successful academic healthcare merger” - aamc · successful academic healthcare merger ... case...
TRANSCRIPT

“Key Drivers of a
Successful Academic Healthcare Merger”
Glenn K. Geeting, MD

Goals of Presentation
Identify drivers of recent merger trends
Identify reasons for failed mergers in the 1990’s.
Elicit key drivers anticipated to lead to successful merger by an Academic Medical Center.
Discussion
4

Healthcare in US is changing
7

agar.io
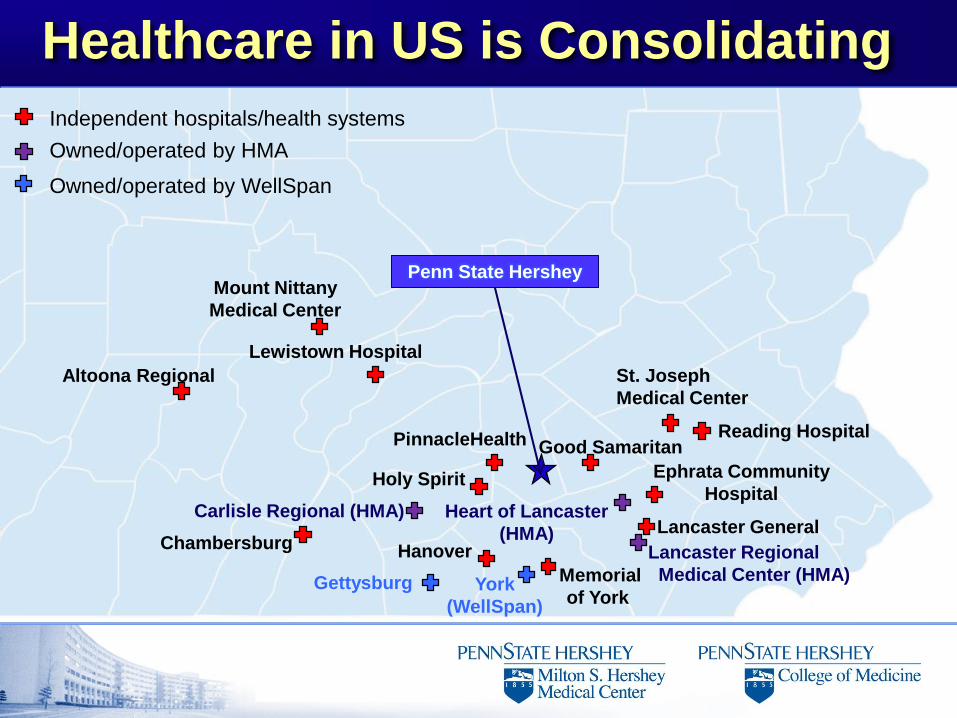
Independent hospitals/health systems
Owned/operated by HMA
Ephrata Community
HospitalCarlisle Regional (HMA) Heart of Lancaster
(HMA)
Lewistown Hospital
Holy Spirit
Good Samaritan
Lancaster Regional
Medical Center (HMA)
Altoona Regional
Memorial
of York
PinnacleHealth
Hanover
Mount Nittany
Medical Center
York
(WellSpan)
St. Joseph
Medical Center
Reading Hospital
Lancaster General
Penn State Hershey
Gettysburg
Owned/operated by WellSpan
Chambersburg
Healthcare in US is Consolidating

