summary of benefits - selecthealth advantage · 1 summary of benefits wasatch essential, wasatch...
TRANSCRIPT

1
Summary of BenefitsWasatch Essential, Wasatch Enhanced, Southwest and Central Utah, Cache Valley.

2
Our Plan. Your Advantage.
> $0 or low monthly premium
> $0 medical deductible
> $0 copay for all Medicare-covered preventive services
> $0 copay for annual comprehensive wellness visit
> Hearing aid benefits where available
> Well eye exams and refraction coverage
> Urgent care covered nationwide
> Emergency care coverage worldwide
> No referrals required
> We handle prior authorizations for you
> Up to $240 reimbursement annually towards wellness activities
> Earn rewards of up to $50 for healthy behaviors
> Local customer service
> Engaged providers committed to improving healthcare and
reducing costs
H1994_8361772_UT Accepted

3
SUMMARY OF BENEFITS
January 1, 2018 to December 31, 2018.This booklet gives you a summary of SelectHealth Advantage (HMO)
and what we cover and what you pay. It doesn’t list every service we
cover or list every limitation or exclusion. To get a complete list of
services we cover, call us and ask for the “Evidence of Coverage.”
You Have Choices About How To Get Your Medicare Benefits
> Option one. Get your Medicare benefits through Original
Medicare (fee-for-service Medicare). Original Medicare is run
directly by the Federal government.
> Option two. Get your Medicare benefits by joining a Medicare
health plan, such as SelectHealth Advantage.
If you want to know more about the coverage and costs of Original
Medicare, look in your current “Medicare & You” handbook. View
it online at medicare.gov or get a copy by calling 800-MEDICARE (800-633-4227), 24 hours a day, 7 days a week. TTY users, please
call 877-486-2048.
SECTIONS IN THIS GUIDE
> Things to Know About SelectHealth Advantage
> Monthly Premium, Deductible, and Limits on How Much You
Pay for Covered Services
> Covered Medical and Hospital Benefits
> Prescription Drug Benefits
> Optional Benefits (you must pay an extra premium for
these benefits)
This guide is available in other formats such as Braille and
large print.
This guide may be available in a non-English language. For
additional information, call us at 855-442-9940 (TTY: 711).
Este guía puede estar disponible en un lenguaje que no sea inglés.
Para información adicional, llámenos al 855-442-9940 (TTY: 711).
ATTENTION: If you speak Spanish, language assistance services,
free of charge, are available to you. Call 1-855-442-9900
(TTY: 711).
SelectHealth is an HMO plan sponsor with a Medicare
contract. Enrollment in SelectHealth Advantage depends on
contract renewal.
HOW TO CONTACT US
SelectHealth Advantage Phone Numbers and Website
> Call Member Services toll-free at 855-442-9940 (TTY: 711) or
visit our website at selecthealthadvantage.org.
Hours of Operation
> October 1 to February 14, weekdays 7:00 a.m. to 8:00 p.m.,
Saturday and Sunday from 8:00 a.m. to 8:00 p.m.
Mountain time.
> February 15 to September 30, weekdays 7:00 a.m. to
8:00 p.m., Saturday from 9:00 a.m. to 2:00 p.m. Mountain
time, closed Sunday.
> Outside of these hours of operation, please leave a message
and your call will be returned within one business day.

4
SUMMARY OF BENEFITS
WHO CAN JOIN?
To join SelectHealth Advantage (HMO), you must be enrolled in
Medicare Part A and Part B and live in our service area.
These are our service areas:
> Wasatch service area, which includes: Davis, Morgan, Salt
Lake, Summit, Utah, Wasatch, and Weber counties in Utah
> Southwest and Central Utah service area, which includes
Garfield, Iron, Sanpete, Sevier, and Washington counties in Utah
> Cache Valley service area, which includes: Box Elder, Cache,
and Rich counties in Utah, and Franklin County in Idaho
WHICH DOCTORS, HOSPITALS, AND PHARMACIES CAN I USE?
SelectHealth Advantage has a network of doctors, hospitals,
pharmacies, and other providers. If you use providers that are not
in our network, the plan may not pay for these services.
You must generally use network pharmacies to fill your
prescriptions for covered Part D drugs.
You can see our most up-to-date provider directory on our
website selecthealthadvantage.org.
You can see our most up-to-date pharmacy directory on our
website selecthealthadvantage.org.
Or, call us and we will send you a copy of the Provider and
Pharmacy Directories.
WHAT DO WE COVER?
Our plan members get more than what is covered by Original Medicare. Some of the extra benefits are outlined in this booklet.
We cover Part D—that’s the part for prescription drugs. Plus, we
cover drugs covered in Part B, such as chemotherapy and some
medications prescribed by your provider.
You can see the complete plan formulary (list of Part D
prescription drugs) and any restrictions on our website,
selecthealthadvantage.org.
Or, call us and we will send you a copy of the formulary.

