surgery versus conservative treatment for symptomatic...
TRANSCRIPT

Spine www.spinejournal.com E1335
LITERATURE REVIEW
SPINE Volume 36, Number 20, pp E1335–E1351©2011, Lippincott Williams & Wilkins
Surgery Versus Conservative Treatment for Symptomatic Lumbar Spinal Stenosis
A Systematic Review of Randomized Controlled Trials
Francisco M. Kovacs , MD, PhD , * � Gerard Urrútia , MD , † ‡ § � and José Domingo Alarcón , MD ¶ �
Study Design. Systematic review. Objective. To compare the effectiveness of surgery versus conservative treatment on pain, disability, and loss of quality of life caused by symptomatic lumbar spinal stenosis (LSS). Summary of Background Data. LSS is the most common reason for spine surgery in persons older than 65 years in the United States. Methods. Randomized controlled trials (RCTs) comparing any form of conservative and surgical treatment were searched in CENTRAL, MEDLINE, EMBASE, and TripDatabase databases until July 2009, with no language restrictions. Additional data were requested from the authors of the original studies. The methodological quality of each study was assessed independently by two reviewers, following the criteria recommended by the Cochrane Back Review Group. Only data from randomized cohorts were extracted. Results. A total of 739 citations were reviewed. Eleven publications corresponding to fi ve RCTs were included. All fi ve scored as high quality despite concerns deriving from heterogeneity of treatment, lack of blinding, and potential differences in the size of the placebo effect across groups. They included a total of 918 patients in whom
Lumbar spinal stenosis is defi ned as the reduction of the surface area of the lumbar spinal canal. It is usu-ally caused by spinal degenerative conditions 1 – 5 and is
commonly found to be asymptomatic. 1 – 9 However, symptoms may appear as a result of neurovascular mechanisms (such as reduced arterial fl ow in cauda equina, venous congestion, and increased epidural pressure), 10 – 13 nerve root excitation by local infl ammation, or direct compression in the central canal or the lateral recess. 14
These mechanisms can concur. As a result, symptoms attributed to lumbar spinal stenosis are diverse and include radicular pain down to the leg, numbness, and/or weakness. Because lumbar fl exion increases the available space in the lumbar spinal canal, 1 , 15 the most typical clinical feature is neu-rogenic claudication (pain in the buttocks or legs when walk-ing, which disappears with sitting or lumbar fl exion). How-ever, radicular symptoms, which do not improve in fl exion, can also be attributed to spinal stenosis at the correspond-ing level, and no clinical feature or diagnostic test is a valid diagnostic “gold standard” for concluding that spinal stenosis is the cause of pain in a given patient. 16 Nevertheless, spinal
Form the * Departamento Científi co, Fundación Kovacs, Palma de Mallorca, Spain ; † Iberoamerican Cochrane Center-Servei d’Epidemiologia Clínica i Salut Pública, Institut d’Investigació Biomèdica Sant Pau, Barcelona, Spain ; ‡ CIBER Epidemiología y Salud Pública, Barcelona, Spain ; § Public Health and Research Methodology Programme, Universitat Autonoma de Barcelona, Barcelona, Spain ; ¶ Iberoamerican Cochrane Network, Universidad Surcolombiana, Neiva, Colombia ; and � Red Española de Investigadores en Dolencias de la Espalda, Paseo Mallorca 36, 07012 Palma de Mallorca, Spain .
Acknowledgement date: June 1, 2010. First Revision date: August 16, 2010. Second Revision date: October 12, 2010. Third Revision date: November 17, 2010. Acceptance date: November 18, 2010.
The device(s)/drug(s) is/are FDA-approved or approved by corresponding national agency for this indication.
Foundation and Governmental funds were received in support of this work. No benefi ts in any form have been or will be received from a commercial party related directly or indirectly to the subject of this manuscript.
Gerard Urrutia and José Domingo Alarcón retrieved and independently assessed the references identifi ed through the electronic search. They also independently assessed the methodologic quality of each article and performed data extraction. Francisco M. Kovacs participated with these two authors in solving by consensus any disagreements in quality assessment and data extraction that arose, and also wrote this manuscript. He reports that he had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Address correspondence and reprint requests to Francisco M. Kovacs, MD, PhD, Departamento Científi co, Fundación Kovacs, Paseo Mallorca 36, 3º, 1a, 07012 Palma de Mallorca, Spain; E-mail: [email protected]
conservative treatments had failed for 3 to 6 months, and included orthosis, rehabilitation, physical therapy, exercise, heat and cold, transcutaneous electrical nerve stimulation, ultrasounds, analgesics, nonsteroidal anti-infl ammatory drugs, and epidural steroids. Surgical treatments included the implantation of a specifi c type of interspinous device and decompressive surgery (with and without fusion, instrumented or not). In all the studies, surgery showed better results for pain, disability, and quality of life, although not for walking ability. Results of surgery were similar among patients with and without spondylolisthesis, and slightly better among those with neurogenic claudication than among those without it. The advantage of surgery was noticeable at 3 to 6 months and remained for up to 2 to 4 years, although at the end of that period differences tended to be smaller. Conclusion. In patients with symptomatic LSS, the implantation of a specifi c type of device or decompressive surgery, with or without fusion, is more effective than continued conservative treatment when the latter has failed for 3 to 6 months. Key words: lumbar spinal stenosis , systematic review , randomized controlled trial , surgery , conservative treatment . Spine 2011 ; 36 : E1335 – E1351
DOI: 10.1097/BRS.0b013e31820c97b1
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
BRS204382.indd E1335BRS204382.indd E1335 25/08/11 11:51 PM25/08/11 11:51 PM

