systematic review of early intensive behavioral interventions for children with autism
TRANSCRIPT

� American Association on Intellectual and Developmental Disabilities 23
VOLUME 114, NUMBER 1: 23–41 � JANUARY 2009 AJIDD
Systematic Review of Early Intensive BehavioralInterventions for Children With Autism
Patricia Howlin and Iliana MagiatiInstitute of Psychiatry, King’s College (London, UK)
Tony CharmanUniversity College, London, Institute of Child Health
AbstractRecent reviews highlight limitations in the evidence base for early interventions for childrenwith autism. We conducted a systematic review of controlled studies of early intensivebehavioral interventions (EIBI) for young children with autism. Eleven studies met inclu-sion criteria (including two randomized controlled trials). At group level, EIBI resulted inimproved outcomes (primarily measured by IQ) compared to comparison groups. At anindividual level, however, there was considerable variability in outcome, with some evi-dence that initial IQ (but not age) was related to progress. This review provides evidencefor the effectiveness of EIBI for some, but not all, preschool children with autism.
DOI: 10.1352/2009.114:23–41
Over the past 2 decades, there has been in-creasing interest in developing effective interven-tions for young children with autism spectrumdisorder. In addition to the many largely untested‘‘alternative’’ therapies (from acupuncture to Zincsupplements; see Research Autism, 2007), a widerange of more soundly based psychoeducationalprograms has been employed. These tend to in-corporate a mix of behavioral, developmental, andeducational approaches (for reviews, see NationalResearch Council, 2001; Scottish IntercollegiateGuidelines Network [SIGN], 2007), and althoughmethods vary, the general goal of such programsis to enhance cognitive, communication, and so-cial skills while minimizing autistic symptomatol-ogy and other problem behaviors. Three mainstrands of intervention have been the focus in themajority of studies conducted to date: programsthat have a specific focus on communication;those in which developmental/educational strate-gies have been employed, and those with a par-ticular emphasis on the use of behavioral princi-ples to improve learning and behavior.
In terms of communication-focused interven-
tions, programs such as the Picture ExchangeCommunication System (Bondy & Frost, 1998)and other alternative/augmentative communica-tion systems were designed in an attempt to pro-vide a communication modality for children whohave no spoken language (see Howlin, 2006).Other programs, designed for both nonverbal andverbal children, use approaches informed by psy-cholinguistic theory to target the early interactionsbetween parents and newly diagnosed children inorder to enhance nonverbal and verbal commu-nication. These include parent communicationtraining approaches (Aldred, Green, & Adams,2004; Drew et al, 2002); More Than Words (Suss-man, 1999), Early Bird (Shields, 2001), and Pre-Linguistic Milieu Therapy (Yoder & Stone, 2006).In addition, there are numerous developmentaland educational programs that combine aspects ofdevelopmental, educational, and behavioral ap-proaches, including Daily Life Therapy (Quill,Gurry, & Larkin, 1989); the Denver Model (Rog-ers et al., 2006); the Douglass Developmental Dis-abilities Center program (Handleman, Harris, Ar-nold, Gordon, & Cohen, 2006); Floor Time/De-

24 � American Association on Intellectual and Developmental Disabilities
VOLUME 114, NUMBER 1: 23–41 � JANUARY 2009 AJIDD
Early intensive behavioral interventions P. Howlin, I. Magiati, and T. Charman
velopmental, Individual Difference Relationshipmodel (Greenspan & Wieder, 2003); Son-Rise(Kaufman, 1994); TEACCH (Treatment and Ed-ucation of Autistic and Communication Handi-capped Children; Schopler, 1997), and manymore.
Although all these programs employ some-what different methodologies, they also have im-portant elements in common; for example, tech-niques developed from learning theory (Skinner,1953) are essential components of most. Operantapproaches, as exemplified in the Applied Behav-ior Analysis (ABA) approach (Dunlap, Kern-Dun-lap, Clark, & Robbins, 1991) are particularly fun-damental to behavioral techniques such as PivotalResponse Training (Schreibman & Koegel, 2005),Discrete Trial Training (Maurice, Green, & Luce,1996) and Verbal Behavior (Barbera & Rasmussen,2007) that form part of many modern-day earlyintervention programs for children with autism.
Recently, reviewers of intervention programsfor children with autism have been critical of thestandards of research in this field, pointing to var-ious methodological limitations and failures of ex-perimental design (Levy, Kim, & Olive, 2006;Scottish Intercollegiate Guidelines, 2007; Wheel-er, Blaggett, Fox, & Blevins, 2006). However, thereis also widespread agreement that interventionsbased on ABA, particularly those involving hometherapy and beginning in the preschool years,have been most comprehensively studied and, asa consequence, have the best established evidencebase (Lord et al., 2005; National Research Coun-cil, 2001; Smith, Donahoe, & Davis, 2006).Among the most thoroughly evaluated are pro-grams involving early intensive home-based be-havioral intervention (EIBI). The EIBI approachunderlies the UCLA Young Autism Project, orig-inally developed by Lovaas and his colleagues(1981). Other more recently developed EIBI pro-grams include those described by Maurice, Green,and Luce (1996), Maurice, Green, and Foxx(2001), and Handleman et al. (2006).
Lovaas was among the earliest researchers todemonstrate the effectiveness of behavioral inter-ventions for children with autism and was alsoone of the first to stress the importance of paren-tal involvement in therapy. Proponents of EIBIrecommend that therapy should begin as early aspossible, preferably before the age of 3 years,should take place for approximately 40 hours perweek and last at least 2 years. The programs arehighly prescriptive, with detailed manuals provid-
ed to guide and monitor treatment. Learning ses-sions are provided in a one-to-one discrete trialformat, focusing on the systematic teaching ofmeasurable behavioral units, repetitive practice,and structured presentation of tasks from the mostsimple to the more complex. It has now been 2decades since Lovaas (1987) published his originalpaper on the effectiveness of EIBI, reporting thatpreschool children involved in 1:1 therapy for 40or more hours a week, over at least 2 years,showed major gains (of up to 30 points) in IQ;rates of integration in mainstream school in-creased significantly; and 47% of children weredescribed as attaining ‘‘normal intellectual and ed-ucational functioning (p. 3).’’ A subsequent fol-low-up (McEachin, Smith, & Lovaas, 1993) alsoconfirmed that the gains were maintained intoearly adolescence.
Although in some quarters this study washailed as ‘‘a triumph of behavioral science andbehaviorally scientific clinical application’’ (Baer,1993, p. 373), critics highlighted problems in ex-perimental design (particularly with regard to non-random assignment and intelligence test–retestmeasures) and the practical and financial difficul-ties of replication given the intensity of the pro-gram. It was claims of ‘‘normal functioning,’’however, that gave rise to most contention (Mes-ibov, 1993; Mundy, 1993). This was partly due tothe limited range of assessments employed onwhich to base judgments of ‘‘normality’’ but alsobecause the figure of 47% showing ‘‘normal func-tioning’’ (McEachin et al., 1993, p. 367) repre-sented only 9 out of 19 children. Smith et al.(2001) noted that the 9 children classified as hav-ing normal functioning accounted for most of thegains in IQ. This subgroup showed an average IQincrease of 37 points compared with an averageincrease of 3 points for the other 10 children.Moreover, Shea (2004) pointed out that the pub-lished data from the studies of Lovaas (1987) andMcEachin et al. (1993) indicated that on the in-struments used, only one child had test scores thatwere all within the average range.
The extent of involvement required by par-ents and therapists to follow the UCLA EIBI pro-gram for the recommended number of hours hasrestricted opportunities for replication, and in thefew studies that have been conducted, researchershave generally used a modified version of thismodel. Nevertheless, a number of replications (orat least partial replications) of the original studyhas now been undertaken, and although many do

� American Association on Intellectual and Developmental Disabilities 25
VOLUME 114, NUMBER 1: 23–41 � JANUARY 2009 AJIDD
Early intensive behavioral interventions P. Howlin, I. Magiati, and T. Charman
not report gains of the magnitude reported by Lo-vaas (1987) or McEachin et al. (1993), the resultshave generally been positive.
Although there have been previous reviews ofearly interventions for children with autism (Lordet al., 2005; Rogers, 1998; Smith, Eikeseth, Klev-strand, & Lovaas, 2007), there have been manynew controlled studies in recent years (Rogers’1998 review, for example, appeared before 8 of the11 studies reviewed here were published). Thus,an updated review is required in order to take ac-count of the new evidence reported. In this sys-tematic review, we examined the findings fromcontrolled EIBI studies published in peer-reviewedjournals. Our goal was to examine what conclu-sions can be drawn from research conducted todate and to identify the challenges for future re-searchers.
Method
The following databases were searched forpeer-reviewed papers from 1985 to May 2007:MEDLINE, EMBASE, Cochrane, PSYCHINFO,CINAHL, ERIC, using the terms autism/autistic/autism spectrum disorder and intervention/early inter-vention/behavio(u)ral intervention/EIBI/ABA. Ad-ditional sources of information were the UnitedKingdom National Autistic Society Research Au-tism website; international reviews published bythe New York State Department of Health EarlyIntervention Program (1999); the state of Maine(Maine Administrators of Services for ChildrenWith Disabilities (Maine, 1999); National Re-search Council (2001); National Initiative for Au-tism: Screening and Assessment (2003); Universi-ty of Sydney (Roberts, 2004); New Zealand Min-istry of Health (2006); and National Health Ser-vice (NHS) Scotland (Scottish IntercollegiateGuidelines Network, 2007). The inclusion criteriafor the review were (a) case-control comparisonstudy (not necessarily randomized design) of EIBIfor children with autism; (b) UCLA-affiliated(home- or center-based) or other home-based EIBIprogram largely based on the UCLA model (notnecessarily for 40 hours per week); (c) minimumof 10 participants in EIBI group; (d) age at startof treatment less than 6 years; (e) interventionminimum 12 hours per week; (e) duration mini-mum 12 months; (f) adequate data on IQ or otherstandard measures to allow calculation of extentof gains.
Results
In total, we identified 641 studies that met thesearch term combinations. We excluded studies inwhich the title indicated clearly that the study wasof a single case or a case series without a compar-ison group and studies with a focus on a specificbehavior(s) (e.g., sleeping problems, challengingbehavior), the use of pharmacological interven-tions or other non-ABA programs, or on out-comes for/views of therapists or parents. Abstractsof review papers were checked, and if these werereviews of ABA/EIBI with participants who hadautism their reference lists were further scrutinizedfor possible papers to include. We initially iden-tified 37 papers that appeared to meet criteria forinclusion; 8 of these were overviews of researchin the area or commentaries on previously pub-lished studies; 5 were non-EIBI or a mix of EIBIand other behavioral interventions; 11 had no re-ported IQs and/or no comparison group and/orhad fewer than 10 participants. Thirteen studies(indicated in boldface in the References) met all in-clusion criteria; 2 of them (Eikeseth, Smith, Jahr,& Eldevik, 2007; McEachin et al., 1993) were ex-tensions of previous reports (Eikeseth, Smith,Jahr, & Eldevik, 2002; Lovaas, 1987, respectively).These are presented as single outcome reports (seeTable 1). Only one study (Smith, Groen, &Wynn, 2000) was a fully randomized control trial.Because data were not available for individual par-ticipants, the following summaries/analyses arebased on comparisons of the published groupmeans. All but 4 studies (Eikeseth et al., 2007,2006; Magiati, Charman, & Howlin, 2007; Rem-ington et al., 2007) were carried out in the UnitedStates.
Characteristics of Participants and TherapeuticInterventions
Diagnostic measures varied across studies,with most relying on clinical judgments based onDiagnostic and Statistical Manual of Mental Disor-ders/International Classification of Diseases criteria.Six studies (Cohen, Amerine-Dickens, & Smith,2006; Eikeseth et al., 2002, 2007; Eldevik, Eike-seth, Jahr, & Smith, 2006; Magiati et al., 2007;Remington et al., 2007; Sallows, & Graupner,2005) used the Autism Diagnostic Interview-Revised ADI-R (Lord, Rutter, & le Couteur,1994) to confirm diagnosis. Reported diagnosesincluded children with autism, autism spectrumdisorder, and pervasive developmental disorder.

