stopping tki therapy in chronic myeloid leukemia
TRANSCRIPT
Stopping TKI therapy in chronic myeloid leukemia
Delphine Rea, MD, PhDPôle Hématologie Oncologie Radiothérapie
INSERM UMR-1160Centre Hospitalo-Universitaire Saint-Louis
AP-HP, Paris
BHS meetingLa Hulpe, BelgiumFebruary 11, 2017
CML: state of the art in 2017
• Five ATP-competitive TKIs are currently approved for CML.
• Life expectancy of optimal responders to TKIs is close to that of the general population and increase in CML prevalence.
• Leukemic stem cells are resistant to TKI-induced cell death and are capable of restoring leukemia in mice and upon TKI discontinuation in most patients, explaining current recommendation of a lifelong therapy.
• However, clinical trial contradicted the notion that TKI may never be stopped and treatment-free remission may be achievable under certain conditions.
Gambacorti-Passerini et al. J Natl Cancer Inst. 2011;103(7):553-61.Huang et al. Cancer. 2012 Jun 15;118(12):3123-7.Hehlmann R. Blood. 2012;120(4):737-47.Bower et al. J Clin Oncol. 2016;34(24):2851-7.
Lauseker et al. J Cancer Res Clin Oncol. 2016;142(7):1441-7.Gunnarsson et al. Eur J Haematol. 2016;97(4):387-92.Pearson et al. Leuk Res. 2016;43:1-8. Cortes et al. J Clin Oncol. 2016;34(20):2333-40.
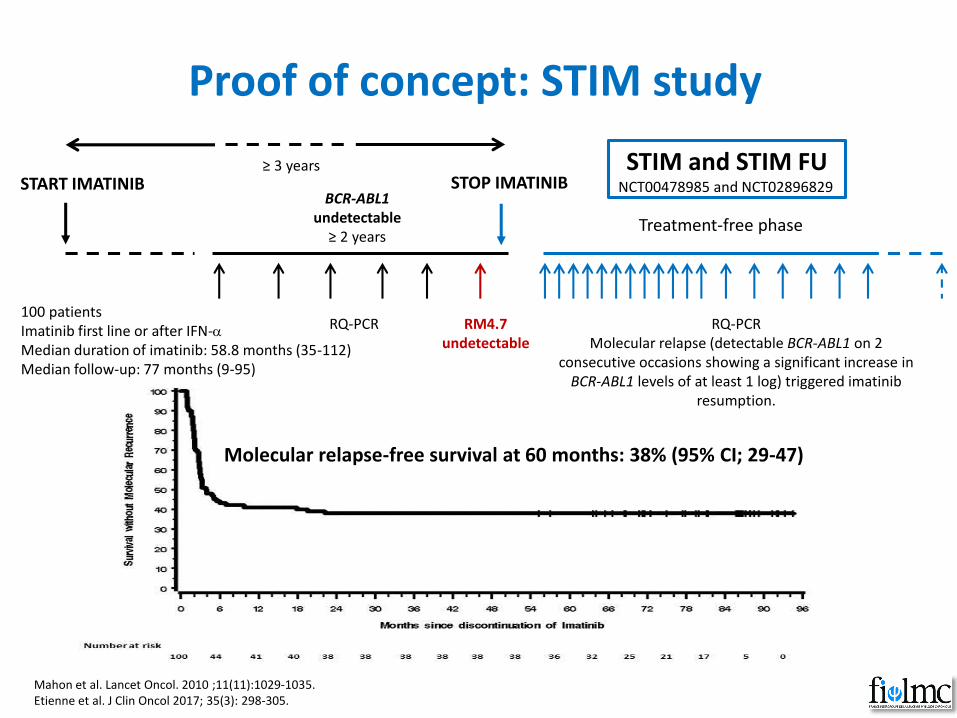
Proof of concept: STIM study
Mahon et al. Lancet Oncol. 2010 ;11(11):1029-1035.Etienne et al. J Clin Oncol 2017; 35(3): 298-305.
START IMATINIBBCR-ABL1
undetectable ≥ 2 years
RQ-PCR RM4.7undetectable
RQ-PCRMolecular relapse (detectable BCR-ABL1 on 2
consecutive occasions showing a significant increase in BCR-ABL1 levels of at least 1 log) triggered imatinib
resumption.
STOP IMATINIB
Treatment-free phase
STIM and STIM FUNCT00478985 and NCT02896829
≥ 3 years
100 patientsImatinib first line or after IFN-aMedian duration of imatinib: 58.8 months (35-112)Median follow-up: 77 months (9-95)
Molecular relapse-free survival at 60 months: 38% (95% CI; 29-47)
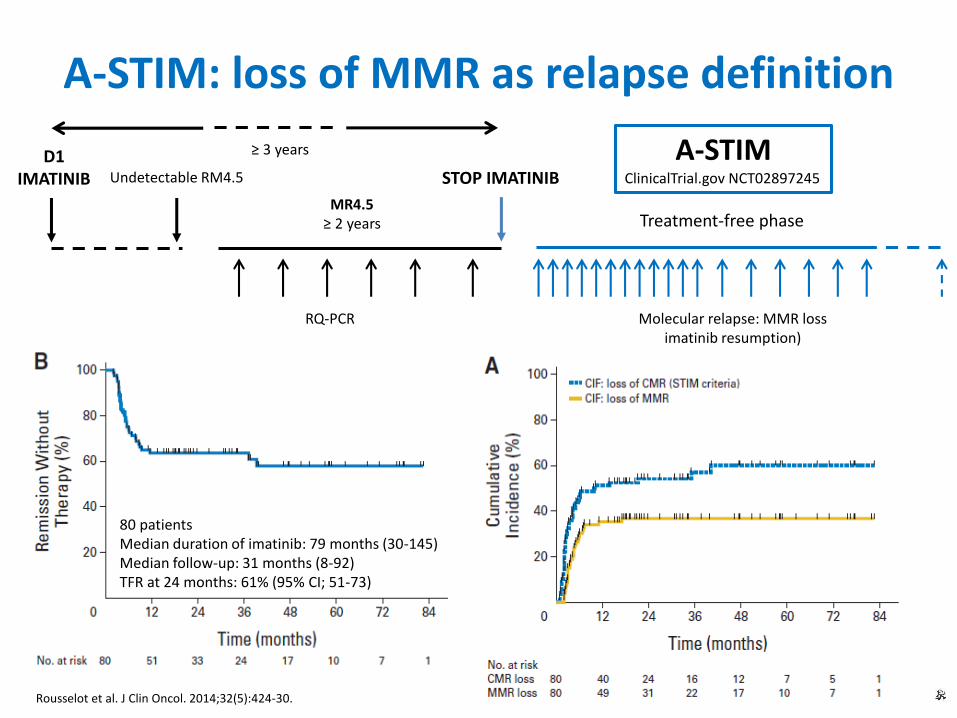
A-STIM: loss of MMR as relapse definition
D1IMATINIB Undetectable RM4.5
MR4.5≥ 2 years
RQ-PCR
STOP IMATINIB
Treatment-free phase
A-STIMClinicalTrial.gov NCT02897245
Molecular relapse: MMR lossimatinib resumption)
Rousselot et al. J Clin Oncol. 2014;32(5):424-30.
