assessment showed moderate to severe periodontal disease and several root caries.
• The MA trained her in optimal oral hygiene and helped her identify ways she could reduce the sugar content in her diet.
• Her primary care provider also referred Ms. G to a dentist with a formal request to evaluate and manage her periodontal disease and root caries.
• The referral included a copy of Ms. G’s problem list, medication list, and allergy list.
• The dentist returned a consultation note to the referring provider in which the dentist noted his impression, described the interventions taken, and outlined a care plan.
Care for Ms. G

30
Oral Health in Primary Care
Goal: Prepare primary care teams to deliver preventive oral health care and improve referrals to dentistry.
• Reviewed recent efforts to integrate behavioral health services • Convened a Technical Expert Panel: Primary care and dental
providers; leaders from medical, dental, and nursing associations; payers and policymakers; patient and family engagement expert; public and oral health advocates

31
Question: What will it take to change the standard of care?
1. Clear definition of what can be done in the primary care setting to protect and promote oral health
2. Streamlined process for fitting oral health into an already packed primary care workflow
3. Practical model for a close collaboration between medicine and dentistry
32
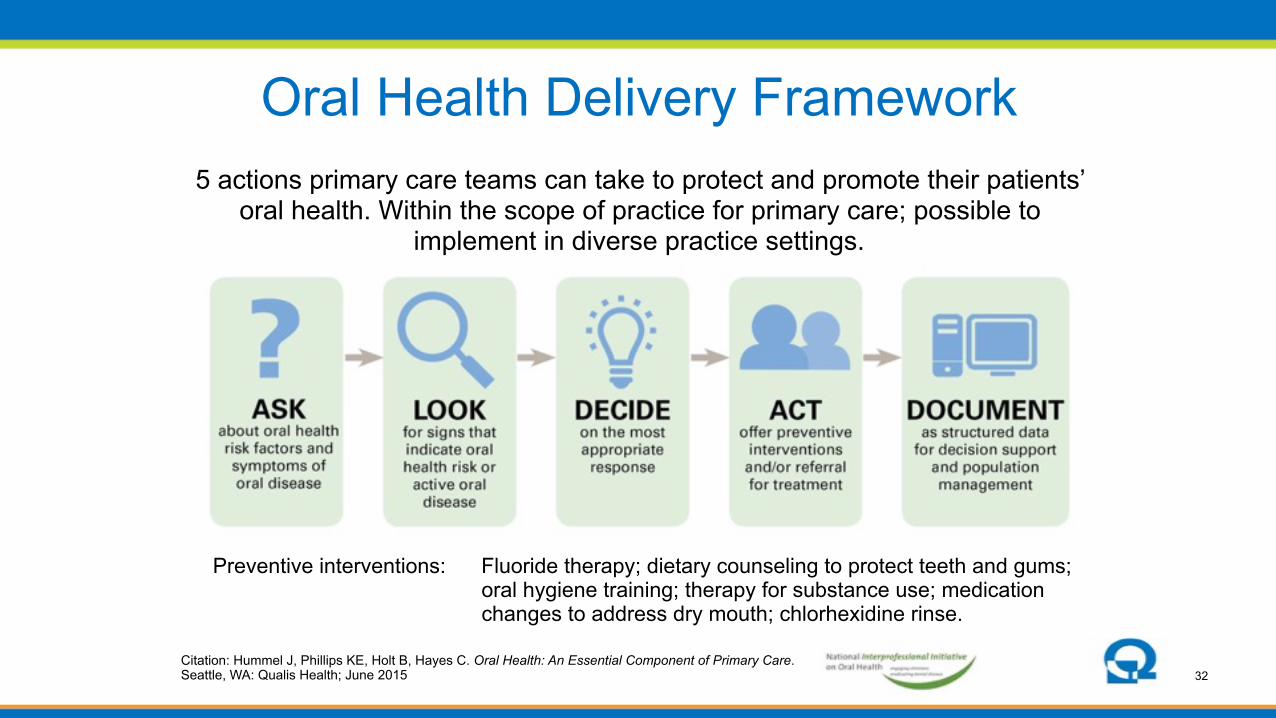
Oral Health Delivery Framework5 actions primary care teams can take to protect and promote their patients’
oral health. Within the scope of practice for primary care; possible to implement in diverse practice settings.
Citation: Hummel J, Phillips KE, Holt B, Hayes C. Oral Health: An Essential Component of Primary Care. Seattle, WA: Qualis Health; June 2015
Preventive interventions: Fluoride therapy; dietary counseling to protect teeth and gums; oral hygiene training; therapy for substance use; medication changes to address dry mouth; chlorhexidine rinse.
33
• Referrals to dentistry ought to be as smooth as referrals to medical specialists -- burden should not be on the patient
• How is a structured referral different? – Issued as a clinical order – Apply referral tracking & care coordination processes – Provide logistical support
• What will this require? ✓ Primary care-dentistry referral networks with adequate
capacity to serve diverse patients
✓ Ability and commitment to share information with one another • Referral agreements help clarify expectations
Structured Referrals
34
White paper, published June 2015 • Case for change
• Oral Health Delivery Framework
• Endorsed by leading organizations
• Case examples from early leaders: Confluence Health, The Child and Adolescent Clinic, Marshfield Clinic
• Supporting actions from stakeholders
• Available at: www.QualisHealth.org/white-paper
Oral Health: An Essential Component of Primary Care
Hummel J, Phillips KE, Holt B, Hayes C. Oral Health: An Essential Component of Primary Care. Seattle, WA: Qualis Health; June 2015