26 � American Association on Intellectual and Developmental Disabilities
VOLUME 114, NUMBER 1: 23–41 � JANUARY 2009 AJIDD
Early intensive behavioral interventions P. Howlin, I. Magiati, and T. Charman
Tabl
e1.
Sum
mar
yof
Inte
rven
tion
and
Part
icip
ant
Cha
ract
eris
tics
Stud
yD
iagn
osti
cla
bela
nb
Mea
nag
esc
atTi
me
1Ty
peof
stud
yEI
BIco
ndit
ion
Com
pari
son
(C)
cond
itio
n
Lova
as,1
987;
McE
achi
net
al.,
1993
(USA
)D
SM/C
linic
aldi
-ag
nosi
sof
auti
sm
EIBI
�19
C1�
19C2
�21
EIBI
�35
C1�
41C2
�42
Case
cont
rolt
rial
UCL
A-
EIBI
C1:l
ess
inte
nsiv
eth
erap
y,C2
:min
i-m
umth
erap
ySm
ith
etal
.,19
97(U
SA)
DSM
:MR
and
auti
smEI
BI�
11C
�10
EIBI
�36
C�
38Re
tros
pect
ive
case
-co
ntro
lstu
dyU
CLA
-EIB
Im
ulti
site
Min
imum
ther
apy
Shei
nkop
f&
Sieg
el,
1998
(USA
)D
SM:a
utis
m;
PDD
EIBI
�11
C�
11EI
BI�
34C
�35
Retr
ospe
ctiv
eca
se-
cont
rolt
rial
Com
mun
ity-
base
dU
CLA
mod
el
Stan
dard
scho
olin
g
Smit
h,G
roen
,&W
ynn,
2000
(USA
)Cl
inic
diag
nosi
s:au
tism
;PD
DEI
BI�
15C
�13
EIBI
�36
C�
36Ra
ndom
ized
con-
trol
tria
lU
CLA
-EIB
Im
ulti
site
Pare
nt-t
rain
ing/
pub-
licsc
hool
Eike
seth
etal
.,20
02/
2007
(Nor
way
)A
DI-R
auti
smEI
BI�
13C
�12
EIBI
�66
C�
65Ca
se-c
ontr
oltr
ial
Scho
ol-b
ased
UCL
Am
odel
Ecle
ctic
educ
atio
n
Sallo
ws
&G
raup
ner,
2005
(USA
)A
DI-R
auti
smEI
BI�
13C�
10EI
BI�
35C
�37
Rand
omiz
edal
loca
-ti
onto
clin
icor
pare
nt-r
ungr
oup
UCL
A-E
IBI
mul
tisi
tePa
rent
-dir
ecte
dEI
BI
How
ard
etal
.,20
05(U
SA)
DSM
(wit
hse
-ve
rity
deta
ils)
auti
sm;P
DD
EIBI
�29
C1�
16C2
�16
EIBI
�31
C1�
39C2
�35
Case
-con
trol
tria
lCo
mm
unit
y-ba
sed
EIBI
C1:6
auti
smsp
ecifi
ced
.C2:
16ge
neri
csp
ecia
led.
Cohe
net
al.,
2006
(USA
)A
DI-R
auti
sm;
PDD
EIBI
�21
C�
21EI
BI�
30C
�33
d
Case
-con
trol
tria
lU
CLA
-EIB
Im
ulti
site
Ecle
ctic
educ
atio
n
Elde
vik
etal
.,20
06(N
orw
ay)
Mos
tA
DI-R
au-
tism
�LD
EIBI
�13
C�
15EI
BI�
53C
�49
Retr
ospe
ctiv
eca
se-
cont
rolt
rial
Scho
ol/h
ome-
base
dU
CLA
mod
el
Ecle
ctic
educ
atio
n
Mag
iati
etal
.,20
07(U
K)
AD
I-Rau
tism
;A
SDEI
BI�
28C
�16
EIBI
�38
C�
42Ca
se-c
ontr
oltr
ial
Com
mun
ity-
base
dEI
BIA
utis
msp
ecifi
cnu
rs-
ery
Rem
ingt
onet
al.,
2007
(UK
)A
DI-R
auti
smEI
BI�
23C
�21
EIBI
�36
C�
38Ca
se-c
ontr
oltr
ial
Com
mun
ity-
base
dEI
BIM
ixof
ther
apie
s,no
ne1:
1a D
SM�
Dia
gnos
tican
dSt
atist
ical
Man
ual
ofM
enta
lD
isord
ers;
PDD
�pe
rvas
ive
deve
lopm
enta
ldi
sord
er;
AD
I-R
�A
utis
mD
iagn
ostic
Inte
rvie
w-R
evis
ed;
MR
�m
enta
lre
tard
atio
n.bE
IBI
�ea
rly
inte
nsiv
ebe
havi
oral
inte
rven
tions
;C
�co
mpa
riso
ngr
oup
(C1
�G
roup
1;C
2�
Gro
up2
inst
udie
sw
ithm
ore
than
1co
mpa
riso
ngr
oup)
.c In
mon
ths.
dO
nly
age
atdi
agno
sis
give
n.

� American Association on Intellectual and Developmental Disabilities 27
VOLUME 114, NUMBER 1: 23–41 � JANUARY 2009 AJIDD
Early intensive behavioral interventions P. Howlin, I. Magiati, and T. Charman
Smith et al. (1997) and Eldevik et al. (2006) fo-cused specifically on children with intellectual im-pairments; the remainder included children withmean IQs ranging from 50 to 80�.
The mean number of EIBI children per studywas 17.8 (SD � 6.6, range � 11 to 29); the meannumber of comparison cases was 14.7 (SD � 4.1,range � 10 to 21). There was no significant dif-ference in the ages of EIBI and comparison chil-dren at baseline; the mean age of the EIBI chil-dren was 40 months, with a range of 31 to 66.Comparison children’s mean age was 42 months,with a range of 35 to 65. However, it was occa-sionally difficult to establish accurately from thepublished data the age at which intervention ac-tually began, with some researchers (e.g., Cohenet al., 2006) reporting only the ages at which chil-dren were diagnosed or first assessed rather thanthe precise age at which intervention started. Inthe majority of interventions, investigatorsclaimed to follow the behavioral program devel-oped by Lovaas and colleagues as part of theUCLA Young Autism Project; 5 were part of theUCLA multisite replication group; 2 were school-based but affiliated with the UCLA program; 4were community-based programs. Of these,Sheinkopf and Siegel (1998), according to parentalreport, followed the UCLA model; Howard,Sparkman, Cohen, Green, and Stanislaw (2005)and Remington et al. (2007) reported that thera-pists had been trained in a number of ABA/EIBItechniques, including the manualized programs ofMaurice et al. (1996, 2001), discrete trial and in-cidental teaching (Anderson & Romanczyk, 1999),Natural Environment Training (Sundberg & Par-tington, 1999), and Verbal Behavior (Partington &Sundberg, 1998); Magiati et al. (2007) included atleast some consultants trained at UCLA.
The comparison conditions varied from in-tensive, parent-directed (as opposed to clinic-di-rected) intervention (Sallows & Graupner, 2005)to reduced intensity of EIBI program (Lovaas,1987; Smith et al., 1997); eclectic, public school-ing (Cohen et al., 2006; Eikeseth et al., 2002,2006; Eldevik et al., 2006; Sheinkopf & Siegel,1998); specialist autism school (Howard et al.,2005; Magiati et al., 2007) or a mixture of differ-ent interventions (Remington et al., 2007). Twostudies (Howard et al., 2005; Lovaas, 1987) in-volved two separate comparison groups.
Duration and Intensity of InterventionsTable 2 provides information on the approx-
imate duration of intervention and the ages at
which participants were followed-up. Not all pa-pers provided clear information on how long chil-dren were involved in the program, and in somecases children had been enrolled in the therapysome time prior to the initial ‘‘baseline’’ assess-ments. For some studies we were not able to es-tablish the length of time children were actuallyinvolved in intervention. Lovaas (1987) stated thatthe EIBI children received between 2 and 6 yearsor more of intervention. Smith et al., 1997) re-ported that the EIBI children received a minimumof 2 years of therapy; control participants receivedless than 2 years. As can be seen in Table 2, ofthe remaining 9 studies, 3 involved interventionsof less than 24 months; 5 interventions were 24to 36 months, and in 1 (Sallows & Graupner,2005), interventions lasted 4 years. The mean in-tervention time in these 9 studies for both EIBIand comparison groups was (as far as could beestimated) 27.4 months (SD � 10.7, range 14 to48 months).
Actual hours of intervention proved evenmore difficult to estimate. Only a minority of re-searchers (Magiati et al., 2007; Remington et al.,2007; Smith, Groen, & Wynn, 2000) providedtheir own figures, based on parental or therapists’reports, of the total number of hours in therapy.Most gave only a general indication of hours ofintervention (e.g., minimum number of hours perweek); several indicated that time in therapy de-clined after the first year, without providing in-formation on the degree of reduction. In others(e.g., Lovaas, 1987), it was clear that individualvariation was considerable, with some children inthis, the original Lovaas study, receiving over 6years and more than 14,000 hours of therapy,while others in the same study received 40 hoursof therapy per week for 2 years (i.e., approximateestimation of 4,000 hours). Although it was notpossible, with one exception (Smith et al., 2000:M � 2,158 hours, SD � 1,305, range � 1,142 to5,452), to derive an accurate estimate of totalnumber of hours in therapy over the duration oftreatment, most investigators gave an indicationof approximate hours per week, at least during themost intensive phase of intervention. On the basisof the information provided, we estimated thatEIBI children received significantly more hours ofintervention per week than did controls (EIBI M� 29.8 hours per week; SD � 7.6, range 12.5 to40; controls M � 19.1 hours , SD � 8.6, range�10.0 to 31.5), t � 3.03, p � .007.
Despite the limited quality of the available

