sustainability and transition: re-framing the issues · joe kutzin, who sharing and debating...
TRANSCRIPT

Joe Kutzin, WHO
Sharing and Debating Country Experiences on
Health Financing Reform
Health Financing Technical Network Meeting 14 December 2016, Geneva, Switzerland
Sustainability and Transition:
re-framing the issues
2 |
TRANSITION AS A MOTIVATOR

3 |
Recognition of limits of donor funding, especially given global financial / economic situation
Big funders (e.g. GFATM, Gavi) seeking to prioritize/target across countries as part of their need to cope with fewer resources
– e.g. Equitable Access Initiative
WHO health programs have also identified this as a major concern, leading to growing interest in revenue sources to ensure sustainability of “my program”
– DRM and “innovative financing”
Growing concerns over past few years from
GHIs and health programs

4 |
What is real in the transition from aid
Many countries can expect a decline in aid
When this happens, total spending moves faster than
public spending
Therefore, countries need to:
– Strengthen public finance, increase tax capacity, etc.
– Improve efficiency to get more from the money they spend on
health
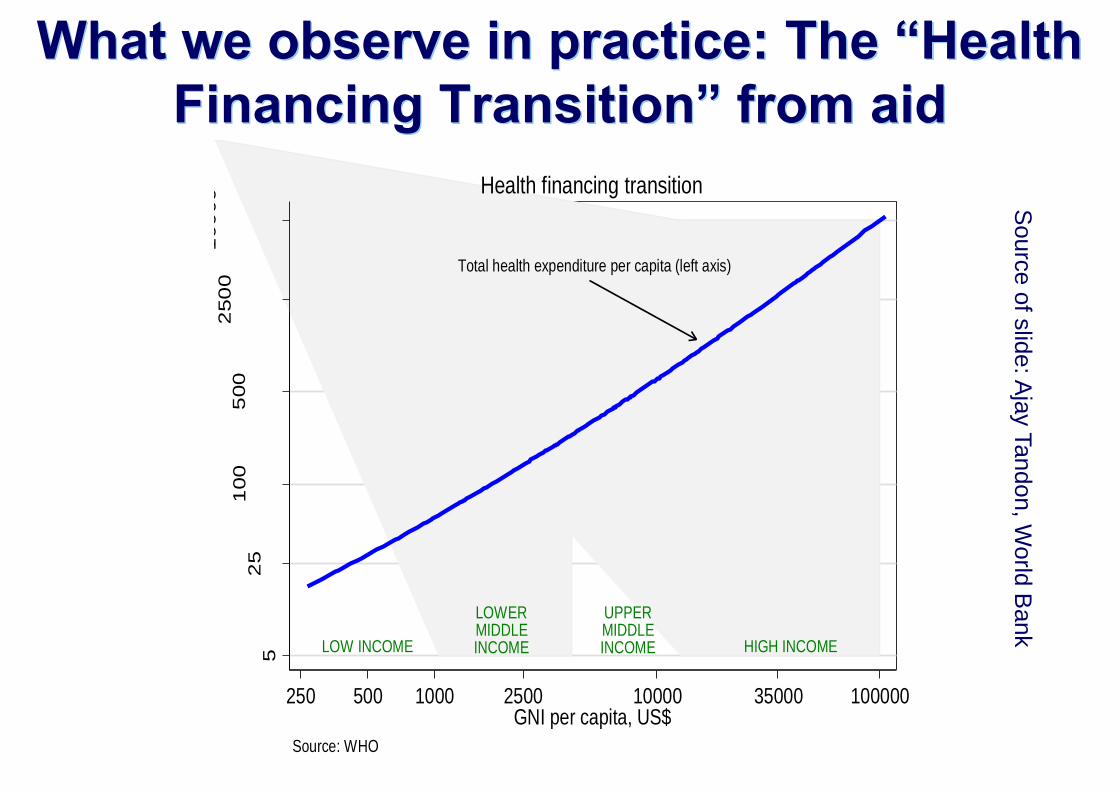
What we observe in practice: The “Health
Financing Transition” from aid
Total health expenditure per capita (left axis)
LOW INCOME
LOWERMIDDLEINCOME
UPPERMIDDLEINCOME HIGH INCOME
52
51
00
500
250
01
00
00
Tota
l h
ea
lth e
xp
en
ditu
re p
er
cap
ita, U
S$
250 500 1000 2500 10000 35000 100000GNI per capita, US$
Source: WHO
Health financing transition
Sourc
e o
f slid
e: A
jay T
andon, W
orld
Bank

