stroke scales you can use - baylor irving ed journal club · and hess stroke scale in the emergency...
TRANSCRIPT

STROKE SCALES YOU CAN USE
Author: Andrew Harding, RN, MS, CEN, NEA-BC, FAHA, Bridgewater, MASection Editors: Reneé Semonin-Holleran, RN, PhD, CEN, CCRN, CFRN, CTRN, FAEN,
and Andrew Harding, RN, MS, CEN, NEA-BC, FAHA
Earn Up to 8 CE Hours. See page 89.
Stroke is the third leading killer in the United States.1
Stroke is an emergency and has recently been an ini-tiative for many quality teams, emergency depart-
ments, and public health education programs.2,3 Themantra “time is muscle” for myocardial infarctions hasbeen adapted to “time is brain” for stroke. The crux of bothof these ailments is tissue perfusion.
The supply of blood and plasma carrying oxygen,nutrients, glucose, and chemical elements is vital to thehomeostasis or survival of brain cells. When this blood sup-ply is interrupted, the cells that are no longer provided withthe contents of our blood and plasma are injured and canprogress to cellular death. Unfortunately, our brain cellstypically do not regenerate themselves. Therefore in theemergency department our best efforts must focus onregaining perfusion to the affected brain cells that areinjured and not “dead,” also known as the penumbra.
The 3 typical types of stroke are hemorrhagic, thrombo-tic, and embolic. Thrombotic and embolic strokes affect bloodflow from a mechanical standpoint, “mechanical” meaningthat an actual thrombus (blood clot) or emboli (fatty plaqueor blood clot) is blocking blood flow to a distal aspect of anartery in the brain. These 2 types of stroke have the potentialto use recombinant tissue-type plasminogen activator (rt-PA).However, a hemorrhagic stroke means that there is bleeding inthe brain, and treatment excludes the use of rt-PA.
Early recognition of the signs and symptoms of strokehelps to reduce the amount of time (“time is brain”) thatbrain cells are deprived of blood and plasma. In this articleand in keeping with the mission of the “Clinical Notebook”section of the Journal, I have gained permission to share a
few pertinent stroke scales used in practice. Each of thesescales is displayed in Figure 1. A brief description of eachscale is found below.
The Cincinnati Stroke Scale (Figure 1) has been deter-mined to have “good validity in identifying patients withstroke who are candidates for thrombolytic therapy [rt-PA],especially those with anterior circulation stroke.”4 This has apositive implication for triage nurses. A triage nurse can com-plete the 3 steps of the Cincinnati Stroke Scale quickly. Know-ing that the sensitivity and specificity of the tool are excellentfor identifying patients with stroke, the triage nurse can quicklyactivate the emergency department’s stroke protocols for care.
The Hunt and Hess Stroke Scale (Figure 2) is used toclassify the severity for nontraumatic subarachnoid hemor-rhage patients.5,6 This scale will typically be used by a con-sulting neuroscience physician. However, using the Huntand Hess Stroke Scale in the emergency department is a goodmeasure to quantify the effects of a subarachnoid stroke. Thiswill provide for a better handoff report between nurses orcommunication with the patient’s family. This tool can alsobe used by registered nurses to trend the severity of the stroke’smanifestation over time in the emergency department.
The National Institutes of Health Stroke Scale (NIHSS)(Figure 3) is the “gold standard” of stroke scales. It measureslevel of consciousness, visual function, motor function,sensation/neglect, and cerebellar function.7,8 Gait and cra-nial nerve deficits are not recorded in the NIHSS. However,these 2 examinations can be completed separately.
Initially, the NIHSS is challenging to master and cantake a novice up to 7 minutes to complete. However, withpractice, this tool can be completed in less than 2 minutes.Education and certification in the NIHSS can be com-pleted online at http://www.nihstrokescale.org/. This edu-cational program also provides free contact hours for nursesand other practitioners.
Transient ischemic attack (TIA) is another cardio-vascular disease that is sometimes referred to as a “mini-stroke.” A TIA is characterized by patients exhibiting a lossof neurologic function due to ischemia that persists for lessthan 24 hours. Reversible ischemic neurologic deficitsymptoms persist for longer than 24 hours but resolvewithout neurologic sequelae.9 Both of these cardiovascularevents are indicative predictors of an impending stroke.
