systematic reviews of categorical versus continuum...
TRANSCRIPT

ANRV407-CP06-16 ARI 22 February 2010 15:31
Systematic Reviews ofCategorical Versus ContinuumModels in Psychosis:Evidence for DiscontinuousSubpopulations Underlyinga Psychometric Continuum.Implications for DSM-V,DSM-VI, and DSM-VIIRichard J. Linscott1,2 and Jim van Os2,3
1Department of Psychology, University of Otago, Dunedin 9054, New Zealand;email: [email protected] of Psychiatry and Psychology, South Limburg Mental Health Researchand Teaching Network, EURON, Maastricht University, 6200 MD Maastricht,The Netherlands; email: [email protected] of Psychological Medicine, Institute of Psychiatry, De Crespigny Park, DenmarkHill, London SE5 8AF, United Kingdom
Annu. Rev. Clin. Psychol. 2010. 6:391–419
First published online as a Review in Advance onJanuary 4, 2010
The Annual Review of Clinical Psychology is onlineat clinpsy.annualreviews.org
This article’s doi:10.1146/annurev.clinpsy.032408.153506
Copyright c© 2010 by Annual Reviews.All rights reserved
1548-5943/10/0427-0391$20.00
Key Words
classification, epidemiology, latent, nosology, schizophrenia,schizotypy
AbstractDiagnostic systems, phenotype models, and theories of etiology in-corporate propositions on the underlying nature of psychosis andschizophrenia phenotypes. These propositions, whether implicit or ex-plicit, are that the distributions of the phenotypes, or the phenotypeexperiences themselves, are dimensional or categorical. On one hand,evidence on the epidemiology of schizophrenia phenotypes suggestssymptom phenotypes may not be bound by conventional diagnosticthresholds but instead may blend imperceptibly with subclinical, statis-tically frequent experience, supporting continuum viewpoints. On theother hand, evidence on the population structure suggests a latent cat-egorical structure; the population may be composed of two types ofpeople. However, both sets of evidence are beset by methodologicallimitations that point unequivocally to the need to move beyond cur-rent diagnostic conceptualizations, observation, and anamnesis of psy-chosis, and toward responsive and scientifically refutable formulationsof schizophrenia.
391
Ann
u. R
ev. C
lin. P
sych
ol. 2
010.
6:39
1-41
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Col
orad
o -
Bou
lder
on
09/0
5/12
. For
per
sona
l use
onl
y.
ANRV407-CP06-16 ARI 22 February 2010 15:31
Contents
INTRODUCTION . . . . . . . . . . . . . . . . . . 392DEFINITIONS . . . . . . . . . . . . . . . . . . . . . . 393
Latent . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 393Continuous . . . . . . . . . . . . . . . . . . . . . . . . 393
EXPECTATIONS. . . . . . . . . . . . . . . . . . . . 393From Classification Systems . . . . . . . . 393From Theories of Phenotypes . . . . . . 394From Theories of Etiology . . . . . . . . . 395Summary . . . . . . . . . . . . . . . . . . . . . . . . . . 398
EVIDENCE AND ITS DEARTH . . . . 398On Continuity of Experience
and Clinical Phenotypes:A Systematic Review . . . . . . . . . . . . 398
Sources of Heterogeneityin Phenotype Studies . . . . . . . . . . . . 401
On Boundaries Between Normalityand Abnormality . . . . . . . . . . . . . . . . 403
On Boundaries AmongPsychopathologies . . . . . . . . . . . . . . 405
Summary . . . . . . . . . . . . . . . . . . . . . . . . . . 406DOES DSM PROVIDE THE
REQUIREMENTS OF ASCIENTIFIC CONCEPT ONWHICH PHENOTYPICFINDINGS CAN ADVANCE? . . . . 407Continuity of Experience as an
Assessment Artifact . . . . . . . . . . . . . 407The Homogenizing Effect
of Diagnostic Tradition . . . . . . . . . 408Statistical Limitations
and Interpretation . . . . . . . . . . . . . . 411The Promise of New Discoveries . . . 412
CONCLUSIONS ANDRECOMMENDATIONS . . . . . . . . . 413
INTRODUCTION
Madness, frenzy, and melancholy are con-founded by Celsus, and many writers; oth-ers leave out frenzy, and make madness andmelancholy but one disease, which JasonPratensis especially labours, and that they dif-fer only secundum majus or minus, in quantityalone, the one being a degree to the other, andboth proceeding from one cause. They differ
intenso et remisso gradu, saith Gordonius, as thehumor is intended or remitted. (Burton 1628,vol. 1, p. 140)
During the past decade, numerous reports onthe epidemiology of schizophrenia have beenpublished such that there are now significantnumbers of reviews of the subject, systematicand otherwise (Bromet & Fennig 1999, Hafner2000, Jablensky 2000, McGrath et al. 2008,Messias et al. 2007, Murray et al. 2003, Sahaet al. 2005, Tandon et al. 2008). On one hand,these reviews appear to paint a consistent pic-ture. The annual incidence of schizophreniais in the order of 0.2 per 1000, the lifetimeprevalence of schizophrenia is around 0.4%to 0.7%, and there is significant variability inincidence and prevalence rates. Variables thatpredict incidence or prevalence rates includefamily history, age, sex, season of birth, pre-natal factors, substance abuse, urbanicity, mi-nority or migrant status, autoimmune disease,and socioeconomic development. For some ofthese predictors the available evidence is notunequivocal.
There also appears to be general agree-ment that research into the epidemiology ofschizophrenia is affected by methodologicallychallenging issues and methodological prob-lems. These include the absence of a pathog-nomonic marker of the disorder, unavoidablereliance on the clinical interview, meeting thedemand for clinical utility, the level of inter-rater agreement or reliability, variability acrossthe lifespan, and the demand for conceptu-ally compatible analysis methods both in pri-mary research and systematic review ( Jablensky2000; McGrath et al. 2008; Murray et al. 2003;Saha et al. 2005, 2008; Tandon et al. 2008). Im-portantly, evidence suggests that study quality iscorrelated with some epidemiological findings(Saha et al. 2005). Less frequently, doubts aboutthe construct validity of the schizophrenia di-agnosis are expressed (McGrath et al. 2008, vanOs & Verdoux 2003).
On the other hand, there is a striking rangeof views on the overall status of the epi-demiology of schizophrenia. Jablensky (2000)
392 Linscott · van Os
Ann
u. R
ev. C
lin. P
sych
ol. 2
010.
6:39
1-41
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Col
orad
o -
Bou
lder
on
09/0
5/12
. For
per
sona
l use
onl
y.

ANRV407-CP06-16 ARI 22 February 2010 15:31
suggested that the main features of the epi-demiology of schizophrenia were well estab-lished by the late 1930s, saying, “the contours ofthe epidemiological map of schizophrenia wereby and large complete before World War II”(p. 274). Messias et al. (2007) hold a quite differ-ent opinion, saying, “even as late as 25 years ago,the epidemiology of schizophrenia was nearly ablank page” (p. 333). In the middle, McGrathet al. (2008) borrow the contours metaphor toemphasize the need to reappraise the estab-lished dogma surrounding the epidemiology ofschizophrenia: “The contours of this landscapecan no longer be considered flat and feature-less” (p. 74).
There are several recent high-quality re-views of the epidemiology of schizophrenia(e.g., McGrath et al. 2008, Messias et al. 2007,Saha et al. 2005, Tandon et al. 2008). It is notour aim to attempt to match these here. In-stead, our objective is to examine the ques-tion: Does schizophrenia have a categorical orcontinuous latent structure? We begin by clar-ifying the meaning of this question and iden-tifying expectations based on diagnostic clas-sifications, theoretical models of causality, andphenotypic models. We go on to consider ev-idence of continuity in phenotypic expression,focusing predominantly on the clinical and sub-clinical phenotypes. We then address what weregard are obstacles to a scientific epidemiol-ogy of schizophrenia and ideas on the future ofresearch and practice in this area.
DEFINITIONS
Latent
Schizophrenia is a latent construct insofar as it isunobservable. In contrast, the observable man-ifestations of schizophrenia are evident acrosssocial, functional, behavioral, motor, cognitive,affective, physiological, anatomical, and otherbiological domains. Given sufficient manifesta-tions in an individual, an inference is made thatschizophrenia is present. Thus, “latent” in thissense has a very narrow meaning, somethingintangible, which cannot be seen despite even
florid manifestations, and “schizophrenia” is aconcept that extends well beyond criteria for itsdiagnosis.
A second referent of “latent” that also re-ceives some use here is an underlying statisticalvariable. Latent variables are those that are in-ferred on the basis of statistical evidence. Com-mon examples include continuous latent vari-ables identified through factor analysis, oftencalled factors, and categorical latent variablesidentified through latent class analysis.
Continuous
Quite how questions on the latent structureof schizophrenia are posed or addressed in re-search varies substantially because there are sev-eral different meanings to which “continuous”and its synonyms and antonyms are applied.Measuring cross-sectional behavior, cognition,and affect, one can identify manifestations ofschizophrenia that resemble experiences re-ported by individuals who do not meet di-agnostic criteria for schizophrenia. Promotingthis notion, Strauss (1969) argued against thepractice of rating manifestations of schizophre-nia dichotomously, and Kretschmer (1936) andCrow (1998) argued against the notion ofa schizophrenia entity. Thus, in this sense,questions about continuity are concerned withwhether the processes giving rise to schizophre-nia are the same as those that give rise to phe-nomena that bear some resemblance to thesigns or symptoms of schizophrenia.
Observing the intrapersonal course ofschizophrenia, one can identify signs or symp-toms that appear to be exacerbations of subclin-ical function or subjective experience that pre-date the onset of schizophrenia by months oryears (an der Heiden & Hafner 2000, Schultze-Lutter 2009). Fluctuations in manifestationsmay arise through moderation or mediation byintrinsic (e.g., sensitization) or extrinsic pro-cesses (e.g., environmental stressors). Thus, inthis second sense, the principal focus is conti-nuity of phenomenology across time.
Third, examining the composition of pop-ulations, general population sample variability
www.annualreviews.org • Categorical Versus Continuum Models 393
Ann
u. R
ev. C
lin. P
sych
ol. 2
010.
6:39
1-41
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Col
orad
o -
Bou
lder
on
09/0
5/12
. For
per
sona
l use
onl
y.

ANRV407-CP06-16 ARI 22 February 2010 15:31
in manifestations of schizophrenia may arisesolely from graduated interpersonal differenceswithin members of a single population, themixing of two or more discontinuous homoge-neous subpopulations, or some combination ofthese situations. Thus, Meehl’s (1990; see alsoLenzenweger 2006) view on the liability forschizophrenia suggests the commingling of twosubpopulations, whereas Crow’s (1990, 1995)and Claridge’s (1997) views are aligned withthe notion of continuous interpersonal differ-ences across representative general populationsamples. A special case of the population com-position question is encountered in contrasts ofdifferences between schizophrenia and otherserious mental disorders. Here, Crow (1990)could be said to belong to a continuum camp,across from the Kraepelinian dichotomy, thedeficit-nondeficit distinction, Meehl’s (1990)schizotaxia-schizotypy-schizophrenia model,and in the extreme, those who attribute concep-tual significance to the formulation providedby the American Psychiatric Association (Am.Psychiatr. Assoc., e.g., 1994). These appear tobe the three chief referents of “continuous.”The focus in this review is on continuity inexperience and population structure.
EXPECTATIONS
From Classification Systems
Clearly, superficial discontinuity is explicit inthe notion of classification. Whether superfi-cial discontinuity implies latent discontinuityor otherwise is less clear. On one hand, theacceptance of the classification systems in re-search settings, the lack of any significant bodyof work on the construct validity of schizophre-nia classifications ( Jansson & Parnas 2007), andthe proliferation of classification systems in the1970s and 1980s are observations that may becalled in defense of the inference that clas-sification implies discontinuity of experienceand population structure. This is the practiceof the field and follows from the pragmaticdemands of administration, provision of care,communication, statistical analysis, and so on.
Certainly, discontinuity is a reasonable hypoth-esis to test.
On the other hand, there is also recognitionthat pragmatic demands do not necessarilyequate to conceptual or theoretical significance.The authors of the most widely used classifi-cation system, the International Classification ofDiseases (ICD-10; World Health Org. 2004),note the instrument emerged from practicaldemands, not theory. The authors of the mostfrequently used system, the Diagnostic andStatistical Manual of Mental Disorders (DSM;Am. Psychiatr. Assoc. 1980, 1987, 1994,2000), are somewhat more thorough in theirdisclaimer. From 1980 onward, the Ameri-can Psychiatric Association (APA) explicitlyrejected any conceptual or theoretical impli-cations arising from the DSM-III structure forthe latent structure of psychopathology in gen-eral, including questions on the relationshipbetween normality and abnormality (Am. Psy-chiatr. Assoc. 1980, p. 6). That is, the authorsdid not intend that the modular categorialmodel inherent in the DSM-III structure beinterpreted as implying that psychopathologyhas a latent categorial structure.
This qualification reflects the APA’s objec-tive to minimize theoretical bias in classifica-tion, particularly where etiology is unknown.This objective was first most evident throughthe removal of “reaction” from the diagnosticlabels that were used in the first edition (Am.Psychiatr. Assoc. 1952). However, in providingthis more robust disclaimer, the authors effec-tively paint schizophrenia and other diagnosesas without epistemic or conceptual merit; al-though there may be pragmatic value or clinicalutility in drafting patients’ problems into var-ious groupings or subgroupings, such group-ings are arbitrary, make-believe constructions.At the very least, if one takes the qualificationseriously, DSM is silent on the latent structureof schizophrenia.
From Theories of Phenotypes
Several theorists have proposed clear bound-aries between or among phenotypes.
394 Linscott · van Os
Ann
u. R
ev. C
lin. P
sych
ol. 2
010.
6:39
1-41
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Col
orad
o -
Bou
lder
on
09/0
5/12
. For
per
sona
l use
onl
y.

