status of newborn health in india and community-based newborn care framework of presentation global...
TRANSCRIPT

Status of Newborn Health in India and Community-based Newborn Care
Framework of presentation• Global status of newborns
• Causes of neonatal deaths
• Significance of newborn deaths
• Status of newborn in SEAR
• Status of newborn in India
• Determinants of newborn health
• Essential newborn care
• Community practices
• NFHS III findings on newborn care practices
• Example: Gadchiroli model
• GOI initiatives
• References

Global status of newborns• Perinatal and neonatal ill health in 2000 consisted of 7
million perinatal deaths (4 million still births and 3 million early neonatal deaths) and 1 million late neonatal deaths
• Globally burden of LBW infants- 16% of all births; while in developed countries (5-7%)
• Challenges in addition to this are bad practices in the community.
• Reductions in perinatal mortality • preventive care before pregnancy,
• improved ANC that includes birth plans and emergency preparedness,
• skilled attendance during childbirth and
• refocused postpartum care for the mother and the baby.


Significance of newborn deaths: IndiaSignificance of newborn deaths: India
Day Under 5 child deaths%
Day 1 20
Day 3 25
Day 7 37
Day 28 50
ICMR Data:2003

Status of Neonatal Health in SEAR
Sr. No.
Country NMR 2000 NMR 2004
1 Bangladesh 36 36
2 Bhutan 38 30
3 Democratic peoples of Korea
22 22
4 India 43 39
5 Indonesia 18 17
6 Maldives 37 24
7 Myanmar 49 49
8 Nepal 40 32
9 Shri Lanka 11 8
10 Thailand 13 9
11 Timor East 40 29
Source: www.who.int/whosis/database

Sr. no.
Type of mortality
Mortality rate
India Maharashtra
1 Neonatal mortality
39 31.8
2 Post Neonatal mortality rate
18 5.7
3 Pere natal mortality rate
48.5 35.8
4 Infant mortality rate
57 37.5
5 Child mortality rate
18 9.5
6 Under 5 mortality 74 46.7
Early Childhood Mortality Rates
Source: NFHS III 2005-06
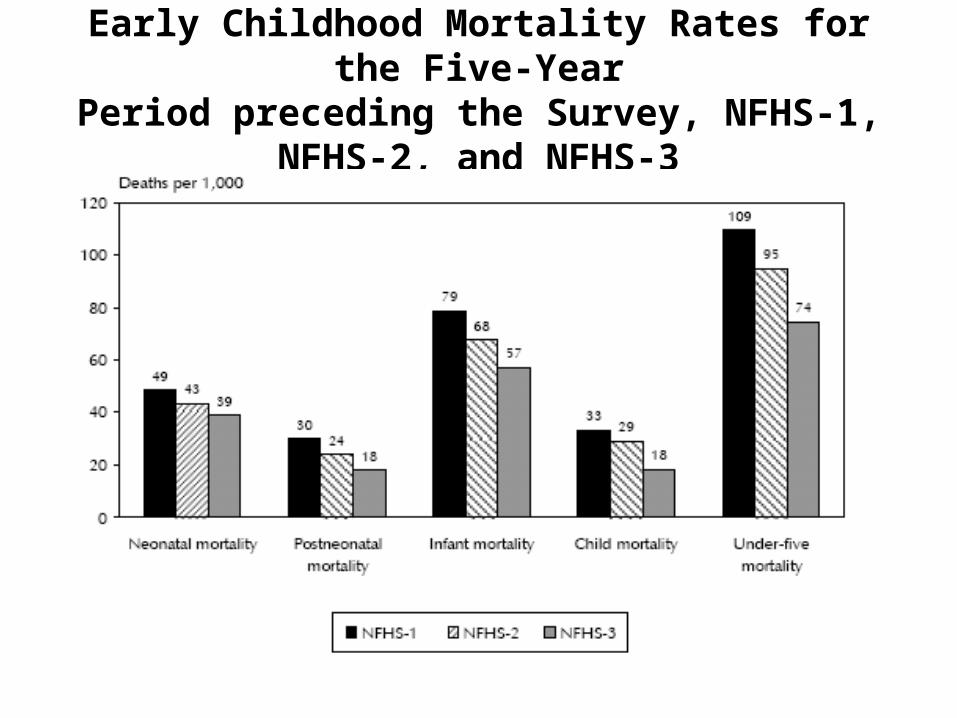
Early Childhood Mortality Rates for the Five-YearPeriod preceding the Survey, NFHS-1, NFHS-2, and
NFHS-3

