systemic lupus erythematosus complicated by crohn’s
TRANSCRIPT
Yeh et al. BMC Gastroenterol (2021) 21:206 https://doi.org/10.1186/s12876-021-01801-w
CASE REPORT
Systemic lupus erythematosus complicated by Crohn’s disease with rectovaginal fistulaHeng Yeh1, Ren‑Chin Wu2, Wen‑Sy Tsai3, Chia‑Jung Kuo4,7, Ming‑Yao Su5,7, Cheng‑Tang Chiu4,7 and Puo‑Hsien Le4,6,7*
Abstract
Background: Systemic lupus erythematosus (SLE) is a multisystemic autoimmune disease, and few cases combine with Crohn’s disease. We present the first SLE patient concurrent with Crohn’s disease and rectovaginal fistula. She was successfully treated with vedolizumab and surgical intervention. Besides, she also had a rare opportunistic infection, cryptococcal pneumonia, in previous adalimumab treatment course.
Case: A 57 year‑old female had SLE in disease remission for 27 years. She suffered from progressive rectal ulcers with anal pain and bloody stool, and Crohn’s disease was diagnosed. She received adalimumab, but the lesion still progressed to a rectovaginal fistula. Besides, she suffered from an episode of cryptococcal pneumonia under adali‑mumab treatment course. Therefore, we changed the biologics to vedolizumab, and arrange a transverse colostomy for stool diversion. She had clinical remission without active inflammation, but the fistula still persisted. Then, she received a restorative proctectomy with colo‑anal anastomosis and vaginal repair. Follow‑up endoscopy showed no more rectal ulcers or fistula tracts, and contrast enema also noted no residual rectovaginal fistula.
Conclusion: When a SLE patient had unusual rectal ulcers, Crohn’s disease should be considered. Biologics combined with surgical intervention is an optimal solution for Crohn’s disease with rectovaginal fistula. Although cryptococcal pneumonia is a rare opportunistic infection in the biological treatment, we should always keep it in mind.
Keywords: Rectovaginal fistula, Crohn’s disease, Cryptococcal pneumonia, Systemic lupus erythematosus, Vedolizumab, Case report
© The Author(s) 2021. Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http:// creat iveco mmons. org/ licen ses/ by/4. 0/. The Creative Commons Public Domain Dedication waiver (http:// creat iveco mmons. org/ publi cdoma in/ zero/1. 0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
BackgroundSystemic lupus erythematosus (SLE) is an autoimmune disease affecting mostly young female adults and charac-terized by skin lesions, arthritis, hematologic disorders, multi-organ involvement and presence of autoantibod-ies [1]. The 53% patients with SLE had lupus enteritis, and 8–40% have digestive system involvement [2]. How-ever, the concurrence of SLE and Crohn disease (CD) is uncommon [3, 4].
Rectovaginal fistula (RVF) is a rare, but troublesome complication of Crohn’s disease (CD). Although some patients attained complete closure with 6 mercaptopu-rine (6-MP), tacrolimus or infliximab, more than 60% patients still required surgical repair [5–8]. Vedolizumab (VDZ) is a humanized monoclonal antibody (IgG1) to α4β7 integrin with demonstrated efficacy in the treat-ment of patients with moderate to severe inflammatory bowel disease. The exploratory analyses of data from GEMINI 2 showed beneficial effect of VDZ treatment for fistulizing Crohn’s disease (CD), but there was no statistical significance [9]. The subgroup of patients with RVF was not analyzed separately, and no other studies reported the efficacy of vedolizumab in rectovaginal fis-tula closure.
Open Access
*Correspondence: [email protected] Department of Gastroenterology and Hepatology, Chang Gung Memorial Hospital, Linkou Branch, Taoyuan, TaiwanFull list of author information is available at the end of the article

Page 2 of 6Yeh et al. BMC Gastroenterol (2021) 21:206
Although there are several opportunistic infections reported in inflammatory bowel disease (IBD), only one patient treated with prednisone, azathioprine and adali-mumab had cryptococcal pneumonia [10]. We report a SLE patient who developed CD with RVF. Besides, she experienced an episode of pulmonary cryptococcosis in previous adalimumab treatment course.
