systemic - thoraxthorax.bmj.com/content/thoraxjnl/48/10/967.full.pdf · and budesonide (given by...
TRANSCRIPT

Thorax 1993;48:967-973
Systemic effects of high dose inhaled steroids:comparison of beclomethasone dipropionate andbudesonide in healthy subjects
Peter H Brown, Simon P Matusiewicz, Catherine Shearing, Laila Tibi,Andrew P Greening, Graham K Crompton
Respiratory MedicineUnitP H BrownS P MatusiewiczA P GreeningG K CromptonDepartments ofClinical ChemistryC ShearingWestern GeneralHospital, Crewe RoadSouth, EdinburghEH4 2XURoyal Infirmary,EdinburghL TibiReprint request to:Dr P H Brown
Received 12 October 1992Returned to authors2 February 1993Revised version received23 April 1993
Accepted 11 May 1993
AbstractBackground-Systemic absorption ofinhaled corticosteroids may adverselyinfluence the function of the hypothal-amo-pituitary-adrenal axis, bone metab-olism, and circulating leucocytes. Thesechanges can be used to assess the safetyof different types and modes of adminis-tration of these drugs.Methods-The study was a randomised,double dummy, crossover design withnine healthy adults. It compared theeffects of beclomethasone dipropionateand budesonide (given by metered doseaerosols with and without their respec-tive large volume spacers (Volumatic andNebuhaler) attached) on serum cortisol,24 hour urinary free cortisol, and plasmaosteocalcin concentrations, and circulat-ing neutrophils and lymphocytes. Sub-jects inhaled the drug (1 mg) andmatching placebo at 0900 and 2200 hourson each of six study days. Blood sampleswere taken hourly for six hours after themorning dose and at the end of the studyperiod.Results-All results were within the ref-erence ranges. Both drugs caused similarreductions in serum cortisol four to sixhours after inhalation. These changeswere not affected by the use of a largespacer and did not persist at 24 hours.Use of spacers tended to increase thehaematological effects of the steroids.Beclomethasone dipropionate inhaledthrough a Volumatic provoked a rise incirculating neutrophils compared withplacebo although lymphocyte numberswere unaffected. Budesonide did notinfluence neutrophil numbers but didreduce circulating lymphocytes, num-bers of which were further reduced whenthe Nebuhaler was used. There were nosignificant changes in plasma osteocalcinconcentration or 24 hour urinary freecortisol excretion with budesonide, withor without a spacer. Beclomethasonedipropionate inhaled without a spacerreduced urinary cortisol and plasmaosteocalcin at 24 hours; however, use ofthe Volumatic protected against theseeffects.Conclusions-Attaching a Volumaticreduces the systemic effects of 2 mgaerosol beclomethasone dipropionate on
the hypothalamo-pituitary-adrenal axisand circulating osteocalcin concentra-tions. This study did not establishwhether the Nebuhaler reduces the sys-temic effects of budesonide. When largespacers are used, 2 mg per day ofbeclomethasone dipropionate and budes-onide seem to be equivalent in terms ofunwanted effects.
(Thorax 1993;48:967-973)
Systemic absorption of inhaled cortico-steroids such as beclomethasone dipropionateor budesonide may influence the activity ofthe hypothalamo-pituitary-adrenal axis, bone,carbohydrate and lipid metabolism, and cir-culating leucocytes.' Such changes can beused as markers of unwanted drug effects. Itis not clear which of these markers is mostsensitive to inhaled corticosteroids, or howchanges relate to the risk of major adversecorticosteroid effects such as osteoporosis,myopathy, and cataracts.
In an early study in adult volunteers,2inhaled beclomethasone dipropionate at adose of 500 ,ug/day caused a rise in circulatingneutrophils and a fall in lymphocyte numberssuggesting that a change in peripheral bloodleucocytes was a sensitive marker of systemiceffects. Tests of hypothalamo-pituitary-adrenal function, usually measurement ofmorning plasma cortisol concentrations, havelong been the standard method of assessingsystemic activity. Recently, there has beenmuch interest in indices of bone formationand resorption. Circulating concentrations ofosteocalcin, a 49 amino acid protein pro-duced by osteoblasts, seem to correlate wellwith bone formation.'-5 Concentrations showa circadian variation but, by contrast withcortisol, are maximal at night and low aroundnoon." Systemic corticosteroids suppressserum osteocalcin9-" and recent studies showthat inhaled corticosteroids may also have thiseffect.8 12-17
In the treatment of asthma beclomethasonedipropionate and budesonide seem to beequipotent in therapeutic efficacy when simi-lar doses are given. Some studies, however,have reported that when doses >800 ug/dayare used, budesonide may have fewer sys-temic effects.18-22 Most of these studies com-pared the drugs given via the conventional
967
on 14 July 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.48.10.967 on 1 October 1993. D
ownloaded from

Brown, Matusiewicz, Shearing, Tibi, Greening, Crompton
metered dose aerosol but current UnitedKingdom recommendations are that highdose inhaled steroid treatment should begiven with a large spacer.23 Although there isevidence that hypothalamo-pituitary-adrenalsuppression from high doses of beclometha-sone dipropionate is reduced by a 750 mlspacer (Volumatic),'s'6 it has been suggestedthat the spacer (Nebuhaler) increases thehypothalamo-pituitary-adrenal suppressionresulting from budesonide."
