susan ann mason - webs
TRANSCRIPT

JOURNAL OF APPLIED BEHAVIOR ANALYSIS
ARTIFACTUAL EFFECTS OF SENSORY-INTEGRATIVE THERAPY ONSELF-INJURIOUS BEHAVIOR
SusAN ANN MASONUNIVrErSIY OF MARYLAND
AND
BRiAN A. IWATAUNIVERSITY OF FLORIDA
Three individuals who exhibited self-injurious behavior (SIB) were exposed to sensory-integrativetherapy. Prior to treatment, a functional analysis baseline was conducted to identify the motivationalfeatures of their SIB. One subject's SIB appeared to be an attention-getting response (maintainedby positive reinforcement), which varied subsequently as a function ofattention being either withheldor provided noncontingently during sensory-integration sessions. The 2nd subject displayed a patternof responding suggestive of stereotypic SIB (maintained by automatic reinforcement), which par-adoxically increased during sensory-integration sessions. The 3rd subject's SIB appeared to functionas an escape response (maintained by negative reinforcement), and his behavior during sensory-integration sessions was similar to that observed during baseline sessions in which demands werenot present. The SIB of all 3 subjects later was reduced when behavioral interventions were applied.The data presented raise questions about the active components of sensory-integrative therapy andthe functional types of SIB for which it might be appropriate.DESCRIPTORS: functional analysis, self-injurious behavior, sensory-integrative therapy, stereo-
typic behavior
A considerable amount of research conductedover the past 20 years has focused on the treatmentof self-injurious behavior (SIB), a serious and chronicdisorder that poses significant physical, social, andeducational risks. The most effective interventions\developed to date have been based on operantconditioning principles (Baumeister & Rollings,1976; Favell, Azrin et al., 1982; Johnson & Bau-meister, 1978). This fact provides support for thegeneral theory that much of SIB is learned behavioror, if not, responds nevertheless to environmentalcontingencies that are applied either directly (e.g.,as in providing reinforcement or punishment for
This research was supported by Grant HD16052 fromthe National Institute of Child Health and Human Devel-opment. We thank Merril Dorsey, Therese Goldfarb, TerriHelinski, Chris House, Michael Richardson, and Marcie Vin-ton for their assistance in conducting various aspects of theresearch.
Reprints may be obtained from Susan Mason, DepartmentofSpecial Education, Benjamin Building, University ofMary-land, College, Park, Maryland 20742, or from Brian Iwata,Department ofPsychology, University of Florida, Gainesville,Florida 32611.
target behaviors) or indirectly (e.g., as in manip-ulating setting events to occasion the occurrence ofan alternative behavior that is automatically rein-forced, thereby competing with the SIB).
Other explanatory accounts for the developmentof SIB offer a theoretical foundation for the use oftherapies in which a contingency is never manip-ulated. One such account is based on a neurodevel-opmental orientation proposed by Ayres (1972,1974) and Norton (1975). In its general form, thetheory conceptualizes the failure to develop motorcoordination as evidence of central nervous system(CNS) dysfunction, which may be alleviatedthrough various types of physiological stimulationcollectively described as sensory-integrative therapy.Lemke (1974) extended this position by suggestingthat stereotypic and self-injurious behaviors seen indevelopmentally disabled individuals may be a fur-ther reflection of poor sensory-motor integration.In support of this position, Lemke presented anuncontrolled case study in which multiple forms ofstimulation (finger massage and ice to the mouth,quiet talk, tooth brushing, towel massage to the
361
1990,23.361-370 NUMBER 3 (FALL 1990)

SUSAN ANN MASON and BRIAN A. IWATA
arms, patty cake, feet slapping, and body rolling)were applied to a self-injurious client. Although noquantitative data were presented, the author notedthat the subject eventually was freed from restraintand was taught to hold a toy in each hand (onetoy was mouthed; the other was banged).
