standards of accreditation in health
TRANSCRIPT

Standards of Accreditation in Health ODHS Kit – v2.2/2020

Standards of Accreditation in Health
ODHS Kit v2.2/2020
ISBN: 978-975-590-545-7
© Authors – General Directorate of Health Services
Department of Quality, Accreditation and Workers' Rights in Health
All publishing rights of this book is reserved by GDHS Department of Quality, Accreditation and Workers' Rights in Health. Excluding references not exceeding single page for promotion purposes, no part of this publication may be reproduced, distributed or transmitted without written permission of General Directorate in any form or by any means. Seperate publication rights of written knowledge in this book are reserved to their respective contributors.
Communication
Ministry of Health, Turkey
Directorate of Healthcare Services
Department of Quality, Accreditation and Workers' Rights in Health
e-mail:[email protected]
Web: www.kalite.saglik.gov.tr
Graphic Design Zeynep ASLAN – [email protected]
Published by

Authors
İrfan ŞENCAN, MD. Prof.
Doğan ÜNAL, MD. Prof.
Hasan GÜLER, MD. Physician,
Abdullah ÖZTÜRK, MD. Physician
Dilek TARHAN, MD. Sp.
Demet GÖKMEN KAVAK
Nurcan AZARKAN
İbrahim H.KAYRAL, PhD.
Ercan KOCA
Elif KESEN
Umut BEYLİK, PhD.
Süleyman Hafız KAPAN
İbrahim DOLUKÜP
Bayram DEMİR
Öznur ÖZEN
Çağlayan SARIOĞLAN
Emine YILDIZ
Şükriye Yüksel BAĞIRSAKÇI
Erol YALÇIN

IV
Department of Quality, Accreditation and Workers' Rights in Health
Study Group Members
• Uz. Abdullah Cüneyt BESLER, Diş Hekimi, İstanbul Eğitim ve AraştırmaHastanesi, İstanbul
• Dr. Abdullah ÖZTÜRK, Tıp Doktoru, S.B. SHGM Kalite ve AkreditasyonDaire Başkanlığı, Ankara
• Bayram DEMİR, Sosyolog, Batman İli Kamu Hastaneleri Birliği, Batman
• Çağlayan SARIOĞLAN, İletişim Uzmanı, S.B. SHGM Kalite veAkreditasyon Daire Başkanlığı, Ankara
• Demet GÖKMEN KAVAK, Sağlık Yönetimi Uzmanı, S.B. SHGM Kaliteve Akreditasyon Daire Başkanlığı, Ankara
• Uzm. Dr. Dilek TARHAN, Tıbbi Mikrobiyoloji ve Klinik MikrobiyolojiUzmanı, S.B. SHGM Kalite ve Akreditasyon Daire Başkanlığı, Ankara
• Elif KESEN, İşletme Yönetimi, S.B. SHGM Kalite ve Akreditasyon DaireBaşkanlığı, Ankara
• Dr. Elif TUNA, Tıp Doktoru, Manisa Turgutlu Devlet Hastanesi, Manisa
• Emine Elvan ÇİFTLİK, Tıp Doktoru, İstanbul Eğitim ve AraştırmaHastanesi, İstanbul
• Emine YILDIZ, Ebe, S.B. SHGM Kalite ve Akreditasyon Daire Başkanlığı,Ankara, Türkiye
• Ercan KOCA, Eczacı, S.B. SHGM Kalite ve Akreditasyon DaireBaşkanlığı, Ankara
• Erol YALÇIN, Yazılım Uzmanı, S.B. SHGM Kalite ve Akreditasyon DaireBaşkanlığı, Ankara
• Dr. Hasan GÜLER, Tıp Doktoru, S.B. Sağlık Hizmetleri Genel Müdürlüğü,Ankara
• İbrahim DOLUKÜP, Yazılım Uzmanı, S.B. SHGM İstatistik Analiz BilgiSistemleri Daire Başkanlığı, Ankara
• Dr. İbrahim H.KAYRAL, İşletme, S.B. SHGM Kalite ve AkreditasyonDaire Başkanlığı, Ankara
• Uzm. Dr. Kemal OKTAY, Genel Cerrahi Uzmanı, Başakşehir DevletHastanesi, İstanbul

V
Standards of Accreditation in Health - ODHS Kit
• Levent SONĞUR, Sağlık Fizikçisi, Van Bölge Eğitim AraştırmaHastanesi, Van
• Prof. Dr. M. Ali KILIÇARSLAN, Ankara Üniversitesi Diş HekimliğiFakültesi, Ankara
• Nurcan AZARKAN, Hemşire, S.B. SHGM Kalite ve Akreditasyon DaireBaşkanlığı, Ankara
• Öznur ÖZEN, Psikolog, S.B. SHGM Kalite ve Akreditasyon DaireBaşkanlığı, Ankara
• Seven KAZAN, Hemşire, Çanakkale ADSM, Çanakkale
• Süleyman DİLEK, Diş Hekimi, Adana İl Sağlık Müdürlüğü, Adana
• Süleyman Hafız KAPAN, Hukuk Müşaviri, S.B. SHGM Mevzuat İşleriDaire Başkanlığı, Ankara
• Tuncay KOYUNCU, Diş Hekimi, S.B. SHGM Teşhisle İlişkili GruplarDaire Başkanlığı, Ankara
• Umut BEYLİK, Mühendis, S.B. SHGM Kalite ve Akreditasyon DaireBaşkanlığı, Ankara
• Volkan SOZAN, Diş Hekimi, Sincan ADSM, Ankara
• Yunus YALÇIN, Diş Hekimi, Gümüşhane Şehit Ebe Kevser CeylanADSM, Gümüşhane

VI
Department of Quality, Accreditation and Workers' Rights in Health
Contributors
• Serpil GÜNER, Hemşire, Ankara Üniversitesi, Diş Hekimliği Fakültesi,Ankara
• Fatma ŞÜKRAN, Sağlık Bakım Hizmetleri Müdürü, İzmir Eğitim ADSH,İzmir
• Mehmet Sinan EVCİL, Diş Hekimi, İzmir Eğitim ADSH, İzmir
• Nükhet TANIŞAN, Kalite Yönetim Birimi Çalışanı, İzmir Eğitim ADSH,İzmir
• Özlem BÜYÜK, Hemşire İzmir Eğitim ADSH, İzmir
• Önder ÖNEY, Antalya ADSM, Antalya
• Nilüfer KURT, Diş Hekimi, Çanakkale ADSM, Çanakkale
• Sultan DURKAN, Sincan ADSM, Ankara
• Ümmühan DİLDAROĞLU, Sincan ADSM, Ankara
• Ünal BAYDAR, Kalite Yönetim Direktörü, Şehit Ebe Kevser CeylanADSM, Gümüşhane

VII
Standards of Accreditation in Health - ODHS Kit
Acknowledgement
SAS ODHS Study Group, various public institutions, ODHCs (public, private, university), specialist and occupational associations, health managers, health employees, academics, patient rights officers who contribute to preparation of SAS ODHS standards were asked for their opinions. Obtained feedback and suggestions via Opinion and Suggestion Platform have been evaluated during studies.
We thank to all Public Institutions, Private Health Institutions, Universities, Civil Public Associations, other institutional stakeholders and personal stakeholders who believes in quality in health by heart.
Department of Quality, Accreditation and Workers' Rights in Health


IX
Standards of Accreditation in Health - ODHS Kit
CONTENTS
PROLOGUE .............................................................. 1Introduction ..........................................................................3
Standards of Accreditation in Health ODHS Set (SAS ODHS) .......5
STANDARDS and GUIDES ...................................... 15
Management and Organization ...................................37Organizational Structure ......................................................39
Core Policies and Ethical Values .........................................43
Quality Management Structure ...........................................46
Document Management .....................................................49
Adverse Event Reporting System .......................................54
Risk Management ..............................................................57
Training Management .........................................................60
Social Responsibility ..........................................................64
Institutional Communication ...............................................66
Performance Measurement and Quality Improvement .....69Monitoring of Indicators .....................................................71
Healthy Work Life ............................................................75Human Resources Management .........................................77
Employee Health and Safety ................................................83
Patient Experience ...........................................................87Basic Patient Rights ...........................................................89Patient Safety ......................................................................93Patient Feedback ................................................................95Access to Service ...............................................................97

X
Department of Quality, Accreditation and Workers' Rights in Health
Health Services .............................................................101Prevention of Infections .....................................................103
Sterilization Management ..................................................113
Medicine Management ......................................................117
Patient Care .....................................................................123
Radiation Safety ...............................................................141
Prosthesis Laboratory Services .........................................145
Surgical Safety .................................................................154
Support Services ..........................................................163Accommodation Services .................................................165
Facility Management ........................................................174
Waste Management .........................................................177
Information Management ..................................................180
Material and Device Management .....................................183
Outsourcing ......................................................................187
Emergency Management ..............................................189Emergency Management ...................................................191
DEFINITIONS AND ABBREVATIONS ....................... 201
REFERENCES ....................................................... 213
RELEVANT LEGİSLATİONS OF STANDARDS ......... 223
ANNEX ................................................................. 231

PROLOGUE


3
Introduction
Nowadays, rapid advances in medical technology and applications have brought significant changes in physical and functional construction of the health services.
Emerging success rates of diagnosis and treatment applications, corresponding increases in number of patients and patient beds turnover, people being more careful about health of themselves and their families can be listed as the cause of the physical and functional changes.
These changes affect structural, administrative and designative practices of hospitals and emphasize the need to provide quality health care for patients who need medical care as soon as possible.
So far, a few patient and organizational structure focused accreditation systems have been established for the purpose of development of patient care in the world at an optimal level of quality, creation of a safe patient care environment, minimizing risks concerning patients and employees, a number of quality improvement and patient safety, and performance of healthcare institutions started to be evaluated within these systems.
In Republic of Turkey, foundations of accreditation have been laid in 2005 with the quality of healthcare evaluations and service standards of evaluations have been determined. These standards which are developed over time in the terms of number and structure have been implemented in four different versions. By 2013, standards got restructured in the terms of four basic principles of accreditation and ten goals, and the fifth version has been finalized with the name of "Standards of Accreditation in Health ODHS Kit".
This set prepared for Oral and Dental Health Services have two sections and consists of Standards, Assessment Criteria and Guides.

Department of Quality, Accreditation and Workers' Rights in Health
In the first part, historical development process and general information about the accreditation standards have been demonstrated. The second part includes guides which consists of Standard Requirements that will help understanding and implementing standards and assessment criteria. SAS-ODHS Kit which contains basic information about accreditation process and requirements for becoming accredited is presented for the benefit of ODHCs and all stakeholders to improve the quality of health care. With the establishment of national accreditation structure in the axis of Standards of Accreditation in Health, three main elements of Transformation of Health Program has been completed. Developed quality of health structure specific for Republic of Turkey consists of two parts: » Turkey Health Quality System» Turkey Health Accreditation SystemTurkey Health Quality System: The system is created by the Ministry of Health to raise the quality of health services in our country to the highest level within the scope of Health Transformation Program and to ensure patient and employee safety and patient and employee satisfaction. The system is mandatory for all public and private healthcare organizations in the 1st, 2nd and 3rd level in our country. Turkey Health Accreditation System: It is a system based on SAS, which health care organizations will apply on a voluntary basis and become accredited according to their success. Accreditation of Health System is a program that will be applied to, for organizations that want to go beyond the current national quality state and put forth the difference in their quality level. It’s organized as incentive for domestic and overseas health tourism because of including a document approved internationally. In Turkey, this structure which is established in the field of health quality by Ministry of Health has significant importance for rising on a sturdy foundation in the framework of an awareness of a service that continuously improves and is sustainable. Standards of Accreditation in Health-ODHS aim to set success goals that will make sure the standards are met firstly in oral and dental health services. Within this context, the standard set has been prepared according to all oral and dental health centers, clinics, policlinics, oral and dental hospitals and university dental hospitals. The statement as "oral and dental health centers" written in the set includes all of these institutions.
4
Prologue

5
Standards of Accreditation in Health ODHS Set (SAS ODHS)
Development of Standards
Work on accreditation in health conducted within the Ministry in Turkey stretches back to the year 2003 and concepts of quality and accreditation have been among the priorities of the health policy with the principles determined within the scope of Health Transformation Program.
In the Health Transformation Program, emphasis is put on the planning and supervising roles of the Ministry of Health, that is on a Ministry structure and practice that determine the standards of service, set rules, and supervise the framework of practices and the level of implementation of these standards. The accreditation system is established with the principle of “quality and accreditation for quality and effective health services” contained in the sixth component of the programme.
On the basis of the necessity of quality studies having international identity, first steps have been taken for establishment of the Health Accreditation System in Turkey in May, 2012. As a result of studies official co-operation have been initiated by negotiations with ISQua-the accreditor of accreditors on 20.03.2013. In the framework of negotiations and the agreement signed with ISQua, “ISQua International Principles for Healthcare Standards” have been analyzed in detail. On the basis of Decree Law No. 669, Standards of Accreditation in Health (SAS) are prepared by the Ministry of Health. Doing surveys and giving the certificate of accreditation for voluntary organizations is carried out by Institute of Turkey Quality and Accreditation in Health (TUSKA), which is established within the body of Turkish Health Institutes Presidency (TUSEB), on the basis of SAS.
ODHS Kit of Standards of Accreditation in Health is prepared considering international and national quality studies, principles of World Health Organization and ISQua. (Appendix: Information Note) This kit has been created taking into account international developments, coverage of all

Department of Quality, Accreditation and Workers' Rights in Health
service sections and compability for teleological interpretation. Also properties such as service and outcome-oriented approach, encouraging innovation in organizations, highlighting of applicability, being easy to use and inclusive were considered.
Objective and Scope of Standards of Accreditation in Health ODHS Standards of Accreditation in Health have been structured in line with minimum risk, optimum quality and maximum safety principles within the framework of the principles of World Health Organization and ISQua which are patient safety, quality improvement, patient and service user-orientedness, institutional planning and performance in the field of quality in health.
Standards of Accreditation in Health-ODHS aim to set success goals that will make sure the standards are met firstly in oral and dental health services. Within this context, the standard set has been prepared according to all oral and dental health centers clinics, policlinics, oral and dental hospitals and university dental hospitals. The statement as "oral and dental health centers" written in the set includes all of these institutions.
Goals of Standards of Accreditation in Health Standards of Accreditation in Health ODHS Set has been developed by taking into account patient safety goals of WHO, principles of ISQua, accreditation programs conducted across the world and needs and priorities of our country with a view to ensuring quality in oral and dental health centers and in order to achieve quality goals contained in the figure below.
6
Patient Safety
Equity Patient Orientedness
Timeliness Healthy Work Life
Suitability
Quality Goals
Continuity
Productivity Effectiveness
Efficiency
Prologue

Prologue
7
Standards of Accreditation in Health - ODHS Kit
In order to be able to say that service provided in oral and dental health centers is of quality, these centers must achieve the above mentioned goals.
These goals can be handled in two categories in general. The goals in the first category are organizational goals that relate to service delivery mode of the institution in other words how the institution puts forwards its services. (Effectiveness, Efficiency, Productivity and Healthy Work Life).
The goals contained in the second category concern those that get service from the institution directly. (Patient Safety, Equity, Patient-Orientedness, Suitability, Timeliness, Continuity).
The categorization is aimed at putting forth the goals in a clear manner. For example, in an institution where there is no healthy work environment, it will not be possible to ensure patient-orientedness. There is no priority relationship between the goals that have been mentioned and the fact that these goals are achieved in compliance with one another is a point that is emphasized by Standards of Accreditation in Health.
The definitions of SAS goals can be found below:
» Effectiveness: The criterion used to achieve the planned goal.
» Efficiency: The ability to do the work in a proper manner.
» Productivity: The relation between the amount of service that isgenerated and the input used to generate these services. It meansachieving the goals by using the least amount of resources.
» Healthy Work Life: Ensuring an ideal and safe work environment andinfrastructure for health professionals.
» Patient Safety: Measures and improvement activities undertakento keep all the foreseeable dangers that may cause harm to thestakeholders that get service on an acceptable risk level.
» Equity: All of the service units of the institutions ensuring that thosegetting service benefit from equal rights based only on their care andtreatment needs regardless of any other difference.
» Patient-Orientedness: Ensuring active participation of the patient inthe services related to diagnosis, treatment and care by taking theirwishes, needs, expectations and values into consideration.

Prologue
8
Department of Quality, Accreditation and Workers' Rights in Health
» Suitability: The health of the person benefiting from the medicalprocedures and processes to be conducted rather than being harmed.
» Timeliness: Providing the services regarding diagnosis, treatmentand care in the most appropriate and acceptable time interval in linewith the needs of the patient.
» Continuity: Ensuring the continuity of medical services in achronological and interdisciplinary manner after the treatment iscompleted.
Structure of Standards of Accreditation in Health ODHS Set
Standards of Accreditation in Health consist of 7 aspects, 30 Chapters, 49 Standards, 189 assessment criteria.
SAS ODHS Set is composed of Standards, Assessment Criteria and the guidelines related to them. In the guidelines there are the objectives, goals and Standard requirements of the Standards. Standards, assessment criteria and the relevant guidelines must be handled as a whole and implemented as such.
Aspects of Standards of Accreditation in Health ODHS
7 aspects that are contained in Standards of Accreditation in Health ODHS Set are as follows:
» Management and Organization
» Performance Measurement and Quality Improvement
» Healthy Work Life
» Patient Experience
» Healthcare Services
» Support Services
» Emergency Management
General Objectives and Scope of the Aspects
Aspects contained in Standards of Accreditation ODHS were determined based on the service provided at ODHS, executive activities and people involved in the service process in such a way as to encompass all the units of the institution.

Prologue
9
Standards of Accreditation in Health - ODHS Kit
» Management and Organization
Under this aspect, it is aimed to establish a management structurethat will make sure the activities are conducted in a systematicmanner by ensuring sustainability in the operation of the institutionand to create an effective quality management structuring in whichsenior management and all the personnel take part in the institution.
To attain this goal, an organization structure must be established inthe institution, main policies and values must be determined, qualitymanagement structure must be created, document management mustbe ensured, an adverse Event Reporting System must be established,risk management and training management must be ensured, workmust be undertaken to promote and develop health and institutionalcommunication must be ensured.
» Performance Measurement and Quality Improvement
It is aimed to determine and address the potential problems regardingservice delivery especially administrative, financial and medicalprocesses and take actions to improve quality. It is planned to achievethese goals by making use of indicators determined by the institutionand SAS indicators.
» Healthy Work Life
Under this aspect it is aimed to make sure that the personnel lead ahealthy life for quality service delivery and to look at the organizationsof ODHS through the perspective of the personnel.
In line with this goal, a structure aimed at human resourcesmanagement must be established, measures must be taken againstfactors that threaten the health and safety of the personnel andrequirements to improve the work life must be determined.
» Patient Experience
Under this aspect it is aimed to look at the services through theperspective of the patient in order to ensure basic patient rights,patient safety and patient satisfaction.
To attain this goal, the services that are provided must be organizedin such a way as to protect the patient and carer rights, to make surethat patients access the services on time and to ensure patient safety.

Prologue
10
Department of Quality, Accreditation and Workers' Rights in Health
» Healthcare Services
It is aimed to provide all the medical service processes provided atODHS within the scope of SAS goals. To that end, work must beundertaken in prevention of infections, sterilization services, medicinemanagement, radiation safety, patient care, prosthesis laboratoryservices and safe surgery.
» Support Services
Under this dimension it is aimed to establish the infrastructurenecessary to ensure the safety and continuity of medical serviceprocesses. To attain this goal, work must focus on accommodation;facility management, waste management, information managementand material and device management must be ensured; activitiesaimed at outsourcing must be planned.
» Emergency Management
Under this aspect it is aimed to intervene in the fastest and mostefficient manner to prevent dangerous situations and harm at ODHSthat may be caused by natural disasters such as earthquake, floodor emergencies like fire, explosion etc., respiratory or cardiac arrestcases and in cases where the personnel is exposed to violence.
Coding of Standards of Accreditation in Health
The coding system was developed with a view to giving the standards an identity and thereby ensuring their monitorability.
Coding System
» The code of the Standard is composed of 4 parts.
» The first two parts are composed of letters and the last two parts offigures.
» The parts where the letters are used are composed of two letters andthese two letters are the acronyms of the relevant aspect and chapter.
» The figures in the last two parts (3rd and 4th Parts) constitute a two-digit number.
• The third part signifies the number of the Standard in the chapter.
• The fourth part signifies the number of the assessment criterion ofthe Standard.

Prologue
11
Standards of Accreditation in Health - ODHS Kit
• “00” in the fourth part signifies the Standard itself, the numbers
starting with “01” signifies the ordering of assessment criteria.
The codes for the aspects are as follows:
Aspects Codes
Management and Organization YO
Performance Measurement and Quality Improvement
PÖ
Healthy Work Life SÇ
Patient Experience HD
Healthcare Services SH
Support Services DH
Emergency Management AD
The codes for each chapter can be found below:
CHAPTER CODE NAME OF THE CHAPTER
YO.OY Organizational Structure
YO.PD Core Policies and Values
YO.KY Quality Management Structure
YO.DY Document Management
YO.OB Adverse Event Reporting System
YO.RY Risk Management
YO.EY Training Management
YO.SS Social Responsibility
YO.Kİ Institutional Communication
PÖ.Gİ Monitoring Of ndicators
SÇ.İK Human Resources Management
SÇ.ÇG Employee Health and Safety
HD.HH Basic Patient Rights
HD.HG Patient Safety

Prologue
12
Department of Quality, Accreditation and Workers' Rights in Health
CHAPTER CODE NAME OF THE CHAPTER
HD.GB Patient Feedback
HD.HE Access to Service
SH.EÖ Prevention of Infections
SH.SY Sterilization Management
SH.İY Medicine Management
SH.HB Patient Care
SH.RG Radiation Safety
SH.PL Prosthesis Laboratory Services
SH.GC Safe Surgery
DH.OH Accommodation Services
DH.TY Facility Management
DH.AY Waste Management
DH.BY Information Management
DH.MC Material and Device Management
DH.DK Outsourcing
AD.AD Emergency Management
An example of coding for a Standard can be found below:

Prologue
13
Standards of Accreditation in Health - ODHS Kit
STANDARD CODE
STANDARD EC CODEASSESSMENT
CRITERIA (AC)
YO.OY.01.00
An organizational structure to cover all ODHS activities must be established.
YO.OY.01.01
Organisational structure must be defined in a way that covers responsibilities related to governance.
YO.OY.01.02
All vertical and horizontal relations in the organizational structure, from senior management to subunits, must be defined.
YO.OY.01.03
Within the organizational structure, duties, powers and responsibilities of all units and staff must be defined.
YO.OY.01.04
Responsibilities must be identified for units defined in organizational structure.
YO.OY.01.05
Implementation of hospital policies, procedures, processes and plans should be provided in all units within the organization structure


STANDARDS and
GUIDES


Standards and Guides
17
Standards of Accreditation in Health - ODHS Kit
Aspe
cts
and
Chap
ters
•Or
gani
zatio
nal S
truct
ure
•Co
re P
olic
ies
and
Ethi
cal V
alue
s •
Qual
ity M
anag
emen
t Stru
ctur
e •
Docu
men
t Man
agem
ent
•Ad
vers
e Ev
ent
Repo
rtin
g Sy
stem
•
Risk
Man
agem
ent
•T r
aini
ng M
anag
emen
t•
Soci
al R
espo
nsib
ility
•In
stitu
tiona
l Com
mun
icat
ion
Man
agem
ent a
nd O
rgan
izatio
n
•M
onito
ring
Of
Indi
cato
rs
Perf
orm
ance
Mea
sure
men
t and
Qua
lity
Impr
ovem
ent
•Hu
man
Res
ourc
es M
anag
emen
t •
Empl
oyee
Hea
lth a
nd S
afet
y
Heal
thy
Wor
k Li
fe
•Ba
sic
Patie
nt R
ight
s•
P atie
nt S
afet
y •
Patie
nt F
eedb
ack
•Ac
cess
to S
ervi
ce
Patie
nt E
xper
ienc
e
•Pr
even
tion
of In
fect
ions
•St
eriliz
atio
n M
anag
emen
t•
Med
icin
e M
anag
emen
t•
Patie
nt C
are
•Ra
diat
ion
Safe
ty
•Pr
osth
esis
Lab
orat
ory
Serv
ices
•Su
rgic
al S
afet
y
Heal
th S
ervi
ces
•Ac
com
mod
atio
n Se
rvic
es•
F aci
lity
Man
agem
ent
•W
aste
Man
agem
ent
•In
form
atio
n M
anag
emen
t•
Mat
eria
l and
Dev
ice
Man
agem
ent
•Ou
tsou
rcin
g
Supp
ort S
ervi
ces
•Em
erge
ncy
Man
agem
ent
Emer
genc
y M
anag
emen
t
GOALS• Efficiency• Efficacy• Productivity• Healthy Work Life• Patient Safety• Fairness/Equity• Patient Focused• Convenience• Timeliness• Continuity
ODHS

Standards and Guides
18
Department of Quality, Accreditation and Workers' Rights in Health
ACCR
EDIT
ATIO
N ST
ANDA
RDS
OF H
EALT
HCAR
E SE
T OD
HS
ASPE
CT
CODE
ASPE
CTCH
APTE
R CO
DECH
APTE
RST
ANDA
RD
CODE
STAN
DARD
AC C
ODE
ASSE
SSM
ENT
CRIT
ERIA
(AC)
YOM
anag
emen
t an
d Or
gani
zatio
n
YO.O
YOr
gani
zatio
nal
Stru
ctur
e
YO.O
Y.01
.00
An o
rgan
isat
iona
l stru
ctur
e to
co
ver a
ll OD
HC a
ctiv
ities
mus
t be
esta
blis
hed.
YO.O
Y.01
.01
Orga
nisa
tiona
l stru
ctur
e m
ust b
e de
fined
in a
way
that
cov
ers
resp
onsi
biliti
es re
late
d to
gov
erna
nce,
fina
ncia
l ste
war
dshi
p an
d cl
inic
al
gove
rnan
ce.
YO.O
Y.01
.02
All v
ertic
al a
nd h
orizo
ntal
rela
tions
in th
e or
gani
satio
nal s
truct
ure,
from
se
nior
man
agem
ent t
o su
buni
ts, m
ust b
e de
fined
.
YO.O
Y.01
.03
With
in th
e or
gani
satio
nal s
truct
ure,
dut
ies, p
ower
s an
d re
spon
sibi
lities
of a
ll un
its a
nd s
taff
mus
t be
defin
ed.
YO.O
Y.01
.04
Resp
onsi
bilit
ies
mus
t be
iden
tifie
d fo
r uni
ts d
efin
ed in
org
anis
atio
nal
stru
ctur
e.
YO.O
Y.01
.05
An in
stitu
tiona
l pla
n sh
ould
be
esta
blis
hed
for t
he a
ctiv
ities
car
ried
out i
n lin
e w
ith th
e or
gani
zatio
n's
aim
s an
d ob
ject
ives
.
YO.O
Y.01
.06
Impl
emen
tatio
n of
ODH
C po
licie
s, p
roce
dure
s, p
roce
sses
and
pla
ns
shou
ld b
e pr
ovid
ed in
all
units
with
in th
e or
gani
zatio
n st
ruct
ure.
YO.O
Y.02
.00
ODHC
mus
t hav
e al
l nec
essa
ry
auth
oris
atio
n an
d pe
rmits
for a
ll its
act
iviti
es
YO.O
Y.02
.01
ODHC
mus
t hav
e al
l nec
essa
ry a
utho
rizat
ion
and
perm
its re
late
d to
in
stitu
tiona
l ser
vice
s an
d st
aff w
orki
ng s
tatu
s fo
r all
its a
ctiv
ities
.
YO.O
Y.02
.02
The
curre
nt a
nd v
alid
sta
tus
of th
e ne
cess
ary
auth
oriza
tion
and
auth
oriza
tion
docu
men
ts fo
r all
serv
ices
and
per
sonn
el m
ust b
e re
view
ed
at le
ast o
nce
a ye
ar a
nd re
gula
rly w
hen
nece
ssar
y.
YO.P
DCo
re P
olic
ies
and
Ethi
cal
Valu
esYO
.PD.
01.0
0Co
re p
olic
ies
and
ethi
cal v
alue
s of
OD
HC m
ust b
e de
fined
.
YO.P
D.01
.01
Mis
sion
, vis
ion
and
ethi
cal v
alue
s of
ODH
C m
ust b
e de
fined
in a
cle
ar
and
unde
rsta
ndab
le m
anne
r. YO
.PD.
01.0
2OD
HC m
ust s
hare
its
mis
sion
, vis
ion
and
ethi
cal v
alue
s w
ith th
e pu
blic
.
YO.P
D.01
.03
Corp
orat
e go
als
and
obje
ctiv
es m
ust b
e de
term
ined
in a
ccor
danc
e w
ith m
issi
on, v
isio
n an
d va
lues
, the
obj
ectiv
es o
f the
med
ical
and
ad
min
istra
tive
depa
rtmen
ts s
houl
d be
com
patib
le w
ith th
e ba
sic
polic
ies
and
valu
es o
f the
ODH
C.
YO.P
D.01
.04
Serv
ice
plan
ning
tow
ards
the
achi
evem
ent o
f ins
titut
iona
l goa
ls a
nd
obje
ctiv
es in
ODH
C m
ust b
e m
ade
taki
ng e
nviro
nmen
tal a
nd fi
nanc
ial
fact
ors
into
acc
ount
as
wel
l.
YO.P
D.01
.05
An e
ffici
ent b
udge
ting
mus
t be
in p
lace
in o
rder
to a
ttain
goa
ls a
nd
obje
ctive
s se
t.
YO.P
D.01
.06
ODHC
mus
t rev
iew
and
ass
ess
its in
stitu
tiona
l res
ourc
es a
t reg
ular
in
terv
als
by ta
king
into
con
side
ratio
n pl
ans
prep
ared
and
bud
gets
dr
afte
d w
ith th
e ai
m o
f rea
lisin
g su
ch p
lans
.

