sutherland 2
TRANSCRIPT
8/6/2019 Sutherland 2
http://slidepdf.com/reader/full/sutherland-2 1/21
Gait and Posture 16 (2002) 159–179
The evolution of clinical gait analysisPart II Kinematics
D.H. Sutherland *
Children’ s Hospital San Diego, 3020 Children’ s Way MC 5054 , San Diego, CA, USA 92123 -4282
Accepted 18 December 2001
Abstract
Kinematics is treated as a single topic in this manuscript and the emphasis is on early history, just as it was in Part I,
Electromyography. Needless to say, neither kinematics nor electromyography, nor kinetics and energy (the latter to be included
in Part III) are stand-alone components of clinical gait analysis. The only reason for this selective format is that it lessens my task
to be able to write about one subject at a time. One of the consequences of this arbitrary separation is that some contributors,
who have enriched more than one portion of clinical gait analysis, are highlighted only in the area in which they have contributed
the most. I began with Kinesiological Electromyography in Part I because the earliest stirrings of the dream of clinical gait
analysis were expressed in the development of KEMG (kinesiological electromyography). The early investigators realized that very
little could be said about the dynamic action of muscles without KEMG. Next, in chronological order, came kinematics. I have
been an active participant and eyewitness, and take full responsibility for attempting to write an early history at a time when most
of the contributors are still alive. Ordinarily, history is written much later, in order to fully grasp the significance of individual
contributions in the tapestry of the whole. As stated in Part I, Electromyography, the emphasis has been placed on the early
history. The application of motion analysis to sports medicine, and sports medicine functional analysis, is covered only lightlyhere, and this should not be interpreted as minimizing its importance. The literature on this subject is now quite voluminous and
it would not be possible to cover it adequately in this manuscript. Later historical writings may differ significantly and will
hopefully give more recognition to pioneers in later generations: those physicians, engineers, physical therapists and kinesiologists
who are lifting the level of clinical gait analysis and directing their energies in expanding clinical directions. It is hoped that this
manuscript will prompt additional manuscripts, as well as letters to the editor of Gait and Posture on the content of this review
paper. © 2002 Published by Elsevier Science B.V.
Keywords: History; Kinematics; Clinical gait analysis
www.elsevier.com/locate/gaitpost
1. Introduction
Accurate measurement of motion is central in any
scientific method of gait analysis. Measurements of
individual joint angular rotations, as well as transla-
tions of segments and of whole body mass, allow the
comparisons with normal that are necessary to distin-
guish pathological from normal gait. Complex hard-
ware and software are necessary to accomplish this task
with accuracy and reliability. This component of clini-
cal gait analysis has proven to be very challenging and
the evolutionary process continues to this day.
The individual joint angles and the displacements of
segments and of the whole body mass were recognized
to be essential measurement requirements in the late
1800s by Braun and Fischer [1– 5]. Their clever ap-
Note from re6iew editor: This article is the second in a series of
three historical narratives that Dr Sutherland has very kindly agreed
to author for Gait and Posture. As Dr Sutherland indicated in his
abstract for Part I, these are very personal accounts that focus
primarily, although not exclusively, on the early history of clinical
motion analysis. He further acknowledged that not all important
contributors or events may be chronicled or weighted in the same
manner as others might have done. Still, these accounts are extremely
valuable because they provide a very alive ‘behind the scenes’ view of
how our field has progressed over the years as told by one of its true
pioneers, with a richness that could never be captured by a mere
listing of names or documented events.
* Tel.: +1-858-966-5807; fax: +1-858-966-7494
E -mail address: [email protected] (D.H. Sutherland).
0966-6362/02/$ - see front matter © 2002 Published by Elsevier Science B.V.
PII: S 0 9 6 6 - 6 3 6 2 ( 0 2 ) 0 0 0 0 4 - 8

8/6/2019 Sutherland 2
http://slidepdf.com/reader/full/sutherland-2 2/21
D.H . Sutherland / Gait and Posture 16 (2002) 159 – 179 160
proach to kinematic analysis was to apply Geissler
tubes to the limb segments, interrupt the illumination at
regular intervals by a large tuning fork, and pho-
tograph the subject walking in total darkness with four
cameras while the lenses were open. One camera was
positioned in front of the subject, one behind, and oneon each side, making their measurements tri-dimen-
sional. The subjects were protected from electrical
shock by wearing rubber suits resembling wet suits. The
process of collecting data required 8 or 10 hours per
subject and then it involved months of work to reduce
the data and calculate kinematic measurements. This
was a fantastic scientific achievement, however, because
it was so time consuming, Braun and Fischer’s method
could only be applied in gait research.
One of the methods used by Eberhardt and Inman [6]
in the 1940s also included the use of interrupted light.
A photograph was obtained with the subject walking in
front of the open lens of a camera while carrying small
light bulbs located at the hip, knee, ankle and foot. A
slotted disk was rotated in front of the camera, produc-
ing a series of white dots at equal time intervals. These
dots could be laboriously connected to provide joint
angles that could be manually measured. Again, this
was a slow and labor-intensive process, not suitable for
clinical application. In order to examine transverse
plane rotations, Vern Inman, MD, PhD, drilled pins
into the pelvis, femur, and tibia, and recorded pin
rotation with the aid of a movie camera located above
the subject [7]. One of his subjects, David Chadwick,
MD, then a student at the University of California,Berkeley, later became the Medical Director of Chil-
dren’s Hospital of San Diego. He described his experi-
ence as ‘very painful’, something he would not have
agreed to had he understood ‘what it would be like’.
Needless to say, this technique gained very few follow-
ers, although there has been some recent use of pins
inserted into bones in normal subjects for a different
purpose, i.e. to determine the difference between move-
ment of markers taped to the skin surface and those
placed into the skeleton.
2. Early pioneers and techniques (post Inman)
2 .1. Strobe light, reflecti 6e strips and manual
goniometer
Mary Pat Murray, PhD, working at the Veteran’s
Administration Hospital in Milwaukee, Wisconsin, de-
vised a simple, effective, and low cost way to record
and measure movements. She and her team attached
reflective targets (including reflective strips in the lower
extremity) to specific anatomic landmarks and the sub-
jects walked in the illumination of a strobe light. The
resultant photograph was used to make measurements
of the individual segments. Her method did include
upper extremity and trunk markers, as well as pelvis
and lower extremity. She successfully used this method
to produce landmark articles in the 1960s, 70s and 80s
outlining the walking patterns, first of normal men [8],
then of normal women [9], and then patients withpathological conditions [10 – 12]. Although, viewed by
today’s standards, this appeared to be a crude method,
the sagittal plane joint angle measurements of normal
subjects in her publications are very similar to those
obtained with current technology, (see Fig. 1) [9]. The
primary problems with Dr Murray’s method were the
need for manual measurements of all the joint angles
and the inherent dif ficulty with the method in providing
hip, knee, and ankle joint rotations in the transverse
plane.
2 .2 . Electrogoniometry
There was a flurry of enthusiasm for recording joint
angles with electrogoniometers. The Karpovich broth-
ers were early contributors who used goniometers to
record joint angles. Their reason for using electrogo-
Fig. 1. Sagittal measurements of pelvis, hip, knee and ankle in normal
women. Reprinted from the Archives of Physical Medicine and
Rehabilitation, with permission from W.B. Saunders Company [9].

