t22 - dm & pregnancy (zaimah) - print version
DESCRIPTION
fileTRANSCRIPT
Tutorial 22
Diabetes and pregnancy

Diabetes In Pregnancy
2 patients
Mother
Develop Diabetes
during Pregnancy
Known Diabetes before
Pregnancy (T1 & T2)
Baby
2

Gestational Diabetes
Definition: Any degree of glucose intolerance of with onset or first recognition during pregnancy
• Glucose tolerance reduce in pregnancy due to increase secretion of insulin antagonist & steroid hormones:
Human placental lactogen
Progesterone
Cortisol
Oestrogen
Glucagon
• Normal pregnancy - pancreatic cells increase secretion of insulin to counteract increased insulin resistance
• Mechanism failed in GDM

Pregnancy physiology
Pregnancy is a diabetogenic state/state of increasing insulin resistance
•Maternal metabolism is altered to ensure appropriate supply of glucose to fetus
• Facilitated diffusion across placenta = Fetal
hyperglycaemia
•Maternal insulin does not cross the placenta

Screening for diabetes Who to screen?
-High risk group screening:
-Diabetes mellitus in 1st degree relatives
-Glycosuria on >2ocassions/in 1 fasting urine sample
-Diabetes in previous pregnancy
-Gross obesity/Maternal weight>90kg
-History of unexplained IUD/early neonatal death
-History of macrosomia (>4kg)
-Recurrent vaginal candidiasis
-Polyhydramnios in current pregnancy
-Congenital abnormality in previous pregnancy

When to screen? – 24 to 28 weeks gestation
– Earlier in women with previous GDM
• First antenatal visit/16-18 weeks
• If negative rescreen at 24 weeks
How to screen ?
- 75g OGTT (patient is asked to fast for 8 hours, blood is taken,
75g of sugar is diluted in 100ml of water, blood is taken again after
2 hours)

• Diagnostic Criteria for diabetes in pregnancy WHO
6/2/2015 7
Fasting blood
glucose
2hr post-
prandial blood
glucose
Normal < 6.0 mmol/L < 7.8mmol/L
GDM ≥6.1 mmol/L ≥7.8 mmol/L
Diabetes
Mellitus
≥ 7.0 mmol/L
≥ 11.1mmol/L

Case Scenario
• A 30 year old school teacher attend you at 6 weeks gestation for a booking visit.
• She has been an insulin-dependent diabetic since the age of 15, has no evidence of diabetic nephropathy, or retinopathy.
• She has already visited you for prepregnancy advice, and has also seen the diabetic physician.
• She has been trying to conceived for several months and had endeavored to maintain good glycaemic control in the months leading up to conception.
• She has taken folic acid supplement.

Insulin-dependent diabetes
• Type 1 diabetes mellitus/juvenile diabetes/early-onset diabetes
• often develops before the age of 40, usually during the teenage years.
• lifelong condition that causes a person's blood sugar level to become too high.
• the pancreas does not produce any insulin.
Pre conception care
• The role of strict glycaemic diet, body weight and exercise.
• The risks associated with pregnancies complicated by diabetes increase with the duration of diabetes
• To use contraception until good glycaemic control (assessed by HbA1c2) has been established.
• Glycaemic targets, glucose monitoring, medications for diabetes (including insulin regimens for insulin-treated diabetes) and medications for complications of diabetes will need to be reviewed before and during pregnancy.
• Frequent contact with healthcare professionals

Question 1 What risk, if any, exist for the fetus in pregnancy such as this, in a well controlled diabetic patient?
• Studies have shown that women who have well-controlled diabetes before becoming pregnant and who maintain low glucose levels
throughout pregnancy are NOT at an increased risk for having a
baby born with birth defects.
• The same goes to GDM
*Organization of Teratology Information Specialists (OTIS)

Fetal Complications Diabetes Embropathy
Maternal hyperglycaemia fetal
hyperinsulinaemia
• Fetal macrosomia (10-20%)
• Birth trauma (shoulder dystocia, bone
fracture, nerve palsy~ 1-4%)
• Operative delivery
• Polycythaemia (Fetal Macrosomia
relative hypoxaemia increase EPO
• Still birth
• Intrauterine death- (fetal hyperinsulinemia causing chronic hypoxia and lactic acedemia)
Diabetes Fetopathy
Hyperglycaemia yolk sac failure
• Congenital anomalies (organogenesis during 1st trimester)
• Spontaneous abortion
12