Standards and Guides
19
Standards of Accreditation in Health - ODHS Kit
ACCR
EDIT
ATIO
N ST
ANDA
RDS
OF H
EALT
HCAR
E SE
T OD
HS
ASPE
CT
CODE
ASPE
CTCH
APTE
R CO
DECH
APTE
RST
ANDA
RD
CODE
STAN
DARD
AC C
ODE
ASSE
SSM
ENT
CRIT
ERIA
(AC)
YOM
anag
emen
t an
d Or
gani
zatio
n
YO.K
YQu
ality
M
anag
emen
t St
ruct
ure
YO.K
Y.01
.00
Plan
ning
, im
plem
enta
tion,
co
ordi
natio
n an
d co
ntin
uity
of
qual
ity im
prov
emen
t act
iviti
es
mus
t be
ensu
red.
YO.K
Y.01
.01
A m
anag
emen
t stru
ctur
e m
ust b
e es
tabl
ishe
d in
ord
er to
ens
ure
the
pla
nnin
g, im
plem
enta
tion,
coo
rdin
atio
n an
d co
ntin
uity
of q
ualit
y im
prov
emen
t act
iviti
es
YO.K
Y.01
.02
The
dutie
s, p
ower
s an
d re
spon
sibi
litie
s of
thos
e in
volv
ed in
the
man
agem
ent s
truct
ure
mus
t be
defin
ed.
YO.K
Y.01
.03
The
man
ager
ial s
truct
ure
shou
ld e
nsur
e th
e pl
anni
ng,
exec
utio
n an
d co
ordi
natio
n of
qua
lity
impr
ovem
ent a
ctiv
ities
.
YO.K
Y.01
.04
Com
mitt
ees
mus
t be
esta
blis
hed
conc
erne
d w
ith a
t lea
st th
e fo
llow
ing
topi
cs:
•Em
ploy
ee s
afet
y•P
atie
nt s
afet
y•T
rain
ing
•Fac
ility
man
agem
ent
•pre
vent
ion
of•i
nfec
tions
•Rad
iatio
n sa
fety
YO.D
YDo
cum
ent
Man
agem
ent
YO.D
Y.01
.00
Man
agem
ent o
f doc
umen
ts a
t OD
HC m
ust b
e en
sure
d.
YO.D
Y.01
.01
Polic
ies,
pro
cedu
res,
pro
cess
es a
nd p
lans
rela
ted
to a
ll m
ain
func
tions
co
vere
d by
the
SAS
ODHS
set
sho
uld
be d
ocum
ente
d.YO
.DY.
01.0
2Fo
rmat
of d
ocum
ents
mus
t be
dete
rmin
ed.
YO.D
Y.01
.03
Prep
arat
ion,
che
ck, a
ppro
val,
up-to
-dat
edne
ss a
nd m
aint
enan
ce o
f do
cum
ents
mus
t be
ensu
red.
YO
.DY.
01.0
4Ru
les
to c
omm
unic
ate
docu
men
ts to
rele
vant
peo
ple
mus
t be
set.
YO.D
Y.01
.05
"Pro
cess
rela
ted
to m
onito
ring
of e
xter
nal d
ocum
ents
to b
e fo
llow
ed b
y OD
HC m
ust b
e de
fined
."
YO.O
BAd
vers
e Ev
ent
Repo
rtin
g Sy
stem
YO.O
B.01
.00
Repo
rtin
g of
adv
erse
eve
nts
that
m
ay o
r doe
s af
fect
the
safe
ty
of p
atie
nts
and
staf
f neg
ativ
ely
mus
t be
ensu
red,
and
nec
essa
ry
mea
sure
s m
ust b
e ta
ken.
YO.O
B.01
.01
"A s
yste
m m
ust b
e es
tabl
ishe
d in
ord
er to
repo
rt a
dver
se e
vent
s th
at
may
or d
oes
affe
ct th
e sa
fety
of p
atie
nts
and
staf
f neg
ativ
ely.
"
YO.O
B.01
.02
Case
spe
cific
ana
lysi
s m
ust b
e co
nduc
ted,
and
act
ions
mus
t be
take
n if
nece
ssar
y.
YO.O
B.01
.03
Notif
icat
ions
mad
e to
the
syst
em m
ust b
e an
alyz
ed, r
epor
ted
and
eval
uate
d.

Standards and Guides
20
Department of Quality, Accreditation and Workers' Rights in Health
ACCR
EDIT
ATIO
N ST
ANDA
RDS
OF H
EALT
HCAR
E SE
T OD
HS
ASPE
CT
CODE
ASPE
CTCH
APTE
R CO
DECH
APTE
RST
ANDA
RD
CODE
STAN
DARD
AC C
ODE
ASSE
SSM
ENT
CRIT
ERIA
(AC)
YOM
anag
emen
t an
d Or
gani
zatio
n
YO.R
YRi
sk
Man
agem
ent
YO.R
Y.01
.00
Risk
s re
late
d to
ODH
C an
d se
rvic
es p
rovi
ded
mus
t be
m
anag
ed.
YO.R
Y.01
.01
Ther
e m
ust b
e a
regu
latio
n re
late
d to
man
agin
g th
e ris
ks th
at m
ay o
ccur
in
an
ODHC
.YO
.RY.
01.0
2A
risk
man
agem
ent p
lan
mus
t be
pre
pare
d in
ord
er to
man
age
risks
rela
ted
to O
DHC
and
serv
ices
pro
vided
.
YO.R
Y.01
.03
Risk
man
agem
ent p
lan
mus
t en
tail
patie
nts,
car
ers,
vis
itors
, sta
ff,
faci
lity
safe
ty a
nd e
nviro
nmen
tal s
afet
y an
d ad
min
istra
tive
and
finan
cial
pro
cess
es.
YO.R
Y.01
.04
Risk
man
agem
ent p
lan
mus
t ent
ail t
he fo
llow
ing
issu
es:
• Pa
tient
s •
Rela
tives
• Ca
rers
• V
isito
rs•
Staf
f • F
acilit
y sa
fety
• En
viro
nmen
tal s
afet
y •
Adm
inis
trativ
e an
d fin
anci
al p
roce
sses
.•
Stra
tegi
c ris
ks•
Com
min
ucat
ion
proc
esse
s w
ith s
take
hold
ers
YO.R
Y.01
.05
"Nec
essa
ry m
easu
res
mus
t be
ado
pted
in li
ne w
ith th
e a
ccor
ding
to
the
risk
leve
l ide
ntifi
ed, a
nd a
ctio
ns m
ust b
e ta
ken
for i
mpr
ovem
ent."
YO.R
Y.01
.06
Risk
s id
entif
ied
and
effe
ctiv
enes
s of
impr
ovem
ent a
ctio
ns m
ust
be
revi
ewed
per
iodi
cial
ly.
YO.R
Y.01
.07
"Indi
cato
rs fo
r mon
itorin
g th
e ef
fect
iven
ess
of ri
sk m
anag
emen
t mus
t be
det
erm
ined
and
mon
itore
d."
YO.E
YTr
aini
ng
Man
agem
ent
YO.E
Y.01
.00
In a
ccor
danc
e w
ith q
ualit
y im
prov
emen
t act
iviti
es, t
rain
ing
need
s of
pat
ient
s, c
arer
s an
d st
aff
mus
t be
dete
rmin
ed, a
nd it
mus
t be
ens
ured
that
nec
essa
ry tr
aini
ng
is c
ondu
cted
effe
ctiv
ely.
YO.E
Y.01
.01
A co
mm
ittee
in c
harg
e of
the
plan
ning
and
coo
rdin
atio
n of
trai
ning
ac
tiviti
es m
ust b
e es
tabl
ishe
d.
YO.E
Y.01
.02
Trai
ning
nee
ds m
ust b
e id
entif
ied
on th
e ba
sis
of p
atie
nts,
car
ers
and
staf
f. YO
.EY.
01.0
3Tr
aini
ng p
lans
mus
t be
prep
ared
and
impl
emen
ted
in li
ne w
ith tr
aini
ng
need
s.
YO.E
Y.01
.04
Effe
ctiv
enes
s of
trai
ning
pla
ns a
nd tr
aini
ngs
carr
ied
out m
ust b
e m
onito
red
and
nece
ssar
y im
prov
emen
t act
ions
mus
t be
take
n.
YO.S
SSo
cial
Re
spon
sibi
lity
YO.S
S.01
.00
ODHC
s m
ust o
rgan
ize p
rogr
ams
for p
rom
otin
g an
d im
prov
ing
heal
th
by ta
king
hea
lth s
truct
ure
and
gene
ral h
ealth
pro
blem
s of
the
soci
ety
into
acc
ount
.
YO.S
S.01
.01
ODHC
s m
ust o
rgan
ize p
rogr
amm
es p
rom
otin
g an
d im
prov
ing
heal
th,
in li
ne w
ith th
e he
alth
stru
ctur
e of
the
regi
on a
nd p
opul
atio
n it
serv
es,
taki
ng in
to c
onsi
dera
tion
serv
ice
qual
ity, w
ithin
the
cont
ext o
f nat
iona
l an
d gl
obal
hea
lth p
robl
ems.
YO.K
İIn
stitu
tiona
l Co
mm
unic
atio
nYO
.Kİ.0
1.00
Inst
itutio
nal c
omm
unic
atio
n ac
tiviti
es m
ust b
e ca
rrie
d ou
t ef
fect
ivel
y.
YO.K
İ.01.
01Un
der t
he s
cope
of i
nstit
utio
nal c
omm
unic
atio
n, ta
rget
aud
ience
mus
t be
iden
tified
by
takin
g OD
HC s
truct
ure,
cor
e po
licies
and
val
ues
into
acc
ount
an
d co
mm
unic
atio
n st
rate
gies
for t
arge
t aud
ience
mus
t be
dete
rmin
ed.
YO.K
İ.01.
02Ta
rget
aud
ienc
e m
ust b
e in
form
ed a
bout
ODH
C ac
tiviti
es a
nd th
eir
orga
nisa
tion.
YO
.Kİ.0
1.03
Nece
ssar
y ac
tions
mus
t be
take
n to
cre
ate
a po
sitiv
e op
inio
n am
ong
targ
et a
udie
nce.

Standards and Guides
21
Standards of Accreditation in Health - ODHS Kit
ACCR
EDIT
ATIO
N ST
ANDA
RDS
OF H
EALT
HCAR
E SE
T OD
HS
ASPE
CT
CODE
ASPE
CTCH
APTE
R CO
DECH
APTE
RST
ANDA
RD
CODE
STAN
DARD
AC C
ODE
ASSE
SSM
ENT
CRIT
ERIA
(AC)
PÖ
Perf
orm
ance
M
easu
rem
ent
and
Qual
ity
Impr
ovem
ent
PÖ.G
İM
onito
ring
Of
Indi
cato
rsPÖ
.Gİ.0
1.00
Inst
itutio
nal i
ndic
ator
s m
ust b
e m
onito
red
and
eval
uate
d in
ord
er
to c
ontin
uous
ly im
prov
e pr
oces
ses
rela
ted
to s
ervi
ce d
eliv
ery,
led
by a
dmin
istra
tive,
fina
ncia
l and
m
edic
al s
teps
.
PÖ.G
İ.01.
01"In
dica
tors
mus
t be
dete
rmin
ed to
incl
ude
proc
esse
s co
ncer
ning
se
rvic
e de
liver
y, p
rimar
ily a
dmin
istra
tive,
fina
ncia
l and
med
ical
ste
ps."
PÖ.G
İ.01.
02In
dica
tor c
ards
mus
t be
crea
ted
to c
over
issu
es re
late
d de
term
inat
ion,
co
llect
ion,
eva
luat
ion
and
mon
itorin
g of
dat
a to
be
used
for i
ndic
ator
s.
PÖ.G
İ.01.
03M
onito
ring,
eva
luat
ing
and
repo
rtin
g of
indi
cato
rs m
ust b
e ca
rrie
d ou
t th
roug
h in
form
atio
n m
anag
emen
t sys
tem
s
PÖ.G
İ.01.
04Ne
cess
ary
impr
ovem
ents
mus
t be
mad
e ta
king
into
con
side
ratio
n th
e an
alys
is re
sults
for t
he in
dica
tors
.
PÖ.G
İ.01.
05Th
e re
sults
of t
he S
AS in
dica
tors
mus
t be
subm
itted
to th
e SA
S In
dica
tor D
ata
Syst
em.

Standards and Guides
22
Department of Quality, Accreditation and Workers' Rights in Health
ACCR
EDIT
ATIO
N ST
ANDA
RDS
OF H
EALT
HCAR
E SE
T OD
HS
ASPE
CT
CODE
ASPE
CTCH
APTE
R CO
DECH
APTE
RST
ANDA
RD
CODE
STAN
DARD
AC C
ODE
ASSE
SSM
ENT
CRIT
ERIA
(AC)
SÇHe
alth
y W
ork
Life
SÇ.İK
Hum
an
Reso
urce
s M
anag
emen
t
SÇ.İK
.01.
00
A m
anag
emen
t stru
ctur
e th
at w
ill fu
lfill
the
requ
irem
ents
con
cern
ing
plan
ning
of h
uman
reso
urce
s,
impr
ovem
ent o
f wor
k lif
e an
d th
e pe
rson
nel m
ust b
e es
tabl
ishe
d.
SÇ.İK
.01.
01Th
e re
latio
n of
the
man
agem
ent s
truct
ure
with
oth
er m
anag
emen
t le
vels
mus
t be
iden
tifie
d.
SÇ.İK
.01.
02Du
ties,
aut
horit
ies
and
resp
onsi
bilit
ies
of th
ose
in th
e m
anag
emen
t st
ruct
ure
and
the
qual
ifica
tions
they
mus
t hav
e m
ust b
e id
entif
ied.
SÇ.İK
.01.
03An
nual
goa
ls a
nd w
ork
plan
s m
ust b
e de
velo
ped.
SÇ.İK
.01.
04Fe
edba
ck p
roce
sses
aim
ed a
t det
erm
inin
g sa
tisfa
ctio
n le
vels
and
co
mm
ents
and
sug
gest
ions
of t
he p
erso
nnel
rega
rdin
g th
eir w
ork
life
mus
t be
iden
tifie
d.
SÇ.İK
.02.
00
The
requ
irem
ents
nec
essa
ry to
co
nsta
ntly
impr
ove
recr
uitm
ent
and
com
plia
nce
proc
esse
s of
the
pers
onne
l and
thei
r wor
k lif
e m
ust
be d
eter
min
ed a
nd fu
lfille
d.
SÇ.İK
.02.
01A
pers
onne
l rec
ruitm
ent p
lan
mus
t be
deve
lope
d in
line
with
hum
an
reso
urce
s ne
eds
of O
DHC.
SÇ.İK
.02.
02Pe
rson
nel r
ecru
itmen
t pro
cess
es m
ust b
e id
entif
ied.
SÇ.İK
.02.
03Pr
oces
ses
rega
rdin
g en
surin
g th
e ad
apta
tion
of th
e ne
wly
recr
uite
d pe
rson
nel t
o OD
HC m
ust b
e id
entif
ied.
SÇ.İK
.02.
04Du
ties,
aut
horit
ies,
resp
onsi
bilit
ies
of th
e pe
rson
nel a
nd th
e qu
alifi
catio
ns
they
sho
uld
have
and
the
perfo
rman
ce c
riter
ia th
eir j
ob re
quire
s m
ust b
e de
term
ined
.
SÇ.İK
.02.
05Pe
rform
ance
of t
he p
erso
nnel
mus
t be
mea
sure
d, tr
aini
ng n
eeds
mus
t be
dete
rmin
ed to
enh
ance
the
perfo
rman
ce a
nd n
eces
sary
trai
ning
s m
ust
be p
rovi
ded.
SÇ.İK
.02.
06
How
and
to w
hat e
xten
t the
cur
rent
sta
ndar
ds, p
roto
cols
and
evi
denc
e-ba
sed
clin
ical
gui
delin
es a
ccep
ted
by O
DHC
are
used
by
the
pers
onne
l m
ust b
e m
onito
red
and
train
ings
aim
ed a
t ens
urin
g th
e us
e of
thes
e st
anda
rds
and
guid
elin
es e
ffici
ently
mus
t be
iden
tifie
d.

Standards and Guides
23
Standards of Accreditation in Health - ODHS Kit
ACCR
EDIT
ATIO
N ST
ANDA
RDS
OF H
EALT
HCAR
E SE
T OD
HS
ASPE
CT
CODE
ASPE
CTCH
APTE
R CO
DECH
APTE
RST
ANDA
RD
CODE
STAN
DARD
AC C
ODE
ASSE
SSM
ENT
CRIT
ERIA
(AC)
SÇHe
alth
y W
ork
Life
SÇ.Ç
GEm
ploy
ee
Heal
th a
nd
Safe
tySÇ
.ÇG.
01.0
0
Fact
ors
thre
aten
ing
the
heal
th
and
safe
ty o
f em
ploy
ees
shou
ld
be id
entif
ied
and
nece
ssar
y pr
ecau
tions
sho
uld
be ta
ken
to e
stab
lish
a he
alth
y an
d sa
fe
wor
king
env
ironm
ent.
SÇ.Ç
G.01
.01
A co
mm
ittee
aim
ed a
t man
agem
ent o
f the
fact
ors
that
thre
aten
em
ploy
ee h
ealth
and
saf
ety
mus
t be
esta
blis
hed.
SÇ.Ç
G.01
.02
Risk
ana
lyse
s m
ust b
e co
nduc
ted
on th
e fa
ctor
s th
at th
reat
en
empl
oyee
hea
lth a
nd s
afet
y an
d m
easu
res
mus
t be
take
n to
elim
inat
e or
dec
reas
e th
e ris
ks th
at th
reat
en th
e sa
fety
.
SÇ.Ç
G.01
.03
It m
ust b
e en
sure
d th
at e
mpl
oyee
s us
e th
e pe
rson
al p
rote
ctiv
e eq
uipm
ent a
gain
st th
e ris
ks.
SÇ.Ç
G.01
.04
Qual
ity im
prov
emen
t act
iviti
es th
at a
im to
ens
ure
the
cont
inui
ty o
f em
ploy
ee s
afet
y m
ust b
e pl
anne
d.
SÇ.Ç
G.01
.05
Phys
ical
and
soc
ial o
ppor
tuni
ties
that
are
nec
essa
ry to
impr
ove
the
wor
k en
viro
nmen
ts a
nd th
e w
ork
life
mus
t be
prov
ided
and
per
sona
l ne
eds
of th
e em
ploy
ee re
gard
ing
wor
k lif
e m
ust b
e m
et.

Standards and Guides
24
Department of Quality, Accreditation and Workers' Rights in Health
ACCR
EDIT
ATIO
N ST
ANDA
RDS
OF H
EALT
HCAR
E SE
T OD
HS
ASPE
CT
CODE
ASPE
CTCH
APTE
R CO
DECH
APTE
RST
ANDA
RD
CODE
STAN
DARD
AC C
ODE
ASSE
SSM
ENT
CRIT
ERIA
(AC)
HDPa
tient
Ex
perie
nce
HD.H
HBa
sic
Patie
nt
Righ
tsHD
.HH.
01.0
0
The
serv
ices
pro
vide
d in
ODH
C m
ust b
e or
gani
zed
in s
uch
a w
ay
as to
pro
tect
pat
ient
and
car
er
right
s.
HD.H
H.01
.01
An e
xecu
tive
stru
ctur
e ai
med
at p
rote
ctin
g, e
xerc
isin
g an
d im
prov
ing
the
right
s of
pat
ient
s an
d ca
rers
mus
t be
esta
blis
hed.
HD.H
H.01
.02
ODHC
mus
t dec
lare
info
rmat
ion
abou
t all
the
serv
ices
that
are
pro
vide
d an
d a
cces
s to
thes
e se
rvic
es a
nd th
e qu
ality
of t
he s
ervi
ces.
HD.H
H.01
.03
Patie
nt a
nd/o
r car
ers
mus
t be
info
rmed
abo
ut th
e se
rvic
es re
late
d to
di
agno
sis,
trea
tmen
t, ca
re a
nd p
atie
nt re
spon
sibi
litie
s.
HD.H
H.01
.04
Durin
g th
e he
alth
car
e pr
oces
s, c
onsi
dera
tion
mus
t be
give
n to
the
choi
ces
and
pref
eren
ces
of th
e pa
tient
.
HD.H
H.01
.05
Activ
ities
mus
t be
plan
ned
in a
ll se
rvic
e pr
oces
ses
for t
he p
atie
nt to
be
resp
ecte
d an
d to
rece
ive
met
icul
ous
serv
ice.
HD.H
H.01
.06
The
patie
nt m
ust b
e in
form
ed p
rior t
o an
y m
edic
al in
terv
entio
n pl
anne
d an
d hi
s/he
r con
sent
mus
t be
obta
ined
and
doc
umen
ted.
HD.H
H.01
.07
Patie
nts
mus
t be
able
to e
xam
ine
the
med
ical
doc
umen
ts a
bout
th
emse
lves
and
rece
ive
a co
py if
requ
este
d.
HD.H
H.01
.08
Arra
ngem
ents
mus
t be
mad
e fo
r the
spi
ritua
l and
cul
tura
l nee
ds o
f the
pa
tient
.
HD.H
H.01
.09
All m
easu
res
nece
ssar
y m
ust b
e ta
ken
to e
nsur
e pa
tient
priv
acy.
HD.H
H.01
.10
Arra
ngem
ents
mus
t be
mad
e fo
r rec
eivi
ng, i
nves
tigat
ing
and
reso
lvin
g co
mpl
aint
s of
pat
ient
s an
d th
eir r
elat
ives
.
HD.H
H.01
.11
Patie
nt’s
con
sent
mus
t be
obta
ined
if th
e pa
tient
is to
take
par
t in
a re
sear
ch o
r exp
erim
ent,
or if
the
info
rmat
ion,
dat
a or
mat
eria
ls a
bout
th
e pa
tient
are
to b
e us
ed in
any
way
.
HD.H
H.01
.12
Proc
esse
s ai
med
at i
nfor
min
g th
e pa
tient
or c
arer
if u
nint
ende
d ev
ents
th
at n
egat
ivel
y af
fect
the
patie
nt s
afet
y oc
cur m
ust b
e id
entif
ied
Standards and Guides
25
Standards of Accreditation in Health - ODHS Kit
ACCR
EDIT
ATIO
N ST
ANDA
RDS
OF H
EALT
HCAR
E SE
T OD
HS
ASPE
CT
CODE
ASPE
CTCH
APTE
R CO
DECH
APTE
RST
ANDA
RD
CODE
STAN
DARD
AC C
ODE
ASSE
SSM
ENT
CRIT
ERIA
(AC)
HDPa
tient
Ex
perie
nce
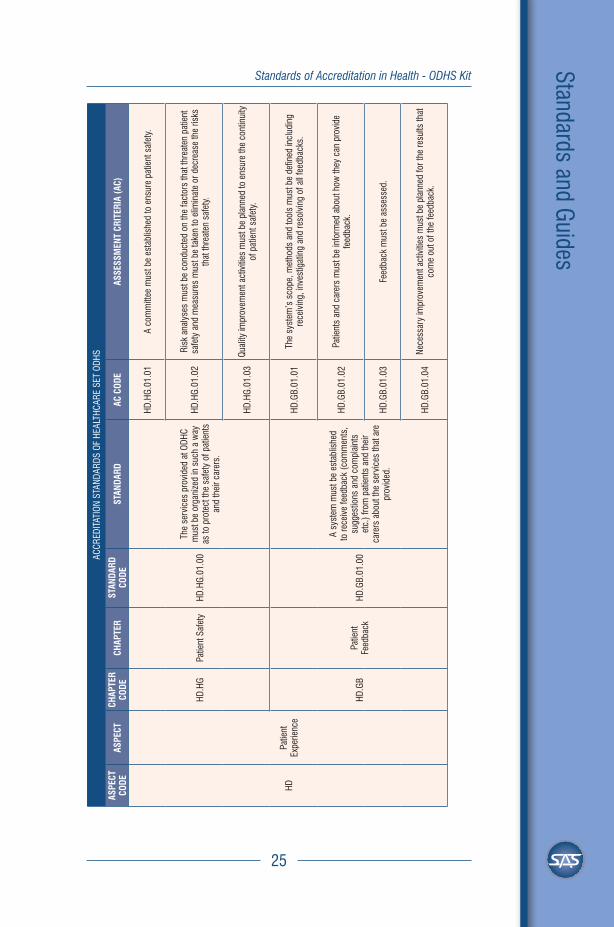
HD.H
GPa
tient
Saf
ety
HD.H
G.01
.00
The
serv
ices
pro
vide
d at
ODH
C m
ust b
e or
gani
zed
in s
uch
a w
ay
as to
pro
tect
the
safe
ty o
f pat
ient
s an
d th
eir c
arer
s.
HD.H
G.01
.01
A co
mm
ittee
mus
t be
esta
blis
hed
to e
nsur
e pa
tient
saf
ety.
HD.H
G.01
.02
Risk
ana
lyse
s m
ust b
e co
nduc
ted
on th
e fa
ctor
s th
at th
reat
en p
atie
nt
safe
ty a
nd m
easu
res
mus
t be
take
n to
elim
inat
e or
dec
reas
e th
e ris
ks
that
thre
aten
saf
ety.
HD.H
G.01
.03
Qual
ity im
prov
emen
t act
iviti
es m
ust b
e pl
anne
d to
ens
ure
the
cont
inui
ty
of p
atie
nt s
afet
y.
HD.G
BPa
tient
Fe
edba
ckHD
.GB.
01.0
0
A sy
stem
mus
t be
esta
blis
hed
to re
ceiv
e fe
edba
ck (c
omm
ents
, su
gges
tions
and
com
plai
nts
etc.
) fro
m p
atie
nts
and
thei
r ca
rers
abo
ut th
e se
rvic
es th
at a
re
prov
ided
.
HD.G
B.01
.01
The
syst
em’s
sco
pe, m
etho
ds a
nd to
ols
mus
t be
defin
ed in
clud
ing
rece
ivin
g, in
vest
igat
ing
and
reso
lvin
g of
all
feed
back
s.
HD.G
B.01
.02
Patie
nts
and
care
rs m
ust b
e in
form
ed a
bout
how
they
can
pro
vide
fe
edba
ck.
HD.G
B.01
.03
Feed
back
mus
t be
asse
ssed
.
HD.G
B.01
.04
Nece
ssar
y im
prov
emen
t act
iviti
es m
ust b
e pl
anne
d fo
r the
resu
lts th
at
com
e ou
t of t
he fe
edba
ck.

Standards and Guides
26
Department of Quality, Accreditation and Workers' Rights in Health
ACCR
EDIT
ATIO
N ST
ANDA
RDS
OF H
EALT
HCAR
E SE
T OD
HS
ASPE
CT
CODE
ASPE
CTCH
APTE
R CO
DECH
APTE
RST
ANDA
RD
CODE
STAN
DARD
AC C
ODE
ASSE
SSM
ENT
CRIT
ERIA
(AC)
HDPa
tient
Ex
perie
nce
HD.H
EAc
cess
to
Serv
ice
HD.H
E.01
.00
Nece
ssar
y pr
ecau
tions
mus
t be
take
n in
ord
er to
pro
vide
pat
ient
ab
le to
reac
h se
rvic
es in
tim
e.
HD.H
E.01
.01
Patie
nts
mus
t be
prov
ided
with
rece
ptio
n, o
rient
atio
n an
d co
nsul
tatio
n se
rvic
es th
at w
ill fa
cilit
ate
the
appl
icat
ion
proc
ess
at O
DHC
and
thro
ugh
whi
ch th
ey c
an a
cces
s al
l the
info
rmat
ion
they
nee
d in
the
appl
icat
ion
proc
ess
at O
DHC.
HD.H
E.01
.02
The
mea
sure
s ne
cess
ary
to m
inim
ize th
e w
aitin
g pe
riod
in th
e ou
tpat
ient
clin
ic m
ust b
e pl
anne
d an
d p
atien
ts m
ust b
e in
form
ed a
bout
how
long
they
w
ill w
ait a
ppro
ximat
ely a
nd w
hen
they
will
be e
xam
ined
by
the
doct
or.
HD.H
E.01
.03
Faci
litat
ing
mea
sure
s co
ncer
ning
acc
ess
to s
ervi
ces
and
wai
ting
perio
ds m
ust b
e ta
ken
base
d on
age
, dis
ease
and
dis
abilit
y.
HD.H
E.01
.04
Serv
ice
deliv
ery
proc
esse
s m
ust b
e or
gani
zed
in s
uch
a w
ay a
s to
en
sure
the
diag
nosi
s an
d tre
atm
ent o
f the
pat
ient
in g
ood
time
and
with
out d
elay
.
HD.H
E.01
.05
Arra
ngem
ents
mus
t be
done
at O
DHC
to fa
cilit
ate
patie
nt a
cces
s to
OD
HCs
in c
ase
of e
mer
genc
ies
over
-hou
rs.

Standards and Guides
27
Standards of Accreditation in Health - ODHS Kit
ACCR
EDIT
ATIO
N ST
ANDA
RDS
OF H
EALT
HCAR
E SE
T OD
HS
ASPE
CT
CODE
ASPE
CTCH
APTE
R CO
DECH
APTE
RST
ANDA
RD
CODE
STAN
DARD
AC C
ODE
ASSE
SSM
ENT
CRIT
ERIA
(AC)
SHHe
alth
Se
rvic
es
SH.E
ÖPr
even
tion
of
Infe
ctio
nsSH
.EÖ.
01.0
0Ne
cess
ary
mea
sure
s m
ust
be ta
ken
for t
he p
reve
ntio
n of
in
fect
ions
.
SH.E
Ö.01
.01
A co
mm
ittee
mus
t be
form
ed fo
r inf
ectio
n co
ntro
l and
pre
vent
ion,
and
re
spon
sibi
litie
s m
ust b
e de
term
ined
.
SH.E
Ö.01
.02
A pr
ogra
mm
e m
ust b
e cr
eate
d fo
r the
con
trol a
nd p
reve
ntio
n of
in
fect
ions
.
SH.E
Ö.01
.03
Effic
ienc
y of
the
prac
tices
aim
ed a
t ens
urin
g pr
even
tion
of in
fect
ions
m
ust b
e m
onito
red.
SH.S
YSt
eriliz
atio
n M
anag
emen
tSH
.SY.
01.0
0Pr
oces
ses
conc
erni
ng s
teril
izatio
n se
rvic
es m
ust b
e id
entif
ied
and
take
n un
der c
ontro
l.
SH.S
Y.01
.01
Phys
ical
are
as a
nd c
ondi
tions
in s
teril
izatio
n un
it m
ust b
e pl
anne
d ac
cord
ing
to th
e pr
oces
s st
eps.
SH.S
Y.01
.02
The
proc
esse
s re
gard
ing
ster
ilizat
ion,
sto
rage
, tra
nsfe
r and
use
of t
he
mat
eria
ls m
ust b
e ta
ken
unde
r con
trol.
SH.S
Y.01
.03
Trac
eabi
lity
of th
e ev
iden
ce re
gard
ing
time,
dev
ice,
met
hod,
im
plem
ente
r and
con
trol p
aram
eter
s m
ust b
e en
sure
d in
eac
h st
age
of
the
ster
ilizat
ion.