Andrew Harding, Mayflower Chapter, is Director of Patient Care Services,Morton Hospital and Medical Center, 88 Washington St, Taunton, MA.
For correspondence, write: Andrew Harding, MS, RN, CEN, NEA-BC, FAHA, Patient Care Services, Morton Hospital and Medical Center,88 Washington St, Taunton, MA 02780.
J Emerg Nurs 2010;36:40-52.
Available online 8 October 2009.
0099-1767/$36.00Copyright © 2010 Emergency Nurses Association. Published by Elsevier Inc.All rights reserved.
doi: 10.1016/j.jen.2009.05.002
C L I N I C A L N O T E B O O K
40 JOURNAL OF EMERGENCY NURSING VOLUME 36 • ISSUE 1 January 2010

The ABCD2 score (Figure 4) is a tool that relates the riskof stroke within 2 days after a TIA occurs.10 This tool is alsoused to predict the likelihood of the patient having a strokewithin 90 days of a TIA.This can be a good tool for emergencydepartments to educate patients about their need for follow-upwith their primary care physician and explain the need to con-tact emergency medical services if they have any neurologicdeficits. There are also care recommendations provided bythe authors for emergency physicians.11
In conclusion, the need for emergency nurses to beproficient in rapidly identifying patients having a strokeis critical. Using the tools shared in this article can be usefulin quantifying a patient’s presentation or risks. More toolsand information can be found on the Internet StrokeCenter Web site.12 Time is brain, and the faster we can
intervene to provide appropriate care to patients in restor-ing blood flow to promote tissue perfusion, the more braincells we can hope to save. Preserving brain cells should alsoassist in preserving neurologic function for our patients tolead active, fulfilling lives.
REFERENCES1. What is stroke? American Stroke Association. http://www.strokeassociation.
org/presenter.jhtml?identifier=3030387. Accessed April 29, 2009.
2. LandroL.Guidelines for heart care showpromise.The InformedPatient column,Wall Street Journal. http://online.wsj.com/article/SB123976160649419643.html. Published April 15, 2009. Accessed May 1, 2009.
3. Paul Coverdell National Acute Stroke Register and the Stroke CollaborativeReaching for Excellence (SCORE). Massachusetts Health and HumanServces, Commonwealth of Massachusetts. http://www.mass.gov/?pageID=eohhs2terminal&L=6&L0=Home&L1=Provider&L2=Guidelines+and+
FIGURE 1
Cincinnati Stroke Scale. Reprinted from Annals of Emergency Medicine,Volume 33, Issue 4, Kothari RU, Pancioli A, Liu T, Brott T, BroderickJ, Cincinnati Prehospital Stroke Scale: Reproducibility and Validity, 373-8,Copyright 1999, with permission from Mosby, Inc.
FIGURE 2
Hunt and Hess Stroke Scale. Reprinted from Journal of Neurosurgery,Volume 28, Issue 1, Hunt WE, Hess RM, Surgical Risk as Related to Time ofIntervention in the Repair of Intracranial Aneurysms, 14-20, Copyright 1968,with permission from the American Association of Neurological Surgeons.
Harding/CLINICAL NOTEBOOK
January 2010 VOLUME 36 • ISSUE 1 WWW.JENONLINE.ORG 41

Resources&L3=Guidelines+for+Services+%26+Planning&L4=Diseases+and+Conditions&L5=Heart+Disease+and+Stroke+Prevention&sid=Eeohhs2&b=terminalcontent&f=dph_com_health_heart_stroke_p_score&csid=Eeohhs2. Accessed May 1, 2009.
4. Kothari RU, Pancioli A, Liu T, Brott T, Broderick J. Cincinnati PrehospitalStroke Scale: Reproducibility and validity.AnnEmergMed. 1999;33(4):373-8.
5. Hunt WE, Hess RM. Surgical risk as related to time of intervention inthe repair of intracranial aneurysms. J Neurosurg. 1968;28(1):14-20.
6. Hunt WE, Meagher JN, Hess RM. Intracranial aneurysm. A nine-yearstudy. Ohio State Med J. 1966;62(11):1168-71.
7. NIH stroke scale. National Institute of Neurological Disordersand Stroke, National Institutes of Health. http://www.ninds.nih.gov/doctors/NIH_Stroke_Scale_Booklet.pdf. Accessed April 29, 2009.