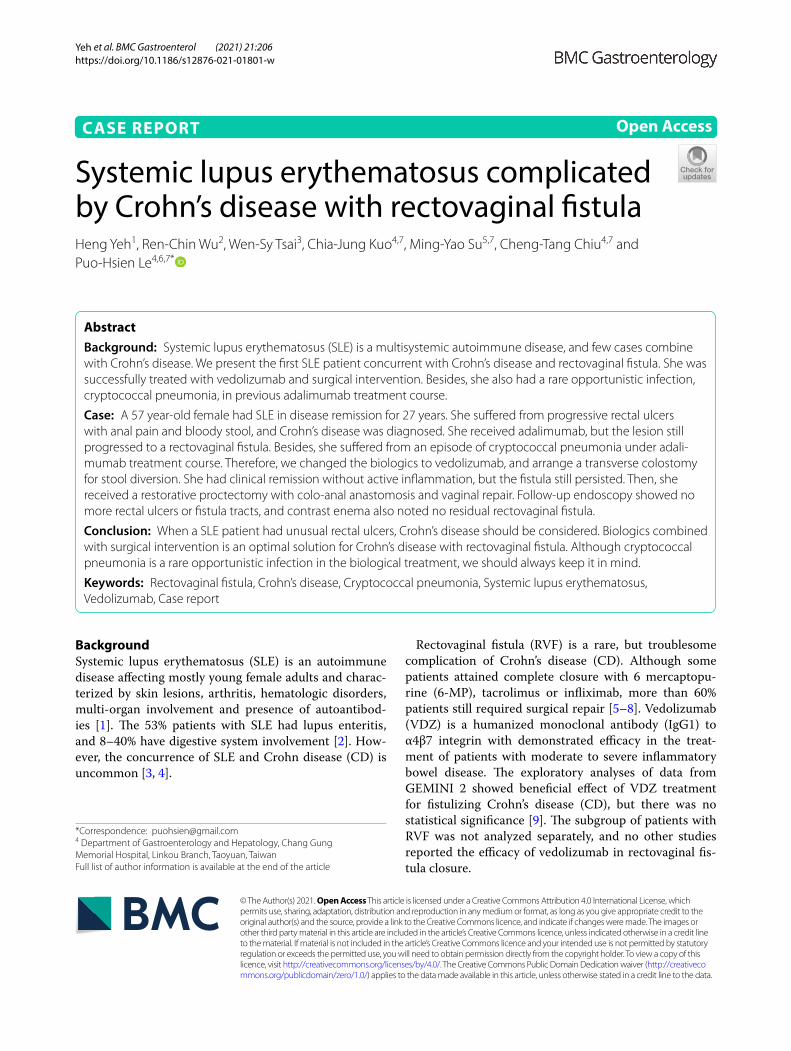
Case presentationThis 57-year-old female had SLE under methotrexate 7.5 mg/week and prednisolone 7.5 mg/day treatment with C3 level 65.00 mg/dL (Normal range 90–180 mg/dL) and C4 level 18.20 mg/dL (Normal range 10–40 mg/dL) for 27 years. She received a right total hip replace-ment due to right hip avascular necrosis on Septem-ber, 2006. She complained progressive anal pain with bloody stool for months. There was no fever, no chills, no abdominal pain, no oral or genital ulcers and negative pathergy test. Laboratory exam showed positive anti-SSA antibody (Ab) and cytomegalovirus (CMV) IgG, but neg-ative anti-SSB Ab, anti-RNP Ab, Amebic AB, CMV IgM, CMV DNA, Epstein–Barr virus (EBV) DNA, blood cul-ture, stool cultures (Salmonella, Shigella, Campylobacter, Clostridium difficile), Clostridium difficile toxin or Rota-virus. Sigmoidoscopy revealed rectal ulcers, 0.5–0.8 cm, 3–10 cm level above anal verge (Fig. 1a), and histology revealed the features of acute inflammation (lymphop-lasmacytic infiltration) and chronic inflammation (crypt branching, dropout and shortfall), which were compat-ible with inflammation bowel disease without evidence of CMV infection or vasculitis. She received hydrocortisone and mesalazine enema once daily. Bloody stool subsided and anal pain improved initially, but the condition pro-gressed after 2 weeks of treatment.