Standards and Guides
28
Department of Quality, Accreditation and Workers' Rights in Health
ACCR
EDIT
ATIO
N ST
ANDA
RDS
OF H
EALT
HCAR
E SE
T OD
HS
ASPE
CT
CODE
ASPE
CTCH
APTE
R CO
DECH
APTE
RST
ANDA
RD
CODE
STAN
DARD
AC C
ODE
ASSE
SSM
ENT
CRIT
ERIA
(AC)
SHHe
alth
Se
rvic
es
SH.İY
Med
icin
e M
anag
emen
tSH
.İY.0
1.00
Effic
ient
and
saf
e m
edic
ine
man
agem
ent m
ust b
e en
sure
d in
th
e in
stitu
tion.
SH.İY
.01.
01A
med
icin
e m
anag
emen
t stru
ctur
e th
at w
ill pr
ovid
e an
effe
ctiv
e im
plem
enta
tion
of d
rug
adm
inis
tratio
n an
d co
ordi
natio
n m
ust b
e cr
eate
d.
SH.İY
.01.
02M
ain
and
criti
cal s
tage
s of
all
the
med
icin
e pr
oces
ses
in th
e in
stitu
tion
mus
t be
dete
rmin
ed a
nd th
e m
etho
ds a
nd ru
les
rega
rdin
g th
ese
stag
es
mus
t be
iden
tifie
d.
SH.İY
.01.
03Th
e rig
ht m
edic
ine
mus
t be
prov
ided
at t
he ri
ght t
ime
and
effe
ctiv
e st
ock
man
agem
ent o
f the
med
icin
es m
ust b
e en
sure
d.
SH.İY
.01.
04M
edic
ines
mus
t be
kept
und
er p
rope
r con
ditio
ns.
SH.İY
.01.
05M
easu
res
mus
t be
take
n to
ens
ure
the
safe
ty o
f the
pat
ient
and
the
pers
onne
l whe
n th
e m
edic
ines
are
bei
ng p
repa
red
and
adm
inis
tere
d.
SH.İY
.01.
06Tr
acea
bilit
y of
med
icin
e pr
oces
ses
mus
t be
ensu
red
by m
akin
g us
e of
feed
back
infra
stru
ctur
es a
nd in
dica
tors
and
the
nece
ssar
y im
prov
emen
t wor
k m
ust b
e un
dert
aken
.
SH.H
BPa
tient
Car
eSH
.HB.
01.0
0
Patie
nt c
are
proc
esse
s m
ust b
e co
nduc
ted
in li
ne w
ith th
e ne
eds
of th
e pa
tient
and
so
as to
ens
ure
patie
nt s
afet
y.
SH.H
B.01
.01
The
proc
ess
rela
ted
to th
e pa
tient
car
e pr
actic
es m
ust b
e pl
anne
d.
SH.H
B.01
.02
Patie
nts
mus
t be
eval
uate
d in
term
s of
thei
r car
e ne
eds.
SH.H
B.01
.03
A ca
re p
lan
for p
atie
nts
mus
t be
deve
lope
d a
ccor
ding
to th
e re
sults
of
the
eval
uatio
n
SH.H
B.01
.04
The
care
pla
n m
ust b
e re
view
ed in
line
with
the
clin
ical
pic
ture
of t
he
patie
nt a
nd b
e up
date
d w
hen
nece
ssar
y.SH
.HB.
01.0
5Pa
tient
s/ca
rers
mus
t be
invo
lved
in th
e ca
re p
roce
sses
.
SH.H
B.01
.06
Ethi
cal d
ilem
mas
suc
h as
not
trea
ting
the
patie
nt, w
ithdr
awal
of t
he
treat
men
t or d
isco
ntin
uing
the
treat
men
t mus
t be
addr
esse
d an
d se
ttled
in
tim
e.
SH.H
B.01
.07
Proc
esse
s re
gard
ing
refe
rral
of t
he p
atie
nt o
r com
plet
ion
of th
e tre
atm
ent m
ust b
e pl
anne
d so
as
to e
nsur
e co
ntin
uity
of t
he c
are.

Standards and Guides
29
Standards of Accreditation in Health - ODHS Kit
ACCR
EDIT
ATIO
N ST
ANDA
RDS
OF H
EALT
HCAR
E SE
T OD
HS
ASPE
CT
CODE
ASPE
CTCH
APTE
R CO
DECH
APTE
RST
ANDA
RD
CODE
STAN
DARD
AC C
ODE
ASSE
SSM
ENT
CRIT
ERIA
(AC)
SHHe
alth
Se
rvic
esSH
.HB
Patie
nt C
are
SH.H
B.02
.00
In th
e pa
tient
car
e pr
oces
s, p
atie
nt
iden
tity
mus
t be
verif
ied
to m
ake
sure
that
the
med
ical
pro
cedu
re is
co
nduc
ted
on th
e rig
ht p
atie
nt.
SH.H
B.02
.01
Iden
tity
verif
icat
ion
met
hods
and
tool
s m
ust b
e id
entif
ied.
SH.H
B.02
.02
Patie
nt a
nd h
ealth
per
sonn
el m
ust b
e tra
ined
on
verif
icat
ion
of t
he
patie
nt id
entit
y.
SH.H
B.02
.03
Patie
nt id
entit
y m
ust b
e ve
rifie
d in
all
the
proc
edur
es to
be
cond
ucte
d in
pa
tient
car
e pr
oces
s.
SH.H
B.03
.00
Mea
sure
s m
ust b
e ta
ken
to p
reve
nt
patie
nt fa
lls.
SH.H
B.03
.01
The
proc
ess
conc
erni
ng p
reve
ntio
n of
falls
mus
t be
plan
ned.
SH.H
B.03
.02
Patie
nts
mus
t be
asse
ssed
for f
all r
isk.
SH.H
B.03
.03
Mea
sure
s m
ust b
e ta
ken
to p
reve
nt fa
lls.
SH.H
B.03
.04
Falls
that
hav
e oc
curr
ed m
ust b
e m
onito
red.
SH.H
B.04
.00
Effe
ctiv
e co
mm
unic
atio
n m
ust b
e en
sure
d in
the
flow
of i
nfor
mat
ion
amon
g th
e he
alth
pro
fess
iona
ls.
SH.H
B.04
.01
The
proc
ess
rega
rdin
g sh
ift h
ando
ver o
f the
per
sonn
el m
ust b
e id
entif
ied.
SH.H
B.04
.02
Actio
n m
ust b
e ta
ken
abou
t ver
bal r
eque
sts.
SH.H
B.04
.03
Actio
n m
ust b
e ta
ken
abou
t abb
revi
atio
ns, s
igns
, sym
bols
and
the
amou
nt o
f dos
e th
at s
houl
d no
t be
used
.
SH.H
B.04
.04
Patie
nt in
form
atio
n m
ust b
e co
nvey
ed p
rope
rly a
nd th
orou
ghly
whe
n th
e pa
tient
is t
rans
ferr
ed b
etw
een
depa
rtm
ents
.
SH.H
B.04
.05
The
proc
ess
rega
rdin
g ta
king
into
acc
ount
the
con
sulta
tions
hel
d in
an
d ou
tsid
e OD
HC m
ust b
e pl
anne
d.
SH.H
B.05
.00
Patie
nts
that
car
ry th
e ris
k of
ha
rmin
g th
emse
lves
or o
ther
s m
ust b
e ta
ken
unde
r con
trol.
SH.H
B.05
.01
Patie
nts
mus
t be
asse
ssed
in te
rms
of th
e ris
k of
har
min
g th
emse
lves
or
oth
ers.
SH.H
B.05
.02
Nece
ssar
y m
easu
res
mus
t be
take
n ag
ains
t pat
ient
s th
at c
arry
the
risk
of h
arm
ing
them
selv
es o
r oth
ers.
SH.H
B.06
.00
The
stan
dard
izatio
n of
car
e fo
r sp
ecifi
c pa
tient
gro
ups
mus
t be
ensu
red.
SH.H
B.06
.01
Proc
esse
s re
gard
ing
spec
ific
patie
nt g
roup
s an
d th
e ca
re p
ract
ices
for
thes
e gr
oups
mus
t be
iden
tifie
d.
SH.H
B.06
.02
Care
pra
ctic
es a
nd p
roce
dure
s ai
med
at s
peci
fic p
atie
nt g
roup
s m
ust
be d
eter
min
ed.

Standards and Guides
30
Department of Quality, Accreditation and Workers' Rights in Health
ACCR
EDIT
ATIO
N ST
ANDA
RDS
OF H
EALT
HCAR
E SE
T OD
HS
ASPE
CT
CODE
ASPE
CTCH
APTE
R CO
DECH
APTE
RST
ANDA
RD
CODE
STAN
DARD
AC C
ODE
ASSE
SSM
ENT
CRIT
ERIA
(AC)
SHHe
alth
Se
rvic
es
SH.R
G.Ra
diat
ion
Safe
tySH
.RG.
01.0
0M
easu
res
mus
t be
take
n to
ens
ure
radi
atio
n sa
fety
for p
atie
nt/c
arer
s an
d th
e pe
rson
nel.
SH.R
G.01
.01
A co
mm
ittee
mus
t be
esta
blish
ed to
ens
ure
radi
atio
n sa
fety.
SH.R
G.01
.02
The
area
s w
here
ther
e ar
e de
vice
s th
at e
mit
radi
atio
n m
ust b
e id
entif
ied
and
prot
ectiv
e m
easu
res
mus
t be
take
n in
thes
e ar
eas.
SH.R
G.01
.03
Rule
s m
ust b
e de
term
ined
for p
roce
dure
s th
at e
ntai
l the
use
of
radi
atio
n.
SH.P
LPr
osth
esis
La
bora
tory
Se
rvic
es
SH.P
L.01
.00
Phys
ical
env
ironm
ent o
f the
pr
osth
esis
labo
rato
ry m
ust b
e ar
rang
ed s
o as
to e
nsur
e sa
fety
of
the
pros
thes
is a
nd th
e pe
rson
nel.
SH.P
L.01
.01
The
area
s th
at h
ave
been
det
erm
ined
for t
he a
dmis
sion
of p
rost
hetic
m
ater
ials
into
the
pros
thes
is la
bora
tory
, the
pre
para
tion
of th
e m
ater
ial
for t
he p
roce
dure
, its
bei
ng p
roce
ssed
and
for t
he d
eliv
ery
mus
t be
arra
nged
so
as to
ens
ure
the
safe
ty o
f the
pro
sthe
sis.
SH.P
L.01
.02
A he
alth
y w
ork
envi
ronm
ent m
ust b
e en
sure
d in
all
area
s in
the
pros
thes
is la
bora
tory
.
SH.P
L.02
.00
The
proc
esse
s th
at p
rece
de th
e fa
bric
atio
n of
pro
sthe
sis
mus
t be
chec
ked.
SH.P
L.02
.01
The
met
hods
and
rules
for t
rans
fer o
f pro
sthe
tic m
ater
ial to
the
pros
thes
is
labor
ator
y, its
adm
issio
n in
to th
e lab
orat
ory
and
its p
repa
ratio
n be
fore
the
proc
edur
e m
ust b
e id
entif
ied.
SH.P
L.02
.02
Rule
s o
n th
e re
new
al o
f im
pres
sion
whe
n ne
cess
ary
mus
t be
det
erm
ined
and
the
rele
vant
den
tists
mus
t be
prov
ided
with
in
form
atio
n.
SH.P
L.02
.03
The
rele
vant
hea
lth p
erso
nnel
mus
t be
prov
ided
with
gen
eral
in
form
atio
n on
the
proc
edur
es c
ondu
cted
in p
rost
hesi
s la
bora
tory
and
w
ith tr
aini
ng o
n sa
fe tr
ansf
er o
f pro
sthe
tic m
ater
ial,
its a
dmis
sion
into
pr
osth
esis
labo
rato
ry a
nd it
s pr
epar
atio
n be
fore
the
proc
edur
e.
SH.P
L.03
.00
The
proc
esse
s re
gard
ing
the
fabr
icat
ion
of p
rost
hesi
s m
ust b
e ch
ecke
d.
SH.P
L.03
.01
The
met
hods
and
rule
s ab
out t
he p
roce
sses
rega
rdin
g fa
bric
atio
n of
pr
osth
esis
in p
rost
hesi
s la
bora
torie
s m
ust b
e id
entif
ied.
SH.P
L.03
.02
Rule
s re
gard
ing
effe
ctiv
e an
d sa
fe u
se o
f the
pro
sthe
tic m
ater
ial i
n pr
osth
esis
labo
rato
ries
and
othe
r mat
eria
ls a
nd d
evic
es m
ust b
e id
entif
ied.
SH.P
L.03
.03
Qual
ity c
ontro
l pro
cedu
res
rega
rdin
g th
e su
itabi
lity
of th
e pr
osth
esis
m
ust b
e id
entif
ied
and
impl
emen
ted.

Standards and Guides
31
Standards of Accreditation in Health - ODHS Kit
ACCR
EDIT
ATIO
N ST
ANDA
RDS
OF H
EALT
HCAR
E SE
T OD
HS
ASPE
CT
CODE
ASPE
CTCH
APTE
R CO
DECH
APTE
RST
ANDA
RD
CODE
STAN
DARD
AC C
ODE
ASSE
SSM
ENT
CRIT
ERIA
(AC)
SHHe
alth
Se
rvic
es
SH.P
LPr
osth
esis
La
bora
tory
Se
rvic
es
SH.P
L.04
.00
The
proc
esse
s th
at fo
llow
the
fabr
icat
ion
of p
rost
hesi
s m
ust b
e ch
ecke
d.
SH.P
L.04
.01
The
pros
thes
is th
at h
as b
een
com
plet
ed m
ust b
e de
liver
ed w
ith
Pros
thes
is D
eliv
ery
Repo
rt.
SH.P
L.04
.02
The
pros
thes
is m
ust b
e in
sert
ed w
ithin
the
set t
ime
of d
eliv
ery.
SH.P
L.04
.03
Patie
nts
mus
t be
info
rmed
abo
ut th
e ru
les
rega
rdin
g th
e us
e of
pr
osth
esis
.
SH.P
L.05
.00
Trac
eabi
lity
of th
e pr
oces
ses
rega
rdin
g pr
osth
esis
labo
rato
ry
mus
t be
ensu
red.
SH
.PL.
05.0
1Re
cord
s m
ust b
e ke
pt to
ens
ure
trace
abilit
y of
the
impr
essi
on a
nd th
e pr
osth
esis
in a
ll th
e pr
oces
ses.
SH.G
CSu
rgic
al S
afet
y
SH.G
C.01
.00
Patie
nt s
afet
y m
ust b
e en
sure
d in
su
rgic
al p
roce
dure
s.SH
.GC.
01.0
1M
easu
res
mus
t be
take
n to
ens
ure
patie
nt s
afet
y be
fore
, dur
ing
and
afte
r the
sur
gica
l pro
cedu
re.
SH.G
C.02
.00
Cond
ition
s of
the
oper
atin
g ro
om
mus
t be
appr
opria
te to
ens
ure
safe
su
rger
y.
SH.G
C.02
.01
Rule
s re
gard
ing
oper
atin
g ro
oms
mus
t be
dete
rmin
ed.
SH.G
C.02
.02
Oper
atin
g ro
oms
mus
t be
arra
nged
so
as to
ens
ure
patie
nt a
nd
empl
oyee
saf
ety.
SH.G
C.02
.03
Man
agem
ent o
f dru
gs, m
ater
ial a
nd d
evic
es m
ust b
e en
sure
d.
SH.G
C.02
.04
Mea
sure
s m
ust b
e ta
ken
to e
nsur
e un
inte
rrup
ted
pow
er s
uppl
y.

Standards and Guides
32
Department of Quality, Accreditation and Workers' Rights in Health
ACCR
EDIT
ATIO
N ST
ANDA
RDS
OF H
EALT
HCAR
E SE
T OD
HS
ASPE
CT
CODE
ASPE
CTCH
APTE
R CO
DECH
APTE
RST
ANDA
RD
CODE
STAN
DARD
AC C
ODE
ASSE
SSM
ENT
CRIT
ERIA
(AC)
DHSu
ppor
t Se
rvic
esDH
.OH
Acco
mm
odat
ion
Serv
ices
DH.O
H.01
.00
All t
he a
reas
at O
DHC
mus
t be
cle
an fo
r the
saf
ety
and
satis
fact
ion
of p
atie
nt, c
arer
and
pe
rson
nel.
DH.O
H.01
.01
Ris
k le
vels
mus
t be
dete
rmin
ed in
all
the
area
s of
ODH
C to
ens
ure
the
cont
rol o
f cle
anin
g an
d in
fect
ions
.
DH.O
H.01
.02
Clea
ning
rule
s fo
r ris
k le
vels
mus
t be
iden
tifie
d an
d an
ODH
C cl
eani
ng
plan
mus
t be
deve
lope
d an
d pu
t int
o pl
ace.
DH.O
H.02
.00
Proc
esse
s re
gard
ing
cate
ring
for
inpa
tient
/ car
er a
nd th
e pe
rson
nel
mus
t be
iden
tifie
d.
DH.O
H.02
.01
Safe
sup
ply
and
stor
age
of th
e fo
od m
ust b
e en
sure
d.
DH.O
H.02
.02
Proc
esse
s re
gard
ing
prep
arat
ion
of th
e fo
od u
nder
the
set c
ondi
tions
m
ust b
e id
entif
ied.
DH.O
H.02
.03
Food
mus
t be
dist
ribut
ed a
ccor
ding
to th
e se
t rul
es.
DH.O
H.02
.04
Heal
th s
cree
ning
of t
he p
erso
nnel
dis
tribu
ting
the
food
mus
t be
cond
ucte
d.
DH.O
H.03
.00
Laun
dry
serv
ices
mus
t be
prov
ided
in
a s
afe
and
effic
ient
man
ner
to e
nsur
e pa
tient
and
per
sonn
el
heal
th a
t ODH
C.
DH.O
H.03
.01
Proc
esse
s re
gard
ing
the
deliv
ery
of la
undr
y se
rvic
es m
ust b
e id
entif
ied.
DH.O
H.03
.02
The
laun
dry
room
mus
t be
arra
nged
so
as to
ens
ure
effic
ient
con
duct
of
ser
vice
pro
cess
es.
DH.O
H.03
.03
Rule
s re
gard
ing
the
use
of la
undr
y eq
uipm
ent m
ust b
e de
term
ined
.
DH.O
H.04
.00
Patie
nt/e
xam
inat
ion
room
s an
d th
e ar
eas
used
by
patie
nts/
care
rs m
ust
be s
afe
and
ergo
nom
ic.
DH.O
H.04
.01
All
depa
rtm
ents
pro
vidi
ng s
ervi
ce m
ust b
e de
sign
ed in
a w
ay th
at
ensu
res
com
fort
of t
he p
atie
nt.
DH.O
H.04
.02
Act
ion
mus
t be
take
n to
ens
ure
easy
acc
ess
of th
e pa
tient
to th
e re
leva
nt h
ealth
per
sonn
el.
DH.O
H.05
.00
Safe
ty/s
ecur
ity s
ervi
ces
mus
t be
prov
ided
in O
DHC
to e
nsur
e sa
fety
of
life
and
pro
pert
y of
pat
ient
/car
er
and
the
pers
onne
l.
DH.O
H.05
.01
Proc
esse
s re
gard
ing
the
deliv
ery
of S
afet
y/Se
curit
y se
rvic
es m
ust b
e id
entif
ied.
DH.O
H.05
.02
Saf
ety
of li
fe a
nd p
rope
rty
of th
e pa
tient
/car
er in
ODH
C m
ust b
e en
sure
d.

Standards and Guides
33
Standards of Accreditation in Health - ODHS Kit
ACCR
EDIT
ATIO
N ST
ANDA
RDS
OF H
EALT
HCAR
E SE
T OD
HS
ASPE
CT
CODE
ASPE
CTCH
APTE
R CO
DECH
APTE
RST
ANDA
RD
CODE
STAN
DARD
AC C
ODE
ASSE
SSM
ENT
CRIT
ERIA
(AC)
DHSu
ppor
t Se
rvic
es
DH.T
YFa
cilit
y M
anag
emen
tDH
.TY.
01.0
0
A qu
ality
faci
lity
man
agem
ent
stru
ctur
e an
d pr
oces
s m
ust b
e es
tabl
ishe
d to
ens
ure
the
qual
ity
and
safe
ty o
f hea
lthca
re s
ervi
ces.
DH.T
Y.01
.01
A co
mm
ittee
resp
onsi
ble
for p
lann
ing
and
coor
dina
ting
activ
ities
rela
ted
to fa
cilit
y m
anag
emen
t mus
t be
form
ed.
DH.T
Y.01
.02
Risk
s or
igin
atin
g fro
m th
e fa
cilit
y m
ust b
e de
tect
ed a
nd n
eces
sary
m
easu
res
mus
t be
take
n.
DH.T
Y.01
.03
Cont
inui
ty a
nd s
afet
y of
cor
e fa
cilit
y re
sour
ces
mus
t be
ensu
red.
DH.T
Y.01
.04
Issu
es re
late
d to
phy
sica
l con
ditio
ns a
nd o
pera
tions
mus
t be
revi
ewed
pe
riodi
cally
.
DH.T
Y.01
.05
Ther
e m
ust b
e ar
rang
emen
ts fa
cilit
atin
g ac
cess
to d
epar
tmen
ts in
side
OD
HC.
DH.T
Y.01
.06
Mea
sure
s m
ust b
e ta
ken
to fa
cilit
ate
acce
ss to
ser
vice
s by
pat
ient
s w
ho a
re d
isab
led,
old
or i
n ne
ed o
f hel
p du
e to
illn
ess.
DH.T
Y.01
.07
Phys
ical
arr
ange
men
ts m
ust b
e m
ade
to e
nsur
e th
e co
mfo
rt o
f ser
vice
us
ers.
DH.A
YW
aste
M
anag
emen
tDH
.AY.
01.0
0
Safe
and
effe
ctiv
e m
anag
emen
t of
was
te p
rodu
ced
at O
DHC
mus
t be
ens
ured
to p
rote
ct h
uman
and
en
viro
nmen
tal h
ealth
.
DH.A
Y.01
.01
A W
aste
Man
agem
ent P
lan
mus
t be
prep
ared
.
DH.A
Y.01
.02
Was
te m
ust b
e so
rted
at t
he s
ourc
e.
DH.A
Y.01
.03
Nece
ssar
y st
eps
mus
t be
take
n to
ens
ure
that
was
te is
tran
spor
ted,
te
mpo
raril
y st
ored
and
dis
pose
d in
app
ropr
iate
con
ditio
ns.
DH.A
Y.01
.04
Pers
onne
l inv
olve
d in
was
te m
anag
emen
t mus
t be
train
ed.

Standards and Guides
34
Department of Quality, Accreditation and Workers' Rights in Health
ACCR
EDIT
ATIO
N ST
ANDA
RDS
OF H
EALT
HCAR
E SE
T OD
HS
ASPE
CT
CODE
ASPE
CTCH
APTE
R CO
DECH
APTE
RST
ANDA
RD
CODE
STAN
DARD
AC C
ODE
ASSE
SSM
ENT
CRIT
ERIA
(AC)
DHSu
ppor
t Se
rvic
es
DH.B
YIn
form
atio
n M
anag
emen
tDH
.BY.
01.0
0A
safe
and
effe
ctiv
e in
form
atio
n m
anag
emen
t sys
tem
mus
t be
pres
ent a
t ODH
C.
DH.B
Y.01
.01
Thos
e in
cha
rge
of c
arry
ing
out a
nd c
oord
inat
ing
activ
ities
rela
ted
to
info
rmat
ion
man
agem
ent m
ust b
e id
entif
ied.
DH.B
Y.01
.02
The
nece
ssar
y te
chni
cal a
nd s
uppo
rtin
g in
frast
ruct
ure
mus
t be
esta
blis
hed
for t
he e
ffici
ency
of i
nfor
mat
ion
man
agem
ent.
DH.B
Y.01
.03
Mea
sure
s m
ust b
e ta
ken
for t
he s
ecur
ity o
f med
ical
reco
rds
that
are
ph
ysic
ally
sto
red.
DH.B
Y.01
.04
Nece
ssar
y m
easu
res
mus
t be
take
n to
ens
ure
info
rmat
ion
secu
rity
and
conf
iden
tialit
y.DH
.BY.
01.0
5It
mus
t be
ensu
red
that
the
info
rmat
ion
is ti
mel
y an
d co
ntin
ual.
DH.B
Y.01
.06
Pers
onne
l mus
t be
train
ed fo
r effe
ctiv
e us
e of
info
rmat
ion
man
agem
ent.
DH.M
CM
ater
ial
and
Devi
ce
Man
agem
ent
DH.M
C.01
.00
Effic
ient
, effe
ctiv
e an
d sa
fe u
se
of m
ater
ials
and
dev
ices
mus
t be
ensu
red.
DH.M
C.01
.01
Thos
e in
cha
rge
of m
anag
emen
t of m
ater
ials
and
dev
ices
mus
t be
dete
rmin
ed.
DH.M
C.01
.02
Mat
eria
ls a
nd d
evic
es m
ust b
e de
term
ined
and
sup
plie
d in
acc
orda
nce
with
the
need
s of
the
inst
itutio
n.
DH.M
C.01
.03
Mat
eria
ls m
ust b
e co
nser
ved
in p
rope
r con
ditio
ns.
DH.M
C.01
.04
Nece
ssar
y ph
ysic
al c
ondi
tions
mus
t be
met
to e
nsur
e th
at th
e de
vice
s w
ork
in p
rope
r wor
king
con
ditio
ns.
DH
.MC.
01.0
5Pe
rson
nel m
ust b
e tra
ined
in m
ater
ial a
nd d
evic
e m
anag
emen
t.
DH.D
KOu
tsou
rcin
gDH
.DK.
01.0
0
The
serv
ices
pro
vide
d th
roug
h ou
tsou
rcin
g m
ust b
e in
line
with
th
e co
re p
olic
ies
and
valu
es
of O
DHC
and
Stan
dard
s of
Ac
cred
itatio
n in
Hea
lth.
DH.D
K.01
.01
The
serv
ices
to b
e ou
tsou
rced
mus
t be
dete
rmin
ed in
line
with
the
core
po
licie
s an
d va
lues
of
ODHC
.
DH.D
K.01
.02
Scop
e an
d pr
oces
s of
the
outs
ourc
ed s
ervi
ces
mus
t be
defin
ed.
DH.D
K.01
.03
It m
ust b
e en
sure
d th
at o
utso
urce
d se
rvic
es w
ill co
mpl
y w
ith H
ealth
Ac
cred
itatio
n St
anda
rds
Nece
ssar
y m
aint
enan
ce, c
alib
ratio
n, a
djus
tmen
ts a
nd te
sts
of th
ede
vice
s ne
eded
mus
t be
cond
ucte
d.Ru
les
mus
t be
set t
o en
sure
saf
e an
d ef
fect
ive
use
of m
ater
ials
a nd
dev
ices
, th
e ne
cess
ary
prot
ectiv
e m
ater
ial a
nd in
form
atio
n co
ncer
ning
the
devi
ces
mus
t be
avai
labl
e.
Trac
eabi
lity
of m
edic
al d
evic
es m
ust b
e pr
ovid
ed.
DH.M
C.01
.06
DH.M
C.01
.07
DH.M
C.01
.08

Standards and Guides
35
Standards of Accreditation in Health - ODHS Kit
ACCR
EDIT
ATIO
N ST
ANDA
RDS
OF H
EALT
HCAR
E SE
T OD
HS
ASPE
CT
CODE
ASPE
CTCH
APTE
R CO
DECH
APTE
RST
ANDA
RD
CODE
STAN
DARD
AC C
ODE
ASSE
SSM
ENT
CRIT
ERIA
(AC)
ADEm
erge
ncy
Man
agem
ent
AD.A
DEm
erge
ncy
Man
agem
ent
AD.A
D.01
.00
Mea
sure
s m
ust b
e ta
ken
for t
he
natu
ral d
isas
ters
or e
vent
s w
hich
re
quire
em
erge
ncy
resp
onse
, st
rivin
g, fi
rst a
id o
r eva
cuat
ion.
AD.A
D.01
.01
Nece
ssar
y m
easu
res
mus
t be
dete
rmin
ed b
y ris
k an
alys
is fo
r the
ev
ents
that
requ
ire e
xtra
ordi
nary
resp
onse
, stri
ving
, firs
t aid
or
evac
uatio
n.AD
.AD.
01.0
2Pl
anni
ng m
ust b
e do
ne fo
r pre
vent
ive
mea
sure
s de
term
ined
and
po
ssib
le e
mer
genc
ies.
AD.A
D.01
.03
Trai
ning
s m
ust b
e pr
ovid
ed o
n em
erge
ncy
man
agem
ent a
nd d
rills
mus
t be
con
duct
ed.
AD.A
D.02
.00
Tim
ely
inte
rven
tions
mus
t be
per
form
ed in
the
case
of
resp
irato
ry o
r car
diac
arr
est.
AD.A
D.02
.01
An e
mer
genc
y al
ert s
yste
m d
efin
ed w
ith C
ode
Blue
mus
t be
form
ed fo
r tim
ely in
terv
entio
n in
cas
es o
f res
pira
tory
arre
st a
nd/o
r car
diac
arre
st.
AD.A
D.02
.02
Thos
e in
cha
rge
of m
anag
emen
t of t
he e
mer
genc
y al
ert s
yste
m m
ust
be d
eter
min
ed.
AD.A
D.02
.03
Inte
rven
tion
team
/team
s m
ust b
e de
term
ined
.
AD.A
D.02
.04
Med
icin
es a
nd e
quip
men
t to
be u
sed
in th
e pr
oced
ures
mus
t be
spec
ified
. AD
.AD.
02.0
5Re
cord
s m
ust b
e ke
pt a
bout
inte
rven
tions
per
form
ed.
AD.A
D.02
.06
Code
Blu
e tra
inin
gs m
ust b
e pr
ovid
ed a
nd d
rills
mus
t be
cond
ucte
d.
AD.A
D.03
.00
Tim
ely
inte
rven
tion
mus
t be
ensu
red
in c
ases
whe
re th
e he
alth
pr
ofes
sion
al is
exp
osed
to a
risk
of
vio
lenc
e, o
r an
act o
f vio
lenc
e is
di
rect
ed to
war
ds h
im/h
er.
AD.A
D.03
.01
An e
mer
genc
y ale
rt sy
stem
def
ined
with
Cod
e W
hite
mus
t be
in p
lace
for
inte
rven
tion
in c
ases
whe
re th
ere
is a
risk
or a
nd a
ctua
l act
of v
iolen
ce
tow
ards
hea
lth p
rofe
ssio
nals.
AD
.AD.
03.0
2Th
ose
in c
harg
e of
the
man
agem
ent o
f the
em
erge
ncy
aler
t sys
tem
m
ust b
e de
term
ined
. AD
.AD.
03.0
3In
terv
entio
n te
am/te
ams
mus
t be
dete
rmin
ed.
AD.A
D.03
.04
Code
Whi
te tr
ainin
gs m
ust b
e pr
ovid
ed a
nd d
rills
mus
t be
cond
ucte
d.
AD.A
D.04
.00
Ther
e m
ust b
e an
arr
ange
men
t in
plac
e to
ens
ure
timel
y re
spon
se
to fi
re.
AD.A
D.04
.01
Ther
e m
ust b
e a
fire
dete
ctio
n sy
stem
.
AD.A
D.04
.02
Emer
genc
y al
ert s
yste
m d
efin
ed w
ith C
ode
Red
mus
t be
esta
blis
hed
to
resp
ond
in ti
me
in th
e ca
se o
f fire
.AD
.AD.
04.0
3Th
ose
in c
harg
e of
man
agem
ent o
f the
em
erge
ncy
aler
t sys
tem
mus
t be
det
erm
ined
.
AD.A
D.04
.04
The
equi
pmen
t to
be u
sed
whi
le re
spon
ding
to fi
re, r
ules
rega
rdin
g sa
fe
use
of th
is e
quip
men
t, si
gns
and
inst
ruct
ions
to b
e ta
ken
into
acc
ount
in
the
cas
e of
fire
mus
t be
iden
tifie
d.
AD.A
D.04
.05
Train
ings
mus
t be
prov
ided
on
Code
Red
and
drill
s m
ust b
e co
nduc
ted.


