table of contents - minds and medicine€¦ · purpose ever since the discovery of the role of brca...
TRANSCRIPT

Table of Contents
Page
Purpose 1
Learning Objectives 1
Accreditation Statements 2
Obtaining Continuing Education Credit 3
Educational Supporters 4
Agenda 5
Disclosure Information 6
Unlabeled/Unapproved Uses 7
Faculty Biographies 8
Presentations BRCA1, BRCA2 and Beyond 12 Susan M. Domchek, MD
Genomic Risk Assessment for Hereditary Cancers: Strategies and Guidelines for Breast and Ovarian Cancers 24 Kathleen N. Moore, MD
Mechanistic Basis and Proof of Concept Trials for Platinum and PARP Inhibitor Sensitivity in Breast Cancer and Associated Companion Diagnostics Development 44 Andrew N.J. Tutt, MB, ChB, MRCP, PhD, FRCR (Oncology)
Biomarker‐Driven Approach to PARP Inhibitor Clinical Trials 47 Hope S. Rugo, MD
References 58 2014 Letters & Sciences. All rights reserved. This audience guide is protected by copyright. No part may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying, recording, or utilizing any information storage or retrieval system, without permission from the copyright owner.
Purpose
Ever since the discovery of the role of BRCA mutations in cancer, clinical research has focused on identifying new strategies for treatment and prevention. Hereditary mutations in the BRCA1 or BRCA2 gene predispose individuals to breast, ovarian, and other cancers as a result of the inability to repair DNA double‐strand breaks (homologous recombination [HR] defect) , and may be sensitized to targeted therapies. Further, the majority of breast tumors that develop in carriers of BRCA mutations − the products of which are involved in HR – are triple‐negative breast cancers (TNBC). Currently, several agents targeting the PARP pathway are being evaluated and have demonstrated potential benefits in BRCA‐associated hereditary cancers and triple‐negative disease. This CME/CNE symposium features a distinguished faculty of clinicians and investigators who will provide perspectives on PARP inhibition strategies for hereditary cancers and TNBC, genomic screening for germline mutations, the role of indicators of HR deficiency for guiding treatment selection, and adaptive trial designs in clinical research.
Learning Objectives
After attending this activity, the participant will be able to: • Explain the epidemiology and clinical implications of BRCA1 and BRCA2
mutations in hereditary cancers and TNBC • Assess poly(ADP‐ribose) polymerase‐1 (PARP‐1) and other novel targets as
important therapeutic strategies • Describe risk assessment tools to identify high‐risk patients for risk reduction
strategies • Discuss development and challenges of using indicators of HR deficiency for
monitoring and guiding therapeutic selection • Identify ongoing biomarker‐driven and adaptive clinical trials used to reveal and
refine potential therapies in order to incorporate significant results into clinical practice
1

Accreditation Statements
Physician Accreditation Statements The University of North Texas Health Science Center at Fort Worth is accredited by the American Osteopathic Association to award continuing medical education to physicians. This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education through the joint sponsorship of The University of North Texas Health Science Center at Fort Worth and Letters & Sciences. The University of North Texas Health Science Center at Fort Worth is accredited by the ACCME to provide continuing medical education for physicians.
Physician Credit Designation The University of North Texas Health Science Center at Fort Worth has requested that the AOA Council on Continuing Medical Education approve this program for 2.5 hours of AOA Category 2A CME credits. Approval is currently pending. The University of North Texas Health Science Center at Fort Worth designates this live activity for a maximum of 2.5 AMA PRA Category 1 Credit(s)TM. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
Continuing Nursing Education & Credit Designation Letters & Sciences is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation. This activity has been designated for 2.5 contact hours. To obtain the full number of contact hours, the participant must participate in the entire activity and complete the evaluation forms.
2

Obtaining Continuing Education Credit
CME Credit for this activity may be claimed online within 30 days following this activity. Paper credit request forms will not be accepted. Learners will not receive credit for this activity if this process is not followed. An email reiterating these instructions will be sent to all activity participants following the symposium. How to claim credit within 30 days following this activity: 1. Point the web browser to PACECentral by typing http://ce.unthsc.edu/getcredit in the address bar 2. In the box marked “Activity Code” type MLS14125 and click “Search”. 3. The activity details will automatically display. Click “Proceed to Credit” on the right side. 4. Learners will be presented options for “Returning Users” or “New Users”, follow this link to complete the appropriate online profile. For new users, the one‐time set‐up should only take 5 minutes. 5. Once you have completed the user profile, the system will link back to the “Get Credit” page. Follow that link. If the page does not take you back, then return to: http://ce.unthsc.edu/getcredit. Choose “Claim Physician Credit”. 6. PACECentral will then require the participant to identify the educational activity and the correct credit designation. Proceed to do so in order to receive a complete, correct certificate. 7. Check the box at the bottom to verify attendance, then, click “Submit”. 8. Complete the posttest and evaluation, then, click “Submit”. 9. The customized CME certificate will appear on the screen for printing. Learners may also view it later by logging in and selecting “Transcript” in the grey bar at the top of the page. If you experience any difficulty using PACECentral to claim credit online, please call the Office of Professional and Continuing Education at 817‐735‐2539 between 8 am – 5 pm CT, Monday‐Friday.
IMPORTANT! The deadline to claim credit for this activity is January 10, 2015
CNE 1. Obtain evaluation form at registration desk 2. Return completed evaluation for onsite CE certificate
3

Educational Supporters
AstraZeneca Myriad
Sharsheret The providers gratefully acknowledge educational grants from AstraZeneca and Myriad in support of this CME/CNE symposium, as well as educational support from Sharsheret. About Sharsheret Sharsheret is a national not‐for‐profit organization supporting young women and their families facing breast and ovarian cancer. The organization’s mission is to offer a community of support to women diagnosed with breast or ovarian cancer or at increased genetic risk, by fostering culturally‐relevant individualized connections with networks of peers, health professionals, and related resources. Although their expertise is in serving young women and Jewish families, their services are not limited to Jewish women and they welcome all women at risk for, or diagnosed with, breast or ovarian cancer in need of their support. Sharsheret supports young women and their families at each stage ‐ before, during, and after diagnosis, helping women make connections in ways that feel most comfortable, taking into consideration their stage of life, diagnoses, and treatments. Since Sharsheret’s founding in 2001, the organization has responded to more than 40,000 cancer inquiries, involved more than 2,800 peer supporters, and presented more than 250 educational programs nationwide.
4

Agenda
Time
Introduction: Challenges and Successes in Targeted Therapies Hope S. Rugo, MD Clinical Professor Department of Medicine (Hematology/Oncology) Director, Breast Oncology Clinical Trials Program University of California San Francisco San Francisco, California
7:30 PM
BRCA1, BRCA2 & Beyond –Genetic Mutations & Research Susan M. Domchek, MD Professor of Medicine, Basser Professor in Oncology Perelman School of Medicine University of Pennsylvania Philadelphia, Pennsylvania
7:50 PM
Genomic Risk Assessment for Hereditary Cancers: Strategies and Guidelines for Breast & Ovarian Cancers Kathleen N. Moore, MD Mai Eager Anderson Chair in Cancer Clinical Trials University of Oklahoma Medical Center Oklahoma City, Oklahoma
8:15 PM
Mechanistic Basis & Proof of Concept Trials for Platinum and PARP Inhibitor Sensitivity in Breast Cancer and Associated Companion Diagnostic Developments Andrew N.J. Tutt, MB ChB, MRCP, PhD, FRCR (Oncology), Director, Breakthrough Breast Cancer Research Centre Institute of Cancer Research King's College London, United Kingdom
8:40 PM
Biomarker‐Driven Approach to PARP Inhibitor Clinical Trials Hope S. Rugo, MD
9:05 PM
Interactive Panel Discussion with Audience Response Keypads
9:30 PM
Concluding Remarks 10:00 PM The contributing faculty developed the content independently. All materials are included with permission. The opinions expressed are those of the faculty and are not to be construed as those of the educational providers or supporters.
5

Disclosure Information
It is the policy of the University of North Texas Health Science Center at Fort Worth, Office of Professional and Continuing Education and Letters & Sciences to ensure balance, independence, objectivity, and scientific rigor in all their sponsored educational activities. All faculty participating in this activity are expected to disclose to the audience any real or perceived conflicts of interest related to the content of their presentations. It is not assumed that these financial interests or affiliations will have an adverse impact on the faculty presentations. They simply are noted here to fully inform symposium participants. Hope S. Rugo, MD Has received grant/research support from Amgen, Eisai, GSK, Genentech/Roche, Novartis, Macrogenics, Merck, OBI, Pfizer, and Plexxikon Has received honoraria from Genomic Health Susan M. Domchek, MD University of Pennsylvania has received grant/research support from AbbVie, AstraZeneca, and Clovis Kathleen N. Moore, MD Has no relationships to disclose Andrew N.J. Tutt, MB ChB, MRCP, PhD, FRCR (Oncology) Employer has received contributions to research costs of conduct of PARP inhibitor trials from AstraZeneca, Clovis, Eisai, Myriad, and Tesaro Has served as a consultant for Eisai and Vertex Has received financial/material support from Institute of Cancer Research, London
External Review In accordance with the policies of the University of North Texas Health Science Center at Fort Worth, Office of PACE and Letters & Sciences, and in compliance with the standards of ACCME and ANCC to identify and resolve any potential conflicts of interest, to assure fair balance, independence and objectivity, and to instill scientific rigor in all CME/CNE activities, all presentations with any potential for conflict of interest, have been reviewed by an external reviewer. The external reviewer, who has no potential conflicts of interest, has determined that no bias exists in these presentations. The external reviewer is:
Shannon L. DeVita, MSN, RN, CNL, DNP (c) Nurse Practitioner San Diego, CA
Michele Nichols, PharmD Pharmacy Consultant, Private Practice Raritan, NJ
6

