stroke: steps to recovery
TRANSCRIPT

Stroke: Steps to Recovery
By
8/6/2020
Copyright Information
Copyright © 2020 MyFreeCE, Inc.

Course DescriptionThe goal of this course is to explain the different types of disabilities related to strokes (strokes) and to describe and assess the effectiveness of new therapeutic approaches and new equipment that is used for rehabilitation and shows promise for repairing damage and restoring movement.
Learning Objectives1. Explain the five basic types of stroke.2. List and explain the 3 aspect of the American Stroke Association’s stroke classification
system.3. List motor, vision, behavior, mentation, and language impairments related to both right
and left hemispheric strokes.4. Explain impairments related to cerebellar and brain stem strokes.5. Explain the five types of motor paralysis.6. Explain the concept of neuroplasticity and learned non-use and how that relates to
current therapeutic approaches to stroke impairment.7. Explain the differences among constraint-induced movement, shaping, active assist,
bilateral movement training, and body-weight supported treadmill training.8. Discuss how robot-assisted movement is utilized in therapy.9. Explain the difference between electromyographically-triggered neuromuscular
electrical stimulation and function electrical stimulation.10. Describe functional electrical stimulation.11. Explain how rhythmic and music therapy is used for rehabilitation.12. Explain how virtual reality and video games can motivate people to complete exercises.13. Discuss Vision Restoration Therapy.
Introduction
When a stroke occurs, parts of the brain are deprived of blood, which carries nutrients and oxygen. Within a few minutes, brain cells begin to die, and this can result in loss of brain function. While strokes, also referred to as brain attacks or cerebrovascular accidents, are the fifth leading (a drop from third place) cause of death in the United States, they are the leading cause of adult disability:
There are approximately 795,000 new victims of stroke each year and 4 million survivors, many with residual neurological deficits.
Strokes kill about 160,000 people in the United States each year, approximately 1 in 18 deaths.
Of those who survive a stroke, about 70% have residual impairment after one year.
Only about 5% of adults regain full function of their impaired arm after a stroke and at least 20% do not regain any functional use.
Between 1997 and 2007, prompt and more effective treatment resulted in a decrease in the death rate from stroke by 44.8%.
Many of those who survive strokes do so with impairments, increasing the need for rehabilitation services. It is projected that the number of people with strokes will increase because of the aging of the population. Additionally, people with spinal cord injuries may face some of the same physical challenges as those who have suffered a stroke (1, 2, 3, 4).
At one time it was believed that brain cells could not regenerate after a stroke, but more recent research has shown that the brain has the ability to heal itself to some degree. After a stroke, some cells don’t die for hours and others for days, so immediate intervention, as with thrombolytic agents, can reduce and prevent further injury to brain cells. If even 10% of cells remain viable, the brain can begin to repair itself, reorganizing and forming new connections as a result of neuroplasticity.
For many years, therapy focused on the first 3 months after a stroke because after 3 months people tended to plateau and show minimal improvement. Most exercises were passive or compensatory, to strengthen the unimpaired limb, such as learning to write with the unimpaired hand. However, there is hope now that more people can recover what they have lost. Some people, even those with long-standing paralysis, have been helped with some of the newer techniques and tools used for rehabilitation (1, 2, 3, 4).
What is a stroke/stroke?
While still usually referred to as a stroke, brain attack is a new term sometimes used for stroke or cerebrovascular accident (CVA), a change meant to equate a stroke to a heart attack. A stroke occurs when there is a disruption in blood flow to a part of the brain. There are two basic types of strokes. ischemic and hemorrhagic, and three additional categories.
Ischemic strokes
Ischemic strokes account for about 85% of all strokes. An ischemic stroke occurs when an artery that supplies blood to the brain becomes blocked.

There are different types of blockage:
Thrombosis in a large artery may block a large area of circulation. It is usually the result of atherosclerosis and primarily occurs in the elderly. It may occur suddenly or slowly over a period of days with episodes of transient ischemic attacks (TIAs).
Penetrating thrombosis in a small artery is known as a lacunar infarct, with lacunar referring to a cavity. This type of stroke occurs most frequently in those with hypertension or diabetes.
Emboli may travel through the arteries to the brain and block a vessel, most commonly the left middle cerebral artery. These are sometimes referred to as cardiogenic emboli because they most often result from heart dysrhythmias, such as atrial fibrillation, or heart surgery. They often occur rapidly and without any previous warning signs.
Cryptogenic strokes cannot be attributed to any specific cause (1, 5, 6).
Hemorrhagic strokes
A hemorrhagic stroke is caused by a rupture of a cerebral artery. As the artery bleeds into the brain tissue, the blood blocks the flow of oxygen and nutrients to the tissue and the pressure causes irritation and swelling that can be widespread. Patients who have hemorrhagic strokes usually have more severe deficits and a longer rehabilitation time than those with ischemic strokes. There are different types of hemorrhagic strokes.
Intracerebral hemorrhage
Occurs when there is bleeding into the brain substance, usually as a result of degenerative changes caused by hypertension and atherosclerosis. This type of hemorrhage may also result from brain tumors, medications (such as
anticoagulants) and illicit drugs (such as amphetamines, crack and cocaine). The bleeding is usually from an artery and may occur in the cerebral lobes, the basal ganglia, the pons, or the cerebellum. An intracerebral hemorrhage usually occurs rapidly with no warning and, if severe, may result in death.
Intracranial aneurysm
Occurs when a weakened, ballooning wall of a cerebral artery bursts. Any artery in the brain can develop an aneurysm, but they are most common at the Circle of Willis, where there is bifurcation of the large arteries. The cause is not clear, but may relate to congenital defects or be the result of hypertension and atherosclerosis.
Arteriovenous malformations (AVMs)
Congenital abnormalities that cause arteries and veins to form a tangle without a capillary bed. The lack of capillaries causes the arteries and veins to dilate and eventually rupture. AVMs are a common cause of hemorrhagic strokes in young people.
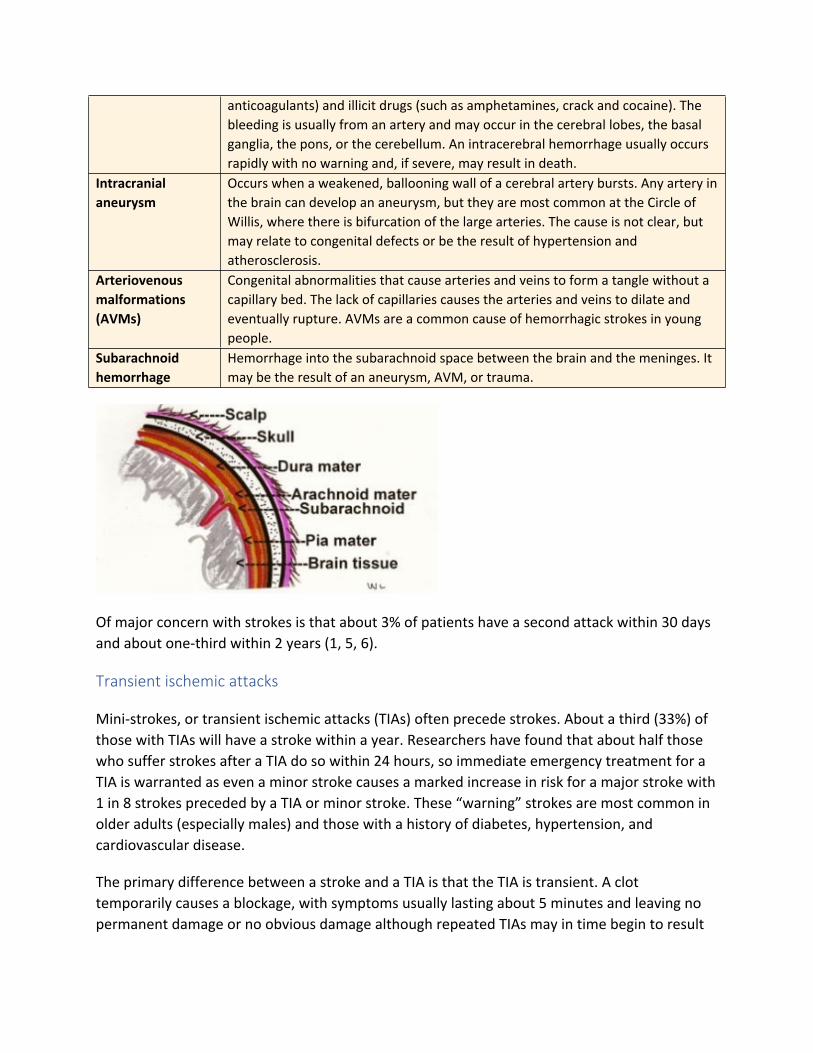
Subarachnoid hemorrhage
Hemorrhage into the subarachnoid space between the brain and the meninges. It may be the result of an aneurysm, AVM, or trauma.
Of major concern with strokes is that about 3% of patients have a second attack within 30 days and about one-third within 2 years (1, 5, 6).
Transient ischemic attacks
Mini-strokes, or transient ischemic attacks (TIAs) often precede strokes. About a third (33%) of those with TIAs will have a stroke within a year. Researchers have found that about half those who suffer strokes after a TIA do so within 24 hours, so immediate emergency treatment for a TIA is warranted as even a minor stroke causes a marked increase in risk for a major stroke with 1 in 8 strokes preceded by a TIA or minor stroke. These “warning” strokes are most common in older adults (especially males) and those with a history of diabetes, hypertension, and cardiovascular disease.
The primary difference between a stroke and a TIA is that the TIA is transient. A clot temporarily causes a blockage, with symptoms usually lasting about 5 minutes and leaving no permanent damage or no obvious damage although repeated TIAs may in time begin to result
in permanent damage. Small clots are more readily absorbed through the body’s natural defense mechanisms than larger clots (1, 72, 73).
Cryptogenic strokes
Cryptogenic strokes are those for which the cause cannot be determined. This type of stroke comprises about 25% of the total and tends to have a higher incidence in African Americans and Hispanics than in other ethnic groups. Some possible causes of cryptogenic strokes include:
Atrial fibrillation: May increase the risk of clots and stroke more than 5 times. Patent foramen ovale: About 1 in 4 adults have a patent foramen ovale, and clots may form
and travel to the brain. Thrombophilia: Increases the risk of blood clotting. Aortic arch atheroma: A piece of plaque may become dislodged and travel to the brain.
Brain stem strokes
The brain stem controls all of the basic activities of the CNS. The degree of symptoms depends on the size of the clot, the amount of occlusion, and how fast the blood flow can be restored. Some patients may have vertigo, dizziness, and impaired balance without one-sided paralysis or weakness that is typical of other types of strokes. Brain stem strokes may result in a locked in state in which the patient is unable to speak and can move only the eyes.
Stroke Assessment
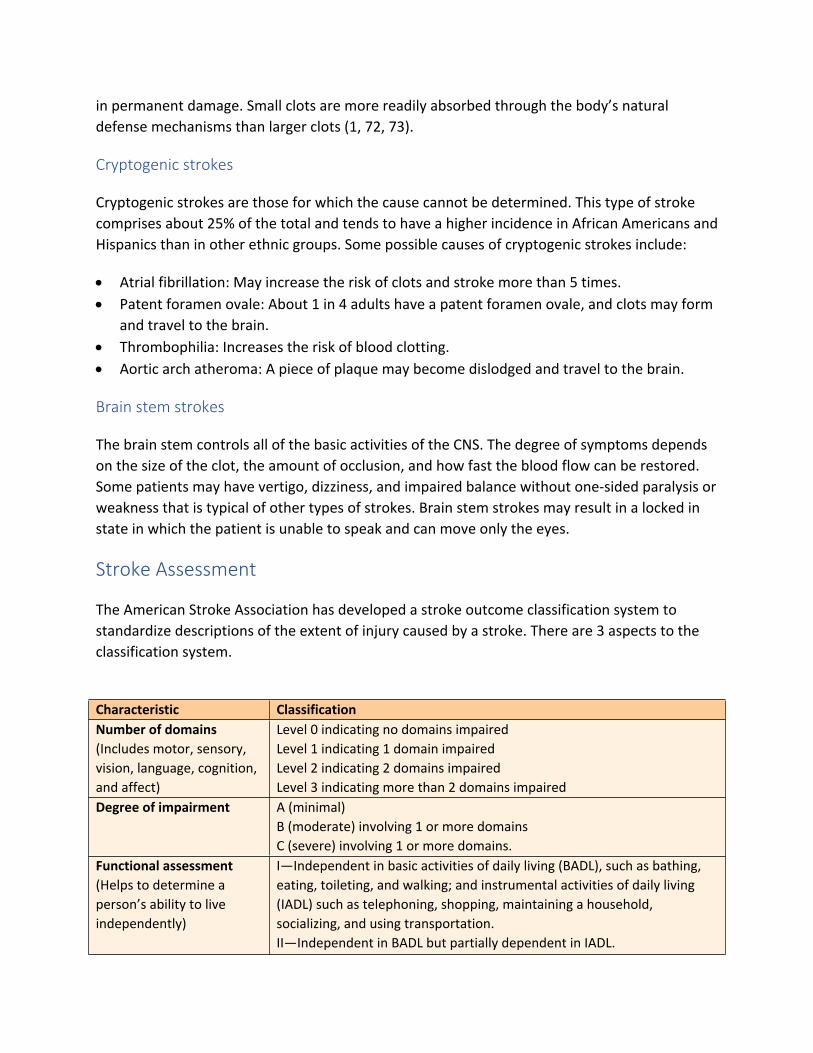
The American Stroke Association has developed a stroke outcome classification system to standardize descriptions of the extent of injury caused by a stroke. There are 3 aspects to the classification system.
Characteristic ClassificationNumber of domains(Includes motor, sensory, vision, language, cognition, and affect)
Level 0 indicating no domains impairedLevel 1 indicating 1 domain impairedLevel 2 indicating 2 domains impairedLevel 3 indicating more than 2 domains impaired
Degree of impairment A (minimal)B (moderate) involving 1 or more domainsC (severe) involving 1 or more domains.
Functional assessment(Helps to determine a person’s ability to live independently)
I—Independent in basic activities of daily living (BADL), such as bathing, eating, toileting, and walking; and instrumental activities of daily living (IADL) such as telephoning, shopping, maintaining a household, socializing, and using transportation.II—Independent in BADL but partially dependent in IADL.

