surgical treatment and prognosis in patients with high-grade soft tissue malignant fibrous...
TRANSCRIPT
ORTHOPAEDIC SURGERY
Surgical treatment and prognosis in patients with high-grade softtissue malignant fibrous histiocytoma of the extremities
Kontogeorgakos A. Vasileios • William C. Eward •
Brian E. Brigman
Received: 1 January 2012 / Published online: 10 April 2012
� Springer-Verlag 2012
Abstract
Background Malignant fibrous histiocytoma (MFH) of
soft tissue is one of the most common sarcoma in adult-
hood. However, only a few series have separately studied
the clinical behavior and prognosis of this malignancy.
Methods We retrospectively reviewed 61 patients treated
for extremity soft tissue high-grade MFH. Four patients
had a history of another malignancy and were excluded
from analysis. In 12 referred patients with incomplete
excision, re-excision of the tumor bed was offered. Clinical
and treatment variables were analyzed for their impact on
treatment complications, local recurrence (LR), metastatic
disease (MD) and overall survival (OS).
Results Four patients underwent primary amputation.
Twenty-three patients necessitated a primary reconstruc-
tive procedure for wound closure. Wound healing com-
plication (WHC) developed in 28.3 % of the limb sparing
group of patients. LR developed in 11 patients (19.3 %),
while 6 of them had second LR. Eighteen patients (31.5 %)
developed MD, involving lung at least. Patients who
developed MD \12 vs [12 months, died within 19.3 vs
8 months mean time (p \ 0.05). Overall survivorship was
66.7 % at 5 years. No statistically significant variables
were identified for LR, while multivariate analysis for MD
revealed tumor size [5 cm as the only statistically signif-
icant variable. For OS, development of MD and age
[70 years emerged as independent prognostic factors.
Conclusions The overall prognosis is poor. LR, although
can be managed with tumor re-excision, has high second
recurrence rate. Increased tumor size is associated with
shorter metastasis-free interval which significantly
decreases survival.
Keywords Malignant fibrous histiocytoma � Pleomorphic
sarcomas � Soft tissue extremity sarcoma � Wound healing
complications � Flap reconstruction
Introduction
Malignant fibrous histiocytoma (MFH) of soft tissue was
first described in 1963 by Ozzelo et al. [1] and then in 1964
by O’Brien and Stout [2]. Although initially MFH was
considered of histiocytic origin, recent molecular data have
failed to show evidence of true histiocytic differentiation.
According to WHO criteria, MFH is defined as an undif-
ferentiated high-grade pleomorphic sarcoma [3]. Four
subtypes have been described: undifferentiated-pleo-
morphic, myxoid, giant cell,and inflammatory [4]. Angio-
matoid fibrous histiocytoma is a lesion with low malignant
potential that has characteristic imaging and histologic
features and likely represents a clinically and morpholog-
ically distinct entity. The typical histologic appearance of
K. A. Vasileios (&)
Department of Orthopaedic Surgery, Orthopaedic Oncology,
University Hospital of Larissa, 41110 Larissa, Greece
e-mail: [email protected]
K. A. Vasileios � W. C. Eward � B. E. Brigman
Department of Orthopaedic Surgery, Duke Cancer Institute,
Duke University Medical Center, Duke University, 3312,
Durham, NC, USA
e-mail: [email protected]
B. E. Brigman
e-mail: [email protected]
W. C. Eward
Division of Orthopaedic Surgery, Orthopaedic Oncology,
University of Toronto, 600 University Avenue, Toronto, ON
M4J 5A4, Canada
123
Arch Orthop Trauma Surg (2012) 132:955–961
DOI 10.1007/s00402-012-1510-y
MFH is that of a hypercellular, neoplasm with a marked
cytological and nuclear pleomorphism, bizarre stromal
cells and storiform or fascicular growth pattern [3, 4].
Diagnosis is usually made by excluding other sarcomas,
primarily leiomyosarcoma, liposarcoma and rhabdomyo-
sarcoma. Oda et al. [5] reassessed 428 soft tissue MFH
cases and revised the initial diagnosis in 32.2 %, mostly to
leiomyosarcoma and liposarcoma. Fletcher et al. [6] reas-
sessed 159 pleomorphic sarcomas and in 61 % of the cases,
a sarcoma other than MFH was diagnosed.
