syndrome of acrofacial dysostosis, cleft lip/palate, and triphalangeal thumb in a brazilian family
TRANSCRIPT
American Journal of Medical Genetics 14:225-229 (1983)
Brief Clinical Report: Syndrome of Acrofacial Dysostosis, Cleft Lip/Palate, and Triphalangeal Thumb in a Brazilian Family
A. Richieri-Costa, Thomaz R. Gollop, and G.M.D.D. Colletto
Human Genetics Laboratory, Department of Biology, Universidade de Siio Paulo (A.R.-C., G.M. D.D.C.), and Semi60 de Genetica Humana da Associaddo Maternidade de Sdo Paulo (7: R. G.), Siio Paulo, Brazil
We describe two daughters of a nonconsanguineous couple. Both had facial and skeletal anomalies, but in quantitatively and qualitatively different ways. In one patient signs of mandibulofacial dysostosis are associated with anomalies of the radial rays of both arms. In the other, cleft lip and cleft palate are associated with hypoplastic thumbs. Clinical and genetical aspects of present case are discussed.
Key words: Nager syndrome, acrofacial dysostosis, mandibulofacial dysostosis, cleft lip/palate, triphalangeal thumbs, autosomal-recessive inheritance
INTRODUCTION
The acrofacial dysostoses are a phenotypically and genetically heterogeneous group of conditions; some half dozen different autosomal-dominant and autosomal- recessive forms have been identified [Halal et al, 19821. Here we report an acrofacial dysostosis syndrome in two sisters which seems different from any of the previously described types.
REPORTS OF PATIENTS Patient 1
L.A.L. (Fig. l) , female, Caucasian, born in 1980, sister of patient 2. Gestation was normal. No exposure to toxic or infectious agents or to x-rays. No trauma was
Received for publication October 8, 1981; revision received June 22, 1982.
Address reprint requests to A. Richieri-Costa, Departamento de Biologia, Universidade de SIo Paulo, Caixa Postal 11.461, CEP 0542 1, SBo Paulo, SP, Brasil.
0148-7299/83/1402-0225$02.00 0 1983 Alan R. Liss, Inc.

226 Richieri-Costa, Gollop, and Colletto
Fig. 1. Frontal (a) and lateral views (b) of patient 1.
Fig. 2. Hands of patient 1. Fig. 3. Roentgenograms of hands of patient 1.
reported. Vaginal delivery at term. Birth weight 2,900 g, length 47 cm, and occipi- tofrontal head circumference (OFC) was 34.5 cm. Her parents had no related abnor- malities and were not consanguineous. There are four normal sibs. A bilaterally cleft lip and a wide cleft of palate were noted at birth.
Examination at 15 months showed an active girl with normal neuropsychological development for age. Weight was 10.2 kg, length 75 cm, and OFC 45 cm. There was frontal bossing. Lip clefts had been repaired but palate was bilaterally cleft; she had mild malar hypoplasia and normal ears. The thumbs were hypoplastic and cone- shaped (Fig. 2).
Roentgenograms showed a wide gap in the median portion of maxilla and palate; mild bilateral shortness of the first metacarpals, marked hypoplasia of the phalanges of the thumbs (Fig. 3); absence of the distal ossification center of the radius, of the distal ossification centers of the metacarpals and of the proximal centers of the proximal phalanges; underdevelopment of the carpal ossification centers; and a bone age of 6 months. Results of renal ultrasonography were normal. No other skeletal abnormalities were found. C-banded chromosomes (peripheral lymphocytes) were normal. Dermatoglyphics showed left simian crease, increased atd angles (Table 1).
