star substance treatment & recovery for dd clients
Post on 20-Dec-2015
214 views
TRANSCRIPT

STARSubstance Treatment &
RecoveryFor DD Clients
STARWhat Is it?
Chemical Dependency treatment within Seattle Mental Health, specifically for adults with developmental disabilities.
STARWho gets to be a STAR?
King County Resident Medicaid, DDD Enrolled (Department of
Developmental Disabilities)
Substance Abuse Issues 18 or older
Additional mental health services are available.

Definition of Developmental Disability A condition defined as mental retardation,
cerebral palsy, epilepsy, autism, or another neurological or other condition (functional impairments, IQ score) that originates before 18 years of age and is expected to continue indefinitely.
W.A.C. 388-823: Determination of a developmental disability (eligibility)
Barriers to Treatment Cognitive Delay
Poor communication/ interpersonal skills
Limited Peer network
Limited vocational skills
Restricted activities and exposure to world
Medical concerns
TIP 29 CSAT
We see what we expect
Misconceptions/Principles DD clients don’t use drugs
DD clients don’t have sex
DD clients don’t benefit from treatment
Maladaptive behavior rarely occurs alone and often the less difficult to manage behavior will be ignored.
The clinical interview alone is rarely diagnostic.
Reasons for use in DD clients Most behaviors are done for a good reason Acceptance into a social group Social control –operant conditioning Communication – attention, fear, love Modulation of pain Modulation of mood Addiction/dependence
How to Accommodate Simplification Language Activities Developmental Level Directive methods Flexible methods Involve others
Creating a Service Design Maximize safety Create and support positive self-view Social skill development Do not punish behaviors
Service Delivery Accommodation does not mean giving special preferences - it
does mean reducing barriers to equal participation in the program. People with coexisting disabilities are harmed by a provider's complicity in their avoidance of all challenges to chemical dependency.
Cross-training between CD treatment providers and agencies that work with people with disabilities, including vocational rehabilitation (VR), medical, and other professional specialists on specific disabilities, disability service providers, and disability education and advocacy organizations.
When treatment teams make the effort to accommodate individuals with coexisting disabilities, the quality of care improves for all clients.
All clients can get more out of treatment that is individualized.
Service Co-ordination Coordination with an agency providing case management services for people with
disabilities should be a priority if those services are not provided by the substance use disorder treatment program. People with both a substance use disorder and a coexisting disability may need assistance and individualized accommodations to:
Escape from abusive situations Learn to protect themselves from victimization Find volunteer work or other means of gaining a sense of productivity Develop prevocational skills such as basic grooming, dressing appropriately, using
public transportation, and cooking Learn social skills that may be missing because of both substance use disorders and
disability-related problems Learn to engage in healthy recreation Become educated about their legal rights to accessible environments and services as
well as employment Obtain financial benefits to which they are entitled Build new peer networks
TIP 29 CSAT
STARSTAR services include: Individualized stabilization services CD assessment CD treatment tailored to the client’s cognitive needs Access to a wide range of fun, informative groups &
therapeutic activities Team & Case Management Support Services (Guardians,
Parents, Care Providers, DDD CW, PCP) Clients with qualifying mental health issues will be offered
CNP (Community Networks Program) services - intensive case management
Psychiatric/Med management 24/7 Crisis Services

STAR Groups
Tuesday 12:00 PM BASKETBALL 2:00 PM POSITIVE LIFE 3:00 PM SOCCER
Wednesday 2:00 PM EDUCATION/SKILLS BUILDING
Thursday 1:00 PM BUTT OUT (Smoking Cessation) 2:00 PM EDUCATION/SKILLS BUILDING
Friday 10:00 AM MUSIC GROUP 11:00 AM DRAMA/ROLE PLAYING 1:00 PM BUTT OUT 2:00 PM SOCCER
Groups
Include the use of visual cues, mixed media Repetition of major points Expressive therapy, or the practice of using movement to
express feelings Role-playing works well for persons with developmental
disabilities-the process of playing a role themselves helps them to internalize it. (TIP 29 CSAT)
Games- ie. Recovery Pictionary, hangman Music BBQ’s – end of group cycle celebration - give each client a
responsibility Outings as rewards and as regular structured programming
ie. sports events, zoo, aquarium, IMAX films Art projects
Case Presentations Dolly (Patrick)
Eric (Norman)
Gordo (Julie)
Dolly Dolly: 44 y.o. female with long history of
drug/alcohol abuse and dependence. Mild MR with prevalent Axis II behavior issues. Mental Health dx is Bipolar I-Mixed.