This study was designed to compare theshort term systemic effects of beclomethasonedipropionate and budesonide given bymetered dose aerosols with and without theirrespective spacers (Volumatic and Nebuhaler).
MethodsSTUDY PROTOCOLNine healthy subjects (mean age 32-7 (range23-56) years, five men) selected from hospi-tal medical and nursing staff participated inthe study, which was of randomised doubleblind double dummy crossover design. Nonehad taken corticosteroids previously. Eachwas studied on six separate days; the washoutperiod between each study day was a mini-mum of three days. On two days, subjectsinhaled beclomethasone dipropionate from ametered dose aerosol with or without aVolumatic attached, matching placebo beingtaken by the alternative route. On anothertwo days, budesonide was inhaled with orwithout a Nebuhaler and matching placebotaken by the other route. Double placeboinhalers were used on the other days. Twodouble placebo days were necessary as it wasimpractical to blind investigators and subjectsas to which spacer was being used and sub-jects had to actuate the budesonide canistermore often than the beclomethasone dipropi-onate canister to take the same total dose byweight.A total daily dose of 2 mg beclomethasone
dipropionate or budesonide (1 mg in themorning and evening) was chosen as thisdose and dosing frequency is widely used andis the maximum recommended.23 Canisters ofbeclomethasone dipropionate dispensed 0-25mg per puff and subjects therefore used activeand placebo inhalers in doses of four puffstwice daily. Canisters of budesonide dis-pensed 0-2 mg per puff and therefore duringthe three budesonide study days, subjectstook five puffs twice daily from active andplacebo inhalers. All subjects were able to usea metered dose aerosol efficiently. Whenusing the spacer, all took two inhalationsfrom the device for each actuation of theaerosol and each inhalation was followed by abreath hold of five seconds. The spacer studymedication was inhaled first, immediatelyfollowed by conventional aerosol use. Mouthswere not rinsed.On each study day, subjects attended at
0830 and a cannula was sited in a forearmvein. They rested for 30 minutes, after whicha venous blood sample (10 ml) was drawn.
Following this, they took study medication,started a 24 hour collection of urine, andcontinued a normal working day. Furtherblood samples were drawn at hourly intervalsfor six hours after which the cannula wasremoved. The second dose of study medica-tion was taken at 2200 hours and the lastblood sample withdrawn at 0900 hours thefollowing day, when the urine collection wascompleted. The study received ethics com-mittee approval and all subjects gave verbalconsent.
ASSAYSBlood samples were assayed for cortisol andosteocalcin and a differential leucocyte countwas taken. Samples for cortisol assay wereallowed to clot and the serum was separatedand stored at -20°C until analysis. Serumcortisol and the 24 hour urinary excretion offree cortisol were measured by the same com-mercial radioimmunoassay (Amerlex, KodakClinical Diagnostics Ltd, Amersham, UK).The interassay coefficient of variation (CV)was 3*7% at 342 nmol/l and 3-2% at 760nmol/l. In our laboratory, the reference rangefor 0900 cortisol is 190-550 nmol/l and forurinary free cortisol excretion 80-450nmol/24 hours. Differential leucocyte countswere performed by Coulter counter analysis.The reference range for neutrophil count is2-7-5 x 109/1 and for lymphocytes 1-5-4x 109/1. Samples for osteocalcin assay werecollected into heparinised containers, cen-trifuged immediately, and the plasma storedat - 20°C. Osteocalcin was analysed by an inhouse radioimmunoassay with an antibodyraised in rabbits to purified bovine osteocal-cin (intra-assay CV 5%; interassay CV 12%;reference range 2-12 pg/l). Differential leuco-cyte counts and urine samples were analysedimmediately after collection. Blood samplesfor cortisol and osteocalcin assays werestored until completion of the study andsamples from an individual subject (48 intotal) were analysed in the same batch.
STATISTICAL ANALYSISAlthough the study was randomised and dou-ble blind with respect to each drug, the differ-ences between the large spacers and the doseper actuation of the aerosols meant that directcomparison between beclomethasone dipro-pionate and budesonide could not be com-pletely blinded without greatly complicatingthe study design. The principal comparisonswere therefore between each drug and modeof inhalation and their respective placebos.The influence of drug and use of spacer onthe various circulating markers during thefirst six hours after inhalation was assessed byarea under the curve analysis with statisticalsignificance determined by paired t tests.These were also used to compare the 24 hourmeasurements between groups. Bonferronicorrections were used to adjust for multiplecomparisons. Changes in 24 hour urinary freecortisol excretion were also analysed withpaired t tests. Statistical significance wastaken at the 5% level.
