surgery hernia
TRANSCRIPT

Mohammed Al-Saffar
SURGICAL MANAGEMENT OF
INGUINAL HERNIAS
RAMKUMAR

HERNIA
• A hernia is defined as an abnormal protrusion of an organ or tissue through a defect in its surrounding walls.
• Groin hernia
• Inguinal
• Direct
• Indirect
• femoraL

EPIDEMIOLOGY
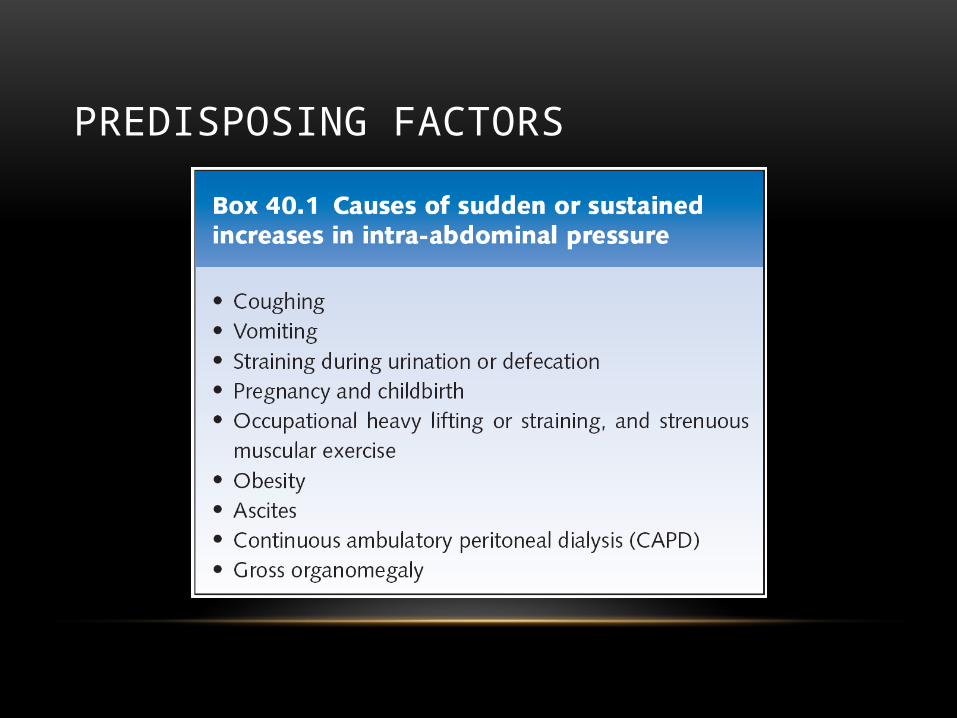
PREDISPOSING FACTORS
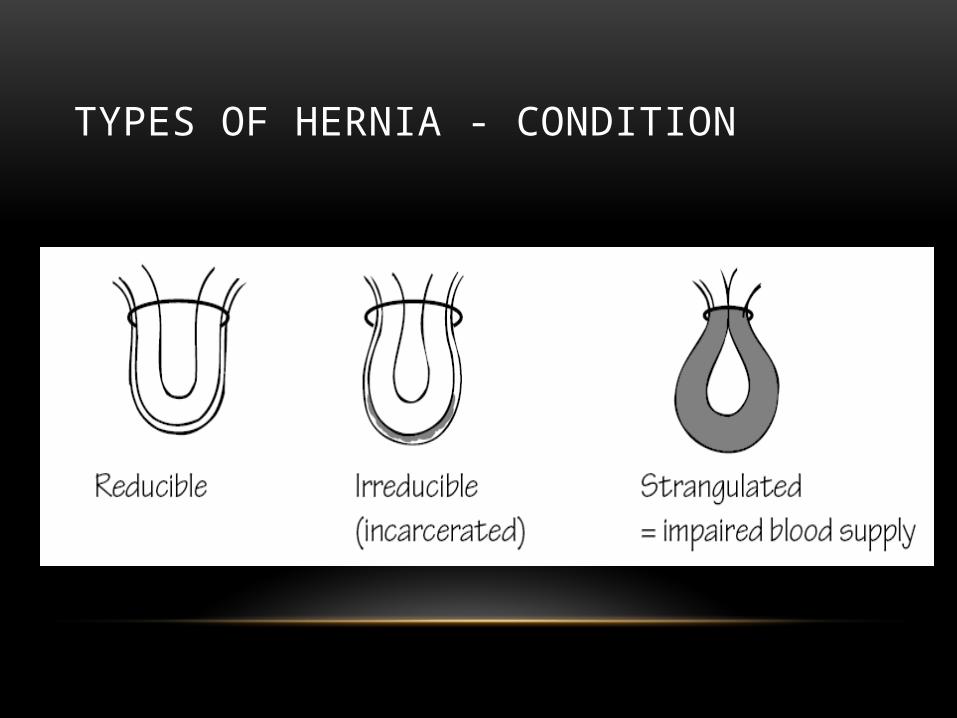
TYPES OF HERNIA - CONDITION
INGUINAL CANAL ANATOMY
• The inguinal canal is an oblique space measuring 4 cm in length that lies above the medial half of the inguinal ligament.