Management and Organization


39
Standard 1
Code Standard Code Assessment Criteria
YO.O
Y.01
.00
An organisational structure to cover all ODHC activities must be established.
YO.O
Y.01
.01
Organisational structure must be defined in a way that covers responsibilities related to governance, financial stewardship.
YO.O
Y.01
.02 All vertical and horizontal relations
in the organisational structure, from senior management to subunits, must be defined.
YO.O
Y.01
.03 Within the organisational structure,
duties, powers and responsibilities of all units and staff must be defined.
YO.O
Y.01
.04
Responsibilities must be identified for units defined in organisational structure.
YO.O
Y.01
.05 An institutional plan should be
established for the activities carried out in line with the organization's aims and objectives.
YO.O
Y.01
.06 Implementation of ODHC
policies,procedures, processes and plans should be provided in all units within the organization structure.
Goal
To identify duties, authorities, responsibilities, liabilities and communication and approval mechanisms in order to attain institutional goals, to ensure sustainability in ODHC functioning, to ensure performance and inspection of the workflow of ODHC in a defined organizational structure
Organizational Structure

Managem
ent and Organization
40
Department of Quality, Accreditation and Workers' Rights in Health
Objectives
» Effectiveness
» Efficiency
» Productivity
» Continuity
Standard Requirements
Establishment of Organisational StructureOrganizational structure of ODHC must be designed in a way that it will lead to the goals and targets defined on the basis of main policy and values. While designing organizational structure in this context, one or several of structure types such as Functional, Sectional or Matrix must be approached by evaluating main elements such as size of ODHC, service type, target group, other related institutions and their positions, internal and external necessities.
The organizational chart should be defined in one or more documents, illustrating the horizontal and vertical relationships among units from the top to the bottom one.
In the organizational scheme, at least topics below must be issued:
» Speciality and division of services
» Responsibilities and relations
» Ways to delegate authority
» Coordination and integration points
» Duties and positions of staff
GovernanceResponsibilities related to governance must be defined including the basic factors listed below:
» Transparency
» Accountability
» Participation
» Responsiveness
» Rule of law

Managem
ent and Organization
41
Standards of Accreditation in Health - ODHS Kit
» Efficiency
» Equality
» Strategic vision
Responsibilities related to clinical governance must be defined including the basic factors listed below:
» Clinical efficiency
» Clinical assessment
» Risk management
» Patient and public participation
» Staff and human resources management
» Education and training
» Use of information
Responsibilities related to financial stewardship must be defined including at least the basic factors listed below:
» Defining budget by institution and unit basis
» Ensuring efficient, economical and efficient use of the budget
» Control and monitoring of expenditures and income / outcome balance
For successful implementation of governance, financial stewardship and clinical governance, an efficient leadership, team work and communication must be ensured in political and clinical processes.
Defining Duties, Powers and Responsibilities of Units and StaffDuties of units and staff included in the organizational scheme must be defined, and their powers and responsibilities must be clarified. Terms of reference must include relations between units as well and must be prepared in such a way as to avoid uncertainty and confusion. Authorities and responsibilities assigned to units and individuals must be consistent.
Determining Unit SupervisorsSupervisors must be determined for the positions from the senior management to subunits.
Establishment of the Institutional PlansAn institutional plan should be established for the activities carried out in line with the organization's aims and objectives. The plan should be compatible with and linked to other institutional plans such as human resources, risk, financial plans.

Managem
ent and Organization
42
Department of Quality, Accreditation and Workers' Rights in Health
Standard 2
Code Standard Code Assessment Criteria YO
.OY.
02.0
0 ODHC must have all necessary authorisation and permits for all its activities
YO.O
Y.02
.01 ODHC must have all necessary
authorization and permits related to institutional services and staff working status for all its activities.
YO.O
Y.02
.02
The current and valid status of the necessary authorization and authorization documents for all services and personnel must be reviewed at least once a year and regularly when necessary.
Goal
To ensure effective check and monitoring of healthcare services and support services provided at ODHC by making sure that these services are delivered only by people and institutions authorized under the national legislation
Objectives
» Effectiveness » Efficiency » Productivity
Standard Requirements
All required authorization and permits described by the national legislation must be determined for all service activities performed by ODHC.
Within this scope;
» ODHC must obtain the required activity permits, licenses, etc at ODHClevel and/or service area level;
» All activities consisting of traditional, complementary, alternativemedicine practices and all other services provided apart fromhealthcare services (administrative, technical, etc.) must be performedby people authorised (diploma, certificate, specialty certificates, etc.)in the framework of all national health policies, legislation and otherlegal regulations. This authorization requirement applies to all staffincluding permanent, temporary, voluntary and casual employees.
» Authorisation documents issued to the work area of the employees must be verified

43
Code Standard Code Assessment Criteria
YO.P
D.01
.00 Core policies
and ethical values of ODHC must be defined.
YO.P
D.01
.01
Mission, vision and ethical values of ODHC must be defined in a clear and understandable manner.
YO.P
D.01
.02
ODHC must share its mission, vision and ethical values with the public.
YO.P
D.01
.03
Corporate goals and objectives must be determined in accordance with mission, vision and values, the objectives of the medical and administrative departments should be compatible with the basic policies and values of the ODHC.
YO.P
D.01
.04
Service planning towards the achievement of institutional goals and objectives in ODHC must be made taking environmental and financial factors into account as well.
YO.P
D.01
.05 An efficient budgeting (income/
expense budget) must be in place in order to attain goals and objectives set.
YO.P
D.01
.06
ODHC must review and assess its institutional resources at regular intervals by taking into consideration plans prepared and budgets drafted with the aim of realising such plans.
Core Policies and Ethical Values

Managem
ent and Organization
44
Department of Quality, Accreditation and Workers' Rights in Health
Goal
To define principles to guide executives and staff in relation to institution’s activities and strategic decisions by determining core policies and ethical values of ODHC.
Objectives
» Efficiency
» Effectiveness
» Productivity
Standard Requirements
Determining Mission, Vision and Ethical Values» Mission and vision of institution must be determined based
on information obtained with analysis of internal and externalenvironmental conditions, and conditions that ODHC intends to attain.
» ODHC must determine ethical values which include principles andrules that will lead all its activities. Issues such as ethical principlesand rules of conduct, principles which highlight the focus on patientand staff, can be addressed within the scope of ODHC ethical values.
» ODHC must pay attention to ensure that its core policies and ethicalvalues are compatible with minimum ethical values of its staff andservice receivers.
Sharing Core policies and ethical values with the Public» Mission, vision and ethical values of ODHC must be shared by the
institution with the public periodically by using various communicationtools (website, boards, promotion activities, etc.).
Determining Goals and Objectives» ODHC must determine its goals and objectives by institution and unit
on the basis of core policies and ethical values.

Managem
ent and Organization
45
Standards of Accreditation in Health - ODHS Kit
» The objectives of the medical and administrative departments should be in line with the objectives of the institution.
» Activities of ODHC must be planned and implemented on the basis of goals and objectives set by the institution and units.
Service PlanningGoals and objectives determined by the institution and units must be taken as basis for planning ODHC activities.
During planning, internal factors (human resources, financial status, size, diversity of services, structural conditions, etc.), external factors (legal environment, corporate relations, public health structure, suppliers, competitors, etc.), features and feedbacks of service users, employees and society must be taken into account.

46
Quality Management Structure
Code Standard Code Assessment Criteria
YO.K
Y.01
.00
Planning, implementation, coordination and continuity of quality improvement activities must be ensured.
YO.K
Y.01
.01
A management structure must be established in order to ensure the planning, implementation, coordination and continuity of quality improvement activities
YO.K
Y.01
.02 The duties, powers and responsibilities
of those involved in the management structure must be defined.
YO.K
Y.01
.03 The managerial structure should
ensure the planning, execution and coordination of quality improvement activities.
YO.K
Y.01
.04
Committees must be established concerned with at least the following topics: » Employee safety» Patient safety» Training» Facility management» Prevention of infections» Radiation safety
Goal
To establish a quality management structure by defining the roles and responsibilities of all the staff from senior management to unit employees at ODHC in quality improvement activities; to ensure that quality is continuously improved through the planning, implementation and coordination of quality improvement activities within this structure.

Managem
ent and Organization
47
Standards of Accreditation in Health - ODHS Kit
Objectives
» Efficiency
» Effectiveness
» Productivity
» Continuity
Standard Requirements
Management Structure Related to Quality
» An management structure must be established within ODHC to ensureplanning, implementation, coordination and continuity of qualityimprovement activities.
» The duties, authorities and responsibilities of people involved in themanagement structure, and the vertical and horizontal relations of thisstructure must be defined.
» Quality supervisors to work in coordination with this managementstructure must be determined on the basis of units and/or processes.
The Planning, Execution and Coordination of Quality Improvement Activities
» Within the framework of Standards of Accreditation in Health, atleast the following activities must be carried out to ensure planning,implementation and coordination of quality improvement activities:
• Ensuring planning and implementation of measurement,assessment, improvement and monitoring activities
√ Defining and implementing processes related to self-assessment (at least twice a year to cover all processes andsections)
√ Defining and implementing the scope and processesconcerning
Patient/employee satisfaction surveys [at least twice a yearand in a way to cover different service areas (outpatient,inpatient, etc.) of ODHC and, to reflect specific expectationsfrom and perception of the specific service area]

Managem
ent and Organization
48
Department of Quality, Accreditation and Workers' Rights in Health
√ Defining and implementing processes with the aim of obtaining patients’/staff’s opinions and suggestions
√ Monitoring performance related to quality improvement activities through indicators; planning and monitoring of activities aiming at the use of results obtained from such study for the purpose of improvement
√ Monitoring the results of the external evaluations carried out within ODHC and defining and implementing processes so that the results can be used for the benefit of the institution
• Monitoring the activities of the committee and coordinating relevant committees
• Defining documentation processes related to quality activities, setting a documentation system, and ensuring its implementation within the rules required by the system
• Monitoring and coordinating unit- and/or process-based quality activities performed in cooperation with unit and/or process quality supervisors
Forming Quality Committees» Within the scope of SAS ODHS, committees must be established in
relation to at least following issues (committees can be merged in line with ODHC size and conditions):
• Employee Safety
• Patient Safety
• Training
• Facility Management
• Prevention of Infections
• Radiation Safety
» Processes must be defined in order to ensure the cooperation and coordination of committees with other committees.

49
Document Management
Code Standard Code Assessment Criteria
YO.D
Y.01
.00 Management of
documents at ODHC must be ensured.
YO.D
Y.01
.01 Policies, procedures, processes and
plans related to all main functions covered by the SAS ODHS set should be documented.
YO.D
Y.01
.02
Format of documents must be determined.
YO.D
Y.01
.03 Preparation, check, approval, up-
to-datedness and maintenance of documents must be ensured.
YO.D
Y.01
.04
Rules to communicate documents to relevant people must be set.
YO.D
Y.01
.05 Process related to monitoring of
external documents to be followed by ODHC must be defined.
Goal
To manage quality activities efficiently by planning and putting into writing practice-related procedures and by conducting practices in line with written rules

Managem
ent and Organization
50
Department of Quality, Accreditation and Workers' Rights in Health
Objectives
» Efficiency
» Effectiveness
Standard Requirements
Establishment of Document Management System
» Processes related to management of documents and rules related to operation of these processes must be defined:
» Definition must entail at least following processes:
• Determining the documents to be prepared
• Determining the format of the document
√ Document Preparation
√ Check and approval of documents
√ Communication of documents to relevant people
√ Document Storage
√ Document Revision
√ Archiving and disposal of documents
• External document tracking
Determining documents to be prepared
» Documents to be prepared must be determined taking into consideration Standards of Accreditation in Health, ODHC size, areas of service provision and processes.
» Policies, procedures, processes and plans related to all main functions of ODHC must be documented.
» Types of documents which can be prepared in line with SAS ODHS are as follows:

Managem
ent and Organization
51
Standards of Accreditation in Health - ODHS Kit
• Procedure
• Instruction
• Guideline
• Form
• Plan
• Consent
• List
• Support documents:
√ Policy
√ Protocol
√ Objectives
√ Duty-Authority-Responsibility
√ Clinical Guidelines
√ Work flow
√ Report of Medicine Disposal
√ Meeting Minutes
Determining the Format of the Document» All documents must include at least the following information:
√ Document name
√ Document code
√ Publication date
√ Revision date
√ Revision number
√ Page number/number of pages
√ Prepared By – Checked By – Approved By details
» In original copy of documents, position and title of individual(s) must be indicated in the section Prepared by – Checked by – Approved by.

Managem
ent and Organization
52
Department of Quality, Accreditation and Workers' Rights in Health
Preparing Documents» Documents must be prepared in accordance with the SAS ODHS
form.
» Document must be prepared by relevant unit/committee/team members.
» Documents must be easy to understand, include concise information and must be clear.
Check and Approval of Documents» Documents must be checked by the quality management unit and
must be approved by the senior management.
Communicating Documents to Relevant People» It must be ensured that the up-to-date versions of the documents are
shared with relevant staff effectively.
» Necessary training must be provided for relevant staff on the documents prepared.
» Unless required, display of documents on boards must be avoided. Attention must be paid in order to ensure that documents displayed do not cause visual pollution.
Storage of Documents» All original documents with wet signs must be stored by the quality
management unit. Original Documents must be stored in line with a systematic filing plan and necessary measures must be taken to keep contents of documents readable.
» Documents in the form of records related to actions taken in line with SAS ODHS (corrective/preventive activity forms, minutes of meeting, etc.) must also be kept.
Revision of Documents» Whenever there is a change in any of the processes of ODHC, revision
must be made immediately.
» During revision, all rules to be followed in the initial preparation of the document must be observed. Following the management approval,

Managem
ent and Organization
53
Standards of Accreditation in Health - ODHS Kit
the revised document must be published, it must be communicated to relevant people, and the revised document must be explained to relevant people within the scope of a training.
» Revision date and revision number must be indicated on the document revised. In the first publication of the document, revision number must be (0) and revision date must be kept blank. Old versions of documents must be archived by the Quality Management Unit in order to track revisions.
» A list of all documents used in ODHC must be kept and the list must enable the tracking of revisions as well. Document list must include following information:
• Document Name
• Document Code
• Publication Date
• Revision Dates
• Revision Number
External Document TrackingTracking and up-to-datedness of external documents must be ensured through a method determined by ODHC. ODHC must identify supervisors in charge of the tracking of external documents.
Archiving and Disposal of DocumentsRules for archiving and destruction of documents should be specified.

54
Adverse Event Reporting System
Code Standard Code Assessment Criteria
YO.O
B.01
.00
RReporting of adverse events that may (near miss) or does (adverse) affect the safety of patients and staff negatively must be ensured, and necessary measures must be taken.
YO.O
B.01
.01 A system must be established in
order to report adverse events that may or does affect the safety of patients and staff negatively.
YO.O
B.01
.02
Case specific analysis must be conducted, and actions must be taken if necessary.
YO.O
B.01
.03
Notifications made to the system must be analyzed, reported and evaluated.
Goal
To ensure that adverse events related to patient and staff safety with a potential to occur (near misses) or occur in ODHC are reported; to monitor them and to take necessary measures against events as a result of reports
Objectives
» Patient safety
» Healthy Working Life

Managem
ent and Organization
55
Standards of Accreditation in Health - ODHS Kit
Standard Requirements
Adverse Event Reporting System
» A reporting system must be established in order to analyze events to take necessary measures and to prevent the repetition of errors by ensuring the reporting of events that may or does harm employees and patients at ODHC or have been noticed before the occurrence of harm.
» Under the scope of the adverse event reporting system, notification, analysis and reporting processes must be defined and supervisors in charge of these processes must be identified.
» Adverse Event Reporting System must consist of two modules:
• Patient Safety Module (Issues threatening the safety of carers and visitors must be notified in this model as well)
• Staff Safety Module
» For the purpose of increasing efficiency and use of the system, cultivating a reporting culture at ODHC, learning lessons from events, developing learning process and devising solutions and encouraging the implementation of solutions; the system must be:
• Designed in a way that makes the staff feel safe, provide information such as name and location when needed,
• Based on voluntary reporting
• Accessible
• Easy to use
• Simple and easy to understand
» Patient safety module must be based on privacy. This module must be designed to collect at least the following information:
• Subject of the event
• Narration of the event
• Comments and suggestions related to event

Managem
ent and Organization
56
Department of Quality, Accreditation and Workers' Rights in Health
Analysis and Improvements» Notifications to the Adverse Event Reporting System must be analyzed
on a case-by-case basis, improvement activities must be planned and implemented after analysis.
» General analysis of notifications to the system must be repeated regularly, reported and evaluated. According to evaluation as a result of general analysis, necessity of unit- or process-based improvement activities must be determined.
» All staff members must be informed about the importance of notification for patient and staff safety, how to do it and improvement activities carried out as a result of notifications.

57
Risk Management
Code Standard Code Assessment Criteria
YO.R
Y.01
.00 Risks related
to ODHC and services provided must be managed.
YO.R
Y.01
.01 There must be a regulation related to
managing the risks that may occur in an ODHC.
YO.R
Y.01
.02 A risk management plan must be
prepared in order to manage risks related to ODHC and services provided.
YO.R
Y.01
.03
Risk management plan must entail the following issues:» Patients » Relatives» Carers » Visitors» Staff » Facility safety» Environmental safety» Administrative and financial processes. » Strategic risks» Comminucation processes withStakeholders
YO.R
Y.01
.04 Risks to be addressed within the
scope of risk management must be determined, analysed and risk levels must be identified.
YO.R
Y.01
.05 Necessary measures must be
adopted in line with the according to the risk level identified, and actions must be taken for improvement.
YO.R
Y.01
.06 Risks identified and effectiveness
of improvement actions must be reviewed periodicially.
YO.R
Y.01
.07 Indicators for monitoring the
effectiveness of risk management must be determined and monitored.

Managem
ent and Organization
58
Department of Quality, Accreditation and Workers' Rights in Health
Goal
To prevent or minimize risks related to ODHC and services provided within the scope of patient, staff, facility safety and environmental safety and administrative/financial processes.
Objectives
» Patient Safety » Healthy Working Life
» Efficiency » Effectiveness
Standard Requirements
Scope of the Risk ManagementRisk management must cover patient, employee, facility and environmental safety including administrative and financial processes.
Risk management must include all physical, chemical, biological, ergonomic, psychosocial factor and service based risks that may be faced in an ODHC.
Policies, processes and methods regarding risk management must be defined in relevant documents.
In risk management procedure, at least the following terms must be defined:
» Goals and objectives» Scope» Risk management method» Obtaining opinions of the relevant employees» Reporting of the defined risks» Analysis of the defined risks, risk level detection and keeping records» Management of processes regarding required improvement actions
Risk Management PlanRisk management plan aims reviewing and observation of the risks.
The plan must cover at least the following topics:

Managem
ent and Organization
59
Standards of Accreditation in Health - ODHS Kit
» Process, action or factor in which the risk is evaluated
» Detected risks relevant to processes, actions or factors mentioned at the previous article
» Designated risk levels
» Precautions against the risks
» Responsible staff
» Designated time period for precautions
All defined risks must be registered in scope of the risk management plan. Risk record is a live document which needs to be updated regularly.
Identification and Analysis of Risks» Taking into consideration the risk management scope, risks must be
identified on the basis of unit, person and/or process.
» Clinical risk evaluations must be conducted to protect patients against adverse results (risk of allergy, fall risks, risks arising from devices etc.).
» Risks must be analysed in line with the method determined by the institution.
» Risk analysis method must be simple and easy to understand and implement.
» Risk levels must be rated in at least three categories (Low, medium, high) considering the possibility to occur and potential effects.
Improvement Actions» According to identified risk levels, measures must be adopted on the basis
of unit, person and/or process, and improvement actions must be taken.
Monitoring the Effectiveness of Risk Management» Risks identified within the framework of risk management and
effectiveness of improvement actions must be reviewed periodically.
» Indicators for monitoring the effectiveness of risk management must be determined and monitered.
» Sustainability of measures taken must be ensured to achieve effectiveness in risk management effectiveness.
» Risk analysis must be updated periodically (at least once a year) or when necessary.

60
Training Management
Code Standard Code Assessment Criteria
YO.E
Y.01
.00
In accordance with quality improvement activities, training needs of patients, carers and staff must be determined, and it must be ensured that necessary training is conducted effectively.
YO.E
Y.01
.01 A committee in charge of the planning
and coordination of training activities must be established.
YO.E
Y.01
.02
Training needs must be identified on the basis of patients, carers and staff.
YO.E
Y.01
.03 Training plans must be prepared and
implemented in line with training needs.
YO.E
Y.01
.04 Effectiveness of training plans
and trainings carried out must be monitored and necessary improvement actions must be taken.
Goal
To deliver necessary trainings to patient/carer and staff efficiently and effectively in line with quality improvement activities of ODHC
Objectives
» Efficiency » Effectiveness » Continuity
» Relevance » Continuity » Productivity

Managem
ent and Organization
61
Standards of Accreditation in Health - ODHS Kit
Standard Requirements
Training Management
» A committee must be formed in order to manage the decision, planning, coordination, communication and evaluation procedures so as to implement effectively and efficiently the necessary trainings which must be provided for quality improvement at ODHC.
» The Committee must determine processes related to trainings and rules concerning the operation of procedures. Within this scope, the minimum processes which must be handled are as follows:
• Identifying training needs
• Preparing training plans
• Implementing the training activities planned
• Monitoring the effectiveness of training plan and trainings conducted and improving them
» Training committee must collaborate with other units and committees which operate under the scope of quality management.
Identifying Training Needs
» In line with the objectives of quality improvement, it must be identified who needs training on which subjects, at what level and scope. While identifying subjects and scope for training needs, the following must be assessed:
• The results of performance evaluation within the scope of quality improvement within ODHC (self-evaluation, data derived from the indicators, etc.)
• Efficiency evaluation results of previous trainings,
• Feedback, requests and observations related to training activities.
» Training subjects must be categorised at least by hierarchical level, occupational group, specific to department and general. It must be identified which training will be delivered to which occupational group and through use of which content. Training subjects must cover at least the following general headings:

Managem
ent and Organization
62
Department of Quality, Accreditation and Workers' Rights in Health
• Quality management trainings
• Patients’ rights training for staff
• Patient and staff safety training for staff
• Risk management training for staff
• Trainings for patients
• Staff compliance trainings
• Device trainings
• Unit-based speciality trainings
• Trainings on new scientific advances
• Trainings for social purposes
• Self-development trainings
Planning and Implementation of Trainings » Training plans must be developed to regulate processes of preparing
content for trainings, determining methods and implementation and evaluation procedures in a systematic manner.
» Training plans must be developed as short-, medium- and long-term plans considering the nature of training need, priority of objectives to be achieved through training, time needed to achieve objectives, institutional policy of ODHC and targets and objectives of change process.
» Training plans must include at least the following:
• Training goals and objectives
• When, to whom and by whom the training will be delivered
• Training method
• Training stages if any (basic training, advanced training, theoretical and practical training, etc.)
• Training location
• Duration of training
• General headings concerning the content of training
• Materials needed for training

Managem
ent and Organization
63
Standards of Accreditation in Health - ODHS Kit
• Methods to evaluate training
» Trainings must be implemented in line with plans.
» Guidelines for general and department orientation training must be prepared and it must be ensured that orientation training is delivered right after a new recruitment is made.
» During the training period, in cases such as arise of a need for a training unforeseen in the plan, a change training content or training method, training plan must be revised in a way that it can be traced back. It must be ensured that staff have access to training materials and resources considered to be appropriate for sharing by training committee.
Evaluation of Training» Compliance with training plan prepared must be monitored, and
measures must be taken to enhance compliance with the plan.
» Efficacy and effectiveness of training programs implemented must be evaluated on the basis of goals and objectives set.
» Evaluation must also cover trainer’s performance.
» Some of the methods that can be used to evaluate the effectiveness and efficiency of training programs implemented are listed below:
• Pre- and post-test
• Self-assessments
• Observations
• Interviews with participants
• Evaluations with unit supervisors
• Questionnaires
• Measurement methods to measure training-induced change in behaviour (such as accepted scales)

64
Social Responsibility
Code Standard Code Assessment Criteria
YO.S
S.01
.00
ODHC, must organize programs for promoting and improving health by taking health structure and general health problems of the society into account.
YO.S
S.01
.01
ODHC, must organize programmes promoting and improving health, in line with the health structure of the region and population it serves, taking into consideration service quality, within the context of national and global health problems.
Goal
To ensure that within the frame of social responsibility, ODHC provides services that promote and improve health and increase the health level of the society that it provides healthcare services for
Objectives
» Patient-orientedness» Relevance» Equity» Effectiveness» Continuity

Managem
ent and Organization
65
Standards of Accreditation in Health - ODHS Kit
Standard Requirements» ODHC must investigate health problems of the region and population
to which it provides healthcare services and national and global health problems. Within this scope, the following must be assessed to identify the current situation:• Demographic data such as population, age, sex, education level• Health statistics including morbidity and epidemiologic data• Clothes, food, cultural and physical activities and social and
cultural structure» Based on the current situation analysis, health promotion and
improvement activities for the target population must be planned under the scope of a programme. ODHC must develop at least two programmes within this scope.
» Results of the programme must be evaluated by ODHC, and how effective the programme is and to what extent it has achieved objectives set must be determined.
» Assessment and effectiveness of the programme must be identified through analysis of the main data at the basis of the programme and the change in information over time, depending on whether the programme is short-, medium- or long-term.
» Improvements must be made and sustainability must be ensured in the programme activities to attain the programme targets in line with assessment results.
Programs to be developed in line with the standard can be organized around the topics listed below or around similar topics:» Fighting smoking» Increasing awareness and knowledge of dental health in society» Training and preventive activities to fight chronic diseases» Healthy diet for a healthy life» Promoting sports among youth for a healthy life» Promoting breastfeeding» Training activities for pregnant women» Cooperation with local administrations in order to fight regional agents
threatening community health» Detection of and information about mouth cancers» Oral and dental health practices for elderly and disabled patients» Oral and dental health practices for chemotherapy and radiotherapy
patients» etc.

66
Institutional Communication
Code Standard Code Assessment Criteria
YO.K
İ.01.
00
Institutional communication activities must be carried out effectively.
YO.K
İ.01.
01
Under the scope of institutional communication, target audience must be identified by taking ODHC structure, core policies and values into account and communication strategies for target audience must be determined.
YO.K
İ.01.
02 Target audience must be informed about ODHC activities and their organisation.
YO.K
İ.01.
03 Necessary actions must be taken to create a positive opinion among target audience.
Goal
To create public opinion based on positive attitude, behaviour towards and trust in ODHC and its activities, to ensure that policies and activities of ODHC are adopted by establishing permanent good relations with its target audience and to improve the effectiveness and quality of services through the feedbacks of target audience.
Objectives
» Patient-orientedness » Equity» Effectiveness » Continuity

Managem
ent and Organization
67
Standards of Accreditation in Health - ODHS Kit
Standard Requirements
Identifying Target Audience and Communication Strategy» Under the scope of institutional communication, target audience must
be identified by taking institution type, size, patient profile, regional features, people and institutions communicated and main policies and values, and communication strategies for target audience must be defined.
» Target audience must be identified by taking internal and external communication stakeholders into account.
» Within the framework of communication strategy, communication rules must be established for target audience within ODHC. Within this scope at least the following issues must be addressed:
• Information and decision flow among units and elements of ODHC
• Information and decision flow in evaluation and inspection functions
• Communication during training and information activities
• Communication during activities aiming at enhancing motivation and taking ownership of institutional identity
Informing Target Audience» Information activities specific to target audience identified must be
conducted
» Activities must be done regarding on-line representation and promotion of the institution. Institutional website must be managed effectively, The website should include adequate and actual information, also should be made easy to use, accessible and available.
» Target audience must be informed about at least the following issues:
• Core policies and values
• Organisational structure
• Service areas
• Activities carried out under the scope of social responsibility
• Human resources

Managem
ent and Organization
68
Department of Quality, Accreditation and Workers' Rights in Health
• Public relations activities
• How to make an appointment
• Communication and travel
• Access to service within ODHC
» Since the staff at ODHC are important representatives for institutional communication they must be trained about the subject.
Creating Positive Public OpinionIn order to create positive public opinion in the target audience, first of all, information activities towards society about services provided and activities carried out must be conducted in line with needs and expectations of target audience.
While these activities can be conducted through information tools, it must be ensured that staff communicates effectively with patients and carers during service provision and senior management represents ODHC effectively outside and establishes good relations.
Monitoring Institutional Communication and PerceptionQuestionnaires about performance of institutional communication activities and in order to measure perception of current identity and image of ODHC in the target audience must be conducted regularly, the results must be evaluated, and necessary actions must be taken to improve institutional communication strategies.

Performance Measurement and Quality Improvement


71
Monitoring of Indicators
Code Standard Code Assessment Criteria
PÖ.G
İ.01.
00
Institutional indicators must be monitored and evaluated in order to continuously improve processes related to service delivery, led by administrative, financial and medical steps.
PÖ.G
İ.01.
01
Indicators must be determined to include processes concerning service delivery, primarily administrative, financial and medical steps.
PÖ.G
İ.01.
02 Indicator cards must be created to cover issues related determination, collection, evaluation and monitoring of data to be used for indicators.
PÖ.G
İ.01.
03 Monitoring, evaluating and reporting of indicators must be carried out through information management systems
PÖ.G
İ.01.
04 Necessary improvements must be made taking into consideration the analysis results for the indicators.
PÖ.G
İ.01.
05 The results of the SAS indicators must be submitted to the SAS Indicator Data System.
Goal
To detect and correct potential problems related to service delivery, primarily administrative, financial and medical processes, and ensure that interventions are carried out to improve quality

Performance M
easurement and Quality Im
provement
72
Department of Quality, Accreditation and Workers' Rights in Health
Objectives
Objectives vary according to the features of indicators.
Standard Requirements
Identifying Indicators
» Institutional indicators must be monitored and evaluated in ODHCconcerning processes related to service delivery in order to improvequality continuously, primarily administrative, financial and medicalsteps.
» In order to continually improve the processes for service delivery, theSAS indicators which has to be monitored according to the type ofinstitution service and patient profile should be determined.
Indicator Cards
Indicator cards must be prepared for indicators identified. Indicator cards should include at least the following information:
» A short description of the indicator
» Reason for monitoring
» Linked process
» Calculation method/formula
» Target value
» Data source
» Data collection period
» Data analysis period
» Supervisors for collecting, monitoring, evaluating and analysing datarelated to indicator
» People to share the results with
» Points of attention concerning indicator

Performance M
easurement and Quality Im
provement
73
Standards of Accreditation in Health - ODHS Kit
Information Management System Infrastructure for Indicator ManagementNecessary information management system infrastructure must be established in the purpose of indicators’ data collection, monitoring and evaluation of results; and must be used effectively.
Collection and Analysis of Data and Improvements It must be ensured that relevant staff members be involved in the data collection and analysis processes.
Based on analysis concerning indicators, required corrective and preventive actions must be planned and implemented.
SAS Indicator Data SystemResults of determined indicators at SAS Indicators List must be Submitted to the SAS Indicator Data System.

Healthy Work Life


77
Human Resources Management
Standard 1
Code Standard Code Assessment Criteria
SÇ.İK
.01.
00
A management structure that will fulfill the requirements concerning planning of human resources, improvement of work life and the personnel must be established.
SÇ.İK
.01.
01 The relation of the management structure with other management levels must be identified.
SÇ.İK
.01.
02 Duties, authorities and responsibilities of those in the management structure and the qualifications they must have must be identified.
SÇ.İK
.01.
03
Annual goals and work plans must be developed.
SÇ.İK
.01.
04
Feedback processes aimed at determining satisfaction levels and comments and suggestions of the personnel regarding their work life must be identified.
Goal
To define a management structure that will perform activities such as assignment, coordination and assessment regarding necessary processes for the establishment of a healthy working life

Healthy Work Life
78
Department of Quality, Accreditation and Workers' Rights in Health
Objectives
» Healthy Work Life » Efficiency
» Efficacy » Productivity
Standard Requirements
Management Structure and Its Relation with Senior Management
» A management structure that will perform all activity planning andcoordination such as employment, orientation, improvement of andsupport to the personnel, providing the personnel with physical andsocial opportunities, minimizing safety risks that threaten employeesand increasing motivation must be established at ODHC.
» Management relations such as where the new management structurewill be in the hierarchy of ODHC management or to whom it will beresponsible, which powers it will have, who will be in this structureand who will be responsible to this structure must be defined.
Duties, Authorities and Responsibilities
Terms of reference must be prepared for people to be involved in management structure, and their responsibilities and authorities must be identified.
» Which qualifications employees involved in the structure musthave must be defined in order to carry out all necessary duties andresponsibilities.
Targets and Planning
» Newly formed management structure must define annual targetsin order to ensure a healthy work life. Key factors such as whichactivities will be carried out, which measures will be taken and howmuch budget will be needed in order to reach the targets must beplanned.