28 � American Association on Intellectual and Developmental Disabilities
VOLUME 114, NUMBER 1: 23–41 � JANUARY 2009 AJIDD
Early intensive behavioral interventions P. Howlin, I. Magiati, and T. Charman
Tabl
e2.
Sum
mar
yof
Tre
atm
ent
Dur
atio
nan
dIn
tens
ity
Stud
yTr
eatm
ent
dura
tion
Follo
w-u
p(F
U)
cond
ucte
d/M
ean
age
App
roxi
mat
enu
mbe
rof
hour
spe
rw
eek
EIBI
grou
pCo
mpa
riso
ngr
oup
Lova
as,1
987;
McE
achi
net
al.,
1993
From
2to
6�ye
ars
FUaf
ter
2�an
d8�
year
s(a
tap
prox
.age
7ye
ars
&11
.5ye
ars)
40ho
urs
for
2ye
ars,
then
decr
easi
ngLe
ssth
an10
hour
spe
rw
eek
both
com
pari
son
grou
psSm
ith
etal
.,19
97EI
BIa
�2
year
s;Cb
�2
year
sFU
afte
r2.
5to
3ye
ars
Age
:EIB
I71
mon
ths;
C64
mon
ths
(but
som
ech
il-dr
enag
ed9–
10ye
ars)
30ho
urs
per
wee
k�
10ho
urs
per
wee
k
Shei
nkop
f&
Sieg
el,
1998
EIBI
16m
onth
s;C
18m
onth
sFU
:EIB
Iaft
er20
mon
ths;
Caf
ter
18m
onth
sA
ge:E
IBI&
C54
m
27ho
urs
per
wee
k11
hour
spe
rw
eek
Smit
h,G
roen
,&W
ynn,
2000
2–3
year
sFU
afte
rap
prox
.5ye
ars
Age
:EIB
I94
mon
ths;
C92
mon
ths
25ho
urs
per
wee
k1s
tye
ar;
then
redu
cing
15–2
0ho
urs
per
wee
k(p
aren
tan
dsc
hool
base
d)Ei
kese
thet
al.,
2002
,20
07EI
BI31
mon
ths;
C33
mon
ths
FUaf
ter
12m
onth
s&
2.5
to3
year
sA
ge:E
IBI&
C,98
mon
ths
28ho
urs
per
wee
k1s
tye
ar;
18ho
urs
2nd
year
29ho
urs
per
wee
k1s
tye
ar;1
6ho
urs
2nd
year
Sallo
ws
&G
raup
ner,
2005
48m
onth
sFU
afte
r48
mon
ths
Age
:EIB
I&C
83m
onth
s39
hour
spe
rw
eek
1st
year
;37
hour
spe
rw
eek,
2nd
year
32ho
urs
per
wee
k1s
tye
ar;3
1ho
urs
per
wee
k,2n
dye
arH
owar
det
al.,
2005
13–1
4m
onth
sFU
afte
r14
mon
ths
Age
:EIB
I46
mon
ths;
C151
mon
ths;
C249
mon
ths
25–4
0ho
urs
per
wee
kC1
25–3
0ho
urs
per
wee
k;C2
mea
n15
hour
spe
rw
eek
Cohe
net
al.,
2006
36m
onth
s(b
utso
me
EIBI
grou
psha
dup
to40
0ho
urs
EIBI
befo
rein
take
)
FUaf
ter
36m
onth
sA
geat
FUun
clea
r35
–40
hour
spe
rw
eek
15–2
5ho
urs
per
wee
k
Elde
vik
etal
.,20
06EI
BI20
mon
ths;
C21
mon
ths
FUaf
ter
20–2
1m
onth
sA
ge:E
IBI7
3m
onth
s;C
70m
onth
s
12.5
hour
spe
rw
eek
12ho
urs
per
wee
k
Mag
iati
etal
.,20
0724
mon
ths
FUaf
ter
26m
onth
sA
ge:E
IBI6
4m
onth
s;C
68m
onth
s
32ho
urs
per
wee
k26
hour
spe
rw
eek
Rem
ingt
onet
al.,
2007
24m
onth
sFU
afte
r12
&24
mon
ths
Age
:EIB
I&C
4&
5ye
ars
26ho
urs
per
wee
kin
EIBI
�22
/23
child
ren
insc
hool
for
9–13
hour
spe
rw
eek
15–1
7ho
urs
per
wee
kin
scho
ol1s
tye
ar;1
4–22
hour
spe
rw
eek
2nd
year
a Ear
lyin
tens
ive
beha
vior
alin
terv
entio
ns.b
Com
pari
son
grou
p(C
1�
Gro
up1;
C2
�G
roup
2in
stud
ies
with
mor
eth
anon
eco
mpa
riso
ngr
oup)
.

� American Association on Intellectual and Developmental Disabilities 29
VOLUME 114, NUMBER 1: 23–41 � JANUARY 2009 AJIDD
Early intensive behavioral interventions P. Howlin, I. Magiati, and T. Charman
information, we also believed it important to at-tempt an approximate estimate of total hours intherapy in order to assess the potential impact ofintensity on outcome. This estimate was derivedby multiplying Approximate Weeks of Interven-tion � Approximate Hours per Week (allowingfor any reduction in hours reported by authorsafter 1 or 2 years in therapy). The resulting figureswere as follows: EIBI group mean was 3,353 hours(SD � 1,960, range � 1,000 to 7,100); compari-son group mean was 1,980 hours (SD � 1,529,range 836 to 5,952). Although the intensity of in-tervention was considerably less in the compari-son groups than for the EIBI children, this differ-ence fell short of statistical significance, t � 1.78,p � .09, reflecting the very wide range of hoursin both groups.
Baseline and Outcome DataJust as the studies varied with respect to the
characteristics of children involved and the dura-tion and intensity of intervention, there was con-siderable variation in the methods used to assessoutcome. First, not all researchers presented out-come data at the time intervention actuallyceased; they instead provided this information asmeasured at follow-up sometime later. Thus,whereas the mean duration of the interventionprogram itself was 27 months for both EIBI chil-dren and controls (at least in the 9 studies forwhich a calculation of duration was possible), themean time between baseline assessment and fol-low-up was 39.2 months (SD � 30.1, range � 12to �121) for EIBI children and 34.5 months (SD� 19.2, range � 12 to 79) for controls. Althoughthe group difference in time from cessation oftreatment to follow-up was not significant, t �.45, p � .66, even a relatively small time lag fol-lowing the end of intervention further complicat-ed any assessment of the association between du-ration of therapy and degree of improvement.
Differences in the outcome measures used area further factor affecting comparisons amongstudies. Although data on IQ changes over timewere provided in all 11 studies, information onthe instruments used was generally sparse. Thetests used varied, not only from study to study,but from child to child and from baseline to fol-low-up within the same study, and this variabilityin assessments over time can result in spuriousconclusions about the extent of cognitive im-provement (Magiati & Howlin, 2001). In 6 studiesdata for verbal and nonverbal IQ were reported
separately and in 2, investigators reported changesin mental age (MA). Remington et al. (2007) alsocalculated the Reliable Change Index (Jacobson &Truax, 1991) in order to establish, with 95% cer-tainty, that the level of IQ change was not due tomeasurement unreliability/score variability.
The Vineland Adaptive Behavior ScalesVABS (Sparrow, Balla, & Cicchetti, 1984) havebeen used in the more recent studies (Cohen etal., 2006; Eikeseth et al., 2002, 2007; Eldevik etal., 2006; Howard et al., 2005; Magiati et al.,2007; Remington et al., 2007; Sallows & Graup-ner, 2005; Smith et al., 1997). Some authors pre-sented standard scores; others, age equivalents orraw scores (e.g., Remington et al., 2007). The lat-ter, in particular, are difficult to interpret with re-spect to the clinical meaning of any changesfound.
Language data have become better standard-ized over time, with most investigators providinginformation on expressive and language skills asassessed by the Reynell scales, although not allused the same versions of the Reynell (Cohen etal., 2006; Eikeseth et al., 2002, 2007; Eldevik etal., 2006; Howard et al., 2005; Magiati et al.,2007; Remington et al., 2007; Sallows & Graup-ner, 2005; Smith et al., 1997).
Again, although some researchers presentedstandard scores, others cited age equivalents. Ma-giati et al. (2007) reported raw scores because sofew children were able to score above basal and,for the same reason, Remington et al. (2007) sim-ply recorded the number of children able toachieve any score. Few investigators provided ad-equate information on how issues relating to testbasals for standard scores and age equivalents weredealt with. Raw scores are, of course, acceptablewhen children are so far below basal that ageequivalents and standard scores cannot be calcu-lated (Charman, 2004), but when only raw scoresare provided by some authors, and only standardscores or age equivalents by others, comparisonsamong studies become extremely difficult. Includ-ing data on age equivalents, standard scores, andraw scores would be far more informative and aidthe interpretation of any significant group differ-ences. Now that many journals provide access toonline-only appendices, this comprehensive re-porting of data should be possible in the future.
Other outcome data vary to such an extentthat comparisons between studies are not feasible.Some (e.g., Lovaas, 1987, Sallows & Graupner,2005) provided information on personality tests