5
SUMMARY OF BENEFITS
HOW WILL I DETERMINE MY DRUG COSTS?
Our plan groups each medication into one of five “tiers.” You
will need to use a current SelectHealth Advantage formulary to
locate which tier your drug is on to determine how much it will
cost you. Generic drugs fall into tiers one and two. The amount
you pay depends on the drug’s tier and what stage of the benefit
you have reached. Later in this document, we discuss the benefit
stages that occur: Deductible, Initial Coverage, Coverage Gap,
and Catastrophic Coverage.
REFERRALS NOT REQUIRED
With SelectHealth, there is no gatekeeper of services and no
referrals—you can see any in-network provider, when you need to.
PRIOR AUTHORIZATION
We require prior approval for some services. This approval is called
Prior Authorization or Preauthorization. Participating providers
will typically get it for you, but if you are seeing a nonparticipating
provider, you may need to get it yourself. Once prior authorization
is submitted to us, we generally process the request in one to
two days, but it can take up to 14 days. For any decision we make
regarding the prior authorization, you and your provider will
receive a notification in writing.
MONTHLY PREMIUM, DEDUCTIBLE, AND LIMITS ON HOW MUCH YOU PAY FOR COVERED SERVICES
How much is the monthly premium? Please refer to the
Premium/Cost-Sharing Table to find out the premium/cost-
sharing in your area.
Is there any limit on how much I will pay for my covered services? Yes. Like all Medicare health plans, our plan protects
you by having yearly limits on your out-of-pocket costs for
medical and hospital care. See Member Out-of-Pocket Maximum
on page 16.
6
SUMMARY OF BENEFITS | WASATCH AREA
MONTHLY PREMIUM, DEDUCTIBLE, AND LIMITS ON HOW MUCH YOU PAY FOR COVERED SERVICES
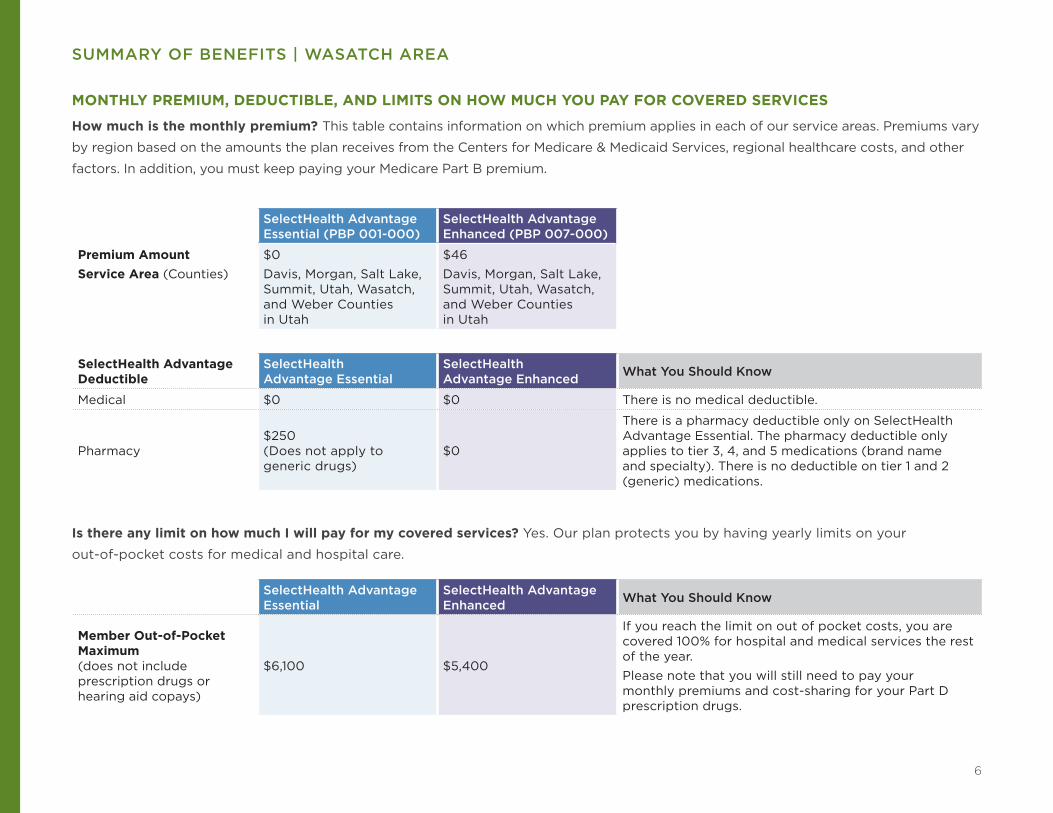
How much is the monthly premium? This table contains information on which premium applies in each of our service areas. Premiums vary
by region based on the amounts the plan receives from the Centers for Medicare & Medicaid Services, regional healthcare costs, and other
factors. In addition, you must keep paying your Medicare Part B premium.
SelectHealth Advantage Essential (PBP 001-000)
SelectHealth Advantage Enhanced (PBP 007-000)
Premium Amount Service Area (Counties)
$0Davis, Morgan, Salt Lake, Summit, Utah, Wasatch, and Weber Counties in Utah
$46Davis, Morgan, Salt Lake, Summit, Utah, Wasatch, and Weber Counties in Utah
SelectHealth Advantage Deductible
SelectHealth Advantage Essential
SelectHealth Advantage Enhanced What You Should Know
Medical $0 $0 There is no medical deductible.
Pharmacy$250 (Does not apply to generic drugs)
$0
There is a pharmacy deductible only on SelectHealth Advantage Essential. The pharmacy deductible only applies to tier 3, 4, and 5 medications (brand name and specialty). There is no deductible on tier 1 and 2 (generic) medications.
SelectHealth Advantage Essential
SelectHealth Advantage Enhanced What You Should Know
Member Out-of-Pocket Maximum (does not include prescription drugs or hearing aid copays)
$6,100 $5,400
If you reach the limit on out of pocket costs, you are covered 100% for hospital and medical services the rest of the year.Please note that you will still need to pay your monthly premiums and cost-sharing for your Part D prescription drugs.
Is there any limit on how much I will pay for my covered services? Yes. Our plan protects you by having yearly limits on your
out-of-pocket costs for medical and hospital care.