8. NIH stroke scale. National Institute of Neurological Disorders andStroke, National Institutes of Health. http://www.ninds.nih.gov/doctors/NIH_Stroke_Scale.pdf. Accessed April 29, 2009.
9. What are the types of stroke? American Stroke Association. http://www.strokeassociation.org/presenter.jhtml?identifier=1014. Accessed April 29,2009.
10. Johnston SC, Rothwell PM, Nguyen-Huynh MN, et al. Validationand refinement of scores to predict very early stroke risk after transientischemic attack. Lancet. 2007;369(9558):283-92.
11. ABCD2 tool. http://www.stroke.org/site/DocServer/NSA_ ABCD2_tool.pdf?docID=5981. Accessed April 29, 2009.
12. The Internet Stroke Center. http://www.strokecenter.org/. Accessed April29, 2009.
Submit descriptions of procedures in emergency care and/or quick-reference charts suitable for placing in a reference file or notebook toReneé Semonin-Holleran, RN, PhD, CEN, CCRN, CFRN,CTRN, FAENorAndrew Harding, RN, MS, CEN, NEA-BC, FAHAhttp://ees.elsevier.com/jen
CLINICAL NOTEBOOK/Harding
42 JOURNAL OF EMERGENCY NURSING VOLUME 36 • ISSUE 1 January 2010

FIGURE 3
National Institutes of Health Stroke Scale (NIHSS). Courtesy of the National Institute of Neurological Disorders and Stroke (NINDS).
Harding/CLINICAL NOTEBOOK
January 2010 VOLUME 36 • ISSUE 1 WWW.JENONLINE.ORG 43

FIGURE 3
Continued.
CLINICAL NOTEBOOK/Harding
44 JOURNAL OF EMERGENCY NURSING VOLUME 36 • ISSUE 1 January 2010

FIGURE 3
Continued.
Harding/CLINICAL NOTEBOOK
January 2010 VOLUME 36 • ISSUE 1 WWW.JENONLINE.ORG 45

FIGURE 3
Continued.
CLINICAL NOTEBOOK/Harding
46 JOURNAL OF EMERGENCY NURSING VOLUME 36 • ISSUE 1 January 2010
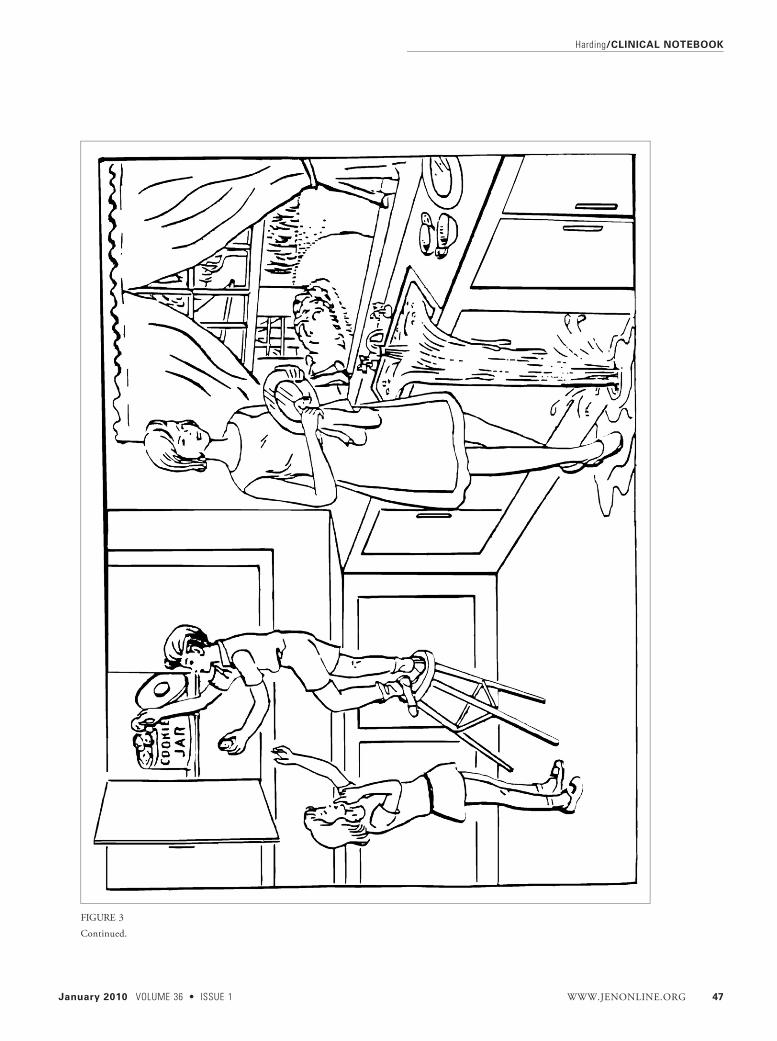
FIGURE 3
Continued.