Neonatal and post neonatal mortality Year preceding the survey Neonatal mortality Post neonatal mortality
Urban
0-4 28.5 13.0
5-9 35.9 18.8
10-14 34.6 18.1
Rural
0-4 42.5 19.7
5-9 53.9 24.2
10-14 57.5 28.1
Total
0-4 39.0 18.0
5-9 49.3 22.8
10-14 51.3 25.3
Neonatal mortality rate has decreased by 12 deaths per 1,000 live births (from 51 to 39), Post neonatal mortality rate has decreased by 7 deaths per 1,000 live births (from 25 to 18),
• In both the neonatal and post neonatal periods, mortality in rural areas is about 50 percent higher than mortality in urban areas.
• In the neonatal period, the decline in mortality was slightly faster in rural areas (26 percent) than in urban areas (18 percent).
• it is possible to stratify states and divisions –1. with very high (above 50/1000 NMR)
2. high (35-50/1000 NMR)
3. moderate (20-34/1000 NMR)
4. low (less than 20/1000 NMR

Socioeconomic Determinants Back ground characteristics Neonatal mortality Post neonatal mortality
Education of mother
No education 45.7 24.0
12th or more 19.6 6.3
Religion
Hindu 40.3 18.2
Muslim 34.1 18.2
Christian 31.5 10.1
Buddhist/neo Buddhist 43.0 9.8
Caste -SC 46.3 20.1
ST 39.9 22.3
OBC 38.3 18.3
Other 34.5 14.5
Wealth index-lowest 48.4 22.0
Middle 39.3 19.1
Highest 22.0 7.2

Demographic Determinants Demographic characteristics
Neonatal mortality Post neonatal mortality
Child’s sex
Male 33.0 10.7
Female 23.4 15.7
Mother’s age at birth
<20 30.5 13.8
20-29 28.4 12.6
Birth size
Very small 91.4 37.2
Small 42.1 19.8
Average or Larger 32.3 16.2
It was found that as the birth interval decreases , both neonatal and post neonatal mortality increases.While, it is less in first order child than the child having order more.
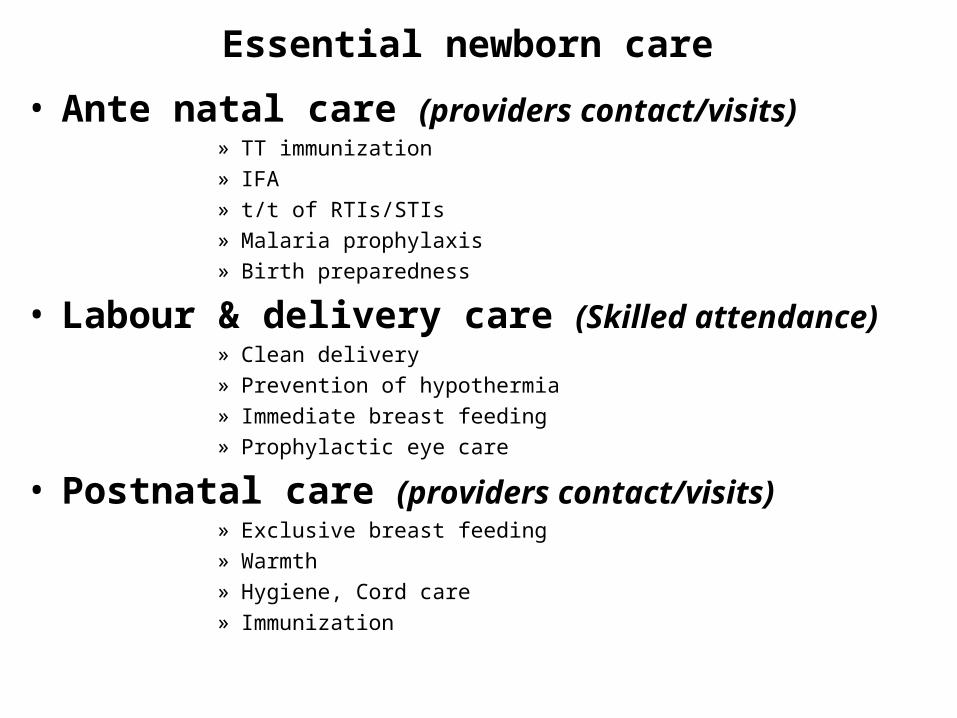
Essential newborn care
• Ante natal care (providers contact/visits)» TT immunization
» IFA
» t/t of RTIs/STIs
» Malaria prophylaxis
» Birth preparedness
• Labour & delivery care (Skilled attendance)» Clean delivery
» Prevention of hypothermia
» Immediate breast feeding
» Prophylactic eye care
• Postnatal care (providers contact/visits)» Exclusive breast feeding
» Warmth
» Hygiene, Cord care
» Immunization