7
SUMMARY OF BENEFITS | WASATCH AREA
COVERED MEDICAL AND HOSPITAL BENEFITS
Benefit / Description SelectHealth Advantage Essential $0
SelectHealth Advantage Enhanced $46 What You Should Know
Inpatient Hospital Coverage1 $295 copay per day for days 1 through 6$0 copay for days 7 and beyond
$280 copay per day for days 1 through 5$0 copay for days 6 and beyond
Our plan covers an unlimited number of days for an inpatient hospital stay.These copays start over each time you are admitted to an inpatient hospital facility.
Outpatient Facility Coverage1
Outpatient surgery $300 copay $250 copay
Ambulatory surgical center $300 copay $250 copay
Diagnostic colonoscopy $300 copay $250 copay
IV infusion therapy 20% coinsurance 20% coinsurance
Non-nuclear cardiac stress tests 20% coinsurance 20% coinsurance
Sleep studies 20% coinsurance 20% coinsurance
Other covered services 20% coinsurance 20% coinsurance
Doctor’s Office Visits SelectHealth does not require referrals.If a prior authorization is required, your in network provider—not you—will request the authorization.
$10 copay $5 copayPrimary care physician visit
Specialist visit $50 copay $40 copay
Preventive Care $0 copay $0 copayAll Medicare $0 preventive services are also $0 in our plan. In addition, we cover an annual physical/comprehensive wellness visit at $0.
Emergency Care $80 copay $80 copayIf you are admitted to the hospital within 24 hours, your emergency care copay is waived. You have worldwide emergency coverage.
Urgently Needed Services$50 copay $45 copay
There will be no extra charge for labs and/or x-rays. You have national coverage for urgently needed care. The Urgent Care copay is waived if you are referred to the Emergency Department or admitted inpatient to the hospital within 24 hours for the same condition, you will instead pay the applicable Emergency Services or Inpatient Hospital copay.
1 Service may require prior authorization.

8
SUMMARY OF BENEFITS | WASATCH AREA
COVERED MEDICAL AND HOSPITAL BENEFITS (CONTINUED)
Benefit / Description SelectHealth Advantage Essential $0
SelectHealth Advantage Enhanced $46 What You Should Know
Diagnostic Services, Lab, and Radiology Services, and X-Rays1
Costs for these services may vary based on place of service. Only one lab or diagnostic test copayment is collected when multiple lab tests are performed during the same visit. Services are in addition to any applicable primary care or specialist copay.
Diagnostic radiology services (such as MRIs, CT scans) $300 copay $250 copay
Diagnostic tests and procedures$0 copay or 20% coinsurance, depending on the service
$0 copay or 20% coinsurance, depending on the service
Lab services $0 copay $0 copay
Outpatient x-rays $20 copay $10 copay
Therapeutic radiology services (such as radiation treatment for cancer) 20% coinsurance 20% coinsurance
Hearing ServicesExam to diagnose and treat hearing and balance issuesHearing AidsCopay for each hearing aid
$50 copay
Tier 1 – Essential: $649Tier 2 – Standard: $949Tier 3 – Advanced: $1,249Tier 4 – Premium: $1,649Tier 5 – Platinum: $1,949
$40 copay
Tier 1 – Essential: $649Tier 2 – Standard: $949Tier 3 – Advanced: $1,249Tier 4 – Premium: $1,649Tier 5 – Platinum: $1,949
Selected hearing aids purchased through participating audiology providers are covered under one of five benefit tiers.The copay includes the device, three fitting and adjustment appointments, and a one-year supply of batteries.
Dental Services1 $50 copay $40 copay Limited dental services related to a medical condition.
Vision Services
Exam to diagnose and treat diseases and conditions of the eye
$50 copay $40 copay
Eyeglasses or contact lenses after cataract surgery
$0 copay $0 copay
Routine and non-routine eye exams
Vision test (Refraction)
$50 copay$0 copay
$40 copay$0 copay
1 Service may require prior authorization.