80 patientsMedian duration of imatinib: 79 months (30-145)Median follow-up: 31 months (8-92)TFR at 24 months: 61% (95% CI; 51-73)
≥ 3 years

Other imatinib discontinuation studies
Study Main inclusion criteria Definition of relapse
TWISTERImatinib ≥ 3 yearsUndetectable MR4.5 ≥ 2 years
Detectable BCR-ABL1 on 2 consecutive tests or MMR loss
STIM2(Fi-LMC)
Imatinib ≥ 3 yearsUndetectable MR4.5 ≥ 2 years
At least 1 log increase in BCR-ABL1 or MMR loss
KIDImatinib ≥ 3 yearsUndetectable MR4.5 ≥ 2 years
MMR loss
ISAVImatinib ≥ 2 yearsUndetectable MR4 ≥ 18 months
Detectable BCR-ABL1 on 2 consecutive tests and MMR loss
STIM123Imatinib ≥ 3 yearsRM4.5 ≥ 2 years
MMR loss
EUROSKITKI ≥ 2 yearsMR4 ≥ 1 year
MMR loss
Ross et al. Blood. 2013;122(4):515-22. Mahon et al. Blood (ASH 2013): abstract 654.Lee et al. Haematologica. 2016;101(6):717-23.Mori et al. Am J Hematol. 2015;90(10):910-4.
Takahashi et al. Blood (ASH 2015): abstract 4035.Mahon et al. Blood (2016): abstract 787.
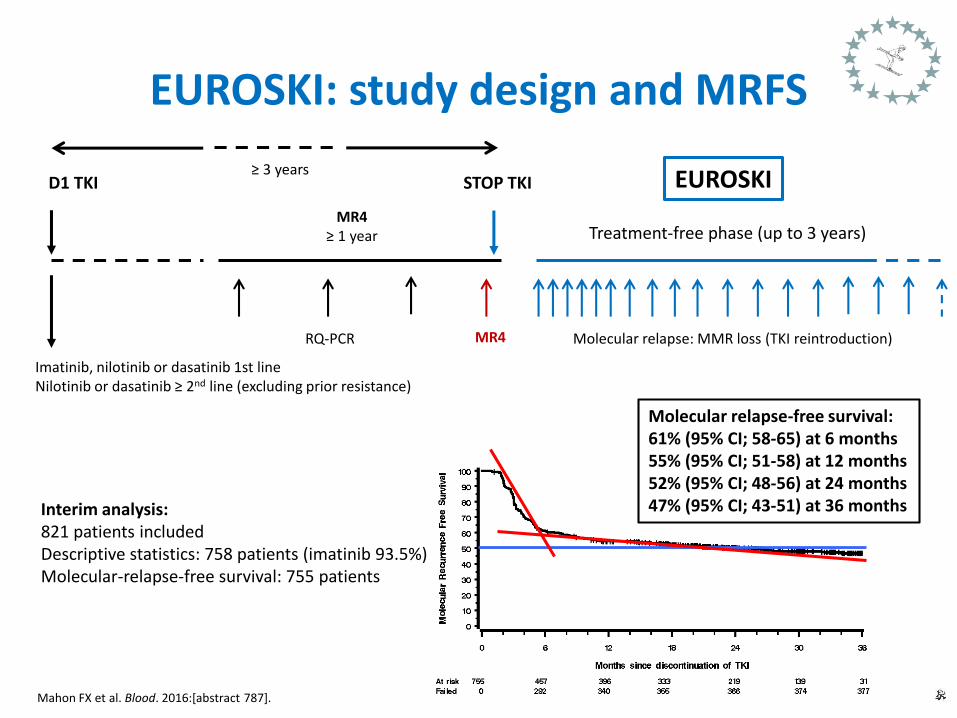
EUROSKI: study design and MRFS
D1 TKI
MR4≥ 1 year
RQ-PCR
STOP TKI
Treatment-free phase (up to 3 years)
EUROSKI≥ 3 years
Molecular relapse: MMR loss (TKI reintroduction)
Imatinib, nilotinib or dasatinib 1st lineNilotinib or dasatinib ≥ 2nd line (excluding prior resistance)
MR4
Interim analysis:821 patients includedDescriptive statistics: 758 patients (imatinib 93.5%)Molecular-relapse-free survival: 755 patients
Mahon FX et al. Blood. 2016:[abstract 787].
Molecular relapse-free survival: 61% (95% CI; 58-65) at 6 months55% (95% CI; 51-58) at 12 months52% (95% CI; 48-56) at 24 months47% (95% CI; 43-51) at 36 months
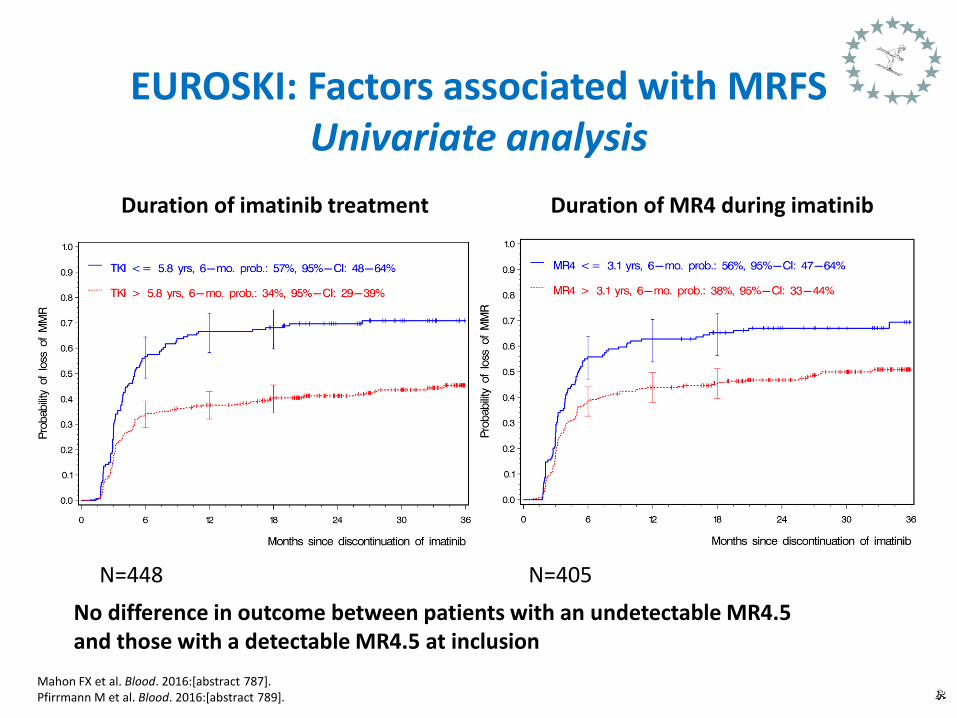
EUROSKI: Factors associated with MRFSUnivariate analysis
Mahon FX et al. Blood. 2016:[abstract 787].Pfirrmann M et al. Blood. 2016:[abstract 789].