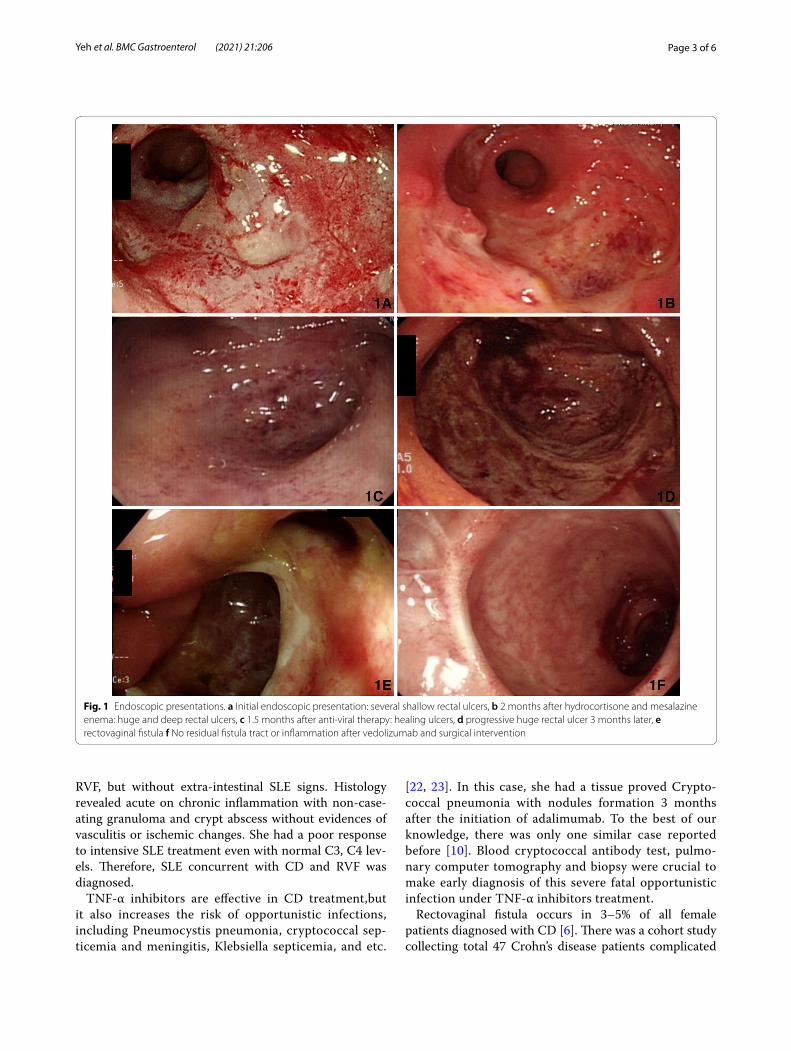
Colonoscopy showed huge and deep rectal ulcers 2 months after first endoscopic examination, and histol-ogy revealed acute on chronic inflammation with crypt abscess, granuloma and positive immunohistochemical staining for CMV (Fig. 2). Ganciclovir (200 mg IV Q12h) was prescribed for 2 weeks followed by valganciclovir (450 mg/tab 1PC BID) for another 6 weeks to treat CMV colitis and hydroxychloroquine (200 mg/tab 1PC BID) and prednisolone (10 mg daily) were given for SLE con-trol. The follow-up sigmoidoscopy 6 weeks after anti-viral treatment showed healing ulcers (Fig. 1c) and repeated immunohistochemical staining for CMV were both nega-tive. We kept valganciclovir, hydroxychloroquine and prednisolone using. However, she had recurrent pain with bloody stool, and sigmoidoscopy showed a huge progressive rectal ulcer 3 months later (Fig. 1d). Blood CMV Ag, CMV IgM, EBV Ag, Clostridial difficile toxin and rectal tissue IHC staining for CMV were all negative. Adalimumab was prescribed for Crohn’s disease.