9
SUMMARY OF BENEFITS | WASATCH AREA
Benefit / Description SelectHealth Advantage Essential $0
SelectHealth Advantage Enhanced $46 What You Should Know
Inpatient Mental Health Services1 $260 copay per day for days 1 through 6$0 copay for days 7 through 90$0 copay for lifetime reserve days
$280 copay per day for days 1 through 5$0 copay for days 6 through 90$0 copay for lifetime reserve days
Our plan covers 90 days for an inpatient hospital stay each time you are admitted. Our plan also covers 60 “lifetime reserve days.” These are “extra” days that we cover. If your hospital stay is longer than 90 days, you can use these extra days. But once you have used up these extra 60 days, your inpatient hospital coverage will be limited to 90 days.Our plan covers up to 190 days in a lifetime for inpatient mental health care in a psychiatric hospital. The inpatient hospital care limit does not apply to inpatient mental services provided in a general hospital.
Outpatient Mental Health Services1
Outpatient group therapy visit $40 copay $40 copay
Outpatient individual therapy visit $40 copay $40 copay
Partial hospitalization for mental health $55 copay $55 copay
Skilled Nursing Facility (SNF)1
Our plan covers up to 100 days in a SNF.
$0 copay per day for days 1 through 20$160 copay per day for days 21 through 100
$0 copay per day for days 1 through 20$125 copay per day for days 21 through 100
No prior hospital stay required.
Outpatient Rehabilitation Services1
There is no limitation on the number of occupational, speech, and physical therapy visits.
Physical therapy and speech and language therapy visit $40 copay $30 copay
Occupational therapy visit $40 copay $30 copay
Cardiac (heart) rehab services (for a maximum of 2 one-hour sessions per day for up to 36 sessions up to 36 weeks)
$40 copay $30 copay
Pulmonary rehab services $30 copay $30 copay
1 Service may require prior authorization.

10
SUMMARY OF BENEFITS | WASATCH AREA
COVERED MEDICAL AND HOSPITAL BENEFITS (CONTINUED)
Benefit / Description SelectHealth Advantage Essential $0
SelectHealth Advantage Enhanced $46 What You Should Know
Ambulance1 $225 copay $200 copayCovered ambulance services include fixed wing, rotary wing, and ground ambulance services to the nearest appropriate facility.
Transportation Not Covered Not Covered This would include services such as getting a ride to or from your doctor.
Medicare Part B DrugsIncludes chemotherapy and other Part B drugs1
20% coinsurance 20% coinsurance
Foot Care (podiatry services) $50 copay $40 copayFoot exams and treatment if you have diabetes-related nerve damage and/or meet certain conditions.
Medical Equipment / Supplies
Coverage for glucose monitors and test strips is limited to FreeStyle and Precision Xtra® brands produced by Abbott Labs. If you or your physician feel that it is medically necessary for you to use a different monitor or test strips, call Member Services.
Durable medical equipment (wheelchairs, oxygen, etc.) 1 20% coinsurance 20% coinsurance
Prosthetic devices and supplies (braces, artificial limbs, etc.)1 20% coinsurance 20% coinsurance
Diabetes monitoring supplies $0 copay $0 copay
Diabetes self-management training $0 copay $0 copay
Therapeutic shoe inserts 20% coinsurance 20% coinsurance
Wellness Programs LiveWell Advantage wellness reimbursement Up to $240 Up to $240
You receive reimbursement for up to a combined total of $240 per year for approved services.SelectHealth will reimburse you for eligible expenses.
Chiropractic Care1 $20 copay $20 copayManipulation of the spine to correct a subluxation (when 1 or more of the bones of your spine move out of position).
Home Health Care1 $0 copay $0 copay
1 Service may require prior authorization.

11
SUMMARY OF BENEFITS | WASATCH AREA
Benefit / Description SelectHealth Advantage Essential $0
SelectHealth Advantage Enhanced $46 What You Should Know
Outpatient Substance Abuse
Individual or group therapy in a provider’s office $40 copay per visit $40 copay per visit
Individual or group therapy in an outpatient facility setting $50 copay per visit $50 copay per visit
Over-the-Counter Items Not Covered Not Covered
Renal Dialysis 20% coinsurance 20% coinsurance
HospiceYou pay nothing for hospice care from a Medicare-certified hospice
You pay nothing for hospice care from a Medicare-certified hospice
You may have to pay part of the costs for drugs and respite care. Hospice is covered outside of our plan. Please contact us for more details.
Connect CareIntermountain Connect Care is a convenient service that provides online access for common medical conditions.
$20 copay $20 copay
Intermountain Connect Care is available 7 days a week and can be accessed through your computer or mobile device. Connect Care is not for medical emergencies. Please call 911 or go to the nearest emergency room for any emergency care.
TeleHealth Services $10-50 copay $5-40 copay
SelectHealth offers a supplemental TeleHealth Services benefit that allows plan-approved providers to offer TeleHealth Services to you directly when you are located anywhere nationwide, including through your home computer or on your mobile device.
1 Service may require prior authorization.