An Acrofacial Dysostosis Syndrome 227
Patient 2
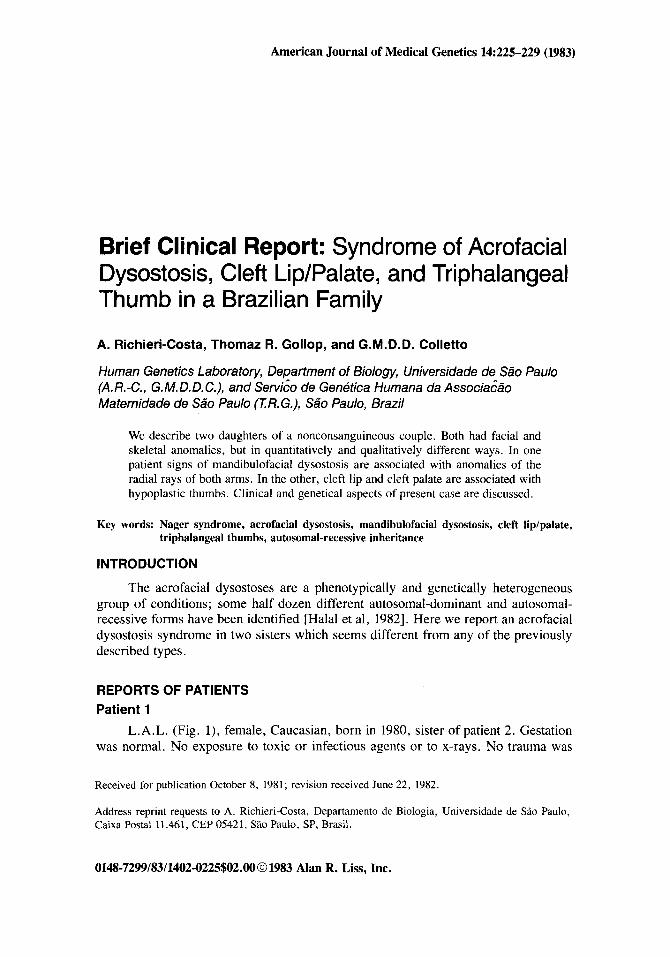
L.L.L. (Fig. 4), female, Caucasian, born in 1960. Gestation was normal, no exposure to toxic or infectious agents or x-rays, no trauma was reported. Vaginal delivery at term. Neuropsychological development was normal. At 22 years she was a shy woman with normal intellect. The OFC was 54.5 cm, height 142 cm, weight
TABLE I. Dermatoglyphic Findings in Present Family
Father Mother Case 1 Case 2 Sister 1 Sister 2 Brother 1 Brother 2 _ _ _ ~ ~ _ _ _ _ _ _ ~ _ _ _ _ ~ MainLines L R L R L R L R L R L R L R L R
A 1 3 5 ' 5 ' 1 1 1 1 1 4 4 3 5 ' 4 3 4 4 B C 7 9 9 9 7 9 1 9 7 7 9 9 7 7 7 7 D 9 9 9 1 1 9 1 1 1 9 9 9 9 9 9 9 9 9 T 11 13' 13' 13' 11 I 1 - 11 13' 13' 13' 13' 13' 13' 13' 13' atdAngle 35" 44" 43" 39" 64" 60" - 147" 50" 50" 50" 57" 73" 44" 50" 39"
5" 5" 5" 7 5 ' 7 1 5" 5" 7 5" 7 5" 5" 5" 5"
a
Fig. 4. Frontal (a) and lateral (b,c) views of patient 2.