968
on 14 July 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.48.10.967 on 1 October 1993. D
ownloaded from
Systemic effects of high dose inhaled steroids: comparison of beclomethasone dipropionate and budesonide in healthy subjects
700 -
600 -
500 -
400 -
300 -
200 -
100 -
0 +1 +2 +3 +4 +5 +6
Time (hours)
0-+24
B
0 +1 +2 +3 +4 +5 +6
Time (hours)
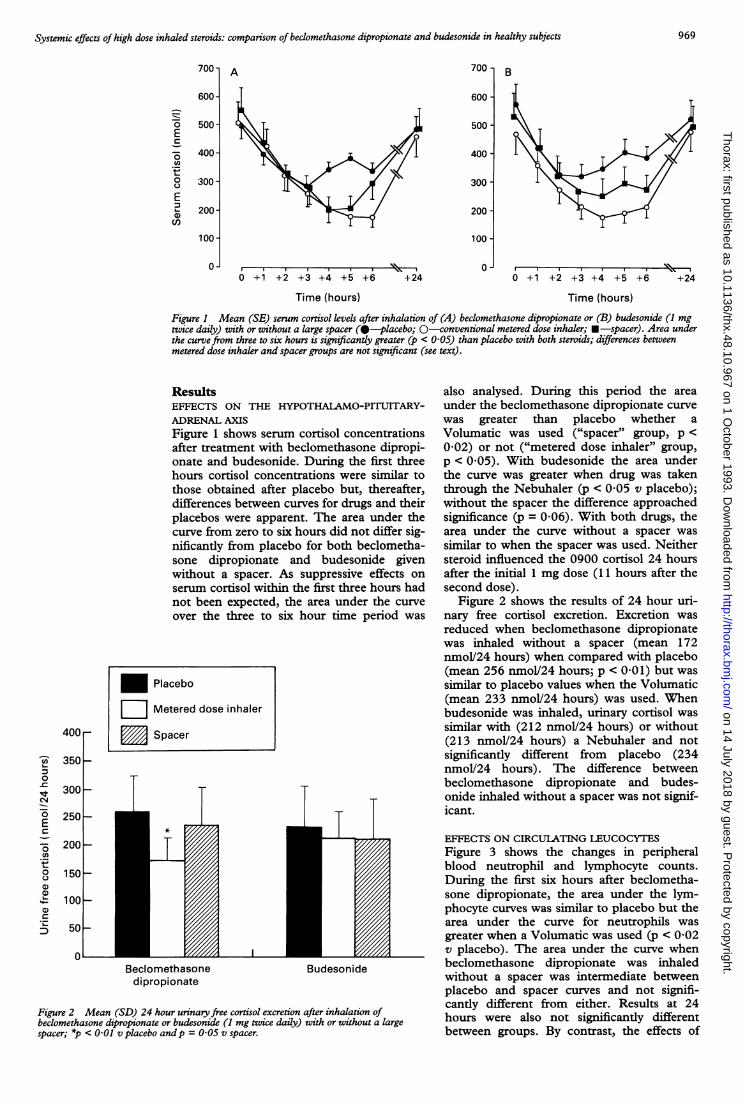
Figure 1 Mean (SE) serum cortisol levels after inhalation of (A) beclomethasone dipropionate or (B) budesonide (1 mgtwice daily) with or without a large spacer (0-placebo; 0-conventional metered dose inhaler; U-spacer). Area underthe curvefrom three to six hours is significantly greater (p < 0-05) than placebo with both steroids; differences betweenmetered dose inhaler and spacer groups are not significant (see text).
ResultsEFFECTS ON THE HYPOTHALAMO-PITUITARY-ADRENAL AXISFigure 1 shows serum cortisol concentrationsafter treatment with beclomethasone dipropi-onate and budesonide. During the first threehours cortisol concentrations were similar tothose obtained after placebo but, thereafter,differences between curves for drugs and theirplacebos were apparent. The area under thecurve from zero to six hours did not differ sig-nificantly from placebo for both beclometha-sone dipropionate and budesonide givenwithout a spacer. As suppressive effects onserum cortisol within the first three hours hadnot been expected, the area under the curveover the three to six hour time period was
Beclomethasone Budesonidedipropionate
Figure 2 Mean (SD) 24 hour urinary free cortisol excretion after inhalation ofbeclomethasone dipropionate or budesonide (1 mg twice daily) with or without a largespacer; *p < 0-01 v placebo andp = 0-05 v spacer.
also analysed. During this period the areaunder the beclomethasone dipropionate curvewas greater than placebo whether aVolumatic was used ("spacer" group, p <0-02) or not ("metered dose inhaler" group,p < 0-05). With budesonide the area underthe curve was greater when drug was takenthrough the Nebuhaler (p < 0-05 v placebo);without the spacer the difference approachedsignificance (p = 0-06). With both drugs, thearea under the curve without a spacer wassimilar to when the spacer was used. Neithersteroid influenced the 0900 cortisol 24 hoursafter the initial 1 mg dose (11 hours after thesecond dose).
Figure 2 shows the results of 24 hour uri-nary free cortisol excretion. Excretion wasreduced when beclomethasone dipropionatewas inhaled without a spacer (mean 172nmolV24 hours) when compared with placebo(mean 256 nmol/24 hours; p < 0-01) but wassimilar to placebo values when the Volumatic(mean 233 nmol/24 hours) was used. Whenbudesonide was inhaled, urinary cortisol wassimilar with (212 nmol/24 hours) or without(213 nmol/24 hours) a Nebuhaler and notsignificantly different from placebo (234nmol/24 hours). The difference betweenbeclomethasone dipropionate and budes-onide inhaled without a spacer was not signif-icant.