• Inguinal canal has 4 walls : anterior, posterior, roof, and floor



CONTENTS OF THE INGUINAL CANAL
• Males : spermatic cord and ilioinguinal nerve
• Females : round ligament and the ilioinguinal nerve
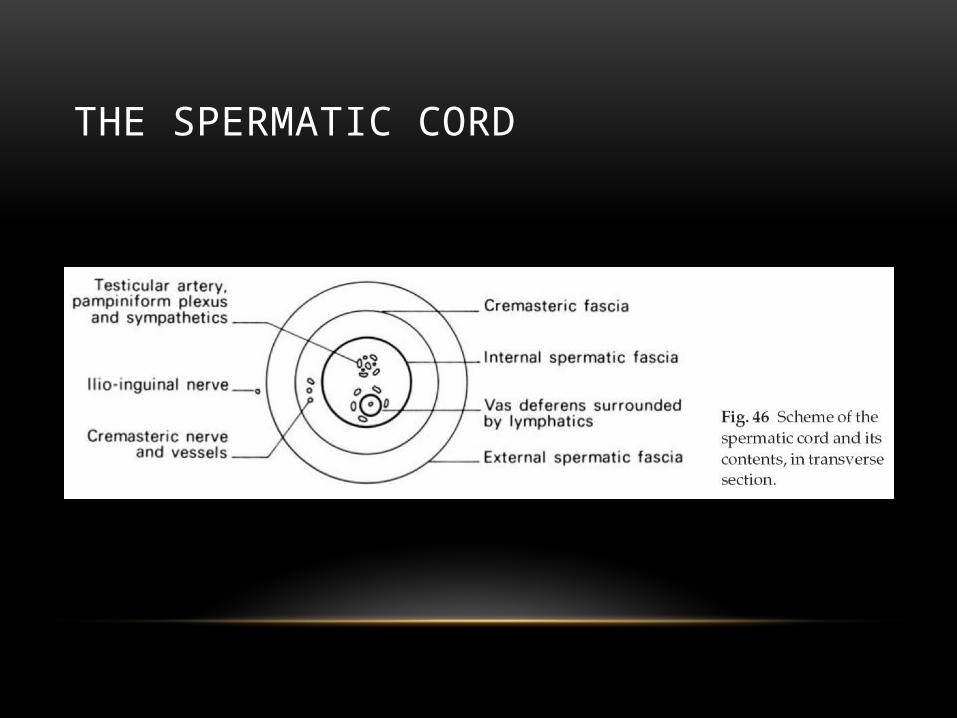
THE SPERMATIC CORD
MANAGEMENT
• Uncomplicated hernias require either :
• No treatment
• Support with a truss
• Operative treatment
• complicated hernias :
• always require surgery, often urgently.