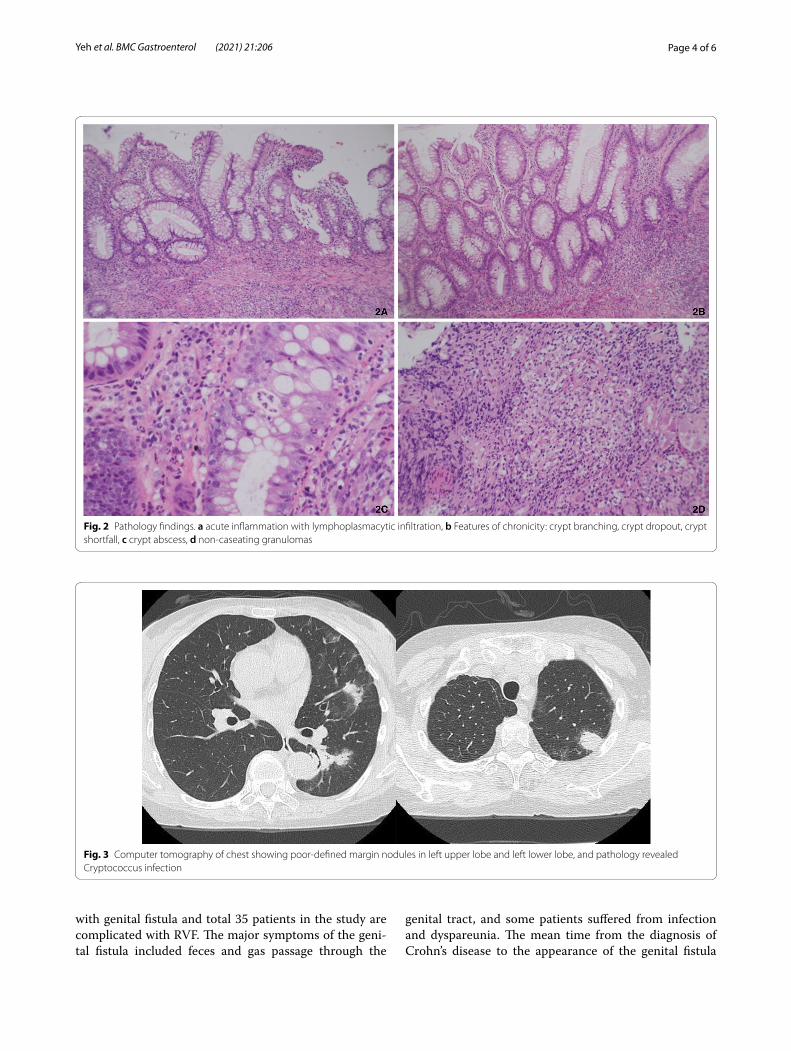
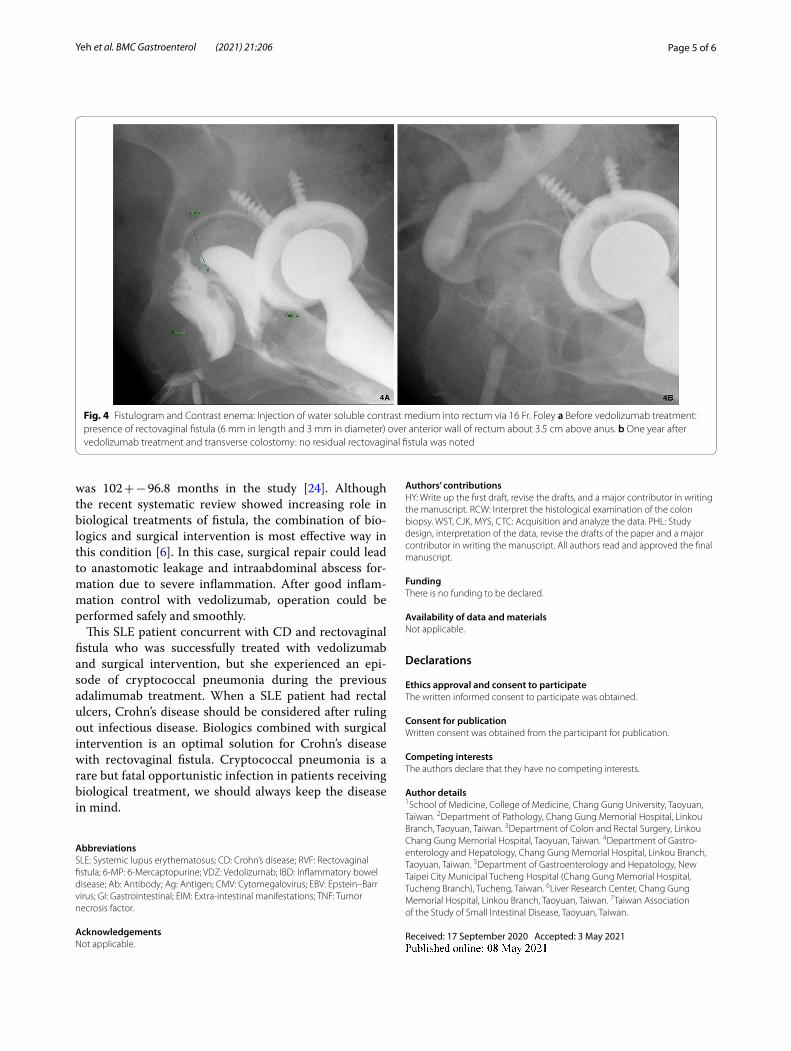
Besides, she had an episode of cryptococcal pneumonia (Fig. 3) proved by lung biopsy and cryptococcal Ag 1:64 3 months after receiving adalimumab therapy. She men-tioned the exposure history to pigeon manure because her neighbor was a pigeon fancier. Amphotericin B and flucytosine were prescribed, and symptoms improved. She also complained progressive bloody stool and noted some stool passage from vagina under adalimumab treatment course. Sigmoidoscopy (Fig. 1e), fistulogram (Fig. 4a) and MRI all confirmed the rectovaginal fistula. Then, we arranged a transverse colostomy and shift the biologics to vedolizumab. She had clinical remission 2 months later, and we kept vedolizumab using. One year later, Sigmoidoscopy revealed no inflammation, and she received a restorative proctectomy with colo-anal anas-tomosis and vaginal repair. Follow-up endoscopy showed no more rectal ulcers or fistula tracts (Fig. 1f ), and con-trast enema (Fig. 4b) also noted no residual rectovaginal fistula 10 months later.
Discussion and conclusionSLE is a multisystemic autoimmune disease with variable presentations. Gastrointestinal (GI) manifestations are noted in 50% SLE patients, including lupus enteritis, pan-creatitis and peritonitis [11, 12]. However, only few SLE patients complicated with rectal ulcers were reported, and some of them were successfully treated with intra-venous steroid, tacrolimus, cyclophosphamide and sur-gery [13–18]. Although Crohn’s disease mainly involves gastrointestinal tract, 6% patients have extraintestinal manifestations (EIM) at