targeting the pi3k pathway in lymphoma - bhs.be · dr loïc ysebaert targeting the pi3k pathway in...
TRANSCRIPT
Dr Loïc Ysebaert
Targeting the PI3K pathway in lymphoma
Institut Universitaire du Cancer de Toulouse-Oncopôle,
CRCT Inserm UMR1037
Toulouse, France
Outline
• How PI-Kinases get activated in cancer ?
– Biology of PI-3Kinases
– In vitro rationale for PI-Kinase delta isoform targeting in lymphoma
• What are the clinical benefits / most common side effects ?
– Idelalisib in clinical trials
• How do lymphomatous cells evade to PI-3K inhibition ?
– Feedback loops
– Future of PI-3K inhibition strategies

Outline
• How PI-Kinases get activated in cancer ?
– Biology of PI-3Kinases
– In vitro rationale for PI-Kinase delta isoform targeting in lymphoma
• What are the clinical benefits / most common side effects ?
– Idelalisib in clinical trials
• How do lymphomatous cells evade to PI-3K inhibition ?
– Feedback loops
– Future of PI-3K inhibition strategies

p110ɑ
p110β
p110δ
p110g
p85ɑ,β
p55ɑ,γ
p50ɑ
p101
PI3K-C2ɑ
PI3K-C2β
PI3K-C2γ
hVps34p
?
p150
I
II
III PI
B
Class Regulation
Tyr kinase /
associations
Gβγ
?
?
PI / PI4P / PI4,5P2
CPIKRas-B C2
PI / PI4P
Adaptor
subunit
Catalytic
subunit
A
Ras-B: Ras binding domain Adapted from Vanhaesebroeck B, et al. Nat Rev Mol Cell Biol 2012;13:195–203.
The different PI3Ks (8 isoforms in mammals)
CPIKRas-B C2
CPIKRas-BC2 PX C2
CPIKC2
p110b
Only PI-3K class I A/B transform PI-4,5 P2 into PI-3,4,5 P3 = PIP3
Substrate/structure
Courtesy of B.Vanhaesebroeck
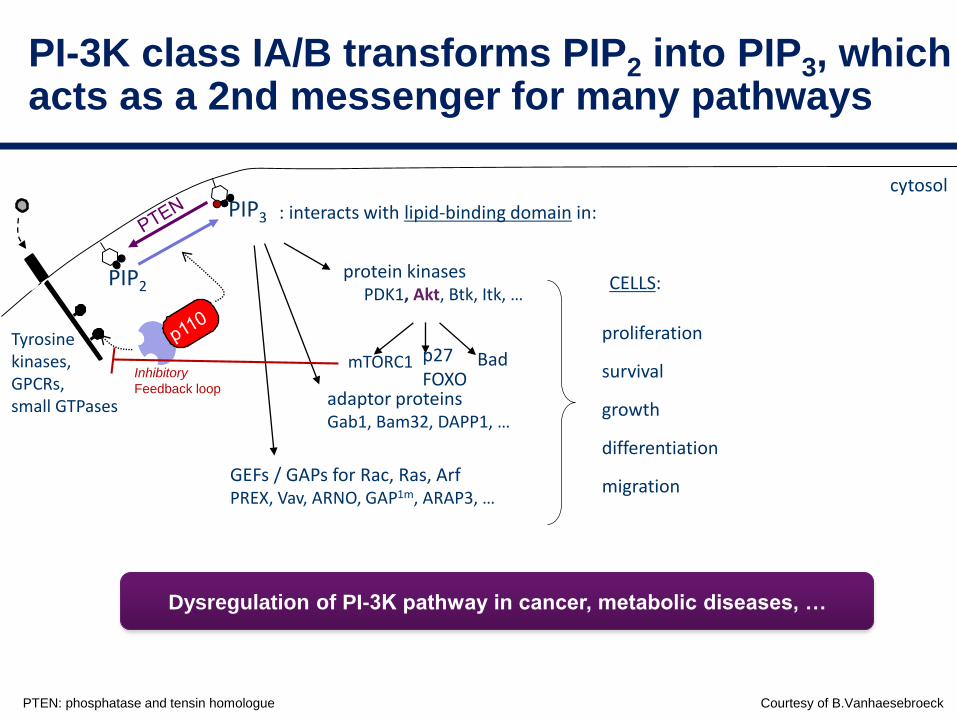
PI-3K class IA/B transforms PIP2 into PIP3, which acts as a 2nd messenger for many pathways
cytosol
Tyrosinekinases,GPCRs,small GTPases
proliferation
survival
growth
differentiation