EFFECTS ON CIRCULATING LEUCOCYTESFigure 3 shows the changes in peripheralblood neutrophil and lymphocyte counts.During the first six hours after beclometha-sone dipropionate, the area under the lym-phocyte curves was similar to placebo but thearea under the curve for neutrophils wasgreater when a Volumatic was used (p < 0-02v placebo). The area under the curve whenbeclomethasone dipropionate was inhaledwithout a spacer was intermediate betweenplacebo and spacer curves and not signifi-cantly different from either. Results at 24hours were also not significantly differentbetween groups. By contrast, the effects of
A700-
600-
0Es
In
0
EI._a)
500-
400*
300
200
100
0+24
400r-
U Placebo
W Metered dose inhaler
Spacer
350 -
300H
250 HT
in0
01E
cn.,
0
a)
200H
150K
100 F-
501-
01
NNI II N.
969 on 14 July 2018 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.48.10.967 on 1 O
ctober 1993. Dow
nloaded from
Brown, Matusiewicz, Shearing, Tibi, Greening, Crompton
6B
5
4-
3-
3-
2-
1-
A-J
0 +1 +2 +3 +4 +5 +6
Time (hours)
+24v -
+24 0 +1 +2 +3 +4 +5 +6
Time (hours)
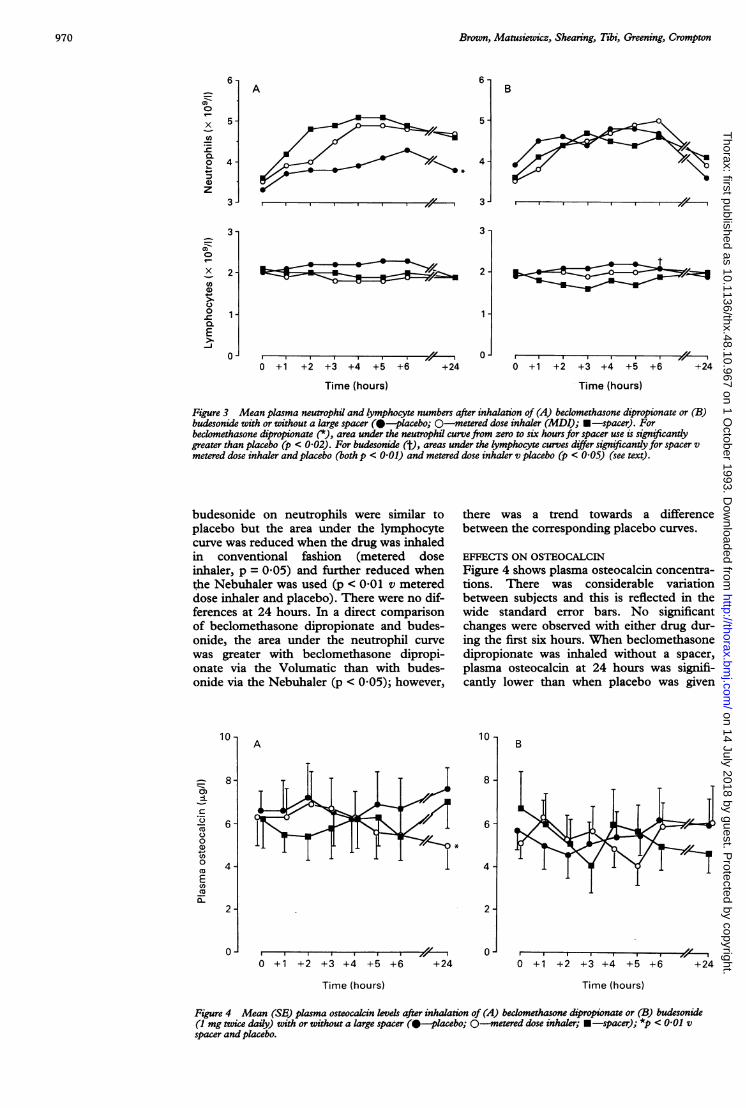
Figure 3 Mean plasma neutrophil and lymphocyte numbers after inhalation of (A) beclomethasone dipropionate or (B)budesonide with or without a large spacer (0-placebo; 0-metered dose inhaler (MDI); -spacer). Forbeclomethasone dipropionate (*), area under the neutrophil curvefrom zero to six hours for spacer use is significantlygreater than placebo (p < 0-02). For budesonide (f), areas under the lymphocyte curves differ significantly for spacer vmetered dose inhaler and placebo (both p < 0-0) and metered dose inhaler v placebo (p < 0-05) (see text).
budesonide on neutrophils were similar toplacebo but the area under the lymphocytecurve was reduced when the drug was inhaledin conventional fashion (metered doseinhaler, p = 0 05) and further reduced whenthe Nebuhaler was used (p < 0-01 v metereddose inhaler and placebo). There were no dif-ferences at 24 hours. In a direct comparisonof beclomethasone dipropionate and budes-onide, the area under the neutrophil curvewas greater with beclomethasone dipropi-onate via the Volumatic than with budes-onide via the Nebuhaler (p < 0 05); however,
there was a trend towards a differencebetween the corresponding placebo curves.
