successfully managing biopharmaceutical manufacturing ... · successfully managing...
TRANSCRIPT
Successfully Managing BiopharmaceuticalManufacturing Outsourcing
Pre-Conference WorkshopIQPC 4th Annual Contract Manufacturing Forum
May 22, 2006
Patricia SeymourBioProcess Technology Consultants, Inc.
Acton, MA
From Clone to Clinic®
Introduction – What is a Biopharmaceutical
Developing Biomanufacturing Processes
Developing a Manufacturing Strategy and the
Availability of Bio-manufacturing Capacity
Identifying and Qualifying the Right CMO
From Clone to Clinic®
What is a Biopharmaceutical Product?
Products made by or composed of viable organisms− Natural & rDNA Proteins, Monoclonal Antibodies− Vaccines, Cell and Gene Therapy− Blood and Blood Derivatives
Traditional Biologics Defined by Manufacturing Process• Difficult to demonstrate purity, identity, potency & consistency
Early biopharmaceutical products included simple proteins, typicallyreplacement for existing natural products, e.g., insulin, alphainterferon
Today’s biologic products more complex proteins with significanttertiary structure and post-translational modifications
Current biologics can be manufactured, characterized, and assayedwith drug-Like control and resolution• Tightly defined production processes with high-resolution
analytical methods
From Clone to Clinic®
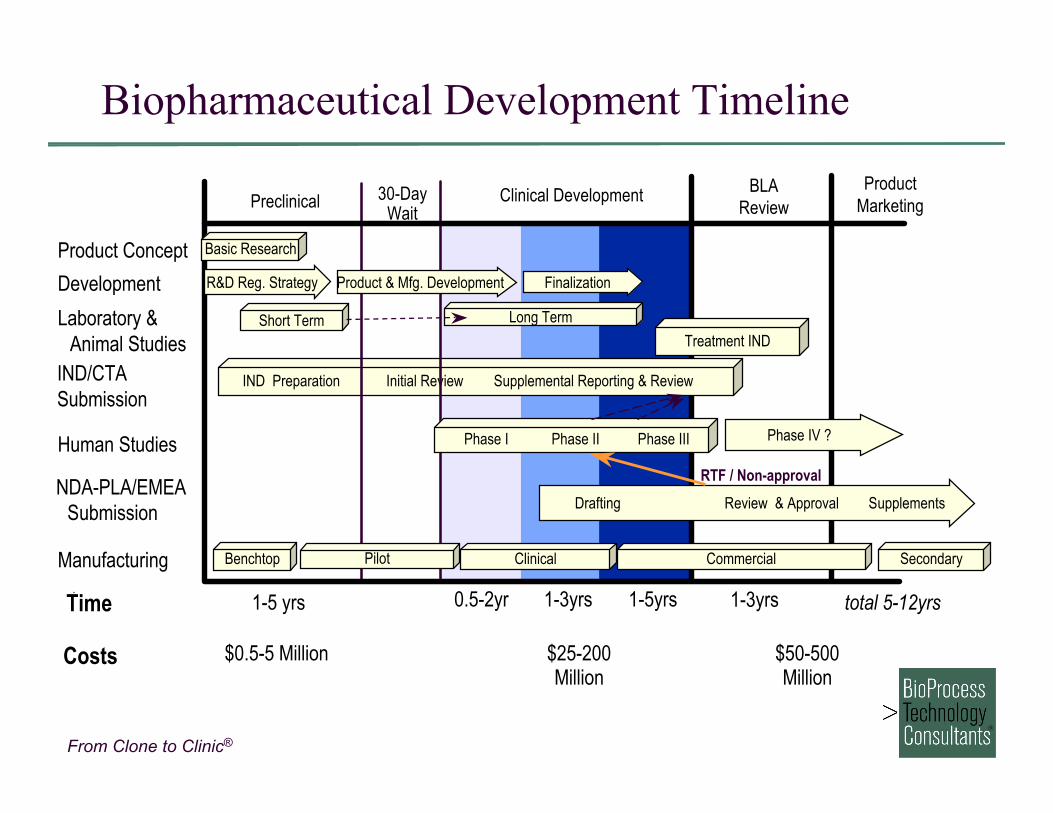
Biopharmaceutical Development Timeline
Costs $0.5-5 Million $25-200Million
Product Concept
Development
Laboratory &Animal Studies
IND/CTASubmission
Human Studies
NDA-PLA/EMEASubmission
Preclinical 30-DayWait
Clinical Development BLAReview
ProductMarketing
Treatment IND
Manufacturing
IND Preparation Initial Review Supplemental Reporting & Review
Phase IV ?Phase I Phase II Phase III
1-5 yrs 1-3yrs0.5-2yr 1-3yrs 1-5yrs
RTF / Non-approval
Short Term Long Term
Basic Research
Benchtop SecondaryClinicalPilot Commercial
R&D Reg. Strategy Product & Mfg. Development Finalization
Drafting Review & Approval Supplements
total 5-12yrsTime
$50-500Million
From Clone to Clinic®
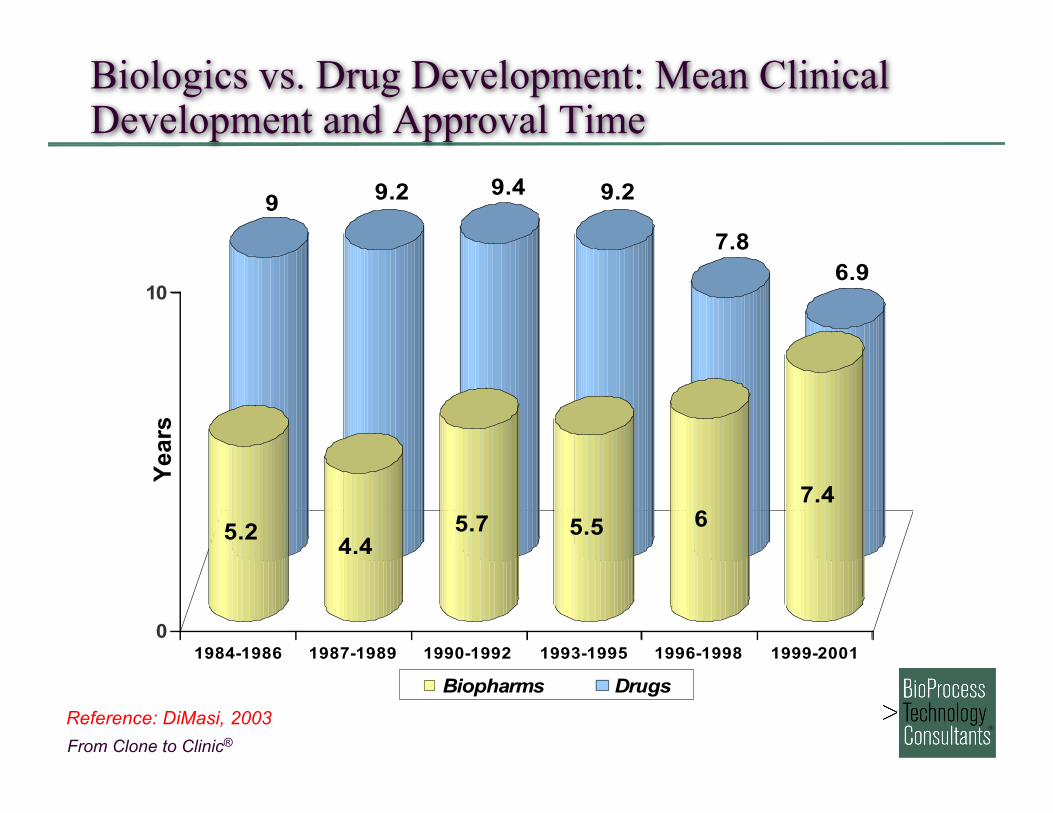
99.2 9.4 9.2
7.8
6.9
5.24.4
5.7 5.5 6
7.4
0
10
1984-1986 1987-1989 1990-1992 1993-1995 1996-1998 1999-2001
Biopharms Drugs
Biologics vs. Drug Development: Mean ClinicalDevelopment and Approval Time
Reference: DiMasi, 2003
Year
s
From Clone to Clinic®
Cost of Manufacturing of Biopharmaceuticals
Processes are fixed-cost driven Manufacturing costs typically 15 – 25% of COGs Basic cGMP background identical to chemical drugs Complexity of products results in demanding technical
processes and high capital investments Factors influencing manufacturing costs
• Process design and plant capacity• Operating Strategy• Equipment and Facilities Costs• Materials Costs• Labor Costs• Overhead Structure
From Clone to Clinic®
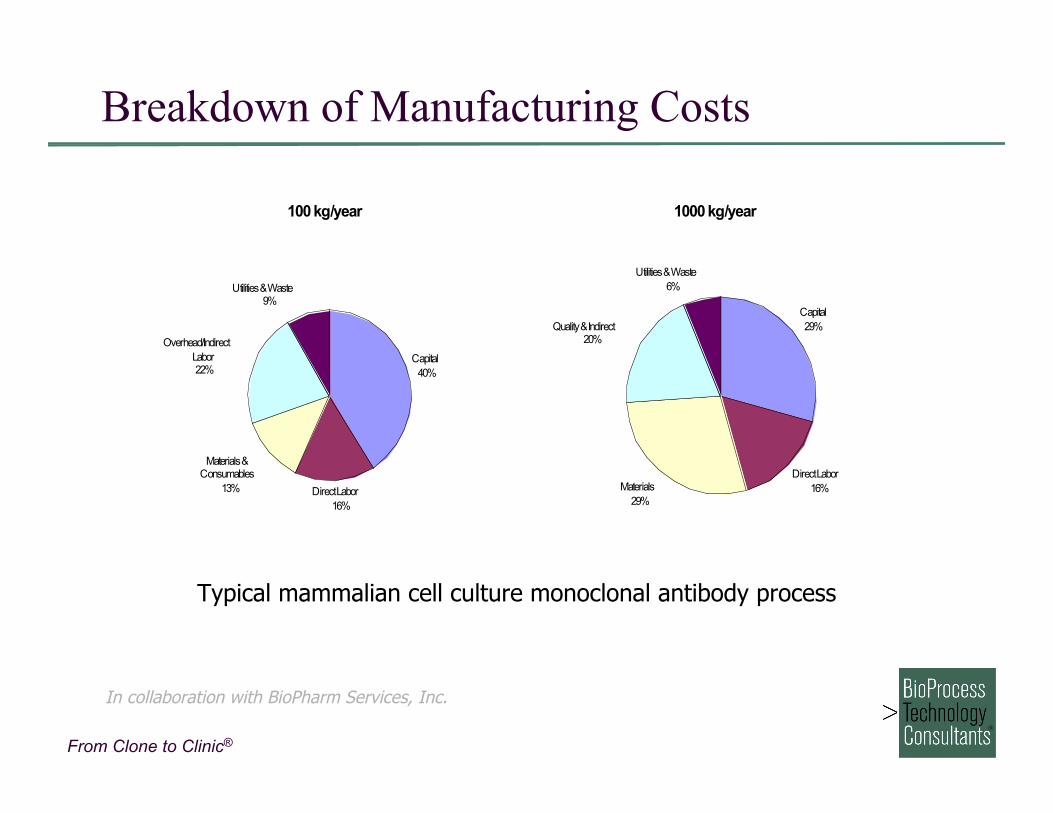
Breakdown of Manufacturing Costs
1000 kg/year
Capital
29%
Direct Labor
16%Materials
29%
Quality & Indirect20%
Utilities & Waste
6%
100 kg/year
Capital
40%
Direct Labor
16%
Materials & Consumables
13%
Overhead/Indirect
Labor22%
Utilities & Waste9%
Typical mammalian cell culture monoclonal antibody process
In collaboration with BioPharm Services, Inc.