Epidemiologically, MFH is one of the most common
primary and secondary soft tissue tumor in adults, with a
peak incidence in the 6th decade [5, 7]. Seventy percent of
these tumors occur in the extremities (49 % lower
extremities vs 19 % upper extremities), followed by trunk
and abdomen or retroperitoneum [7, 8]. Head and neck
location is rare (1–3 %) and carries a more dismal prog-
nosis [7–9]. The inflammatory type is more commonly
encountered in the retroperitoneum [7]. Clinically, tumors
involving extremities, frequently present as a deep seated
(93 %), painless, enlarging mass for months [10]. In con-
trast, patients with retroperitoneal tumors can demonstrate
constitutional symptoms, including anorexia, weight loss,
fever and malaise [7].
On plain X-rays MFH can demonstrate abnormal soft
tissue calcifications (5–20 %) and pressure effect or ero-
sions on the adjacent bone [10]. MRI reveals a lobulated
mass, with intermediate signal on T1 and high on T2 [10].
Heterogenous signal is usually seen on all images. Areas
with tumor necrosis and hemorrhage are commonly found;
sometimes so extensive that the tumor is erroneously
interpreted as soft tissue hematoma [11].
MFH is considered as a malignant tumor with poor
prognosis. We retrospectively report on the management,
complications, local and distal recurrence and survivorship
of 57 patients diagnosed and treated for soft tissue
extremity high-grade MFH.
Materials and methods
After IRB approval, all patients from 1999 to 2005 surgi-
cally treated at our institution, for high-grade extremity soft
tissue primary MFH/undifferentiated pleomorphic sar-
coma, were retrospectively reviewed.
Tumor size was determined by the maximum dimension
measured in the pathology specimens. All patients were
classified according to the 2002 American Joint Committee
in Cancer (AJCC) staging system [12]. Histologic grade
was determined on a three tiered classification scale: low
(G1), intermediate (G2), high grade (G3). G2 and G3
tumors were considered high grade with respect to the
AJCC classification.
Surgical margins were considered positive when tumor
cells were found at the inked margins of the specimens.
WHCs were classified as minor (mWHC) when only
repetitive wound changes resulted in secondary healing and
major (MWHC) when surgical irrigation and debridement
(I&D) or a flap reconstruction were needed. Time to local
recurrence (LR) and metastatic disease (MD) defined as
time interval in months from definite surgical treatment to
detection of recurrent tumor. MD diagnosed within
12 months was characterized as early MD, while diagnosis
after 12 months as late MD. Overall survival (OS) was
estimated as time interval in months from definite surgical
treatment to death.
Patient characteristics
There were 61 patients. Four patients with MFH had pre-
vious history of carcinoma and excluded from oncological
statistical analysis. Thus, 57 patients were studied for
surgical outcome, LR, MD and OS (Table 1). Mean fol-
low-up was 51 months (range 3 months–9 years). Mean
follow-up time for the surviving patients was 60 months,
with a minimum of 30 months. Five patients presented
with pain at the involved anatomic site. One patient pre-
sented with radial nerve palsy due to tumor mass
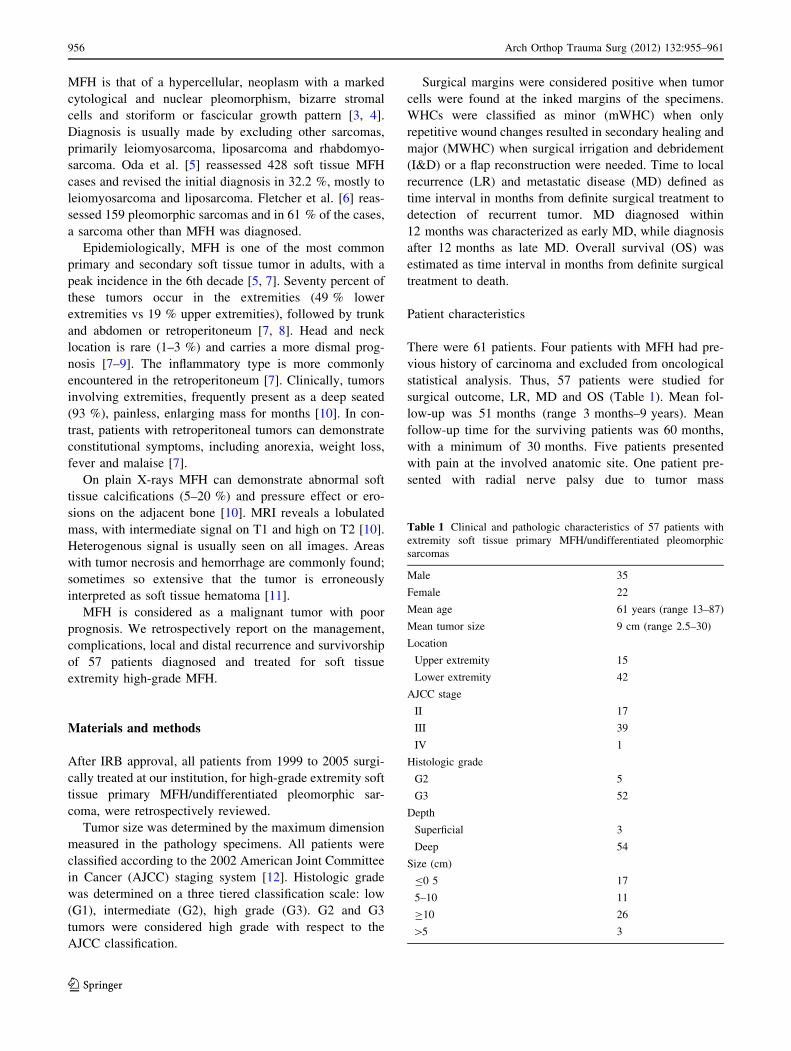
Table 1 Clinical and pathologic characteristics of 57 patients with
extremity soft tissue primary MFH/undifferentiated pleomorphic
sarcomas
Male 35
Female 22
Mean age 61 years (range 13–87)
Mean tumor size 9 cm (range 2.5–30)
Location