III—Partially dependent in BADL (<3 areas) and IADL.IV—Partially dependent in BADL (3 or more areas)V—Completely dependent in BADL (5 or more areas) and IADL. (7)Only I and II can live independently with no or little assistance. Level III requires much assistance and Levels IV and V cannot live independently.
The National Institutes of Health has developed the NIH Stroke Scale, which is now commonly used to assess the degree of impairment after a stroke. The higher the score, the greater the disability.
NIH Stroke Scale1 Level of consciousness a. Response to simple questions b. Ability to state month and age c. Ability to open/close eyes and grip with non-paretic hand.
Each section scored 0 to 2
2. Best gaze (horizontal eye movements) Scored 0 to 23. Visual (tests visual fields) Scored 0 to 34. Facial palsy (show teeth, raise eyebrows, close eyes, grimace) Scored 0 to 35. Motor arm (ability to hold arm extension at 45 and 90 degrees) Scored 0 to 4, UN for
amputation or joint fusion6. Motor leg (ability to hold leg at 30 degrees) Scored 0 to 4 or UN7. Limb ataxia (finger-nose, heel-shin) Scored 0 to 2 or UN8. Sensory (pinprick response) Scored 0 to 29. Best language (Describe picture, name items, read text) Scored 0 to 310. Dysarthria Scored 0 to 2, UN for
intubated/physical barrier11. Extinction and inattention (determines is bilateral testing done simultaneously blocks sensations on one side.
Scored 0 to 2
(77)
The extent of damage as well as the area affected by the stroke determines the type of residual disability. There are 4 main parts to the brain: the right cerebral hemisphere, the left cerebral hemisphere, the cerebellum, and the brain stem.

Most strokes occur in the right or left hemisphere, but even within those hemispheres, the exact location of the damage can affect the outcome. For example, if there is damage to the frontal lobe, where reasoning is processed, there may be more evidence of memory and learning difficulties as well as increased frustration with rehabilitation efforts. With a stroke, there may be impairment of some or all bodily functions.
Area Right hemisphere Left hemisphere Motor Left paralysis/ paresis. Right paralysis/paresis.Vision Left visual field deficit (homonymous
hemianopsia).Spatial and perceptual deficits may cause people to misjudge distance and interfere with fine motor skills required to dress.
Right visual field deficit.
Behavior Impulsivity and lack of awareness regarding disability may lead people to do things that are dangerous, such as driving or walking without an assistive device.People may develop “left-sided neglect,” ignoring and not perceiving things or people on their left side as well as denial of impairment.May become easily depressed.
Slow and cautious behavior may result, and people may need frequent instruction for even simple tasks and reinforcement.May become depressed.
Mentation May have loss of short-term memory.Easily distracted.
May have altered intellectual ability that can include loss of short-term memory as well as

May have trouble following directions such as up/down or front/back.May have difficulty finding objects and understanding maps.
difficulty learning new information and understanding concepts and generalizations.May have difficulty with mathematics and skills requiring reasoning or organizing.May have problem reading, writing, and learning new material.
Language Intact. May have expressive, receptive, or global aphasia.
Stroke in brain stemThe brain stem, located at the base of the brain, controls the major life support systems of the body, such as the cardiac and respiratory systems. Brain stem attacks often result in death, but if people survive, they may have a number of different problems:
Cardiac and respiratory dysfunction Lack of temperature control Imbalance and lack of coordination Quadriplegia or quadriparesis Dysphagia Dysarthria Visual deficits Coma. Locked in syndrome.
Stroke in cerebellumThe cerebellum receives sensory information from the spinal cord and us involved with coordination, movement, and balance. Strokes are rare in the cerebellum, but they may have severe results:
Ataxia, inability to walk Nausea and vomiting Dizziness and headache
(1, 5, 6)
A major problem encountered by people with strokes is paralysis because it interferes with mobility and with the ability to live independently. Damage anywhere along the motor pathway of the nerve, from the brain, through the spinal cord and to the muscle, can result in paresis (weakness) or if the communication is completely disrupted, paralysis. Spinal cord injuries,

although different from strokes, can result in similar types of paralysis because of damage to the motor pathway.
It can be difficult to delineate paresis from paralysis. Weakness may progress to paralysis, and paralysis may be reversed with nerve regeneration or overgrowth. Paralysis often makes a change in muscle tone, which may result in a limb becoming flaccid or spastic. While paralysis may be confined to an individual muscle, it is usually more widespread, affecting an entire side of the body or an entire limb. In some cases, people may develop a global paralysis/paresis with generalized weakness throughout the body.
There are a number of sensations that may be present with paralysis/paresis, including numbness, tingling, and pain.
Types of paralysisMonoplegia Paralysis of one extremity. This may result if there is isolated brain damage.Diplegia Paralysis affecting the same body region on both sides, such as both arms, both sides
of the face, both legs.Hemiplegia Paralysis of one side of the body, right or left. Hemiplegia is the most common type of
paralysis found after a stroke. Vocal chord paralysis may also occur.Paraplegia Paralysis of both lower extremities and part of the trunk.Quadriplegia Paralysis of all four extremities and all or most of the trunk. Extensive quadriplegia
may occur with a stroke of the brain stem.
(5, 8)
What are new trends in post-stroke rehabilitation?
The goal of any rehabilitation program for those who have had a stroke or spinal cord injury is for the person to regain as much functional independence as possible, allowing the person to return to an active life in the family and the community. A thorough and adequate assessment is an absolute requirement for any rehabilitation program so that realistic goals can be set and the proper mode of treatment instituted for each individual.
Research has demonstrated that there are predictive elements. For example, the probability of regaining dexterity in a flaccid upper extremity can be predicted with good accuracy at 4 weeks. Also, the inability to voluntarily control the leg at 1 week coupled with lack of emergence of arm control by the 4th week often leads to poor outcomes at 6 months. However, new research suggests that therapy, even in chronic stroke patients may show positive results.
Strokes are often classified according to the length of time since the event:
Acute—up to 3 months

Sub-acute—3-6 months Chronic—more than 6 months
Because there is no real curative treatment for the after-effects of stroke, rehabilitation offers the best chance for people. However, despite numerous studies, there is no clear-cut evidence about the type of rehabilitative care that is the most efficacious.
A review of numerous studies found that programs that focused on impairment, such as biofeedback, neuromuscular or transcutaneous nerve stimulation and fitness programs, failed to produce substantial functional improvements. Additionally, the Bobath or neurodevelopmental treatment (NDT), which is similar to the patterning that is used with children with cerebral palsy, has not shown clear-cut evidence to support its use.
There is, however, good evidence for functional training, such as constraint-induced movement therapy, treadmill training with or without body weight support, and aerobics (2).
Neural (cortical) plasticity
The concept of neuroplasticity, the ability of the central nervous system to modify connections by strengthening or weakening them or forming new connections, is central to new concepts in rehabilitation. It’s clear that the old concept that the brain could only generate neurons during the early years of life is incorrect. There is now clear evidence that the brain retains the ability to respond to changes and strives to heal itself.
New neural connections can form. At a child’s birth, each neuron contains about 2500 connections, but by age 2 or 3, each neuron has about 15,000 connections. Over time, this number lessons because neuroplasticity can result in creation of new connections or loss of old ones—those that are inefficient or unused. After a stroke, neurons can take over the function of those that have died. Through axonal sprouting, healthy axons can grow new nerve endings to reconnect neurons where damage has broken the pathway.
Neuroplasticity helps to heal the brain in 4 ways:
Functional map extension: Healthy cells surrounding an area that is damaged take over the function of the missing cells.
Compensatory masquerade: Existing neural pathways reorganize to compensate for damaged areas of the brain.
Homologous region adoption: A new area of the brain takes over the function of a distant area that was damaged.
Cross-model reassignment: One sensory area is enhanced to compensate for losses of another sensory area (such as the enhanced sense of touch or hearing in those who are blind) (9).

The basic tenant of neuroplasticity is that brain activity promotes and stimulates reorganization. This tenant is paramount to many of the new therapies for stroke patients.
The organization of the cortex of the brain, cortical organization, is often described in terms of maps, showing how different parts of the brain relate to sensory input. This mapping is important in helping researchers determine the degree of damage and a plan for rehabilitation. For example, researchers have learned that if 37% of the map area related to hand function is damaged, there is complete loss of function of the hand.
Researchers have also discovered there is both a fast and slow form of plasticity. The fast form can occur within minutes but is relatively transitory. The slow form may take days or weeks but results in changes in cortical organization and the results are persistent (3, 9, 10).
US NIH
A finding that is significant for rehabilitation is that, while new axons can form rapidly, the neurons require stimulation through activity to promote connection. Animal studies have shown that, if there is paralysis and no activity, the neurons surrounding the damaged area begin to die as well, resulting in further impairment. Thus, neurons must be stimulated in order to retain the neurons that survive and to promote new connections. The phenomenon of

“learned non-use” makes the recovery of functions in the extremities a challenge for rehabilitation.
Essentially, when there is damage to brain cells, the part of the body that is linked through the motor pathway to those cells loses mobility, forcing the person to compensate by using other parts of the body. After a period of time, even if the brain heals itself and readapts, the body has “learned” that part of the body cannot function. Therefore, timing of rehabilitative efforts is critical.
Animal studies have shown that if rehabilitation is started too soon, it can increase brain damage, suggesting therapy should be delayed for a week or two. Studies are in progress to determine the optimal time to begin therapy after a stroke, not so soon as to cause damage but not so late as to incur atrophy (3, 9, 10).
Since stimulating the neurons through activity promotes neurogenesis and new connections, therapy aims at promoting this through motor activities, practicing the same movement repeatedly in order to “jumpstart” the process of rebuilding nerves. Forcing activity, such as supported walking on a treadmill, can repair damage.
However, there is a fine line. If the activity is repeated too much, there can be excessive regeneration that interferes with other connections, so that the person may gain in one area of function and lose in another. Promising studies indicate that drugs that increase availability of norepinephrine in the brain stimulate synapses, making it easier for them to form connections with other nerves (3, 9, 10).
Interestingly, the success of cochlear implants has demonstrated aspects of brain plasticity as the brain adjusts to the implant and begins to process and make sense of sound impulses it had not been receiving, allowing the person to understand and begin to produce understandable speech. Most people initially experience sound as undifferentiated noise, but as the brain adapts, usually within 3 to 5 months, people can begin to understand words even over the telephone, especially those with previous hearing.
Those without previous hearing, especially those fluent in sign language, have more difficulty because sign language is processed in the visual parts of the brain, competing with the hearing parts of the brain, and compensating for this competition is an important concept in neuroplasticity (74).
Many biomedical companies are now targeting neuroplasticity and developing applications to exploit the new knowledge about the ability of the central nervous system to modify and form new connections. Some researchers have focused on stroke motor rehabilitation but others are working on language, hearing, and vision. The next few years should give rise to many new innovations for rehabilitation (11).

What are some of the new therapies being used for rehabilitation?
There are a number of new therapeutic approaches that are being used at rehabilitation centers across the United States. These therapies are not mutually exclusive. Often, two or more therapies are combined in the rehabilitation plan for an individual, depending upon the extent of impairment. Because applying the concept of neuroplasticity to rehabilitation is still essentially in its infancy, there are on-going studies with all of the following therapies, so definitive judgments about which are the most effective and at what point in the rehabilitation process are not yet clear.
Constraint-induced movement therapy
Constraint-induced movement therapy (CI or CIMT) was developed by Dr. Edward Taub, who believed that people who have developed a weakness related to a stroke are discouraged from using the weakened side (learned non-use) from initial failures. He developed CIMT to counteract the learned non-use for those who may have pronounced weakness but are able to extend their wrists and move the affected arm and fingers.
A number of studies have shown that people with chronic or acute strokes receiving this therapy showed definite improvement, far more than control groups doing a general fitness program. Follow-up studies have demonstrated that the large improvements noted after therapy persisted at the 2-year mark. Another important finding is that the improvements seen in the clinical setting appeared to carry over into the home environment.
CIMT includes the following:
Constraining the uninvolved extremity (arms only). Forced use of the weakened limb for 90% of waking hours. Massed practice.
In practice, constraining of the uninvolved arm was originally done by placing the arm in a sling to prevent its use; however, for safety reasons, some centers have substituted a glove to remind people not to use the arm or a mitt (specialized or an oven-type mitt) that encloses the lower arm and/or hand, preventing the use of the hand and fingers.