SURGICAL APPROACHES
• For any hernia the surgical option comprises 2 components :
• Herniotomy
• Herniorrhaphy or hernioplasty
• It is either :
• Open repair
Bassini repair
Shouldice repair
Tension free mesh repair
• Laparascopic repair

COMPONENTS OF THE HERNIA
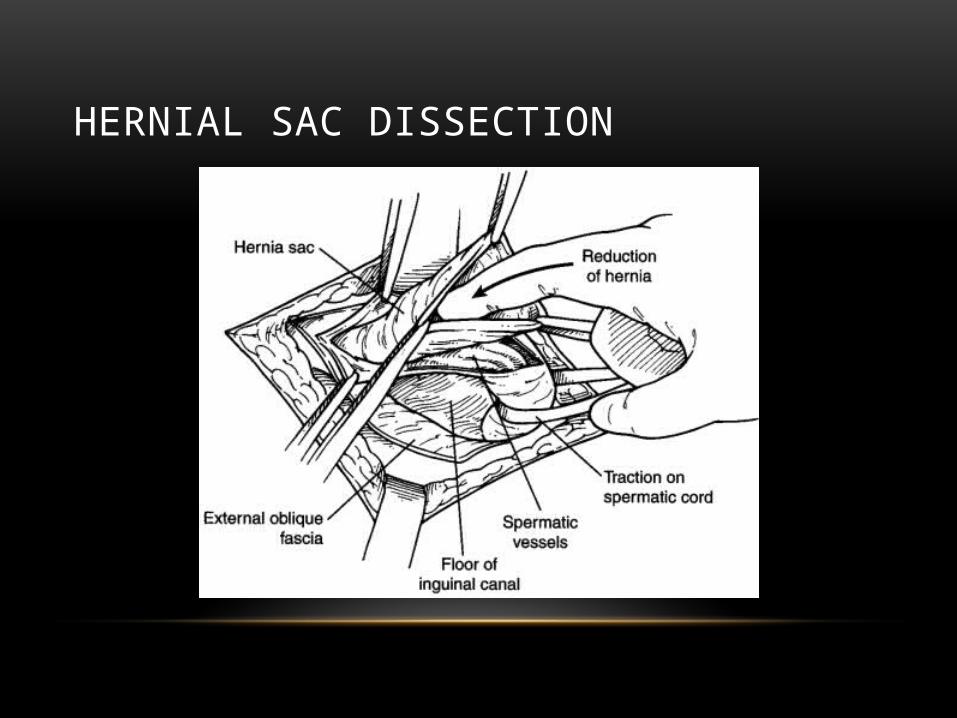
HERNIAL SAC DISSECTION
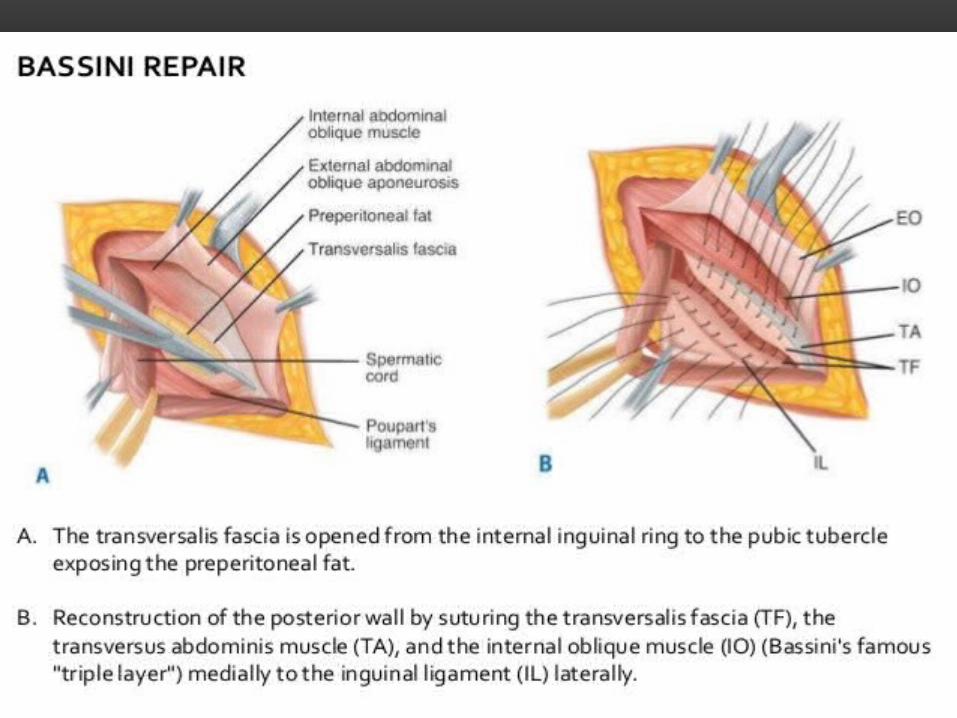
BASSINI REPAIR• The Bassini technique is a "tension" repair, in which the
edges of the defect are sewn back together, without any mesh.The conjoined tendon is retracted upward
• the aponeurosis of the transversus abdominis muscle is approximated to the iliopubic tract that lies adjacent to the inguinal ligament with several interrupted 3-0 silk sutures.