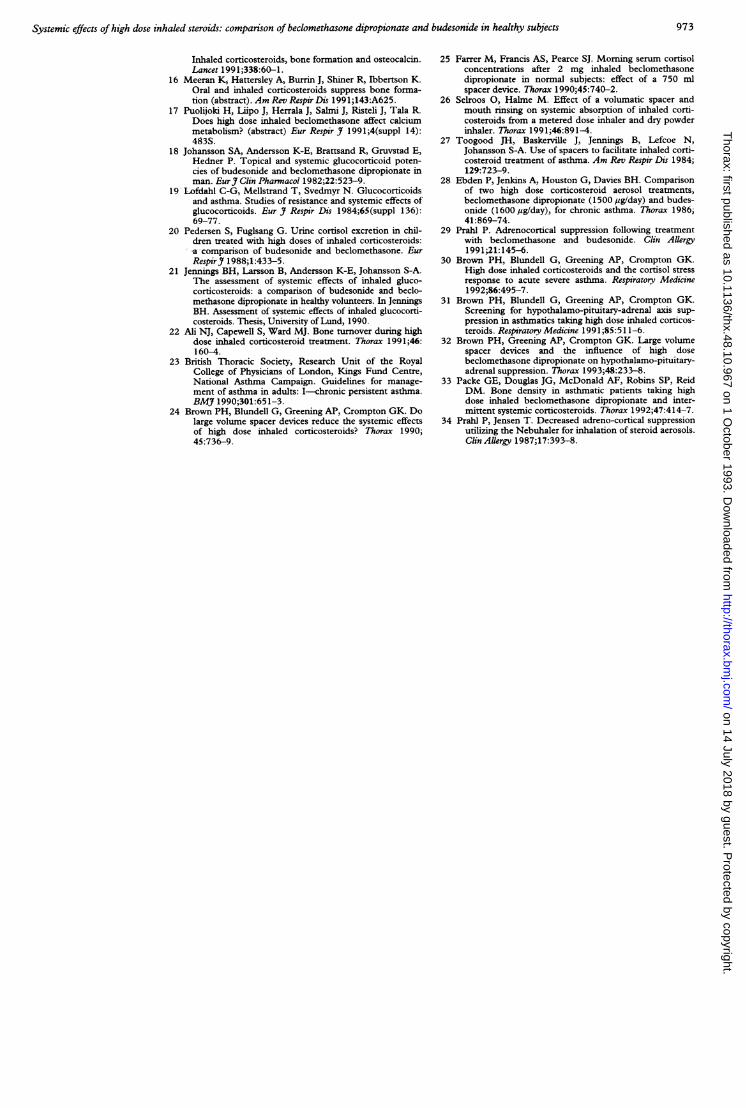
EFFECTS ON OSTEOCALCINFigure 4 shows plasma osteocalcin concentra-tions. There was considerable variationbetween subjects and this is reflected in thewide standard error bars. No significantchanges were observed with either drug dur-ing the first six hours. When beclomethasonedipropionate was inhaled without a spacer,plasma osteocalcin at 24 hours was signifi-cantly lower than when placebo was given
A
0 +1 +2 +3 +4 +5 +6
Time (hours)
+24
10 -
8-
6-
4-
2-
0-
B
0 +1 +2 +3 +4 +5 +6
Time (hours)
Figure 4 Mean (SE) plasma osteocalcin levels after inhalation of (A) beclomethasone dipropionate or (B) budesonide(I mg twice daily) with or without a large spacer ( -placebo; 0-metered dose inhaler; -spacer); *p < 0-01 v
spacer and placebo.
970
A0)0
x
._CO
0.
G1)z
6-
5-
4-
3-
0)0
x
ax
WE)
0-C
0).E
3-
2-
1-
0-
10 -
0)i
CU.0
co0)a)u)0
coEcoEL
8-
6-
4-
2
0*
+24
lor l ~~~~~~~~~~~oA}
-s-1X Zi x .g . . Jr~~~~~~~~~O-
010,
t
on 14 July 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.48.10.967 on 1 October 1993. D
ownloaded from

Systemic effects of high dose inhaled steroids: compatison of beclomethasone dipropionate and budesonide in healthy subjects
(p < 0 01) or the spacer was used (p < 0 02).By contrast budesonide did not influence 24hours osteocalcin. In a direct comparison, theeffect of beclomethasone dipropionate wasnot significantly different from that of budes-onide;
DiscussionWith increasing use of high dose inhaled cor-ticosteroid treatment, there is a need to estab-lish whether similar doses of beclomethasonedipropionate and budesonide have clinicallyimportant differences in unwanted systemiceffects. This study compared the short terminfluences of these drugs, administered bymetered dose aerosol, on the adrenal axis,plasma osteocalcin concentrations, and circu-lating leucocytes. After inhalation of 1 mg ofeach drug at 0900 hours, similar suppressiveeffects on serum cortisol concentrations wereobserved after four to six hours althoughresults were still within normal limits.Attaching a large spacer did not significantlyinfluence the degree of suppression duringthis period although examination of thecurves for beclomethasone dipropionate (fig1) suggested that serum cortisol concentra-tions were recovering at six hours when thedrug was taken through a spacer but notwhen taken in conventional fashion.Unfortunately serum cortisol was not mea-sured between six and 12 hours to establishwhether this possible protective effect wassustained. When the effects of the total doseof 2 mg on the hypothalamo-pituitary-adrenalaxis were assessed by 24 hour urinary freecortisol determination, excretion was onlymaintained when a Volumatic was used. Thisis consistent with a protective effect of thisspacer on suppression of the hypothalamo-pituitary-adrenal axis as shown in earlierstudies.2426 The 2 mg total dose of budes-onide did not significantly reduce urinarycortisol whether or not a Nebuhaler was used.The spacer was also shown to protect
against the effects of beclomethasone dipropi-onate on circulating osteocalcin. At the endof the 24 hour study period, plasma osteocal-cin concentrations were significantly lowerafter beclomethasone dipropionate inhaledwithout the spacer than when the Volumaticwas used. Budesonide with or without theNebuhaler did not significantly affect plasmaosteocalcin concentrations. When comparedwith placebo, there were also differencesbetween the systemic effects of beclometha-sone dipropionate and budesonide on circu-lating neutrophils and lymphocytes.Neutrophil counts rose after inhalation ofeither placebo, possibly due to the presenceof an indwelling cannula although an effectfrom aerosol propellants could not beexcluded. When compared with placebo,neutrophil numbers were significantly higherafter beclomethasone dipropionate wasinhaled through a Volumatic. There was noevidence for a protective effect from thespacer for this marker of systemic effect.Budesonide did not influence neutrophils but