E1336 www.spinejournal.com September 2011
LITERATURE REVIEW Surgery Versus Conservative Treatment • Kovacs et al
stenosis is the most common reason for lumbar spine surgery in persons older than 65 years in the United States. 17 , 18
When conservative treatments fail for 3 to 6 months, decompressive surgery is usually considered. The most recent Cochrane review concluded that there was only heteroge-neous and limited evidence on its effectiveness, but it was issued in 2005. 19
Therefore, the objectives of this study were to: (1) system-atically review the evidence on the effectiveness and safety of any form of surgery versus conservative treatment for symptomatic lumbar spinal stenosis, and (2) explore whether available data made it possible to refi ne indication criteria for either type of treatment, on the basis of the existence of spon-dylolisthesis or neurogenic claudication.
MATERIALS AND METHODS
Search and Study Selection An electronic search was performed in CENTRAL (Cochrane library 2009, issue 2), MEDLINE (January 1966–July 2009), EMBASE (January 1980–July 2009), and on the Inter-net through TripDatabase (only for reviews and technical reports). The terms “spinal stenosis,” “lumbar stenosis,” “claudication,” “spinal stenos,” “surgery or surgical,” and “low back pain, lumbago, back pain or backache” were com-bined with the highly sensitive search strategy to identify ran-domized controlled trials (RCTs) developed by the Cochrane Collaboration. 20
Studies were included in this review if they were RCTs pro-viding data on the comparison of the effectiveness or safety of any surgical procedure with any form of conservative treat-ment in patients with neurogenic claudication or sciatica, and lumbar spinal stenosis that had been confi rmed by imaging. No language restriction was applied.
References identifi ed were retrieved and assessed indepen-dently by two authors (G.U. and J.D.A.) to check for inclu-sion criteria. Disagreements were solved by consensus with the third author (F.M.K.).
For studies that included randomized and nonrandomized cohorts, this review considered data only from the random-ized cohort to compare the effectiveness of surgical and con-servative treatments, although adverse events from all patients were gathered. Separate data were also requested from the authors with regard to patients with and without spondylolis-thesis, and neurogenic claudication.
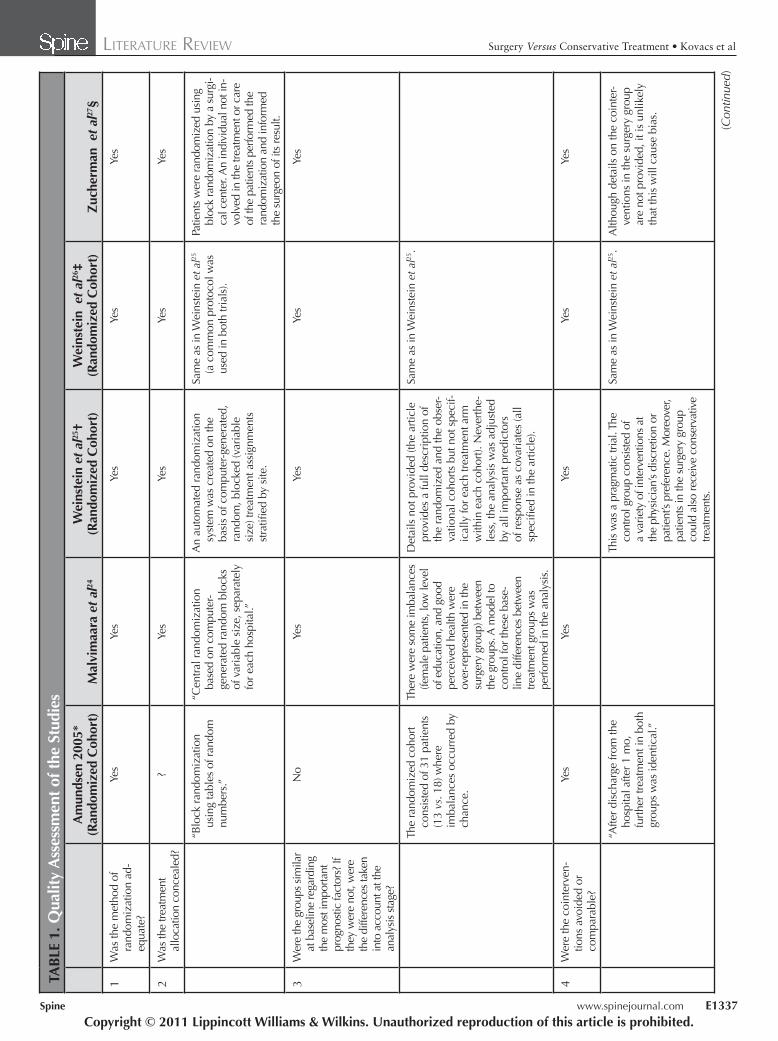
Quality Assessment and Data Analysis Methodological quality of each study was independently assessed by two of the three reviewers (G.U., J.D.A., and F.M.K.), following the criteria recommended by the Cochrane Back Review Group. 21 , 22 Criteria on blindness of patients and therapists were disregarded because they were not appli-cable when comparing surgery with conservative treatment ( Table 1 ). Therefore, the maximum possible score was 9 points and a study was considered as being of “high quality” if it scored 5 points or more.
Data extraction was independently undertaken (G.U. and J.D.A.). Disagreements in quality assessment and data extrac-tion were solved by consensus (G.U., J.D.A., and F.M.K.). Despite what was planned at the design phase, neither a quan-titative synthesis of data nor a sensitivity analysis was possible because of the variability of outcome measures and the het-erogeneity of the methods used across the studies ( Table 2 ). Therefore, a qualitative analysis of data was performed on the basis of the methodological quality of included trials and the consistency of their fi ndings.
RESULTS The electronic search identifi ed 739 references. A total of30 publications, corresponding to 17 studies were identi-fi ed as eligible. Ten publications (nine studies) were excluded because they did not focus on spinal stenosis, 28 – 37 eight publi-cations (two studies) because they were not randomized, 38 – 45 and one publication because it mixed patients who had and had not been randomized, and the authors were not able to provide their data separately. 46
The remaining 11 publications (fi ve studies) were included in this review. 23 – 27 , 47 – 52 For the purpose of this review, individ-ual studies are identifi ed by using the fi rst publications report-ing primary clinical endpoints. 23 – 26 , 50 Three of these studies included data from both observational and randomized cohorts, 23 , 25 , 26 but they were included because the authors provided separate data for those patients in the randomized cohorts. 25 , 26
All studies scored as being of high quality, although the sample size of one of them was very small. 23 Most outcomes were self-reported by the patients and blinding of care provid-ers and patients was not feasible. Hence, outcome assessment was not blinded ( Table 1 ).
The mean age of patients included in the studies ranged between 62 and 70 years. Imaging had documented spinal ste-nosis in all the participants. One study included only patients with spondylolisthesis, 25 one included only patients without spondylolisthesis, 26 one included only patients with spondy-lolisthesis of grade I and lesser, 50 and the other two included patients both with and without spondylolisthesis. 23 , 24 When contacted, the authors from the two latter studies were unable to provide separate data for patients with and without this radiological fi nding ( Table 2 ).
One study included only patients with neurogenic claudica-tion, 50 whereas the other four included patients with pain radi-ating down to the leg, both with and without neurogenic clau-dication. 23 – 26 The authors from two of these studies were able to provide separate data for patients with and without neu-rogenic claudication. 25 , 26 Most patients included in the other two studies reported neurogenic claudication, 23 , 24 although separate data on their evolution were not available ( Table 2 ).
Four studies assessed the effectiveness of decompressive surgery (laminectomy, medial facetectomy, discectomy, and/or removal of osteophytes and hypertrophic ligament fl ava) with or without instrumented or noninstrumented fusion. 23 – 26 The fi fth study assessed the effectiveness of a specifi c type of interspinous implant. 50 The latter was the only study funded
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
BRS204382.indd E1336BRS204382.indd E1336 25/08/11 11:51 PM25/08/11 11:51 PM
Spine www.spinejournal.com E1337
LITERATURE REVIEW Surgery Versus Conservative Treatment • Kovacs et al TA
BLE
1. Q
ualit
y A
sses
smen
t of t
he S
tudi
es
Am
unds
en 2
005*
(R
ando
miz
ed C
ohor
t)M
alvi
maa
ra e
t al
24
Wei
nste
in e
t al 25
†(R
ando
miz
ed C
ohor
t)W
eins
tein
et a
l 26 ‡
(Ran
dom
ized
Coh
ort)
Zuc
herm
an e
t al 27
§
1W
as th
e m
etho
d of
ra
ndom
izat
ion
ad-
equa
te?
Yes
Yes
Yes
Yes
Yes
2W
as th
e tre
atm
ent
allo
catio
n co
ncea
led?
?Ye
sYe
sYe
sYe
s
“Blo
ck ra
ndom
izat
ion
usin
g ta
bles
of r
ando
m
num
bers
.”
“Cen
tral r
ando
miz
atio
n ba
sed
on c
ompu
ter-
gene
rate
d ra
ndom
blo
cks
of v
aria
ble
size
, sep
arat
ely
for e
ach
hosp
ital.”
An
auto
mat
ed ra
ndom
izat
ion
syst
em w
as c
reat
ed o
n th
e ba
sis
of c
ompu
ter-g
ener
ated
, ra
ndom
, blo
cked
(var
iabl
e si
ze) t
reat
men
t ass
ignm
ents
st
ratifi
ed
by s
ite.
Sam
e as
in W
eins
tein
et a
l 25
(a c
omm
on p
roto
col w
as
used
in b
oth
trial
s).
Patie
nts
wer
e ra
ndom
ized
usi
ng
bloc
k ra
ndom
izat
ion
by a
sur
gi-
cal c
ente
r. A
n in
divi
dual
not
in-
volv
ed in
the
treat
men
t or c
are
of th
e pa
tient
s pe
rform
ed th
e ra
ndom
izat
ion
and
info
rmed
th
e su
rgeo
n of
its
resu
lt.
3W
ere
the
grou
ps s
imila
r at
bas
elin
e re
gard
ing
the
mos
t im
porta
nt
prog
nost
ic fa
ctor
s? If
th
ey w
ere
not,
wer
e th
e di
ffere
nces
take
n in
to a
ccou
nt a
t the
an
alys
is s
tage
?
No
Yes
Yes
Yes
Yes
The
rand
omiz
ed c
ohor
t co
nsis
ted
of 3
1 pa
tient
s (1
3 vs
. 18)
whe
re
imba
lanc
es o
ccur
red
by
chan
ce.
Ther
e w
ere
som
e im
bala
nces
(fe
mal
e pa
tient
s, lo
w le
vel
of e
duca
tion,
and
goo
d pe
rcei
ved
heal
th w
ere
over
-rep
rese
nted
in th
e su
rger
y gr
oup)
bet
wee
n th
e gr
oups
. A m
odel
to
cont
rol f
or th
ese
base
-lin
e di
ffere
nces
bet
wee
n tre
atm
ent g
roup
s w
as
perfo
rmed
in th
e an
alys
is.
Det
ails
not
pro
vide
d (th
e ar
ticle
pr
ovid
es a
full
desc
riptio
n of
th
e ra
ndom
ized
and
the
obse
r-va
tiona
l coh
orts
but
not
spe
cif-
ical
ly fo
r eac
h tre
atm
ent a
rm
with
in e
ach
coho
rt). N
ever
the-
less
, the
ana
lysi
s w
as a
djus
ted
by a
ll im
porta
nt p
redi
ctor
s of
resp
onse
as
cova
riate
s (a
ll sp
ecifi
ed in
the
artic
le).
Sam
e as
in W
eins
tein
et a
l 25 .
4W
ere
the
coin
terv
en-
tions
avo
ided
or
com
para
ble?
Yes
Yes
Yes
Yes
Yes
“Afte
r dis
char
ge fr
om th
e ho
spita
l afte
r 1 m
o,
furth
er tr
eatm
ent i
n bo
th
grou
ps w
as id
entic
al.”
This
was
a p
ragm
atic
tria
l. Th
e co
ntro
l gro
up c
onsi
sted
of
a va
riety
of i
nter
vent
ions
at
the
phys
icia
n’s
disc
retio
n or
pa
tient
’s pr
efer
ence
. Mor
eove
r, pa
tient
s in
the
surg
ery
grou
p co
uld
also
rece
ive
cons
erva
tive
treat
men
ts.
Sam
e as
in W
eins
tein
et a
l 25 .
Alth
ough
det
ails
on
the
coin
ter-
vent
ions
in th
e su
rger
y gr
oup
are
not p
rovi
ded,
it is
unl
ikel
y th
at th
is w
ill c
ause
bia
s.
(Con
tinue
d)
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
BRS204382.indd E1337BRS204382.indd E1337 25/08/11 11:51 PM25/08/11 11:51 PM

E1338 www.spinejournal.com September 2011
LITERATURE REVIEW Surgery Versus Conservative Treatment • Kovacs et al TA
BLE
1.
(Con
tinue
d)
Am
unds
en 2
005*
(R
ando
miz
ed C
ohor
t)M
alvi
maa
ra e
t al 24
W
eins
tein
et a
l 25 †
(Ran
dom
ized
Coh
ort)
Wei
nste
in e
t al 26
‡(R
ando
miz
ed C
ohor
t)Z
uche
rman
et a
l 27 §
5W
as th
e co
mpl
ianc
e ra
te a
ccep
tabl
e in
all
grou
ps?
Yes
Yes
Yes
Yes
Yes
Of t
he 1
8 pa
tient
s w
ho
wer
e ra
ndom
ized
into
th
e co
ntro
l gro
up,
10 p
atie
nts
cros
sed
over
to
the
surg
ery
grou
p.
Of t
he 5
0 pa
tient
s w
ho w
ere
rand
omiz
ed in
to th
e su
rgi-
cal g
roup
, 4 p
atie
nts
wer
e no
t sub
ject
ed to
sur
gery
w
hile
4 o
f the
44 p
atie
nts
rand
omiz
ed
into
the
no-s
urge
ry g
roup
w
ere
oper
ated
upo
n du
r-in
g th
e 2-
yr fo
llow
-up.
Com
plia
nce
with
ass
igne
d tre
at-
men
t was
low
and
a s
ignifi -
cant
pro
porti
on o
f pat
ient
s in
bo
th g
roup
s cr
osse
d ov
er to
th
e tre
atm
ent a
ssig
ned
for t
he
othe
r gro
up. H
owev
er, r
esul
ts
wer
e an
alyz
ed a
ccor
ding
to
the
“int
entio
n to
trea
t” p
rin-
cipl
e; s
o, th
is w
as u
nlik
ely
to
caus
e bi
as.
Sam
e as
in W
eins
tein
et a
l 25 .
6W
as th
e ca
re p
rovi
der
blin
ded?
Not
app
licab
leN
ot a
pplic
able
Not
app
licab
leN
ot a
pplic
able
Not
app
licab
le
7W
as th
e pa
tient
bl
inde
d?N
ot a
pplic
able
Not
app
licab
leN
ot a
pplic
able
Not
app
licab
leN
ot a
pplic
able
Was
the
outc
ome
as-
sess
or b
linde
d??
?N
oN
oN
o
8A
ll pa
tient
s w
ere
seen
by
the
sam
e ph
ysic
ian
(not
a s
urge
on).
Furth
er
deta
ils n
ot p
rovi
ded.
Not
des
crib
ed.
Mos
t out
com
es c
onsi
sted
of
patie
nt-r
epor
ted
outc
omes
.Sa
me
as in
Wei
nste
in e
t al 25
.M
ost o
utco
mes
con
sist
ed o
f pa
tient
-rep
orte
d ou
tcom
es.
9W
as th
e w
ithdr
awal
/dr
opou
t rat
e un
likel
y to
cau
se b
ias?
Yes
Yes
Yes
Yes
?
Cas
es o
f 1 p
atie
nt a
s-si
gned
to s
urge
ry a
nd
1 pa
tient
ass
igne
d to
th
e co
ntro
l gro
up w
ere
lost
to fo
llow
-up
at 4
yr
beca
use
of d
eath
. At
10 y
r, ca
ses
of 2
pat
ient
s an
d 1
patie
nt, f
rom
the
resp
ectiv
e gr
oups
, wer
e lo
st to
follo
w-u
p fo
r the
sa
me
reas
on.
Ther
e w
ere
3 pa
tient
s in
the
surg
ery
grou
p an
d4
in th
e no
-sur
gery
gro
up,
the
case
s of
who
m w
ere
lost
to fo
llow
-up
(reas
ons
prov
ided
).
In e
ach
grou
p, 1
7% o
f the
pa
tient
s w
ere
not a
vaila
ble
at
the
last
vis
it (2
yr)
for s
imila
r re
ason
s. M
oreo
ver,
the
high
ra
te o
f cro
ssov
ers
(42%
ove
r-al
l) m
ight
cre
ate
a bi
as to
war
d th
e nu
ll hy
poth
esis
.
In e
ach
grou
p, 2
2% a
nd
25%
of t
he p
atie
nts
wer
e no
t ava
ilabl
e at
the
last
vi
sit (
2 yr
) for
sim
ilar
reas
ons.
Mor
eove
r, th
e hi
gh ra
te o
f cro
ssov
ers
(38%
ove
rall)
mig
ht c
reat
e a
bias
tow
ard
the
null
hypo
thes
is.
Out
of 1
00, 9
pat
ient
s as
sign
ed
to c
ontro
l gro
up w
ithdr
ew
from
the
stud
y be
fore
rece
ivin
g th
eir i
nitia
l epi
dura
l inj
ectio
n as
they
ent
ered
the
stud
y ho
ping
to b
e ra
ndom
ized
to
surg
ery.
Mor
eove
r, at
2-y
r fo
llow
-up
of th
e ca
se, 7
pa
tient
s in
the
surg
ery
grou
p an
d 10
add
ition
al p
atie
nts
in
the
cont
rol g
roup
wer
e no
t av
aila
ble
for a
naly
sis.
Thi
s co
uld
even
tual
ly b
ias
resu
lts
agai
nst s
urge
ry.
(Con
tinue
d)
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
BRS204382.indd E1338BRS204382.indd E1338 25/08/11 11:51 PM25/08/11 11:51 PM