• The second layer of the repair involves suturing the conjoined tendon to the inguinal ligament with interrupted 2-0 silk sutures.
• This suture line extends from the pubic tubercle to the medial border of the internal ring.
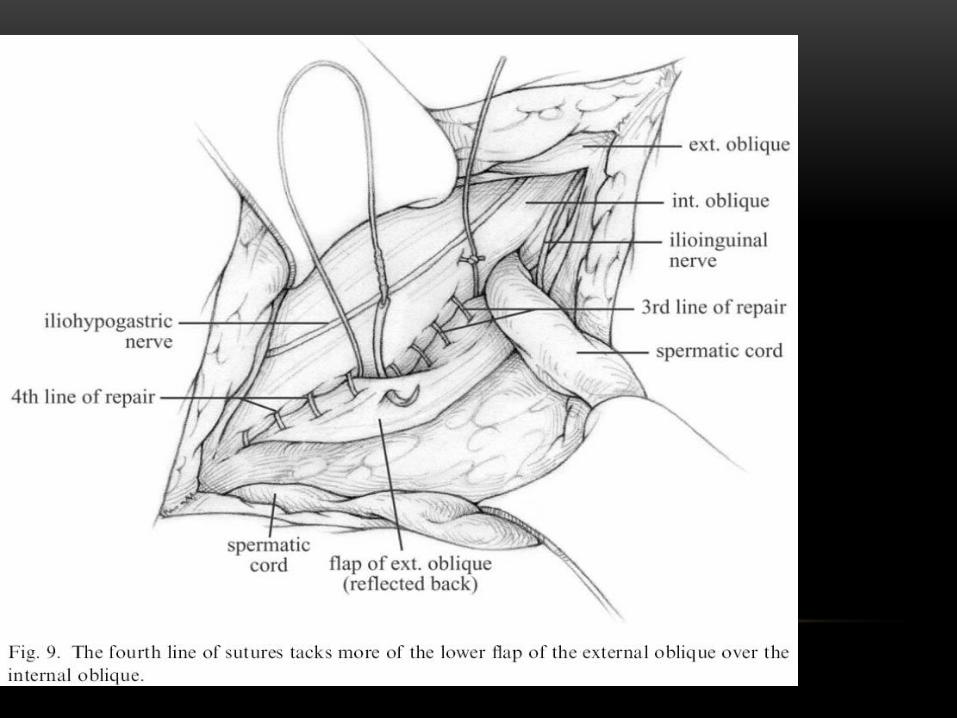
SHOULDICE REPAIR
• With a no. 15 scalpel an incision is made in the transversalis fascia. This incision is extended from the internal ring to the pubic tubercle.
• The repair involves placing four lines of sutures.