30 � American Association on Intellectual and Developmental Disabilities
VOLUME 114, NUMBER 1: 23–41 � JANUARY 2009 AJIDD
Early intensive behavioral interventions P. Howlin, I. Magiati, and T. Charman
(e.g., the Personality Inventory for Children: Wirt,Lachar, Klinedinst, & Seat, 1984; Smith et al.,1997); several authors assessed levels of problembehaviors using a range of different measures, in-cluding maladaptive behavior scales, behavioralobservations, or parental reports (Lovaas, 1987;Magiati et al., 2007; Remington et al., 2007;Smith et al., 1997; Smith et al., 2000). In somelater studies (Magiatii et al., 2007; Sallows &Graupner, 2005), researchers also used the ADI-Rto monitor changes in the severity of autismsymptomatology over time (although the AutismDiagnostic Observation Schedule-GenericADOS-G (Lord et al., 2000) might be a better po-tential outcome measure of autism severity (seeAldred et al., 2004; Howlin, Gordon, Pasco,Wade, & Charman, 2007). Most studies providesome limited information on the school status ofparticipants following intervention (e.g., whetherunsupported in mainstream school).
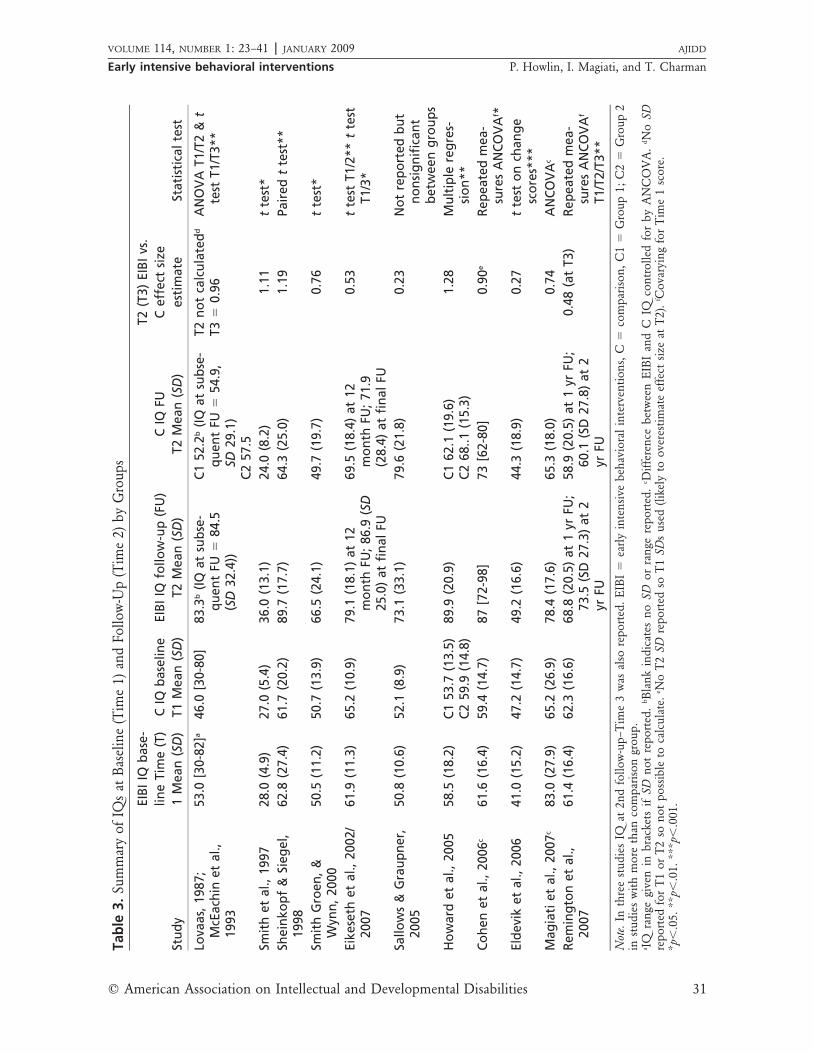
Table 3 presents the information on changesin IQ over time as provided in all studies. The IQdata indicate that in the majority of studies, therewere no significant differences between EIBI andcomparison children at baseline; in one study(Magiati et al., 2007), where there was a groupdifference in IQ (though not MA), this was con-trolled for in the analysis of change. Comparisonof group scores on other tests for which the ma-jority of studies provide information (VinelandComposite; Language Comprehension, and Ex-pression) also indicates no significant group dif-ferences at intake. In the studies reviewed differentstrategies for analysis were used. The most com-mon analysis was a simple t test, ANOVA, orMann Whitney U test on outcome scores (Eike-seth et al., 2002; Lovaas, 1987; Sheinkopf & Sie-gel, 1998; Smith et al., 1997; Smith et al., 2000),including for Smith et al. and Eikeseth et al., one-tailed t tests). Eikeseth et al. (2002, 2007) and Eld-evik et al. analyzed change scores.
In several of the more recent studies, research-ers reported either simple ANCOVAs on outcomescores (Howard et al., 2006; Remington et al.,2007), repeated measures ANOVA (Sallows &Graupner, 2005), or ANCOVA (Cohen et al.,2006; Remington et al., 2007), partly reflectingtheir larger sample size that enabled them to meetmore of the statistical assumptions that such testsrequire. Although these different analyses do notallow a uniform estimate of effect size to be cal-culated from the available group scores, in orderto provide a simple estimate of effect size for IQ,
we calculated EIBI versus comparison group meandifferences divided by the SD of the two groupscombined (Cohen’s d) (see Table 3).
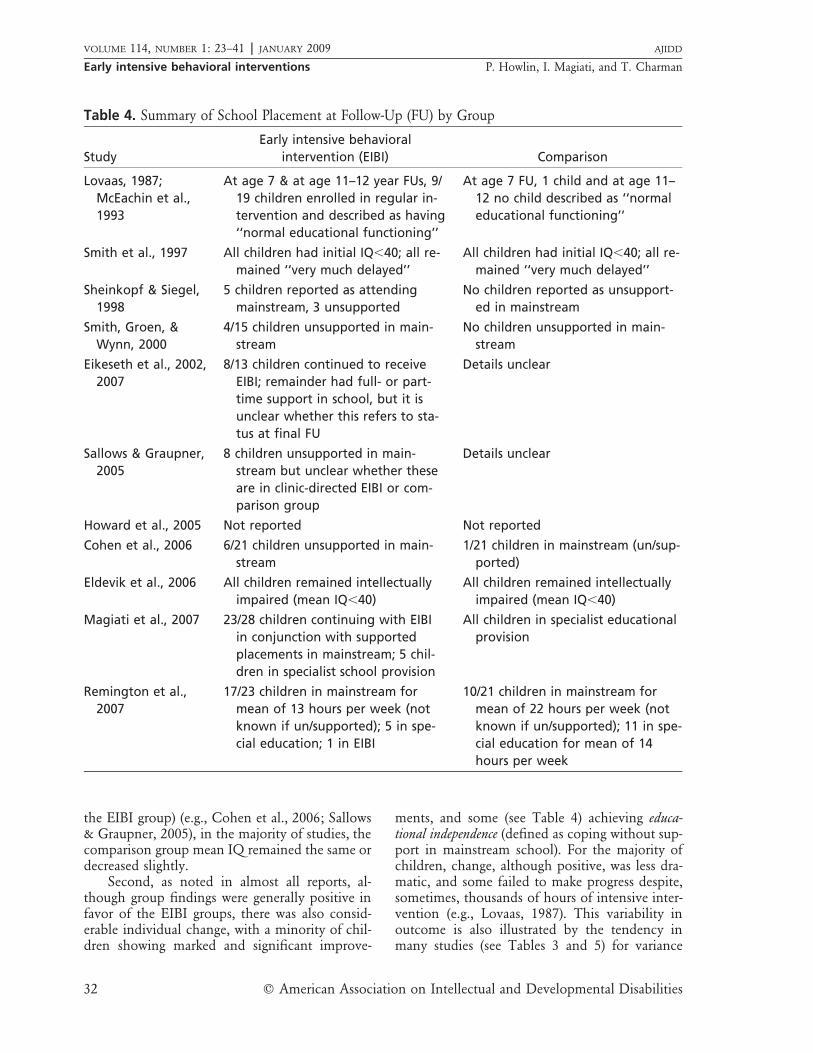
Data on school placement at follow-up wereprovided in the majority of studies (see Table 4).Overall differences, based on study group meansfor IQ, VABS, and language test standard scoresare reported in Table 5 (some data were extrapo-lated from the published MA scores).
At final follow-up, there were significantgroup differences in IQ in 9 of the 11 reports. Ofthe remaining 2 studies, Magiati et al. (2007) re-ported no differences between the EIBI and com-parison groups. Sallows and Graupner (2005) didnot analyze for Group � Time differences; in-stead, they reported IQ improvements in bothgroups while noting considerable variability inboth groups at outcome. Estimated effect sizeswere moderate, �0.60, to large, �0.80, in the ma-jority of studies. However, in other studies show-ing significant results (e.g., Eldevik et al., 2005),the effect size was small, 0.27. The significantgroup difference in this case is due in part to theanalysis of change scores (Time 1 to Time 2) andthe fact that although the group mean score in-creased somewhat for the EIBI group, it decreasedin the comparison group. As is evident from thesummary data shown in Table 5, there was a sub-stantial mean increase in IQs in the EIBI groupsover time. There were also positive changes, of asimilar magnitude, in language scores. The im-provement in VABS scores, although significantin the summary EIBI versus comparison groupanalysis, was relatively small (average 5 standardscore points).
Several additional points should be noted.First, the extent of change reported in the differ-ent studies is considerable, as is clear from Table5. For example, for IQ, investigators in 3 studies(Eldevik et al., 2006; Magiati et al., 2007; Smithet al., 1997) reported changes of less than 10points; 2 (Remington et al., 2007; Sheinkopf &Siegel, 1998), a 10 to 20 points increase; 4 (Cohenet al., 2006; Eikeseth et al., 2002, 2007; Sallows &Graupner, 2005; Sheinkopf & Siegel, 1998), a 21to 30 points increase; and in 2 studies (Howardet al., 2005; Lovaas, 1987), an increase of 31points. The data on language and VABS scoresshow similar variation. Also of note is the varia-tion of the change in mean scores of the compar-ison groups. Although in some studies the meancomparison group IQ increased between baselineand outcome (albeit not as much on average as
� American Association on Intellectual and Developmental Disabilities 31
VOLUME 114, NUMBER 1: 23–41 � JANUARY 2009 AJIDD
Early intensive behavioral interventions P. Howlin, I. Magiati, and T. Charman
Tabl
e3.
Sum
mar
yof
IQs
atB
asel
ine
(Tim
e1)
and
Follo
w-U
p(T
ime
2)by
Gro
ups
Stud
y
EIBI
IQba
se-
line
Tim
e(T
)1
Mea
n(S
D)
CIQ
base
line
T1M
ean
(SD
)EI
BIIQ
follo
w-u
p(F
U)
T2M
ean
(SD
)C
IQFU
T2M
ean
(SD
)
T2(T
3)EI
BIvs
.C
effe
ctsi
zees
tim
ate
Stat
isti
calt
est
Lova
as,1
987;
McE
achi
net
al.,
1993
53.0
[30-
82]a
46.0
[30-
80]
83.3
b(IQ
atsu
bse-
quen
tFU
�84
.5(S
D32
.4))
C152
.2b
(IQat
subs
e-qu
ent
FU�
54.9
,SD
29.1
)C2
57.5
T2no
tca
lcul
ated
d
T3�
0.96
AN
OV
AT1
/T2
&t
test
T1/T
3**
Smit
het
al.,
1997
28.0
(4.9
)27
.0(5
.4)
36.0
(13.
1)24
.0(8
.2)
1.11
tte
st*
Shei
nkop
f&
Sieg
el,
1998
62.8
(27.
4)61
.7(2
0.2)
89.7
(17.
7)64
.3(2
5.0)
1.19
Pair
edt
test
**
Smit
hG
roen
,&W
ynn,
2000
50.5
(11.
2)50
.7(1
3.9)
66.5
(24.
1)49
.7(1
9.7)
0.76
tte
st*
Eike
seth
etal
.,20
02/
2007
61.9
(11.
3)65
.2(1
0.9)
79.1
(18.
1)at
12m
onth
FU;8
6.9
(SD
25.0
)at
fina
lFU
69.5
(18.
4)at
12m
onth
FU;7
1.9
(28.
4)at
fina
lFU
0.53
tte
stT1
/2**
tte
stT1
/3*
Sallo
ws
&G
raup
ner,
2005
50.8
(10.
6)52
.1(8
.9)
73.1
(33.
1)79
.6(2
1.8)
0.23
Not
repo
rted
but
nons
igni
fica
ntbe
twee
ngr
oups
How
ard
etal
.,20
0558
.5(1
8.2)
C153
.7(1
3.5)
C259
.9(1
4.8)
89.9
(20.
9)C1
62.1
(19.
6)C2
68..1
(15.
3)1.
28M
ulti
ple
regr
es-
sion
**Co
hen
etal
.,20
06c
61.6
(16.
4)59
.4(1
4.7)
87[7
2-98
]73
[62-
80]
0.90
eRe
peat
edm
ea-
sure
sA
NCO
VA
f *El
devi
ket
al.,
2006
41.0
(15.
2)47
.2(1
4.7)
49.2
(16.
6)44
.3(1
8.9)
0.27
tte
ston
chan
gesc
ores
***
Mag
iati
etal
.,20
07c
83.0
(27.
9)65
.2(2
6.9)
78.4
(17.
6)65
.3(1
8.0)
0.74
AN
COV
Ac
Rem
ingt
onet
al.,
2007
61.4
(16.
4)62
.3(1
6.6)
68.8
(20.
5)at
1yr
FU;
73.5
(SD
27.3
)at
2yr
FU
58.9
(20.
5)at
1yr
FU;
60.1
(SD
27.8
)at
2yr
FU
0.48
(at
T3)
Repe
ated
mea
-su
res
AN
COV
Af
T1/T
2/T3
**
Not
e.In
thre
est
udie
sIQ
at2n
dfo
llow
-up–
Tim
e3
was
also
repo
rted
.E
IBI
�ea
rly
inte
nsiv
ebe
havi
oral
inte
rven
tions
,C�
com
pari
son,
C1
�G
roup
1;C
2�
Gro
up2
inst
udie
sw
ithm
ore
than
com
pari
son
grou
p.a I
Qra
nge
give
nin
brac
kets
ifSD
not
repo
rted
.bB
lank
indi
cate
sno
SDor
rang
ere
port
ed.
c Diff
eren
cebe
twee
nE
IBI
and
CIQ
cont
rolle
dfo
rby
AN
CO
VA
.dN
oSD
repo
rted
for
T1
orT
2so
not
poss
ible
toca
lcul
ate.
e No
T2
SDre
port
edso
T1
SDs
used
(like
lyto
over
estim
ate
effe
ctsi
zeat
T2)
.f C
ovar
ying
for
Tim
e1
scor
e.*p
�.0
5.**
p�.0
1.**
*p�
.001
.
32 � American Association on Intellectual and Developmental Disabilities
VOLUME 114, NUMBER 1: 23–41 � JANUARY 2009 AJIDD
Early intensive behavioral interventions P. Howlin, I. Magiati, and T. Charman
Table 4. Summary of School Placement at Follow-Up (FU) by Group
StudyEarly intensive behavioral
intervention (EIBI) Comparison
Lovaas, 1987;McEachin et al.,1993
At age 7 & at age 11–12 year FUs, 9/19 children enrolled in regular in-tervention and described as having‘‘normal educational functioning’’
At age 7 FU, 1 child and at age 11–12 no child described as ‘‘normaleducational functioning’’
Smith et al., 1997 All children had initial IQ�40; all re-mained ‘‘very much delayed’’
All children had initial IQ�40; all re-mained ‘‘very much delayed’’
Sheinkopf & Siegel,1998
5 children reported as attendingmainstream, 3 unsupported
No children reported as unsupport-ed in mainstream
Smith, Groen, &Wynn, 2000
4/15 children unsupported in main-stream
No children unsupported in main-stream
Eikeseth et al., 2002,2007
8/13 children continued to receiveEIBI; remainder had full- or part-time support in school, but it isunclear whether this refers to sta-tus at final FU
Details unclear
Sallows & Graupner,2005
8 children unsupported in main-stream but unclear whether theseare in clinic-directed EIBI or com-parison group
Details unclear
Howard et al., 2005 Not reported Not reported
Cohen et al., 2006 6/21 children unsupported in main-stream
1/21 children in mainstream (un/sup-ported)
Eldevik et al., 2006 All children remained intellectuallyimpaired (mean IQ�40)
All children remained intellectuallyimpaired (mean IQ�40)
Magiati et al., 2007 23/28 children continuing with EIBIin conjunction with supportedplacements in mainstream; 5 chil-dren in specialist school provision
All children in specialist educationalprovision
Remington et al.,2007
17/23 children in mainstream formean of 13 hours per week (notknown if un/supported); 5 in spe-cial education; 1 in EIBI
10/21 children in mainstream formean of 22 hours per week (notknown if un/supported); 11 in spe-cial education for mean of 14hours per week
the EIBI group) (e.g., Cohen et al., 2006; Sallows& Graupner, 2005), in the majority of studies, thecomparison group mean IQ remained the same ordecreased slightly.
Second, as noted in almost all reports, al-though group findings were generally positive infavor of the EIBI groups, there was also consid-erable individual change, with a minority of chil-dren showing marked and significant improve-
ments, and some (see Table 4) achieving educa-tional independence (defined as coping without sup-port in mainstream school). For the majority ofchildren, change, although positive, was less dra-matic, and some failed to make progress despite,sometimes, thousands of hours of intensive inter-vention (e.g., Lovaas, 1987). This variability inoutcome is also illustrated by the tendency inmany studies (see Tables 3 and 5) for variance