Special care
Maternal and fetal complications
•Prevention of mother to child transmission of HIV
•M/M or referral of obstetrics & neonatal complications
Infection, malformation, and other problems
•Antibiotics
•Supportive care
•ART if in needReferral if necessary
Low birth weight•Special warmth , KMC
•Hygiene, Cord care
•Assisted feeding, if necessary
Birth Asphyxia•Resuscitation
•Post resuscitation care
•Referral if necessary

Intervention PackagesSkilled obstetric and immediate newborn care including resuscitation
Emergency obstetric care to manage complications such as obstructed labour and hemorrhage
Antibiotics for preterm rupture of membranes#
Corticosteroids for preterm labour#
Emergency newborn care for illness, especially sepsis management and care of very low birth weight babies
Clin
ical
ca
re
Folic acid #
Counseling and preparation for newborn care and breastfeeding, emergency preparedness
Healthy home care including breastfeeding promotion, hygienic cord/skin care, thermal care, promoting demand for quality care
Extra care of low birth weight babies
Case management for pneumonia
Fam
ily-c
omm
unity Clean home delivery
Simple early newborn care 15 - 32%
4-visit antenatal package including tetanus immunization,detection & management of syphilis, other infections, pre-eclampsia, etc
Malaria intermittent presumptive therapy*
Detection and treatment of bacteriuria#
Out
reac
h se
rvic
es
Postnatal care to support healthy practices
Early detection and referral of complications
6 - 9%
23 - 50%NMR effect
InfancyNeonatal periodPre- pregnancy PregnancyBirth

Ante natal check ups NFHS III
Type of Ante Natal care India MH
% of women had at least one ANC
76.4 90.8
% of women had ≥ 3 ANC 52.0 75.1
% of women received ≥ 2 TT injection during Pregnancy
76.3 85.1
% of women received 1 booster TT injection during 2nd or Pregnancy after 3 years or more yr
1.5 1.7
% women received IFA tabs 65.1 80.9
% of women consumed 90 or more IFA tabs
23.1 31.4

