supporting breastfeeding in the hospital breastfeeding education copyright © 2007 georgia chapter,...
TRANSCRIPT

Supporting Breastfeeding
in the Hospital
Breastfeeding Education
Copyright © 2007 Georgia Chapter, American Academy of Pediatrics. All rights reserved.

Faculty Disclosure Information
In accordance with ACCME* standards for commercial support, all faculty members are required to disclose to the program audience any real or apparent conflict(s) of interest to the content of their presentation. I would like to disclose the following:
* Accreditation Council for Continuing Medical Education

Program Objectives
•Examine current hospital breastfeeding policies and promote the use of evidence based guidelines
•Emphasize mother/ infant bonding by avoiding separation of mother and baby
•Define the 10 steps to successful breastfeeding.

EPIC Breastfeeding Program Partners
• Georgia Chapter – American Academy of Pediatrics
• Georgia OB/GYN Society• American Academy of Family
Physicians• Georgia Department of Public Health• Centers for Disease Control (CDC)

Supportive Research
• Healthy People 2020
• Baby Friendly Initiative
• CDC’s Guide to Breastfeeding Interventions
• Academy of Breastfeeding Medicine
• Policy Statements– American Academy of Pediatrics– OB/GYN Society– Family Practice Physicians
• Surgeon General’s “Call to Action” to Support Breastfeeding

Benefits for Mom
• Reduces risk of postpartum hemorrhage• Reduced risk of cardiovascular disease• Promotes uterine involution and weight
loss• Decreases incidence of breast and uterine cancer• Enhances bonding• Decreases postpartum depression• Saves money
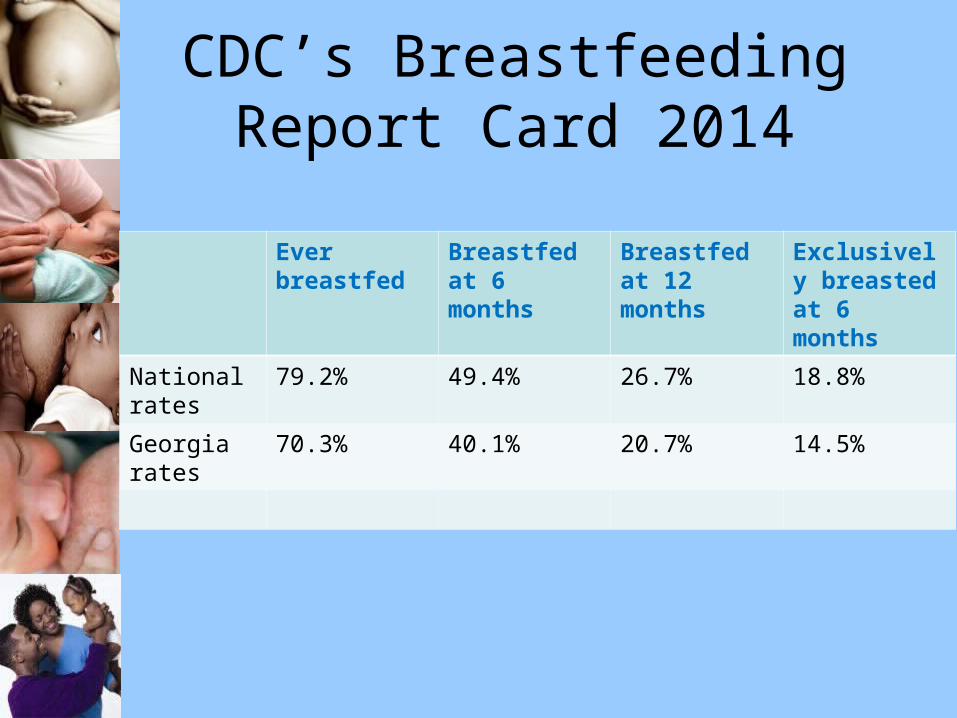
CDC’s Breastfeeding Report Card 2014
Ever breastfed
Breastfed at 6 months
Breastfed at 12 months
Exclusively breasted at 6 months
National rates
79.2% 49.4% 26.7% 18.8%
Georgia rates
70.3% 40.1% 20.7% 14.5%

Childhood illness and disease risk reduction with breastfeeding

Obstacles to Breastfeeding
• Lack of knowledge among parents and staff
• Inconsistent messages/advice
• Disruptive hospital policies
• Lack of adequate follow-up

Baby Friendly 10 Steps1. Have a written breastfeeding policy that us routinely
communicated to all health care staff.
2. Train all healthcare staff in skills necessary to implement this policy.
3. Inform all pregnant women about the benefits and management of breastfeeding.
4. Help mothers initiate breastfeeding within one hour of birth.
5. Show mothers how to breastfeed and how to maintain lactation, even if they are separated from their infants.

10 steps - continued
6. Give newborn infants no food or drink other than breastmilk, unless medically indicated.
7. Practice “rooming-in” – allow mothers and infants to remain together 24 hours a day.
8. Encourage breastfeeding on demand.
9. Give no pacifiers or artificial nipples to breastfeeding infants.
10. Foster the establishment of breastfeeding support groups and refer mothers to them on discharge from the hospital or clinic.