N=448 N=405
Duration of imatinib treatment Duration of MR4 during imatinib
No difference in outcome between patients with an undetectable MR4.5and those with a detectable MR4.5 at inclusion
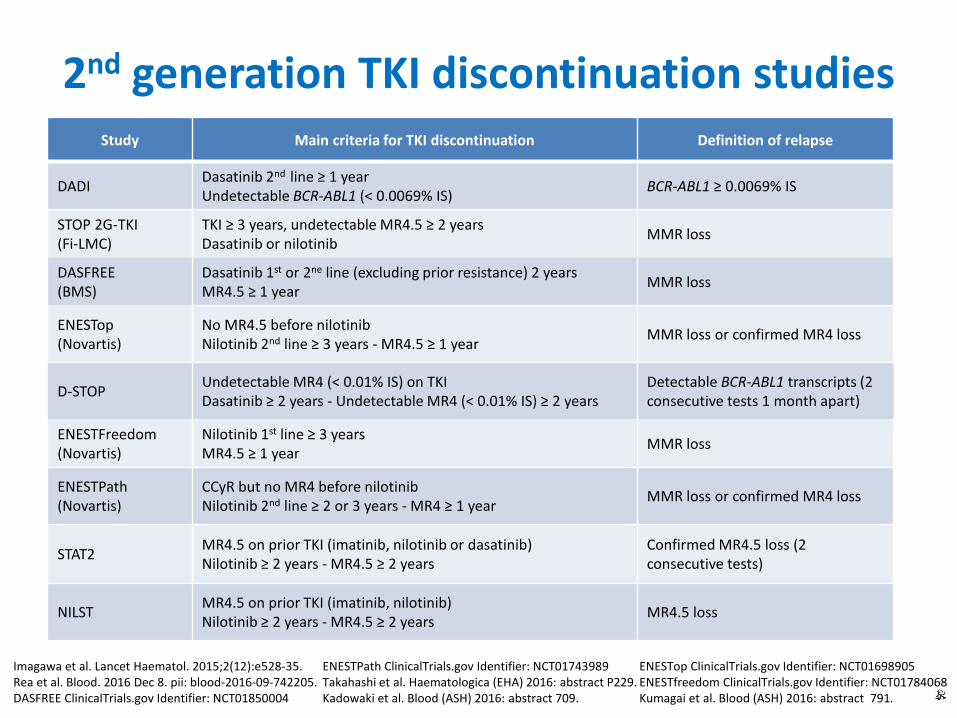
2nd generation TKI discontinuation studiesStudy Main criteria for TKI discontinuation Definition of relapse
DADIDasatinib 2nd line ≥ 1 yearUndetectable BCR-ABL1 (< 0.0069% IS)
BCR-ABL1 ≥ 0.0069% IS
STOP 2G-TKI(Fi-LMC)
TKI ≥ 3 years, undetectable MR4.5 ≥ 2 yearsDasatinib or nilotinib
MMR loss
DASFREE(BMS)
Dasatinib 1st or 2ne line (excluding prior resistance) 2 yearsMR4.5 ≥ 1 year
MMR loss
ENESTop(Novartis)
No MR4.5 before nilotinibNilotinib 2nd line ≥ 3 years - MR4.5 ≥ 1 year
MMR loss or confirmed MR4 loss
D-STOPUndetectable MR4 (< 0.01% IS) on TKIDasatinib ≥ 2 years - Undetectable MR4 (< 0.01% IS) ≥ 2 years
Detectable BCR-ABL1 transcripts (2 consecutive tests 1 month apart)
ENESTFreedom(Novartis)
Nilotinib 1st line ≥ 3 yearsMR4.5 ≥ 1 year
MMR loss
ENESTPath(Novartis)
CCyR but no MR4 before nilotinibNilotinib 2nd line ≥ 2 or 3 years - MR4 ≥ 1 year
MMR loss or confirmed MR4 loss
STAT2MR4.5 on prior TKI (imatinib, nilotinib or dasatinib)Nilotinib ≥ 2 years - MR4.5 ≥ 2 years
Confirmed MR4.5 loss (2 consecutive tests)
NILSTMR4.5 on prior TKI (imatinib, nilotinib)Nilotinib ≥ 2 years - MR4.5 ≥ 2 years
MR4.5 loss
Imagawa et al. Lancet Haematol. 2015;2(12):e528-35.Rea et al. Blood. 2016 Dec 8. pii: blood-2016-09-742205. DASFREE ClinicalTrials.gov Identifier: NCT01850004
ENESTop ClinicalTrials.gov Identifier: NCT01698905ENESTfreedom ClinicalTrials.gov Identifier: NCT01784068Kumagai et al. Blood (ASH) 2016: abstract 791.
ENESTPath ClinicalTrials.gov Identifier: NCT01743989Takahashi et al. Haematologica (EHA) 2016: abstract P229.Kadowaki et al. Blood (ASH) 2016: abstract 709.