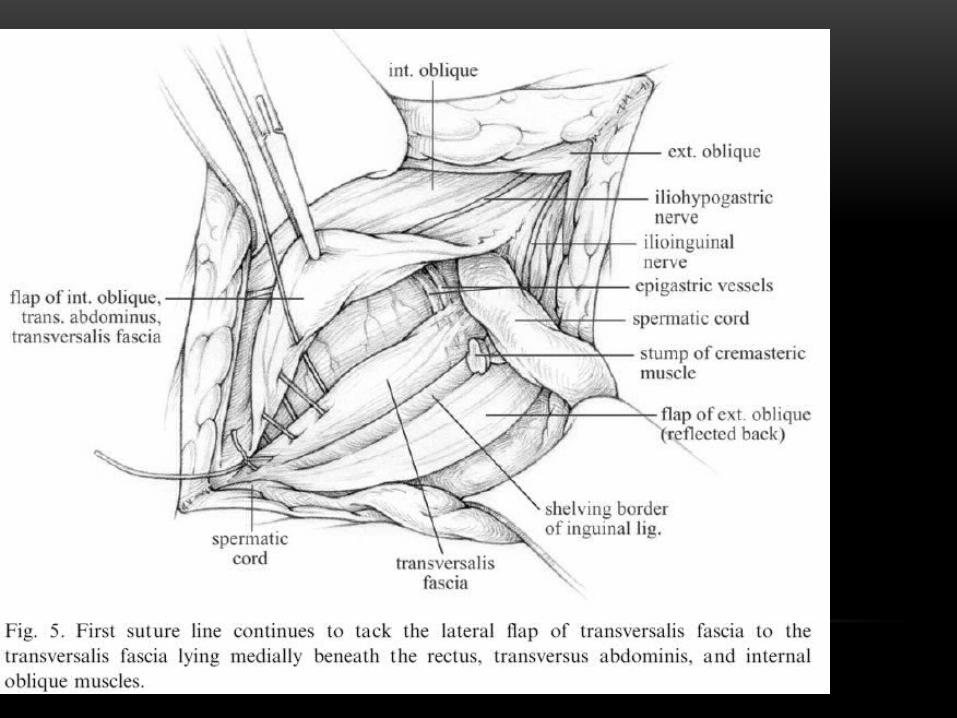
• The first suture line
• is started at the pubic tubercle using 3-0 continuous polypropylene, and the white line is approximated to the free edge of the inferior transversalis fascial flap.

SHOULDICE REPAIR
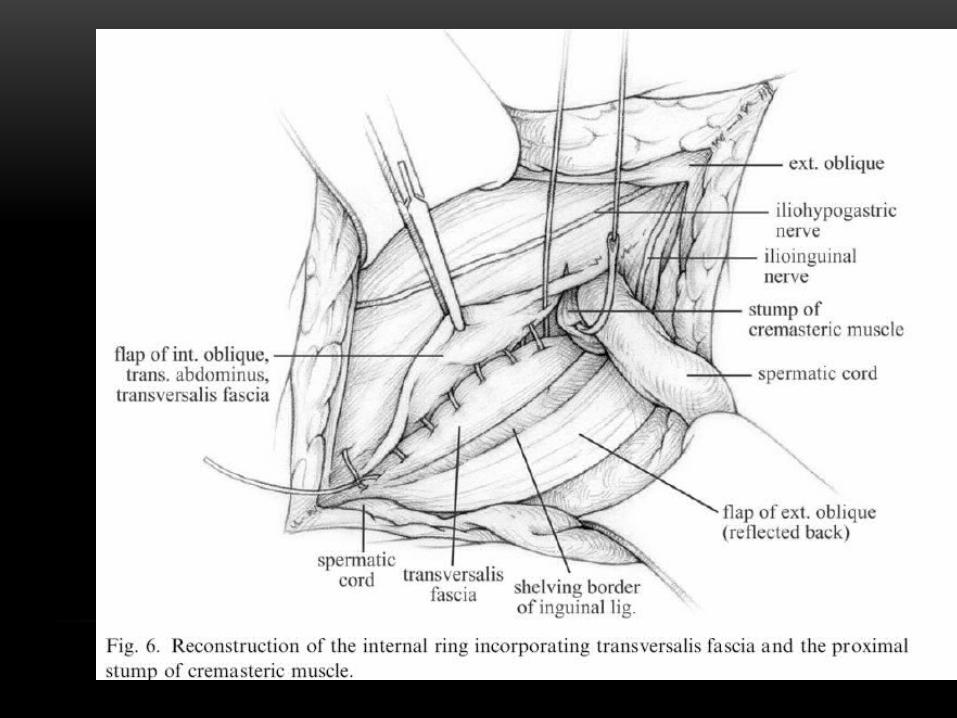
• The 2nd suture line :
• At the internal ring the suture is tied and then continued medially by approximating the free edge of the superior flap to the shelving edge of the inguinal ligament. When the pubic tubercle is reached, the suture is tied and divided.