From Clone to Clinic®
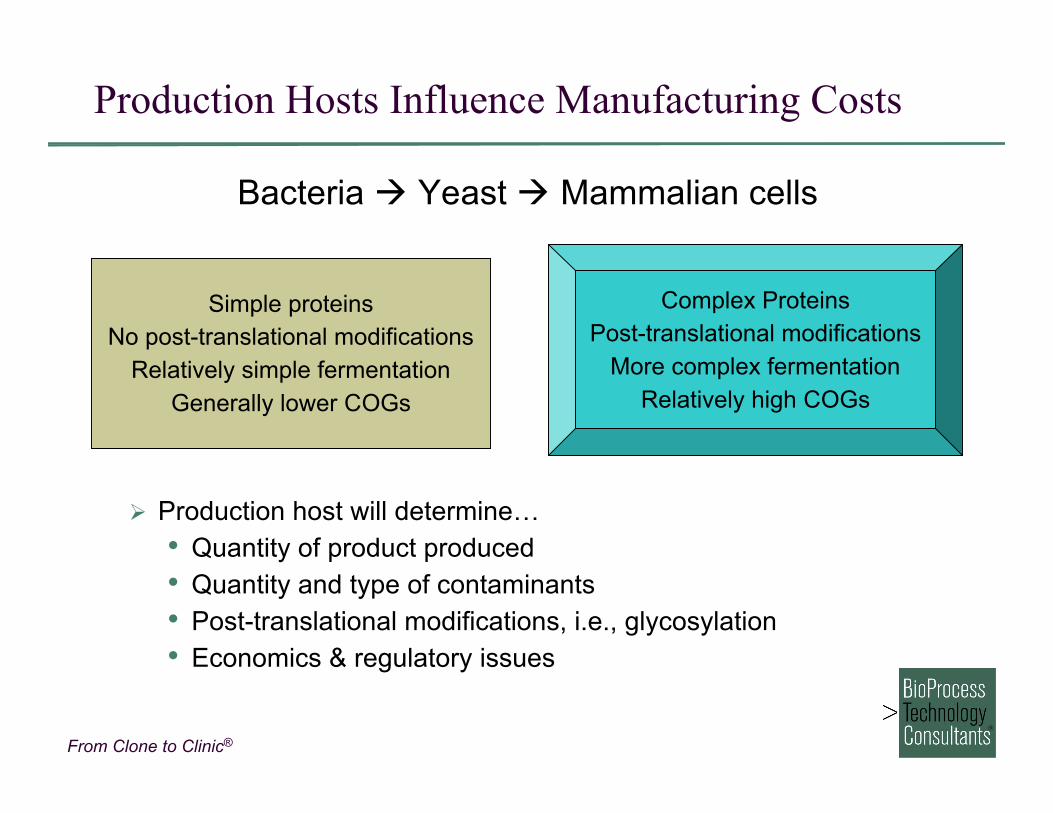
Production Hosts Influence Manufacturing Costs
Bacteria Yeast Mammalian cells
Simple proteinsNo post-translational modifications
Relatively simple fermentationGenerally lower COGs
Complex ProteinsPost-translational modifications
More complex fermentationRelatively high COGs
Production host will determine…• Quantity of product produced• Quantity and type of contaminants• Post-translational modifications, i.e., glycosylation• Economics & regulatory issues
From Clone to Clinic®
General Considerations for Host Selection
Overproduction may cause aggregation or degradation byhost, toxicity to host cell, inaccurate or incomplete processingof product.
For each product, it is necessary to evaluate source so thatmaximum amount of biologically active product can beobtained.
Availability of appropriate expression vectors• Inducible expression for potentially toxic proteins• Proven technology for selecting cell lines with high
expression levels• Access to reasonable licenses for use of existing technology
COGS analysis for production of clinical and commercialmaterial consistent with predicted dose and price of finalproduct
From Clone to Clinic®
General Considerations for Host Selection
Proven track record with regulatory authorities• Untested production organism require higher burden of
proof of safety and reproducibility Anticipated expression levels and ease of downstream
processing• Secreted product often easier to process than intracellular
Approximate productivities• Mammalian cell culture: 0.01 - 3 g/L – MAbs at high end
(~1+ g/L); rProteins lower; Expression levels likely to rise to~10 g/L by 2015
• Microbial fermentation: 1 - 10 g/L – dependent on product,formation of inclusion bodies, secretion of product, etc.

From Clone to Clinic®
Bacteria
Advantages• Well understood molecular biology; Simple vector construction• High intracellular expression levels; periplasmic secretion
possible• Simple cell bank characterization• Rapid cell growth in inexpensive media• Established regulatory track record
Disadvantages• Protein refolding & separation of incorrectly folded from
properly folded product• Proteins lack post-translational modifications• Micro-heterogeneity, including N-terminal methionine• Fusion partner may be required• Removal of endotoxins from product (Gram-negative)
From Clone to Clinic®
Yeast
Advantages• High expression levels & rapid growth• Established large-scale fermentation technology; Low media
costs• Genetics well understood; natural secretor• Proteins properly folded• Lack endotoxins
Disadvantages• Heterologous proteins may be incorrectly glycosylated and
folded; often over glycosylated• Complex vector construction• Difficult to lyse
From Clone to Clinic®
Mammalian Cell Culture
Advantages• Correct post-translational modifications• Properly folded proteins• Easily secreted• Good regulatory track record
Disadvantages• Expensive• Require expensive media• Slow growth & low production levels• Potential oncogene contamination• Extensive cell bank characterization
From Clone to Clinic®
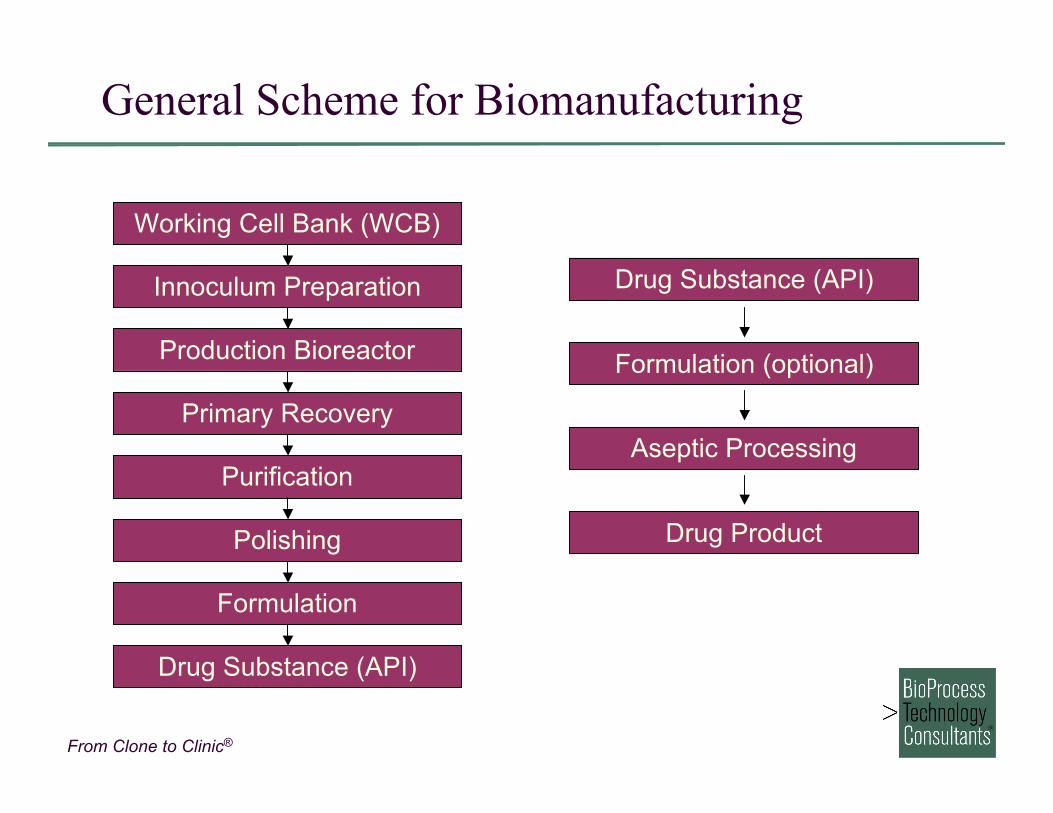
General Scheme for Biomanufacturing
Working Cell Bank (WCB)
Formulation
Polishing
Purification
Primary Recovery
Production Bioreactor
Innoculum Preparation
Drug Substance (API)
Drug Product
Aseptic Processing
Formulation (optional)
Drug Substance (API)
From Clone to Clinic®
Drug Substance Manufacturing
Innoculum preparation• Thaw vial from Working Cell Bank• Expand culture to desired production volume
Production bioreactor• Maximize cell density• Maximize product expression
Primary recovery• Separate cells from culture media• Concentrate and stabilize product for ease of handling
Purification• Removal of majority of host cell contaminants, media components,
product-related impurities Polishing
• Removal of final traces of host cell contaminants, product-relatedimpurities
Formulation• Transfer product to final storage conditions• Prepare for Drug Product manufacturing
From Clone to Clinic®
Drug Product Manufacturing
Formulation• Adjust protein concentration• Add additional excicipients and/or stabilizers
Aseptic Processing• Most biologics can not be terminally sterilized• Sterile filtration required to achieve sterile product
Container/closure Considerations• For early-stage clinical trials, glass vial with rubber stopper most