STOP 2G-TKI study
STARTIMA
NILO or DASA uMR4.5DEEP MOLECULAR RESPONSE
(uMR4.5 for ≥ 2 y)
RQ-PCR uMR4.5 RQ-PCR (Molecular relapse: loss of MMR: 2G-TKI resumption)
STOP NILOor DASA
Treatment-free phase up to 5 years
STOP 2G-TKIIRB 00006477 Registration n°15-050
≥ 3 years
Rea et al. Blood. 2016 Dec 8. pii: blood-2016-09-742205. [Epub ahead of print]
Interim analysis:60 patients includedMinimum follow-up of 12 months (median 47, range: 12-65)Median duration of TKI: 76 months (36-153)
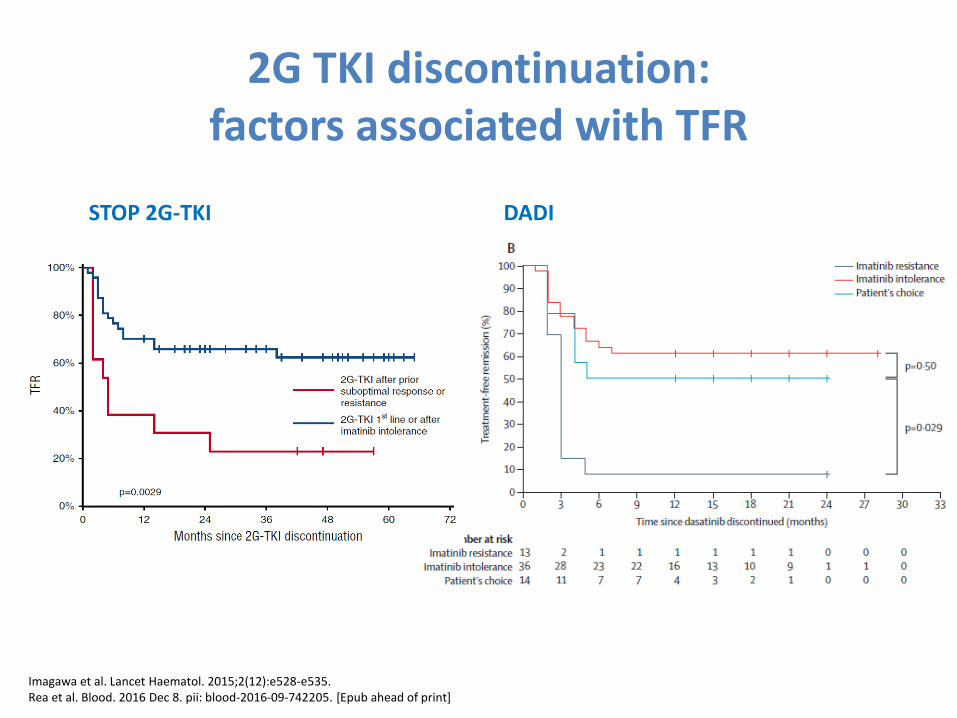
2G TKI discontinuation:factors associated with TFR
STOP 2G-TKI DADI
Imagawa et al. Lancet Haematol. 2015;2(12):e528-e535.Rea et al. Blood. 2016 Dec 8. pii: blood-2016-09-742205. [Epub ahead of print]
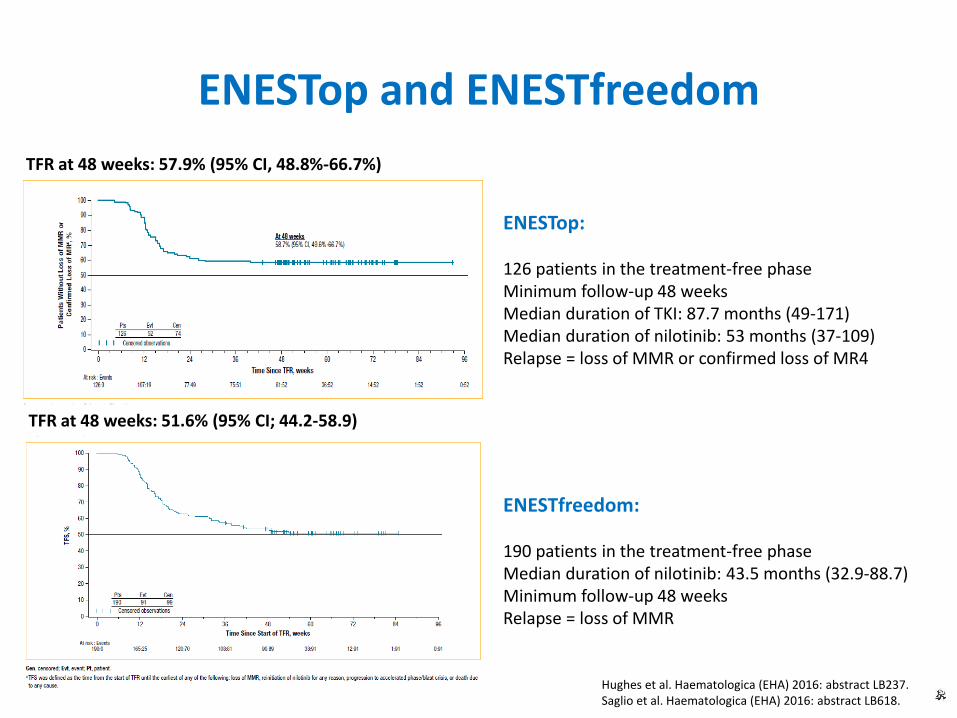
ENESTop and ENESTfreedom
Hughes et al. Haematologica (EHA) 2016: abstract LB237.Saglio et al. Haematologica (EHA) 2016: abstract LB618.
ENESTop:
126 patients in the treatment-free phaseMinimum follow-up 48 weeksMedian duration of TKI: 87.7 months (49-171)Median duration of nilotinib: 53 months (37-109)Relapse = loss of MMR or confirmed loss of MR4
ENESTfreedom:
190 patients in the treatment-free phaseMedian duration of nilotinib: 43.5 months (32.9-88.7)Minimum follow-up 48 weeksRelapse = loss of MMR
TFR at 48 weeks: 57.9% (95% CI, 48.8%-66.7%)
TFR at 48 weeks: 51.6% (95% CI; 44.2-58.9)
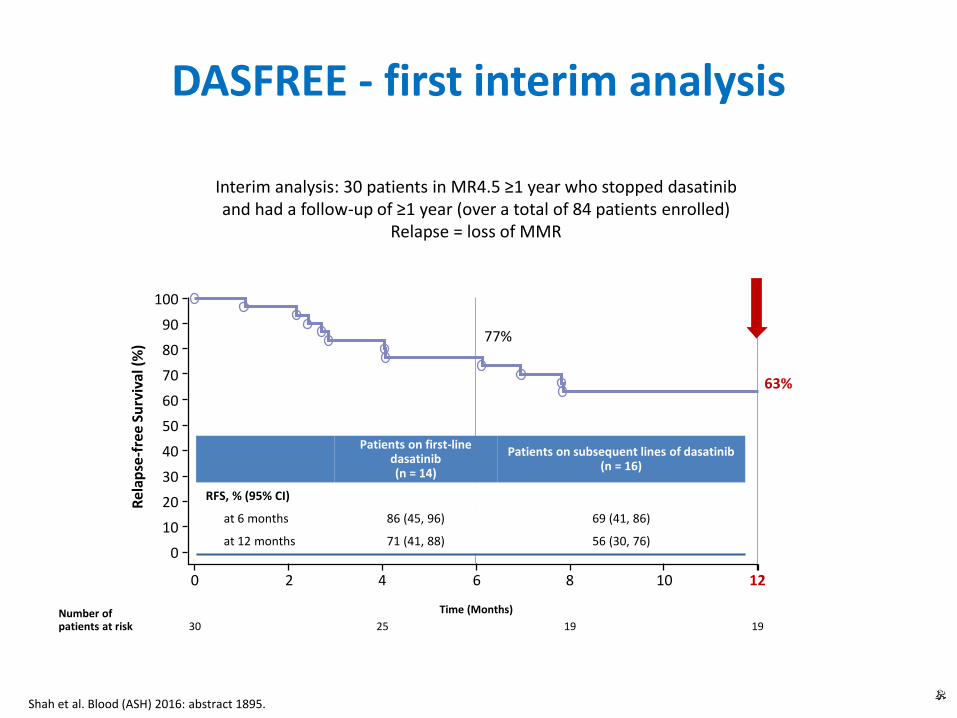
DASFREE - first interim analysis
Interim analysis: 30 patients in MR4.5 ≥1 year who stopped dasatiniband had a follow-up of ≥1 year (over a total of 84 patients enrolled)
Relapse = loss of MMR
Shah et al. Blood (ASH) 2016: abstract 1895.
