surgical repair of postinfarction ventricular septal defect: 10-year experience
TRANSCRIPT

World J. Surg. 23, 64–67, 1999WORLDJournal of
SURGERY© 1999 by the Societe
Internationale de Chirurgie
Surgical Repair of Postinfarction Ventricular Septal Defect: 10-Year Experience
Kalliopi Athanassiadi, M.D., Ph.D.,1 Efstratios Apostolakis, M.D., Ph.D.,1 Georgios Kalavrouziotis, M.D., Ph.D.,1
Christos Charitos, M.D., Ph.D.,1 Evangelia Karamichali, M.D., Ph.D.,2 Dimitrios Kakavos, M.D., Ph.D.,1
Christos Lolas, M.D., Ph.D.1
1Department of Cardiac Surgery, “Evangelismos” General Hospital, Papagou Ave. 119, 15773 Zografou, Athens, Greece2Department of Anesthesiology, “Evangelismos” General Hospital, Papagou Ave. 119, 15773 Zografou, Athens, Greece
Abstract. Postinfarction ventricular septal defect (PIVSD) remains asurgical challenge resulting in devastating mortality rates. We presentour 10-year experience in surgical management of this catastrophiccomplication of acute myocardial infarction. During a decade (1987–1996) 14 patients with PIVSD were treated surgically in our department.There were 10 men and 4 women, ranging in age from 51 to 78 years. Therupture occurred within the first 4 days after the infarction in most cases(n 5 10). Eight patients were supported perioperatively by intraaorticballoon counterpulsation (IABP). In all cases the surgical techniqueincluded infarctectomy and ventricular septum reconstruction with syn-thetic patches. Coronary artery bypass grafting was synchronously per-formed in four patients. Seven patients died perioperatively (mortalityrate 50%) due to heart failure and to multiple organ failure. The mostfrequent complications were low cardiac output syndrome, hemorrhage,and respiratory and renal insufficiency. The PIVSD needs urgent surgicalintervention with the patient hemodynamically stable after cardiac cath-eterization. Long-term results are favorable for survivors.
Postinfarction ventricular septal defect (PIVSD), first describedby Latham in 1846 [1], occurs in approximately 1% of allmyocardial infarctions (MIs) but accounts for up to 2% of deathssubsequent to MI. When treated nonoperatively, it carries a 65%mortality rate within 2 weeks of perforation and 86% within 2months [2, 3]. Since Cooley et al.’s 1957 report of the firstsuccessful surgical repair of PIVSD, surgical therapy has becomethe treatment of choice [4–6].
The purpose of the present study was to review the clinicaloutcomes of patients with PIVSD treated at “Evangelismos”Hospital from 1987 to 1996. In particular, the presence or absenceof shock, the timing of operation and RV impairment as prog-nostic factors were investigated.
Materials and Methods
Patients
Our series comprises 14 patients operated on early after thedevelopment of PIVSD over the the period of a decade (1987–1996). There were 10 men and 4 women, ranging in age from 51
to 78 years. Their charts were retrospectively reviewed andanalyzed. All but one were in New York Heart Association(NYHA) class III, and most (n 5 12) had a history of hyperten-sion for an average of 10 years prior to the PIVSD. There was ahistory of cigarette smoking in 11 patients, angina in 9, andprevious MI in 5. There were no patients with a history ofcongestive heart failure.
Review of each patient’s electrocardiogram resulted in thediagnosis of anterior or anterolateral MI in half of the cases andinferior MI in the other half. At clinical examination all patientswere noted to have a murmur. In each patient the presence ofVSD was documented by detecting an increase of blood oxygensaturation in the pulmonary artery compared to that of the rightatrium. The diagnosis of PIVSD was confirmed by echocardiog-raphy (Table 1).
All of our patients underwent coronary artery angiography,which revealed one-vessel disease in three, two or three-vesseldisease in four, and three-vessel disease in four. The pulmonaryartery pressure ranged from 18 to 44 mmHg (mean 28 mmHg),the right atrium pressure from 11 to 19 mmHg (mean 15.2mmHg), the end-diastolic pressure of the left ventricle from 14 to28 mmHg (mean 18 mmHg). The rupture occurred within the first4 days after the MI in most cases (n 5 10).