� American Association on Intellectual and Developmental Disabilities 33
VOLUME 114, NUMBER 1: 23–41 � JANUARY 2009 AJIDD
Early intensive behavioral interventions P. Howlin, I. Magiati, and T. Charman
Tabl
e5.
Sum
mar
yD
ata
From
All
Stud
ies
onC
hang
esin
IQ,V
AB
S,an
dLa
ngua
geSc
ores
Ove
rT
ime
byG
roup
Mea
sure
a
EIBI
b
base
line
Mea
nSD
Com
pari
son
base
line
Mea
nSD
EIBI
follo
w-u
p(F
U)b
Mea
nSD
Com
pari
son
FU
Mea
nSD
EIBI
chan
gesc
ore
Mea
nSD
Rang
e
Com
pari
son
chan
gesc
ore
Mea
nSD
Rang
e
Gro
upch
ange
scor
edi
ffer
ence
Man
nW
hitn
eyZc
IQ(1
1)55
.713
.953
.611
.274
.017
.659
.015
.518
.311
.5�
5.0–
31.5
5.4
9.3
�3.
3–27
.5–2
.27*
VA
BSco
mpo
site
SSd
(8)
61.2
6.4
61.5
6.7
66.2
10.2
56.2
9.3
5.1
6.2
�2.
0–2.
0�
2.4
4.5
�10
.5–5
.8–2
.58*
*Ex
pres
sion
SS(7
)49
.411
.949
.37.
961
.112
.750
.911
.911
.610
.8�
5–5.
01.
78.
5�
7.5–
15.0
–1.7
9Co
mpr
ehen
sion
SS(7
)42
.810
.945
.05.
358
.510
.949
.612
.115
.76.
07.
0–24
.04.
512
.1�
10.8
–27.
0–1
.98*
Not
e.V
AB
S�
Vin
elan
dA
dapt
ive
Beh
avio
rSc
ales
.a N
umbe
rof
stud
ies
prov
idin
gda
tain
pare
nthe
ses.
No
diff
eren
ces
ingr
oup
mea
nsat
base
line.
bD
ata
prov
ided
for
final
FUif
mor
eth
anon
eFU
asse
ssm
ent
repo
rted
.c N
onpa
ram
etri
can
alys
isus
edbe
caus
ech
ange
scor
eshi
ghly
skew
ed.e S
tand
ard
scor
e.*p
�.0
5.**
p�.0
1.
scores in both the EIBI and comparison groupsto increase over time, indicating greater individualvariability over time. As is also evident from Table5, the range of change scores reported was oftensimilar in both EIBI and comparison groups. Im-portantly, these data suggest, in addition to anygroup mean differences, that while some childrenin both groups do well, others do not. However,only a minority of studies (Cohen et al., 2006;Magiati et al., 2007; Remington et al., 2007; Sal-lows & Graupner, 2005; Sheinkopf & Siegel, 1998)present clear data on individual patterns ofchange.
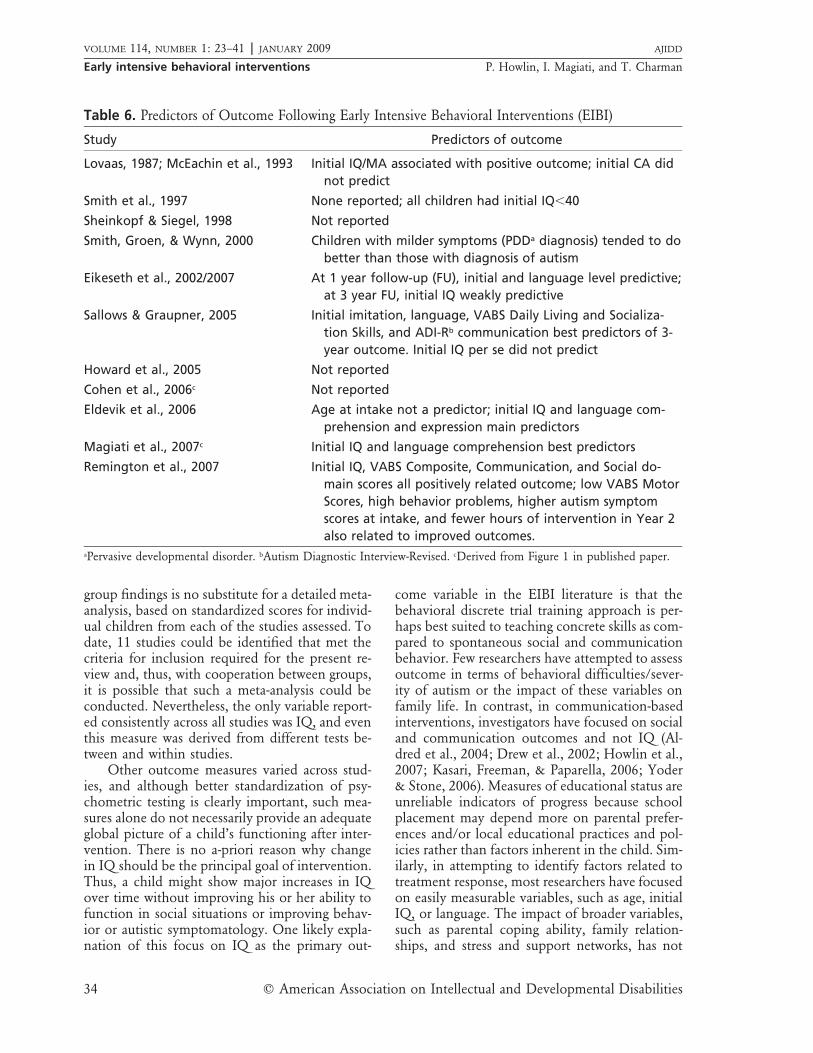
Predictors of OutcomeIndividual variability in response to treatment
resulted in investigators in 7 out of the 11 studiesexploring more systematically variables thatseemed to be related to the extent of change (gen-erally as measured by increases in IQ). Some re-searchers also considered in detail variables thatappeared to distinguish between children with the‘‘best’’ and ‘‘poorest’’ outcomes. Table 6 providesa summary of the intake variables reported as be-ing predictors of favorable outcome, although itis not possible to draw any consistent conclusionsfrom these findings because different variables (orcombinations of variables) were assessed in differ-ent studies. In 4 studies, initial IQ was stronglypositively associated with degree of improvement,but in one (Sallows & Graupner, 2005) initial IQshowed no relationship with outcome. Chrono-logical age was not reported to be associated withoutcome, and although the age range of childrenin these studies was limited (from 3 to 5.5 years),there was nothing in these data to support theclaims of some EIBI proponents that in order tobe effective, intervention must begin by around 3years. Initial language level (particularly receptivelanguage) did appear to be associated with out-come in 4 of the 7 studies in which predictivefactors were explored. Smith et al. (2000) reportedthat children with less severe autism symptom-atology tend to make better progress, but Rem-ington et al. (2007) found that children with high-er levels of behavior problems and autism symp-toms at intake were most likely to show the great-est change.
DiscussionLimitations of the Present Analysis
In order to interpret the true effects of intakevariables on outcome, reliance on the reports of
34 � American Association on Intellectual and Developmental Disabilities
VOLUME 114, NUMBER 1: 23–41 � JANUARY 2009 AJIDD
Early intensive behavioral interventions P. Howlin, I. Magiati, and T. Charman
Table 6. Predictors of Outcome Following Early Intensive Behavioral Interventions (EIBI)
Study Predictors of outcome
Lovaas, 1987; McEachin et al., 1993 Initial IQ/MA associated with positive outcome; initial CA didnot predict
Smith et al., 1997 None reported; all children had initial IQ�40
Sheinkopf & Siegel, 1998 Not reported
Smith, Groen, & Wynn, 2000 Children with milder symptoms (PDDa diagnosis) tended to dobetter than those with diagnosis of autism
Eikeseth et al., 2002/2007 At 1 year follow-up (FU), initial and language level predictive;at 3 year FU, initial IQ weakly predictive
Sallows & Graupner, 2005 Initial imitation, language, VABS Daily Living and Socializa-tion Skills, and ADI-Rb communication best predictors of 3-year outcome. Initial IQ per se did not predict
Howard et al., 2005 Not reported
Cohen et al., 2006c Not reported
Eldevik et al., 2006 Age at intake not a predictor; initial IQ and language com-prehension and expression main predictors
Magiati et al., 2007c Initial IQ and language comprehension best predictors
Remington et al., 2007 Initial IQ, VABS Composite, Communication, and Social do-main scores all positively related outcome; low VABS MotorScores, high behavior problems, higher autism symptomscores at intake, and fewer hours of intervention in Year 2also related to improved outcomes.
aPervasive developmental disorder. bAutism Diagnostic Interview-Revised. cDerived from Figure 1 in published paper.
group findings is no substitute for a detailed meta-analysis, based on standardized scores for individ-ual children from each of the studies assessed. Todate, 11 studies could be identified that met thecriteria for inclusion required for the present re-view and, thus, with cooperation between groups,it is possible that such a meta-analysis could beconducted. Nevertheless, the only variable report-ed consistently across all studies was IQ, and eventhis measure was derived from different tests be-tween and within studies.
Other outcome measures varied across stud-ies, and although better standardization of psy-chometric testing is clearly important, such mea-sures alone do not necessarily provide an adequateglobal picture of a child’s functioning after inter-vention. There is no a-priori reason why changein IQ should be the principal goal of intervention.Thus, a child might show major increases in IQover time without improving his or her ability tofunction in social situations or improving behav-ior or autistic symptomatology. One likely expla-nation of this focus on IQ as the primary out-
come variable in the EIBI literature is that thebehavioral discrete trial training approach is per-haps best suited to teaching concrete skills as com-pared to spontaneous social and communicationbehavior. Few researchers have attempted to assessoutcome in terms of behavioral difficulties/sever-ity of autism or the impact of these variables onfamily life. In contrast, in communication-basedinterventions, investigators have focused on socialand communication outcomes and not IQ (Al-dred et al., 2004; Drew et al., 2002; Howlin et al.,2007; Kasari, Freeman, & Paparella, 2006; Yoder& Stone, 2006). Measures of educational status areunreliable indicators of progress because schoolplacement may depend more on parental prefer-ences and/or local educational practices and pol-icies rather than factors inherent in the child. Sim-ilarly, in attempting to identify factors related totreatment response, most researchers have focusedon easily measurable variables, such as age, initialIQ, or language. The impact of broader variables,such as parental coping ability, family relation-ships, and stress and support networks, has not

