taiwan tanabe 陳榮明 jimmy chen 藥師 - 地區經理 嘉南 – 藥學 for cardiovascular...
TRANSCRIPT

TAIWAN TANABE
陳榮明 Jimmy Chen 藥師 - 地區經理
嘉南 –藥學
FOR CARDIOVASCULAR DISEASES
CONCORTM 5mg/1.25mg
Bisoprolol hemifumarate
Indications: Hypertension,Angina,CHFDosage:5 ~ 10mg QD ,1.25-QD
TANABE/MERCK KGaA
The Highest ß1-selectivity. The Best Quality of Life
TAIWAN TANABE

Are the β-blockers all the same?

TAIWAN TANABE
Classification of -Blockers
-Blockers
1-Selective Non-1-Selective
Without ISA
Bisoprolol
Atenolol
Betaxolol
Metoprolol
With ISA
Acebutolol
Without ISA
Nadolol
Propranolol
Sotaolol
Timolol
Carvedilol
With ISA
Carteolol
Pindolol
Labetalol
ISA:Intrinsic Sympathomimetic ActivityAdapted from: European Heart Journal (2004) 25, 1341-1362

Secondary prevention of myocardial infarction with different types of β -blockers
-30
-20
-10
%
Reduction of mortality β1-selective without ISA
Non-selective without ISA
β1-selective with ISA
Non-selective with ISA
Adapted form:Progress in Cardiovascular Diseases. 27(5):335-71, 1985 Mar-Apr
β-blockers without ISA β-blockers with ISA
TAIWAN TANABE

β1 selectivity:

β 2
Kidney β 1 Renin release
Smooth muscle of bronchi β 2 Bronchodilatation
α 1 Vasoconstriction
β 2 Vasodilatation
β 1 Vasodilatation(cononary)
α 2 Inhibition of lipolysis
β 2>β 1 Stimulation oflipolysis
α 1 Glycogenolysis
α 2 Inhibition of insulinrelease
β 2 Stimulation of insulinrelease
Pancreas
Fat tissue
Liver
β 2 Glycogenolysis ,Gluconeogenesis
Myocardium β 1 Stimulation ofcontractility and HR
Blood vessel smooth muscle
Adapted from:European Heart Journal. 21(5):354-64, 2000 Mar
Physiological effect of adrenergic receptor

300:1
1:35 1:35
1:75
increasing ß1-selectivity
increasing ß2-selectivity
ICI 118.551
1.8:1 Propranolol
Atenolol Betaxolol
Bisoprolol
no selectivity
Ratio of constants of inhibition
1:20
Metoprolol
Bisoprolol: ß1-selectivity of various ß-blockersBisoprolol: ß1-selectivity of various ß-blockers
Wel
lste
in A
et a
l. J
Car
diov
asc
Pha
rmac
ol 1
986;
8 (
Sup
pl. 1
1): 3
6-40
Wel
lste
in A
et a
l. E
ur H
eart
J 1
987;
8 (
Sup
pl. M
): 3
–8

b 21 h3 6 12 1 3 6 12 1 3 6 12
4 8 24 b 2 4 8 24 b 2 4 8 24
Placebo Bisoprolol(20mg) Atenolol(100mg)
50
70
90
7
8
9
AWR (cm H2 O/I/s)
HR (beats/min)
b = beforen = 12
± SEM
Bisoprolol: ß1-selectivity and lung function in coronary patients with chronic obstructive bronchitis
Bisoprolol: ß1-selectivity and lung function in coronary patients with chronic obstructive bronchitis
Dor
ow P
. Eur
J C
lin P
harm
acol
198
6; 3
1:14
3–14
7
x