W. Lockwood
This constraint is kept in place for 90% of waking hours to force use of the affected limb. Massed practice is an essential element of the therapy. Intensive therapy involving use of the affected extremity is done for 6 hours a day with a 1-hour break, 5 days a week, for 2-3 weeks (10, 12, 13). The intensive training involves functional exercises, including practicing daily activities such as eating, dressing, or dialing a phone. Shaping (adaptive task practice) techniques are often combined with CIMT.
A typical functional activity would involve performing a task for a set number of times repeatedly for 15-20 minutes. The activity may be broken down into component exercises; for example, using a phone might first involve exercises to flex fingers and grasp (8).
CIMT has also been used successfully with lower limbs, but the uninvolved leg is not constrained since both legs are needed for balance and ambulation. Massed practice for the leg includes “treadmill walking, over-ground walking, sit-to-stand, lie-to-sit, step climbing, various balance and support exercises) with a partial body weight support harness when necessary for 7 hours/day with interspersed rest intervals over 3 weeks.” Forced use and mass practice are done for the lower extremities (13).
The use of CIMT has been extended to include those with traumatic brain injuries, spinal cord injuries, and hip fractures. It is believed that this technique stimulates the damaged area of the brain, promoting intense cortical reorganization and increasing the area of the cortex that innervates the affected limb (10, 12, 13).
Some concerns about CIMT have been lack of patient compliance with such a rigorous program and safety, one of the reasons that some programs no longer use the sling but opt for a glove instead. Some researchers, in fact, believe that constraint isn’t necessary if people use the
affected arm as much as possible. The issue of compliance is being dealt with in some studies where variations to the standard CIMT are being studied. One modified version involves daily half-hour exercise sessions with just 5 hours of restraint daily over a 10-week period. A number of studies are currently underway to determine the best application of CIMT (15).
A recent study compared results of two groups of patients with paresis or paralysis of an upper extremity in the sub-acute phase of stroke recovery. Both groups had repetitive exercises 5 days a week for two weeks, but one group’s unaffected arms were restrained while the other group’s unaffected arms were not restrained. The outcomes for both groups were the same, suggesting that it is the exercise rather than the restraint that is most effective although neither group received exercises with the same intensity as others in research projects that showed CIMT with constraints to be superior (36).
Shaping (adaptive task practice)
Shaping therapy was conceived as a separate alternative therapy building from the principles of CIMT, but the two are currently often combined in rehabilitation programs. Shaping is based on conditioning and positive reinforcement: Patients are trained individually to perform increasingly difficult tasks with their affected arm, and then are rewarded for improvement (16).
One major difference between shaping and CIMT is that shaping exercises—if done alone—are typically done for 90 minutes each day rather than 6 hours. Shaping involves approaching objectives in small steps by completing just part of a task and then making the tasks more difficult as the patient shows progress. Shaping also does not involve the use of constraints. It is believed that combining CIMT and shaping increases neural activity, leading to better overall outcomes (14, 16).
A typical shaping exercise would be to pick up an object, such as a pencil, with the affected hand, and place the pencil in a container, attempting to move as many pencils as possible in 30 seconds: “Each functional activity is practiced for a set of 10 trials. Following completion of each task or trial, participants are given verbal feedback regarding their performance.”
A record of performance is kept and people are given activities to practice at home. The exercises and activities are individualized, depending upon the type of deficit that the person exhibits. Typically, feedback is provided by a therapist who works intensively with the patient, but a study is underway to determine if robot-assisted shaping therapy is an effective alternative. This method uses a computerized robot that is programmed to assist the patient to carry out motor tasks, such as “reaching to touch a visual target or guiding an object on screen.” The researchers believe that robot-assisted therapy can improve use of the upper extremities as well as therapist-guided therapy.

The robotic software can be programmed to provide specific levels of assistance for each task, depending upon the individual needs. One goal of this approach is to increase the capacity of therapists to manage larger numbers of patients (14).
Active-assist
Active-assist is an integral part of many of the current therapies, especially with task-specific types of repetitive exercises. With active-assist, the patent is asked to do a particular movement and attempts to do so with a therapist providing some assistance through support of the extremity or the use of an electronic or mechanical device.
Such assistive devices as “overhead slings and arm skateboards” are sometimes used as well as robotic devices. The theory behind active-assist is that completing a movement stretches muscles and tissue, relieving spasticity, and provides sensory input to promote neural reorganization (17). Interestingly, some studies have shown that assistance that enhances error rather than eliminating and guiding the limb close to the correct path is more effective, perhaps because it forces the person to adjust and compensate for weakness rather than just being passive (18).
Body-weight supported treadmill training
Training in locomotion is very important for patients with impairment of the lower extremities after a stroke. For those with severe impairment, standing can be impossible, but body-weight supported treadmill training allows people to ambulate while suspended in a special harness over a treadmill. Some people may be able to move their limbs independently, but others may need manual assistance with therapists moving the patients’ legs or robotic assistance (19).
A number of studies show that this type of gait training is effective in enhancing recovery after a stroke although the most effective training uses have not been determined. Improving the ability of patients to walk is very important because, in the initial period after a stroke, about 63% of people have impairment of ambulation, and after 3 months, 29% still need ambulatory assistance or cannot ambulate at all.
Because repetitive locomotor training is necessary to promote cortical reorganization, body weight supported gait training can be a valuable adjunct to therapy. To date, studies have been somewhat inconclusive with some studies showing that weight-supported gait has advantages but others showing that, compared to bracing-assisted gait, the difference was insignificant.
However, results did show that those with “major hemispheric stroke” showed significant improvements compared to the control group (20), perhaps because the degree of impairment made unsupported ambulation more difficult. Studies are on- going to determine the best use of weight-supported treadmill training.

Robot-assisted movement
The field of robotics has expanded considerably in the last few years, especially in relation to research regarding wearable robotic devices to augment human performance. Much of the impetus for this research has related to providing exoskeletons that can improve the speed, endurance, and carrying capacity of soldiers and secondarily civilian workers, such as firefighters. However, there is also much interest in robotic assist devices for people with neurological injuries or strokes’ (21).
Robot-assisted movement is now often used as part of shaping and other repetitive therapies. While traditional therapy is staff intensive, with sometimes 2 or 3 therapists needed to assist one patient, robot-assisted movement is less staff-intensive and can be calibrated for each individual patient. There are robotic devices for both upper extremities and lower. Since the field of robotics is fairly new, a number of studies are in progress to determine the best use.
One study involves robotic-assisted movement of the upper extremity, assisting the patients through exercises in which they use a joystick to move a cursor on a computer screen toward a target. The patient attempts the movement and is assisted toward completion by the robotic device (22).
An upper extremity robotic therapy device, Armeo™, has been marketed by Hocoma for use in rehabilitation of upper limb impairment after stroke. It has an adjustable arm support with “augmented feedback and a large 3-D workspace that allows functional therapy exercises in a virtual reality environment.” The device contains a grip sensor, and it can be used to input software and games. The computer provides visual movement feedback. (23).
Photo of Armeo™ used with permission of Hocoma (www.hocoma.com)
A number of studies have indicated that robot-assisted movement enhances recovery of arm movement after a stroke, but results have been inconclusive. One study divided patients in to 2 groups with one group performing active-assistive reaching exercises with the assistance of a robotic device. The second group attempted the same tasks but without any assistance. Both groups had 24 sessions, and there was little difference in outcome between those receiving assistance and those simply doing the repetitive exercises (17).
Another study compared the use of robotic-assisted movement with active assist, in which the therapist assisted the patient to complete movements, in patients with chronic arm impairment resulting from hemiparesis. Again, there was little difference in the outcome, suggesting that it was the repetitive movements that brought about the positive results rather than the robotic assistance (24).
Because most studies involve relatively small numbers of patients and sometimes use different methods, different robotic devices, and measure different outcomes, it can be difficult to really determine the value of robot-assisted devices for the upper extremities. A study at a university found that while there was no difference in hand/wrist improvement when comparing traditional neurodevelopmental therapy with robot-assisted therapy, the group receiving robot-assisted therapy showed significant improvement in shoulder and elbow function and greater gains in strength (25).
However, a number of studies have shown that traditional neurodevelopmental therapy is not a particularly successful therapy for stroke patients, so it’s unclear if the results would have been the same if a different form of therapy were used in the control group. Many studies have demonstrated that acute and chronic stroke patients who receive extensive upper extremity exercise recover more movement, and robot-assisted exercise can help to ensure that patients receive adequate exercise.
Additionally, the robot-assisted devices can be carefully calibrated for the individual needs and individual exercise regimens programmed into the devices. Some studies have indicated that robotic-devices that only assist when the patient uses the correct muscles show better results, making tasks difficult but not impossible (26).
More conclusive studies should be completed within the next year or two, providing better guidelines for the use of upper extremity robot-assisted movement. However, since robotic equipment is very costly, it appears that centers that can’t afford or don’t have robotic equipment can still achieve good results with the upper extremities if they have adequate numbers of well-trained staff to provide repetitive movement training.
Functional MRIs are helping to shed light on brain activity. Researchers used hand-operated robotic devices with chronic stroke patients to track rehabilitation therapy. They studied patients at least 6 months post-stroke with residual impaired use of the right hand. Functional
MRIs done before, during, and after therapy showed that there was increased cortical activation in the area of the brain that corresponds with hand use and that this increased cortical activation persisted for months after the one-month period of exercise stopped, suggesting that the brain is able to repair itself for longer periods than previously believed (51).
It is more difficult to assist a hemiparetic patient to ambulate without robotic-assist devices because, if a patient is unable to stand, the patient must be hoisted upright over a treadmill and then the legs manually moved by two therapists, one on each side. Attaining a normal gait in that manner is almost impossible (27).
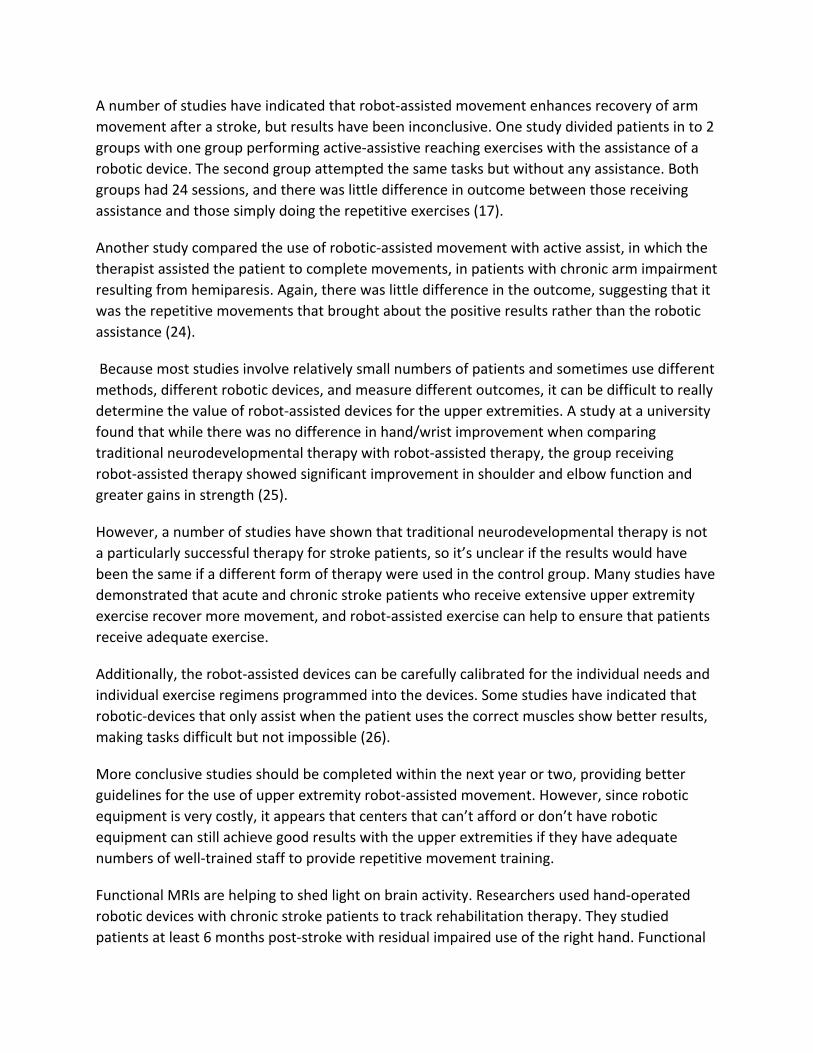
The robot-assisted treadmill is being utilized frequently in rehabilitation centers. One such robotic device is the Lokomat™, which is an exoskeleton device that uses a body weight suspension system.
Diagram used with permission of Saso Jezernik, Institut fur Automatik.
The Lokomat™ is attached to the lower extremities, providing support to the legs as they move through normal gait patterns. There are joints at the hip area and the knee of the exoskeleton that are electronically controlled individually. Sensors in the motors that control the joints also sense the amount of effort that the patient is expending (28).
Generally, people who participate in robot-assisted locomotion have some sensation or movement in at least one major muscle group in the leg. While treatment protocols may vary, that devised by the Rehabilitation Institute of Chicago is fairly typical: 60 minutes per day, 3 days per week, for 4-8 weeks (29).