8/6/2019 Sutherland 2
http://slidepdf.com/reader/full/sutherland-2 3/21
D.H . Sutherland / Gait and Posture 16 (2002) 159 – 179 161
Fig. 2. Triaxial Goniometer as applied to a subject for bilateral hip
and ankle joint motion analysis. Reprinted from the Journal of Biomechanics, vol. 13, 1980, pp. 989 – 1006, Chao: ‘Justi fication of
triaxial goniometer for the measurement of joint rotation ’; with permis-
sion from Elsevier Science [22].
the necessity for matching the size of the individual
with the appropriate goniometers, the offset of the
recording device to the side of the limb segments, and
the inability to obtain simultaneous measurements of
all of the moving segments. Quoting from Dr Chao’s
article entitled, Justi fication of Triaxial Goniometer forthe Measurement of Joint Rotation, ‘‘This paper at-
tempts to provide the theoretical and experimental jus-
tifications of the existing triaxial goniometer design so
that these potential problems can be resolved’’ [22]. The
experimental device used for the justification was a
mechanical model, thus any problems with skin motion
were not considered. Quoting further, in the ‘Discus-
sions’ section of the article, Dr Chao states, ‘‘Although
the triaxial goniometer is the only instrument that can
provide instantaneous angular motion of a joint in
three dimensions, its user must realize the potential
drawbacks of the method in order to avoid unnecessary
complications. First of all, the external attachment of
the device could introduce error in the data due to
relative movement of the underlying soft tissues’’. Chao
goes on to mention other critical points to consider in
the use of the triaxial goniometers relating to align-
ment, lateral projection, and the weight of the measur-
ing device. Although these dif ficulties have prevented
widespread adoption of electrogoniometers for routine
clinical gait analysis, goniometers are effective when
multiple recordings are required, when studies are being
carried out outside of a motion analysis laboratory, and
when sagittal movements are suf ficient for data acquisi-
tion. A final objection yet remains: moment studiescannot be made without the measurements of the posi-
tion of joint centers in space, something that goniome-
ters do not provide.
2 .3 . Cine film and passi 6e marker systems with manual
entry of marker positions
2 .3 .1. Vanguard Motion Analyzer
Other investigators concentrated on developing pho-
tographic techniques for gait analysis. Photographic
methods have a key advantage over other techniques in
that the whole body can be included and the relation-
ship of each extremity and the trunk can be simulta-
neously viewed. The opportunities for measurement are
thus greatly expanded over prior techniques. A further
advantage is that individuals of all sizes are suitable for
clinical analysis. Initially, however, there were
formidable obstacles, including the need for excessive
time spent in reducing the data and the absence of
computer availability for storing data and performing
voluminous mathematical computations.
While casually scanning a technical journal, my eyes
focused on an advertisement for a Vanguard Motion
Analyzer. The very name was intriguing and its capabil-
ity for projection of movie film on a backlit screen for
niometers was that many gait cycles could be collected
quickly, and analog graphs of motion could be dis-
played, without the need for data reduction by hand
[13]. In 1976, Bajd et al. [14] published an article
describing online electrogoniometric gait analysis using
six precision potentiometers, giving time-dependent an-
gles in hip, knee, and ankle of both legs in the sagittal
plane. Their reasons for choosing this method of instru-
mentation were that it was suitable for online process-ing of measured data, and was simple, reliable and
inexpensive. Other important contributors to electrogo-
niometry are McLeod [15], Tata [16], Johnston and
Smidt [17], Lamoreux [18], Kinzel et al. [19] and
Townsend et al. [20]. Foort presented the electronic
recording of joint function with analog recordings of
three-dimensional hip, knee, and ankle joint motion
[21] at a workshop on Human Locomotion and Clinical
Analysis of Gait in Philadelphia, in 1976. Edmund Y.S.
Chao, PhD published a report in 1980 on the design of
a triaxial goniometer, based on the gyroscope concept
utilizing Eulerian angles in the computation of the
measurements (see Fig. 2) [22]. Again, this did not gain
wide acceptance, arguably because of the dif ficulty in
preventing cross talk from the three motion axes. An
anecdotal description by Jacquelin Perry (unpublished)
of significant motion recorded in the hip joint of a
patient with a solid hip fusion did not help promote
adoption of this method. At first glance, the goniomet-
ric method holds great appeal. However, with the
tremendous range of height and weight of subjects, and
the dif ficulty for small subjects to walk comfortably
with this amount of hardware, widespread adoption of
this technique never occurred. The dif ficulties encoun-
tered with the use of goniometers, then and now, are

8/6/2019 Sutherland 2
http://slidepdf.com/reader/full/sutherland-2 4/21
D.H . Sutherland / Gait and Posture 16 (2002) 159 – 179 162
easy frame-by-frame viewing, and measurement of se-
lected points with x and y coordinates, was most ap-
pealing. Dick Freeborg, later President of
Instrumentation Marketing Corporation and now a
Vice-President in the Kodak Corporation, suggested
that I contact Ray Linder at Lockheed Aircraft Corpo-ration Missiles and Space Company, Sunnyvale, Cali-
fornia. Ray Linder was the leader of a section charged
with making measurements of machines, rocket trajec-
tories, etc. In 1965, he published a description of the
methods that he and his team had developed to mea-
sure pitch, yaw, and roll, using mathematical formulae,
two or more cameras, and a two-dimensional coordi-
nate system of measurements [23]. After a telephone
call and a letter from me, Ray Linder invited me to
come to his section during their lunch hour and explain
the need for human gait measurements. Roger Mann,
MD, accompanied me. Ray Linder made a prescient
comment after our presentation to the group, ‘‘You
mean you would like to measure the movements of the
skeleton from surface markers with skin movements
confounding the interpretation. Is not that like trying
to measure the movements of a broomstick within a
gunny sack?’’ Nothing daunted, we were fascinated to
see about 17 Vanguard Motion Analyzers in one room.
We were introduced to an interested and bright group
of people employed at the task of making measure-
ments of pitch, yaw and roll. Their level of interest in
our project was very exciting. Out of this contact, John
Hagy and Richard Oyama came forward as volunteers
to the Shriners Hospital in San Francisco, bringingwith them high-speed movie cameras, generously
loaned by Lockheed Missiles and Space Company. In a
relatively short time, Hagy, Oyama, and Keller helped
us establish a system to add kinematics to the elec-
tromyography already in clinical use in our laboratory.
Hagy assisted during evenings and weekends until we
were able to persuade him to come full-time in April of
1971. John Hagy and Cecil Keller, also a Lockheed
employee, assisted in the development of our movement
measurement system, first reported in 1967 in the arti-
cle, ‘Measurement of Movements and Timing of Mus-
cle Contraction from Movie Film’ [24]. Initially, our
methods of computation were very time consuming.
After recording x and y coordinate measurements from
the cine film displayed on the Vanguard Motion Ana-
lyzer, we used a slide rule to perform the trigonometric
computations. Later, an optical encoder was added to
replace the necessity of manually recording the x and y
coordinates. This task was further simplified by utiliz-
ing a sonic digitizer to input the data (see Fig. 3) [25].
Significant progress in time reduction came when a
computer was added to store and perform the mathe-
matical calculations, (see description of our first use of
a dedicated computer by Electronic Processors, Inc. in
Appendix C). We used this method for many years, but
hand digitizing continued to be an obstacle. Individuals
were trained and employed to do the digitizing. They
were enthusiastic, but in time became bored with the
repetitious nature of their task. The average length of
time for a technician to be employed in our laboratory
was 2 – 4 years; many used this opportunity as a step-ping stone in their career.
We made use of these gait analysis data to provide
treatment recommendations and to study the outcome
of treatment intervention. Some of the papers from our
laboratory were on the subjects of crouch gait [26], gait
analysis in cerebral palsy [27], the role of the ankle
plantar flexors [28], and the pathomechanics of gait in
Duchenne muscular dystrophy [29]. When our methods
and results were given, many were enthusiastic about
the possibilities for further development of this emerg-
ing application of science, but very few were willing to
undertake such a labor-intensive effort. The real break-
through, needed to bring about widespread adoption of
three-dimensional movement measurements for clinical
gait analysis, was yet to come when the measurements
could be automated. In fact, had there been no further
improvements in technology, clinical motion analysis
might have continued in only a few locations. The time
and energy required to digitize film prevented many
centers from using gait analysis as a clinical tool. In
spite of the dif ficulties, the stage was set for
automation.
2 .4 . A turning point! Fully automated mo6ement
measurements
2 .4 .1. European contributors and techniques
Engineers and physicists deserve full credit for devel-
oping methods to automate human movement measure-
Fig. 3. Vanguard motion analyzer and Graf-Pen sonic digitizer used
to determine the X and Y coordinates of the markers shown on the
viewing screen. Reprinted with permission from the Journal of Bone
and Joint Surgery [25].
8/6/2019 Sutherland 2
http://slidepdf.com/reader/full/sutherland-2 5/21
D.H . Sutherland / Gait and Posture 16 (2002) 159 – 179 163
Fig. 4. Cat on a treadmill with reflective markers. Reprinted with
permission from Dr Hans Furnee [30].
Measurement Systems: Aspects of Data Acquisition,
Signal Processing and Performance’ [36].
J. Paul, PhD, who started his kinematic measurementswith two orthogonal Bolex cine film cameras driven by
synchronous electric motors at 50 Hz and a homemade
ground-to-foot force platform, wrote this personal letterto me in response to some questions I had posed:
‘‘As you may imagine, the processing of the cine film
and hand digitizing was an onerous procedure, and I
was therefore very excited when, in 1967, I saw the
presentation of Furnee, hybrid instrumentation inProsthetics Research Proceedings in the 7th Interna-
tional Conference on Medical and Biomedical Engi-
neering in Stockholm. Furnee presented his invention
of a single camera television system for 2-D move-
ment analysis. As soon as possible thereafter, I gottwo of our research students to develop a 2-camera
system for 3-D video/computer movement analysis.In 1972, M.O. Jarrett, and B.J. Andrews started their
PhD studies with the remit of developing the system.
Between them, they got our system up and runningbased on a PDP-12 computer, which allowed us a
total of 36 analog inputs. Brian Andrews did not
complete his PhD at that time, but came back to us
in 1980 as a member of the staff. At that time, he did
further development on the system to allow it towork with a PDP-11 computer and took the opportu-
nity to try the use of shutters on the camera to
improve definition, but then implemented what I
believe was the first application of strobe infrared
lighting.’’
‘‘When Jarrett finished his studentship, he was em-
ployed jointly by ourselves and George Murdoch at
Dundee to develop a system for implementation atDundee. He did this, but to my great astonishment,
implemented a two-dimensional system there, and
Julian Morris became aware of this, and went on to
develop the Oxford Metrics System, which was devel-
oped to be three-dimensional. Julian was very sur-prised, at a later date, to find that our first and only
computer television movement analysis system had
been three-dimensional. Apparently Jarrett, withwhom he was interacting had not told him!’’
‘‘At that time, we were not very assiduous at publica-
tion of our work, and the only one which I can cite
is, Jarrett, Andrews and Paul, 1976, which is the text
of a conference presentation as you will see on mypublication list [37 – 39]’’.
From the letters of Hans Furnee and J. Paul, andtheir publications, there is an unmistakable sequence
of interweaving paths and shared enthusiasm for au-
tomating gait analysis. Hans Furnee led the effort; J. Paul
ments. E.H. Furnee, PhD, Faculty of Applied Physics,
Technical University, Delft, The Netherlands, began
around 1967 to develop TV/motion analysis systems withautomated recording of reflective marker positions. His
experiment, capturing multiple joint angles of a cat
running on a treadmill, was a strong portent of the future
widespread adoption of the photo-electronic method to
measure the kinematics of human walking. The markers
used by Furnee were passive paper disks that were
brightly visible in ultraviolet light, and the ultraviolet
light was pulsed to prevent ‘smearing’, (see Figs. 4 and
5) [30].
Prior to the first publication directly authored by
Furnee [31,32], a student of Furnee, P.C. Steilberg,
reported the method more completely as BS and MSthesis work in 1967 and 1968 [33,34]. Furnee is the
originator of the Primas System, from the Motion
Studies Lab, Delft University of Technology. The current
Primas system emphasizes real-time marker identifica-
tion and real-time marker centers by circle fitting (pilot),
developed, respectively at Delft University in 1990 and
1992. Additional publications authored by Dr Furnee
include: ‘TV/Computer Motion Analysis Systems: The
First Two Decades’ [35] and ‘Opto-Electronic Movement
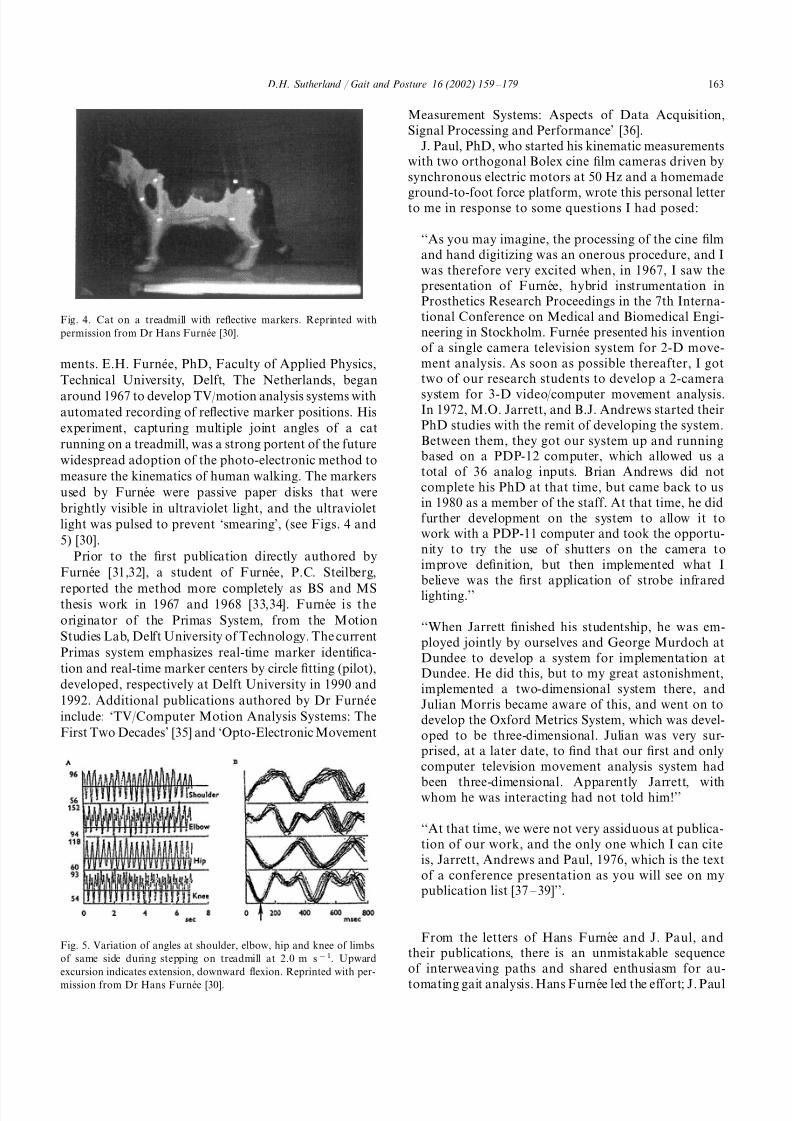
Fig. 5. Variation of angles at shoulder, elbow, hip and knee of limbs
of same side during stepping on treadmill at 2.0 m s−1. Upward
excursion indicates extension, downward flexion. Reprinted with per-
mission from Dr Hans Furnee [30].