Propranolol
Metoprolol
Labetalol
Carvedilol
Atenolol
Nadolol
Sotalol
PindololTimolol
Lipophilic Hydrophilic
TAIWAN TANABE
Balance Clearance
Bisoprolol
TAIWAN TANABE
*dose-dependent
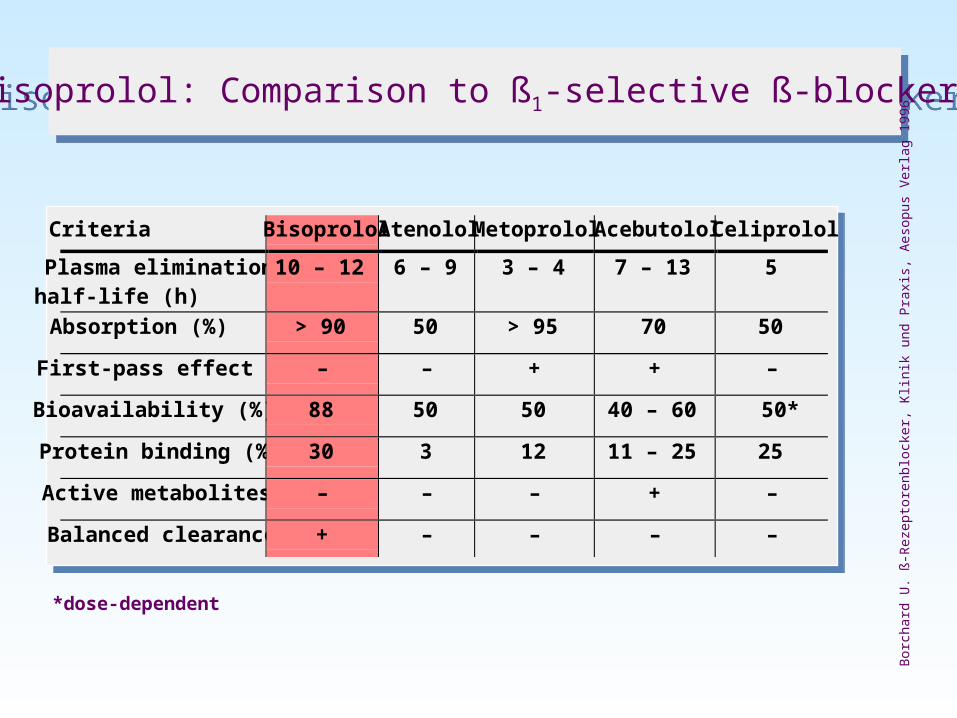
Criteria Bisoprolol Atenolol Metoprolol Acebutolol Celiprolol
Plasma eliminationhalf-life (h)
10 – 12 6 – 9 3 – 4 7 – 13 5
Absorption (%) > 90 50 > 95 70 50
First-pass effect – – + + –
Bioavailability (%) 88 50 50 40 – 60 50*
Protein binding (%) 30 3 12 11 – 25 25
Active metabolites – – – + –
Balanced clearance + – – – –
Bisoprolol: Comparison to ß1-selective ß-blockersBisoprolol: Comparison to ß1-selective ß-blockers
Bor
char
d U
. ß-R
ezep
tore
nblo
cker
, Klin
ik u
nd P
raxi
s, A
esop
us V
erla
g 19
96
Three indications of BisoprololThree indications of Bisoprolol
Essential Hypertension
Angina
Stable Chronic Heart Failure (Moderate~Severe)
Three Indications of BisoprololThree Indications of Bisoprolol
Essential Hypertension
Angina
Stable Chronic Heart Failure (Moderate~Severe)

28 56 84 91 days
Bisoprolol
Bisoprolol 5 mg n = 15/group
Bisoprolol 10 mg
Bisoprolol 20 mg
Placebo Bisoprolol PlaceboΔ SBP
0
– 10
– 20
– 30
– 40
(mm
Hg
)
28 56 84 91 days0
Δ DBP
– 10
– 20
– 30
(mm
Hg
)
Bisoprolol: Dose-dependent blood pressure reductionin hypertensives
Bisoprolol: Dose-dependent blood pressure reductionin hypertensives
Kirs
ten
R e
t al.
J C
ardi
ovas
c P
harm
acol
198
6; 8
(S
uppl
. 11)
: 113
–121
± SEMx

Bisoprolol: Dose-dependent blood pressure reduction3 and 24 hours after administration
Bisoprolol: Dose-dependent blood pressure reduction3 and 24 hours after administration
Da
vid
ov
ME
et
al.
Clin
Ca
rdio
l 19
94
; 1
7: 2
63
–2
680
– 2
– 4
– 6
– 8
– 10
– 12
– 14
– 16
DB
P s
itti
ng
(m
m H
g)
Bisoprolol dose
Placebo 5 mg 10 mg 20 mg
–3.6 –3.0
–10.5
–7.4
–12.7 –12.8
–14.7
–13.4
3 h p.a.
24 h p.a.
3 h p.a.
24 h p.a.
n = 240
S ± SEM
SBP
DBP
180
160
140
120
100
80
60
1 3 5 7 9 11 13 15 17 19 21 23 h
(mm
Hg
)
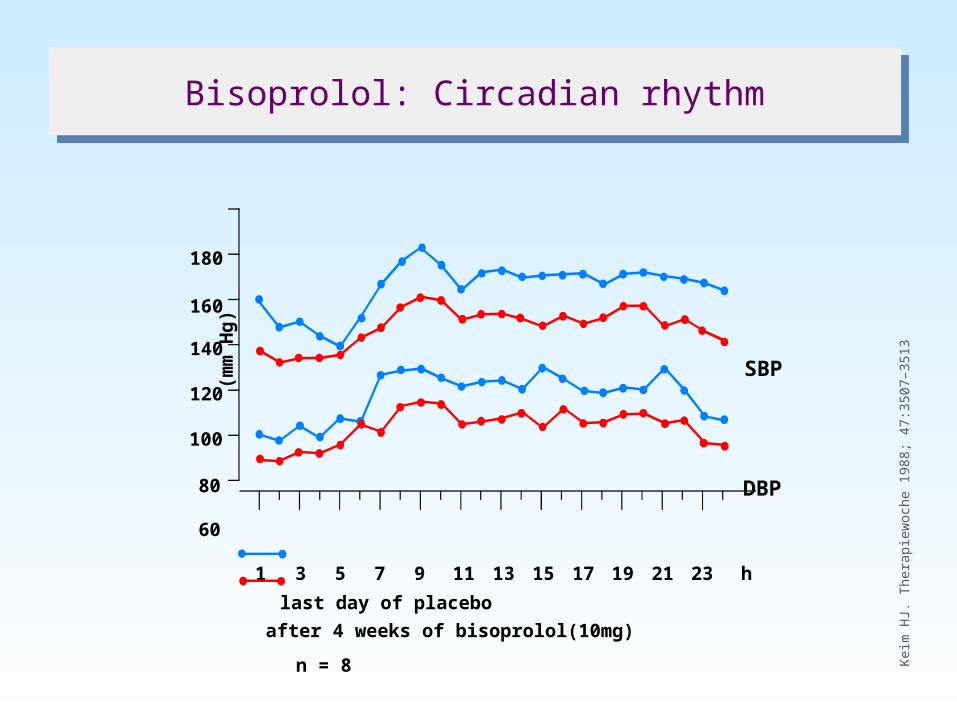
last day of placebo
after 4 weeks of bisoprolol(10mg)
n = 8
Bisoprolol: Circadian rhythmBisoprolol: Circadian rhythm
Kei
m H
J. T
hera
piew
oche
198
8; 4
7:35
07–3
513