There are a number of advantages to robotic-assisted gait training, including relief of physical strain on therapists, longer training periods, easy monitoring of progress, and adjustment of gait and level of assistance (28). The Lokomat™ is designed so that patients in wheelchairs can use a ramp to access the treadmill where they can be fit into the robotic-assist devices.
Additionally, the Lokomat™ can be moved out of the way so that the treadmill can be used as a weight-supported treadmill gait-training device without robotic assist. Passive guidance characteristics of the Lokomat™ can be adjusted so that patients have to work harder.
Photo used with permission of Hocoma (www.hocoma.com)
There are optical light sensors that focus on the patient’s feet so that the Lokomat™ and treadmill automatically shut down if a problem with gait occurs. The Lokomat includes a computer screen that provides instant feedback to the patient about his/her progress during the treatment (30).
The National Capital Area Rehabilitation Research Project (NACRRN) is currently conducting a number of studies with Lokomat™ focusing on activity-dependent neural plasticity, including one study to determine if intensive step training in sub-acute stroke patients results in improvement in gait in over-ground walking. Researchers believe that use of locomotor training with Lokomat® will reduce spasticity, bone loss and other complications resulting from loss of motor functions (31).
Bilateral movement training
It appears that this type of robot-assisted movement strengthens muscles and improves circulation, and the weight bearing facilitated by the device may decrease the risk of osteoporosis (29). Another positive aspect of robot-assisted locomotion is that it allows for

consistency because the program is automated and can be standardized for each individual, according to height and weight (32).
Another system is called AutoAmbulator™ by HealthSouth. While developed by a different company, AutoAmbulator™ is a similar device to the Lokomat™ in that it is a weight-supported treadmill device that offers advanced robotics to simulate normal gait. The device holds the patient’s body upright while mechanized braces bend the knees and guide legs across the treadmill (33).
HealthSouth owns and operates numerous rehabilitation centers throughout the United States and is installing AutoAmbulator™ equipment in these centers for use in rehabilitation of motor impairment (33). Ongoing studies of AutoAmbulator™ are determining to what degree the device can improve circulation, decrease spasms, improve respirations, and facilitate neurological recovery (34).
Despite some clear advantages to robotic-assisted gait training, a recent study published by the American Heart Association showed that patients assisted to walk by therapists showed significantly more improvement than those with robotic assistance. Both groups showed improvement, but researchers theorize that those in harnesses with physical therapists helping to move their limbs were allowed more mistakes in movement and that the brain uses these mistakes to learn, in the same way children learning to walk at first stagger and fall but then learn to compensate (53).
Another interesting approach to rehabilitation incorporates the forced use of CIMT with bilateral movement on the theory that the good side can strengthen the response of the weak side. Rather than using constraint on the unaffected extremity, the unaffected side is used to “increase the functional recovery of the impaired limb by the facilitative coupling effects

between the two limbs.” That is, both upper extremities practice the same motor actions, with shaping or assistance of the impaired limb as needed.
Research has shown that there is much synchronicity bilaterally when both hands or arms are used, suggesting that mirrored-symmetrical movement is part of coordination and that both upper arms are linked within the central nervous system. If one hand, for example, is used, then the hemisphere on the same side (which controls the opposite hand) is inhibited, as are the links between the hemispheres (intracortical) to prevent mirror motions. It is hypothesized that an intracortical link is at the corpus callosum.
When both hands are used, there is activation of both hemispheres as well as the intracortical links, coordinating the two hands so that they function together as a unit. This “locked” effect is referred to as entrainment. This entrainment can make it difficult to do such things as drawing a line with one hand while drawing a circle with the other. Both hands tend to draw the same form. Bilateral movement training attempts to use this natural coupling of like muscles to promote recovery.
A number of studies have been conducted, but the conclusions have been mixed; however, most studies have been small and used different approaches. One study that showed positive results involved 6 hours of training over 4 days in 2 weeks. In this study of wrist extension movements, the unimpaired hand was moved simultaneously with the impaired hand, which received “electromyography-triggered neuromuscular stimulation” with a specially designed arm-training machine. When compared with the control group that exercised just the impaired hand, those doing bilateral movement showed more improvement (3, 4, 35).
A modification of this approach is called Bilateral Arm Training with Rhythmic Auditory Cueing (BATRAC), in which both arms do exercises that involve pushing and pulling in coordination with auditory cueing of a rhythmic beat from a metronome. A robot assist device is usually used to “deliver controlled, bilateral, rhythmic movements to the upper limbs” (15).
One study of participants who had suffered strokes 4 years earlier required them to exercise for 1 hour, 3 times weekly for 6 weeks. Functional MRIs were done to determine if there was increased brain activation during and after treatment. Those that showed this activation also showed improvement of motor function. An interesting finding was increased activation of the side of the brain controlling the unaffected side, suggesting that it had assumed some control from the damaged side of the brain. Bilateral movement therapy has been used primarily with those with moderate to severely impaired movement (15, 35).
Many studies point to the positive results of augmented feedback as part of bilateral movement training, such as through electrical stimulation or visual input. One study involved chronic stroke patients doing bilateral movement exercises while looking at a mirrored reflection of the moving unimpaired limb. These participants showed improved motor

functions, suggesting that they were able to use visual cues to substitute for the lack of normal sensory feedback.
Ongoing studies will attempt to determine the optimum use of bilateral movement training, but some researchers believe that the large differences shown by participants and the inconsistent results may relate to damage done to the area of the corpus callosum as it may be necessary to retain a sufficient number of intracortical links in order for the therapy to be effective (35).
Of note is the fact that bilateral movement training is an inherent part of therapy of the lower extremities as gait training automatically involves both limbs. Researchers believe this may be the reason that lower extremities tend to recover more quickly than upper extremities. In order to increase feedback, some rehabilitation centers place a mirror in front of the treadmill.
Not all rehabilitation centers have advanced robotic treadmills, but some centers have used the NuStep TRS4000™, the recumbent cross trainer, which allows for people to simulate a walking motion while in the sitting position. While this type of equipment is usually used for strength training for geriatric patients, it has been successfully adapted for bilateral movement training. A study assessing the use of NuStep for stroke rehabilitation showed that it improved balance and ambulation with marked increases in the velocity of gait and balance (15).
Photo of NuStep TRS4000™ used with permission of NuStep, Inc.
Overall, it appears that bilateral movement training is effective as a means of improving motor functions for many who are in the sub-acute or chronic phases of recovery after a stroke (3, 15).

Electromyographically-triggered Neuromuscular electrical stimulation (EMG-NMES)
There is good evidence that electromyographically-triggered neuromuscular electrical stimulation (EMG-NMES), one form of functional electrical stimulation, can help people to regain function of an impaired limb.
The NeuroMove™ is such a device and can be used by people in a rehabilitation center or at home. The device has been approved by the FDA for stroke rehabilitation and has been the subject of a number of studies with positive results. It is a small, computerized device with a screen that shows muscle activity. Three self-adhesive electrodes are attached to the muscle (the forearm for hand and wrist work) and they are able to detect electrical signals sent from the brain to a muscle (37).
Photo used with permission of James Cauraugh, University of Florida.
It is important that the patient concentrate very hard on moving a particular part of the body or muscle. Even though obvious movement may not be noticeable, the electrodes can sense even slight electrical activity: “The computer inside the NM900 evaluates the amount of activity present in the muscle, then sets a higher standard than the patient should try to reach by concentration” (38).
When the NeuroMove™ detects an attempt at movement, it responds (rewards) with electrical stimulation for 5 seconds that causes muscle contraction that results in both visual and sensory feedback, helping the brain to reorganize to compensate for damaged areas. Stimulation is followed by a 12 second period of relaxation. NeuroMove™ can also be used to prompt relaxation of muscles. Treatments are usually done 1-3 times daily for periods lasting about 20-30 minutes, with therapy continuing for at least 4 weeks.

NeuroMove™ is specifically marketed for both upper extremities and feet to reduce muscle spasms and increase the following:
Finger movement Hand and wrist movement Dorsiflexion (to reduce foot drop) Elbow movement Shoulder movement
The NeuroMove™ is easy to use at home because it adjusts automatically to the individual and does not require programming. This device is different from those that deliver just electrical stimulation. The NeuroMove™ stimulates the muscle only in response to effort on the part of the patient, so the stimulation serves as positive reinforcement. Some patients have found that the treatments reduce muscle tone and spasticity. Because this therapy requires active participation on the part of the patient, it is not useful for those who are confused and not able to do simple tasks or for those who lack motivation (37, 38).
Studies have shown that the length of time since a stroke does not appear to affect outcomes, so this suggests a possibility of improvement for those with long-term paralysis or paresis. About 90% of those using this therapy achieve and maintain functional improvements. Patients with spinal cord injuries have similar results as patients with impairments caused by strokes (37, 38).
One study that compared those receiving EMG-NMES applied to the forearm to stimulate hand opening to a control group receiving sham treatments found those receiving the EMG-NMES showed improvement of functional use of the hand, and a functional MRI showed stimulation of the cortical areas, facilitating improvement in motor functions (39).
Functional electrical stimulation
While some studies have shown that passive electrical stimulation has little effect on impairment, a new approach, functional electrical stimulation, appears to be a positive tool for stroke rehabilitation. Functional electrical stimulation uses electrodes placed on the skin to stimulate nerves, resulting in contraction of muscles.
A recent double-blind study evaluated progress in sub-acute stroke patients who received 1 hour of functional electrical stimulation daily for 3-4 weeks as part of an exercise regimen that included reaching, grasping, manipulating, and releasing objects. A control group did the same exercises but received sham electrical stimulation below motor threshold. Results showed significant improvement in most measures for those receiving functional electrical stimulation, suggesting that traditional therapy should be supplemented, even for short periods, with functional electrical stimulation (40).