common• Lyophilization often required for stabilization• Late-stage and commercial products, alternate container/closures
for added patient compliance/ease of use− Pre-filled syringes− Dual chamber vials
From Clone to Clinic®
Developing a Manufacturing Strategy and the
Availability of Biomanufacturing Capacity
From Clone to Clinic®
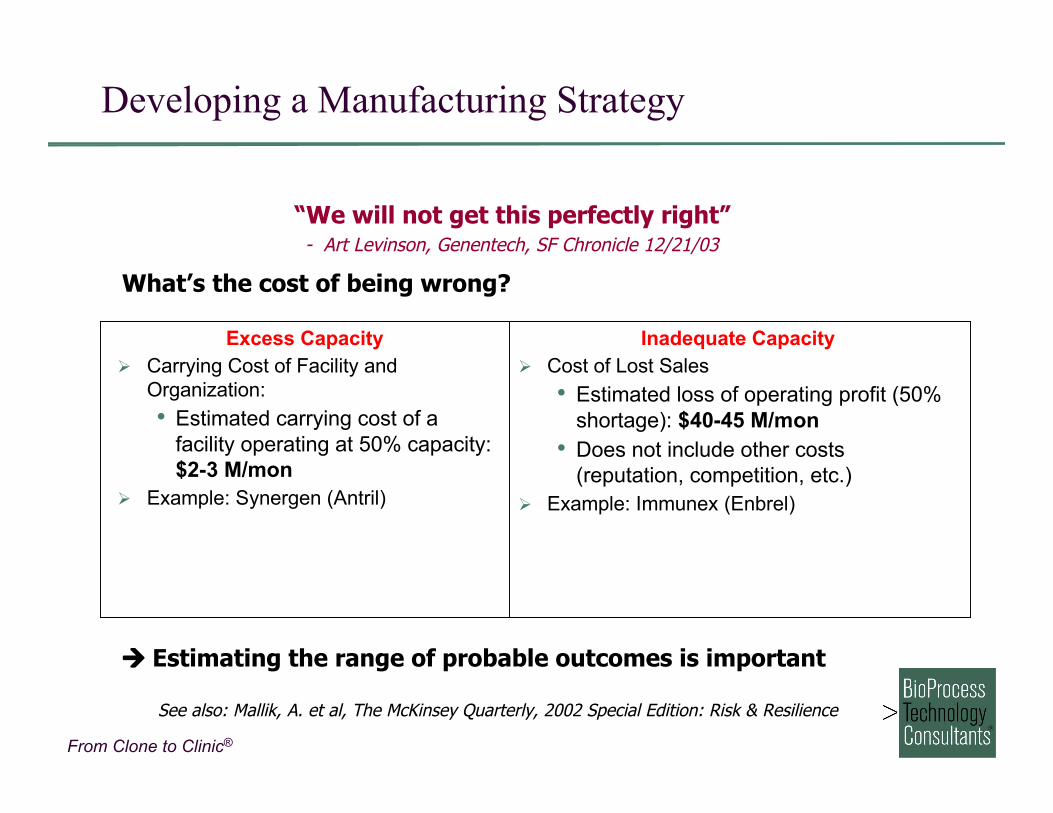
Developing a Manufacturing Strategy
“We will not get this perfectly right”- Art Levinson, Genentech, SF Chronicle 12/21/03
Inadequate Capacity Cost of Lost Sales
• Estimated loss of operating profit (50%shortage): $40-45 M/mon
• Does not include other costs(reputation, competition, etc.)
Example: Immunex (Enbrel)
Excess Capacity Carrying Cost of Facility and
Organization:• Estimated carrying cost of a
facility operating at 50% capacity:$2-3 M/mon
Example: Synergen (Antril)
What’s the cost of being wrong?
Estimating the range of probable outcomes is important
See also: Mallik, A. et al, The McKinsey Quarterly, 2002 Special Edition: Risk & Resilience
From Clone to Clinic®
Developing a Manufacturing Strategy
Company pipeline• Technology biased towards a certain product type or production
technology? Development stage
• Does company require early stage, clinical, and/or commercialmanufacturing capacity?
Manufacturing technology/growth objectives• Does company own or control proprietary manufacturing or
process technology?• Would internal manufacturing capabilities provide a competitive
edge?• Would ability to expand pipeline by in-licensing be enhanced by
controlling manufacturing capacity? Manufacturing strategy must address needs throughout the product
life-cycle from R&D through production of clinical trial materials tocommercial manufacturing
From Clone to Clinic®
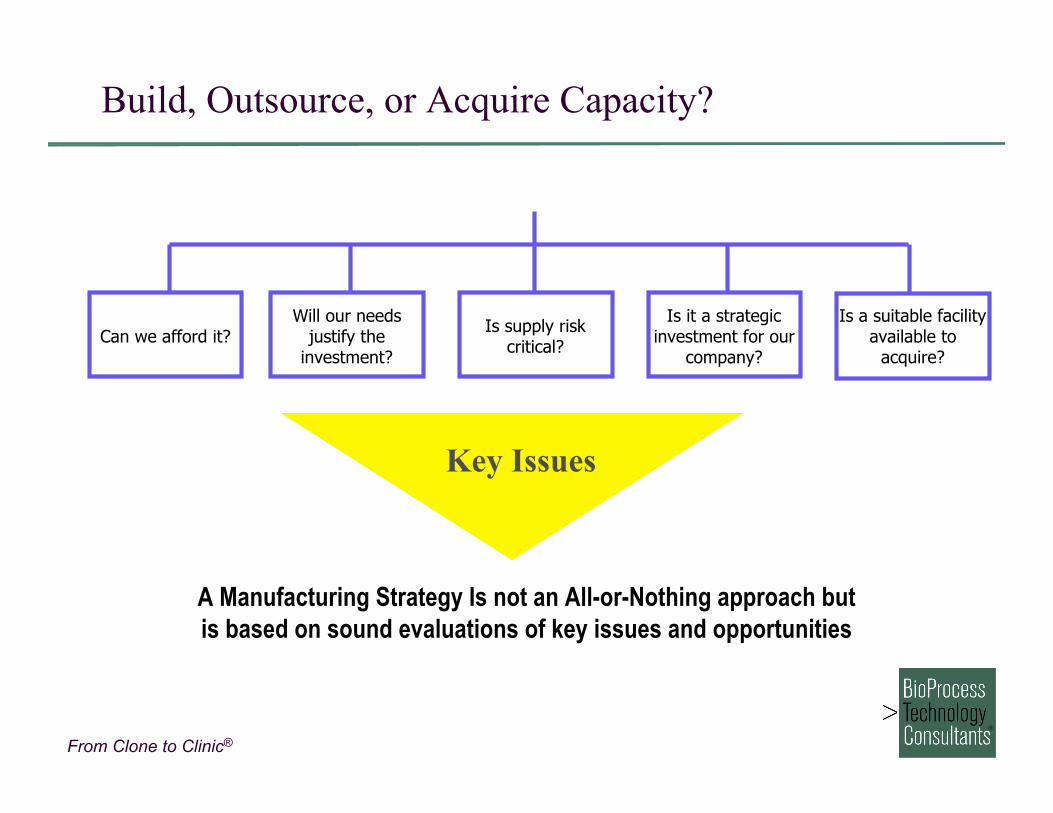
Build, Outsource, or Acquire Capacity?
Can we afford it?Will our needs
justify theinvestment?
Is it a strategicinvestment for our
company?
Is supply riskcritical?
Key Issues
A Manufacturing Strategy Is not an All-or-Nothing approach butis based on sound evaluations of key issues and opportunities
Is a suitable facilityavailable to
acquire?
From Clone to Clinic®
Drivers for Build vs. Buy Decision
Core CompetencyAssessment• We’re Good At It• Not Many Others Are
Is “Buy” an Option?• Technology
Requirements• Scale• Capacity Availability –
Supply vs. Demand
Strategic Fit• Pipeline• Competitive Advantage• Development Stage
Risk Management• Control• Cost and Probability of
Failure Financial Considerations
• Return on Capital• Cost of Capital• Operating Costs
From Clone to Clinic®
Managing Risk
From Clone to Clinic®
Mammalian Cell Culture Capacity
Distribution by Company – 2004
Contract ManufacturersTotal installed capacity ~400,000 L
Product Development Cos.Total installed capacity ~950,000 L
From Clone to Clinic®
Capacity Utilization – What is “Full Utilization”
“What is the current industry-wide level of capacity utilization”
Ref: BioPlan Associates, “A Survey of Industry Capacity,” 2003Survey of 100 biopharmaceutical manufacturers
From Clone to Clinic®
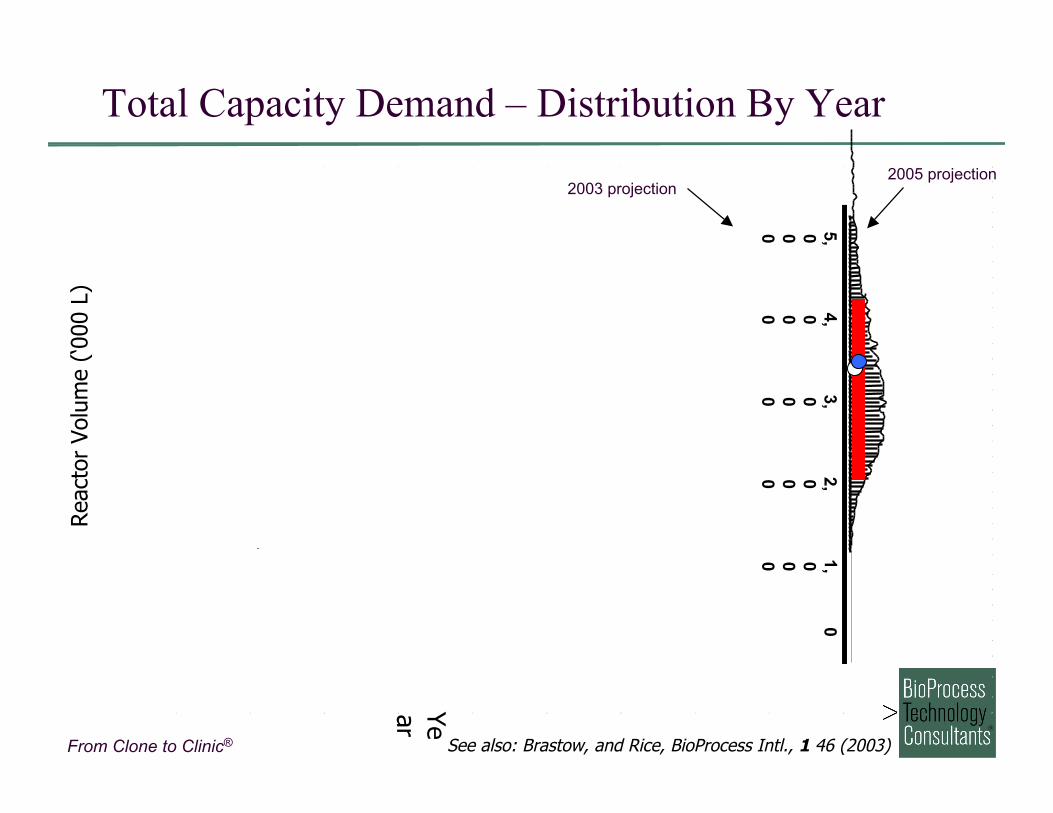
Future Availability of Biomanufacturing Capacity
Named for the casinos of Monte Carlo, Monaco Mathematical simulation based on distribution of values
for each input variable rather than single fixed value Calculates a probable range of output scenarios based on
multiple iterative calculations using random values fromwithin the defined probability ranges for each inputvariable
Useful in identifying and quantifying risk in complex multi-variable problems
From Clone to Clinic®
Total Capacity Demand – Distribution By YearRea
ctor
Vol
ume
(‘000
L)
Year
5,000
4,000
3,000
2,000
1,000
0
2003 projection2005 projection
See also: Brastow, and Rice, BioProcess Intl., 1 46 (2003)
From Clone to Clinic®
Let’s walk through the build or acquire scenarios
From Clone to Clinic®
Mammalian Cell Culture Facility Costs
Ref: Barnett International’s BioManufacturing Conference, Boston, 2002
From Clone to Clinic®
Cost of Capital vs. Return on Capital
A company’s Cost of Capital defines the scaleof investment in capacity that makes economic sense
Can/will Return on Capital beshifted higher from… more products higher throughput more efficient technology
So that Cost of Capital is lessthan the Return on Capital?