In another case study, Bright, Bittick, and Flee-man (1981) administered tactile, vestibular, andsocial stimulation (rocking in a hammock, strokingthe back, holding in a rocking chair while providingsocial interaction), and reported that their subject'sfrequency of SIB decreased during treatment ses-sions. Wells and Smith (1983) provided similartypes of stimulation (rocking in a hammock androcking chair, battery-operated vibratory stimula-tion, massage, rolling the body over a large ball,rolling bolsters over arms and legs). Results ob-tained with 4 subjects showed that the frequencyofSIB decreased during therapy sessions when com-pared to baseline, although it was noted that SIBwas prevented periodically through manual re-straint.The studies by Bright et al. (1981), Lemke
(1974), and Wells and Smith (1983) contained anumber of methodological problems that preventdear interpretation of the reported data. None ofthe studies provided evidence of adequate mea-surement or assessment of interobserver agreement,and only Wells and Smith (1983) presented datafrom a baseline condition. A third problem witheach of the studies was confounding of the inde-pendent variable. Physiological stimulation waspresented concurrent with other events, most no-tably noncontingent social stimulation, that bythemselves may have been responsible for reportedchanges in behavior. Some of these problems wereaddressed in a recent investigation by Dura, Mulick,and Hammer (1988). The authors compared theeffects of vestibular stimulation (movement backand forth on a swing while the client was seatedon a therapist's lap) with those of a control con-dition in which a therapist provided attention with-out apparent vestibular stimulation (playing catchwith assistance, rolling a toy, and taking turns atan activity while seated). Results showed that thesubject exhibited no SIB during sessions containing
vestibular stimulation and variable rates of SIBduring the attention control.
The Dura et al. (1988) study is noteworthy inthat it is the first controlled evaluation of sensory-integrative therapy showing positive results withSIB; additional research is needed to darify theconditions under which similar or different resultswould be obtained. For example, it is now generallyagreed that SIB is a complex disorder that may bedeveloped and maintained through a variety ofmechanisms; from a learning perspective, these in-dude positive, negative, and automatic reinforce-ment. The theoretical basis for sensory-integrativetherapy suggests that the most appropriate test con-dition would be with stereotypic (automatically re-inforced) SIB that is not maintained by environ-mental contingencies. By contrast, SIB that is dearlyrelated to environmental events may be affected bycoincidental features of sensory-integrative therapy.Attention-motivated SIB would be suppressedthrough noncontingent attention, which is a com-ponent of sensory-integrative therapy; therein liesthe importance of the attention control providedby Dura et al. Escape-motivated SIB also may showa decrease during sensory-integration sessions mere-ly as a function of reduced aversive stimulationthrough withdrawal of demands.
The present study extends previous research onsensory-integrative therapy by examining its effectswith 3 self-injurious individuals selected on thebasis of data obtained during a functional analysisbaseline. One subject exhibited SIB that seemed tofunction as an attention-getting response, the 2ndsubject's SIB appeared to be stereotypic in nature,and the 3rd subject's SIB functioned as escapebehavior.
METHOD
Subjects and SettingSally, a 6-year-old severely retarded female, could
feed herself with assistance, but she had no otherindependent self-care skills. She responded to hername but otherwise exhibited no language skills.Kathy, a 3-year-old profoundly retarded female,
362

SENSORY-INTEGRATIVE THERAPY AND SIB
had cerebral palsy and scoliosis. She required fillassistance with feeding, dressing, toileting, and oth-er self-care skills, and she did not have any languageskills. Mort, an 18-year-old profoundly retardedmale, had microcephaly and scoliosis. He couldfeed himself and dress with minimal assistance, buthe had no other independent self-care or languageskills.
All subjects displayed SIB that produced tissuedamage and was judged to pose moderate risk (i.e.,lacerations and contusions required minor woundcare by a physician or nurse, but they had neverrequired inpatient care, nor were they likely toimpair vision or hearing). Sessions for Kathy andMort were conducted in therapy rooms equippedwith one-way observation windows. Sally's sessionswere conducted in a small empty dassroom thatdid not contain observation windows. Observers forSally's sessions were seated behind a fine-mesh screenplaced at least 3 m from the subject.
Response Measurement and ReliabilitySelf-injurious responses were defined as follows:
hand biting (Kathy)-closure of upper and lowerteeth on hand or wrist; hand mouthing (Kathy)-insertion of fingers or hand into the mouth; headbanging (Mort)-audible contact between the headand either a fist or an object; and slapping (Kathy,Sally, Mort)-audible contact between the handand another part of the body. Data were collectedon hand-held computer (Panasonic Model RL-H1800 or Hewlett Packard Model HP-71B) andwere summarized as the percentage of 10-s intervalsduring which one or more SIBs occurred.
Interobserver agreement was assessed by havinga second observer simultaneously but independentlyrecord data during 38%, 39%, and 35% of thesessions overall for Sally, Kathy, and Mort, re-spectively, and during at least 20% of the sessionsin each phase of the study. Agreement percentageswere calculated via computer based on interval-by-interval comparisons of observers' records bydividing agreements by agreements plus disagree-ments and multiplying 100. Mean overall, occur-rence, and nonoccurrence agreement percentages,respectively, were as follows: Sally-93%, 95%,
91%; Kathy-96%, 96%, 97%; and Mort-97%,97%, 93%.