Bisoprolol: Treatment of hypertensionin comparison to atenolol
Bisoprolol: Treatment of hypertensionin comparison to atenolol
Ne
ute
l JM
et
al.
Am
J M
ed
19
93
; 9
4:1
81
–1
87
0
–5
–10
–15
–2010 a.m. 4 p.m. 10 p.m. 4 a.m. 10 a.m.
time of day
me
an
ch
an
ge
in d
iast
olic
blo
od
pre
ssu
re
(mm
Hg )
DBPBisoprolol (n = 107)
night
Atenolol (n = 96)
doseintake

BisoDIAS Endgültig 27
180
140
100
60
0 12 15 18 21 24 27 30 33 36
102 102 97 102 101 102 102 102 100 102
months
SBP (mm Hg)
DBP (mm Hg)
HR (beats/min)
n =
Bisoprolol: Long-term treatment of hypertensionBisoprolol: Long-term treatment of hypertension
Gie
seck
e H
G e
t al.
J C
ardi
ovas
c P
harm
acol
199
0; 1
6 (S
uppl
5):
175

Diabetic Hypertension
Beta-Blockers:Continue to surprise us

JNC ⅦClinical Trial and Guideline Basis for Compelling Indications for Individual Drug Classes
JNC ⅦClinical Trial and Guideline Basis for Compelling Indications for Individual Drug Classes
High-Risk Conditions With Compelling Indication*
Heart Failure
Post-myocardial infarction
High coronary disease risk
Diabetes
Chronic kidney disease
Recurrent stroke prevention
Recommended Drugs
Diuretic Beta-Blocker ACE Inhibitor ARB CCB Aldosterone Antagonist
Clinical Trial Basis
ACC/AHA Heart Failure Guideline, MERIT-HF, COPERNICUS, CIBIS, SOLVD, AIRE, TRACE, ValHERT, RALES
ACC/AHA Post-MI Guideline, BHAT, SAVE, Capricorn, EPHESUS
ALLHAT, HOPE, ANBP2, LIFE, CONVINCE
NKF-ADA Guidelin, UKPKS, ALLHAT
NKF Guideline, Captopril Trial, RENAAL, IDNT, REIN, AASK
PROGRESS
• • • • •
• • • • •
• • • •
• • •
• •
• •
Adapted from: JAMA. 2003 ; 289 : 2560-2572

UK Prospective Diabetes Study
largest multi-centre randomised controlled trial of different therapies of Type 2 diabeteslargest study ever conducted in the prevention of diabetic complications in type II diabetics:study duration: 1977 - 199723 clinical centrespatient population: 5102 type 2 diabetic patients53,000 patient years follow-up

UKPDS Blood Pressure Control Study tight vs. less tight: results
Tight blood pressure control significantly reduces risks for
any diabetes-related endpoint 24% (p=0.0046)diabetes-related deaths 32% (p=0.019)stroke 44% (p=0.013)microvascular disease 37% (p=0.0092)heart failure 56% (p=0.0043)retinopathy progression 34% (p=0.0038)deterioration of vision 47% (p=0.0036)