8/6/2019 Sutherland 2
http://slidepdf.com/reader/full/sutherland-2 6/21
D.H . Sutherland / Gait and Posture 16 (2002) 159 – 179 164
was excited by his work and set graduate students,
Andrews and Jarrett, to work, with the resultant pro-
duction of a 3-D automated video camera system for
movement measurement. Prior to his entry into auto-
mated movement measurements, J. Paul had already
become an expert in gait analysis, using a digitizedcine-film system for movement measurements. His pub-
lications cover a wide range of clinical subjects, with a
special emphasis on the gait of amputees. A large
number of students of Dr Paul are spread worldwide
and it is fair to say that he has been a central figure in
the development and expansion of clinical motion
analysis.
In response to questions posed to Julian Morris,
DPhil, I received a personal correspondence dated
April 13, 1996. The following correspondence is printed
in its entirety.
The history of the development of Oxford Metrics
and VICON is as follows:
‘‘I first met Mick Jarrett at an ISPO1973
conference in Montreux,
Switzerland, while he and I were
both graduate students. He was
working (together with Brian
Andrews, now in Edmonton,
Alberta) on a 2-D TV computer
system and I was using
accelerometers for measuring gait.Mick and I both presented our
doctoral theses later the same year,
his to Strathclyde University and
mine to Oxford.
Mick was by now working with1974 –75
David Condie in University of
Dundee, and I was working at the
Nuf field Orthopaedic Centre in
University of Oxford. We both
wanted to set up automated,
non-cine gait analysis facilities in
our respective hospitals.
I arranged for an Oxford
engineering friend of mine, Malcolm
Herring, who was a far more
experienced electronics designer than
either of us, to redesign Mick’s
prototype from Strathclyde. Three of
these (multi-camera but still 2-D)
systems were built — one for
Strathclyde, one for Dundee, and
one for Oxford.
Having left the Nuf field Orthopaedic1979
in 1977 (Mike Whittle took over my
job), I was now Technical Director
of Oxford Medical Systems, part of
the Oxford instruments group.
Although our main product range
was for cardiology (Holter
monitors), I believed that there was
a commercial market for anautomatic 3-D gait analysis system.
I hired Malcolm Herring (see
above), Graham Klyne, and Annabel
MacLeod as the development team,
and made a licensing deal with
Universities of Strathclyde, Dundee,
and Mick Jarrett personally, for the
existing technology. Over the next 2
years, the VICON (the name derives
from video-converter) development
team redesigned the hardware and
wrote the first 3-D photogrammetry
software applied to this field. The
first system was shipped to Eric
Radin, MD, in West Virginia in
1980, and the second to Sheldon
Simon, MD, Boston Children’s
Hospital, a few months later.
The Oxford Instruments Group1983 –84
decided to float on the London
Stock Market and focus on their
core businesses, primarily building
cryogenic magnets for MRI. They
‘spun-off ’ the biomechanics business,
by then called Oxford Dynamics,which was sold to myself and other
members of the VICON
development team. We renamed the
company, Oxford Metrics Ltd.
(Graham Klyne won a bottle of
wine for the name).
During the 70s I was aware, through
publications, of the work of Hans
Furnee and David Winter. However,
I do not think I first met either of
them until after VICON was
launched. To my knowledge, Hans
did not ever spend time working in
Oxford.
The connection between Hans and
VICON is largely technical, rather
than historical. The hardware tech-
nology used by VICON is basically
the same as that developed by Hans.
Whether either one derived from the
other is hard to say. Certainly, I
believe that Hans published his early
work and may have been visited in
Holland by Mick Jarrett while the
latter was a graduate student.’’

