strategic plan 2015 -2019 - malawi online...
TRANSCRIPT
1
STRATEGIC PLAN 2015 -2019 (A tool for Stability, Growth and Sustainability)

2
ACKNOWLEDGEMENT
This Strategic Plan is a product of committed Management and Staff of Likuni Mission Hospital
guided by the Proprietor, Board of Governors and several stakeholders of the Hospital. Their pieces of
advice especially those of the Board of Governors made this work to move smoothly and in the right
direction. The processes of consultation were far and wide through meetings, telephone calls, emails
and literature review of organizational and national documents. Consultations were inspired by King
Solomon’s wise words in Proverbs15:22 which say “Without counsel plans go but with many advisors
they succeed”. It is Management’s hope that this plan will successfully be implemented and that the
operations of Likuni Hospital will stabilize and grow sustainably. Development partners both local
and international are assured of Management and Staff commitment to the cause set in the Plan and
that through different feedback mechanisms they will be kept informed on progress that will be
achieved at regular interviews.
Management wishes to thank Mr. Austin Mazinga Mwale, a Technical Consultant, for guiding the
Strategic Planning Taskforce in every step through participatory approach. He worked at the pace of
Task team to ensure that every step reached was understood and linked to the next step. That approach
promoted ownership of the choices made. Importantly was the involvement of all staff of the Hospital
which promotes ownership of the Plan. Management assures its key stakeholders of regular and
timely updates on progress of the Plan and requests.
Management further wishes to thank Heads of Sections, Ward In-charges and other external partners
for their contributions towards the development of this Strategic Plan.

3
DECLARATION
The Strategic Plan Task Team was composed of the following:-
1. Sr. Agness Lungu Principal Hospital Administrator
2. Dr. James Kachingwe Medical Director
3. Mrs. Mary Chosamata Principal Nursing Officer
4. Mr. Louis Chamoto Senior Administrative Officer
5. Mr. Anthony Chiyabwa Hospital Accountant
6. Mrs. Tiyah Salimu Human Resource Management Officer
7. Mr. Austin Mazinga Mwale Consultant

4
FOREWORD
If you were a military general on the march, you would want your troops to have plenty of maps with
detailed information about the mission they are on, the roads they would travel, the campaigns they
would undertake, and the weapons at their disposal. The same holds true in management of hospitals:
A hospital needs clear and detailed information to execute its business successfully. Strategic Plan lets
an organization describe and illustrate in clear and general language its objectives, initiatives, targets,
performance measures and the links between all the pieces of its parts.
This Strategic Plan will guide the proprietor, board of governors, management, partners and staff of
Likuni Mission Hospital in walking through a strategy map of five strategic areas. These strategic
areas (goals) are; Service delivery with patients and clients centeredness, Sustainable Revenue
generation and accountability, Availability of adequate, competent and committed employees, Sound
infrastructure and appropriate technologies.
A semantic boundary would be loosened to translate the Plan among departments as they interpret
what they require in order to achieve the objectives set out in this Plan. Common interests need to be
developed to transform knowledge in each profession, as managers will be charged with creative or
innovative tasks to lead implementation and monitoring of the Plan. Success of the Plan depends on
their creativeness, innovativeness and knowledge.
Sister Agness Lungu
Principal Hospital Administrator

5
Table of Contents DECLARATION ...................................................................................................................................................... 3 FOREWORD ............................................................................................................................................................ 4 ABBREVIATIONS .................................................................................................................................................. 9 EXECUTIVE SUMMARY ..................................................................................................................................... 10 INTRODUCTION .................................................................................................................................................. 12 1.1 GEOGRAPHICAL LOCATION, ADMINISTRATIVE SYSTEM AND ECONOMY OF MALAWI .......................................... 12 1.2 AN OVERVIEW OF MALAWI’S ECONOMY ............................................................................................................ 12 1.3 DELIVERY OF HEALTH CARE IN MALAWI ........................................................................................................... 13 1.4 BURDEN OF DISEASE IN MALAWI (SOURCE: MALAWI HEALTH SECTOR STRATEGIC PLAN 2011-16) ............... 13 2.0 BACKGROUND INFORMATION OF LIKUNI MISSION HOSPITAL ........................................................ 15 2.1OTHER HEALTH FACILITIES ................................................................................................................................ 15 2.2 POPULATION IN THE CATCHMENT AREA ............................................................................................................. 15 2.3 SOCIAL AND ECONOMIC BACKGROUND OF LMH CATCHMENT AREA ............................................................... 16 2.4 GOVERNANCE .................................................................................................................................................... 16 2.4.1MISSION STATEMENT ...................................................................................................................................... 16 2.4.2VISION ............................................................................................................................................................. 16 2.4.3ORGANIZATIONAL ETHICS AND VALUES ......................................................................................................... 16 2.4.4 THE VALUES LISTED ABOVE WILL BE SUPPORTED BY THE FOLLOWING CODE OF ETHICS FOR BOTH
MANAGERS AND STAFF: ........................................................................................................................................... 17 2.5RATIONALE FOR STRATEGY ................................................................................................................................ 18 3.0 SITUATIONAL ANALYSIS FOR LIKUNI MISSION HOSPITAL ............................................................... 19 3.1 SWOT ANALYSIS .............................................................................................................................................. 19 STRENGTHS: ............................................................................................................................................................ 19 WEAKNESSES .......................................................................................................................................................... 19 OPPORTUNITIES ....................................................................................................................................................... 19 THREATS ................................................................................................................................................................. 20 3.2 POLITICAL, ECONOMIC, SOCIAL AND TECHNOLOGICAL ANALYSIS .................................................................... 20 4.0 STRATEGIC CHOICES ................................................................................................................................... 21 4.1 GOALNO. 1: IMPROVED QUALITY OF ACCESSIBLE AND SUSTAINABLE CLINICAL AND
CLINICAL SUPPORT SERVICES ........................................................................................................................ 21 OVERVIEW: .............................................................................................................................................................. 21 A. THEATRE AND SURGICAL SERVICES .................................................................................................................... 21 CHALLENGES: .......................................................................................................................................................... 22 OBJECTIVE NO. 1: .................................................................................................................................................... 22 STRATEGY 1: ........................................................................................................................................................... 22 ACTIVITIES: ............................................................................................................................................................. 22 STRATEGY 2: ........................................................................................................................................................... 22 ACTIVITIES .............................................................................................................................................................. 22 B. OUT-PATIENT DEPARTMENT (OPD) SERVICES: .................................................................................................. 23 CHALLENGES: .......................................................................................................................................................... 23 OBJECTIVE NO. 2: .................................................................................................................................................... 23 STRATEGY: .............................................................................................................................................................. 23 ACTIVITIES .............................................................................................................................................................. 23 OBJECTIVE NO. 3: .................................................................................................................................................... 23 STRATEGY: .............................................................................................................................................................. 23 ACTIVITIES: ............................................................................................................................................................. 23 C. IN-PATIENT SERVICES ......................................................................................................................................... 24 I. MATERNITY WING ...................................................................................................................................... 24 II. PEDIATRICS: ................................................................................................................................................ 25 OVERVIEW: .............................................................................................................................................................. 25 SENTINEL/SPECIALIZED CARE UNIT SERVICES .......................................................................................... 25 OVERVIEW: .............................................................................................................................................................. 25 III. FEMALE WARD ........................................................................................................................................... 26 OVERVIEW: .............................................................................................................................................................. 26 IV. MALE WARD............................................................................................................................................... 26 OVERVIEW: .............................................................................................................................................................. 26 V. TB WARD ................................................................................................................................................... 26

6
OVERVIEW ............................................................................................................................................................... 26 VI. PRIVATE WING ........................................................................................................................................... 26 VII. ISOLATION WARD ....................................................................................................................................... 26 CHALLENGES FOR IN-PATIENT SERVICES ................................................................................................................ 26 OBJECTIVE NO. 4: .................................................................................................................................................... 26 STRATEGY 1: ........................................................................................................................................................... 26 ACTIVITIES: ............................................................................................................................................................. 26 III. MATERNAL AND CHILD HEALTH (MCH) .................................................................................................... 27 CHALLENGES: .......................................................................................................................................................... 27 OBJECTIVE NO. 5: .................................................................................................................................................... 27 STRATEGY: .............................................................................................................................................................. 27 ACTIVITIES: ............................................................................................................................................................. 27 IV. ORTHOPAEDIC SERVICES: ........................................................................................................................... 28 OVERVIEW: .............................................................................................................................................................. 28 CHALLENGES ........................................................................................................................................................... 28 OBJECTIVES NO. 6: .................................................................................................................................................. 28 STRATEGY: .............................................................................................................................................................. 28 ACTIVITY:................................................................................................................................................................ 28 D. HIV/STI/NUTRITION/TB SERVICES: ................................................................................................................... 28 CHALLENGES: .......................................................................................................................................................... 29 OBJECTIVE NO. 7: .................................................................................................................................................... 29 STRATEGY: .............................................................................................................................................................. 29 ACTIVITIES: ............................................................................................................................................................. 29 E. DRUGS AND MEDICAL SUPPLIES ......................................................................................................................... 29 OVERVIEW: .............................................................................................................................................................. 29 OBJECTIVE NO. 8: .................................................................................................................................................... 29 STRATEGY: .............................................................................................................................................................. 29 ACTIVITIES: ............................................................................................................................................................. 29 OBJECTIVE NO. 9: .................................................................................................................................................... 30 STRATEGY: .............................................................................................................................................................. 30 ACTIVITIES: ............................................................................................................................................................. 30 F. ESSENTIAL MEDICAL EQUIPMENT ....................................................................................................................... 30 OVERVIEW: .............................................................................................................................................................. 30 OBJECTIVE NO. 10: .................................................................................................................................................. 30 STRATEGY: .............................................................................................................................................................. 30 ACTIVITIES .............................................................................................................................................................. 31 G. MEDICAL LABORATORY SERVICES: .................................................................................................................... 31 OVERVIEW: .............................................................................................................................................................. 31 CHALLENGES: .......................................................................................................................................................... 31 OBJECTIVE NO. 11: TO EQUIP THE LABORATORY SECTION WITH ESSENTIAL TESTING AND STORAGE
EQUIPMENT BY SEPTEMBER 2016 ............................................................................................................................ 31 STRATEGY: .............................................................................................................................................................. 31 ACTIVITIES .............................................................................................................................................................. 31 H. RADIOLOGICAL SERVICES: .................................................................................................................................. 31 CHALLENGES: .......................................................................................................................................................... 31 OBJECTIVE NO. 12: .................................................................................................................................................. 32 STRATEGY 1: ........................................................................................................................................................... 32 ACTIVITIES: ............................................................................................................................................................. 32 STRATEGY 2: ........................................................................................................................................................... 32 ACTIVITIES .............................................................................................................................................................. 32 I. DENTAL SERVICES: ............................................................................................................................... 32 OVERVIEW: .............................................................................................................................................................. 32 CHALLENGES: .......................................................................................................................................................... 32 OBJECTIVE NO. 13: .................................................................................................................................................. 33 STRATEGY: .............................................................................................................................................................. 33 ACTIVITIES: ............................................................................................................................................................. 33 J. COMMUNITY HEALTHPROGRAMMES: ...................................................................................................... 33 OVERVIEW: .............................................................................................................................................................. 33 CHALLENGES: .......................................................................................................................................................... 33

7
OBJECTIVE NO. 14: TO ACQUIRE RELIABLE TRANSPORT FORCOMMUNITY HEALTH CARE ACTIVITIES BYMARCH
2017 33 STRATEGY: .............................................................................................................................................................. 33 ACTIVITIES: ............................................................................................................................................................. 33 OBJECTIVE NO. 15: .................................................................................................................................................. 33 STRATEGY: .............................................................................................................................................................. 33 ACTIVITIES: ............................................................................................................................................................. 33 4.2 GOAL NO.2: SUSTAINED REVENUE GENERATION AND ACCOUNTABILITY ................................. 34 OVERVIEW: .............................................................................................................................................................. 34 OBJECTIVE NO. 1: .................................................................................................................................................... 34 STRATEGY: .............................................................................................................................................................. 34 ACTIVITIES: ............................................................................................................................................................. 34 OBJECTIVE NO. 2: .................................................................................................................................................... 34 STRATEGY: .............................................................................................................................................................. 34 ACTIVITIES: ............................................................................................................................................................. 34 OBJECTIVE NO. 3: .................................................................................................................................................... 34 STRATEGY: .............................................................................................................................................................. 34 ACTIVITIES: ............................................................................................................................................................. 34 OBJECTIVE NO. 4: .................................................................................................................................................... 34 STRATEGY NO. 1: .................................................................................................................................................... 34 ACTIVITIES: ............................................................................................................................................................. 35 STRATEGYNO. 2:LIMIT UNBUDGETED EXPENDITURE ............................................................................................... 35 ACTIVITIES .............................................................................................................................................................. 35 4.3 GOALNO. 3: AVAILABILITY OF ADEQUATE, COMPETENT AND COMMITTED EMPLOYEES........ 35 OVERVIEW: .............................................................................................................................................................. 35 HRH POLICIES AND PROCEDURES ........................................................................................................................... 35 HRH DATA .............................................................................................................................................................. 35 HRH PLANNING, TRAINING AND DEVELOPMENT .................................................................................................... 35 HRH BUDGET .......................................................................................................................................................... 36 OBJECTIVE NO. 1: .................................................................................................................................................... 36 STRATEGY: FILL VACANCIES ................................................................................................................................... 36 ACTIVITIES .............................................................................................................................................................. 36 OBJECTIVE NO. 2: .................................................................................................................................................... 36 STRATEGY: .............................................................................................................................................................. 36 ACTIVITIES: ............................................................................................................................................................. 36 OBJECTIVE NO. 3: .................................................................................................................................................... 36 STRATEGY: .............................................................................................................................................................. 36 ACTIVITIES: ............................................................................................................................................................. 36 CAPACITY BUILDING FOR MANAGEMENT AND LEADERSHIP ................................................................ 37 OVERVIEW: .............................................................................................................................................................. 37 OBJECTIVE NO. 4: .................................................................................................................................................... 37 STRATEGY: DEVELOP MANAGEMENT AND LEADERSHIP SKILLS IN MANAGERS ........................................................ 37 ACTIVITIES: ............................................................................................................................................................. 37 4.4 GOAL NO. 4: SOUND AND ADEQUATE INFRASTRUCTURE AND NON-MEDICAL
TECHNOLOGIES .................................................................................................................................................. 37 OBJECTIVE NO. 1: .................................................................................................................................................... 37 STRATEGY: .............................................................................................................................................................. 37 ACTIVITIES: ............................................................................................................................................................. 37 4.5 GOAL NO. 5: EFFICIENT ADMINISTRATIVE AND SUPPORTIVE SYSTEMS ..................................... 38 OVERVIEW: .............................................................................................................................................................. 38 OBJECTIVE NO.1: ..................................................................................................................................................... 38 STRATEGY: .............................................................................................................................................................. 38 ACTIVITIES: ............................................................................................................................................................. 38 OBJECTIVE NO.2: TO MAINTAIN AND INCREASE NUMBER OF SUPPORTIVE FUNDING PARTNERS BY JANUARY
2018 38 STRATEGY: .............................................................................................................................................................. 38 ACTIVITIES .............................................................................................................................................................. 38 OBJECTIVE NO.3: ..................................................................................................................................................... 38 STRATEGY: .............................................................................................................................................................. 38