12
SUMMARY OF BENEFITS | WASATCH AREA
Benefit / Description SelectHealth Advantage Essential $0 SelectHealth Advantage Enhanced $46
DEDUCTIBLEYou begin in this payment stage, when you fill your first nongeneric prescription of the year. During this stage, you pay the full cost for your brand name and specialty drugs, until you have reached your annual deductible. Generic drugs do not count towards your deductible.
Pharmacy DeductibleTiers 1 and 2 (Generics) $0 $0
Tiers 3, 4, and 5 (Brands) $250 $0
INITIAL COVERAGEDuring this stage, the plan pays its share of the cost of your drugs and you pay your share of the cost.You stay in this stage until the amount of your year-to-date “total drug costs” reaches $3,750. Then, you move to the COVERAGE GAP.
Retail Cost-Sharing One-Month Supply
Two-Month Supply
Three-Month Supply
One-Month Supply
Two-Month Supply
Three-Month Supply
Tier 1 (Preferred Generic) $3 $6 $9 $0 $0 $0
Tier 2 (Generic) $15 $30 $45 $10 $20 $30
Tier 3 (Preferred Brand) $45 $90 $135 $45 $90 $135
Tier 4 (Nonpreferred Brand) $95 $190 $285 $95 $190 $285
Tier 5 (Specialty Tier) 28% coinsurance
Not Offered Not Offered 33% of the cost
Not Offered Not Offered
Mail Order Cost-Sharing One-Month Supply
Two-Month Supply
Three-Month Supply
One-Month Supply
Two-Month Supply
Three-Month Supply
Tier 1 (Preferred Generic) $3 $6 $6 $0 $0 $0
Tier 2 (Generic) $15 $30 $30 $10 $20 $20
Tier 3 (Preferred Brand) $45 $90 $135 $45 $90 $135
Tier 4 (Nonpreferred Brand) $95 $190 $285 $95 $190 $285
Tier 5 (Specialty Tier) 28% coinsurance
Not Offered Not Offered 33% of the cost
Not Offered Not Offered
If you reside in a long-term care facility, you pay the same as at a retail pharmacy.
If you reside in a long-term care facility, you pay the same as at a retail pharmacy.
You may get drugs from an out-of-network pharmacy, but may pay more than you pay at an in-network pharmacy.
You may get drugs from an out-of-network pharmacy, but may pay more than you pay at an in-network pharmacy.
PRESCRIPTION DRUG BENEFITS

13
SUMMARY OF BENEFITS | WASATCH AREA
Benefit / Description SelectHealth Advantage Essential $0 SelectHealth Advantage Enhanced $46
COVERAGE GAP (DONUT HOLE)
You stay in this stage until the amount of your year-to-date “out-of-pocket costs” reaches $5,000.
You generally pay no more than 35% on applicable brand name drugs and 44% on applicable generic / nonapplicable drug cost.
You generally pay no more than 35% on applicable brand name drugs and 44% on applicable generic / nonapplicable drug cost.
CATASTROPHIC COVERAGEDuring this payment stage, the plan pays most of the cost for your covered drugs. You stay in this stage for the rest of the calendar year through December 31, 2018.
$3.35 for generic drugs and $8.35 for all other drugs; or 5% coinsurance, whichever is greater.
$3.35 for generic drugs and $8.35 for all other drugs; or 5% coinsurance, whichever is greater.
OPTIONAL BENEFITS You must continue to pay your Medicare Part B premium and your monthly plan premium, an extra premium will be added each month for these benefits.
PACKAGE 1: $35
SelectHealth Dental Comprehensive Benefit
Benefits include: Preventive dental care, and Comprehensive dental care.
How much is the monthly premium? Additional $35 per month.
How much is the deductible? $0 deductible.
Is there a limit on how much the plan will pay?
Our plan pays up to $1,000 every year and has additional coverage limits for certain benefits. $0 copay for preventive dental services including: Two exams/cleanings with x-rays per year. You pay 50% for all other covered dental services, such as fillings, extractions, root canal, crowns, dentures (rebasing & relining), bridges, and implants.
PACKAGE 2: $40
SelectHealth Dental Comprehensive Plus Eyewear
Benefits include: Preventive dental care, comprehensive dental care, and eyewear.
How much is the monthly premium? Additional $40 per month.
How much is the deductible? $0 deductible.
Is there a limit on how much the plan will pay?
This optional supplemental benefit package offers the same coverage for dental preventive and corrective services as Package #1. You also have a $200 retail value allowance for glasses or contacts at participating locations. See the Evidence of Coverage for more information on these benefits.