migration
CELLS:
: interacts with lipid-binding domain in:
protein kinasesPDK1, Akt, Btk, Itk, …
adaptor proteinsGab1, Bam32, DAPP1, …
GEFs / GAPs for Rac, Ras, ArfPREX, Vav, ARNO, GAP1m, ARAP3, …
mTORC1 Badp27FOXO
PIP3
PIP2
PTEN: phosphatase and tensin homologue
Dysregulation of PI-3K pathway in cancer, metabolic diseases, …
Inhibitory
Feedback loop

Courtesy of B.Vanhaesebroeck
PI-3K : almost invariably activated in cancers
cytosol
PIP3
PIP2

PI-3Kinase class I isoforms in normal PI-3Kinase i d g b a
mainly mainlyadaptive innate
mainly inleukocytes
mainly inleukocytes
ubiquitous ubiquitous
PI-3kinase class I isoforms in leucocytes
Okkenhaug K, Science 2002, Vanhaesebroeck B, et al. PNAS 1997
p110δ is important in normal B-cell responses:
p110d
BtkSyk
CHEMOKINES[migration]GPCR-linked (d>g)
B-CELL ANTIGEN RECEPTORBAFF-R / CD19 / CYTOKINES …[(co)-stimulation]
ADHESION[retention,homing]
B-cell

mutation CNA
p110a <5% DLBCL MCL: 68.2%
DLBCL: 16.7%
p110b DLBCL:20%
p110g
p110d APDSImmune deficiency
predisposing to lymphoma
PIK3R1
PIK3R2 DLBCL: 20%
PIK3R3
PIK3R5
PTEN loss MCL, FL: 20%
GC-DLBCL: 30%
CLL: 5%
PI-3K is mainly triggered by chronic activation of cellular surface receptor(s)
How PI-3Kinases get activated in lymphoma ?
Gene mutations and chromosome copy number abnormalities (CNA) are rare
Idelalisib: low ORR

BCAP: B-cell adaptor for PI3K; BCR: B-cell receptor; BTK: Bruton's tyrosine kinase; GEF: guanine nucleotide exchange factor; mTOR: mammalian target of rapamycin; PI3K: phosphatidylinositol-3-kinase; PKC: protein kinase C; SFK: Src family kinase; SYK: spleen tyrosine kinase Coutre S, et al. Leuk Lymphoma 2015
Multiple culprits for chronic PI3Kactivation in lymphoma: it is not only the BCR !