slightly reduced circulating lymphocytes, aneffect that was significantly more pronouncedwhen the Nebuhaler was used.The difference in appearance of the large
spacers and the greater number of puffs oftrial medication on budesonide study daysmeant that direct comparison of beclometha-sone dipropionate with budesonide for anymarker of systemic effect was not completelyblinded. When beclomethasone dipropionateand budesonide were directly compared withor without spacers, however, there were nosignificant differences for any marker of sys-temic effect (apart from neutrophil numberswhen analysis may have been confounded bya trend towards a difference between placebocurves). We cannot exclude the possibilitythat differences would have been found if alarger number of subjects had been studied orchronic dosing used.The systemic effects of high doses of
beclomethasone dipropionate and budeson-ide have been compared in at least sevenstudies. In a double blind study, Johanssonet al 18 measured plasma cortisol and periph-eral white cell counts in 12 healthy adults at0800, 1000, and 1200 hours, after singledoses of 0-4, 0-8, and 3-2 mg of beclometha-sone dipropionate or budesonide had beentaken at 2200 hours the night before. Areaunder the curve analysis of the limited num-ber of plasma cortisol data points showedgreater suppression caused by beclometha-sone dipropionate at the highest dose. In anopen study, Lofdahl'9 selected 12 healthyadults who showed pronounced reductions inserum cortisol in response to 4-5 mgbeclomethasone dipropionate a day for twodays. In these subjects, 1-5 mg beclometha-sone dipropionate and 2-4 mg budesonide,both given for two days, caused similar reduc-tions (20%) in morning serum cortisol con-centrations. The increases in cortisolsuppression when these doses were doubledand trebled were also similar, suggesting thatif the same doses were given, budesonidewould have less systemic effect thanbeclomethasone dipropionate. Pedersen20reported an open crossover study in whichasthmatic children (some using spacers) weretreated with beclomethasone dipropionate orbudesonide (0-8-1-2 mg/day), each treatmentperiod lasting six weeks. Twenty four hoururinary free cortisol excretion was signifi-cantly higher during budesonide treatment.No effect of the spacer was seen. In a doubleblind study of asthmatic adults, Ebden et al28found similar reductions in morning plasmacortisol resulting from treatment with 1-5 mgbeclomethasone dipropionate and 1-6 mgbudesonide (given by a small collapsiblespacer), each for six weeks. Jennings2' com-pared the drugs at doses of 0-8 and 2-5mg/day in an open study of healthy subjects.Dose related suppression of adrenal functionand serum osteocalcin was seen with bothdrugs and effects were significantly greaterwith beclomethasone dipropionate. Twostudies have compared the drugs given bylarge spacer. Ali et al 22 measured indices of
971 on 14 July 2018 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.48.10.967 on 1 O
ctober 1993. Dow
nloaded from

Brown, Matusiewicz, Shearing, Tibi, Greening, Crompton
bone resorption (urine hydroxyproline/creati-nine ratio) and formation (serum alkalinephosphatase) in healthy men and found thatthese were adversely influenced bybeclomethasone dipropionate (2 mg/day) butnot by budesonide (1'8 mg/day). The drugswere not compared at the same dose and thenumber of data points used in the area underthe curve analysis was small. Prahl gave bothdrugs via a Nebuhaler in an open study29 andfound interindividual differences in degree ofsuppression of urinary cortisol in some chil-dren but no difference between beclometha-sone dipropionate and budesonide.