A number of different functional electrical stimulation devices have been marketed, but they have been primarily confined to rehabilitation centers and were often difficult to apply, position, and remove, broke easily, and required much energy to use. The Freehand system requires surgical implantation. Some devices have been used primarily for people with spinal cord injuries but are now expanding uses to include those with stroke impairments (41).
Bioness®, Inc. produces functional electrical stimulation equipment that is user-friendly enough that it can be easily used in the home environment, the Ness H200™ for the arm and hand and the Ness L300™ for the leg and foot. Because the Bioness® devices are wireless or easily portable, patients are able to use them as part of an active repetitive movement-oriented exercise program without being tethered by wires. The devices are powered by rechargeable batteries, which last for about 15 hours of continuous use.
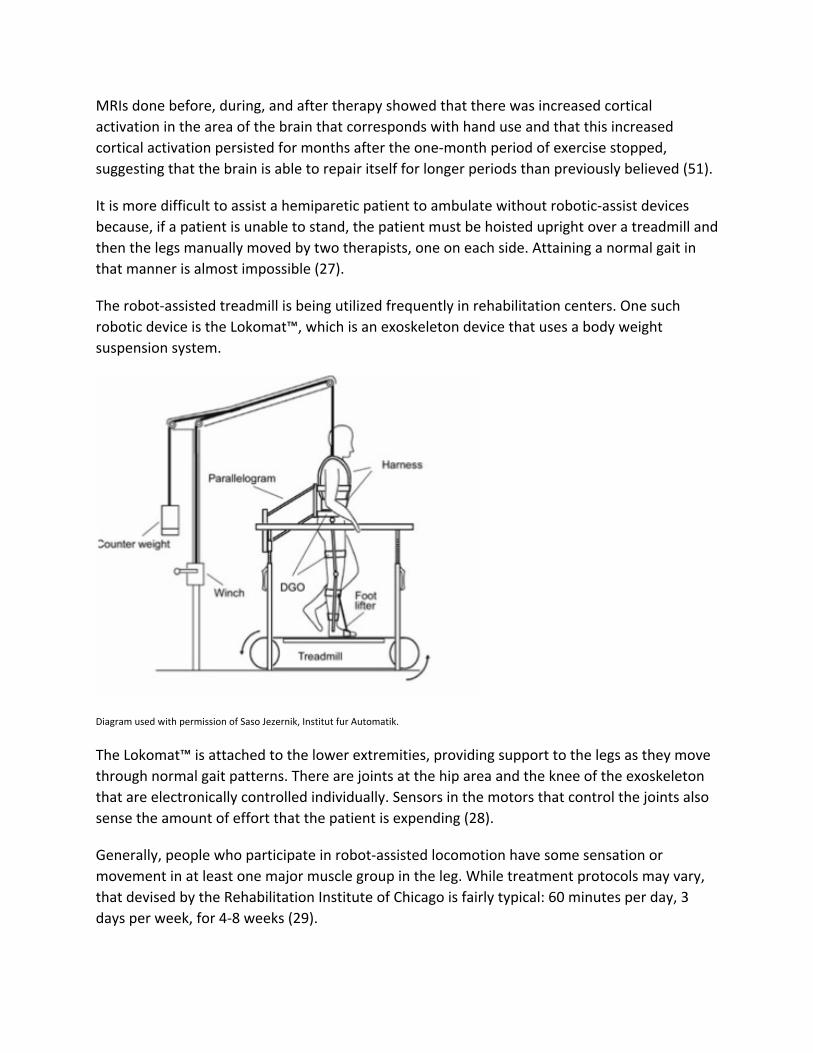
The Ness H200™ is designed for rehabilitation of the arm and hand. The control unit can be placed on a work surface or strapped onto the body. The device is portable and has a stimulator (with electrodes that deliver mild electrical stimulation) that fits around the forearm, extending to a spiral hand-wrist orthosis that wraps around the wrist into the palm. The hand-wrist orthosis holds the hand and wrist in a functional position. Its modular design in different sizes allows it to be fit precisely for each individual patient so that electrodes in the forearm piece are placed correctly on the muscles.
Photo used with permission of Bioness®, Inc. (www.bioness.com).
The Ness H200™ has 7 operating modes: personal (preset for personalized use for the individual), exercise, open-exercise, grasp exercise, open, grasp, and key. Thus, the device can be used for a series of therapeutic repetitive movement exercises to lesson impairments, strengthen muscles, and lesson spasticity and muscle atrophy. It can also be set for functional use, such as for grasping and releasing an item (42, 44).
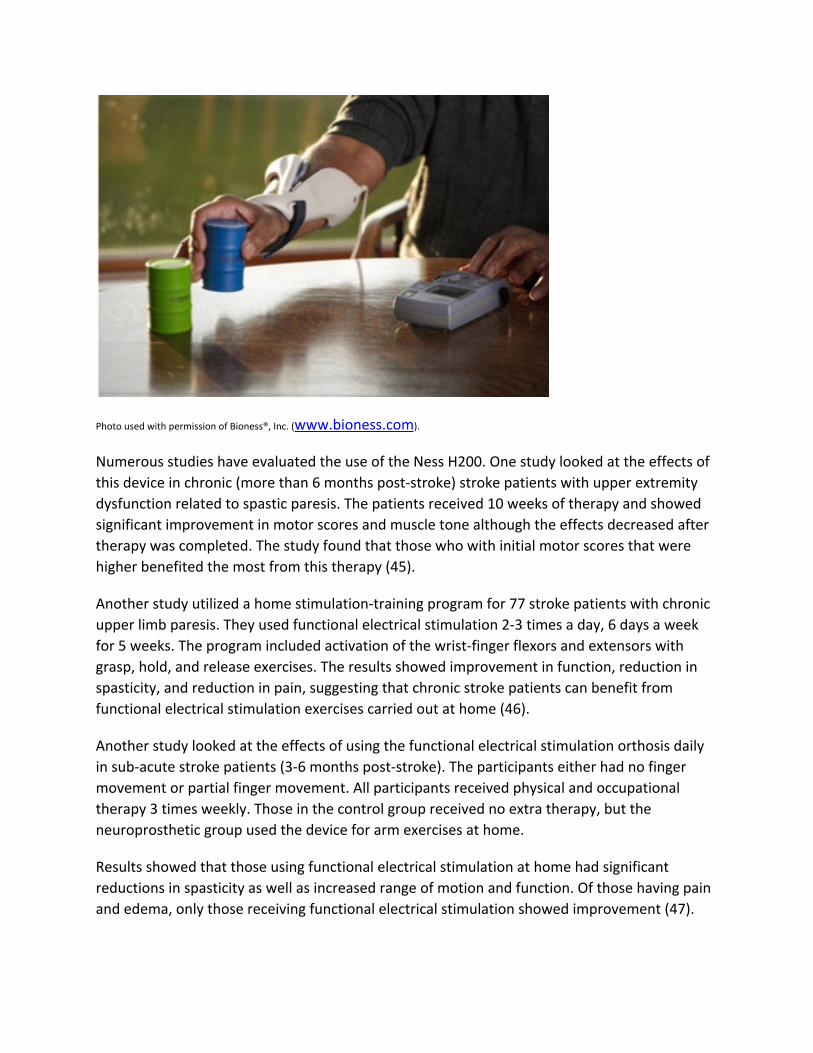
Photo used with permission of Bioness®, Inc. (www.bioness.com).
Numerous studies have evaluated the use of the Ness H200. One study looked at the effects of this device in chronic (more than 6 months post-stroke) stroke patients with upper extremity dysfunction related to spastic paresis. The patients received 10 weeks of therapy and showed significant improvement in motor scores and muscle tone although the effects decreased after therapy was completed. The study found that those who with initial motor scores that were higher benefited the most from this therapy (45).
Another study utilized a home stimulation-training program for 77 stroke patients with chronic upper limb paresis. They used functional electrical stimulation 2-3 times a day, 6 days a week for 5 weeks. The program included activation of the wrist-finger flexors and extensors with grasp, hold, and release exercises. The results showed improvement in function, reduction in spasticity, and reduction in pain, suggesting that chronic stroke patients can benefit from functional electrical stimulation exercises carried out at home (46).
Another study looked at the effects of using the functional electrical stimulation orthosis daily in sub-acute stroke patients (3-6 months post-stroke). The participants either had no finger movement or partial finger movement. All participants received physical and occupational therapy 3 times weekly. Those in the control group received no extra therapy, but the neuroprosthetic group used the device for arm exercises at home.
Results showed that those using functional electrical stimulation at home had significant reductions in spasticity as well as increased range of motion and function. Of those having pain and edema, only those receiving functional electrical stimulation showed improvement (47).

The Ness L300™, first marketed by Bioness®, Inc., in 2006, is a device for the leg and foot that is used to facilitate ambulation by electrical stimulation and to retrain muscles as well as increase range of motion and improve circulation. The Ness L300™ is used to compensate for the foot drop that so often occurs with hemiparesis. Physical therapy for foot drop has been time-intensive, often without good results. Because the foot literally “drops” when lifted, people must lift the foot high or lift the hip and swing the foot to compensate and prevent tripping (48).
Many people have been prescribed braces to stabilize the foot, but braces maintain the foot at a fixed 90-degree angle to the leg, making for an unstable and awkward gait. Unfortunately, applying a brace only mechanically corrects the problem; it doesn’t treat the underlying weakness or impairment (49, 50). The wireless Ness L300™ allows the ankle to move in a more normal gait pattern without the use of braces, making ambulation more stable.
The Ness L300™ consists of three parts:
Electronic orthosis in the form of a flexible cuff fits below the knee and contains electrodes and houses a stimulation unit to stimulate the nerves.
Control unit is wireless and small enough to fit into a pocket and allows simple on/off operation and displays real-time system status information.
Gait sensor fits under the heel with a transmitter that clips to the edge of a shoe.
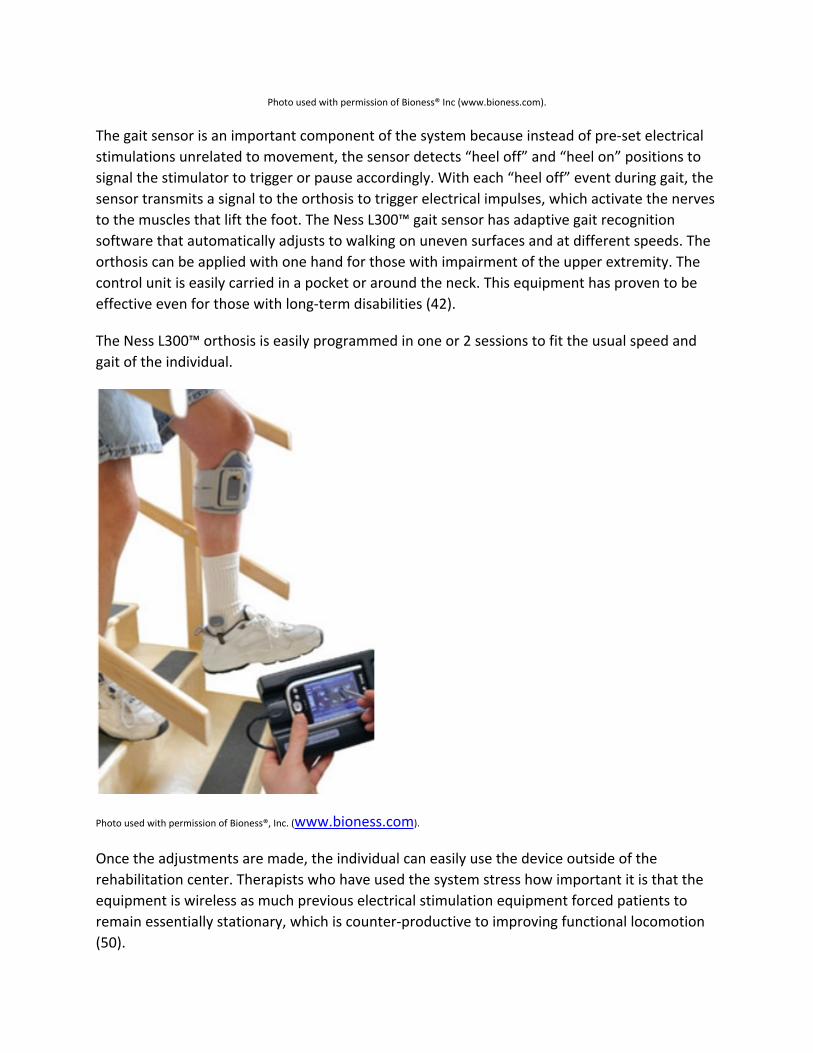
Photo used with permission of Bioness® Inc (www.bioness.com).
The gait sensor is an important component of the system because instead of pre-set electrical stimulations unrelated to movement, the sensor detects “heel off” and “heel on” positions to signal the stimulator to trigger or pause accordingly. With each “heel off” event during gait, the sensor transmits a signal to the orthosis to trigger electrical impulses, which activate the nerves to the muscles that lift the foot. The Ness L300™ gait sensor has adaptive gait recognition software that automatically adjusts to walking on uneven surfaces and at different speeds. The orthosis can be applied with one hand for those with impairment of the upper extremity. The control unit is easily carried in a pocket or around the neck. This equipment has proven to be effective even for those with long-term disabilities (42).
The Ness L300™ orthosis is easily programmed in one or 2 sessions to fit the usual speed and gait of the individual.
Photo used with permission of Bioness®, Inc. (www.bioness.com).
Once the adjustments are made, the individual can easily use the device outside of the rehabilitation center. Therapists who have used the system stress how important it is that the equipment is wireless as much previous electrical stimulation equipment forced patients to remain essentially stationary, which is counter-productive to improving functional locomotion (50).
The Ness L300™ has been used on both legs for a boy with cerebral palsy, helping him to walk better and trip less. He is able to easily turn the device on and off with the remote control unit. One aspect of the device that is especially helpful for those with neurological diseases, such as multiple sclerosis, is that it helps to conserve energy, thus allowing more activity and increased stamina.
In a National Public Radio interview, Dr. David Lowell, Medical Director of the Rehabilitation Hospital of the Cape and Islands (the first center in New England to receive the device) spoke at some length about how this technology was transforming rehabilitation, with patients using the device for gait training within one week of a stroke. The Ness L300™ not only frees therapists from many manual tasks but also engages the patient in the rehabilitation process because the facilitated ambulation is a functional activity, not just an “exercise” (49).
While the Ness L300 device has been used successfully for those with neurological impairments caused by stroke, cerebral palsy, and multiple sclerosis, it is not recommended for those with foot drop related to diabetic neuropathy or compression of the nerves in the lumbar region (49).
The focus of both the Ness H200™ and L300™ is on recovery of function rather than adaptation, reversing learned non-use and promoting cortical reorganization. Because this equipment is easy for patients to apply and use, therapists are finding that patient compliance with exercise increases and that, after patients leave the hospital, they are often willing to use the devices at home for multiple hours daily, improving their chances of recovery. Additionally, Bioness has developed a collection of 241 exercises and activities for the H200™, providing pre-designed activities that can be modified as needed, such as range of motion, weight bearing, assisted, functional mobility, and balance (57).
Electrical stimulation devices are contraindicated for those with a cardiac pacemaker and should not be used with high-frequency surgical equipment or near short wave or microwave therapy equipment. Stimulation should not be applied over malignant tumors, fractures, or dislocations.
Rhythmic and music therapy
Repetitive rhythmic cueing in gait training and other motor activities is often used because evidence shows that it improves performance. One study compared two groups receiving conventional gait training with one of the groups receiving rhythmic auditory stimulations (RAS). Treatment was 30 minutes 2 times daily 5 days a week. A metronome was used to pace one group with the metronome cadence matched to the subject’s gait initially and then the speed slowly increased 5-10%, depending upon the individual’s ability, and then decreased back to the original cadence during the last few minutes. Results showed that rhythmic cueing had a