� American Association on Intellectual and Developmental Disabilities 35
VOLUME 114, NUMBER 1: 23–41 � JANUARY 2009 AJIDD
Early intensive behavioral interventions P. Howlin, I. Magiati, and T. Charman
been systematically investigated and, indeed, willprove a major methodological challenge.
Treatment fidelity is a further issue requiringgreater consideration. In only a minority of the11 studies did researchers provide data on thequality of the alternative therapies offered, and invery few studies was the comparison interventionautism-specific. Thus, aside from not employingthe EIBI approach, it is likely that the staff mem-bers involved with these children would have lessunderstanding of or expertise in autism and wouldalso be less well-informed about appropriate ed-ucational practice for children with autism in gen-eral. Details of EIBI interventions are also less de-tailed than might be expected, for although reas-surances are given about the high quality controlof these programs, the supporting informationprovided is generally anecdotal. In community-based studies, perhaps, details of treatment fidelityare less important because these are ‘‘effective-ness’’ trials of implementation in real life. How-ever, in many of the studies reviewed, includingthe UCLA-based ones, it was even difficult to pre-cisely establish how many hours of interventionchildren had received. In several investigations, wealso found it difficult to establish whether baselinemeasures had actually been conducted prior to orat the time of the child’s enrollment in the pro-gram. Indeed, there were indications in some stud-ies that children had already been exposed to theintervention for some time previously. Thus, Co-hen et al. (2006) stated that one inclusion criteri-on was that children should have received ‘‘nomore than 400 hours behavioral intervention pri-or to intake’’ (p. 146). Moreover, a few investiga-tors (e.g., Magiati et al., 2007; Sallows & Graup-ner, 2005) mentioned the fact that children in ei-ther or both the EIBI or comparison conditionswere receiving a number of additional, alternativetreatments (e.g., special diets; biological interven-tions such as Secretin injections or megavitamins;or more controversial therapies such as auditoryintegration, cranial osteopathy, or pet therapy) aswell as being involved in extracurricular activities(e.g., music or play therapy). Few, if any, of thesealternative ‘‘treatments’’ have been empiricallytested, with the exception of Secretin, where theevidence is clear that it has no empirical basis asan autism treatment (Williams et al., 2005).
A further issue concerns the optimal durationof EIBI programs. Neither the summary overview(Table 5) nor the data provided in the individualstudies suggests that length of intervention was
related to outcome. Indeed, Remington et al.(2007) noted that children who responded mostpositively to intervention had fewer hours of ther-apy in the second year than those who made theleast progress.
In those studies reporting IQ changes at sev-eral time points, change scores for the period be-tween the first and subsequent follow-up weregenerally much smaller than the changes betweenbaseline and Follow-Up 1 (see Table 7 for a sum-mary of studies with three or more time points).For example, in Lovaas’ (1987) study, the meanincrease in IQ between initial assessment and fol-low-up at 6 to 7 years was 30 points; at the nextfollow-up, when children were 11 to 12 years ofage, the further increase in IQ was 1.5 points. Ei-keseth et al. (2002) found that the first year in-crease was around 17 points, with an 8-point in-crease in the following year. Cohen et al. (2006)reported that mean IQ rose approximately 16points in the first year but then increased byabout 3 to 4 points the following year and about5 points in the final year (data in this study arepresented graphically and, thus, not easy to readprecisely). In Remington et al.’s (2007) study,there was a mean increase in IQ of 8 points inthe first year and a further increase of 4 points inthe subsequent year. Although these subsequentincreases are not negligible, they do suggest thatthe main impact of intervention is in the first year,and, thereafter, increases, at least in IQ, tend toplateau. Of course, IQ is not the only variable ofinterest and, as noted above, is not necessarily themost important indicator of treatment effective-ness. However, in those 3 studies that also showedchanges in VABS scores over several time points,the diminution in progress after the first year waseven more marked, with few changes in standardscores occurring after 12 months (Eikeseth et al.,2002, 2007; Remington et al., 2007; Sallows &Graupner, 2005). Cohen et al. (2006) reported asteady increase in expressive language from 12 to24 months post-intake, but this progressive in-crease was not replicated in the only other study(Remington et al., 2007) in which language scoresover more than two time points were tracked.
Implications for Future Intervention ResearchThe need to improve the quality of autism
intervention research generally has been stressedin a number of recent reviews, with specific rec-ommendations concerning the need to address is-sues such as small sample sizes, nonrandomized

36 � American Association on Intellectual and Developmental Disabilities
VOLUME 114, NUMBER 1: 23–41 � JANUARY 2009 AJIDD
Early intensive behavioral interventions P. Howlin, I. Magiati, and T. Charman
Tabl
e7.
IQC
hang
esin
Early
Inte
nsiv
eB
ehav
iora
lInt
erve
ntio
ns(E
IBI)
Gro
upfo
rSt
udie
sPr
esen
ting
Dat
aO
ver
Thr
eeor
Mor
eT
ime
Poin
ts
Stud
y
Tim
e1
Ave
rage
age
mea
naIQ
(SD
)
Tim
e2
Ave
rage
(app
rox.
)ag
em
ean
IQ(S
D)
Tim
e3
Ave
rage
(app
rox.
)ag
em
ean
IQ(S
D)
Tim
e4
Ave
rage
(app
rox.
)ag
em
ean
IQ
Lova
as,1
987;
McE
achi
net
al.,
1993
3553
b6–
7ye
ars
83.3
b11
.5ye
ars
84.5
(32.
4)N
/Ac
Eike
seth
etal
.,20
02/2
007
6661
.9(1
1.3)
79m
onth
s79
.1(1
8.1)
98m
onth
s86
.9(2
5.0)
N/A
Cohe
net
al.,
2006
30b
61.6
(16.
4)In
itia
lage
�1
year
77c
Init
iala
ge�
2ye
ars
Init
iala
ge�
3ye
ars
87d
Rem
ingt
onet
al.,
2007
3661
.4(1
6.4)
Init
iala
ge�
1ye
ar68
.8(2
0.5)
Init
iala
ge�
2ye
ars
73.5
(27.
3)N
/A
a In
mon
ths.
bSD
not
prov
ided
;ag
eat
diag
nosi
s.c N
otap
plic
able
(onl
yth
ree
time
poin
tsre
port
ed).
dD
eriv
edfr
omFi
gure
1in
publ
ishe
dpa
per.
assignment, inadequate information on the char-acteristics of participants and therapy, and thelimitations of outcome measures (see Charman etal., 2003; Lord et al., 2005; Rogers, 1998). Thevery small number of evaluations conducted byresearchers who had no direct involvement in thetherapy is another source of concern. Althoughthe research base for studies involving behavioralinterventions is, in general, methodologicallystronger than for many other types of interven-tion, it is clear from our review that none of eventhe better controlled EIBI studies met the mostrigorous standards for intervention methodology(National Research Council, 2001). Moreover, dif-ferences in therapeutic intensity, in participants,and in intake and outcome measures have led toconsiderable disagreement and controversyamong researchers and professionals. In turn, thishas resulted in confusion and distress for manyparents of young children with autism spectrumdisorders, who are faced with conflicting claims ofeffectiveness when seeking appropriate treatment.
There is little question now that early inten-sive behavioral intervention is highly effective forsome children. However, gains are not universal,and some children make only modest progresswhile others show little or no change, sometimesafter extremely lengthy periods in treatment. Gur-alnick (2005) noted that one of the most impor-tant tasks in autism early intervention research isto understand why outcomes vary so dramaticallyacross different children, and the crucial questionto be systematically addressed is for which chil-dren is EIBI most and least effective? Unfortu-nately, because of the focus on group differences,existing research provides only limited informa-tion on the outcome for individual children andfew data on moderators or mediators of therapy(Lord et al., 2005; Yoder & Compton, 2004). It isalmost impossible to draw reliable conclusionsabout possible child, family, or environmentalvariables associated with outcome when moststudies involve relatively small numbers of partic-ipants. More detailed, multisite studies with largesamples (see the current United Kingdom Pre-School Autism Communication Trial (2008) for arare exception) and the sharing of data on indi-vidual cases are necessary for such investigations.At the very least, when sample size is small, as iscurrently the case for most treatment evaluationstudies, it is important that more detailed infor-mation on individual differences is presented, inorder to ensure that group differences are not due