14
SUMMARY OF BENEFITS | SOUTHWEST AND CENTRAL, CACHE VALLEY
MONTHLY PREMIUM, DEDUCTIBLE, AND LIMITS ON HOW MUCH YOU PAY FOR COVERED SERVICES
How much is the monthly premium? Please refer to the Premium/Cost-Sharing Table to find out the premium/cost-sharing in your area.
This table contains information on which premium applies in each of our service areas. Premiums vary by region based on the amounts the
plan receives from the Centers for Medicare & Medicaid Services, regional healthcare costs, and other factors. In addition, you must keep
paying your Medicare Part B premium.
Southwest and Central (PBP 002-000)
Cache Valley (PBP 005-000)
Premium Amount Service Area (Counties)
$74Sanpete, Sevier, Iron, Garfield, Washington Counties in Utah
$67Box Elder, Cache, Rich Counties in Utah, and Franklin County in Idaho
SelectHealth Advantage Deductible
Southwest and Central (PBP 002-000)
Cache Valley (PBP 005-000) What You Should Know
Medical $0 $0 There is no medical deductible.
Pharmacy $250 $250 The pharmacy deductible only applies to tier 3, 4, and 5 medications (brand name and specialty). There is no deductible on tier 1 and 2 (generic) medications.
Southwest and Central (PBP 002-000)
Cache Valley (PBP 005-000) What You Should Know
Member Out-of-Pocket Maximum (does not include prescription drugs or hearing aid copays)
$6,700 $6,700
If you reach the limit on out-of-pocket costs, you continue to receive covered hospital and medical services and we will pay the full cost for the rest of the year.Please note that you will still need to pay your monthly premiums and cost-sharing for your Part D prescription drugs.
Is there any limit on how much I will pay for my covered services? Yes. Like all Medicare health plans, our plan protects you by having
yearly limits on your out-of-pocket costs for medical and hospital care.

15
SUMMARY OF BENEFITS | SOUTHWEST AND CENTRAL, CACHE VALLEY
COVERED MEDICAL AND HOSPITAL BENEFITS
Benefit / Description Southwest and Central (PBP 002-000) $74
Cache Valley (PBP 005-000) $67 What You Should Know
Inpatient Hospital Coverage1 $295 copay per day for days 1 through 6$0 copay for days 7 and beyond
$295 copay per day for days 1 through 6$0 copay for days 7 and beyond
Our plan covers an unlimited number of days for an inpatient hospital stay.These copays start over each time you are admitted to an inpatient hospital facility.
Outpatient Facility Coverage1
Outpatient surgery $300 copay $300 copay
Ambulatory surgical center $300 copay $300 copay
Diagnostic colonoscopy $300 copay $300 copay
IV infusion therapy 20% coinsurance 20% coinsurance
Non-nuclear cardiac stress tests 20% coinsurance 20% coinsurance
Sleep studies 20% coinsurance 20% coinsurance
Other covered services 20% coinsurance 20% coinsurance
Doctor’s Office Visits SelectHealth does not require referrals.If a prior authorization is required, your in-network provider—not you—will request the authorization.
$10 copay $10 copayPrimary care physician visit
Specialist visit $50 copay $50 copay
Preventive Care $0 copay $0 copayAll Medicare $0 preventive services are also $0 in our plan. In addition, we cover an annual physical/comprehensive wellness visit at $0.
Emergency Care $80 copay $80 copayIf you are admitted to the hospital within 24 hours, your emergency care copay is waived. You have worldwide emergency coverage.
Urgently Needed Services$50 copay $50 copay
There will be no extra charge for labs and/or x-rays. You have national coverage for urgently needed care. The urgent care copay is waived if you are referred to the emergency department or admitted inpatient to the hospital within 24 hours for the same condition, you will instead pay the applicable emergency services or inpatient hospital copay.
1 Service may require prior authorization.

16
SUMMARY OF BENEFITS | SOUTHWEST AND CENTRAL, CACHE VALLEY
COVERED MEDICAL AND HOSPITAL BENEFITS (CONTINUED)
Benefit / Description Southwest and Central (PBP 002-000) $74
Cache Valley (PBP 005-000) $67 What You Should Know
Diagnostic Services, Lab, and Radiology Services, and X-Rays1
Costs for these services may vary based on place of service. Only one lab or diagnostic test copayment is collected when multiple lab tests are performed during the same visit. Services are in addition to any applicable primary care or specialist copay.
Diagnostic radiology services (such as MRIs, CT scans) $300 copay $300 copay
Diagnostic tests and procedures$10 copay or 20% coinsurance, depending on the service
$10 copay or 20% coinsurance, depending on the service
Lab services $10 copay $10 copay
Outpatient x-rays $20 copay $20 copay
Therapeutic radiology services (such as radiation treatment for cancer) 20% coinsurance 20% coinsurance
Hearing ServicesExam to diagnose and treat hearing and balance issuesHearing AidsCopay for each hearing aid
$50 copay
Hearing aids: Not covered
$50 copay
Tier 1 – Essential: $649Tier 2 – Standard: $949Tier 3 – Advanced: $1,249Tier 4 – Premium: $1,649Tier 5 – Platinum: $1,949
Selected hearing aids purchased through selected audiology providers are covered under one of five benefit tiers.The copay includes the device, three fitting and adjustment appointments, and a one-year supply of batteries.
Dental Services1 $50 copay $50 copay Limited dental services related to a medical condition.
Vision Services
Exam to diagnose and treat diseases and conditions of the eye
$50 copay $50 copay
Eyeglasses or contact lenses after cataract surgery
$0 copay $0 copay
Routine and non-routine eye exams
Vision test (Refraction)
$50 copay$0 copay
$50 copay$0 copay
1 Service may require prior authorization.