diagnosis, and 25–47% patients experience EIM in lifetime [19–21]. The most common EIM include arthritis, skin involvement, and ocular man-ifestations, etc. Besides, it sometimes combined with other autoimmune diseases. It’s not easy to differentiate between SLE with GI involvement and Crohn’s disease. There are still some hints to make the differential diagno-sis according to previous study results [3, 4]. Compared to SLE, CD presents more frequently as diarrhea, hema-tochezia and perianal lesions. In the perspective of image studies, lupus enteritis is characterized with segmental bowel dilatation and air fluid level, fingerprint sign and false obstruction. CD has comb sign and skipped lesions over the whole alimentary tract. When a SLE patient has GI symptoms, but the clinical presentations and image features are more suggestive of CD, we should arrange endoscopic exam with biopsy to confirm the diagnosis. If the colonoscopy shows skipped, longitudinal ulcers with cobble stone like mucosal changes, CD is the pre-ferred diagnosis. Furthermore, non-caseating granuloma and crypt abscess are more specific for CD, and vascu-litis or vascular ischemic changes are more common in SLE. In this patient, she had hematochezia, rectal ulcers,
Page 3 of 6Yeh et al. BMC Gastroenterol (2021) 21:206
RVF, but without extra-intestinal SLE signs. Histology revealed acute on chronic inflammation with non-case-ating granuloma and crypt abscess without evidences of vasculitis or ischemic changes. She had a poor response to intensive SLE treatment even with normal C3, C4 lev-els. Therefore, SLE concurrent with CD and RVF was diagnosed.