UKPDS Study
Adapted from:BMJ, Volume 317(7160).September 12, 1998.713-720
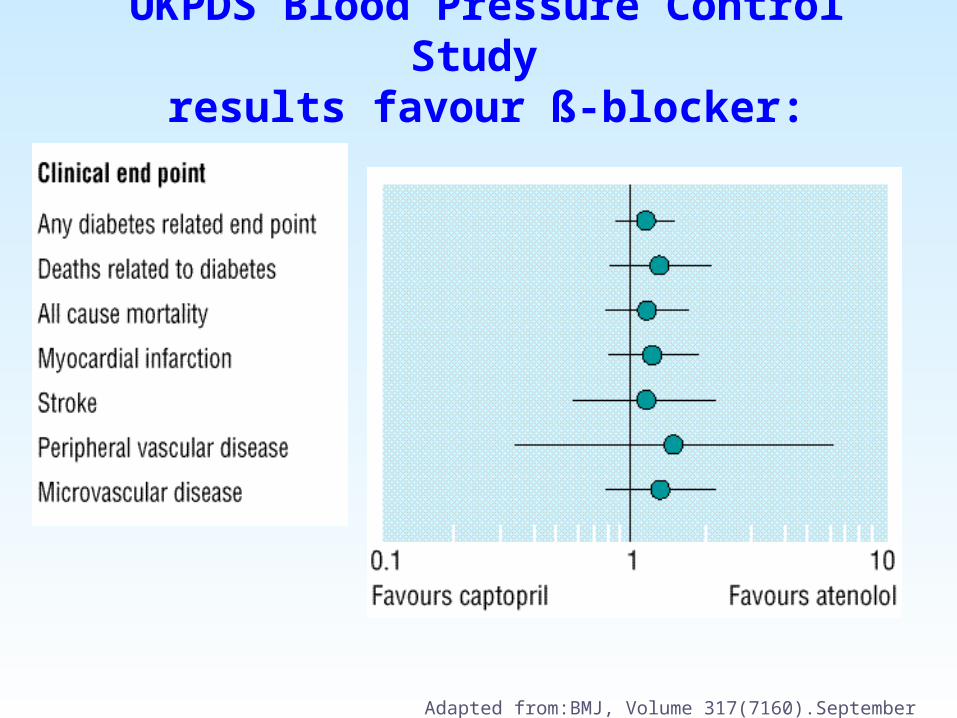
UKPDS Blood Pressure Control Study results favour ß-blocker:
Adapted from:BMJ, Volume 317(7160).September 12, 1998.713-720

After UKPDS
management of blood pressure was not a high priority for type 2 diabetics
first choice treatment
ACE inhibitors
management of blood pressure was not a high priority for type 2 diabetics
first choice treatment
ACE inhibitors
management of blood pressure should have high priority in the treatment of type 2 diabetesfirst choice treatment
ACE inhibitor or or Beta-blockerBeta-blocker
management of blood pressure should have high priority in the treatment of type 2 diabetesfirst choice treatment
ACE inhibitor or or Beta-blockerBeta-blocker
Before UKPDS
UKPDS Blood Pressure Control Study implications

Treatment of Hypertensionin Adults With Diabetes
A-level evidence: Initial drug therapy may be with ACE inhibitors, ARBs, β-blockers, or diuretics. Additional drugs may be chosen from these classes or another drug class. In patients with a recent myocardial infarction, β-blockers, in addition,should be considered to reduce mortality.
•Adapted from:DIABETES CARE, VOLUME 25, NUMBER 1, JANUARY 2002

Three Indications of BisoprololThree Indications of Bisoprolol
Essential Hypertension
Angina
Stable Chronic Heart Failure (Moderate~Severe)

Objectives:
To evaluate the effects of Bisoprolol o.d.
and Nifedipine slow release b.i.d.on the occurrence and circadian
distributionof ischaemic episodes in patients
with stable angina pectoris
Randomised double-blind controlled studywith two parallel groups
T I B B STotal Ischaemic Burden Bisoprolol Study
T I B B STotal Ischaemic Burden Bisoprolol Study
von
Arn
im T
h et
al.
JAC
C 1
995;
1: 2
31–2
30

10 days 4 weeks 4 weeks
48 h Holter 48 h Holter
History ETT Inclusion for prephase
If > 2 ischaemicepisodes,inclusion for active treatment
20 mg o.d. Bisoprolol
10 mg o.d. Bisoprolol
40 mg b.i.d. Nifedipine s.r.20 mg b.i.d. Nifedipine s.r.
Placebo
48 h Holter
TIBBS: Flow chartTIBBS: Flow chart
von
Arn
im T
h et
al.
JAC
C 1
995;
1: 2
31–2
38