228 Richieri-Costa, Gollop, and Colletto
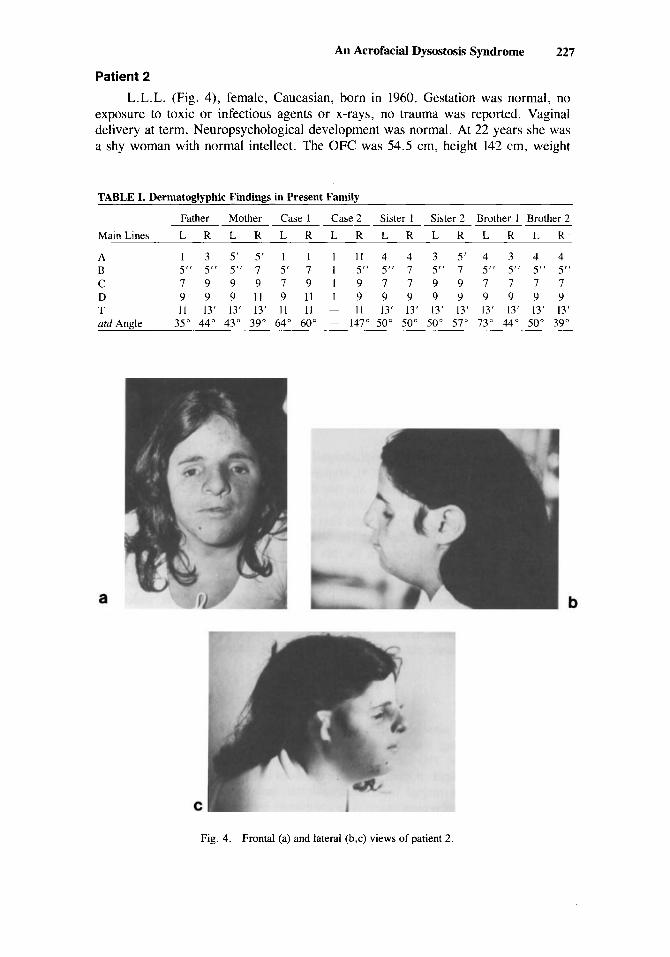
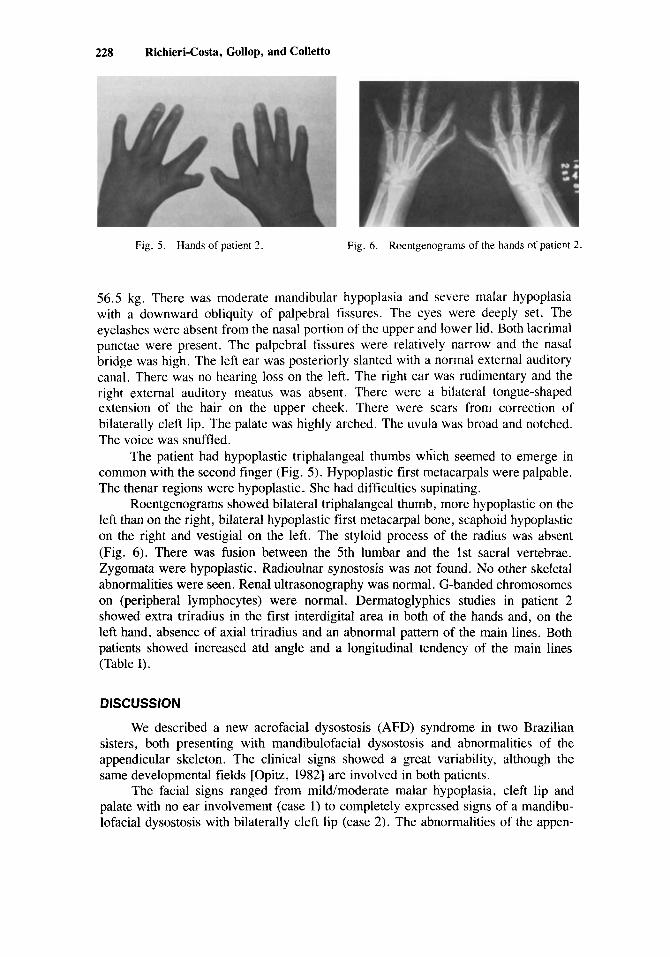
Fig. 5 . Hands of patient 2. Fig. 6 . Roentgenograms of the hands of patient 2.
56.5 kg. There was moderate mandibular hypoplasia and severe malar hypoplasia with a downward obliquity of palpebral fissures. The eyes were deeply set. The eyelashes were absent from the nasal portion of the upper and lower lid. Both lacrimal punctae were present. The palpebral fissures were relatively narrow and the nasal bridge was high. The left ear was posteriorly slanted with a normal external auditory canal. There was no hearing loss on the left. The right ear was rudimentary and the right external auditory meatus was absent. There were a bilateral tongue-shaped extension of the hair on the upper cheek. There were scars from correction of bilaterally cleft lip. The palate was highly arched. The uvula was broad and notched. The voice was snuffled.
The patient had hypoplastic triphalangeal thumbs which seemed to emerge in common with the second finger (Fig. 5). Hypoplastic first metacarpals were palpable. The thenar regions were hypoplastic. She had difficulties supinating.