Survival
Survival
Proliferation
Chemokine secretion
Motility
Homing
Retention
Adhesion
chronic BCR signaling

1. Herman SE, et al. Blood 2010;116:2078‒882. Yahiaoui OI, et al. BMC Cancer 2014; 14:565
3. Leseux L, et al. Blood 2006;108:4156–4162
Chronic BCR signaling leads to constitutive PI3Kd activity
• PI3K pathway may be constitutively activated in some patients with
follicular2,3, marginal zone, or lymphoplasmacytic lymphomas
CLL cells have a significantly higher intrinsic PI3K activity
than normal B cells (p=0.006)1P
I3K
acti
vit
y p
er
µg
of
pro
tein
1.75
1.00
0.75
0.50
0.25
0
1.25
1.50
CLL cellsNormal B cells
Hoellenriegel J, Blood 2011.
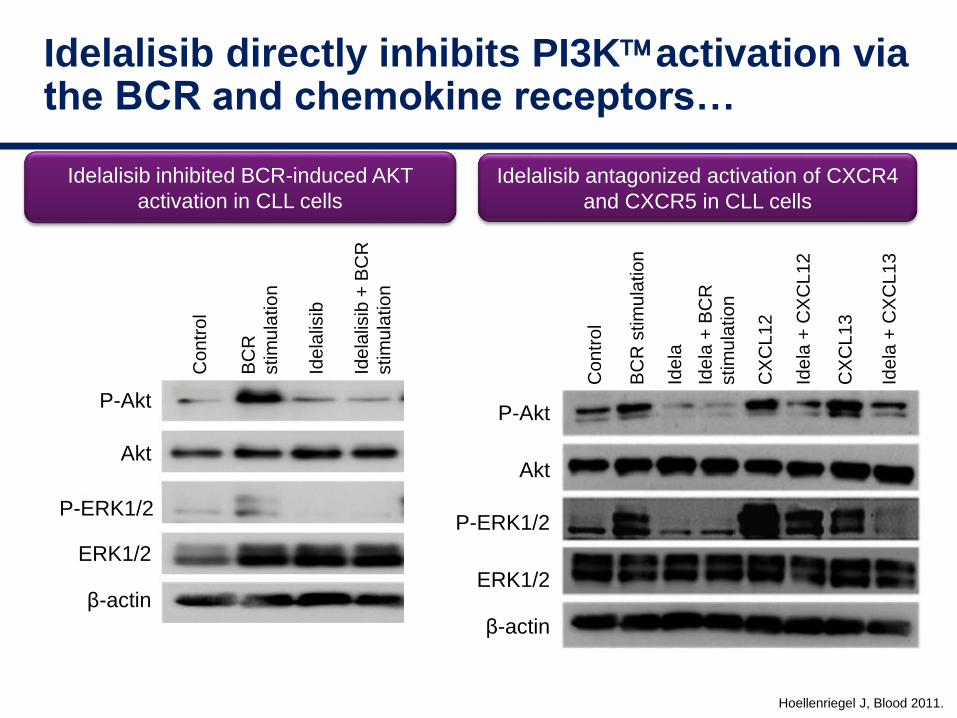
Idelalisib directly inhibits PI3Kactivation via the BCR and chemokine receptors…
Co
ntr
ol
BC
R
stim
ula
tion
Ide
lalis
ib
Idela
lisib
+ B
CR
stim
ula
tio
nP-Akt
Akt
ERK1/2
β-actin
P-ERK1/2
Idelalisib inhibited BCR-induced AKT
activation in CLL cells
Idelalisib antagonized activation of CXCR4
and CXCR5 in CLL cells
P-Akt
Akt
ERK1/2
β-actin
P-ERK1/2
Co
ntr
ol
BC
R s
tim
ula
tio
n
Ide
la+
BC
R
stim
ula
tio
n
CX
CL
12
Ide
la
Ide
la+
CX
CL
12
CX
CL
13
Ide
la+
CX
CL
13
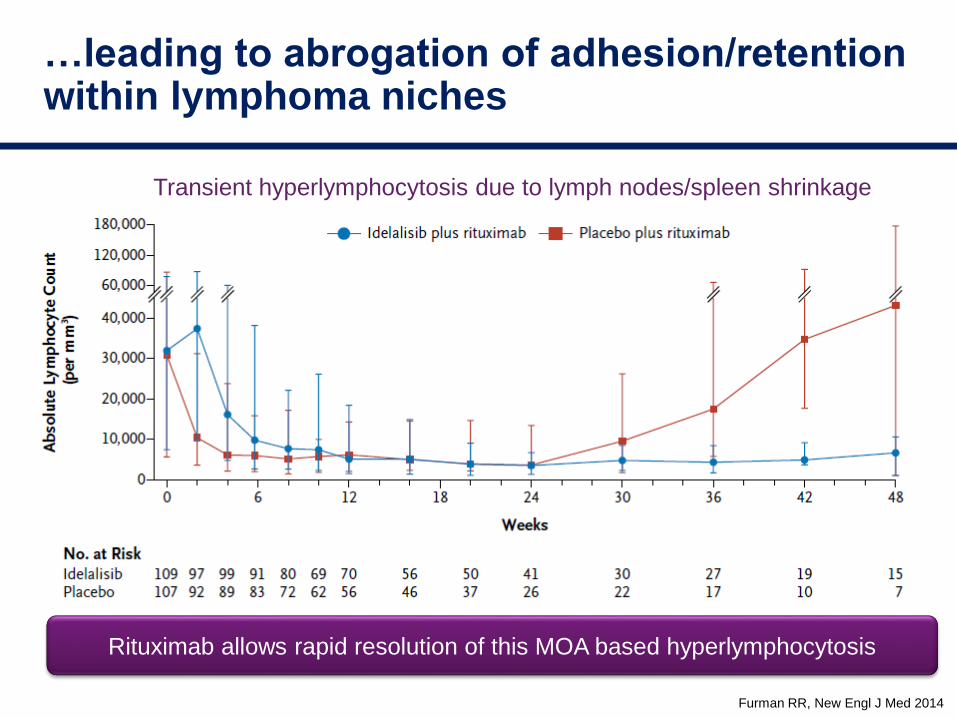
Furman RR, New Engl J Med 2014
…leading to abrogation of adhesion/retention within lymphoma niches
Rituximab allows rapid resolution of this MOA based hyperlymphocytosis
Transient hyperlymphocytosis due to lymph nodes/spleen shrinkage
Outline
• How PI-Kinases get activated in cancer ?
– Biology of PI-3Kinases
– In vitro rationale for PI-Kinase delta isoform targeting in lymphoma
• What are the clinical benefits / most common side effects ?
– Idelalisib in clinical trials
• How do lymphomatous cells evade to PI-3K inhibition ?
