tb in south african mines - world health organization · tb in south african mines ilo/ who...
TRANSCRIPT

TB in South African mines
ILO/ WHO Consultation to promote the
engagement of workplaces
12th October 2009
Dr Salome Charalambous

The Aurum InstituteThe Aurum InstituteThe Aurum InstituteThe Aurum Institute
� Independent public benefit organisation that
originated in the South African gold mining industry
� Mission: “An internationally respected African institution that transforms health in the community.”
� TB and HIV prevention and treatment
� Medical research and health systems management
OverviewOverviewOverviewOverview
� Epidemiology of TB in miners
� TB control amongst miners:
� INH preventive therapy
� Active case finding
� TB risk reduction in HIV-infected miners:
� INH preventive therapy
� Active case finding
� Antiretroviral therapy

Epidemiology HIV and TBEpidemiology HIV and TBEpidemiology HIV and TBEpidemiology HIV and TB

TB in South African minersTB in South African minersTB in South African minersTB in South African miners
incidence per 100 000 pop p.a.

Risk factors for TB incidenceRisk factors for TB incidenceRisk factors for TB incidenceRisk factors for TB incidence
2.2
4.4
1.7
4.1
Age
HIV
Silicosis
<40
>40
-ve
+ve*
No
Early
Advanced*
* remained significant in multivariate analysis
p trend <0.001
(Corbett. Am J Resp Crit Care Med 2004:170:673-9)

TB risk with HIV & silicosisTB risk with HIV & silicosisTB risk with HIV & silicosisTB risk with HIV & silicosis
None Possible Probable Early
Silicosis
0
2
4
6
8
10
12
14
16
Per
100 p
ers
on y
ears
HIV-positive HIV-negative
(Corbett EL, AIDS 2000;14:2759-68 )

Silicosis & TB case fatalitySilicosis & TB case fatalitySilicosis & TB case fatalitySilicosis & TB case fatality
(Churchyard GJ, Int J Tuberc Lung Dis, 2000;4;705-712)
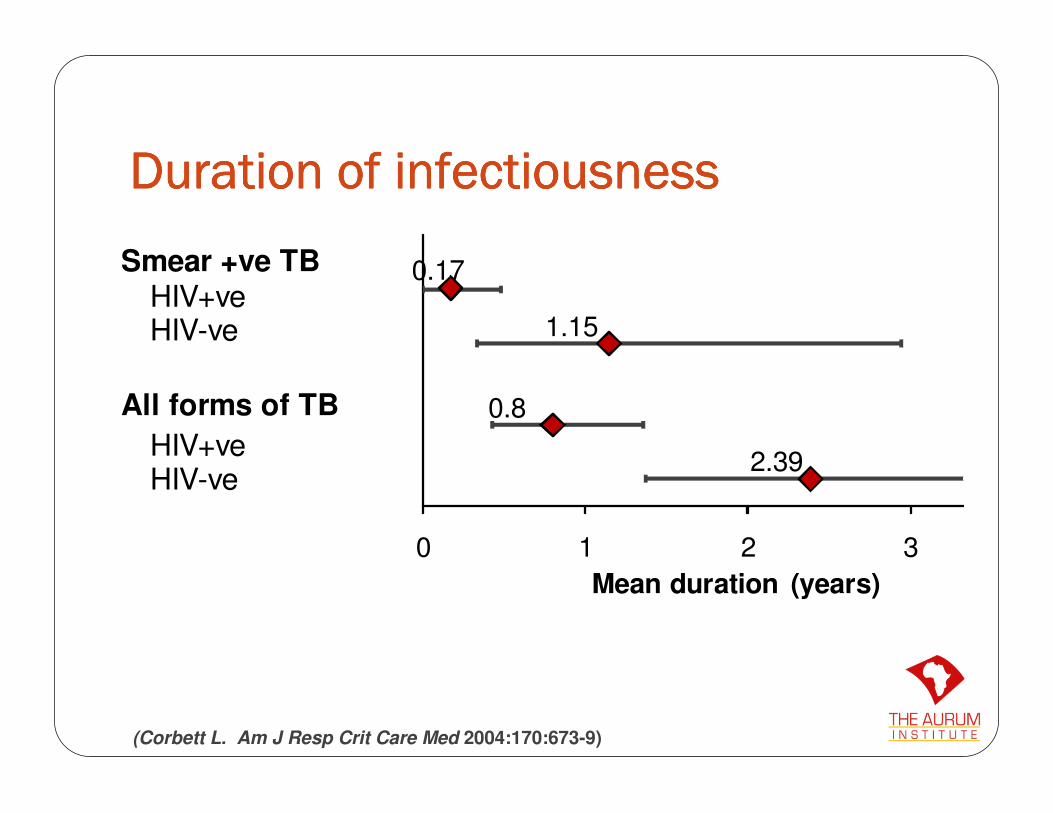
Duration of infectiousnessDuration of infectiousnessDuration of infectiousnessDuration of infectiousness
(Corbett L. Am J Resp Crit Care Med 2004:170:673-9)
Smear +ve TBHIV+veHIV-ve
All forms of TB
HIV+veHIV-ve
0.17
1.15
0.8
2.39
0 1 2 3
Mean duration (years)