• Development of obesity/ diabetes in childhood and later adulthood
• Prematurity
• Perinatal asphyxia
• Respiratory distress syndrome (due
to hypoxemia causing impaired
fetal growth)
• Neonatal hypoglycaemia (mother’s
hyperglycemia causes fetal
hyperinsulinmia)
• Hyperbilirubinaemia (due to
polycythemia, so increase in
bilirubin, maternal liver overloads to
remove, so excess in blood)
Late complications Neonatal effect Child/ adulthood effect
13

Maternal Complications
• Microvascular: nephropathy, retinopathy, neuropathy
• Macrovascular: coronary artery diseases
• Hyperglycemia / hypoglycemia /ketoacidosis
• Pre-eclampsia
• Infection
• Thromboembolism

Question 2
Outline the medical management of this patient through her pregnancy.
1. Routine first booking antenatal care.
2. Admit patient for Blood Sugar Profile.
Fasting, Pre-lunch, Pre-dinner, Pre-bed (normal range: 4-6 mmol/L)

3. Choice of therapy:
- Diet control: High fibre diet, balanced nutritional meal. (Refer to dietician)
- combination of diet control and insulin
(choice of therapy and dose of insulin depends on Blood Sugar Profile)
- NOTE: ORAL HYPOGLYCAEMICS such as metformin CAN still BE USED IN PREGNANCY, but since she is T1DM…so:
- Subcutaneous injections of short acting insulin/combination of short and intermediate acting insulin in the morning and evening.

4. Investigation:
- 2 weekly Blood Sugar Profile
- detailed U/S 18-20 weeks to exclude foetal malformation.
- Urine Full Examination Microscopic Examination
- Renal profile
- HbA1c per trimester , aiming for < 6.5%
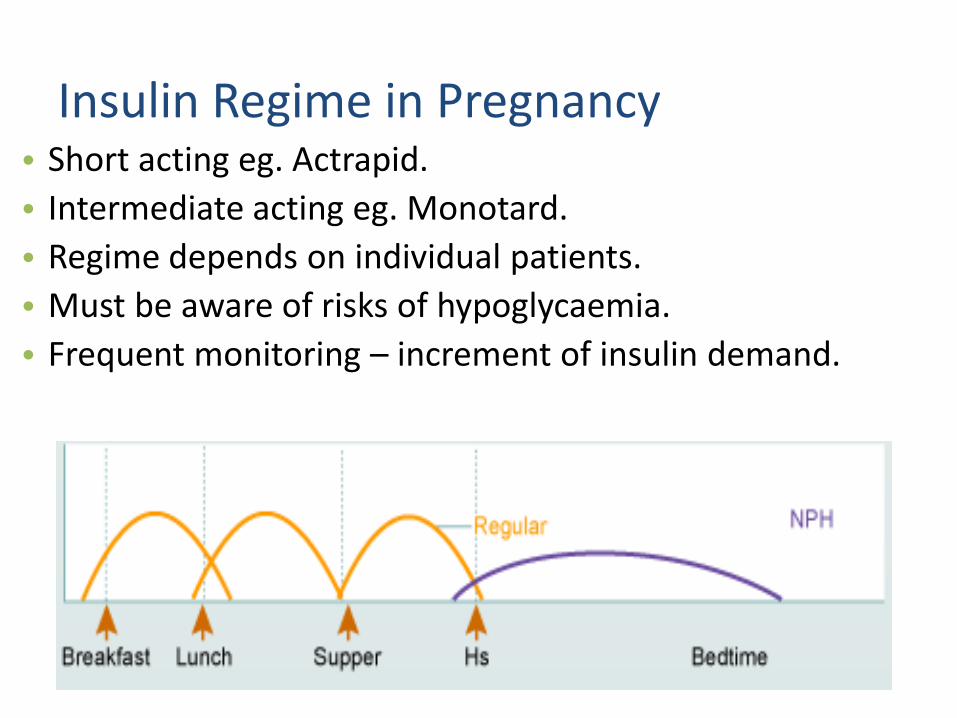
Insulin Regime in Pregnancy • Short acting eg. Actrapid.
• Intermediate acting eg. Monotard.
• Regime depends on individual patients.
• Must be aware of risks of hypoglycaemia.
• Frequent monitoring – increment of insulin demand.