8
ACTIVITIES .............................................................................................................................................................. 38 0 CONCLUSION .................................................................................................................................................... 41 8.0 APPENDIX ................................................................................................................................................ 51 8.1 STAFF ESTABLISHMENT FOR LIKUNI MISSION HOSPITAL ............................................................... 51 JOB TITLE ............................................................................................................................................................. 51 8.2 KEY HEALTH INDICATORS 2009/10 ......................................................................................................... 53 SOURCE: MALAWI HEALTH SECTOR STRATEGIC PLAN 2011-16.............................................................................. 53 8.3 LIST OFREQUIRED EQUIPMENT FOR THE THEATRE............................................................................. 54 8.4 LIST OF REQUIRED EQUIPMENT FOR RADIOLOGY SECTION ............................................................ 55 8.5 LIST OF REQUIRED EQUIPMENT FOR LABORATORY SECTION ......................................................... 55 8.6 LIST OF EQUIPMENT FOR DENTAL DEPARTMENT ............................................................................. 56

9
ABBREVIATIONS
ADC Area Development Committee
AIDS Acquired Immuno Deficiency Syndrome
ASEC Association of Sisters Education Collaboration
ANC Antenatal Clinic
ARI Acute Respiratory Infection
BEMONC Basic Emergency Obstetric and Neonatal Care
CHAM Christian Health Association of Malawi
CBDA Community Based Distribution Agents
CPR Contraceptive Prevalence Rate
CBM Christoffel Blinden Mission
ECM Episcopal Conference of Malawi
EHP Essential Health Package
ETAT Emergency, Triage, Assessment and Treatment
GoM Government of Malawi
GE Gastro Enteritis
GVH Group Village Headman
GDP Gross Domestic Product
HDU High Dependence Unit
HSSP Health Sector Strategic Plan
HBB Help Baby Breath
HCC HIV Care Clinic
HIV Human Immunodeficiency Virus
HSA Health Surveillance Assistant
HTC HIV Testing and Counseling
I&D Incision and Drainage
IMCI Integrated Management of Child Illness
KMC Kangaroo Mother Care
MASAF Malawi Social Action Fund
MoLGRD Ministry of Local Government and Rural Development
M2M Mother2Mother
MCH Maternal and Child Health
MCC Malawi Council of Churches
MIVA Missionary International Vehicle Association
MoH Ministry of Health
MP Member of Parliament
NCD Non-Communicable Diseases
NRU Nutritional Rehabilitation Unit
OPD Out Patient Department
OIs Opportunistic Infections
PESTI Political Economical Social Technological Infrastructure
PITC Provider Initiated Testing and Counseling
PMTCT Prevention of Mother to Child Transmission
QECH Queen Elizabeth Central Hospital
SVD Spontaneous Vertex Delivery
SWOC Strength, Weakness, Opportunity, Challenges
SHOPS Strengthening Health Outcomes through the Private Sector
SP Strategic Plan
SWOT Strength, Weakness, Opportunity, Threats
TB Tuberculosis
TFR Total Fertility Rate
TA Traditional Authority
ToR Terms of Reference
USAID United States Agency for International Development
VCT Voluntary, Counseling and Testing
VHC Village Health Committee
VDC Village Development Committee
WFP World Food Programme

10
EXECUTIVE SUMMARY
In May 2012, SHOPS Project with support from USAID conducted a comprehensive analysis of
financial, programme and organizational development performance of Likuni Mission Hospital. The
analysis revealed multiple opportunities and weaknesses; some of the challenges are being addressed
while others required a strategic approach.
The SHOPS Report helped Board of Governors and Managers of Likuni Mission Hospital contrast
how things should be with how things really are and then decided to close the gap between the two.
The Hospital like most health care facilities in Malawi is threatened by multiple challenges which
demand solutions. This Strategic Plan is a deep probe into the anatomy of the challenges and a
proposal of radical and new methodologies that will enable the organization encounter the challenges.
Board of governors and management realized that if nothing was done this ship (the hospital) would
sink and they won’t blame those who set the anchors, (the missionaries who established the Hospital).
This strategy was developed to defend the mission and vision of the organization against challenges of
all types and sizes. The situational analysis revealed the following as key challenges: - unsatisfied
patients; inadequate medical/surgical supplies, outdated technologies, long waiting times,
unsustainable financing mechanisms, high staff turnover, unreliable and expensive utility services and
poor infrastructure. The Plan helps stakeholders challenge the situation with focus, unity and
cooperation. It helps to isolate symptoms from the disease to avoid mistaking the effect of the
challenges for their causes. It gives insights to avoid misapplication of scarce resources. Questions
were ruthlessly asked about organization’s mission, vision, rules, policies, structures, services,
procedures, departments, plans, budgets and philosophy. None of these were sacred. However
management realized that asking questions alone would not produce changes desired. The questions
were translated into goals, objectives and activities and these were centered on the following
concepts: increased access to quality clinical and support services; good customer care, sustained
health care, financing and accountability, maintenance of sound infrastructure and appropriate
technologies, efficient and supportive administrative services and partnerships and availability of
adequate, qualified and committed staff.
There are opportunities to improve, expand and sustain service delivery at Likuni Mission Hospital as
it is possible to change leopard’s spots without really changing the leopard. To do this, certain things
would be done differently supported by informed and quick decision making. Management Team
commits itself to communicate truthfully and timely to employees and patients. It realizes that giving
half-truths or defending the status quo will not help the organization. Priorities were set to maximize
staff energies and resources. Objectives were set around guiding concepts that support goals. Every
patient would be treated with uttermost courtesy and respect without compromising integrity and
quality. Members of staff would be empowered to do performance self-assessments to enhance
quality service delivery.
.
Health outcomes achieved per Kwacha spent will be improved through efficiency and patient-
centeredness so that value results that individual patient’s desire are met. The Strategy emphasizes on
the whole patient which calls for teamwork and coordination of care across departments. Information
will help to know how resources and care are allocated and delivered respectively and whether new
interventions or practices actually improve outcomes or lower costs.

11
Investment in health management information system that supports care efficiency and effectiveness
would be improved to enable refinement of performance standards. So will cost information be used
wisely to know what care costs and how much time care processes take because without the ability to
understand the costs of care, or how costs compare to outcomes, efforts at cost reduction would revert
to power struggles and arbitrary cuts. Management realizes that without cost information efforts to
improve performance would be mired in turf wars, personal opinions, and clashes of ego. Resources
would flow to services whose advocates are most skilled in internal politics.
This plan is wholly owned by all staff of Likuni Mission Hospital and its key partners. It will be
regularly reviewed to remain relevant to the health care environment of Malawi and the catchment
area.
The Plan has a budget of US $2,056,746.00 for the next five years.

12
INTRODUCTION
1.1 Geographical location, administrative system and economy of Malawi
Malawi is a small, narrow and landlocked country and shares boundaries with Zambia in the west,
Mozambique in the east, south and south west and Tanzania in the north. It has an area of 118,484
km2
of which 94,276 km2
is island. The country is divided into four administrative regions namely
the Northern, Central, Southern and Eastern regions. Malawi has 28 districts and each district is
further divided into Traditional Authorities (T/As) which are ruled by chiefs. The village is the
smallest administrative unit in Malawi and falls under the T/As. In some villages, there are village
health committees (VHCs) whose responsibility is to work with Health Surveillance Assistants
(HSAs) on health issues at village level. HSAs are the lowest cadre employed by the Ministry of
Health (MoH), resident within communities and are attached to a health facility. These HSAs
constitute a link between the community and the health facilities. A group village headman (GVH)
oversees several villages. There is a Village Development Committee (VDC) at GVH level which is
responsible for development activities. Development activities at the higher T/A level are coordinated
by the Area Development Committee (ADC). Politically, each district is further divided into
constituencies which are represented by Members of Parliament (MPs) and in some cases these
constituencies can combine more than one T/As.
In 2008 Malawi’s population was estimated at 13.1 million and growing at the rate of 2.8% per
annum. The proportion of Malawi’s population residing in urban areas is estimated at 15.3%. Malawi
is one of the most densely populated countries in Africa: the population density was estimated at 105
persons per km2 in 1998 and increased to 139 persons per km
2 in 2008 with the Southern Region
having the highest population density at 184 persons per km2. Between 1998 and 2008, Malawi’s
population grew by 4.2 million people. This high population growth is predominantly due to the high
Total Fertility Rate (TFR) now estimated at 5.7 and the low Contraceptive Prevalence Rates (CPR) of
42%1. Almost half of the population is under 15 years of age, and the dependence ratio has risen from
0.92 in 1966 to 1.04 in 2008. The 2008 Population and Housing Census also found that about 7% of
the population in Malawi is comprised of infants aged less than 1 year, 22% were under-fives, and
about 46% were aged 18 years and above. Malawi is predominantly a Christian country (80%). The
literacy rate for women is lower at 59% compared to males at 69%2. Low literacy levels especially
among women and the prevailing cultural diversity have impacts on the lives of Malawians including
health seeking behavior and acceptance of new developments in the fields of agriculture, health and
education, among other sectors.
1.2 An overview of Malawi’s economy
Malawi is one of the poorest countries in the world with a GDP per capita at US$290 in 2009. Poverty
levels are high: in 2009 the proportion of the population living below the poverty line was estimated
at 39% a slight drop from 40% in 2008. Forty three percent of the rural population lives below the
poverty line while in urban areas the proportion is at 14%3. Malawi is predominantly an agricultural
country and this sector accounts for about 35% of the GDP, 93% of export earnings (primarily
tobacco), and provides more than 80% of employment. The sources of revenue from which public
services are funded are mainly taxes on personal income, company profits, trade taxes and grants from
donors.
1NSO.(2011). Demographic and health survey 2010 – preliminary results. Zomba: NSO. 2NSO.(2009). Malawi housing and population census 2008. Zomba: NSO. 3 NSO. (2009). Welfare monitoring survey 2009. Zomba: NSO.

13
In the event of insufficient revenue to cover the budgeted expenditure, the financing of the resultant
deficit is met either from the domestic bank and non-bank sources, or from foreign financing in a
form of donor and overseas bank loans. In such a scenario, the financing of public services in Malawi
is inextricably linked to the aggregate of each of these revenue sources. For instance, in the 2008/09
financial year, the major public sector sources of finance contributed in the following proportions:
domestic taxes had a share of 77.9% and trade taxes had a share of 10.1%, while non-tax revenue was
12.0%. These revenues represented 24.5% of GDP. In terms of recurrent expenditures, health was the
fourth at 10.2% after General Administration (33.9%), Agriculture (18.9%) and Education (13.7%).
The budgetary allocation to the health sector is inadequate despite recommendations from the Abuja
Declaration that Governments should allocate 15% of the funds to health. The Government of Malawi
has made great effort towards achieving the 15% mark. The HSSP (2011-2016) will, among other
things, ensure universal access to health services for the people of Malawi and explore other
alternative sustainable sources of funding for example; by promoting universal access to social health
insurance.
1.3 Delivery of health care in Malawi
In Malawi, health care services are delivered by the public and the private sector. The public sector
includes all facilities under the MoH, Ministry of Local Government and Rural Development
(MoLGRD), the Ministry of Forestry, the Police, Prisons and the Army. The private sector consists of
private for profit and private not for profit providers (CHAM). The public sector provides services
free of charge at point of access while the private sector charges user fees for sustainability and
growth.
The Christian Health Association of Malawi (CHAM) is an ecumenical organization which is owned
by the Episcopal Conference of Malawi (ECM) and Malawi Council of Churches (MCC). The
institution was established in 1966 with the aim of promoting the healing ministry of Jesus Christ
through the provision of supportive, administrative and technical support in the provision and delivery
of health care to member units across the country.
CHAM has one hundred and seventy two (172) member health facilities. These include; twenty (20)
hospitals, twenty (20) community hospitals and the rest are health centers with or without maternity.
CHAM also has ten (10) training colleges. The member facilities have a total of 8,000 health workers
that are deployed across the 172 health facilities. On average, CHAM hospitals reach out to about
4,000,000 people in Malawi. Likuni Mission Hospital is a member of CHAM and is represented in its
structures.

14
1.4 Burden of Disease in Malawi (Source: Malawi Health Sector Strategic Plan 2011-16)

15
2.0 BACKGROUND INFORMATION OF LIKUNI MISSION HOSPITAL
Likuni Mission Hospital located about nine kilometers west of Lilongwe Capital City in the Central
Region of Malawi is a long established health facility. The hospital was founded as a Dispensary in
1940 by the Missionary Sisters of Africa under the Local Ordinary Bishop Julien of the White
Fathers. The dispensary started experiencing a large number of men, women and children coming for
treatment for all sorts of diseases especially pregnant women for delivery. In the first 5 to 6 years,
around 5,000 babies were delivered at an average of 100 babies per month. Half of the babies died
and 50% who survived, two out of five were malnourished and not properly developed. A nursing
training school started in 1956 in order to meet the demand for nursing services and was closed in
1981 due to various managerial problems.
By 1964 Likuni Mission Hospital had developed into a fully-fledged rural hospital with departments
for maternity, pediatrics, General Wards, OPD and Laboratory, apart from the nursing school.
2.1Other Health facilities
2.2 Population in the catchment area
The present day Likuni Mission Hospital is a 231 bed health facility with bed occupancy rate of 50%,
the second largest hospital under CHAM. The hospital refers patients to Kamuzu Central Hospital and
Ethel Mutharika Maternity Wing. The facility conducts 11 fully established outreach clinics. It also
runs a Mental Health Services Centre in partnership with St John of God.
The Hospital serves about40, 000patients per year. The Outpatient Department as point of entry is the
busiest because it is from here where all patients are seen first before being referred to any other
department within the hospital. The hospital has dental, laboratory and radiology services.
The inpatient department is divided into four wards namely; general male ward, general female ward,
pediatric ward, and the maternity wing. The most common causes of admissions for example in the
year 2013 were malaria, pneumonia, malnutrition, tuberculosis, acute respiratory infections,
pregnancy related illnesses, HIV and AIDS, opportunistic infections, and meningitis.