17
SUMMARY OF BENEFITS | SOUTHWEST AND CENTRAL, CACHE VALLEY
Benefit / Description Southwest and Central (PBP 002-000) $74
Cache Valley (PBP 005-000) $67 What You Should Know
Inpatient Mental Health Services1 $260 copay per day for days 1 through 6$0 copay for days 7 through 90$0 copay for lifetime reserve days
$260 copay per day for days 1 through 6$0 copay for days 7 through 90$0 copay for lifetime reserve days
Our plan covers 90 days for an inpatient hospital stay each time you are admitted. Our plan also covers 60 “lifetime reserve days.” These are “extra” days that we cover. If your hospital stay is longer than 90 days, you can use these extra days. But once you have used up these extra 60 days, your inpatient hospital coverage will be limited to 90 days.Our plan covers up to 190 days in a lifetime for inpatient mental health care in a psychiatric hospital. The inpatient hospital care limit does not apply to inpatient mental services provided in a general hospital.
Outpatient Mental Health Services1
Outpatient group therapy visit $40 copay $40 copay
Outpatient individual therapy visit $40 copay $40 copay
Partial hospitalization for mental health $55 copay $55 copay
Skilled Nursing Facility (SNF)1
Our plan covers up to 100 days in a SNF.
$0 copay per day for days 1 through 20$160 copay per day for days 21 through 100
$0 copay per day for days 1 through 20$160 copay per day for days 21 through 100
No prior hospital stay required.
Outpatient Rehabilitation Services1
There is no limitation on the number of visits on occupational, speech, and physical therapy.
Physical therapy and speech and language therapy visit $40 copay $40 copay
Occupational therapy visit $40 copay $40 copay
Cardiac (heart) rehab services (for a maximum of 2 one-hour sessions per day for up to 36 sessions up to 36 weeks)
$40 copay $40 copay
Pulmonary rehab services $30 copay $30 copay
1 Service may require prior authorization.

18
SUMMARY OF BENEFITS | SOUTHWEST AND CENTRAL, CACHE VALLEY
COVERED MEDICAL AND HOSPITAL BENEFITS (CONTINUED)
Benefit / Description Southwest and Central (PBP 002-000) $74
Cache Valley (PBP 005-000) $67 What You Should Know
Ambulance1 $225 copay $225 copayCovered ambulance services include fixed wing, rotary wing, and ground ambulance services to the nearest appropriate facility.
Transportation Not Covered Not Covered This would include services such as getting a ride to or from your doctor.
Medicare Part B DrugsIncludes chemotherapy and other Part B drugs1
20% coinsurance 20% coinsurance
Foot Care (podiatry services) $50 copay $50 copayFoot exams and treatment if you have diabetes-related nerve damage and/or meet certain conditions.
Medical Equipment / Supplies
Coverage for glucose monitors and test strips is limited to FreeStyle and Precision Xtra® brands produced by Abbott Labs. If you or your physician feel that it is medically necessary for you to use a different monitor or test strips, call Member Services.
Durable medical equipment (wheelchairs, oxygen, etc.) 1 20% coinsurance 20% coinsurance
Prosthetic devices and supplies (braces, artificial limbs, etc.)1 20% coinsurance 20% coinsurance
Diabetes monitoring supplies $0 copay $0 copay
Diabetes self-management training $0 copay $0 copay
Therapeutic shoe inserts 20% coinsurance 20% coinsurance
Wellness Programs LiveWell Advantage wellness reimbursement
Up to $240 Up to $240
You receive reimbursement for up to a combined total of $240 per year for approved services.SelectHealth will reimburse you for eligible expenses.
Chiropractic Care1 $20 copay $20 copayManipulation of the spine to correct a subluxation (when 1 or more of the bones of your spine move out of position).
Home Health Care1 $0 copay $0 copay
1 Service may require prior authorization.