Experimental SequenceThe study consisted of three phases. In Phase 1,
subjects were observed in a series of baseline con-ditions to assess the functional properties of theirSIB. In Phase 2, they were exposed to sensory-integrative therapy. Additional control procedureswere implemented with Sally and Mort based onresults obtained during sensory-integration sessions.Finally, subjects' SIB was treated via behavioralinterventions in Phase 3.
Phase 1:functional analysis baseline. Subjectswere exposed to four conditions, each presentedduring 15-min sessions in a multielement format(Sidman, 1960; Ulman & Sulzer-Azaroff, 1975).A brief description of these conditions is providedhere; more complete details can be found in Iwata,Dorsey, Slifer, Bauman, and Richman (1982) andIwata, Pace, Kalsher, Cowdery, and Cataldo (1990).During the demand condition, a therapist presentedacademic tasks to the subject in a discrete-trialformat, delivered praise contingent on correct re-sponses, and implemented a 30-s time-out contin-gent on the occurrence of SIB. During the attentioncondition, a therapist initially instructed the subjectto play with toys that were in the room and pro-ceeded to do paperwork. Contingent on the oc-currence of SIB, the therapist delivered a verbalreprimand, expressed concern, and briefly inter-rupted the SIB. During the alone condition, thesubject was observed while alone in the room, whichwas empty except for a chair (Kathy and Mort) orobservers positioned behind the screen (Sally). Thefinal condition, play, served as a control for theother three conditions. The therapist provided ac-cess to toys, provided praise approximately every30 s contingent on the absence of SIB, and ignoredoccurrences of SIB.
Phase 2: sensory-integrative therapy. Sensory-integrative therapy refers to a variety of techniqueswhose major components involve the delivery ofmultisensory stimulation, although operational de-scriptions are difficult to find even in primary sources.In addition, the techniques that have been applied
363

SUSAN ANN MASON and BRIAN A. IWATA
as treatment for SIB represent only a few of themany components that have been described by oth-ers (e.g., Ayres, 1972, 1974), and these techniquesvaried significantly across studies (Bright et al.,1981; Dura et al., 1988; Lemke, 1974; Wells &Smith, 1983). The modalities and specific stimuliselected for indusion in this study were based onavailable literature and recommendations providedby occupational therapists who were trained in andwho used sensory-integration techniques. The pro-cedures were designed to be representative of thoseused by Bright et al., Dura et al., and Wells andSmith, with exceptions noted below.
Sensory-integration sessions were begun imme-diately upon completion of the baseline phase andwere implemented in a multiple baseline acrosssubjects design. During these sessions, subjects wereprovided noncontingent access to apparatus thatdelivered auditory, kinesthetic, tactile, vestibular,and visual stimulation. The apparatus for all sub-jects were similar and consisted of (a) a flashingamber or blue light suspended from the ceiling,(b) a rocking chair with a vibrating pillow attachedat neck level, and (c) a cassette tape recorder thatplayed rock or jazz music. During each 15-minsession, all apparatus were activated. A therapistremained in the room to monitor the subject's safetybut did not otherwise interact with the subject. Theabsence of interaction was designed to allow con-tinuous access to several sources of physiologicalstimulation independent of the potentially con-founding effects of social stimulation. Although thisseems like a significant departure from the mannerin which sensory-integrative therapy usually is de-livered, the lack of social interaction should beunimportant if physiological stimulation is the crit-ical component. Moreover, this variation not onlywas considered acceptable but was specifically sug-gested by Wells and Smith (1983), who recom-mended ". . . the automated provision of sensorystimulation through vibratory chairs and magic-finger beds, as well as audio-visual and other formsof sensory stimuli" (p. 666). With 1 subject (Sally)the effects of sensory-integrative therapy with andwithout attention were examined systematically ina reversal design.
Phase 3: behavior intervention. Based on dataobtained during Phase 1, behavioral treatments weredesigned for each subject that seemed appropriateto the apparent function of their SIB. These pro-cedures were implemented in a staggered sequenceacross baselines but, because the treatments nec-essarily differed across subjects, the design cannotbe considered a true multiple baseline (i.e., theeffects of the same variable were not replicated).Treatment for Sally and Mort involved extinctionthrough removal of the reinforcement contingencyfound to be maintaining their SIB during baseline.An analogous extinction procedure for Kathy-sensory extinction (Rincover & Devaney, 1982)-was not possible because we could not identify thespecific reinforcing stimuli produced by her behav-ior. As in previous conditions, sessions lasted for15 min.
