stroke major classifications - @@ home - kku web hosting
TRANSCRIPT

10/14/2013
1
Jureerat Thammaroj , M.D. Radiology Department Khon Kaen University
Ischemic
Stroke
80-85%
Stroke major classifications
Hemorrhagic
Stroke 15-20%
The ” Early ischemic sign “
(Subtle hypodense changes ) ---Strictly within the first 6 Hrs. after symptom onset
Purpose in NCCT --- Hemorrhage ?
Vanishing lentiform nucleus maleus margins
due to isodensity (caused by edema) relative
to the surrounding inner and outer capsule [Radiology 1988:168:463-7, AJNR Am J Neuroradiol 1989:10:1215-22,
Stroke 1992:23:20-3]
“loss of insular ribbon” sign [Radiology 1990:176:801-6]
Early Ischemic Signs
Detection -prox. MCA occlusion effecting deep M1 perforators-

10/14/2013
2
Sensitivity 5-50% , depending on the
population under study [Neuroradiol 1996:17:1743-8 , Stroke 1992:23:317-24]
False – positive mimics caused by high
hematocrit or vessel wall calcifications [AJNR Am J Neuroradiol 1993:14:669-73]
Dense MCA sign
CBF of less than 10 ml/100g of tissue/min
- - - tissue cannot be tolerated beyond a
few minutes before infarction occurs,
CBF between 10 and 20 ml/100gm/min,
--- cell death in minutes to hours
CBF falls at approximately 18 to 20 ml/100g
of tissue/minute --- Neurological dysfunction occurs in a tissue
CBF and Duration Factors

10/14/2013
3
Subcortical LMCA ischemic Infarction Hemorrhagic infarction
DWI is far superior to NECT and other
routine MRI sequences in the detection of
acute ischemia, with very high sensitivity and specficity (LOE: A)
The gradient-echoMR sequence
can detect microhemorrhage,
both old and new, better than
CT, indicating the pressence of
amyloid angiopathy, hyper
tension , small vascular
malformations, and other
vascular diseases (LOE: strong B)
PENUMBRA PWI –DWI mismatch
Purpose ; to save the salvageable tissue
Stroke time resolution & imaging modalites

10/14/2013
4
Is it a true stroke?... Stroke mimics approx. 13%
If yes, is it ischemic VS hemorrhagic stroke?
If it is an ischemic stroke, is there any potential hemorrhagic transformation evidence?
Before start Rx
Parenchyma: CT/MRI
Pipe :angio. /US/CTA-V/MRA-V
Perfusion: CT/MRI/SPECT/PET
Penumbra: DWI/PWI mismatch
CBV/MTT mismatch
Stroke Imaging: The “ 4 P’S ”
1. Is there hemorrhage? Unenhanced CT , MRI
(gradient echo/SWI) (parenchyma) 1. Is there intravascular thrombus that can be targeted
for thrombolysis? CTA , MRA (Pipe)
2. Is there a core of critically ischemic irreversibly infarcted tissue (umbra)? DWI,CTP (abn CBV) (Perfusion)
3. Is there a penumbra of severely ischemic but
4. potentially salvageable tissue? , MR&CT perfusion
5. (PWI-DWI / MTT-CBV mismatch)
The “4 Keys and 4 Ps” Application in the imagine evaluation of acute stroke
Brain stem hemorrhage
History : A 33-years old male,
underlying HT in the young
and gout , presented with left
hemiparesis and aphasia
Brain stem
infaction
Parenchyma: CT/MRI
Pipe :angio. /US/CTA-V/MRA-V
Perfusion: CT/MRI/SPECT/PET
Penumbra: DWI/PWI mismatch
CBV/MTT mismatch
Stroke Imaging: The “ 4 P’S ”
10/14/2013
5
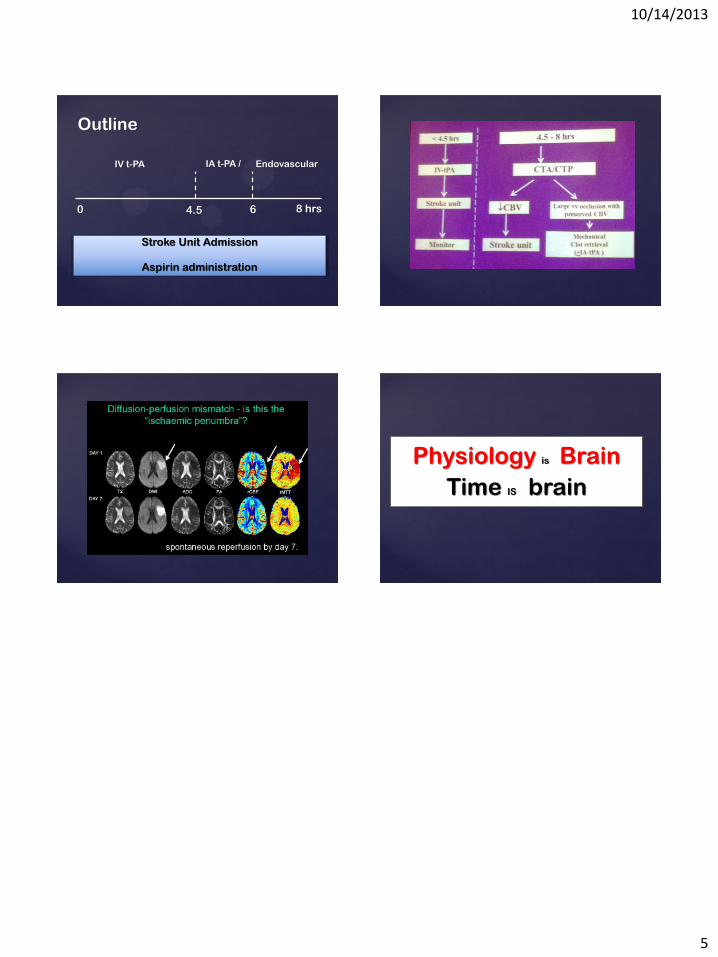
Outline
Stroke Unit Admission
Aspirin administration
4.5
Endovascular
6 0 8 hrs
IA t-PA / IV t-PA
Physiology is Brain
Time IS brain