Healthy Work Life
79
Standards of Accreditation in Health - ODHS Kit
Comments and Suggestions from the Staff
» A system identifying in which scope and through which mechanisms feedback will be received from the staff in order to detect the needs and expectations of the staff and to ensure that they participate in the decision mechanisms.
» Activities towards identifying the needs and expectations of the staff must meet at least the following requirements:
• Regularly conducted satisfaction questionnaires
• Personal and face-to-face interviews with the staff
• Taking comments and suggestions from the staff
Standard 2
Code Standard Code Assessment Criteria
SÇ.İK
.02.
00
The requirements necessary to constantly improve recruitment and compliance processes of the personnel and their work life must be determined and fulfilled.
SÇ.İK
.02.
01 A personnel recruitment plan must be developed in line with human resources needs of ODHC.
SÇ.İK
.02.
02
Personnel recruitment processes must be identified.
SÇ.İK
.02.
03 Processes regarding ensuring the adaptation of the newly recruited personnel to ODHC must be identified.
SÇ.İK
.02.
04
Duties, authorities, responsibilities of the personnel and the qualifications they should have and the performance criteria their job requires must be determined.
SÇ.İK
.02.
05
Performance of the personnel must be measured, training needs must be determined to enhance the performance and necessary trainings must be provided.

Healthy Work Life
80
Department of Quality, Accreditation and Workers' Rights in Health
Code Standard Code Assessment Criteria
SÇ.İK
.02.
06
How and to what extent the current standards, protocols and evidence-based clinical guidelines accepted by ODHC are used by the personnel must be monitored and trainings aimed at ensuring the use of these standards and guidelines efficiently must be identified.
Goal
To ensure that needs regarding continuous improving of work life and the processes of recruitment and adaptation of staff are identified and met***
Objectives
» Healthy Work Life » Efficiency
» Efficacy » Productivity
Standard Requirements
Recruitment of Staff
» ODHC must define in which service area and staff with whichqualifications is needed, must determine the feasibility of recruitmentand must plan main processes such as recruitment and training inadvance.
» In recruitment plan, the number and the quality of staff needed(training, knowledge, skills, etc.) must be included consideringdifferent disciplines and professional groups that will be able to meetneeds concerning services to be provided.

Healthy Work Life
81
Standards of Accreditation in Health - ODHS Kit
» Need for staff must be regularly reviewed by preparing terms of references on the basis of departments and processes, and human resources must be planned by taking legal regulations into account. Measures must be taken regarding how recruitment will be made and which qualifications new staff must have and how many people will be recruited.
» Which documents and information is needed in the process of application and recruitment and steps regarding evaluation and approval process must be defined.
» ODHC must inform new recruits about from which facilities of the ODHC they can benefit, opportunities provided and employee rights.
Recruitment Processes
» Recruitment processes in ODHC must be described, and how staff planned to be recruited for previously defined tasks in the departments in need must be defined. Principles and processes regarding recruitment processes must be announced.
Adaptation of Staff
» ODHC must define the processes that will enable new staff, recruited for the position opened in line with the needs, to adapt to the new working environment quickly and accurately. All kind of information such as main and professional rules, basic working principles, elements that may threaten personnel health and safety, hierarchical order and all facilities that may be used by the personnel must be provided to the personnel during recruitment and later regularly.
» Adaptation of staff to job and work environment must be assessed, and if needed, activities towards adaptation must be repeated.
Duties, Powers, Responsibilities and Performance Criteria
» Duties, powers and responsibilities of staff that is working or planned to be recruited must be identified in line with service processes in a way that they will encompass previously defined duties and responsibilities.
Healthy Work Life
82
Department of Quality, Accreditation and Workers' Rights in Health
» Performance criteria defined as the performance of the duties by staffsuccessfully must be identified, and staff should be informed aboutthe criteria.
»
» In order to increase the employee performance, it must be determinedwhich trainings will be provided and what their scope will be in linewith the qualifications and needs of staff and required planning inrelation to training must be done. Objectives of the trainings that willbe provided within this scope must be defined in advance and it mustbe assessed after trainings whether the objectives set have beenattained.
» Only trained and authorized staff must use specific and medicaldevices and in the training plans, the need for training on such issuesmust be taken into account.
» How and to what extent the current standards, protocols and evidencebased clinic guidelines accepted by ODHC are used must be monitoredand trainings must be planned in order to ensure effective utilization ofthe standard and guidelines.
Performance of staff must be measured on the basis of performancecriteria set by ODHC. Performance measurements should be plannedat least once a year.

83
Employee Health and Safety
Code Standard Code Assessment Criteria
SÇ.Ç
G.01
.00
Factors threatening the health and safety of employees should be identified and necessary precautions should be taken to establish a healthy and safe working environment.
SÇ.Ç
G.01
.01
A committee aimed at management of the factors that threaten employee health and safety must be established.
SÇ.Ç
G.01
.02 Risk analyses must be conducted on
the factors that threaten employee health and safety and measures must be taken to eliminate or decrease the risks that threaten the safety.
SÇ.Ç
G.01
.03
It must be ensured that employees use the personal protective equipment against the risks.
SÇ.Ç
G.01
.04
Quality improvement activities that aim to ensure the continuity of employee safety must be planned.
SÇ.Ç
G.01
.05
Physical and social opportunities that are necessary to improve the work environments and the work life must be provided and personal needs of the employee regarding work life must be met.
Goal
To establish healthy work life environment in ODHC by removing or minimizing the elements that threaten the safety of staff

Healthy Work Life
84
Department of Quality, Accreditation and Workers' Rights in Health
Objectives
» Healthy Work Life
Standard Requirements
Committee on Personnel Health and Safety
A committee must be establish to detect threats that exist or may exist against the ODHC personnel and to take measures against those threats. Committee structure must be shaped in line with the size of ODHC and risks posed by safety threats with the aim of ensuring the performance of activities effectively, continuously and systematically and achieving coordination.
Risk Analyses
» First of all, assessment must be performed by identifying the risk factors that threaten the safety in terms of employee safety within ODHC and again by identifying their risk levels. After identifying risk factors, necessary action must be undertaken in order to remove or minimize the detected threats according to their priorities
» In order to secure personnel health and safety at ODHC, at least the following issues must be addressed:
• Developing management policies in relation to health and safety of personnel
• Preventing infections
• Planning and implementation of health screenings
• Chemicals and radiation safety
• Food safety
• Noise
• Lighting
• Falls prevention
• Managing facility-borne risks
• Reducing needle stick injuries.

Healthy Work Life
85
Standards of Accreditation in Health - ODHS Kit
• Ergonomic factors
• Preventing violence against healthcare staff and responding to violence as soon as possible
• Preventing mobbing among staff
• Managing wastes threatening the safety of personnel
• Immunization
• Reducing unnecessary workload
• Stress management
» At ODHC, action must be taken in order to ensure that medical, psychological and other counseling and support services are always available for the staff.
» It must be ensured that near misses and adverse events which threaten employee safety are reported in order to treat staff with occupational disease and injuries.
Personal Protective Equipment
» Which personal safety equipment will be used in which departments must be defined and measures must be taken in order to ensure the use of these equipments.
» It is required that sufficient number of personal safety equipment having protective qualities is made available in designated working areas and trainings are organized for the employees about the operation of such equipment.
Quality Improvement
In order to secure personnel health and safety, ODHCs must plan and implement quality improvement activities in order to remove or avoid the elements that pose risks.
Improving Working Environment
» Improvement plans on issues such as physical environments of the personnel, materials and devices they use, chemical, physical and biological materials and working methods must be planned by taking personnel expectations into account.

Healthy Work Life
86
Department of Quality, Accreditation and Workers' Rights in Health
» Achieving harmony between duties and employees’ physical and mental capacities
» In order to reach an adequate level of health and safety; activities and trainings in order to encourage employees’ professional improvement or motivation, to achieve communication of employees between units and departments and to ensure collaboration and dialogue effectively must be planned and implemented
» Activities to improve working life such as resting, reading and sports areas that personnel may benefit from, kindergartens and children clubs, individual improvement trainings must be organized by ODHC.
» Arrangements must be made at ODHC for disabled and sick staff.
» It must be ensured that facilities offered to staff are easily accessible, practical and employee-oriented.

Patient Experience


89
Basic Patient Rights
Code Standard Code Assessment Criteria
HD.H
H.01
.00
The services provided in ODHC must be organized in such a way as to protect patient and carer rights.
HD.H
H.01
.01 An executive structure aimed at
protecting, exercising and improving the rights of patients and carers must be established.
HD.H
H.01
.02 ODHC must declare information about
all the services that are provided and access to these services and the quality of the services.
HD.H
H.01
.03 Patient and/or carers must be
informed about the diagnosis, treatment, care services, patient rights, patient responsibilities and other services.
HD.H
H.01
.04 During the health care process,
consideration must be given to the choices and preferences of the patient.
HD.H
H.01
.05
Activities must be planned in all service processes for the patient to be respected and to receive meticulous service.
HD.H
H.01
.06 The patient must be informed prior to
any medical intervention planned and his/her consent must be obtained and documented.
HD.H
H.01
.07
Patients must be able to examine the medical documents about themselves and receive a copy if requested.

Patient Experience
90
Department of Quality, Accreditation and Workers' Rights in Health
Code Standard Code Assessment Criteria
HD.H
H.01
.08
Arrangements must be made for the spiritual and cultural needs of the patient.
HD.H
H.01
.09
All measures necessary must be taken to ensure patient privacy.
HD.H
H.01
.10 Arrangements must be made for
receiving, investigating and resolving complaints of patients and their relatives.
HD.H
H.01
.11
Patient’s consent must be obtained if the patient is to take part in a research or experiment, or if the information, data or materials about the patient are to be used in any way.
HD.H
H.01
.12 Processes aimed at informing the
patient or carer if unintended events that negatively affect the patient safety occur must be identified.
Goal
To ensure that the rights of patients and carers are under guarantee in the delivery of services provided by the ODHC and that services are processes are arranged with this target in mind
Objectives
» Patient-orientedness
» Equity
» Relevance
» Timeliness
» Continuity

Patient Experience
91
Standards of Accreditation in Health - ODHS Kit
Standard Requirements
Management Structure
» A management structure must be established for the protection, exercise and improvement of the rights of patients and carers.
Information about Services and Patient Rights
» ODHC should declare information about all services it provides and access to and quality of these services.
» Patients and/or carers should be informed about diagnosis, treatment, care services which can be provided, responsibilities of the patient and additional services.
»
• Privacy
• Esteem and being respected
• Confidentiality of patient information
• Patient safety and security
• Informative actions about health services which will be provided and consent of the patient
• Right to decline the treatment
» In case adverse events that affect patient’s safety negatively occur, processes in relation to informing the patient or his/her carer must be defined.
Choices and Preferences of Patients
» During the health care process, consideration must be given to the choices and preferences of the patient, such as selecting the physician and accepting treatment or refusing treatment.
Patient’s Consent
» Patient must be informed verbally by using a simple and understandable language before any planned medical intervention.
Patient and/or caretaker must be informed about patient rights during
the application. This information must include the following topics:

Patient Experience
92
Department of Quality, Accreditation and Workers' Rights in Health
» Before any medical intervention, patients must be informed about theoperation by the person who will perform the operation, and a writtenconsent must be taken from patient and it must be approved. Thiswritten consent must include minimum following information:
• Name of the person to perform the procedure
• Expected benefits of the procedure
• Results likely to be encountered if the procedure is not performed
• If any, alternatives to the procedure
• Risks and complications of the procedure
• Estimated length of the procedure
• Name, surname and signature of the patient (regulatory agenciesfor Patients who do not have the competence to make decisionmaking for diagnosis and treatment, such as child patients, andemergency situations must be determined)
• Name, surname, title and signature of the person to perform theprocedure
• Date and time when the consent was taken
» Required measures must be taken to inform the disabled and to taketheir consent considering their condition (Patient’s Rights Regulation).
Access to Medical DocumentsIt must be ensured that patients have access to and take a copy of applied procedures, analyses or all the documents entailing private information about themselves both while receiving and after receiving the service. A policy needs to be determined for sharing of above-mentioned patient records with nonpatients.
Spiritual/Cultural NeedsODHC must ensure that patients receive service in accordance with their cultural and spiritual values.
Complaints» The complaints of patients and their caretakers should be recieved,
investigated and resolved in a fair and timely way.
» An evaluation commission should be established to assess complaints.

93
Code Standard Code Assessment Criteria
HD.H
G.01
.00
The services provided at ODHC must be organized in such a way as to protect the safety of patients and their carers.
HD.H
G.01
.01
A committee must be established to ensure patient safety.
HD.H
G.01
.02
Risk analyses must be conducted on the factors that threaten patient safety and measures must be taken to eliminate or decrease the risks that threaten safety.
HD.H
G.01
.03
Quality improvement activities must be planned to ensure the continuity of patient safety.
Goal
To ensure the safety of patients and carers in services provided by ODHC, and to organize provided services and processes in line with safety of patients and the carers by determining in advance the elements that could threaten their safety.
Objectives
Patient safety
Patient Safety

Patient Experience
94
Department of Quality, Accreditation and Workers' Rights in Health
Standard Requirements
Patient Safety Committee» A committee must be established to work regularly and systematically
in this field in order to be to identify existing or possible safety threats at ODHC and to take measures.
» The structure and the composition of the committee must be described considering the size of the institution and types of services to ensure effectiveness, continuity and systematic structure of activity.
Quality Improvement» The risks for patient safety must be analyzed and evaluated; levels of
risk must be determined and necessary improvement actions must be taken on the basis of the results of the analysis. Effectiveness of activities must be monitored.
» In this context, ODHC must address following issues related to patient safety, which is mentioned in various sections of Standards of Accreditation in Health:
• Prevention of infections
• Medication safety
• Radiation safety
• Falls prevention
• Safe surgery
• Safe injection practicesIdentity verification
• Information safety
• Emergency management
• Facility safety
• Medical device safety
• Adverse Event reporting system
• Waste management

95
Patient Feedback
Code Standard Code Assessment Criteria
HD.G
B.01
.00
A system must be established to receive feedback (comments, suggestions and complaints etc.) from patients and their carers about the services that are provided.
HD.G
B.01
.01 The system’s scope, methods and
tools must be defined including receiving, investigating and resolving of all feedbacks.
HD.G
B.01
.02
Patients and carers must be informed about how they can provide feedback.
HD.G
B.01
.03
Feedback must be assessed.
HD.G
B.01
.04
Necessary improvement activities must be planned for the results that come out of the feedback.
Goal
To make sure that necessary improvement is made by receiving systematic feedback from those who are provided with service in the institution.
Objectives
Patient-orientedness

Patient Experience
96
Department of Quality, Accreditation and Workers' Rights in Health
Standard Requirements
Feedback systemA feedback system must be established to receive all kinds of feedback (comments, suggestion, complaints etc.) from those who are provided with service at ODHC. Within this system; methods such as satisfaction surveys conducted regularly to receive comments and suggestions from patients and carers, one-on-one interviews or face-to-face meetings held when necessary, assessment of expectations and satisfaction levels before and after the service must be used.
Information on Feedback System» Patients and their caretakers should be informed about how they can
give feedback about services which they are offered, problems they face during service processes or issues related to ODHC and ODHC staff.
Assessment of Feedback» Feedback received from patients and carers must be analyzed in a
systematic manner, and the findings must be assessed.
» The findings obtained through data analyses must be shared with the top management and relevant units and benefit must be derived from feedback in an efficient manner.
Quality ImprovementAs a result of the findings obtained from the feedback, what kind of improvements are necessary must be determined and how these improvements will be made must be planned according to the order of importance and these plans must be put into practice.

97
Code Standard Code Assessment Criteria
HD.H
E.01
.00
Necessary precautions must be taken in order to provide patient able to reach services in time.
HD.H
E.01
.01
Patients must be provided with reception, orientation and consultation services that will facilitate the application process at ODHC and through which they can access all the information they need in the application process at ODHC.
HD.H
E.01
.02
The measures necessary to minimize the waiting period in the outpatient clinic must be planned and patients must be informed about how long they will wait approximately and when they will be examined by the doctor.
HD.H
E.01
.03 Facilitating measures concerning
access to services and waiting periods must be taken based on age, disease and disability.
HD.H
E.01
.04 Service delivery processes must be
organized in such a way as to ensure the diagnosis and treatment of the patient in good time and without delay.
HD.H
E.01
.05
Arrangements must be done at ODHC to facilitate patient access to ODHCs in case of emergencies over-hours.
Access to Service

Patient Experience
98
Department of Quality, Accreditation and Workers' Rights in Health
Goal
To put forward the measures that must be taken by the institution and to ensure the access to service to make sure that patients access the services provided by ODHC in a timely, efficient, effective and sufficient manner.
Objectives
» Patient-orientedness » Equity
» Suitability » Timeliness
» Continuity
Standard Requirements
Reception, Orientation, Consultation
» In line with the information declared by ODHC about the services it provides, ODHC must provide patients that wish to receive service with detailed information they might need to help them make decisions.
» How the information concerning reception, consultation and orientation such as all the important locations within ODHC necessary for the application procedures that must be conducted by the patient and the carer, information and documents they might need and waiting rooms etc will be provided for the patient must be planned and put into practice in advance.

Patient Experience
99
Standards of Accreditation in Health - ODHS Kit
Facilitating Arrangements
» Arrangements must be in place for shared areas like stairs, elevators,
toilets, parking areas and to ensure ramps and wheelchair services so
that elderly, disabled people and people in need of help due to disease
can access the services easily.
» Action must be taken to give priority to elderly, disabled people and
people in need of help, due to disease that receive service from ODHC.
Providing The Service On Time
» Procedures and steps of procedures must be examined in detail to
detect system-related problems that might pose a risk for patient
safety by prolonging diagnosis and treatment and measures must
be taken to shorten the procedure time in an optimal manner and to
increase efficiency.
» ODHC must assess its service processes within this framework and
document its work and plans aimed at increasing efficieny, productivity
and safety.
» Action must be taken to facilitate access of the patient with an
emergency to the service in ODHC out of working hours. Emergency
shift services and the treatments to be administered must be managed
by the institution.


Health Services


103
Prevention of Infections
Code Standard Code Assessment Criteria
SH.E
Ö.01
.00
Necessary measures must be taken for the control and prevention of infections.
SH.E
Ö.01
.01
A committee must be formed for infection prevention, and responsibilities must be determined.
SH.E
Ö.01
.02
A programme must be created for the prevention of infections.
SH.E
Ö.01
.03
Efficiency of the practices aimed at ensuring prevention of infections must be monitored.
Goal
To identify and prevent risks of health services-related infections threatening the employees and patients

Health Services
104
Department of Quality, Accreditation and Workers' Rights in Health
Objectives
» Patient Safety
» Healthy Work Life
Standard Requirements
Establishment of the Committee for Infection PreventionA committee responsible for the process of infection prevention at ODHC must be established. Members of this committee must be determined by taking the legislation of the country, personnel capacity of ODHC, patient profile and needs of ODHC into consideration.
The responsibilities of the committee for infection prevention are as stated below:
» To determine an infection control programme in accordance withthe features and conditions of ODHC within the scope of scientificprinciples
» To ensure the coordination of infection control activities at ODHC
» To monitor the efficiency of activities specified and implemented inthe programme for infection prevention, to make decisions on thenecessary improvement activities, and to make suggestions to theadministration
Creation of a Programme for Infection PreventingScope of work for infection control and prevention and the programme to be established also covers the assigned position of the committee, and must be analysed according to following subjects at least:
» Assessment of health care processes in terms of infection risk
» Hand hygiene
» Isolation measures
» Rational use of antibiotics

Health Services
105
Standards of Accreditation in Health - ODHS Kit
» Cleaning, disinfection, sterilisation, asepsis, antisepsis
» Occupational infections of employees
Prevention of infections in plant-based studies » Making plans for extraordinary situations (epidemics, rare
infections,etc.)
» Prevention of infections in support services such as laundry, catering, waste management and air conditioning systems
Assessment of Health Care Processes in Terms of Infection Risk
Health care delivery must be assessed in terms of the patient and employee safety in all areas and processes. Measures must be taken and maintained against the risks determined.
For a detailed risk assessment, see Management and Organisation Aspect- Risk Management Section
Hand Hygiene
Improvement activities of hand hygiene quality must cover the following subjects at least:
» Determination of Hand Hygiene Rules
» Assessment of Hand Hygiene Compliance
» Activities for Hand Hygiene Compliance
Setting Hand Hygiene Rules
WHO’s “5 Indication Rules” describes when the healthcare professional needs to apply hand hygiene.
According to “5 Indication Rules”:
1. Before contact with the patient,
2. Before aseptic procedures,
3. After contact with bodily fluids,
4. After contact with the patient,
5. After contact with the patient’s surroundings, hand hygiene must be applied.

Health Services
106
Department of Quality, Accreditation and Workers' Rights in Health
On the other hand, ODHC has various areas without patient care where the healthcare services are indirectly provided to the patient. Laboratories, pharmacies, sterilisation units, units allocated for medication preparation etc can exemplify these areas. Rules regarding hand hygiene in all healthcare delivery areas, including the ones mentioned above, must be set and the application thereof must be realized within the frame of these rules, to ensure both patient and employee safety.
Assessment of Hand Hygiene Compliance
Hand hygiene compliance refers to the application of hand hygiene at the right time, using the appropriate method, in the correct way and for the right duration. Hand hygiene compliance means not only washing and rubbing the hand, but also practicing it in the correct way.
Hand hygiene compliance must be measured by such methods as monitoring of hand hygiene materials, surveys (for the awareness, level of knowledge and compliance of health care professionals) as well as the informed prospective observations. In accordance with the data obtained as a result of the assessments, necessary improvement must be planned.
Actions For Improving Hand Hygiene Compliance
Following actions must be taken to improve hand hygiene compliance:
» Establishing hand hygiene policy
» Determining hand hygiene responsibilities
» Supporting skincare of healthcare professionals
» Trainings
» Reminder and warning messages
» Facilitating material access
Some points are stated below in detail:
Supporting skincare of healthcare professionals
Appropriate material must be provided to the healthcare professionals with skin irritations and allergy history.
Trainings
All employees must receive training on hand hygiene. Contents and periods of the trainings must be determined by ODHC according to the

Health Services
107
Standards of Accreditation in Health - ODHS Kit
occupational groups and needs detected through the measuring results. Trainings must cover at least:
» Importance of hand hygiene
» Hand hygiene methods and indications
» Points to take into consideration
» Wearing gloves
Facilitating material access
Materials for hand hygiene must be available in all areas of health care. ODHC must prepare plans for access to materials such as liquid soap, single-use towel in the hand washing areas/ lavatories.
Within the framework of recommendations in WHO guidelines, alcohol-based hand antiseptic must be available at patient point of care. Patient point of care is the place where three elements come together:
1. Patient
2. Healthcare professional
3. Care or treatment procedure including contact with the patient or his/her surroundings (within the patient’s area)
This term precisely covers the setting of care and, thus, the need of hand hygiene in this setting. Alcohol-based antiseptic must be easily accessible in patient point of care.
All areas where patients are provided care and treatment must be regarded within this scope. The aim here is to organize the bedside products in such a way that the patient can reach them without leaving his/her area.
Access to alcohol-based antiseptics is provided through health professionals’ pocket bottles, dispensers fixed on the walls, containers fixed to the patient bed and through bottles on the bedside table or in the medication trolleys.
Isolation Measures
ODHC must determine the conditions in which isolation measures must be implemented; the implementing rules and the required physical conditions (separate room/unit, adequate distance between beds/units, adequate numbers of personnel etc). Healthcare professionals must be

Health Services
108
Department of Quality, Accreditation and Workers' Rights in Health
provided with training, sufficient personal protective equipment must be supplied and this equipment must be used in compliance with isolation measures.
Republic of Turkey Ministry of Health has determined descriptive symbols in order to ensure the unity of implementation and language in the subjects of isolation measures in institutions, and to benefit from memorability of visual figures. Various colours and figures of nature have given inspiration to the creation of these descriptive symbols, aimed as an example to the entire world in this field. The use of these symbols is recommended by the Ministry of Health , as determined by the ODHC in order to warn the employees in all areas where the patient present or where the patient is transferred to.
Yellow Leaf:
Used in respiratory isolation. Trees are the lungs of nature, leaves are lungs of trees. A yellow leaf (sarı yaprak in Turkish) was used to make it easy to associate it with respiration (solunum in Turkish), their initials being the same letter, S.
Blue Flower:
Used in droplet isolation. The point in the centre represents the patient, and the surrounding petals represent droplets. Patient is surrounded by droplets and s/he poses the risk of spreading them. The droplets gathering at one point intends to attract the attention to the point (patient).
Red Star:
Used in contact isolation. Five points of the star represent five fingers of a hand. The red colour is used on the basis of connection between the disadvantages of contact with fire and those of contact with a patient.

Health Services
109
Standards of Accreditation in Health - ODHS Kit
Rational Use of Antibiotics
For the ideal use of antibiotics; correct antibiotics must be administered in the most suitable way, in effective doses, at optimum intervals and for a suitable duration after the correct diagnosis.
The minimum actions needed to be taken at ODHC regarding Rational Use of Antibiotics are as follows:
» Policies on antibiotic use at ODHC must be determined; the required practices must be applied and monitored.
» A team responsible for creating awareness on rational use of antibiotics and planning and conducting the required studies on this subject must be set up. Duties, authorities and responsibilities of the team must be determined.
» Guidelines on the principles of rational use of antibiotics and proper antibiotic prophylaxis must be drawn up. In order to ensure that practices are applied in line with the guidelines, training and informing activities must be organised. Clinical practices of the implementations must be monitored (To illustrate; rate of proper use of antibiotics in surgical prophylaxis)
» International and national and/or local guidelines (if available) must be benefited from when determining policies on antibiotic use. Data on local resistance must be analysed.
» The status of antibiotics use in line with guidelines must be monitored.
Cleaning, Disinfection, Sterilisation, Asepsis, Antisepsis
All areas used during service delivery and all equipment contacting with human tissues can be the cause of infection. Therefore, various procedures are applied in order to bring relevant areas and instruments under control in terms of microorganisms:
» Cleaning
» Disinfection
» Sterilisation
» Asepsis
» Antisepsis

Health Services
110
Department of Quality, Accreditation and Workers' Rights in Health
Rules of cleaning, disinfection, sterilisation and antisepsis processes must be determined.
Following issues must be determined within these periods:
» Duration of application
» Range of application
» Method of application and material to be used
» Process for monitoring efficiency of implementation
Cleaning
» Policies for ODHC cleaning must be determined, plans must be drawn, specific areas for infection must be determined, supervising staff must be identified. It must also be determined who will use which cleaning materials in which area, and who would check how the materials would be applied and the effectiveness of the application must be determined.
Disinfection
» The medical equipments used in patient care should be classified as critical, semi-critical and non-critical in the framework of internationally accepted guidelines used to determine the need for disinfection and sterilization methods.
» Disinfected surface, material, equipment and waste must be determined.
» Disinfection type, disinfectant to be used and rules on how to use it (duration, quantity, controls or measures for ensuring efficient concentration, points to take into consideration in terms of patient and employee safety etc) must be determined according to the material used during disinfection procedures.
» There must be a sufficient amount of equipment in order to effectively conduct disinfection procedures in the sufficient time, taking into consideration the patient circulation.
» In the areas where high-level disinfectant is used, ventilation must be configured in such a way as to provide employee safety.
» Technicians must be trained, and the status of application of disinfection must be monitored by the supervising staff under the rules of infections prevention and control.

Health Services
111
Standards of Accreditation in Health - ODHS Kit
Sterilisation
» Materials and equipment used in patient care and needing disinfection must be determined.
» Rules and operations for sterilisation processes must be determined. Authorities of infection prevention must monitor their implementation within the framework of rules determined.
» See Healthcare Services Aspect- Sterilisation Section for detailed information.
Asepsis and Antisepsis
» Implementing rules must be determined within the framework of asepsis and antisepsis principles and the relevant healthcare professional must be trained.
Occupational Infection of Employees
Healthcare professionals are responsible for taking measures in order to protect both themselves and their patients against infectious agents. These measures are presented in three groups:
1. Measures to be taken before contact: Immunisation against infections which can be immunised, routine screening.
2. Measures to be taken to prevent contact: Protective measures to be taken against the risks which might be encountered during healthcare delivery (standard measures, isolation measures).
3. Measures to be taken after contact: Procedures of immunisation, prophylaxis, follow-up and treatment which must be conducted in case of contact with any infectious agent.
» ODHC must define all the processes on the above measures.
» Actions must be taken to improve the levels of knowledge and awareness on infection protection of employees at ODHC.
» Appropriate working environment and conditions must be provided for the employees to take necessary measures against infections. Necessary equipment must be supplied.
» Medical screening, which must be performed within the framework of risk analysis based upon the section at regular intervals, must be determined. A programme must be created for the medical screenings.
» The procedures must be determined for the cases with positive scans.

Health Services
112
Department of Quality, Accreditation and Workers' Rights in Health
» Efficiency of applications within the framework of the programme must be monitored.
» Actions to be taken in case of contact with any infectious agent must be determined. Authorities must be designated in order to ensure that these actions are carried out and controlled.
Infection Control in Support Services such as Laundry, Kitchen, Waste Management and Ventilation Systems
» Cleaning process of textile materials used in healthcare delivery must be monitored for infection control. It must be ensured that necessary measures are taken and maintained.
» Employees taking charge in the processes of supplying, storing, preparing and distributing foods given to the healthcare providers and service users must be monitored. Necessary measures must be taken and maintained.
» Processes of safe removal and disposal of infected wastes produced in healthcare delivery must be monitored. Necessary measures must be taken and maintained.
» End of life services, morgue (if available) and its operation must be monitored to control infections, necessary measures must be taken and maintained.
» Ventilation and air filter systems must be monitored for infection control. Necessary measures must be taken and maintained.
Monitoring and Evaluation» Actions for infections prevention at ODHC must be monitored on the
basis of process and outcome. Necessary actions must be taken for continuous improvement. In monitoring and evaluations; routine observations and controls, process-based indicators determined for implementations must be used.
» Outcomes obtained from monitoring and evaluation must be analysed. The compliance with targets that are set must be evaluated. They must be improved if necessary.
» Outcomes obtained must be shared with the management and relevant employees.
» Information and training must be provided for infection control and prevention of employees.