Johns Hopkins
PinnacleHealth
Hanover
Reading Hospital
St. Joseph
Medical Center
Memorial
of YorkYork
Lancaster General
Owned by/affiliated with WellSpan
Community Health
SystemsGeisinger
UPMC
Altoona Regional
Mount Nittany
Medical Center
Owned by/affiliated with Geisinger
Owned/operated by CHS
Seeking a partner/merger
Penn
Heart of Lancaster
Lewistown Hospital
Holy Spirit
Good
Samaritan
Ephrata Community
Hospital
Lancaster Regional
Medical Center
Carlisle Regional
Owned/operated by UPMC
Gettysburg
Chambersburg
Healthcare in US is Consolidating
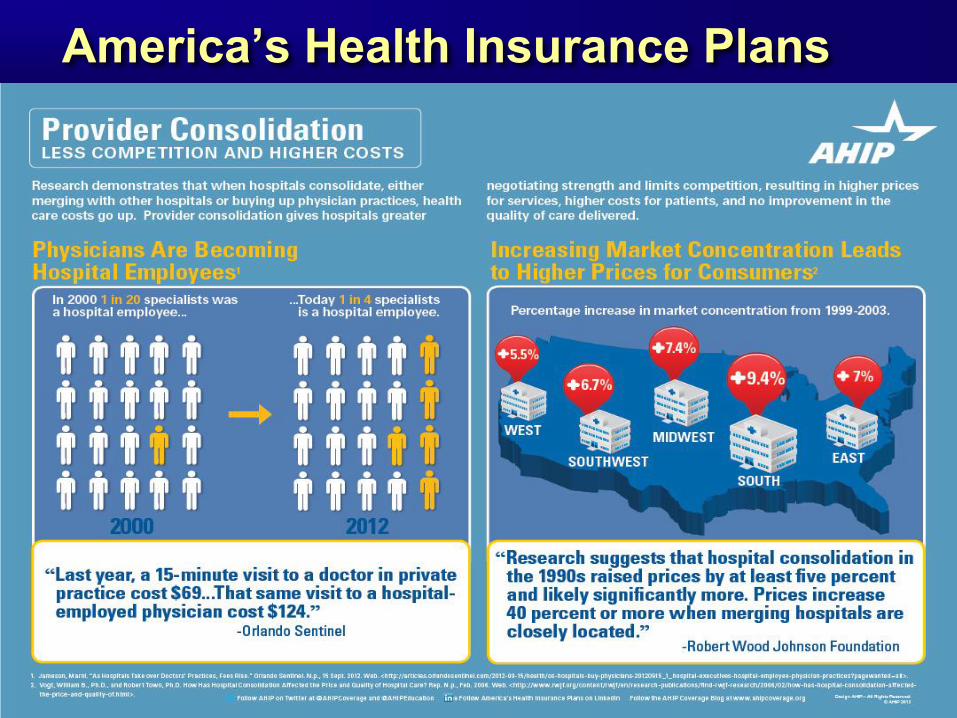
America’s Health Insurance Plans

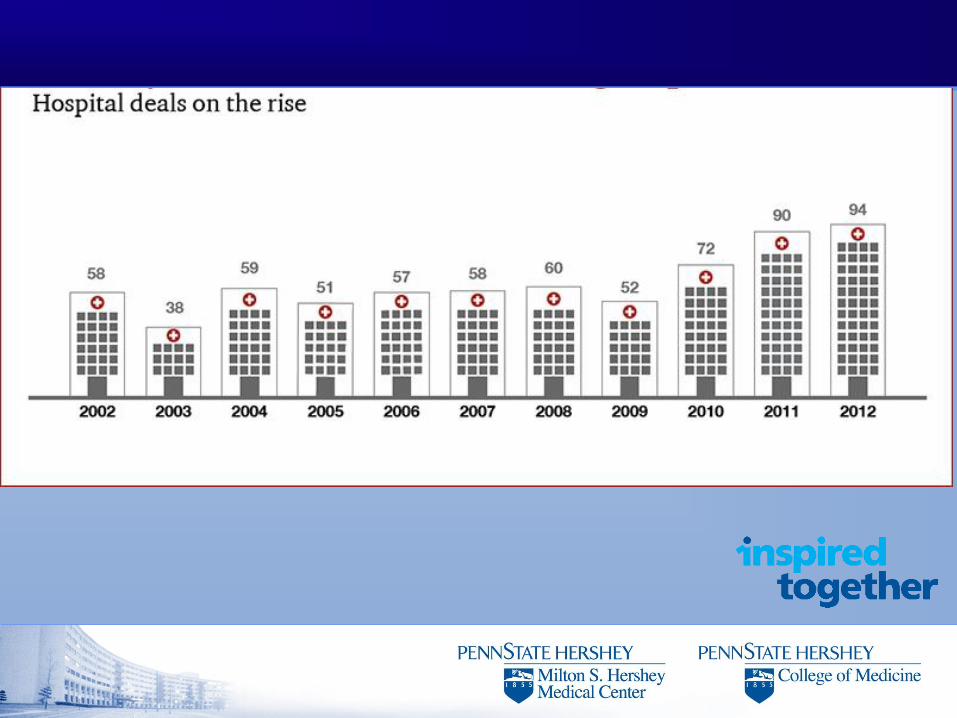
Pace of consolidation is increasing
71 hospital deals in 2015 announced as of Aug 31, the most since 1999
The top 5 companies are being consolidated into 3 massive corporations
Mathews AW, Health Law Speeds Merger Frenzy. Wall Street Journal, 9/22/15, B1-2.