16
The hospital’s Maternal and Child Health Department (MCH) attends to antenatal and postnatal
mothers, health and nutrition of children under the age of five, health and nutrition education to
mothers, and feeding programs to the catchment area and outreach clinics, expanding the reach of
health services to the underserved areas in Malawi. The outreach clinics primarily focuses on
healthcare for under five children including nutrition, immunizations, growth monitoring, palliative
care, ART clinic, HIV testing and counseling.
2.3 Social and Economic Background of LMH Catchment Area
The Hospital’s catchment area has a population of over 168,904 which is largely of low income rural
subsistent farmers, small scale traders and peri-urban wage earners. The majority are within the area
of Traditional Authority Malili. The facility is surrounded by a number of schools namely: Likuni
Boys’ Primary School, Likuni Girls’ Primary School, Likuni Girls’ Secondary School, Likuni Boys’
Secondary School, Likuni Private Secondary School, Skyway Girls’ Secondary School and finally
Natural Resources College. The Facility is accessible to most City residents which has a projected
population of 978,700 people in 2014. Its capacity is equivalent to that of a district hospital.
2.4 Governance
2.4.1Mission Statement
Likuni Mission Hospital exists to provide accessible, sustainable and holistic quality health services to
the catchment area and beyond by following the healing ministry of Jesus Christ.
2.4.2Vision
To be a centre of clinical excellence in Lilongwe District and the surrounding districts. This vision is
a realistic, credible and attractive future for the organization. It will help unleash staff potential
because it serves as beacon for hope and common purpose. It will attract staff commitment, energize
workers, create meaning in employees’ lives, establish standards of excellence, promote high ideals
and bridge the gap between the organization present problems and its future goals and aspirations.
2.4.3Organizational Ethics and Values
Likuni Mission Hospital’s culture, shared values and beliefs that underlie the hospital’s identity are:
a. Christian identity: love, kindness, honest, trustworthy,
b. Accountability
c. Transparency
d. Community participation
e. Ethical consideration
f. Inter-sectoral collaboration
g. Human rights and equity
h. Gender sensitivity
i. Efficiency
j. Effectiveness
k. Sustainability
l. Cost sharing
m. creativeness
n. Responsibility

17
2.4.4 The values listed above will be supported by the following code of ethics for both
managers and staff:
a. At all times provide health care services professionally and ethically, demonstrating attitude of
proficiency, competence and discipline.
b. Comply, at all times, with all applicable laws, legislation and regulations relevant to health
service provision.
c. Take joint ownership for Board decisions and work as partners with all stakeholders.
d. Treat everyone as equal regardless of status, religion, gender or race.
e. Treat everyone, and all things around us, in a way that shows care.
f. Respect the confidentiality of patients at all times.
g. Always have an ‘open door’ policy and be accessible by patients.
h. Not involved in advertising or in statements that mislead people about services.
i. Not forget that Clinics are custodians of people’s health and that health workers owe them a duty
of care and a promise to deliver value for their money.
j. Declare any personal conflict of interest that may compromise health services provision to our
patients.
k. Manage personal and financial affairs in a responsible manner. Anyone with conflict of interest
in a matter or business of the organization will disclose such interest to the Chairperson of the
Board.
l. Managers and staff to show the highest standards of probity, integrity and conduct demonstrated
by:
i. Acting in accordance with the letter of spirit and of the law
ii. Dealing equitably, honestly and responsively with the public and patients
iii. Avoiding real or apparent conflict of interest
m. A strong commitment to patients shown by protecting them from arbitrary and discriminatory
treatment
n. Responsive to LMH shown by:
i. Serving loyally and impartially
ii. Providing frank, honest and comprehensive advice
o. Protecting privacy of patients and clients
p. Actively facilitating the implementation of organization’s policies
q. A strong commitment to accountability demonstrated by:
i. Contributing fully to the accountability of the organization.
ii. Fully supporting administrative measures set to enhance accountability
iii. Recognising that those delegating authority for performance do not lose responsibility
and may be called to account
r. A close focus on results shown by:
i. Pursuing efficiency and effectiveness at all levels
ii. Delivering services to the patients and clients consciously and courteously
iii. Making decisions and taking actions in a timely and competent manner
s. Continuous improvement by teams and individuals through:-
i. Striving for creativity and innovation
ii. Making individuals and team performance count
t. Merit as the basis for achieving excellence in staff by:
i. Ensuring equality of opportunity
ii. Providing fair and reasonable rewards and incentives to high performance
18
2.5Rationale for Strategy
Likuni Mission Hospital has had without a strategic direction for many years. Attempts to develop
one in 2010 were not successful because of lack of management commitment and resources for
paying an external consultant who produced an incomplete copy with minimal stakeholder
consultations. The approach undertaken lacked ownership and comprehension of direction by
management and staff; hence the exercise could not be completed.
It was after a technical and administrative audit by SHOPS Project in 2012 that the new Managing
Agents, (Franciscan Missionary Sisters of Assisi) together with the incoming Management and the
new Board of Governors were motivated to develop a Strategic Plan.
Likuni Mission Hospital once acted as a regional CHAM Hospital for the Central Region with good
reputation. The glory was declining as the Hospital was threatened by multiple challenges which
further threatened its survival and continuity. This recognition and conclusion necessitated the
strategic approach. The need for strategy was also pushed by financial challenges which weakened
financial health of the organization.
SHOPS Project, a USAID funded health systems strengthening project conducted capacity needs
assessment in-services delivery, financial management and organization development. The general
findings were clinical inefficiency, inadequate revenue, staff, medical equipment and lack of strategic
direction. Some of the interventions provided were training of management team and the governing
board in strategy development and implementation, financial management, resource mobilization,
good governance and accountability. Senior management team was oriented on strategy development,
supported in formulation of the terms of reference for the task force. Thereafter a thorough situational
analysis was conducted which included consultations with key stakeholders such as donors, close
CHAM Hospitals, Lilongwe District Health Office, implementing partners such; Mother2Mother,
Elizabeth Glazier Pediatric Aids Foundation, Support for Service Delivery and Integration (SSDI),
Patients, Staff, Ministry of Health (MoH), Christian Health Association of Malawi (CHAM)
Secretariat, donors, Board Members and many more.

19
3.0 SITUATIONAL ANALYSIS FOR LIKUNI MISSION HOSPITAL
The Strategic Plan Task force carried out situational analysis using the Strengths, Weaknesses,
Opportunities and Threats (SWOT) approach. Also applied alongside SWOT was the Political,
Economic, Social and Technological (PEST) analysis. Both qualitative and quantitative data was
collected from within the organization and outside and analyzed to inform choices of strategic areas
(goals). The positives, (Strengths and Opportunities) and negatives, (Weaknesses and Threats) were
related so as to exploit the former and eliminate or reduce impact of the latter in the process of
implementing strategies. Information on strengths and weaknesses was collected from interviews with
staff and patients, SHOPS Project report, financial, clinical, administration and human resource
reports while opportunities and threats data came from competitors, government, community, social
and economic profiles and media. A checklist containing the following was used to generate strengths
and weaknesses of the Hospital: management quality and efficiency, staffing numbers and quality,
degree of centralization, organizational chart, planning, information and control systems, market
share, patients satisfaction, services quality and reputation, equipment obsolesce, procurement system,
quality assurance, productivity/efficiency, employees experience, education, turnover, work
satisfaction, grievances and infrastructure status. The SWOT and PEST findings are summarized
below:
3.1 SWOT Analysis
Strengths:
a. Sound infrastructure;
b. Committed proprietor, management and staff;
c. History of providing quality care;
d. Increase in the number of outpatient clients ( Jan, 2013 to-date);
e. The hospital still enjoys a relatively good reputation;
f. Good relationship with District Health Office and CHAM Secretariat;
g. New Managing Agents of the hospital (Franciscan Missionary Sisters of Assisi);
h. New Board of Governors for the hospital.
Weaknesses
a. Increasing operational costs;
b. Lack of basic resources: human, equipment, medical and surgical supplies;
c. Low cash flow;
d. High technical staff turnover;
e. Unmaintained infrastructure;
f. Old and inadequate medical and non-medical equipment;
g. Low capacity in drugs and medical supplies management;
h. Manual financial systems;
i. Unsatisfied patients and clients;
j. Inadequate administrative policies and systems;
k. Ineffective communication between management and staff;
l. Low prices;
m. Experienced drug stock out.
Opportunities
a. Increasing population;
b. Close to town with potential for insurance patients and clients;
c. Committed government and non-governmental partners;
d. Good road network.

20
Threats
a. Increase cost of medical and surgical supplies;
b. Increasing expectations from patients and health workers;
c. Low disposable income for health service;
d. Global financial crisis that has led to donor fatigue.
3.2 Political, Economic, Social and Technological Analysis
Political: There is political stability in Malawi which is also committed to promotion of cost effective
health care and partnership between Government and CHAM.
Economy: Malawi is one of the lowly ranked economies in the world and it is a landlocked country.
Therefore landing cost for imported good is high. High level of poverty means that few patients can
afford to pay for health services.
Social: There is high burden of preventable and non-communicable diseases and HIV&AIDS which
increases demand for health care.
Technology: Health care industry relies on medical technologies which are expensive. Acquiring
such technologies is challenging is challenging with poor economy.

21
4.0 STRATEGIC CHOICES
Based on the SWOT and PEST analysis, Malawi Health Sector Strategic Plan (2011-2016) and review
of relevant organizational and national documents the following are selected goals for this Plan.
4.1 GOALNO. 1: IMPROVED QUALITY OF ACCESSIBLE AND SUSTAINABLE
CLINICAL AND CLINICAL SUPPORT SERVICES
Overview: Health service delivery is the core business of Likuni Mission Hospital. Clinical and
clinical support sections provide theatre and surgical services, out-patients services (OPD), in-
patients, MNCH services, Orthopedics, HIV, Nutrition, STI, TB, PMTCT, Dental, Primary Health
Care and Services, Laboratory Services and Radiology Services.
a. Theatre and Surgical Services
The unit was partially renovated in2012 with financial help from Professor Emidio Grisostomi.
However essential infrastructure and equipment are still required to meet the minimum health
standards and patients’ needs.
The unit has 5 caesarean sets, 2 major sets, 1medium set and 1special set. On Tuesdays and Thursdays
the department operates on cold list and the rest of the days are for emergencies. The most commonly
performed procedure is the caesarean section which represents over 44% of all procedures performed
in 2013 (See table 2 below).

22
Table 2: Theatre Procedure 2013.
THEATRE
Total
Percentage (%)
Caesarian 212 44.07%
Evacuation 101 21%
Circumcision 36 7.48%
Laparotomy 13 2.7%
Hysterectomy 7 1.46%
Manual removal of Placenta 5 1.04%
Ectopic 4 0.83%
Suturing 3 0.62%
Hernia repair 3 0.62%
Debridement 2 0.42%
2nd degree 2 0.42%
3rd degree 1 0.21%
D&C 0 0%
Others(not mentioned above) 92 19.13%
TOTAL
481
100%
Challenges:
Despite being partially renovated the Unit has inadequate essential surgical equipment such as vital
monitoring and suction machines, oxygen concentrators, shower rooms, scale, baby resuscitaire,
chipped flour, wrong type of tiles, ineffective lamps and lack of aeration .
Objective No. 1: To fully equip the Unit with lacking essential equipment by June 2015
Strategy 1: Write proposals to potential donors for donation of lacking equipment
Activities:
a. Purchase new equipment
b. Repair the faulty equipment
c. Replacing theatre lamps
d. Installing air conditioners
Strategy 2: Fully renovate the Unit
Activities
i. Build shower rooms and doctor’s office.
ii. Replacing the floor

23
B. Out-Patient Department (OPD) Services:
The hospital has General and Private OPDs. OPDs provide general medical consultations and
admissions. In 2013 about 40,000cases were attended. (See Table 3 Below)
Table 3: Out patients 2013
OUTPATIENT DEPT
Total
Percentage (%)
General OPD 38,601 96.48
Private OPD 1,409 3.52
TOTAL
40,010
100
Challenges:
a. Long waiting time;
b. Nurses and patient attendants working in OPD lack ETAT skills;
c. Inadequate clinical officers to attend to referrals from medical assistants;
d. No proper follow up of patients with major chronic non-communicable diseases such as
diabetes, hypertension, heart diseases, and asthma;
e. No established clinics for Non Communicable Diseases
Objective No. 2: To increase knowledge and skills of all staff in ETAT by June 2017
Strategy: Train technical and support staff in ETAT
Activities
a. Plan and organize ETAT training and NCDs
b. Set a room for NCDs Clinics
c. Equip NCDs Clinic Room
d. Monitor and evaluate application of new skills
Objective No. 3: To reduce waiting time from 45 minutes to 30 minutes by May 2015
Strategy: Create adequate space in the General OPD
Activities:
a. Relocate cashier to create space for clinical staff
b. Re-enforce security in new Cashier’s Office
c. Recruit clinical officers for OPD
d. Introduce coupons for controlling patients’ traffic

24
C. In-Patient Services
i. Maternity Wing
Overview: The section has the Antenatal, Labour, and Postnatal Wards. On average the Labour Ward
conducts 300 deliveries per month with an average of 10 deliveries per day. The Maternity Wing is
being renovated. The Labour Ward has 6 delivery suites and 11 postnatal beds. The unit refers
complicated cases to Ethel Mutharika Maternity Wing and Bwaila Hospital for further management.
Likuni Mission Hospital gets referral cases from Malingunde Health Center and Nkhalango Maternity
Clinic which are 20 and 2kilometers respectively. The hospital has Service Level Agreement on
Maternal and Neonatal Health with Lilongwe District Health Office.
Statistics of 2013 were as follows: - neonatal complication cases were 230, maternal complication
cases were 123, deliveries were 2,177 and deaths 50 (i.e. neonatal death and still birth).(See Tables 4,
5 and 6 below).
Table 4: Neonatal Complications 2013
NEONATAL COMPLICATIONS
Total
Percentage (%)
Low Birth weight 98 42.6
Neonatal Sepsis 87 37.8
Asphyxia 45 19.6
Congenital Abnormalities 0 0
TOTAL
230
100

25
Table 5: Maternal Complications 2013
MATERNITY COMPLICATIONS
Total
Percentage (%)
PPH 38 30.9
Obstructed Labor 32 26.0
Malaria In Pregnancy 27 22.0
Eclampsia 14 11.4
APH 6 4.9
Anemia In Pregnancy 3 2.4
Puerperal Sepsis 2 1.6
Ruptured Uterus 1 0.8
Maternal Death 0 0
TOTAL
123
100
Table 6: Labour Wards
LABOUR WARD
Total
Percentage (%)
Caesarian Section 160 7.3
Normal Deliveries 1,909 87.7
Still Births/Fresh 28 1.3
Neonatal Deaths 22 1.0
Vacuum Extraction 32 1.5
Breech 26 1.2
TOTAL
2,177
100
ii. Pediatrics:
Overview: The unit has a capacity of 60 beds and most common conditions for admissions are
malaria, pneumonia, malnutrition, gastroenteritis, organophosphate poisoning, and tuberculosis.
SENTINEL/SPECIALIZED CARE UNIT SERVICES
Overview: Sick patients who need specialized care are admitted in a special unit for close monitoring.
There is lack of neonatal HDU, adult HDU and pediatric HDU. There is a pediatric special care unit
in the children’s ward which is not fully equipped. The unit lacks basic medical equipment.
Because of lack of HDUs; patients in need of such services are referred either to Kamuzu Central or
Bwaila Hospitals which poses risks during referrals.