Spine www.spinejournal.com E1339
LITERATURE REVIEW Surgery Versus Conservative Treatment • Kovacs et al
TAB
LE 1
. (C
ontin
ued)
A
mun
dsen
200
5*
(Ran
dom
ized
Coh
ort)
Mal
vim
aara
et a
l 24
Wei
nste
in e
t al 25
†(R
ando
miz
ed C
ohor
t)W
eins
tein
et a
l 26 ‡
(Ran
dom
ized
Coh
ort)
Zuc
herm
an e
t al 27
§
10W
as th
e tim
ing
of th
e ou
tcom
e as
sess
men
t in
bot
h gr
oups
com
-pa
rabl
e?
Yes
Yes
Yes
Yes
Yes
Det
ails
not
pro
vide
d bu
t re
leva
nt d
iffer
ence
s ar
e un
likel
y to
be.
11W
as a
n an
alys
is b
y in
tent
ion
to tr
eat
perfo
rmed
?
Yes
Yes
Yes
Yes
No
Ther
e w
ere
10 p
atie
nts
who
cro
ssed
ove
r fro
m
cont
rol g
roup
to s
urge
ry
grou
p, fo
rmin
g a
new
gr
oup
desi
gnat
ed a
s gr
oup
RC
+ . T
hese
wer
e re
cord
ed a
s tre
atm
ent
failu
res
in th
eir o
rigin
al
grou
p on
the
basi
s of
IT
T an
alys
is d
urin
g th
e fi r
st 4
yr.
All
patie
nts
wer
e an
alyz
ed
in th
eir o
rigin
al g
roup
re
gard
less
of t
he a
ctua
l tre
atm
ent r
ecei
ved.
Dro
p-ou
ts d
urin
g ca
se fo
llow
-up
wer
e as
sum
ed to
be
negl
igib
le.
The
prim
ary
anal
ysis
was
pe
rform
ed a
ccor
ding
to th
e “i
nten
tion
to tr
eat”
prin
cipl
e.
In a
dditi
on, a
n “a
s tre
ated
” an
alys
is (a
djus
ted
for p
oten
tial
conf
ound
ing
fact
ors)
was
als
o pe
rform
ed to
stu
dy th
e po
ten-
tial e
ffect
s of
cro
ssov
ers.
Sam
e as
in W
eins
tein
et a
l 25 .
Out
com
es fr
om p
atie
nts
who
w
ithdr
ew fr
om th
e st
udy
(7 in
th
e su
rger
y gr
oup
and
19 in
th
e co
ntro
l gro
up) w
ere
not
incl
uded
in th
e re
sults
.
5/9
8/9
8/9
8/9
6/9
Stud
ies
with
mul
tiple
rel
ated
pub
licat
ions
:
* Am
unds
en e
t al 47
and
Am
unds
en e
t al 23
.
† Birk
mey
er e
t al 48
and
Wei
nste
in e
t al 25
.
‡ Birk
mey
er e
t al 48
, Wei
nste
in e
t al 26
, and
Wei
nste
in e
t al 49
.
§ Zuc
herm
an e
t al 50
, Zuc
herm
an e
t al 27
, Hsu
et a
l 51 , a
nd A
nder
son
et a
l 52 .
ITT
indi
cate
s “i
nten
tion
to tr
eat’’
; R
C, r
ando
miz
ed c
ohor
t.
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
BRS204382.indd E1339BRS204382.indd E1339 25/08/11 11:51 PM25/08/11 11:51 PM

E1340 www.spinejournal.com September 2011
LITERATURE REVIEW Surgery Versus Conservative Treatment • Kovacs et al TA
BLE
2. C
hara
cter
istic
s of
the
Incl
uded
Stu
dies
Stud
yPa
tient
sSu
rgic
al P
roce
dure
Con
serv
ativ
e Tr
eatm
ent
Follo
w-u
pLo
sses
to
Follo
w-u
p
Am
unds
en e
t al 23
(Ran
dom
ized
co
hort)
A to
tal o
f 31
patie
nts
with
sci
atic
a to
geth
er w
ith ra
diol
ogic
sig
ns o
f st
enos
is a
nd c
ompr
essi
on o
f the
cl
inic
ally
affl
icte
d ne
rve
root
s.
Dis
c he
rnia
tions
and
spo
ndyl
olis
is
excl
uded
.
Mos
t pat
ient
s w
ith n
euro
geni
c cl
audi
-ca
tion
(num
ber u
nkno
wn)
.*
No.
of p
atie
nts
with
spo
ndyl
olis
thes
is
unkn
own.
*
n =
13
patie
nts.
Dec
ompr
essi
on (l
amin
ecto
my,
face
tec-
tom
y, d
isce
ctom
y, re
mov
al o
f ost
eo-
phyt
es, a
nd h
yper
trofi c
liga
men
t fl a
va),
with
out f
usio
n.
+ S
tabi
lizin
g or
thos
is fo
r 3 m
o, “
back
sc
hool
,” re
habi
litat
ion
for 1
mo,
and
su
bseq
uent
sta
biliz
ing
exer
cise
s.
n =
18
patie
nts.
Stab
ilizi
ng o
rthos
is (f
or a
ll ac
tiviti
esdu
ring
the
day)
for 3
mo,
“ba
ck s
choo
l,”
reha
bilit
atio
n fo
r 1 m
o, a
nd s
ubse
quen
t st
abili
zing
exe
rcis
es.
6 m
o, 1
, 4, a
nd
10 y
rSu
rger
y: 1
(4 y
r), 2
(1
0 yr
)
Con
trol:
2 (4
yr),
4
(10
yr)
Mal
miv
aara
et a
l 24
A to
tal o
f 94
patie
nts
(mea
n ag
e: 6
2 yr
) w
ith p
ain
irrad
iatin
g to
legs
or b
ut-
tock
s fo
r ≥ 6
mo,
fatig
ue o
r los
s of
se
nsat
ion
in th
e le
gs a
ggra
vate
d by
w
alki
ng, n
o ne
urol
ogic
dys
func
tion,
an
d sp
inal
ste
nosi
s (s
agitt
al d
iam
eter
of
the
dura
l sac
< 10
mm
).
No.
of p
atie
nts
with
spo
ndyl
olis
-th
esis
or n
euro
geni
c cl
audi
catio
n un
know
n. †
n =
50
assi
gned
(45
wer
e ac
tual
ly o
per-
ated
on)
.
Segm
enta
l dec
ompr
essi
on a
nd u
nder
-cu
tting
face
tect
omy,
with
or w
ithou
t fu
sion
(with
or w
ithou
t tra
nspe
dicu
lar
inst
rum
enta
tion)
.
+ B
roch
ure
on s
pina
l ste
nosi
s an
d th
e pr
inci
ples
of a
ctiv
atio
n an
d ph
ysic
al
train
ing,
edu
catio
n on
pai
n-re
lievi
ng
body
pos
ture
s, e
rgon
omic
s, a
nd in
di-
vidu
aliz
ed e
xerc
ises
.
n =
44
assi
gned
(40
actu
ally
trea
ted
with
-ou
t sur
gery
).
NSA
IDs,
phy
siot
hera
py (u
ltras
ound
and
tra
nscu
tane
ous
nerv
e st
imul
atio
n an
d ex
erci
se) f
or 2
4% o
f the
pat
ient
s.
+ B
roch
ure
on s
pina
l ste
nosi
s an
d th
e pr
inci
ples
of a
ctiv
atio
n an
d ph
ysic
al
train
ing,
edu
catio
n on
pai
n-re
lievi
ng
body
pos
ture
s, e
rgon
omic
s, a
nd in
di-
vidu
aliz
ed e
xerc
ises
.
6 m
o, 1
and
2
yrSu
rger
y: 3
(2 y
r)
Con
trol:
4 (2
yr)
Wei
nste
in e
t al 25
(Ran
dom
ized
co
hort)
A to
tal o
f 304
pat
ient
s (m
ean
age:
66 y
r) w
ith n
euro
geni
c cl
audi
catio
n or
sci
atic
a fo
r ≥ 3
mo,
and
spi
nal
sten
osis
and
deg
ener
ativ
e sp
ondy
lo-
listh
esis
see
n on
imag
ing.
Spon
dylo
lisis
and
isth
mic
spo
ndyl
olis
-th
esis
exc
lude
d.
Spon
dylo
listh
esis
in 1
00%
.
Neu
roge
nic
clau
dica
tion
in 8
6%.
n =
159
ass
igne
d (1
01 w
ere
actu
ally
op
erat
ed o
n).
Post
erio
r dec
ompr
essi
ve la
min
ecto
my
with
or w
ithou
t bila
tera
l sin
gle-
leve
l fus
ion
(with
or w
ithou
t pos
terio
r pe
dicl
e sc
rew
inst
rum
enta
tion)
.
n =
145
ass
igne
d (7
0 w
ere
actu
ally
tre
ated
with
out s
urge
ry).
At l
east
act
ive
phys
ical
ther
apy,
edu
catio
n,
or c
ouns
elin
g in
clud
ing
inst
ruct
ions
for
exer
cisi
ng a
t hom
e, N
SAID
s if
tole
rate
d.
6 w
k, 3
and
6 m
o, 1
, 2,
and
4 yr
‡
Surg
ery:
15
(1 y
r), 2
7 (2
yr),
52
(4 y
r)
Con
trol:
11 (1
yr),
25
(2 y
r), 4
6 (4
yr)
Wei
nste
in e
t al 26
(Ran
dom
ized
co
hort)
A to
tal o
f 289
pat
ient
s (m
ean
age:
65.5
yr)
with
neu
roge
nic
clau
dica
-tio
n or
sci
atic
a fo
r ≥ 3
mo
and
spin
al
sten
osis
see
n on
imag
ing.
Spon
dylo
lysi
s an
d sp
ondy
lolis
thes
is,
excl
uded
.
Spon
dylo
listh
esis
in 0
%.
Neu
roge
nic
clau
dica
tion
in 7
9%.
n =
138
ass
igne
d (9
2 w
ere
actu
ally
op
erat
ed o
n).
Post
erio
r dec
ompr
essi
ve la
min
ecto
my.
n =
151
ass
igne
d (8
6 w
ere
actu
ally
tre
ated
with
out s
urge
ry).
At l
east
act
ive
phys
ical
ther
apy,
edu
catio
n,
or c
ouns
elin
g in
clud
ing
inst
ruct
ions
for
exer
cisi
ng a
t hom
e, N
SAID
s if
tole
rate
d
6 w
k, 3
and
6
mo,
1, 2
, and
4
yr
§
Surg
ery:
18
(1 y
r), 3
0 (2
yr),
54
(4 y
r)
Con
trol:
25 (1
yr),
38
(2 y
r), 6
5(4
yr)
(Con
tinue
d)
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
BRS204382.indd E1340BRS204382.indd E1340 25/08/11 11:51 PM25/08/11 11:51 PM