From Clone to Clinic®
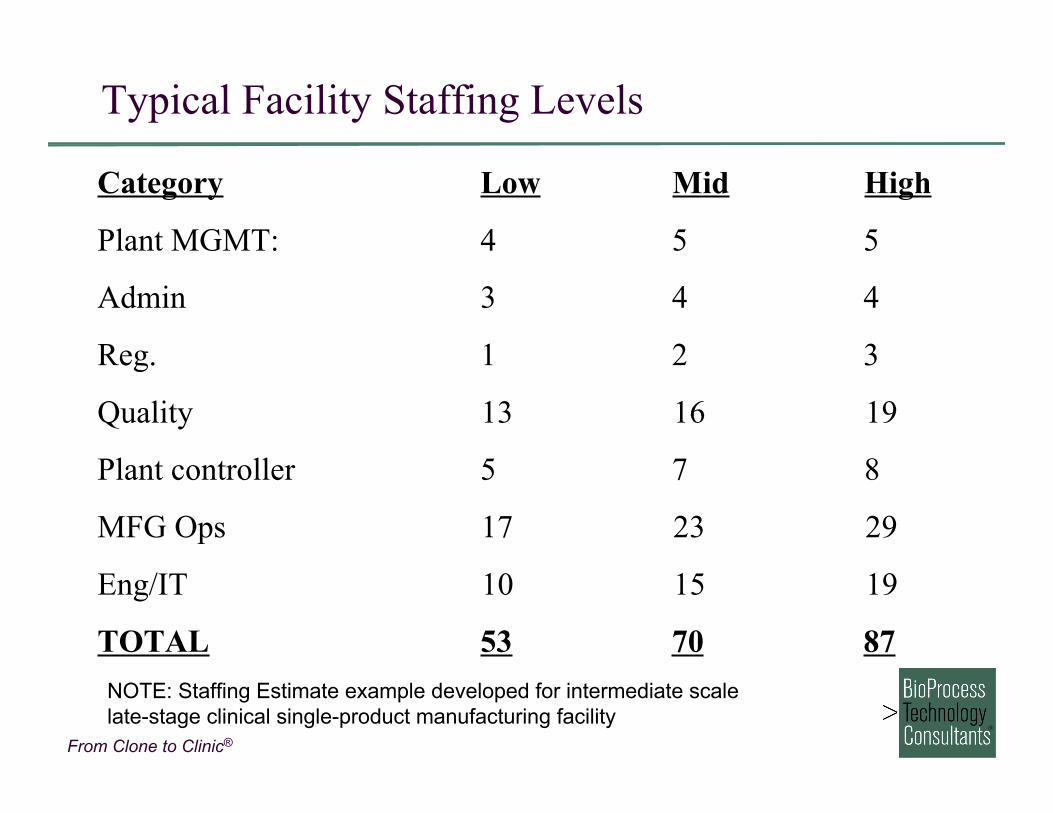
Typical Facility Staffing Levels
Category Low Mid High
Plant MGMT: 4 5 5
Admin 3 4 4
Reg. 1 2 3
Quality 13 16 19
Plant controller 5 7 8
MFG Ops 17 23 29
Eng/IT 10 15 19
TOTAL 53 70 87NOTE: Staffing Estimate example developed for intermediate scale late-stage clinical single-product manufacturing facility
From Clone to Clinic®
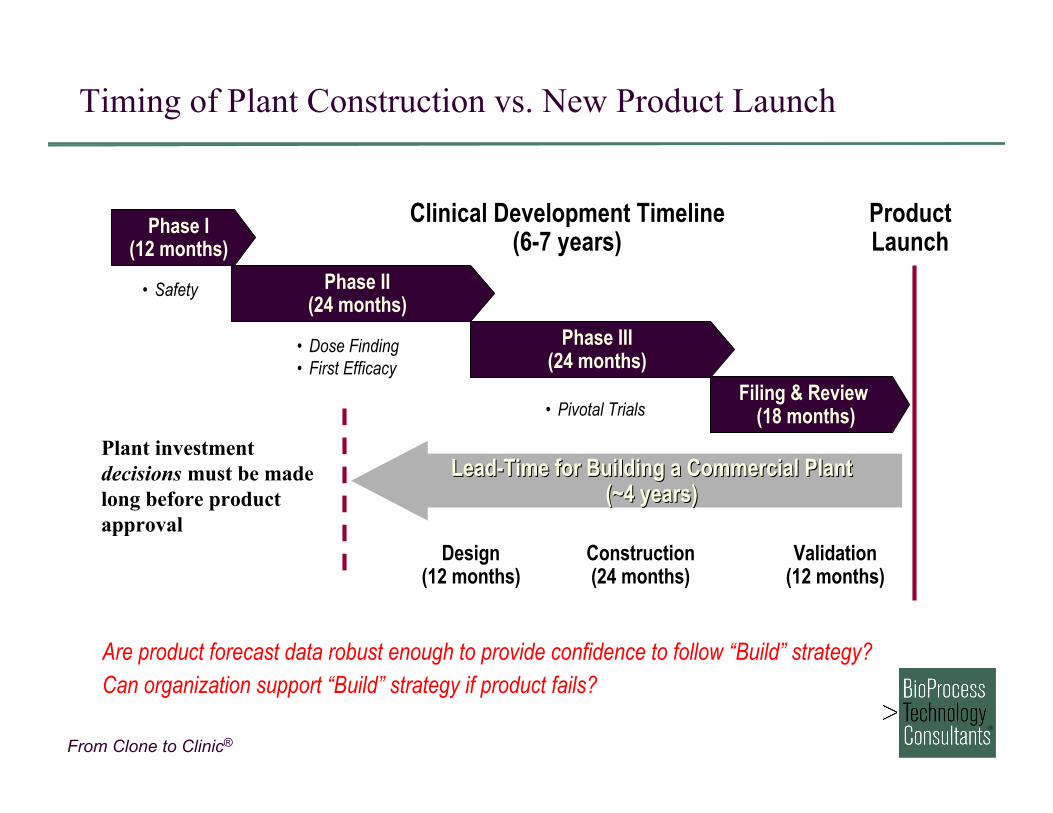
Phase I(12 months)
Phase II(24 months)
Phase III(24 months)
Filing & Review (18 months)
• Dose Finding • First Efficacy
• Safety
• Pivotal Trials
Lead-Time for Building a Commercial PlantLead-Time for Building a Commercial Plant(~4 years)(~4 years)
Design(12 months)
Construction(24 months)
Validation(12 months)
Clinical Development Timeline(6-7 years)
ProductLaunch
Plant investmentdecisions must be madelong before productapproval
Are product forecast data robust enough to provide confidence to follow “Build” strategy?Can organization support “Build” strategy if product fails?