Upper extremity 15
Lower extremity 42
AJCC stage
II 17
III 39
IV 1
Histologic grade
G2 5
G3 52
Depth
Superficial 3
Deep 54
Size (cm)
B0 5 17
5–10 11
C10 26
[5 3
956 Arch Orthop Trauma Surg (2012) 132:955–961
123

compression. Twelve out of 61 patients (20 %) were
referred to our department due to incomplete excision of
the tumor by an outside physician. Five of these patients
had initial diagnosis of intramuscular hematoma/abscess,
and were treated with surgical drainage at an outside
institution. Another three patients had undergone unplan-
ned excision without pre-operative adequate imaging.
Surgical Treatment and Adjuvant Therapy modalities
All patients were treated surgically. Fifty-three underwent
limb salvage with tumor excision (Fig. 1). Four patients
(7 %) underwent primary amputation. The 12 patients, who
were referred to our institution due to incomplete initial
excision, all had re-resection of the tumor bed. The mean
time to re-excision was 2 months (range 1–4 months).
Twenty-nine out of 53 patients treated with limb salvage
received pre-operative and 10 post-operative radiation
therapy (RT). RT was offered to all the patients treated
with tumor bed re-resection before definite surgical exci-
sion and was considered as pre-operative for analytic
purposes. Five patients had post-operative chemotherapy.
Statistical analysis
Variables entered into the univariate analysis were gender,
tumor size (B5 vs C10 vs 5–10 cm), age (B50 vs 50–70 vs
C70 years), location (upper vs lower extremity), RT (yes
vs no), (pre-op vs post-op vs no), type of tumor resection
(tumor bed re-resection vs primary tumor resection vs
amputation), type of wound closure (primary wound
closure vs primary reconstructive procedure), WHC (yes vs
no), LR (yes vs no), MD (no vs early MD vs late MD) and
AJCC stage (II vs III vs IV).
Differences in proportions were assessed using
Chi-square test. Multiple logistic regression analysis was
applied to examine the effect of measured variables on
WHC. The effect of independent variables on time to LR,
time to MD and OS was initially examined with the Kap-
lan–Meier method using the log–rank test and factors with
a p value \0.05 were subsequently analyzed for indepen-
dent prognostic significance by the Cox (proportional
hazards) model. The results of the Cox regression analysis
were reported with 95 % confidence intervals (CI). Statis-
tical significance level was in all cases set at p \ 0.05.
Results
Surgical treatment
Negative surgical margins on final pathology report were
achieved in all patients. In one patient treated primarily at
our institution, pathologic examination reported micro-
scopic positive margins and tumor bed resection was
performed. Thus including 12 patients referred with
incomplete resection, 13 patients underwent second surgi-
cal procedure in order to achieve clear margins. Of the 53
patients treated with limb salvage, 30 patients (56 %) had
primary wound closure. The other 23 patients (44 %) had a
primary reconstructive procedure. No major nerve or vessel
had to be reconstructed in the re-resection group, but more
reconstructive procedures were necessary compared to the
primary resection group (46 vs 35 %, p[ 0.05). A total of
3 spilt thickness skin grafts and 27 free or rotational flaps
were performed for primary wound closure, skeletal
reconstruction, MWHC and limb salvage after LR. Flap
congestion due to decreased venous outflow occurred in 2
free flaps. Surgical exploration and venous anastomosis
redo was performed in one case because of thrombosis.