26
iii. Female Ward
Overview: The Ward has a capacity of 37 beds and the commonest conditions that are treated are
malaria, pneumonia; gynecological conditions, gastroenteritis and good percentage are HIV related
infections. TB cases are diagnosed here and sent to the TB ward. TB patients with other complicated
co-morbidities are also stabilized here and sent back to TB ward after they have recovered.
iv. Male Ward
Overview: The Ward has a capacity of 36 beds and the commonest conditions are malaria,
pneumonia; gastroenteritis and HIV related infections. TB cases are diagnosed here and sent to the TB
ward. TB patients with other complicated co-morbidities are also stabilized here and sent back to TB
ward after they have recovered.
v. TB Ward
Overview: The section admits all newly diagnosed and retreatment TB cases and on average the unit
admits 5 patients per month. The Hospital receives TB drugs from Ministry of Health and patients do
not pay.
vi. Private Wing
Overview: The Wing has a capacity of 21 beds with a mini pharmacy, a Labour ward with a capacity
of 2 patients and a kitchen. The section has both out- patient and in-patient services. The section was
face lifted with funding from Active Africa and friends of Likuni Mission Hospital through
Association of Sisters Education Collaboration (ASEC).
vii. Isolation Ward
The hospital does not have adequate isolation wards, as currently there is only TB ward. As
recommended by the Infection prevention guidelines, there is need to have TB and skin conditions as
isolation wards.
Challenges for In-Patient Services
Challenges for in-patients services are poor infection prevention (IP) standards, inadequate
pharmaceutical supplies, lack of specialized care services (HDUs), linen, and cleaning materials and
poor traffic control due to multiple entries to wards. All these affect the implementation of the
standard infection prevention practices which reduces quality of care provided. Lack of linen also
results in patients sleeping on bare mattresses, which is uncomfortable and unhygienic.
Objective No. 4: To improve quality of health care outcomes for in-patients by April 2015
Strategy 1: Provide adequate resources
Activities:
a. Provide special care units for critically ill patients
b. Provide enough linen
c. Adequate cleaning materials
d. Improve infection prevention in all departments

27
iii. Maternal and Child Health (MCH)
The Maternal and Child Health Section runs antenatal and under five clinics.
Services offered in this section are: Antenatal, PMTCT, postnatal and under-five. Table 7 and 8 are
showing statistics for 2013.
Table 7: Vaccinations 2013
MCH (VACCINATIONS)
Total
Percentage (%)
Pentavalent 1,Polio 1,PCV 1 10,530 24.6
Pentavalent 2,Polio2,PCV 2 10,362 24.2
Pentavalent 3,Polio 3,PCV 3 9,685 22.6
TTV 6,047 14.1
BCG 3,146 7.3
Measles 3,071 7.2
TOTAL
42,841
100
Table 8: Antenatal clinic 2013
MCH (ANTENATAL CLINIC)
Total
Percentage (%)
Subsequent 6,908 66.1
New visits 3,393 32.5
1st Trimester 148 1.4
TOTAL VISITS
10,449
100
Challenges:
a. The building is too small to accommodate all outlined services as above.
b. There is lack of equipment
Objective No. 5: To build a structure for maternal and child health unit by June2018
Strategy: Fundraise for building a structure
Activities:
a. Draw plan for under five building
b. Cost the project
c. Send proposals to potential donors for funding the Project
28
d. Equip the Unit with proper equipment
iv. Orthopaedic Services:
Overview:
The department provides the following services: Plaster of Paris (POP) application, fracture
manipulation under Anaesthesia (MUAs), reduction of dislocations, arthrotomy, debridement and
Disarticulation.
Challenges
The Unit is unable to perform other procedures due to lack of equipment
Objectives No. 6: To construct and equip the Unit by December 2016
Strategy: Follow with a donor (Ferno Rotary Club) who showed interest to fund and equip the Unit
Activity:
To draw a Memorandum of Understanding with Ferno Rotary Club
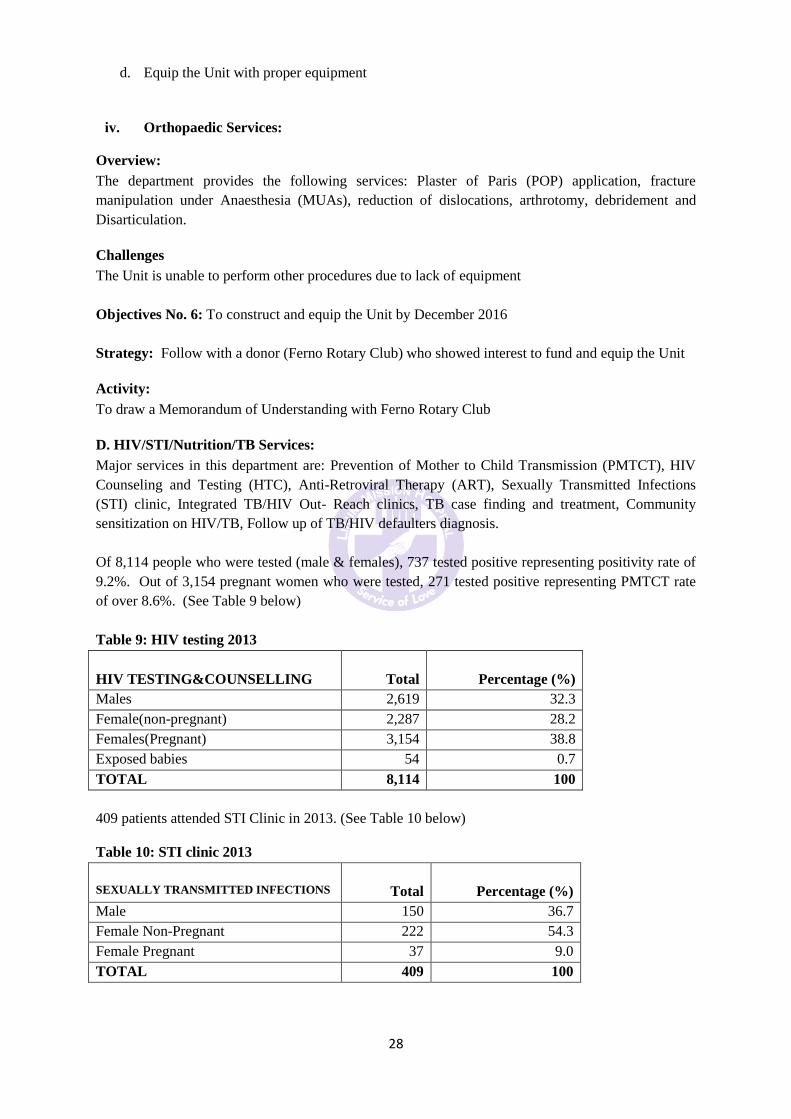
D. HIV/STI/Nutrition/TB Services:
Major services in this department are: Prevention of Mother to Child Transmission (PMTCT), HIV
Counseling and Testing (HTC), Anti-Retroviral Therapy (ART), Sexually Transmitted Infections
(STI) clinic, Integrated TB/HIV Out- Reach clinics, TB case finding and treatment, Community
sensitization on HIV/TB, Follow up of TB/HIV defaulters diagnosis.
Of 8,114 people who were tested (male & females), 737 tested positive representing positivity rate of
9.2%. Out of 3,154 pregnant women who were tested, 271 tested positive representing PMTCT rate
of over 8.6%. (See Table 9 below)
Table 9: HIV testing 2013
HIV TESTING&COUNSELLING
Total
Percentage (%)
Males 2,619 32.3
Female(non-pregnant) 2,287 28.2
Females(Pregnant) 3,154 38.8
Exposed babies 54 0.7
TOTAL 8,114 100
409 patients attended STI Clinic in 2013. (See Table 10 below)
Table 10: STI clinic 2013
SEXUALLY TRANSMITTED INFECTIONS
Total
Percentage (%)
Male 150 36.7
Female Non-Pregnant 222 54.3
Female Pregnant 37 9.0
TOTAL 409 100

29
Challenges:
HIV&AIDS, TB and PMTCT services are provided at different sites and are difficult to integrate
effectively as patients can be lost during internal referrals as they move to and fro the sites.
Youth friendly services and access to information on HIV&AIDS and STI are lacking.
Objective No. 7: To house HIV&AIDS, TB and PMTCT Services in one building for easy integration
by September 2017
Strategy: Follow up potential funding from CDC for construction of one stop centre
Activities:
a. Review budget for unit construction
b. Follow-up with CDC on proposal for construction of a building for integration
c. Train staff in services integration
d. Buy portable ultra sound machine and CTG machine to improve PMTCT services
e. Integrated MCH/HIV/TB services
f. To address lack of youth friendly services
E. Drugs and Medical Supplies
Overview: There is chronic shortage of drugs in every clinical section of the hospital.Drugs and
medical supplies would be improved through use of tools that classify types of drugs, minimum and
maximum stock levels, expiry dates, suppliers, fast moving items and storage capacity and security.
Such information will be used by physicians, pharmacy technicians, Accountant, nursing officers for
stock control, maintenance of supplies, accountability and assessment of prices. Regular checks on
stock will be encouraged and improvements on purchasing practices. Physicians and nurses will be
encouraged to use drug protocals. Patients levels will be monitored against drug usage. Management
is aware that the cost of drugs and medical supplies is very high.
Management discourages unethical practices such as poly pharmacy and unnecessary prescriptions by
physicians. Through prescription monitoring and introduction of essential drug list, it is hoped that the
cost of drugs would be monitored and controlled. Administratively procurement in bulk through IPC
would be encouraged to make savings per unit cost.
Objective No. 8: To increase availability of essential drugs and supplies from 45% to 90% by June
2018
Strategy: Increase budget for drugs and medical supplies
Activities:
a. Develop an essential drug list and review it annually
b. Monitor drugs and medical supply chain
c. Monitor prescription practices
d. Develop medical equipment list
e. Cost the essential drug and essential equipment Lists
f. Write proposals for funding the essential drug and essential medical equipment lists to
potential donors
g. Review drug and medical supply budgets
h. Improve security in pharmacy and dispensary areas by:-
i. Reinforcing the structure

30
ii. Controlling entry into the drug store
iii. Employing new guards
Objective No. 9: To automate drugs and medical supply systems in Pharmacy by March 2017
Strategy: Computerize drugs inventory system
Activities:
a. Train pharmacy personnel in pharmaceutical logistic management
b. Procure computer software package for pharmaceutical management
c. Procure computer for pharmaceutical management
d. Produce monthly drugs consumption and balances report
F. Essential Medical Equipment
Overview: World Bank reported in 1993 that developing countries accounted for 5 billion dollars or 7%
of the 71 billion dollars spent each year on medical equipment. The global estimate included medical and
dental supplies, surgical instruments, electro medical, x-ray, diagnostic tools and implanted products. The
Bank estimated that the market value in sub-Saharan Africa had jumped from 6.3 million dollars in the late
70s to 3.4 billion dollars in the 80s. This tells that the ability of the medical equipment industry to develop
new health care technologies has vastly exceeded the capacity of purchasers to evaluate the clinical value
and cost effectiveness of such innovations. By 1993 there were appropriately 6000 distinct types of medical
devices, and more 750,000 brands, models and sizes produced by 12,000 manufacturers worldwide. The
medical equipment market advertises medical equipment expansion as war against all suffering. It
undermines the reality to accept inevitable and often irremediable pain and impairment, decline and death.
Use of state of art medical equipment is promoted by professionals for improved diagnosis and treatment
results and also for prestige. Patients also demand use of latest technologies.
Challenges facing Likuni Mission Hospital on medical equipment includes: - aged equipment, lack of some
essential equipment: lack of maintenance, lack of trained maintenance personnel and lack of spare parts.
The Hospital lacks policy on donation of medical equipment which results in receipt of unnecessary
equipment that may address needs of the organization.
In deciding appropriateness of technologies to procure, Likuni Mission Hospital will be guided by
relevance of the technology to health problems, safety, effectiveness, appropriate life span, cost, ease of
use, capacity to function in the unit environment, acceptability and accessibility by patients and clients,
addition of value, reputable source and maximum benefits.
The hospital will draw an essential equipment list to guide procurement and acceptance of donated
essential equipment.
The hospital lacks adequate essential medical technologies for disease investigations and treatments.
The following equipment is required for effective service delivery: blood pressure machines, pulse
dosimeters, thermometers, glucometers, suction machines, nebulizers, vacuum extractors, oxygen
concentrators, digital and manual scales, fluid calibrators and vital monitoring machines.
Objective No. 10: To have adequate essential medical equipment by December 2018
Strategy: Purchase of essential medical equipment