Unlabeled Uses/Investigational Uses/ Not Yet Approved Commercial Products
It is the policy of University of North Texas Health Science Center At Fort Worth, Office of Professional and Continuing Education and Letters & Sciences to ensure balance, independence, and scientific rigor in all educational activities/programs. Those who may have the opportunity to influence content must disclose all relevant, significant financial relationships with commercial entities so that any conflicts of interest may be resolved prior to the program. Additionally, faculty members have been instructed to disclose any limitations of data and unlabeled or investigational uses of product(s), device(s) or clinical strategies to the participants at the time of the presentations. The faculty, have disclosed the following:
Hope S. Rugo, MD Will be discussing PARP inhibitors in clinical trials Susan M. Domchek, MD Will be reviewing PARP inhibitor clinical trials Kathleen N. Moore, MD Will not be referring to unlabeled/investigational uses Andrew N.J. Tutt, MB ChB, MRCP, PhD, FRCR (Oncology) Will be reviewing PARP inhibitors only in clincial trials and HRD companion diagnostics only in clinical trials Advice to Clinicians Clinicians are advised that the educational content contained in these presentations was developed by and reflect the expert clinical experience and opinions of the faculty. Clinician judgment must remain central to the selection of therapeutic options. The evidence‐based medical information in these presentations is not intended to be a substitute for professional advice, diagnostic decision making, or treatment strategies. Clinicians should refer to the most current product labeling before prescribing or recommending medications or therapies.
7

Faculty Biographies
Hope S. Rugo, MD, is a Professor of Medicine in the Division of Hematology and Oncology at the University of California San Francisco (UCSF), Helen Diller Family Comprehensive Cancer Center, where she directs the Breast Oncology Clinical Trials Program. Dr. Rugo graduated summa cum laude from Tufts University in Medford, Massachusetts, and then, matriculated a medical degree from the University of Pennsylvania in Philadelphia. She completed both a residency in internal medicine and fellowship in hematology and oncology at the University of California San Francisco, and completed a postdoctoral fellowship in immunology at Stanford University. She received the Cancer Care Physician‐of‐the‐Year Award in 2010.
Dr. Rugo’s research interests include novel therapies for advanced breast cancer, immune modulation to restore chemotherapy sensitivity, evaluation of circulating cells, as novel markers of response and resistance to therapy, neoadjuvant therapy, and supportive care.
A member of the Breast Oncology Program at the UCSF Breast Cancer Center, Dr. Rugo is an investigator in the national multi‐center ISPY2 trial, and is the principal investigator of a number of clinical trials. She is one of three recipients of a Komen Promise Award, receives funding from the Breast Cancer Research Foundation, and serves on a number of steering committees for national and international trials. She is a member of the ALLIANCE Breast Core Committee and the Translational Breast Cancer Research Consortium, is the UCSF representative to the NCCN Guidelines Committee, and serves on several committees for the American Society of Clinical Oncology.
A significant contributor to oncology literature, Dr. Rugo has published many peer‐reviewed papers and is an invited speaker on a variety of cancer related topics.
8

Faculty Biographies
Susan M. Domchek, MD is Professor of Medicine and the Basser Professor in Oncology at the Perelman School of Medicine of the University of Pennsylvania in Philadelphia. She also serves as Executive Director of the Basser Research Center for BRCA1/2 at the Abramson Cancer Center of the University of Pennsylvania, and Director of the Mariann and Robert MacDonald Women's Cancer Risk Evaluation Program at the Abramson Cancer Center, which focuses on genetic evaluation and medical management of patients and individuals with BRCA1/2 mutations and other inherited risk factors for cancer. She is a Senior Fellow at the Leonard Davis Institute of Health Economics. Dr. Domchek graduated from Dartmouth College and received her medical degree from Harvard Medical School. As a resident in Internal Medicine, she received her clinical training at the Massachusetts General Hospital, where she was appointed Chief Resident in Medicine. Dr. Domchek went on to complete a fellowship in hematology/oncology at the Dana‐Farber Cancer Institute, and in 2001, joined the University of Pennsylvania faculty. An elected member of the American Society of Clinical Investigation, Dr. Domchek is also a member of the American Society of Clinical Oncology. A significant contributor to the oncology literature, she has authored/co‐authored more than 150 articles appearing in scholarly journals, and serves on a number of editorial review boards, including the NCI PDQ in Cancer Genetics and the Journal of Clinical Oncology.
9

Faculty Biographies
Kathleen N. Moore, MD is an Associate Professor of Gynecologic Oncology at the Stephenson Cancer Center, Division of Gynecologic Oncology at the University of Oklahoma Health Science Center in Oklahoma City, OK. She graduated with high honors from the University of Washington School of Medicine in Seattle, Washington, then, completed a residency at Magee‐Womens Hospital in Pittsburgh, PA, and a fellowship at the University of Oklahoma. Dr. Moore now holds the Mai Eager Anderson Chair in Cancer Clinical Trials at the Stephenson Cancer Center, and serves as the Gynecologic Oncology Fellowship Director and Associate Director of the TSET Phase I Clinical Trials Unit. Her research is focused on early drug development in gynecologic cancers and care of gynecologic cancers in the elderly. Dr. Moore is active in the Gynecologic Oncology Group, now NRG, and is an active member of the Ovarian, Developmental Therapeutics, and Phase I Committees, as well as the Elderly Working Group. Currently, she is one of the international coordinators for the SOLO‐1 trial, evaluating the use of olaparib as front‐line maintenance therapy in ovarian cancer, as well as the GOG PI for the OUTBACK trial in local regionally advanced cervical cancer. She has served on two SGO program committees, and was recently appointed to the SGO Clinical Practice Committee.
10

Faculty Biographies
Professor Andrew N.J. Tutt, MB ChB, MRCP, PhD, FRCR (Oncology), is a consultant clinical oncologist in the Breast Unit at Guy’s Hospital and Professor of Breast Oncology at The Institute of Cancer Research, King’s College, London. He trained in clinical oncology at the Royal Marsden Hospital and in breast cancer research at The Institute of Cancer Research in London. Professor Tutt won a Medical Research Council Fellowship to pursue a doctorate in Professor Alan Ashworth’s group at The Institute of Cancer Research addressing “The role of the BRCA2 protein in the maintenance of genome stability”. In his postdoctoral work he elucidated, with Professor Ashworth, the role of PARP inhibition in synthetic lethal strategies in BRCA1 and BRCA2 deficient cells, and further developed a translational clinical trials program of PARP inhibitor therapy for patients with BRCA1 and BRCA2‐associated cancers. Working at his own laboratory at King’s College, London his particular research interest is in Triple Negative and BRCA1 and BRCA2‐associated breast cancers (specifically, target identification, validation and biomarker development). Currently, Professor Tutt directs the Breakthrough Breast Cancer Research Centres at The Institute of Cancer Research and King’s College, London. In addition, he leads clinical trials in the UK and with the Breast International Group focusing on these patient populations. Professor Tutt has previously received the AstraZeneca Scholars Award at the San Antonio Breast Cancer Symposium. In 2009, as a distinguished academic, he was appointed Visiting Professor by the British Columbia Cancer Agency in Vancouver; and in 2010, he was named the Jean H. Lubrano Distinguished Visiting Scholar by Harvard Medical School. A significant contributor to the oncology literature, Professor Tutt has presented a large number of breast cancer research papers. He is an invited speaker and session chair at major European and North American cancer medicine conferences.
11

BRCA1, BRCA2, and Beyond
SusanM.Domchek,MDThe identification of germline mutations in BRCA1 and BRCA2 allows for interventions that can decrease cancer risk and are associated with improved mortality. In addition, BRCA1/2‐associated cancers appear to be susceptible to specific chemotherapy agents (e.g., platinums) and novel targeted therapies (e.g., PARP inhibitors). The use of genetic testing for risk assessment, cancer prevention, and cancer management has evolved over the last 20 years for BRCA1/2 and has been incorporated into routine oncologic care. More recently, the development of multiplex or multigene panels allows for the sequencing of many genes simultaneously. There are advantages to this approach (in terms of time and cost efficiency) but potential disadvantages as well. As many genes are simultaneously sequenced, the potential for finding a variant of unknown significance is high; such a finding can be confusing to patients and providers alike. Most “breast cancer” panels include both high and moderate penetrance genes. There is uneasiness regarding the management of a patient who is found to have a mutation in a high penetrance susceptibility gene without evidence of the corresponding syndrome (e.g., CDH1 mutations and hereditary diffuse gastric cancer). For many of the moderate penetrance genes, the magnitude of risk is imprecise and there are no corresponding clinical guidelines. Individuals undergoing genetic testing with these multiplex panels need to be counseled regarding the potential for uncertainty. Work is ongoing to resolve these concerns and to define the optimal ways to use information from multiplex panels for clinical management.
12

BRCA1, BRCA2, and BeyondSusan M. Domchek, MD
Director, Basser Research Center for BRCAUniversity of Pennsylvania
Disclosure Information
• University of Pennsylvania has received grant/research support from AbbVie, AstraZeneca, and Clovis
• Dr. Domchek will be reviewing PARP inhibitor clinical trials
Learning Objectives
• To discuss how germline testing for BRCA1/2 has helped:
– Risk assessment
– Cancer prevention
– Targeted therapeutics
Domchek - BRCA1, BRCA2, and Beyond
13

Evolution in Genetic Testing
Assess patient
Test for most likely gene(s)
Disclose result and reassess
Test for most likely gene(s)
New Approach?
Assess patient
Send multigene panel
Disclose result and reassess
• Risk assessment
• Cancer prevention
• Targeted therapeutics
How Has Germline Testing For BRCA1/2 Testing Helped?
How Has Germline Testing For BRCA1/2 Testing Helped?
Domchek - BRCA1, BRCA2, and Beyond
14

• Breast and ovarian in a single lineage
• Breast cancer <40
• Male breast cancer
• 2 or more women with breast cancer <50
• Ashkenazi Jewish with breast or ovarian cancer
• Breast cancer <60 and triple negative
• Bilateral breast cancer <60
• Ashkenazi Jewish individuals?
• All women at age 30?
Who Should Get Tested?Who Should Get Tested?
Series Number Design Invasive breast cancers
Follow up(years)
Risk Ratio (95% CI)
Reference
British series
258 Retrospective 28 __ 5.3 (3.5‐7.7) Smith et al, JMG 2007
Polishseries
130.5 RetrospectiveEstimated
2.5 __ 2 Gronwald et al, JMG 2007
Toronto 101 Prospective 3 8 2.9 (1.0‐8.6) Rowan et al; JMG 2007
Penn and MSKCC
375 Prospective 2 4.9 0.52 (0.13–2.09) Domchek et al, BCRT 2010
NCI 395 Prospective 10 17.7 0.95 (0.45–1.74) Korde et al, BCRT 2010
kConFab 728 Prospective 6 6.1 1.14 (0.51‐2.53) Harvey et al,BCRT 2011
Breast Cancer Risk In “True Negatives”Breast Cancer Risk In “True Negatives”
Domchek - BRCA1, BRCA2, and Beyond
15