Timing of Plant Construction vs. New Product Launch
From Clone to Clinic®
Acquiring Existing Capacity
As the biopharmaceutical industry matures, oldermanufacturing facilities may become available for acquisition
Examples:• Amgen acquires Synergen
− Primary motivator for acquisition not manufacturingcapacity
• Centocor acquires plant from Wyeth− Plant history:Invitrogen Centocor Chiron Wyeth Centocor
• Cephalon acquires Bio Science plant #1− Converts CMO capacity to captive capacity
• Cambrex acquires Bio Science and Marathon− Allows Cambrex’s entry into biologics CMO business
From Clone to Clinic®
Acquiring Existing Capacity
Additional examples:• Dow acquires Collaborative BioAlliance
− Allows Dow’s entry into biologics CMO business− Dow has exited the CMO business; facility may be
available• Genentech acquires Porrino plant
− Establishes European manufacturing capacity• Tanox acquires Biogen Idec Torreyana facility
− Allows shift from outsourced manufacturing to in-housesupply
• Genentech acquires Biogen Idec NIMO facility− Additional manufacturing capacity to support Avastin
production
From Clone to Clinic®
Let’s walk through the outsourcing scenarios
From Clone to Clinic®
Benefits of Outsourcing
Capital Conservation Speed to Market Redundancy Available capacity/optimized technology Flexible production schedule to suit client’s timing needs Qualified cGMP-trained staff Full documentation, regulatory and quality systems in place Captive technical and regulatory “consultants;” access
additional expertise Maintain low overhead and minimize cash flow Release capacity required for other products Lower price of product Minimize risk
From Clone to Clinic®
Risks of Outsourced Manufacturing
Lack of Control
Avoiding capacity crunches
Monitoring remote site(s)
Technology transfer
Ensuring schedules
Protecting technology
Documentation
Compliance
Underestimating internal resource requirements
From Clone to Clinic®
When Outsourcing Makes Sense
Limited technical and monetary resources Product development efforts focused Product pipeline small and/or very diverse Need for Process Development assistance Need to meet milestones to obtain additional financing Availability of capacity/capabilities No in-house capacity Technology outside core competence and readily available

From Clone to Clinic®
Let’s walk through the trade-offs
From Clone to Clinic®
RIS
K
Product Launch
DevelopmentUncertainty
MarketUncertainty
Maturity
Manufacturing costsset at decision point
Make
Make or Buy
Product Life Cycle
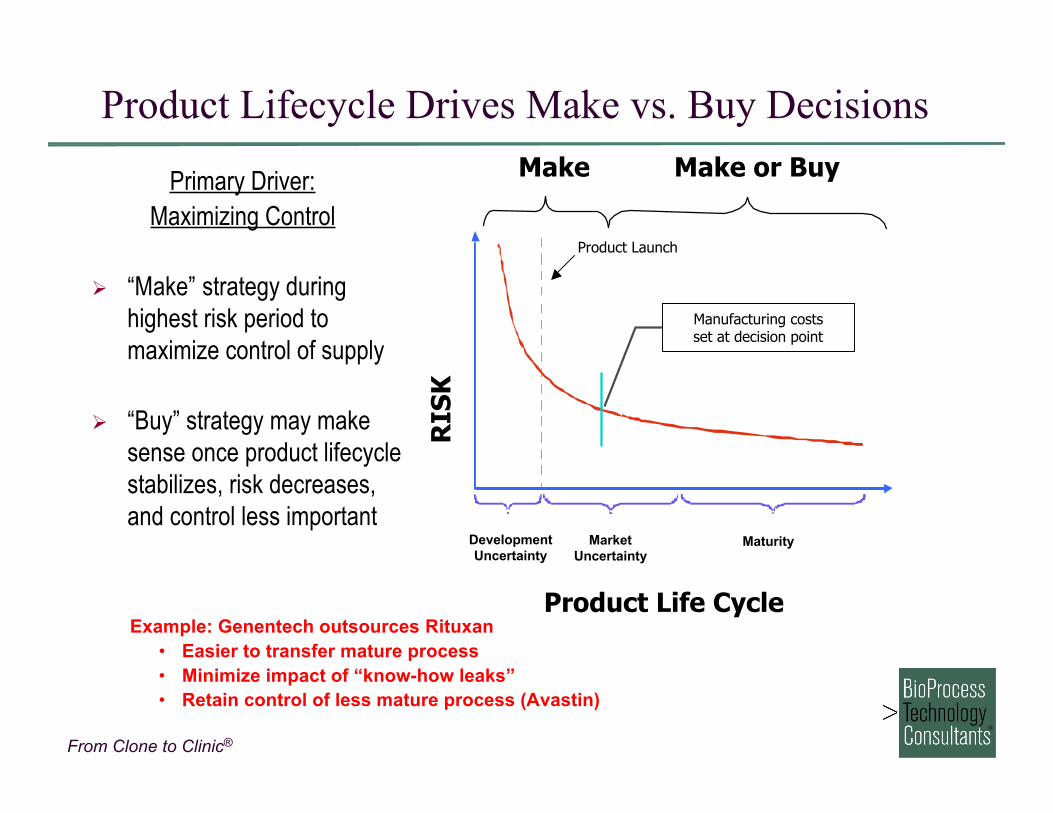
Product Lifecycle Drives Make vs. Buy Decisions
Primary Driver:Maximizing Control
“Make” strategy duringhighest risk period tomaximize control of supply
“Buy” strategy may makesense once product lifecyclestabilizes, risk decreases,and control less important
Example: Genentech outsources Rituxan• Easier to transfer mature process• Minimize impact of “know-how leaks”• Retain control of less mature process (Avastin)
From Clone to Clinic®
Product Launch
DevelopmentUncertainty
MarketUncertainty
Maturity
Manufacturing costsset at decision point
Buy
Buy or Make
Product Life Cycle
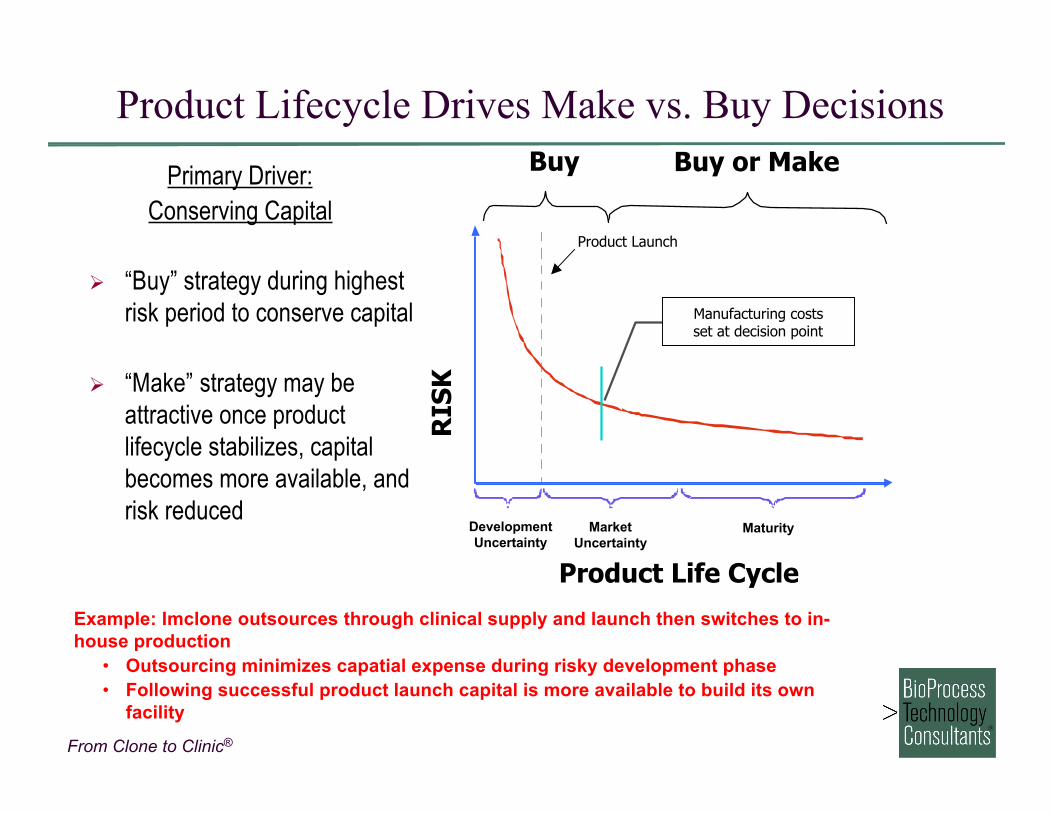
Primary Driver:Conserving Capital
“Buy” strategy during highestrisk period to conserve capital
“Make” strategy may beattractive once productlifecycle stabilizes, capitalbecomes more available, andrisk reduced
RIS
K
Product Lifecycle Drives Make vs. Buy Decisions
Example: Imclone outsources through clinical supply and launch then switches to in-house production
• Outsourcing minimizes capatial expense during risky development phase• Following successful product launch capital is more available to build its own
facility
From Clone to Clinic®
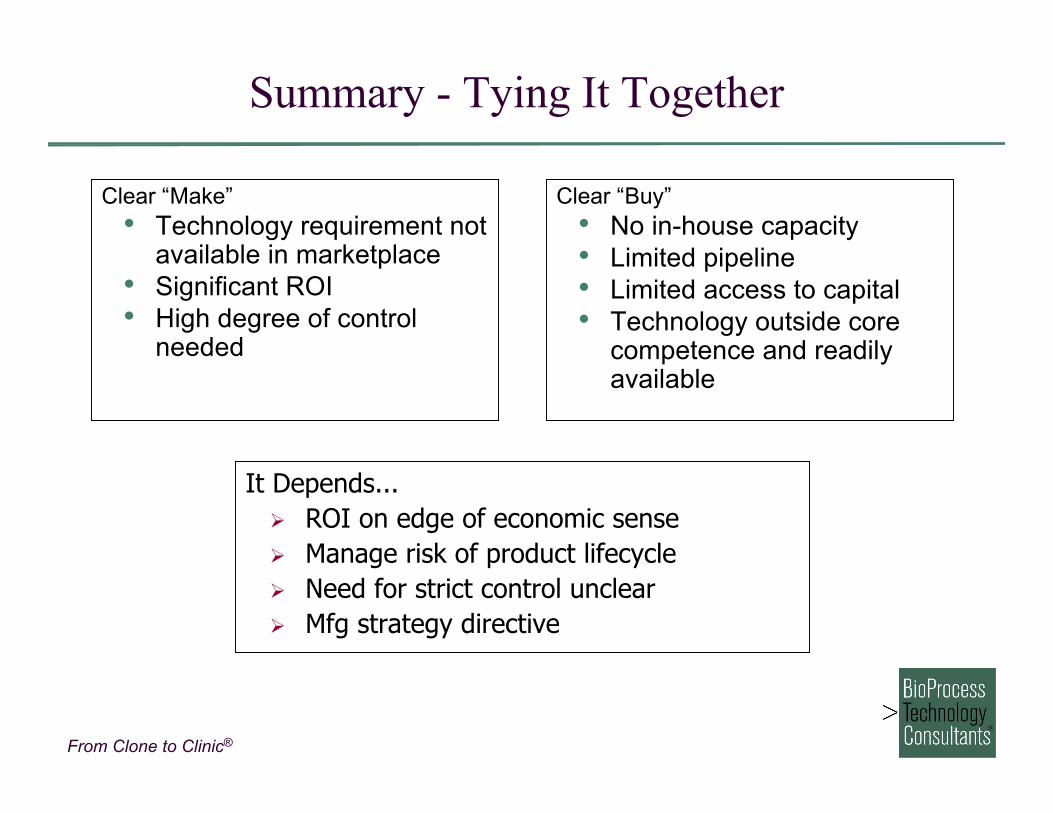
Summary - Tying It Together
Clear “Make”• Technology requirement not
available in marketplace• Significant ROI• High degree of control
needed
Clear “Buy”• No in-house capacity• Limited pipeline• Limited access to capital• Technology outside core
competence and readilyavailable
It Depends... ROI on edge of economic sense Manage risk of product lifecycle Need for strict control unclear Mfg strategy directive
From Clone to Clinic®
Summary
Decisions related to manufacturing biopharmaceuticals arestrategically significant and involve significant capital andresources
A range of analysis should support a company’s make vs. buyvs. acquire decision, including:• Assessment of the company’s pipeline and development
stage• Determination of strategic fit with business• Risk assessment• Evaluation of the industry environment for manufacturing
capacity and external buy/acquire options
From Clone to Clinic®
Identifying and Qualifying
the Right Contract Manufacturer
From Clone to Clinic®
Selecting a Contract Manufacturer
Single most important decision to be made
Make a detailed list of your requirements
Prioritize and weight the requirements
Rank each of your needs for each contractor
Cost should not be the number one priority
From Clone to Clinic®
Identifying Vendors for Process Development
Experience in desired host organism• i.e., Microbial expertise does not automatically mean
capability in both bacteria and yeast Availability of proprietary host cell lines or cell line construction
methodology that can enable more rapid progress towardclinical trials• Review all applicable IP associated with proposed
production system and determine fees in advance Ability to continue to develop manufacturing process
• Availability of manufacturing capacity at anticipated scalefor the program
From Clone to Clinic®
Outsourcing Process Development & GMP Production
Ability to develop processes and availability of GMP compliantmanufacturing facilities and quality systems• Pre-selection compliance audit of candidate vendors
recommended Track record in process development at similar scale and for
similar product types• For antibody products, previous antibody experience
desirable GMP manufacturing capacity at anticipated scale and timeline
• Flexibility in scheduling desirable in case processdevelopment is delayed
Supporting analytical capability to support processdevelopment and manufacturing
From Clone to Clinic®
CMO Selection Process
Define critical parameters and create list of suitable vendors Contact vendors to determine interest and availability Create short list of vendors and sign CDAs
• CMOs will insist on CDA prior to submitting proposals withtimeline or financial information
Prepare and circulate Request for Proposal (RFP) to vendors Compare proposals Site visits to top 2 – 3 vendors Selection
Entire selection process takes 2-3 months per major activity
From Clone to Clinic®
Example of Critical Parameters Definition
Technical• Mammalian cell culture experience, preferably including
some non-antibody products• Process Development and scale-up experience• 500L clinical GMP manufacturing capacity• Analytical development capability
Other• Location?• Availability of PD and manufacturing capacity• Perceived cost• Responsiveness to customer inquiries and requests
From Clone to Clinic®
Use Detailed RFP to Select and Evaluate CMOs
RFP will ideally outline all activities for which a time and costestimate is required• Omission of desired SOW in RFP leads to proposals that
are not easily comparable RFP should be sent to candidate vendors at same time, with
same deadline for response• Ability to meet the initial deadline indicative of future
responsiveness of CMO• Deadline must be realistic and allow time for CMO to
prepare project-specific timeline and budget Decision making mechanisms should be in place and process
and timing of final decision should be known
From Clone to Clinic®
Biopharmaceutical Manufacturing Vendors
Manufacture of Bulk Drug Substance (DS)• GMP suites will contain bioreactors and harvesting
equipment• Downstream processing equipment in separate suite• Analytical methods to support all stages of manufacture
Manufacture of Final Drug Product (DP)• Fill/finish facilities will contain compounding rooms for
formulation (dilution, addition of excipients)• One or more GMP filling lines for aseptically filling product
into final containers (vials, syringes)• Potentially will contain lyophilization capability