8/6/2019 Sutherland 2
http://slidepdf.com/reader/full/sutherland-2 7/21
D.H . Sutherland / Gait and Posture 16 (2002) 159 – 179 165
Author’s comment: In a letter to me, Hans Furnee
confirmed the visit of M.O. Jarrett to his laboratory
and stated that he had freely shared information with
Jarrett.
Again, back to Julian Morris’ letter:
‘‘Although they both use video, there is minimal
technical connection between what David Winter
published and VICON. I certainly believe that Hans
and David developed video-based systems a year or
two ahead of Mick, but as you imply, this is, for
some, a sensitive area! Mick Jarrett and Brian An-
drews, I believe, wrote most of the software for the
1973 Strathclyde TV system jointly. However, the
VICON development team never saw or used any of
it. The first true VICON 3-D software was designed
by Graham Klyne and myself, and written entirely
by Graham. We drew on the published ideas of
many others, including Herman Woltring.’’
Eric Radin, MD, used the technology supplied by
VICON to study the running and walking gait of
sheep on a treadmill. In 1983, along with gait col-
leagues from San Diego, Ed Biden, and Marilynn Wy-
att, I visited Eric Radin’s Laboratory in Morgantown,
West Virginia. The Laboratory provided an extraordi-
nary scene of stacked bales of straw, sheep in a pen at
the side of the room, and the odor of sheep lying like
a pall over all. I asked Dr Radin, ‘Eric, do you do
any studies of human patients?’ Eric, in his inimitablestyle, said, ‘‘Well, yes, of course, but we only let
people in on Fridays’’. I silently wondered how well
human subjects responded to being studied in this
environment! Following this visit, we purchased VI-
CON hardware and Ed Biden, DPhil, wrote custom
software in 1984 for clinical application in our San
Diego Gait Laboratory. After a period of comparison
of studies on normal individuals with cine-film digi-
tization, and data collected on the same individuals
with the VICON hardware and Ed Biden’s software,
we made the transition from film digitization to auto-
mated data capture. The initial problems were associ-
ated with the dif ficulty of identifying and tracking
markers; this was initially done in two dimensions. A
tremendous move forward occurred with the contribu-
tion of Andrew Dainis, who wrote three-dimensional
tracking software (details to follow later).
Michael Whittle, MD, PhD, spent 2 years doing
surgical research after internship, which led to a mas-
ter’s degree in biomechanics. As a research medical
of ficer in the Royal Air Force, he was loaned for 3
years to NASA in Houston to supervise the muscu-
loskeletal experiments on the Skylab Space Station.
One of these experiments was on the 3-D measure-
ments of the astronaut’s body form [40], and this
became the subject of his PhD dissertation, which he
obtained after he returned to Great Britain. He took
over the directorship of the Motion Laboratory at
Oxford after Julian Morris left to found Oxford Met-
rics. The only software available for the new Oxford
Metrics system was for data capture, so Dr Whittlewrote full 3-D motion capture software, ‘‘So, in effect,
we had the first 3-D TV computer system in the
world’’. (Author’s comment: Communication from J.
Paul indicates earlier 3-D development in Strathclyde.)
Michael Whittle now holds the Cline Chair of Reha-
bilitation Technology at the University of Tennessee at
Chattanooga. He is author of a book entitled, ‘Gait
Analysis: An Introduction’, which is now in its 2nd
edition [41].
Another important player in the exciting world of
motion capture is the Bioengineering Technology Sys-
tems, or BTS, which is home-based in Milan, Italy.
BTS traces its origins to the contribution of the bio-
engineering center of the Pro Juventute Foundation
and the Politecnico di Milano. The company was
formed in 1986. The engineering contributions of Fer-
rigno, Pedotti, and Cappozzo were key in the develop-
ment of the ELITE System [42 – 44]. BTS rapidly
expanded into the complete world of clinical gait anal-
ysis, combining kinematics, kinetics, and electromyo-
graphy in a robust, all-inclusive approach to clinical
gait analysis and research in motor skeletal function.
In point of time, BTS entered the field of clinical
motion analysis after Oxford Metrics, Inc. and Motion
Analysis Corporation.The story does not stop here. The entry of many
new companies and new systems of motion capture
attests to the enduring fascination with movement
analysis. The competition between the companies now
marketing motion capture systems has resulted in
more rapid processing of information, new methods of
displaying the data, and a surging interest in clinical
gait analysis. Laboratories are now available in all of
the developed countries and in many of the developing
countries.
2 .5 . Automated mo6ement measurements
2 .5 .1. North American early contributors and
techniques
While the early advances in gait analysis and auto-
mated movement measurements were occurring in the
Netherlands, England, and Scotland, exciting activities
were also taking place in Canada. Robert K. Green-
law, MD, then the Chief Surgeon of the Shriners Hos-
pital, Winnipeg, Canada, and a former resident in the
Shriners Hospital in San Francisco, was aware of Dr
Inman’s work and of my work in the San Francisco
Shriners Hospital Gait Laboratory. It was not obvious

8/6/2019 Sutherland 2
http://slidepdf.com/reader/full/sutherland-2 8/21
D.H . Sutherland / Gait and Posture 16 (2002) 159 – 179 166
Fig. 6. Gait studies data acquisition system. ‘Locomotion studies as an aid in clinical assessment of childhood gait ’—reprinted from, by permission
of the publisher, CMAJ , 1975; 112 (9), pp. 1091 – www.cma.ca [46].
to me then that orthopedic resident Greenlaw had an
interest in motion analysis, but the events that followed
proved otherwise. He had the good judgment to ask
David Winter, PhD, to design the first gait analysis
laboratory in the Shriners system in Canada.
David Winter, PhD, then with the Department of
Electrical Engineering and the Department of Surgery,
University of Manitoba, Winnipeg, designed a Gait
Laboratory for the Winnipeg Shriners Hospital. Dinn
et al. submitted a manuscript in 1969 entitled, ‘Com-
puter Interface for Television’, which was ultimately
published in IEEE Transaction of Computers in 1970
[45]. In a letter to me, Dr Winter states, ‘‘Our first
routine use of the interface began early in 1970 at the
Shriners Hospital in Winnipeg. For the 5 years I was
there it was the backbone of all our kinematic data
collection. Actually, it goes back to the time of Furnee.
Our first operational TV interface was reported at
biomedical engineering conferences on this side of the
Atlantic at the same time (unknown to us) as he was
reporting in The Netherlands’’, (see Fig. 6), [46]. Winter
et al. subsequently published an article entitled: ‘Televi-
sion – Computer Analysis of Kinematics of Human
Gait’ in Computer and Biomedical Research in 1972 [47].
Winter et al. published an important study of the
kinematics of normal locomotion in the Journal of
Biomechanics in 1974 [48]. Doctor Winter’s publications
since that time are legendary [49]. He has profoundly
influenced the course of clinical gait analysis through
his scientific studies, teaching, mentoring of many grad-
uate students and his many publications. His book
entitled, ‘Biomechanics and Motor Control of Human
Movement’, now in its 2nd edition, is a ‘must read’ for
all who are interested in gait analysis [50].
Sheldon Simon, MD, obtained his medical degree
from Harvard and his residency training was completed
in the Harvard Training Program. During his residency
training, he worked in the laboratory of Robert Mann,
PhD, at the Massachusetts Institute of Technology. He
received a Cave Traveling Fellowship and, in January
through June 1974, divided his time between the San
Francisco Shriners Gait Analysis Laboratory, then di-
rected by Roger Mann, MD, and the Pathokinesiology
Laboratory at Rancho Los Amigos, directed by
Jacquelin Perry, MD. He says that he was very im-
pressed by the electromyographic studies at Rancho
and the force and kinematic studies in San Francisco.
By the time of his return, the Kistler force plate was
available as a commercial product, but the price was
steep for his budget in Boston. He persuaded Walt
Synutis, President and CEO of AMTI, to design a new
strain-gauge force plate at a price within his budget.
The space available for him in Boston was small and he
realized that a three-dimensional coordinate software
system for kinematic measurements should be devel-
oped. The laboratory opened in Boston Children’s Hos-
pital in September 1974, with two AMTI strain gauge
force plates, a three-camera 16 mm high speed camera
system, a Vanguard Motion Analyzer and a computer
which stored the measurements from force plates and
electromyograph simultaneously. The software for kine-
matic measurements utilizing a three-dimensional coor-
dinate system from film was conceived by Dr Simon
and written by Roy Nuzzo, MD, an orthopaedic resi-
dent at the time [51]. Mick Jarrett, PhD spent a good
deal of time at Boston Children’s Hospital in 1982
perfecting software for clinical application of the VI-
CON system. According to Dr Simon, initially it took