– Feedback loops
– Future of PI-3K inhibition strategies
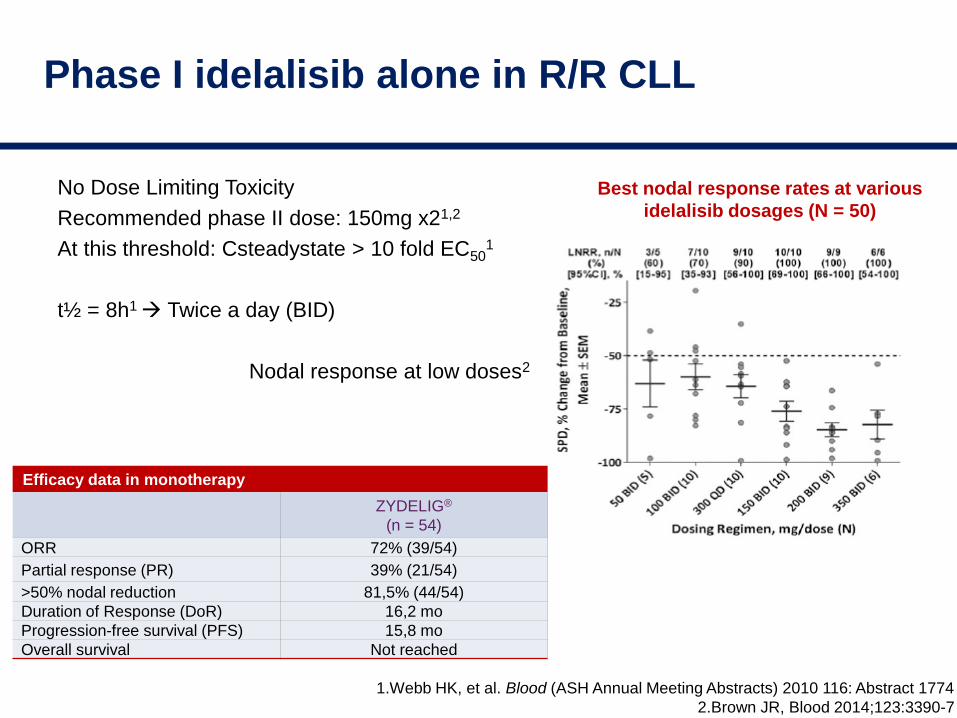
Phase I idelalisib alone in R/R CLL
No Dose Limiting Toxicity
Recommended phase II dose: 150mg x21,2
At this threshold: Csteadystate > 10 fold EC501
t½ = 8h1 Twice a day (BID)
Nodal response at low doses2
1.Webb HK, et al. Blood (ASH Annual Meeting Abstracts) 2010 116: Abstract 1774
2.Brown JR, Blood 2014;123:3390-7
Best nodal response rates at various
idelalisib dosages (N = 50)
Efficacy data in monotherapy
ZYDELIG®
(n = 54)
ORR 72% (39/54)
Partial response (PR) 39% (21/54)
>50% nodal reduction 81,5% (44/54)
Duration of Response (DoR) 16,2 mo
Progression-free survival (PFS) 15,8 mo
Overall survival Not reached
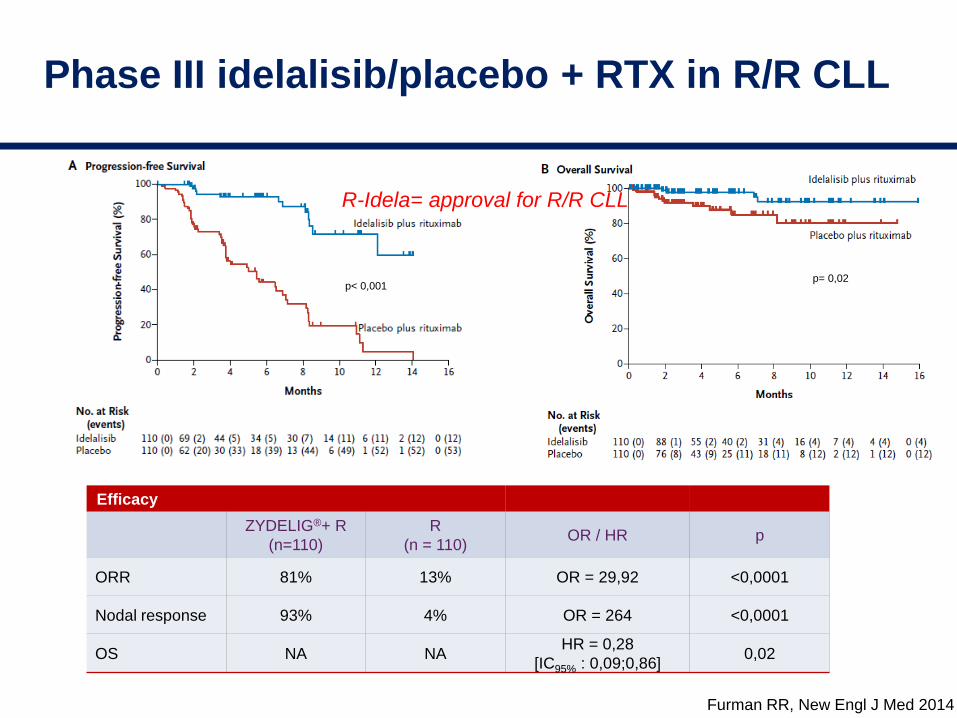
Phase III idelalisib/placebo + RTX in R/R CLL
Furman RR, New Engl J Med 2014
Efficacy
ZYDELIG®+ R
(n=110)
R
(n = 110)OR / HR p
ORR 81% 13% OR = 29,92 <0,0001
Nodal response 93% 4% OR = 264 <0,0001
OS NA NAHR = 0,28
[IC95% : 0,09;0,86]0,02
p< 0,001p= 0,02
R-Idela= approval for R/R CLL

Phase II idelalisib alone in R/R indolent NHL
-100
-75
-25
0
-50a
+25
+50
Individual Patients (N=125)
SP
D o
f M
easu
red
Lym
ph
No
des
,B
est
% C
han
ge
fro
m B
asel
ine
•90% had improvement in lymphadenopathy
•57% had ≥50% decrease from baseline
Gopal A, New Engl J med 2014
Idela = approval for double-refractory FL