31
Activities
a. Draw a list of needed essential medical equipment
b. Identify potential suppliers
c. Budget for procurement of equipment
d. Write proposals to potential donors and partners
e. Increase budget for essential medical equipment
G. Medical Laboratory Services:
Overview: The Laboratory Section conducts the following tests: Hematology, Biochemistry,
Serology, Microbiology and Parasitology.
Challenges:
a. Lack of blood bank refrigerator in the hematology subsection, hence, most patients who
qualify for blood transfusion are either referred to Kamuzu Central Hospital (KCH) or are
asked to get a blood donor;
b. There is lack of important machines such as Viral Load Machine, Manual FBC, Differential
Counter and Tally Counter;
c. There is no PCR machine for Microbiology tests.
Objective No. 11: To equip the Laboratory Section with essential testing and storage equipment by
September 2016
Strategy:To procure lacking equipment
Activities
a. Write grant proposals
b. Buy the blood bank fridge and machines
c. Train laboratory personnel in management of laboratory machines
H. Radiological Services:
Overview: The Unit provides the following services: X-rays, Ultrasound, and Echocardiography. A
total of 4480 radiological procedures were conducted between January and December2013. The most
commonly performed procedure was Ultrasound representing about 70.1%.
Table11. Radiology Procedures 2013
RADIOLOGY TOTAL PERCENTAGE %
Ultrasound 3,139 70.1
X-Ray 1,341 29.9
TOTAL 4,480 100
Challenges:
a. Small waiting area which has a small space for entry into the darkroom;
b. The ultrasound room is hot and therefore not an ideal room for examination;
c. Actinic markers for patient’s information are not available;
d. The section doesn’t have radiation monitoring devices such as badges/dosimeters and there
is no quality control equipment such as densitometers for measuring the density of machine
permeation.
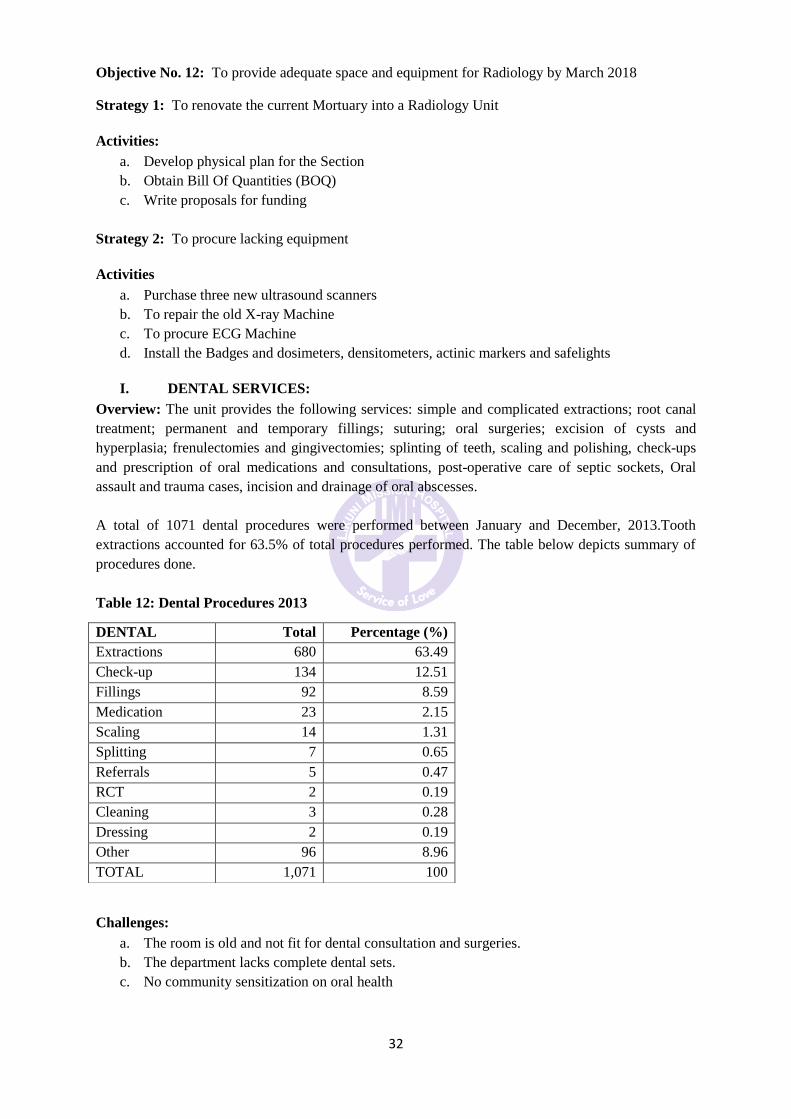
32
I. DENTAL SERVICES:
Overview: The unit provides the following services: simple and complicated extractions; root canal
treatment; permanent and temporary fillings; suturing; oral surgeries; excision of cysts and
hyperplasia; frenulectomies and gingivectomies; splinting of teeth, scaling and polishing, check-ups
and prescription of oral medications and consultations, post-operative care of septic sockets, Oral
assault and trauma cases, incision and drainage of oral abscesses.
A total of 1071 dental procedures were performed between January and December, 2013.Tooth
extractions accounted for 63.5% of total procedures performed. The table below depicts summary of
procedures done.
Table 12: Dental Procedures 2013
Challenges:
a. The room is old and not fit for dental consultation and surgeries.
b. The department lacks complete dental sets.
c. No community sensitization on oral health
Objective No. 12: To provide adequate space and equipment for Radiology by March 2018
Strategy 1: To renovate the current Mortuary into a Radiology Unit
Activities:
a. Develop physical plan for the Section
b. Obtain Bill Of Quantities (BOQ)
c. Write proposals for funding
Strategy 2: To procure lacking equipment
Activities
a. Purchase three new ultrasound scanners
b. To repair the old X-ray Machine
c. To procure ECG Machine
d. Install the Badges and dosimeters, densitometers, actinic markers and safelights
DENTAL Total Percentage (%)
Extractions 680 63.49
Check-up 134 12.51
Fillings 92 8.59
Medication 23 2.15
Scaling 14 1.31
Splitting 7 0.65
Referrals 5 0.47
RCT 2 0.19
Cleaning 3 0.28
Dressing 2 0.19
Other 96 8.96
TOTAL 1,071 100

33
Objective No. 13: To have a new Dental Unit by March 2018
Strategy: To construct and equip new Dental Unit
Activities:
a. Draw physical plan for the Unit
b. Obtain Bill Of Quantities (BOQ)
c. Write proposals for funding
d. Purchase new dental instruments including a dental chair
J. COMMUNITY HEALTHPROGRAMMES:
Overview:The concept of primary health care has the following elements: health education, local
disease control and treatment of communicable diseases, Immunization against childhood illnesses,
nutrition and food supply, treatments of common childhood illnesses, sanitation and safe water
supply, outreach clinics for ante-natal and child health, Prevention and treatment of community
malnutrition and community oral health education.
Community health services are delivered through traditional leadership structures in coordination with
other social sectors that influence peoples’ health e.g. education and agriculture.
Challenges:
The Unit faces several challenges for comprehensive PHC service delivery. The challenges include
the following:-
a. Inadequate motor cycles for outreach clinics and community supervision
b. Inadequate financial support for outreach activities
c. Poor waste management in communities
d. Inadequate personnel in the department
Objective No. 14: To acquire reliable transport for community health care activities by March 2017
Strategy: Procure an off load vehicle and motor bikes for community health care services
Activities:
a. Identify of possible donor
b. Write grant proposals for purchase of a vehicle and three motor cycles
c. Coordinate with other social sectors
d. Increase budget for community health
Objective No. 15: To improve waste management in the community by April 2016
Strategy: Provide health education in waste management in the community
Activities:
a. Intensifying community supervision
b. Engaging traditional leaders as gate keepers in hygiene and sanitation
c. Train Village Health Committees in hygiene and sanitation

34
4.2 GOAL NO.2: SUSTAINED REVENUE GENERATION AND ACCOUNTABILITY
Overview: Success of the Plan depends among other factors on availability of adequate financial
resources. The Hospital’s cash flow has been poor for the past years due to multiple factors including;
poor credit and debt management, decreasing revenue from services and donations and lack of
accountability. The accounts have not been externally audited for five years. SHOPS Report cited the
following as key challenges in revenue generation and accountability:-
a. Balancing financial sustainability with preferential treatment for the poor
b. Insufficient working capital to cover operational expenses
c. High dependency on Ministry of Health
d. Declining revenue from services
e. Inability to leverage assets
Objective No. 1: To conduct annual external financial audit by the April 2015
Strategy: Hire competitive external auditors
Activities:
a. Budget and prepare for external auditing
b. Advertise and hire external auditors
Objective No. 2: To improve generation and use of financial management information system by
June 2015
Strategy: Automate the financial information system
Activities:
a. Assess capacity needs of the Accounting Department
b. Develop and implement training plan in Accounts computerization process
c. Procure ten computers
d. To procure photocopier, printers and filing cabinets
e. Improve supportive supervision
f. Produce regular, accurate and timely financial report and management accounts
Objective No. 3: To increase revenue from hospital fees from38 % to60% by January 2016
Strategy: Invest in areas where the hospital generates more income
Activities:
a. Lobby for revised SLA prices
b. Maintain physical quality in the Private Wing
c. Revision of dental fees
d. To train staff on customer care
e. To train staff on clinical quality care
Objective No. 4: To use budgets to control hospital expenditures and coordinate activities by January,
2016
Strategy No. 1: Orient budget holders on budgeting and budget monitoring
35
Activities:
a. Decentralize budgets to cost centers
b. Train budget holders on budget management
c. Accounts office to provide monthly budget versus actual reports with variance analysis
StrategyNo. 2:Limit unbudgeted expenditure
Activities
a. Promote custodial, authorization and recording control systems
4.3 GOALNO. 3: AVAILABILITY OF ADEQUATE, COMPETENT AND COMMITTED
EMPLOYEES
Overview: Generally there is chronic shortage of appropriately trained human resource for health in
Malawi. Human Resources for Health (HRH) are a critical resource that influences quality and
quantity of care provided. It holds the largest wage bill on unit’s budget and yet there is a general
complaint of shortage of staff which results in high locum and overtime bills. Making available
competent, adequate and committed HRH requires managerial skills to rethink HRH management and
development. Things that HRH find rewarding is not only extrinsic but also patients’ satisfaction,
recognition, patients’ contact, responsibility, opportunities for career development, autonomy and
successful team work. It is obvious that people who joined the Hospital are not primarily motivated by
money. However the opportunity to enhance performance through pay incentives cannot be ignored.
With financial incentives for performance and other factors the organization will be able to attract and
retain high performers if they are motivated by chance to earn more.
The Hospital has a workforce of 207 of which is trained technical staff. (See appendix 1)
HRH Policies and Procedures
For efficient organizational performance, supporting policies in recruitment and selection, training
and development and motivation are needed. The current policies are outdated and therefore they
need to be updated to be in line with HRH expectations and local Labour Laws
HRH Data
Data on staff is manually collected, stored and analyzed which delays decision making and planning
for efficiency. Human resource development plan is a necessary tool to operationalize training and
development policy which should be supported by policies on recruitment and selection.
HRH Planning, Training and Development
An HRH Plan when available will answer questions of: Current number of employees, age profile,
biggest department, skills that employees possess, number of employees resigning every year and
department often affected. These questions currently cannot be ably answered because of lack of HRH
data and a coherent plan. A plan will help in recruitment, training needs assessment and management
development.
Without a written plan and unclear training and development policies, needs for skills relevant to the
organization are unclear and opportunities for training and development become blurred. Apart from
skills development, training enhances motivation and offers opportunities for promotion.

36
Current job descriptions do not set clear performance targets which makes performance measurement
challenging. There is a culture prevailing which disables employees to deal with problems outside
their immediate work domain because job descriptions are restrictive.
HRH Budget
Apart from budget for emolument, HRH does not have budgets for training and development.
Objective No. 1: To reduce vacancy rate for trained professionals from 19.75% to 3% by January,
2017
Strategy: Fill vacancies and review job descriptions
Activities
a. Analyze critical posts that need to be filled
b. Negotiate the review of CHAM approved establishment
c. Recommend current employees with good performance records for promotions
d. Review job descriptions
Objective No. 2: Reduce attrition rate from 6% to 2% by December, 2015
Strategy: Motivate staff sustainably
Activities:
a. Pay salaries and locum timely
b. Provide staff uniforms
c. To recognize and appreciate high performing staff
d. Re-introduce departmental competitions and awards.
e. Improve tools for performance measurement
f. Set pre-agreed key performance indicators
g. Induct managers on performance measurement
h. Improve communication structures and tools
Objective No. 3: To develop and implement training and development plan by March 2015
Strategy: Lobby for the review of the training and development policy with health institutions within
the Archdiocese.
Activities:
a. Analyze training requirements for effective work performance
b. Decide on appropriate training methods
c. Allocate resources for training and development
d. Implement the training plan, monitor and evaluate training
e. Improve managers skills in supportive supervision, mentorship and coaching
37
CAPACITY BUILDING FOR MANAGEMENT AND LEADERSHIP
Overview: Getting things done through others and soliciting staff commitment towards set goals
require managerial and leadership skills in managers and supervisors. As the Hospital competes with
the best providers of health care, it needs managers who can lead on what works well, be innovative
and take initiative. Management requires abilities to control transactions using policies, directions and
other incentives.
Objective No. 4: To improve management and leadership capacity of the organization by December,
2015
Strategy: Develop management and leadership skills in managers
Activities:
a. Conduct needs assessment
b. Plan for capacity building in management and leadership
c. Orient managers and supervisors on performance management
d. Managers should help their teams clarify goals and objectives set out in the Plan
e. Focus on vision and shared values in order to build relationships among different disciplines
f. Provide common ground to enlist teams in the strategy implementation process.
4.4 GOAL NO. 4: SOUND AND ADEQUATE INFRASTRUCTURE AND NON-MEDICAL
TECHNOLOGIES
Overview: Sound infrastructure is also an integral part of health care provision. Where buildings are
old, dilapidated and left in state of disrepair they pose physical risks to health workers, patients and
the public and could also be a source of infections and litigations. On the other hand, well maintained
and sound buildings form part of physical quality and attract patients who want to be associated with
such facilities.
During the Strategic Plan period and beyond, attention will be paid to maintenance of soundness of
infrastructure through preventive maintenance, routine repairs and maintenance. It is recognised that
neglected buildings and faulty equipment carry financial and social costs to organizations.
Objective No. 1: To improve physical condition of buildings by September 2017
Strategy: Lobby for partners to assist in infrastructure development
Activities:
a. Increase space for guardian shelter
b. Renovate dilapidated buildings including staff houses
c. Construct new structures for pharmacy
d. Renovate staff houses
e. Construct High Dependency Units
f. Construct hospital kitchen
g. Construct hospital mortuary
h. Hire a competitive site engineer to plan for new structures
i. Obtain Bill Of Quantities (BOQ)
j. Fundraise for new structures

38
k. Produce preventive maintenance plans
l. Steel fence for demarcations
m. Put fly screens in the wards
4.5 GOAL NO. 5: EFFICIENT ADMINISTRATIVE AND SUPPORTIVE SYSTEMS
Overview: Efficient administrative and supportive systems ensure that clinical health workers have
resources they need in timely and appropriate quantities in order to deliver quality health
services.
Objective No.1: To generate accurate and timely information for rational decision making by
September, 2015
Strategy: Computerize information collection, storage, analysis and retrieval
Activities:
a. Computerise and integrate information system of the hospital
b. Train appropriate staff in computer data collection, storage and analysis
c. Buy and install computers with appropriate capacity
d. Monitor and evaluate data management
e. Maintain website
Objective No.2: To maintain and increase number of supportive funding partners by January 2018
Strategy: Improve governance, accountability and publicity of Hospital services and performance.
Activities
a. Develop a database for potential funding partners
b. Share Strategic Plan with potential donors and partners
c. Share hospital performance outcome report
d. Publicise website address and related features
Objective No.3: To promote good governance and ethical principles by June 2015
Strategy: Re-enforce professional code of ethics, effective management and leadership.
Activities
a. Translate and communicate code of ethics
b. Orient staff on professional code of ethics
c. Maintain competency and proficiency through training, coaching and supervision
d. Avoid exploitation of professional relationships for personal gain
e. Encourage reporting of cases of malpractices and unethical practices
f. Improve managers and supervisors’ communication, problem solving and decision making
skills.