8/6/2019 Sutherland 2
http://slidepdf.com/reader/full/sutherland-2 9/21
D.H . Sutherland / Gait and Posture 16 (2002) 159 – 179 167
just as long to process 3-D VICON measurements as
3-D film measurements. Nonetheless, it was clear that
further developments would establish automated video
measurements and there would be no turning back. In
1986, Dr Simon moved to Ohio State University, where
he held the positions of Chairman of the Department of Orthopedic Surgery and Medical Director of the new
Motion Analysis Laboratory. Numerous clinical and
research publications have followed [52]. One of Dr
Simon’s many interests has been the application of
artificial intelligence to gait data. He says that he
realized that interpretation would continue to offer the
greatest challenge and, in 1984, began work on an
artificial intelligence application. This work has contin-
ued to this time and a system, which can be separately
used as a decision helper and as a trainer, is currently
being tested. Dr Simon is the editor of a book entitled,
‘Orthopaedic Basic Science’, published by the American
Academy of Orthopaedic Surgeons [53]. He now resides
in New York City and continues his career-long interest
in clinical gait analysis.
In 1978, James R. Gage, MD, visited Eugene Bleck’s
Gait Laboratory at Stanford Children’s Hospital,
Jacquelin Perry’s laboratory at Rancho Los Amigos
Hospital, and my laboratory at San Diego Children’s
Hospital, in preparation for beginning his first labora-
tory at Newington Children’s Hospital. United Tech-
nology Research Corporation, located in Newington,
Connecticut, had offered extraordinary engineering and
financial support for the establishment of a Gait Labo-
ratory. In early 1980, Gage returned to the San DiegoLaboratory for an in-depth look, bringing with him
Ken Taylor, United Technology Project Engineer, and
Jim Clark, Manager of the Newington Gait Laboratory
project. The three men asked many questions, including
what we would do if we were starting another labora-
tory with optimal funding and full technical assistance.
We answered openly, even with ideas that were not yet
fully realized in our own laboratory. This cooperation
and sharing of information continued during the devel-
opment of the Newington Laboratory. The Newington
Gait Laboratory opened in July 1981. Special features
of this laboratory included synchronization of all gait
data, full custom clinical software and rapid processing
of data. Scott Tashman, MS (now PhD), validated and
continued the United Technologies software package.
Follow-up gait studies were regularly performed on
patients who had undergone preoperative gait studies,
thus opening the way for a great many clinical papers
[54 – 59] and a book entitled ‘Gait Analysis in Cerebral
Palsy’ [60].
Following Dr Gage’s move to Gillette Children’s
Hospital in 1990, the Newington laboratory continued
under Peter DeLuca, MD, as Medical Director, with
Roy B. Davis, PhD, as Director until 1998. Sylvia
O . unpuu, M Sc., a prior student of David Winter, is the
current Director. The Newington Gait Laboratory
moved to Hartford Connecticut, with the opening of
Children’s Hospital of Connecticut as an integral part
of the University of Connecticut Medical Center. Many
papers have been published both by Gillette Children’s
Hospital and Newington/Children’s Hospital of Con-necticut covering a variety of subjects, including: run-
ning patterns of normal children [61] [62], outcome of
multilevel surgery in cerebral palsy [63], stiff-knee gait
[64,65], the utility of basing treatment decisions in
cerebral palsy on preoperative gait analysis, [66], and a
gait analysis data collection and reduction technique,
which includes Davis’ much referenced joint center
determination method [67]. Gage has pushed the envel-
ope in advocating gait analysis routinely in patients
with cerebral palsy [60]. Some surgeons, none of whom
have gait laboratories, have criticized this. An anecdote
illustrating this point follows:
At a course jointly sponsored by the American
Academy of Orthopaedic Surgeons (AAOS) and the
Pediatric Orthopaedic Society of North America
(POSNA) in San Francisco, May 6, 1990, entitled Con-
troversies in the Treatment of Cerebral Palsy, the
course chairpersons were Dr Michael Sussman and Dr
Walter Greene, myself, Dr Simon, and Dr Gage, in that
order. We had just finished giving views on the impor-
tance of clinical gait analysis when, from near the back
row, Hugh Watts, MD, a pediatric orthopaedist and
friend, but never one to avoid controversy, rose to
challenge the clinical usefulness of gait analysis. Heclaimed that the gait laboratory setting is not a suitable
environment for arriving at the true walking patterns of
children with cerebral palsy. He implied that observa-
tional analysis of children in the playground, or in
other familiar surroundings, is better. The entire back
section of the auditorium, filled mostly with ortho-
paedists, burst into spontaneous applause. The heated
discussion that followed resulted in back-to-back edito-
rials by Gage and Watts in the Journal of Pediatric
Orthopaedics [59,68]. Be that as it may, acceptance of
clinical gait analysis has steadily increased and new
laboratories are being established throughout theworld. The new generation of orthopaedic surgeons,
introduced to gait analysis in their training, increasingly
demands functional analysis, before and after treat-
ment, in order to better understand the magnitude of
the disability and to ascertain the impact of their inter-
vention. As my ‘parting shot over the bow’ on this
subject, I would like to quote Max Planck, the famous
German physicist, who pioneered modern physics by
proposing the quantum theory and won the 1918 Nobel
Prize. He said, ‘‘An important scientific innovation
rarely makes its way by gradually winning over and
converting its opponents. What does happen is that the
opponents gradually die out’’ [69].

8/6/2019 Sutherland 2
http://slidepdf.com/reader/full/sutherland-2 10/21
D.H . Sutherland / Gait and Posture 16 (2002) 159 – 179 168
Murali Kadaba, PhD, became interested in gait anal-
ysis when he joined Helen Hayes Hospital as a research
scientist in 1979. Dr George Van Cochran was influen-
tial in his decision to work in the area of clinical gait
analysis. Dr Kadaba states that his interest was inten-sified after a visit with Dr Perry at Rancho Los Amigos
Pathokinesiology Laboratory in Downey, California,
and with me at the Motion Analysis Laboratory at San
Diego Children’s Hospital. He received a NIH grant in
1984 to study the reproducibility and reliability of gait
data [70]. Following completion of this study, he be-
came interested in the numerical representation of kine-
matic and kinetic data for pattern recognition in spastic
diplegia [71]. The Helen Hayes clinical software was
completed in 1985. ‘‘This was a cooperative effort; the
other team members were H.K. Ramakrishnan, Mary
Wootten, Janet Burn (Gainey) and Dr Van B.Cochran’’ [72]. This clinical software served a critical
need for software to be used in a clinical setting. It was
implemented at the following centers: Richmond Chil-
dren’s; Shriners Hospital, Houston Unit; Methodist
Hospital, Houston, Texas; Children’s Memorial Hospi-
tal, Chicago; Children’s Milwaukee; and Shriners Hos-
pital, Portland Unit. The Helen Hayes Team, under the
leadership of Dr Kadaba, deserve great credit for devel-
oping and supporting clinical software (no small task),
in the precarious early years. At that time, the writers
of commercial software were attuned to the diverse
needs of researchers, but they lacked confidence in the
ability of clinical laboratories to agree on nomenclatureand formats for data presentation. As a consequence,
new laboratories were forced to adapt commercial soft-
ware to their own tastes. The Helen Hayes Software
helped fill this temporary void. Happily, the common
needs of most of us are now met with commercially
available software.
The original Helen Hayes software could now be
named the Helen Hayes marker set as software is
available that can handle both the Helen Hayes marker
set and the Cleveland Clinic marker set. The competing
marker set is the Cleveland Clinic, credited to Kevin
Campbell of the Cleveland Clinic Foundation. Thedifferences in the two marker sets are briefly outlined as
follows:
Both marker sets are used to define joint centers and
segmental coordinate systems (SCS) needed to calculate
angular kinematics. The main difference between both
sets is in the way the joint centers and coordinate
systems are defined. Helen Hayes (HH) is a ‘wand-
based’ marker set, in which joint centers and segmental
coordinate systems are defined using a wand marker on
each segment (i.e. thigh and shank). As joint markers
are shared between segments and, therefore, each seg-
ment has at least three markers for its definition, the
Helen Hayes is considered a simplified marker set,
which along with a static trial of markers on the medial
and lateral sides of each joint (ankle and knee), gives
everything that is needed to calculate joint angles (i.e.
location and orientation of each joint axis) [73].The Cleveland Clinic Foundation (CCF) marker set
is a ‘cluster-based’ marker set, in which clusters or
arrays of three (or sometimes four) markers are used to
define joint centers and segmental coordinate systems.
With this marker set, the clusters are placed on each
segment along with the medial and lateral markers,
which define the flexion-extension axis of each joint,
during the static trial. As the clusters define a coordi-
nate system to reference the positions of the medial and
lateral markers, all medial and lateral joint markers can
be removed after the static trial, and a dynamic trial
can be collected, while still maintaining the location
and orientation of each joint axis [74].
The advantage of the Helen Hayes marker set is that
it is relatively simple to use and more applicable to gait
analysis of children. The arrays used in the Cleveland
Clinic marker set have been known to hit each other in
smaller children. In a recent comparison study, con-
ducted in our Motion Analysis Laboratory by Arnel
Aguinaldo, MA, ATC, and the laboratory team, we
observed less variability in the transverse plane kine-
matics with the Cleveland Clinic marker set. This was
probably because there was less marker movement, due
to the fact that there are at least three markers fixed to
a rigid frame, although skin motion over the segmentdefined by the array is still a factor.
2 .6 . Methods of joint angle calculation
Although, there are two methods of joint angle calcu-
lation most frequently used: Euler/Cardan and Helical
screw axis, there are at least three additional methods,
with definitions and pros and cons noted in Table 1.
Further use and description of joint movement and
rotational three-dimensional motion by Kenton Kauf-
man, PhD, includes the transformation matrix method
for complete representation [78]. The Euler/Cardan
method lends itself well to clinical interpretation.
Therefore, we utilize it for most of our clinical studies
that do not involve translational movement, such as
that found in patients with anterior cruciate insuf fi-
ciency. For persons with knee instability, which may
add more than normal translation to angular rotation,
the use of the helical screw axis method of joint angle
calculation is more appropriate.
John Greaves, PhD, a graduate in electrical engineer-
ing from the University of California, Santa Barbara,
while he was a student with Glen Culler, worked on a
project they dubbed ‘the bug watcher’. The researchers
in the biological sciences department were interested in