Series Number Design Invasive breast cancers
Follow up(years)
Risk Ratio (95% CI)
Reference
British series
258 Retrospective 28 __ 5.3 (3.5‐7.7) Smith et al, JMG 2007
Polishseries
130.5 RetrospectiveEstimated
2.5 __ 2 Gronwald et al, JMG 2007
Toronto 101 Prospective 3 8 2.9 (1.0‐8.6) Rowan et al; JMG 2007
Penn and MSKCC
375 Prospective 2 4.9 0.52 (0.13–2.09) Domchek et al, BCRT 2010
NCI 395 Prospective 10 17.7 0.95 (0.45–1.74) Korde et al, BCRT 2010
kConFab 728 Prospective 6 6.1 1.14 (0.51‐2.53) Harvey et al,BCRT 2011
Breast Cancer Risk In “True Negatives”Breast Cancer Risk In “True Negatives”
Potential that there is a modest risk in BRCA2 mutation carriersEvans, DR et al CEBP 2013
In the US this is unlikely to change clinical management
Estimates of Breast Cancer Risk in BRCA1 Carriers:Significant Variability in Penetrance
Estimates of Breast Cancer Risk in BRCA1 Carriers:Significant Variability in Penetrance
No Prior Breast Cancer
Total BRCA1 BRCA2
Total Participants 1,370 869 501
HR (95% CI) 0.54 (0.37-0.79) 0.63 (0.41-0.96) 0.36 (0.16-0.82)
Domchek et al, JAMA 2010
Breast cancer prior
Total BRCA1 BRCA2
Total Participants 1060 684 376
HR (95% CI) 0.14 (0.04‐0.59) 0.15 (0.04‐0.63) No cancer events
Risk Reducing Salpingo‐oophorectomy and the Risk of First Breast Cancer
Risk Reducing Salpingo‐oophorectomy and the Risk of First Breast Cancer
RRSO and the risk of ovarian cancerRRSO and the risk of ovarian cancer
Domchek - BRCA1, BRCA2, and Beyond
16

All eligible women
All BRCA1 BRCA2
Total Participants 2,482 1587 895
HR (95% CI) 0.40 (0.26-0.61) 0.38 (0.24-0.62) 0.52 (0.22-1.23)
Domchek et al, JAMA 2010
RRSO and All Cause MortalityRRSO and All Cause Mortality
Domchek et al, JAMA 2010
• Olaparib (AZD‐2281, KU‐0059436) Astra Zeneca
• Veliparib (ABT‐888) AbbVie
• Rucaparib (AG014699/PF01367338/CO288) Clovis
• Niraparib (MK4827) Tesaro
• BMN‐673 Biomarin
• Iniparib (BSI201) Sanofi
• Significant responses seen in gBRCA1/2 breast, ovarian, pancreatic and prostate as well as unselected ovarian cancer
Treatment of BRCA1/2 Associated Cancers:Platinum and PARP Inhibitors
Treatment of BRCA1/2 Associated Cancers:Platinum and PARP Inhibitors
Tutt et al, Lancet 2010Audeh et al, Lancet 2010Gelmon et al, Lancet Oncology 2011Kaufman et al, JCO 2014
Kaufman et al JCO 2014
Domchek - BRCA1, BRCA2, and Beyond
17

• Knowing WHY a woman is at risk for breast cancer:
• Can help with risk assessment
– But one size does not fit all
– Significance of the “true negative”
• Can help with prevention
– But we do harm with our interventions too
– Need to understand risk and benefits
• Can help with treatment
– But still no approved therapy
What we Have Learned From BRCA1/2What we Have Learned From BRCA1/2
Adapted from Couch, Nathanson, Offit Science 2014
Who is at Risk? Other Genes….Who is at Risk? Other Genes….
GeneMyriad MyRisk
Ambry Cancer Next
Invitae GeneDxUwash BROCA
Fulgent*
# of genes 25 28 28 30 50 110
APC x x x x x x
ATM x x x x x x
BMPR1A x x x x x x
BRCA1 x x x x x x
BRCA2 x x x x x x
BRIP1 x x x x x x
CDH1 x x x x x x
CDK4 x x x x x x
CDKN2A x x x x x x
CHEK2 x x x x x x
EPCAM x x x x x x
MLH1 x x x x x x
MSH2 x x x x x x
MSH6 x x x x x x
MUTYH x x x x x x
NBN x x x x x x
PALB2 x x x x x x
PMS2 x x x x x x
PTEN x x x x x x
RAD51C x x x x x x
SMAD4 x x x x x x
STK11 x x x x x x
TP53 x x x x x x
GeneMyriad MyRisk
Ambry Cancer Next
Invitae GeneDxUwash BROCA
Fulgent*
BARD1 x x x x x
RAD51D x x x x x
MRE11A x x x
RAD50 x x x
NF1 x x
VHL Renal/PGL x x x x
MEN1 x x x
RET PGL x x x
PTCH1 x x
PALLD x
XRCC2 x x x
CHEK1 x xAXIN2 x x
FANCC x x
ATR x x
BAP1 x xGALNT12 x x
HOXB13 x x
POLD1 x x
PRSS1 x x
RAD51A x x
SDHB Renal/PGL x x
SDHC Renal/PGL x x
SDHD Renal/PGL x x
AKT1 x
CTNNA1 x
FAM175A x
GEN1 x
GREM1 xPIK3CA x
POLE x
PPM1D x
TP53BP1 x
*Rest of genes on Fulgent: BLM, BUB1B, CTNNB1, CYLD, DDB2, DICER1, EGFR, EGLN1, ERCC2, ERCC3, ERCC4, ERCC5, EXO1, EXT1, EXT2, FANCA, FANCB, FANCD2, FANCE, FANCF, FANCG, FANCI, FANCL, FANCM, GPC3, HRAS, KIF1B, KIT, MC1R, MPL, MSH3, NF2, PDGFRA, PICALM, PMS1, PRKAR1A, PRKDC, PTPN11, RB1, RBBP8, RBM15, RECQL4, ROBO2, SBDS, SLX4, SMARCB1, SUFU, TERT, TSHR, TYR, WRN ,WT1, XPA, XPC, XRCC3
GeneAmbry Renal or PGL
Fulgent*
FH x x
FLCN x x
MAX x x
MET x x
MITF x x
SDHA x x
SDHAF2 x xTMEM127 x x
TSC1 x x
TSC2 x x
Hereditary Cancer Panels as of ASCO 2014
Domchek - BRCA1, BRCA2, and Beyond
18
• May be more cost effective (for the testing) to do multigene rather than serial testing
• Patients (and providers!) can get testing fatigue
• Phenotypes can overlap
– Ovarian cancer in both BRCA1/2 and Lynch
– Uterine cancer in Lynch and Cowden
– Breast in Li‐Fraumeni and BRCA1/2
• Isn’t more better?
Why do This?
• High penetrance and moderate penetrance genes are on one panel– Implications for counseling
– Keeping track of it all
• Variants of uncertain significance– Reminder that management should be based on family history
• Clinical utility?– General philosophy that we order tests that we will act on
Considerations for Caution
Domchek et al, JCO 2013
• TP53– Li Fraumeni syndrome
• CDH1– Hereditary diffuse gastric cancer
• STK11– Peutz Jegher syndrome
• PTEN– Cowden syndrome
• Generally felt that these are recognizable syndromes– Is this true? Particularly for PTEN it may not be
High Penetrance Genes
Domchek - BRCA1, BRCA2, and Beyond
19

• Risks and benefit and potential changes in clinical management are reviewed prior to testing
• Option to decline testing
• Can you do this with 10, 20, 30 genes?
• We need new models
Tenets of Pre‐test Counseling
Bradbury et al, GIM 2014
Ambry Genetics experience
• In BRCA1/2 negative patients, most series have demonstrated
<10% with mutations in other genes
• In 3% or fewer are mutations detected with clinical guidelines
•VUS rate is approximately 20%LaDuca et al., GIM 2014Tung et al., Cancer 2014Kurian et al, JCO 2014Couch et al, in press JCO 2014Maxwell et al, in press GIM 2014
What Will We Find?
• Risk assessment
– Value of the true negative
– Risk of breast and as well as risk of second primary cancer
– Risk of other cancers (Ovarian cancer risk for BRCA1/2 was a major reason for rapid uptake of testing)
• Cancer prevention
– Need to understand risks and benefits
– We do harm to people
• Therapeutics
– Prognosis
– Drug development/selection
Clinical Utility
Domchek - BRCA1, BRCA2, and Beyond
20

Incomplete Co‐segregation of CHEK2?Value of the True Negative?
Meijers‐Heijboer, et al, Nature Genetics 2002
• Clearly demonstrated for PALB2
– Pancreatic cancer
– What is the lifetime risk?
– What do you do about it?
• Other genes – less clear/ unclear
– CHEK2 1100delC and colon cancer: potentially RR 2
– Others? Prostate, melanoma
Other Cancers?
• Risk assessment
– Value of the true negative
– Risk of breast and as well as risk of second primary cancer
– Risk of other cancers (Ovarian cancer risk for BRCA1/2 was a major reason for rapid uptake of testing)
• Cancer prevention
– Need to understand risks and benefits
– We do harm to people
• Therapeutics
– Prognosis
– Drug development/selection
Clinical Utility
Domchek - BRCA1, BRCA2, and Beyond
21

• Risk assessment
– Value of the true negative
– Risk of breast and as well as risk of second primary cancer
– Risk of other cancers (Ovarian cancer risk for BRCA1/2 was a major reason for rapid uptake of testing)
• Cancer prevention
– Need to understand risks and benefits
– We do harm to people
• Therapeutics
– Prognosis
– Drug development/selection
Clinical Utility
Unanticipated High Penetrance Gene Mutation
No family history of gastric cancer
Sister with breast and colon cancer at 63
• New methods of counseling needed to deal with “mixed” panels
• Variants of unknown significance should NOT be managed as mutations
• Be wary of the true negative
• Data on how to use this information in clinical management is critically needed
• In the face of rising prophylactic mastectomies need to emphasize to patients how mutations in these genes are different from those in BRCA1/2
Conclusions
Domchek - BRCA1, BRCA2, and Beyond
22