Timings of Post natal check ups NFHS IIIBack ground characteristics
Time between delivery & first Post natal check up %
No post natal check up
< 4 hrs 4-23 hrs 1-2 days 3-41 days
Urban 45.2 8.1 7.7 2.7 34.3
Rural 20.8 3.7 4.4 4.4 66.1
Type of health care provider for PNC
Residence Doctor ANM/ Nurse
Other health provider
TBA
Urban 53.0 8.1 0.2 2.3
Rural 20.9 7.8 0.8 3.4
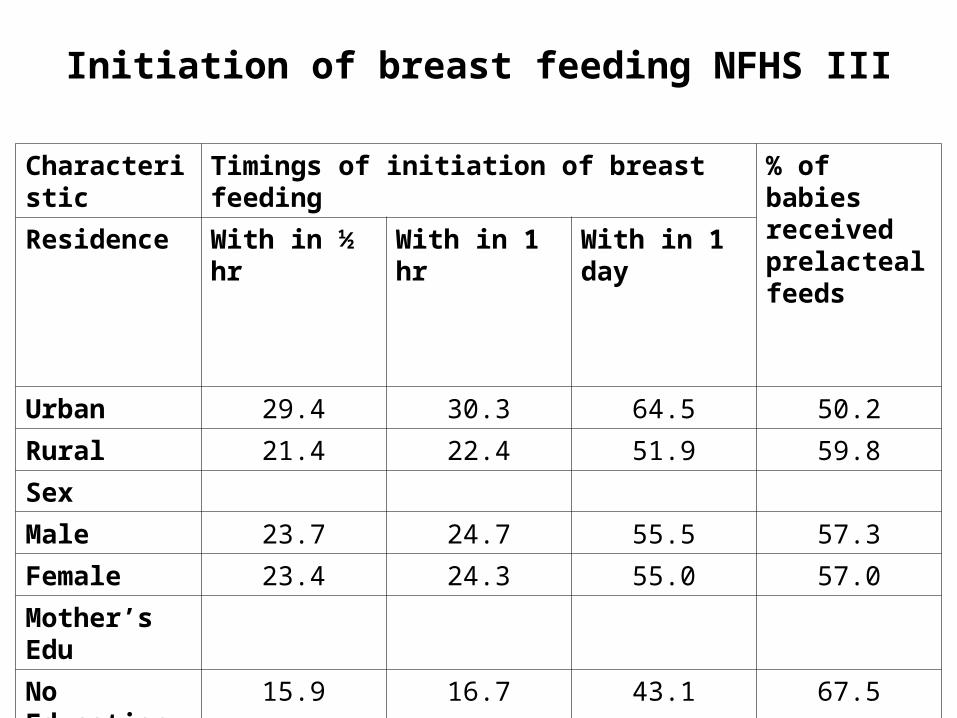
Initiation of breast feeding NFHS III
Characteristic Timings of initiation of breast feeding % of babies received prelacteal feeds
Residence With in ½ hr With in 1 hr With in 1 day
Urban 29.4 30.3 64.5 50.2
Rural 21.4 22.4 51.9 59.8
Sex
Male 23.7 24.7 55.5 57.3
Female 23.4 24.3 55.0 57.0
Mother’s Edu
No Education 15.9 16.7 43.1 67.5
≥ 12th std 33.5 34.6 71.6 43.4

Morbidity pattern NFHS III
Characteristic % ARI % fever % diarrhea % diarrhea with blood in
stool
Age < 6 months
6.2 11.6 10.6 0.2
Urban 5.1 14.0 8.9 0.6
Rural 6.0 15.1 9.0 1.0
Treatment sought
69.0 71.0 57.1 -

Do we have Solution ?
• A mix of community and facility-based interventions
• A mix of integrated child health approaches
• Integrated management of neonatal and child hood illnesses is proven tool

Evidence-based Interventions to Reduce Newborn Deaths
Infection36%
Sepsis/PneumoniaTetanusDiarrhea
Asphyxia23%
Other7%
Complications of Prematurity
27%
Cong. Anom
7%
Low birth weight is a significantcontributor in 40–70% of neonatal deaths.
Tetanus Toxoid Immunization of MotherClean DeliveryCord CareEarly & Exclusive BreastfeedingAntibiotics for mother and baby
Warming ResuscitationSkilled Birth Attendants
Syphilis Control Folate Supplementation
Adapted from Lancet 2005
Malaria ControlAntenatal CorticosteriodTreatment of Bacteriuria
Kangaroo Mother CareBirth SpacingMaternal Nutrition