� American Association on Intellectual and Developmental Disabilities 37
VOLUME 114, NUMBER 1: 23–41 � JANUARY 2009 AJIDD
Early intensive behavioral interventions P. Howlin, I. Magiati, and T. Charman
mainly to improvements in a small subgroup ofindividuals.
Furthermore, from the papers reviewed here,there is an indication that the immediate impactof EIBI reduces over time, with the first year ofintervention appearing to produce the most sub-stantial gains, at least in IQ. EIBI is a relativelyexpensive form of intervention, and the cost canbe a major deterrent for many parents and foreducation authorities who may be asked to pro-vide funding. The demands on family life are alsoconsiderable. Clearer evidence concerning boththe optimal duration of therapy and the age atwhich it should begin could result in the devel-opment of better targeted, more cost effective pro-grams that could then be made more widely ac-cessible to families. There is also a need to dem-onstrate that EIBI is substantially more effectivethan alternative, high quality autism specific in-terventions, such as specialized preschool provi-sion. In the majority of the studies included inthis review, the alternative intervention has gen-erally been of lower intensity and/or lesser quality(certainly in terms of autism expertise) than theEIBI program to which it is compared. In addi-tion, the failure to control for time in interventionmeans that in some studies the fact that EIBI ap-pears to be more effective than the comparisoncondition could be due simply to differences intreatment intensity, not quality. As noted above,a systematic meta-analysis is required in order toexplore both child and intervention variables thatmay be related to outcome. However, given thevariability of data, it is likely that such an analysisat the present time could only assess the role of avery limited number of variables.
Conclusions and Recommendationsfor Future Research
Since we initially submitted this paper, oneother comprehensive review of early intensive be-havioral interventions based on the UCLA YoungAutism Project model has been published (Rei-chow & Wolery, 2008). Although that analysiswas focused on some different issues and includespapers that did not meet our criteria for inclusion,the principal conclusion parallels our own; that is,there is strong evidence that EIBI is effective forsome, but not all, children with autism spectrumdisorders, and there is wide variability in responseto treatment. The data we present in this reviewalso suggest that if gains are made, they are likely
to be greatest in the first 12 months of interven-tion. It is evident, too, that in recent studies re-searchers have followed some of the recommen-dations arising from earlier reviews (e.g., Lord etal., 2005; Rogers, 1988; Smith et al., 2007), in par-ticular by including a wider range of child mea-sures, especially those related to social and com-munication skills. However, broader measures offamily functioning are rarely included and as yetthere are no data on how these may affect out-come. There remains a dearth of randomized con-trol trials, which are needed in order to provideunbiased evidence of efficacy.
If research and practice in the area of earlyintervention for children with autism are to im-prove, it is clear that increasing the number ofrandomized control trials should be made a highpriority. Nevertheless, because the number of pri-mary outcome measures of such trials is, of ne-cessity, limited, other case control comparisonstudies will continue to be needed but with ad-equate sample sizes in order to explore individualvariables associated with outcome. For such stud-ies to be informative, the following minimum re-quirements need to be adequately addressed: (a)Baseline data on participants should be collectedimmediately prior to, or at the very beginning, ofthe intervention program. (b) The age at whichindividual children begin treatment, the durationand intensity of treatment (measured in hours perweek), and the exact time to follow-up, should bemade explicit. (c) The same data should be avail-able for children in the comparison conditions,with as much additional information as possibleprovided in order to enable readers to assess thetrue quality of that intervention. (d) Data on childvariables need to be better standardized. Assess-ments used should include those currently in gen-eral use (IQ, VABS, language comprehension andexpression), but additional measures of behavioraldisturbance (e.g., the Developmental BehaviourChecklist: Einfeld & Tonge, 1995) are also re-quired. Standard scores, age equivalent scores, andraw scores (at least in an online appendix) shouldbe reported for all assessments. (e) Diagnostic sta-tus should be clearly defined using the ADI-R andADOS-G because these instruments can also beused to monitor changes in autistic symptomatol-ogy over time. (f) Measures of family functioningneed to be included; not only data on marital andeconomic status, but also measures (such as thoseemployed by Remington et al., 2007) of parentalwell-being and support.

38 � American Association on Intellectual and Developmental Disabilities
VOLUME 114, NUMBER 1: 23–41 � JANUARY 2009 AJIDD
Early intensive behavioral interventions P. Howlin, I. Magiati, and T. Charman
Finally, it is important to recognize that au-tism is a highly complex and heterogeneous dis-order characterized by impairments in social be-havior, in communication, and in many aspectsof learning, together with fundamental problemsin acquiring functional, adaptive, and flexible be-haviors. Although behavioral approaches are animportant element of any comprehensive pro-gram (perhaps especially in the early years), otherelements that focus more specifically on social de-velopment and communication will also be re-quired for optimal effectiveness. This will also re-quire more development of appropriate measuresof social and communicative competence to assesschanges in these skills (Lord et al., 2005). More-over, wide variation in child characteristics and inresponsiveness to treatment may require a farmore individualized approach to interventionthan can be delivered using manualized treatmentpackages.
There is good evidence now, from a numberof randomized control trials (Aldred et al., 2004;Howlin et al., 2007; Kasari et al., 2006; Yoder &Stone, 2006), that other, nonintensive interven-tions, particularly those with a focus on commu-nication and joint social interaction, can have asignificant and positive impact on children’s func-tioning. A switch of focus to examining the com-parative effects of interventions with a strong ev-idence base, called equivalence trials, rather thansimply comparing high quality interventions withlow quality/low intensity alternatives, is likely tobe of benefit to many more children and theirfamilies. Assessing what treatments work forwhich children and identifying the individualcharacteristics that predict responsiveness to spe-cific programs and approaches are the challengesthat lie ahead.
References (* indicates reference ishighlighted in tables)Aldred, C., Green, J., & Adams, C. (2004). A new
social communication intervention for chil-dren with autism: Pilot randomized con-trolled treatment study suggesting effective-ness. Journal of Child Psychology and Psychiatry,45, 1420–1430.
Anderson, S. R., & Romanczyk, R. G. (1999). Ear-ly intervention for young children with au-tism: Continuum-based behavioral models.Journal of the Association for Persons with SevereHandicaps, 24, 162–173.
Baer, D. (1993). Quasi random assignment can beas convincing as random assignment. Ameri-can Journal on Mental Retardation, 97, 373–375.
Barbera, M. L., & Rasmussen, T. (2007). The verbalbehavior approach: How to teach children withautism and related disorders. London: JessicaKingsley.
Bondy, A. S., & Frost, L. A. (1998). The PictureExchange Communication System. Seminarsin Speech and Language, 19, 373–389.
Charman, T. (2004). Matching preschool childrenwith autism spectrum disorders and compar-ison children for language ability: Methodo-logical challenges. Journal of Autism and De-velopmental Disorders, 34, 59–64.
Charman, T., & Howlin, P. (with Aldred, C.,Baird, G., degli Espinosa, F., Diggle, T., Kov-shoff, H., Law, J., et al.). (2003). Research intoearly intervention for children with autismand related disorders: Methodological and de-sign issues. Autism, 7, 217–225.
*Cohen, H., Amerine-Dickens, M. S., & Smith,T. (2006). Early Intensive Behavioral Treat-ment: Replication of the UCLA model in acommunity setting. Journal of Developmentaland Behavioral Pediatrics, 27, S2, 145–155.
Drew, A., Baird, G., Baron-Cohen, S., Cox, A.,Slonims, V., Wheelwright, S., Swettenham, J.,Berry, B., & Charman, T. (2002). A pilot ran-domised control trial of a parent training in-tervention for pre-school children withautism Preliminary findings and methodo-logical challenges. European Child and Adoles-cent Psychiatry, 11, 266–272.
Dunlap, G., Kern-Dunlap, L., Clark, S., & Rob-bins, F. (1991). Functional assessment, curric-ular revision, and severe problem behaviors.Journal of Applied Behavior Analysis, 4, 387–397.
Einfeld, S. L., & Tonge, B. J. (1995). The Devel-opmental Behaviour Checklist: The develop-ment and validation of an instrument to as-sess behavioural and emotional disturbance inchildren and adolescents with mental retar-dation. Journal of Autism and DevelopmentalDisorders, 25, 81–104.
*Eikeseth, S., Smith, T., Jahr, E., & Eldevik, S.(2002). Intensive behavioral treatment atschool for 4- to 7-year-old children with au-tism: A one-year comparison controlledstudy. Behavior Modification, 26, 49–68.
*Eikeseth, S., Smith, T., Jahr, E. & Eldevik, S.

