successful treatment of pityriasis rubra pilaris (type 1) under...
TRANSCRIPT
DOI: 10.1111/j.1610-0387.2009.07154.x Case Reports 1071
© The Authors • Journal compilation © Blackwell Verlag GmbH, Berlin • JDDG • 1610-0379/2009/0712 JDDG | 12˙2009 (Band 7)
SummaryPityriasis rubra pilaris (PRP) is oftendifficult to treat. A 65-year-old womenpresented with a two week history ofwidespread erythroderma and scal-ing with areas of sparing (nappesclaires). She also had follicular hyperk-eratoses and palmar fissuring. Theclinical picture and histology led tothe diagnosis of PRP. She failed torespond to initial therapy whichincluded topical and systemic corti-costeroids. She was then treated withintravenous methotrexate (MTX)15–30 mg weekly. Because of thepoor response we intensified herregime with infliximab (5 mg/kg).Altogether our patient received inflix-imab three times together with MTX,which was later given orally. Wereport for the first time the successfulcombination of infliximab and MTXfor the treatment of PRP.
Keywordspityriasis rubra pilaris – infliximab –methotrexate – combination of treatments
Clinical findingsThen patient appeared chronically illwith widespread erythematous patchesespecially of the upper body with roughfollicular hyperkeratoses. Further, severescaling, islands of uninvolved skin –“nappes claires” – as well as fissures of thehands were present (Figure 1, 2).