TB recurrenceTB recurrenceTB recurrenceTB recurrence0.0
00.2
50.5
00.7
51.0
0
0 1 2 3analysis time
hiv3 = HIV negative hiv3 = HIV positive
Kaplan Meyer graph by HIV status
3.5 / 100 py
8.7 / 100 py
• Re-infection accounted for 68% of recurrence
(N=609, FU = 1.02 years)
(Charalambous S et al. Int J Tuberc Lung Dis 2008;12(8):942–948)

Strategies to reduce TB incidenceStrategies to reduce TB incidenceStrategies to reduce TB incidenceStrategies to reduce TB incidence

Reduced burden of
disease, health care
and compensation
costs
HIV prevention
Reduce HIV
incidence/prevalenceReduce silicosis
prevalence
Better dust control
Reduce latent
TB prevalence
Preventive therapy
Reduce active
TB prevalence
Increase active case finding
Reduce institutional TB
transmission
Reduce TB
transmissionReduce rate of
TB in HIV +ves
Diagnose HIV & treat
with ART
(Churchyard GJ, Corbett EL. Handbook of Occupational Health. SIMRAC, 2001)
Strategic framework for TB controlStrategic framework for TB controlStrategic framework for TB controlStrategic framework for TB control

morbidity
infectiousness
asymptomatic
symptomatic, does
not seek care
symptomatic, seeks
care
smear neg, culture neg
smear neg, culture pos
smear pos, culture pos
Passive TB case findingPassive TB case findingPassive TB case findingPassive TB case finding

morbidity
infectiousness
asymptomatic
symptomatic, does
not seek care
symptomatic, seeks
care
smear neg, culture neg
smear neg, culture pos
smear pos, culture pos
Active TB case finding

Active case findingActive case findingActive case findingActive case finding
(Lewis, Am J Resp Crit Care Med in press; Day J, Int J Tuberc Lung Dis 2006;10(5):523-9)
Miners (general) HIV-infected miners
N 1960 899
TB Prevalence 54 (2.7%) 44 (4.9%)
Sensitivity Specificity Sensitivity Specificity
% % % %
Symptoms* 29.4 90.3 59.1 75.6
Symptoms & CXR 49.0 89.4 90.9 59.2
*Symptoms: Night sweats, cough or reported weight loss

Community INH preventive therapy Community INH preventive therapy Community INH preventive therapy Community INH preventive therapy
(IPT): Thibela TB (IPT): Thibela TB (IPT): Thibela TB (IPT): Thibela TB
Standard TB control plus
Community wide IPT
Standard TB control

1954 1957 1960 1963 1966 1969 1972
500
1,000
1,500
2,000
2,500
3,000Passive CFT
INH RCT: 42% pop INH 12mos
INH all residents
TB
incid
ence r
ate
per
100,0
00 p
op p
a
Year
CommunityCommunityCommunityCommunity----wide IPTwide IPTwide IPTwide IPT
(Bethel(Bethel(Bethel(Bethel district, Alaska)district, Alaska)district, Alaska)district, Alaska)

Preliminary results: EnrollmentPreliminary results: EnrollmentPreliminary results: EnrollmentPreliminary results: Enrollment
0%
20%
40%
60%
80%
100%
1 3 5 7 9 11 13 15 17 19 21 23 25 27
recruitment month
% c
onsenting o
f clu
ste
r
1st and 2nd clusters
3rd and 4th clusters
5th, 6th and 7th clusters
8th cluster
N ~27,500