TNF-α inhibitors are effective in CD treatment,but it also increases the risk of opportunistic infections, including Pneumocystis pneumonia, cryptococcal sep-ticemia and meningitis, Klebsiella septicemia, and etc.
[22, 23]. In this case, she had a tissue proved Crypto-coccal pneumonia with nodules formation 3 months after the initiation of adalimumab. To the best of our knowledge, there was only one similar case reported before [10]. Blood cryptococcal antibody test, pulmo-nary computer tomography and biopsy were crucial to make early diagnosis of this severe fatal opportunistic infection under TNF-α inhibitors treatment.
Rectovaginal fistula occurs in 3–5% of all female patients diagnosed with CD [6]. There was a cohort study collecting total 47 Crohn’s disease patients complicated
Fig. 1 Endoscopic presentations. a Initial endoscopic presentation: several shallow rectal ulcers, b 2 months after hydrocortisone and mesalazine enema: huge and deep rectal ulcers, c 1.5 months after anti‑viral therapy: healing ulcers, d progressive huge rectal ulcer 3 months later, e rectovaginal fistula f No residual fistula tract or inflammation after vedolizumab and surgical intervention
Page 4 of 6Yeh et al. BMC Gastroenterol (2021) 21:206
with genital fistula and total 35 patients in the study are complicated with RVF. The major symptoms of the geni-tal fistula included feces and gas passage through the
genital tract, and some patients suffered from infection and dyspareunia. The mean time from the diagnosis of Crohn’s disease to the appearance of the genital fistula
Fig. 2 Pathology findings. a acute inflammation with lymphoplasmacytic infiltration, b Features of chronicity: crypt branching, crypt dropout, crypt shortfall, c crypt abscess, d non‑caseating granulomas
Fig. 3 Computer tomography of chest showing poor‑defined margin nodules in left upper lobe and left lower lobe, and pathology revealed Cryptococcus infection
Page 5 of 6Yeh et al. BMC Gastroenterol (2021) 21:206
was 102 + − 96.8 months in the study [24]. Although the recent systematic review showed increasing role in biological treatments of fistula, the combination of bio-logics and surgical intervention is most effective way in this condition [6]. In this case, surgical repair could lead to anastomotic leakage and intraabdominal abscess for-mation due to severe inflammation. After good inflam-mation control with vedolizumab, operation could be performed safely and smoothly.
This SLE patient concurrent with CD and rectovaginal fistula who was successfully treated with vedolizumab and surgical intervention, but she experienced an epi-sode of cryptococcal pneumonia during the previous adalimumab treatment. When a SLE patient had rectal ulcers, Crohn’s disease should be considered after ruling out infectious disease. Biologics combined with surgical intervention is an optimal solution for Crohn’s disease with rectovaginal fistula. Cryptococcal pneumonia is a rare but fatal opportunistic infection in patients receiving biological treatment, we should always keep the disease in mind.
AbbreviationsSLE: Systemic lupus erythematosus; CD: Crohn’s disease; RVF: Rectovaginal fistula; 6‑MP: 6‑Mercaptopurine; VDZ: Vedolizumab; IBD: Inflammatory bowel disease; Ab: Antibody; Ag: Antigen; CMV: Cytomegalovirus; EBV: Epstein–Barr virus; GI: Gastrointestinal; EIM: Extra‑intestinal manifestations; TNF: Tumor necrosis factor.
AcknowledgementsNot applicable.
Authors’ contributionsHY: Write up the first draft, revise the drafts, and a major contributor in writing the manuscript. RCW: Interpret the histological examination of the colon biopsy. WST, CJK, MYS, CTC: Acquisition and analyze the data. PHL: Study design, interpretation of the data, revise the drafts of the paper and a major contributor in writing the manuscript. All authors read and approved the final manuscript.