Laboratory diagnosticsLaboratory parameters were in the nor-mal range with exception of a HbA1c of 6.3 % (normal range 4.6–5.9) and a GT von 0.93 ukat/l (normal range forwomen � 0.65). Differential bloodcount, rheumatoid factors, desmoglein 1and 3, complement components C2 andC4, anticardiolipin IgG and IgM anti-bodies as well as ANAs and ANCAs werenormal.
HistologyIn the upper dermis a perivascular lym-phocytic inflammatory infiltrate withsome eosinophils was observed. At somepoints the inflammatory cell infiltratedinvolved the epidermis with vacuolar de-generation of basal keratinocytes. The al-cian blue stain revealed mucin depositsin the upper dermis. A superficialperivascular and lichenoid lymphocyticdermatitis and folliculitis were diag-nosed. Direct immunofluorescence ex-amination was negative.
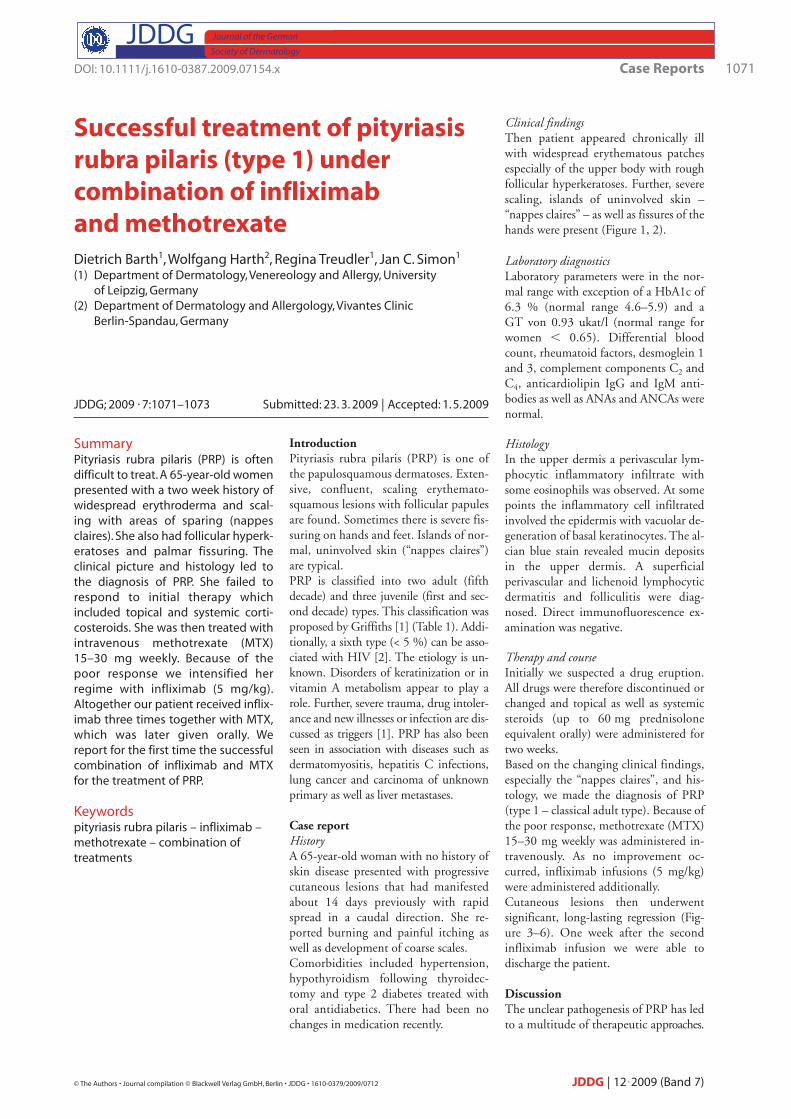
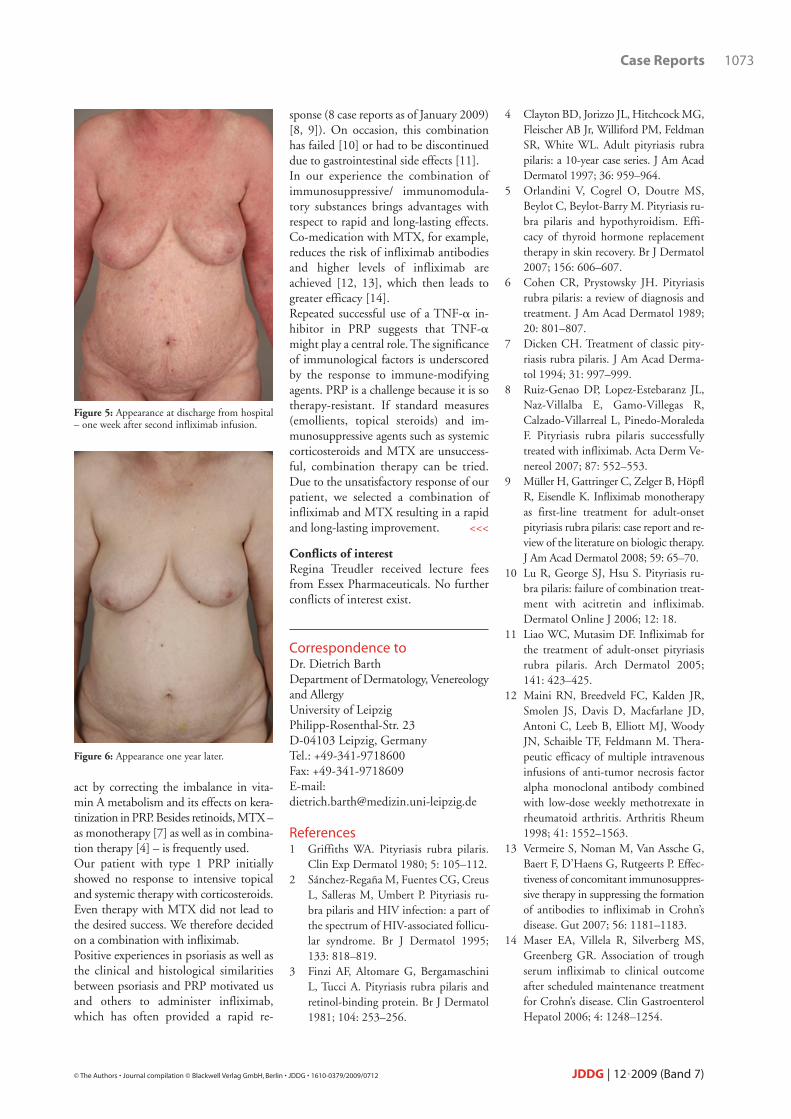
Therapy and courseInitially we suspected a drug eruption.All drugs were therefore discontinued orchanged and topical as well as systemicsteroids (up to 60 mg prednisoloneequivalent orally) were administered fortwo weeks. Based on the changing clinical findings,especially the “nappes claires”, and his-tology, we made the diagnosis of PRP(type 1 – classical adult type). Because ofthe poor response, methotrexate (MTX)15–30 mg weekly was administered in-travenously. As no improvement oc-curred, infliximab infusions (5 mg/kg)were administered additionally. Cutaneous lesions then underwent significant, long-lasting regression (Fig-ure 3–6). One week after the second infliximab infusion we were able to discharge the patient.
DiscussionThe unclear pathogenesis of PRP has ledto a multitude of therapeutic approaches.