Reasonable retention is achievableReasonable retention is achievableReasonable retention is achievableReasonable retention is achievable0.0
00.2
50.5
00.7
51.0
0pro
portio
n s
till
in the s
tudy
0 30 60 90 120 150 180 210 240 270 300days since first dispensed INH
I1 I2 I3 I4 I5 I6 I8
Clusters
1st & 2nd
3rd & 4th
5th - 7th

INH is safeINH is safeINH is safeINH is safe
� 23,585 pts started INH between July 06 – 31Mar 09
� 126 adverse events recorded� 60 hypersensitivity� 49 peripheral neuropathy� 14 hepatitis� 3 convulsions
� 4 SAEs� 3 hepatitis; 1 definitely related� 1 convulsion; possibly related
� 33 deaths� 31 not related � 1 possibly related� 1 relationship to INH not coded

Control s : Lab subControl s : Lab subControl s : Lab subControl s : Lab sub----studystudystudystudy
First First First First
episodesepisodesepisodesepisodes
Retreatment Retreatment Retreatment Retreatment
episodesepisodesepisodesepisodes
Mean (95% CI)
INH resistance INH resistance INH resistance INH resistance
Controls : Routine dataControls : Routine dataControls : Routine dataControls : Routine data
(Van Halsema, IAS Cape Town 2009)

Strategies to reduce the risk of TB Strategies to reduce the risk of TB Strategies to reduce the risk of TB Strategies to reduce the risk of TB
among HIV positive minersamong HIV positive minersamong HIV positive minersamong HIV positive miners

pre-clinic phase
post-clinic phase
Effectiveness of IPT preEffectiveness of IPT preEffectiveness of IPT preEffectiveness of IPT pre----ARTARTARTART
(Grant AD, JAMA, 2005; 293:2719-2725)

0
500
1000
1500
2000
0 6 12 18 24
time (months)
no
. p
art
icip
an
ts
pre-clinic phase
post-clinic phase
Effectiveness of IPT preEffectiveness of IPT preEffectiveness of IPT preEffectiveness of IPT pre----ART ART ART ART
(Grant AD, JAMA, 2005; 293:2719-2725)
Adjusted IRR 0.54 (0.35-0.83)
IR: 10.9/100PYO
IR: 8.4/100PYO

Antiretroviral therapyAntiretroviral therapyAntiretroviral therapyAntiretroviral therapy
0
5
10
15
20
25
30
35
40
45
<90days 91-180days 181-365days 365-545days 546-720days 721 -900 days
TB
cases/1
00p
yrs
Days since ART initiation
TB incidence (first episode) following ART initiation
>900days

INH preventive therapy on ARTINH preventive therapy on ARTINH preventive therapy on ARTINH preventive therapy on ART0.0
00.2
50.5
00.7
51.0
0
0 5 10 15analysis time in months
inhstart = 0 inhstart = 1
Kaplan-Meier survival estimates
Unadjusted analysis
3.5/100pyrs vs 9.8/100pyrs
Hazard ratio: 0.37 (95%CI 0.25-0.54)
Adjusted analysis
Hazard ratio: 0.57 (95%CI 0.38-0.88)

Conclusions
� Miners high burden of disease due to dual risk factors: silicosis and HIV infection
� Additional strategies are required to control TB:� Active case finding
� INH preventive therapy may be an additional mechanism
� HIV infected individuals� ART
� INH preventive therapy

Aurum Institute for Health Research
Prof. G J Churchyard
Dr D Clark
Dr F Randera
Dr L Coetzee
V. Chihota
Dr C. Van Halsema
Dr J. Day
M. Luttig
T. Crawford
K. Mngadi
London School of Hygiene and Tropical Medicine
Dr K Fielding
Dr A Grant
Dr L Corbett
Dr J Lewis
Dr Y Hanifa
Acknowledgments

INH preventive therapy: Thibela TB INH preventive therapy: Thibela TB INH preventive therapy: Thibela TB INH preventive therapy: Thibela TB
Standard TB control
plus
Community wide IPT
Standard TB control

ResourcesResourcesResourcesResources• TB/HIV tool kit for South African businesses. Global
Health Initiative 2008
• Good Practice Guidance on HIV/AIDS, Tuberculosis and Malaria. International Chamber of Mines and Minerals 2007
• Isoniazid preventive therapy for patients with silicosis 2007. www.wahsa.net.
• Medical surveillance of silicosis and silica-related diseases. Expert Group Meeting. 2008