BisoDIAS Endgültig 43
No./48 h
Baseline 40 mg20 mgBaseline 20 mg10 mg
Nifedipine s.r. b.i.d. (n = 112)Bisoprolol o.d. (n = 111)
2
4
6
8
10
0
TIBBS: Number of ischaemic episodes at baseline,on low dose and on high dose
TIBBS: Number of ischaemic episodes at baseline,on low dose and on high dose
von
Arn
im T
h et
al.
JAC
C 1
995;
1: 2
31–2
38
±SEMx
BisoDIAS Endgültig 44
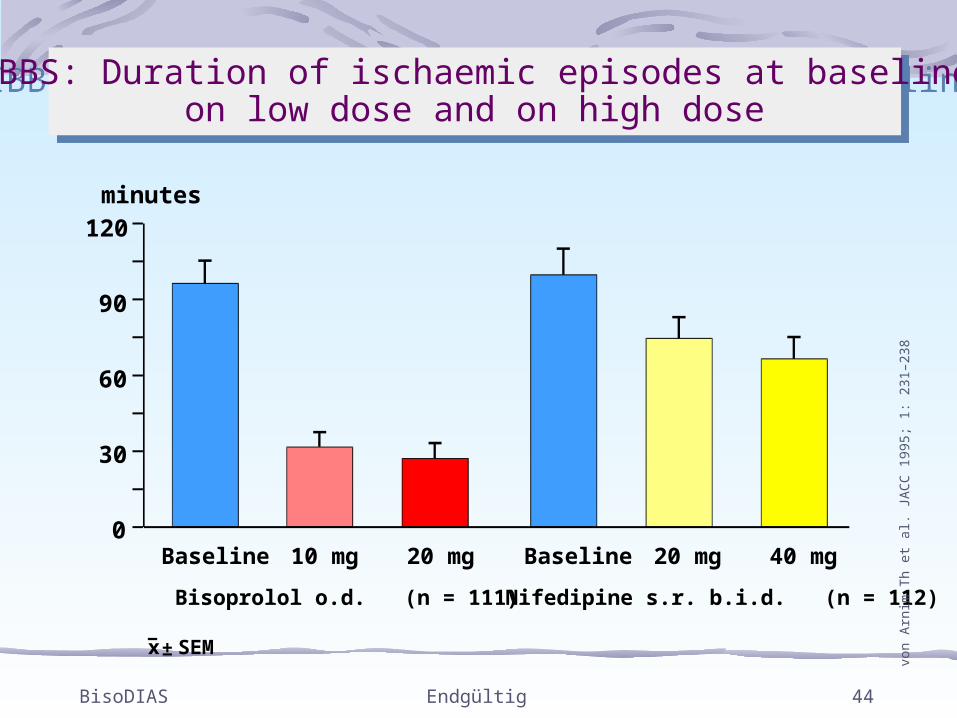
minutes120
90
60
30
0Baseline 40 mg20 mgBaseline 20 mg10 mg
Nifedipine s.r. b.i.d. (n = 112)Bisoprolol o.d. (n = 111)
TIBBS: Duration of ischaemic episodes at baseline,on low dose and on high dose
TIBBS: Duration of ischaemic episodes at baseline,on low dose and on high dose
von
Arn
im T
h et
al.
JAC
C 1
995;
1: 2
31–2
38
±SEMx
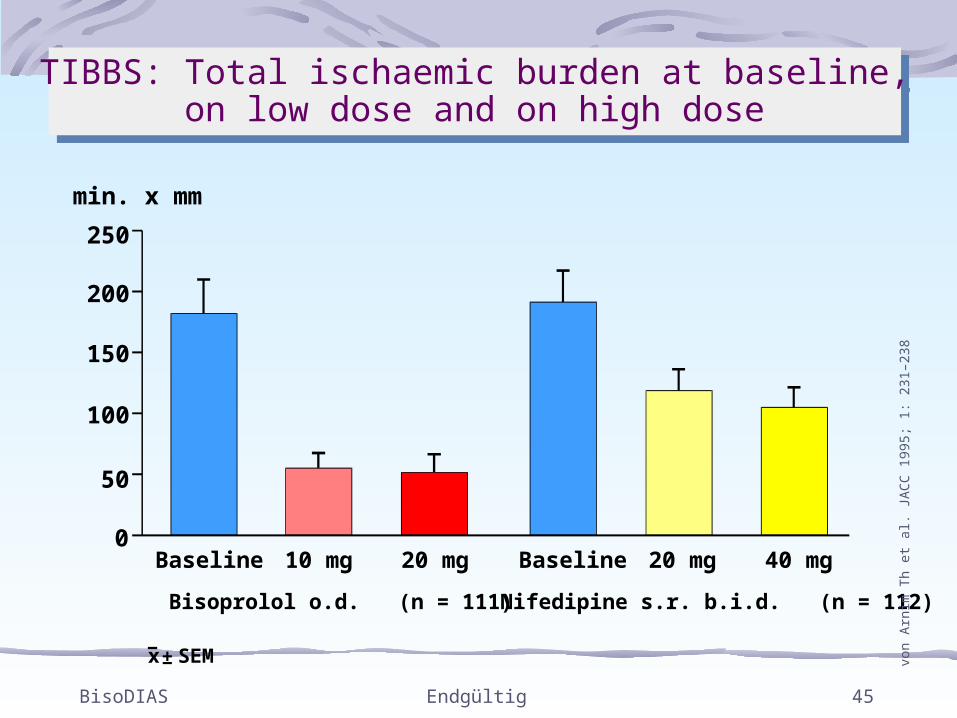
BisoDIAS Endgültig 45
min. x mm
50
100
150
200
250
0Baseline 40 mg20 mgBaseline 20 mg10 mg
Nifedipine s.r. b.i.d. (n = 112)Bisoprolol o.d. (n = 111)
TIBBS: Total ischaemic burden at baseline,on low dose and on high dose
TIBBS: Total ischaemic burden at baseline,on low dose and on high dose
von
Arn
im T
h et
al.
JAC
C 1
995;
1: 2
31–2
38
±SEMx

Three Indications of BisoprololThree Indications of Bisoprolol
Essential Hypertension
Angina
Stable Chronic Heart Failure (Moderate~Severe)

Heart Failure
From Contraindication to Indication
Beta-Blockers:Continue to surprise us