ANRV407-CP06-16 ARI 22 February 2010 15:31
Historically, the most recognized pheno-type boundary is that which Emil Kraepelinproposed between dementia praecox andmanic-depressive insanity, now referred to asthe Kraepelinian dichotomy (Angst 2002). Thisdichotomy has received extensive criticism(e.g., Crow 1990, 1991; Curtis et al. 2000;Greene 2007; Ovsiew 2000). Finding fault withthe broadening of the schizophrenia notion,Murray & O’Callaghan (1991) suggest theKraepelinian dichotomy may still hold fora more narrowly defined dementia praecox,or “congenital psychosis.” They characterizecongenital psychosis as having an insidiousonset with prominent negative symptomsand neurocognitive impairment and withoutsignificant affective symptoms. A similarconstruct was identified by Carpenter et al.(1988, Kirkpatrick et al. 2001), who describea qualitatively distinct class they referred toas the deficit syndrome or, latterly, deficitschizophrenia. The key feature of this classi-fication is the presence of primary enduringnegative symptoms in the context of DSMschizophrenia.
Tsuang et al. (2000a,b) argued for a qualita-tively distinct phase in the course of schizophre-nia, predating the onset of schizophreniaproper, that they referred to as schizotaxia orpreschizophrenia. They describe the conditionas equivalent to schizophrenia in the absenceof psychosis, although the criteria are a littlenarrower than this would imply. Schizotaxia isdiagnosed in individuals who exhibit prominentnegative symptoms and neuropsychological im-pairments and who are first-degree biologicalrelatives of individuals with schizophrenia. Ifsuch an individual subsequently develops psy-chosis, schizophrenia is diagnosed.
A notable irony with the deficit schizophre-nia and schizotaxia constructions is that theserequire the assumption that schizophrenia is anatural category. Kirkpatrick et al. (2001) referto deficit schizophrenia as being a discrete dis-ease within the schizophrenia syndrome. Thus,if deficit schizophrenia is a latent disease entity,its boundaries do not cross those of schizophre-nia. Yet there is no clear reason why deficit
schizophrenia could not occur in the absenceof DSM schizophrenia. The same illogic ap-plies to Tsuang et al’s (2000a) schizotaxia be-cause of the criterion that this is only diag-nosed in first-degree relatives of individualswith schizophrenia.
There are also prominent theories of pheno-type onset and course in which discrete classesare identified (an der Heiden & Hafner 2000,Bromet & Fennig 1999, Schurhoff et al. 2004,Welham et al. 2000). A recent example is pro-vided by McGorry’s (2007, McGorry et al.2006) clinical staging theory in which five keystages in the course of schizophrenia are identi-fied. However, as stated above, continuity ver-sus discontinuity in the course of schizophreniais not within the scope of this review.
From Theories of Etiology
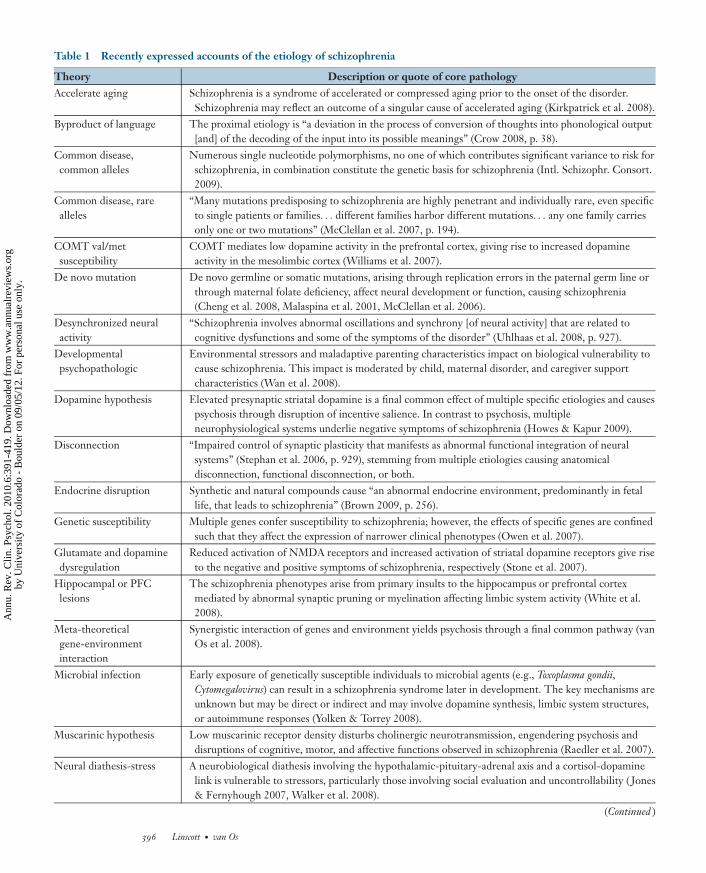
Theories of etiology may incorporate, explic-itly or implicitly, hypotheses on the nature ofschizophrenia. Table 1 contains a summaryof contemporary theories of the etiology ofschizophrenia, or, at least, important signs andsymptoms of the disorder, identified througha selective review of recent literature. In thisliterature, biological explanations preponder-ate, although this may simply be a function ofthe literature we considered. In outlining theirtheories, few authors identify explicit propo-sitions on continuity or otherwise of experi-ence or population structure (Crow 1990, 2008;Lenzenweger 2006; Meehl 2004; van Os et al.2000). On the whole, this issue is rarely ad-dressed in a direct manner.
When considering each theory, we askedtwo questions that derive from the narrow as-sumption that a latent categorical etiologicalmodel would require a singular dichotomouscausal agent: Does the key mechanism of cau-sation operate in an all-or-none fashion? Is thekey mechanism singular or characterized as afinal common pathway or bottleneck in thecausal chain? We reasoned that if either of theseconditions were not met, there would be littlereason for anticipating the schizophrenia phe-notype would be a unitary latent category. Our
www.annualreviews.org • Categorical Versus Continuum Models 395
Ann
u. R
ev. C
lin. P
sych
ol. 2
010.
6:39
1-41
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Col
orad
o -
Bou
lder
on
09/0
5/12
. For
per
sona
l use
onl
y.
ANRV407-CP06-16 ARI 22 February 2010 15:31
Table 1 Recently expressed accounts of the etiology of schizophrenia
Theory Description or quote of core pathologyAccelerate aging Schizophrenia is a syndrome of accelerated or compressed aging prior to the onset of the disorder.
Schizophrenia may reflect an outcome of a singular cause of accelerated aging (Kirkpatrick et al. 2008).Byproduct of language The proximal etiology is “a deviation in the process of conversion of thoughts into phonological output
[and] of the decoding of the input into its possible meanings” (Crow 2008, p. 38).Common disease,common alleles
Numerous single nucleotide polymorphisms, no one of which contributes significant variance to risk forschizophrenia, in combination constitute the genetic basis for schizophrenia (Intl. Schizophr. Consort.2009).
Common disease, rarealleles
“Many mutations predisposing to schizophrenia are highly penetrant and individually rare, even specificto single patients or families. . . different families harbor different mutations. . . any one family carriesonly one or two mutations” (McClellan et al. 2007, p. 194).
COMT val/metsusceptibility
COMT mediates low dopamine activity in the prefrontal cortex, giving rise to increased dopamineactivity in the mesolimbic cortex (Williams et al. 2007).
De novo mutation De novo germline or somatic mutations, arising through replication errors in the paternal germ line orthrough maternal folate deficiency, affect neural development or function, causing schizophrenia(Cheng et al. 2008, Malaspina et al. 2001, McClellan et al. 2006).
Desynchronized neuralactivity
“Schizophrenia involves abnormal oscillations and synchrony [of neural activity] that are related tocognitive dysfunctions and some of the symptoms of the disorder” (Uhlhaas et al. 2008, p. 927).
Developmentalpsychopathologic
Environmental stressors and maladaptive parenting characteristics impact on biological vulnerability tocause schizophrenia. This impact is moderated by child, maternal disorder, and caregiver supportcharacteristics (Wan et al. 2008).
Dopamine hypothesis Elevated presynaptic striatal dopamine is a final common effect of multiple specific etiologies and causespsychosis through disruption of incentive salience. In contrast to psychosis, multipleneurophysiological systems underlie negative symptoms of schizophrenia (Howes & Kapur 2009).
Disconnection “Impaired control of synaptic plasticity that manifests as abnormal functional integration of neuralsystems” (Stephan et al. 2006, p. 929), stemming from multiple etiologies causing anatomicaldisconnection, functional disconnection, or both.
Endocrine disruption Synthetic and natural compounds cause “an abnormal endocrine environment, predominantly in fetallife, that leads to schizophrenia” (Brown 2009, p. 256).
Genetic susceptibility Multiple genes confer susceptibility to schizophrenia; however, the effects of specific genes are confinedsuch that they affect the expression of narrower clinical phenotypes (Owen et al. 2007).
Glutamate and dopaminedysregulation
Reduced activation of NMDA receptors and increased activation of striatal dopamine receptors give riseto the negative and positive symptoms of schizophrenia, respectively (Stone et al. 2007).
Hippocampal or PFClesions
The schizophrenia phenotypes arise from primary insults to the hippocampus or prefrontal cortexmediated by abnormal synaptic pruning or myelination affecting limbic system activity (White et al.2008).
Meta-theoreticalgene-environmentinteraction
Synergistic interaction of genes and environment yields psychosis through a final common pathway (vanOs et al. 2008).
Microbial infection Early exposure of genetically susceptible individuals to microbial agents (e.g., Toxoplasma gondii,Cytomegalovirus) can result in a schizophrenia syndrome later in development. The key mechanisms areunknown but may be direct or indirect and may involve dopamine synthesis, limbic system structures,or autoimmune responses (Yolken & Torrey 2008).
Muscarinic hypothesis Low muscarinic receptor density disturbs cholinergic neurotransmission, engendering psychosis anddisruptions of cognitive, motor, and affective functions observed in schizophrenia (Raedler et al. 2007).
Neural diathesis-stress A neurobiological diathesis involving the hypothalamic-pituitary-adrenal axis and a cortisol-dopaminelink is vulnerable to stressors, particularly those involving social evaluation and uncontrollability ( Jones& Fernyhough 2007, Walker et al. 2008).
(Continued )
396 Linscott · van Os
Ann
u. R
ev. C
lin. P
sych
ol. 2
010.
6:39
1-41
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Col
orad
o -
Bou
lder
on
09/0
5/12
. For
per
sona
l use
onl
y.

ANRV407-CP06-16 ARI 22 February 2010 15:31
Table 1 (Continued )
Theory Description or quote of core pathologyNeurodevelopment-neurogenesis
Disruption of neurogenesis mediated by genetic (e.g., DISC1) and environmental (e.g., viral infection)factors contributes to risk for schizophrenia and related severe mental disorders (Hennah et al. 2006,Mao et al. 2009).
Neurodynamic A reduced prevalence of rapidly conducting cortico-cortical axons gives rise to reduced functional andanatomic asymmetry and, critically, disrupts time-sensitive neurointegration, particularly in the righthemisphere (Miller 2008).
Nutritional deficiency Nutritional deficiency (e.g., folate deficiency) during critical developmental periods disturbs fetaldevelopment, creating congenital abnormalities and risk for schizophrenia (Zammit et al. 2007).
Schizotaxia-schizotypy Schizotaxia is a dichotomously inherited brain state, affecting neurointegration through aberrantsynaptic transmission, producing through interaction with the environment a personality phenotypethat is the liability for schizophrenia (Lenzenweger 2006, Meehl 2004).
Sensitization Psychosis is a sensitized response to recurring psychosocial stressors that engender social defeat. Theresponse is mediated by dopamine sensitization disrupting the hypothalamic-pituitary-adrenal axis (vanWinkel et al. 2008).
Traumatogenic Psychotic experience arises from the interaction of external stressors with information-processingproclivities or impairments: hallucinations, when trauma gives rise to intrusive cognition that ismisattributed to external agents because of poor source monitoring; delusions, when attachment andtrauma interact with processing biases and negative self-esteem, engendering perceived threat andparanoia (Bentall & Fernyhough 2008).
appraisal of this literature suggested that onlyone theory (Lenzenweger 2006, Meehl 1990)occupies this general conceptual space; theoverwhelming majority of authors proposeone or more graded (nondichotomous) mecha-nisms, nonsingular pathways, or both, althoughsome authors did not address the issue in a man-ner that allowed a determination.
In other words, the majority of theoreticalmodels appear consistent with the view that,at the latent level, schizophrenia is continuouswith experience and in population structure. In-deed, a commonly encountered notion is thatmultiple genes of small effect together consti-tute the liability for schizophrenia (e.g., Intl.Schizophr. Consort. 2009; Table 1). If additivein effect, this may strongly imply that the pop-ulation structure is continuous and that phe-notypes are also continuous, with distinctionsamong schizotypy, schizophrenia, and otherdisorder entities a matter of (arbitrary) con-vention or determined by auxiliary variables(resources, resilience, coping, disability).
In many instances, an inference of continu-ity is drawn because the theory is inconsistent
with a latent categorical model, because theauthors propose a mechanism alongside otheretiologies without distinguishing a phenotype,or because the authors implicate the combinedaction of numerous binary components. Sev-eral implicated mechanisms appear to have adichotomous nature, such as de novo muta-tions (Cheng et al. 2008) and rare highly pene-trant genes (McClellan et al. 2007), or a singularpathway, such as specific etiologies for acceler-ated aging (Kirkpatrick et al. 2008) and estro-gen disruption (Brown 2009). However, theseattributes in isolation do not lead to the suppo-sition that schizophrenia is a latent class expe-rience or structure.
The majority of these theoretical notions orhypotheses are not readily converted into con-jectures on the latent structure of schizophre-nia. Understandably, the models are couchedin low- or no-risk speculative terms. Authorsqualify their accounts as relating to one of manypaths to schizophrenia, as providing a generaldisposition to the disorder, as accounting fora subset of cases of schizophrenia, or as re-lating to the symptoms but not the disorder.
www.annualreviews.org • Categorical Versus Continuum Models 397
Ann
u. R
ev. C
lin. P
sych
ol. 2
010.
6:39
1-41
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Col
orad
o -
Bou
lder
on
09/0
5/12
. For
per
sona
l use
onl
y.

ANRV407-CP06-16 ARI 22 February 2010 15:31
However, two exceptions are those put forwardby Crow (1990, 2000, 2008) and Meehl (1962,1990, 2004).
In Crow’s (1995, 2008) theory of psychosis,dimensionality is a proposition alongsideuniversality and absence of an environmen-tal determinant, which together form the ba-sis of his theory that psychoses—affective andnonaffective—emerge from a breakdown in themechanisms that translate thought to utteranceand speech perception to thought. Crow arguesthat schizophrenia and affective psychoses dif-fer in a quantitative manner only, that both de-rive from a single genetic mechanism.
Meehl (1962, 1990, 2001, 2004) proposedthat schizophrenia is the product of gene–environment interaction. The key inherited at-tribute is schizotaxia,1 which was defined asa brain state characterized by reduced differ-entiation of synaptic response probabilities totemporo-spatial input patterns, the proximaloutcome of which is impaired neurointegra-tion. In all cases in which schizotaxia is present,a personality phenotype, schizotypy, devel-ops, although the expressivity of schizotypy isvariable and heterogeneous. The relationshipbetween schizotypy and schizophrenia is con-tinuous; there is a discontinuity between schizo-types and the complement nonschizotypes; andaffective psychoses fall within the complementgroup.
Summary
Throughout the history of schizophrenia the-orizing and research, few have proposed ex-planatory models that imply or specify thatschizophrenia exists as a discrete latent entityclearly demarcated from other states of psy-chopathology as well as from normality. In-deed, a commonality of accounts dating back toHippocrates is the inference of continuous fun-damental processes underpinning normality,
1Meehl’s schizotaxia is fundamentally different from theschizotaxia notion proposed by Tsuang et al. (2000a); thesetwo conceptions occupy different levels of analysis.
eccentricity, and mental disease (Maher &Maher 1994), just as is portrayed in the openingquotation from Burton (1628). In contrast, epi-demiologists aim to elucidate cause by count-ing things. Understandably, then, the study ofthe epidemiology of schizophrenia has beenvery well served by categorical definitions ofthe disorder and its subtypes (e.g., Am. Psy-chiatr. Assoc. 1994). Much of the research onschizophrenia falls into this conceptual hodge-podge: The essence of the disorder is thoughtto be or is treated as dimensional, but diagnosisis categorial.
EVIDENCE AND ITS DEARTH
There are clear theoretical bases for a broad setof hypotheses on the nature of the experienceand population structures of schizophrenia. Byfar the most commonly implied or expressedview is that schizophrenia is a dimensionalconstruct, although authors seldom verbalizewhether they are referring to continuity ofexperience or population structure. There isalso notable support for discontinuities: dis-continuities between normalcy and risk statesas well as among disorders. Drawing theseexpectations together, we consider evidencefocused on three core expectations.
On Continuity of Experienceand Clinical Phenotypes:A Systematic Review
We reasoned that, if the symptom phenotypesare continuous, the rates at which these occur inthe general population should be greater thanthe rate of schizophrenia. To examine this ex-pectation, we undertook a systematic review asfollows.
We obtained the intersection of three setsof MEDLINE entries for research publishedfrom 1950 to (17 July) 2008: (a) entriescontaining one or more of the (truncated) key-word phrases “delus,” “hallucinat,” “paranoi,”“thought disorder,” “disorgani∗ speech,” “looseassociation∗,” “incoherence,” “derailment,”“tangential,” “negative symptom,” “flat affect,”
398 Linscott · van Os
Ann
u. R
ev. C
lin. P
sych
ol. 2
010.
6:39
1-41
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Col
orad
o -
Bou
lder
on
09/0
5/12
. For
per
sona
l use
onl
y.