Over 300 police contacts and about 160 or so arrests. Multiple infractions in different counties.
Drug of choice is marijuana, but also developed a taste for crack. Drinks moderate amounts of alcohol.
Dead Man Walking In jail on possession charges Released to streets Visits SMH and/or mom for money, clothes
etc Hits the streets, runs crack for dealers,
gets stoned Gets arrested for possession Loops over and over
Safety Legal Behavior Basic Needs/Self-Care Community Living/Recreational Interpersonal/Social Productivity Physical/Medical Family Emotional/Psychological Spiritual/Cultural Cognitive
STAR
Unique needs
Assessment changes (erik??)
Membership benefits
Underlying Affective Illness Affective Chemical due to Illness Dependency CD issues

The Underpinnings: Developmental abnormalities predispose to Affect Disorders and potential for Addiction. Normal Body and Brain Development is:
• Controlled by multiple systems “Attachment is the beginning.”(biological and social)
• Responsive to/dependent on experiences (which cannot happen with inadequate attachment chemistry
or inadequate caregiver)• Dependent on age/stage
• ( critical periods)• Modifiable throughout life ( neuroplastic)• Normally fluctuate in a healthy mixed mood or well modulated shifting mood
(bipolar pattern?) affected by circadian rhythm, seasonal variation. This becomes extreme with inadequate synapses +/- trauma in the Developmentally Disabled.
Drugs of abuse replicate positive attachment chemistry, but damage synapses further.
The most common damage is Bipolar Disorder.