The overall WHC for 53 patients treated with limb
salvage surgery was 28.3 %. The rate for WHC for tumors
Fig. 1 MRI T1 FS with Gadolinium axial image. a Heterogeneous
mass of the volar and radial side of the forearm with peripheral
enhancement. b Closed biopsy was consistent with MFH. The patient
underwent pre-op radiation therapy and 3 weeks later, excision of the
tumor to negative margins
Arch Orthop Trauma Surg (2012) 132:955–961 957
123

\10 vs C10 cm, RT yes vs RT no, primary wound closure
vs primary reconstructive procedure, lower vs upper
extremities and AJCC stage II vs III, was 18 vs 38.5 %,
33.4 % vs 14.3 %, 23.3 % vs 34.8 %, 31 % vs 13.3 % and
11.8 % vs 40 %, respectively. The rate of MWHC was
17 %. All MWHCs were associated with RT, while 50 %
of these were complicated with local infection. 90 % of all
MWHC were involved the lower extremity. However, no
statistically significant factors were revealed.
Local recurrence
LR developed in 11 out of the 57 patients (19.3%) (Fig. 2)
with a mean time of 38 months (SD ± 19.6, range 7–70)
from surgery to detection of recurrence. Two out of the 13
(15.4 %) who underwent tumor bed re-excision demon-
strated LR, and 9 out of the remaining 44 patients (20.5 %)
received initial tumor resection at our institution
(p [ 0.05). No patient with amputation developed LR.
Mean tumor size was 9.7 vs 9.3 cm (p [ 0.05) for patients
with and without LR, respectively. Of the 11 patients, 1
denied any sort of further treatment. The remaining ten
underwent surgical excision of the recurrent tumor and
eight received adjuvant RT. Five out of these 10 patients
(50 %) developed MWHC. Six out of the 10 patients
(60 %) developed second LR treated with new local
resection and 5 of these 10 patients underwent amputation,
either due to LR or MWHC.
Patients with local recurrence were analyzed for gender,
age, tumor size, tumor location, WHC, RT, type of resec-
tion, type of wound closure and AJCC stage. No statisti-
cally significant parameters were detected.
Metastatic disease
Eighteen of the 57 patients (31.5 %) developed MD
(Fig. 3). Seventeen patients were classified as AJCC stage
III and one as IV at initial presentation. All four patients
treated initially with amputation developed metastases.
Mean time to metastases detection after tumor excision was
16.5 months (SD ± 21, range 1–78). The mean tumor size
for patients with metastases was 13 cm vs 7 cm for the
patients without metastases. Patients with a tumor
size C10 cm had a metastatic rate of 58 %, while patients
with tumor size 5–10 cm had a rate of 27 % (p = 0.029).
Ninety-two percent of patients with early lung metastasis
had tumor size [10 cm. Two out of 11 patients with LR
developed metastatic disease. Only 1 out of 13 patients
treated with tumor bed re-excision demonstrated metastasis
(7.7 %), compared to 36.4 % of patients with primary
tumor resection (p [ 0.05). Seventeen patients had
metastases in the lung as the first site of metastatic disease,