Spine www.spinejournal.com E1341
LITERATURE REVIEW Surgery Versus Conservative Treatment • Kovacs et al TA
BLE
2.
(Con
tinue
d)
Stud
yPa
tient
sSu
rgic
al P
roce
dure
Con
serv
ativ
e Tr
eatm
ent
Follo
w-u
pLo
sses
to
Follo
w-u
p
Zuc
herm
an e
t al 27
(2
005)
A to
tal o
f 200
pat
ient
s, ≥
50 y
r (m
ean
age:
70
yr),
able
to w
alk
≥ 50
feet
, w
ith le
g, b
utto
ck, o
r gro
in p
ain
that
w
as re
lieve
d du
ring fl e
xion
.
Mot
or d
efi c
it, s
pond
ylol
isth
esis
>
Gra
de I,
and
pre
viou
s lu
mba
r sur
-ge
ry e
xclu
ded.
Spon
dylo
listh
esis
gra
de I
in 3
9%. †
Neu
roge
nic
clau
dica
tion
in 1
00%
.
n =
100
Inte
rspi
nous
Pro
cess
Dis
tract
ion
Syst
em
(X S
TOP)
.
n =
100
(91
wer
e ac
tual
ly tr
eate
d w
ithou
t su
rger
y).
Patie
nts
rand
omiz
ed to
the
cont
rol g
roup
re
ceiv
ed a
t lea
st o
ne e
pidu
ral s
tero
id
inje
ctio
n af
ter e
nrol
lmen
t and
wer
e pr
e-sc
ribed
add
ition
al e
pidu
ral s
tero
id in
jec-
tions
, non
ster
oida
l ant
i-infl
am
mat
ory
med
icat
ions
, ana
lges
ics,
and
phy
sica
l th
erap
y as
nec
essa
ry. P
hysi
cal t
hera
py
cons
iste
d of
bac
k sc
hool
and
met
hods
su
ch a
s ic
e pa
cks,
hea
t pac
ks, m
assa
ge,
stab
iliza
tion
exer
cise
s, a
nd p
ool t
hera
py.
6 w
k, 6
mo,
1 an
d 2
yrSu
rger
y: 7
(2 y
r)
Con
trol:
19 (2
yr)
* A to
tal o
f 100
pat
ient
s w
ere
recr
uite
d in
this
stu
dy, 9
1 of
who
m h
ad n
euro
geni
c cl
audi
catio
n. A
mon
g th
ose
100
patie
nts,
onl
y 31
wer
e ra
ndom
ized
. Mea
n ag
e of
thos
e 31
pat
ient
s an
d ho
w m
any
of th
em h
ad
spon
dylo
listh
esis
or
neur
ogen
ic c
laud
icat
ion
is u
nkno
wn.
The
se d
ata
are
not g
iven
in th
e ar
ticle
and
the
auth
ors
coul
d no
t pro
vide
the
sam
e.
† And
erso
n et
al 52
.
‡ Wei
nste
in e
t al 49
.
§ Dat
a su
pplie
d by
the
auth
ors
of th
e or
igin
al s
tudy
.
by the industry, as opposed to public or not-for-profi t sources, in which at least one author had potentially relevant confl ict of interest. 50
Treatments in the conservative arms of those studies included different or nonspecifi ed types of orthosis, rehabilita-tion, physical therapy, exercise, nonsteroidal anti-infl ammatory drugs, analgesics, and education, as well as heat and cold, transcutaneous electrical nerve stimulation, ultrasound, and epidural steroids.
The decision on the kind of surgery or conservative treat-ment applied to each patient was left up to the therapists and no explicit criteria were used.
Follow-up ranged between 2 and 10 years. Variables that were assessed during follow-up included pain, function, clau-dication distance, quality of life, and patients’ overall rating and satisfaction, although instruments used to assess those variables varied across studies ( Table 3 ). Disability, as mea-sured by the Oswestry Disability Index at 2 years, was the only outcome that was assessed in 3 studies or more ( Figure 1 ). 24 – 26 Losses to follow-up ranged between 7.7% (at 1 year) and 44.0% (at 4 years), and were roughly similar between the sur-gical and conservative arms ( Table 2 ).
Small improvements were generally seen in the patients treated conservatively and in whom no catastrophic com-plications such as cauda equina syndrome arose. Changes in claudication distance were similar between conservative and surgical groups. 24 However, results of all the studies consis-tently favored decompressive surgery (with or without fusion) for improvement of pain, function, and quality of life, as well as in terms of patients’ satisfaction. 23 – 26 Crossover rates ranged between 9% and 54%, and affected patients assigned to both the conservative and surgical groups ( Table 3 ). In the two studies with higher crossover rates, 25 , 26 differences between conservative and surgical treatments were statisti-cally signifi cant only in the “as treated” analysis. The only exception was 36-item Medical Outcomes Study Short-Form General Health Survey (SF-36)—“bodily pain,” which even in the “intention to treat” analysis favored surgery at 2 years in one of these studies. 26
The advantage of surgery was already noticeable at 3 to 6 months and remained constant for up to 2 to 4 years, although by the end of that period the differences tended to be smaller ( Table 3 ). In general, the magnitude of the addi-tional improvement triggered by surgery in pain and function was clinically relevant. 53 , 54 Surgery was more effective than conservative treatment for patients with and without spondy-lolisthesis. Surgery was also more effective than conservative treatment for patients with and without neurogenic claudica-tion, although the advantage of surgery was generally greater for the former ( Table 3 ).
The interspinous implant also led to a better evolution than conservative treatment with regard to pain, function, quality of life, and patients’ satisfaction. 27 , 50 – 52 Differences were statisti-cally signifi cant at 6 weeks and remained so till 2 years later. Results favored the implant over conservative treatment to the same extent in patients with and without (Grade I) spondylolis-thesis. This radiological feature was not predictive of outcome. 52
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
BRS204382.indd E1341BRS204382.indd E1341 25/08/11 11:51 PM25/08/11 11:51 PM

E1342 www.spinejournal.com September 2011
LITERATURE REVIEW Surgery Versus Conservative Treatment • Kovacs et al
surgery should be balanced against expected improvements for each individual patient.
In patients aged 50 years or older with neurogenic claudi-cation and spondylolisthesis of Grade I who are able to walk 50 feet or more and have no motor defi cit, the implantation of a specifi c type of interspinous distraction device also leads to better results than conservative treatment for up to 2 years. 27 Results beyond this time period are unknown. The evidence supporting these results derives from industry-funded studies whose authors harbored confl icts of interests. 27 The effective-ness or safety of other interspinous implants is unknown and no study has directly compared decompressive surgery with the interspinous implant.
Only among patients who have spondylolisthesis, adding fusion to decompression may improve the results of surgery for lumbar spinal stenosis. 58 – 60 However, fusion increases major complications, 30-day mortality, and resources used. 55 In patients who have fusion, instrumented and noninstru-mented fusion lead to similar results. 27 , 61 , 62 Among patients who undergo instrumented fusion, simpler procedures ( i.e ., anterior or transverse process or posterior fusion, at only 1 or 2 levels) are safer than complex ones ( i.e. , any combination of simple procedures, 360º fusion, or fusion of more than two levels) 19 , 55 , 62 – 64 and lead to similar results. 61
In all the studies included in this review, each care provider decided the form of conservative or surgical treatment applied to a given patient without following any predefi ned indication criteria. This approach was probably the only feasible one, but it led to treatments within the conservative and surgical groups being as heterogeneous as they are in routine practice both across studies and across patients in the same study. This precludes any conclusion on the comparative effectiveness of any particular form of surgery or conservative treatment. However, surgery was more effective than conservative treat-ment across all the studies and results of surgery were roughly consistent among different surgeons in trials conducted in the United States and Scandinavia. This may suggest that their criteria were somehow consistent or that potential differences in their criteria or in the different surgical techniques used do not have a signifi cant infl uence on results.
Data from observational or nonrandomized cohorts were excluded from this review because of concerns regarding the risk of unknown biases. However, despite being classifi ed as “high quality” according to methodological criteria, 21 , 22 con-cerns exist with regard to the studies included in this review. One study recruited only 31 patients, 23 another included only 94, 24 and none conducted a power analysis. As a result, sample sizes may have been insuffi cient to detect differences for some outcomes. Treatments used in both the surgical and conservative groups were heterogeneous and were not selected according to explicit criteria. To be eligible, patients had to have previously undergone conservative treatment unsuc-cessfully, which may have made it diffi cult to recruit large samples, affected the comparability of the unspecifi c effects across groups ( e.g ., Hawthorne or placebo), and increased rates of withdrawal, dropout, and crossover. 23 , 25 , 26 Although results consistently favored surgery, in the two studies with
Adverse events among patients treated conservatively included injection intolerance, symptom fl are, leg paresthe-sia, and increased back pain. Among patients who under-went decompressive surgery, with or without spinal fusion, between 5.4% and 14% suffered from perioperative compli-cations (the most common being, in all studies, dural tears). Postoperative complications arose in between 8.2% and 18% of the patients and included pulmonary edema, peri-dural hematoma, sepsis, and misjudgment of stenotic level. Reported reoperation rates were 1.3% to 2% at 1 year, 6% to 11% at 2 years, and 15% at 4 years. The rate of recurrent stenosis at 4 years was 5%. The mean duration of the opera-tion was 120 to 199 minutes and the mean blood loss was 198 to 589 mL. 25 , 26 The number of deaths were similar in the surgical and conservative groups. The overall postoperative death rate ranged between 0.3% and 0.5%. Approximately 90% of the patients undergoing surgery did not suffer from any adverse event.
Adverse events related to the implantation of the inter-spinous distraction device included asymptomatic spinous process fracture (1%), malpositioned implant (1%), implant dislodgement or migration (1%), increased pain at implant level (1%), wound dehiscence (1%), wound swelling (1%), incisional pain (1%), and hematoma (1%). In addition, one patient suffered from respiratory distress, another from a transient ischemic coronary episode, and a patient with a his-tory of cardiovascular disease died from pulmonary edema 2 days after device implantation. The reported mean blood loss was 46 mL, the mean duration of the procedure was54 minutes, and 96% of the patients stayed in the hospital for less than 24 hours. Among the patients in whom the inter-spinous distraction device was implanted, 7% subsequently underwent a laminectomy. Among those with spondylolisthe-sis, this percentage was 11.9%.
DISCUSSION These results suggest that in patients with radicular pain caused by spinal stenosis, in whom conservative treatment has failed for 3 to 6 months, decompressive surgery (with or without fusion) does not improve walking ability but improves pain, function, and quality of life to a greater extent than continuing conservative treatment. Surgery is superior to conservative treatment irrespective of the patients’ degree of affectation whether they have spondylolisthesis or neuro-genic claudication. However, slightly better results for surgery can be anticipated in patients with neurogenic claudication. Patients should be aware that the benefi ts of surgery decrease with time but still remain signifi cant till 4 (and possibly 10) years later. 23 , 49 Results in the longer term are unknown. How-ever, obtaining a clinically relevant improvement for such a period is worthwhile even if it were to fade thereafter.
Surgery for spinal stenosis can be effective despite advanced age, multilevel involvement, or common comorbidities such as diabetes, obesity, chronic coronary disease, or chronic lung diseases. 26 , 55 – 57 However, these features, especially the latter, and hospitalizations in the previous year are associated with more complications and mortality. 55 Therefore, the risks of
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
BRS204382.indd E1342BRS204382.indd E1342 25/08/11 11:51 PM25/08/11 11:51 PM