IntroductionPityriasis rubra pilaris (PRP) is one ofthe papulosquamous dermatoses. Exten-sive, confluent, scaling erythemato-squamous lesions with follicular papulesare found. Sometimes there is severe fis-suring on hands and feet. Islands of nor-mal, uninvolved skin (“nappes claires”)are typical. PRP is classified into two adult (fifthdecade) and three juvenile (first and sec-ond decade) types. This classification wasproposed by Griffiths [1] (Table 1). Addi-tionally, a sixth type (< 5 %) can be asso-ciated with HIV [2]. The etiology is un-known. Disorders of keratinization or invitamin A metabolism appear to play arole. Further, severe trauma, drug intoler-ance and new illnesses or infection are dis-cussed as triggers [1]. PRP has also beenseen in association with diseases such asdermatomyositis, hepatitis C infections,lung cancer and carcinoma of unknownprimary as well as liver metastases.
Case reportHistoryA 65-year-old woman with no history ofskin disease presented with progressivecutaneous lesions that had manifestedabout 14 days previously with rapidspread in a caudal direction. She re-ported burning and painful itching aswell as development of coarse scales. Comorbidities included hypertension,hypothyroidism following thyroidec-tomy and type 2 diabetes treated withoral antidiabetics. There had been nochanges in medication recently.
Successful treatment of pityriasisrubra pilaris (type 1) undercombination of infliximab and methotrexateDietrich Barth1, Wolfgang Harth2, Regina Treudler1, Jan C. Simon1
(1) Department of Dermatology, Venereology and Allergy, University of Leipzig, Germany
(2) Department of Dermatology and Allergology, Vivantes Clinic Berlin-Spandau, Germany
JDDG; 2009 • 7:1071–1073 Submitted: 23. 3. 2009 | Accepted: 1.5.2009

For example, immunosuppressive/ im-munomodulatory systemic treatmentswith steroids, azathioprine, fumaric acidesters, MTX, retinoids, cyclosporine andothers have been employed. Due to the small number of cases (inci-dence 1/35000–1/50000) therapy is oftenbased on single case reports. Retrospectivestudies on the use of retinoids [3] andMTX [4] have to be viewed with caution,as spontaneous healing occurs in up to 80 % [5]. Most frequently retinoids areadministered [3–6]. As the histologicalfeatures of PRP resemble those of hypovi-taminosis A, vitamin A analogues possibly
1072 Case Reports
JDDG | 12˙2009 (Band 7) © The Authors • Journal compilation © Blackwell Verlag GmbH, Berlin • JDDG • 1610-0379/2009/0712
Table 1: PRP types as classified by Griffiths [1].
PRP type Nomenclature Frequency Features and course
1 Classic adult type 50 %Spreads caudally, 80 % healwithin 3 years
2Atypical adulttype
5 %No caudal spread, keratotic andeczematous lesions especially
3Classic juveniletype
10 %Benign type – healing usually af-ter 1 year, 75 % of cases followinfections
4Circumscript juvenile type
25 %Difficult to differentiate from pso-riasis, lesions on elbows and knees
5Atypical juvenile type
5 %Unfavorable prognosis, scleroderma-like lesions
Figure 1: Areas of unaffected skin – “nappes claires”.
Figure 2: Prominent follicular hyperkeratosis.
Figure 3: Appearance of the 65-year-old femalepatient two weeks after onset.
Figure 4: Appearance five weeks after onset andtwo weeks after the start of i.v. methotrexate.
sponse (8 case reports as of January 2009)[8, 9]). On occasion, this combinationhas failed [10] or had to be discontinueddue to gastrointestinal side effects [11].In our experience the combination ofimmunosuppressive/ immunomodula-tory substances brings advantages withrespect to rapid and long-lasting effects.Co-medication with MTX, for example,reduces the risk of infliximab antibodiesand higher levels of infliximab areachieved [12, 13], which then leads togreater efficacy [14]. Repeated successful use of a TNF-� in-hibitor in PRP suggests that TNF-�might play a central role. The significanceof immunological factors is underscoredby the response to immune-modifyingagents. PRP is a challenge because it is sotherapy-resistant. If standard measures(emollients, topical steroids) and im-munosuppressive agents such as systemiccorticosteroids and MTX are unsuccess-ful, combination therapy can be tried.Due to the unsatisfactory response of ourpatient, we selected a combination ofinfliximab and MTX resulting in a rapidand long-lasting improvement. <<<
Conflicts of interestRegina Treudler received lecture feesfrom Essex Pharmaceuticals. No furtherconflicts of interest exist.
Correspondence toDr. Dietrich BarthDepartment of Dermatology, Venereologyand AllergyUniversity of LeipzigPhilipp-Rosenthal-Str. 23D-04103 Leipzig, Germany Tel.: +49-341-9718600Fax: +49-341-9718609E-mail: [email protected]
References1 Griffiths WA. Pityriasis rubra pilaris.