Sally's assessment data suggested that her SIBwas maintained by attention, which was furtherconfirmed through attention manipulations (absentvs. continuously present) during sensory-integrationsessions in Phase 2. Therefore, we examined theeffects of another attention manipulation-time-out from attention-in Phase 3. The therapist satdose to Sally and provided praise, pats on the back,etc., during each 10-s interval in which Sally didnot exhibit SIB. Contingent on the occurrence ofSIB, the therapist moved her chair away (approx-imately 1 m) and turned her back to Sally. Atten-tion was resumed after SIB had ceased for 10 s.The effects of extinction were evaluated in a reversaldesign (ABA) in which the A condition consistedof extinction and the B condition consisted of theoriginal baseline, in which the therapist attendedto Sally only when she exhibited SIB.
Kathy's intervention consisted of providing herwith access to materials whose manipulation mightcompete with hand biting, hand mouthing, andslapping (Favell, McGimsey, & Schell, 1982). Sev-eral hanging toys were suspended on a pole fromhere wheelchair in such a way that she could graspthem and either hold or guide them to her mouth.This procedure was supplemented with a differ-ential reinforcement of other behavior (DRO) con-tingency in which the therapist provided praise for
364

SENSORY-INTEGRATIVE THERAPY AND SIB
the absence of SIB (a 1-min schedule initially thatwas extended to 2 min on Session 52) and a mildverbal reprimand ("No") plus brief response in-terruption contingent on the occurrence of SIB.
Because Mort's SIB decreased during sensory-integration sessions, a return to baseline in the de-mand condition was implemented before initiatinghis behavioral program. Treatment was then im-plemented, still within the context of the demandcondition, and consisted of "escape extinction"(Iwata et al., 1990). The therapist issued instruc-tions as before but did not terminate trials contin-gent on the occurrence of SIB. Instead, wheneverMort hit himself, he was immediately guided tocomply with the therapist's request.
RESULTS
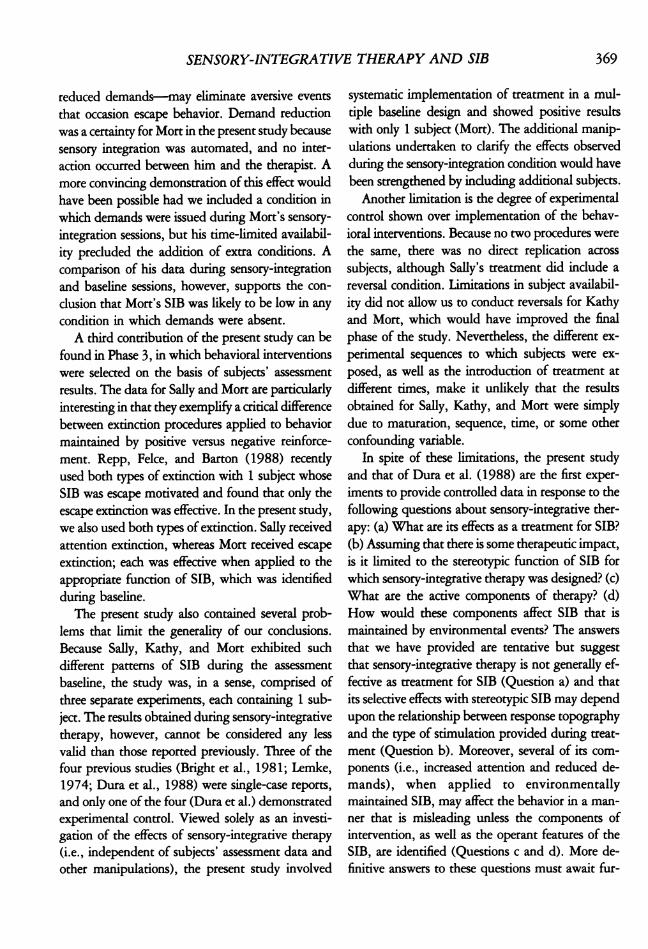
Figure 1 shows that the occurrence of SIB, ex-pressed as percentage of 10-s intervals, for all sub-jects during all experimental conditions. Due todifferences observed across subjects during the in-itial baseline that determined subsequent variationsin procedure, each subject's experimental sequenceand results are described separately.
SallyDuring baseline, Sally's SIB occurred almost ex-
dusively during the attention condition, suggestingthat the behavior was maintained by positive re-inforcement. Little or no SIB occurred during con-ditions in which attention was provided noncon-tingently (demand), contingent on the absence ofSIB (play), or when stimuli associated with atten-tion were completely absent (alone).