ANRV407-CP06-16 ARI 22 February 2010 15:31
“blunt∗ affect,” “affective flattening,” “alogia,”“poverty of speech,” “avolition,” “disorgani∗
behavio∗,” “catatoni,” “social isolation,”“social withdrawal,” “psychos,” “psychot,”“schizophr,” or “schizotyp”; (b) entriescontaining one or more of “incidence,”“prevalence,” “sensitivity,” or “specificity”; and(c) entries containing “general population,”“normal population,” “normal individuals,”“normal sample,” “healthy population,”“healthy individuals,” “healthy sample,” “com-munity individuals,” “community sample,”“nonpsychotic,” “survival,” “screening,” or“subclinical.” The resulting intersection setcontained 2652 entries. We read the title ofeach paper and, as necessary, the abstract andthe paper itself to find reports on the incidenceor prevalence of symptoms of schizophreniain general population samples. Papers wereretained in the review if they met all ofthe following criteria and there was sufficientinformation to determine that this was the case:
1. The paper describes one or more studiesof schizophrenia symptom phenotypes,or experiences resembling such pheno-types, in general population samples.
2. The sample n available for analysis was atleast 100.
3. The results included precise incidence orprevalence rates of dichotomous pheno-type outcomes, or count data or scoresfrom which such rates could be derived.
4. Participants were not recruited throughsecondary or tertiary health services(e.g., ophthalmology services), prisons, oraged-care facilities.
5. At least 80% of the sample was less than65 years of age.
6. Outcome indices do not conflateschizophrenia with nonschizophre-nia phenotypes, such as affective ordissociative phenotypes.
7. Schizophrenia symptom phenotypeswere not sleep-related (e.g., hypnopom-pic and hypnagogic hallucinations).
We also searched for other relevant researchamong citations in papers meeting these crite-ria. Where possible, we extracted the following
variables from each report: A cohort nameand attributes, including: sampling population;method of recruitment; response rate; age(range, mean, and standard deviation); theproportions of males and participants olderthan 64 years; and important sample inclusionand exclusion criteria. Where the proportion ofparticipants older than 64 was not reported, anddescriptive statistics for age were available, thestandard normal distribution was used to esti-mate the likely proportion older than 64 years.We also noted the symptom phenotype andthe methods for its assessment, including:instrument names; mode of assessment (self-report, lay interview, professional interview, orobserver ratings); number of items in the instru-ment; the reference timeframe; the thresholdnumber of items with affirmative responses bywhich phenotype outcome was determined; ex-clusion criteria applied to affirmative responses(such as stemming from misunderstanding,relating to plausible experience, due to drug useor medical conditions, or relating to inconse-quential experience); and in the case of gradedratings, severity, frequency, or other thresholdfor phenotype presence. If the outcome scoreconflated two or more schizophrenia symptomphenotypes (e.g., hallucinations and delusions),we recorded the ratio of phenotype items.We recorded the rate data and data-handlingattributes, including weighting to correctfor sampling design, reporting of mean rateversus any endorsement, and the denominator.Where more than one rate was available froma cohort or an article, each nonredundant ratewas recorded along with the above variablesthat characterized its derivation.
The analysis objective was to examine thedistribution of observed rates in these samples.Following Saha et al. (2008), we did not reducerates from included studies to meta-analytic orweighted means. This has the considerable dis-advantage of obscuring variability in rates. In-stead, as Saha et al. (2008) propose, we focus onvariability of rates primarily by presenting thecollated data graphically. A second advantageof this approach is that it can permit inclusionof multiple rates from cohorts. However, if a
www.annualreviews.org • Categorical Versus Continuum Models 399
Ann
u. R
ev. C
lin. P
sych
ol. 2
010.
6:39
1-41
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Col
orad
o -
Bou
lder
on
09/0
5/12
. For
per
sona
l use
onl
y.

ANRV407-CP06-16 ARI 22 February 2010 15:31
methodological characteristic is correlated withphenotype rates as well as the number of ratesor publications per cohort, inclusion of multi-ple rates from a single cohort could alter theoverall observed variability in rates. Therefore,in the case of hallucinations, delusions, and psy-chosis, for which there were large numbers ofprevalence rates, we also used Monte Carlo per-mutation sampling to model the variability thatwould have been observed had only one preva-lence rate per cohort been reported. Specifi-cally, each of 10,000 permutations involved ran-domly selecting one prevalence rate from eachmultirate cohort and the sole rate for single-ratecohorts. The median rate × cumulative rela-tive frequency curve was then obtained, as werethe observed 95% margins. Observed marginswere smoothed using the loess local polynomialregression smoothing function in R (R Dev.Core Team 2004). Monte Carlo permutationsampling was not used for incidence rates, ofwhich there were not large numbers.
We identified 56 papers that met criteriafor inclusion in the review. These 56 reports
contained 285 rates for the prevalence (254rates) or incidence (31 rates) of hallucinations(81 rates), delusions (68 rates), disorganizedspeech (6 rates), negative symptoms (7 rates),disorganized behavior (2 rates), or catatonic be-havior (2 rates). Some rates related to the pres-ence of any feature of psychosis (here, defined ashallucinations, delusions, or both; 82 rates), anycriterion A symptom of schizophrenia (9 rates),social isolation (18 rates), or the combination ofpsychosis with disorganized speech (10 rates).The 285 rates were derived from analyses of 42study cohorts. Among the 56 papers, 16 pro-vided a single rate whereas the median numberof rates obtained was 3 per paper; one paperprovided 48 rates (Rossler et al. 2007).
Table 2 contains descriptive statistics for theobserved prevalence and incidence rates, givenas percentages. Figure 1 shows cumulative rel-ative frequencies for the prevalence rates. Ifthe prevalence rate of schizophrenia is approx-imately 0.4% to 0.7% (McGrath et al. 2008)and the annual incidence of schizophrenia isapproximately 0.02%, it is clear that specific
Table 2 Percentiles and quartiles for recorded phenotype rates
Percentile
Percentile n 10th25th Lower
quartile 50th Median75th Upper
quartile 90thPrevalence ratesHallucinations All 75 0.6 1.5 4.1 10.0 20.8
Permuted 31 1.2 3.1 7.1 14.6 22.5Delusions All 63 0.5 1.7 5.9 17.6 24.7
Permuted 29 0.9 2.2 7.2 17.7 25.9Psychosis All 69 1.5 4.2 7.4 16.3 23.3
Permuted 42 1.3 3.9 11.1 20.9 28.1Disorganized speech 5 1.1 2.2 4.8 18.0 20.2Negative symptoms 6 0.6 1.1 2.3 16.9 26.1Social isolation 17 5.6 7.2 10.0 22.0 26.8
Incidence ratesHallucinations 6 0.8 1.4 1.7 3.9 08.0Delusions 5 1.2 1.6 5.9 11.2 15.7Psychosis 13 1.0 1.0 2.0 11.4 14.4Disorganized speech 1 — — 6.7 — —Negative symptoms 1 — — 0.9 — —Social isolation 1 — — 9.0 — —
Note: Phenotype rates are given as percentages.
400 Linscott · van Os
Ann
u. R
ev. C
lin. P
sych
ol. 2
010.
6:39
1-41
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Col
orad
o -
Bou
lder
on
09/0
5/12
. For
per
sona
l use
onl
y.

ANRV407-CP06-16 ARI 22 February 2010 15:31
0.60.50.40.30.20.10.0
Rate
1.0
0.8
0.6
0.4
0.2
0.0
Cum
ulat
ive
rela
tive
freq
uenc
y
Hallucinations
0.60.50.40.30.20.10.0
Rate
1.0
0.8
0.6
0.4
0.2
0.0
Cum
ulat
ive
rela
tive
freq
uenc
y
Delusions
0.60.50.40.30.20.10.0
Rate
1.0
0.8
0.6
0.4
0.2
0.0
Cum
ulat
ive
rela
tive
freq
uenc
y
Psychosis
1.0
0.8
0.6
0.4
0.2
0.0
Cum
ulat
ive
rela
tive
freq
uenc
y
0.60.50.40.30.20.10.0
Rate
Disorganized speech Negative symptomsSocial isolation
Figure 1Cumulative relative frequencies of schizophrenia phenotype prevalence rates. For disorganized speech, negative symptoms, and socialisolation, the plot (lower right) shows all available rates. For hallucinations, delusion, and psychosis, the curve is the median cumulativerelative frequency obtained using Monte Carlo permutation sampling, with 95% confidence intervals (dashed lines) and loess smoothed95% confidence intervals (shading).
symptom phenotypes are more common thanschizophrenia itself. Specific symptoms are 3 to28 times more prevalent and up to 2.6 orders ofmagnitude more incident than the disorder.
A second key observation from these data isthat there is significant variability of the ratesacross studies. In an earlier but narrower re-view (van Os et al. 2009), we found that higher
prevalence rates of the psychosis phenotypewere associated with less education, unemploy-ment, immigrant status, ethnic minority status(except Asian ethnic status), lower income, be-ing unmarried, being male, history of substancemisuse (alcohol, marijuana, and other drugs),exposure to trauma or significant stressors,and greater urban density. Similarly, higher
www.annualreviews.org • Categorical Versus Continuum Models 401
Ann
u. R
ev. C
lin. P
sych
ol. 2
010.
6:39
1-41
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Col
orad
o -
Bou
lder
on
09/0
5/12
. For
per
sona
l use
onl
y.