What we observe in practice: The “Health
Financing Transition” from aid
Total health expenditure per capita (left axis)
External share (right axis)
LOW INCOME
LOWERMIDDLEINCOME
UPPERMIDDLEINCOME HIGH INCOME
01
02
03
04
05
0
Sh
are
of to
tal he
alth
exp
en
ditu
re (
%)
52
51
00
500
250
01
00
00
Tota
l h
ea
lth e
xp
en
ditu
re p
er
cap
ita, U
S$
250 500 1000 2500 10000 35000 100000GNI per capita, US$
Source: WHO
Health financing transition
Sourc
e o
f slid
e: A
jay T
andon, W
orld
Bank

What we observe in practice: The “Health
Financing Transition” from aid
Total health expenditure per capita (left axis)
External share (right axis)
OOP share (right axis)
LOW INCOME
LOWERMIDDLEINCOME
UPPERMIDDLEINCOME HIGH INCOME
01
02
03
04
05
0
Sh
are
of to
tal he
alth
exp
en
ditu
re (
%)
52
51
00
500
250
01
00
00
Tota
l h
ea
lth e
xp
en
ditu
re p
er
cap
ita, U
S$
250 500 1000 2500 10000 35000 100000GNI per capita, US$
Source: WHO
Health financing transition
Sourc
e o
f slid
e: A
jay T
andon, W
orld
Bank
8 |
And don’t tell anyone, but…
For those countries not experiencing transition, important
health financing priorities are to…
– Strengthen public finance, increase tax capacity, etc.
– Improve efficiency to get more from the money they spend on
health
So let’s use the momentum attached to transition to
reinvigorate efforts to do what should already have been
done in any case

9 |
The international response has largely
focused on revenues
How much can we raise from “innovative financing”,
lobbying the MOF, and donor funding to meet our “magic
number” targets?
Health programs and their partners each addressing
these issues and approaching Finance Ministries
– …for sustainability of their program (HIV/AIDS, NCDs, NTDs,
nutrition, RMNCAH, TB, malaria,…)

10 |
Some concerns
We can’t (or shouldn’t) be arguing that every important
disease deserves its own tax and revenue stream
Sustainability is not only a revenue question; we have to
think about managing expenditures better to get better
results from our spending
– “Can’t just spend your way to UHC”
Need comprehensive rather than piecemeal engagement
between health and finance
11 |
A POSSIBLE WAY FORWARD

12 |
We need to learn from the MDG era, and put
the “S” in SDG!
Great progress made on critical health issues
But also unintended consequences – MDGs stimulated fragmentation: separate plans, budget,
funding, procurement, monitoring, etc.
– SDG targets may lead to continued emphasis on vertical approaches: more separate plans, monitoring mechanisms, funding streams and implementation efforts; with only limited investment in harmonization and alignment across programs
The UHC target can provide “umbrella” to enable move away from silos and fragmentation
– Requires much more active collaboration with programs within the health sector, and focus on prioritization within unified national health strategies

13 |
What is needed to take this in a more
productive direction?
Get the questions right
Use the appropriate unit of analysis
Without these two fundamentals, all the tools and
techniques we have at our disposal can easily be mis-
used

14 |
Getting the sustainability question right
Not this:
– How can we make the TB (or HIV, or immunization, or MCH,
or…) program sustainable?
Instead this:
– How can we sustain increased effective coverage of priority
interventions?
– Because almost certainly, we can’t do it with 5 procurement
systems, 3 information systems, fragmented governance,
distorted HRH incentives, etc. etc.