113
Code Standard Code Assessment Criteria
SH.S
Y.01
.00
Processes concerning sterilization services must be identified and taken under control.
SH.S
Y.01
.01
Physical areas and conditions in sterilization unit must be planned according to the process steps.
SH.S
Y.01
.02 The processes regarding sterilization,
storage, transfer and use of the materials must be taken under control.
SH.S
Y.01
.03
Traceability of the evidence regarding time, device, method, implementer and control parameters must be ensured in each stage of the sterilization.
Goal
To take sterilization process, which is one of the important steps to prevent and control infectious diseases that might develop in relation to healthcare services, under control to ensure patient safety
Objectives
» Patient safety » Efficiency
» Effectiveness » Continuity
Sterilization Management

Health Services
114
Department of Quality, Accreditation and Workers' Rights in Health
Standard Requirements
Measures Related to Physical Areas and Conditions in Sterilization Unit
Physical areas and conditions in sterilization unit must be planned according to the process steps minimum in three fields.
» Area that can be cleaned and decontaminated (Dirty area, decontamination area etc.)
» Area where packaging and loading to sterilization device procedures take place (clean area, semi-clean area, packaging area etc.)
» Area where unloading of sterilized materials and storing procedures take place (sterile area, clean area, sterile storage area)
» Surfaces in sterilization unit must be cleanable easily and disinfect.
» Appropriate temperature and humidity ranges must be determined for the areas and temperature and humidity rates must be followed up on a constant basis.
» Airflow must be from the sterile area to clean area and contaminated area. The air provided by the ventilation system must be filtered at least 10 times an hour. Any method that may cause turbulence must not be used.
» Systems like lighting, water, uninterrupted power supply must be planned and monitored so as to ensure sterilization safety.
» Storage conditions in sterile areas must not prevent air circulation and must ensure preservation of sterile material.
» Necessary equipment, working conditions and rules must be determined according to the physical areas in the unit and the services given in these areas.
Process Control in Sterilization Service
Process of sterilization service is composed of steps of procedure that proceed in a circular manner:
» Transfer from area of use to the contaminated area
» Cleaning-Care
» Packaging
» Loading

Health Services
115
Standards of Accreditation in Health - ODHS Kit
» Sterilization
» Storage
» Distribution (Transfer to the area of use)
» Use of sterile material
In all of the processes quality of the material, sterilization management, working and control rules regarding the equipment used and area of use must be determined and the relevant personnel must be provided with training on the issue. Corrective and preventive action must be taken to address irregularities identified in the processes.
Washing, Disinfection and Packaging Processes
» Dirty materials should be counted from the material list and accepted into the sterilization unit.
» Dirty materials must be pre-cleaned and decontaminated.
» The washing activity should be checked at regular intervals.
» Washing effectiveness control should also cover luminous appliances in use.
» The materials should be delivered to the clean area with the material list.
» Packing of materials should be done in clean area.
» Textile materials should be packed separately from other materials
Quality Control for Sterilization Process
» Physical-mechanical controls must be conducted according to the method of sterilization that is used and a record must be kept.
• Physical-mechanical controls contain records of program cycle including parameters like pressure, gas concentration, temperature, humidity, time and also records of maintenance and calibration of the device.
» Efficiency of sterilization must be assessed through chemical control methods.
• Each package must bear Class 1 process indicators.
• Class 2 indicators must be applied every day while the device is empty and before starting sterilization process.

Health Services
116
Department of Quality, Accreditation and Workers' Rights in Health
• Each pack should be provided with a suitable chemical indicator (at least class 3) that meets the quality of the pack contents and provides the specified performance conditions .
» Whether sterilization has taken place or not must be assessed through biological control methods.
• ODHC must determine minimum frequency of use of indicator for each sterilization method by taking into account issues like material load, patient profile, working frequency of the device and especially scientific requirements and ODHC must increase frequency of use when necessary.
• If the biological indicator is positive after the procedure, a retrospective follow-up of the material and patient must be conducted. All of the sterile material distributed until the use of biological indicator that tested negative must be reviewed and if the material was used for the patient, the patient must be monitored for risk of infection.
Traceability of Sterilization Processes» Traceability of the evidence regarding time, device, method,
implementer and control parameters must be ensured in each stage of the sterilization.
» It is necessary that information concerning sterile material be included in patient file or a record must be kept about which material was used for which patient. Records on which material was used for which patient must be accessible retrospectively when necessary.
» The following information concerning the records on the materials must be available at minimum:
• Assessment of color change in the indicator that is used (record on the control of users during usage)
• Information of sterilization date, method, device and cycle
• Records on maintenance, repair and calibration of sterilization device
• Cycle records of the device
• Tests on the device (like vacuum leakage test, Bowie Dick test )
• Result of biological indicator
• Information on when and by whom it was received
• Information on who applied the procedure in the stages
• Records on quality control work that is undertaken in each stage

117
Medicine Management
Code Standard Code Assessment Criteria
SH.İY
.01.
00
Efficient and safe medicine management must be ensured in the institution.
SH.İY
.01.
01 A medicine management structure that will provide an effective implementation of drug administration and coordination must be created.
SH.İY
.01.
02
Main and critical stages of all the medicine processes in the institution must be determined and the methods and rules regarding these stages must be identified.
SH.İY
.01.
03 The right medicine must be provided at the right time and effective stock management of the medicines must be ensured.
SH.İY
.01.
04
Medicines must be kept under proper conditions.
SH.İY
.01.
05 Measures must be taken to ensure the safety of the patient and the personnel when the medicines are being prepared and administered.
SH.İY
.01.
06
Traceability of medicine processes must be ensured by making use of feedback infrastructures and indicators and the necessary improvement work must be undertaken.
Goal
To minimize the risks to the patient and the employees in all processes that involve the drug, ensure that the processes are carried out effectively and efficiently.

Health Services
118
Department of Quality, Accreditation and Workers' Rights in Health
Objectives
» Patient Safety » Healthy Work Life
» Efficiency » Patient-orientedness
» Productivity » Suitability
» Timeliness » Continuity
Standard Requirements
Management and Documentation» In order to establish an efficient medicine management system in ODHC,
first of all an active management design that includes an adequate level of documentation must be created. Duties and responsibilities of people involved in this management design regarding medicine safety must be identified, necessary training opportunities must be provided in order to improve the competencies.
» Documents on medicine management must be created by taking into account needs of ODHC and critical processes. The documents must address the following issues at minimum:
• Supply of medicines
• Duties and responsibilities of the personnel involved in medicine management
• Conservation of medicines
• Medicine orders
• Transfer of medicines
• Preparation of medicines
• Administration of medicines
• Use and disposal of half-finished ampoules after treatment
• Notifications about adverse effects
• Medication error reporting and indicators about medicine management
• Hazardous medicines and intervention methods in the case of error
• Tables on specific medicines that aim to ensure medicine safety

Health Services
119
Standards of Accreditation in Health - ODHS Kit
» Specific medicine groups must be determined by ODHC in line with the legislation and efficient use of these medicines must be ensured by making use of warning mechanisms (like colorful or audible warning signals) aimed at ensuring efficient and safe use of these medicines.
» Examples of specific medicine groups are as follows:
• Pediatric emergency medicines
• Medicines with a similar appearance
• Medicines with similar spelling and pronunciation
• Psychotropic medicines
• Narcotic medicines
• Medicines that should be protected from light
• High-risk medicines
• Medicines that require special technique/equipment/expertise to be prepared
• Concentrated electrolytes
• Medications that should not be used in pregnancy and lactation
• Cytotoxic drugs
• Drugs that require secondary follow-up
Communication in Medicine ManagementCommunication between patient and employee and between employee and employee in medicine management is of great importance in terms of patient safety. Therefore, an efficient medicine methodology must be ensured for each stage of medicine management at ODHC.
» Personnel must be trained to increase their awareness and knowledge levels about medicine management.
» Patients must be informed about the medicines that are administered to them.
Supply of Medicines» Rules and methods about demands for supply of medicine must be
determined at ODHC. Within the scope of these rules, who can make a medicine request, the method of demand, who will evaluate the demands and how they will evaluate the requests are all points that must be identified.

Health Services
120
Department of Quality, Accreditation and Workers' Rights in Health
» While determining types and amount of medicine to be supplied, evaluations made for a needs assessment, demands for supply and consumption analyses must be taken into account.
Conservation of MedicinesStorage areas for medicines encompass pharmacy warehouses and all the warehouses of the unit where medicines are kept for more than 24 hours (outpatient clinic, service, operating room etc.)
» Access of people except for the personnel in charge to the warehouses must be limited due to safety and security reasons.
» Medicines must be kept under appropriate conditions in line with their characteristics. To that end, action must be taken to ensure air-conditioning and lightning control and physical conditions must be monitored. Measures should be taken to protect the cold chain in extreme cases such as power failure.
» It is also important to prevent storage of any materials in the medicine warehouses and medicine refrigerators other than medicines and vaccines.
» Pillboxes must not be placed on direct ground level and the minimum height of the lowermost shelf must be determined so as to make sure the medicines are not affected in the case of flood.
» Medicine arrangement plans of warehouses and refrigerators must be easy to use, accessible and the plans must be kept up-to-date.
• While the arrangement plan is being prepared, separate areas must be allocated for specific medicines and medicines with similar pronunciation/spelling/appearance must be stored far away from one another.
» Necessary storage measures must be taken in all the areas of ODHC to ensure safety of psychotropic medicines and narcotic medicines.
» Warning signals (labels etc.) must be used efficiently for high risk medicines.
Medicine OrdersODHC must determine the authorities, methods and rules for all phases of order in line with the legislation. Abbreviations must not be used in the name of the medicine while ordering a medicine. Medicine orders are basically divided into three groups.
» Patient-based administration orders (verbal, written or electronic) that are made for treatment

Health Services
121
Standards of Accreditation in Health - ODHS Kit
» Storage orders that are made to the pharmacy by units having the medicine in stock
» Supply orders that are made for medicines with low levels of stock or which are out of stock
Administration orders that are transferred to the treatment plan prepared for the inpatients must include the following information at minimum:
» Full name of the medicine and pharmaceutical form
» Administration time
» Dosage
» Mode of administration
» Duration of administration
Transfer of Medicines» Necessary measures must be taken to prevent breakage and spillage
during the transfer of medicines.
» Equipment necessary for safe transfer of medicines (medicine boxes, tools like forklift etc.) must be provided. This equipment may change depending on the amount of the medicine to be transferred.
» The Health staff who will transfer the medicine must be trained on safe transfer of medicine and intervention in the case of breakage of hazardous medicine.
Preparation of Medicines» People preparing medicines in the pharmacy must have enough
information and experience about medicines.
» Measures must be taken to identify divided packages (blister tablet that have been cut etc.), expiry dates of all the medicines that have been prepared must be checked and the orders must be confirmed.
» The medicines that require special technique/equipment or expertise must be transferred to the relevant unit for the administration process after having been prepared by the specialist under proper conditions. Color directives must be taken into consideration during preparation of the medicines with colored label.
Administration of Medicines» Medicines should be prepared specifically for each patient in the
drug preparation environment before application, carefully applied in

Health Services
122
Department of Quality, Accreditation and Workers' Rights in Health
the framework of the specified rules, and the application should be recorded.
» Administration of the medicine must be conducted only by the personnel (dentist, nurse, intern under the supervision of the nurse etc.) authorized to administer the medicine. Patient identity must be verified before the administration and treatment information must be confirmed. Especially after administration of risky medicines patients must be monitored, it is necessary to be ready for any adverse effect that may occur.
Control of Medicines that Patients have with Them» Processes for the management of the medicines brought by the patient
must be defined.
» There must not be any medicine left near the patient, the medicines that patients have with them must be checked during admission to ODHC.
» Expiry dates and physical conditions of medicines that are taken from the patient must be checked.
» Medicines the expiry dates of which are over and the physical structure of which has changed must be disposed of after having informed the patient.
Traceability» Traceability and continuity of the data obtained during medicine
management process must be ensured within the scope of information management systems.
» An information infrastructure that will enable the personnel to report the problem that may arise in any phase must be established and it must be used efficiently.
» Problems about medicine management that must be reported must encompass adverse effects and medication errors at minimum.
» Adverse reactions should be recorded and reported to the pharmacovigilance system. The pharmacovigilance officer must be defined.
» Inaccuracies in drug-related processes should be reported to the relevant experts and improvements should be made to the identified error sources.

123
Standard 1
Code Standard Code Assessment Criteria
SH.H
B.01
.00
Patient care processes must be conducted in line with the needs of the patient and so as to ensure patient safety.
SH.H
B.01
.01
The process related to the patient care practices must be planned.
SH.H
B.01
.02
Patients must be evaluated in terms of their care needs.
SH.H
B.01
.03
A care plan for patients must be developed according to the results of the evaluation
SH.H
B.01
.04
The care plan must be reviewed in line with the clinical picture of the patient and be updated when necessary.
SH.H
B.01
.05
Patients/carers must be involved in the care processes.
SH.H
B.01
.06 Ethical dilemmas such as not treating
the patient, withdrawal of the treatment or discontinuing the treatment must be addressed and settled in time.
SH.H
B.01
.07 Processes regarding referral of the
patient or completion of the treatment must be planned so as to ensure continuity of the care.
SH.H
B.01
.08 Records which are relevant to patient
care process must be complete, accurate and shall include required notes/warnings for patient’s clinical trial.
Patient Care

Health Services
124
Department of Quality, Accreditation and Workers' Rights in Health
Goal
All the patients getting service from ODHC must be provided with the same Standard of care in each stage of the patient care process.
Objectives
» Patient Safety» Efficiency» Suitability» Continuity» Timeliness» Equity
Standard Requirements
» Patient care encompasses the whole health service processes starting from admission of the patient to ODHC to monitoring of the patient after discharge.
» It also includes service processes of all other relevant occupational groups beside diagnosis/treatment processes provided in policlinics for outpatients and in clinics for inpatients.
Identification of Patient Care Processes» In order to ensure efficiency of services to be provided for patient care
within this period of time, care processes must be identified. This identification must include the following issues at minimum:
• How, when and by whom the care needs of the patient will be evaluated
• Care planning after the evaluation
• Providing the patient with the planned care service
• Putting the care plan into practice
• Monitoring the patient in order to understand the results of the care

Health Services
125
Standards of Accreditation in Health - ODHS Kit
• Making changes about care when needed.
» All the stages concerning determination of patient needs, care planning, its implementation and follow-up must be realized by all of the members of the care team with a multi-disciplinary understanding and in a coordinated manner. The said procedures must be recorded simultaneously.
» Patient/carer must be involved in the care processes.
» It must be ensured that follow-up results of the evaluation, care plan and implementation concerning outpatients and inpatients are monitorable.
Determination of Patient Care Needs
» Care needs of outpatients must be determined in outpatient clinics and those of inpatients must be evaluated while the patient is being admitted to ODHC by the relevant personnel.
» While care needs of the patient are being determined, overall condition of the patient must be evaluated through an integrated approach.
» Within the framework of identified care needs, measures must be taken to ensure patient safety in the procedures to be performed on the patient (filling, root canal therapy etc.) the right procedure must be performed on the right area.
Patient Care Plans
» Care plan is a document which includes treatment and care needs of the patient, goals with regard to these needs, implementation and evaluation of implementation.
» Continuity of treatment and care is essential to patient care. Care plans must be prepared in a way that also encompasses post-treatment checks.
» Any change or improvement (change of care needs, any intervention performed on the patient, change of medicines used by the patient etc.) must be reflected to the care plan concurrently and care plan must be updated when necessary. Relevant health personnel must be kept abreast of the updates in the care plan.

Health Services
126
Department of Quality, Accreditation and Workers' Rights in Health
Involvement of Patient/Carer in the Care Process
» Relevant health employees who provide service must establish a communication with the patient in a way that take expectations, needs and values of patient/carers into account. The care team must establish a positive diaologue with patient/carers.
» Patient/carers must be trained on ensuring continuity of care (about subjects such as prosthesis care at home, tooth brushing correctly, points to be careful after completion of treatment etc.)
» Patient/carer must be informed about the procedures to be perfomed on the patient by the person that will perform the procedure and a written consent must be received.
» Patients must be encouraged to be involved in their own care processes. Patient/carers must be informed about the course of patient care and issues to pay attention to in the process etc.
» Adaptation of inpatient/carer to inpatient unit must be ensured. Patient/carers must be informed about breakfast and meal times, how they can contact health personnel, and how they can get information about care services etc.
Resolving Ethical Dilemmas
Ethical dilemmas like not treating, withdrawing the treatment or discontinuing the treatment must be addressed beforehand and resolved.
When there are ethical dilemmas, a solution must be found through decisions made jointly by the patient and doctor in a way that ensures patient safety.
Procedures to undertake in the case of patient leaving ODHC without permission of the doctor or patient declining treatment must be determined.
Referral of the Patient
Referral procedures of patients to be referred to ODHC in line with the identified care needs must be conducted in keeping with the current plan developed by ODHC.
» Involvement of patient and carer in referral procedures must be ensured and patient/carer must be informed.

Health Services
127
Standards of Accreditation in Health - ODHS Kit
» Prior to referral, coordination must be ensured with the institution to which the patient will be referred.
» Information and documents about clinical status of the patient, diagnosis/treatment, interventions performed on the patient (if any) must be transferred in an accurate and complete manner.
Completion of Treatment of the PatientProcedures regarding completion of treatment of the patient must be planned.
» Patients whose treatment has been completed by the doctor must be informed about issues like points to pay attention to at home after treatment and how and when they must contact the health personnel for control.
» Records must be kept about completion of treatment.
Patient RecordsThere must be required regulations for keeping patient records complete and accurate.
Information about diagnostic practices done during patient care
process with by who and when the practice is done must be included
in the records. Also, these records must be accessible at future
admissions of the patient.
» It must be ensured that information in patient files and records are complete and accurate.
» Date information must be in patient records.
» Patient records must be written in a readable and understandable manner.
» Alert notations, which have importance for patient’s clinical trial must be included in the patient file.
Death of PatientBy ODHC, a plan must be prepared regarding services to be provided for cases when a patient dies.

Health Services
128
Department of Quality, Accreditation and Workers' Rights in Health
Standard 2
Code Standard Code Assessment CriteriaSH
.HB.
02.0
0
In the patient care process, patient identity must be verified to make sure that the medical procedure is conducted on the right patient.
SH.H
B.02
.01
Identity verification methods and tools must be identified.
SH.H
B.02
.02
Patient and health personnel must be trained on verification of the patient identity.
SH.H
B.02
.03
Patient identity must be verified in all the procedures to be conducted in patient care process.
Goal
Performing the procedure on the right patient within the context of patient care practices such as administering medicine to the patient, examinations, treatment, operation etc.
Objectives
» Patient Safety » Efficiency
» Effectiveness » Suitability
Standard Requirements
Identity Verification Tools
Identity identifier is used for verification of identity. To that end;
» For outpatients;
• Official documents with picture containing patient’s identity information
» For inpatients;
• Wrist bands/bracelets
Health Services
129
Standards of Accreditation in Health - ODHS Kit
• Barcoding systems
• Biometric systems (Retinal scanning, fingerprint scanning, palmprint verification system etc.)
• Other methods that are determined by ODHC and that can verify patient identity.
If wrist bands/bracelets are to be used as identifiers, the following points must be taken into account:
» White wrist band/bracelet must be used for inpatients and a red one must be used for allergic patients.
» Wrist bands/bracelets must include at least patient name/surname, date of birth, and protocol number.
» There must be 4 identifying parameters at most on wrist bands/bracelets.
» Information written on wrist band/bracelet must be legible and not erasable.
» Processes concerning identification and verification of identity must be identified for patients with an unclear identity, patients who stay in the same service and have similar names and those who have physical or medical disabilities and thus cannot use wrist band/bracelet etc.
Trainings
Work must be undertaken to raise awareness in health personnel about sources of error regarding identity verification and health personnel must be trained on identity verification. Patients must be informed about the use of identifiers and the importance of identity verification.
Verification of Patient IdentityIdentity verification can be defined as a set of practices that makes sure that whether the person getting service is the right person is determined in a reliable way.
» In all the processes starting from application of the patient to ODHC to leaving ODHC (transfer of impression, model and prosthesis of the patient, prior to any test or procedure, prior to administration of a medicine etc., during the transfer of the patient etc.), patient identity must be verified through identification parameters. Identification parameters can be composed of the following:

Health Services
130
Department of Quality, Accreditation and Workers' Rights in Health
• Patient’s Name-surname
• Date of birth (day/month/year)
• Name of father
• Protocol number
• Information on up to four parameters must be found on the identifier.
Below, there are examples of methods to be used during identity verification procedure:
» For inpatients;
• Verbally asking the patient about identity parameters that are available in patient records and confirmation
• Comparing identification parameters on the wrist band of the patient with patient records
• Verbally asking the patient about identification parameters written on the wrist band and confirmation
» For outpatients;
• Verification of patient identity through control of ID with photo
• Adding defining parameters such as barcode, label etc. to impression, model, prosthesis and equipment that will verify patient identity while establishing communication with prosthesis and orthodontics laboratories.
• Verbally asking the patient about identifiation parameters written on test and radiography order form and confirmation
• Comparing identification parameters on the laboratory test sample container with patient records or asking the patient about them verbally

Health Services
131
Standards of Accreditation in Health - ODHS Kit
Standard 3
Code Standard Code Assessment Criteria
SH.H
B.03
.00 Measures must
be taken to prevent patient falls.
SH.H
B.03
.01
The process concerning prevention of falls must be planned.
SH.H
B.03
.02
Patients must be assessed for fall risk.
SH.H
B.03
.03
Measures must be taken to prevent falls.
SH.H
B.03
.04
Falls that have occurred must be monitored.
Goal
The goal is to prevent patient falls in ODHC and to minimize risk of harm caused by falls.
Objectives
» Patient Safety
» Efficiency
» Suitability
Standard Requirements
ODHC management must ensure involvement of all the personnel in the efforts aimed at prevention of patient falls and the system to be established

Health Services
132
Department of Quality, Accreditation and Workers' Rights in Health
for fall prevention strategies in all the units of ODHC must be plannaed in an integrated manner. This plan must include the following:
» How the fall risks will be determined (Patient fall risk evaluation, Determination of ODHC based fall risks)
» How the risk levels of patients will be assessed (which patients will go through risk assessment, which measurement will be used in the risk assessment and how the risk levels will be identified etc.)
» What kind of measures will be taken for the risks that have been determined (patient/disease based measures, environmental measures etc.)
» Follow-up processes concerning the falls that have occurred (when, how and to whom the falls will be reported and how the results will be assessed etc.)
Fall Risk Assessment
» A risk assessment must be made to determine the risk levels of inpatients.
» Fall risk assessment of the inpatient must be made by the nurse of the relevant unit following the admittance of the patient to the unit. The risk assessment must be repeated in the case of transfer between units, in the postoperative period, in the case of a change in the condition of the patient or in the case of fall.
» Fall risk scoring scales must be used to make a risk assessment for inpatients. Morse, Hendrich II, Itaki Fall risk Scale, Harizmi Falling Risk Scale (for child patients) are among the national and international scales that can be used to make an assessment. Measures to take according to the identified risk levels must be planned.
Measures to Take According to the Risk Levels» The following measures must be taken at minimum to address risks
specific to ODHC environment (ODHC-based):
• Clinics and patient rooms must be arranged in a simple and plain manner, there must not be unnecessary tools, material and objects in these areas and adequate level of lightning must be ensured in these areas.

Health Services
133
Standards of Accreditation in Health - ODHS Kit
• Units and patient beds must be positioned so as to prevent patient falls.
• Walking areas must be kept dry so as to prevent patient falls, there must be warning signs on slippery surfaces and there must not be objects and things that hinder walking in the walking areas.
• There must be handrails for patients where necessary.
» ODHC must take measures for special out-patient groups (minor surgery patients, disabled, kids) by accepting them as high risk patients without conducting risk assessments.
In order to prevent in-patient falls, patient-based measures must be taken according to the risk levels determined.
Patient-based measures can be identified as general measures to be taken as per the the risk levels of the patients and also patient specific measures that will be taken according to the risk factors determined in the patients as a result of the risk assessment.
» The general measures to be taken for high-risk patients at miminum are as follows:
• High-risk patients must be identified with the symbol of four-leaf clover. This symbol must be used in the way the ODHC, deems sutiable in the areas where the patient stays or to which the patient is transferred in order to warn the personnel.
• Care of high-risk patients must be planned and preventive measures that have been taken must be monitored.
• The frequency of monitoring of high-risk patients must be determined. Patient/carer must be informed about fall risk.
Monitoring Fall Events
» Fall events in ODHC must be monitored, a statistical analysis must be made and improvement work must be undertaken in line with the results of the analysis.
» It must be ensured that the personnel report fall events to the Adverse Event reporting system.

Health Services
134
Department of Quality, Accreditation and Workers' Rights in Health
Standard 4
Code Standard Code Assessment Criteria
SH.H
B.04
.00
Effective communication must be ensured in the flow of information among the health professionals.
SH.H
B.04
.01
The process regarding shift handover of the personnel must be identified.
SH.H
B.04
.02
Action must be taken about verbal requests.
SH.H
B.04
.03
Action must be taken about abbreviations, signs, symbols and the amount of dose that should not be used.
SH.H
B.04
.04 Patient information must be conveyed
properly and thoroughly when the patient is transferred between departments.
SH.H
B.04
.05
The process regarding taking into account the consultations held in and outside ODHC must be planned.
Goal
The goal is to prevent threats against patient safety that may be caused by communication setbacks betweeen the health personnel.
Objectives
» Patient Safety » Efficiency
» Effectiveness » Suitability
» Timeliness » Productivity

Health Services
135
Standards of Accreditation in Health - ODHS Kit
Standard Requirements
Shift changes among the personnel, orders taken verbally or by phone, use of abbreviations, symbols and signs, patient transfer between units, referrals made to other institutions and consultations held within and outside ODHC (internal and external) are all important processes that affect the flow information among the health personnel in terms of patient safety.
Shift Handover of the Personnel
» Shift handover processes in the ODHC must be identified. The following issues must be taken into account at miminum in shift handover processes:
• Shift handover must be conducted with at least two people, one side as the outgoing shift owner and the other side as the incoming shift owner.
• In the shift handover process, the information available on the record must be communicated to the incoming shift owner and the patient must be visited by the outgoing shift owner and handed over to the incoming shift owner as such.
• All the information concerning patient care process must be transferred in the shift handover process.
The Practice of Verbal Order
Verbal order can be defined as the doctor conveying the order to the nurse verbally in cases where the doctor cannot make a written order.
» The practice of verbal order must be avoided as much as possible and be used only when there is no other choice.
» When a written order cannot be received and there is no other choice but to receive a verbal order, a verbal order must be received within the scope of the following issues:
• ODHC must determine the rules regarding verbal order in a clear manner.
• The cases where the verbal orders can be used must be identified.

Health Services
136
Department of Quality, Accreditation and Workers' Rights in Health
• A mechanism must be established to ensure prescribing, authorization and validity of the presciptions.
• While the verbal order is being received, the name, dosage, mode and frequency of administration of the medicine must be clarified.
• When the verbal order is received, it must definitely be confirmed. Confirmation must be ensured in the following manner:
√ When the order is being received, it is listened to first.
√ The order is recorded.
√ Then the order which is written is read again and is confirmed by the person making the order. The one receiving the order can read back the order for confirmation through following ways:
– Spelling out the name of the medicine
– Using both generic and commercial names of the medicine
– Specifying for what purpose the medicine will be used
– Not using the figures that may be confused when speaking
– Avoiding names of medicines that may be confused in terms of prefix and suffix. To adress this problem a method can be developed to help with distinctive spelling. (such as Bursa for B)
– If necessary, asking for a repetition of the name of medicine through coding method (like Bursa for B)
• If there is any correction to be made, the order is recorded again after having made the correction.
• All the verbal orders must be documented as soon as possible, be included in the medical records of the ODHC and be signed by the person making the order.
• How the order was received (verbal or by phone) must be specified in verbal order records.
• Name-surname, age, weight of the patient; name, dosage form (tablet-capsule-inhalant), concentration, dose, mode and cause of administration, amount and/or time of the medicine; name-surname of the person making the order must be included in verbal order records.
• Verbal order must not be made for medicines deemed to be high-risk by ODHC.

Health Services
137
Standards of Accreditation in Health - ODHS Kit
• Nurses and doctors must be trained on the practice of verbal order.
Abbreviations that must not be Used
» Abbreviations, signs and symbols that must not be used must be determined and listed by ODHC.
» No abbreviation, symbol or sign that are included in the list must be used in any stage of order processes.
» Rules for the use of abbreviations outside the list must be defined.
Communication during Patient Transfer
» Patient transfer between the units must be conducted through proper management of transfer (stretcher, wheelchair etc.).
» The patient must be accompanied by a member of the health staff during transfer. During transfer and referral of the patient necessary personal information concerning the patient and information about the care process must be conveyed by the health personnel through understandable and practical methods (Handover communication technique etc.) in an accurate and thorough manner.
Communication in the Consultation Process
» The process concerning taking into account consultation held within or outside the unit must be planned. The following issues must be handled at miminum:
• How the consultation services deemed to be necessary for diagnosis and treatment will be provided must be determined.
• How the records about consultation will be kept must be determined.
• The process regarding pathology consultation that is conducted in an intraoperative manner must be identified.
• The process concerning external consultation of examination material must be identified. (transfer of the material, how the result of consultation will be reported, how the patient and/or doctor will be informed about the result of the consultation)
» Consultation process must be controlled by the relevant primary doctor and patient care process must be reevaluated in line with the consultation report.

Health Services
138
Department of Quality, Accreditation and Workers' Rights in Health
Standard 5
Code Standard Code Assessment Criteria
SH.H
B.05
.00
Patients that carry the risk of harming themselves or others must be taken under control.
SH.H
B.05
.01
Patients must be assessed in terms of the risk of harming themselves or others.
SH.H
B.05
.02
Necessary measures must be taken against patients that carry the risk of harming themselves or others.
Goal
Agitated, confused and aggressive patients, patients diagnosed with dementia, delirium or suicide attempt and certain patient groups with psychiatric disorders are among the patient groups that carry a high risk of harming themselves or others. The goal is to prevent the patients from harming themselves or others in the case of the above-mentioned conditions.
Objectives
» Patient Safety
» Healthy Work Life
» Suitability
» Timeliness
» Continuity
Standard Requirements
Risk Assessment of Patients that may Harm Themselves or OthersPatients that may harm themselves or others during the care service must be determined and the relevant personnel must be informed about the situation.

Health Services
139
Standards of Accreditation in Health - ODHS Kit
Measures to be Taken
Measures to be taken against patients that may harm themselves or others must be planned.
Measures to be taken at minimum against patients that carry the risk of harming themselves or others are as follows:
» Patient that carry a high risk of harming themselves or others must be monitored more frequently.
» Action must be taken to make sure that health personnel can access the patient easily when necessary.
» Patient room must be rendered safe (such as appropriate lightning, not using risky furniture, accessorier etc., rendering the windows safer)
» The practices that may be necessary in terms of patient care for certain patients must be determined together with the psychiatry consultant.
Standard 6
Code Code Assessment Criteria
SH.H
B.06
.00
The standardization of care for specific patient groups must be ensured.
SH.H
B.06
.01
Processes regarding specific patient groups and the care practices for these groups must be identified.
SH.H
B.06
.02
Care practices and procedures aimed at specific patient groups must be determined.
Goal
The goal is to ensure standardization of patient groups that are specific in terms of care practices and care practices that are specific to units that provide these groups with service within the scope of scientific rules and recognized approaches.