39
5.0 PERFORMANCE MONITORING AND DOCUMENTATION
In the process of health services delivery use of information, technologies, finance and human
resource for health to achieve short term outputs and long term outcomes would be robust
and effectively coordinated. How the Hospital does this now is under scrutiny because of
concerns of inefficiencies and infectiveness. Monitoring, (the routine tracking of
programmes’ activities on regular basis to determine if a programme is going in the right
direction), will help understand whether resources are used efficiently and for desired
purposes. Staff capacity would be assessed and be strengthened through training and
supportive supervision so that they appreciate the reason for collecting data, type of data to
collect, how and who will be collecting it. Questions will be formulated around different
programmes ran by the organization. Indicators would be simplified so that processes of
monitoring and evaluation using both qualitatively and quantitative information are made
easy and participatory. Monitoring as pointed out will help determine improvements or
changes to be made. Regular meetings of the Board, Management and staff of the
organization will discuss, make necessary changes and learn from successes and failures.
Unit meetings on performance reports under relevant objectives will also be shared, discussed
and impact measured against set milestones and targets. It would be appropriate to strengthen
capacity of managers and supervisors to enable them lead analysis of data and use of
information for operational and strategic decision making. Best practices will be documented
and shared for learning and improvements.
Data Collection Tools
In collecting data, both quantitative and qualitative methods will be used with collection tools
such as patients’ charts, tally sheets, open ended questions or check lists. For easy application
tools will be designed in participatory format, simplified, made concise and pre-tested to
ensure their friendliness. It is hoped that quality of data collected would be promoted by
training staff in monitoring and evaluation, incorporating quality checks at all stages and by
attending to errors that may arise due to transposition, copying, coding, routing, consistency
and range.
Data Flow
The flow of data will be mapped by answering questions on who will be responsible for data
collection, supervision and data quality. The flow would also show frequency of data
collection, compilation, submission and analysis.
Data Analysis
This would compare data collected against monitoring and evaluation questions set. And its
purpose would be to check if objectives set were being met. It would help summarise data
and generate new objectives. Analysis will focus on programmes description and conformity
to its design. The analysis would be through comparison of actual performance against
targets, current performance against prior performance and the general trend in performance.
Data Interpretation
There is no point in collecting information unless results are used to improve programmes.

40
Results generated from data analysis will help highlight successful strategies for replication
and scale up. They would also help to determine whether targets set were being reached or
not, identify weaknesses that need to be improved. In summary it would be used to make
decisions, modify or improve programmes delivery.
Presentation of information
Information analyzed from data will be presented in several formats such as tables, line, bar
and pie charts with clear explanatory notes to show trends over time, compare similar items
or show components of a whole.
Data Types
The following data types would be collected for processing into information:
a. Health determinants data (socioeconomic, environmental, behavioural and genetic
factors) and the contextual environments within which the Company operate);
b. Inputs data such as staff, finances, drugs, medical supplies, utilities, equipment,
infrastructure information and transport
c. Process related data (policies, service acquisition and delivery systems, protocols,
accountability tools)
d. Performance or output data such as clinical attendances, new clients, discharges,
trained staff , operations, x-ray and lab investigations, revenue, debts, credits
e. Outcomes data (mortality, morbidity, disease outbreaks, health status, disability and
wellbeing), solvency ratio.
Inputs would be monitored using set company systems and policies. The frequency will
depend on resource availability and capacity of data collectors in the Company and at Head
Office. Indicators and tools for monitoring inputs will include data from admission records,
patients/clients records, clients’ feedback, laboratory results, clinic registers, and records on
causes of morbidity and mortality and of course of disability adjusted life years (DALYs)
Data will be collected from different sources such as programmes, facility based surveys and
where necessary from local surveys. Management will decide selection of types of data to
collect, analyse and use. Roles and responsibilities of data collectors and users would be
defined for smooth data flow and information use. They would be trained to be ethical in
order to get cooperation from patients, service providers and other people who act as
informants. Methods used will include routine sources as such patients’ treatment files, health
passport booklets, observations, interviews and questionnaires or surveys. Data will be
analysed through frequency distribution and by comparing indicators of actual performance
against set targets and bench marking among Company. Interpretation will involve analysis
why performance was met, exceeded or not met and what external factors influenced the
performance levels. To enable learning information presented will have to confirm what was
expected or already known, change or illuminated new ideas.
Although high level inputs are generally associated with satisfactory performance;
management will pay attention to efficiency so that resources are converted to bring desired
achievements through acceptable processes of converting them to outputs. Health
Management Information System (HMIS) would help identify problems and needs, make
evidence-based decisions on organizational policies and allocate scarce resources optimally.
Data collected will be segregated by age, sex, disease condition in case of clinical data. The
following simplified table will help in monitoring and evaluation.

41
Clinical and Clinical Support Data
CONCLUSION
The Strategic Planning Taskforce team conclude the assignment with the conviction that development of
the Strategic Plan for Likuni Mission Hospital was long overdue. The process itself provided an
opportunity for the key stakeholders to review and reflect upon the operations of the hospital. The
conclusion is that the Strategic Plan, as the output of a joint effort, is worthwhile implementing.
TYPE OF
INFORMATION
SOURCE PURPOSE FREQUENCY DATA
COLLECTOR
Out Patient
Department Services
OPD Registers a. Resources allocation
b. Forecast utilization rate
c. Quality improvement
d. Analysis of cost
effectiveness
Daily Data Clerk
In-Patient (
Admission) Services
In- patient
Registers
a. Assets utilization rate
b. Budgeting for resources
c. Quality improvement
d. Analysis of cost
effectiveness
Daily Data Clerk
Disease Specific
Service e.g.
HIV&AIDS, ART,
TB, Cancer, ANC,
Diabetes,
Hypertension
Specific
patients’
registers
a. Accessibility
b. Allocation of resources
c. Quality improvement
e. National reporting
Daily Data Clerk
Stock levels of
essential drugs and
medical supplies
Pharmacy a. Procurement planning
b. Budgeting
c. Efficiency analysis
d. Cost recovery analysis
Weekly Pharmacy
Technician
Dental Services Dental
Register
a. Access analysis
b. Quality improvement
c. Resources allocation
Daily Data Clerk
Stock levels of
essential drugs and
medical supplies
Pharmacy a. Procurement planning
b. Budgeting
c. Efficiency analysis
d. Cost recovery analysis
e. Loss reduction
Weekly Pharmacy
Technician

42
Goal
No.
Objective
Related Activities Key
Performance
Indicators
Timeframe in years Responsible
officer
Estimated
costs
Remarks/
Major
Assumptions
2015
2016
2017
2018
2019
1 To fully equip the
Theatre Unit with
lacking essential
equipment by Dec,
2019
Renovate shower rooms (Theatre) and
doctor’s office.
Construction
Report
X PHA $
1,200.00
Replacing floor Renovation
Report
X PHA 5,000.00
Write proposal for donated equipment
and or funding for purchase of
equipment
Submitted
proposal
X
PHA 100.00
Procure vital monitoring and suction
machines, oxygen concentrator, and
scale and baby resuscitaire.
Procurement
Report
X
X MD 64,000.00
Procure theatre beds, recovery beds,
autoclave, equipment trolleys, lockable
shelves and mobile operating lamps
Procurement
Report
X X X X MD 65,700.00
2. To increase
knowledge and
skills of all staff in
quality of care by
Dec,2017
Plan and organize ETAT training. Training report X X X X MD 10,000.00 Seek DHO
Support
Plan and organize NCDs Training Report X X X X X MD 5,000.00
Set a room for NCDs Clinics Room set X X X X X PNO 500.00
Monitor and evaluate application of
new skills
Performance
report
X X X X X MD 50
3. To reduce
waiting time from
45 minutes to 30
minutes by May,
2015
Relocate cashier’s office to create
space for clinical staff
Re-allocation
Report
X Accountant 300.00
Reinforce security in new cashier’s
office
X Accountant
Recruit clinical officers for OPD X HRO 200.00
Introduce coupons for monitoring
patients’ traffic
Patients
satisfaction
Survey feedback
X PNO 1,500.00
4. To improve
quality of health
care outcomes for
in-patients by
Conduct regularly clinical audits and
act on recommendations
Reduced cases of
infections
X X X X X MD 500.00 As cases occur
Revise and negotiate for revised SLA
prices and invest in quality of care
Revised SLA
prices
X X X PHA 100 Lobby through
CHAM

43
April, 2015 Train and orient staff in IP
IP Training
Report
X X X X X PNO 10,000.00
Provide IP supplies and regularly
replenish them
Renovation
Report
X X X X X PNO 68,000.00
Renovate and equip specialist unit for
adults (HDU)
Renovation
Report
X PHA 60,000.00
Renovate and equip paediatric
specialized unit
Renovation
report
X PHA 30,000.00
5. To renovate and
extend current
maternal and child
health unit by
June, 2017
Draw and cost plan for new under five
building
Cost plan X PHA 641
Submit plan to potential donors for
funding
Correspondence
letters
X
PHA 150
Renovate and extend the Unit Project plan X PHA 60,000.00
Equip the renovated unit with ultra
sound machine
Equipment
procurement
report
X PHA 10,000.00
6. To construct
and equip
Orthopaedic with
necessary
equipment such as
minor ORIF,
amputation and
Sequestrectomy by
December,2017
Follow up with a prospective donor on
funding and equipping the Unit
Follow up with
potential donor
X 100
Construct and equip the Unit
Construction
Report X PHA 70,000
7. To accommodate
HIV&AIDS, TB
and PMTCT in one
building for easy
integration by
September, 2017
Review budget for unit construction
Review Report X Accountant 20
Follow-up with CDC on proposal for
construction of a building for
integration
Follow up report X PHA 10
Orient staff on services integration
Orientation
Report
X PNO 180.00
8.To increase Develop and cost an essential drug list Available X X X X MD 324,924.92
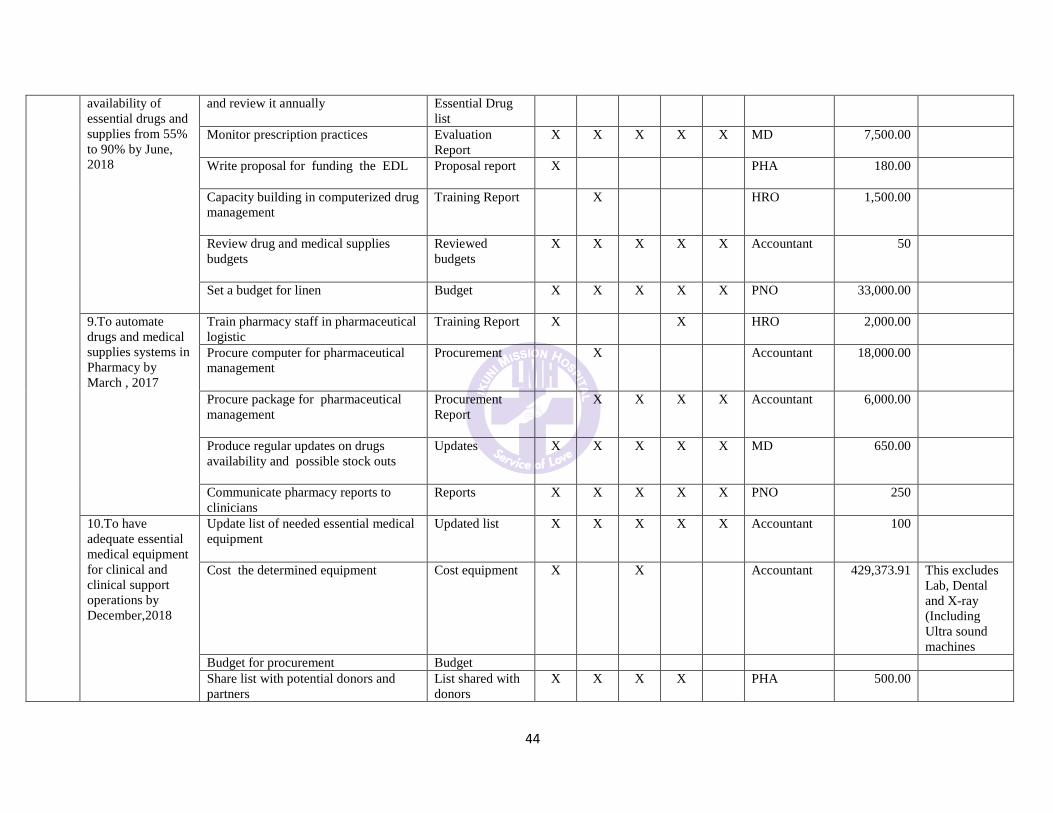
44
availability of
essential drugs and
supplies from 55%
to 90% by June,
2018
and review it annually
Essential Drug
list
Monitor prescription practices
Evaluation
Report
X
X X
X X MD 7,500.00
Write proposal for funding the EDL
Proposal report X PHA 180.00
Capacity building in computerized drug
management
Training Report X HRO 1,500.00
Review drug and medical supplies
budgets
Reviewed
budgets
X X X X X Accountant 50
Set a budget for linen
Budget X X X X X PNO 33,000.00
9.To automate
drugs and medical
supplies systems in
Pharmacy by
March , 2017
Train pharmacy staff in pharmaceutical
logistic
Training Report X X HRO 2,000.00
Procure computer for pharmaceutical
management
Procurement X Accountant 18,000.00
Procure package for pharmaceutical
management
Procurement
Report
X X X X Accountant 6,000.00
Produce regular updates on drugs
availability and possible stock outs
Updates X X X X X MD 650.00
Communicate pharmacy reports to
clinicians
Reports X X X X X PNO 250
10.To have
adequate essential
medical equipment
for clinical and
clinical support
operations by
December,2018
Update list of needed essential medical
equipment
Updated list X X X X X Accountant 100
Cost the determined equipment Cost equipment X
X Accountant 429,373.91 This excludes
Lab, Dental
and X-ray
(Including
Ultra sound
machines
Budget for procurement Budget
Share list with potential donors and
partners
List shared with
donors
X X X X
PHA 500.00