median PFS 11 mo
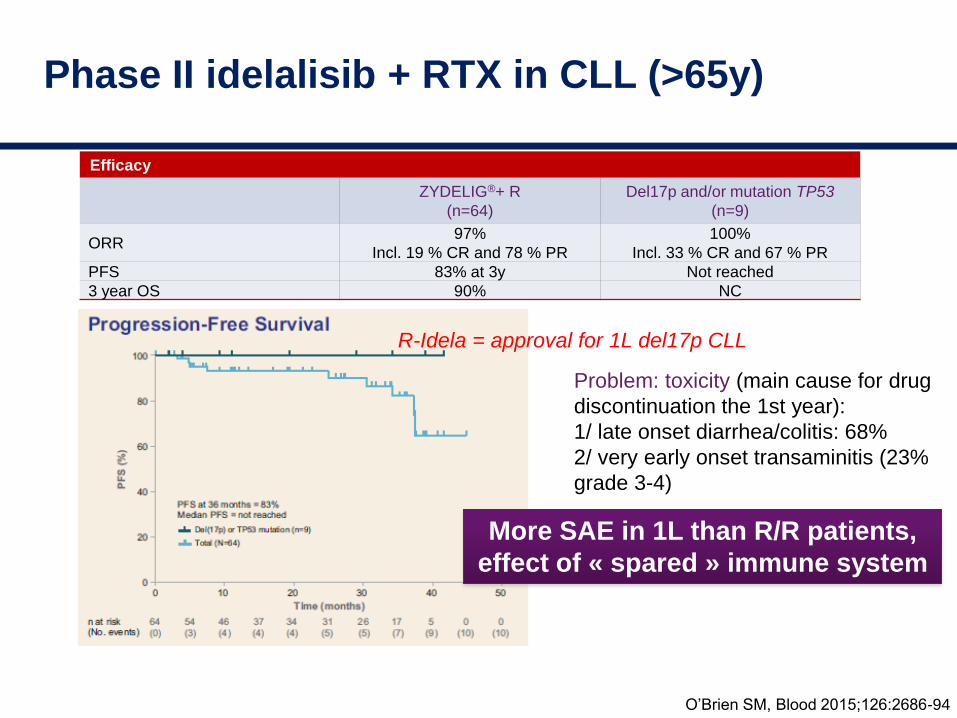
Phase II idelalisib + RTX in CLL (>65y)
O’Brien SM, Blood 2015;126:2686-94
Efficacy
ZYDELIG®+ R
(n=64)
Del17p and/or mutation TP53
(n=9)
ORR97%
Incl. 19 % CR and 78 % PR
100%
Incl. 33 % CR and 67 % PR
PFS 83% at 3y Not reached
3 year OS 90% NC
Problem: toxicity (main cause for drug
discontinuation the 1st year):
1/ late onset diarrhea/colitis: 68%
2/ very early onset transaminitis (23%
grade 3-4)
More SAE in 1L than R/R patients,
effect of « spared » immune system
R-Idela = approval for 1L del17p CLL

Summary of most common AEs
Compilation of trials: phase III (0116) and 7 phase I-II trials, idelalisib alone or with RTX (N=600)
Allergy/auto-immunity
On-target Top 5 to know
FrequencyReversible at short Tx
interruptionTime of onset % Grade ≥3
Infections Yes No specific pattern ≥10%
Neutropenia Yes (+G-CSF if >grade 3) 1-6mo≥10%
2nd most frequent (40%)
Increased transaminase
levelsYes 1-3 mo ≥10%
Diarrhoea/colitis
NO, but YES at prolonged
interruption 4 wks
(+budesonide if grade 3-4)
6-24mo
DELAYED
≥10%
Most frequent (40-60%)
Rash Yes 0-1 mo 1 to <10%
Increased triglyceride
levelsYes 0-1 mo 1 to <10%
Pyrexia no Tx interruption needed 0-1 mo 1 to <10%
Pneumonitis/pneumonitis NO 3-6mo 1 to <10%
Adapted from: Zydelig SmPC (May 2015; available at www.ema.europa.eu)

Auto-immunity with idelalisib ?