Analytical Methods Development and Stability Testing• Usually performed by the DS or DP vendor
From Clone to Clinic®
Biopharmaceutical Manufacturing Vendors
Formulation Development• Must have strong analytical capability to support
formulation decision making experiments• Must have stability chambers for forced degradation and
accelerated stability Packaging, Labeling, and Distribution
• May be provided by Drug Product CMO• Offered by some vendors as separate service• Capability to distribute within countries targeted for clinical
trials or commercial license essential
From Clone to Clinic®
CMO vs. In-house ManufacturingAvailability and Capabilities
S. Fox, American PharmaceuticalOutsourcing, 1: 17-24 (2000)
Directory of Contract Services, Vol. II, H.Levineand J. Miller, eds. Pharmsource InformationServices, Inc. (2001).
From Clone to Clinic®
Who Are The Contractors?
Small R&D laboratories
Small scale development companies
Phase I/Phase II manufacturers
Full service contract manufacturers
Companies with excess capacity
From Clone to Clinic®
Preparing a Request for Proposal
Content of RFP depends on activity being outsourced and clinicaldevelopment phase of program• RFP for cell line and early stage program contains desired
process yields, timelines, and scale• RFP for clinical distribution contains complete description of
clinical program for blinded labeling and coding RFP may be composite or single focus
• Analytical and formulation development often performed at sameCMO
• Benefits to single RFP and proposal but may take more time tonegotiate
• Fill/finish and distribution may be combined• Vendor can provide quotation on those areas that are within the
CMO’s capability
From Clone to Clinic®
Outsourcing Early Stage Activities for DrugSubstance Production Construction of expression vector and isolation of production
cell line• Often performed in-house, prior to outsourcing• May not be a strength of late stage manufacturing
organizations Develop initial cell culture and purification process
• Benefit to outsource for “platform” products such asantibodies− Utilizing a generic process at an experienced CMO often
saves time and money• For unique products with unknown performance, in-house
early development activities can be more cost-effective
From Clone to Clinic®
Outsourcing GMP Manufacturing of DS
Cell line and process already developed in-house• CMO and client often disagree on definition of a “developed
process” Outsource GMP production
• Minimal development activities necessary at CMO• Technology transfer through documentation and in-person
transfer meetings• Adapt process to run using equipment at CMO
− Different scale bioreactors− Alternate instrumentation for HPLC, pH, etc.
Deliverable is fully released active DS, ready for fill/finish
From Clone to Clinic®
Analytical Methods Development Outsourcing
Key component necessary to support process development andmonitor product stability• In process assays to monitor yield and performance critical for
effective decision making during process development• Determine key product release assays• Analytical development usually initiated in-house with methods
transfer to CMO for final development and qualification (orvalidation)
Some methods are routine and CMOs have generic SOPs• pH, osmolality, appearance, endotoxin, particulate matter
Analytical methods different for different products• Specific binding to therapeutic target• Bioassay is essential to determine potency
From Clone to Clinic®
Formulation Development Outsourcing
Knowledge of protein properties essential to initiate formulationdevelopment• Observed stability at various pH, temperatures, other
conditions• Tendency to aggregate, dissociate (multimers), oxidize, or
degrade through proteolytic cleavage Stability analysis performed rigorously by CMO using existing
knowledge as a basis for experimental design• Prior formulation development experience essential• Proper stability testing will insure selection of optimal
formulation Analytical method development and execution essential
From Clone to Clinic®
Drug Product Manufacturing Outsourcing
Fill/finish is often outsourced even when DS produced in-house
Selection criteria based on desired presentation of finalproduct• Lyophilized or liquid• Vial or pre-filled syringe• Storage temperature
Analytical capabilities essential for DP manufacturing CMO Deliverable is product in final configuration, ready for shipment
to distribution facility or clinic• DP vendors may provide packaging and distribution
services, or this may be outsourced to a third vendor
From Clone to Clinic®
Preparing an Effective RFP: A DS Example
Expected deliverables• When material needed and how much?• Analytical methods development, qualification, or validation?• Overall program timeline• Desired scale of final process
Process details• More detail will enable vendors to provide accurate pricing and
timelines• Information about desired product and potential variants essential
− Yield and purity obtained thus far in process development, ifknown
From Clone to Clinic®
DS Manufacturing Decisions
Prior to preparation of RFP for DS GMP manufacturingservices, customer must determine the following:• Production host
− Different CMOs have experience in mammalian cell culture,microbial fermentation, or both
• Desired product quantity to support preclinical and clinicalactivities− Determines scale and number of GMP runs; therefore
determines which CMOs can meet the demand• Timing of preclinical and clinical activities
− Customers often unrealistic about necessary developmenttimes
− CMOs often offer timelines that are difficult to achieve, inorder to obtain the business
From Clone to Clinic®
Effective Project Description
Statement of work with specific tasks and goals outlined• Prepare CHO production cell line using vector provided by
client− Deliverable: Fully characterized MCB (and WCB?)
• Develop cell culture process with yield of at least 1.0 g/L− Deliverable: Master batch record defining process
• Develop purification process with acceptable viralclearance and >50% product yield− Deliverable: Master batch record, results of scale-down
viral clearance study• Scale process to >200L scale; provide material from
engineering run to client for tox studies− Deliverable: 100 gm Bulk Drug Substance
From Clone to Clinic®
Ineffective Project Description for Drug Substance
Describe product and clinical approach in detail General statement of work with no delineated activities,
deliverables or timelines: “We need the product to support ourpre-clinical tox studies in June 2007 and to support humanclinical trials in Dec 2007”• Is there a cell line?• Desired (realistic) yield and purity of process?• Analytical methods?
Minimal process details: “The product is produced in CHOcells and purified by a two column procedure”• Scale and yield thus far?• Perfusion or fed-batch?• Type of columns?
From Clone to Clinic®
Sample RFP Table of Contents
1. Background and Objectives2. Scope of Services Requested
a. Analysis of Product Provided Materialb. Construction of Expression Vector, Cell Line, and RCBc. Preparation of Master (and Working) GMP Cell Banksd. Development and Scale-up of Cell Culture Processe. Development and Scale-up of Purification Processf. Quality and Analytical Support Servicesg. Production of DS for Tox Studies and Phase 1 Trialsh. Documentation Required
3. Project Estimates and Fee Schedule4. Qualifications5. Deadline for Submission of Proposals6. Appendices
From Clone to Clinic®
Process Information for RFP
Production cell line• Host cell system• Current productivity and conditions in which that
productivity is obtained (shake-flask, small bioreactor?)• Factors known to influence productivity
Purification methods• Number and types of chromatography steps utilized• Any information on viral clearance using existing process• Filtration or other steps currently used
− Scaleability of filtration and centrifugation steps
From Clone to Clinic®
Analytical Methods Information for DS RFP
Lot release tests and specifications if known• All methods and specifications should be listed• Provide product-specific or unusual methods to help CMO
provide accurate timeline and pricing Status of method development
• Will assays be transferred in only or is developmentneeded at the vendor?