Shock and PIVSD
All patients experienced a mean drop in blood pressure (BP) of10 mmHg when the murmur appeared, and cardiogenic shockdeveloped in 10 patients. Cardiogenic shock was defined as (1)systolic BP , 80 mmHg or mean BP , 60 mmHg, with evidenceof end-organ hypoperfusion (obtundation, decreased urineoutput, elevated creatinine or blood urea nitrogen levels, cooland clammy skin); or (2) requirement for mechanical orpharmacologic interventions to maintain BP and end-organperfusion. Intraaortic balloon counterpulsation (IABP) andpreoperative catecholamine support was used in these 10patients in shock. The rest of the patients needed only inotro-pic support before surgery.
Correspondence to: K. Athanassiadi, M.D., Ph.D., 34A Konstantinoupo-leos Str., 15562 Holargos, Athens, Greece

Operative Technique
In all cases surgical technique included infarctectomy and VSDrepair. The anatomic location of the VSD, confirmed at opera-tion, correlated with the distribution of the infarcted area asindicated in the preoperative electrocardiogram. All operationswere performed with conventional cardiopulmonary bypassthrough a median sternotomy incision using moderate hypother-mia: 25° to 28°C esophageal temperature. Myocardial preserva-tion was achieved with cold crystalloid cardioplegia and topicalhypothermia. The mean ischemia time and the mean cardiopul-monary bypass time was 65 and 144 minutes, respectively (Ta-ble 2).
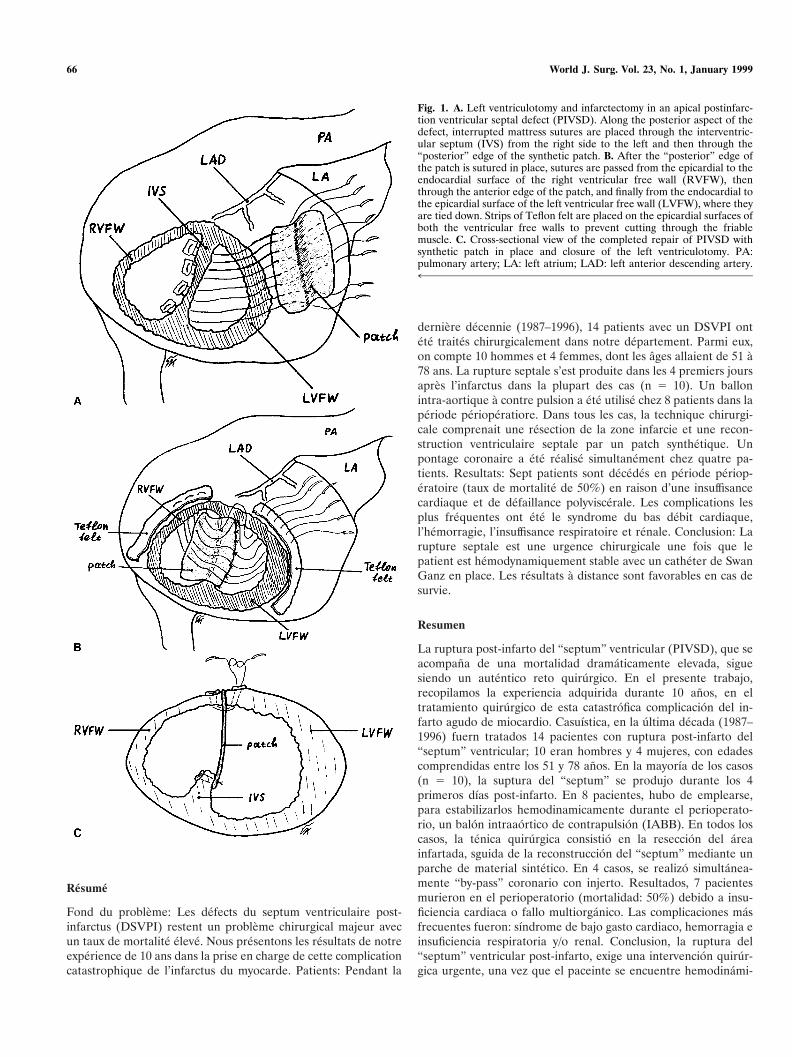
The VSD was approached through a left ventriculotomy, whichwas parallel to and 5 to 10 mm away from either the left anteriordescending artery (LAD) or posterior descending artery, accord-ing to the area of the infarction. The demarcation line betweenhealthy and infarcted myocardium was easy to identify. LargeVSDs required patch closure to avoid tension that could lead tothe disruption of the sutures. A series of pledgeted interruptedmattress sutures were placed along the posterior aspect of the
VSD from the right side of the septum to the left and thenthrough the posterior edge of the synthetic patch (Fig. 1A).Another series of sutures were passed from the epicardial to theendocardial surface of the right ventricular free wall, then throughthe anterior edge of the patch, and finally from the endocardial tothe epicardial surface of the left ventricular free wall, where theywere tied down (Fig. 1B, C). Strips of Teflon felt were placed onthe epicardial surfaces of both ventricular free walls to preventcutting through the friable muscle. Small VSDs were repairedusing interrupted mattress sutures with buttressing strips ofTeflon felt within the interior of the left and right ventricles aswell as on the epicardial surface of each ventricle.
Coronary artery bypass grafting was performed synchronouslyin four patients, using reverse saphenous vein with the proximalanastomoses performed first. Two patients underwent a doublebypass in the LAD 1 OM, and two a single one in the LAD orOM each.