significant impact on both the speed of gait and the length of the average stride (54). Similar results have been found when rhythmic auditory cueing is combined with constraint-induced movement and bilateral arm training (4).
Music therapy’s role in pain control is recognized and increasingly utilized, as is the role of music in reducing anxiety and promoting a sense of well-being, but its role in stroke rehabilitation is also noteworthy. Beth Abraham Institute for Music and Neurological Function is at the forefront in research applying music therapy to rehabilitate those with impairments caused by strokes.
Music therapy is used to promote movement and muscle control, to facilitate speech, and improve cognition. Research has shown that rhythmic patterns, such as playing a drum or exercising to up-beat music as well as timing music to the natural walking rhythm can increase movement and improve control of muscles. It is theorized that strokes damage executive function so that people may not be able to voluntarily use muscles and that musical cueing may bypass this executive function, allowing people to move muscles (55, 56, 57).
Music therapy has added an interesting dimension to speech therapy. Researchers have found that people who suffer from aphasia may be able to sing because the part of the brain that controls speech is different from that which controls singing. It appears that healthy areas of the brain may compensate for injured parts. The speech center is located on the left, but the area of the brain that controls singing is on the right, but once this part of the brain is engaged (by singing), it activates other areas of the brain.
Tapping into the music center to compensate for damage to the speech center is called melodic intonation therapy and incorporates singing and rhythmic tapping. Patients begin by singing phrases and gradually transitioning to speech. Singing also exercises and strengthens the muscles of the mouth. Therapy includes rhyming, chanting, and rapping (55, 56, 57).
A recent ABC News program about Congressman Gabby Giffords, recovering from a brain injury, showed that therapists used music to help her learn to talk. Because of damage to the speech centers on the left side of the brain, she suffered aphasia, but because music activates areas on both sides of the brain, having her sing (which she was able to do) trained her brain to create new pathways for language (57).
Additionally, writing songs and music is used to improve cognition, including the ability to focus attention, to remember, to organize, and to solve problems. Patients are helped to create songs that contain important information, for example (56).
An interesting approach to music therapy includes the use of a “camera-based human computer interface called ‘Music Maker,’” which allows people who have had strokes and lack the dexterity to play a musical instrument to make music. Active music therapy is based on the
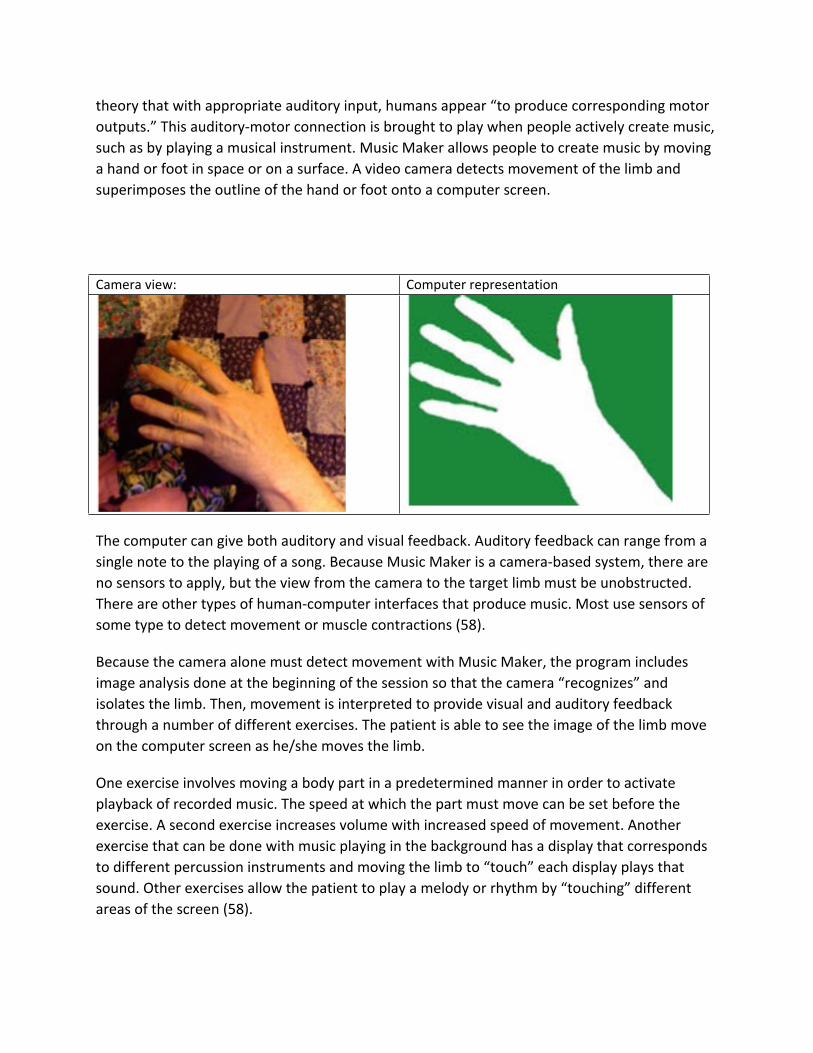
theory that with appropriate auditory input, humans appear “to produce corresponding motor outputs.” This auditory-motor connection is brought to play when people actively create music, such as by playing a musical instrument. Music Maker allows people to create music by moving a hand or foot in space or on a surface. A video camera detects movement of the limb and superimposes the outline of the hand or foot onto a computer screen.
Camera view: Computer representation
The computer can give both auditory and visual feedback. Auditory feedback can range from a single note to the playing of a song. Because Music Maker is a camera-based system, there are no sensors to apply, but the view from the camera to the target limb must be unobstructed. There are other types of human-computer interfaces that produce music. Most use sensors of some type to detect movement or muscle contractions (58).
Because the camera alone must detect movement with Music Maker, the program includes image analysis done at the beginning of the session so that the camera “recognizes” and isolates the limb. Then, movement is interpreted to provide visual and auditory feedback through a number of different exercises. The patient is able to see the image of the limb move on the computer screen as he/she moves the limb.
One exercise involves moving a body part in a predetermined manner in order to activate playback of recorded music. The speed at which the part must move can be set before the exercise. A second exercise increases volume with increased speed of movement. Another exercise that can be done with music playing in the background has a display that corresponds to different percussion instruments and moving the limb to “touch” each display plays that sound. Other exercises allow the patient to play a melody or rhythm by “touching” different areas of the screen (58).

Virtual Reality/ Video games
Much of therapy today aims at repetitive activities that can be boring for patients. Virtual reality adds another dimension to this type of therapy by making the practice more interesting and motivating. Virtual reality uses a computer interface to create a simulation of an environment, allowing the patient to interact in real time in that environment. Virtual reality has been used in the entertainment field, but much current research looks for applications of virtual reality in medicine, science and education.
Virtual reality tries to create an environment that is similar to what the person knows so that the person can become both mentally and physically involved in the environment. The person in true virtual reality therapy wears a head-mounted display unit that allows the person to look around a three-dimensional space, giving the illusion that the person is inside that space. Essentially, the person is able to view “three walls” at one time. Sensors are attached to the person to track movement and infrared cameras capture movements and an avatar inside the “environment” provides visual feedback, mimicking the movements, and thus providing positive enforcement.
For example, if a person raises an arm, the person will see the avatar’s arm rise inside the virtual environment. A typical virtual reality environment may be, for example, a kitchen, where people will practice opening drawers or making coffee, functional tasks that the person must master in real life.
One study focused on improving both hand and arm function at the same time through games such as Plasma Pong and Hammer Task. Games used to improve grip and finger motion include Virtual Piano and Hummingbird Hunt. Patients showed increased control of hand and arm with better efficiency and smoother motions after training 2 to 3 hours a day for 8 days, with an average improvement of 20% to 22% (59).
One virtual reality system has been used for hand rehabilitation after a stroke. Two input devices, “a CyberGLove and Rutgers Master force feedback glove” allow the patient to interact within the virtual environment. Using performance-based targets individualized for the patient helps to increase patient motivation, resulting in improvement of hand function. Chronic stroke patients who used this system daily for 2 weeks showed improvement in hand movement, including range, speed of movement, and strength (60).
While virtual reality systems can be very expensive, engineers at Rutgers University have created a virtual reality hand rehabilitation system by using “an Xbox and its Essential Reality P5 glove controller,” which is a gaming glove able to detect movement of the fingers and wrists to manipulate images on the screen. While this system doesn’t use the 3-D helmet, the patient is able to interact with the computer screen. The patient’s hand movements are mirrored by “virtual” hands” on the computer screen For example, one exercise promotes finger flexing

speed, by having the patient try to make a fist quickly enough to “scare away” a butterfly that is flying about the screen.
This system is less sophisticated than those especially designed for medical use, but it’s a cost-effective way to achieve some of the same results. While initial studies were small, the results have been impressive: “After three weeks of the new therapy, the researchers found up to a 140 percent improvement in range of motion for the thumb and up to a 118 percent improvement in the ability to move one finger at a time. There were also significant improvements in such areas as finger speed and finger strength.” Significantly, there was improvement by just the use of virtual reality without more traditional rehabilitation exercises (61).
One interesting research project involved the development of a virtual reality-based locomotor training system with a self-paced treadmill and a virtual reality projected onto a screen in front of the patient. The virtual reality is synchronized with the speed of walking. Exercises included such things as walking in a corridor, up slopes, and avoiding collisions. Tasks were made increasingly more difficult. Patients were able to increase gait speed and adapt to changes in the “environment” (62).
A study reported by the American Heart Association stated that playing interactive virtual reality games could significantly improve motor function and help to reorganize brain functions. In the study, 5 patients received more traditional stroke therapy, but 5 patients with hemiparesis received virtual reality therapy using 3 games: Stepping Up/Down (simulating climbing and descending stairs), Sharkbait (simulating deep sea diving), and Snowboarding (simulating snowboarding down narrow slopes as well as avoiding obstacles. Patients received therapy for 1 hour daily, 5 times a week, for a month.
At the end of the study time, those who had received the computer-assisted virtual reality training showed a 23% improvement in functional ambulation compared to 5% in the control group. Additionally, on a motor scale used to evaluate the ability to stand and walk up and down four steps, those receiving virtual reality therapy showed a 17.4% improvement compared to no improvement for the control group (63).
The potential for gaming and virtual reality for rehabilitation is just beginning to be realized. The Interdisciplinary Study of Neuroplasticity and Stroke Rehabilitation, based at the University of Southern California (USC), is exploring the use of these technologies with such things as Vivid’s Irex™ system, which allows patients to be engaged in activities that may range from being a “soccer goalies to skydiving.” Irex™ provides directed feedback to patients about the time an activity took and the success rate.
A much less expensive system, PlayStation 2’s EyeToy™, also shows potential for modification for rehabilitation use. Additionally, Nintendo’s Wii is an affordable system that encourages

patients to exercise and is being used more and more frequently with stroke patients. The team at USC has created exercises for shoulders, arms, hands, and feet. According to a recent study, patients who played video games on Wii and Playstation were 5 times more likely to show improvement in arm function than those with standard therapy (75).
Patient compliance with “boring” repetitive exercises is often a problem with therapies, but the team found that patients wanted to continue playing the games even when the goals of the session had been met, “and in cases where patients had considerable difficulties, instead of quitting in frustration, they seemed to be motivated to succeed despite the challenges they faced” (64).
It seems clear that therapists who are innovative can develop virtual reality or gaming therapies for people after strokes, and can do so without exorbitant expense if they make creative use of systems that are marketed for gaming enthusiasts.
Vision Rehabilitation Therapy (NovaVision™)
The normal visual field is about 180 horizontally and 120 vertically with overlap of both eyes in the nasal fields. A visual field deficit is a loss of part of the field of vision. In stroke patients, visual field deficits may involve loss of half of the field of vision on the same side in both eyes. That is, damage to the right side of the posterior part of the brain can result in loss of the left visual field in both eyes, resulting in a blind spot, requiring the person to scan with the eyes or move the head to see the entire field.
This can make reading, walking, or shopping difficult and even dangerous. Sometimes, there is spontaneous improvement within the first few months after a stroke, but after 6 months, spontaneous recovery does not usually occur (65).

Additionally, the condition may be complete or partial. If complete, the person may only be able to see one side of vision by looking straight ahead; if partial, vision may seem distorted with some parts of the field brighter than others. Depending upon the area of the stroke, people may also have quadrantanopia (loss of one-quarter of the visual field), scotoma (island-like blind spot), or diffuse field defects (scattered areas of vision distortion or blindness) (66).
A typical computerized visual field test involves looking straight ahead at the midpoint of a screen onto which pinpoints of light flicker on and off, with the person being tested clicking a button each time he/she sees a light. The lights flicker at random across the entire visual field, so computer analysis can determine if there are areas of lights that weren’t observed, thus a visual field deficit.
This is the basic technology behind NovaVision™ (the only FDA-approved device to restore vision loss) except that the flickering lights are programmed to light up around the existing visual field deficit using the theory of neuroplasticity to retrain the brain to “see” and then moving the lights as the vision field improves.
Because of the nature of treatments, NovaVision VRT therapy should not be used with those with a history of seizure disorders as it may trigger seizures or with those with severe cognitive defects because of the need to concentrate for prolonged periods. Those at risk for DVT should discuss the prolonged sitting with a physician before beginning treatment. Patients with acute inflammatory diseases of the eyes or CNS should wait until the acute phase has passed before beginning treatments.
Treatment is usually performed for 15 to 25 minutes two times daily, six days a week for 6-7 months or more with patients doing all or part of the treatments at home. Patients wear a chin support to keep the head stable as they look at a monitor that is about 1 foot in front of their eyes. They stare at a center point while stimuli are provided by white lights against a dark background (67).
Some patients report mild headaches or fatigue associated with treatment; and if this occurs, the patients may need to take breaks or have treatments for shorter periods of time.
Prior to the advent of NovaVision™, treatment involved primarily teaching patients strategies to compensate or fitting them with optical devices that helped to shift the visual field. Whether or not there is actual improvement in vision with NovaVision™ or if people just believe subjectively that there is remains an area of controversy. The claim for NovaVision™ is that over 70% of those who completed visual restoration therapy with NovaVision™ have improvement of vision (citing a study involving 302 patients) (66).
There are many anecdotal reports of patients who report improvement. Additionally, a number of studies prior to 2005 indicated that patients had improvement of vision and that this