Spine www.spinejournal.com E1343
LITERATURE REVIEW Surgery Versus Conservative Treatment • Kovacs et al
Figure 1. Forest plot showing the results on disability in the three studies that used this instrument, according to the (A) “intention to treat” and (B) “as treated.” In these studies, the disability was measured by the Oswestry Disability Index at 2 years.
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
BRS204382.indd E1343BRS204382.indd E1343 25/08/11 11:51 PM25/08/11 11:51 PM

E1344 www.spinejournal.com September 2011
LITERATURE REVIEW Surgery Versus Conservative Treatment • Kovacs et al TA
BLE
3. S
umm
ary
of R
esul
ts
Stud
y
Patie
nt’s
Glo
bal A
s-se
ssm
ent*
(“G
ood
Res
ult”
) †
Pain
(“W
ith-
out P
ain”
or
“M
ild
Pain
”) ‡
Leg
Pain
§ B
ack
Pain
§ D
isab
ility
(OD
I) ¶
SF-3
6B
odily
Pai
n � SF
-36
Phys
ical
Fun
ctio
n **
Oth
er O
utco
mes
Am
unds
en e
t al 23
(Ran
dom
ized
coh
ort)
1 yr
: RR
2.0
7 (0
.98–
4.38
)
4 yr
: RR
1.9
4 (1
.14–
3.31
)
10 y
r: R
R 3
.18
(0.9
7–10
.41)
1 yr
: NR
4 yr
: RR
3.3
3 (0
.77–
14.3
3)
10 y
r: R
R 1
.59
(0.5
5–4.
55)
Oth
er o
utco
mes
(cla
udic
a-tio
n or
wal
king
dis
tanc
e;
leve
l of d
aily
act
ivity
; an
d ne
urol
ogic
defi
cits
) w
ere
not r
epor
ted
sepa
-ra
tely
for t
he ra
ndom
-iz
ed c
ohor
t.
Mal
miv
aara
et a
l 24
1 yr
: MD
1.6
9 (0
.41–
2.96
)
2 yr
: MD
1.5
1 (0
.25–
2.77
)
1 yr
: MD
2.3
3 (1
.12–
3.55
)
2 yr
: MD
2.1
3 (0
.98–
3.28
)
1 yr
: MD
11.
3 (4
.3–1
8.8)
2 yr
: MD
7.8
(0.8
–14.
9)
≥ 1
0-po
int r
educ
tion
(OD
I):
1 yr
: RR
2.1
6 (1
.31–
3.57
)
2 yr
: RR
1.3
6 (0
.88–
2.10
)
Wal
king
dis
abili
ty (w
alki
ng
dist
ance
< 1.
250
m)*
**
1 yr
: RR
0.9
3 (0
.61–
2.03
)
2 yr
: RR
1.0
8 (0
.70–
2.42
)
Wal
king
dis
abili
ty (w
alki
ng
dist
ance
< 40
0 m
) ***
1 yr
: RR
0.9
1 (0
.51–
4.24
)
2 yr
: RR
1.1
8 (0
.67–
4.72
)
Wei
nste
in e
t al 25
(Ran
dom
ized
coho
rt—al
l)
“Int
entio
n to
trea
t”:
2 yr
: DM
C 2
.2 ( −
2.3
to 6
.8)
4 yr
: DM
C 4
.1 ( −
0.8
to 9
.1)
“As
treat
ed”:
2 yr
: DM
C −
15.9
( − 20
.2
to −
11.7
)
4 yr
: DM
C −
16.2
( − 20
.7
to −
11.6
)
“Int
entio
n to
trea
t”:
2 yr
: DM
C 1
.5 ( −
4.2
to 7
.3)
4 yr
: DM
C −
2 ( −
8.6
to 4
.6)
“As
treat
ed”:
2 yr
: 17.
8 (1
2.5
to 2
3)
4 yr
: 17.
1 (1
0.9
to
23.4
)
“Int
entio
n to
trea
t”:
2 yr
: DM
C 1
.9 ( −
3.7
to 7
.5)
4 yr
: DM
C −
3.1
( − 9.
2 to
3.0
)
“As
treat
ed”:
2 yr
: 16.
7 (1
1.4
to 2
2.1)
4 yr
: DM
C 1
9.2
(13.
4 to
25.
1)
Oth
er o
utco
mes
(pat
ient
’s sa
tisfa
ctio
n; S
teno
sis
Bot
hers
omen
ess
Inde
x,
Leg
Pain
Bot
hers
omen
ess
Scal
e; a
nd L
ow B
ack
Pain
Bot
hers
omen
ess
Scal
e) w
ere
not p
rovi
ded
sepa
rate
ly fo
r the
ran-
dom
ized
coh
ort.
(Ran
dom
ized
co
hort—
with
neu
-ro
geni
c cl
audi
ca-
tion)
� �
“Int
entio
n to
trea
t”:
2 yr
: DM
C −
2 ( −
7.8
to 3
.9)
4 yr
: DM
C −
1.2
( − 7.
5 to
5.
1)
“As
treat
ed”:
2 yr
: DM
C −
8.3
( − 13
.1
to −
3.4)
4 yr
: DM
C −
6.1
( − 12
.3
to 0
.1)
“Int
entio
n to
trea
t”:
2 yr
: DM
C 5
.9 ( −
1.8
to 1
3.5)
4 yr
: DM
C 0
.1 ( −
8.3
to 8
.4)
“As
treat
ed”:
2 yr
: DM
C 1
1.3
(5.1
to
17.
6)
4 yr
: DM
C 8
.8 (0
.6 to
16
.9)
“Int
entio
n to
trea
t”:
2 yr
: DM
C −
3.4
( − 10
.6
to 3
.9)
4 yr
: DM
C −
3.1
( − 10
.9
to 4
.8)
“As
treat
ed”:
2 yr
: DM
C 5
.1 ( −
0.8
to
11.1
)
4 yr
: DM
C 6
.9 ( −
0.7
to
14.5
)
(Con
tinue
d)
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
BRS204382.indd E1344BRS204382.indd E1344 25/08/11 11:51 PM25/08/11 11:51 PM

Spine www.spinejournal.com E1345
LITERATURE REVIEW Surgery Versus Conservative Treatment • Kovacs et al TA
BLE
3.
(Con
tinue
d)
Stud
y
Patie
nt’s
Glo
bal A
s-se
ssm
ent*
(“G
ood
Res
ult”
) †
Pain
(“W
ith-
out P
ain”
or
“M
ild
Pain
”) ‡
Leg
Pain
§ B
ack
Pain
§ D
isab
ility
(OD
I) ¶
SF-3
6B
odily
Pai
n � SF
-36
Phys
ical
Fun
ctio
n **
Oth
er O
utco
mes
(Ran
dom
ized
co
hort—
with
out
neur
ogen
ic c
laud
i-ca
tion)
� �
“Int
entio
n to
trea
t”:
2 yr
: DM
C −
8.6
( − 20
to
2.8)
4 yr
: DM
C 4
.2 ( −
8.1
to
16.5
)
“As
treat
ed”:
2 yr
: DM
C −
8.1
( − 17
.2
to 0
.9)
4 yr
: DM
C −
8.8
( − 20
.2
to 2
.7)
“Int
entio
n to
trea
t”:
2 yr
: DM
C 1
4.9
(0.1
to
29.
7)
4 yr
: DM
C 2
(�13
.9
to 1
7.9)
“As
treat
ed”:
2 yr
: DM
C 1
3.7
(2.3
to
25.
2)
4 yr
: DM
C 1
8.7
(4.5
to
33)
“Int
entio
n to
trea
t”:
2 yr
: DM
C 1
1.6
( − 2.
4 to
25.
6)
4 yr
: DM
C −
4.5
( − 19
.5
to 1
0.5)
“As
treat
ed”:
2 yr
: DM
C 1
1.4
(0.5
to
22.2
)
4 yr
: DM
C 1
1.8
( − 1.
6 to
25.
3)
Wei
nste
in e
t al 26
“I
nten
tion
to tr
eat”
:“I
nten
tion
to tr
eat”
:“I
nten
tion
to tr
eat”
:Sa
me
as in
Wei
nste
in et
al 25
(R
ando
miz
ed c
o-ho
rt—al
l)2
yr: D
MC
− 3.
5 ( −
8.7
to
1.7)
2 yr
: DM
C 7
.8 (1
.5 to
14
.1)
2 yr
: DM
C 0
.1 ( −
6.4
to 6
.5)
“As
treat
ed”:
“As
treat
ed”:
“As
treat
ed”:
2 yr
: �8.
7 ( −
13.3
to −
4.0)
2 yr
: 11.
7 (6
.2 to
17.
2)2
yr: 8
.1 (2
.8 to
13.
5)
(Ran
dom
ized
co
hort—
with
ne
urog
enic
cl
audi
catio
n)� �
“Int
entio
n to
trea
t”:
“Int
entio
n to
trea
t”:
“Int
entio
n to
trea
t”:
2 yr
: DM
C +
1.1
( − 3.
9 to
6)
2 yr
: DM
C 2
( − 4.
6 to
8.7
)2
yr: D
MC
3.2
( − 2.
9 to
9.2
)
4 yr
: DM
C +
− 3.
7 ( −
1.6
to 9
.0)
4 yr
: DM
C −
3.6
( − 10
.8 to
3.5
)4
yr: D
MC
− 3
( − 9.
6 to
3.5
)
“As
treat
ed”:
“As
treat
ed”:
“As
treat
ed”:
2 yr
: DM
C −
16.8
( − 20
.9
to −
12.6
)2
yr: D
MC
20
(14.
3 to
25.
6)2
yr: D
MC
17.
9 (1
2.6
to 2
3.3)
4 yr
: DM
C −
18.4
( − 23
.3
to −
13.5
)4
yr: D
MC
20.
6 (1
3.9
to 2
7.3)
4 yr
: DM
C 2
0.4
(14.
1 to
26.
8)
(Ran
dom
ized
co
hort—
with
-ou
t neu
roge
nic
clau
dica
tion)
� �
“Int
entio
n to
trea
t”:
“Int
entio
n to
trea
t”:
“Int
entio
n to
trea
t”:
(Con
tinue
d)
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
BRS204382.indd E1345BRS204382.indd E1345 25/08/11 11:51 PM25/08/11 11:51 PM