15 |
…emerged when public health programs were seen as
sufficiently “different” to require entirely separate
arrangements for all health system functions:
– Consequences of communicable diseases certainly require
heavy subsidy or should be fully free
– But there is no a priori reason for separate pooling and
purchasing arrangements
– Same with service delivery
– And certainly not separate information, procurement, supply
chain, governance, HRH, etc.
The vertical program (silo) problem…

There seems to be an inverse relation between a
country’s level of income and the complexity of
its financial flows: can we move away from this?

17 |
What a “UHC lens” brings to this issues
Unit of analysis is the system, not the program or single
disease
– Budget dialog makes sense at sectoral level, not disease-by-
disease
– Assess progress at level of population, not for “scheme
members” or program beneficiaries
– Just as an insurance scheme can make its members better off at
the expense of the rest of the population, so too with a health
program
– Similarly with efficiency, need a whole system, whole population
unit of analysis (the cross-programmatic approach)

B A
Le
vel of goal att
ain
ment
Level of resource inputs
maximum attainable for
given resource input level
Adapted from P. Travis
An efficiency agenda is central to the ability of
governments to sustain progress on their
coverage goals (not their programs)

Not just a concept: empirically, wide variation in
performance at similar expenditure levels
Service coverage: systematic increase in performance with increased public spending; also systematic fall in variation across countries (less poor performers).
Financial protection: performance increases in Q4 and Q5. High variation remains.
10%
20%
30%
40%
50%
60%
70%
80%
90%
100
%
Q1 Q2 Q3 Q4 Q5
Q1 to Q5 denote quintiles of public spending on health per capita, US$(PPP)
Financial protection (proxy)Average all service coverage indicators
n=16 or 17
<$37 $38 to $59 $61 to $198 $207 to $500 >$520
Jow
ett e
t al. (2
016). S
pendin
g ta
rgets
for h
ealth
:
no m
agic
num
ber. W
HO
.

20 |
Be clear on what are we trying to sustain
Neither “health programs” nor even “health systems”
– These are means, not ends
Aim of policy is to improve performance (mix of health
system goals, as e.g. embodied in UHC) to the extent
possible subject to the constraint of living within our
budget
Therefore, what we want to sustain is increased effective
coverage of priority interventions

21 |
How to meet the challenge?
Look beyond just revenues
Not about meeting a “magic” target or “innovative
financing”, donor funds, investment cases for a particular
program
Health programs and their partners each
addressing these issues and approaching finance for
sustainability of their own program (HIV/AIDS, NCDs,
NTDs, nutrition, RMNCAH, TB, malaria,…)
Can’t (and shouldn’t) argue that every important disease
needs its own tax and revenue stream

22 |
We need to move from silos to
sustainability
Imagine you are a Minister of Health of a newly middle-
income country, confronted with all of these demands,
as well as learning that because of your country’s
economic progress, donors will reduce their funding…
– You are responsible for the entire sector, and you have to
make better use of all of your resources
– Aim to streamline system architecture across programs
while ensuring good results
But enabling efficiency gain may actually require
investment
– Potentially large agenda to strengthen underlying systems

23 |
CONCLUSION AND SOME
QUESTIONS FOR DISCUSSION

24 |
An approach to sustaining improvement
through the transition
Ensure that the sustainability and transition agenda is not only about revenues; the expenditure/institutional side (improving efficiency) must be part of the dialog
Ensure unit of analysis is system level, not program level
Maintain or even increase accountability for results that is typically associated with “health programs”, focusing on
– Clear accountability for ensuring delivery of priority, quality services to the populations that need them (i.e. effective coverage)
– Reduce costs to the system of doing this (e.g. addressing duplication and overlap) so that progress towards coverage goals can be sustained

25 |
Some questions to consider for discussion
How does this “transition” debate play out at country level? – Is it all about spending gaps or reference to global targets?
Is efficiency on the agenda? What are you doing about it? – Efficiency only within programs/schemes, but also across them
(dealing with duplication, overlap?)
– Reforms and/or investments needed?
Are there points of conflict between country and “donor” perspectives and priorities? Can we identify these so that they can be addressed? Where do views converge?
What differences in priorities and perspectives between “programs” and MOH? Implications?