Coutre S, Leuk Lymphoma 2015
Nature 2014:509:407
PI-3Kd inhibition blocks Treg differentiation favoring CTL expansion
This immunomodulatory effect is INdependent from PI-3Kd activity within tumor cells
Outline
• How PI-Kinases get activated in cancer ?
– Biology of PI-3Kinases
– In vitro rationale for PI-Kinase delta isoform targeting in lymphoma
• What are the clinical benefits / most common side effects ?
– Idelalisib in clinical trials
• How do lymphomatous cells evade to PI-3K inhibition ?
– Feedback loops
– Future of PI-3K inhibition strategies
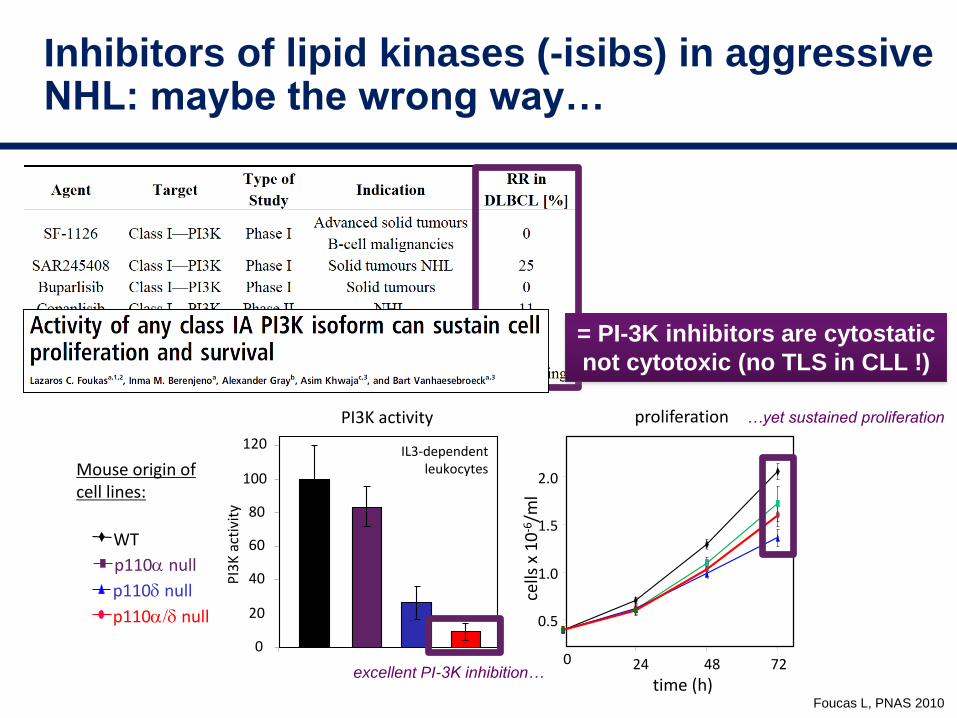
Foucas L, PNAS 2010
Inhibitors of lipid kinases (-isibs) in aggressive NHL: maybe the wrong way…
cells
x 1
0-6
/ml
time (h)
0.5
1.0
1.5
2.0
24 48 720
proliferation
p110a null
p110d null
p110a/d null
WT
0
20
40
60
80
100
120
PI3K activity
IL3-dependent leukocytes
PI3
K a
ctiv
ity
Mouse origin of cell lines:
excellent PI-3K inhibition…
…yet sustained proliferation
= PI-3K inhibitors are cytostatic
not cytotoxic (no TLS in CLL !)