You need buy-in from staff

Stakeholders
• Physicians• Labor and delivery staff• Postpartum staff• Administrators• Lactation staff• Health educators• Quality assurance personnel

Joint Commission
• Exclusive breastfeeding is a “Core Measure”– document breastfeeding exclusivity– supplement ONLY if medically indicated– mother “changing her mind” is not cause
to abandon exclusive breastfeeding but highlights need for breastfeeding support

Prenatal Breastfeeding Education
• Monitor breast changes and provide encouragement
• All providers are responsible for encouraging breast milk feedings
• Breastfeeding classes for mom and her support person
• Breastfeeding materials, free of formula advertisements

Staff Training
• Policy training for all new staff• Periodic breastfeeding trainings
– lunch and learns– online breastfeeding education– conferences/workshops
• 18 hours of training for mother/baby staff
• Three hour physician training
Breastfeeding Champions

Breast or formula
• What does the mom really want to do?– breastfeed– formula feed– both?

After Delivery Skin to Skin

Skin to Skin
• Educate staff / parents on benefits • Baby placed between the breasts
– better temperature regulation– normalizes breathing and heart rate– procedures done skin to skin– prevents hypoglycemia– assist with breastfeeding
www.skintoskincontact.com

Delay Procedures

Rooming-in
• 24 hour rooming-in is encouraged• Physicals, weight checks, hearing
screenings are done in mother’s room– facilitates questions from the mother– minimal infant separation
• Limit visitors
Some hospitals have a quiet time, no visitors for
several hours in the afternoon so that mom and
baby can get rest and practice breastfeeding.

Getting Started
• Assist with breastfeeding at delivery• Teach mother:
– positioning– latch– feeding cues– hand expression– signs of sufficient intake

Exclusive Breastfeeding
• No food or drink other than breast milk• Mothers own milk is the first choice• No promotion of breast milk
substitutes, bottles or pacifiers given to parents.
• Supplement only when necessary

Risks of Supplementing
• Interferes with the establishment of maternal milk supply
• Increased risk of engorgement• May cause nipple confusion• Alters infant bowel flora• Undermines maternal confidence in her
ability to provide her baby with sufficient milk
• Shortened duration of exclusive breastfeeding

Teaching Effective Breastfeeding
•Audible swallowing•Appropriate out put – urine/stools•Adequate weight gain

Staff Documentation
• Observe a feeding once per 8 hours
• Ask mom, “How does it feel”
• Check wet diapers and stools
• Check LATCH
LATCH Score• L - latch on• A - audible swallowing• T - type of nipple• C - comfort level• H - hold
Each of these 5 things are rated from 0-2 and then totaled. (Similar to an
apgar) If a mother has a score of ≤ 7 the mother will need further assistance.
What makes more milk????
Removing milk from
the Breasts!

Reasons to supplement
• Maternal Medication– Most medications are compatible– Weigh benefit of breastfeeding vs. risks
of medications• Excessive weight loss• Hypoglycemia• Jaundice
Every hospital should have a written policy on supplementing
Maternal Medications
• Hale’s Medication and Mother’s Milk• Lactmed
@http://toxnet.nlm.nih.gov/cgi-bin/sis/htmlgen?LACT
• Poison Control 1.800.222.1222• Rarely necessary to interrupt breastfeeding• Short list of contraindicated medications
LithiumPhenindioneRadioactive CompoundsRetinoidsTetracyclines (chronic use >3weeks)
AmiodaroneChemotherapy agentsChloramphenicolDrugs of AbuseErgotamineGold salts

Separation of mother and baby
• Encourage early and frequent pumping
• Pumping frequency every 2-3 hours• Bonding is encouraged
– Skin to skin– Pumping at baby’s bedside– Pump rental information
Hand expression has been proven to increase milk supply
Infant in NICU
Encourage skin-to-skin (Kangaroo)– promotes better oxygen levels– increases mom’s milk production– baby’s temperature is
regulated
Dad can “Kangaroo” too

Barriers
• No buy-in from administration• Lack of staff support• Inconsistent information• Formula distribution/advertisement• Formula bags• Financial costs

Discharge “gifts”
• Do they have formula samples in them?• Do they support breastfeeding?• Ban the Bags

Discharge Instructions
• Instruct mom on signs of sufficient intake– wet diapers– changes in stool color
• Frequent feedings are common
– 8-12 feedings in 24 hours – cluster feeding
• Give mom realistic expectations
Follow-up• Baby should see the pediatrician 1-2
days after discharge• Provide telephone number for
breastfeeding questions• Provide mom with information about
where and how to get a breast pump• Provide a list of community lactation
support– WIC– LaLeche League
WIC Formula feeding package

WIC Breastfeeding Mothers Food Package
What do you tell a mother who ask that her baby remain in the nursery at night so she can sleep?

What do you say to the mother who says she doesn’t have milk or it’s not sufficient?

Your patient says that she is going to breastfeed but has to go back to work and wants to get her baby used to the bottle. What is your response to her?

“While breastfeeding may not seem the right choice for every parent, it is the best
choice for every baby.”