8/6/2019 Sutherland 2
http://slidepdf.com/reader/full/sutherland-2 11/21
D.H . Sutherland / Gait and Posture 16 (2002) 159 – 179 169
monitoring the motion of the microscopic marine
plankton known as dynoflagellates. Greaves tackled the
problem for them by designing and building a system
using a video camera to look into a microscope coupled
with a computer to process the video signals and
provide position and velocity information about thedynoflagellates. The system worked. After some inter-
vening post-doctoral activities, John Greaves founded
Motion Analysis Corporation; a company that provides
3-D motion capture systems for many clinical gait
laboratories, sports analysis research facilities, and
equipment for use in the movie industry. This company
utilizes ORTHOTRAK software for processing of move-
ment, developed jointly by the Cleveland Clinic Foun-
dation and Motion Analysis Corporation, in
conjunction with Chet Tylkowski, MD, then at the
Human Motion Laboratory, Department of Ortho-
paedics, University of Florida, Gainesville. The current
version is a joint development effort with James
Richards, PhD, Freeman Miller, MD, and Patrick Cas-
tagno, MS, from the University of Delaware and the
Alfred I. duPont Hospital for Children.
Chester Tylkowski, MD, became interested in gait
analysis while working as a fellow with Dr Sheldon
Simon at Boston Children’s Hospital, 1978 – 79. He set
up a clinical gait laboratory at the University of Flor-
ida, Gainesville, in 1980. Subsequently, in 1989, Dr
Tylkowski and the laboratory moved to the Miami
Children’s Hospital. His third move was to the Shriners
Hospital, Lexington, Kentucky, in 1995, where he holds
the position of Chief of Staff. He holds the unof ficialrecord for the physician responsible for forming the
largest number of clinical gait laboratories. This is an
indication of his commitment to the importance of
clinical gait analysis throughout his orthopaedic career
[79 – 81]. A kinesiologist, Susan Sienko Thomas, MA, a
former student of David Winter, holds a similar record
for involvement in three gait laboratories. In 1985,
Susan was hired to oversee the operation of the South-
ern Illinois University Motion Analysis Laboratory in
Springfield, Illinois, after the tragic death of Maxine
Covert. The laboratory had been established with a
VICON system in 1983. In 1989, she assisted in the set
up and operation of the Motion Analysis Laboratory at
Children’s Memorial Hospital, Chicago, where the He-
len Hayes clinical software package was used. She
currently holds the position of Clinical Research Coor-
dinator at the Shriners Hospital in Portland, Oregon
[82,83].
Steven J. Stanhope, PhD, from the Biomechanics
Laboratory, National Institutes of Health, has stronglyadvocated inter-laboratory reliability and the need for
demonstrating proven means of testing kinematic
movement measurements. His efforts have lifted the
standards for all gait laboratories in the U.S. Similar
efforts are occurring in Europe under initial funding by
the European Union. The testing of laboratories should
be a requirement for certification. Although many ef-
forts have been exerted to move this important task
forward, it still remains in the discussion stage. There
should be no objection to the concept that patients,
referring physicians, and payers have a right to know
that a laboratory is capable of providing accurate and
reliable data. There is little doubt that testing and
certification will be instituted, hopefully in the near
future.
The majority of clinical patients seen at the Biome-
chanics Laboratory, National Institutes of Health, are
adults referred by physiatrists or internists. Thus, the
clinical applications have been primarily for subjects
with rheumatoid arthritis, osteoarthritis, limb defi-
ciency, diabetes, stroke, and neuromuscular disorders
[84 – 86]. The establishment of a three-dimensional mus-
culoskeletal database is a research effort that will con-
tribute greatly to clinical applications [87]. Software for
clinical applications, as well as for research, were devel-oped in this laboratory, and provided to laboratories
throughout the world. The program is called Move 3D.
This software is very robust and, according to Dr
Stanhope, is the first software to provide six degrees of
freedom gait measurements.
3. Shriners network of gait laboratories
There are 19 orthopedic Shriners Hospitals in the
U.S., Canada and Mexico. Of these, 12 currently have
gait laboratories, with a 13th laboratory being estab-
lished in Tampa, all of them carrying out clinical
analysis before and after treatment. In addition, they
Table 1
Methods of joint angle calculation (A. Aguinaldo, MA, ATC, Motion Analysis Laboratory, Children ’s Hospital, San Diego)
Method Pros ConsDefinition
Angles projected onto plane Simple ParallaxPlane projections
Not clinically relevantComplete representationDirection cosines Transformation matrix
Gimbal locksEuler/Cardan Sequence of rotations Clinical interpretation
Euler with floating axis Not suitable for kineticsSequence independentGrood and Suntay
Screw axisHelical Rotation and translation Sensitive to noise
References: [75,76,73,77].

8/6/2019 Sutherland 2
http://slidepdf.com/reader/full/sutherland-2 12/21
D.H . Sutherland / Gait and Posture 16 (2002) 159 – 179 170
are involved in collaborative research. This confirma-
tion of the usefulness of clinical gait laboratories has
not gone unnoticed by physicians in the children’s
hospitals of North America. This powerful statement
by a major block of children’s hospitals may well
have helped spur the establishment of centers foranalysis in the other Children’s Hospitals, both pri-
vate and University af filiated.
3 .1. Acti 6e marker systems
The Selcom Company of Sweden developed the
Selspot System, which used active markers taped to
the limb segments, prior to the advent of VICON and
Motion Analysis Corporation. The first Selspot move-
ment capture systems in the U.S. were installed in the
laboratory of Thomas Andriacchi, PhD, at Rush
Presbyterian Medical Center in Chicago, and in the
laboratory of Robert Mann, PhD, at Massachusetts
Institute of Technology, Cambridge, MA. Herman
Woltring, PhD, did some of the early work with the
Selspot System as did Andrew Dainas. Robert Mann,
PhD, and Eric Antonsson, PhD, established a clinical
laboratory at Massachusetts General Hospital in 1984,
along with several orthopedists, William Harris, MD,
Henry Mankin, MD, Donald Madeiras, MD, and
Michael Erlich, MD, PhD. Their system was designed
for cerebral palsy gait analysis. David Krebs, PhD,
PT, continues this work, collecting data on human
subjects with a variety of problems, including cerebralpalsy and disorders of posture and balance. This lab-
oratory utilizes Selspot active markers, arranged in
clusters on a fixed base, applied to each of the body
segments being studied. A large database of children
and adults with neuromuscular disorders, including
many with problems of balance, has been established.
One area of investigation is sitting-to-stand move-
ments.
Although the Selspot system eliminates the need for
marker identification and tracking, it contains other
less positive features including its propensity to pick
up reflections, the necessity for the subjects to carrycumbersome apparatus, and the trade-off between
sampling rate and the number of markers. These in-
herent drawbacks in this active marker system served
to energize the proponents of passive marker systems
and to keep them working to solve the dif ficulties
with marker identification and tracking. In spite of
the current preponderance of passive marker systems,
some active marker systems are emerging to compete
with the passive models. Examples of active marker
systems are those by CODA and Skill Technologies,
(see Appendix A). The brief discussion contained in
this manuscript will be useful to clinicians, but engi-
neers and physicists will be well served by reading
Furnee’s very complete, and highly technical, descrip-
tions of passive and active motion capture systems
[35,36].
3 .2 . Three-dimensional marker identi fication and
tracking
Andrew Dainas deserves much credit, along with
Doug McGuire, for more ef ficient processing of raw
TV data to 3-D coordinates. In a personal communi-
cation Dainas writes,
‘‘By 1988 we had finished the first version of the
AMASS software. The software development was
carried independently of NIH, and was not sup-
ported by NIH. At that time, we installed it on theNIH VICON system and offered it as a replace-
ment to Oxford Metrics for their aged system. As it
turned out, in 1988, Oxford Metrics had completed
their new VAX – VX hardware system but lacked
appropriate software, and they agreed to market
AMASS with their systems. Between 1988 and 1993,
Oxford Metrics sold some 70 VICON systems bun-
dled with the AMASS hardware. In 1993, Oxford
Metrics announced the VICON 370 system, with
their own software (which replicates many functions
of AMASS). We (at ADTECH) in turn ported
AMASS to the PC computer, and adapted it to workwith raw data from both Motion Analysis Corpora-
tion systems and ELITE systems. Currently, we of-
fer AMASS as alternative software for these systems.
AMASS can claim to be the first software used in
clinical and gait applications to provide:
1. Intelligent marker reduction to 2-D centers in the
camera image data by fitting circles to the pixels
outlining the markers.
2. Provide the user with the ability to linearize each
camera for distortions, etc.
3. Do automatic identification of reference markers
in the 3-D camera calibration process.4. Do completely hands-off 3-D reconstruction and
tracking of unidentified camera image data.
In 1994, I wrote and incorporated into AMASS the
first program to carry out the 3-D camera system
calibrations using a large number of markers whose
locations in 3-D space need not be measured before-
hand. This technique does away with the need for
rigid calibration objects, or hanging strings or rods,
and is capable of eliminating a chief source of inaccu-
racies in most currently used 3-D measurement sys-
tems. The method has since been also implemented
by Oxford Metrics.’’