Rise in oxygen consumption
Arrhythmogenicity
Diminished diastolic filling
Systolic function impairment
Cardiotoxic effect of endogenous catecholamines
Down-regulation of the -receptors
Metabolic disorders
TAIWAN TANABE
Chronically raised sympathetic tonus is accompanied by a number of unfavourable cadiovascular effects
Chronically raised sympathetic tonus is accompanied by a number of unfavourable cadiovascular effects
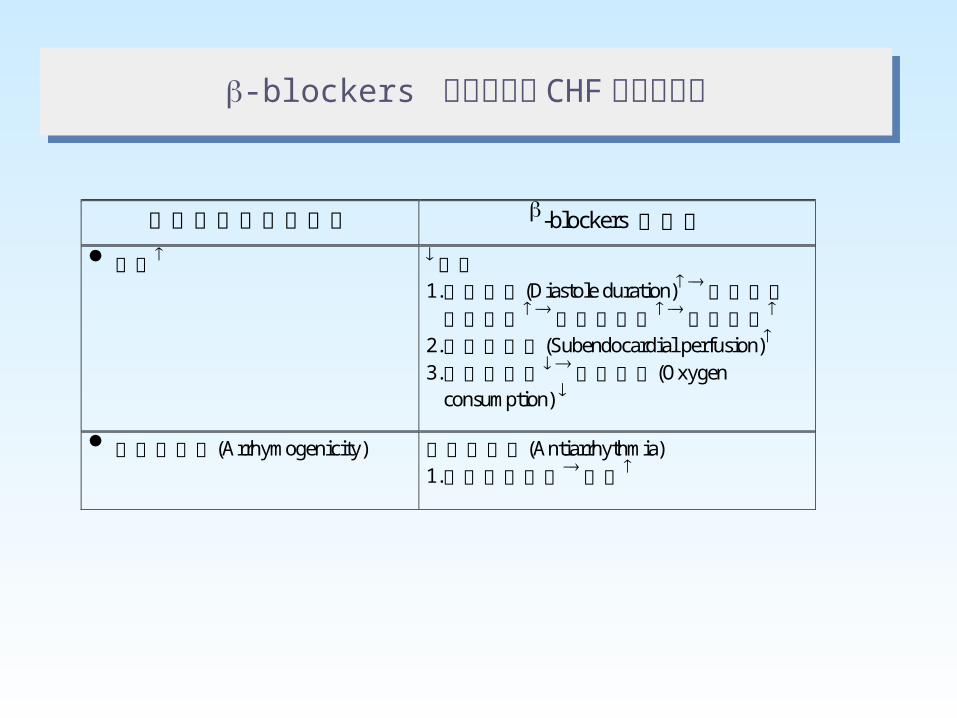
交感神經系統的活化 -blockers 的作用
心跳 心跳 1. 心舒張期(Diastole duration) 心舒張期注血時間 回心血流量 心搏出量
2. 心內膜灌流(Subendocardial perfusion) 3. 心肌工作量 氧氣消耗(Oxygen
consumption)
心律不整性(Arrhymogenicity) 抗心律不整(Antiarrhythmia) 1. 心肌保護作用預後
-blockers 應用於治療 CHF 的理論基礎-blockers 應用於治療 CHF 的理論基礎
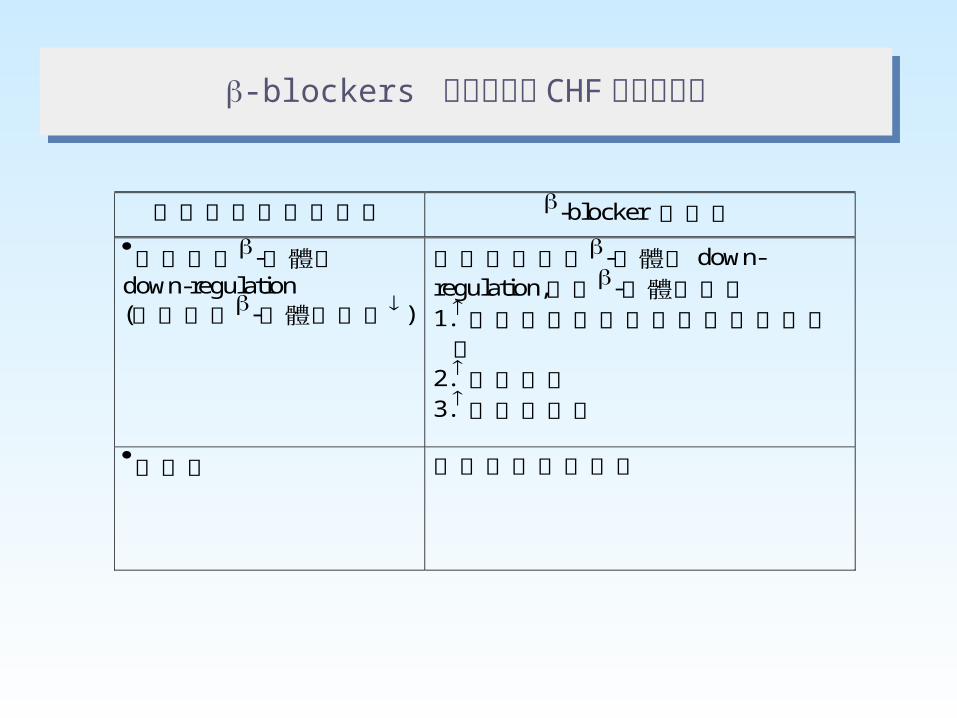
-blockers 應用於治療 CHF 的理論基礎-blockers 應用於治療 CHF 的理論基礎
交感神經系統的活化 -blocker 的作用
心肌細胞-受體的down-regulation (心肌細胞-受體的密度 )
阻止心肌細胞-受體的 down- regulation,恢復-受體的密度 1.心肌細胞對交感神經刺激的反應性
2.心收縮力 3.運動耐受度
心毒性 具有心臟保護作用