Sally's behavior during baseline indicated thatcontingent or discriminative arrangements based onattention would differentially affect her SIB; thispossibility was explored in Phase 2. Sensory-inte-gration sessions with no attention were alternatedin a reversal design with sessions in which the ther-apist provided noncontingent attention (praise,reading a story aloud, pats on the head or back)during every 10-s interval. During sensory inte-gration without attention, Sally's SIB remained un-changed from the baseline attention condition. Al-
though these negative results were not consistentwith those from previous studies on sensory-inte-grative therapy, they were very consistent with herbaseline pattern of responding, which suggestedthat the presence of a therapist during sensory-integration sessions was discriminative for SIB. Be-cause it was not possible to eliminate the therapistcompletely from the immediate situation due tothe electrical apparatus in the room, the therapistnext provided continuous attention concurrent withsensory-integrative therapy. This operation presum-ably would amount to noncontingent reinforce-ment, which would remove the motivational basisfor responding. When the attention was imple-mented and later removed, Sally's SIB decreasedrapidly and later returned to its previous level.
The final three conditions for Sally involved stillanother evaluation of attention-related effects. Thepositive reinforcer (attention) for her SIB was with-held contingent on SIB during extinction, deliveredcontingent on SIB during the return to baseline,and withheld again. During these three conditions,her behavior showed orderly changes similar tothose observed when attention was manipulatedduring the baseline assessment and sensory-inte-grative therapy.
KathyDuring baseline, Kathy's SIB was somewhat
lower in the play condition; in demand, attention,and alone conditions, her SIB was rather variableand undifferentiated. Responding of this type sug-gests several interpretations. One is that Kathy failedto discriminate among the different conditions. Ifsuch were the case, one would expect eventualseparation of the data based on repeated contactwith the contingencies, but that did not occur over37 sessions. A second possibility is that SIB wasmaintained by more than one source of reinforce-ment (i.e., some combination of positive, negative,and/or automatic reinforcement). However, thecontinued occurrence of SIB during the alone con-dition, in which the absence of a therapist washighly discriminable for extinction (assuming thatattention was a motivational factor) or the absenceof aversive events (assuming that escape from de-
365

366 SUSAN ANN MASON and BRIAN A. IWATA
100 BASEUNE SENSORY NTEGRATION EXTINCTIONNo Attention Attention
SALLY _ \W~~~~~~~~~~~ithdrawal)80 ~~~~~~~~~~Continuous I
Attentlo ~~LINE
60-
40
20
TOYS + DRO +(0 100- RESPONSE INTERRUPT
W KTHY
CL,
80 - -DemandcI-a-- Attention>~~~~~~~~~~~--Alone
T- 0~~~~~~~~~~-a PlayWL 60 -' Sens.Integrationz
40 -
lE-zWI 20-
100 BL~~~~~~~~~~~11 EXTINCTION100 ~~~~~~~~~~~~DemandNOW ~ ~~ ~~~~~~~~~(Continuation)
80
60-
40-
20-
0-20 40 60 80
SESSIO0NS
FOLLOW-UP
Figure 1. Percentage of 10-s intervals of SIB exhibited by Sally, Kathy, and Mort during baseline assessment, sensory-integration therapy, and behavioral treatment.

SENSORY-INTEGRATIVE THERAPY AND SIB
mands was a motivational factor), suggests thatneither positive nor negative reinforcement weremaintaining variables for Kathy's SIB. The mostplausible explanation is that her SIB was stereo-typed in nature (Baumeister, 1978) and unrelatedto any of the events that were manipulated duringbaseline conditions.
Kathy's SIB actually got worse during sensory-integration sessions, increasing to a level higher thanthat observed during any of her baseline conditions.Although this condusion is based on data obtainedduring only six sessions of treatment, the trend wasrather dear. In addition, it is unlikely that extendedapplication of sensory integration would have pro-duced different results because, as Bright et al.(1981) predicted, the reductions in SIB demon-strated in later studies using sensory integration(Dura et al., 1988; Wells & Smith, 1983) wereimmediate. Thus, Kathy's results were not consis-tent with findings from previous studies on sensory-integrative therapy and were surprising in light ofher baseline data, which indicated that she wouldbe a "positive responder."When access to toys, reinforcement, and response
interruption were implemented with Kathy, an im-mediate reduction was seen in her SIB comparedto the preceding condition (sensory-integrative ther-apy). During subsequent sessions, as she began tomanipulate the toys more frequently, her SIB grad-ually decreased further. These results are consistentwith those presented by Favell, McGimsey, andSchell (1982), who found with some subjects thatit was necessary to supplement a toy-available con-dition with explicit reinforcement and interruptionprocedures. In Kathy's case, the effects of thesesupplementary interventions were undear. Becauseher SIB continued in a downward trend throughoutthe final condition (which ended when she was nolonger available for participation in the study), wewere unable to evaluate the relative effects of thedifferent components of her treatment.