Drivers of Healthcare Consolidation
Look at insurance, airlines, and telecommunications
national or international industries that are now oligopolies
Georgia Tech’s “rule of 3s”

“The ACA is the trigger.”• Robert Kocher, former White House health adviser
Cost is the biggest driver of healthcare reform
The Federal Trade Commission held a 2-day conference last year on healthcare consolidation

Three Basic Financial Drivers of Healthcare Consolidation Liquidity and balance sheet drivers
Economies of scale
Spreading fixed overhead costs to a larger base, gaining efficiency
Withstand systemic shocks
Operational metrics
Smaller hospitals desire a broader base to fill beds
“Uncontrolled variation is the enemy of quality.” Deming
Purchasing power

Case Study of a Failed MergerJaan Sidorov MD, Managed Care, November 2003
July 1997-November 1999
Geisinger Health System + Hershey Medical Center = Penn State Geisinger Health System
Both financially healthy
Climate of consolidation
Board of Directors
Chair appointed by Geisinger had the tie-breaking vote

Penn State Geisinger Health System
Advantages of Merging
Broad customer base, >1million people
No longer had to compete
Support of financially threatened academic health center
Access to greater capital
Integration of managed care principles
Greater negotiating leverage
Predicted 3y cost reductions of $105 million

Geisinger Health System
Northeast PA
Strong reputation for health care management
Geisinger Health Plan: not-for-profit HMO, physician-led, owned by the health system
Wanted the luster of affiliation with an academic health center

Hershey Medical Center
South Central PA
Penn State College of Medicine
Health insurance, education, and research costs were considerable
College of Medicine support formula
Academic structure, strong chairs of independent departments

”The Great Divorce” November 1999
“Winners and losers are inevitable”
Clinical and residency programs challenged with tackling leadership and ownership
Cost savings not realized. First year deficit of $30 million
Culture clash
strong academic departments vs. managing salaried physicians

Distrust from nearby providers and hospitals
The Final Straw- Microbiology service consolidation to Geisinger
Microbiology, Pathology, ID protest
“Long after the merger failed, there is still no shortage of unflattering anecdotes about delay, gaming, passive resistance, demeaning colleagues, bullying opponents, and failing to address conflicts of interest in a setting that was supposed to be dedicated to healing and service.”

Case Study of a Failed Merger
Lessons Learned
Leadership: manage winners and losers
Cultural differences are easily underestimated
Mergers do not automatically result in economies of scale
Not all stakeholders will welcome a merger
Mergers vs Systems
Unique definition in healthcare
Merger = combination of separate facility licenses into a single license
Allows shift of inpatient services across facilities
Reorganization or elimination of services
Potentially greater cost savings
May bypass state regulations
System = common ownership but separate facilities, licenses, and financial records
may impede clinical consolidation

Mergers vs Systems
Mergers in which hospitals consolidate financial reporting and licenses generate savings of approximately 14%: 2, 3, and 4 years after merger
Consolidation into Systems does not generate savings, even after 4 years
D. Dranove, R. Lindrooth , Hospital consolidation and costs: another look at the evidence. Journal of Health Economics 22 (2003) 983–997

Does Consolidation Affect Quality of Care?
Study of CA hospitals 1991-1996
No evidence that mergers and acquisitions measurably affect inpatient mortality, may increase myocardial infarction readmissions and early discharge for normal newborns
V. Ho, B.H. Hospital mergers and acquisitions: does market consolidation harm patients? Hamilton Journal of Health Economics 19 (2000) 767–791

9
* Source: Hospital Mergers and Acquisitions….Does Market Consolidation Harm Patients; Journal of Health Economics, March 2000
No Consolidation Pre
Merger
Post
Merger
Mortality
Rates
1991 1995 1991 1995
Heart
Attack
Mortality
9.6% 7.7% 9.7% 9.3%
Consolidation and Mortality

Reasons for failure in the 1990’s
Cultural differences
Emotional vs rational decision-making
Forced structure Failed to coordinate care
Information technology
Lack of payment reform/incentives
Health Affairs. November 2012;31:11 8
Drivers of a Successful Merger
Culture: everybody has a shared goal new unified values, mission & vision
Clear communications
Leadership: 2% of people in organization have huge impact on the other 98% (Ram Charan)
Collaboration is a key value
Ability to synchronize different points of view
10

Drivers of a Successful Merger
• Structured approach to managing change (ie.
don’t force change)
• Population Management / Grow Patient Base
– Payment reform will change provider behavior
11

Recommendations
Potential
Partners
Similar
Culture
Patient Base Triple
Aim
Change
Manage
ment
12

Recommendations
Communication (trust)
establish clear expectations
Develop capabilities for partnership
Learn from the past: rational decisions What is best for the new organization
Identify service lines that coordinate the continuum of care identify experts and develop teams
Have contingency plans13