4. At follow up:
– If diabetes is well controlled, patient is taught to do home monitoring and can be managed as out-patient (at Health Clinics).
– Antenatal care: 2 week intervals.
– check for maternal complication, eg: HTN, infection (UTI, URTI, candidiasis), ketonuria, polyhydramnios, retinopathy, nephropathy, neuropathy
– Check for foetal well being- foetal movement chart, CTG after 30 weeks.
– Serial scan every 4 weeks to check foetal growth (macrosomia, polyhydramnios or IUGR).

5. Admission
- if control is poor
for assessment of BSP
adjustment of insulin
any complication present
6. Timing of delivery:
DM on insulin treatment : 38 weeks
DM on diet control : 40 weeks

Question 3 She attends regularly & maintains good glycaemia control.
At 20 weeks gestation a detailed ultrasound scan show no evidence of any fetal abnormality.
Serum alpha-fetoprotein measurement had previously been normal.
She is reassured but 1 week later is referred as emergency by her GP as she is complaining of rigors and abdominal pain.
On examination, she has temperature of 39ºC, her abdomen is tender and she has bilateral renal angle tenderness.
What is the likely diagnosis, and what implication does it have on her pregnancy?

Acute Pyelonephritis in Pregnancy Incidence
• Occurs more commonly than any other medical problem in
pregnancy
• Overall incidence is 1 - 2.5% in those receiving UNIVERSAL
SCREENING and treatment of asymptomatic bacteriuria
(ASB)
• As high as 40% of pregnancies with untreated ASB will
develop pyelonephritis

Predisposing Factors
Physiologic changes of pregnancy: Hydronephrosis (growing fetus blocks mother’s ureter), vesicoureteral
reflux (a/w UTI)
Increased bladder capacity (pregnancy causes smooth muscle relaxation of bladder), incomplete emptying (due to fetus)
Increased urine pH during pregnancy (due to diet and other changes)
Coexistent factors: Urinary anomalies, calculi, multiple UTI’s
Dehydration, poor hygiene
Resistant organisms, noncompliance to treatment
Diabetes, Sickle disease

Diagnostic Criteria
• Clinical Findings: • Fever, chills, malaise
• Costovertebral angle pain/tenderness, dysuria, frequency
• 50% unilateral right sided flank pain
• 25% bilateral or unilateral left sided pain
• Laboratory Findings: • Pyuria, bacteriuria
• White blood cell casts highly predictive
• Positive urine culture
• 10 – 20% bacteremic

Pathophysiology of Pyelonephritis in Pregnancy
Infections result from ascending colonization of the urinary tract, primarily by existing vaginal, perineal, and fecal flora.
• E coli (80-90% of cases) – from fecal flora that colonizing periurethral area.
• Klebsiella pneumoniae (5%)
• Proteus mirabilis (5%)
• Enterobacter species (3%)
• Staphylococcus saprophyticus (2%)
• Group B beta-hemolytic Streptococcus (GBS; 1%)
• Proteus species (2%)

• Urinary retention caused by the weight of the enlarging uterus and urinary stasis due to progesterone-induced ureteral smooth muscle relaxation.
• Loss of ureteral tone combined with increased urinary tract volume results in urinary stasis, which can lead to dilatation of the ureters, renal pelvis, and calyces.
• This dilatation appears to begin by about 10 weeks’ gestation and worsens throughout pregnancy
• Urinary stasis and the presence of vesicoureteral reflux predispose some women to upper urinary tract infections (UTIs) and acute pyelonephritis.
Complications:
1. Septic shock (rare)
2. Renal dysfunction : have a decreased glomerular filtration rate
3. Hypoxic fetal events : uterine hypoperfusion due to maternal dehydration, maternal anemia, and direct bacterial endotoxin damage to the placental vasculature may cause fetal hypoxia
4. Premature delivery (spontaneous abortion in early pregnancy)

5. Pulmonary injury may also complicate UTI in pregnancy. Approximately 2% of women with severe pyelonephritis during pregnancy have evidence of pulmonary injury due to systemic inflammatory response syndrome and respiratory insufficiency. Endotoxins that alter alveolar-capillary membrane permeability are produced; subsequently, pulmonary edema and acute respiratory distress syndrome develop.
6. Untreated upper UTIs are associated with low birth weight, prematurity, premature labor, hypertension, preelampsia, maternal anemia, and amnionitis.