Health Services
140
Department of Quality, Accreditation and Workers' Rights in Health
Objectives
» Patient Safety
» Efficiency
» Suitability
» Timeliness
» Equity
Standard Requirements
Determination of Specific Patient Groups and the Processes regarding Care Practices Specific to These Groups» The following examples can be given for specific patient groups.
ODHC must determine specific patient groups in ODHC based on these examples:
• Psychiatric patients
• Patients receiving radiotherapy/chemotherapy
• Geriatric patients
• Patients whose immune systems have been suppressed
• Pregnant women
• Substance addicts
• Patient groups with bacterial endocarditis risk
• Patients with critical orofacial post-trauma injuries or maxillomandibular fractures etc.
» The processes concerning care practices that are particular to specific patient groups must include the following issues at minimum:
• Processes of service provision
• Conditions of the environment where the service will be provided
• Necessary equipment
• Specific care practices and procedures
Determination of Practices and Procedures that are Particular to Specific Patient GroupsPractices and procedures that are particular to care needs of specific patient groups must be determined and conducted.

141
Radiation Safety
Code Standard Code Assessment Criteria
SH.R
G.01
.00
Measures must be taken to ensure radiation safety for patient/carers and the personnel.
SH.R
G.01
.01
A committee must be established to ensure radiation safety.
SH.R
G.01
.02 The areas where there are devices
that emit radiation must be identified and protective measures must be taken in these areas.
SH.R
G.01
.03
Rules must be determined for procedures that entail the use of radiation.
Goal
To take measures in order to reduce exposure of patients and employees to radiation in radiation areas
Objectives
» Patient safety
» Healthy work life
» Efficiency
» Timeliness
» Compliance

Health Services
142
Department of Quality, Accreditation and Workers' Rights in Health
Standard Requirements
Committee on Radiation Safety
A committee must be established in order to carry out radiation safety activities. The committee must carry out the activities below:
» To reduce the risks arising from medical irradiation practices at ODHC
» To plan the measures to be taken
» Decision making on the evaluation of radiation sources in terms of patient and employee safety by monitoring the said sources
» To monitor implementation of the decisions taken
Supervisors must be designated by the committee in order to follow the process or section-based actions to ensure the radiation safety of patient and employees.
Radiation Areas
The area must be defined according to the quality of radiation practice in radiation in ODHC. Radiation units must be classified in accordance with their radiation levels.
Preventive measures and Rules of Procedure
Patient-, carer- and employee-oriented rules of procedure must be determined taking into consideration the properties of the radiation areas defined and the processes of medical irradiation performed. Measures must be taken to reduce radiation exposure.
Physical Arrangements
» Authorised agencies and institutions must be licensed in accordance with the relevant legislation.
» There must be shielding in place in areas where there is a radiation source.
» There must be warning signs in radiation areas.
» Suitable ventilation conditions must be provided for radiation areas.

Health Services
143
Standards of Accreditation in Health - ODHS Kit
» Physical arrangements must be planned in such a way as to ensure that patients, carers and employees are away from the radiation source as far as possible. Waiting rooms must be outside the radiation zones.
» Measures to be taken in case of a probable accident which could jeopardize radiation safety, must be determined. Wastes arising from radioactive substance usage must be brought under control.
Arrangements for Patient and Carers
» It must be ensured that the patient uses the necessary radiation protective equipment.
» Only the area which will be imaged must be irradiated. The area necessary for the diagnosis in the panoramic radiography and cephalography must be determined, and only the area to be imaged must be irradiated.
» Within the framework of measures for reducing the exposure to radiation, only the patient to be imaged must be taken into the imaging room.
» Attention must be paid to the position errors in panoramic radiography.
» Inquiries on the pregnancy and pregnancy suspicion must be carried out in the processes of request and implementation respectively.
» If medical irradiation is obligatory for pregnant women and the women with pregnancy suspicion, they must be informed about radiation safety and protective measures must be taken.
» Arrangements must be in place to ensure patient comfort and privacy at every stage of the medical irradiation process.
» Measures must be taken to reduce children’s exposure to radiation during imaging. Repeated imagings must be kept to a minimum.
» Doors of imaging unit must be closed while the imaging is conducted.
» Carers must not be let into the imaging area unless it is not necessary. If they are let in, they must use protective equipment.
» Calibration and quality control tests must be periodically carried out in accordance with the utilisation frequency of devices emitting radiation.

Health Services
144
Department of Quality, Accreditation and Workers' Rights in Health
Arrangement for Employees» It must be ensured that employees use protective equipment.
» Radiation protectors must be controlled (at least once a year and if necessary).
» It must be ensured that employees use their own personal dosimeter.
» Dosimeter results must be monitored and evaluated, and if necessary, actions must be taken to improve them.

145
Standard 1
Code Standard Code Assessment Criteria
SH.P
L.01
.00
Physical environment of the prosthesis laboratory must be arranged so as to ensure safety of the prosthesis and the personnel.
SH.P
L.01
.01
The areas that have been determined for the admission of prosthetic materials into the prosthesis laboratory, the preparation of the material for the procedure, its being processed and for the delivery must be arranged so as to ensure the safety of the prosthesis.
SH.P
L.01
.02
A healthy work environment must be ensured in all areas in the prosthesis laboratory.
Goal
To design physical conditions so that prosthetic material belonging to patient is admitted under appropriate conditions, it is prepared before process, it is processed and the prosthesis is delivered after process, and to create a healthy work environment for laboratory staff.
Objectives
» Patient Safety
» Healthy Work Life
Prosthesis Laboratory Services
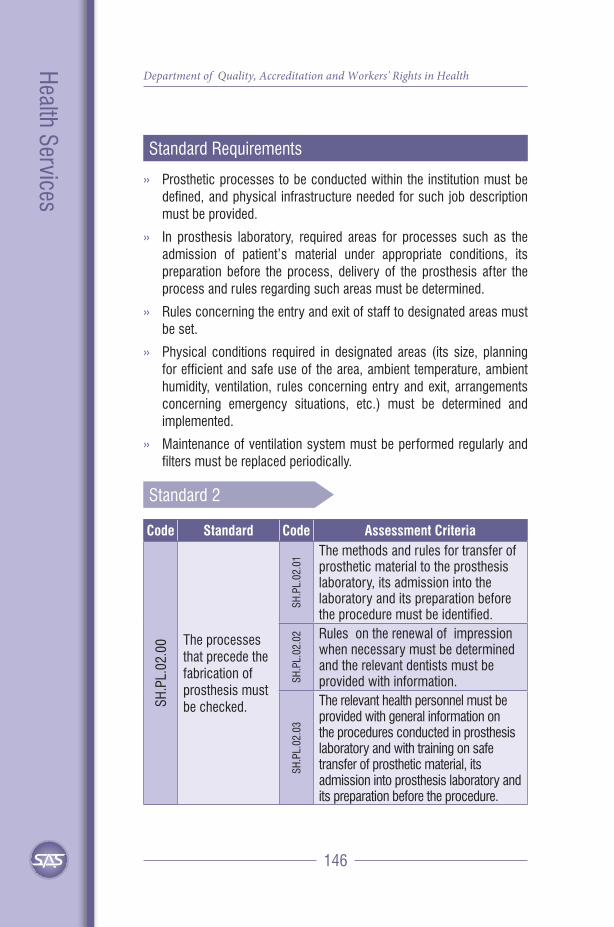
Health Services
146
Department of Quality, Accreditation and Workers' Rights in Health
Standard Requirements
» Prosthetic processes to be conducted within the institution must be defined, and physical infrastructure needed for such job description must be provided.
» In prosthesis laboratory, required areas for processes such as the admission of patient’s material under appropriate conditions, its preparation before the process, delivery of the prosthesis after the process and rules regarding such areas must be determined.
» Rules concerning the entry and exit of staff to designated areas must be set.
» Physical conditions required in designated areas (its size, planning for efficient and safe use of the area, ambient temperature, ambient humidity, ventilation, rules concerning entry and exit, arrangements concerning emergency situations, etc.) must be determined and implemented.
» Maintenance of ventilation system must be performed regularly and filters must be replaced periodically.
Standard 2
Code Standard Code Assessment Criteria
SH.P
L.02
.00 The processes
that precede the fabrication of prosthesis must be checked.
SH.P
L.02
.01 The methods and rules for transfer of
prosthetic material to the prosthesis laboratory, its admission into the laboratory and its preparation before the procedure must be identified.
SH.P
L.02
.02 Rules on the renewal of impression
when necessary must be determined and the relevant dentists must be provided with information.
SH.P
L.02
.03
The relevant health personnel must be provided with general information on the procedures conducted in prosthesis laboratory and with training on safe transfer of prosthetic material, its admission into prosthesis laboratory and its preparation before the procedure.

Health Services
147
Standards of Accreditation in Health - ODHS Kit
Goal
To ensure the suitability and safety of the prosthesis by controlling all its related processes from impression taking to the transfer of the prosthetic material to the laboratory, its admission and preparation
Objectives
» Patient safety
» Efficiency
» Effectiveness
» Productivity
» Suitability
Standard Requirements
Impression Taking» General rules concerning impression taking must be set, and relevant
staff members must be trained.
» The time the impression is taken must be recorded correctly.
» Impression taking, its admission to or refusal by the laboratory must be recorded on the Information Management System (IMS) as separate stages, and they must be seen by authorized users.
Transfer of Prosthetic Material» Relevant staff must be informed about such necessities as the transfer
box to be used for the transfer of prosthetic material to laboratory, the method of transfer (manual methods, air system, etc.), suitable impression position, transfer temperature, etc.
» Maximum acceptable transfer periods for prosthetic material must be determined. Relevant training must be provided for staff members in charge for the purposes of carrying out the transfer through correct method and within time set.

Health Services
148
Department of Quality, Accreditation and Workers' Rights in Health
Admission of Prosthetic Material to Laboratory and Its Preparation for Procedure
» In order to ensure prosthesis safety, arrangements must be made with the aim of assessing the suitability of admitted prosthetic material to impression taken and admitting or refusing the material on the basis of this assessment.
» In the records concerning the admission or refusal of prosthetic material, date and time, department/physician sending the material, by whom it was admitted or refused, and if it was refused, reasons for refusal must be indicated.
» No action must be taken in relation to prosthetic material before its admission to laboratory.
» Admission or refusal of prosthetic material must be made through IMS.
» Relevant staff must be trained on how to run admission and refusal processes.
» Analyses must be made in relation to prosthetic material refused, and necessary corrective actions must be taken.
Standard 3
Code Standard Code Assessment Criteria
SH.P
L.03
.00 The processes
regarding the fabrication of prosthesis must be checked.
SH.P
L.03
.01 The methods and rules about the
processes regarding fabrication of prosthesis in prosthesis laboratories must be identified.
SH.P
L.03
.02 Rules regarding effective and safe use
of the prosthetic material in prosthesis laboratories and other materials and devices must be identified.
SH.P
L.03
.03
Quality control procedures regarding the suitability of the prosthesis must be identified and implemented.

Health Services
149
Standards of Accreditation in Health - ODHS Kit
Goal
To ensure patient safety through the continuity of quality improvement activities concerning prosthesis production processes
Objectives
» Patient safety
» Efficiency
» Effectiveness
» Productivity
» Continuity
Standard Requirements
Standard requirements concerning prosthesis production process include the followings:
Modeling
» Stages involved in modeling must be defined, and rules concerning the stages must be set.
» Training must be provided for relevant staff about the rules set.
Completion of Prosthesis
» After modeling, all stages until the completion of the prosthesis must be defined, and rules concerning these stages must be set.
» Training must be provided for relevant staff about the rules set
Material and Device Management
» Arrangements must be made concerning the control and safe use of all devices and materials used in prosthesis making in prosthesis laboratories.
Health Services
150
Department of Quality, Accreditation and Workers' Rights in Health
» Plans must be developed for the management of devices and materials.
» An inventory of all devices must be available, and their maintenance and calibration must be made.
» Descriptive information about devices must be recorded. Such records must include at minimum the following information:
• Name of the device
• Brand and model of the device
• Date of production and launch
• Serial number
• Details of distributor
» A folder containing information about the operation of the device must be prepared, and attention should be paid to the fact that information included in the folder is current and it is easy to understand for staff. This folder should include at minimum the following information and documents:
• User manual or CD
• If any, calibration records and certificates of the device
• If any, quality control results
• Failure report form
• Contact details of firm
• User training certificates
» Training must be provided for users about operation of the device, maintenance and cleaning of the device, frequently encountered problems while operating the device and how to solve these problems.
» Failures, failure reporting and repair processes must be recorded.
Rules must be set in order to ensure safe and economic use of materials.
Quality Control of Prosthesis» Quality control actions concerning the suitability/unsuitability of the
prosthesis must be defined and implemented.
» Data on quality control process of prosthesis must be traceable.

Health Services
151
Standards of Accreditation in Health - ODHS Kit
Standard 4
Code Standard Code Assessment Criteria
SH.P
L.04
.00 The processes
that follow the fabrication of prosthesis must be checked.
SH.P
L.04
.01
The prosthesis that has been completed must be delivered with Prosthesis Delivery Report.
SH.P
L.04
.02
The prosthesis must be inserted within the set time of delivery.
SH.P
L.04
.03
Patients must be informed about the rules regarding the use of prosthesis.
Goal
To take required measures to ensure patient safety in all processes from the completion of the prosthesis to its use to the benefit of patient
Objectives
» Patient safety » Efficiency
» Suitability » Timeliness
» Continuity » Patient oriented
Standard Requirements
Extra laboratory processes taking place after the completion of the prosthesis include reporting of the prosthesis’ delivery and use of the prosthesis made for the benefit of the patient.

Health Services
152
Department of Quality, Accreditation and Workers' Rights in Health
Prosthesis Delivery Reports
» Laboratory should determine at minimum what of kind information must be included in prosthesis delivery reports.
» Minimum time parameters to be included in delivery reports are as follows:
• Date and time when impression was taken
• Date and time when impression was admitted to laboratory
• Date and time when modeling started
• Date and time when prosthesis delivery report was recorded.
» Prosthesis delivery reports must have a dynamic structure to which comments, suggestions and opinions of relevant staff members can be added.
» Time of the prosthesis delivery and information to be provided in relation to them are as follows:
• Time of prosthesis delivery must be determined on the basis of ODHC conditions, its needs and scientific requirements.
• Relevant healthcare staff must be informed about the time of delivery determined.
• Patients must be informed about the time of the prosthesis delivery.
• If there is a delay in the delivery of the prosthesis due to any reason it should be determined how information will be provided.
Standard 5
Code Standard Code Assessment Criteria
SH.P
L.05
.00
Traceability of the processes regarding prosthesis laboratory must be ensured.
SH.P
L.05
.01
Records must be kept to ensure traceability of the impression and the prosthesis in all the processes.

Health Services
153
Standards of Accreditation in Health - ODHS Kit
Goal
To ensure the traceability of processes related to prosthesis with the aim of collecting data to analyze and improve prosthesis laboratory processes.
Objectives
» Efficiency » Effectiveness
» Timeliness » Continuity
» Patient safety
Standard Requirements
» In prosthesis laboratories, it must be ensured that each stage of prosthesis, from impression taking to prosthesis making, is traceable.
» In prosthesis laboratory information management system minimum following records must be available in relation to prosthesis making process:
• Name and surname of the patient
• Protocol number
• Date and time of examination
• Name, surname and specialty of the dentist examining the patient
• Material used for impression taking
• In relation to the impression taken
√ Date and time
√ Date and time on which it was admitted to laboratory and by whom it was admitted
• Date and time on which modeling started
• If there is, repetition of impression taking and its results
• Date and time on which prosthesis delivery report was recorded
• Name and surname of staff member and/or laboratory supervisor approving the report

154
Surgical Safety
Standard 1
Code Standard Code Assessment Criteria
SH.G
C.01
.00 Patient safety
must be ensured in surgical procedures. SH
.GC.
01.0
1
Measures must be taken to ensure patient safety before, during and after the surgical procedure.
Goal
To ensure that surgical practices are in conformity with the universal protocol and patient safety solutions determined by the World Health Organisation in safe surgery, which occupies an important place in terms of preventing medical errors
Objectives
» Patient Safety
» Patient-orientedness
» Efficiency
» Effectiveness
» Equity

Health Services
155
Standards of Accreditation in Health - ODHS Kit
Standard Requirements
Documentation
ODHC must document the procedures, steps and rules on the processes of safe surgery. Documents cover:
» Rules on surgical processes
» Parameters on operating room environment
» Operating room entry and exit rules
» Management of medicine, material and devices in operating rooms
Informing Patient and Receiving Consent
» The dentist and anaesthesiologist must verbally inform the patient about the surgery and anaesthesia. With this information, it is aimed that the patient knows about his/her problem and treatment, the procedure offered and its risks, who would do the operation when and where.
» After the patient is given the right to decide completely by his/her own free will, a consent form must be signed showing that s/he agrees the surgical operation and the anaesthesia method to be carried out by her/his own free will.
Marking Surgical Area
Surgical area must be marked prior to surgical operation if the extraoral area is subjected to intervention:
» Marking must be done by the person who will carry out the surgical operation or a dentist from the team. Marking must be done before the patient is taken to operating room.
» Surgical area marking must be done within the period of time when the patient is awake and conscious, and the patient must confirm the marking area during the marking process.
» Marking must be done through a clear method which is determined beforehand.
» The area to be operated must be marked. If there will be more than one operation, all the areas must be marked.

Health Services
156
Department of Quality, Accreditation and Workers' Rights in Health
» Marking must be done in a way that is not erased easily. Marking must not be swept during surgical area cleaning.
» Marking must be done to the area or its surroundings, and it must be clear.
» Contraindications relevant to the surgical area marking must be determined by ODHC. If a contraindication is found, we must define how the confirmation processes will be conducted.
ODHC Safe Surgery ChecklistTR
“Safe Surgery Checklist” drawn up by World Health Organisation (DSÖ) was put into practice under the title of Safe Surgery ChecklistTR after being developed exclusively for Turkey in 2009. It has been decided that observance to the Safe Surgery ChecklistTR is necessary because nowadays Oral and Dental Health Centres are also places where surgical operations take place.
ODHC Safe Surgery ChecklistTR covers 4 sections:
1. The period before leaving the clinic (Before Leaving the Clinic)
2. The period before anaesthesia is administered (Before Administering Anaesthesia)
3. The period after anaesthesia and before surgical incision (Before Surgical Incision)
4. The period before the patient leaves the operating room, during wound closure or right after its closure (Before Leaving the Operation Room)
» Responsibilities for the implementation of the checklist must be determined for every step and Safe Surgery Checklist must be implemented efficiently.
» All steps must be verbally checked in order to ensure that key activities are implemented. The person who carries out the checklist must check whether or not they are implemented and allow to proceed the next step.
» ODHC Safe Surgery ChecklistTR must be archived in the patient file.
Patient Transfer
» Patient identity must be confirmed at every step of patient transfer and patient delivery should be realised through written and verbal information and records.

Health Services
157
Standards of Accreditation in Health - ODHS Kit
» Measures must be taken to ensure safety during patient transfer. The patient must be transferred in company with healthcare professionals.
Check and Safety of Personal Belongings and Prosthesis
» The process of delivering patient’s removable prosthesis and valuable items must be defined before operation.
» Procedure for the protection of patient’s belongings must be determined.
» Final check for non-removed belongings and prosthesis must be carried out by operating room staff.
Pre-operative Preparations
» Necessary preparations for pre-operative procedures before planned and emergency operations must be determined and planned.
» Medicines and materials to be used during surgical operations must be supplied and necessary checks must be done. Relevant devices must be ready for use.
» Planning of blood and blood products must be done for the cases having risks of haemorrhage in the pre-operative period. Blood and blood products which may be necessary during surgical operation must be available within the scope of this plan.
» Patients and carers must be informed about the pre-operative preparations and the points to take into consideration. Healthcare professionals must check the preparations.
Anesthesia Applications
» The patient should be evaluated by the anesthesiologist and reanimation specialist in the preoperative period, according to which anesthesia method and necessary premedication should be planned.
» A checklist should be used to ensure the safety of anesthesia applications.
» The anesthesia safety checklist should be kept in the patient file .
Surgical Prophylaxis
Prophylaxis guidelines must be drawn up within the framework of rational use of antibiotics. Efficiency of practices must be monitored in line with these guidelines, and improvements must be made when necessary.

Health Services
158
Department of Quality, Accreditation and Workers' Rights in Health
Postoperative Care» Rules on transferring patients from the operating room and recovery
room must be determined.
» Records on patients must be kept at every stage. It must be ensured that information and records on patients must be transferred to the next stage safely.
» The patient must be closely monitored in the postoperative period. Follow-ups relevant to the complications and risks jeopardising the patient safety must be planned and those follow-ups must be recorded.
Safety of Tissues Taken for DiagnosisArrangements on accurately labelling tissues taken for diagnosis during surgical operation and delivering them to the relevant laboratories must be in place. Employees must be trained on ensuring the safety of the tissue.
RecordsAll records on surgical operation must be kept completely and accurately in order to ensure safety and continuity of care and treatment.
Safe Surgery
3
Arrangements on accurately labelling tissues taken for diagnosis during surgical operation and delivering them to the relevant laboratories must be in place. Employees must be trained on ensuring the safety of the tissue. Records: All records on surgical operation must be kept completely and accurately in order to ensure safety and continuity of care and treatment.
ODHC SAFE SURGERY CHECKLISTTR
Name and surname of the patient Surgery/Area Surgery Date
I. Before Leaving the Clinic
II. Before Administering Anaesthesia
III. Before Surgical Incision
IV. Before Leaving the Operation Room
1. Patient’s: □ identity has been confirmed. □ surgery has been confirmed. □ surgical area has been confirmed.
9. Patient confirmed his/her □ identity □ surgery □ surgical area □ consent to the operation.
16. Have the team members introduced themselves with their names, surnames and roles? □ Yes
24. For the surgery performed, □ The patient □ The surgery □ The surgical area have been confirmed.
2. Has the patient consented to the operation?
□ Yes
10. Is there any marking in the surgical area? □ Yes □ Marking cannot be done
17. Has one of the team members confirmed the identity, the surgery and surgical area verbally?
25. Have the tools, sponges/compressors and needles been counted?
3. Is the patient hungry? □ Yes □ No
□ Yes □ Yes/Complete □ No
4. Is the surgical area shaved? □ Yes □ No
18. Have the critical events been reviewed? □ Estimated duration of surgery
26. On the label of sample taken from the patient: □ Patient’s name is written
5. Does the patient wear make-up/nail polish, valuable items or prosthesis?
□ Yes □ No
□ Expected haemorrhage □ Unexpected events which might take place during surgery □ Probable risks of anaesthesia □ Position of the patient
accurately □ The area where the sample has been taken from is written
6. Has the patient taken off all of her/his clothes and worn bonnet?
□ Yes □ No
11. Has the Anaesthesia Safety Checklist been completed? □ Yes
19. Has the prosthetic antibiotic been inquired about? □ It was administered within the last 60 minutes before incision
27. Have the postoperative critical requirements been reviewed? □ Recommendations of the anaesthetist:
7. Has the preparation of special material, implant, blood and blood product been confirmed?
□ Yes □ No
12. Is the pulse oximetry on the patient and operating? □ Yes
Risk Assessment of the Patient
□ cannot be used □ Recommendations of surgeon:
8. Are the necessary laboratory and radiology test results of the patient present? □ Yes
13. Does the patient have any known allergy? □ Yes □ No
20. Are the materials to be used ready? □ Yes
28. Has department where the patient is transferred after surgery been confirmed? □ Yes
14. Are the required imaging devices available?
21. Is the sterilisation of the materials suitable? □ Yes
□ Yes □ No 22. Is blood glucose control necessary? □ Yes
15. Does the patient have the risk of haemorrhage for 500 ml or more? □ No □ Yes; suitable vascular access and liquid have been planned.
23. Will anticoagulant be used? □ Yes
Checklist supervisor: Name-Surname, Signature
Checklist supervisor: Name-Surname, Signature
Checklist supervisor: Name-Surname, Signature
Checklist supervisor: Name-Surname, Signature
•Each section must be checked and marked by the relevant supervisors.
55 54 53 52 51
18 17 16 15 14 13 12 11
61 62 63 64 65
21 22 23 24 25 26 27 28
48 47 46 45 44 43 42 41
85 84 83 82 81
31 32 33 34 35 36 37 38
71 72 73 74 75

Health Services
159
Standards of Accreditation in Health - ODHS Kit
Standard 2
Code Standard Code Assessment Criteria
SH.G
C.02
.00
Conditions of the operating room must be appropriate to ensure safe surgery.
SH.G
C.02
.01
Rules regarding operating rooms must be determined.
SH.G
C.02
.02
Operating rooms must be arranged so as to ensure patient and employee safety.
SH.G
C.02
.03
Management of drugs, material and devices must be ensured.
SH.G
C.02
.04
Measures must be taken to ensure uninterrupted power supply.
Goal
To arrange the conditions of the operating room for patient and employee safety
Objectives
» Patient Safety » Efficiency
» Effectiveness » Healthy Work Life
Standard Requirements
Operating Room Areas
» Operating room areas must be handled in at least three different categories in accordance with the procedures taking place in these areas as well as the working conditions and rules. These areas must be defined as:

Health Services
160
Department of Quality, Accreditation and Workers' Rights in Health
• Sterile (First) Area: Operating rooms and the place for surgical hand wash.
• Clean (Second) Area: The area between sterile and non-sterile areas. Sterile area must not be opened to non-sterile area without a barrier in between.
• Non-sterile (Third) (Unclean) (Dirty) Area: Area which connects the operating room with the other departments.
» The areas defined must be separated and rules must be established according to the features of each. Rules must be established on patient and personnel entry to and exit from the operating room as well as on transfer of personnel between the areas.
» Cross-domain transitions must comply with national and international rules and norms.
» There must be waiting rooms for the carers/family members of the patient. These areas must be ergonomic and comfortable.
» Arrangements for informing carers/family members must be put in place.
Operating Rooms
» Operating rooms must have such a size and such capacity that the surgical team is dressed and the patient is covered in a sterile way which would not pose any obstacles for the anaesthesia team.
» In the operating room: The floor, ceiling and wall surfaces must be smooth. There must not be any cracks on the surfaces. Junction points of door, windows and walls must be smooth and without protrusion. Materials to be used in the wall, ceiling and the floor of the operating rooms must be antibacterial, suitable for disinfection and cleaning.
Ventilation Conditions
» Ideal temperature and humidity rates of operating areas must be determined and controlled.
» HEPA-filtered ventilation system must be used in sterile areas.
» Air stream must circulate from sterile area to unclean area (positive-pressure air stream).

Health Services
161
Standards of Accreditation in Health - ODHS Kit
» Ventilation systems must complete at least 15 filtered air exchanges per hour and at least three of them (20%) must be exchanged with fresh air.
» Periodical measurements must be carried out in accordance with the number of particles in the air and supervisors must evaluate the results. Measurements must be recorded.
» Ventilation system must be maintained regularly and filters must be changed at certain intervals deemed necessary.
Medical Gas Systems
Medical gas pressure measurements must be regularly checked through medical gas panel and indicators on the anaesthetic apparatus. Medical gas system must be regularly checked and maintained.
Management of Medicines, Materials and Devices
» Plans for the management of devices used in operating rooms must be developed. All devices must have inventories. Periodical maintenance and calibration must be carried out.
» Technical control of the devices must be carried out before surgery. Equipment and devices, which are suspected to be defective, must not be used.
» There must be sufficient number of sockets which are connected to the uninterrupted power supply in order to meet the energy requirements until the generator starts in case of power cut in the operating rooms. Devices which must not interrupt the process of surgery must be connected to those sockets. Uninterrupted power supplies must be periodically maintained within the scope of a plan.
» Sterile materials let into the operating room must be checked (in terms of expiry date, durability of package, colour change of indicator inside the package). Rules on packaging and preservation of the sterile materials must be abided by.
» Medicines used in operating room must be efficiently managed.


Support Services


165
Standard 1
Code Standard Code Assessment Criteria
DH.O
H.01
.00
All the areas at ODHC must be clean for the safety and satisfaction of patient, carer and personnel.
DH.O
H.01
.01
Risk levels must be determined in all the areas of ODHC to ensure the control of cleaning and infections.
DH.O
H.01
.02
Cleaning rules for risk levels must be identified and an ODHC cleaning plan must be developed and put into place.
Goal
To ensure safety and satisfaction of patient, carer and personnel by ensuring continuity and efficiency of cleaning in all the areas of ODHC
Objectives
» Patient-Orientedness » Patient Safety
» Healthy Work Life » Efficiency
» Continuity
Accommodation Services

Support Services
166
Department of Quality, Accreditation and Workers' Rights in Health
Standard Requirements
Determination of Risk Levels and Cleaning Rules with regard to These Levels» Risk assessment for cleaning and infection control must be made in
all the areas of ODHC.
» Cleaning rules, material to be used and physical conditions necessaryto increase efficiency of cleaning must be determined in line with therisk levels that have been determined.
Development and Implementation of ODHC Cleaning Plan» Cleaning plan and related documents must be created so as to
encompass all the areas of ODHC and the necessary work must beundertaken.
» The following issues must be handled at minimum in the documents:
• Risk level that is determined based on the unit or area
• Cleaning material to be used in the area in question
• Rules about cleaning and safe use of material and equipment
• Frequency of cleaning
• Cleaning rules
• Rules about how cleaning will be done after accidents that maycause potential mess
• How and by whom the control of cleaning will be conducted
Standard 2
Code Standard Code Assessment Criteria
DH.O
H.02
.00
Processes regarding catering for inpatient/ carer and the personnel must be identified.
DH.O
H.02
.01
Safe supply and storage of the food must be ensured.
DH.O
H.02
.02
Processes regarding preparation of the food under the set conditions must be identified.

Support Services
167
Standards of Accreditation in Health - ODHS Kit
Code Standard Code Assessment Criteria
DH.O
H.02
.03
Food must be distributed according to the set rules.
DH.O
H.02
.04
Health screening of the personnel distributing the food must be conducted.
Goal
To provide inpatient, carer and personnel with efficient and safe catering services by taking into account their wishes, needs, expectations and values
Objectives
» Patient-Orientedness
» Patient Safety
» Healthy Work Life
» Efficiency
Standard Requirements
Supply and Storage of Food» Rules to pay attention to with regard to supply according to types
of food (qualifications that must be sought in line with types of food, quality control criteria, minimum documents and requirements necessary for admission of the supplier, transportation of food and its delivery) must be determined.
» Storage conditions (temperature, preservation time, packaging conditions if any, rules regarding arrangement of the food on the shelves and in the cabinets etc.) must be identified in line with types of food.

Support Services
168
Department of Quality, Accreditation and Workers' Rights in Health
» When storing food, expiry dates must be followed-up in an efficientmanner.
» The products in the storehouse must be arranged so as not to comeinto contact with the ground or wall and food products must bearranged separately.
Preparation Processes of the Food» Food must be prepared by taking into account the requirements of the
medical treatment of the patient.
» Cultural and moral values of the patient must be taken into accountwithin the scope of catering services.
» Food must be prepared in a hygienic way:
• The areas where the food is prepared must be different fromother areas. (food storage areas, area where the filthy material iscleaned.)
• All the personnel must use protective equipment such as mask,bonnet, gloves and footwear)
• Material and equipment used while preparing food must be clean.
• Rules about sanitation of the food (like washing fruit andvegetables) must be determined and followed.
• Necessary conditions must be provided to ensure personalhygiene of personnel in charge of food in an efficient manner.
» Replicate samples must be taken from food to make the necessaryanalyses in the case of food poisoning.
Distribution of Food» Food must be distributed in line with the types of the food and by
taking into account warmth and presentation of the meal and hygienerules.
» There must be a cover or lid on the food.
» Dinner trolleys and other equipment and material used in transportation and distribution of food must be cleaned and disinfected.
» The personnel distributing the food must use equipment like bonnet,gloves and mask.