There are critical times when negative experiences are more likely to have serious & sustained effects
Exposure to trauma, abuse, & neglect can interfere with brain development at any age, but most severe at younger ages.
Quality of care & security of attachment affect capacity for empathy, emotional regulation, & behavior control and therefore protect against the potential damage of poorly timed trauma.
Developmentally delayed individuals are often lacking in attachment related brain structure ( synaptic connectivity) and/or chemistry, therefore prone to attachment disorders, PTSD, and disinhibition.
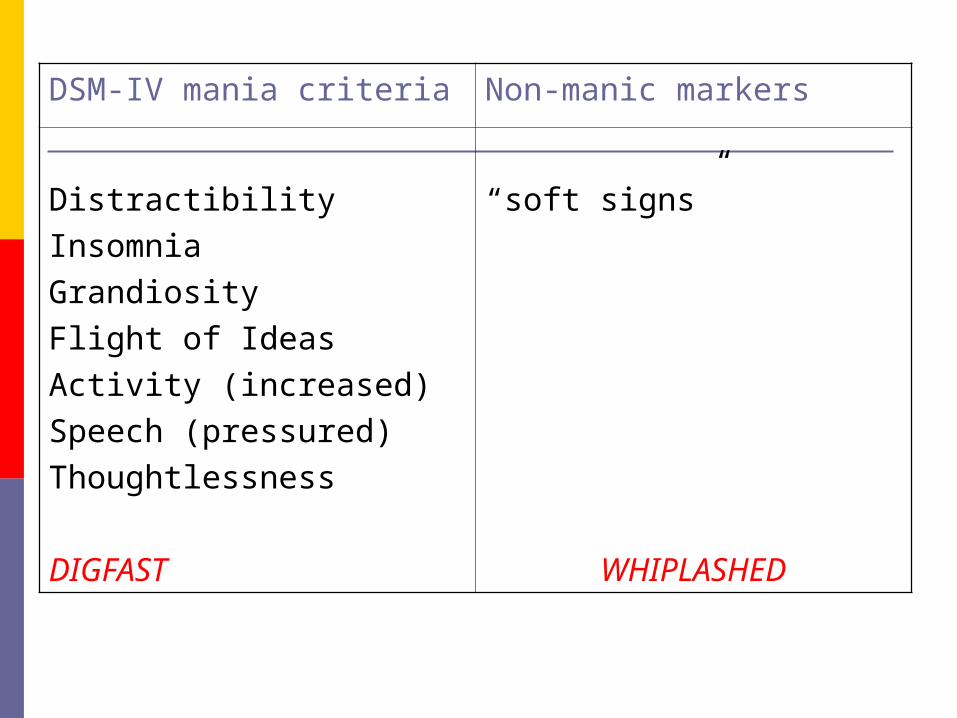
DSM-IV mania criteria Non-manic markers
DistractibilityInsomniaGrandiosityFlight of IdeasActivity (increased)Speech (pressured)Thoughtlessness
DIGFAST
“soft signs”
WHIPLASHED
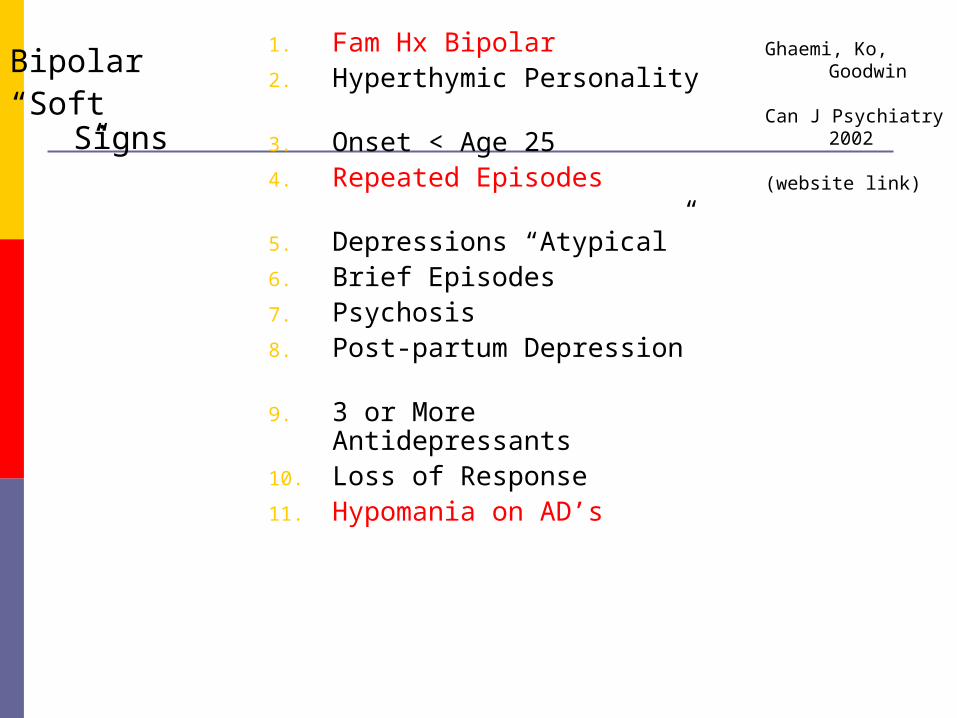
1. Fam Hx Bipolar2. Hyperthymic Personality
3. Onset < Age 254. Repeated Episodes
5. Depressions “Atypical”6. Brief Episodes7. Psychosis8. Post-partum Depression
9. 3 or More Antidepressants10. Loss of Response11. Hypomania on AD’s
Ghaemi, Ko, Goodwin
Can J Psychiatry 2002
(website link)
Bipolar“Soft
Signs”
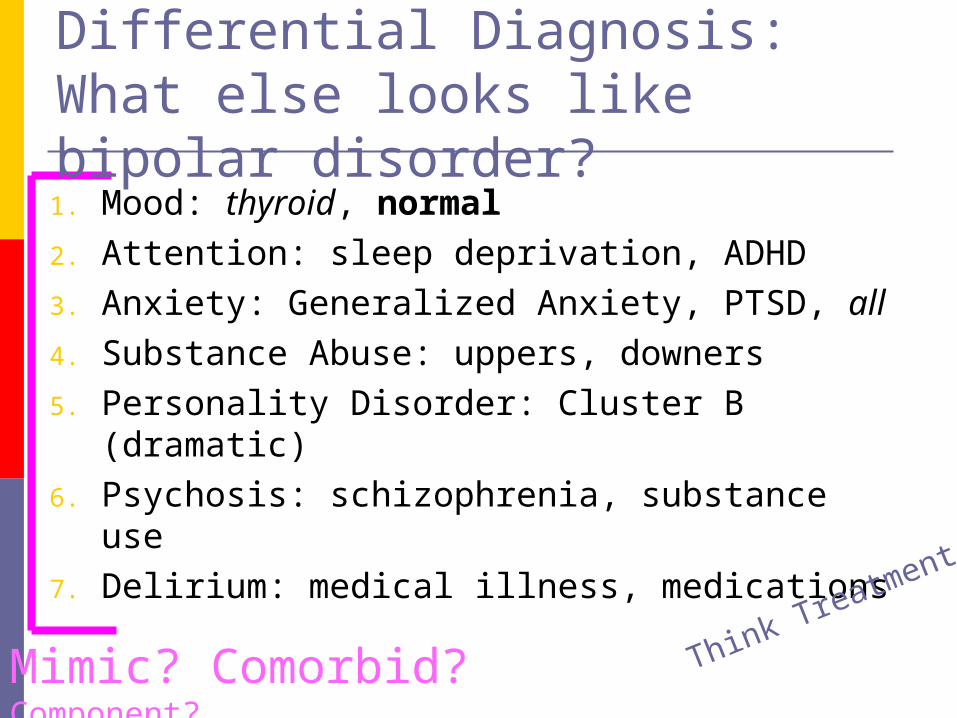
1. Mood: thyroid, normal2. Attention: sleep deprivation, ADHD3. Anxiety: Generalized Anxiety, PTSD, all4. Substance Abuse: uppers, downers5. Personality Disorder: Cluster B (dramatic) 6. Psychosis: schizophrenia, substance use7. Delirium: medical illness, medications
Differential Diagnosis:What else looks like bipolar disorder?