-beneficial concomitant therapy in CHF
Publication:The Lancet 1999; 353:9-13
TAIWAN TANABE

• Double-blind, placebo-controlled, randomised trial
• 2,647 patients included (NYHA III + IV)
• Bisoprolol administered on top of standard therapy(diuretic + ACE inhibitor)
CIBIS IICardiac Insufficiency Bisoprolol Study
CIBIS IICardiac Insufficiency Bisoprolol Study
CIB
IS II
Inve
stig
ator
s an
d C
omm
ittee
s. L
ance
t 199
9; 3
53: 9
–13

• Primary objective– All-cause mortality
• Secondary objectives– Cardiovascular mortality
– Hospital admissions
– Cardiovascular mortality orcardiovascular hospital admissions
– Permanent treatment withdrawal
CIBIS IIObjectivesCIBIS II
Objectives
CIB
IS II
Inve
stig
ator
s an
d C
omm
ittee
s. L
ance
t 199
9; 3
53: 9
–13

7.50
10.00
5.00
3.75
2.50
1.25
W1 W2 W3 W4 W5 W6 W7 W8 W9 W10W11W12 W13W14W15W16 Week
Bisoprolol dose (mg)
No run-in period Dose increased according to tolerability
CIBIS IIDose titration
CIBIS IIDose titration
CIB
IS II
Inve
stig
ator
s an
d C
omm
ittee
s. L
ance
t 199
9; 3
53: 9
–13

34% reduction in all-cause mortality with bisoprolol
1.0
0.8
0.6
0
0 200 400 600 800Time after inclusion (days)
Su
rviv
al
Bisoprolol: 156 deaths(11.8%) (n = 1327)
Placebo: 228 deaths(17.3%) (n = 1320)
log rank test, p < 0.0001
CIBIS IISurvivalCIBIS IISurvival
CIB
IS II
Inve
stig
ator
s an
d C
omm
ittee
s. L
ance
t 199
9; 3
53: 9
–13

Patients
Unknown causeof death
Non-cardio-vascular deaths
Other cardio-vascular deaths
Myocardialinfarction
Pumpfailure
Suddendeath
0.45(0.27 – 0.74)
0.75(0.37 – 1.50)
1.17(0.67 – 2.03)
0.85(0.31 – 2.34)
836%
p=0.0011
484%
363%
0.56(0.39 – 0.80)
0.74(0.48 – 1.14)
Hazard ratio:(95% CI)
p=0.17
p=0.75
p=0.58
p=0.41
p=0.0012
Bisoprolol (n = 1327)
Placebo (n = 1320)
0
20
40
60
80
100
474%
71%
81%
282% 23
2%
141%
181%
232%
494%
CIBIS II Causes of deaths
CIBIS II Causes of deaths
CIB
IS II
Inve
stig
ator
s an
d C
omm
ittee
s. L
ance
t 199
9; 3
53: 9
–13
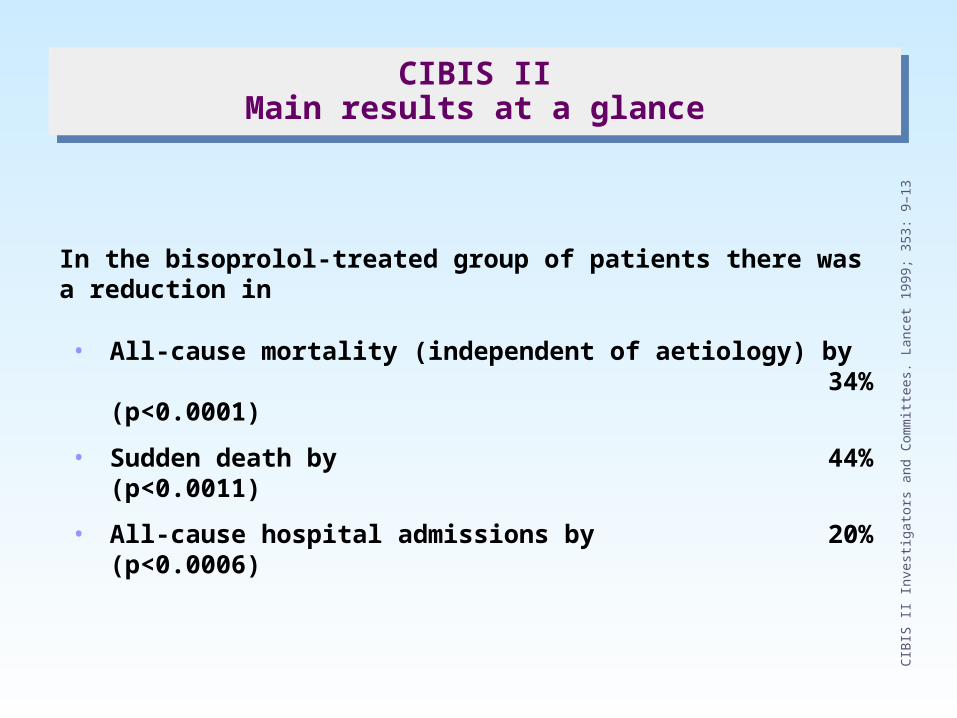
In the bisoprolol-treated group of patients there was a reduction in
• All-cause mortality (independent of aetiology) by34% (p<0.0001)
• Sudden death by44% (p<0.0011)
• All-cause hospital admissions by20% (p<0.0006)
CIBIS IIMain results at a glance
CIBIS IIMain results at a glance
CIB
IS II
Inve
stig
ator
s an
d C
omm
ittee
s. L
ance
t 199
9; 3
53: 9
–13