• Critically important that those with mutations and variants in these “lesser known” genes be enrolled in registries with prospective follow up
– PROMPT Study
– ENIGMA
– Individual institution registries
Conclusions
Academic‐Corporate partnershipDana‐Farber, Mayo Clinic, MSKCC, Penn
Ambry Genetics, GeneDx, Myriad, Pathway Genomics, Quest
www.promptstudy.org
Domchek - BRCA1, BRCA2, and Beyond
23

Genomic Risk Assessment for Hereditary Cancers: Strategies and Guidelines for Breast and Ovarian Cancers
Kathleen N. Moore, MD Appropriate application of genomic screening is one of the most powerful tools available for personalized medicine. For breast cancer, we have known about highly penetrant cancer predisposition genes such as BRCA1, BRCA2, DNA mismatch repair genes in Lynch syndrome, TP53 in Li Fraumeni, PTEN in Cowden, STK11 in Peutz Jegher, and CDH1 in hereditary diffuse gastric cancer. For ovarian cancer, we have known about BRCA1, BRCA2 and mismatch repair genes in Lynch syndrome. Despite knowledge of these predisposition genes and the potential for prevention of cancers among first and second degree relatives (and prevention of secondary cancers among affected individuals), appropriate referral for genetic testing has been underutilized. With the advent of next generation sequencing (NGS) and the development of multigene or multiplex genetic panels, patients with breast and ovarian cancer who undergo genetic testing now are being tested with these newer technologies. This has resulted in patients and families found to have genes with unclear cancer risk estimates for which treatment and risk modification have not been well defined. This presentation will focus on the known breast and ovarian cancer predisposition genes, the advent of NGS and multi‐gene testing, and discuss the challenges these tests pose as we move into the next phase of genetic medicine.
24

Genomic Risk Assessment for Hereditary Cancers:
Strategies and Guidelines for Breast & Ovarian Cancers
Kathleen N. Moore, MDAssociate Professor, Div Gyn Oncology
Mai Eager Anderson Chair in Cancer Clinical Trials
Disclosure Information
• Has no relationships to disclose
• Will not be referring to unlabeled/investigational uses
Learning Objectives
• Review the epidemiology and heritability of genetic syndromes in breast and ovarian cancer
• Discuss genetic risk assessment for patients and families affected by breast and ovarian cancer– Family History
– NCCN Guidelines
• Identify pros and cons of multi-gene testing
Moore - Genomic Risk Assessment
25

Definitions• High penetrance gene
– A gene that, when mutated, causes high risk for cancer
– Rare, well‐defined phenotypes, explain most of a family’s risk of cancer
• Moderate penetrance gene– A gene that, when mutated, may have a small to moderate effect on
cancer risk
– May not explain all of a family’s risk of cancer
• Gene with uncertain significance– A gene where the significance of a deleterious mutation is uncertain
– Usually b/c of limited data
• Variant of uncertain significance (VUS)– Sequence variant with unknown effect on gene function which may or
may not be associated with cancer risk
Rich et al. J Surg Oncology (2014)
Objectives
• Discuss the epidemiology and heritability of genetic syndromes in breast and ovarian cancer
• Discuss genetic risk assessment for patients and families affected by breast and ovarian cancer
– Family History
– NCCN Guidelines
• Discuss multi‐gene testing
Epidemiology: Breast and Ovary Cancer
• In 2014, there are an estimated 235,030 new cases of breast cancer and 21,980 new cases of ovarian cancer
1. American Cancer Society: Cancer Facts and Figures 2014. Atlanta, GA
Moore - Genomic Risk Assessment
26

Hereditary Disposition is a Significant Cause in Breast and Ovarian Cancers
1. American Cancer Society: Cancer Facts and Figures 2014. Atlanta, GA
2014 Estimated New Ovarian Cancer cases100%=21,980
10‐15% Hereditary disposition
20‐25% Hereditary disposition
2014 Estimated New Breast Cancer cases100%=235,030
Nature Reviews Clinical Oncology 7, 251‐265 (May 2010)
• High penetrance
• Moderate penetrance
• Low penetrance
Hereditary Breast Cancer Predisposition Genes
High Penetrance Breast Cancer Genes Are Rare But Can Lead to Significant Effects
Syndrome/GeneClinical Mutation Positivity Rate Lifetime BC Risk Other features
BRCA1/BRCA2 5‐10% for each 65‐81% BRCA145‐85% BRCA2
•BRCA1: basal like TNBC, EOC•BRCA2: HR+ BC, male BC, pancreas, EOC
Li‐Fraumeni (TP53) <1% >50% •Sarcomas, brain,adrenocortical ca•Very young age at dx•90% lifetime risk of cancer
Cowden (PTEN) <1% 77‐85% •Thyroid, uterine, RCC•99% with skin and oral mucosal tumors, macrocephaly, autism
Peutz‐Jeghers (STK11/LKB1)
<1% 24‐32% •GI, pancreas, ovarian (SCST) 18‐21%
Hereditary diffuse gastric cancer (CDH1)
<1% 39‐52% •Diffuse gastric cancer (67‐83%), lobular breast cancer
Rich et al. J Surg Onc 2014; Euhus D. Ann Surg Oncol 2014
Moore - Genomic Risk Assessment
27

Other Highly Penetrant Genes in Breast Cancer are Emerging, like PALB2With Complex Mutations
• PALB2 is a partner and localizer of BRCA2
• Families included in the study: BRCAneg breast cancer and at least one family member with loss of function mutation in PALB2
• 154 families included in analysis (including 229 women and 7 men with Breast Cancer)
Antoniou AC et al. NEJM (2014): 371(6):497‐506
Study identified 48 LOF mutations in PALB2Study: Antoniou AC et al. NEJM (2014): 371(6):497‐506Background:
Breast‐cancer Risk for PALB2Mutation may Overlap With That for BRCA2Mutation
Highly Penetrant Genes = Actionable Genes
Current NCCN Management for BRCA1/2:
• Clinical BE every 6‐12 months starting at age 25
• Breast screening
– Annual MRI age 25‐29
– Age >30 annual MRI/mammography
• Risk reducing mastectomy/BSO
• Chemoprevention
Age at Diagnosis of First BC
Within 10years
Within 25 years
< 40 21‐31% 63%
40‐50 11‐13% 44‐49%
>50 8‐9% 17‐20%
1. Graeser et al. JCO 2009
Reduction in second primaries1
Moore - Genomic Risk Assessment
28

TP53
PTEN
CDH1
STK11
•Breast MRI/MMR starting at early age•Consider prophylactic mastectomy•Increased colonoscopy screening•Comprehensive physical/ dermexam•No radiation
•Breast MRI/MMR starting at early age•Pt education regarding DUB•Prophylactic mastectomy/TAH ?•Routine colonoscopy at an early age•Comprehensive physical/dermexams•Baseline thyroid US at an early age•Consider renal ultrasounds
•Breast MRI/MMR•Routine endoscopy starting at an early age•Consideration of prophylactic gastrectomy•Routine colonoscopy
•Breast MRI/MMR•Frequent colonoscopy starting at early age•Routine upper endoscopy and small bowel visualization starting early•Routine pancreatic cancer screening•Physical exams
Gene Recommendations Gene Recommendations
Highly Penetrant Genes = Actionable Genes
Causes of Hereditary Susceptibility to Ovarian Cancer
Hereditary(~23%)
Sporadic
BRCA1 (~45%)
Other single genes (~27%)
BRCA2 (~27%)
HNPCC (1-2%)
Ovarian Cancer Predisposition Genes
Syndrome/Gene Clinical Mutation Positivity Rate
Lifetime OC Risk Other features
BRCA 11 11% 35‐46% OC at earlier age (50)
BRCA 21 6% 13‐23% OC at same age as general population (60)
Lynch Syndrome2,3
(HNPCC)<1% 3‐14% OC at earlier age (43‐50);
endometrial and colon cancer risks have highest risk
RAD51C4,7 1.3% (RR 6‐8) 10‐15%
RAD51D5,7 0.6% (RR 6‐9) 10‐15%
BRIP16 1.4% (RR 8) 10‐15%
1.Walsh T, Casadei S et al. PNAS. 2011; 108:18032‐372.Koornstra JJ et al. Lancet Oncol. 2009; 10(4):400;3. Barrow et al. Clin Genet. 2009; 75(2): 141. 4. Meindl et al. Nat Genet 2010 5. Loveday et al. Nat Genetics 2011 6. Rafnar et al. Nat Genet 20117. Peltari et al. J Med Gen 2012
Moore - Genomic Risk Assessment
29

Cases BRCA1/2mutation Other Gene Mutation Total
N=360 64 (17.8%) 23 (6.4%) 87 in 90 (23.6%)
• Minimal mutation rate• 11 more genes identified 6% of cases• Other genes account for 29% of cases
with germline mutations• 1/3 of cases with mutations had no
family history• 40% were over 60 at diagnosis
Screening All Genes Identifies Additional Cases
TP53
BRIP1
CHEK2
BARD1
MRE11MSH6
NBNPALB2
RAD51CRAD51D
1
4
5
12
12
1 3 3
PNAS, Walsh, Swisher et al 2011
BRCA1/2 Mutation
• Ovarian, fallopian tube, and peritoneal cancer
– BRCA1: 40% chance for OC by age 70 (18 to 54% across studies) 20 x risk in general population
– BRCA2: 10% chance for OC by age 70 (2.4 to 19% across studies) 5 x the risk in general population
• Known prognostic biomarker for OC
• May be a predictive biomarker for PARPi
• Unlike BC, there is no effective screening but there is risk reduction
Organization Screening Recommendation
American Cancer Society
Women may be screened but it is not known how helpful the screening tests are
American College of Obstetrics and Gynecology (ACOG)
If appropriate, these women may be offered OC screening. Screening with Ca‐125 measurements and TVUS every 6 months has been recommended by the NCCN, although evidence is insufficient to demonstrate current screening methods improve survival rates
Canadian TaskForce on Preventative Health Care
Insufficient evidence to recommend for or against screening, but expert opinion suggests that these women be referred to an academic health center for regular combination screening
NCCN Screen with TVUS and Ca‐125 every 6 months starting at age 35y or 5‐10 y before the youngest relative received and OC dx
USPSTF The PPV of an initially positive screening test would be more favorable for women at higher risk; if ongoing clinical trials show that screening has a beneficial effect on mortality rates, then women at higher risk are likely to experience the greatest benefit
Mannis et al. JAMA Intern Med. 2013
Screening Recommendations
Moore - Genomic Risk Assessment
30