35
19 diverse healthcare delivery organizations: Private practices, Federally Qualified Health Centers; medical only and on-site dental
Adults with diabetes (12), pediatrics (5), pregnancy (1), adult well visits (1) eCW (5), EPIC (8), NextGen (2), Centricity (2), Success EHS (2)
Field-Testing a Conceptual Framework
Oregon Primary Care Assoc. Kansas Assoc. Medically Underserved (*)
Massachusetts League of CHCs *Support also provided by: Kansas Health Foundation United Methodist Health Ministry Fund

36
Implementation guide—toolkit for primary care practices (Sept 2016)
• Sample workflows • Referral agreements
• Case studies and impact data
Resources Resulting From Field-Testing
37
What have we learned?This work requires team-based care
• Many options, exact division of activities depends upon: – Size and structure of the practice – Needs and preferences of patient population – Provider comfort with delegation (most activities can be
performed by a trained medical assistant or LPN; most payers allow delegation)
• Major benefit of activated team? – It makes robust patient support possible – Successful practices think creatively about who can help:
AmeriCorps Volunteer, WIC Specialist, Community Health Workers, patient partners, waiting room video
38
Strategies for Engaging the Team
• Harness intrinsic motivation of ‘support staff’ to contribute to clinical care of patients
• Ensure representative roles in workflow mapping and optimization
• Include medical assistants, reception staff, and referral coordinators in clinical content training

39
Follow-up questions? Reactions?
Resources available at: www.QualisHealth.org/white-paper
Kathryn E. Phillips, MPH, Program Director Phone: 206-288-2462 |Cell: 206-619-7723
e-mail: [email protected]
40
Appendix A, Framework Endorsed by:
American Academy of Pediatrics American Academy of Nursing
American Association for Community Dental Programs American Association of Public Health Dentistry
American College of Nurse Midwives American Public Health Association – Oral Health Section
Association for State and Territorial Dental Directors Association of Clinicians for the Underserved
Institute for Patient- and Family-Centered Care National Association of Pediatric Nurse Practitioners
National Network for Oral Health Access National Organization of Nurse Practitioner Faculties
National Rural Health Association Patient-Centered Primary Care Collaborative
Physician Assistant Education Association
Team-BasedCareinthePCMHCarlyParry,PhD,MSW,MA(Moderator/Speaker),PCORI
DouglasTynan,PhD,ABPP,APARhoniqueShields-Harris,MD,MHA,FAAP,HealthServicesforChildrenwithSpecialNeeds,Inc.KathrynPhillips,MPH,QualisHealth