• The third suture line is started at the level of the internal ring where the conjoined tendon is approximated to the inguinal ligament and tied when the pubic tubercle is reached.
• Using the same suture, the fourth suture line attaches these same structures to one another and is tied at the level of the internal ring.


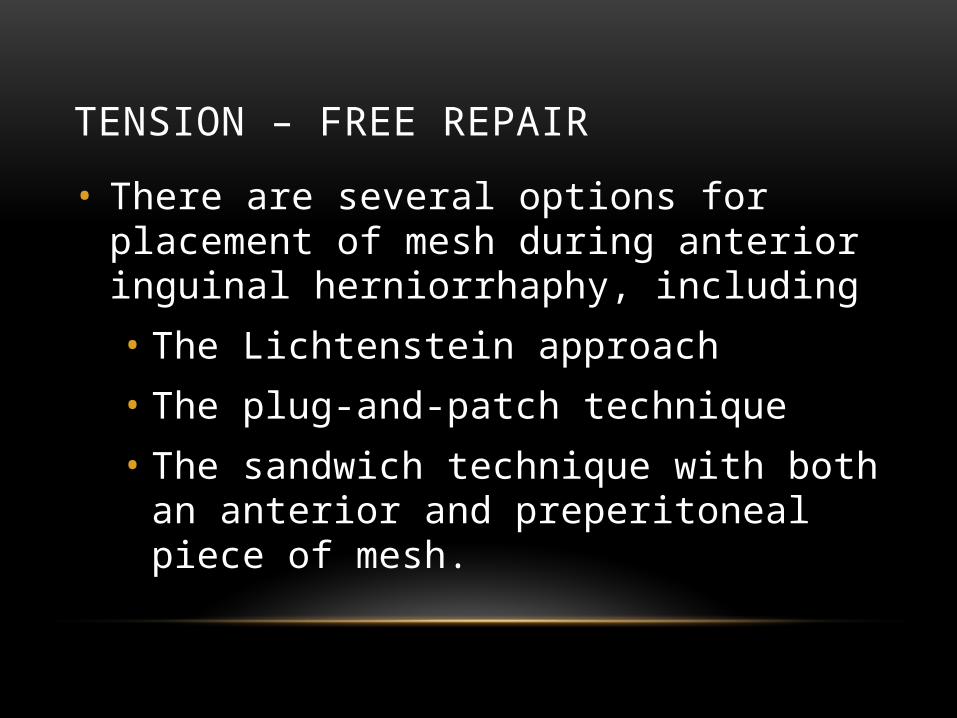
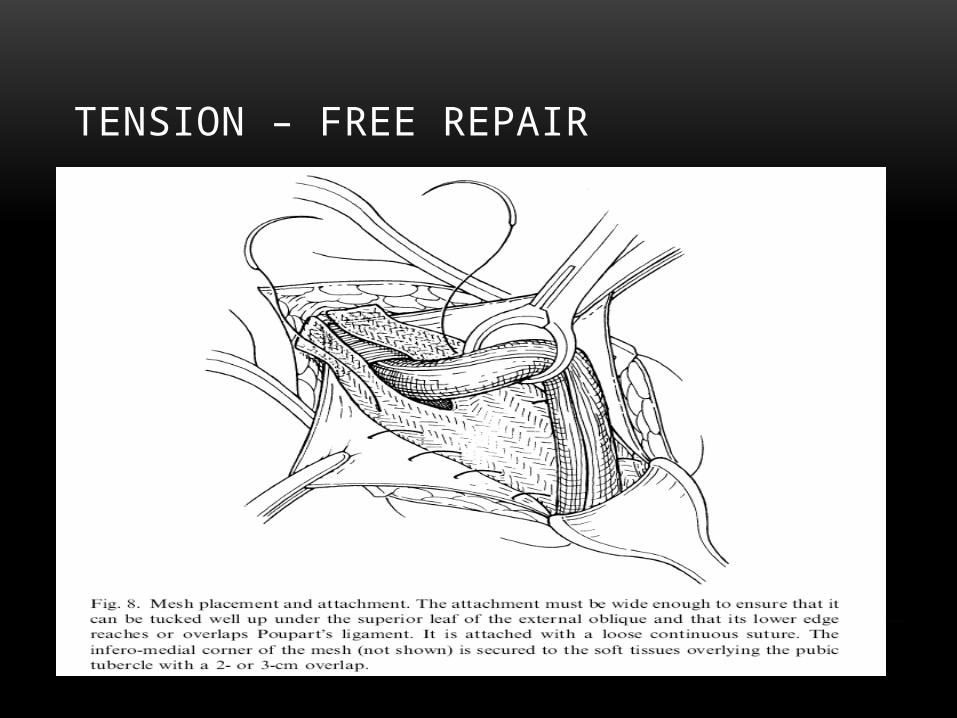
TENSION – FREE REPAIR
• There are several options for placement of mesh during anterior inguinal herniorrhaphy, including
• The Lichtenstein approach
• The plug-and-patch technique
• The sandwich technique with both an anterior and preperitoneal piece of mesh.
TENSION – FREE REPAIR

TENSION – FREE REPAIR
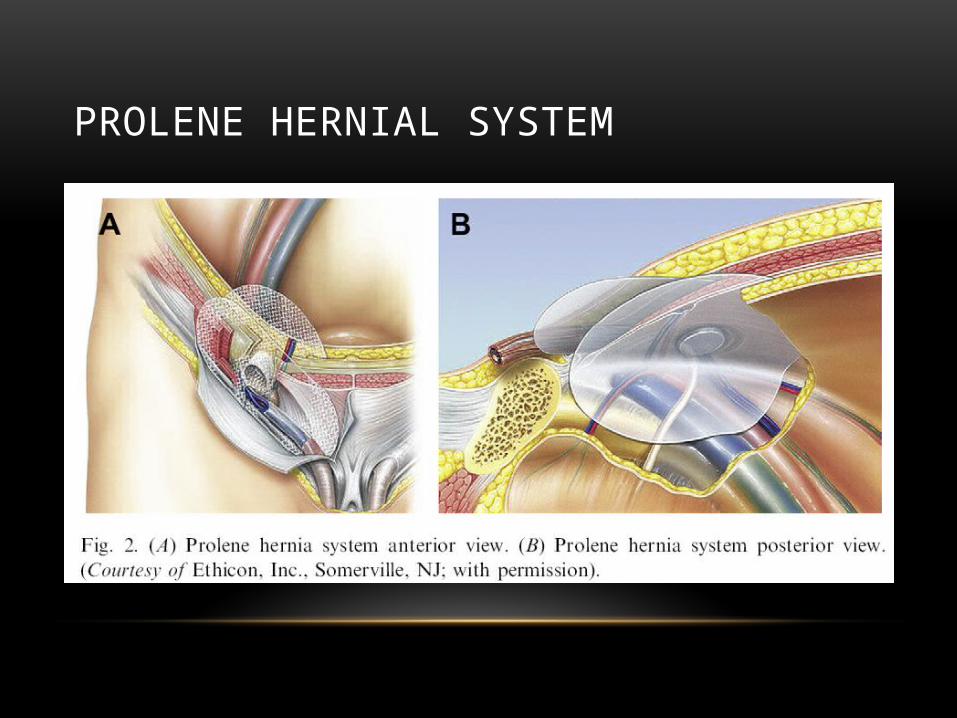
PROLENE HERNIAL SYSTEM