Risk Reduction for High Risk Patients
• Current recommendations are for risk reducing bilateral salpingo‐oophorectomy and bilateral salpingectomy between the age of 35 and 40 or when childbearing complete
• Ongoing studies are evaluating the safety of salpingectomy alone as a preventative measure followed by oophorectomy later to delay menopause
RAD51D
• RR estimated to be 6.30 (95% CI 2.86–13.85, P = 4.8 × 10–6)1
• Analysis of specific Finnish founder mutation (c.576+1G>A) identified OR for OC of 9.16 (1.07 to 78.56).
• LOF mutations found in 0.8‐1% of unselected OC cases• 10‐15% lifetime risk• Age of cancer diagnoses 34‐79 years• At least two OC were of endometrioid histology and one OC
occurred with a synchronous endometrial cancer
1. Loveday et al 2011, Nat Genet
RAD51C
• Es mated RR for OC of 5.88 (95% CI = 2.91−11.88; P = 7.65 ×10−7), which constitutes >9% cumulative risk by age 80
• Two Finnish founder mutations associated with OR of 6.31 (95% CI 1.15‐34.6, P= 0.032)
• LOF mutations found in 0.6‐1% of unselected OC cases• 10% lifetime risk• Age of cancer diagnoses years 42‐81 years
1. Loveday et al, Nat Genet 2012 2. Pelttari et al, Hum Molec Genet 2011
Moore - Genomic Risk Assessment
31

BRIP1
• Truncating Icelandic founder mutation (c.2040_2041insTT, allelic frequency 0.3%) associated with approximate 8‐fold RR for OC (95% CI 4.74, 13.95; P = 2.8 × 10−14)1
• Rare Spanish founder mutation (c.1702_1703del, allelic frequency 0.03%) associated with OR for OC of 25 (CI 1.8, 340; P=.016)
• 10‐15% lifetime risk• Identified in 1.4% of unselected cases: most common cause of
hereditary OC after BRCA1 and BRCA2• Median age of cancer diagnoses 65 years
1. Rafnar et al, Nat Genet 2011
Lynch Syndrome (LS)
• Lifetime risk for OC among women with LS is 6.7 to 12% 1
• Mean age at diagnosis 42 to 50 y/o2,3
• Cancers may be found at an earlier stage (77 to 85% stage I‐II) and some report over‐representation of endometrioid and clear cell as compared to sporadic OC3
• Synchronous cancers (OC and Endo Ca) have been reported
– 21% of LS related OC may have a synchronous Endo ca3
– 7 to 29% of LS related Endo Ca may have a synchronous OC4
1. Watson P et al. Cancer 2008;2. Ketabi Z et al. Gynecol Oncol 2011;3. Watson P et al. Gynecol Oncol 2001; 4. Solimon et al. Obstet Gynecol 2005.
Management of Women with Lynch Syndrome Mutations: NCCN 2.2014
• Colonoscopy at age 20‐25 or 2‐5 years prior to earliest colon cancer if < 25y. Repeat q 1‐2 y
• Endometrial and Ovarian Cancer
– TAH/BSO at completion of childbearing
– Dysfunctional uterine bleeding =work up
– Screening not supported
• Breast Cancer
– Limited data on risk of BC in LS patients, no screening recommendations
Moore - Genomic Risk Assessment
32

Objectives
• Review the epidemiology and heritability of genetic syndromes in breast and ovarian cancer
• Discuss genetic risk assessment for patients and families affected by breast and ovarian cancer
– Family History
– NCCN Guidelines
• Describe multi‐gene testing
Traditional Model of Cancer Genetics
Stadler ZK. JCO 2014
“Genetic factors are a key component of precision medicine because they can unlock important
information that can help an oncologist determine the best course of individualized treatment”
“An adequate family history is key to identifying those patients whose cancer may be associated with inherited genetic factors.”
Clifford A. Hudis, MD, FACP
Genetic Risk Assessment‐Family History
Moore - Genomic Risk Assessment
33

Genetic Risk Assessment‐Family History
• ASCO recommends that the minimum adequate family history for patients with cancer be defined as:– Family history of cancer in first‐ and second‐degree relatives.
– For each relative with cancer, the following should be recorded:
• Type of primary cancer(s)• Age at diagnosis of each primary cancer • Lineage (maternal and/or paternal) • Ethnicity• Results of any cancer genetic testing in any relative
2014 by American Society of Clinical Oncology
General Genetic Testing Strategy
Rich et al. J Surg Oncology 2014
Recommendations for BRCA1 and BRCA2 Testing: NCCN 2.2014• Individual with a family h/o deleterious mutation• Personal h/o breast cancer (including DCIS)
– < 45 y/o– < 50 y/o (with 2 primaries, > 1 relative w/BC, limited family hx)– <60 y/o with TNBC– Any age with > 1 relative with BC < 50 y/o or OC or male BC– Any age with > 2 relatives with BC any age or pancreatic or
prostate cancer (Gleason >7)
• Personal h/o EOC• Personal h/o pancreatic & prostate ca (Gleason > 7) with > 2
relatives with BC, OC and/or pancreas or prostate cancer
Moore - Genomic Risk Assessment
34

Li‐Fraumeni Syndrome: NCCN 2.2014
• Individual from family with known TP53mutation• Classic LFS
– Sarcoma < 45 y/o AND 1st deg relative with cancer < 45 y/o ANDadditional FDR or SDR with cancer < 45 or sarcoma any age
• Chompret criteria– LFS tumor spectrum cancer < 46 y/o AND FDR or SDR with LFS‐
associated cancer < 56 or multiple cancers of any age– OR individual with multiple tumors (x BC), 2 of which are LFS <
46 y/o– OR individual with adrenocortical or choroid plexus carcinoma
• Early age breast cancer– BC < 35 y/o– Order BRCA1, BRCA2 and TP53mutation testing
Cowden Syndrome/PTEN Hamartoma Tumor Syndrome: NCCN 2.2014
• Individual from family with known PTENmutation• Clinical criteria for Cowden/PHTS
– Major Criteria (>3)• BC, Endo Ca, Follicular Thyroid Ca, GI hamartomas, Macrocephaly,
mucocutaneous lesions
– Minor Criteria (2 major + 3 minor)• Autism spectrum, colon ca, lipomas, MR, RCC, vascular abnormalities, thyroid
ca (papillary or follicular variant), esophageal glycogenic acanthoses, testicular lipomatosis, thyroid structural lesions, vascular abnormalities
• Personal Hx– 3 major criteria (no macrocephaly), 2 major criteria (1 must be
macrocephaly), 1 major and > 3 minor or > 4 minor
• Relative with clinical diagnosis of Cowden/PHTS but no genetic testing
Lynch Syndrome: NCCN 2.2014
• CRC in a patient < 50 y/o• Presence of synchronous or metachronous CRS or other LS related tumor regardless of age– CRC, Endo Ca, Ovarian Ca, Pancreatic Ca, Ureteral & renal pelvis, biliary tract, brain (GBM) & small intestinal tumors
• CRS with MSI‐H histology < 60• CRS in a patient with > 1 FDR with a LS‐related cancer diagnosed < 50 y/o
• CRC diagnosed in a patient with >2 FDR or SDR with LS‐related cancers, regardless of age
Moore - Genomic Risk Assessment
35

Objectives
• Discuss the epidemiology and heritability of genetic syndromes in breast and ovarian cancer
• Discuss genetic risk assessment for patients and families affected by breast and ovarian cancer
– Family History
– NCCN Guidelines
• Describe multi‐gene testing
Multi‐gene Testing
• NCCN recommendations have largely relied on comprehensive family history, physical exam & patient/disease characteristics to direct targeted gene testing with serial testing should the first test be uninformative
• Next‐generation sequencing and the increasing availability of multi‐gene panels (multiplex) have changed this serial testing paradigm
Single Gene Test vs Panel testing
Moore - Genomic Risk Assessment
36

Shift in Counseling & Testing Paradigm
Genomic consent
NGS
Post test counseling
Clinical Evaluation
Specific Pre‐test
counseling
Limited genetic testing
Post‐test counseling
Genetic Counseling NGS counseling
Adapted from Robson M, Offit K, MSKCC
Challenging The Traditional Model Of Cancer Genetic Counseling
Pros: Multi‐gene Testing
• Increased likelihood of finding mutations in pts who do not meet specific criteria
– Multiple genes contribute to BC/OC phenotype
– Patients with limited or atypical family structure
– Patients with new mutations
– Up to 17% of high‐risk BC families without BRCAmutation and as many as 24% of unselected OC families will have a mutation
• Higher mutation detection fewer high‐risk families with uninformative results
• More cost and time effective
• May reveal more than one pathogenic mutation
Moore - Genomic Risk Assessment
37

Multi‐gene Testing Cons
• Technical
– Tests differ in genes analyzed, depth of gene coverage, turnaround time, cost, insurance coverage, annotation of VUS
• Must include discussion of VUS in pre‐test counseling
• No validated algorithms for classification of VUS
• Mutations may be missed with NGS
• Clinical– Pre‐test counseling becomes more conceptual rather than gene
specific
– Limited data on the degree of cancer risk associated with some mutations
– Lack of guidelines for risk management for some mutations
– Turnaround time may be prohibitively long for some panels
Examples of Available Multi‐Gene Panels Company Test Name # Genes Cost Time
wksVUS
Ambry Genetics
BRCA plus 5 $3,300 3 7%
Breast Next 17 $3,900 2‐4 wks 22.4%
Ova Next 23 2‐4 wks 26.7%
U. of Wash BROCA risk panel 51 $3,350 12 9.5%
Myriad My Risk 25 $3,700 3 40%
GeneDx BC High Risk Panel 6 * 10 9%
BC/OC panel 21 * 10 30%
Quest BRCAvantage Plus 7 * * Not enough data yet
Moore - Genomic Risk Assessment
38