ANRV407-CP06-16 ARI 22 February 2010 15:31
incidence was associated with fewer years of ed-ucation, ethnic minority status, substance mis-use (alcohol, marijuana, and other drugs), andexposure to trauma or significant stressors. Be-low we consider other contributions to this het-erogeneity in rates.
In conclusion, these reviews show there isclear evidence that is consistent with continuummodels of schizophrenia signs and symptoms.
Sources of Heterogeneityin Phenotype Studies
When reviewing this research on rates of symp-tom phenotypes, it became apparent that sev-eral method, sample, and data-handling vari-ables might account for some of the significantvariance in the rate data. Therefore, a secondset of analyses was undertaken to evaluate thecontribution of cohort and design variables tovariance in observed rates. These analyses wereconducted on prevalence rates collapsed acrosshallucination, delusion, and psychosis pheno-types. Again, Monte Carlo permutation sam-pling was used to simulate outcomes that wouldhave been observed if just one rate per cohortwas available. Permutation sampling was con-ducted in the same manner as described above.Two independent permutation-sampling anal-yses were conducted.
The first permutation sampling was used toexamine bivariate associations between preva-lence rates and individual design and cohortvariables. The latter included cohort variables(convenience sampling, response rate, mean ageof cohort, percentage of males in cohort, andsample size), assessment variables (mode of as-sessment, number of items in assessment in-strument, the proportion of items pertainingto delusions, and the reference interval or pe-riod), experience criterion variables (applica-tion of phenotype exclusion criterion, quanti-tative response criterion, qualitative criterion),and analysis variables (use of population weight-ing and reporting of mean endorsement versusany endorsement scores). Convenience sam-pling of participants was coded 1 = conve-nience sampling or 0 = any other method of
recruitment. Mode of assessment was coded0 = self-report, 1 = lay assessment, or 2 =professional assessment. Phenotype exclusionswas scored using four levels: 3 = excluded ex-perience judged to be inconsequential (i.e., hav-ing no impact on the respondent) or cultur-ally appropriate, 2 = excluded experience at-tributable to drugs or general medical condi-tions, 1 = excluded experience judged to berealistic or as arising from misunderstanding ofitem content, or 0 = no reported exclusions.Quantitative response criterion refers to thenumber of affirmative item responses requiredfor the phenotype to be judged present. Quali-tative criterion represented frequency, severity,or probability criteria and was scored 0 = noneor ≥ low frequency or none or ≥ low severity orno criterion, 1 = ≥ sometimes or ≥ mediumseverity or likely or possible probability, or 2= ≥ often or ≥ high severity or ≥ definiteor probable presence. Independent permuta-tion samples were obtained for each variable.On each permutation, point-biserial r was cal-culated for dichotomous variables and Spear-man’s rho from rankings of the remainder. Themedian correlation coefficients were used to es-timate r2 and exact 95% margins and p valueswere derived from the distributions of r-values.
The second permutation sampling proce-dure was used to evaluate a weighted multi-variate least-squares regression model of preva-lence using cohort and design variables forwhich the observed bivariate p values were≤0.10. In these analyses, the dependent mea-sure was the arcsine-root transformed preva-lence rates, and the independent variables werethe ranks of the cohort and design variables;sample size was used as a weighting coefficient.Where there was a missing value for a depen-dent variable, the mean rank was used. The pri-mary result of interest from these permutationswas the multiple r2.
Microsoft Excel was used to compute bi-variate correlation coefficients and to obtainall Monte Carlo permutation samples. The R(R Dev. Core Team 2004) lm (linear mod-eling) command was used to run regressionmodels.
402 Linscott · van Os
Ann
u. R
ev. C
lin. P
sych
ol. 2
010.
6:39
1-41
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Col
orad
o -
Bou
lder
on
09/0
5/12
. For
per
sona
l use
onl
y.
ANRV407-CP06-16 ARI 22 February 2010 15:31
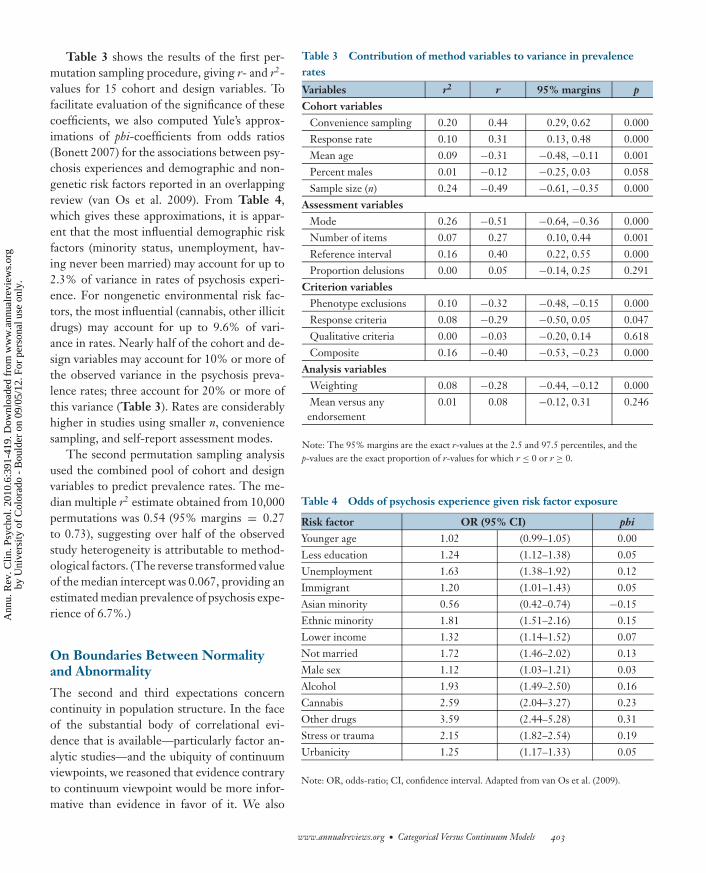
Table 3 shows the results of the first per-mutation sampling procedure, giving r- and r2-values for 15 cohort and design variables. Tofacilitate evaluation of the significance of thesecoefficients, we also computed Yule’s approx-imations of phi-coefficients from odds ratios(Bonett 2007) for the associations between psy-chosis experiences and demographic and non-genetic risk factors reported in an overlappingreview (van Os et al. 2009). From Table 4,which gives these approximations, it is appar-ent that the most influential demographic riskfactors (minority status, unemployment, hav-ing never been married) may account for up to2.3% of variance in rates of psychosis experi-ence. For nongenetic environmental risk fac-tors, the most influential (cannabis, other illicitdrugs) may account for up to 9.6% of vari-ance in rates. Nearly half of the cohort and de-sign variables may account for 10% or more ofthe observed variance in the psychosis preva-lence rates; three account for 20% or more ofthis variance (Table 3). Rates are considerablyhigher in studies using smaller n, conveniencesampling, and self-report assessment modes.
The second permutation sampling analysisused the combined pool of cohort and designvariables to predict prevalence rates. The me-dian multiple r2 estimate obtained from 10,000permutations was 0.54 (95% margins = 0.27to 0.73), suggesting over half of the observedstudy heterogeneity is attributable to method-ological factors. (The reverse transformed valueof the median intercept was 0.067, providing anestimated median prevalence of psychosis expe-rience of 6.7%.)
On Boundaries Between Normalityand Abnormality
The second and third expectations concerncontinuity in population structure. In the faceof the substantial body of correlational evi-dence that is available—particularly factor an-alytic studies—and the ubiquity of continuumviewpoints, we reasoned that evidence contraryto continuum viewpoint would be more infor-mative than evidence in favor of it. We also
Table 3 Contribution of method variables to variance in prevalencerates
Variables r2 r 95% margins p
Cohort variablesConvenience sampling 0.20 0.44 0.29, 0.62 0.000Response rate 0.10 0.31 0.13, 0.48 0.000Mean age 0.09 −0.31 −0.48, −0.11 0.001Percent males 0.01 −0.12 −0.25, 0.03 0.058Sample size (n) 0.24 −0.49 −0.61, −0.35 0.000
Assessment variablesMode 0.26 −0.51 −0.64, −0.36 0.000Number of items 0.07 0.27 0.10, 0.44 0.001Reference interval 0.16 0.40 0.22, 0.55 0.000Proportion delusions 0.00 0.05 −0.14, 0.25 0.291
Criterion variablesPhenotype exclusions 0.10 −0.32 −0.48, −0.15 0.000Response criteria 0.08 −0.29 −0.50, 0.05 0.047Qualitative criteria 0.00 −0.03 −0.20, 0.14 0.618Composite 0.16 −0.40 −0.53, −0.23 0.000
Analysis variablesWeighting 0.08 −0.28 −0.44, −0.12 0.000Mean versus anyendorsement
0.01 0.08 −0.12, 0.31 0.246
Note: The 95% margins are the exact r-values at the 2.5 and 97.5 percentiles, and thep-values are the exact proportion of r-values for which r ≤ 0 or r ≥ 0.
Table 4 Odds of psychosis experience given risk factor exposure
Risk factor OR (95% CI) phi
Younger age 1.02 (0.99–1.05) 0.00Less education 1.24 (1.12–1.38) 0.05Unemployment 1.63 (1.38–1.92) 0.12Immigrant 1.20 (1.01–1.43) 0.05Asian minority 0.56 (0.42–0.74) −0.15Ethnic minority 1.81 (1.51–2.16) 0.15Lower income 1.32 (1.14–1.52) 0.07Not married 1.72 (1.46–2.02) 0.13Male sex 1.12 (1.03–1.21) 0.03Alcohol 1.93 (1.49–2.50) 0.16Cannabis 2.59 (2.04–3.27) 0.23Other drugs 3.59 (2.44–5.28) 0.31Stress or trauma 2.15 (1.82–2.54) 0.19Urbanicity 1.25 (1.17–1.33) 0.05
Note: OR, odds-ratio; CI, confidence interval. Adapted from van Os et al. (2009).
www.annualreviews.org • Categorical Versus Continuum Models 403
Ann
u. R
ev. C
lin. P
sych
ol. 2
010.
6:39
1-41
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Col
orad
o -
Bou
lder
on
09/0
5/12
. For
per
sona
l use
onl
y.

ANRV407-CP06-16 ARI 22 February 2010 15:31
FMM: factor mixturemodeling
CCK: coherent-cutkinetic
reasoned that only evidence which was derivedusing factor mixture modeling (FMM; Muthen& Asparouhov 2006) or coherent-cut kinetic(CCK; Waller & Meehl 1998) methods couldprovide a robust basis for rejection of a con-tinuum model in favor of a model involving anonarbitrary boundary between normality andschizophrenia. This is because, unlike factoranalysis, cluster analysis, and latent class analy-sis, only FMM and CCK procedures provide foreither outcome. In contrast, one can never usefactor analysis to contrast categorical and con-tinuum models; it always results in the identifi-cation of continua, regardless of the true latentstructure. Similarly, latent class analysis will al-ways result in the identification of categories,regardless of the true latent structure. More de-tail on these procedures and their limitationsis available elsewhere (Linscott et al. 2009a,b;Meehl 2004; Muthen & Asparouhov 2006).
Therefore, our second hypothesis is thatthere is a nonarbitrary boundary betweenschizophrenia and normality. To examine thishypothesis we undertook a systematic searchfor CCK and FMM studies of schizophreniasigns and symptoms. We used the followingapproach.
We obtained the intersection of three setsof MEDLINE entries for research publishedfrom 1950 to ( July) 2009: (a) entries containingone or more of the (truncated) keyword phrases“schizophren,” “schizoaffect,” “psychosis,”“psychotic,” or “schizotyp”; (b) entries con-taining one or more of “class,” “kind,” “type,”“subtype,” “taxa,” “taxon,” “taxanomic,” “taxo-nomic,” “categorical,” “categorial,” “continu,”“discontinu,” “discrete,” or “mixture”; and(c) entries containing “latent,” “underlying,”“structure,” “structural,” “hidden,” or “unob-serv.” The resulting intersection set contained1247 entries, of which 864 were nonreview hu-man research papers. We read the title of eachpaper and, as necessary, the abstract and thepaper itself to find reports on the latent struc-ture of schizophrenia or schizophrenia-relatedphenotypes in general population samples.
We identified 15 reports that address anaspect of this issue, the majority of which
described studies of self-report data fromschizotypy questionnaires completed by uni-versity students (Blanchard et al. 2000, Fossatiet al. 2007, Horan et al. 2004, Keller et al. 2001,Korfine & Lenzenweger 1995, Lenzenweger1999, Lenzenweger & Korfine 1992, Linscott2007). Several other similar studies examinedprimary health patients (van Kampen 1999),school children (Fossati et al. 2007, Linscottet al. 2006), or mixed-source samples (Meyer &Keller 2001, Rawlings et al. 2008). Two reportsdescribe data from biological offspring of moth-ers with schizophrenia (Erlenmeyer-Kimlinget al. 1989, Tyrka et al. 1995), but only thelatter of these used measures of schizophrenia-related symptoms. One report examined datafrom endophenotype measures (attention andeye-movement variables) in a general popula-tion sample (Lenzenweger et al. 2007).
The 12 reports examining psychometric riskinclude 50 analyses conducted on 14 samples;only two of the analyses (Keller et al. 2001) in-volved an FMM-like analysis method. Of these50 analyses, four yielded ambiguous results,16 yielded results that are consistent with adimensional interpretation, and the remaining30 yielded results consistent with a categoricalinterpretation. However, 10 of these analyses,relating to 1 ambiguous result, 7 dimensionalresults, and 2 categorical results, were funda-mentally flawed because of significant violationsof test assumptions (Fossati et al. 2007) or se-rious biases inherent in the population sample(Rawlings et al. 2008). None of the studies in-volved representative epidemiological samplesof the general population.
Among those unambiguous findings thatclearly pertained to positive or negative featuresof psychometric risk, regardless of the sam-ple or multiple analyses, 26 findings suggestedrisk for schizophrenia is categorical, whereas13 suggested it is dimensional. The probabil-ity of observing this pattern of results, assum-ing outcomes were random and equally likely, is0.015, suggesting this is not a chance pattern offindings. These findings included some sample-measure instances that were analyzed withmore than one CCK- or FMM-related method,
404 Linscott · van Os
Ann
u. R
ev. C
lin. P
sych
ol. 2
010.
6:39
1-41
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Col
orad
o -
Bou
lder
on
09/0
5/12
. For
per
sona
l use
onl
y.
ANRV407-CP06-16 ARI 22 February 2010 15:31
1.0
0.8
0.6
0.4
0.2
0.0
Cum
ulat
ive
rela
tive
freq
uenc
y
0.60.50.40.30.20.10.0
Rate
Positive schizotypy Negative schizotypy
1.0
0.8
0.6
0.4
0.2
0.0
Cum
ulat
ive
rela
tive
freq
uenc
y
0.60.50.40.30.20.10.0
Rate
Positive schizotypy Negative schizotypy
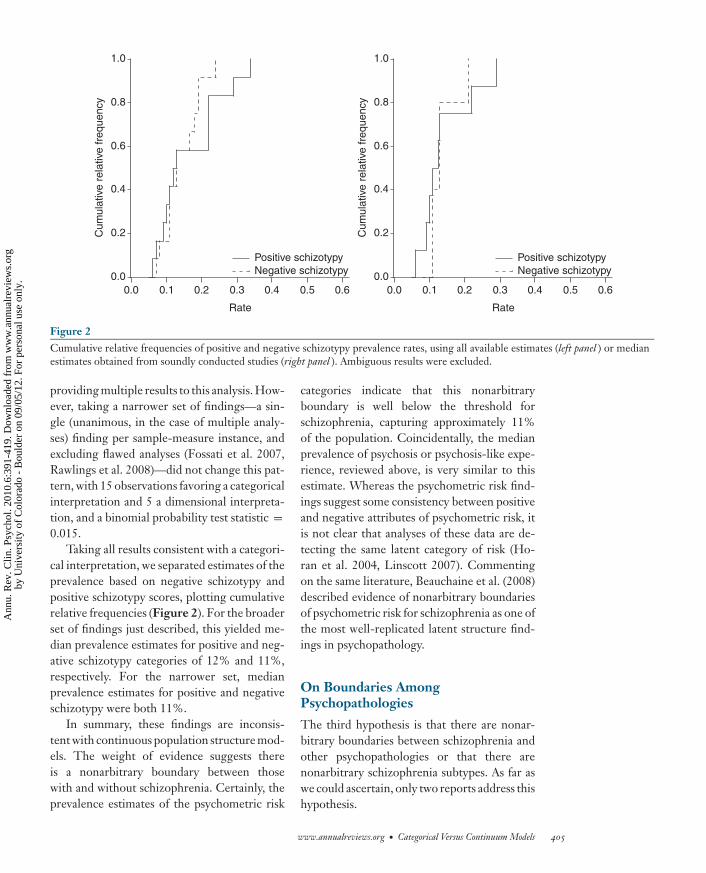
Figure 2Cumulative relative frequencies of positive and negative schizotypy prevalence rates, using all available estimates (left panel ) or medianestimates obtained from soundly conducted studies (right panel ). Ambiguous results were excluded.
providing multiple results to this analysis. How-ever, taking a narrower set of findings—a sin-gle (unanimous, in the case of multiple analy-ses) finding per sample-measure instance, andexcluding flawed analyses (Fossati et al. 2007,Rawlings et al. 2008)—did not change this pat-tern, with 15 observations favoring a categoricalinterpretation and 5 a dimensional interpreta-tion, and a binomial probability test statistic =0.015.
Taking all results consistent with a categori-cal interpretation, we separated estimates of theprevalence based on negative schizotypy andpositive schizotypy scores, plotting cumulativerelative frequencies (Figure 2). For the broaderset of findings just described, this yielded me-dian prevalence estimates for positive and neg-ative schizotypy categories of 12% and 11%,respectively. For the narrower set, medianprevalence estimates for positive and negativeschizotypy were both 11%.
In summary, these findings are inconsis-tent with continuous population structure mod-els. The weight of evidence suggests thereis a nonarbitrary boundary between thosewith and without schizophrenia. Certainly, theprevalence estimates of the psychometric risk
categories indicate that this nonarbitraryboundary is well below the threshold forschizophrenia, capturing approximately 11%of the population. Coincidentally, the medianprevalence of psychosis or psychosis-like expe-rience, reviewed above, is very similar to thisestimate. Whereas the psychometric risk find-ings suggest some consistency between positiveand negative attributes of psychometric risk, itis not clear that analyses of these data are de-tecting the same latent category of risk (Ho-ran et al. 2004, Linscott 2007). Commentingon the same literature, Beauchaine et al. (2008)described evidence of nonarbitrary boundariesof psychometric risk for schizophrenia as one ofthe most well-replicated latent structure find-ings in psychopathology.
On Boundaries AmongPsychopathologies
The third hypothesis is that there are nonar-bitrary boundaries between schizophrenia andother psychopathologies or that there arenonarbitrary schizophrenia subtypes. As far aswe could ascertain, only two reports address thishypothesis.
www.annualreviews.org • Categorical Versus Continuum Models 405
Ann
u. R
ev. C
lin. P
sych
ol. 2
010.
6:39
1-41
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Col
orad
o -
Bou
lder
on
09/0
5/12
. For
per
sona
l use
onl
y.