Question 4 What is the likely effect of the pregnancy on her diabetes?
1. Insulin requirement often increases in late pregnancy. Reverts to usual requirement post-partum.

2. The tight glucose control may lead to increase risk of hypoglycaemia.
3. The kidneys of non-pregnant women start to excrete glucose at the threshold of 11mmol/L. In pregnancy, it often decrease so glycosuria may occur at physiological blood glucose concentration.
4. Exacerbate pre-existing diabetic retinopathy and nephropathy

Question 5
What maternal complication are more likely in this pregnancy, and what special care is therefore required?
1. Hypoglycemia
2. Diabetic ketoacidosis
3. Pre-eclampsia
4. Diabetic retinopathy
5. Diabetic nephropathy
6. Increase risk of infection, esp. vaginal candidiasis.

• Tight glycemic control without severe hypos
• Medical nutritional therapy
• Physical activity(exercise)
Principle of Management

HYPOGLYCAEMIA • Women with insulin-treated diabetes should be advised of the risks
of hypoglycaemia and hypoglycaemia unawareness in pregnancy, esp. in the 1st trimester.
• During pregnancy, women with insulin-treated diabetes should be provided with a concentrated glucose solution and women with type 1 diabetes should also be given glucagon; women and their partners/other family members should be instructed in their use.
• During pregnancy, women with insulin-treated diabetes should be offered continuous subcutaneous insulin infusion (CSII/insulin pump therapy) if adequate glycaemic control is not obtained by multiple daily injections of insulin without significant disabling hypoglycaemia.

DIABETIC KETOACIDOSIS • If diabetic ketoacidosis is suspected during pregnancy, admit women
immediately for level 2 critical care, where both medical and obstetric care are available.
• For women with type 1 diabetes:
– offer ketone testing strips and advise women to test their ketone levels if they are hyperglycaemic or unwell
– exclude diabetic ketoacidosis as a matter of urgency in women who become unwell
* Level 2 critical care is defined as care for patients requiring detailed observation or
intervention, including support for a single failing organ system or postoperative care and
those ‘stepping down’ from higher levels of care.

PREECLAMPSIA
• Pre-eclampsia 7 fold more likely – offer low dose aspirin
as prophylaxis
• LMW heparin if proteinuria > 3g

RETINAL ASSESSMENT • Pregnant women with pre-existing diabetes should be offered retinal
assessment by digital imaging with mydriasis using tropicamide following their 1st antenatal clinic appointment and again at 28 weeks if the first assessment is normal. If any diabetic retinopathy is present, an additional retinal assessment should be performed at 16–20 weeks.
• If retinal assessment has not been performed in the preceding 12 months, it should be offered as soon as possible after the 1st contact in pregnancy in women with pre-existing diabetes.

• Diabetic retinopathy should not be considered a contraindication to rapid optimisation of glycaemic control in women who present with a high HbA1c in early pregnancy.
• Women who have preproliferative diabetic retinopathy diagnosed during pregnancy should have ophthalmological follow-up for at least 6 months following the birth of the baby.
• Diabetic retinopathy should not be considered a contraindication to vaginal birth

RENAL ASSESSMENT • If renal assessment has not been undertaken in the preceding
12months in women with pre-existing diabetes, it should be arranged at the 1st contact in pregnancy.
• If serum creatinine is abnormal (≥120µmol/L) or if total protein excretion >2 g/day, referral to a nephrologist should be considered (eGFR should not be used during pregnancy).
• Thromboprophylaxis should be considered for women with proteinuria >5 g/day (macro-albuminuria).
Question 6
• At 30 weeks gestation, in the course of her combined obstetric-diabetic review, you find that her blood pressure is
130/95 mmHg. On rechecking it is 120/90 mmHg. Her
booking blood pressure was 110/78 mmHg. What would
your concern be and how would you assess the situation?