Variants of Uncertain Significance
• The risk for VUS is considerably higher when testing for multiple genes in tandem
• Most VUS will eventually be classified as benign
• Clinical decisions – should NOT be made based on VUS
• Designated programs to track VUS within families are emerging
High Penetrance Genes: BC
Gene Syndrome Lifetime BC risk
BRCA1 HBOC 50‐85%
BRCA2 HBOC 50‐85%
PALB2 Familial BC 40‐60%
TP53 Li‐Fraumeni 50‐90%
PTEN Cowden 25‐50%
STK11 Peutz Jeghers 45‐50%
CDH1 Hereditary diffuse gastric cancer
39‐52%
Rainville IR, Rana HQ. Next Curr Oncol Rep (2014) 16: 371
Moore - Genomic Risk Assessment
39

Moderate Penetrance Genes: BC
Gene Syndrome Lifetime BC risk
CHEK2 Familial BC 20‐40%
ATM Familial BC 20%
NBN Familial BC 20‐30%
MRE11A Familial BC Undetermined
RAD50 Familial BC Undetermined
BRIP1 Familial BC 20%
RAD51C, RAD51D, XRCC2 Familial BC/OC Undetermined
BARD1 Familial BC and BC/OC Undetermined
Rainville IR, Rana HQ. Next Curr Oncol Rep (2014) 16: 371; Rich TA et al. J Surg Oncology (2014): 1‐16
Classification Of Predisposition Genes Is Not Quite That Clear….
Euhus D. Ann Surg Oncol (2014) 21:3209‐3215
Moore - Genomic Risk Assessment
40

Closing Remarks (1)
• Thorough evaluation of every cancer patient for family history, physical exam findings and context of tumor is critical
• Family history alone as the trigger for genetic counseling misses 30‐40%1 of hereditary BC, while using family history and/or age as the trigger for genetic counseling misses 20‐44% of hereditary OC2
• Historically, clinicians have under‐utilized cascade testing of FDR of the patient identified with a mutation
2. Norquist B et al. Gynecol Oncol 2013
Women’s Cancer Moonshot: Flagship 1
1A‐Making cancer history for the family Universal BRCA testing of all high‐grade serous ovarian cancer
(HGSOC) and triple‐negative breast cancer (TNBC) patients Active outreach and navigation to family members, facilitated
by creative and innovative IT platforms1B‐Novel therapy approaches to target BRCA1/2 or HR defects Develop and implement a clinical based platform on synthetic
lethal targeting of tumors Target the most common mutations in HGSOC and TNBC Homologous recombination pathway BRCA1/2
1C‐Providing Effective screening/prevention for previvors
Germline BRCA‐1 and ‐2 testingNo charge to patient or MDACC
Myriad
FP1A Active Outreach to family
FP1C Screening Prevention; 90% decrease in high risk patients with preventive surgery
Universal genetic testing for all TNBC and HGSOC patients; NCCN Guidelines
Making Cancer History for the Family Immediate Impact on the Patient Population
Moore - Genomic Risk Assessment
41

Scope of Problem: Preventing Future Ovarian Cancers by Testing for BRCAMutations
Reference strategy0 tested 0 test+
SGO criteria4,005 tested900 test+
Test serous CA9,337 tested1,252 test+
Test all14,000 tested1,481 test+
14,000 women with ovarian cancer in U.S. index
cases
0 FDR tested
0 test+
216 Ov Ca
1,800 FDR tested
988 test+
157 Ov Ca
2,504 FDR tested
1,288 test+
137 Ov Ca
2,962 FDR tested
1,418 test+
121 Ov Ca
27% 37% 44%
Kwon et al, JCO 2009
Only 15% of patients were offered testing !!
• Age less than 50 years regardless of family history should be tested (17% positive rate)
• Prevention of breast cancer: 10,000 cases/year !
Kwon & Arun JCO 2010 20;28(27):4214‐20
Only 50% of patients are offered testing !!
Scope of Problem: Preventing Future Breast Cancers by Testing for BRCAMutations
Ovarian Breast
Number of patients 1346 298
Number of patients tested 982 187
Percentage tested >80% 81%
BRCA Positive Pts. 80 34
Percent positive* 8% 18%
TNBC percent positive 19%
*Includes patients with non‐TNBC and family history
Current Reporting Metrics (9/1/2012 – 6/30/2014)
Moore - Genomic Risk Assessment
42

Closing Remarks (2)
• The widespread availability of NGS/MGP as well as discontinuation of BRCA1/BRCA2 isolated testing by some vendors has added complexity to genetic screening
• BC
– Genetic counseling by clinician with expertise
– Test for highly penetrant gene(s) most likely to be relevant to your patient (soon including PALB2)
– Reserve MGP for patients in whom family history is limited or for whom directed gene testing is uninformative
• OC
– Given that several genes appear highly penetrant and all patients should be tested, MGP are a consideration
– Genetic counseling by a clinician with expertise
Moore - Genomic Risk Assessment
43

Mechanistic Basis & Proof of Concept Trials for Platinum and PARP Inhibitor Sensitivity in Breast Cancer & Associated Companion Diagnostic Developments
Andrew N.J. Tutt, MB ChB, MRCP, PhD, FRCR (Oncology) Triple Negative Breast Cancer (TNBC) is only considered an entity by virtue of not being one of the two other forms of breast cancer defined by the presence of the therapeutic predictive biomarkers HER2 and ER/PgR. It is therefore, a heterogeneous form of the disease within which lies a number of poorly understood biological groups, most of which have yet to reveal validated treatment targets. One of the features of a high proportion of these TNBCs is a high degree of genome instability. This genome instability leads to a very large number of copy number aberrations and mutations, many of which have low frequency or recurrence across the disease. This genome instability is itself heterogeneous in form resulting from likely variations in DNA repair competency between and within the reported biological groups. It has long been recognized that there is an association between familial predisposition to breast cancer and the TNBC forms of the disease. This is driven by the specific enrichment for TNBC in the breast cancers arising in BRCA1 mutation carriers. Loss of function of BRCA1 or BRCA2 leads to impairment of an accurate DNA repair process referred to as “Homologous Recombination (HR)” used by proliferating cells, which causes a high degree of genome instability that can have distinctive features driven by the cell’s need to use other DNA repair processes. HR is also used to repair damage caused by platinum salts. This leads to high levels of platinum cell kill in preclinical studies of BRCA1 and BRCA2 mutation. Recently, the use of PARP inhibitors has been shown to kill malignant cells with deficient HR, such as those with BRCA1 and BRCA2 mutation, through “synthetic lethality”. While there have been few successful targeted therapy approaches in TNBC, recent studies and some clinical trials have begun to address whether the specific defects in DNA repair that underlie BRCA1/2‐associated breast cancer and sub‐populations within TNBC may lead to sensitivity to platinum salts and PARP inhibitors. In this lecture, the biological mechanisms relevant to these approaches and breast cancer types will be reviewed. Additionally, relevant clinical trials that have been recently reported, including the UK TNT trial will be highlighted, as well as others that are ongoing. Finally, emerging companion diagnostic approaches that seek to identify breast cancers that have deficiencies in HR and might benefit from platinum or PARP inhibitor therapeutic approaches will be discussed.
44

Notes
Slides are embargoed at time of printing due to late breaking presentation of TNT trial
[Thursday, December 11, General Session 3, S3‐01. Tutt A, Ellis P, Kilburn L, Gilett C, Pinder S,
Abraham J et al. The TNT trial: A randomized phase III trial of carboplatin (C) compared with
docetaxel (D) for patients with metastatic or recurrent locally advanced triple negative
or BRCA1/2 breast cancer (CRUK/07/012)] .
45

Notes
46

Biomarker‐Driven Approach to PARP Inhibitor Clinical Trials
Hope S. Rugo, MD
Cancer drug development is complex, and has traditionally been complicated by
difficulties identifying subpopulations who benefit from specific therapies, leading to
prolonged times for active drug approvals. Indeed, biomarker studies generally identify
those patients whose tumors are less likely to respond to a specific therapy, rather than
identifying those who are most likely to respond. One of the areas of most intense
interest is identifying specific therapies for subsets within triple negative breast cancers,
as these cancers have both aggressive biology and limited treatment options. The
neoadjuvant setting offers the possibility of a new paradigm for both evaluation of new
agents and real time assessment of biomarkers.
I‐SPY2 is a multicenter standing phase II randomized trial designed to evaluate the
impact of a series of novel agents in combination with standard therapy. In this
presentation, Dr. Rugo will discuss the first results from I‐SPY2, combining the PARP
inhibitor veliparib, carboplatin and paclitaxel as neoadjuvant therapy for HER2 negative
breast cancer with a novel adaptive trial design allowing small numbers of patients but
resulting in data with significant impact. In addition, Dr. Rugo will share new biomarker
data that will be presented at SABCS 2014 from both I‐SPY2 as well as CALGB 40603 that
offers initial insight into which patients may benefit from carboplatin and veliparib.
Lastly, Dr. Rugo will review several studies with PARP inhibition that will take these
questions to the next level in the neoadjuvant and metastatic settings.
47

Biomarker-Driven Approach to PARP Inhibitor Clinical Trials
Hope S. Rugo, MD
Professor of Medicine
Director, Breast Oncology and Clinical Trials Education
University of California, San Francisco
San Francisco, CA
Disclosure Information
• Has received grant/research support from Amgen, Eisai, GSK, Genentech/Roche, Novartis, Macrogenics, Merck, OBI, Pfizer, and Plexxikon
• Has received honoraria from Genomic Health
• Will be discussing PARP inhibitors in clinical trials
Learning Objectives
• Describe the role of neoadjuvant clinical trials in drug development
• Assess the potential of the neoadjuvant setting to identify biomarkers that will power future definitive trials
Rugo -Biomarker Approach to Clinical Trials
48