• Assays should be qualified or validated? Analytical methods for MCB testing
• Must meet regulatory guidelines• Additional testing desired• Known issues with chosen host cell (if unusual)
From Clone to Clinic®
The Vendor Selection Process
Consider at least 5 – 6 vendors
Obtain a minimum of 3 competitive bids
Request contract terms as part of bid response
Talk to references
Capture data for future reference
From Clone to Clinic®
Sponsor Top Issues and Concerns
Ref: “Moving the Bioindustry into the Manufacturing Phase”, Coopers & Lybrand Survey, 1996
From Clone to Clinic®
Additional Sponsor Expectations
Rapid turn around time
On-time manufacturing
Cost-efficient processes
Up-to-date regulatory compliance
Customized manufacturing processes
Scale-up engineering
From Clone to Clinic®
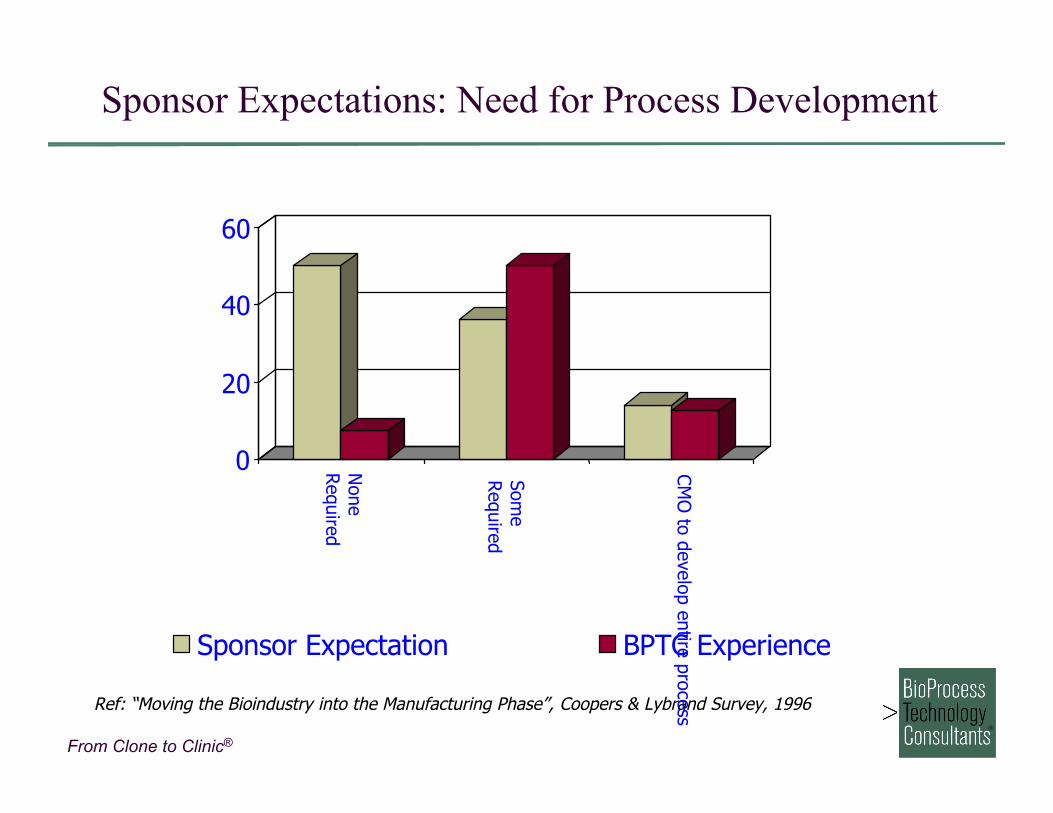
Sponsor Expectations: Need for Process Development
Ref: “Moving the Bioindustry into the Manufacturing Phase”, Coopers & Lybrand Survey, 1996
0
20
40
60
None
Required
Some
Required
CM
O to develop entire process
Sponsor Expectation BPTC Experience
From Clone to Clinic®
Selecting a CMO – One Example
From Clone to Clinic®
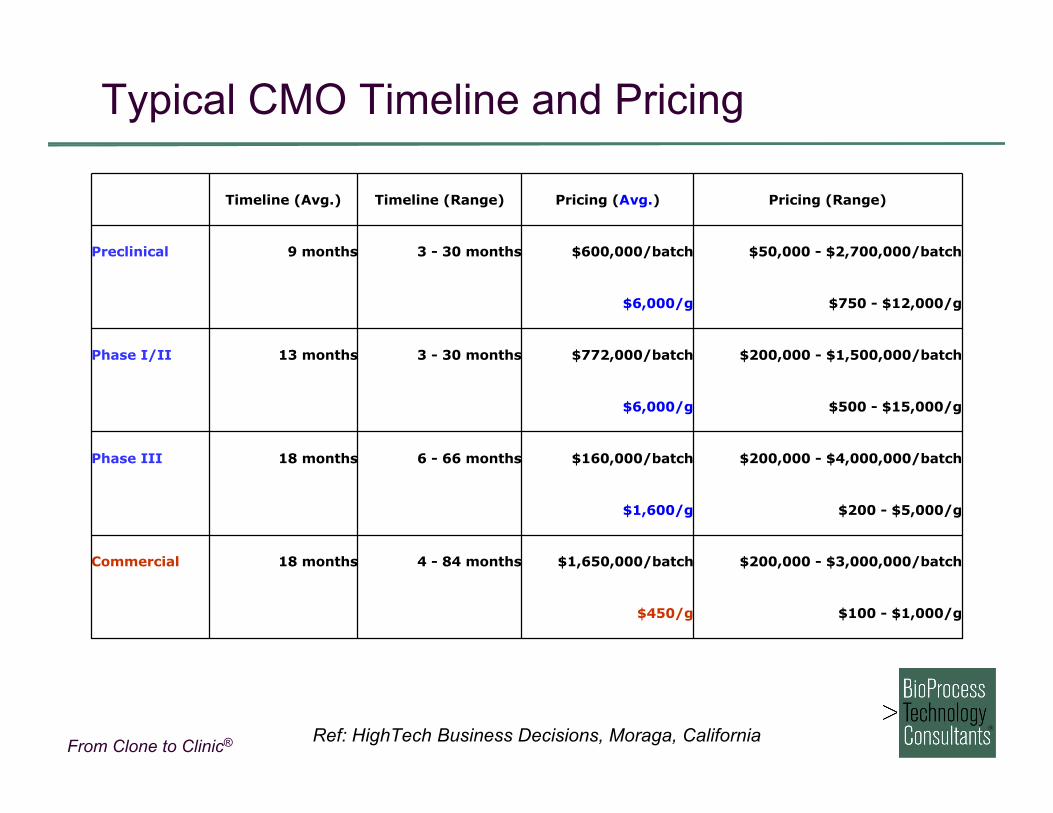
$100 - $1,000/g$450/g
$200,000 - $3,000,000/batch$1,650,000/batch4 - 84 months18 monthsCommercial
$200 - $5,000/g$1,600/g
$200,000 - $4,000,000/batch$160,000/batch6 - 66 months18 monthsPhase III
$500 - $15,000/g$6,000/g
$200,000 - $1,500,000/batch$772,000/batch3 - 30 months13 monthsPhase I/II
$750 - $12,000/g$6,000/g
$50,000 - $2,700,000/batch$600,000/batch3 - 30 months9 monthsPreclinical
Pricing (Range)Pricing (Avg.)Timeline (Range)Timeline (Avg.)
Ref: HighTech Business Decisions, Moraga, California
Typical CMO Timeline and Pricing
From Clone to Clinic®
Examples of CMO Manufacturing Costs
Costs listed are for process development and manufacture of earlystage clinical trial material (Phase I/II) for mammalian cell culture
From Clone to Clinic®
Essential Elements to Successful Outsourcing
Business Terms• Tie pay to performance• Pay attention to signals and be proactive• Establish the core team early• Keep the group small• Divide the key responsibilities• Have clear expectations about deliverables and timelines• Each relationship is unique
From Clone to Clinic®
The Sponsor/CMO Relationship
Finding the right match is key for success No ideal contractor for any one sponsor No ideal sponsor for any one contractor Not a traditional customer - supplier relationship Relationship is similar to a partnership “Customer is always right” adage does not apply exclusively to
Sponsor Typically not a “one-shot” deal Each relationship is unique Must understand each other’s culture
From Clone to Clinic®
Effect of Negotiations on the Relationship
ImplementationNegotiationSelection
From Clone to Clinic®
Why the Problems During Negotiation?
Realization that this is not a partnership• Fee for service relationship• CMO puts up no money, assumes no risk• CMO gets paid whether or not product is successful
Switch from process to deliverables• Focus on specific tasks to be performed, cost, and what
Sponsor will receive• Buying service not product• “Oh, you want us to do that too?”• “You want it when?”
From Clone to Clinic®
Why the Problems During Negotiation?
Risk avoidance becomes key objective• Contracts deal with worst cases• What-ifs breed distrust• Excessive coverage/risk transfer demanded
Sources of Risk• Business loss
− No efficacy, safety, cash, sales• Property loss
− Fire, loss/damage in transit, data destruction• Contractor performance
− Batch failure, non-compliance• Product liability
− Subject/patient adverse event
From Clone to Clinic®
Major Contracting Issues
Respective Obligations• Detail mutual responsibilities−Who, what, when, how−Standards for performance−Task and payment schedule
• Procedures for changes and deviations• Resource allocation• Procedures to remedy faulty performance−Discussion, arbitration, litigation−Refund vs. Rework−Limitation of liability
From Clone to Clinic®
Major Contracting Issues
Intellectual Property• Who is actually contributing knowledge and value vs. who
happens to be around when it is created• Ownership, right to license, right to negotiate, option• Joint inventorship – not as easy as it sounds!• Patents vs. Trade Secrets
− Patent: utility, novelty, non-obviousness, fulldislosure
− Trade Secret: kept secret, not generally known,commercial advantage
From Clone to Clinic®
Major Contracting Issues
Regulatory Compliance• Performance guarantee and certification• Contractor’s QC and QA responsibilities• Validation documentation and rigor• Control of applications• Reference rights• Disclosure of FDA inquires and inspections• Non-FDA obligations: EPA, OSHA, State, Federal, Foreign• Post-contractual needs and obligations
From Clone to Clinic®
Major Contracting Issues
Warranties, Indemnifications, and Remedies• Warranty – promise on current or future status• Indemnification – coverage against third party action• Remedies – rights in event of breach
Dispute Resolution and Enforcement
From Clone to Clinic®
Development and Supply Agreements
Purchase Order• Cost per gram vs. cost per batch
Development Agreement• Cost• Milestones• Access to process and ownership of technology
Supply Agreement• Duration• Market share and pricing• Cancellation notice, “take or pay,” etc.