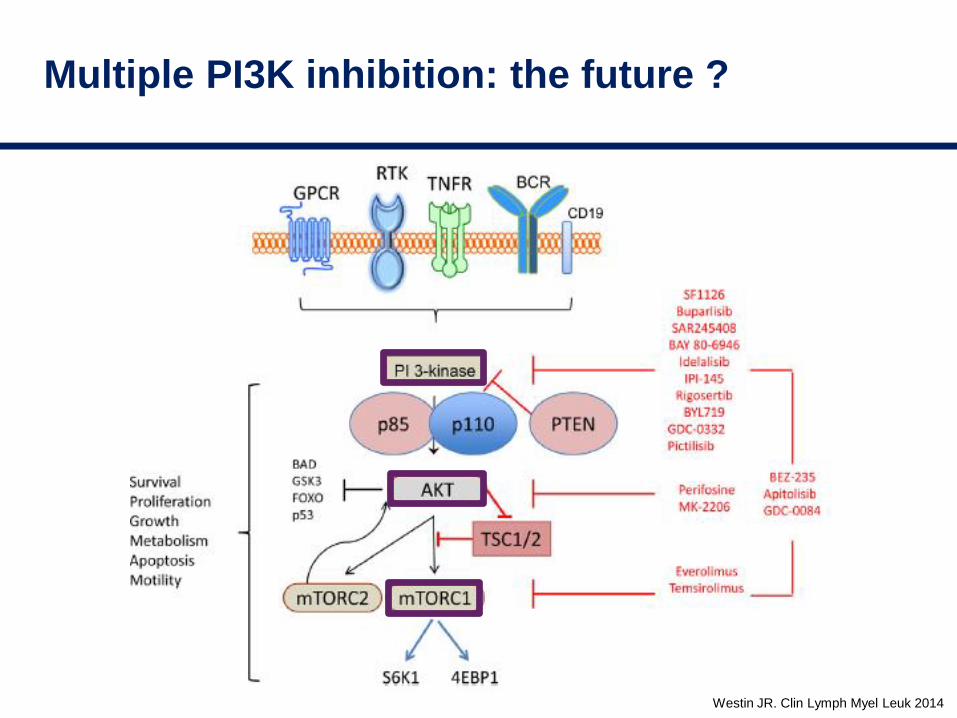
Westin JR. Clin Lymph Myel Leuk 2014
Multiple PI3K inhibition: the future ?
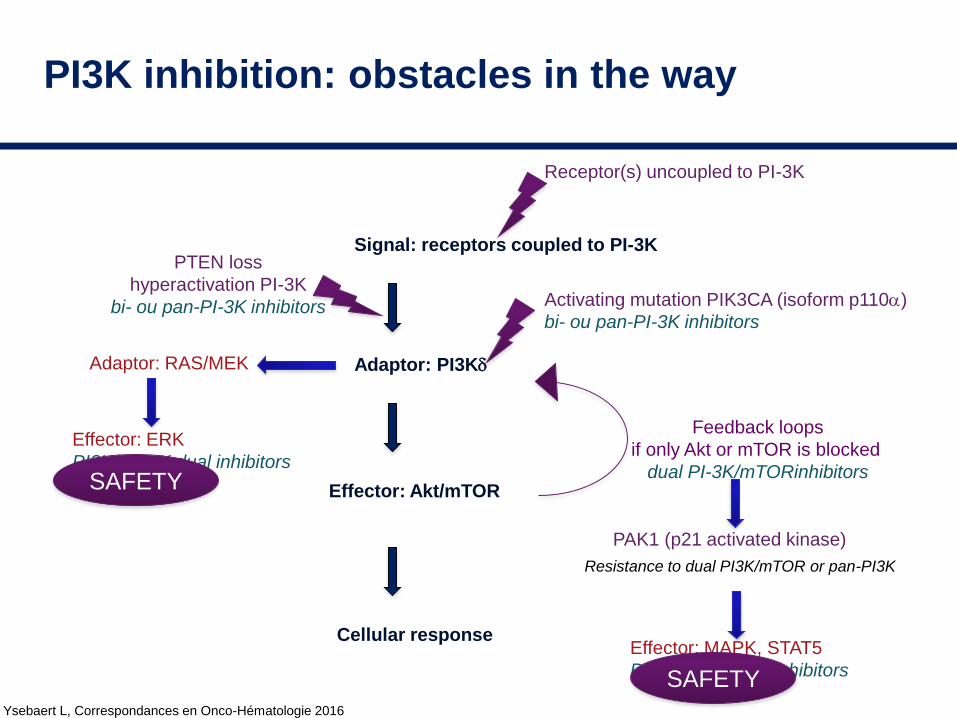
Ysebaert L, Correspondances en Onco-Hématologie 2016
PI3K inhibition: obstacles in the way
Signal: receptors coupled to PI-3K
Adaptor: PI3Kd
Effector: Akt/mTOR
Cellular response
Feedback loops
if only Akt or mTOR is blocked
dual PI-3K/mTORinhibitors
Activating mutation PIK3CA (isoform p110a)
bi- ou pan-PI-3K inhibitors
PTEN loss
hyperactivation PI-3K
bi- ou pan-PI-3K inhibitors
Adaptor: RAS/MEK
Effector: ERK
PI3K/MEKK dual inhibitors
Receptor(s) uncoupled to PI-3K
Effector: MAPK, STAT5
PI3K/MEKK dual inhibitors
Resistance to dual PI3K/mTOR or pan-PI3K
PAK1 (p21 activated kinase)
SAFETY
SAFETY

Will M, Cancer Discov 2014
PI3K inhibition: use alternative conceptsModel: breast cancer Her2 activated, PIK3CA mutated
Apoptosis = PI3K/ERK rather than PI3K/Akt, avoid mTOR inhibition
Low dose range and pulsatile inhibition of PI-3K = combination of AKT+MEK
BUT much less toxicity and no feedback loop reactivating PI3K !