Results
The early mortality was 50%. Causes of death identified were lowcardiac output syndrome (n 5 4), hemorrhage (n 5 1), neurologicdeficit (n 5 1), acute renal failure (n 5 1), and sepsis (n 5 1). Thepostoperative complication rate was high in survivors. Fourpatients experienced low cardiac output syndrome, two respira-tory insufficiency, one hemorrhage, and one acute renal failure.
The mean intensive care unit (ICU) stay was 21 days (range14–92 days). Of the seven late survivors, one died at 4 years of astroke, one at 3 years of lung cancer, and one of multiple organfailure due to pneumonia. Four patients are still alive 1 to 5 yearsafter operation; one is NYHA functional class I, and three areclass II.
Discussion
Rupture of the interventricular septum is a rare complication ofMI. It occurs more often in men than in women. Although theoverall incidence of PIVSD may have slightly decreased duringthe past decade as a result of aggressive pharmacologic therapyfor ischemia in patients with evolving MI [6, 7], the occurrence ofPIVSD remains a challenge to clinical management. Increasingawareness of the bleak outcome of the PIVSD treated medically[3, 6], has led us to the evolution of the modern treatment of thisproblem. Early surgical intervention has been a major determi-nant in the improved outcome of patients with PIVSD [7–9],although an operative mortality between 20% and 48% is stillreported in the literature [9, 10]. There are many preoperativefactors considered to be associated with early mortality andlong-term survival, including the presence of cardiogenic shock,the location of the VSD, the presence of impaired RV function asmanifested by increased right atrial and ventricular pressures, thetime interval between MI, the presence of IABP preoperatively,and finally the extent of coronary artery disease [10–12]. Despiteall the studies in the literature, we have to admit that we still havea long way to go.
It must be stressed that the PIVSD needs urgent surgicalintervention, with the patient hemodynamically stable after car-diac catheterization. Unfortunately, perioperative mortality is stillhigh, but long-term results have been favorable regarding bothsurvival and functional rehabilitation [9–11].
Table 1. Preoperative patient data.
Variable No. of patients
NYHA classificationIII 13IV 1
Cardiogenic shock 10IABP 10Catecholamines 10Systolic BP (mmHg) 70 (45–150)LVEDP (mmHg) 18 (14–28)Mean PAP (mmHg) 28 (18–44)RAP (mmHg) 15.2 (11–19)Qp/Qs 3.8 (2/1–4.9/1)Renal function (BUN in mg/dl) 154 (31–400)Extent of CAD
One-vessel disease 3Two-vessel disease 4Three-vessel disease 4
BP: blood pressure; BUN: blood urea nitrogen; CAD: coronary arterydisease; IABP: intraaortic balloon pump; NYHA: New York HeartAssociation; PAP: pulmonary artery pressure; LVEDP: left ventricleend-diastolic pressure; Qp/Qs: pulmonary/systemic shunt ratio; RAP: rightatrial pressure.