1220 4 86 10
30 25 19 19Number of patients at risk
Rel
apse
-fre
e Su
rviv
al (
%)
Time (Months)
63%
0
10
20
30
40
50
60
70
80
90
100
77%
Patients on first-line dasatinib (n = 14)
Patients on subsequent lines of dasatinib(n = 16)
RFS, % (95% CI)
at 6 months 86 (45, 96) 69 (41, 86)
at 12 months 71 (41, 88) 56 (30, 76)
Attempting TFR: safety in clinical studies
• Resistance after resumption of the same TKI has not been reported yet with the exception of 1 case in ENESTstop.
• Blast crisis seems exceptional and has been reported in 1 case (sudden blast crisis after imatinib resumption in A-STIM).
• The “TKI withdrawal syndrome “ consisting in musculoskeletal pain and/or arthralgia soon after treatment discontinuation is frequent (~30% of patients) but benign and transient.
Hughes et al. Haematologica (EHA) 2016: abstract LB237.Rousselot et al. J Clin Oncol. 2014;32(5):424-30.Richter et al. J Clin Oncol. 2014; 32(25): 2821-23.Lee et al. Haematologica 2016; 101(6): 717-23.
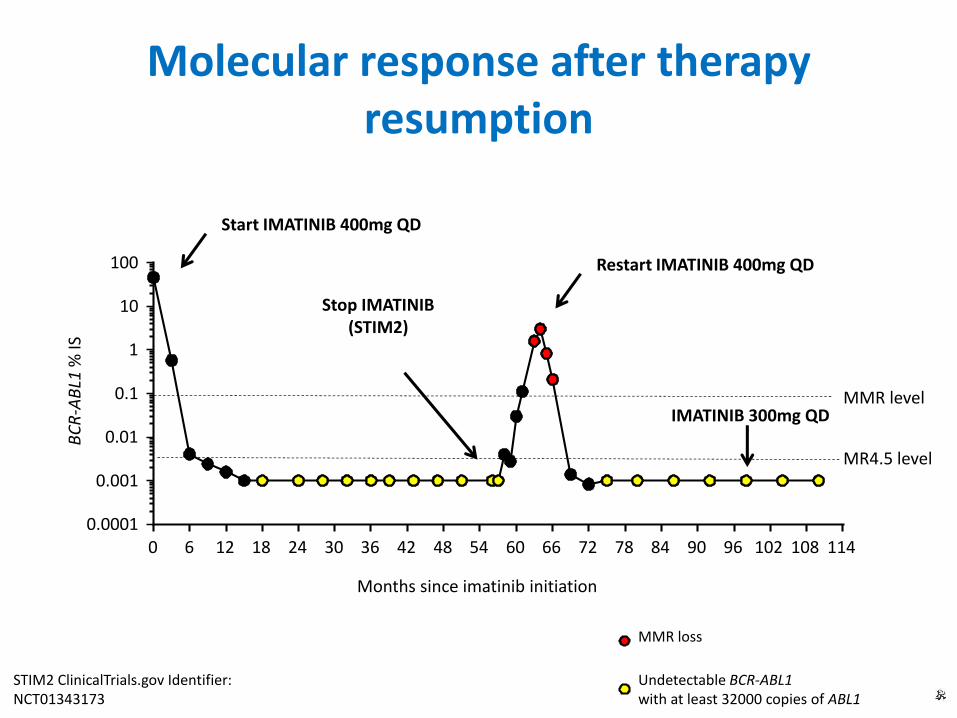
Molecular response after therapy resumption
0 6 12 18 24 30 36 42 48 54 60 66 72 78 84 90 96 102 108 1140.0001
0.001
0.01
0.1
1
10
100
Months since imatinib initiation
BC
R-A
BL1
% IS
Stop IMATINIB(STIM2)
Start IMATINIB 400mg QD
Restart IMATINIB 400mg QD
MMR level
MR4.5 level
Undetectable BCR-ABL1with at least 32000 copies of ABL1
STIM2 ClinicalTrials.gov Identifier:NCT01343173
MMR loss
IMATINIB 300mg QD
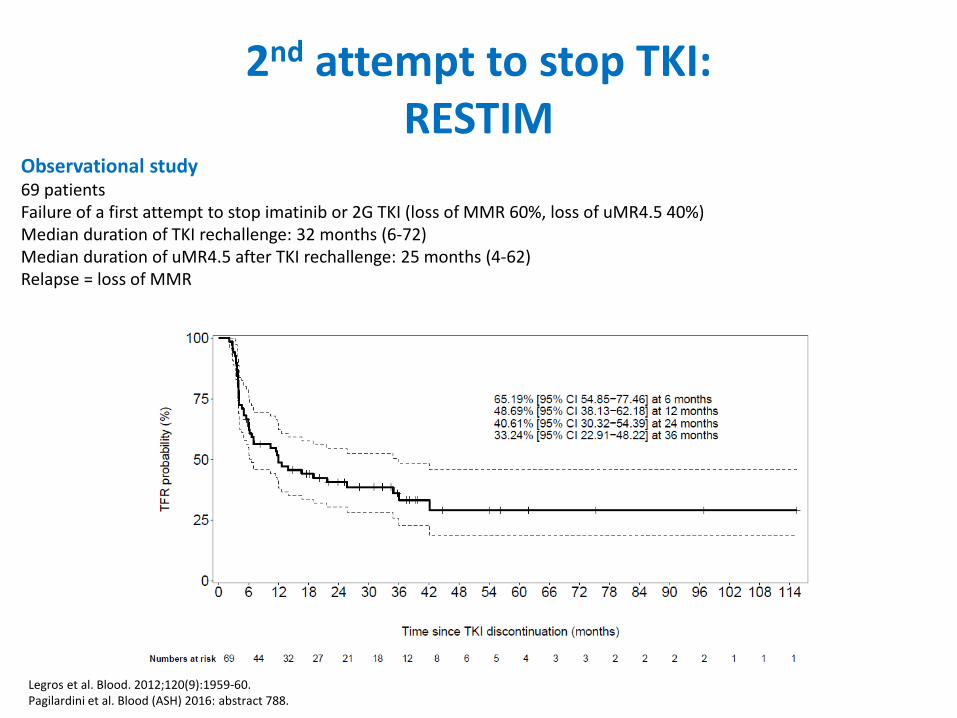
2nd attempt to stop TKI:RESTIM
Observational study69 patientsFailure of a first attempt to stop imatinib or 2G TKI (loss of MMR 60%, loss of uMR4.5 40%)Median duration of TKI rechallenge: 32 months (6-72)Median duration of uMR4.5 after TKI rechallenge: 25 months (4-62)Relapse = loss of MMR
Legros et al. Blood. 2012;120(9):1959-60.Pagilardini et al. Blood (ASH) 2016: abstract 788.