E1346 www.spinejournal.com September 2011
LITERATURE REVIEW Surgery Versus Conservative Treatment • Kovacs et al TA
BLE
3.
(Con
tinue
d)
Stud
y
Patie
nt’s
Glo
bal A
s-se
ssm
ent*
(“G
ood
Res
ult”
) †
Pain
(“W
ith-
out P
ain”
or
“M
ild
Pain
”) ‡
Leg
Pain
§ B
ack
Pain
§ D
isab
ility
(OD
I) ¶
SF-3
6B
odily
Pai
n � SF
-36
Phys
ical
Fun
ctio
n **
Oth
er O
utco
mes
2 yr
: DM
C 6
.7 ( −
5.6
to
18.9
)2
yr: D
MC
− 2.
3 ( −
18.5
to 1
3.9)
2 yr
: DM
C −
1.9
( − 16
.7
to 1
2.8)
4 yr
: DM
C 5
.7 ( −
7.6
to
19.0
)4
yr: D
MC
9.3
( − 8.
7 to
27.
4)4
yr: D
MC
− 2.
8 ( −
19.3
to
13.
7)
“As
treat
ed”:
“As
treat
ed”:
As
treat
ed”:
2 yr
: DM
C −
12.9
( − 21
.8 to
−
4.1)
2 yr
: DM
C 1
6.3
(4.5
to 2
8.1)
2 yr
: DM
C 8
.1 ( −
3.1
to
19.2
)
4 yr
: DM
C −
10.2
( − 21
.2
to 0
.8)
4 yr
: DM
C 1
.9 ( −
13.2
to
17)
4 yr
: DM
C 1
8.9
(4.7
to
33.1
)
Zuc
herm
an e
t al 27
20
052
yr: 7
3.1%
(s
urge
ry) v
s.
35.9
% (c
ontr
ol)
( P <
0.0
01)
Sym
ptom
s Se
verit
y Sc
ore ††
Surg
ery
bett
er a
t 6 w
k,6
mo,
1 a
nd 2
yr
(gra
phs)
( P
< 0
.001
)
2 yr
: MPC
45.
4% (s
urge
ry)
vs . 7
.4%
(con
trol
) ( P
<
0.00
1)
“Clin
ical
ly re
leva
nt im
-pr
ovem
ent (
patie
nts)
”:
2 yr
: 60.
2% (s
urge
ry) v
s .
18.5
% (c
ontr
ol)
( P <
0.0
01)
Sym
ptom
s Se
verit
y Sc
ore ††
Surg
ery
bett
er a
t 6 w
k,6
mo,
1 a
nd 2
yr
(gra
phs)
( P
< 0
.001
)
2 yr
: MPC
44.
3% (s
urge
ry)
vs . −
0.4%
(con
trol
) ( P
< 0
.001
)
“Clin
ical
ly re
leva
nt
impr
ovem
ent (
as m
easu
red
by p
atie
nts)
”:
2 yr
: 57%
(sur
gery
) vs .
14
.8%
(con
trol
) ( P
<
0.00
1)
(Con
tinue
d)
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
BRS204382.indd E1346BRS204382.indd E1346 25/08/11 11:51 PM25/08/11 11:51 PM

Spine www.spinejournal.com E1347
LITERATURE REVIEW Surgery Versus Conservative Treatment • Kovacs et al TA
BLE
3.
(Con
tinue
d)
Stud
y
Patie
nt’s
Glo
bal A
s-se
ssm
ent*
(“G
ood
Res
ult”
) †
Pain
(“W
ith-
out P
ain”
or
“M
ild
Pain
”) ‡
Leg
Pain
§ B
ack
Pain
§ D
isab
ility
(OD
I) ¶
SF-3
6B
odily
Pai
n � SF
-36
Phys
ical
Fun
ctio
n **
Oth
er O
utco
mes
ZC
Q §§
(glo
bal s
ucce
ss) ¶
¶
6 m
o: 5
2% (s
urge
ry) v
s .
9% (c
ontro
l) ( P
val
ue n
ot
repo
rted)
1 yr
: 59%
vs .
12%
( P v
alue
no
t rep
orte
d)
2 yr
: 48.
4% (s
urge
ry)
vs . 4
.9%
(con
trol
) ( P
<
0.00
1)
Qua
lity
of li
fe (S
F-36
)
At a
ll po
st-t
reat
men
t tim
e po
ints
(6 w
k, 6
mo,
1 y
r, an
d 2
yr),
the
mea
n do
-m
ain
scor
es d
ocum
ente
d in
the
X S
TOP
grou
p w
ere
sign
ifi ca
ntly
gre
ater
than
th
ose
in th
e no
nope
rativ
e gr
oup,
with
the
exce
p-tio
n of
the
mea
n G
ener
al
Hea
lth, R
ole
Emot
iona
l, an
d M
enta
l Com
pone
nt
Sum
mar
y sc
ores
at 2
yr
(Sub
grou
p w
ith s
pon-
dylo
listh
esis
)Pa
tient
s sa
tis-
fact
ion
(ZC
Q
dom
ain)
: ‡‡
2 yr
: Bet
ter
surg
ery
(sta
tisti-
cally
sig
nifi c
ant)
(gra
phs)
Sym
ptom
s Se
verit
y Sc
ore ††
2 yr
: Bet
ter
surg
ery
( P <
0.
0001
)
Sym
ptom
s Se
verit
y Sc
ore ††
2 yr
: Bet
ter
surg
ery
( P <
0.
0001
)
ZC
Q §
§ (gl
obal
suc
cess
) ¶¶
2 yr
: 63.
4% (s
urge
ry) v
s .
12.9
% (c
ontr
ol) (
“hig
hly
stat
istic
ally
sig
nifi
cant
”)
(Con
tinue
d)
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
BRS204382.indd E1347BRS204382.indd E1347 25/08/11 11:51 PM25/08/11 11:51 PM

E1348 www.spinejournal.com September 2011
LITERATURE REVIEW Surgery Versus Conservative Treatment • Kovacs et al
TAB
LE 3
. (C
ontin
ued)
Stud
y
Patie
nt’s
Glo
bal A
s-se
ssm
ent*
(“G
ood
Res
ult”
) †
Pain
(“W
ith-
out P
ain”
or
“M
ild
Pain
”) ‡
Leg
Pain
§ B
ack
Pain
§ D
isab
ility
(OD
I) ¶
SF-3
6B
odily
Pai
n � SF
-36
Phys
ical
Fun
ctio
n **
Oth
er O
utco
mes
* The
pat
ient
s w
ere
aske
d to
eva
luat
e th
eir
own
situ
atio
n an
d to
sta
te w
heth
er it
was
bet
ter,
wor
se, o
r un
chan
ged
as c
ompa
red
with
thei
r co
nditi
on o
n en
terin
g th
e st
udy.
Thi
s, to
geth
er w
ith th
e op
inio
n of
the
exam
-in
ing
phys
icia
n, c
onst
itute
d th
e ba
sis
for
the
stat
emen
t of o
vera
ll tr
eatm
ent r
esul
t (ex
celle
nt, f
air,
unch
ange
d, a
nd w
orse
).
† Exc
elle
nt (
full
or a
lmos
t ful
l res
titut
ion
cons
ider
ing
pain
and
phy
sica
l fun
ctio
n) o
r fa
ir (p
artia
l res
titut
ion
with
less
er p
robl
ems
and
clea
r im
prov
emen
t ove
r th
e co
nditi
on a
t ent
ry to
the
stud
y) w
as c
onsi
dere
d to
be
a go
od r
esul
t.
‡ The
inte
nsity
of p
ain
was
sta
ted
verb
ally
(se
vere
, mod
erat
e, o
r lig
ht).
§ The
inte
nsity
of p
ain
was
ass
esse
d by
a N
umer
ical
Rat
ing
Scal
e (0
, no
pain
to 1
0, w
orst
pos
sibl
e pa
in).
¶ O
swes
try
Dis
abili
ty In
dex,
whe
re 0
indi
cate
s no
dis
abili
ty a
nd 1
00 in
dica
tes
wor
st p
ossi
ble
disa
bilit
y. W
eins
tein
, 200
7 an
d 20
08, e
xpre
ssed
the
resu
lts a
s th
e pe
rcen
tage
of t
he m
axim
um s
core
.
� SF-
36 H
ealth
Sta
tus
Que
stio
nnai
re (
phys
ical
func
tion
subs
cale
), w
here
hig
her
scor
es in
dica
te b
ette
r ou
tcom
es.
** SF
-36
Hea
lth S
tatu
s Q
uest
ionn
aire
(pa
in s
ubsc
ale)
, whe
re h
ighe
r sc
ores
indi
cate
bet
ter
outc
omes
.
†† A
dom
ain
of th
e Z
CQ
(1–
4), w
here
1 is
the
best
pos
sibl
e ou
tcom
e an
d re
pres
ents
no
pain
.
‡‡ A
dom
ain
of th
e Z
CQ
(1–
5), w
here
1 is
the
best
pos
sibl
e ou
tcom
e an
d re
pres
ents
no
limita
tion
in fu
nctio
n.
§§ Z
uric
h C
laud
icat
ion
Que
stio
nnai
re (
capt
ures
dat
a in
thre
e di
stin
ct d
omai
ns:
sym
ptom
sev
erity
; ph
ysic
al fu
nctio
n; a
nd p
ost-t
reat
men
t pat
ient
sat
isfa
ctio
n) (
3–13
), w
here
3 is
the
best
pos
sibl
e ou
tcom
e.
¶¶ Tr
eatm
ent i
s co
nsid
ered
suc
cess
ful i
f the
pat
ient
is a
t lea
st “
som
ewha
t sat
isfi e
d” (
an a
vera
ge s
core
of 2
.5)
and
has
at le
ast a
0.5
impr
ovem
ent i
n bo
th s
ympt
om s
ever
ity a
nd p
hysi
cal f
unct
ion.
� � D
ata
prov
ided
by
the
auth
ors
at r
eque
st (
not p
ublis
hed)
.
*** W
alki
ng c
apac
ity w
as a
sses
sed
on a
trea
dmill
at a
spe
ed o
f 2.5
km
/h fo
r a
max
imum
of 3
0 m
in o
r 1.
25 k
m. R
estr
ictio
n of
wal
king
was
defi
ned
as
the
dist
ance
afte
r w
hich
a p
atie
nt d
id n
ot w
ant t
o go
on
beca
use
of p
ain,
or
fatig
ue o
r w
eakn
ess
in le
gs, o
r a
com
bina
tion
of th
ese.
36-it
em M
edic
al O
utco
mes
Stu
dy S
hort
-For
m G
ener
al H
ealth
Sur
vey
DM
C in
dica
tes
diffe
renc
es in
mea
n ch
ange
s fr
om b
asel
ine
(with
95%
con
fi den
ce in
terv
al);
MD
, mea
n di
ffere
nce
(with
95%
con
fi den
ce in
terv
al);
MPC
, mea
n pe
rcen
tage
cha
nge
(with
95%
con
fi den
ce in
terv
al);
R
R, r
isk
ratio
(w
ith 9
5% c
onfi d
ence
inte
rval
).
Bol
d le
tters
indi
cate
the
resu
lts th
at fa
vor
surg
ery
(sig
nifi c
ant d
iffer
ence
s).
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
BRS204382.indd E1348BRS204382.indd E1348 25/08/11 11:52 PM25/08/11 11:52 PM