while one patient had nodal metastasis then later demon-
strated lung disease. Metastases were managed in 13
patients with a combination of chemotherapy, RT and/or
surgical excision, while 5 did not receive a specific type of
treatment other than symptomatic management. Patients
with metastatic disease were analyzed for gender, age,
tumor size, tumor location, WHC, RT, type of resection,
type of wound closure, LR and AJCC stage. On univariate
analysis, tumor size [5 cm age [50 years, WHC, AJCC
stage III, and primary amputation were statistically sig-
nificant factors for development of MD. Multivariate
analysis of these parameters showed that only tumor
size C5 cm (95 % CI 1.13–1.47; p = 0.000) was a statis-
tically significant factor. For each 1 cm increase in tumor
size, there was 29 % increase in the risk for developing
MD.Fig. 2 Kaplan–Meier local recurrence curve of 57 high-grade
extremity MFH patients
Fig. 3 Kaplan–Meier metastatic disease curve of 57 high-grade
extremity MFH patients
958 Arch Orthop Trauma Surg (2012) 132:955–961
123
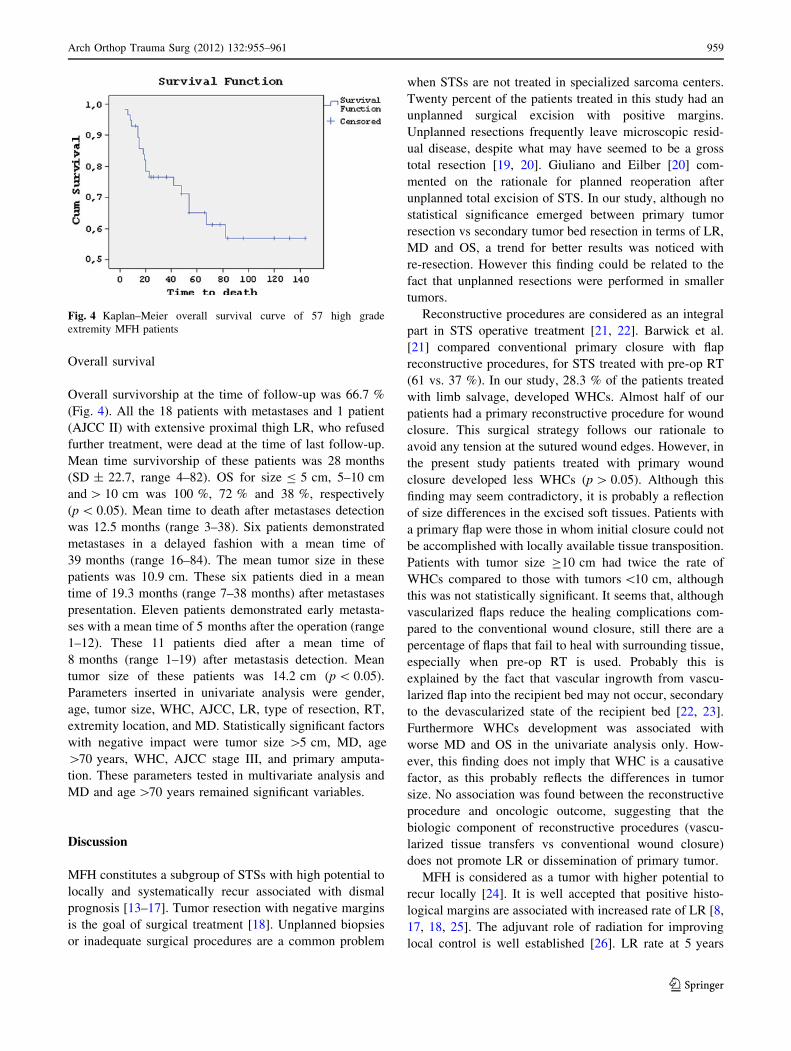
Overall survival
Overall survivorship at the time of follow-up was 66.7 %
(Fig. 4). All the 18 patients with metastases and 1 patient
(AJCC II) with extensive proximal thigh LR, who refused
further treatment, were dead at the time of last follow-up.
Mean time survivorship of these patients was 28 months
(SD ± 22.7, range 4–82). OS for size B 5 cm, 5–10 cm
and [ 10 cm was 100 %, 72 % and 38 %, respectively
(p \ 0.05). Mean time to death after metastases detection
was 12.5 months (range 3–38). Six patients demonstrated
metastases in a delayed fashion with a mean time of
39 months (range 16–84). The mean tumor size in these
patients was 10.9 cm. These six patients died in a mean
time of 19.3 months (range 7–38 months) after metastases
presentation. Eleven patients demonstrated early metasta-
ses with a mean time of 5 months after the operation (range
1–12). These 11 patients died after a mean time of
8 months (range 1–19) after metastasis detection. Mean
tumor size of these patients was 14.2 cm (p \ 0.05).
Parameters inserted in univariate analysis were gender,
age, tumor size, WHC, AJCC, LR, type of resection, RT,
extremity location, and MD. Statistically significant factors
with negative impact were tumor size [5 cm, MD, age
[70 years, WHC, AJCC stage III, and primary amputa-
tion. These parameters tested in multivariate analysis and
MD and age [70 years remained significant variables.
Discussion
MFH constitutes a subgroup of STSs with high potential to
locally and systematically recur associated with dismal
prognosis [13–17]. Tumor resection with negative margins
is the goal of surgical treatment [18]. Unplanned biopsies
or inadequate surgical procedures are a common problem
when STSs are not treated in specialized sarcoma centers.
Twenty percent of the patients treated in this study had an
unplanned surgical excision with positive margins.