From Clone to Clinic®
Goal: Successful Fee-for-Service Relationship
Sponsor gets• Fair price• Deliverables that meet
specifications andtimelines
• Competence andquality
• Excellent service
Vendor gets• Reasonable margin• No FDA problems or
hazard losses• Repeat business• Good reference
From Clone to Clinic®
Dos and Don’ts of Successful OutsourcingRelationships
Don’t say it’s urgent unless it really isShare your objectivesTake advantage of the Contractor’s experience and expertiseStick to your deadlinesDon’t assume things will happen just because you want them toDon’t blame the Contractor for things it can’t controlDon’t assume you are the Contractor’s only clientDon’t be a “serial shopper”Don’t be overly concerned about priceInvestigate significant differences before making decisionsDon’t change the project after it startsDon’t destroy your relationship over an occasional error
Remember the Golden Rule of Outsourcing: Treat your contractor theway you would like them to treat you
From Clone to Clinic®
Conclusions
Effective RFPs for any outsourced activity should generateproposals that can be compared
Detailed description of desired service essential Use Scope of Work format in RFP and request line by line
responses in proposal from CMO• CMO not always cooperative in providing breakdown
pricing Request quality/compliance history
• Formal pre-selection audit should be performed afterreceipt of proposals and before final choice
All manufacturing activities can be outsourced• Client has final responsibility for product quality, timeline,
and budget
From Clone to Clinic®
One final view of outsourcing…

From Clone to Clinic®
Thank you!
BioProcess Technology Consultants, Inc.289 Great Road, Suite 303
Acton, MA 01720
[email protected] (o)617-417-9240 (m)
www.bioprocessconsultants.com
From Clone to Clinic®
Appendix
From Clone to Clinic®
Success Rate and Turnover Data
Turnover statistics (2003/2004) No BLA products remained in the same stage
• All either approved or rejected 60 – 65% of Phase III products remained in Phase III
• ≤40% moved forward or failed 61 – 67% of Phase II products remained in Phase II
From Clone to Clinic®
Biopharmaceutical Production Objectives
Quality
Timeliness
Quantity
Cost
Safe for humans Meets standards (GMP) Reproducible
First to market launch Rapid material supply
Adequate productivity to meet clinicalsupply & market supply
Meet cost target Depends on dose and price Economics acceptable and
predictable
From Clone to Clinic®
Sample Final Product Specifications
Purity >98 %Purity typically determined by two or more assaysPotency As defined by assayProduct-related Impurities Identified for >1%
No single impurity >2%Host Cell Protein <100 ppmDNA <100 pg/doseEndotoxin <y eu/mgBased on dose & a limit of <50 eu/Kg body weight
From Clone to Clinic®
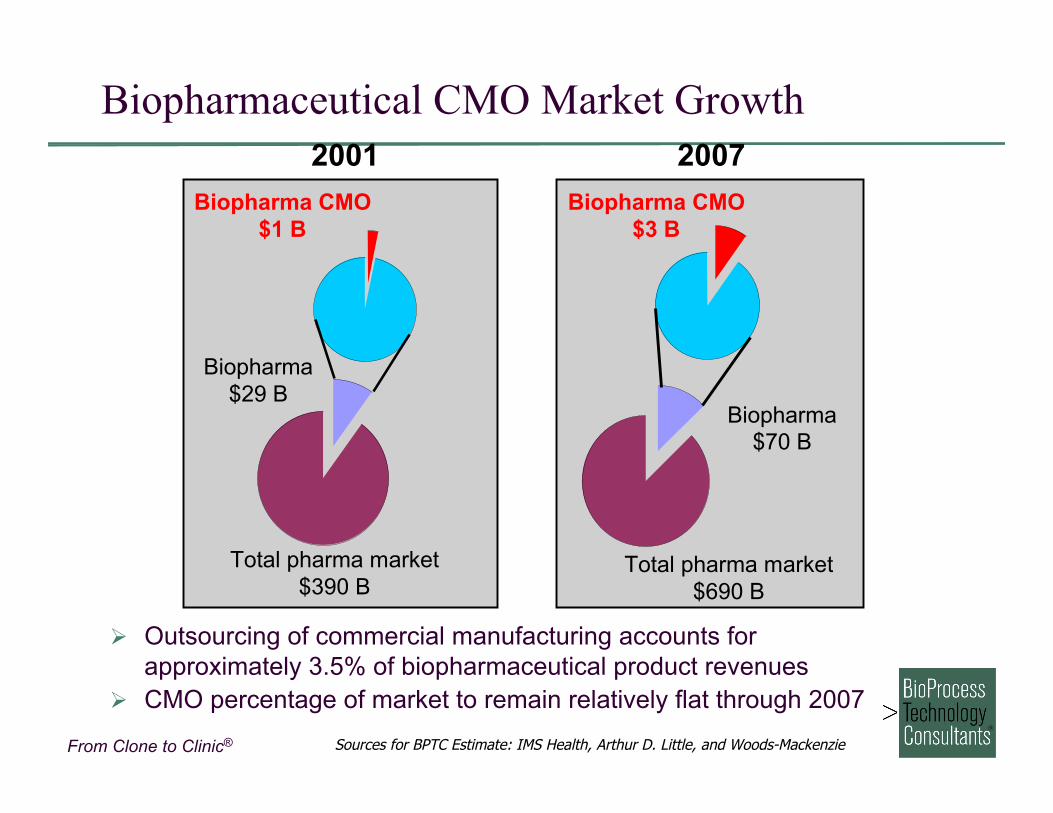
Biopharmaceutical CMO Market Growth
Biopharma$29 B
Biopharma CMO$1 B
Total pharma market$390 B
Biopharma CMO$3 B
Biopharma$70 B
Total pharma market$690 B
2001 2007
Sources for BPTC Estimate: IMS Health, Arthur D. Little, and Woods-Mackenzie
Outsourcing of commercial manufacturing accounts forapproximately 3.5% of biopharmaceutical product revenues
CMO percentage of market to remain relatively flat through 2007
From Clone to Clinic®
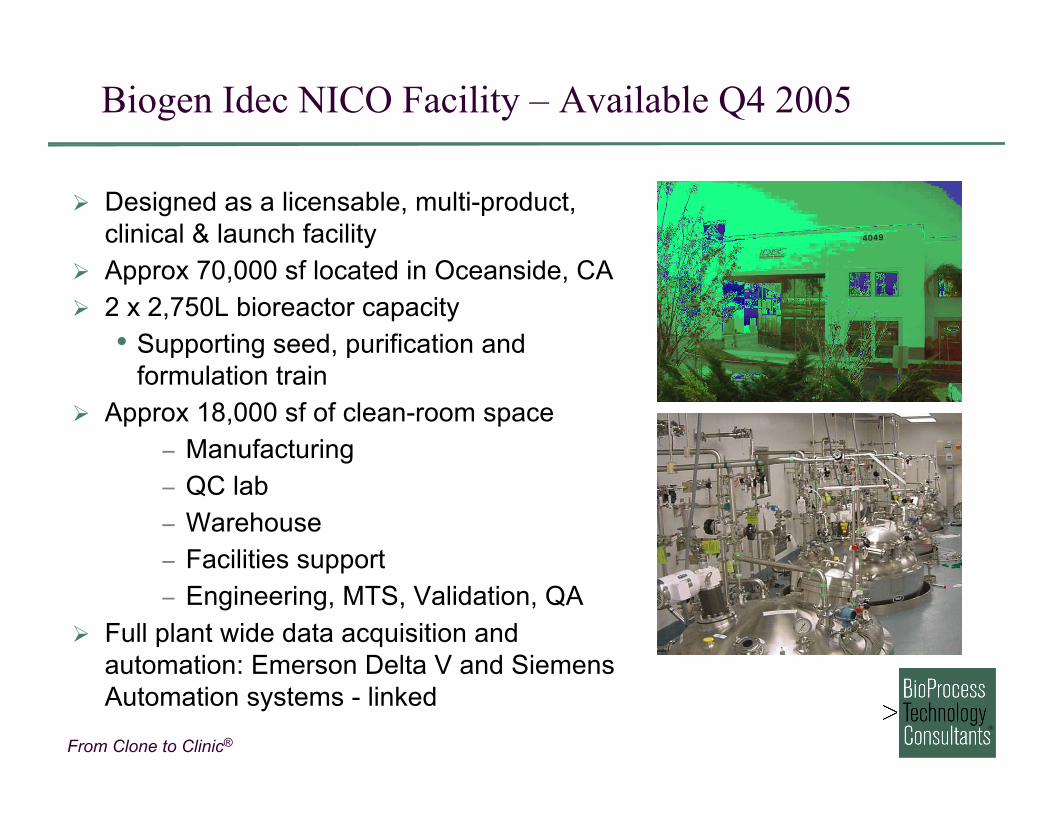
Biogen Idec NICO Facility – Available Q4 2005
Designed as a licensable, multi-product,clinical & launch facility
Approx 70,000 sf located in Oceanside, CA 2 x 2,750L bioreactor capacity
• Supporting seed, purification andformulation train
Approx 18,000 sf of clean-room space− Manufacturing− QC lab− Warehouse− Facilities support− Engineering, MTS, Validation, QA
Full plant wide data acquisition andautomation: Emerson Delta V and SiemensAutomation systems - linked
From Clone to Clinic®
Success Rate and Turnover Data
Turnover statistics (2003/2004) No BLA products remained in the same stage
• All either approved or rejected 60 – 65% of Phase III products remained in Phase III
• ≤40% moved forward or failed 61 – 67% of Phase II products remained in Phase II
From Clone to Clinic®
Manufacturing: Outsource or Perform In-House?
In-house
Capital for design, land, structure,equip
Utilize existing equipment & facilities Staffing & operating costs fixed
regardless of utilization Validation cGMP infrastructure & regulatory
compliance Impact on existing operations
Outsourcing
Finding, qualifying & negotiatingw/vendor
Monitoring, project management,inspection
Technology transfer Economies of scale Access to proprietary technology Actual work/delivered materials Loss of control Improve time to market