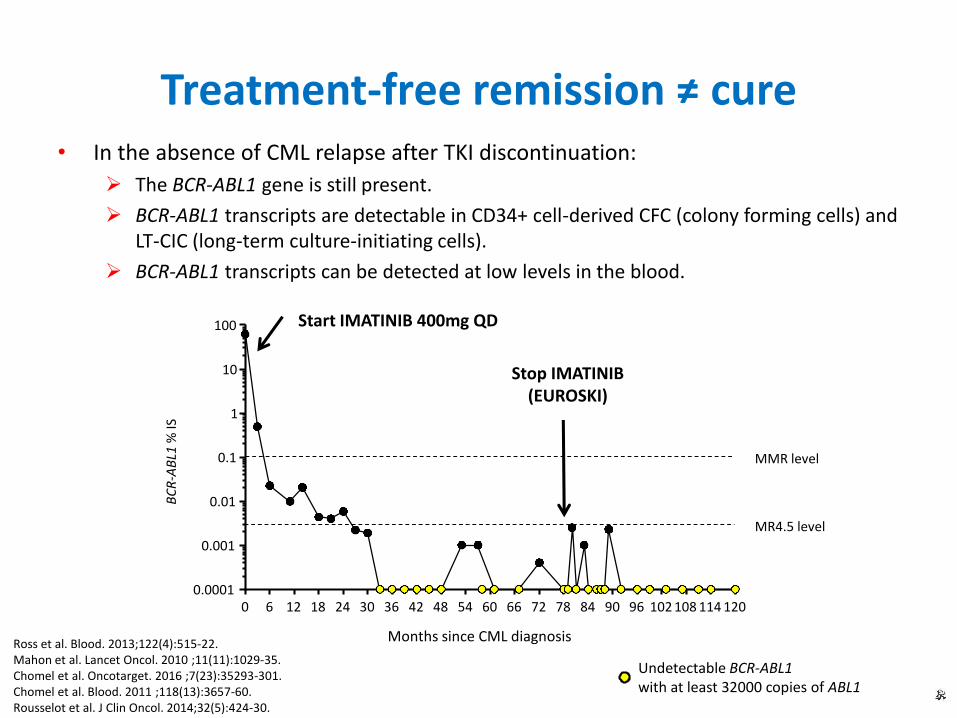
Treatment-free remission ≠ cure• In the absence of CML relapse after TKI discontinuation:
The BCR-ABL1 gene is still present.
BCR-ABL1 transcripts are detectable in CD34+ cell-derived CFC (colony forming cells) and LT-CIC (long-term culture-initiating cells).
BCR-ABL1 transcripts can be detected at low levels in the blood.
Ross et al. Blood. 2013;122(4):515-22.Mahon et al. Lancet Oncol. 2010 ;11(11):1029-35.Chomel et al. Oncotarget. 2016 ;7(23):35293-301.Chomel et al. Blood. 2011 ;118(13):3657-60. Rousselot et al. J Clin Oncol. 2014;32(5):424-30.
0 6 12 18 24 30 36 42 48 54 60 66 72 78 84 90 96 102 108 114 1200.0001
0.001
0.01
0.1
1
10
100
Months since CML diagnosis
Stop IMATINIB(EUROSKI)
Start IMATINIB 400mg QD
Undetectable BCR-ABL1with at least 32000 copies of ABL1
BC
R-A
BL1
% IS
MMR level
MR4.5 level

Reasons to aim at TFR in clinical practice
To avoid worrying side effects including those predisposing to other chronic diseases.
To get rid of low grade but chronic side effects.
To become free from daily constraints of medication intake.
Not to care anymore about drug-drug/food-drug interactions.
Fight against cost burden of targeted therapy borne by society or individuals.
Steegmann JL, et al. Leukemia. 2016;30(8):1648-1671.Rea D. Ann Hematol. 2015;94 Suppl 2:S149-158.Palani R, et al. Ann Hematol. 2015;94 Suppl 2:S167-176.Jiang Q, et al. J Cancer Res Clin Oncol. 2016;142(7):1539-1547.
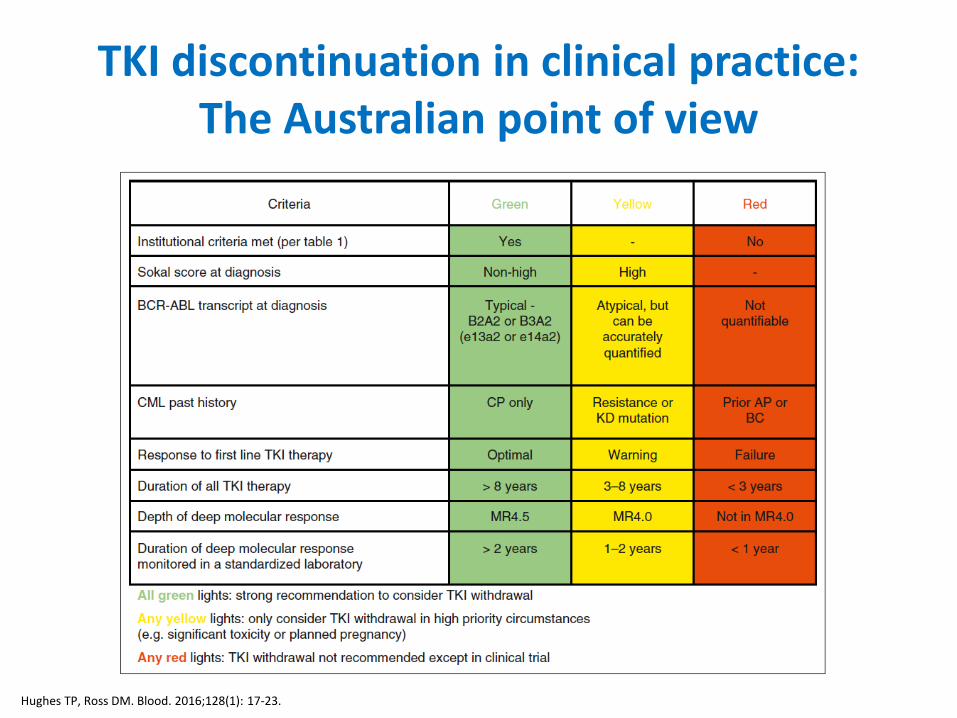
TKI discontinuation in clinical practice:The Australian point of view
Hughes TP, Ross DM. Blood. 2016;128(1): 17-23.