Table 2. Operative variables.
Variable Data
Mean bypass time (min) 144 (28–225)Mean ischemia time (min) 65 (0–99)IABP (no.) 12Inotropic support (no.) 14Infarctectomy (no.) 3Aneurysmectomy (no.) 2Closure of the VSD (no.) 14Positive concomitant CABG (no.) 4
LAD (no.) 1OM (no.) 1LAD 1 OM (no.) 2
CABG: coronary artery bypass graft; LAD: left anterior descendingartery; OM: marginal branch of the circumflex artery; VSD: ventricularseptal defect.
Athanassiadi et al.: Postinfarction VSD 65
Resume
Fond du probleme: Les defects du septum ventriculaire post-infarctus (DSVPI) restent un probleme chirurgical majeur avecun taux de mortalite eleve. Nous presentons les resultats de notreexperience de 10 ans dans la prise en charge de cette complicationcatastrophique de l’infarctus du myocarde. Patients: Pendant la
derniere decennie (1987–1996), 14 patients avec un DSVPI ontete traites chirurgicalement dans notre departement. Parmi eux,on compte 10 hommes et 4 femmes, dont les ages allaient de 51 a78 ans. La rupture septale s’est produite dans les 4 premiers joursapres l’infarctus dans la plupart des cas (n 5 10). Un ballonintra-aortique a contre pulsion a ete utilise chez 8 patients dans laperiode perioperatiore. Dans tous les cas, la technique chirurgi-cale comprenait une resection de la zone infarcie et une recon-struction ventriculaire septale par un patch synthetique. Unpontage coronaire a ete realise simultanement chez quatre pa-tients. Resultats: Sept patients sont decedes en periode periop-eratoire (taux de mortalite de 50%) en raison d’une insuffisancecardiaque et de defaillance polyviscerale. Les complications lesplus frequentes ont ete le syndrome du bas debit cardiaque,l’hemorragie, l’insuffisance respiratoire et renale. Conclusion: Larupture septale est une urgence chirurgicale une fois que lepatient est hemodynamiquement stable avec un catheter de SwanGanz en place. Les resultats a distance sont favorables en cas desurvie.
Resumen
La ruptura post-infarto del “septum” ventricular (PIVSD), que seacompana de una mortalidad dramaticamente elevada, siguesiendo un autentico reto quirurgico. En el presente trabajo,recopilamos la experiencia adquirida durante 10 anos, en eltratamiento quirurgico de esta catastrofica complicacion del in-farto agudo de miocardio. Casuıstica, en la ultima decada (1987–1996) fuern tratados 14 pacientes con ruptura post-infarto del“septum” ventricular; 10 eran hombres y 4 mujeres, con edadescomprendidas entre los 51 y 78 anos. En la mayorıa de los casos(n 5 10), la suptura del “septum” se produjo durante los 4primeros dıas post-infarto. En 8 pacientes, hubo de emplearse,para estabilizarlos hemodinamicamente durante el perioperato-rio, un balon intraaortico de contrapulsion (IABB). En todos loscasos, la tenica quirurgica consistio en la reseccion del areainfartada, sguida de la reconstruccion del “septum” mediante unparche de material sintetico. En 4 casos, se realizo simultanea-mente “by-pass” coronario con injerto. Resultados, 7 pacientesmurieron en el perioperatorio (mortalidad: 50%) debido a insu-ficiencia cardiaca o fallo multiorganico. Las complicaciones masfrecuentes fueron: sındrome de bajo gasto cardiaco, hemorragia einsuficiencia respiratoria y/o renal. Conclusion, la ruptura del“septum” ventricular post-infarto, exige una intervencion quirur-gica urgente, una vez que el paceinte se encuentre hemodinami-
Fig. 1. A. Left ventriculotomy and infarctectomy in an apical postinfarc-tion ventricular septal defect (PIVSD). Along the posterior aspect of thedefect, interrupted mattress sutures are placed through the interventric-ular septum (IVS) from the right side to the left and then through the“posterior” edge of the synthetic patch. B. After the “posterior” edge ofthe patch is sutured in place, sutures are passed from the epicardial to theendocardial surface of the right ventricular free wall (RVFW), thenthrough the anterior edge of the patch, and finally from the endocardial tothe epicardial surface of the left ventricular free wall (LVFW), where theyare tied down. Strips of Teflon felt are placed on the epicardial surfaces ofboth the ventricular free walls to prevent cutting through the friablemuscle. C. Cross-sectional view of the completed repair of PIVSD withsynthetic patch in place and closure of the left ventriculotomy. PA:pulmonary artery; LA: left atrium; LAD: left anterior descending artery.4™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™
66 World J. Surg. Vol. 23, No. 1, January 1999

camente estable y se haya realizado una cateterizacion cardiaca.Los resultados tardıos, para los supervivientes, son buenos.