improvement persisted after therapy was discontinued. In 2005, at the American Stroke Association’s International Stroke Conference, Sabel et al. reported that those receiving Vision Restoration Therapy were able to regain some vision after 6-12 months of therapy. They also asserted that patients with vision loss attributed to a stroke benefited from the treatment regardless of the severity of the stroke or the degree of vision deficit (68).
Subsequent to that conference presentation, other researchers reported that one problem with the data was “that the same software program used for visual restoration therapy was also used to show improvement in the visual fields.” Further, when some of these patients were administered independent visual field testing, no benefit was detected (67).
Some researchers postulated that the early positive results related to that fact that people with visual field deficits scan with their eyes to fill in the blind spots, and preventing people from doing this by having them stare at a center point is almost impossible. The center point does change color, and patients have to signal this change to show their eyes remain fixated, but researchers argued that the center point was large enough that even with a slight degree of scanning, patients could detect the change. Despite these findings, patients continue to report subjectively that their vision has improved (67, 70).
Moreover, a study using functional MRIs to examine for brain activity of stroke survivors done before and after vision restoration therapy found that brain activity increased for those using vision restoration therapy although how this correlates with improved vision is not yet clear (69).
A study of 7 patients at the Rochester Eye Institute showed that patients who had become partially blind as the result of strokes damaging the primary visual cortex were able to regain some vision after several months of daily computerized therapy (71). In 2008, a retrospective study involving 161 patients with stroke or traumatic brain injury with stable visual field defects showed that the average stimulus detection improvement was 12.8% or a 4.9-degree border shift between the seeing and blind field (76).
As with many current therapies, studies are ongoing, and the true benefits of NovaVision™, and the extent of possible vision recovery, may be demonstrated when these studies are completed.
Summary
Strokes, also referred to as strokes or cerebrovascular accidents, are the leading cause of adult disability. Strokes can be caused by ischemia from blockage of arteries by thrombi or emboli or by hemorrhage as the result of an aneurysm, intracerebral or subarachnoid bleeding, or arteriovenous malformations. The American Stroke Association has developed a classification

system for strokes that classifies according to the number of impaired domains, the degree of impairment, and the assessment of function.
Most strokes occur in the right or left hemispheres although they can occur in the cerebellum or brain stem as well. The type of disability relates to the area of the brain that is damaged. Hemiparesis and hemiplegia are common results of a stroke. The concept of neuroplasticity, the ability of the central nervous system to modify connections by strengthening or weakening them or forming new connections is central to new concepts in rehabilitation.
Since there is clear evidence that the brain retains the ability to respond to changes and heal itself through cortical reorganization and that stimulating the neurons through activity promotes neurogenesis, much new therapy attempts to encourage this process. There are ongoing studies for all of the new therapies to determine the best way to apply the treatments. Often, two or more therapies may be combined in a rehabilitation program for an individual.
Constraint-induced movement therapy involves constraining the uninvolved extremity, forced use of the weakened limb for 90% of waking hours, and massed practice to encourage cortical reorganization.
Shaping (adaptive task practice) does not involve constraints and approaches objectives in small steps, completing part of a task and them moving to a more difficult task.
Active assist involves asking the patient to attempt to do a particular while a therapist or robot provides some assistance to complete the motion.
Body-weight supported treadmill training allows people to ambulate while suspended in a special harness over a treadmill.
Robot-assisted movement includes robot-assist devices for both upper and lower extremities to facilitate movement, such as the Lokomat™ or AutoAmbulator™.
Bilateral movement training incorporates the forced us of CI with bilateral movement on the theory that the good side can strengthen the response of the weak side.
Electromyographically-triggered neuromuscular electrical stimulation, such as provided by NeuroMove™, uses sensors to detect attempts at movement, which is then rewarded with electrical stimulation to assist muscle contraction.
Functional electrical stimulation uses electrical stimulation to assist people to do functional exercises. The Ness H200™ is used for the upper extremities. The Ness L300™ facilitates ambulation by compensating for foot drop.
Rhythmic and music therapy uses repetitive rhythmic cueing for gait training and other motor activities as well as computer programs, such as Music Maker, to assist people to create or manipulate music. Singing is also used for people with aphasia.
Virtual Reality and video games takes advantage of computer programs to create virtual realities in which patients can function, making practice more interesting and motivating.

Vision Restoration Therapy with NovaVision™ attempts to reduce visual field deficits and improve vision.
References1. Types of Strokes. (2020). American Stroke Association. Retrieved from
http://www.strokeassociation.org/STROKEORG/AboutStroke/TypesofStroke/Types-of-Stroke_UCM_308531_SubHomePage.jsp
2. Kollen, B.; Kwakkel, G.; and Lindeman, E. (2006). Functional recovery after stroke: A review of current developments in stroke rehabilitation research. Reviews on Recent Clinical Trials 1: 75-80.
3. Stewart, K.C.; Cauraugh, J.H.; & Summers, J.J. (2006). Bilateral movement training and stroke rehabilitation: a systematic review and meta-analysis. Journal of the Neurological Sciences 244: 89-95.
4. Whitall, J.; McCombe Waller, S.; Silver, K.H.C.; & Macko, R.F. (2000). Repetitive bilateral arm training with rhythmic auditory cueing improves motor function in chronic hemiparetic stroke. Stroke 31:2390.
5. Smeltzer, S.C., Bare, B., Hinkle, J.L, & Cheever, K.H. (2010). Brunner & Suddarth’s Textbook of Medical-Surgical Nursing, 12th edition. Philadelphia: Lippincott, Williams, & Wilkins.
6. Stroke treatment and rehabilitation. (n.d.). Ohio State Medical Center, Wexner Medical Center. Retrieved https://wexnermedical.osu.edu/brain-spine-neuro/stroke
7. Kelly-Hayes, M.; Robertson, J.T.; Broderick, J.P., Duncan, P.W.; et al. (1998). AHA scientific statement: The American Heart Association stroke outcome classification. Stroke 29: 1274-1280.
8. Causes of paralysis. (2020). Christopher & DanaReeve Foundation. Retrieved from https://www.christopherreeve.org/living-with-paralysis/health/causes-of-paralysis
9. Ackerman, C. E. (2020, April 28). What is neuroplasticity? A psychologist https://positivepsychology.com/neuroplasticity/
10. Mang, CS, Campbell, KL, Ross, CDF, & Boyd, LA. (2013, December). Promoting Neuroplasticity for Motor Rehabilitation After Stroke: Considering the Effects of Aerobic Exercise and Genetic Variation on Brain-Derived Neurotrophic Factor. Physical Therapy, 93 (12): 17017-1716.
11. Cavuoto, J. [n.d.]. Business report: Neurotech vendors seek to exploit cortical plasticity. Neurotech Reports. Retrieved from http://www.neurotechreports.com/pages/corticalplasticity.html
12. Constraint-induced movement therapy. (2020). Physiopedia. Retrieved from https://www.physio-pedia.com/Constraint_Induced_Movement_Therapy
13. Taub, E.; Uswatte, M.A.; & Pidikiti, R. (1999, July) Constraint-induced movement therapy: A new family of techniques with broad application to physical rehabilitation—A clinical review. Journal of Rehabilitation, Research, & Development 36 (3).

14. Kwakkel,G, et al.(2015, February 14). Constraint-induced movement therapy after stroke. Lancet Neurology, 14(2):224-234. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4361809/
15. Biomechanics of upper-limb stroke rehabilitation therapy. (2015, June 15). IATSL. Retrieved from http://www.iatsl.org/projects/biomechanics.html
16. “Shaping” technique found effective and efficient in stroke rehab. (2003, September). American Academy of Neurology at Science Blog. Retrieved from http://www.scienceblog.com/community/older/2003/C/2003176.html
17. Kahn, L.E.; Zygman, M.L.; Rymer, W.Z.; & Reinkensmeyer, D.J. (2006, June 21). Robot-assisted reaching exercise promotes arm movement recovery in chronic hemiparetic stroke: a randomized controlled pilot study. Journal of NeuroEngineering and Rehabilitiation 3:12
18. Patton, J.L.; Stoykov, M.E.; Kovic, M., and Mussa-Ivaldi, F.A. (2006, January). Evaluation of robotic training forces that either enhance or reduce error in chronic hemiparetic stroke survivors. Experimental Brain Research. 168(3): 368-383.
19. Nustgep cross trainers: Designed with inclusivity in mind. (2018). NuStep, Inc. Retrieved from http://www.nustep.com/our-products
20. Fulk, G. (2004, March). Locomotor training with body weight support after stroke: The effect of different training parameters. Journal of Neurologic Physical Therapy.
21. Ferris, D.P.; Czerniecki, J.M.; & Hannaford, B. (2004, June 25) An ankle-foot orthosis powered by artificial pneumatic muscles. Robotics Laboratory, University of Washington.
22. Rehabilitation therapy after a stroke. (2019, May 14.) Stroke.org. Retrieved from https://www.stroke.org/en/life-after-stroke/stroke-rehab/rehab-therapy-after-a-stroke
23. Armeo™ therapy concept. (2020). Hocoma. Retrieved from https://www.hocoma.com/solutions/arm-hand/
24. Kahn, L.E.; Averbuch, M.; Rymer, W.Z., & Reinhensmeyer, D.J. [n.d.]. Comparison of robot-assisted reaching to free reaching in promoting recovery from chronic stroke. University of California, Irvine. Retrieved from http://gram.eng.uci.edu/~dreinken/publications/us03.pdf
25. Kahn, L.E., Zygman, M.L. Rymer, W.Z., & Reinkensmeyer, D.J. (2006, June 21). Robot-assisted reaching exercise promotes arm movement recovery in chronic hemiparetic stroke: a randomized controlled pilot study. Journal of Neuroengineering Rehabilitation 3: 12. Retrieved from http://www.ncbi.nlm.nih.gov:80/pmc/articles/PMC1550245/
26. Kahn, L.E.; Lum, P.S.; Rymer, W.Z.; & Reinkensmeyer, D.J. (2006, August/September). Robot-assisted movement training for the stroke-impaired arm: Does it matter what the robot does? Journal of Rehabilitation Research & Development 43 (5): 610-630.
27. Gomes, MA, Silveira, GLM, & Siqueira, AAG. (2009, November). On-line Trajectory Adaptation for Active Lower Limbs Orthoses based on Neural Networks. COBEM. Retrieved from http://www.mecatronica.eesc.usp.br/wiki/upload/c/c0/Cobem09.pdf

28. Lokomat®--Relearning to walk from the beginning. (2018). Hocoma. Retrieved from https://www.hocoma.com/us/solutions/lokomat/
29. Lokomat® gait training. (2018). Shirley Ryan Ability Lab. Retrieved from https://www.sralab.org/services/lokomat
30. Erigo®. (2018). Hocoma. Retrieved from https://www.hocoma.com/services/product-training/erigo/
31. Qian, Z. & Bi, Z. (2014, October 20). Recent development of rehabilitation robots. Sage Journals. Retrieved from http://journals.sagepub.com/doi/full/10.1155/2014/563062
32. Versweyveld, L. (2001, November 13). Lokomat has paralysed patients use their legs again in robot-steered treadmill. Virtual Medical Worlds. Retrieved from http://www.hoise.com/vmw/01/articles/vmw/LV-VM-12-01-12.html
33. HealthSouth’s AutoAmbulator. (n.d). HealthSouth. Retrieved from http://daytonrehab.com/es-ES/experience-healthsouth/the-healthsouth-difference/leading-technology/autoambulator?sc_lang=en
34. AutoAmbulator®. (2020). Encompass Health. Retrieved, from https://www.encompasshealth.com/what-we-do/inpatient-rehabilitation/irf-our-technology/autoambulator
35. Cauraugh, J.H., & Summers, J.J. (2005). Neural plasticity and bilateral movements: A rehabilitation approach for chronic stroke. Progress in Neurobiology 75: 309-320.
36. American Physical Therapy Association (2009, August 3). Use Of A Restraining Device In The Subacute Phase After A Stroke No Better Than Rehabilitation Alone. ScienceDaily. Retrieved from http://www.sciencedaily.com/releases/2009/08/090803185834.htm
37. Stroke rehabilitation with NeuroMove™. (2018). Zynex Medical. Retrieved from http://www.zynexneuro.com/neuromove/
38. NeuroMov NM900™ (n.d.). Biomation. Retrieved from http://www.biomation.com/physiotherapy/neuromove.html
39. Kimberley, T.J.; Lewis, S.M.; Auerbach, E.J., et al. (2004). Electrical stimulation driving functional improvements and cortical changes in subjects with stroke. Experimental Brain Research 154(4): 450-460.
40. Kowalczewski, J.; Gritsenko, V.; Ashworth, N. et al. (2007, July). Upper-Extremity Functional Electric Stimulation–Assisted Exercises on a Workstation in the Subacute Phase of Stroke Recovery. Archives of Physical Medicine and Rehabilitation 88: 833-839.
41. Tan, Z et al. (2014, July 10). The effectiveness of functional electrical stimulation based on a normal gait pattern on subjects with early stroke: A randomized controlled trial. BioMed Research International. Retrieved from hhttps://www.ncbi.nlm.nih.gov/pmc/articles/PMC4119719/
42. Home. (2020). Bioness® Inc. Retrieved from http://www.bionessmobility.com/dtcinquiries?utm_source=PPC&utm_medium=Ads&utm_campaign=WP_Brand&gclid=EAIaIQobChMI0JOjvdT 82wIVhTFpCh3sZAiqEAAYASAAEgIjp_D_BwE