Problems with Oncologic Drug Development
• New oncology drugs take 10-15 years to reach patients
• Price tag is $2 billion
• Absence of innovation in trial design/data collection tools
• Cancer is a subset of diseases; Blockbuster approach won’t work
Current path is UNSUSTAINABLE
Potential Advantages of the Neoadjuvant Setting for Drug Development
• In vivo assessment of pharmacodynamic markers to provide evidence of biological effect– Hitting target > cytostatic/cytotoxic effect?
• New agents tested in treatment naïve population– Metastatic response does not always translate to adjuvant benefit
• Early surrogates provide proximate measure of response correlating with long-term outcomes– Early estimate of effect and effect size in adjuvant setting
Goal: Shorten the time, cost and number of patients needed to bring efficacious new drugs to market
The “Neoadjuvant Hypothesis” for Drug Development
An increase in pCR with the addition of a new agent to standard therapy in the neoadjuvant setting will predict a survival benefit (EFS or OS) in the early breast cancer setting
Rugo -Biomarker Approach to Clinical Trials
49

CTNeoBC Meta-Analysis Results
• Individual patients with pCR have superior outcomes
• HER2+ and triple negative have highest pCR rates
• Eradication of invasive cancer from breast + nodes predicts best outcome– Residual DCIS not
prognostically important
Cortazar et al, Lancet 2014; 384: 164-72
Did Increased pCR Lead to Increased EFS?
No relationship between magnitude of improvement in pCR rate and EFS/OS at trial level
• Low pCR rates in included trials
• Only one small trial included targeted therapy
• Validation of pCR as endpoint is needed
Cortazar et al, Lancet 2014; 384: 164-72
Incremental Increase of pCR Rates in TNBC
1 Huober BCRT 2010, 2 von Minckwitz NEJM 2012, 3Gerber, ASCO 2011
GeparTrio1 GeparQuinto2,3 GeparSixto
Rugo -Biomarker Approach to Clinical Trials
50

CALGB 40603: Schema – Randomized phase II
Paclitaxel 80 mg/m2 wkly x 12 ddAC x 4
Bevacizumab 10 mg/kg q2wks x 9
Bevacizumab 10 mg/kg q2wks x 9
Carboplatin AUC 6 q3wks x 4
Carboplatin AUC 6 q3wks x 4
Paclitaxel 80mg/m2 weekly x 12
Surgery&*
XRT*
No Adjuvant Systemic Treatment Planned*
Paclitaxel 80 mg/m2 wkly x 12
Paclitaxel 80 mg/m2 wkly x 12
Paclitaxel 80 mg/m2 wkly x 12
2 X 2 Randomization
ddAC x 4
ddAC x 4
ddAC x 4
CALGB 40603: Randomized Phase II in TNBC
Sikov et al. JCO 2014
CALGB 40603: pCR Breast/Axilla (ypT0/is N0)
41% (35-48%) 54% (48-61%)
Odds ratio: 1.71 p = 0.0029
N=212 N=221
CALGB 40603 pCR Breast/Axilla (ypT0/is N0) +/- Carboplatin and +/- Bevacizumab
Sikov et al. JCO 2014
44% (38-51%) 52% (45-58%)
N=218 N=215
Accelerated FDA Drug Approval through Neoadjuvant Trials using pCR as Surrogate with Biomarker Partner
Achieve surrogate endpoint predicting clinical outcome
Promising drug candidate and associated biomarker
Replicate effect of drug/biomarker pair on surrogate
Achieve clinical outcome (regulatory standard for FDA approval)
Accelerated drug approval
Approval of biomarker
Full drug approval
“SCREENING TRIAL”
Smaller“CONFIRMATORY
TRIAL”
“FDA APPROVAL”
Esserman & Woodcock, JAMA, 2011, Prowell & Pazdur, NEJM, 2012
Rugo -Biomarker Approach to Clinical Trials
51

I‐SPY 2 Multicenter Trial
• 18 sites accruing• >975 patients screened;
>550 randomized• 6 drug companies• 3 device companies• 2 drug/biomarkers
“graduated”• New pipeline drugs
• Canada
Funding: Public/Private Partnerships
• Screen phase 2 agents in combination with standard chemotherapy in neoadjuvant setting
• Endpoint is pCR• Design is adaptive within the trial• “threshold” is 85% predicted likelihood of success in a 300-
patient phase 3 trial for drug biomarker pair
• Accelerate process of identifying drugs that are effective for specific breast cancer subtypes– Integration of biomarkers, analysis within subsets by design
• Reduce the cost, time, and numbers of patients needed to get effective drugs to market through accelerated approval
• Utilize multiple funding sources to avoid dependence on pharmaceutical companies
I-SPY 2 Multicenter Randomized Phase II Trial
Paclitaxel + Trastuzumab* +
New Agent A
Paclitaxel + New Agent C
Patient is on Study
Paclitaxel+ Trastuzumab
Paclitaxel + Trastuzumab* +
New Agent B
Paclitaxel
Paclitaxel + New Agent E
AC
ACHER 2 (+)
HER 2(–)
Randomize
Randomize
Surgery
Surgery
Learn and adapt from each patient as
we go along
Paclitaxel + New Agent F
Paclitaxel + Trastuzumab* +
New Agent C
Paclitaxel + New Agent DPaclitaxel +
New Agent GH
Paclitaxel + Trastuzumab* +
New Agent F
*Investigational agent may be used in place
MRI
ResidualDisease
(Pathology)
Key
I-SPY 2 TRIAL:Learn, Drop, Graduate, and Replace Agents Over Time
Rugo -Biomarker Approach to Clinical Trials
52

Rugo -Biomarker Approach to Clinical Trials
53

Rugo et al, SABCS 2013
Next Steps
• I-SPY2 is an ongoing trial, adding new agents as current agents graduate– Agents currently in trial include
• AMG 386 (angiopoietin inhibitor, all)• AMG 479 and meformin (IGFR inhibitor, HER2 neg)• MK-2206 (AKT inhibitor, all)• Ganitespib (HSP90 inhibitor, HER2 neg)• Pertuzumab/trastuzumab (HER2+ only)• TDM-1/pertuzumab (HER2+ only, no taxane)
• What happens when a drug graduates?– International I-SPY3 trial
• 300 patient randomized trial to be used for accelerated approval
Rugo -Biomarker Approach to Clinical Trials
54

PARPi-7: An In Vitro Derived Signature Of Olaparib Response As A Predictive Biomarker Of
Response To Veliparib/Carboplatin
• 7 gene DNA-repair deficiency expression signature– BRCA1, CHEK2, MAPKAPK2, MRE11A, NBN, TDG, and
XPA
• Developed from breast cancer cell lines
• Distinguishes between olaparib-sensitive and olaparib-resistant cell lines
• Robust over multiple platformsDaemen A, et al. Breast Cancer Res Treat, 2012
Measured response:•7 sensitive cell lines•15 resistant cell lines
Measured response:•7 sensitive cell lines•15 resistant cell lines
Collected 22 breast cancer cell lines
Gene expression:Affymetrix Exonarray and U133A;Illumina RNA-seq,
Limit to DNA repair pathways: BER, NER,MMR, HR/FA, NHEJ, DDR; 118 genes
Derived signature:•Linear regression• Forward feature selection• Fivefold CV• Weighted voting algorithm
Wolf et al, SABCS 2014
Rugo -Biomarker Approach to Clinical Trials
55

PARPi-7 dichotomized using published in vitroderived cutpoint yields 62 PARPi-7 Low and
53 PARPi-7 High patients
• The PARPi-7 signature associates with patient response in the V/C arm (p=0.00056) but not in the control arm (p=0.68)
• There is significant biomarker x treatment interaction– OR in V/C arm relative to control arm = 4.48, p=0.0028
• P=0.0018 adjusted for HR status
V/C arm Control arm
The PARPI-7 High/Low classification associates with patient response in the V/C arm (OR = 6.8, p=0.0005) but
not in the control arm (OR = 0.75, p=1) p value = 0.018 for biomarker x treatment interaction (OR in
V/C arm relative to control arm = 9.3) p value adjusted for HR status is 0.016
Rugo -Biomarker Approach to Clinical Trials
56
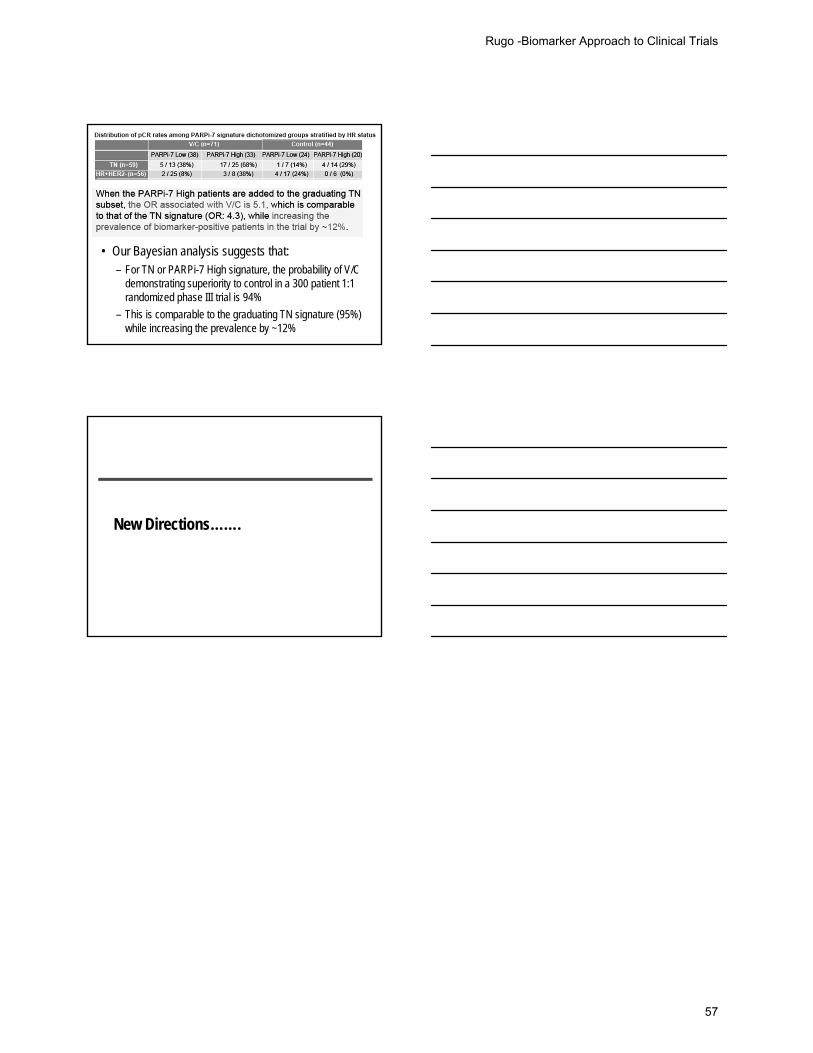
• Our Bayesian analysis suggests that:– For TN or PARPi-7 High signature, the probability of V/C
demonstrating superiority to control in a 300 patient 1:1 randomized phase III trial is 94%
– This is comparable to the graduating TN signature (95%) while increasing the prevalence by ~12%
New Directions…….
Rugo -Biomarker Approach to Clinical Trials
57