45
11. To equip
Laboratory with
essential testing
and storage
equipment such as
blood bank, manual
FBC and tally
counter and PCR
machines by Dec,
2016
Write funding proposals
Proposal
Report X
X X X
PHA 100
Buy the blood bank fridge and
machines
Procurement
report
X Accountant 8,788.00
Equip the laboratory with FBC
differential counter, tally count,
automated chemistry machine, viral
load machine and PCR machine
Procurement
report
X
Accountant
47,691.37
To purchase adequate lab reagents
Procurement X Accountant 20,512.82
12.To provide
adequate space and
equipment for
radiology by
March, 2018
Develop physical plan for radiology Plan X PHA 641.00
Cost the plan
Renovation Plan X PHA 20,000.00
Write proposal for funding
construction
Proposal
submitted
X PHA 500.00
Equip renovated unit into X-ray Unit
with ultra sound scanner and X Ray
machine
Procurement
Report X PHA 73,887.97
Install badges and dosimeters,
densitometers, actinic markers and
safelights
Installation
Report
X
MD 100
13.To have a new
Dental Unit by
March 2018
Draw physical plan for the Unit
Construction
Plan X PHA 641.00
Write proposals for funding
construction
Proposal
submitted X
PHA 30,000.00
Buy new dental instruments including a
dental chair
Procurement
Report X Accountant 25,000.00
14. To have
reliable transport
system for
community health
care activities by
March, 2017
To buy a vehicle for community health
Approved
quotation
X PHA 42,000.00
Increase budget for community health
projects
Revised budget X MD 10,000.00
To buy an ambulance
Approved
quotation X PHA 42,000.00
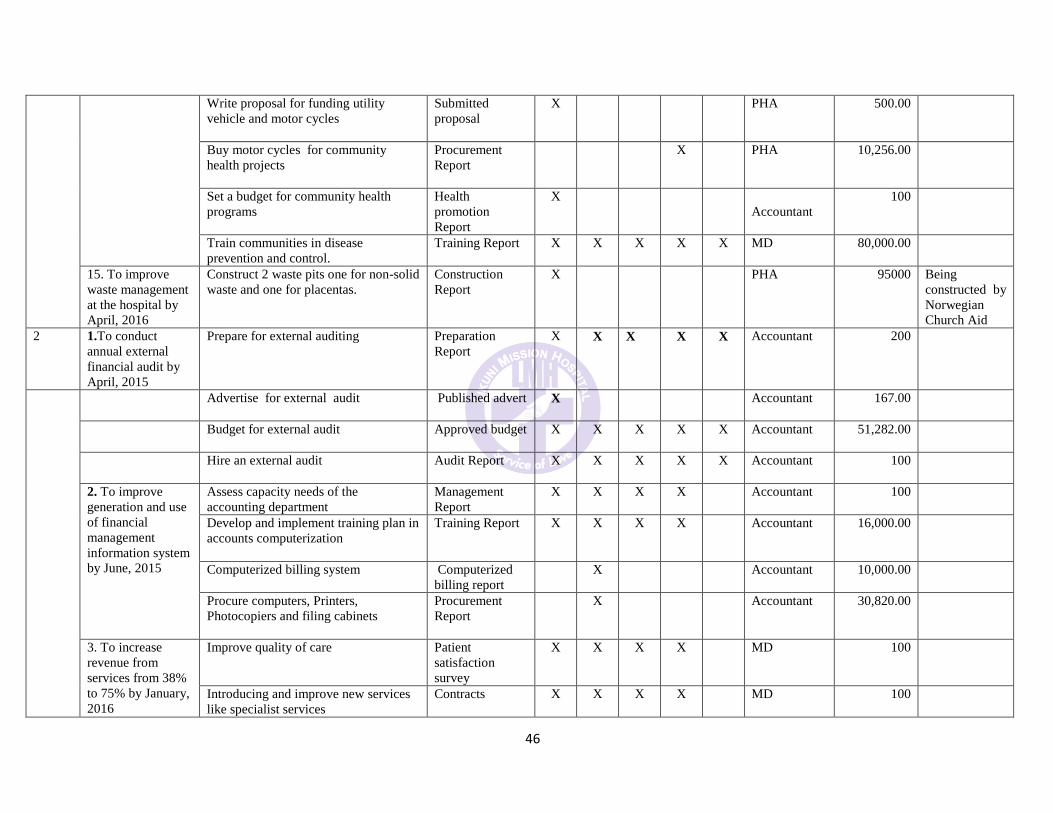
46
Write proposal for funding utility
vehicle and motor cycles
Submitted
proposal
X PHA 500.00
Buy motor cycles for community
health projects
Procurement
Report X PHA 10,256.00
Set a budget for community health
programs
Health
promotion
Report
X
Accountant
100
Train communities in disease
prevention and control.
Training Report X X X X X MD 80,000.00
15. To improve
waste management
at the hospital by
April, 2016
Construct 2 waste pits one for non-solid
waste and one for placentas.
Construction
Report
X PHA 95000 Being
constructed by
Norwegian
Church Aid
2 1.To conduct
annual external
financial audit by
April, 2015
Prepare for external auditing
Preparation
Report
X X X X X Accountant 200
Advertise for external audit
Published advert X Accountant 167.00
Budget for external audit
Approved budget X X X X X Accountant 51,282.00
Hire an external audit
Audit Report X X X X X Accountant 100
2. To improve
generation and use
of financial
management
information system
by June, 2015
Assess capacity needs of the
accounting department
Management
Report
X X X X
Accountant 100
Develop and implement training plan in
accounts computerization
Training Report X X X X
Accountant 16,000.00
Computerized billing system
Computerized
billing report X Accountant 10,000.00
Procure computers, Printers,
Photocopiers and filing cabinets
Procurement
Report X Accountant 30,820.00
3. To increase
revenue from
services from 38%
to 75% by January,
2016
Improve quality of care Patient
satisfaction
survey
X X X X
MD 100
Introducing and improve new services
like specialist services
Contracts X X X X
MD 100

47
Attract more insured patients Attendance/
Invoice value
X X X X
MD 250
Negotiate for revised SLA prices
Minutes of
negotiation
meeting
X X X
Accountant 100
Invest in potential services that are
underutilized
Investment Plan X X X
MD 100
4. To improve use
of budgets to
control hospital
expenditures and
coordinate
activities by June,
2016
Re-orient budget holders on budgeting
and budgets management
Training Plan X Accountant 100
Decentralize budgets to cost centers X Accountant 0
Accounts office to provide monthly
budget versus actual reports with
variances analysis
Budgets vs.
actual reports
X X X X X Accountant 150
Sanction unbudgeted expenditure. Budget
compliance
Reports
X X X X X Accountant 0
3
1.To reduce
vacancy rate from
19.75% to 3% by
January 2017
Analyze critical posts that need to be
filled
Analysis report
X HRO 100
Negotiate review of CHAM approved
establishment
Minutes of
negotiation
meeting
X X X X X HRO 50
Trade in some positions Report on traded
in posts HRO 100
2.Reduce attrition
rate from 6% to 2%
by December ,2015
Advertise, conduct interviews and
select capable candidates
Advertisements
X
X
X
X
X
HRO
2,880.00
Provide staff uniforms. Purchase report X X X X X 4,620.00
Review system of providing free
medical care to control
Reviewed
allowance
X HRO
Improve tools for performance
measurement/management
Improved tools
report
X HRO 4,000.00
Induct managers on performance
measurement
Induction Report X HRO 0
Introduce non-monetary incentives Incentives
Report X PHA 100
Improve communicate structures and New structures X HRO 100
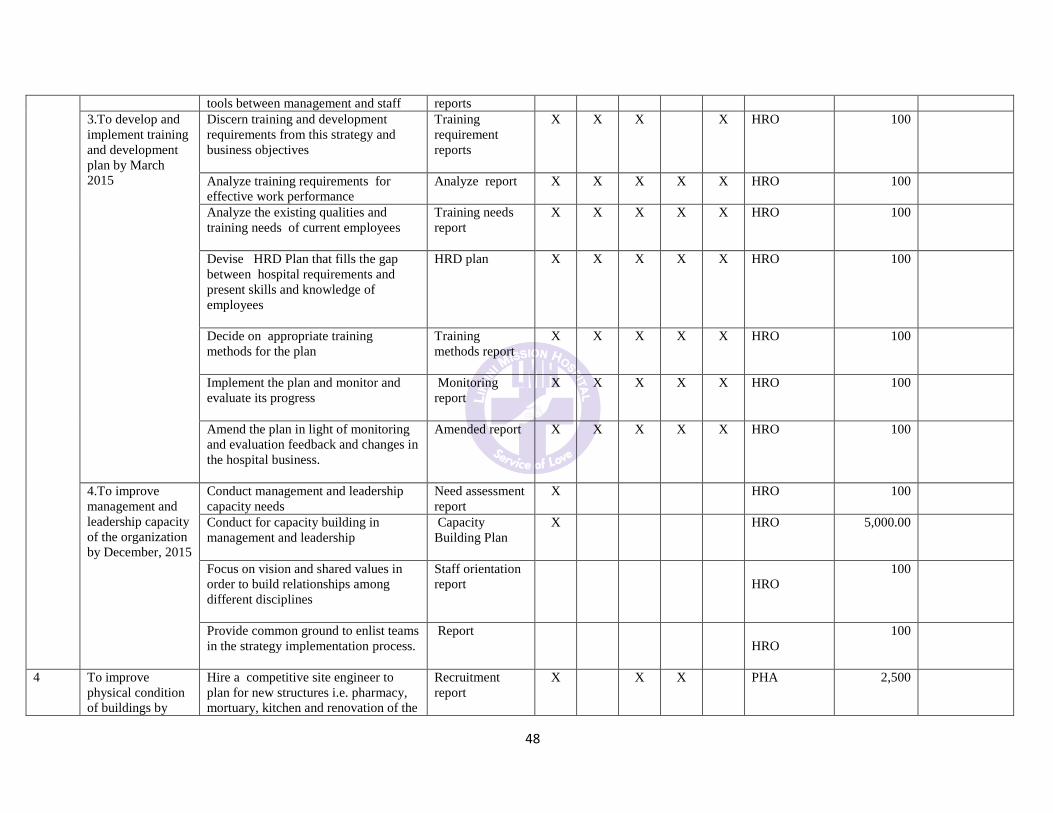
48
tools between management and staff reports
3.To develop and
implement training
and development
plan by March
2015
Discern training and development
requirements from this strategy and
business objectives
Training
requirement
reports
X X X
X HRO 100
Analyze training requirements for
effective work performance
Analyze report X X X X X HRO 100
Analyze the existing qualities and
training needs of current employees
Training needs
report
X X X X X HRO 100
Devise HRD Plan that fills the gap
between hospital requirements and
present skills and knowledge of
employees
HRD plan X X X X X HRO 100
Decide on appropriate training
methods for the plan
Training
methods report
X X X X X HRO 100
Implement the plan and monitor and
evaluate its progress
Monitoring
report
X X X X X HRO 100
Amend the plan in light of monitoring
and evaluation feedback and changes in
the hospital business.
Amended report X X X X X HRO 100
4.To improve
management and
leadership capacity
of the organization
by December, 2015
Conduct management and leadership
capacity needs
Need assessment
report
X HRO 100
Conduct for capacity building in
management and leadership
Capacity
Building Plan
X HRO 5,000.00
Focus on vision and shared values in
order to build relationships among
different disciplines
Staff orientation
report
HRO
100
Provide common ground to enlist teams
in the strategy implementation process.
Report
HRO
100
4
To improve
physical condition
of buildings by
Hire a competitive site engineer to
plan for new structures i.e. pharmacy,
mortuary, kitchen and renovation of the
Recruitment
report
X
X X
PHA 2,500
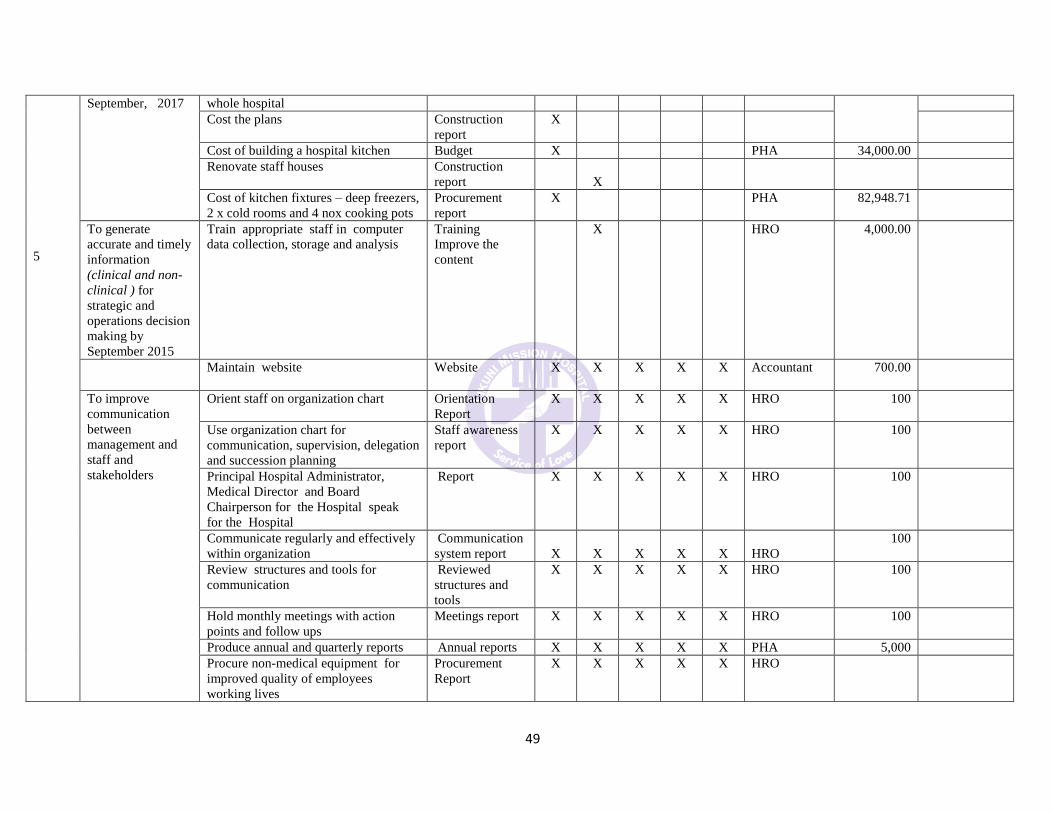
49
5
September, 2017
whole hospital
Cost the plans
Construction
report
X
Cost of building a hospital kitchen Budget X PHA 34,000.00
Renovate staff houses Construction
report
X
Cost of kitchen fixtures – deep freezers,
2 x cold rooms and 4 nox cooking pots
Procurement
report
X PHA 82,948.71
To generate
accurate and timely
information
(clinical and non-
clinical ) for
strategic and
operations decision
making by
September 2015
Train appropriate staff in computer
data collection, storage and analysis
Training
Improve the
content
X HRO 4,000.00
Maintain website
Website X X X X X Accountant 700.00
To improve
communication
between
management and
staff and
stakeholders
Orient staff on organization chart Orientation
Report
X X X X X HRO 100
Use organization chart for
communication, supervision, delegation
and succession planning
Staff awareness
report
X X X X X HRO 100
Principal Hospital Administrator,
Medical Director and Board
Chairperson for the Hospital speak
for the Hospital
Report X X X X X HRO 100
Communicate regularly and effectively
within organization
Communication
system report
X
X
X
X
X
HRO
100
Review structures and tools for
communication
Reviewed
structures and
tools
X X X X X HRO 100
Hold monthly meetings with action
points and follow ups
Meetings report X X X X X HRO 100
Produce annual and quarterly reports Annual reports X X X X X PHA 5,000
Procure non-medical equipment for
improved quality of employees
working lives
Procurement
Report
X X X X X HRO