This study provides further evidence thatwhen high dose inhaled corticosteriods aregiven by metered dose aerosol without a largespacer attached, the systemic effects withbeclomethasone dipropionate are greater thanwith budesonide. The magnitude of changesin serum and urinary cortisol and plasmaosteocalcin concentrations and circulatingneutrophils was small with results remainingwithin reference ranges. This study did notexamine the effects of chronic dosing but iflong term treatment of asthmatic patientscaused changes of similar magnitude, it isunlikely that these would be clinically impor-tant. Also evident is the relative insensitivityof 0900 serum cortisol concentration as ascreening test for the systemic effects ofinhaled steroids. Changes in serum cortisolprofile, 0900 plasma osteocalcin and 24 hoururinary free cortisol were not accompanied byany change in 0900 serum cortisol. Studiesthat do not find any differences in the sys-temic effects of different doses or types ofinhaled corticosteroid should be interpretedwith caution if the sole marker of systemiceffect is the morning cortisol concentration.The relation between effects of steroids on
indices of hypothalamo-pituitary-adrenalfunction and bone metabolism and clinicallyimportant adverse effects such as osteoporo-sis, cataracts, myopathy, and risk of adrenalcrisis, is still unclear. We have not found evi-dence of a reduced cortisol stress response toacute asthma in patients taking high doseinhaled steroids30 and have suggested thatidentifying hypothalamo-pituitary-adrenalaxis suppression may be useful in predictingwhich patients are more likely to sufferadverse effects on connective tissue.3132 Proofis lacking that the frequency of these effects isincreased if subnormal hypothalamo-pitu-itary-adrenal axis function is present. There isconsiderable concern that long term use ofhigh dose inhaled steroids might cause osteo-porosis but if systemic absorption of aninhaled steroid causes only minor reductionin endogenous steroid production, it isunlikely that the net result will be increasedsteroid effects on bone. The value of markersof bone metabolism such as circulating osteo-calcin has yet to be established: a recentcross sectional study did not find reducedconcentrations in asthmatic patients withreduced bone density." Longitudinal studiesof bone density with parallel measurements ofhypothalamo-pituitary-adrenal function and
bone biochemistry should determine whichtest is most useful in predicting a high risk ofosteoporosis; such studies have yet to bereported.
This study found that the Volumatic pro-tects against systemic effects of high doseaerosol beclomethasone dipropionate on thehypothalamo-pituitary-adrenal axis and alsoprovides some evidence of protection againstbone effects. We did not establish whetherthe Nebuhaler affords similar protectionagainst the systemic effects of budesonide.We studied healthy subjects and it may beargued that systemic absorption of an inhaledsteroid might be increased across an inflamedasthmatic airway. Reports of a similar benefi-cial effect from spacer use in adults2426 andchildren34 with asthma suggest that this doesnot occur. When large spacers are used, cur-rently recommended maximum doses ofbeclomethasone dipropionate and budes-onide seem to have equivalent systemiceffects.
We thank Dr Mike Mackie and the staff of the haematologylaboratory, Western General Hospital, for performing the dif-ferential leucocyte counts and Dr Gillian Blundell,Department of Clinical Chemistry, Western General Hospital,for her support. We also thank Dorothy McArthur for treat-ment coding, Dr Rob Elton, University of Edinburgh, foradvice regarding statistical analysis, and our colleagues (CS,FB, KL, CMcM, CA) for their enthusiastic participation.
1 Geddes DM. Inhaled corticosteroids: benefits and risks.Thorax 1992;47:404-7.
2 Harris DM. Clinical pharmacology of beclomethasonedipropionate. In Mygind N, Clark TJH, eds. Topicalsteroid treatment for asthma and rhinitis. London: BailliereTindall, 1980:34-47.
3 Brown JP, Delmas PD, Malaval L, Edouard C, ChapuyMC, Meunier PJ. Serum bone Gla-protein: a specificmarker for bone formation in postmenopausal osteo-porosis. Lancet 1984;i:1091-3.
4 Delmas PD, Malaval L, Arlot ME, Meunier PJ. Serumbone Gla-protein compared to bone histomorphometryin endocrine disease. Bone 1985;6:339-41.
5 Garcia-Carrasco M, Grason M, Vernejoul MC de, DenneMA, Miravet L. Osteocalcin and bone histomorpho-metric parameters in adults without bone disease. CalcifTissue Int 1988;42:13-7.
6 Gundberg CM, Markowitz ME, Mizruchi M, Rosen JF.Osteocalcin in human serum: a circadian rhythm. J ClinEndocrinol Metab 1985;60:736-9.
7 Nielsen HK, Laurberg P, Brixen K, Mosekilde L.Relations between diurnal variations in serum osteocal-cin, cortisol, parathyroid hormone and ionised calciumin normal individuals. Acta Endocrinol 1991;124:391-8.
8 Pouw EM, Prummel MF, Oosting H, Roos CM, EndertE. Beclomethasone inhalation decreases serum osteocal-cin concentrations. BMJ 1991;302:627-8.
9 Reid IR, Chapman GE, Fraser TRC, Davies AD, SurusAS, Meyer J, Huq NL, Ibbertson HK. Low serumosteocalcin levels in glucocorticoid-treated asthmatics.GClin Endocrinol Metab 1986;62:379-83.
10 Peretz A, Praet J-P, Bosson D, Rozenberg S, Bourdoux P.Serum osteocalcin in the assessment of corticosteroid-induced osteoporosis. Effect of long and short term cor-ticosteroid treatment. J Rheumatol 1989;16:363-7.
11 Prummel MF, Wiersinga WM, Lips P, Sanders GTB,Sauerwein HP. The course of biochemical parametersof bone turnover during treatment with corticosteroids.J Clin Endocrinol Metab 1991;72:382-5.
12 Jennings BH, Andersson K-E, Johansson SA. Assessmentof systemic effects of inhaled glucocorticosteroids: com-parison of the effects of inhaled budesonide and oralprednisolone on adrenal function and markers of boneturnover. Eury Clin Pharmacol 1991;40:77-82.