Selected References
American Cancer Society: Cancer Facts and Figures 2014. Atlanta, GA Antoniou AC, Casadei S, Heikkinen T, Barrowdale D, Pylkäs K, Roberts J, et al. Breast‐cancer risk in families with mutations in PALB2. N Engl J Med. 2014 Aug 7;371(6):497‐506. Barrow E, Robinson L, Alduaji W et al. Cumulative lifetime incidence of extracolonic cancers in Lynch syndrome: a report of 121 families with proven mutations. Clin Genet. 2009; 75(2): 141. Chen S, Parmigiani G. Meta‐analysis of BRCA1 and BRCA2 penetrance. J Clin Oncol. 2007; 25(11): 1329. Cortazar P, Zhang L, Untch M, Mehta K, Costantino JP, Wolmark N, et al. Pathological complete response and long‐term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet. 2014 Jul 12;384(9938):164‐72. Daemen A, Wolf DM, Korkola JE, Griffith OL, Frankum JR, Brough R, Jakkula LR, Wang NJ, Natrajan R, Reis‐Filho JS, Lord CJ, Ashworth A, Spellman PT, Gray JW, van't Veer LJ. Cross‐platform pathway‐based analysis identifies markers of response to the PARP inhibitor olaparib. Breast Cancer Res Treat. 2012 Sep;135(2):505‐17. Domchek SM, Friebel TM, Singer CF, Evans DG, Lynch HT, Isaacs C, Garber JE, Neuhausen SL, Matloff E, Eeles R, Pichert G, Van t'veer L, Tung N, Weitzel JN, Couch FJ, Rubinstein WS, Ganz PA, Daly MB, Olopade OI, Tomlinson G, Schildkraut J, Blum JL, Rebbeck TR. Association of risk‐reducing surgery in BRCA1 or BRCA2 mutation carriers with cancer risk and mortality. JAMA. 2010 Sep 1;304(9):967‐75. Domchek SM, Nathanson KL. Panel testing for inherited susceptibility to breast, ovarian, and colorectal cancer. Genet Med. 2014 Nov;16(11):827‐9. Esserman LJ, Woodcock J. Accelerating identification and regulatory approval of investigational cancer drugs. JAMA. 2011 Dec 21;306(23):2608‐9. Euhus D. Genetic testing today. Ann Surg Oncol. 2014 Oct;21(10):3209‐15. Graeser MK, Engel C, Rhiem K, Gadzicki D, Bick U, Kast K, Froster UG, Schlehe B, Bechtold A, Arnold N, Preisler‐Adams S, Nestle‐Kraemling C, Zaino M,Loeffler M, Kiechle M, Meindl A, Varga D, Schmutzler RK. Contralateral breast cancer risk in BRCA1 and BRCA2 mutation carriers. J Clin Oncol. 2009 Dec 10;27(35):5887‐92. Harris TJ, McCormick F. The molecular pathology of cancer. Nat Rev Clin Oncol. 2010 May;7(5):251‐65. Ketabi Z, Bartuma K, Bernstein I, Malander S, Grönberg H, Björck E, Holck S, Nilbert M. Ovarian cancer linked to Lynch syndrome typically presents as early‐onset, non‐serous epithelial tumors. Gynecol Oncol. 2011 Jun 1;121(3):462‐5.
58

Koornstra JJ, Mouris MJ et al. Management of extracolonic tumours in patients with Lynch syndrome. Lancet Oncol. 2009; 10(4):400. Kurian AW, Hare EE, Mills MA, Kingham KE, McPherson L, Whittemore AS, McGuire V, Ladabaum U, Kobayashi Y, Lincoln SE, Cargill M, Ford JM Clinical evaluation of a multiple‐gene sequencing panel for hereditary cancer risk assessment. J Clin Oncol. 2014 Jul 1;32(19):2001‐9. Kwon JS, Gutierrez‐Barrera AM, Young D, Sun CC, Daniels MS, Lu KH, Arun B. Expanding the criteria for BRCA mutation testing in breast cancer survivors. J Clin Oncol. 2010 Sep 20;28(27):4214‐20. LaDuca H, Stuenkel AJ, Dolinsky JS, Keiles S, Tandy S, Pesaran T, Chen E, Gau CL, Palmaer E, Shoaepour K, Shah D, Speare V, Gandomi S,Chao E. Utilization of multigene panels in hereditary cancer predisposition testing: analysis of more than 2,000 patients. Genet Med. 2014 Nov;16(11):830‐7. Mannis GN, Fehniger JE, Creasman JS, Jacoby VL, Beattie MS.Risk‐reducing salpingo‐oophorectomy and ovarian cancer screening in 1077 women after BRCA testing. JAMA Intern Med. 2013 Jan 28;173(2):96‐103. Norquist BM, Pennington KP, Agnew KJ, Harrell MI, Pennil CC, Lee MK, Casadei S, Thornton AM, Garcia RL, Walsh T, Swisher EM. Characteristics of women with ovarian carcinoma who have BRCA1 and BRCA2 mutations not identified by clinical testing. Gynecol Oncol. 2013 Mar;128(3):483‐7. Prowell TM, Pazdur R. Pathological complete response and accelerated drug approval in early breast cancer. N Engl J Med. 2012 Jun 28;366(26):2438‐41.
Rafnar T, Gudbjartsson DF, Sulem P, Jonasdottir A, Sigurdsson A, Jonasdottir A, et al. Mutations in BRIP1 confer high risk of ovarian cancer. Nat Genet. 2011 Oct 2;43(11):1104‐7. Rainville IR, Rana HQ. Next Generation Sequencing for Inherited Breast Cancer Risk: Counseling through the complexity. Curr Oncol Rep. 2014;16:371. Rich TA, Woodson AH, Litton J, Arun B. Hereditary Breast Cancer Syndromes and Genetic Testing. J Surg Oncol .2014;Nov 7:1‐16. Robson M. Multigene panel testing: planning the next generation of research studies in clinical cancer genetics. J Clin Oncol. 2014;Jul 1;32(19):1987‐9. Rugo HS, Olopade O, DeMichele A, et al: Veliparib/carboplatin plus standard neoadjuvant therapy for high‐risk breast cancer: First efficacy results from the I‐SPY 2 trial. 2013 San Antonio Breast Cancer Symposium. Abstract S5‐02. Presented December 13, 2013. Schrader KA, Stratton KL, Murali R, Laitman Y, Cavallone L, Offit L, et al. Genome Sequencing of Multiple Primary Tumors Reveals a Novel PALB2 Variant. J Clin Oncol. 2014 Jun 30. pii: JCO.2013.50.0272.
59

Sikov WM, Berry DA, Perou CM, Singh B, Cirrincione CT, Tolaney SM, et al. Impact of the Addition of Carboplatin and/or Bevacizumab to Neoadjuvant Once‐per‐Week Paclitaxel Followed by Dose‐Dense Doxorubicin and Cyclophosphamide on Pathologic Complete Response Rates in Stage II to III Triple‐Negative Breast Cancer: CALGB 40603 (Alliance). J Clin Oncol. 2014 Aug 4. pii: JCO.2014.57.0572. Stadler ZK, Schrader KA, Vijai J et al Cancer Genomics and Inherited Risk. J Clin Oncol. 2014;32(7): 687‐698. Solimon PT, OH JC, Schmeler KM et al. Risk factors for young premenopausal women with endometrial Obstet Gynecol. 2005 Mar; 105(3):575‐80. Tung N, Battelli C, Allen B, Kaldate R, Bhatnagar S, Bowles K, Timms K, Garber JE, Herold C, Ellisen L, Krejdovsky J, DeLeonardis K, Sedgwick K, Soltis K, Roa B, Wenstrup RJ, Hartman AR. Frequency of mutations in individuals with breast cancer referred for BRCA1 and BRCA2 testing using next‐generation sequencing with a 25‐gene panel. Cancer. 2014 Sep 3. Tutt A, Robson M, Garber JE, Domchek SM, Audeh MW, Weitzel JN, et al. Oral poly(ADP‐ribose) polymerase inhibitor olaparib in patients with BRCA1 or BRCA2 mutations and advanced breast cancer: a proof‐of‐concept trial. Lancet. 2010 Jul 24;376(9737):235‐44. von Minckwitz G, Eidtmann H, Rezai M, Fasching PA, Tesch H, Eggemann H, et al ; German Breast Group; Arbeitsgemeinschaft Gynäkologische Onkologie–Breast Study Groups. Neoadjuvant chemotherapy and bevacizumab for HER2‐negative breast cancer. N Engl J Med. 2012 Jan 26;366(4):299‐309. Walsh T, Casadei S, Lee MK, Pennil CC, Nord AS, Thornton AM, et al. Mutations in 12 genes for inherited ovarian, fallopian tube, and peritoneal carcinoma identified by massively parallel sequencing. Proc Natl Acad Sci U S A. 2011 Nov 1;108(44):18032‐7. Watson P, Vasen HF, Mecklin JP et al. The risk of extra‐colonic, extra‐endometrial cancer in the Lynch Int J Cancer. 2008 Jul 15; 123(2):444‐9. Watson P, Butzow R, Lynch HT et al. The clinical features of ovarian cancer in hereditary nonpolyposis colorectal International Collaborative Group on HNPCC Gynecol Oncol. 2001 Aug; 82. Wolf DM, Yau C, Sanil A, Chien J, Wallace A, DeMichele A, et al. MammaPrint High1/High2 risk class as a biomarker of response to veliparib/carboplatin plus standard neoadjuvant therapy for breast cancer in the I‐SPY 2 TRIAL Poster Session (P3‐06‐25). San Antonio Breast Cancer Symposium. December 9‐13, 2014.
60