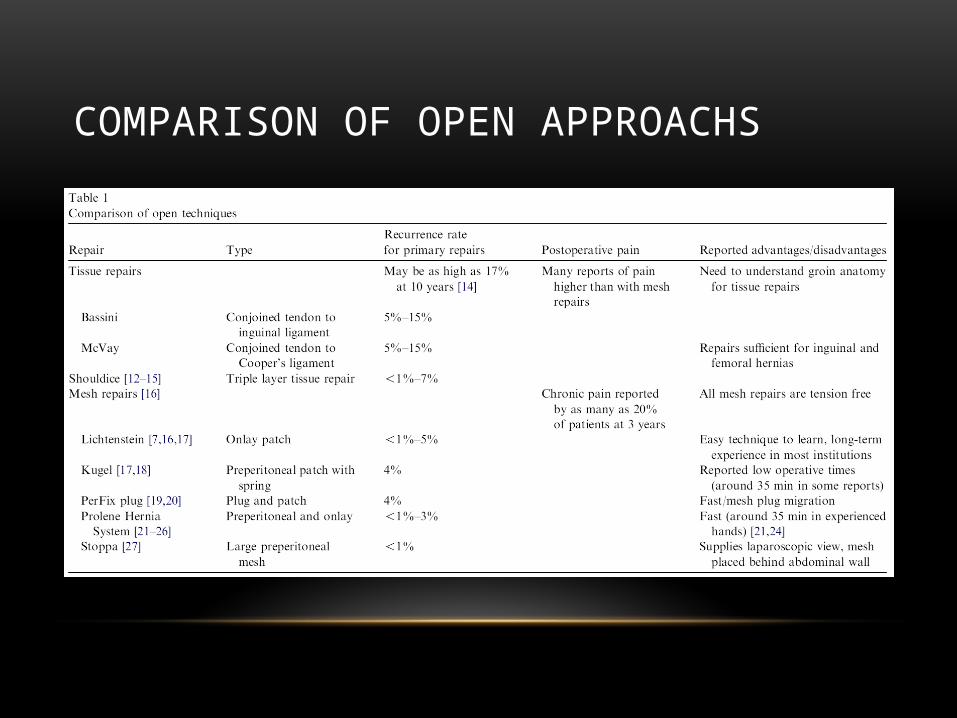
COMPARISON OF OPEN APPROACHS
INDICATIONS FOR LAPAROSCOPIC REPAIR
• Bilateral inguinal hernia
• When the diagnosis of inguinal hernia is uncertain
• When the patient want to return to normal physical life
Laparoscopic repair is done by 2 approaches :
1. Transabdominal preperitoneal “TAPP”
2. Totally extraperitoneally “TEP”

CONTRAINDICATIONS
• The patient medical condition makes general anesthesia more risky
• Patient who have planned pelvic or extraperitoneal operations (eg, radical prostatectomy)
• Patient who have had a recurrence from a prior laparoscopic repair
• Patient presented with strangulated hernia
• Less acute postoperative pain
• Shorter convalescence
• Earlier return to work
• increased risk of femoral nerve injury and
• Increased risk of spermatic cord damage
• risk of developing intraperitoneal adhesions with the TAPP
• greater cost and duration of the operation
ADVANTAGES DISADVANTAGES

TRANSABDOMINAL PREPERITONEAL
• The TAPP approach, first described by Arregui and colleagues in 1992
• It requires laparoscopic access into the peritoneal cavity and placement of mesh in the preperitoneal space after reducing the hernia sac.

TOTALLY EXTRAPERITONEALLY
• The first TEP inguinal hernia repair was described by McKernan and Laws in1993.
• This approach involves preperitoneal dissection and mesh placement without entering into the abdominal cavity.

THE MERCEDES BENZ SIGN
COMPLICATION
• Urinary retention
• Nerve injury
• Testicular ischemia and atrophy
• Injury to vas deferens
• recurrence

Thank You