50
To maintain and
increase number of
supportive funding
partners by
January, 2018
Develop a database for potential funding
partners
Database
available
X X X X X PHA 1,000
Publicise website address and related
features
Newspaper
adverts
X X X X X PHA 2,880.00
Coordinate planning with Lilongwe
District Health Office
Joint meetings
report
X X X X X MD 200
To promote good
governance and
ethical principles
by June, 2015
Translate and communicate code of
ethics
Discuss ethics
during meetings,
issue warning
letter for
unethical
behavior.
X X X X X HRO 100
Orient staff on professional code of
ethics
Orientation
report
X
X
X
X
X
HRO
100
Managers and staff to conduct all
personal and professional activities
with honesty, integrity, respect,
fairness and good faith in a manner that
reflects well among the profession and
organization
Managers
conduct report
X
X
X
X
X
HRO
0
Comply with all laws in Malawi No of legal cases X X X X X HRO
Maintain competency and proficiency Competency
report
X X X X X HRO 100
Avoid exploitation of professional
relationships for personal gain
No cases of
exploitation
X X X X X HRO 0
Encourage reporting of cases of
malpractices and unethical practices.
Reported cases X X X X X HRO 0
Improve managers and supervisors’
communication, problem solving and
decision making skills.
Training report X X X X X HRO 100
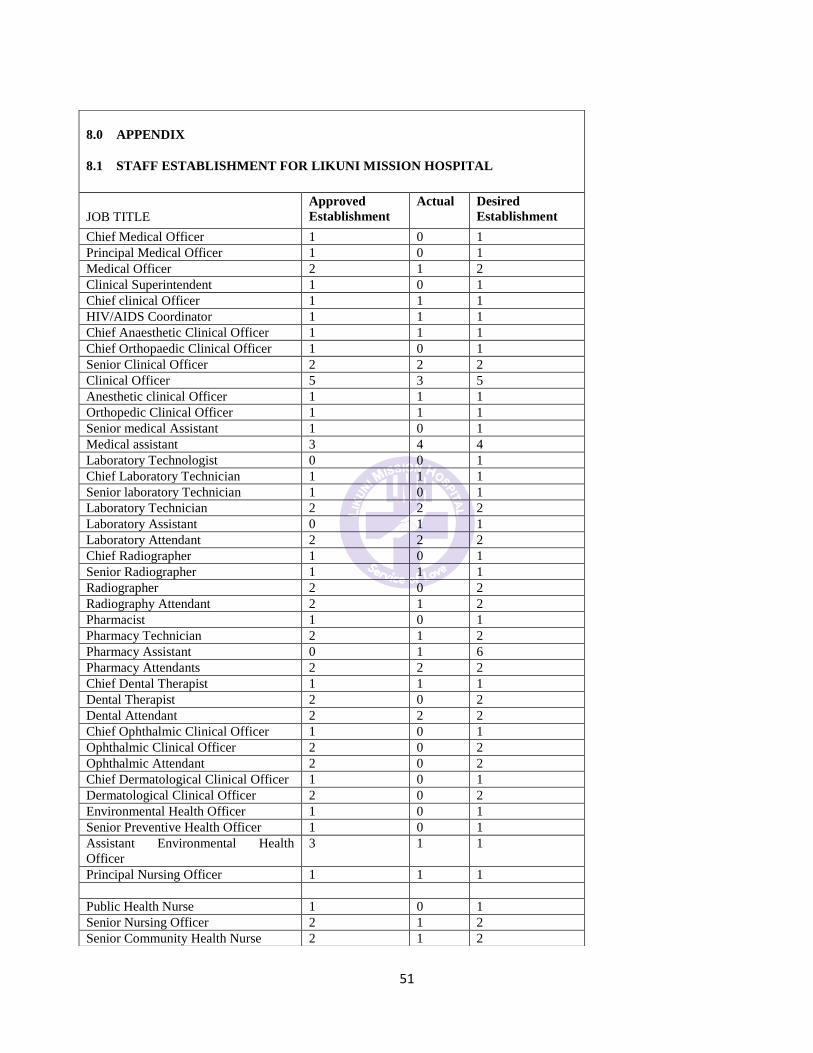
51
8.0 APPENDIX
8.1 STAFF ESTABLISHMENT FOR LIKUNI MISSION HOSPITAL
JOB TITLE
Approved
Establishment
Actual Desired
Establishment
Chief Medical Officer 1 0 1
Principal Medical Officer 1 0 1
Medical Officer 2 1 2
Clinical Superintendent 1 0 1
Chief clinical Officer 1 1 1
HIV/AIDS Coordinator 1 1 1
Chief Anaesthetic Clinical Officer 1 1 1
Chief Orthopaedic Clinical Officer 1 0 1
Senior Clinical Officer 2 2 2
Clinical Officer 5 3 5
Anesthetic clinical Officer 1 1 1
Orthopedic Clinical Officer 1 1 1
Senior medical Assistant 1 0 1
Medical assistant 3 4 4
Laboratory Technologist 0 0 1
Chief Laboratory Technician 1 1 1
Senior laboratory Technician 1 0 1
Laboratory Technician 2 2 2
Laboratory Assistant 0 1 1
Laboratory Attendant 2 2 2
Chief Radiographer 1 0 1
Senior Radiographer 1 1 1
Radiographer 2 0 2
Radiography Attendant 2 1 2
Pharmacist 1 0 1
Pharmacy Technician 2 1 2
Pharmacy Assistant 0 1 6
Pharmacy Attendants 2 2 2
Chief Dental Therapist 1 1 1
Dental Therapist 2 0 2
Dental Attendant 2 2 2
Chief Ophthalmic Clinical Officer 1 0 1
Ophthalmic Clinical Officer 2 0 2
Ophthalmic Attendant 2 0 2
Chief Dermatological Clinical Officer 1 0 1
Dermatological Clinical Officer 2 0 2
Environmental Health Officer 1 0 1
Senior Preventive Health Officer 1 0 1
Assistant Environmental Health
Officer
3 1 1
Principal Nursing Officer 1 1 1
Public Health Nurse 1 0 1
Senior Nursing Officer 2 1 2
Senior Community Health Nurse 2 1 2

52
Nursing officers 4 4 4
Senior Nursing Sister 10 10 10
Community health nurse 4 1 4
NMT/EN/M 39 34 39
Senior Patient attendant 3 3 3
Home craft workers 3 3 3
Senior Hospital Attendant 5 5 5
Patient attendant 15 16 16
Hospital attendant 25 27 27
FINANCE &ADMINISTRATION DEPARTMENT
Principal Hospital Administrator 1 1 1
Senior Administrative Officer 1 0 1
Accountant 1 1 1
Senior Assistant Accountant 1 1 1
Assistant Accountant 1 0 1
Senior Accounts Assistant 1 1 1
Accounts Assistant 4 7 9
Human Resources Officer 1 1 1
Statistician 1
IT Officer 1
Assist Human Resources Officer 1 0 1
Assistant Records Officer 1 0 1
Senior Records Assistant 1 1 1
Clerical Officer 1 2 1
Records Assistant 2 2 2
Stores Supervisor 1 1 1
Maintenance Supervisor 1 1 1
Laundry Supervisor 1 1 0
Short hand Typist 1 1 1
Senior Clerk Officer 1 1 0
Senior Data Preparation Clerk 1 1 1
Stores Clerk 1 1 0
Receptionist 1 1 0
Data Preparation Clerk 2 2 2
Copy typist 3 3 2
Plumber 1 1 0
Electrician 1 1 1
Boiler Attendant 1 1 1
Drivers 4 4 6
Senior PBX Operator 1 0 1
Mortuary Attendant 3 2 3
Senior Laundry Attendant 1 0 1
PBX Operator 2 2 2
Head and Deputy Security Guard 3 2 2
Laundry Attendant 5 4 5
Messenger 2 2 2
Security Guard 5 6 17
Cooks 0 0 5
Tailor 1 1 2
Capitao 1 1 1
Ground Workers 10 10 15

53
8.2 KEY HEALTH INDICATORS 2009/10
Source: Malawi Health Sector Strategic Plan 2011-16
INDICATOR 2009/2010
Total Population 13.1 million
Maternal Mortality Rate/100,000 live births 510 (UN
Estimates)
Infant Mortality Rate (Per 1,000 live births) 66
Under five mortality Rate (per 1,000 live births) 112
Contraceptive Prevalence Rate (DHS 2000) 42
Antenatal care Coverage (%) 97
% of U5 children with fever 2 weeks prior to survey 34.5
% of U5 children with fever who received anti-
malarial drugs within 24 hours after onset of fever
43.4
% of households who own ITNs 56.8
% of children sleeping under ITNs 47.1
% of pregnant women sleeping under ITNs 43.3
% of pregnant women who took recommended 2 or
more doses of IPT
60 (2010)
Tuberculosis treatment success rate (%) 86 (2009)
Death rates due to TB 8 (20`0)
TB default rate (%) 2 (2009/2010)
HIV prevalence among 15-49 year olds 12% (2007)
HIV prevalence among young people aged 15-24 -
% of health facilities providing a minimum package
of PMTCT services
100 (2010)
% of U5 children with ARIs 8.5 (2006)
% of U5 children with an ARI taken to health
facility for treatment
65.7
% of U5 children with diarrhea 24.1 (2006)
Percentage of children underweight (Percentage) 13
Measles vaccination coverage (%) 93
% of deliveries taking place in health facilities 71.5

54
8.3 LIST OFREQUIRED EQUIPMENT FOR THE THEATRE
ITEM NO.
DESCRIPTION
QUANTITY
1 Anaesthetic Machine 2
2 Oxygen Concentrator 3
3 Laryngscope Set 4
4 Theatre Bed 2
5 Suction Machines 3
6 Resuscitator 1
7 Monitors 2
8 BP Machines 2
9 Thermometer 2
10 Autoclave 2
11 Laparatomy Set (Major) 1
12 Laparatomy Set (Minor) 1
13 Suture Set 1
15 Trolleys for spreading sets during surgery 4
16 Quarterisation Machine 2
17 Operating lamps both mobile and fixed to the roof 4
18 Lockable shelves to store drugs 3
19 Linen
20 Boots 10 pairs
21 Recovery Bed 2
22 Oxygen Cylinders 3
23 Electric Blanket 1
24 Chairs 10
25 Tables 3
26 Refrigerator 1
27 Theatre Cape and Attire 20 pairs
28 Macintosh sheets 10
29 Goggles 5
30 Fluid Warmer 2
31 Triple Stand 1
32 Basin 7
33 Plastic Buckets 5

55
8.4 LIST OF REQUIRED EQUIPMENT FOR RADIOLOGY SECTION
ITEM NO.
DESCRIPTION
QUANTITY
1
Digital Radiography X-Ray Machine
1
2
X-Ray Machines
2
3
PL X 160 Digital Medical X-Ray Machines
1
4
X-Ray Accessories: Cassettes, Scatter Grids
5
Barium Suphate
12 bottles
6
Japamiron 300
6 bottles
7
Gastrografin
6 bottles
8
Ultrasound Machine
1
9
Black and White Ultrasound Printer
1
8.5 LIST OF REQUIRED EQUIPMENT FOR LABORATORY SECTION
ITEM NO.
DESCRIPTION
QUANTITY
1
Blood Bank
1
2
Automated Chemistry Machine
1
3
Viral Load Machine
1
4
Adequate Lab Reagents
5
FBC Machine
1
6
PCR Machine
1

56
8.6 LIST OF EQUIPMENT FOR DENTAL DEPARTMENT
ITEM NO.
DESCRIPTION
QUANTITY
1 Dental Chair 1
2 Complete Mobile Dental Filing Unit
3 (Operating Light) Dental Lamp 1
4 Hand Pieces (slow and high speed) 2
5 X-Ray (Intra-Oral) processors and accessories 1
6 Curing Light Unit 1
7 Scalers (Ultra-sonic)
8 Autoclave (Sterilizer) 1
9 Dental Stool 2
10 Suction Unit & WAP Portable Suction 2
11 Cabinets
12 Dental Intra-oral camera – Endoscope WI-FI 1
13 Ligature Wires
15 Arch Bars and Endodontic Kit 4
16 Composite/Plastic filing instruments 4 sets
17 Elevators – Straight Cryers 20 pieces
18 Haemostats 10
19 Tweezers 10
20 Crown and Bridge Removers
21 Probes/Explorers (Double ended) 20
22 Spatulas 10
23 Excavators 20
24 Plastic/Amalgamator Instruments 5 liters
25 Hand Scalers
26 Retractors
27 Scissors 10
28 Periodontics instrument
29 Carvers 10
30 Forceps – both upper and lower
31 Pins and Posts
32 X-Ray Consumables and accessories
33 Rotary Instruments and accessories
34 Dental Syringes 10