Spine www.spinejournal.com E1349
LITERATURE REVIEW Surgery Versus Conservative Treatment • Kovacs et al
are not present, decompressive surgery could be envisaged. In patients with signifi cant spondylolisthesis, the surgeon may consider complementing decompressive surgery with nonin-strumented posterolateral fusion or with the simplest possible instrumented fusion procedure. This approach would not be suitable for patients who show spinal stenosis on imaging but are asymptomatic or report only back pain (without pain or neurological symptoms in the legs), or for those with serious neurological impairment, especially in those with cauda equina syndrome in whom surgery should be conducted urgently. 67
Generalizability of these results to clinical practice should be discussed. Care providers participating in these RCTs were volunteers as opposed to a random selection of those work-ing in the setting where the studies took place and whether their criteria and level of skills are representative of the rest of care providers in their environment is unknown. Moreover, no data are available on the learning curves necessary before application of some of the forms of treatment that were used in these studies, such as epidural injections or surgery. Educa-tion and training standards for these procedures in routine practice should match those required in these RCTs because these standards are essential for generalizability of any non-pharmacological health technology. 66 Postmarketing surveil-lance should also be implemented, ideally by setting up a registry including all patients seeking care for symptomatic spinal stenosis, minimizing losses to follow-up, and using validated methods to gather clinically relevant data (including demographic data, clinical features, comorbidities, conserva-tive and surgical treatments applied to each patient, experi-ence and training standards of the care providers applying them, and patient’s clinical evolution). 66 Such postmarketing surveillance would not substitute RCTs but would be valu-able to: (1) determine the effects in routine clinical practice, of treatments that have previously shown to be effective through RCTs, (2) compare, in routine practice conditions, the results from treatments that have shown to be effective for the same subset of patients as in previous RCTs, (3) identify factors that predict the result of each treatment to refi ne its indication criteria, and (4) gather data on unexpected safety concerns.
In conclusion, this review shows that decompressive sur-gery with or without fusion and implantation of a specifi c interspinous distraction device are more effective than con-tinued conservative treatment for radicular pain due to spi-nal stenosis in patients in whom the latter has failed for 3 to 6 months.
the largest crossover rates, most differences were statistically signifi cant only in the “as treated” analysis and not in the “intention to treat” one. 25 , 26 Moreover, blindness (of thera-pists, patients, and outcome assessors) is unfeasible in studies comparing surgical with nonsurgical procedures and the pla-cebo effect from surgery is likely to be more powerful than the one from conservative treatment, especially among patients in whom the latter has already failed. This is a special concern because outcome variables are subjective and assessed by the patients ( e.g ., pain severity, function, and satisfaction).
However, these are the variables that make clinical sense, were assessed using previously validated methods, the studies’ design was reasonable ( Table 1 ), and their limitations are inher-ent to the kind of treatments being assessed and to the patient characteristics. The only way of controlling for potential dif-ferences in the placebo effect would be to undertake RCTs comparing decompressive surgery with sham surgery, which might face ethical and practical diffi culties. Despite differences in methods and geographical settings, results from the stud-ies included in this review consistently favor surgery and are biologically plausible. All this suggests that, although method-ological weaknesses make it inappropriate to consider each of the reviewed studies as representing “the best evidence in ideal conditions,” the general conclusions from this review may be seen as deriving from “the best possible evidence in this fi eld.”
Further RCTs could also compare different surgical tech-niques in specifi c subsets of patients and should compare the interspinous device with surgery in the subset of patients in whom the former is indicated. Such a study appears to have been initiated. 65 Further RCTs could also assess the effective-ness of specifi c forms or combinations of conservative treat-ments to compare surgery with truly effective alternatives. All these studies should be of high methodological quality and conducted independently from the industry by authors with no confl icts of interest. 66 They should be designed as large multicenter trials with strategies to reduce withdrawals and crossovers. There may be ethical concerns regarding further RCTs using the same methods as those used in the studies included in this review to compare the same miscellanea of surgical and conservative treatments.
No catastrophic events ( e.g ., cauda equina syndrome) arose among the patients receiving conservative treatment. Results from surgery were similar among patients initially assigned to surgery and those who crossed over to this group after failure of the conservative treatment they had been initially assigned to. 23 , 25 , 26 This suggests that delaying surgery is not associated with a poorer prognosis. On the contrary, the interspinous implant is less aggressive and resulted in less blood loss and a shorter hospital stay than decompressive surgery (with or without fusion). Taken together, these results may counsel a step-by-step approach in the treatment of spinal stenosis. The fi rst step could be a conservative treatment for 3 to 6 months. If such an approach fails, the implantation of a specifi c type of inerspinous device should be considered in patients aged 50 years and older, with neurogenic claudication and spon-dylolisthesis of Grade I or less who are able to walk 50 feet or more and have no motor defi cit. If these indication criteria
➢ Key Points
Five high-quality randomized controlled trials (RCTs), including a total of 918 patients, compared surgi-cal procedures (the implantation of a specifi c type of interspinous distraction device or decompressive surgery, with or without fusion, whether instru-mented or not) with a miscellanea of conservative treatments, in patients with symptomatic lumbar spinal stenosis in whom the latter had failed for 3 to 6 months.
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
BRS204382.indd E1349BRS204382.indd E1349 25/08/11 11:52 PM25/08/11 11:52 PM

E1350 www.spinejournal.com September 2011
LITERATURE REVIEW Surgery Versus Conservative Treatment • Kovacs et al
11. Porter RW . Spinal stenosis and neurogenic claudication . Spine 1996 ; 21 : 2046 – 52 .
12. Takahashi K , Kagechika K , Takino T , et al. Changes in epidural pressure during walking in patients with lumbar spinal stenosis . Spine 1995 ; 20 : 2746 – 9 .
13. Takahashi K , Miyazaki T , Takino T , et al. Epidural pressure mea-surements. Relationship between epidural pressure and posture in patients with lumbar spinal stenosis . Spine 1995 ; 20 : 650 – 3 .
14. Kobayashi S , Kokubo Y , Uchida K , et al. Effect of lumbar nerve root compression on primary sensory neurons and their central branches: changes in the nociceptive neuropeptides substance P and somatostatin . Spine 2005 ; 30 : 276 – 82 .
15. Hall S , Bartleson JD , Onofrio BM , et al. Lumbar spinal stenosis: clinical features, diagnostic procedures, and results of surgical treat-ment in 68 patients . Ann Intern Med 1985 ; 103 : 271 – 5 .
16. De Graaf I , Prak A , Bierma-Zeinstra S , et al. Diagnosis of lumbar spinal stenosis. A systematic review of the accuracy of diagnostic tests . Spine 2006 ; 31 : 1168 – 76 .
17. Deyo RA , Ciol MA , Cherkin DC , et al. Lumbar spinal fusion: a cohort study of complications, reoperations, and resource use in the Medicare population . Spine 1993 ; 18 : 1463 – 70 .
18. Deyo RA , Gray DT , Kreuter W , et al. United States trends in lumbar fusion surgery for degenerative conditions . Spine 2005 ; 30 : 1441 – 5 .
19. Gibson JN , Waddell G . Surgery for degenerative lumbar spon-dylosis; updated cochrane review . Cochrane Database Syst Rev 2005 ; 19 ( 4 ): CD001352 .
20. Higgins JPT , Green S , eds. Cochrane Handbook for Systematic Reviews of Interventions Version 5.0.2 . Oxfordshire: The Cochrane Collaboration, 2008. Updated September 2008 . Available at: http//www.cochrane-handbook.org . Accessed May 17, 2010.
21. Van Tulder MW , Assendelft WJJ , Koes BW , et al. Method guidelines for systematic reviews in the Cochrane Collaboration Back Review Group for spinal disorders . Spine 1997 ; 22 ( 20 ): 2323 – 30 .
22. Van Tulder M , Furlan A , Bombardier C , et al. Updated method guidelines for systematic reviews in the Cochrane Collaboration Back Review Group . Spine 2003 ; 28 : 1290 – 9 .
23. Amundsen T , Weber H , Nordal HJ , et al. Lumbar spinal stenosis: conservative or surgical management? A prospective 10-year study . Spine 2000 ; 25 : 1424 – 36 .
24. Malmivaara A , Slatis P , Heliovaara M , et al. Surgical of nonopera-tive treatment for lumbar spinal stenosis? A randomized controlled trial . Spine 2007 ; 32 : 1 – 8 .
25. Weinstein JN , Lurie JD , Tosteson TD , et al. Surgical versus nonsur-gical treatment for lumbar degenerative spondylolisthesis . N Engl J Med 2007 ; 356 ( 22 ): 2257 – 70 .
26. Weinstein JN , Tosteson TD , Lurie JD , et al. SPORT Investigators. Surgical versus nonsurgical therapy for lumbar spinal stenosis . N Engl J Med 2008 ; 358 : 794 – 810 .
27. Zucherman JF , Hsu KY , Hartjen CA , et al. A multicenter, prospec-tive, randomized trial evaluating the X STOP interspinous process decompression system for the treatment of neurogenic intermit-tent claudication: two-year follow-up results . Spine 2005 ; 30 ( 12 ): 1351 – 8 .
28. Osterman H , Seitsalo S , Karppinen J , et al. Effectiveness of microd-iscectomy for lumbar disc herniation: a randomized controlled trial with 2 years of follow-up . Spine 2006 ; 31 : 2409 – 14 .
29. Peul WC , van Houwelingen HC , van den Hout WB , et al. Surgery versus prolonged conservative treatment for sciatica . N Engl J Med 2007 ; 356 : 2245 – 56 .
30. Brox JI , Sorensen R , Friis A , et al. Randomized clinical trial of lum-bar instrumented fusion and cognitive intervention and exercises in patients with chronic low back pain and disc degeneration . Spine 2003 ; 28 : 1913 – 21 .
31. Brox J , Reikeras O , Nygaard O , et al. Lumbar instrumented fusion compared with cognitive intervention and exercises in patients with chronic back pain after previous surgery for disc herniation: a pro-spective randomized controlled study . Pain 2006 ; 122 : 145 – 55 .
32. Fairbank J , Frost H , Wilson-MacDonald J , et al. Randomised controlled trial to compare surgical stabilisation of the lumbar spine with an intensive rehabilitation programme for patients with chronic low back pain: the MRC spine stabilisation trial . BMJ 2005 ; 330 : 1233 .
In all the studies, surgery led to better results for pain, disability, and quality of life, although not for walking ability. Results of surgery were similar among patients with and without spondylolisthesis, and slightly better among those with neurogenic claudi-cation than among those without it. The advantage of surgery was noticeable at 3 to 6 months and remained for up to 2 to 4 years, although at the end of that period diff erences tended to be smaller.
Main methodological concerns in these RCTs include the heterogeneity of treatments within the conser-vative and surgical groups, the fact that all patients included had unsuccessfully undergone conserva-tive treatments previously, which may have led to diff erences in the placebo eff ect across groups and increased crossover, withdrawal, and dropout rates, and the lack of blindness of care provider, patients, and outcome assessment. However, these concerns are inherent to the type of patients included and the kind of treatments compared. Therefore, evidence from these RCTs can be seen as the “best possible” in this fi eld. There may be ethical concerns regard-ing further RCTs comparing the forms of surgery and conservative treatments, which have been used in these trials.
Further RCTs should: (1) compare the interspinous device with surgery in patients aged 50 years or older, with neurogenic claudication and spondylolisthesis of Grade I and lesser, who are able to walk 50 feet or more, and have no motor defi cit; (2) compare dif-ferent surgical techniques and interspinous devices in specifi c subsets of patients; (3) defi ne indication criteria for the diff erent surgical procedures;(4) defi ne learning curves for all these procedures;(5) implement registries and postmarketing surveil-lance methods; and (6) not be conducted by the in-dustry or by authors who harbor confl icts of interest.
References 1. Epstein NE , Maldonado VC , Cusick JF . Symptomatic lumbar spi-
nal stenosis . Surg Neurol 1998 ; 50 : 3 – 10 . 2. Alvarez JA , Hardy RH Jr . Lumbar spine stenosis: a common cause
of back and leg pain . Am Fam Physician 1998 ; 57 : 1825 – 40 . 3. Postacchini F . The diagnosis of lumbar spinal stenosis: analysis
of clinical and radiographic fi ndings in 43 cases . Ital J OrthopTraumatol 1985 ; 11 : 5 – 21 .
4. Tan SB . Spinal canal stenosis . Singapore Med J 2003 ; 44 : 168 – 9 . 5. Jacobsen S , Sonne-Holm S , Rovsing H , et al. Degenerative spon-
dylolisthesis: an epidemiological perspective: the CopenhagenOsteoarthritis Study . Spine 2007 ; 32 : 120 – 5 .
6. Boden SD , Davis DO , Dina TS , et al. Abnormal magnetic-resonance scans of the lumbar spine in asymptomatic subjects: a prospective investigation . J Bone Joint Surg Am 1990 ; 72 : 403 – 8 .
7. Haig AJ , Tong HC , Yamakawa KSJ , et al. Predictors of pain and function in persons with spinal stenosis, low back pain, and no back pain. Spine 2006 ; 31 : 2950 – 7 .
8. Kalichman L , Li L , Kim HD , et al. Facet joint osteoarthritis and low back pain in the community-based population . Spine 2008 ; 33 : 2560 – 5 .
9. Kalichman L , Kim HD , Li L , et al. Spondylolysis and spondylolis-thesis prevalence and association with low back pain in the adult community-based population . Spine 2009 ; 34 : 199 – 205 .
10. Kobayashi S , Baba H , Uchida K , et al. Blood circulation of cauda equina and nerve root [in Japanese] . Clin Calcium 2005 ; 15 : 63 – 72 .
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
BRS204382.indd E1350BRS204382.indd E1350 25/08/11 11:52 PM25/08/11 11:52 PM