Think Treatment
Mimic? Comorbid? Component?
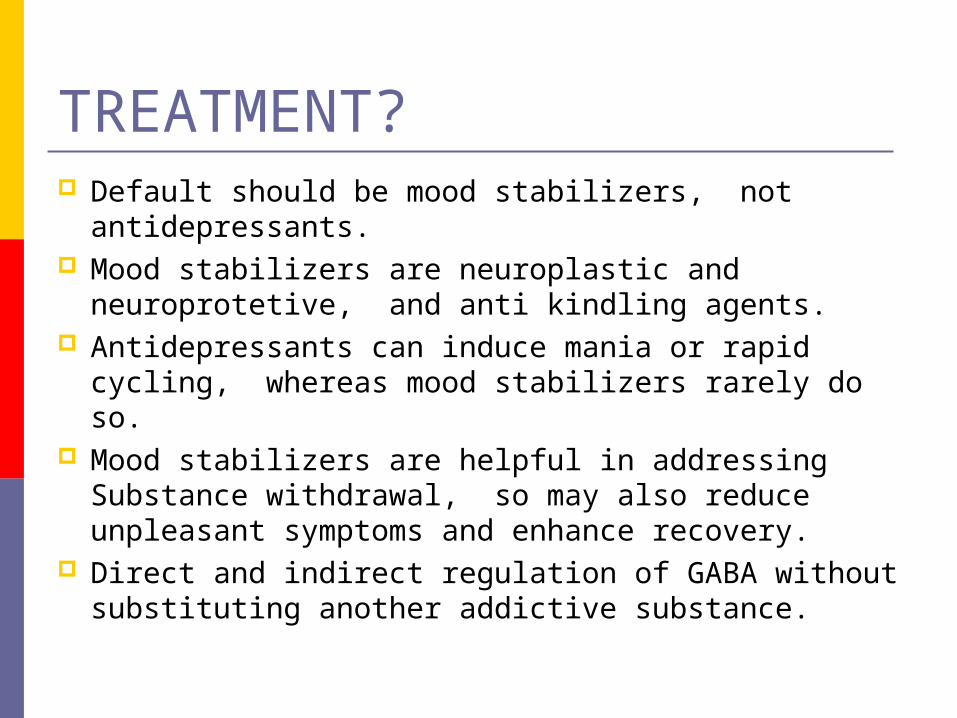
TREATMENT? Default should be mood stabilizers, not
antidepressants. Mood stabilizers are neuroplastic and
neuroprotetive, and anti kindling agents. Antidepressants can induce mania or rapid
cycling, whereas mood stabilizers rarely do so. Mood stabilizers are helpful in addressing
Substance withdrawal, so may also reduce unpleasant symptoms and enhance recovery.
Direct and indirect regulation of GABA without substituting another addictive substance.
STARContact Us
Schedule an intake:SMH Access/Admission’s office @ 206-302-2300.
2 SMH locations - Capital Hill & Tukwila
STAR assessment & enrollment will usually occur within a week.Urgent care is offered on an as needed basis.
In a crisis?SMH DD Crisis line at 1-888-435-7056 Client contact information will initiate a follow up within 72 hours.
If you would like to know more about STAR services please contact Rick Tabor at 206-302-2372 David O’Neal 206.302.2370