Harding/CLINICAL NOTEBOOK
January 2010 VOLUME 36 • ISSUE 1 WWW.JENONLINE.ORG 47

FIGURE 3
Continued.
CLINICAL NOTEBOOK/Harding
48 JOURNAL OF EMERGENCY NURSING VOLUME 36 • ISSUE 1 January 2010
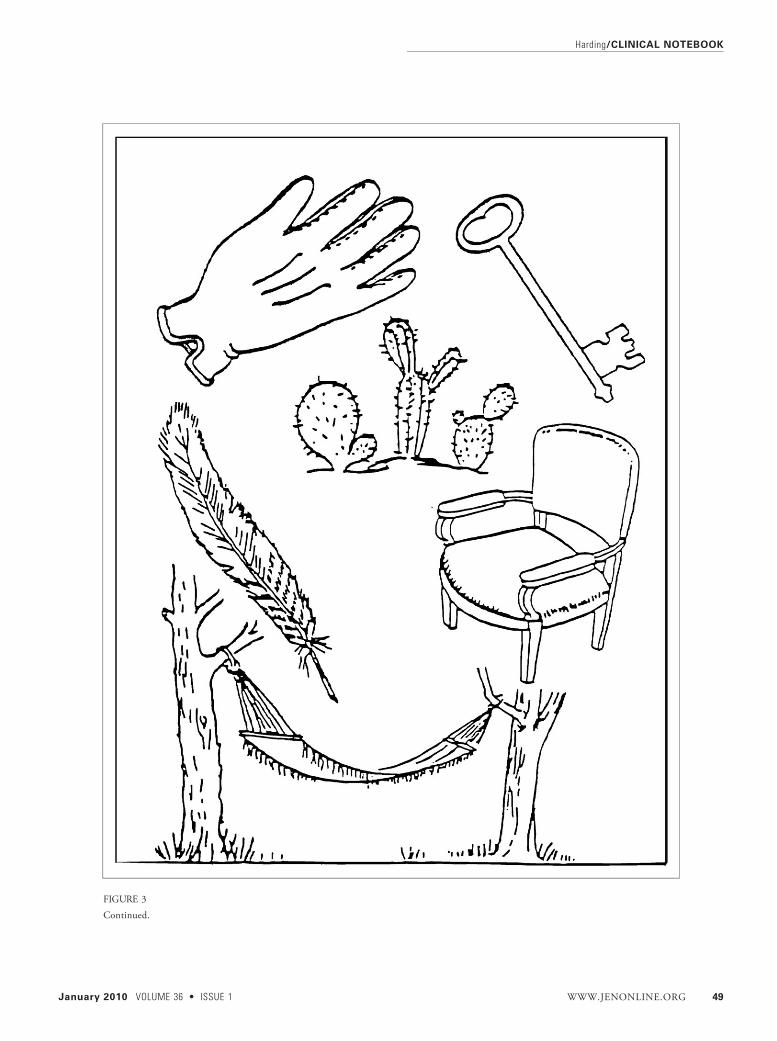
FIGURE 3
Continued.