Spine www.spinejournal.com E1351
LITERATURE REVIEW Surgery Versus Conservative Treatment • Kovacs et al
33. Fritzell P , Hagg O , Wessberg P , et al. Swedish Lumbar Spine Study Group. 2001 Volvo Award Winner in Clinical Studies: lumbar fusion versus nonsurgical treatment for chronic low back pain: a multicenter randomized controlled trial from the Swedish Lumbar Spine Study Group . Spine 2001 ; 26 : 2521 – 32 .
34. Weber H . Lumbar disc herniation. A controlled, prospective study with ten years of observation . Spine 1983 ; 8 : 131 – 40 .
35. Weinstein JN , Tosteson TD , Lurie JD , et al. Surgical vs. nonop-erative treatment for lumbar disk herniation: the Spine Patient Outcomes Research Trial (SPORT): a randomized trial . JAMA 2006 ; 296 : 2441 – 50 .
36. Ekman P , Moller H , Hedlund R . The long-term effect of postero-lateral fusion in adult isthmic spondylolisthesis: a randomized con-trolled study . Spine J 2005 ; 5 ( 1 ): 36 – 44 .
37. Moller H , Hedlund R . Surgery versus conservative management in adult isthmic spondylolisthesis—a prospective randomized study: Part 1 . Spine 2000 ; 25 ( 13 ): 1711 – 5 .
38. Atlas SJ , Deyo RA , Keller RB , et al. The Maine Lumbar Spine Study, Part III. 1-year outcomes of surgical and nonsurgical management of lumbar spinal stenosis . Spine 1996 ; 21 ( 15 ): 1787 – 94 .
39. Atlas SJ , Deyo RA , Keller RB , et al. The Maine Lumbar Spine Study, Part II. 1-year outcomes of surgical and nonsurgical manage-ment of sciatica . Spine 1996 ; 21 ( 15 ): 1777 – 86 .
40. Atlas SJ , Singer DE , Keller RB , et al. Application of outcomes research in occupational low back pain: the Maine Lumbar Spine Study . Am J Ind Med 1996 ; 29 ( 6 ): 584 – 9 .
41. Atlas SJ , Keller RB , Robson D , et al. Surgical and nonsurgical man-agement of lumbar spinal stenosis: four-year outcomes from the Maine Lumbar Spine Study . Spine 2000 ; 25 ( 5 ): 556 – 62 .
42. Atlas SJ , Keller RB , Wu YA , et al. Long-term outcomes of surgi-cal and nonsurgical management of lumbar spinal stenosis: 8 to 10 year results from the Maine Lumbar Spine Study . Spine 2005 ; 30 ( 8 ): 936 – 43 .
43. Chang Y , Singer DE , Wu YA , et al. The effect of surgical and non-surgical treatment on longitudinal outcomes of lumbar spinal ste-nosis over 10 years . J Am Geriatr Soc 2005 ; 53 ( 5 ): 785 – 92 .
44. Keller RB , Atlas SJ , Singer DE , et al. The Maine Lumbar Spine Study, Part I. Background and concepts . Spine 1996 ; 21 ( 15 ): 1769 – 76 .
45. Jhonsson KE , Uden A , Rosen I . The effect of decompression on the natural course of spinal stenosis. A comparison of surgically treated and untreated patients . Spine 1991 ; 16 ( 6 ): 615 – 9 .
46. Mariconda M , Fava R , Gatto A , et al. Unilateral laminectomy for bilateral decompression of lumbar spinal stenosis: a prospective comparative study with conservatively treated patients . J Spinal Disord Tech 2002 ; 15 ( 1 ): 39 – 46 .
47. Amundsen T , Weber H , Lilleas F , et al. Lumbar spinal stenosis. Clinical and radiologic features . Spine 1995 ; 20 : 1178 – 86 .
48. Birkmeyer NJ , Weinstein JN , Tosteson AN , et al. Design of the Spine Patient Outcomes Research Trial (SPORT) . Spine 2002 ; 27 ( 12 ): 1361 – 72 .
49. Weinstein JN , Lurie JD , Tosteson TD , et al. Surgical compared with nonoperative treatment for lumbar degenerative spondylolisthesis. Four-year results in the Spine Patient Outcomes Research Trial (SPORT) randomized and observational cohorts . J Bone Joint Surg Am 2009 ; 91 : 1295 – 304 .
50. Zucherman JF , Hsu KY , Hartjen CA , et al. A prospective random-ized multicenter study for the treatment of lumbar spinal stenosis with the X STOP interspinous implant: 1-year results . Eur Spine J 2004 ; 13 ( 1 ): 22 – 31 .
51. Hsu KY , Zucherman JF , Hartjen CA , et al. Quality of life of lumbar stenosis-treated patients in whom the X STOP interspinous device was implanted . J Neurosurg Spine 2006 ; 5 ( 6 ): 500 – 7 .
52. Anderson PA , Tribus CB , Kitchel SH . Treatment of neurogenic claudication by interspinous decompression: application of theX STOP device in patients with lumbar degenerative spondylolis-thesis . J Neurosurg Spine 2006 ; 4 ( 6 ): 463 – 71 .
53. Van der Roer N , Ostelo RWJG , Bekkering G , et al. Minimal clini-cally important change for pain intensity, functional status, and general health status in patients with nonspecifi c low back pain . Spine 2006 ; 31 : 578 – 82 .
54. Kovacs F , Abraira V , Royuela A , et al. Minimal clinically important change for pain intensity and disability in patients with nonspecifi c low back pain . Spine 2007 ; 32 : 2915 – 20 .
55. Deyo RA , Mirza SK , Martin BI , et al. Trends, major medical com-plications and charges associated with surgery for lumbar spinal stenosis in older adults . JAMA 2010 ; 303 ( 13 ): 1259 – 65 .
56. Park DK , An HS , Lurie JD , et al. Does multilevel lumbar steno-sis lead to poorer outcomes? A subanalysis of the Spine Patient Outcomes Research Trial (SPORT) lumbar stenosis study . Spine 2010 ; 35 : 439 – 46
57. Jansson KA , Németh G , Granath F , et al. Health-related quality of life (EQ-5D) before and one year after surgery for lumbar spinal stenosis . J Bone Joint Surg Br 2009 ; 91 ( 2 ): 210 – 6 .
58. Fischgrund JS , Mackay M , Herkowitz HN , et al. Degenerative lum-bar spondylolisthesis with spinal stenosis: a prospective, random-ized study comparing decompressive laminectomy and arthrod-esis with and without spinal instrumentation . Spine 1997 ; 22 ( 24 ): 2807 – 12 .
59. Herkowitz HN , Kurz LT . Degenerative lumbar spondylolisthesis with spinal stenosis: a prospective study comparing decompression with decompression and intertransverse process arthrodesis . J Bone Joint Surg Am 1991 ; 73 ( 6 ): 802 – 8 .
60. Grob D , Humke T , Dvorak J . Degenerative lumbar spinal stenosis: decompression with and without arthrodesis . J Bone Joint Surg Am 1995 ; 77 ( 7 ): 1036 – 41 .
61. Abdu WA , Lurie JD , Spratt KF , et al. Degenerative spondylolisthe-sis. Does fusion method infl uence outcome? Four-year results of the Spine Patient Outcomes Research Trial . Spine 2009 ; 34 : 2351 – 60 .
62. Thomsen K , Christensen FB , Eiskjaer SP , et al. The effect of pedicle screw instrumentation on functional outcome and fusion rates in posterolateral lumbar spinal fusion: a prospective randomized clini-cal study . Spine 1997 ; 22 ( 24 ): 2813 – 22 .
63. Fritzell P , Hagg O , Nordwall A . Swedish Lumbar Spine Study Group. Complications in lumbar fusion surgery for chronic low back pain: comparison of three surgical techniques used in a pro-spective randomized study . Eur Spine J 2003 ; 12 ( 2 ): 178 – 89 .
64. Mirza SK , Deyo RA , Heagerty PJ , et al. Development of an index to characterize the “invasiveness” of spine surgery: validation by comparison to blood loss and operative time . Spine 2008 ; 33 ( 24 ): 2651 – 61 .
65. Moojen WA , Arts MP , Brand R , et al. The Felix-trial. Double-blind randomization of interspinous implant or bony decompression for treatment of spinal stenosis related intermittent neurogenic claudi-cation . BMC Musculoskelet Disord 2010 ; 27 ( 11 ): 100 .
66. Carragee EJ , Deyo RA , Kovacs FM , et al. Clinical research. Is the spine fi eld a mine fi eld? Spine 2009 ; 34 : 423 – 30 .
67. Kohles SS , Kohles DA , Karp AP , et al. Time-dependent surgical out-comes following cauda equina syndrome diagnosis. Comments on a meta-analysis . Spine 2004 ; 29 : 1281 – 7 .
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
BRS204382.indd E1351BRS204382.indd E1351 25/08/11 11:52 PM25/08/11 11:52 PM