Unplanned resections frequently leave microscopic resid-
ual disease, despite what may have seemed to be a gross
total resection [19, 20]. Giuliano and Eilber [20] com-
mented on the rationale for planned reoperation after
unplanned total excision of STS. In our study, although no
statistical significance emerged between primary tumor
resection vs secondary tumor bed resection in terms of LR,
MD and OS, a trend for better results was noticed with
re-resection. However this finding could be related to the
fact that unplanned resections were performed in smaller
tumors.
Reconstructive procedures are considered as an integral
part in STS operative treatment [21, 22]. Barwick et al.
[21] compared conventional primary closure with flap
reconstructive procedures, for STS treated with pre-op RT
(61 vs. 37 %). In our study, 28.3 % of the patients treated
with limb salvage, developed WHCs. Almost half of our
patients had a primary reconstructive procedure for wound
closure. This surgical strategy follows our rationale to
avoid any tension at the sutured wound edges. However, in
the present study patients treated with primary wound
closure developed less WHCs (p [ 0.05). Although this
finding may seem contradictory, it is probably a reflection
of size differences in the excised soft tissues. Patients with
a primary flap were those in whom initial closure could not
be accomplished with locally available tissue transposition.
Patients with tumor size C10 cm had twice the rate of
WHCs compared to those with tumors \10 cm, although
this was not statistically significant. It seems that, although
vascularized flaps reduce the healing complications com-
pared to the conventional wound closure, still there are a
percentage of flaps that fail to heal with surrounding tissue,
especially when pre-op RT is used. Probably this is
explained by the fact that vascular ingrowth from vascu-
larized flap into the recipient bed may not occur, secondary
to the devascularized state of the recipient bed [22, 23].
Furthermore WHCs development was associated with
worse MD and OS in the univariate analysis only. How-
ever, this finding does not imply that WHC is a causative
factor, as this probably reflects the differences in tumor
size. No association was found between the reconstructive
procedure and oncologic outcome, suggesting that the
biologic component of reconstructive procedures (vascu-
larized tissue transfers vs conventional wound closure)
does not promote LR or dissemination of primary tumor.
MFH is considered as a tumor with higher potential to
recur locally [24]. It is well accepted that positive histo-
logical margins are associated with increased rate of LR [8,
17, 18, 25]. The adjuvant role of radiation for improving
local control is well established [26]. LR rate at 5 years
Fig. 4 Kaplan–Meier overall survival curve of 57 high grade
extremity MFH patients
Arch Orthop Trauma Surg (2012) 132:955–961 959
123

follow up was 19.3 %. In the literature, LR rate of MFH
ranges from 19.2 to 44 % [14–17, 27, 28]. Our favorable
results are probably the combined result of negative
resection margins and supplementary RT. When surgical
margins were expected to be close with important struc-
tures, we offered pre-op RT to enhance tumor resectability.
We did not offer RT for primarily treated patients, when a
wide margin could be achieved based on the pre-op MRI
and final pathology confirmed a resection margin of at least
2.5 cm at all directions.
LR is considered a negative prognostic factor for sub-
sequent re-recurrence [16, 29]. Detection of LR is very
challenging. Usually on clinical examination a firm nodule
can be palpated. A MRI in these cases frequently reveals a
heterogenous nodule. A core needle biopsy of the nodule
can facilitate the diagnosis in questionable cases. Although
limb salvage is feasible in over than 90 % of primary STS,
the salvage rate after recurrence drops abruptly [30]. The
decision when to amputate or not, in primary or recurrent
cases, is a balance between tumor resectability, ability for
reconstruction of the resected tissues, and expected com-
plications; and functional outcome, keeping in mind that
these patients frequently need or have already received RT,
are old and may have comorbidities. In our series, while
initial amputation incidence was 7, 60 % of the patients
who developed LR eventually underwent an amputation
either for tumor local control or due to MWHC.
The relation of LR to MD and OS in soft-tissue sarco-
mas is still unclear. Local recurrence can be a result of
inadequate local treatment or a sequel of an aggressive
tumor phenotype [31, 32]. The nature of LR, rather than its
presence per se is a more useful guide to prognosis. In our
study no causal association between LR and MD or OS was
found.
For localized untreated extremity STSs, the two most
important tumor-related prognostic factors regarding MD
and OS are the histologic grade and tumor size [18, 25, 32].
The most important treatment-related factor is surgical
margins [25]. The MD rate in our study was similar to the
reported rate for high grade extremity soft tissue MFH [15,
16, 29]. In multivariate analysis, size emerged as the only
significant factor for the development of MD. It seems that
there is a linear increase in the risk for developing MD as
size of the tumor increases. Additionally, shorter metasta-
sis-free interval was noticed with larger tumor size.