Discussion

Group Members
Carolyn Barbieri
Glenn Geeting
Jerry Griffin
Brenda Mallory
John Potochny
Scott Russell
Sponsors: Jeff Miller, Mike Freeman 2

Interviews Conducted
Craig Hillemeier, MD, CEO of Penn State Hershey Medical Center and Health System, Senior Vice President for Health Affairs for Penn State, and Dean of College of Medicine
Robin Wittenstein, COO of Penn State Hershey Health System
Michael Freeman, Senior Director of Strategic Planning, Penn State Hershey Health System
Wayne Zolko, Associate Vice President for Finance and Business and Controller at Penn State Hershey Medical Center
Steve Ettinger, MD, Interventional Cardiology Program Director, E-MBA student with Penn State Smeal College of Business
R. Kevin Grigsby, MSW, DSW, 1st Senior Director, Member Organizational Development at Association of American Medical Colleges
David J Handel, MBA, former director of Indiana University Hospitals, and former executive vice president and chief operating officer, Clarian Health Partners, Indianapolis, Indiana.
Daniel A. Handel, MD, MBA, MPH, Chief Medical Officer and Executive Medical Director, Medical University of South Carolina 3

References
Mathews AW, Health Law Speeds Merger Frenzy. Wall Street Journal, 9/22/15, B1-2.
Washington, AE, Coye MJ, Feinberg DT. Academic Health Centers and the Evolution of the Health Care System. JAMA. 2013; 310(18): 1929-1930.
Handel, DJ, Kleit, SA, Handel, DA. The Development and Maturation of a Statewide Academic Health Care System: Clarian Health Partners/Indiana University Health. Academic Medicine. 2014; 89: 230-235.
Fuchs, VR. Current Challenges to Academic Health Centers. JAMA. 2013; 310(10): 1021-1022.
Fernandez B, Giger A. Three Prescriptions for Successful healthcare Mergers. Gallup Business Journal. Available at: http://www.gallup.com/businessjournal/179486/three-prescriptions-successful-healthcare-mergers.aspx.

References Saxena SB, Sharma A, Wong A. Succeeding in Hospital & Health Systems M&A and Why So Many Deals Have
Failed, and How to Succeed in the Future. Booz & Company. 2013.
Kastor JA. Mergers of Teaching Hospitals: Three Case Studies. Amer J Med. 2001;110:76-79.
Ahgren B. Is it Better to be Big? The Reconfiguration of 21st Century Hospitals: Responses to a Hospital Merger in Sweden. Health Policy. 2008;87:92–99.
Barro J, Cutler DM. Consolidation in the Medical Care Marketplace, A Case Study from Massachusetts. In National Bureau of Economic Research, Volume Title: Mergers and Productivity, ed. Kaplan SN. 2000. University of Chicago Press. Pg. 9-50.
Ho V, Hamilton BH. Hospital Mergers and Acquisitions: Does Market Consolidation Harm Patients? J Health Eco. 2000;19:767–791.
Dranove D, Lindrooth R. Hospital Consolidation and Costs: Another Look at the Evidence. J Health Eco. 2003;22:983–997.
Sidorov J. Case Study of a Failed Merger of Hospital Systems. Managed Care. 2003;Nov:56-60.
Andreopoulos S. Book Explores Successes, Failures of Academic Hospital Mergers Including UCSF-Stanford. Stanford Report, May 9, 2001. Available at: http://news.stanford.edu/news/2001/may9/book.html
Betbeze P. Greater Than the Sum of Its Parts Case Study: Bayhealth Medical Center Fierce Competitors Become Allies in Delaware Merger. Breakthroughs. 2010;September. Available at: http://www.healthleadersmedia.com/breakthroughs/257025/Hospital-Merger-and-Acquisition-Strategies
Maria Finarelli. Academic Medical Centers: What’s Their Role in Consolidating Health Care Markets? Health Strategies and Solutions. July 02, 2012
Institute of Medicine. Academic Health System Case Material. A corresponding document, Academic Health System Case Material. Available at: www.iom.edu/EssentialPrioritiesforAHSs.
Dzau V, Gottlieb G, Lipstein S, Schlichting N, Washington E . Essential Stewardship Priorities for Academic Health Systems. Institute of Medicine. 2014, September. Available at: http://www.iom.edu/Global/Perspectives/2014/AcademicHealthSystems.aspx
Meyer JA, Silow-Carroll S, Kutyla T, Stepnick LS, Rybowski LS. Hospital Quality: Ingredients for Success. A Case Study of Beth Israel Deaconess Medical Center. The Commonwealth Fund Available at: http://www.commonwealthfund.org/programs/quality/761_Meyer_hospital_quality_overview.pdf