MortSIB occurred reliably in the demand condition
during baseline and much less frequently in theattention, alone, and play conditions, suggesting
that the temporary removal of academic tasks (es-cape) served as negative reinforcement for Mort'sSIB. During sensory-integration sessions, SIB oc-curred at low levels comparable to those observedduring baseline conditions in which demands werenot presented (e.g., play). Mort's SIB increasedwhen baseline demand contingencies were rein-stated and decreased to zero during the final con-dition, when the therapist continued to present de-mands independent of Mort's behavior and did notallow him to escape by engaging in SIB.
Follow-UpAt the end of Phase 3, a maintenance/gener-
alization program was designed and implementedfor each subject. The general approach involvedtraining other therapist and caretakers (parents,teachers, etc.) in the use of interventions in effectduring Phase 3 through written instructions, dem-onstration, and supervised practice, and thinningthe reinforcement schedules for Sally and Kathy.Periodic follow-up and observation were then con-ducted either at the clinic (Kathy and Mort) or atthe subject's regular school (Sally). Data collectedat the end of the 6-month follow-up period indi-cated that Sally's and Mort's SIB remained at 0%and that Kathy's SIB occurred at a level equivalentto that obtained at the end of Phase 3 (8%).
DISCUSSION
The results ofseveral studies (Bright et al., 1981;Dura et al., 1988; Lemke, 1974; Wells & Smith,1983) have indicated that sensory-integrative ther-apy might be a promising treatment for SIB. Thisconclusion, however, is not based on data collectedusing adequate experimental techniques. Only Duraet al. used appropriate measurement proceduresand attempted to control for coincidental effects ofintervention. A doser examination of the existingresearch, in light of the theoretical basis for sensory-integrative therapy and variables known to main-tain SIB, suggested the need for additional subject-selection and control procedures. When theseprocedures were incorporated into the present study,the data obtained during sensory-integrative ther-
367

SUSAN ANN MASON and BRIAN A. IWATA
apy were paradoxical for 1 subject and artifactualfor the other 2. These results extend previous re-search on SIB in several ways and raise importantquestions about the effectiveness of sensory-inte-grative therapy as a specific treatment for this dis-order.
First, this study further demonstrates the utilityof assessment procedures that identify the func-tional properties of behavior disorders. Data ob-tained during baseline provided a means ofselectingindividuals whose SIB might be affected by sensory-integrative therapy in different ways. More specif-ically, the baseline allowed us to identify 1 subjectwhose SIB was not maintained by environmentalevents. Kathy's behavior most dearly met thedefinition for stereotypic or self-stimulatory re-sponding, and it is this function of SIB for whichsensory-integrative therapy reportedly was de-signed. Additionally, we were able to identify twoindividuals (Sally and Mort) whose SIB was main-tained by environmental events; their indusion inthe study allowed us to examine the effects ofadditional control procedures.
Second, the results obtained during sensory-in-tegrative therapy were not consistent with previousfindings and/or reflected the influence ofconfound-ing variables. Based on previous research and dataobtained during baseline, we expected to see amarked reduction in Kathy's SIB; instead, her be-havior got worse. A number of hypotheses are sug-gested by her negative results; one is based on therelationship between her SIB and type of stimu-lation provided during sensory-integration sessions.Previous research has shown that noncontingentstimulation related to that produced by stereotypicSIB can suppress responding. For example, Baileyand Meyerson (1970) used vibratory stimulationwith an individual who banged his head, and Fav-ell, McGimsey, and Schell (1982) provided visualtoys to an individual who engaged in eye pokingand popcorn to an individual who exhibited pica.These types of stimulation apparently were similarto that produced by the subjects' SIB and alleviateda condition of deprivation. In the present study,the stimulation provided to Kathy during sensory-integration sessions was not dosely related to her
target behaviors (primarily hand mouthing and bit-ing), whereas the toys provided during her finaltreatment condition were such that toy manipu-lation may have competed with SIB. Thus, theeffects of sensory-integration therapy might be sole-ly a function of competing stimulation; the morevaried the stimulation, the more likely it is to ac-commodate the specific topography ofthe SIB. Thisinterpretation of the differences in Kathy's SIB dur-ing these two conditions is a tentative one becauseother treatment components-DRO and responseinterruption-were induded. In the absence of fur-ther manipulations to determine why Kathy's SIBresponded in a countertherapeutic direction duringsensory-integration therapy, no condusive expla-nation for her results can be offered at this time.At best, we can describe the effects seen with Kathyas paradoxical in that they were unexpected, givenprevious data.