Harding/CLINICAL NOTEBOOK
January 2010 VOLUME 36 • ISSUE 1 WWW.JENONLINE.ORG 49
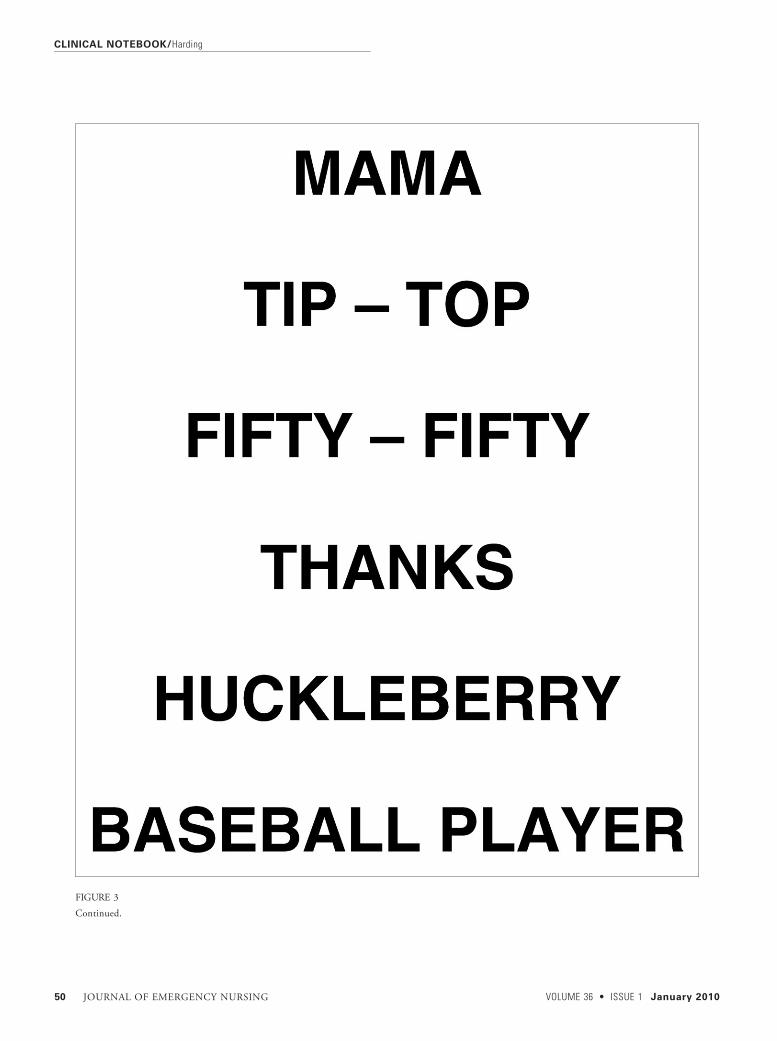
FIGURE 3
Continued.
CLINICAL NOTEBOOK/Harding
50 JOURNAL OF EMERGENCY NURSING VOLUME 36 • ISSUE 1 January 2010
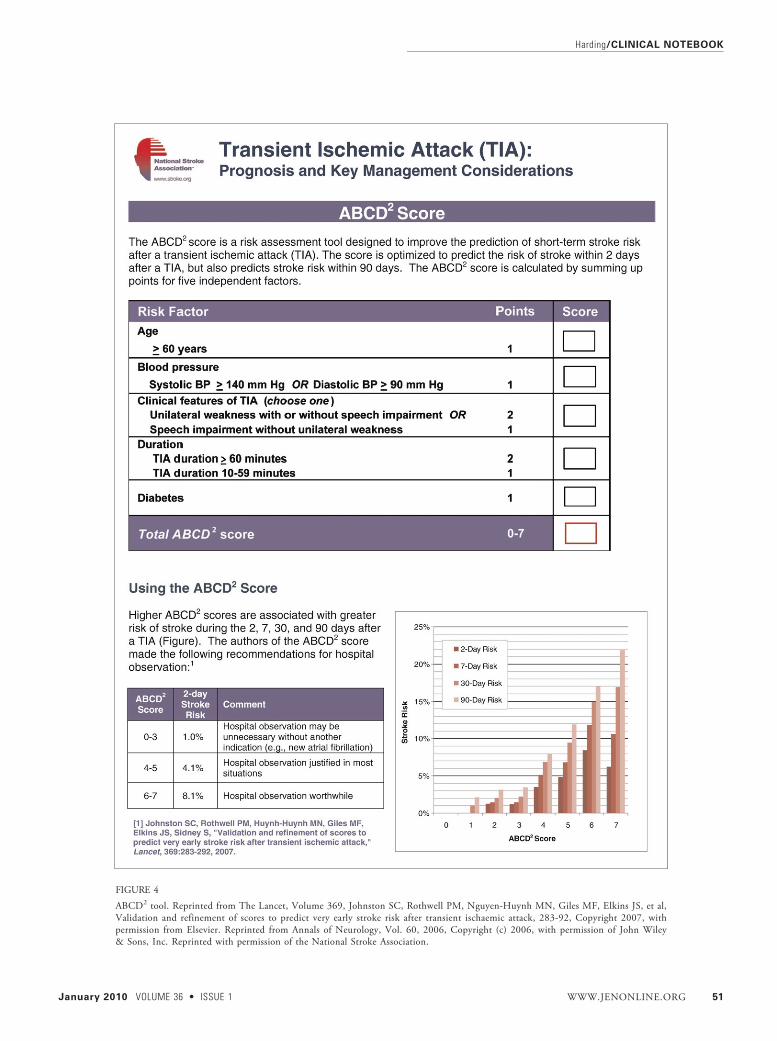
FIGURE 4
ABCD2 tool. Reprinted from The Lancet, Volume 369, Johnston SC, Rothwell PM, Nguyen-Huynh MN, Giles MF, Elkins JS, et al,Validation and refinement of scores to predict very early stroke risk after transient ischaemic attack, 283-92, Copyright 2007, withpermission from Elsevier. Reprinted from Annals of Neurology, Vol. 60, 2006, Copyright (c) 2006, with permission of John Wiley& Sons, Inc. Reprinted with permission of the National Stroke Association.