1. Pregnancy Induced Hypertension
• new onset hypertension develops in the second half of pregnancy (>20weeks) ≥BP 140/90 mmHg on 2 separate occasions 4-6 hours apart in a previously normotensive patient or
• rise SBP of 30mmHg and/ or
• a rise in DBP of 15mmHg compared to pre pregnancy level

2. Pre-eclampsia
-The risk of pre-eclampsia is increased two- to four-fold in women with diabetes
Dx :
PIH + proteinuria (>0.3g/24 hr urine)

Assess the situation..
•History of presentation: -usually mild-moderate may be asymptomatic, -pre-eclampsia in previous pregnancies Symptoms: -nausea & vomiting -headache & giddiness 6 signs of impending eclampsia
-epigastric pain & blurring of vision -massive edema (face&abdomen) -HPT and proteinuria Other signs to seek: i)Abdomen:larger than date (polyhydramnios,macrosomia) ii)Reflexes:hyperreflexia, clonus iii)Fundoscopy: Retinopathy

Assessment
Investigation Indication
To confirm Dipstick urinalysis
-Proteinuria for confirmation if Albumin 2+, 24hr >0.3g/L:confirm the dx
MSU Culture to rule out infection
To assess severity
FBC (Hb,Pt) Coagulation profile
Hb is often high (haemoconcentration), Plt decrease (impending HELLP or DIC)
U&E Renal function
Renal failure (elevation of creatinine) Pre-eclampsia (elevation of uric acid)
Liver function test Increase in impending liver damage or HELLP
Fetal well-being 1)U/S 2)CTG 3)Doppler
-estimate fetal weight,size -evaluate fetal well-being -Blood flow in placenta
To monitor Watch BP every 4 hours, serial FBC, U&E, LFTs

Question 7 A series of US scans between 28 and 36 weeks gestation have demonstrated that the fetus is indeed macrosomic, despite good glycaemic control with the fetus lying above the 95th centile for gestation in term of weight as assessed by abdominal circumference. At 36 weeks of gestation, you discuss delivery with her. She is keen to have a spontaneous labour & delivery but is conscious that she is at increased
risk of caesarean section because of the fetal macrosomia Regular fetal assessment have shown no evidence of fetal compromise and you plan to continue twice weekly assessment until delivery.
How should labour be managed?

• The timing of delivery will depend on the degree of control diabetes and the condition of fetus.
• Insulin treated GDM: at 38 weeks
• Diet controlled GDM : at 40 weeks, but not past the due date
• GDM with complications: at 38 weeks or earlier after confirming fetal lung maturity
• Mode of delivery
– Diabetes is not an indication for C-sec
– Vaginal delivery is possible in uncomplicated diabetic pregnancies

•Factors that would favour an elective Caesarean section in diabetes:
•Fetus>4kg,
•Macrosomia,
•suspicion of cephalo-pelvic disporportion,
•malpresentation,
•polyhydramnios,
•evidence of fetal compromise,
•bad obstetric history of recurrent stillbirth.
•Method: C-section: fetal macrosomia
•If she insists to continue with VD, explain the risks involved:
– traumatic birth,
– shoulder dystocia and therefore possible hypoxia damage.

Penang Hospital Protocol
On the day on induction of labour
a. Nil orally
b. GXM blood
c. FBS and BUSE
d. Check urine 4hourly for acetone
e. 5% of Dextrose drip + units of insulin to run for 5 hours at 5 to 15 dpm (the dose of additional insulin has to be titrated against blood sugar level assessed 2hourly by Reflometer and 4hourly by RBS aiming for level 4-6mmol/L)
Or Glucose-insulin-kalium (GIK) regime (refer protocol pg 77)

f) Keep blood sugar levels between 4-6 mmol/L
g)ARM + Oxytocin
h)Partogram
i) Foetal monitoring with CTG
j)Beware of shoulder dystocia (senior staff advised to be present at delivery)
k)Refer paediatric for assessment at delivery
*steroid is given if labour is foreseen to be earlier than expected so that lung can mature. It causes insulin resistance so insulin dosage needs to be adjusted to higher level to counter this problem.

Question 8
Frequent variable tachycardia (normal=8beats/min) and
late decelerations (fetal distress) occur at 3 cm cervical dilatation (unfavourable for induction and VG) and you perform a caesarean section for the suspected fetal distress. The baby is born in
good condition. What complication would
the baby be at risk post-natally?