Metastatic disease is closely related to disease-specific
survival. This is clearly seen in our study as all the patients
with MD were not alive at latest follow-up. The OS rate in
our study was 66.7 %, which is identical to survival for
high-grade STSs. In our study, size, age, WHC, AJCC
stage III, and primary amputation were statistically sig-
nificant variables in univariate analysis for both MD and
OS. For OS, the development of MD and time of
development were also significant Salo et al. [16] pointed
out the significance of tumor size as a shorter metastasis
free and disease-specific survival rates were reported with
increasing size category. In their study as in ours, patients
with tumor size[10 cm were in a significantly greater risk
for developing early MD and experienced worse OS. Za-
gars et al. [33] reported that for patients presenting with
metastasis as the first relapse, the time to metastasis was
the major determinant of survival ([12 vs B12 months).
When we performed multivariate analysis for OS, time to
MD and age [70 years remained independent prognostic
factors.
In conclusion, this is a retrospective study of 57 patients
treated for soft tissue high-grade extremity MFH. Complete
tumor excision is the cornerstone of surgical treatment.
Almost half of the patients needed a reconstructive pro-
cedure for wound closure. Patients with tumor size larger
than 10 cm and pre-op RT tend to develop more WHCs.
Tumors with initial incomplete resection undergoing tumor
bed re-resection behaved like tumors with initial negative
margins with respect to LR, MD and OS. Overall prognosis
is poor. Increased tumor size is associated with shorter
metastasis-free interval which significantly decreases
survival.
Conflict of interest The authors declare that they have no conflict
of interest.
References
1. Ozzello L, Stout AP, Murray MR (1963) Cultural characteristics
of malignant histiocytomas and fibrous xanthomas. Cancer
16:331–344
2. O’Brien JE, Stout AP (1964) Malignant fibrous xanthomas.
Cancer 17:1445–1455
3. Fletcher CDM, Unni KK, Mertens F (eds) (2002) World Health
Organization Classification of Tumours. Pathology and Genetics
of Tumours of Soft Tissue and Bone. IARC Press, Lyon
4. Nascimento A, Chandrajit R (2008) Diagnosis and Management
of Pleomorphic Sarcomas (So-Called ‘‘MFH’’) in Adults. J Surg
Oncol 97:330–339
5. Oda Y, Tamiya S, Oshiro Y et al (2002) Reassessment and
clinicopathological prognostic factors of malignant fibrous histi-
ocytoma of soft parts. Pathol Int 52:595–606
6. Fletcher CDM, Gustafson P, Rydholm A, Ville0n H, Akerman M
(2001) Clinicopathologic re-evaluation of 100 malignant fibrous
histiocytomas: prognostic relevance of subclassification. J Clin
Oncol 19:3045–3050
7. Weiss SW, Enzinger FM (1978) Malignant fibrous histiocytoma:
an analysis of 200 cases. Cancer 41:2250–2266
8. Gibbs JF, Huang PP, Lee RJ et al (2001) Malignant fibrous his-
tiocytoma: an institutional review. Cancer Invest 19:23–27
9. Sabesan T, Xuexi Wu, Qi Yongfa, Tang Pingzhang, Ilankovan V
(2006) Malignant fibrous histiocytoma: Outcome of tumours in
the head and neck compared with those in the trunk and
extremities. Brit J Oral Maxillofac Surg 44:209–212
10. Murphey MD, Gross TM, Rosenthal HG (1994) From the
archives of the AFIP, Musculoskeletal malignant fibrous
960 Arch Orthop Trauma Surg (2012) 132:955–961
123
histiocytoma: radiologic–pathologic correlation. Radiographics
14:807–826
11. Kontogeorgakos VA, Martinez S, Dodd L, Brigman B (2010)
Extremity soft tissue sarcomas presented as hematomas. Arch
Orthop Trauma Surg 130:1209–1214
12. American Joint Committee on Cancer (2002) AJCC cancer
staging manual, 6th edn. Springer, New York
13. Geller DS, Hornicek FJ, Mankin HJ, Raskin KA (2007) Soft
tissue sarcoma resection volume associated with wound-healing
complications. Clin Orthop Relat Res 459:182–185
14. Hsu HC, Huang EY, Wang CJ (2004) Treatment Results and
Prognostic Factors in Patients with Malignant Fibrous Histiocy-
toma. Acta Oncol 43:530–535
15. Belal A, Kandil A, Allam A et al (2002) Malignant fibrous his-
tiocytoma: a retrospective study of 109 cases. Am J Clin Oncol
25:16–22
16. Salo JC, Lewis JJ, Woodruff JM, Leung DH, Brennan MF (1999)
Malignant fibrous histiocytoma of the extremity. Cancer
85:1765–1772
17. LeDoussal V, Coindre JM, Leroux A et al (1996) Prognostic
factors for patients with localized primary malignant fibrous
histiocytoma: a multicenter study of 216 patients with multivar-
iate analysis. Cancer 77:1823–1830
18. Zagars GK, Ballo MT, Pisters PWT et al (2003) Prognostic
factors for localized soft tissue sarcoma treated with conservation
surgery and radiation therapy: an analysis of 1,225 patients.