ANRV407-CP06-16 ARI 22 February 2010 15:31
The first of these conducted a test of the hy-pothesis that deficit schizophrenia is a discreteclass comprising approximately 30% of thosewith schizophrenia (Blanchard et al. 2005). Thesample (n = 238) was one ascertained for atreatment outcome study conducted by the Na-tional Institute of Mental Health. The pri-mary analysis variables were asociality, alogia,blunted affect, and avolition during the pastweek. These were derived from ratings on theScale for the Assessment of Negative Symptoms(SANS) and the Brief Psychiatric Rating Scale(BPRS) taken during the treatment baseline andat six-month follow-up. Carefully conductedCCK analyses yielded compelling evidence ofa categorical latent structure, with a deficitclass prevalence of 28%. Subsequent compar-ison of the deficit and nondeficit classes sug-gested members of the former were more prob-ably male and never married, exhibited poorersocial functioning across multiple relationshipdomains, and had higher BPRS scores, partic-ularly on anergia and disorganization items.
Although the study was well executed, onepotential interpretive problem stands out. Datafrom treatment outcome studies contain aclear source of systematic variance: Some par-ticipants receive the active treatment; othersdo not. Blanchard et al. (2005) demon-strated that treatment condition did not pre-dict class membership. However, it is not treat-ment assignment that is the primary concern.Rather, treatment response—regardless oftreatment condition—could have significantlyaffected the follow-up assessment and intro-duced a treatment response–related nonarbi-trary boundary within the data.
The second major report in this area wasless theoretically driven (Cuesta et al. 2007).It explored reality distortion, disorganization,and negative symptom variables in a sample of660 consecutive admissions with one or moresigns or symptoms of psychosis. The analysisvariables were derived from a factor analysis ofSANS and Scale for the Assessment of PositiveSymptoms (SAPS) scores. Results from CCKanalyses were quite ambiguous, supporting nei-ther continuum nor categorical interpretations.
This ambiguity appears to be attributable to asimple violation of the assumptions of the CCKmethods they used: These methods requireunidimensional monotonically related variables(Maraun & Slaney 2005, Meehl 1999). Thatis, if CCK methods are to be applied appro-priately, the variables included in the analysismust all be more or less uniformly and non-negatively correlated (i.e., correlations amongvariables must all be ≥0 or ≤0). If a class struc-ture is present and some correlations amongvariables are positive and others negative, thevariables likely tap into multiple different la-tent categories (Meehl 1999). This was the casein Cuesta et al. (2007): Reality distortion wasnegatively correlated with both disorganizationand negative symptoms, whereas disorganiza-tion and negative symptoms were positivelycorrelated.
In summary, there is a significant dearth ofevidence on schizophrenia-related phenotypeboundaries within psychopathology. One re-port suggests evidence of a nonarbitrary bound-ary between deficit and nondeficit schizophre-nia; however, this may be attributable to asource of systematic error variance. A secondapplied CCK methods to symptom dimensionscores in a manner that invalidated its results.Several other smaller reports appear in the lit-erature but lack the detail required to judge thesignificance of the findings. For example, Bell(1997) reported disorganization symptoms arecategorical, and Blanchard et al. (2005) also re-fer to having analyzed disorganization symptomscores but did not describe the results.
Summary
Theory and practice give rise to diverse ex-pectations about the latent structure and ex-perience of schizophrenia phenotypes. Extantresearch provides clear evidence of continuitybetween clinical signs and symptoms, whetherpositive or negative, and schizophrenia-likesubclinical experience and behavior. However,a range of methodological and design variablesaffect observed rates. Evidence also suggeststhat differences among members of the general
406 Linscott · van Os
Ann
u. R
ev. C
lin. P
sych
ol. 2
010.
6:39
1-41
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Col
orad
o -
Bou
lder
on
09/0
5/12
. For
per
sona
l use
onl
y.

ANRV407-CP06-16 ARI 22 February 2010 15:31
population, in respect to these experiences andbehavior, are not solely quantitative; evidenceof a nonarbitrary, qualitative boundary exists.As far as we can tell, there have been no un-biased examinations of whether there are alsononarbitrary boundaries within the psychoses.
It was demonstrated that narrowing the fo-cus onto specific symptom phenotypes in thegeneral population might assist in elucidatingboundary issues reflecting different aspects ofcontinuity. It was also shown, however, thatthis strategy is vulnerable to systematic errorvariance introduced by cohort and design vari-ables. Using studies of the prevalence of psy-chosis phenotypes, we show that this source oferror variance can account for up to 10 times thevariance explained by demographic risk factorsand more than twice the variance explained bythe most potent nongenetic environmental riskfactor.
DOES DSM PROVIDE THEREQUIREMENTS OF ASCIENTIFIC CONCEPT ONWHICH PHENOTYPICFINDINGS CAN ADVANCE?
Without dampening enthusiasm for continuum(van Os et al. 2000) and categorical (Linscott2007) viewpoints, there are significant chal-lenges and limitations inherent in the literaturereviewed here. These include methodologicalexplanations for evidence of continuity of ex-perience; the influence of tradition on defini-tions of schizophrenia; calls for incorporation ofgenotype or endophenotype measures in clas-sification; and limitations on the interpretationof evidence of boundaries derived from pheno-type measures.
Continuity of Experience as anAssessment Artifact
There are two reasons for suggesting that con-tinuity of experience may be an assessment arti-fact of sorts. Evidence that psychosis and otherphenotypes of schizophrenia are more commonthan the disorder itself may be due entirelyto the arbitrary nature of the threshold for its
diagnosis, the diagnostic requirement of im-pairment in functioning, or both. Taking a dif-ferent viewpoint, continuity of experience is ev-ident because, for example, DSM is artificiallyrestrictive, requiring the combination of twokey features—or in some presentations, one—as well as significant compromise in function-ing. Consequently, to say that the prevalence ofschizophrenia is 0.7% is simply to say that thecurrent-day arbitrary convention places the cutfor the disorder above the 99th percentile of thegeneral population (Crow 2008, Meehl 1973).Although this criticism undermines the logic ofthe argument that continuity is implied whenphenotype prevalence is greater than diagnosisprevalence, the crux of the problem lies withthe diagnosis, not the phenotype. Argumentsfor the continuum viewpoint are redeemed bythe more compelling evidence that the pheno-type, in subclinical forms, is associated with thesame demographic and nongenetic risk factorsas schizophrenia (van Os et al. 2009; see alsoTable 4).
Second, evidence that psychosis and otherphenotypes of schizophrenia are more com-mon than the disorder may be due entirelyto the facility of language—the item contentof measures as a vehicle for creative portray-als of lesser phenotypes or euphemistic inter-pretations of clinical experience. Compare thecontrasting hallucination-related content of in-struments. DSM-IV schizophrenia may be di-agnosed where “hallucinations consist of a voicekeeping up a running commentary on the per-son’s behavior or thoughts, or two or morevoices conversing with each other” (Am. Psy-chiatr. Assoc. 2000, p. 312). However, experi-ence may be indicated with an affirmative re-sponse to the item “Did you at any time hearvoices saying quite a few words or sentenceswhen there was no-one around that might ac-count for it?” ( Johns et al. 2004, p. 300), “Overthe past year, have there been times when youheard or saw things that other people couldn’t?”( Johns et al. 2004, p. 300), “No matter howhard I try to concentrate, unrelated thoughtsalways creep into my mind” (Bentall & Slade1985, p. 528), or “Sometimes a passing thought
www.annualreviews.org • Categorical Versus Continuum Models 407
Ann
u. R
ev. C
lin. P
sych
ol. 2
010.
6:39
1-41
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Col
orad
o -
Bou
lder
on
09/0
5/12
. For
per
sona
l use
onl
y.

ANRV407-CP06-16 ARI 22 February 2010 15:31
will seem so real that it frightens me” (Bentall& Slade 1985, p. 528). The first two questionsare items in the Psychosis Screening Question-naire; the others are items in the Launay-SladeHallucination Scale (LSHS; Launay & Slade1981). Each of these items was relied upon byauthors of papers included in the systematic re-view of phenotype experience (Aleman et al.2001; Bentall & Slade 1985; Johns et al. 2002,2004; Larøi et al. 2004; Stefanis et al. 2004;Wiles et al. 2006).
What is the true significance of affirmativeresponses to these sorts of questions? A clearvulnerability conferred by these sorts of rat-ing scales is tautological reasoning. Considerthe LSHS (Launay & Slade 1981). The au-thors’ intention was to write some items thatare clearly of a clinical nature (e.g., “I havebeen troubled by hearing voices in my head”)as well as items focused on related but milderexperiences, as above. Moreover, the authorsalso used an item-analysis method to whittledown the content of the LSHS to produce aunidimensional instrument with items with dif-fering completion probabilities (item difficul-ties). That is, the authors explicitly presupposeda latent dimensional structure to their instru-ment. A similar but more gross item-difficultyvariation is evident in the Psychosis Screen-ing Questionnaire. Finding that the prevalenceof experience, measured with these and simi-lar measures, is higher than the prevalence ofschizophrenia is a simple consequence of in-strument design. In itself, the tautology is not afatal problem (Miller 2008). However, it leavesus pondering whether clinician- and self-reportmeasures, such as those used in studies reviewedhere, are the best tools available for rigoroustesting of continuum versus category models ofschizophrenia.
The Homogenizing Effectof Diagnostic Tradition
The flip side of the assessment-artifact criticismis that the field is intrigued by continuity be-cause of the homogenizing effect of diagnostictradition. According to many, advances in the
understanding and treatment of schizophreniago hand in hand with advances in the classifica-tion of the disorder (e.g., Bentall & Fernyhough2008, Craddock et al. 2006, Intl. Schizophr.Consor. 2009, Jansson & Parnas 2007, Owenet al. 2007, Raedler et al. 2007, Stephan et al.2006, Tsuang et al. 2000a, Uhlhaas et al. 2008,Yolken & Torrey 2008). However, tradition hasa powerful influence over current-day diagnos-tic practice.
Consider DSM-IV (Am. Psychiatr. Assoc.2000). By far the most frequently counted thingin schizophrenia research is evidence meetingor surpassing the APA’s criteria for schizophre-nia, published in editions of the DSM (Am.Psychiatr. Assoc. 1980, 1987, 1994). Manymore definitions of schizophrenia are available( Jansson & Parnas 2007), and the ICD (e.g.,World Health Org. 2004) and Research Diagnos-tic Criteria (RDC; Spitzer et al. 1978) also fea-ture prominently in contemporary literature.Nevertheless, DSM is the most commonly usedinstrument for diagnosis in schizophrenia re-search. Without a sea change in this field, thiswill continue to be the case. However, survey-ing its history, several observations give riseto the suggestion that DSM significantly con-strains advancement in schizophrenia researchand, more specifically, understanding of its na-ture and causes.
First, DSM was designed to serve as broadan array of interests as possible, although notequally well (Am. Psychiatr. Assoc. 1952, 1968).In the history of DSM, science has been boththe latecomer and the poor cousin to clinicalutility. Contrary to a claim in DSM-IV (Am.Psychiatr. Assoc. 1994, p. xvi), DSM nomen-clature is not grounded in empirical evidencebut rather in clinical utility, tradition, and con-sensus agreement (APA 1952, 1980, 1987, 1994;Crow 2008). Beneath these, of course, is the vi-tal contribution of clinical experience of gener-ations of clinicians schooled in psychiatric tradi-tion. Other factors influencing its development,including the desire for consistency acrossrevisions, administrative expediencies, reim-bursement issues, and pedagogical merit, havebeen at least on par with scientific evidence.
408 Linscott · van Os
Ann
u. R
ev. C
lin. P
sych
ol. 2
010.
6:39
1-41
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Col
orad
o -
Bou
lder
on
09/0
5/12
. For
per
sona
l use
onl
y.

ANRV407-CP06-16 ARI 22 February 2010 15:31
Consequently, DSM-IV does very well in clini-cal practice and, no doubt, DSM-V will do evenbetter; clinical utility is a key strength of DSM-IV. However, just as Crow (1990) savored thepossibility that his propositions about psychosiswould be demonstrated to be erroneous, a sci-entific epidemiology of schizophrenia desper-ately needs a conceptual model of schizophre-nia that can be rejected and left behind. TheDSM development and revision process is nei-ther nimble nor quick enough to serve this pur-pose, nor is it focused on this purpose.
Second, the APA’s (1980, 1987, 1994, 2000)assertion that DSM classifications have no con-ceptual meaning creates a significant conun-drum. In this context, evidence of inadequateconstruct validity for a particular DSM classifi-cation is neither here nor there—perhaps evenconsistent with the goal to have an atheoret-ical classification system. It is not simply thatthe DSM schizophrenia concept cannot be re-jected. Instead, there is no concept to reject.
This qualification also constrains interpreta-tion of research findings. For example, there isabundant evidence that may be construed as val-idating DSM schizophrenia: Modeling analysessuggest the clinical phenotype of schizophreniaconstruct is multifaceted (Liddle 1987); longi-tudinal analyses suggest a small number of out-come profiles (an der Heiden & Hafner 2000);neuropsychological studies indicate strong as-sociations with neuromotor, attention, mem-ory, and higher-order impairments (Heinrichs& Zakzanis 1998); epidemiological studies in-dicate robust associations with exposure tostress-laden environmental factors (van Winkelet al. 2008)—we could go on and on. If DSMschizophrenia is atheoretical, these consisten-cies relate to a cluster of symptoms that co-occur yet possess no meaning.
Third, the level of attention given to thereliability of classifications combined with lit-tle or no attention to diagnostic validity is se-riously problematic. The reliability of a mea-sure (diagnosis) is readily improved by basicmechanical changes to the device, such as by re-ducing heterogeneous item content or increas-ing the number of items. DSM-I and DSM-II
diagnoses were unreliable in part because thesewere single-item or prototype instruments.By replacing the single item, or prototype,with multiple items (criteria) and a basic al-gorithm for combining item data, as in DSM-III, the influence of observer variance in thethreshold for diagnosis is significantly restrictedand overall error variance is reduced, improv-ing reliability. Improved reliability may be ex-pected to have two effects. First, improvedreliability engenders increased confidence inthe authenticity of the associated latent con-struct. If this construct is an arbitrary classifi-cation, reliability contributes to its reification.Secondly, it strengthens the sense that the fieldcan agree that it is looking at the same thing,from which some may infer that the field agreeson what it is looking at, despite the epistemiccautions.
In summary, despite its frequent use, DSMdoes not provide the basic requirements of ascientific concept on which the epidemiology ofschizophrenia can advance (Cronbach & Meehl1955). There is a significant gulf between thetradition on which DSM-IV schizophrenia isbased and the knowledge that has accumulatedin the recent decades, knowledge that could beemployed to identify, examine, and reject morehomogeneous disorder concepts.
One could counter that DSM does not nec-essarily constrain a scientific epidemiology ofschizophrenia: Researchers could develop andtest criteria in samples of patients with DSM-IV schizophrenia or in relatives of DSM-IVschizophrenia probands, and so on. However,this counterargument requires the assumptionsthat (a) the DSM-IV criteria correspond to em-pirical and not arbitrary boundaries, and (b) theresearch classification is a true subset of DSM-IV schizophrenia. Both these assumptions areuntenable, as described in respect to schizotaxia(Tsuang et al. 2000a) and deficit schizophrenia(Kirkpatrick et al. 2001).
Our focus on DSM also invites the criti-cism that other classification systems are moremeaningfully construed. This is a fair criticism.In defense, however, although there are somedissimilarities among the available systems for
www.annualreviews.org • Categorical Versus Continuum Models 409
Ann
u. R
ev. C
lin. P
sych
ol. 2
010.
6:39
1-41
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Col
orad
o -
Bou
lder
on
09/0
5/12
. For
per
sona
l use
onl
y.