43. Woerner, A. (2013, May 20.). Young stroke victim recovered with help from new electrical stimulation technology. Fox News. Retrieved from http://www.foxnews.com/health/2013/05/20/electric-stimulation-treatments-help-young-stroke-victim/
44. Regain more natural hand function—with wireless freedom. (2020). Bioness. Retrieved from https://www.bioness.com/Products/H200_for_Hand_Paralysis.php
45. Hendricks H.T.; Ijzerman, M.J.;de Kroon J.R.; Groen F.A.; & Zilvold G. (2001). Functional electrical stimulation by means of the “Ness Handmaster Orthosis” in chronic stroke patients: an exploratory study. Clinical Rehabilitation 15:217-220.
46. Alon, G.; Sunnerhage, K.S.; Geurts, A.C.H.; & Ohry, A. (2003). A home-based self-administered stimulation program to improve selected hand functions of chronic stroke. Neurorehabilitation 18 (3): 215-225.
47. Ring, H, & Rosenthal, N. (2005). Controlled study of neuroprosthetic functional electrical stimulation in sub-acute post-stroke rehabilitation. Journal of Rehabilitation Medicine 37: 32-36.
48. Golden, S. [n.d.]. New technology heralds new hope for those with foot drop. Good Shepherd Rehabilitiation Center. Provided by Bioness®, Inc.
49. Lowell, D. & Juhanson, D. Interviewed by M. Todd. (2007, February 21). The point: Strokes and treatment options. NPR: WGBH.
50. Long. F. (2007). Wireless device hailed as new modality for foot drop, but can patients afford it. Rehab management. Retrieved from http://www.rehabpub.com/2007/02/wireless-device-hailed-as-new-modality-for-foot-drop-but-can-patients-afford-it/
51. Radiological Society of North America (2008, December 23). Robotic Technology Improves Stroke Rehabilitation. ScienceDaily. Retrieved from http://www.sciencedaily.com/releases/2008/12/081203084306.htm
52. Ness® H200™ Exercise and activity collection. [Undated]. PowerPoint Presentation. Bioness®, Inc.
53. American Heart Association (2008, May 11). Stroke Survivors Walk Better After Human-assisted Rehabilitation. ScienceDaily. Retrieved from http://www.sciencedaily.com/releases/2008/05/080508164414.htm
54. Thaut, M.H., McIntosh, G.C.; & Rice, R.R. (1997). Rhythmic facilitation of gait training in hemiparetic stroke. Journal of Neurological Science. 1997;151: 07-212.
55. Glausiusz, (2001, August). The genetic mystery of music. Discover Magazine 22 (8).56. Draper, K. (2016) Music and stroke rehabilitation: A narrative synthesis of music-based
treatmnts used to rehabilitate disorders of speech and language following left-hemispheric stroke. (2015). Voices. Retrieved from htthttps://voices.no/index.php/voices/article/view/789/708
57. Moisse, K. (2011, November 14). Gabby Giffords: Finding words through song. ABC News. Retrieved from http://abcnews.go.com/Health/w_MindBodyNews/gabby-giffords-finding-voice-music-therapy/story?id=14903987#.TyGn5pjDnoc

58. Gorman, M., Betke, M.; Saltzman, E.; Lahav, A. (2005). Music Maker - a camera-based music making tool for physical rehabilitation. BU Computer Science Technical Report, No. 2005-032. Retrieved from http://www.cs.bu.edu/techreports/pdf/2005-032-music-maker.pdf
59. BioMed Central (2011, May 15). Next generation gamers: Computer games aid recovery from stroke. ScienceDaily. Retrieved from http://www.sciencedaily.com- /releases/2011/05/110515201320.htm
60. Jack, D. ; Boian, R. ; Merians, A.S.; Tremaine, M. ; Burdea, G.C. ; Adamovich, S.V.; Recce, M.; Poizner, H. (2001, September). Virtual reality-augmented rehailitation for patients following stroke. Neural Systems and Rehabilitation Engineering 9 (3): 308-318.
61. Rutgers develops virtual reality treatment for hand impairment in chronic stroke patients. (2002, January 28). ScienceDaily. Retrieved from http://www.sciencedaily.com/releases/2002/01/020128080804.htm
62. Fung, J.; Richards, C.L.; Malouin, F.; McFadyen, B.J.; & Lamontagne, A. (2006, April). A treadmill and motion coupled virtual reality system for gait training post-stroke. CyberPsychology & Behavior 9(2): 157-162.
63. Virtual reality therapy wows stroke victims. (2018). Wall Street Daily. Retrieved from http://www.wallstreetdaily.com/2015/05/12/mindmaze-virtual-reality-therapy/
64. Moore, EA. (2011, April 7). Study: Video games aid post-stroke motor skills. CNET. Retrieved from http://news.cnet.com/8301-27083_3-20051881-247.html
65. Rummel, E. Loss of visual field due to brain injury hemianopsia and neglect. Optometrists network. Retrieved from http://www.braininjuries.org/hemianopsia_field_loss.html
66. Vision restoration therapy. (2018). NovaVision. Retrieved from http://www.novavision.com/vision-restoration-therapy-vrt/
67. Horton, J.C. (2005). Disappointing results from NovaVision’s visual restoration therapy. British Journal of Ophthalmology 89 1-2.
68. Sabel, B.A.; Kenkel, S.; Kasten, E.; & Mueller, I. (2004, November 24). Abstract: Vision Restoration Therapy (VRT) for the treatment of visual field deficits after brain damage: the role of eye movements and fixation behavior. Journal of Vision 4(11): 29. Retrieved, from http://www.journalofvision.org/4/11/29/
69. Columbia University Medical Center (2007, August 19). Vision Restoration Therapy Shown To Improve Brain Activity In Brain Injured Patients. ScienceDaily. Retrieved from http://www.sciencedaily.com/releases/2007/08/070814082950.htm
70. Reinhard, J.; Schreiber, A.; Schiefer, E.; Kasten, B.A.; Sabel,S.; et al. (2005). Abstract: Does visual restitution training change absolute homonymous visual field defects? A fundus controlled study. British Journal of Ophthalmology 89: 30-35.
71. University of Rochester Medical Center (2009, March 31). Rigorous Visual Training Teaches The Brain To See Again After Stroke. ScienceDaily. Retrieved from http://www.sciencedaily.com- /releases/2009/03/090331183508.htm

72. American Academy of Neurology (2009, June 3). Suffer Stroke Symptoms? Second Strokes Often Follow Within Hours. ScienceDaily. Retrieved from http://www.sciencedaily.com/releases/2009/06/090601182700.htm
73. American Academy of Neurology (2009, September 29). One In Eight Strokes Is Preceded By 'Warning Stroke'. ScienceDaily. Retrieved from http://www.sciencedaily.com/releases/2009/09/090928172342.htm
74. Campbell, G. (2009, February 13) Interview with M. Merzenich on Neuroplasticity (Podcast episode 54) [Transcript]. Brain Science Podcasts. Retrieved from http://docartemis.com/Transcripts/54-brainscience-Merzenich.pdf
75. St. Michael's Hospital (2011, April 7). Video games effective treatment for stroke patients. ScienceDaily. Retrieved from http://www.sciencedaily.com- /releases/2011/04/110407121441.htm
76. Romano, JG, et al. . Visual field changes after a rehabilitation intervention: Vision restoration therapy, J Neurol Sci (2008), doi:10.1016/j.jns.2008.06.026
77. NIH Stroke Scale (n.d.). NIH. Retrieved from https://www.ninds.nih.gov/sites/default/files/NIH_Stroke_Scale_Booklet.pdf

Course Exam
1. What percentage of those who survive a stroke have residual impairment after one year?
a. 30%.b. 50%.c. 70%.d. 85%.
2. Which types of ischemic stroke blockage occurs most often in patients with hypertension or diabetes?
a. Thrombosis of large artery resulting from atherosclerosis.b. Lacunar infarct.c. Cardiogenic emboli.d. Cryptogenic.
3. Intracranial aneurysms occurs most commonly at the:a. brain stem.b. ventricles.c. circle of Willis.d. cerebellum.
4. Illicit drugs, such as amphetamines, crack, and cocaine, may lead to which type of hemorrhagic stroke?
a. Intracranial aneurysm.b. Subarachnoid hemorrhage.c. Arteriovenous malformations.d. Intracerebral hemorrhage.
5. Which of the following is a common type of stroke associated with young people?a. Arteriovenous malformations.b. Cardiogenic emboli.c. Lacunar infarct.d. Subarachnoid hemorrhage.
6. What percentage of patients who experience a transient ischemic attack (TIA) will have a stroke within a year?
a. 20%.b. 33%.

c. 50%.d. 70%.
7. Which of the following are possible causes for a cryptogenic stroke?a. Atrial fibrillation.b. Patent foramen ovale.c. Thrombophilia.d. All of the above.
8. The three aspects assessed with the American Stroke Association classification tool include:
a. Number of domains, degree of impairment, and functional assessment.b. Level of consciousness, limb mobility. and language.c. Level of consciousness, degree of impairment, and language.d. Number of domains, language, and limb mobility.
9. with the NIH Stroke scale, if the patient has fusion of the right elbow, how would motor function be assessed?
a. 0.b. 2.c. 4.d. UN.
10. Which of the following characteristics indicate a stroke of the right hemisphere?a. Left visual field deficit.b. Short term memory loss.c. Left paralysis/paresis.d. All of the above.
11. Which of the following is characteristic of a stroke in the cerebellum?a. Cardiac and respiratory dysfunction.b. Ataxia, inability to walk.c. Dysphagia and dysarthria.d. All of the above.
12. Which type of paralysis affects the same body region bilaterally, such as both arms?a. Monoplegia.b. Hemiplegia.c. Diplegia.d. Paraplegia.

13. A stroke would be classified as sub-acute at what length of time since the event?a. 0 to 3 months.b. 3 to 6 months.c. >6 months.d. >12 months.
14. With neuroplasticity, if healthy cells about a damaged area take over the function of the missing cells, this is referred to as:
a. functional map extension.b. compensatory masquerade.c. homologous region adoption.d. cross-model reassignment.
15. Learned non-use refers to which of the following?a. Patients learn to compensate for deficits.b. Patients prefer to avoid exercises.c. The body learns that a part of the body can’t function.d. The inability to correct lack of mobility.
16. Keeping surviving neurons and making new connections in the brain require:a. medicationsb. rest.c. stimulation.d. motivation.
17. With a cochlear implant, how long does it generally take people with a cochlear implant to begin to process and understand sounds?
a. 3 to 5 hours.b. 3 to 5 days.c. 3 to 5 weeks.d. 3 to 5 months.
18. With constraint-induced movement therapy, what percentage of waking hours should the patient have forced use of the weakened arm?
a. 50%.b. 60%.c. 80%.d. 90%.
19. Which of the following therapies involves conditioning and positive reinforcement?a. Constraint-induced movement therapy.

b. Shaping.c. Active assist.d. Bilateral movement training.
20. Which of the following may be used with active assist?a. Positive reinforcement.b. Overhead slings and arm skateboards.c. Treadmill.d. All of the above.
21. Three months after a stroke, what percentage of patients still need ambulatory assistance or are non-ambulatory?
a. 72%.b. 68%.c. 29%.d. 20%.
22. What schedule of exercise is typical for robot-assisted gait training, such as with the Lokomat™?
a. 20 minutes daily x 5 days per week.b. 30 minutes daily X 3 days per week.c. 60 minutes daily X 3 days a week.d. 30 minutes daily X 5 days a week.
23. Robot-assisted gait training is appropriate for patients with:a. Some sensation or movement in one major muscle group of the leg.b. Sensation throughout all major muscle groups in the leg.c. Movement in all major muscle groups in the leg.d. No sensation in the muscle groups of the leg.
24. When both hands are used and the coordination links the hands so they function together as a unit, this “locked” effect is referred to as:
a. forced use.b. entrainment.c. learned non-use.d. estrangement.
25. An important component of electromyographically-triggered neuromuscular electrical stimulation (EMG-NMES) is:
a. the patient must concentrate very hard on moving a body part or muscle.b. the patient must remain passive and allow the device to stimulate movement.

c. the device stimulates muscle activity before the patient attempts to move.d. the patient must have good sensation and some movement in the target
muscles.
26. Functional electrical stimulation with the Bioness® arm device allows the device to be programed to:
a. strengthen muscles.b. lesson spasticity.c. grasp and release items.d. all of the above.
27. If using repetitive rhythmic cueing in gait training, how should the cadence be set?a. Matched to patient’s cadence initially, increased 5% to 10%, and then decreased
again.b. Increased over the patient’s cadence by 5% to 10% over the course of the
exercise.c. Matched to the patient’s cadence initially and then decrease 5% to 10% over the
course of the exercise.d. Decreased under the patient’s cadence by 5% to 10% over the course of the
exercise.
28. With virtual reality that involves use of a 3-D helmet:a. the patient’s movement controls the movement of an avatar.b. the patient generally shows little improvement.c. the patient tries to mimic the movement of an avatar.d. the patient’s role is essentially passive.
29. Because of the nature of treatment, NovaVision VRT therapy should not be used for:a. ischemic stroke patients.b. patients with a history of seizure disorders.c. patients with long-term deficits.d. all of the above.