CIBIS IIICardiac Insufficiency Bisoprolol Study
CIBIS IIICardiac Insufficiency Bisoprolol Study
CIBIS III
Comparison of the efficacy and safety of initiation of
treatment
with bisoprolol or enalapril as monotherapy followed by their
combination in patients with chronic heart failure (CHF)
Initiation of treatment in patients with CHF
with the β1-selective β-blocker bisoprolol
(to which enalapril is subsequently added)
is as effective and safe as a regimen
beginning with the ACEi enalapril
(to which bisoprolol is subsequently added).
DOI: 10.1161/CIRCULATIONAHA.105.582320
Hypothesis

6 months 6 to 18 months
week week week week week week week week week week week week0 10 12 ... 28 30 32 34 36 ...
6 months
bisoprolol(mg/d)
enalapril(mg/d)
bisoprolol(mg/d)
Monotherapy Combination therapy
Randomisation
24months
1.25 2.5 3.75 57.5
10
1.25 2.5 3.75 57.5
10
510
20
510
20
enalapril(mg/d)
2 4 6 8
CIBIS IIIDose titration
CIBIS IIIDose titration

To show that initial mono-therapy with bisoprolol
followed by combination therapy with enalapril
is comparable (non-inferior) to the reverse order
in preventing death and hospitalization for all causes (combined endpoint).
DOI: 10.1161/CIRCULATIONAHA.105.582320
Primary objective

Intention-to-treat (ITT) population
50
60
70
80
90
100
0 6 12 18
Bisoprolol-firstEnalapril-first
Per-protocol (PP) population
50
60
70
80
90
100
0 6 12 18
Combined primary endpoint
% withoutendpoint
% withoutendpoint
B/E vs E/B163 vs 165 ptsHR 0.97 (95% CI 0.78-1.21)non-inferiority P=0.046
B/E vs E/B178 vs 186 ptsHR 0.94 (95% CI 0.77-1.16)non-inferiority P=0.019
503498
356353
265259
8073
505505
389388
291277
8776
months
months
Bisoprolol-first significantly non-inferior to enalapril-first if upper limit of 95% CIbelow hazard ratio (HR) 1.17, P<0.025.(=RR 1.125, AR +5%)
In the PP population, bisoprolol-first was not significantly non-inferior toenalapril-first
In the ITT population, bisoprolol-first was significantly non-inferior toenalapril-first
Numbers at risk
Numbers at risk
3%risk reduction
6%risk reduction
DOI: 10.1161/CIRCULATIONAHA.105.582320

Conclusions (1)
In terms of combined mortality / hospitalization
Bisoprolol-first was non-inferior to enalapril-first
in the ITT sample
Bisoprolol-first was close to non-inferior to enalapril-
first
in the PP sample
DOI: 10.1161/CIRCULATIONAHA.105.582320

There was no difference in safety
between the two strategies,
showing that a bisoprolol-first strategy
does not cause concerns
Conclusions (2)
DOI: 10.1161/CIRCULATIONAHA.105.582320

Clinical implication
The CIBIS III result supports a free choice
of initial treatment for CHF - enalapril or bisoprolol -
based on the physician’s individual judgment in each patient
DOI: 10.1161/CIRCULATIONAHA.105.582320
Put into clinical practiceCHF specific
logo
dosage easyto identify from
all sides
dose specificcolor code
CHF specific color code

β1:β2= 75:1β1:β2= 75:1
BisoprololBisoprolol
Non-ISANon-ISA
CIBIS ⅡCIBISIIITIBBS
DECREASE
CIBIS ⅡCIBISIIITIBBS
DECREASEBalance ClearanceBalance Clearance
NHI price: Concor 5= NT 7.6
NHI price: Concor 5= NT 7.6
TAIWAN TANABE
HypertensionAngina
CHF
HypertensionAngina
CHF

Thanks for your coming!
TAIWAN TANABEConcor wins your heart!!