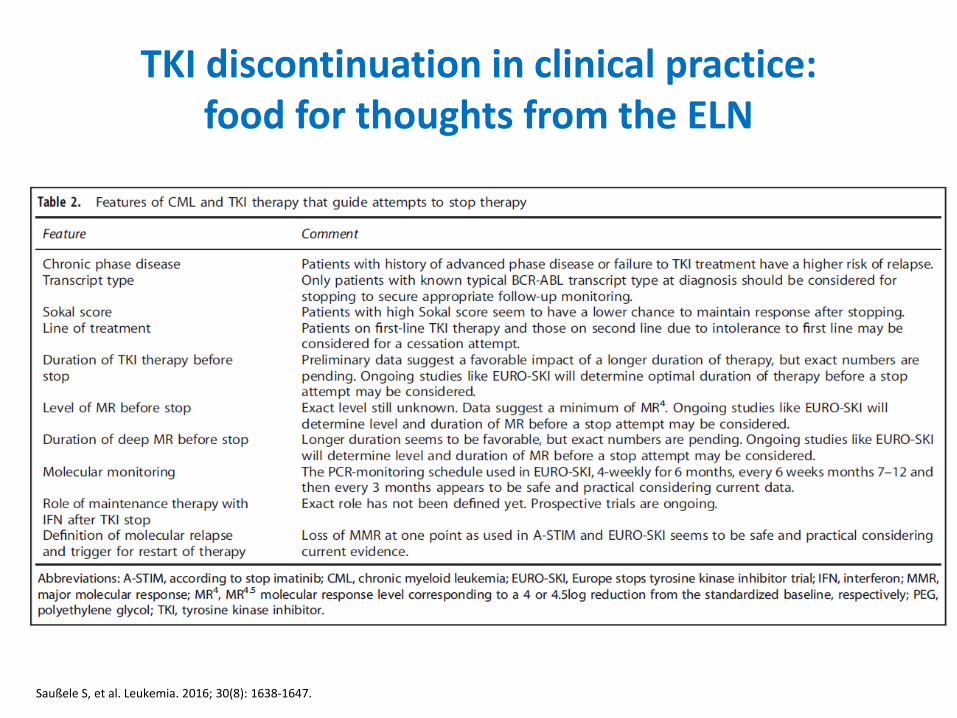
TKI discontinuation in clinical practice:food for thoughts from the ELN
Saußele S, et al. Leukemia. 2016; 30(8): 1638-1647.

Patient selection for TKI discontinuation in clinical practice: provisional choices of
the FiLMC
FAVORABLE CONDITIONS
≥18 years old at CML diagnosisCharacterized M-bcr transcriptsAny Sokal risk groupChronic phase First line imatinib for at least 5 yearsOptimal responseMR4.5 for at least 2 years
WITH CAUTION
First line dasatinib or nilotinibDasatinib or nilotinib 2nd or subsequent line due to prior intoleranceAll favorable conditions with the exception of type of TKI treatment
NOT RECOMMENDED IN CLINICAL PRACTICE
<18 years old at CML diagnosis (enroll patients in pediatric TFR studies)History of accelerated phase or blast crisisNon major-type bcr-abl or untyped transcriptsBosutinib and ponatinibHistory or suboptimal response or resistance or bcr-abl mutationTreatment duration less than 5 years, less than a MR4.5 or MR4.5 duration < 2 years

DASISION AND ENESTnd
Dasatinib100mg QD
N=259
Imatinib400mg QD
N=260
Nilotinib300mg BID
N=282
Imatinib400mg QD
N=283
Still on initial therapy
61% 63% 59.9% 49.8%
MMR by 5 years 76%* 42% 77%* 60%
MR4.5 by 5 years 42%* 33% 54%* 31%
On study AP/BC 4.6% 7.3% 10/282 21/283
5-year OS on study 91% 90% 93.7% 91.7%
5-year PFS on study 85%** 86%** 92.2%*** 91%***
**PFS: survival without loss of CHR, increase in Ph+ metaphases to ≥30% from nadir, AP/BC or death ***PFS: survival without AP/BC or death
*versus imatinib: statistically significant
Cortes et al. J Clin Oncol. 2016;34(20):2333-40.Hochhaus et al. Leukemia. 2016;30(5):1044-54.
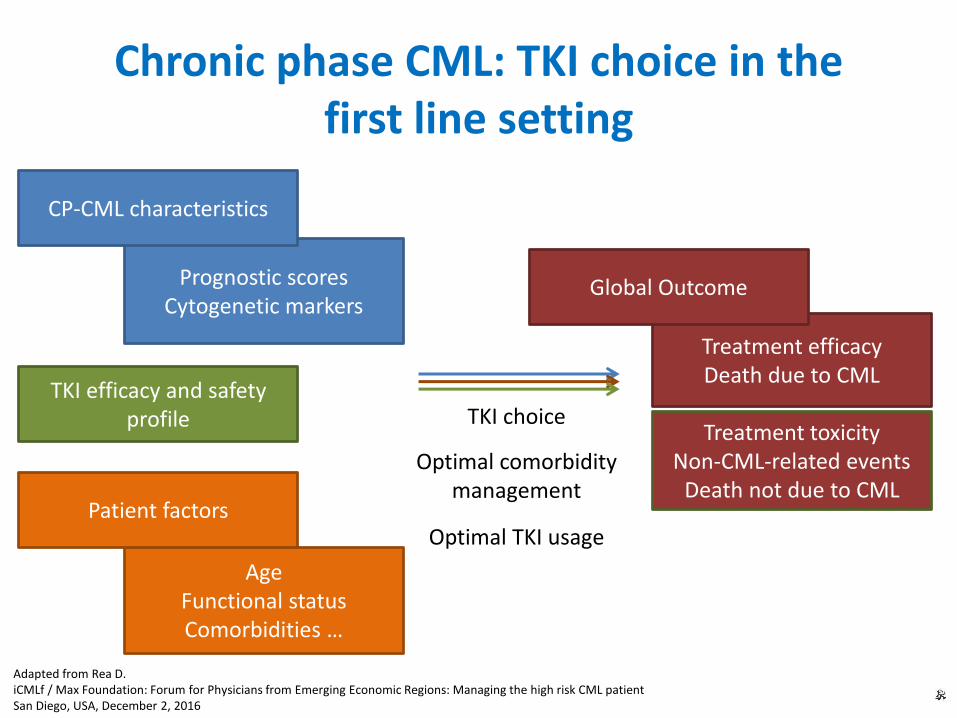
Prognostic scoresCytogenetic markers
Chronic phase CML: TKI choice in thefirst line setting
CP-CML characteristics
AgeFunctional statusComorbidities …
Patient factors
Treatment efficacyDeath due to CML