ANRV407-CP06-16 ARI 22 February 2010 15:31
A B
1.0
0.5
0.0
Gen
eral
sch
izop
hren
ia fa
ctor
load
ing
1.00.50.0
Inter-rater reliability (kappa)
Schneider
Cloninger
PSE
NHSI
LandmarkVienna
Figure 3(A) Factor loadings reported by Peralta & Cuesta (2005) and interpreted as indicating the presence of a general schizophrenia factor.(B) Scatter plot of factor loadings for the general schizophrenia factor against inter-rater reliability estimates. ICD, InternationalClassification of Disease; IPSS, International Pilot Study of Schizophrenia; NHSI, New Haven Schizophrenia Index; PSE, PresentState Examination; RDC, Research Diagnostic Criteria.
diagnosing schizophrenia, similarities out-weigh these. In several studies, authors have ex-amined the consistency of schizophrenia diag-nostic systems (Bell et al. 1998, Gift et al. 1980,Peralta & Cuesta 2005). In the most recent ofthese, patients meeting the inclusion criterionof exhibiting one or more psychotic or negativesymptoms were diagnosed using 23 systems forthe classification of schizophrenia.
The resulting data were subject to factoranalysis, and three dimensions were identi-fied (Figure 3): a general schizophrenia factorthat loaded heavily on 20 of the 23 systems; aSchneiderian factor that captured a contrast be-tween the Schneider and Cloninger systemson the one hand, and Feighner, Kraepelin,Langfeldt, and DSM systems on the other; anda Bleulerian factor that captured a contrast be-tween the Bleuler and Vienna systems on theone hand, and the ICD-10, DSM, RDC, andSchneider systems on the other. With the sec-ond and third factors having more contrast-ing loadings, the authors interpreted these re-sults as indicating that there is a single general
schizophrenia factor, analogous to the generalintelligence factor, g (Peralta & Cuesta 2005).
A more mundane interpretation is thatthose who have developed diagnostic systemstend to hold roughly similar conceptions ofschizophrenia, with some minor departuresfrom a generalized or modal concept reflect-ing the impact of, for example, Schneider’s andBleuler’s viewpoints, respectively. Thus, the un-derlying dimension is item difficulty conflatedwith the expressivity of schizophrenia; it is moredifficult to obtain a diagnosis of schizophreniawith Feighner’s criteria than with Cloninger’scriteria ( Jansson & Parnas 2007). In a similarvein, Faraone & Tsuang (1994) encourage theapplication of related statistical procedures toderive evidence of diagnostic accuracy for psy-chiatric classifications.
This alternative mundane interpretationproceeds from the fact that experts’ concep-tions of schizophrenia are more proximal toPeralta & Cuesta’s (2005) observed data thanthe essence of schizophrenia (Figure 4). Out-come variance may be rooted in phenotype
410 Linscott · van Os
Ann
u. R
ev. C
lin. P
sych
ol. 2
010.
6:39
1-41
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Col
orad
o -
Bou
lder
on
09/0
5/12
. For
per
sona
l use
onl
y.
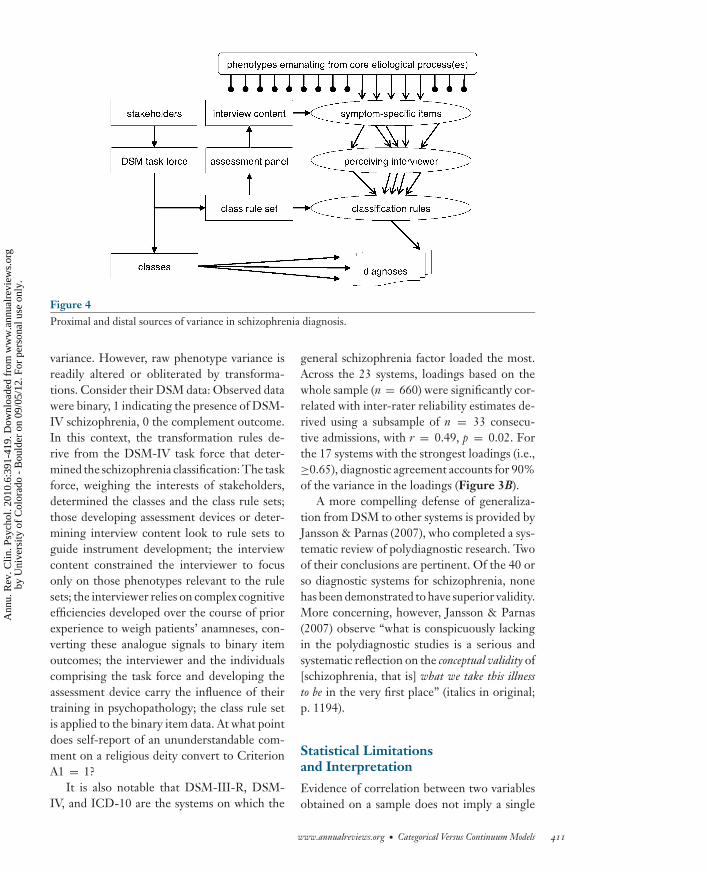
ANRV407-CP06-16 ARI 22 February 2010 15:31
Figure 4Proximal and distal sources of variance in schizophrenia diagnosis.
variance. However, raw phenotype variance isreadily altered or obliterated by transforma-tions. Consider their DSM data: Observed datawere binary, 1 indicating the presence of DSM-IV schizophrenia, 0 the complement outcome.In this context, the transformation rules de-rive from the DSM-IV task force that deter-mined the schizophrenia classification: The taskforce, weighing the interests of stakeholders,determined the classes and the class rule sets;those developing assessment devices or deter-mining interview content look to rule sets toguide instrument development; the interviewcontent constrained the interviewer to focusonly on those phenotypes relevant to the rulesets; the interviewer relies on complex cognitiveefficiencies developed over the course of priorexperience to weigh patients’ anamneses, con-verting these analogue signals to binary itemoutcomes; the interviewer and the individualscomprising the task force and developing theassessment device carry the influence of theirtraining in psychopathology; the class rule setis applied to the binary item data. At what pointdoes self-report of an ununderstandable com-ment on a religious deity convert to CriterionA1 = 1?
It is also notable that DSM-III-R, DSM-IV, and ICD-10 are the systems on which the
general schizophrenia factor loaded the most.Across the 23 systems, loadings based on thewhole sample (n = 660) were significantly cor-related with inter-rater reliability estimates de-rived using a subsample of n = 33 consecu-tive admissions, with r = 0.49, p = 0.02. Forthe 17 systems with the strongest loadings (i.e.,≥0.65), diagnostic agreement accounts for 90%of the variance in the loadings (Figure 3B).
A more compelling defense of generaliza-tion from DSM to other systems is provided byJansson & Parnas (2007), who completed a sys-tematic review of polydiagnostic research. Twoof their conclusions are pertinent. Of the 40 orso diagnostic systems for schizophrenia, nonehas been demonstrated to have superior validity.More concerning, however, Jansson & Parnas(2007) observe “what is conspicuously lackingin the polydiagnostic studies is a serious andsystematic reflection on the conceptual validity of[schizophrenia, that is] what we take this illnessto be in the very first place” (italics in original;p. 1194).
Statistical Limitationsand Interpretation
Evidence of correlation between two variablesobtained on a sample does not imply a single
www.annualreviews.org • Categorical Versus Continuum Models 411
Ann
u. R
ev. C
lin. P
sych
ol. 2
010.
6:39
1-41
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Col
orad
o -
Bou
lder
on
09/0
5/12
. For
per
sona
l use
onl
y.

ANRV407-CP06-16 ARI 22 February 2010 15:31
continuous population structure underlies thedata. Nor would this imply the absence of acommingled (two- or more-group) populationstructure. Indeed, CCK methods, which can beused to test for latent categorical populationstructures, do not work when variables are notcorrelated (Waller & Meehl 1998). Similarly,methods such as factor analysis cannot rule outthe presence of latent categories of people, andlatent class analysis cannot rule out continuummodels of schizophrenia (Linscott et al. 2009a).Very few methods provide exploratory and un-biased contrasts of continuum versus categorymodels (Muthen & Asparouhov 2006, Waller& Meehl 1998).
Some of these methods have been usedto demonstrate evidence of latent struc-tures consistent with categorical viewpointsof schizophrenia. However, there are notablelimitations of this evidence. Foremost amongthese is that demonstration of a latent cate-gorical structure does not imply identificationof a natural kind. Instead, all that can be saidwith any confidence is that the data appearto derive from a population in which there isa latent statistical discontinuity that happensto be large enough to be noticeable (Meehl2004). Whether discontinuity or dimensional-ity derives from a disease etiology, research de-sign (Beauchaine & Waters 2003), psychomet-ric properties (Launay & Slade 1981), or someartifact (Blanchard et al. 2005) is a matter ofinterpretation.
In the bulk of studies that yield evidence ofcategorical latent structures, researchers havenot gone nearly as far as they could to fa-cilitate interpretation through convincing de-sign and methodology. For example, the in-ventor of CCK methods envisaged that testingof latent structure models would be based onvariables spanning a diversity of schizophreniaphenotypes, including anatomical features (e.g.,dermatoglyphic asymmetry), neurological soft-signs (e.g., dysdiadochokinesia), psychophysi-ological anomalies (e.g., as in smooth pursuiteye movements), impaired cognition (e.g., ofattention), language disturbance (e.g., reduced
referential cohesion), and self-report schizo-typy questionnaires (Meehl 1973, 1990). Un-fortunately, the majority of studies we identifiedexamined only a single level of descrip-tion, typically self-report of psychosis-likeexperiences.
Use of a broad range of variables has twodistinct advantages. First, this strategy is muchless vulnerable to artifacts that may be inherentin single measures that operate at a single levelof description (e.g., the LSHS). Second, thisstrategy affords more compelling evidencethat any latent class is meaningfully relatedto the construct researchers are presumingto measure. If the data derive from a singlelevel (e.g., self-report or performance on acontinuous performance test, but not both),confidence that the resulting class reallyrepresents schizophrenia and is etiologicallymeaningful is likely to be a function of howconvinced one is in the construct validity of themeasure. In contrast, if data span the range ofphenotypes, endophenotypes, and even geno-types that are strongly associated with—albeitnot pathognomonic of—schizophrenia, a clearCCK or FMM result would have a much lessconfounded interpretation.
Finally, it is unclear how these statisticalmethods handle nonlinear continua. That is,if the population structure of schizophrenia iscontinuous but the relationship between loadfor schizophrenia—whether genetic (G), envi-ronmental (E), or G × E—and expression ofschizophrenia is not linear, at what point dothese methods convert the nonlinear contin-uum to a class solution? This question is partic-ularly important in light of polygenic accountsof schizophrenia (e.g., Intl. Schizophr. Con-sort. 2009) and arguments in favor of synergis-tic gene-environment interactions (van Os et al.2008).
The Promise of New Discoveries
The restriction of focus to signs and symptomsmeasured by observation and anamnesis starklycontrasts with the opportunities afforded by
412 Linscott · van Os
Ann
u. R
ev. C
lin. P
sych
ol. 2
010.
6:39
1-41
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Col
orad
o -
Bou
lder
on
09/0
5/12
. For
per
sona
l use
onl
y.

ANRV407-CP06-16 ARI 22 February 2010 15:31
new discoveries. In many instances where ev-idence favoring a theory of schizophrenia is ev-ident, authors remark on the potential for re-fining the nosology of schizophrenia throughthe use of alternative genotype or endopheno-type criteria (e.g., Bentall & Fernyhough 2008,Craddock et al. 2006, Intl. Schizophr. Consort.2009, Jansson & Parnas 2007, Owen et al. 2007,Raedler et al. 2007, Stephan et al. 2006, Tsuanget al. 2000a, Uhlhaas et al. 2008, Yolken &Torrey 2008). Whereas the clinical communityis well served by DSM, DSM is not well suitedto the construct validation process (Cronbach& Meehl 1955) that this research communityhopes to see. Yet, scientific explorations of al-ternative diagnostic systems (Tsuang & Faraone2002; Tsuang et al. 2000a,b) and endopheno-types as the basis of classification (Lenzenwegeret al. 2007) have produced dramatic insightsinto the nature of schizophrenia. The consen-sus method for the assessment of neurocogni-tion in schizophrenia (Green & Nuechterlein2004) provides a sort of precedent for the de-velopment of a consensus diagnostic constructvalidation process.
CONCLUSIONS ANDRECOMMENDATIONS
As it stands, the literature on the phenotypes ofschizophrenia suggests discontinuous subpopu-lations underlie a continuum of experience. Thesymptom phenotypes may not be bound by theDSM thresholds but rather may blend imper-ceptibly with subclinical, statistically frequentexperience. Assuming this continuum corre-sponds to a broader notion of schizophrenia,such as load or liability, the population may becomposed of two types of people; those who areliable, some of whom may also have the disor-der, and those who are not.
A raft of limitations and challenges pointsunequivocally to the need to move beyondself-report, observation, and anamnesis of psy-chosis, disorganization, and negative symptomsto address questions on the latent structure
of schizophrenia. Cohort and design variablesplay a major role in evidence of an experiencecontinuum. Tradition and clinical utility pro-vide no guarantees of a scientific epidemiol-ogy of schizophrenia. With a few important ex-ceptions (e.g., Erlenmeyer-Kimling et al. 1989,Lenzenweger et al. 2007), research into popu-lation structure has an entrenched focus on thesame DSM-like phenotypes. Advancing under-standing and treatment is widely understoodto be linked to advances in nosology. Thereis a huge divide between findings formulatedin contemporary theories of schizophrenia andthe (nonevidence-based) way psychosis is con-ceptualized in DSM.
Thus, there is dire need for robust ex-plorations of empirically grounded definitionsof schizophrenia or schizophrenia subtypes;of inclusion of genotypes and endopheno-types as criteria for classification alongsidepsychosis, disorganization, and negative symp-toms; and of classifications linked with candi-date etiologies. Our expectation is that clas-sifications that cater to a fuller picture ofschizophrenia will also stimulate multimodaland multilevel research paradigms that areless vulnerable to the limitations we describeabove.
Pragmatically, carefully constructed tests ofspecific hypotheses on the latent structure ofschizophrenia are required. Large-scale, large-sample studies that endeavor to answer mul-tiple questions simultaneously using variablesspanning the breadth of psychopathology areexpensive ways of finding out a hypothesis iswrong. Instead, the judicious selection of good(inevitably imperfect) variables, the avoidanceof sample biases, and the application of unbi-ased analysis methods are critical. Initial ex-plorations with modest samples can yield im-portant insights (e.g., Blanchard et al. 2005)and may provide the impetus for larger stud-ies. General population surveys of represen-tative samples to test population structurequestions will certainly demand much largersamples.
www.annualreviews.org • Categorical Versus Continuum Models 413
Ann
u. R
ev. C
lin. P
sych
ol. 2
010.
6:39
1-41
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Col
orad
o -
Bou
lder
on
09/0
5/12
. For
per
sona
l use
onl
y.
ANRV407-CP06-16 ARI 22 February 2010 15:31
SUMMARY POINTS
1. Few authors have proposed explanatory models that imply or specify that schizophreniaexists as a discrete latent entity clearly demarcated from other states of psychopathologyas well as from normality.
2. The prevailing viewpoint is that the fundamental processes underpinning schizophreniaare such that there is continuity of experience and population distribution.
3. Intermediate phenotypes of schizophrenia can be readily identified, are more prevalentthan the clinical phenotypes, and are associated with many of the same environmentaland nongenetic risk factors as the clinical phenotypes, implying continuity of experience.
4. Taxometric evidence suggests that although there is continuity of experience, the pop-ulation structure of schizophrenia—defined broadly to include liability states—is notcontinuous with normality.
5. Significant methodological limitations constrain interpretations based on research intocontinuity of experience and population structure.
6. DSM-IV is an important clinical instrument and well suited to clinical practice, but itdoes not meet the basic requirements for a scientific concept on which the epidemiologyof schizophrenia can advance.
FUTURE ISSUES
1. Many authors remark on the potential for refining the nosology of schizophrenia throughthe use of alternative genotype or endophenotype criteria, yet there is currently noconsensus infrastructure promoting sound construct validation of refutable diagnosticconcepts of schizophrenia.
2. Can continuity of experience, or more broadly, continuity of phenotype, be demonstratedusing endophenotype indices, or more broadly, indices that are not based on anamnesisor observation?
3. Can taxonicity in population distributions be demonstrated with indices that span mul-tiple levels of description for the schizophrenia liability?
DISCLOSURE STATEMENT
The authors are not aware of any affiliations, memberships, funding, or financial holdings thatmight be perceived as affecting the objectivity of this review.
LITERATURE CITED
Aleman A, Nieuwenstein MR, Bocker KBE, De Haan EHF. 2001. Multi-dimensionality of hallucinatorypredisposition: factor structure of the Launay-Slade Hallucination Scale in a normal sample. Personal.Individ. Differ. 30:287–92
Am. Psychiatr. Assoc. 1952. Diagnostic and Statistical Manual: Mental Disorders. Washington, DC: Am. Psychiatr.Assoc.
414 Linscott · van Os
Ann
u. R
ev. C
lin. P
sych
ol. 2
010.
6:39
1-41
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Col
orad
o -
Bou
lder
on
09/0
5/12
. For
per
sona
l use
onl
y.