FundingThere is no funding to be declared.
Availability of data and materialsNot applicable.
Declarations
Ethics approval and consent to participateThe written informed consent to participate was obtained.
Consent for publicationWritten consent was obtained from the participant for publication.
Competing interestsThe authors declare that they have no competing interests.
Author details1 School of Medicine, College of Medicine, Chang Gung University, Taoyuan, Taiwan. 2 Department of Pathology, Chang Gung Memorial Hospital, Linkou Branch, Taoyuan, Taiwan. 3 Department of Colon and Rectal Surgery, Linkou Chang Gung Memorial Hospital, Taoyuan, Taiwan. 4 Department of Gastro‑enterology and Hepatology, Chang Gung Memorial Hospital, Linkou Branch, Taoyuan, Taiwan. 5 Department of Gastroenterology and Hepatology, New Taipei City Municipal Tucheng Hospital (Chang Gung Memorial Hospital, Tucheng Branch), Tucheng, Taiwan. 6 Liver Research Center, Chang Gung Memorial Hospital, Linkou Branch, Taoyuan, Taiwan. 7 Taiwan Association of the Study of Small Intestinal Disease, Taoyuan, Taiwan.
Received: 17 September 2020 Accepted: 3 May 2021
Fig. 4 Fistulogram and Contrast enema: Injection of water soluble contrast medium into rectum via 16 Fr. Foley a Before vedolizumab treatment: presence of rectovaginal fistula (6 mm in length and 3 mm in diameter) over anterior wall of rectum about 3.5 cm above anus. b One year after vedolizumab treatment and transverse colostomy: no residual rectovaginal fistula was noted
Page 6 of 6Yeh et al. BMC Gastroenterol (2021) 21:206
• fast, convenient online submission
•
thorough peer review by experienced researchers in your field
• rapid publication on acceptance
• support for research data, including large and complex data types
•
gold Open Access which fosters wider collaboration and increased citations
maximum visibility for your research: over 100M website views per year •
At BMC, research is always in progress.
Learn more biomedcentral.com/submissions
Ready to submit your researchReady to submit your research ? Choose BMC and benefit from: ? Choose BMC and benefit from:
References 1. Manson JJ, Rahman A. Systemic lupus erythematosus. Orphanet J Rare
Dis. 2006;1:6. 2. Katsanos KH, Tsianos VE, Tsianos EV. Intolerance of folic acid in a patient
receiving methotrexate for Crohn’s disease. J Crohns Colitis. 2012;6(9):960. 3. Jin X, Wang G, Xu X, Bai Y, An R, Jiang D. Coexistence of Crohn’s disease
and systemic lupus erythematosus: a case report and literature review. Eur J Gastroenterol Hepatol. 2020;32(9):1256–62.
4. Yamashita H, Ueda Y, Kawaguchi H, Suzuki A, Takahashi Y, Kaneko H, et al. Systemic lupus erythematosus complicated by Crohn’s disease: a case report and literature review. BMC Gastroenterol. 2012;12:174.
5. Korelitz BI, Present DH. Favorable effect of 6‑mercaptopurine on fistulae of Crohn’s disease. Dig Dis Sci. 1985;30(1):58–64.
6. Kaimakliotis P, Simillis C, Harbord M, Kontovounisios C, Rasheed S, Tekkis PP. A systematic review assessing medical treatment for rectovagi‑nal and enterovesical fistulae in Crohn’s disease. J Clin Gastroenterol. 2016;50(9):714–21.
7. Sands BE, Blank MA, Patel K, van Deventer SJ. Long‑term treatment of rec‑tovaginal fistulas in Crohn’s disease: response to infliximab in the ACCENT II Study. Clin Gastroenterol Hepatol. 2004;2(10):912–20.
8. González‑Lama Y, Abreu L, Vera MI, Pastrana M, Tabernero S, Revilla J, et al. Long‑term oral tacrolimus therapy in refractory to infliximab fistulizing Crohn’s disease: a pilot study. Inflamm Bowel Dis. 2005;11(1):8–15.