Harding/CLINICAL NOTEBOOK
January 2010 VOLUME 36 • ISSUE 1 WWW.JENONLINE.ORG 51
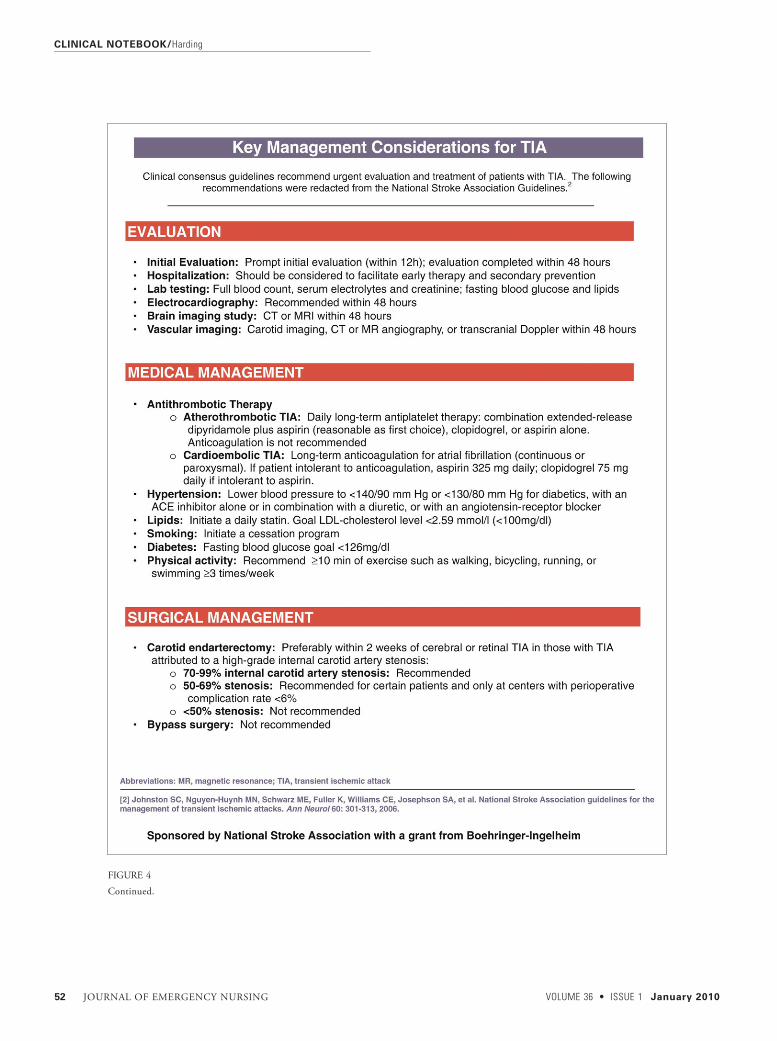
FIGURE 4
Continued.
CLINICAL NOTEBOOK/Harding
52 JOURNAL OF EMERGENCY NURSING VOLUME 36 • ISSUE 1 January 2010