Global Outcome
TKI choiceTreatment toxicity
Non-CML-related eventsDeath not due to CML
Optimal comorbidity management
Adapted from Rea D. iCMLf / Max Foundation: Forum for Physicians from Emerging Economic Regions: Managing the high risk CML patientSan Diego, USA, December 2, 2016
TKI efficacy and safety profile
Optimal TKI usage
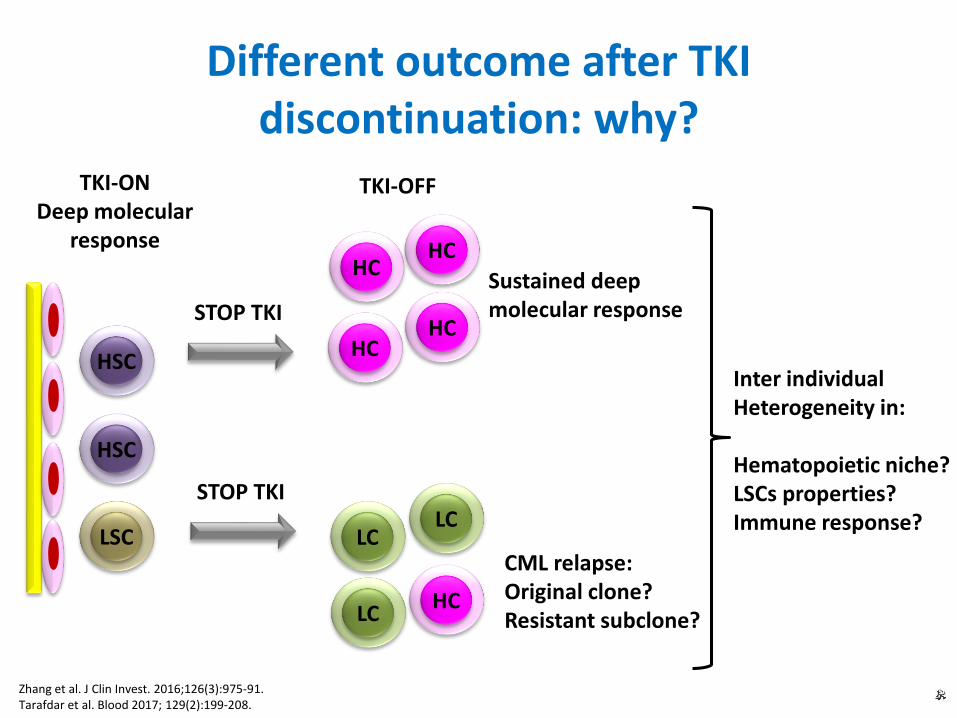
Different outcome after TKI discontinuation: why?
STOP TKI
TKI-ONDeep molecular
response
HSC
LSC
HSC
HC
LC
HC
HC
HC
LC
LC
HC
TKI-OFF
Sustained deepmolecular response
CML relapse:Original clone?Resistant subclone?
STOP TKI
Inter individualHeterogeneity in:
Hematopoietic niche?LSCs properties?Immune response?
Zhang et al. J Clin Invest. 2016;126(3):975-91.Tarafdar et al. Blood 2017; 129(2):199-208.
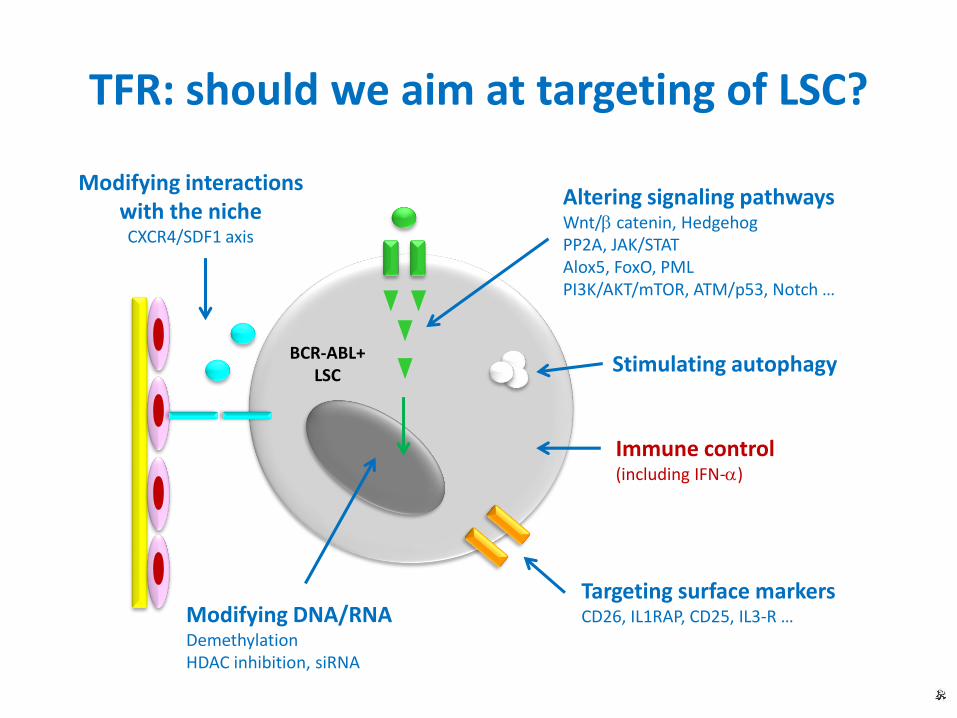
Altering signaling pathwaysWnt/b catenin, HedgehogPP2A, JAK/STATAlox5, FoxO, PMLPI3K/AKT/mTOR, ATM/p53, Notch …
Modifying DNA/RNADemethylationHDAC inhibition, siRNA
Targeting surface markersCD26, IL1RAP, CD25, IL3-R …
Modifying interactionswith the nicheCXCR4/SDF1 axis
Stimulating autophagy
Immune control(including IFN-a)
BCR-ABL+LSC
TFR: should we aim at targeting of LSC?
Conclusion and perspective
• Maximum protection from blast crisis remains an essential goal in CML management and requires an optimal response.
• TKI discontinuation may be successful in patients with deep and durable molecular responses but best pre requisite in terms of depth and duration of molecular response and duration of therapy are not completely known.
• Nevertheless, recommendations on attempting TFR in clinical practice will be provided soon by the ELN. The French CML group will also provide national recommendations.
• Further research is needed in order to better understand underlying mechanisms leading to treatment-free relapse and to increase access to TFR strategies.
TFR