The results obtained for Sally and Mort raise adifferent question: What features of sensory-inte-gration therapy affect SIB that is related to attention(positive reinforcement) and escape (negative re-inforcement)? In Sally's case, the effects of sensoryintegration with and without attention identifiedan artifactual component in previous research onsensory-integrative therapy. All of the studies con-ducted to date induded noncontingent social stim-ulation, ranging from continuous physical contactto multiple forms of physical and social interaction,as part of the treatment process. The Dura et al.(1988) study, the only one to indude an attentioncontrol, compared the effects of continuous atten-tion plus sensory integration versus intermittentattention without sensory integration. Thus, it ispossible that schedule effects alone might accountfor the differences they obtained. The extent towhich observed behavior change in previous studieswas a function of attention per se is unknown,because the functional properties of subjects' SIBwere not identified. Nevertheless, for individualswhose SIB is attention motivated, results obtainedfor Sally indicate that the confounding effects ofattention may be misinterpreted as therapeutic ben-efit derived from sensory-integrative therapy.
Another feature of sensory-integrative therapy-
368
SENSORY-INTEGRATIVE THERAPY AND SIB
reduced demands-may eliminate aversive events
that occasion escape behavior. Demand reductionwas a certainty for Mort in the present study becausesensory integration was automated, and no inter-action occurred between him and the therapist. Amore convincing demonstration of this effect wouldhave been possible had we induded a condition inwhich demands were issued during Mort's sensory-
integration sessions, but his time-limited availabil-ity precluded the addition of extra conditions. Acomparison of his data during sensory-integrationand baseline sessions, however, supports the con-
dusion that Mort's SIB was likely to be low in anycondition in which demands were absent.A third contribution of the present study can be
found in Phase 3, in which behavioral interventionswere selected on the basis of subjects' assessment
results. The data for Sally and Mort are particularlyinteresting in that they exemplify a critical differencebetween extinction procedures applied to behaviormaintained by positive versus negative reinforce-
ment. Repp, Felce, and Barton (1988) recentlyused both types of extinction with 1 subject whoseSIB was escape motivated and found that only theescape extinction was effective. In the present study,we also used both types of extinction. Sally receivedattention extinction, whereas Mort received escape
extinction; each was effective when applied to theappropriate function of SIB, which was identifiedduring baseline.
The present study also contained several prob-lems that limit the generality of our condusions.Because Sally, Kathy, and Mort exhibited suchdifferent patterns of SIB during the assessment
baseline, the study was, in a sense, comprised ofthree separate experiments, each containing 1 sub-ject. The results obtained during sensory-integrativetherapy, however, cannot be considered any lessvalid than those reported previously. Three of thefour previous studies (Bright et al., 1981; Lemke,1974; Dura et al., 1988) were single-case reports,
and only one of the four (Dura et al.) demonstratedexperimental control. Viewed solely as an investi-gation of the effects of sensory-integrative therapy(i.e., independent of subjects' assessment data andother manipulations), the present study involved
systematic implementation of treatment in a mul-tiple baseline design and showed positive resultswith only 1 subject (Mort). The additional manip-ulations undertaken to darify the effects observedduring the sensory-integration condition would havebeen strengthened by induding additional subjects.Another limitation is the degree of experimental
control shown over implementation of the behav-ioral interventions. Because no two procedures werethe same, there was no direct replication acrosssubjects, although Sally's treatment did indude areversal condition. Limitations in subject availabil-ity did not allow us to conduct reversals for Kathyand Mort, which would have improved the finalphase of the study. Nevertheless, the different ex-perimental sequences to which subjects were ex-posed, as well as the introduction of treatment atdifferent times, make it unlikely that the resultsobtained for Sally, Kathy, and Mort were simplydue to maturation, sequence, time, or some otherconfounding variable.
In spite of these limitations, the present studyand that of Dura et al. (1988) are the first exper-iments to provide controlled data in response to thefollowing questions about sensory-integrative ther-apy: (a) What are its effects as a treatment for SIB?(b) Assuming that there is some therapeutic impact,is it limited to the stereotypic function of SIB forwhich sensory-integrative therapy was designed? (c)What are the active components of therapy? (d)How would these components affect SIB that ismaintained by environmental events? The answersthat we have provided are tentative but suggestthat sensory-integrative therapy is not generally ef-fective as treatment for SIB (Question a) and thatits selective effects with stereotypic SIB may dependupon the relationship between response topographyand the type of stimulation provided during treat-ment (Question b). Moreover, several of its com-ponents (i.e., increased attention and reduced de-mands), when applied to environmentallymaintained SIB, may affect the behavior in a man-ner that is misleading unless the components ofintervention, as well as the operant features of theSIB, are identified (Questions c and d). More de-finitive answers to these questions must await fur-
369

370 SUSAN ANN MASON and BRIAN A. IWATA
ther research that extends and improves method-ology in the areas of subject selection, assessmentof behavioral finction, and component analysis.