Cancer 97:2530–2543
19. Davis AM, Kandel RA, Wunder JS et al (1997) The impact of
residual disease on local recurrence in patients treated by initial
unplanned resection for soft tissue sarcoma of the extremity.
J Surg Oncol 66:81–87
20. Giuliano AE, Eilber FR (1985) The rationale for planned reop-
eration after unplanned total excision of soft-tissue sarcomas.
J Clin Oncol 3:1344–1348
21. Barwick WJ, Goldberg JA, Scully SP, Harrelson JM (1992)
Vascularized tissue transfer for closure of irradiated wounds after
soft tissue sarcoma resection. Ann Surg 216:591–595
22. Tseng JF, Ballo MT, Langstein HN et al (2006) The effect of
preoperative radiotherapy and reconstructive surgery on wound
complications after resection of extremity soft-tissue sarcomas.
Ann Surg Oncol 13:1209–1215
23. Schultze-Mosgau S, Grabenbauer GG, Radespiel-Troger M,
Wiltfang J, Ries J, Neukam FW, Rodel F (2002) Vascularization
in the transition area between free grafted soft tissues and pre-
irradiated graft bed tissues following preoperative radiotherapy in
the head and neck region. Head Neck 24:42–51
24. Al-Absi E, Farrokhyar F, Sharma R, Whelan K, Corbett T, Patel
M, Ghert M (2010) A systematic review and meta-analysis of
oncologic outcomes of pre- versus postoperative radiation in
localized resectable soft-tissue sarcoma. Ann Surg Oncol
17:1367–1374
25. Stojadinovic A, Leung DH, Allen P, Lewis JJ, Jaques DP,
Brennan MF (2002) Primary adult soft tissue sarcoma: time-
dependent influence of prognostic variables. J Clin Oncol
20:4344–4352
26. Jebsen NL, Trovik CS, Bauer HC et al (2008) Radiotherapy to
improve local control regardless of surgical margin and malig-
nancy grade in extremity and trunk wall soft tissue sarcoma: a
Scandinavian sarcoma group study. Int J Radiat Oncol Biol Phys
71:1196–1203
27. Pritchard DJ, Reiman HM, Turcotte RE, Ilstrup DM (1993)
Malignant fibrous histiocytoma of the soft tissues of the trunk and
extremities. Clin Orthop Relat Res 289:58–65
28. Zagars GK, Mullen JR, Pollack A (1996) Malignant fibrous
histiocytoma: outcome and prognostic factors following conser-
vation surgery and radiotherapy. Int J Radiat Oncol Biol Phys
5:983–994
29. Lehnhardt M, Daigeler A, Homann HH et al (2009) MFH
revisited: outcome after surgical treatment of undifferentiated
pleomorphic or not otherwise specified (NOS) sarcomas of the
extremities - an analysis of 140 patients. Langenbecks Arch Surg.
394:313–320
30. Eilber FC, Brennan MF, Riedel E, Alektiar KM, Antonescu CR,
Singer S (2005) Prognostic factors for survival in patients with
locally recurrent extremity soft tissue sarcomas. Ann Surg Oncol
12:228–236
31. Evans RA (1993) Soft tissue sarcoma: the enigma of local
recurrence. J Surg Oncol 53(2):88–91
32. Ramanathan RC, A’Hern R, Fisher C, Thomas JM (2001) Prog-
nostic index for extremity soft tissue sarcomas with isolated local
recurrence. Ann Surg Oncol 8:278–289
33. Zagars GK, Ballo MT, Pisters PW, Pollock RE, Patel SR, Ben-
jamin RS (2003) Prognostic factors for disease-specific survival
after first relapse of soft-tissue sarcoma: analysis of 402 patients
with disease relapse after initial conservative surgery and radio-
therapy. Int J Radiat Oncol Biol Phys 57:739–747
Arch Orthop Trauma Surg (2012) 132:955–961 961
123