PD901: ERKi (5d/wk)
MK2206: AKTi (5d/wk)
PD+MK
BAY80-6946: PI3Ka/d i
(3d/wk)
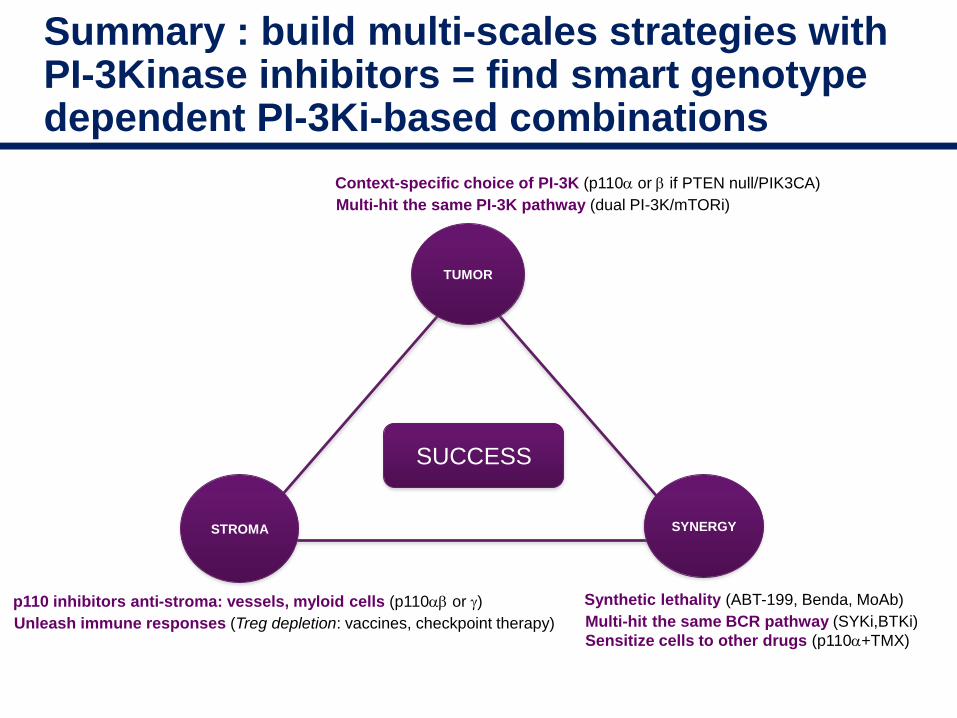
Summary : build multi-scales strategies with PI-3Kinase inhibitors = find smart genotype dependent PI-3Ki-based combinations
SUCCESS
TUMOR
SYNERGYSTROMA
Synthetic lethality (ABT-199, Benda, MoAb)
Multi-hit the same BCR pathway (SYKi,BTKi)
Sensitize cells to other drugs (p110a+TMX)
Context-specific choice of PI-3K (p110a or b if PTEN null/PIK3CA)
Multi-hit the same PI-3K pathway (dual PI-3K/mTORi)
p110 inhibitors anti-stroma: vessels, myloid cells (p110ab or g)
Unleash immune responses (Treg depletion: vaccines, checkpoint therapy)
Summary : build multi-scales strategies with PI-3Kinase inhibitors: beware the AEs !
Transaminitis Interstitial pneumopathyDiarrhea/colitis Neutropenia