8/6/2019 Sutherland 2
http://slidepdf.com/reader/full/sutherland-2 13/21
D.H . Sutherland / Gait and Posture 16 (2002) 159 – 179 171
3 .3 . Present reality
Commercial hardware and software now available
have nearly eliminated problems with marker identifica-
tion and tracking, thus removing the chief objection to
passive marker systems. As a consequence, the develop-ment and utilization of active marker systems was on
hold for a time. In today’s state-of-the-art laboratory, a
subject can be fitted with appropriate reflective markers
and walk down a calibrated walkway, while the mark-
ers are automatically tracked and thousands of compu-
tations are performed by a dedicated high-end PC
computer or a computer work station. The resultant
joint angles can be viewed within minutes from the end
of collection of the data. An increase in the number of
cameras, plus 3-D identification and tracking of mark-
ers, now enable laboratory personnel to examine the
data for reliability and potential errors while the subject
is still present in the laboratory. This represents an
enormous evolution in automated movement measure-
ments in the 34 plus years since the technology was first
developed. There are still some problems to be worked
out. For example, accurate timing of toe-off is prob-
lematic with kinematic methods. The incorporation of
force platform input establishes the events of foot-strike
and toe-off accurately for those patients able to contact
two or more force platforms. However, it is the slow
walkers, using crutches or a walker, who often exhibit
variable or even inaccurate foot-contact times, as calcu-
lated from the trajectory velocities of markers on the
foot. Yet another problem is that of marker movementdue to skin movements over the underlying skeleton. A
number of research studies address this problem, but
none have discovered a way to totally eliminate inaccu-
racies due to skin movement [88 – 95].
If these reasons are not enough to convince the
reader of the need for additional research, or even
investigation of other methods of measuring movement,
there is yet another problem, that of placing markers
accurately and reliably. Mistakes can alter the calcula-
tions of joint centers. The models for establishing hip
center, used in all of the commercial software systems,
have come from cadaver studies and are not patient
specific. This inherent flaw in patients with pathology
of the hip makes moment and power calculation of the
hip suspect. Discussion of this topic will be included in
The Evolution of Clinical Gait Analysis Part III, Kinet-
ics and Energy.
3 .4 . Future
It would be a mistake to assume from the rapid
development of 3-D passive marker systems that tech-
nological advances in active marker systems are not
occurring. There are currently several companies em-
ploying active marker systems. Why, with good passive
systems dominating the field, is this occurring? The
passive marker systems are expensive, considerable
training is still required for optimal use of the hardware
and software, and flexibility in programming for special
studies requires the talents of engineers. Our laboratory
currently uses an 8-camera, passive marker system, andeven larger camera arrays are in use in some
laboratories.
Possible developments in the next decade are:
(1) The elimination of the need for either passive or
active targets and a reduction in the number of cameras
now in use. With increasing computer memory and disc
capacity, markerless measurements of 3-D motion loom
on the horizon as a possibility.
(2) The development of an active marker system with
radio-frequency active emitters is a promising approach
for the economics of gait analysis hardware. This wouldbring about economies in the number of cameras re-
quired. The technology for 3-D identification of radio-
frequency signals is already well established in military
applications. The active emitters are lightweight and
relatively inexpensive and there is little to prevent the
use of a large number of markers. If such a system is to
be implemented, there must be initial research and
development investment, following which the costs for
purchase of software and hardware would be well
below the present costs for passive marker systems.
(Tera Research has a patent pending for this technol-
ogy. For further information, contact Dr Walter Heine
at [email protected].)
(3) Better methods of defining joint centers, especially
with regard to hip joint center, will be required, possi-
bly with the aid of CT and MRI scanning. Moment
measurements are sensitive to the accuracy of joint
center calculations; consequently, errors in joint centers
degrade the accuracy of moment calculations.
(4) The use of neural network statistical analysis is
still in its infancy in clinical gait analysis [96] and
computer assisted diagnostic and problem identification
[97] will surely expand in the next decade.
(5) In addition to whole body gait analysis, foot
models are emerging. Analyzing joints distal to theankle remains a major challenge for the future [98,99].
The treatment of individuals with pathological gait
will steadily change as data are gathered and published
from multiple sources. A quantum change has already
occurred in the treatment of cerebral palsy. A new
generation of multidisciplinary motion analysis teams is
forging new standards of quality and pushing the limits
of application to a wide variety of disabilities. Rapid
changes are occurring in the treatment of myelodys-
plasia, and improvements in the recognition and treat-
ment of a large variety of neurological disorders are on

8/6/2019 Sutherland 2
http://slidepdf.com/reader/full/sutherland-2 14/21
D.H . Sutherland / Gait and Posture 16 (2002) 159 – 179 172
the horizon. We now have the tools to perform func-
tional analysis and to replace guesswork with a scien-
tific framework for evaluation and treatment. Oral drug
treatment, injections of Botulinum Toxin Type A, in-
trathecal baclofen pump, physical therapy, orthotic
management, orthopedic and neurosurgery must all beevaluated on both a short and long term basis, and gait
analysis must play a pivotal role. The changes in treat-
ment will be incremental, wide-ranging, and will come
from all parts of the globe. There is much work to do
and the beneficiaries will be patients with disorders of
movement. It is a source of great satisfaction to pa-
tients, their parents, and their physicians to know that
locomotion and movement disorders are at last receiv-
ing the attention they deserve.
Acknowledgements
My special thanks to all of the individuals who
responded to my letters and phone calls, supplying
details that give life to this account. For the administra-
tive assistance provided by Sherill Marciano, Jill Jor-
dano, and Kit Holm, who put up with my many
changes to the manuscript, and for Kit’s tenacity with
research, which helped immensely with reviewer re-
sponse and final publication requirements. To bioengi-
neer, Arnel Aguinaldo, and physical therapists,
Marilynn Wyatt and Janet Buttermore, for their assis-
tance with the search for details and review of the
manuscript. To John Hagy who filed and saved corre-spondence and other documents from the early days of
the San Francisco Gait Lab. Finally, my thanks to Dr
Hank Chambers, Medical Director of the Motion Anal-
ysis Laboratory at Children’s Hospital, San Diego, for
his helpful comments.
Appendix A. A partial list of commercial kinematic
systems
Ariel dynamics
6 Alicante Street
Trabuco Canyon, CA 92679
USA
Tel.: (949) 858 4216
Fax: (949) 858 5022
BTS
Via C. Columbo, 1A 20094 Corsico
Milano, Italy
Tel.: +39 02458751
Fax: +39 0245867074
CODA
Charnwood Dynamics Ltd.
17 South Street, Barrow on Soar
Leicestershire, LE12 8LY
Tel.: +44 (0) 116 230 1060
Fax: +44 (0) 116 230 1857
Motion analysis corporation
3617 Westwind Blvd
Santa Rosa, CA 95403
USA
Tel.: (707) 579-6500
Fax: (707) 526-0629
Peak performance
7388 S. Revere Parkway
Suite 603
Englewood, CO 80112
USA
Tel.: (303) 799 8686
Fax: (303) 799 8690Primas
Motion Studies Laboratory
Delft University of Technology
P.O. Box 5
2600 AA Delft
The Netherlands
Tel.: +31 (0) 15 278 9111
Fax: +31 (0) 15 278 6522
Qualisys Inc.
148 Eastern Blvd, Suite 110
Glastonbury, CT 06033
USA
Tel.: +1 860 627 5060
Fax: +1 860 627 4041
Qualisys AB
Drottninggatan 31
Goteborg 41114
Sweden
Tel.: +46 (u) 317743830
Fax: +46 (u) 317014145
Selspot, AB
Sallarangsgatan 3
S-431 37 Molndal, Sweden
Skill Technologies, Inc.
1202 E. Maryland Ave., Suite IG
Phoenix, AZ 85014
USA
Tel.: 602-277-7678
Fax: 602-277-2326
VICON motion systems
Oxford Metrics Limited
Unit 14, MINNS ESTATE
7 West Way
Oxford OX20JB

8/6/2019 Sutherland 2
http://slidepdf.com/reader/full/sutherland-2 15/21
D.H . Sutherland / Gait and Posture 16 (2002) 159 – 179 173
UK
Tel.: +44 (1865) 26 1800
Fax: +44 (1865) 24 05 27
Appendix B
B.1. Copy of letter to Raymon Linder, from Dr
David Sutherland, dated August 23, 1965.

8/6/2019 Sutherland 2
http://slidepdf.com/reader/full/sutherland-2 16/21
D.H . Sutherland / Gait and Posture 16 (2002) 159 – 179 174
B.2. Copy of letter to John Hagy, from Dr E. R.
Schottstaedt, dated November 29, 1965.

8/6/2019 Sutherland 2
http://slidepdf.com/reader/full/sutherland-2 17/21

8/6/2019 Sutherland 2
http://slidepdf.com/reader/full/sutherland-2 18/21
D.H . Sutherland / Gait and Posture 16 (2002) 159 – 179 176
D e s c r i p t i o n o f o u r fi r s t u s e o f a d e d i c a t e d c o m p u t e r f o r ‘ D i a g n o s t i c G a i t A n a l y s i s ’ , b y E l e c t r o n i c P r
o c e s s o r s , I n c . ( t w o p a g e s ) .
8/6/2019 Sutherland 2
http://slidepdf.com/reader/full/sutherland-2 19/21