References
1. Latham, P.M.: Lectures on Subjects Connected with Clinical Medi-cine, Comprising Diseases of the Heart (Vol. 2). London, Longman,Brown, Green and Longmans, 1846, pp. 168–176
2. Oyamada, A., Queen, F.B.: Spontaneous rupture of the interventric-ular septum following acute myocardial infarction with some clinico-pathological observation on survival in 5 cases. Presented at thePan-Pacific Pathology Congress, Tripler US Army Hospital, Hono-lulu, HI, Oct. 12, 1961. Cited in: Murphy, T.E., DeBoer, A.: Surgicalmanagement of ventricular septal defects following myocardial infarc-tion. In Surgery for the Complications of Myocardial Infarction, J.M.Moran, L.L. Michaelis, editors. Orlando, FL, Grune & Stratton, 1980,pp. 191–210
3. Sanders, R.J., Kern, W.H., Blount, S.G.: Perforation of the interven-tricular septum complicating myocardial infarction. J. Thorac. Cardio-vasc. Surg. 61:186, 1971
4. Cooley, D.A., Belmonte, B.A., Zeis, L.B., Schnur, S.: Surgical repairof ruptured interventricular septum following acute myocardial infarc-tion. Surgery 41:930, 1957
5. Daggett, W.M.: Postinfarction ventricular septal defect repair: retro-spective thoughts and historical perspectives. Ann. Thorac. Surg.50:1006, 1990
6. Von Segesser, L., Bauer, F., Laske, A., Jenni, R., Turina, M.: DerVentrikelseptumdefekt nach Myokardinfarkt. Schweiz. Med.Wochenschr. 119:1421, 1989
7. Kitamura, S., Mendez, A., Kay, J.H.: Ventricular septal defect follow-ing myocardial infarction. J. Thorac. Cardiovasc. Surg. 85:191, 1983
8. Skillington, P.D., Davis, R.H., Luff, A.J.: Surgical treatment forinfarct-related ventricular septal defects: improved early results com-bined with analysis of late functional status. J. Thorac. Cardiovasc.Surg. 99:798, 1990
9. Jones, M.T., Schofield, P.M., Bray, C.L.: Surgical repair of acquiredventricular septal defect: determinants of early and late outcome.J. Thorac. Cardiovasc. Surg. 93:680, 1987
10. Muehrcke, D.D., Daggett, W.M., Buckley, M.J., Akins, C.W., Hilgen-berg, A.D., AUsten, G.: Postinfarct ventricular septal defect repair:effect of coronary artery bypass grafting. Ann. Thorac. Surg. 54:876,1992
11. Blache, C., Khan, S.S., Chaux, A., Matloff, J.M.: Postinfarctionventricular septal defect in the elderly: analysis and results. Ann.Thorac. Surg. 57:1244, 1994
12. Hill, J.D., Stiles, Q.R.: Acute ventricular septal defect. Circulation79(Suppl. I):1112, 1989
Athanassiadi et al.: Postinfarction VSD 67