REFERENCES
Ayres, A. J. (1972). Sensory integration and learningdisorders. Los Angeles: Western Psychological Services.
Ayres, A.J. (1974). The development ofsensory integrativetheory and practice. Dubuque, IA: Kendall/Hunt.
Bailey,J., & Meyerson, L. (1970). Effect of vibratory stim-ulation on a retardate's self-injurious behavior. Psycho-logical Aspects of Disability, 17, 133-137.
Baumeister, A. A. (1978). The origins and control of ste-reotpyed behavior. In C. E. Meyers (Ed.), Quality of lifein severely and profoundly mentally retarded people(pp. 353-384). Washington, DC: American Associationon Mental Deficiency.
Baumeister, A. A., & Rollings, J. P. (1976). Self-injuriousbehavior. In N. R. Ellis (Ed.), International review ofresearch in mental retardation (Vol. 8, pp. 1-34). NewYork: Academic Press.
Bright, T., Bittick, K., & Fleeman, B. (1981). Reductionof self-injurious behavior using sensory integrative tech-niques. American Journal of Occupational Therapy,35, 167-172.
Dura,J. R., Mulick,J. A., & Hammer, D. (1988). Rapidclinical evaluation of sensory integrative therapy for self-injurious behavior. Mental Retardation, 26, 83-87.
Favell, J. E., Azrin, N. H., Baumeister, A. A., Carr, E. G.,Dorsey, M. F., Forehand, R., Foxx, R. M., Lovaas, 0.I., Rincover, A., Risley, T. R., Romanczyk, R. G., Russo,D. C., Schroeder, S. R., & Solnick, J. V. (1982). Thetreatment of self-injurious behavior. Behavior Therapy,13, 529-554.
Favell, J. E., McGimsey, J. F., & Schell, R. M. (1982).Treatment of self-injury by providing alternative sensoryactivities. Analysis and Intervention in DevelopmentalDisabilities, 2, 83-104.
Iwata, B. A., Dorsey, M. F., Slifer, K. J., Bauman, K. E.,
& Richman, G. S. (1982). Toward a functional analysisof self-injury. Analysis and Intervention in Develop-mental Disabilities, 2, 3-20.
Iwata, B. A., Pace, G. M., Kalsher, M. J., Cowdery, G. E.,& Cataldo, M. F. (1990). Experimental analysis andextinction of self-injurious escape behavior. Journal ofApplied Behavior Analysis, 23, 11-27.
Johnson, W. L., & Baumeister, A. A. (1978). Self-injuriousbehavior: A review and analysis of methodological detailsof published studies. Behavior Modification, 2, 465-487.
Lemke, H. (1974). Self-abusive behavior in the mentallyretarded. American Journal of Occupational Therapy,28, 94-97.
Norton, V. (1975). Neurodevelopmental and sensory in-tegration for the profoundly retarded multiply handi-capped child. American Journal of Occupational Ther-apy, 29, 93-100.
Repp, A. C., Felce, D., & Barton, L. E. (1988). Basingthe treatment of stereotypic and self-injurious behaviorson hypotheses of their causes. Journal of Applied Be-havior Analysis, 21, 281-289.
Rincover, A., & Devaney, J. (1982). The application ofsensory extinction procedures to self-injury. Analysis andIntervention in Developmental Disabilities, 2, 67-81.
Sidman, M. (1960). Tactics of scientific research. NewYork: Basic Books.
Ulman, J. D., & Sulzer-Azaroff, B. (1975). Multielementbaseline design in educational research. In E. Ramp &G. Semb (Eds.), Behavior analysis: Areas of researchand application (pp. 359-376). Englewood Cliffs, NJ:Prentice-Hall.
Wells, M., & Smith, D. W. (1983). Reduction of self-injurious behavior of mentally retarded persons usingsensory integrative techniques. American Journal ofMental Deficiency, 87, 664-666.
Received August 7, 1989Initial editorial decision October 6, 1989Revision received January 11, 1990Final acceptance Marrh 6, 1990Action Editor, David P. Wacker