8/6/2019 Sutherland 2
http://slidepdf.com/reader/full/sutherland-2 20/21
D.H . Sutherland / Gait and Posture 16 (2002) 159 – 179 178
tion —a statistical study based on TV data. J Biomech
1974;7(6):479 – 86 November.
[49] Winter DA, Yack HJ. EMG profiles during normal human
walking: stride-to-stride and inter-subject variability. Electroen-
cephalogr Clin Neurophysiol 1987;67(5):402 – 11.
[50] Winter DA. Biomechanics and motor control of human move-
ment, 2nd ed. New York: Wiley, 1990.[51] Simon SR, Knirk J, Mansour JM, Koskinen MF. A comprehen-
sive clinical system for four-dimensional motion analysis. Bull
Hosp Joint Dis 1977;38(1 April):41 – 4.
[52] Simon SR, Deutsch SD, Nuzzo RM, Mansur MJ, Jackson JL,
Koskinen M, Rosenthal RK. Genu-recurvatum in spastic cere-
bral palsy. J Bone Joint Surg 1978;60A:882 – 94.
[53] Simon SR, editor. Orthopaedic basic science. American
Academy of Orthopaedic Surgeons, 1994.
[54] Gage JR, Fabian D, Hicks R, Tashman S. Pre- and postopera-
tive gait analysis in patients with spastic diplegia: a preliminary
report. J Pediatr Orthop 1984;4:715 – 25.
[55] Gage JR, Perry J, Hicks RR, Koop S, Werntz JR. Rectus
femoris transfer to improve knee function in children with
cerebral palsy. Dev Med Child Neurol 1987;29:159 – 66.
[56] Gage JR. Surgical treatment of knee dysfunction in cerebralpalsy. Clin Orthop 1990;253:45 – 54.
[57] Gage JR. An overview of normal walking. Instr Course Lect
1990;39:291 – 303.
[58] Gage JR. Gait analysis. An essential tool in the treatment of
cerebral palsy. Clin Orthop 1993;288:126 – 34.
[59] Gage JR. The role of gait analysis in the treatment of cerebral
palsy. J Pediatr Orthop 1994;14(6):701 – 2.
[60] Gage JR. Gait analysis in cerebral palsy. New York: MacKeith
Press, 1991.
[61] Ounpuu S. The biomechanics of running: a kinematic and
kinetic analysis, Inst. Course Lect. 1990:305 – 318.
[62] Ounpuu S, Gage JR, Davis RB. Three-dimensional lower ex-
tremity joint kinetics in normal pediatric gait. J Pediatr Orthop
1991;11:341 – 9.
[63] DeLuca PA, Ounpuu S, Davis RB, Walsh JH. Effect of ham-string and psoas lengthening on pelvic tilt in patients with spastic
diplegic cerebral palsy. J Pediatr Orthop 1998;18(6):712 – 8.
[64] Ounpuu S, Muik E, Davis RB, Gage JR, DeLuca PA. Rectus
femoris surgery in children with cerebral palsy. Part II: a com-
parison between the effect of transfer and release of the distal
rectus femoris on knee mot ion. J Pediatr Orthop
1993;13(3):331 – 5.
[65] Ounpuu S, Muik E, Davis RB, Gage JR, DeLuca PA. Rectus
femoris surgery in children with cerebral palsy. Part I: the effect
of rectus femoris transfer location on knee motion. J Pediatr
Orthop 1993;13(3):325 – 30.
[66] DeLuca PA, Davis RB, Ounpuu S, Rose S, Sirkin R. Alterations
in surgical decision making in patients with cerebral palsy based
on three-dimensional gait analysis. J Pediatr Orthop
1997;17(5):608 – 14.[67] Davis RB, O 8 unpuu S, Tyburski DJ, Gage JR. A gait analysis
data collection and reduction technique. Hum Mov Sci
1991;10:575 – 87.
[68] Watts HG. Gait laboratory analysis for preoperative decision
making in spastic cerebral palsy: is it all it’s cracked up to be? J
Pediatr Orthop 1994;14:703 – 4.
[69] Bartlett J. In: Kaplan J, editor. Bartlett’s familiar quotations,
16th ed. Little, Brown and Co, London, UK 1992.
[70] Kadaba MP, Ramakrishnan HK, Wootten ME, Gainey J, Gor-
ton G, Cochran GV. Repeatability of kinematic, kinetic, and
electromyographic data in normal adult gait. J Orthop Res
1989;7(6):849 – 60.
[71] Kadaba MP, Ramakrishnan HK, Jacobs D, Chambers C, Scar-
borogh N, Goode B. Pattern recognition in spastic diplegia.
Biomecanica 1995;III(4):49 – 58.
[72] Kadaba MP, Wootten ME, Gainey J, Cochran GV. Repeatabil-
ity of phasic muscle activity: performance of surface and intra-
muscular wire electrodes in gait analysis. J Orthop Res
1985;3(3):350 – 9.
[73] Kadaba MP, Ramakrishnan HK, Wootten ME. Measurement of
lower extremity kinematics during level walking. J Orthop Res
1990;8(3):383 – 92.[74] Campbell KR. Expert vision, data acquisition and analysis, in:
ASME International Computers in Engineering Conference and
Exhibition, New York, NY, 1987.
[75] Craig JJ. Introduction to robotics. Addison-Wesley, Boston, MA
1989.
[76] Grood ES, Suntay WJ. A joint coordinate system for the clinical
description of three-dimensional motions: application to the
knee. J Biomech Eng 1983;105:136 – 44.
[77] http://guardian.curtin.edu.au /cga/faq/angles.html O, Methods
for representation of angular rotations.
[78] Sutherland DH, Kaufman KR, Moitoza JR. Kinematics of
normal human walking. In: Rose J, Gamble JG, editors. Human
walking. Baltimore: Williams and Wilkins, 1994:23 – 43.
[79] Oef finger DJ, Pectol RWJ, Tylkowski CM. Foot pressure and
radiographic outcome measures of lateral column lengthening
for pes planovalgus deformity. Gait and Posture 2000;12(3):189 –
95.
[80] Tylkowski CM, Simon SR, Mansour JM. The Frank Stinchfield
Award Paper. Internal rotation gait in spastic cerebral palsy, in
Hip, 1982:89 – 125.
[81] Tylkowski CM, Rosenthal RK, Simon SR. Proximal femoral
osteotomy in cerebral palsy. Clin Orthop
1980;151(September):183 – 92.
[82] Mazur JM, Sienko-Thomas S, Wright N, Cummings RJ. Swing-
through vs. reciprocating gait patterns in patients with thoracic-
level spina bifida. Z Kinderchir 1990;45(Suppl. 1):23 – 5.
[83] Buckon CE, Sienko-Thomas S, Aiona MD, Piatt JH. Assess-
ment of upper-extremity function in children with spastic diple-
gia before and after selective dorsal rhizotomy. Dev Med Child
Neurol 1996;38(11):967 – 75.
[84] Cooper RA, Quatrano LA, Stanhope SJ, Cavanagh PR, Miller
F, Kerrigan DC, Esquenazi A, Harris GF, Winters JM. Gait
analysis in rehabilitation medicine: a brief report. Am J Phys
Med Rehab 1999;78(3):278 – 80 May – June.
[85] O’Connell PG, Lohmann Siegel K, Kepple TM, Stanhope SJ,
Gerber LH. Forefoot deformity, pain, and mobility in rheuma-
toid and nonarthritic subjects. J Rheumatol 1998;25(9):1681 – 6
September.
[86] Siegel KL, Kepple TM, O’Connell PG, Gerber LH, Stanhope SJ.
A technique to evaluate foot function during the stance phase of
gait. Foot Ankle Int 1995;16(12):764 – 70 December.
[87] Kepple TM, Sommer H Jr., Lohmann Siegel K, Stanhope SJ. A
three-dimensional musculoskeletal database for the lower ex-
tremities. J Biomech 1998;31(1):77 – 80 January.
[88] Holden J, Orsini J, Siegel K, Kepple TM, Gerber L, Stanhope S.
Surface movement errors in shank kinematics and knee kinetics
during gait. Gait and Posture 1997;5:217 – 27.
[89] Reinschmidt C, van den Bogert AJ, Nigg BM, Lundberg A,
Murphy N. Effect of skin movement on the analysis of skeletal
knee joint motion during running. J Biomech 1997;30(7):729 – 32.
[90] Cappozzo A, Catani F, Leardini A. Skin movement artifacts in
human movement photogrammetry, in: Abstracts of the XIVth
Congress of the International Society of Biomechanics, Paris,
1993.
[91] Angeloni C, Cappozzo A, Catani F, Leardini A. Quantification
of relative displacement between bones and skin and plate
mounted markers, in: Eighth Meeting of the European Society of
Biomechanics, Rome, 1992.
[92] Perry J, Enwemeka CS, Gronley JK. The stability of surface
markers during knee flexion, in: 34th Annual Meeting of the
Orthopaedic Research Society, 1988.

8/6/2019 Sutherland 2
http://slidepdf.com/reader/full/sutherland-2 21/21
D.H . Sutherland / Gait and Posture 16 (2002) 159 – 179 179
[93] Lafortune MA, Cavanagh PR, Kalenak A, Skinner SM, Sommer
HJ. The use of intra-cortical pins to measure the kinematics of
the knee joint, in: Proceedings of the Second Biennial Conference
of the Canadian Society for Biomechanics, Kingston, 1982.
[94] Lucchetti L, Cappozzo A, Cappello A, Croce UD. Skin move-
ment artefact assessment adn compensation in the estimation of
knee-joint kinematics. J Biomech 1998;31:977 – 84.[95] Alexander EJ, Andriacchi TP. Correcting for deformation in
skin-based marker systems. J Biomech 2001;34:355 – 61.
[96] Biafore S, Cottrell G, Focht L, Kaufman K, Wyatt M, Suther-
land D. Neural network analysis of gait dynamics. Trans Orthop
Res Soc 1991;16(1):225.
[97] Weintraub MA, Bylander T, Simon SR. QUAWDS: a composite
diagnostic system for gait analysis. Comput Methods Programs
Biomed 1990;32(1):91 – 106.
[98] Kidder SM, Abuzzahab FS, Harris GF, Johnson JE. A system
for the analysis of foot and ankle kinematics during gait. IEEE
Trans Rehab Eng 1996;4(1):25 – 32.[99] Kaufman KR, Kitaoka HP, Hansen D, Shaughnessy WJ. Tech-
nique for measurement of foot and ankle kinematics in children,
in: IEEE/EMBS 19th International Conference, Chicago, IL,
1997.