ANRV407-CP06-16 ARI 22 February 2010 15:31
Am. Psychiatr. Assoc. 1968. Diagnostic and Statistical Manual of Mental Disorders. Washington, DC: Am. Psy-chiatr. Assoc. 2nd ed.
Am. Psychiatr. Assoc. 1980. Diagnostic and Statistical Manual of Mental Disorders. Washington, DC: Am. Psy-chiatr. Assoc. 3rd ed.
Am. Psychiatr. Assoc. 1987. Diagnostic and Statistical Manual of Mental Disorders. Washington, DC: Am. Psy-chiatr. Assoc. 3rd ed., rev.
Am. Psychiatr. Assoc. 1994. Diagnostic and Statistical Manual of Mental Disorders. Washington, DC: Am. Psy-chiatr. Assoc. 4th ed.
Am. Psychiatr. Assoc. 2000. Diagnostic and Statistical Manual of Mental Disorders. Washington, DC: Am. Psy-chiatr. Assoc. 4th ed., text rev.
an der Heiden W, Hafner H. 2000. The epidemiology of onset and course of schizophrenia. Eur. Arch.Psychiatry Clin. Neurosci. 250:292–303
Angst J. 2002. Historical aspects of the dichotomy between manic-depressive disorders and schizophrenia.Schizophr. Res. 57:5–13
Beauchaine TP, Lenzenweger MF, Waller NG. 2008. Schizotypy, taxometrics, and disconfirming theories insoft science. Personal. Individ. Differ. 44:1652–62
Beauchaine TP, Waters E. 2003. Pseudotaxonicity in MAMBAC and MAXCOV analyses of rating-scale data:turning continua into classes by manipulating observer’s expectations. Psychol. Methods 8(1):3–15
Bell M. 1997. Cognitively disorganized schizophrenia: a taxometric analysis of PANSS ratings. Schizophr. Res.24(1–2):98
Bell RC, Dudgeon P, McGorry PD, Jackson HJ. 1998. The dimensionality of schizophrenia concepts infirst-episode psychosis. Acta Psychiatr. Scand. 97(5):334–42
Bentall RP, Fernyhough C. 2008. Social predictors of psychotic experience: specificity and psychologicalmechanisms. Schizophr. Bull. 34(6):1012–20
Bentall RP, Slade PD. 1985. Reliability of a scale measuring disposition towards hallucination: a brief report.Personal. Individ. Differ. 6:527–29
Blanchard JJ, Gangestad SW, Brown SA, Horan WP. 2000. Hedonic capacity and schizotypy revisited: Ataxometric analysis of social anhedonia. J. Abnorm. Psychol. 109:87–95
Blanchard JJ, Horan WP, Collins LM. 2005. Examining the latent structure of negative symptoms: Is there adistinct subtype of negative symptom schizophrenia? Schizophr. Res. 77(2–3):151–65
Bonett DG. 2007. Transforming odds ratios into correlations for meta-analytic research. Am. Psychol.62(3):254–55
Bromet EJ, Fennig S. 1999. Epidemiology and natural history of schizophrenia. Biol. Psychiatry 46(7):871–81Brown JS Jr. 2009. Effects of bisphenol-A and other endocrine disruptors compared with abnormalities of
schizophrenia: an endocrine-disruption theory of schizophrenia. Schizophr. Bull. 35(1):256–78Burton R. 1628. The Anatomy of Melancholy. London: J. M. DentCarpenter WT Jr, Heinrichs DW, Wagman AMI. 1988. Deficit and nondeficit forms of schizophrenia: the
concept. Am. J. Psychiatry 145:578–83Cheng JYW, Ko JSN, Chen RYL, Ng EML. 2008. Meta-regression analysis using latitude as moderator of
paternal age related schizophrenia risk: High ambient temperature induced de novo mutations or is itrelated to the cold? Schizophr. Res. 99(1–3):71–76
Claridge G. 1997. Theoretical background and issues. In Schizotypy: Implications for Illness and Health, ed. GClaridge, pp. 3–18. New York: Oxford Univ. Press
Craddock N, O’Donovan MC, Owen MJ. 2006. Genes for schizophrenia and bipolar disorder? Implicationsfor psychiatric nosology. Schizophr. Bull. 32(1):9–16
Cronbach LJ, Meehl PE. 1955. Construct validity in psychological tests. Psychol. Bull. 52(4):281–302Crow TJ. 1990. The continuum of psychosis and its genetic origins: the sixty-fifth Maudsley lecture. Br. J.
Psychiatry 156:788–97Crow TJ. 1991. The failure of the Kraepelinian binary concept and the search for the psychosis gene. In
Concepts of Mental Disorder: A Continuing Debate, ed. A Kerr, H McClelland, pp. 31–47. London: Roy.Coll. Psychiatr.
Crow TJ. 1995. A continuum of psychosis, one human gene, and not much else—the case of homogeneity.Schizophr. Res. 17:135–45
www.annualreviews.org • Categorical Versus Continuum Models 415
Ann
u. R
ev. C
lin. P
sych
ol. 2
010.
6:39
1-41
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Col
orad
o -
Bou
lder
on
09/0
5/12
. For
per
sona
l use
onl
y.

ANRV407-CP06-16 ARI 22 February 2010 15:31
Crow TJ. 1998. From Kraepelin to Kretschmer leavened by Schneider: the transition from categories ofpsychosis to dimensions of variation intrinsic to Homo sapiens. Arch. Gen. Psychiatry 55:502–4
Crow TJ. 2000. Schizophrenia as the price that Homo sapiens pays for language: a resolution of the centralparadox in the origin of the species. Brain Res. Rev. 31:118–29
Crow TJ. 2008. The “big bang” theory of the origin of psychosis and the faculty of language. Schizophr. Res.102(1–3):31–52
Cuesta MJ, Ugarte MD, Goicoa T, Eraso S, Peralta V. 2007. A taxometric analysis of schizophrenia symptoms.Psychiatry Res. 150(3):245–53
Curtis VA, van Os J, Murray RM. 2000. The Kraepelinian dichotomy: evidence from developmental andneuroimaging studies. J. Neuropsychiatry Clin. Neurosci. 12(3):398–405
Erlenmeyer-Kimling L, Golden RR, Cornblatt BA. 1989. A taxometric analysis of cognitive and neuromotorvariables in children at risk for schizophrenia. J. Abnorm. Psychol. 98(3):203–8
Faraone SV, Tsuang MT. 1994. Measuring diagnostic accuracy in the absence of a “gold standard.” Am. J.Psychiatry 151(5):650–57
Fossati A, Raine A, Borroni S, Maffei C. 2007. Taxonic structure of schizotypal personality in nonclinicalsubjects: issues of replicability and age consistency. Psychiatry Res. 152(2–3):103–12
Gift TE, Strauss JS, Ritzler BA, Kokes RF, Harder DW. 1980. How diagnostic concepts of schizophreniadiffer. J. Nerv. Ment. Dis. 168(1):3–8
Green MF, Nuechterlein KH. 2004. The MATRICS initiative: developing a consensus cognitive battery forclinical trials. Schizophr. Res. 72(1):1–3
Greene T. 2007. The Kraepelinian dichotomy: the twin pillars crumbling? Hist. Psychiatry 18(3):361–79Hafner H. 2000. Epidemiology of schizophrenia. a thriving discipline at the turn of the century. Eur. Arch.
Psychiatry Clin. Neurosci. 250:271–73Heinrichs RW, Zakzanis KK. 1998. Neurocognitive deficit in schizophrenia: a quantitative review of the
evidence. Neuropsychology 12:426–45Hennah W, Thomson P, Peltonen L, Porteous D. 2006. Beyond schizophrenia: the role of DISC1 in major
mental illness. Schizophr. Bull. 32(3):409–16Horan WP, Blanchard JJ, Gangestad SW, Kwapil TR. 2004. The psychometric detection of schizotypy: Do
putative schizotypy indicators identify the same latent class? J. Abnorm. Psychol. 113(3):339–57Howes OD, Kapur S. 2009. The dopamine hypothesis of schizophrenia: version III—the final common
pathway. Schizophr. Bull. 35(3):549–62Intl. Schizophr. Consort. 2009. Common polygenic variation contributes to risk of schizophrenia and bipolar
disorder. Nature 460:748–52Jablensky A. 2000. Epidemiology of schizophrenia: the global burden of disease and disability. Eur. Arch.
Psychiatry Clin. Neurosci. 250(6):274–85Jansson LB, Parnas J. 2007. Competing definitions of schizophrenia: What can be learned from polydiagnostic
studies? Schizophr. Bull. 33(5):1178–200Johns LC, Cannon M, Singleton N, Murray RM, Farrell M, et al. 2004. Prevalence and correlates of self-
reported psychotic symptoms in the British population. Br. J. Psychiatry 185:298–305Johns LC, Nazroo JY, Bebbington P, Kuipers E. 2002. Occurrence of hallucinatory experiences in a community
sample and ethnic variations. Br. J. Psychiatry 180:174–78Jones SR, Fernyhough C. 2007. A new look at the neural diathesis–stress model of schizophrenia: the primacy
of social evaluative and uncontrollable situations. Schizophr. Bull. 33(5):1171–77Keller F, Jahn T, Klein C. 2001. Anwendung von taxometrischen methoden und von mischverteilungsmod-
ellen zur erfassung der schizotypie. In Schizotypie: Psychometrische Entwicklungen und BiopsychologischeForschungsansatze, ed. B Andresen, R Maß, pp. 391–412. Gottingen, Germany: Hogrefe
Kirkpatrick B, Buchanan RW, Ross DE, Carpenter WT Jr. 2001. A separate disease within the syndrome ofschizophrenia. Arch. Gen. Psychiatry 58:165–71
Kirkpatrick B, Messias E, Harvey PD, Fernandez-Egea E, Bowie CR. 2008. Is schizophrenia a syndrome ofaccelerated aging? Schizophr. Bull. 34(6):1024–32
Korfine L, Lenzenweger MF. 1995. The taxonicity of schizotypy: a replication. J. Abnorm. Psychol. 104:26–31Kretschmer E. 1936. Physique and Character: An Investigation of the Nature of Constitution and of the Theory of
Temperament. London: Kegan, Paul, Trench, Trubner
416 Linscott · van Os
Ann
u. R
ev. C
lin. P
sych
ol. 2
010.
6:39
1-41
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Col
orad
o -
Bou
lder
on
09/0
5/12
. For
per
sona
l use
onl
y.

ANRV407-CP06-16 ARI 22 February 2010 15:31
Larøi F, Marczewski P, Van Der Linden M. 2004. Further evidence of the multi-dimensionality of hallucinatorypredisposition: factor structure of a modified version of the Launay-Slade Hallucinations Scale in a normalsample. Eur. Psychiatry 19(1):15–20
Launay G, Slade PD. 1981. The measurement of hallucinatory predisposition in male and female prisoners.Personal. Individ. Differ. 2:221–34
Lenzenweger MF. 1999. Deeper into the schizotypy taxon: on the robust nature of maximum covarianceanalysis. J. Abnorm. Psychol. 108:182–87
Lenzenweger MF. 2006. Schizotaxia, schizotypy, and schizophrenia: Paul E. Meehl’s blueprint for the exper-imental psychopathology and genetics of schizophrenia. J. Abnorm. Psychol. 115(2):195–200
Lenzenweger MF, Korfine L. 1992. Confirming the latent structure and base rate of schizotypy: a taxometricanalysis. J. Abnorm. Psychol. 101:567–71
Lenzenweger MF, McLachlan G, Rubin DB. 2007. Resolving the latent structure of schizophrenia endophe-notypes using expectation-maximization-based finite mixture modeling. J. Abnorm. Psychol. 116(14):16–29
Liddle PF. 1987. The symptoms of chronic schizophrenia: a re-examination of the positive-negative dichotomy.Br. J. Psychiatry 151:145–51
Linscott RJ. 2007. The latent structure and coincidence of hypohedonia and schizotypy and their validity asindices of psychometric risk for schizophrenia. J. Personal. Disord. 21(3):225–42
Linscott RJ, Allardyce J, van Os J. 2009a. Seeking verisimilitude in a class: a systematic review of evidence thatthe criterial clinical symptoms of schizophrenia are taxonic. Schizophr. Bull. In press
Linscott RJ, Lenzenweger MF, van Os J. 2009b. Continua or classes? Vexed questions on the latent structure ofschizophrenia. In Advances in Schizophrenia Research: Search for the Causes of Schizophrenia, ed. WF Gattaz,GF Busatto, pp. 333–56. New York: Springer
Linscott RJ, Marie D, Arnott KL, Clark BL. 2006. Over-representation of Maori New Zealanders amongadolescents in a schizotypy taxon. Schizophr. Res. 84(2–3):289–96
Maher BA, Maher WB. 1994. Personality and psychopathology: a historical perspective. J. Abnorm. Psychol.103:72–77
Malaspina D, Harlap S, Fennig S, Heiman D, Nahon D, et al. 2001. Advancing paternal age and the risk ofschizophrenia. Arch. Gen. Psychiatry 58:361–67
Mao Y, Ge X, Frank CL, Madison JM, Koehler AN, et al. 2009. Disrupted in Schizophrenia 1 regulatesneuronal progenitor proliferation via modulation of GSK3β/β-catenin signaling. Cell 136(6):1017–31
Maraun MD, Slaney K. 2005. An analysis of Meehl’s MAXCOV-HITMAX procedure for the case of contin-uous indicators. Multivar. Behav. Res. 40(4):489–518
McClellan JM, Susser E, King M-C. 2006. Maternal famine, de novo mutations, and schizophrenia. JAMA296(5):582–84
McClellan JM, Susser E, King M-C. 2007. Schizophrenia: a common disease caused by multiple rare alleles.Br. J. Psychiatry 190:194–99
McGorry PD. 2007. Issues for DSM-V. Clinical staging: a heuristic pathway to valid nosology and safer, moreeffective treatment in psychiatry. Am. J. Psychiatry 164(6):859–60
McGorry PD, Hickie IB, Yung AR, Pantelis C, Jackson HJ. 2006. Clinical staging of psychiatric disorders:a heuristic framework for choosing earlier, safer and more effective interventions. Aust. NZ J. Psychiatry40:616–22
McGrath J, Saha S, Chant D, Welham J. 2008. Schizophrenia: a concise overview of incidence, prevalence,and mortality. Epidemiol. Rev. 30:67–76
Meehl PE. 1962. Schizotaxia, schizotypy, schizophrenia. Am. Psychol. 17:827–38Meehl PE. 1973. MAXCOV-HITMAX: a taxonomic search method for loose genetic syndromes. In Psychodi-
agnosis: Selected Papers, ed. PE Meehl, pp. 200–24. Minneapolis: Univ. Minn. PressMeehl PE. 1990. Toward an integrated theory of schizotaxia, schizotypy, and schizophrenia. J. Personal. Disord.
4:1–99Meehl PE. 1999. Clarifications about taxometric method. Appl. Prev. Psychol. 8:165–74Meehl PE. 2001. Primary and secondary hypohedonia. J. Abnorm. Psychol. 110:188–93Meehl PE. 2004. What’s in a taxon? J. Abnorm. Psychol. 113(1):39–43Messias EL, Chen C-Y, Eaton WW. 2007. Epidemiology of schizophrenia: review of findings and myths.
Psychiatr. Clin. N. Am. 30(3):323–38
www.annualreviews.org • Categorical Versus Continuum Models 417
Ann
u. R
ev. C
lin. P
sych
ol. 2
010.
6:39
1-41
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Col
orad
o -
Bou
lder
on
09/0
5/12
. For
per
sona
l use
onl
y.