0
20
40
60
80
100
1983 2000 1983 2000
Post-neonatal mortality
Late neonatal mortality
Early neonatal mortality
Developing Regions
Developed Regions
Source: RHR/WHO, 2003
Deaths among infants under 7 days are decreasing more slowly than among older infants
Goals of IMNCI
• Standardized case management of sick newborns and children
• Focus on the most common causes of mortality • Nutrition assessment and counselling for all sick
infants and children• Home care for newborns to
– promote exclusive breastfeeding– prevent hypothermia– improve illness recognition & timely care seeking
IMNCI-INDIA-Major Adaptations
• The entire 0-5 year period covered including the first week of life
• 50% of training time for management of young infants (0-2 months)
• The order of training reversed; now begins with management of young infants
• Reduced training duration (8 days), separate training materials for physicians & health workers
• Management now consistent with current policies of MoHFW, DWCD,IYCF,PD & NAMP
• Home-based care of young infants by health workers added
What does IMNCI not provide at all or fully
• Antenatal care
• Skilled birth attendance
• Birth asphyxia management
• Inpatient care modules for first level referral hospitals
A way forwards
• SBA is a newer strategy adopted by GOI in addition to IMNCI
• Inclusion of care at birth

Where to start?Build policy commitment & Develop a national strategy
• Interlinking the strategies to reduce neonatal mortality with related fields like Reproductive health, safe motherhood and child survival
Improve newborn health services & household practices
• Plan based on maternal and newborn health status, existing services, newborn care practices to be developed
Create demand of services
• As most of the deliveries are taking place at home so, research into attitudes and dynamics of decision making at family level to be considered and appropriate plan for corrective measures

Dahanu Experience 1987-90
• Under the Rural neonatal care project, started by Govt of Maharashtra, in Dahanu Block TBA played important role for caring the newborn
• Maintence of warm chain and resuscitation of newborn recognized as a most important intervention besides detection of LBW/ preterm baby and safe transport of such baby
• Foot length by foot print was used as indicator for referral
• Neonatal mortality rate dropped from 57.1 to 33.6
• Perinatal mortality rate dropped from 74.8 to 28.7
Conclusion: domiciliary neonatal care by TBAs supported by facilities for neonatal care at PHCs and community hospitals can influence neonatal survival in our country

Gadchiroli Newborn Case Study
• SEARCH introduced home-based neonatal care.
• VHW are trained –• provide prenatal care,
• resuscitate asphyxiated babies,
• prevent and treat hypothermia,
• support breastfeeding, and
• recognize and treat infections.
• TBA are given training and basic supplies (clean delivery kits, IFA pills, condoms).
• By the third year, there was a 62% decline in neonatal mortality, and significant declines in neonatal and maternal morbidities.
• RCH II is supporting this home-based model for rural communities.

Other studies
Bangladesh study:Effect of topical treatment with skin barrier-enhancing emollients on nosocomial
infections in preterm infants in Bangladesh: a randomized controlled trial
Use of sunflower oil or Aquaphor (petrolatum, mineral oil, mineral wax, lanolin alcohol daily for massage and found infants treated with sunflower seed oil were 41% less likely to develop nosocomial infections than controls
Lancet: Volume 365, Number 9464 19 March 2005
Nepal study:Randomized trial of the effect on birth weight of a daily multiple-micronutrient
supplement given to Nepalese women during pregnancy.
The investigators found an average increase in birth weight of 77 g and a 25% reduction in the rate of low birth weight compared with the controls who received iron and folate.
Lancet: Volume 365, Number 9463 12 March 2005