1) Metabolic
Hypoglycemia
-hyperinsulinaemia due to hyperplasia of fetal pancreatic beta cell
Hypocalcaemia and Hypomagnesaemia
– delay in parathyroid hormone synthesis after birth
2) Haematological
Polycythemia –
-increased erythropoiesis triggered by chorionic fetal hypoxia

52
3) Liver •Jaundice/Hyperbilirubinaemia-due to polycythemia
4) Lung -Respiratory Distress Syndrome (metabolic effect of hyperglycemia on the lecithin:sphingomyelin ratio in the lung alveoli)
5) Cardiovascular -Cardiomyopathy
-Cardial septal hypertrophy

Question 9
Should the mother’s insulin dose be adjusted after delivery?
YES!
Recommence oral hypoglycemic or previous insulin therapy when the patient takes orally

Question 10
If a patient is not diabetic,
a) When should screening for gestational
diabetes be done?
Based on RCOG guideline
If the patient has the risk factors,
•24 to 28 weeks
•Earlier if suspect undiagnosed diabetes

b) Which woman should be screened?
HPP protocol: Indication for MGTT (if one or more) :
• History of DM in 1st degree relative • Glycosuria in 2 occasions or in a single fasting urine sample • Previous GDM • Maternal weight >90 kg (BMI>35) • Previous baby >4.0 kg • Previous unexplained intrauterine death or early neonatal death • Congenital abnormality in a previous pregnancy • Polyhydramnios in present or previous pregnancy • Recurrent vaginal candidiasis
After diagnosis has been made, admit the patient for blood sugar profile and therapy (Protocol HPP 2009)
Aim of BSP
Fasting,Pre-lunch,Pre-dinner,Pre-bed
4-6 mmol/L
Therapy
a)Diet control only 1800-2000 kcal daily, high fibre diet
b)Combination of diet control and insulin
Oral hypoglycemics should preferably be avoided because
1)Risk of teratogenicity in early pregnancy
2)Does not provide as good a control of blood sugars as insulin
c) What are the principles of management during the pregnancy if GDM is diagnosed?

• Choice of therapy and the dose of insulin depend on BSP.
• Vast majority of diabetics require insulin therapy and all patients should receive 2-3 daily
• Subcutaneous injection of a short acting insulin (eg:Actrapid, Humulin R) or preferably twice daily combination of short and intermediate acting insulin in the morning and evening.
• The initial dose of Humulin R is 5 units tds and subsequently increased to 2-5 units in a stepwise fashion.
• Patient who need more than 30units of short acting insulin a day should be converted to a combination of short acting (Actrapid) tds and intermediate (Monotard) insulin at night

Investigation after diagnosis
a) 2 to 4 weekly BSP (depending on control)
b) Detailed ultrasound scan at 18-20weeks to exclude foetal malformation and confirm gestational age
c) Urine FEME (renal nephropathy,infection)
d) Renal profile
e) If facilities are available, do HbA1c per trimester or/and fructosamine level monthly.
At follow up visit
-When diabetes is well controlled, patient is taught to do home monitoring and managed as outpatient
-Antenatal care: should be at 2 weekly intervals

•Check for maternal Cx :
-HPT
-infection eg: UTI,URTI, candidiasis
-Ketonuria, retinopathy, nephropathy, neuropathy
•Check for foetal well being:
-foetal movement chart
-CTG after 30 weeks
-Serial scans every 4 weeks to check foetal growth (macrosomia, IUGR,polyhydramnios)
•Admit patient
-if control is poor for assessment of BSP and patient may need adjustment of insulin
-if any complication present
•Timing of delivery
-well controlled diabetics with diet control alone – induce at 40 weeks
-well controlled diabetics with insulin – 38 weeks
-not well controlled diabetics – induced earlier than 38 weeks

d) Is this management likely to be different from 1-9 above? •No.
•Principles of management similar to established DM.
Except that:
•Insulin can be discontinued after delivery.
•Put back on normal diet.
•Appointment for OGTT at 6 weeks.
•Recheck Blood Sugar Profile prior to discharge.
•Follow up as there is a risk of Type II DM in patients with GDM.