Clin Exp Dermatol 1980; 5: 105–112.2 Sánchez-Regaña M, Fuentes CG, Creus
L, Salleras M, Umbert P. Pityriasis ru-bra pilaris and HIV infection: a part ofthe spectrum of HIV-associated follicu-lar syndrome. Br J Dermatol 1995;133: 818–819.
3 Finzi AF, Altomare G, BergamaschiniL, Tucci A. Pityriasis rubra pilaris andretinol-binding protein. Br J Dermatol1981; 104: 253–256.
act by correcting the imbalance in vita-min A metabolism and its effects on kera-tinization in PRP. Besides retinoids, MTX –as monotherapy [7] as well as in combina-tion therapy [4] – is frequently used. Our patient with type 1 PRP initiallyshowed no response to intensive topicaland systemic therapy with corticosteroids.Even therapy with MTX did not lead tothe desired success. We therefore decidedon a combination with infliximab.Positive experiences in psoriasis as well asthe clinical and histological similaritiesbetween psoriasis and PRP motivated usand others to administer infliximab,which has often provided a rapid re-
4 Clayton BD, Jorizzo JL, Hitchcock MG,Fleischer AB Jr, Williford PM, FeldmanSR, White WL. Adult pityriasis rubrapilaris: a 10-year case series. J Am AcadDermatol 1997; 36: 959–964.
5 Orlandini V, Cogrel O, Doutre MS,Beylot C, Beylot-Barry M. Pityriasis ru-bra pilaris and hypothyroidism. Effi-cacy of thyroid hormone replacementtherapy in skin recovery. Br J Dermatol2007; 156: 606–607.
6 Cohen CR, Prystowsky JH. Pityriasisrubra pilaris: a review of diagnosis andtreatment. J Am Acad Dermatol 1989;20: 801–807.
7 Dicken CH. Treatment of classic pity-riasis rubra pilaris. J Am Acad Derma-tol 1994; 31: 997–999.
8 Ruiz-Genao DP, Lopez-Estebaranz JL,Naz-Villalba E, Gamo-Villegas R,Calzado-Villarreal L, Pinedo-MoraledaF. Pityriasis rubra pilaris successfullytreated with infliximab. Acta Derm Ve-nereol 2007; 87: 552–553.
9 Müller H, Gattringer C, Zelger B, HöpflR, Eisendle K. Infliximab monotherapyas first-line treatment for adult-onset pityriasis rubra pilaris: case report and re-view of the literature on biologic therapy.J Am Acad Dermatol 2008; 59: 65–70.
10 Lu R, George SJ, Hsu S. Pityriasis ru-bra pilaris: failure of combination treat-ment with acitretin and infliximab.Dermatol Online J 2006; 12: 18.
11 Liao WC, Mutasim DF. Infliximab forthe treatment of adult-onset pityriasisrubra pilaris. Arch Dermatol 2005;141: 423–425.
12 Maini RN, Breedveld FC, Kalden JR,Smolen JS, Davis D, Macfarlane JD,Antoni C, Leeb B, Elliott MJ, WoodyJN, Schaible TF, Feldmann M. Thera-peutic efficacy of multiple intravenousinfusions of anti-tumor necrosis factoralpha monoclonal antibody combinedwith low-dose weekly methotrexate inrheumatoid arthritis. Arthritis Rheum1998; 41: 1552–1563.
13 Vermeire S, Noman M, Van Assche G,Baert F, D’Haens G, Rutgeerts P. Effec-tiveness of concomitant immunosuppres-sive therapy in suppressing the formationof antibodies to infliximab in Crohn’s disease. Gut 2007; 56: 1181–1183.
14 Maser EA, Villela R, Silverberg MS,Greenberg GR. Association of troughserum infliximab to clinical outcomeafter scheduled maintenance treatmentfor Crohn’s disease. Clin GastroenterolHepatol 2006; 4: 1248–1254.
Case Reports 1073
© The Authors • Journal compilation © Blackwell Verlag GmbH, Berlin • JDDG • 1610-0379/2009/0712 JDDG | 12˙2009 (Band 7)
Figure 5: Appearance at discharge from hospital– one week after second infliximab infusion.
Figure 6: Appearance one year later.
本文献由“学霸图书馆-文献云下载”收集自网络,仅供学习交流使用。
学霸图书馆(www.xuebalib.com)是一个“整合众多图书馆数据库资源,
提供一站式文献检索和下载服务”的24 小时在线不限IP
图书馆。
图书馆致力于便利、促进学习与科研,提供最强文献下载服务。
图书馆导航:
图书馆首页 文献云下载 图书馆入口 外文数据库大全 疑难文献辅助工具