ANRV407-CP06-16 ARI 22 February 2010 15:31
Meyer TD, Keller F. 2001. Exploring the latent structure of the perceptual aberration, magical ideation, andphysical anhedonia scales in a German sample. J. Personal. Disord. 15:521–35
Miller R. 2008. A Neurodynamic Theory of Schizophrenia and Related Disorders. Morrisville, NC: Lulu Inc.Murray RM, Jones PB, Susser E, van Os J, Cannon M, eds. 2003. The Epidemiology of Schizophrenia. London:
Cambridge Univ. PressMurray RM, O’Callaghan E. 1991. The congenital and adult-onset psychoses: Kraepelin lost, Kraepelin found.
In Concepts of Mental Disorder: A Continuing Debate, ed. A Kerr, H McClelland, pp. 48–65. London: GaskellMuthen B, Asparouhov T. 2006. Item response mixture modeling: application to tobacco dependence criteria.
Addict. Behav. 31:1050–66Ovsiew F. 2000. An end to Kraepelinian nosology? J. Neuropsychiatry Clin. Neurosci. 12(3):297–99Owen MJ, Craddock N, Jablensky A. 2007. The genetic deconstruction of psychosis. Schizophr. Bull. 33(4):905–
11Peralta V, Cuesta MJ. 2005. The underlying structure of diagnostic systems of schizophrenia: a comprehensive
polydiagnostic approach. Schizophr. Res. 79(2–3):217–29R Dev. Core Team. 2004. R: A Language and Environment for Statistical Computing. Vienna, Austria: R Found.
Statist. Comput.Raedler TJ, Bymaster FB, Tandon R, Copolov D, Dean B. 2007. Towards a muscarinic hypothesis of
schizophrenia. Mol. Psychiatry 12:232–46Rawlings D, Williams B, Haslam N, Claridge G. 2008. Taxometric analysis supports a dimensional latent
structure for schizotypy. Personal. Individ. Differ. 44:1640–51Rossler W, Riecher-Rossler A, Angst J, Murray R, Gamma A, et al. 2007. Psychotic experiences in the general
population: a twenty-year prospective community study. Schizophr. Res. 92(1–3):1–14Saha S, Chant D, McGrath J. 2008. Meta-analyses of the incidence and prevalence of schizophrenia: conceptual
and methodological issues. Int. J. Methods Psychiatr. Res. 17(1):55–61Saha S, Chant D, Welham J, McGrath J. 2005. A systematic review of the prevalence of schizophrenia. PLoS
Med. 2(5):e141, 413–33Schultze-Lutter F. 2009. Subjective symptoms of schizophrenia in research and the clinic: the basic symptom
concept. Schizophr. Bull. 35(1):5–8Schurhoff F, Golmard J-L, Szoke A, Bellivier F, Berthier A, et al. 2004. Admixture analysis of age at onset in
schizophrenia. Schizophr. Res. 71(1):35–41Spitzer RL, Endicott J, Robins E. 1978. Research Diagnostic Criteria (RDC) for a Selected Group of Functional
Disorders. New York: NIMH Clin. Res. Branch Collab. Prog.Stefanis NC, Delespaul P, Smyrnis N, Lembesi A, Avramopoulos DA, et al. 2004. Is the excess risk of psychosis-
like experiences in urban areas attributable to altered cognitive development? Soc. Psychiatry Psychiatr.Epidemiol. 39(5):364–68
Stephan KE, Baldeweg T, Friston KJ. 2006. Synaptic plasticity and dysconnection in schizophrenia. Biol.Psychiatry 59(10):929–39
Stone JM, Morrison PD, Pilowsky LS. 2007. Glutamate and dopamine dysregulation in schizophrenia—asynthesis and selective review. J. Psychopharmacol. 21(4):440–52
Strauss JS. 1969. Hallucinations and delusions as points on continua function: rating scale evidence. Arch. Gen.Psychiatry 21:581–86
Tandon R, Keshavan MS, Nasrallah HA. 2008. Schizophrenia, “just the facts” what we know in 2008. 2.Epidemiology and etiology. Schizophr. Res. 102(1–3):1–18
Tsuang MT, Faraone SV. 2002. Diagnostic concepts and the prevention of schizophrenia. Can. J. Psychiatry47:515–17
Tsuang MT, Stone WS, Faraone SV. 2000a. Toward reformulating the diagnosis of schizophrenia. Am. J.Psychiatry 157:1041–50
Tsuang MT, Stone WS, Faraone SV. 2000b. Towards the prevention of schizophrenia. Biol. Psychiatry 48:349–56
Tyrka AR, Cannon TD, Haslam N, Mednick SA, Schulsinger F, et al. 1995. The latent structure of schizotypy:I. Premorbid indicators of a taxon of individuals at risk for schizophrenia-spectrum disorders. J. Abnorm.Psychol. 104:173–83
418 Linscott · van Os
Ann
u. R
ev. C
lin. P
sych
ol. 2
010.
6:39
1-41
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Col
orad
o -
Bou
lder
on
09/0
5/12
. For
per
sona
l use
onl
y.

ANRV407-CP06-16 ARI 22 February 2010 15:31
Uhlhaas PJ, Haenschel C, Nikolic D, Singer W. 2008. The role of oscillations and synchrony in corticalnetworks and their putative relevance for the pathophysiology of schizophrenia. Schizophr. Bull. 34(5):927–43
van Kampen D. 1999. Genetic and environmental influences on preschizophrenic personality: MAXCOV-HITMAX and LISREL analyses. Eur. J. Personal. 13(1):63–80
van Os J, Hanssen M, Bijl RV, Ravelli A. 2000. Strauss (1969) revisited: a psychosis continuum in the generalpopulation? Schizophr. Res. 45(1–2):11–20
van Os J, Linscott RJ, Myin-Germeys I, Delespaul P, Krabbendam L. 2009. A systematic review and meta-analysis of the psychosis continuum: evidence for a psychosis proneness-persistence-impairment modelof psychotic disorder. Psychol. Med. 39(2):179–95
van Os J, Rutten BPF, Poulton R. 2008. Gene-environment interactions in schizophrenia: review of epidemi-ological findings and future directions. Schizophr. Bull. 34(6):1066–82
van Os J, Verdoux H. 2003. Diagnosis and classification of schizophrenia: categories versus dimensions,distributions versus disease. In The Epidemiology of Schizophrenia, ed. RM Murray, PB Jones, E Susser,J van Os, M Cannon, pp. 364–410. London: Cambridge Univ. Press
van Winkel R, Stefanis NC, Myin-Germeys I. 2008. Psychosocial stress and psychosis. A review of the neu-robiological mechanisms and the evidence for gene-stress interaction. Schizophr. Bull. 34(6):1095–105
Walker EF, Mittal V, Tessner K. 2008. Stress and the hypothalamic pituitary adrenal axis in the developmentalcourse of schizophrenia. Annu. Rev. Clin. Psychol. 4:189–216
Waller NG, Meehl PE. 1998. Multivariate Taxometric Procedures: Distinguishing Types From Continua. ThousandOaks, CA: Sage
Wan MW, Abel KM, Green J. 2008. The transmission of risk to children from mothers with schizophrenia:a developmental psychopathology model. Clin. Psychol. Rev. 28:613–37
Welham J, McLachlan G, Davies G, McGrath J. 2000. Heterogeneity in schizophrenia; mixture modelling ofage-at-first-admission, gender and diagnosis. Acta Psychiatr. Scand. 101:312–17
White T, Cullen K, Rohrer LM, Karatekin C, Luciana M, et al. 2008. Limbic structures and networks inchildren and adolescents with schizophrenia. Schizophr. Bull. 34(1):18–29
Wiles NJ, Zammit S, Bebbington P, Singleton N, Meltzer H, Lewis G. 2006. Self-reported psychotic symp-toms in the general population: results from the longitudinal study of the British National PsychiatricMorbidity Survey. Br. J. Psychiatry 188:519–26
Williams HJ, Owen MJ, O’Donovan MC. 2007. Is COMT a susceptibility gene for schizophrenia? Schizophr.Bull. 33(3):635–41
World Health Org. 2004. ICD-10: International Statistical Classification of Diseases and Related Health Problems,Tenth Revision. Geneva: World Health Org. 2nd ed.
Yolken RH, Torrey EF. 2008. Are some cases of psychosis caused by microbial agents? A review of the evidence.Mol. Psychiatry 13:470–79
Zammit S, Lewis S, Gunnell D, Smith GD. 2007. Schizophrenia and neural tube defects: comparisons froman epidemiological perspective. Schizophr. Bull. 33(4):853–58
www.annualreviews.org • Categorical Versus Continuum Models 419
Ann
u. R
ev. C
lin. P
sych
ol. 2
010.
6:39
1-41
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Col
orad
o -
Bou
lder
on
09/0
5/12
. For
per
sona
l use
onl
y.

AR407-FM ARI 6 March 2010 12:23
Annual Review ofClinical Psychology
Volume 6, 2010 Contents
Personality Assessment from the Nineteenth to Early Twenty-FirstCentury: Past Achievements and Contemporary ChallengesJames N. Butcher � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 1
Prescriptive Authority for PsychologistsRobert E. McGrath � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �21
The Admissibility of Behavioral Science Evidence in the Courtroom:The Translation of Legal to Scientific Concepts and BackDavid Faust, Paul W. Grimm, David C. Ahern, and Mark Sokolik � � � � � � � � � � � � � � � � � � � � � �49
Advances in Analysis of Longitudinal DataRobert D. Gibbons, Donald Hedeker, and Stephen DuToit � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �79
Group-Based Trajectory Modeling in Clinical ResearchDaniel S. Nagin and Candice L. Odgers � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 109
Measurement of Functional Capacity: A New Approach toUnderstanding Functional Differences and Real-World BehavioralAdaptation in Those with Mental IllnessThomas L. Patterson and Brent T. Mausbach � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 139
The Diagnosis of Mental Disorders: The Problem of ReificationSteven E. Hyman � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 155
Prevention of Major DepressionRicardo F. Munoz, Pim Cuijpers, Filip Smit, Alinne Z. Barrera, and Yan Leykin � � � � � � 181
Issues and Challenges in the Design of Culturally AdaptedEvidence-Based InterventionsFelipe Gonzalez Castro, Manuel Barrera Jr., and Lori K. Holleran Steiker � � � � � � � � � � � � 213
Treatment of PanicNorman B. Schmidt and Meghan E. Keough � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 241
Psychological Approaches to Origins and Treatments of SomatoformDisordersMichael Witthoft and Wolfgang Hiller � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 257
vi
Ann
u. R
ev. C
lin. P
sych
ol. 2
010.
6:39
1-41
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Col
orad
o -
Bou
lder
on
09/0
5/12
. For
per
sona
l use
onl
y.

AR407-FM ARI 6 March 2010 12:23
Cognition and Depression: Current Status and Future DirectionsIan H. Gotlib and Jutta Joorman � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 285
The Genetics of Mood DisordersJennifer Y.F. Lau and Thalia C. Eley � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 313
Self-InjuryMatthew K. Nock � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 339
Substance Use in Adolescence and Psychosis: Clarifying theRelationshipEmma Barkus and Robin M. Murray � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 365
Systematic Reviews of Categorical Versus Continuum Models inPsychosis: Evidence for Discontinuous Subpopulations Underlyinga Psychometric Continuum. Implications for DSM-V, DSM-VI,and DSM-VIIRichard J. Linscott and Jim van Os � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 391
Pathological Narcissism and Narcissistic Personality DisorderAaron L. Pincus and Mark R. Lukowitsky � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 421
Behavioral Treatments in Autism Spectrum Disorder:What Do We Know?Laurie A. Vismara and Sally J. Rogers � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 447
Clinical Implications of Traumatic Stress from Birth to Age FiveAnn T. Chu and Alicia F. Lieberman � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 469
Emotion-Related Self-Regulation and Its Relation to Children’sMaladjustmentNancy Eisenberg, Tracy L. Spinrad, and Natalie D. Eggum � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 495
Successful Aging: Focus on Cognitive and Emotional HealthColin Depp, Ipsit V. Vahia, and Dilip Jeste � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 527
Implicit Cognition and Addiction: A Tool for Explaining ParadoxicalBehaviorAlan W. Stacy and Reineout W. Wiers � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 551
Substance Use Disorders: Realizing the Promise of Pharmacogenomicsand Personalized MedicineKent E. Hutchison � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 577
Update on Harm-Reduction Policy and Intervention ResearchG. Alan Marlatt and Katie Witkiewitz � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 591
Violence and Women’s Mental Health: The Impact of Physical, Sexual,and Psychological AggressionCarol E. Jordan, Rebecca Campbell, and Diane Follingstad � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 607
Contents vii
Ann
u. R
ev. C
lin. P
sych
ol. 2
010.
6:39
1-41
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Col
orad
o -
Bou
lder
on
09/0
5/12
. For
per
sona
l use
onl
y.