9. Feagan BG, Schwartz D, Danese S, Rubin DT, Lissoos TW, Xu J, et al. Effi‑cacy of vedolizumab in fistulising crohn’s disease: exploratory analyses of data from GEMINI 2. J Crohns Colitis. 2018;12(5):621–6.
10. Fraison JB, Guilpain P, Schiffmann A, Veyrac M, Le Moing V, Rispail P, et al. Pulmonary cryptococcosis in a patient with Crohn’s disease treated with prednisone, azathioprine and adalimumab: exposure to chicken manure as a source of contamination. J Crohns Colitis. 2013;7(1):e11–4.
11. Bailey M, Chapin W, Licht H, Reynolds JC. The effects of vasculitis on the gastrointestinal tract and liver. Gastroenterol Clin N Am. 1998;27(4):747–82.
12. Sultan SM, Ioannou Y, Isenberg DA. A review of gastrointestinal manifestations of systemic lupus erythematosus. Rheumatology (Oxf ). 1999;38(10):917–32.
13. Sohn KC, Heo WG, Chu MS, Kim EJ, Chung JH, Choi SC, et al. Rectal ulcer developed in systemic lupus erythematosus without ischemic colitis. Korean J Gastroenterol. 2019;73(5):299–302.
14. Kaieda S, Kobayashi T, Moroki M, Honda S, Yuge K, Kawano H, et al. Successful treatment of rectal ulcers in a patient with systemic lupus erythematosus using corticosteroids and tacrolimus. Mod Rheumatol. 2014;24(2):357–60.
15. Yau AH, Chu K, Yang HM, Ko HH. Rectal ulcers induced by systemic lupus erythematosus. BMJ Case Rep. 2014;bcr2014205776. https:// doi. org/ 10. 1136/ bcr‑ 2014‑ 205776.
16. Teramoto J, Takahashi Y, Katsuki S, Sato T, Sakamaki S, Kobayashi D, et al. Systemic lupus erythematosus with a giant rectal ulcer and perforation. Intern Med. 1999;38(8):643–9.
17. Yuasa S, Suwa A, Hirakata M, Hibi N, Iwao Y, Koizumi K, et al. A case of systemic lupus erythematosus presenting with rectal ulcers as the initial clinical manifestation of disease. Clin Exp Rheumatol. 2002;20(3):407–10.
18. Wang Z, Wu C, Ruan F, Li Z, Peng X, Wang P. A case of systemic lupus erythematosus with rectal necrosis. Lupus. 2020;29(3):334–9.
19. Bernstein CN, Blanchard JF, Rawsthorne P, Yu N. The prevalence of extraintestinal diseases in inflammatory bowel disease: a population‑based study. Am J Gastroenterol. 2001;96(4):1116–22.
20. Vavricka SR, Schoepfer A, Scharl M, Lakatos PL, Navarini A, Rogler G. Extraintestinal manifestations of inflammatory bowel disease. Inflamm Bowel Dis. 2015;21(8):1982–92.
21. Bernstein CN, Wajda A, Blanchard JF. The clustering of other chronic inflammatory diseases in inflammatory bowel disease: a population‑based study. Gastroenterology. 2005;129(3):827–36.
22. Murdaca G, Negrini S, Pellecchio M, Greco M, Schiavi C, Giusti F, et al. Update upon the infection risk in patients receiving TNF alpha inhibitors. Expert Opin Drug Saf. 2019;18(3):219–29.
23. Lee WS, Azmi N, Ng RT, Ong SY, Ponnampalavanar SS, Mahadeva S, et al. Fatal infections in older patients with inflammatory bowel disease on anti‑tumor necrosis factor therapy. Intest Res. 2017;15(4):524–8.
24. de la Poza G, Lopez‑Sanroman A, Taxonera C, Marin‑Jimenez I, Gisbert JP, Bermejo F, et al. Genital fistulas in female Crohn’s disease patients: clinical characteristics and response to therapy. J Crohns Colitis. 2012;6(3):276–80.
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims in pub‑lished maps and institutional affiliations.