Roentgenograms showed bilateral triphalangeal thumb, more hypoplastic on the left than on the right, bilateral hypoplastic first metacarpal bone, scaphoid hypoplastic on the right and vestigial on the left. The styloid process of the radius was absent (Fig. 6) . There was fusion between the 5th lumbar and the 1st sacral vertebrae. Zygomata were hypoplastic. Radioulnar synostosis was not found. No other skeletal abnormalities were seen. Renal ultrasonography was normal. G-banded chromosomes on (peripheral lymphocytes) were normal. Dermatoglyphics studies in patient 2 showed extra triradius in the first interdigital area in both of the hands and, on the left hand, absence of axial triradius and an abnormal pattern of the main lines. Both patients showed increased atd angle and a longitudinal tendency of the main lines (Table I).
DISCUSSION
We described a new acrofacial dysostosis (AFD) syndrome in two Brazilian sisters, both presenting with mandibulofacial dysostosis and abnormalities of the appendicular skeleton. The clinical signs showed a great variability, although the same developmental fields [Opitz, 19821 are involved in both patients.
The facial signs ranged from mild/moderate malar hypoplasia, cleft lip and palate with no ear involvement (case 1) to completely expressed signs of a mandibu- lofacial dysostosis with bilaterally cleft lip (case 2). The abnormalities of the appen-

An Acrofacial Dysostosis Syndrome 229
dicular skeleton ranged from thumb hypoplasia (case 1) to hypoplastic metacarpals and triphalangeal thumbs (case 2).
Halal et a1 [ 19821 have delineated four AFD syndromes besides Nager acrofacial dysostosis: 1) AFD postaxial defect syndrome; 2) AFD split-foot syndrome; 3) AFD distal dup (2q) syndrome; and 4) the AFD cardiomelic syndrome. The nature of the involvement of the appendicular skeleton is a nosologically valuable sign to differen- tiate between AFD syndrome described here and the AFD postaxial defect syndrome [Miller et al, 19791, the AFD split-foot syndrome [Fontaine et al, 19741 and the AFD distal dup (2q) syndrome [Zankl et al, 19791. The presence of cleft lip/palate in the present cases and the absence of cardiac involvement and club arm deformity also excludes the AFD cardiomelic syndrome [Burton and Nadler, 19771.
The main differential diagnosis in the present family is with Nager AFD. In this syndrome signs of mandibulofacial dysostosis are associated with abnormalities of the radial ray, the occurence of cleft palate is significantly high, and the acral anomalies in upper limbs range from thumb hypoplasia to absence of the radial ray [Halal et al, 19821. No references of cleft lip and triphalangeal thumb were made in the cases reported with Nager syndrome [Halal et al, 19823. The findings in the patients here reported suggests that our patients do not have the Nager syndrome.
Although there was no parental consanguinity in the cases here reported, the absence of signs in the parents and in the four normal sibs of the affected patients suggests autosomal-recessive inheritance with variable expressivity.
REFERENCES
Burton BK, Nadler HL (1977): Nager acrofacial dysostosis. Report of a case. J Pediatr 91:84-86. Fontaine G, Farriaux JP, Delattre P, Gidlecki Z, Poupard B, Durieux G , Piquet JJ (1974): Une
observation familiale du syndrome ectrodactylie et dysostose mandibulo-faciale. J Genet hum
Halal F, Herrmann J, Pallister PD, Opitz JM, Desgranges M-F, Grenier G (1982): Acrofacial dysostosis syndromes: Report of four patients with Nager syndrome and delineation of four further acrofacial dysostosis syndromes. Am J Med Genet 14:000-000.
Miller M, Fineman R, Smith DW (1979): Postaxial acrofacial dysostosis syndrome. J Pediatr 95:970- 975.
Opitz JM (1982): The developmental field concept in clinical genetics. J Pediatr (in press). Zankl M, Schwanitz G, Scmid P, Zankl H, Dockter G, Rodewald A, Zang KD, Grosse KP (1979):
Distal 2q duplication: Report of two familial cases and an attempt to define a syndrome. Am J Med Genet 4:s-16.
22:289-307.
Edited by John M. Opitz