13 Toogood JH, Jennings B, Hodsman AB, Baskerville J,Fraher U. Effects of dose and dosing schedule ofinhaled budesonide on bone turnover. J AUlergy ClinImmunol 1991;88:572-80.
14 Hodsman AB, Toogood JH, Jennings B, Fraher U,Baskerville JC. Differential effects of inhaled bude-sonide and oral prednisolone on serum osteocalcin.J Clin Endocrinol Metab 1991;72:530-40.
15 Teelucksingh S, Padfield PL, Tibi L, Gough KJ, Holt PR.
972 on 14 July 2018 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.48.10.967 on 1 O
ctober 1993. Dow
nloaded from
Systemic effects of high dose inhaled steroids: comparison of beclomethasone dipropionate and budesonide in healthy subjects
Inhaled corticosteroids, bone formation and osteocalcin.Lancet 1991;338:60-1.
16 Meeran K, Hattersley A, Burrin J, Shiner R, Ibbertson K.Oral and inhaled corticosteroids suppress bone forma-tion (abstract). Am Rev Respir Dis 1991;143:A625.
17 Puolijoki H, Liipo J, Herrala J, Salmi J, Risteli J, Tala R.Does high dose inhaled beclomethasone affect calciummetabolism? (abstract) Eur Respir J 199 1;4(suppl 14):483S.
18 Johansson SA, Andersson K-E, Brattsand R, Gruvstad E,Hedner P. Topical and systemic glucocorticoid poten-cies of budesonide and beclomethasone dipropionate inman. EurJ Clin Pharmacol 1982;22:523-9.
19 Lofdahl C-G, Mellstrand T, Svedmyr N. Glucocorticoidsand asthma. Studies of resistance and systemic effects ofglucocorticoids. Eur J Respir Dis 1984;65(suppl 136):69-77.
20 Pedersen S, Fuglsang G. Urine cortisol excretion in chil-dren treated with high doses of inhaled corticosteroids:a comparison of budesonide and beclomethasone. EurRespiry 1988;1:433-5.
21 Jennings BH, Larsson B, Andersson K-E, Johansson S-A.The assessment of systemic effects of inhaled gluco-corticosteroids: a comparison of budesonide and beclo-methasone dipropionate in healthy volunteers. In JenningsBH. Assessment of systemic effects of inhaled glucocorti-costeroids. Thesis, University of Lund, 1990.
22 Ali NJ, Capewell S, Ward MJ. Bone turnover during highdose inhaled corticosteroid treatment. Thorax 1991;46:160-4.
23 British Thoracic Society, Research Unit of the RoyalCollege of Physicians of London, Kings Fund Centre,National Asthma Campaign. Guidelines for manage-ment of asthma in adults: I-chronic persistent asthma.BMJ 1990;301:651-3.
24 Brown PH, Blundell G, Greening AP, Crompton GK. Dolarge volume spacer devices reduce the systemic effectsof high dose inhaled corticosteroids? Thorax 1990;45:736-9.
25 Farrer M, Francis AS, Pearce SJ. Morning serum cortisolconcentrations after 2 mg inhaled beclomethasonedipropionate in normal subjects: effect of a 750 mlspacer device. Thorax 1990;45:740-2.
26 Selroos 0, Halme M. Effect of a volumatic spacer andmouth rinsing on systemic absorption of inhaled corti-costeroids from a metered dose inhaler and dry powderinhaler. Thorax 1991;46:891-4.
27 Toogood JH, Baskerville J, Jennings B, Lefcoe N,Johansson S-A. Use of spacers to facilitate inhaled corti-costeroid treatment of asthma. Am Rev Respir Dis 1984;129:723-9.
28 Ebden P, Jenkins A, Houston G, Davies BH. Comparisonof two high dose corticosteroid aerosol treatments,beclomethasone dipropionate (1500,ug/day) and budes-onide (1600 pg/day), for chronic asthma. Thorax 198641:869-74.
29 Prahl P. Adrenocortical suppression following treatmentwith beclomethasone and budesonide. Clin Allergy1991;21:145-6.
30 Brown PH, Blundell G, Greening AP, Crompton GK.High dose inhaled corticosteroids and the cortisol stressresponse to acute severe asthma. Respiratory Medicine1992;86:495-7.
31 Brown PH, Blundell G, Greening AP, Crompton GK.Screening for hypothalamo-pituitary-adrenal axis sup-pression in asthmatics taking high dose inhaled corticos-teroids. Respiratory Medicine 1991;85:511-6.
32 Brown PH, Greening AP, Crompton GK. Large volumespacer devices and the influence of high dosebeclomethasone dipropionate on hypothalamo-pituitary-adrenal suppression. Thorax 1993;48:233-8.
33 Packe GE, Douglas JG, McDonald AF, Robins SP, ReidDM. Bone density in asthmatic patients taking highdose inhaled beclomethasone dipropionate and inter-mittent systemic corticosteroids. Thorax 1992;47:414-7.
34 Prahl P, Jensen T. Decreased adreno-cortical suppressionutilizing the Nebuhaler for inhalation of steroid aerosols.ClinAlergy 1987;17:393-8.
973 on 14 July 2018 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.48.10.967 on 1 O
ctober 1993. Dow
nloaded from