19
SUMMARY OF BENEFITS | SOUTHWEST AND CENTRAL, CACHE VALLEY
Benefit / Description Southwest and Central (PBP 002-000) $74
Cache Valley (PBP 005-000) $67 What You Should Know
Outpatient Substance AbuseIndividual or group therapy in a provider’s office $40 copay per visit. $40 copay per visit.
Individual or group therapy in an outpatient facility setting $50 copay per visit. $50 copay per visit.
Over-the-Counter Items Not Covered Not Covered
Renal Dialysis 20% coinsurance 20% coinsurance
HospiceYou pay nothing for hospice care from a Medicare-certified hospice.
You pay nothing for hospice care from a Medicare-certified hospice.
You may have to pay part of the costs for drugs and respite care. Hospice is covered outside of our plan. Please contact us for more details.
Connect CareIntermountain Connect Care is a convenient service that provides online access for common medical conditions.
$20 copay $20 copay
Intermountain Connect Care is available 7 days a week and can be accessed through your computer or mobile device. Connect Care is not for medical emergencies. Please call 911 or go to the nearest emergency room for any emergency care.
TeleHealth Services $10-50 copay $10-50 copay
SelectHealth offers a supplemental TeleHealth Services benefit that allows plan-approved providers to offer TeleHealth Services to you directly when you are located anywhere nationwide, including through your home computer or on your mobile device.
1 Service may require prior authorization.

20
SUMMARY OF BENEFITS | SOUTHWEST AND CENTRAL, CACHE VALLEY
Benefit / Description SelectHealth Advantage Southwest & Central and Cache Valley DeductibleYou begin in this payment stage when you fill your first prescription of the year. During this stage, you pay the full cost of your brand name and specialty drugs until you have reached the annual deductible. Annual deductible does not apply to generic drugs.
Pharmacy DeductibleTiers 1 and 2 $0
Tiers 3, 4, and 5 $250
INITIAL COVERAGEDuring this stage, the plan pays its share of the cost of your drugs and you pay your share of the cost.You stay in this stage until the amount of your year-to-date “total drug costs” reaches $3,750. Then, you move to the COVERAGE GAP.
Standard Retail Cost-Sharing One-Month Supply Two-Month Supply Three-Month SupplyTier 1 (Preferred Generic) $3 $6 $9
Tier 2 (Generic) $15 $30 $45
Tier 3 (Preferred Brand) $45 $90 $135
Tier 4 (Nonpreferred Brand) $95 $190 $285
Tier 5 (Specialty Tier) 28% of the cost Not Offered Not Offered
Standard Mail Order Cost-Sharing One-Month Supply Two-Month Supply Three-Month SupplyTier 1 (Preferred Generic) $3 $6 $6
Tier 2 (Generic) $15 $30 $30
Tier 3 (Preferred Brand) $45 $90 $135
Tier 4 (Nonpreferred Brand) $95 $190 $285
Tier 5 (Specialty Tier) 28% of the cost Not Offered Not Offered
If you reside in a long-term care facility, you pay the same as at a retail pharmacy.
You may get drugs from an out-of-network pharmacy, but may pay more than you pay at an in-network pharmacy.
PRESCRIPTION DRUG BENEFITS

21
SUMMARY OF BENEFITS | SOUTHWEST AND CENTRAL, CACHE VALLEY
Benefit / Description SelectHealth Advantage Southwest & Central and Cache Valley
COVERAGE GAP (DONUT HOLE)
You stay in this stage until the amount of your year-to-date “out-of-pocket costs” reaches $5,000.
You generally pay no more than 35% on applicable brand name drugs and 44% on applicable generic / nonapplicable drug cost.
CATASTROPHIC COVERAGE
During this payment stage, the plan pays most of the cost for your covered drugs. You stay in this stage for the rest of the calendar year through December 31, 2018.
$3.35 for generic drugs and $8.35 for all other drugs; or 5% coinsurance, whichever is greater.
OPTIONAL BENEFITS You must continue to pay your Medicare Part B premium and your monthly plan premium, an extra premium will be added each month for these benefits.
PACKAGE 1: $35
SelectHealth Dental Comprehensive Benefit
Benefits include: Preventive dental care and comprehensive dental care.
How much is the monthly premium? Additional $35 per month.
How much is the deductible? $0 deductible.
Is there a limit on how much the plan will pay?
Our plan pays up to $1,000 every year and has additional coverage limits for certain benefits. $0 copay for preventive dental services including: two exams/cleanings with x-rays per year. You pay 50% for all other covered dental services, such as fillings, extractions, root canal, crowns, dentures (rebasing & relining), bridges, and implants.
PACKAGE 2: $40
SelectHealth Dental Comprehensive Plus Eyewear
Benefits include: Preventive dental care, comprehensive dental care, and eyewear.
How much is the monthly premium? Additional $40 per month.
How much is the deductible? $0 deductible.
Is there a limit on how much the plan will pay?
This optional supplemental benefit package offers the same coverage for dental preventive and corrective services as Package #1. You also have a $200 retail value allowance for glasses or contacts at participating locations. See the Evidence of Coverage for more information on these benefits.

22
© 2017 SelectHealth. All rights reserved. 8362280 09/17