� American Association on Intellectual and Developmental Disabilities 39
VOLUME 114, NUMBER 1: 23–41 � JANUARY 2009 AJIDD
Early intensive behavioral interventions P. Howlin, I. Magiati, and T. Charman
(2007). Outcome for children who began in-tensive behavioral treatment between ages 4-7: A comparison controlled study. BehaviorModification, 31, 264–278.
*Eldevik, S., Eikeseth, S., Jahr, E., & Smith, T.(2006). Effects of low intensity behavioraltreatment for children with autism and men-tal retardation. Journal of Autism and Develop-mental Disorders, 36, 211–224.
Greenspan, S. L., & Wieder, S. (2003). Engagingautism: The Floortime Approach to helping chil-dren relate, communicate and think. Jackson,TN: Perseus Books.
Guralnick, M. (2005). Early intervention for chil-dren with intellectual disabilities: Currentknowledge and future prospects. Journal ofApplied Research in Intellectual Disabilities, 18,313–324.
Handleman, J. S., Harris, S. L., Arnold, M., Gor-don, R., & Cohen, M. (2006). The DouglassDevelopmental Disabilities Center: Optionsfor school-age students. In J. S. Handleman,& S. L. Harris (Eds.), School-age education pro-grams for children with autism. The in-betweenyears (pp. 89–113). Austin, TX: Pro-Ed.
*Howard, J. S., Sparkman, C. R., Cohen, H. G.,Green, G., & Stanislaw, H. (2005). A compar-ison of intensive behavior analytic and eclec-tic treatments for young children with autism.Research in Developmental Disabilities, 26, 359–383.
Howlin, P. (2006). Augmentative and alternativecommunication systems for children with au-tism. In T. Charman & W. Stone (Eds.), Socialand communication development in autism spec-trum disorders (pp. 236–266). New York: Guil-ford Press.
Howlin, P., Gordon, K., Pasco, G., Wade, A., &Charman, T. (2007). A group randomised,controlled trial of the Picture Exchange Com-munication System for children with autism.Journal of Child Psychology and Psychiatry, 48,473–481.
Jacobson, N. S., & Truax, P. (1991). Clinical sig-nificance: A statistical approach to definingmeaningful change in psychotherapy re-search. Journal of Consulting and Clinical Psy-chology, 59, 12–19.
Kasari, C., Freeman, S., & Paparella, T. (2006).Joint attention and symbolic play in youngchildren with autism: A randomized con-trolled intervention study. Journal of Child Psy-chology and Psychiatry, 47, 611–620.
Kaufman, B. N. (1994). Son-Rise: The miracle con-tinues. Tiburon, CA: Kramer.
Levy, S., Kim, A.-H., & Olive, M. (2006). Inter-ventions for young children with autism: Asynthesis of the literature. Focus on Autism andOther Developmental Disabilities, 21, 55–62.
Lord, C., Risi, S., Lambrecht, L., Cook, E. H.,Leventhal, B. L., DiLavore, P. C., Pickles, A.,& Rutter, M. (2000). The Autism DiagnosticObservation Schedule-Generic: A standardmeasure of social and communication deficitsassociated with the spectrum of autism. Jour-nal of Autism and Developmental Disorders, 30,205–223.
Lord, C., Rutter, M., & Le Couteur, A. (1994).Autistic Diagnostic Interview–Revised: A re-vised version of a diagnostic interview forcaregivers of individuals with possible perva-sive developmental disorders. Journal of Au-tism and Developmental Disorders, 24, 659–686.
Lord, C., Wagner, A., Rogers, S., Szatmari, P.,Aman, M., Charman, T., et al. (2005). Chal-lenges in evaluating psychosocial interven-tions for autistic spectrum disorders. Journalof Autism and Developmental Disorders, 35,695–711.
*Lovaas, O. I. (1987). Behavioral treatment andnormal educational and intellectual function-ing in young autistic children. Journal of Con-sulting and Clinical Psychology, 55, 3–9.
Lovaas, O. I., Ackerman, A., Alexander, D., Fire-stone, P., Perkins, M., Young, D. B., et al.(1981). Teaching developmentally disabled chil-dren: The ME book. Austin, TX: Pro-Ed.
*Magiati, I., Charman, T., & Howlin, P. (2007). Atwo-year prospective follow-up study of com-munity-based early intensive behavioural in-tervention and specialist nursery provision forchildren with autism spectrum disorders. Jour-nal of Child Psychology and Psychiatry, 48, 803–812.
Magiati, I., & Howlin, P. (2001). Monitoring theprogress of pre-school children with autismenrolled in early intervention programmes:Problems of cognitive assessment. Autism, 5,399–406.
Maine Administrators of Services for ChildrenWith Disabilities (MADSEC). (1999). Reportof the MADSEC Autism Task Force, Man-chester, ME: Author.
Maurice, C., Green, G., & Foxx, R. M. (Eds.),(2001). Making a difference: Behavioral interven-tion for autism. Austin, TX: Pro-Ed.
40 � American Association on Intellectual and Developmental Disabilities
VOLUME 114, NUMBER 1: 23–41 � JANUARY 2009 AJIDD
Early intensive behavioral interventions P. Howlin, I. Magiati, and T. Charman
Maurice, C., Green, G., & Luce, S. (Eds.). (1996).Behavioral intervention for young children withautism: A manual for parents and professionals.Austin, TX: Pro-Ed.
*McEachin, J. J., Smith, T., & Lovaas, O. I.(1993). Long-term outcome for children withautism who received early intensive behavior-al treatment. American Journal on Mental Re-tardation, 97, 359–372
Mesibov, G. B. (1993). Treatment outcome is en-couraging: Comments on McEachin et al.American Journal on Mental Retardation, 97,379–380.
Mundy, P. (1993). Normal versus high-function-ing status in children with autism (Commentson McEachin, Smith, and Lovaas). AmericanJournal on Mental Retardation, 97, 373–391.
National Initiative for Autism: Screening and As-sessment (NIASA). (2003). National AutismPlan for Children (NAPC). Plan for the identifi-cation, assessment, diagnosis and access to earlyinterventions for pre-school and primary schoolaged children with ASD. London: National Au-tistic Society.
National Research Council. (2001). Educating chil-dren with autism (Committee on EducationalInterventions for Children With Autism, Di-vision of Behavioral and Social Sciences andEducation). Washington, DC: National Acad-emy Press.
New York State Department of Health Early Inter-vention Program. (2000). Clinical practice guide-line: Report of the Recommendations for Autism/Pervasive Developmental Disorders: Assessment andintervention for young children (age 0–3 years). Re-trieved October, 10, 2000, from http://www.health.state.ny.us/nysdoh/eip/autism/index.htm
New Zealand Ministry of Health. (2006). Evidencebased guidelines for autism spectrum disorders(Draft report). Wellington, NZ: Author.
Partington, J. W., & Sundberg, M. L. (1998). TheAssessment of Basic Language and LearningSkills: An assessment, curriculum guide andtracking system for children with autism orother developmental disabilities. Danville,CA: Behavior Analysts.
Pre-School Autism Communication Trial (PACT).(2008). Retrieved September 29, 2008, fromhttp://www.medicine.manchester.ac.uk/pact
Quill, K., Gurry, S., & Larkin, A. (1989). Daily lifetherapy: A Japanese model for educating chil-
dren with autism. Journal of Autism and De-velopmental Disorders, 19, 625–635.
Reichow, B., & Wolery, M. (2008). Comprehen-sive synthesis of early intervention behavioralinterventions for young children with autismbased on the UCLA Young Autism Projectmodel. Journal of Autism and DevelopmentalDisorders. DOI 0. 1007/S10803-008-0596-0
*Remington, B., Hastings, R. P., Kovshoff, H., de-gli Espinosa, F., Jahr, E., Brown, T., et al.(2007). Early intensive behavioral interven-tion: Outcomes for children with autism andtheir parents after two years. American Journalon Mental Retardation, 112, 418–438.
Research Autism. (2007). Retriever August 9,2007, from http://www.researchautism.net/pages/welcome/home.ikml
Roberts, J. M. (2004). A review of the research toidentify the most effective models of best practice inthe management of children with autism spectrumdisorders. Centre for Disability Studies, Uni-versity of Sydney, Australia.
Rogers, S. J. (1998). Empirically supported com-prehensive treatments for young childrenwith autism. Journal of Clinical Child Psycholo-gy, 27, 168–179.
Rogers, S. J., Hayden, D., Hepburn, S., Charlifue-Smith, R., Hall, T., & Hayes, A. (2006).Teaching young nonverbal children with au-tism useful speech: A pilot study of the Den-ver model and PROMPT interventions. Jour-nal of Autism and Developmental Disorders, 36,1007–1024.
*Sallows, G. O., & Graupner, T. D. (2005). Inten-sive behavioral treatment for children with au-tism: Four-year outcome and predictors.American Journal on Mental Retardation, 110,417–438.
Schopler, E. (1997). Implementation of TEACCHphilosophy. In D. J. Cohen & F. R. Volkmar(Eds.), Handbook of autism and pervasive devel-opmental disorders. (2nd ed., pp. 767–798).New York: Wiley.
Schreibman, L., & Koegel, R. L. (2005). Trainingfor parents of children with autism: Pivotalresponses, generalization, and individualiza-tion of interventions. In E. D. Hibbs & P. S.Jensen (Eds.), Psychosocial treatment for childand adolescent disorders: Empirically based strat-egies for clinical practice (2nd ed., pp. 605–631).Washington, DC: American PsychologicalAssociation.
Scottish Intercollegiate Guidelines Network

� American Association on Intellectual and Developmental Disabilities 41
VOLUME 114, NUMBER 1: 23–41 � JANUARY 2009 AJIDD
Early intensive behavioral interventions P. Howlin, I. Magiati, and T. Charman
(SIGN). (2007). Assessment, diagnosis, and clin-ical interventions for children and young peoplewith autism spectrum disorders. Edinburgh Scot-land: National Health Service Education forScotland.
Shea, V. (2004). A perspective on the research lit-erature related to early intensive behaviouralintervention (Lovaas) for young children withautism. Autism, 8, 349–367.
*Sheinkopf, S. J., & Siegel, B. (1998). Home-basedbehavioral treatment of young children withautism. Journal of Autism and DevelopmentalDisorders, 28, 15–23.
Shields, J. (2001). The NAS Early Bird pro-gramme: Partnership with parents in early in-tervention. Autism, 5, 49–56.
Skinner, B. F. (1953). Science and human behavior.New York: Macmillan.
Smith, T., Donahoe, P. A., & Davis, B. J. (2006).The UCLA Young Autism Project. In J. S.Handleman & S. L. Harris (Eds.), Preschool ed-ucation programs for children with autism (2nded., pp. 29–48). Austin, TX: Pro-Ed.
Smith, T., Eikeseth, S., Klevstrand, M., & Lovaas,I. (1997). Intensive behavioral treatment forpreschoolers with severe mental retardationand pervasive developmental disorder. Amer-ican Journal on Mental Retardation, 102, 238–249.
*Smith, T., Groen, A. D., & Wynn, J. W. (2000).Randomized trial of intensive early interven-tion for children with pervasive developmen-tal disorder. American Journal on Mental Retar-dation, 105, 269–285
*Smith, T., Scahill, L., Dawson, G., Guthrie, D.,Lord, C., Odom, S., et al. (2007). Designingresearch studies on psychosocial interventionsin autism. Journal of Autism and DevelopmentalDisorders, 37, 354–366.
Sparrow, S. S., Balla, D., & Cicchetti, D. V.(1984). Vineland Adaptive Behavior Scales. Cir-cle Pines, MN: American Guidance Service.
Sundberg, M. L., & Partington, J. W. (1999). Theneed for both discrete trial and natural envi-ronmental language training for children withautism. In P. M. Ghezzi, W. L. Williams, &J. E. Carr (Eds.), Autism behavior analytic per-spectives (pp. 139–156). Reno, NV: ContextPress.
Sussman, F. (1999). More than words: Helping par-ents promote communication and social skills inchildren with autism spectrum disorders. Toronto:Hanen Center.
Wheeler, J. J., Baggett, B. A., Fox, J., & Blevins,L. (2006). Treatment integrity: A review of in-tervention studies conducted with childrenwith autism. Focus on Autism and Other Devel-opmental Disabilities, 21, 45–54.
Williams, K. W., Wray, J. J., & Wheeler, D. M.(2005). Intravenous secretin for autism spec-trum disorder. Cochrane Database SystematicReviews, 20, CD003495.
Wirt, R. D., Lachar, D., Klinedinst, J. K., & Seat,P. D. (1984). Multi-dimensional description ofchild personality: A manual for the PersonalityInventory for Children. Los Angeles: WesternPsychological Services.
Yoder, P. J., & Compton, D. (2004). Identifyingpredictors of treatment response. Mental Re-tardation and Developmental Disabilities ResearchReviews, 10, 162–168.
Yoder, P. J., & Stone, W. L. (2006). Randomizedcomparison of two communication interven-tions for preschoolers with autism spectrumdisorders. Journal of Consulting and ClinicalPsychology, 74, 426–235.
Received 9/3/07, accepted 1/16/08.Editor-in-charge: William E. MacLean, Jr.
Correspondence regarding this article should besent to Patricia Howlin, Department of Psychol-ogy, Institute of Psychiatry, Henry WellcomeBldg., PO 77, De Crespigny Park, London SE58AF, UK. E-mail: [email protected]