Support Services
169
Standards of Accreditation in Health - ODHS Kit
Health Screening of the Personnel
All the personnel responsible for catering services must go through health screening periodically and the things to do if a problem that might threaten food safety is detected in screenings must be identified.
Standard 3
Code Standard Code Assessment Criteria
DH.O
H.03
.00
Laundry services must be provided in a safe and efficient manner to ensure patient and personnel health at ODHC.
DH.O
H.03
.01
Processes regarding the delivery of laundry services must be identified.
DH.O
H.03
.02
The laundry room must be arranged so as to ensure efficient conduct of service processes.
DH.O
H.03
.03
Rules regarding the use of laundry equipment must be determined.
Goal
The goal is to make sure that laundry services provided in ODHC are safe in terms of patient and employee health.
Objectives
» Patient-Orientedness
» Patient Safety
» Healthy Work Life
» Efficiency

Support Services
170
Department of Quality, Accreditation and Workers' Rights in Health
Standard Requirements
Identification of Processes
Processes regarding collection, transport, sorting out, washing, ironing of all the textile products used in ODHC, distribution of the washed products to the areas where they will be used, storing the products and arrangement of the laundry room must be identified.
Laundry Room
» Laundry room must have enough space for washing, drying, ironing and storing; there must be separate areas for clean and dirty laundry.
» The floor and walls of the laundry room must be made of smooth and strong material that is easy to clean.
» Ventilation and lightning conditions must be appropriate so as to make sure the laundry is clean in an efficient manner and to ensure safety and comfort of the personnel.
» Rules must be determined about the use of equipment in the laundry room and cleaning, maintenance, repair and control of the equipment must be ensured.
» Relevant personnel must be trained on the use of equipment in the laundry room.
Standard 4
Code Standard Code Assessment Criteria
DH.O
H.04
.00
Patient/examination rooms and the areas used by patients/carers must be safe and ergonomic.
DH.O
H.04
.01
All departments providing service must be designed in a way that ensures comfort of the patient.
DH.O
H.04
.02
Action must be taken to ensure easy access of the patient to the relevant health personnel.

Support Services
171
Standards of Accreditation in Health - ODHS Kit
Goal
To boost the morale and motivation of patients/carers by making sure that they are in a safe and comfortable environment
Objectives
» Patient-Orientedness
» Patient Safety
Standard Requirements
Patient Comfort
» The following aspects should be taken into account with respect to the services rendered at the ODHC:
• Clean and spacious ODHC service areas,
• Waiting areas to sit and relax when needed,
• Regulation of compulsory areas such as stairs, elevators, toilets, bathrooms, car parking areas in regard to needs of the patient (geriatric patients, pediatric patients, disabled patients etc.)
• Deleting factors that are dangerous to the safety of the patient
• The examination rooms containing the requirements for the medical service processes (such as inspection tables, washbasins, hand antiseptics, necessary examination instruments according to the relevant situation)
• Finding baby care and breastfeeding arrangements in outpatient clinics
Patient Rooms
» In clinics and patient rooms ventilation and lightning conditions must ensure safety and comfort of the patient.
» There must be the furniture necessary for patients in clinics and patient rooms.

Support Services
172
Department of Quality, Accreditation and Workers' Rights in Health
» The position of units and patient beds must be adjustable and must ensure safety of the patient.
» In clinics and patient rooms, there must be the equipment and material necessary for diagnosis and treatment of the patient. This equipment and material must be cleaned and disinfected.
» Areas must be determined to meet cleaning needs of patients and carers. There must be material necessary for personal hygiene in these areas.
» An area must be created so that carers can have rest.
Ensuring Easy Access to the Health Personnel
» Action must be taken to make sure that patient and carer can access the health personnel if needed (a call bell etc.)
» The call system for example must be accessible in clinics and patient rooms and in areas allocated for personal hygiene.
» Patient/carer must be informed about how to use the call system.
Standard 5
Code Standard Code Assessment Criteria
DH.O
H.05
.00
Safety/security services must be provided in ODHC to ensure safety of life and property of patient/carer and the personnel.
DH.O
H.05
.01
Processes regarding the delivery of Safety/Security services must be identified.
DH.O
H.05
.02
Safety of life and property of the patient/carer in ODHC must be ensured.
Goal
The goal is to ensure safety of life and property of patient/carer and the personnel in ODHC in an effective and efficient manner.
Support Services
173
Standards of Accreditation in Health - ODHS Kit
Objectives
» Patient Safety
» Healthy Work Life
» Efficiency
Standard Requirements
Planning of Safety/Security Services» There must be a plan in place to protect ODHC and people within
ODHC from all kinds of threats, dangers and harm such as sabotage, theft, looting and blow and to maintain surveillance, supervision and control services in an uninterrupted manner.
» There must be a security officer and security equipment in the designated areas of ODHC (surveillance camera, alarm system etc.)Storage times for security camera records must be determined.
» Working area, time and terms of reference of security officers must be determined.
Ensuring Safety/Security of Patient/Carer» Risk analyses must be made in the field of safety of life and property
and necessary measures must be taken.
» Risk analyses must encompass all the areas and units of ODHC. There must be areas where patients and carers can safely keep their personal belongings.
» Reporting process about events that threaten safety of life and property must be identified.
» Necessary improvement work must be undertaken as a result of the analyses made.

174
Facility Management
Code Standard Code Assessment Criteria
DH.T
Y.01
.00
A quality facility management structure and process must be established to ensure the quality and safety of healthcare services.
DH.T
Y.01
.01
A committee responsible for planning and coordinating activities related to facility management must be formed.
DH.T
Y.01
.02
Risks originating from the facility must be detected and necessary measures must be taken.
DH.T
Y.01
.03
Continuity and safety of core facility resources must be ensured.
DH.T
Y.01
.04
Issues related to physical conditions and operations must be reviewed periodically.
DH.T
Y.01
.05
There must be arrangements facilitating access to departments inside ODHC.
DH.T
Y.01
.06 Measures must be taken to facilitate
access to services by patients who are disabled, old or in need of help due to illness.
DH.T
Y.01
.07
Physical arrangements must be made to ensure the comfort of service users.

Support Services
175
Standards of Accreditation in Health - ODHS Kit
Goal
To establish the necessary infrastructure for permanent, safe and easily accessible service delivery for the patients and the personnel
Objectives
» Efficiency
» Patient safety
» Patient-orientedness
» Timeliness
» Continuity
» Healthy Work Life
Standard Requirements
Management and Documentation
» A committee must be formed in order to ensure planning and coordination of facility management-related activities. The duties and responsibilities of the personnel involved in facility management must be defined.
» Core and critical processes regarding facility management must be defined, and methods and rules thereof must be determined. The documents to be generated for this purpose must include at least the following:
• Duties and responsibilities of the facility management committee and supervisors
• Processes related to the identification of the current status of the health facility
• Improvement processes
• Core facility resources

Support Services
176
Department of Quality, Accreditation and Workers' Rights in Health
• Access to facility services
• Facility safety
Determination of Current Status and Improvements
» Current physical status and functional service efficiency of the health facility must be evaluated at regular intervals or when necessary.
» Risk analyses must be performed for facility safety.
» Necessary improvement activities must be carried out with regards to the current status and results of the risk analysis.
Please See Risk Management chapter
Core Facility Resources and Safety
» Continuity of core facility resources (Electricity, water natural gas, heating, cooling medical gas etc.) must be ensured for the uninterrupted delivery of healthcare services.
» Timely maintenance and checks of core facility resources in all systems must be performed.
» Backup systems must be set in the case of possible critical errors. The risky areas covered by these systems must be determined by the facility management committee.
Access to Facility Services
» Necessary arrangements to access the departments inside the ODHC must be provided to ensure patient and caretaker satisfaction and timely treatment. Necessary physical and functional arrangements must be realized, with the groups of disabled patients and patients in need of special care. These arrangements must include at least the following:
• Guiding sings and services
• Waiting areas used by patients, carers and visitors
• Comfort and safety of patient rooms
• ODHC-wide arrangements for the disabled, the elderly or patients in need of help due to their illness
• Environmental arrangements (car lots, landscape, etc)

177
Code Standard Code Assessment Criteria
DH.A
Y.01
.00
Safe and effective management of waste produced at ODHC must be ensured to protect human and environmental health.
DH.A
Y.01
.01
A Waste Management Plan must be prepared.
DH.A
Y.01
.02
Waste must be sorted at the source.
DH.A
Y.01
.03 Necessary steps must be taken to
ensure that waste is transported, temporarily stored and disposed in appropriate conditions.
DH.A
Y.01
.04
Personnel involved in waste management must be trained.
Goal
To prevent waste from harming human health and the environment starting from the composition of the waste at ODHC until its delivery to the competent authority for the disposal.
Objectives
» Patient Safety» Healthy Work Life» Patient-orientedness
Waste Management

Support Services
178
Department of Quality, Accreditation and Workers' Rights in Health
Standard Requirements
Preparation of Waste Management Plan
» A Waste Management Plan must be prepared at ODHC. The Waste Management Plan must include at least the following:
• Source, amount and types of waste
• Measures related to the minimization of waste at the source
• Equipment and tools to be used in waste management
• Collection frequency and rules
• Temporary storage systems
• Cleaning and disinfection of relevant equipment
• Measures to be taken in the case of an accident
• Training of the personnel assigned to collect and transport waste
• Determining the institution to which the waste will be delivered
• Delivery of waste
• Monitoring of waste processes
» Waste management supervisor must be identified.
Waste Sorting at Source
» Waste must be defined at least in the following categories/types per unit basis:
• Domestic Waste
• General domestic waste
• Packaging waste
• Medical Waste (infectious, pathogenic, sharp objects)
• Infectious waste
• Pathological waste
• Sharpy waste
• Hazardous Waste
• Radioactive Waste

Support Services
179
Standards of Accreditation in Health - ODHS Kit
» Waste generated at the units must be sorted in accordance with their type.
» Waste must be put in separate bags/boxes having the required properties in accordance with their types.
» The amount of medical and hazardous waste must be measured and monitored on the basis of ODHC and unit. Processes related to waste should be examined in terms of requirements for reducing waste quantities..
» Arrangements must be made for recyclable waste.
Waste Transportation, Temporary Storage and Disposal Operations» Waste must be collected by personnel trained to perform such tasks.
» The clothes worn by the personnel assigned with the collection and transportation of waste must possess the necessary properties.
» The collection and transport of waste should be carried out as far as possible from areas where human traffic is concentrated.
» Waste must be collected at the temporary storage area.
» There must be containers or temporary waste storerooms in sizes suitable to the size of ODHC and having the suitable properties.
» Waste must be stored temporarily in such a way as not to exceed the maximum waiting period determined within the scope of the national legislation.
» The stored waste must be submitted to the competent authority for the ultimate disposal.
» Waste storerooms must be cleaned and disinfected.
Waste Management TrainingsPersonnel working on waste management must be trained. Trainings must include at least the following:
» Types of waste and sorting of waste in accordance with their types
» Collection, transportation and temporary storage of waste
» Health risks, injuries and diseases which might be caused by waste
» Measures to be taken in the case of an accident or injury

180
Code Standard Code Assessment Criteria
DH.B
Y.01
.00
A safe and effective information management system must be present at ODHC.
DH.B
Y.01
.01 Those in charge of carrying out and
coordinating activities related to information management must be identified.
DH.B
Y.01
.02 The necessary technical and
supporting infrastructure must be established for the efficiency of information management.
DH.B
Y.01
.03
Measures must be taken for the security of medical records that are physically stored.
DH.B
Y.01
.04
Necessary measures must be taken to ensure information security and confidentiality.
DH.B
Y.01
.05
It must be ensured that the information is timely and continual.
DH.B
Y.01
.06
Personnel must be trained for effective use of information management.
Goal
To ensure that medical and personal information obtained in the ODHC processes are recorded and stored properly and safely, and to ensure the communication of the needed information to the right person at the right time.
Information Management

Support Services
181
Standards of Accreditation in Health - ODHS Kit
Objectives
» Efficiency
» Patient Safety
» Timeliness
» Continuity
» Healthy work life
Standard Requirements
Management and Documentation» Information management supervisors must be identified, and their
roles and responsibilities must be defined. The supervisors must identify the current situation in information management, detect the possible risks in the processes and initiate the necessary corrective and preventive activities.
» Information to be used in the information management process and the methods and rules pertaining to those must be determined with the needs and critical processes of ODHC in mind. Documents to be prepared must comprise at least the following topics:
• Physical and technological measures
• Information security
• Information confidentiality
• Information continuity
• Access to external information sources
• Authorization
• Remote access
Technical Support InfrastructureRisks related to hardware and software problems must be detected, against which measures must be taken for the uninterrupted operation of information management systems.

Support Services
182
Department of Quality, Accreditation and Workers' Rights in Health
Information Security and Confidentiality» The confidentiality and security of personal or medical, written or
electronic information obtained about personnel or patients is essential. Access to these records must be limited by way of authorization, and access by external sources must be under control.
» What information can be accessed by the users and when and how they can access it within the scope of the authorization must be defined; measures must be taken against unauthorized access.
» Computers connected to information management at ODHC must be monitored to track unauthorized access.
» Data must be backed up on a regular basis in order to prevent data loss in cases of failure or unauthorized access; regular maintenance and tests must be performed on the servers to prevent failures, and the operation systems or software used in the server must be up-to-date.
» A system must be set to track the changes or deletion in the data when there is unauthorized or erroneous interference with the data from internal or external sources.
» Physically stored medical records must be stored in such conditions as to prevent any harm to the records, within the rules of the relevant legislation. The necessary physical and functional measures must be taken, and security of written information must be ensured for these types of records.
Timeliness and Continuity of Information» Cases where information management systems have been disabled
to make sure healthcare services are delivered on time and to ensure continuity, or where there are slowdowns or failures in the systems must be tracked, improvement must be made and it must be ensured that the information is timely.
» Retrospective follow-up of all the information collected must be performed in information management systems; thus, the continuity of information must be ensured.

183
Material and Device Management
Code Standard Code Assessment Criteria
DH.MC.01.00 Efficient,
effective and safe use of materials and devices must be ensured.
DH.MC.01.01
Those in charge of management of materials and devices must be determined.
DH.MC.01.02
Materials and devices must be determined and supplied in accordance with the needs of the institution.
DH.MC.01.03
Materials must be conserved in proper conditions.
DH.MC.01.04
Necessary physical conditions must be met to ensure that the devices work in proper working conditions.
DH.MC.01.05
Personnel must be trained in material and device management.
183
Material and Device Management
Code Standard Code Assessment Criteria
DH.MC.01.00
Efficient, effective and safe use of materials and devices must be ensured.
DH.MC.01.01
Those in charge of management of materials and devices must be determined.
DH.MC.01.02
Materials and devices must be determined and supplied in accordance with the needs of the institution.
DH.MC.01.03
Materials must be conserved in proper conditions.
DH.MC.01.04
Necessary physical conditions must be met to ensure that the devices work in proper working conditions.
DH.MC.01.05
Personnel must be trained in material and device management.
Rules must be set to ensure safe and effective use of materials and devices, the necessary protective material and information concerning the devices must be available.
Necessary maintenance, calibration, adjustments and tests of the devices needed must be conducted.
Traceability of medical devices must be provided.
DH.M
C.01
.06
DH.M
C.01
.07
DH.M
C.01
.08

Support Services
184
Department of Quality, Accreditation and Workers' Rights in Health
Goal
To ensure that materials and devices to be used are supplied in a timely manner and are used safely, with a view to guarding the needs of the patients and the personnel
Objectives
» Efficiency
» Productivity
» Suitability
» Timeliness
» Healthy Work Life
Standard Requirements
Management and Documentation» In order to provide an effective management of materials and devices,
all those in charge of planning, coordination and carrying out of all theprocesses must be determined; the tasks assigned to these peopleand their responsibilities must be identified.
»
• Tasks and responsibilities of staff working on material and devicemanagement
• Detection of material and device needs• Procurement of materials and devices• Storage of materials• Material orders
Methods and rules regarding the procurement, storage, tracking anduse of materials and devices must be clearly identified. Arrangementsmust be made to use of material and devices. Inventory ofall equipment should be maintained and regularly checked formaintenance and update changes. Documents regarding material anddevice management must be generated taking into consideration theneeds of the ODHC and the critical processes.Documents to be generated must comprise at least the following:

Support Services
185
Standards of Accreditation in Health - ODHS Kit
• Transfer and preparation of materials
• Safe use of materials and devices
• Indicators for management of materials and devices
• Methods of intervention for dangerous situations which might occur during use of materials and devices
• Materials and devices possessing special properties, requiring special storage conditions or require specific technique or expertise to use
• Maintenance, adjustment and calibration of devices
Procurement of Materials and Devices
» Necessary measures must be taken for the timely procurement of the right materials and devices in order to ensure efficient delivery of healthcare services at ODHC.
» Rules and methods regarding the procurement requests for materials and devices must be determined. Within the framework of this action, ODHC must determine who can request materials and devices, the method for the request, and by whom and how the requests would be assessed.
» Materials routinely used or compulsory to keep must be detected, their critical stock levels must be determined and tracked.
» Procurement requests, consumption analyses and the needs of the community must be taken into consideration while carrying out assessments to determine the types and quantity of materials and devices to be procured.
Storage and Transfer of Materials
» Unauthorized access to identified material storerooms and all the unit storages where medical consumption materials are preserved for over 24 hours must be restricted in line with patient safety and security.
» Materials must be preserved in suitable perseveration conditions in the storage areas in accordance with their properties. For this purpose, the necessary measures must be taken, and these measures must be monitored.

Support Services
186
Department of Quality, Accreditation and Workers' Rights in Health
» Storage layout plans must be developed to ensure easy access tomaterials by the personnel and to prevent time loss in emergencies;the plans must be kept up-to-date.
» Measures must be taken against breaking and spilling during transfer,and the necessary equipment for safe transfer must be provided. Thetransfer personnel must be trained in the safe transfer of materials,and regarding special-property or hazardous materials.
Safety of Devices» Protective equipment for the devices, information on safe usage
information and guides must be available at usage areas; the relevantpersonnel must be trained in safe use of the devices.
» Physical arrangements in the areas where the devices are presentmust be realized in accordance with the working conditions of thedevices.
» Calibrations, adjustments, tests and/or maintenance must berealized as frequently as stated in the technical documents of themanufacturers, in such a way as to meet the needs of the ODHC andin line with the usage intensity and within a plan, for the purposesof safe operation, obtaining correct results, keeping the harm whichmight occur at a minimum.
» It must be ensured that devices requiring special technique/equipment/expertise (autoclave, generators, etc) are used by trainedand authorized persons.
Traceability of Medical DevicesMedical devices should have inventory by department. Medical devices must have a device identification card. At least the following information should be on the device ID card:o Device nameo Serial numbero Brando Asset numbero LocationMaintenance, adjustment and calibration of medical devices should bemonitored according to a plan.

187
Outsourcing
Code Standard Code Assessment Criteria
DH.D
K.01
.00
The services provided through outsourcing must be in line with the core policies and values of ODHC and Standards of Accreditation in Health.
DH.D
K.01
.01
The services to be outsourced must be determined in line with the core policies and values of ODHC.
DH.D
K.01
.02
Scope and process of the outsourced services must be defined.
DH.D
K.01
.03
It must be ensured that outsourced services will comply with Health Accreditation Standards.
Goal
To ensure that the services provided through outsourcing are in line with the core policies and values of ODHC and that they are provided in line with the targets determined in the Standards of Accreditation in Health.
Objectives
» Patient-orientedness » Safety
» Continuity » Effectiveness
» Productivity » Efficiency

Support Services
188
Department of Quality, Accreditation and Workers' Rights in Health
Standard Requirements
Determining the Services to be Provided through Outsourcing» Based on core policies and values, the reasons for the need to
outsource and the targets aimed at the service to be provided must be determined.
» ODHC must conduct a needs analysis and make assessments on the services to be provided through outsourcing, and must determine its strategy.
Defining the Scope and Process of Outsourcing» The services which the external service provider will provide for
ODHC must be clearly defined and the completion process must be determined.
» Business processes must be clearly and precisely defined.
» The number and qualifications of the personnel, the equipment and devices required for the external service provider to carry out its activities must be determined.
Compliance with the Standards of Services Provided through Outsourcing» In accordance with the defined scope and business processes,
methods for constant check of the services provided through outsourcing and checking criteria along with performance indicators must be identified.

Emergency Management


191
Emergency Management
Standard 1
Code Standard Code Assessment Criteria
AD.A
D.01
.00
Measures must be taken against cases like natural disasters or events that necessitate emergency response, intervention, first aid or evacuation.
AD.A
D.01
.01 Necessary measures must be
determined by risk analysis for the events that require extraordinary response, striving, first aid or evacuation.
AD.A
D.01
.02
Planning must be done for preventive measures determined and possible emergencies.
AD.A
D.01
.03
Trainings must be provided on emergency management and drills must be conducted.
Goal
To define the requirements to prevent people or physical elements from being harmed or to minimize that harm in emergencies such as natural disasters like earthquakes and floods, or in emergencies which would require medical intervention such as fires or explosions at ODHCs.
Objectives
» Healthy Work Life » Patient Safety

Emergency M
anagement
192
Department of Quality, Accreditation and Workers' Rights in Health
Standard Requirements
Risk Analyses
ODHC must determine the specific situations for the preventive measures needed to be taken for incidents requiring extraordinary response and intervention, analyze which emergency situations may bring about what kind of dangers at the institution and must put forth what the necessary preventive measures must be.
Planning
» ODHC must plan for the implementation of the preventive measuresdetermined for the emergencies. The planning for the preventivemeasures must include at least the following:
• Deciding which preventive tasks must be performed
• Planning the necessary preventive investments and activities
• Budgeting investments and activities
Constant reviewing through drills and observations done to see whether the measures and implementations developed serve their purpose
» What to do in case an incident requiring extraordinary response takes place,despite necessary preventive measures taken against possible emergencies which might take place at ODHCs, must be pre-planned as well.
• An emergency management team must be formed at ODHC andits responsibilities must be defined.
• Investments which would make the management of emergencieseasier (emergency alert system, communication system, etc)must be identified and planned.
Trainings and Drills
The most important point about emergency management is the fact that one must be prepared to bring into action the measures planned.
» The necessary trainings must given to all staff for emergencysituations at the end of identifying risk analysis.
» Exercises should be carried out at the determined frequency tocreate awareness in personnel, to cover all relevant processes and tominimize the risks at the time of the incident.

Emergency M
anagement
193
Standards of Accreditation in Health - ODHS Kit
Standard 2
Code Standard Code Assessment Criteria
AD.A
D.02
.00
Measures must be taken for the natural disasters or events which require extraordinary response, striving, first aid or evacuation.
AD.A
D.02
.01 An emergency alert system defined
with Code Blue must be formed for timely intervention in cases of respiratory arrest and/or cardiac arrest.
AD.A
D.02
.02
Those in charge of management of the emergency alert system must be determined.
AD.A
D.02
.03
Intervention team/teams must be determined.
AD.A
D.02
.04
Medicines and equipment to be used in the procedures must be specified.
AD.A
D.02
.05
Records must be kept about interventions performed.
AD.A
D.02
.06
Code Blue trainings must be provided and drills must be conducted.
Goal
To define the requirements for the fastest and most effective intervention to take place in cases of respiratory or cardiac arrest at ODHC.
Objectives
» Healthy Work Life
» Patient Safety

Emergency M
anagement
194
Department of Quality, Accreditation and Workers' Rights in Health
Standard Requirements
Emergency Alert System (Code Blue)
» An emergency alert system must be put in place in order to respondin the shortest time possible to the patients, carers and all the ODHCpersonnel who need emergency medical intervention.
» The emergency alert system must be structured in such a way as tocover the whole of ODHC and to enable reaching the scene of incidentin the shortest time possible at any time of day (3 minutes at the latest),taking into consideration the size of the institution and whether theinstitution comprises multiple buildings. The call system to be set upfor the emergency alert system must be designed in such a way asto inform the personnel in a timely manner, ensure efficient and fastcommunication through short and clear messages, and prevent panic.
Supervisors
» Code Blue supervisors must be identified so as to ensure effectiveoperation in line with ODHC structure and type.
» The responsibilities of the Code Blue supervisors must include atleast the following: trainings for the personnel, identifying the CodeBlue intervention teams, organizing drills, tracking records, initiatingcorrective-preventive activities when necessary.
Intervention Teams
» There must be at least one physician and one other health professionaltrained in CPR (Cardio-Pulmonary Resuscitation) present in the CodeBlue intervention team. The intervention team is responsible for goingto the scene of the incident for which a Code Blue call has been alertedand for performing the intervention.
» There must be arrangement in place for the 24-hour active functioningof the Code Blue alert system.
Medicines and Equipment
» The medicines and equipment that would be needed must bedetermined beforehand and an emergency response kit must be

Emergency M
anagement
195
Standards of Accreditation in Health - ODHS Kit
prepared. The emergency response kit must have at least the following: laryngoscope set and additional batteries (for children and adults), balloon-valve-mask system, masks in different sizes, oxygen pipe and masks, intubation tube (in child and adults sizes), auxiliary airway tools (laryngeal mask, airway or kombi tube, etc), injectors, personal protection equipment.
» The medicines to be kept in the emergency response kit must be determined in accordance with the needs of the department and the patient portfolio. The emergency response kit must be in useable condition.
Record-keeping
» Records must be kept about the intervention performed following Code Blue call. The following information must be present at least in the records kept:
• When the call was made
• Information about the person who needed intervention
• Which interventions were performed
• Where the interventions were performed
• When and in how much time the team arrived at the scene of intervention
• Result of the intervention
• Who was present in the intervention team
» Analyses must be performed on the records kept and the results acquired from this practice must be periodically monitored.
Trainings and Drills
» Trainings to be provided for all the staff from managers to department staff, from cleaning personnel to security officers, regarding the importance of Code Blue and how it would be implemented must be planned.
» Drills regarding Code Blue must be conducted at least once a year. Records must be kept about the drill, the results of which must be assessed, and the necessary corrective measures must be taken.

Emergency M
anagement
196
Department of Quality, Accreditation and Workers' Rights in Health
Standard 3
Code Standard Code Assessment Criteria
AD.A
D.03
.00
Timely intervention must be ensured in cases where the health professional is exposed to a risk of violence, or an act of violence is directed towards him/her.
AD.A
D.03
.01 An emergency alert system defined
with Code White must be in place for intervention in cases where there is a risk or and actual act of violence towards health professionals.
AD.A
D.03
.02
Those in charge of the management of the emergency alert system must be determined.
AD.A
D.03
.03
Intervention team/teams must be determined.
AD.A
D.03
.04
Code White trainings must be provided and drills must be conducted.
Goal
To ensure intervention in the shortest time possible in the case of a risk/attempt of violence, or when an actual act of violence is directed towards health professionals working at ODHC.
Objectives
» Patient Safety
Standard Requirements
Emergency Alert System (Code White)» An emergency alert system must be established for cases of risk/act
of violence towards health professionals.

Emergency M
anagement
197
Standards of Accreditation in Health - ODHS Kit
» The emergency alert system must be structured in such a way as to cover the whole of ODHC and to enable intervention at any time of day, taking into consideration the size of the institution and whether the institution comprises multiple buildings. The call system to be set up for the emergency alert system must be designed in such a way as to inform the personnel in a timely manner, ensure efficient and fast communication through short and clear messages, and prevent panic.
Supervisors» Code White supervisors must be identified by ODHC so as to ensure
effective operation in line with ODHC structure and type.
» The responsibilities of the Code White supervisors must at least include the following: trainings for the personnel, organizing the drills, tracking records, initiating corrective-preventive activities when necessary.
Intervention Teams» How the relevant staff, led by security officers, will intervene, and unit
and institution- based measures will be implemented when there is a Code White alert must be determined. Security officers at ODHC are responsible to intervene in the incident taking place in their area of responsibility as determined in Code White system.
» There must be arrangement in place for the 24-hour active functioning of the Code White alert system.
Record-keeping» Records must be kept about the intervention performed after the Code
White call. The following information must be present at least in the records kept:
• When the call was made
• Information about the person who needed intervention and the person who committed the act of violence
• Reason for the act of violence
• How and where the intervention was performed
• When and in how much time the team arrived at the scene of intervention
• Result of the intervention

Emergency M
anagement
198
Department of Quality, Accreditation and Workers' Rights in Health
• Who were present in the intervention team
• Information about notification of legal authorities about the incident
» Analyses must be performed on the records kept and the results acquired from this practice must be periodically monitored.
Trainings and Drills» Trainings to be provided for all the staff from managers to department
staff, from cleaning personnel to security officers, regarding the importance of Code White and how it would be implemented must be planned.
» Drills regarding Code White must be conducted at least once a year. Records must be kept about the drill, the results of which must be assessed, and the necessary corrective measures must be taken.
Standard 4
Code Standard Code Assessment Criteria
AD.A
D.04
.00 There must be
an arrangement in place to ensure timely response to fire.
AD.A
D.04
.01
There must be a fire detection system.
AD.A
D.04
.02
Emergency alert system defined with Code Red must be established to respond in time in the case of fire.
AD.A
D.04
.03
Those in charge of management of the emergency alert system must be determined.
AD.A
D.04
.04 The equipment to be used while
responding to fire, rules regarding safe use of this equipment, signs and instructions to be taken into account in the case of fire must be identified.
AD.A
D.04
.05
Trainings must be provided on Code Red and drills must be conducted.

Emergency M
anagement
199
Standards of Accreditation in Health - ODHS Kit
Goal
To minimize and/or prevent any danger or harm by responding quickly to fire, in the case of danger of fire at ODHC.
Objectives
» Patient Safety
Standard Requirements
Fire Detection System» There must be a fire detection system at ODHC covering all the
areas, not being affected by power blackouts and which can perform addressing. The system must be connected to the uninterruptible power supply so as not to be affected by the power interruption.
Emergency Alert System (Code Red)» An emergency warning system must be set at ODHC to respond to fire
in a timely manner. The emergency warning system to be set must be audiovisual, taking into consideration the size of the institution and whether the institution comprises multiple buildings. While setting the emergency warning system, coordination must be ensured with such bodies as the fire department etc.
» The emergency warning system to be defined with Code Red must be set in such a way as to inform the institution’s staff, ensure efficient and fast communication in the case of risk, enable the communication of short and clear messages, save time for correct intervention, and prevent panic.
Supervisors» Code Red supervisors must be identified by ODHC so as to ensure
effective operation in line with ODHC structure and type.

Emergency M
anagement
200
Department of Quality, Accreditation and Workers' Rights in Health
» The responsibilities of the Code Red supervisors must include at least the following: trainings for the personnel, organizing the drills, tracking records, initiating corrective-preventive activities when necessary. Supervisors must also follow the legislation on fire prevention and extinguishment, and monitor the implementation of the necessary arrangements.
Response to Fire» How the relevant staff will respond, how the unit- and institution-
based measures will be implemented, and who will be present in the fire response team or who would notify the fire department in the case of incidents where response is not possible when a code red alert is given, must be determined.
» Tools and equipment such as fire hydrants, fire extinguishers and fire hoses must be identified, and rules regarding their use must be defined. Also, the usability and operability of the equipment must be periodically checked.
Trainings and Drills» Trainings to be provided for all the staff from managers to department
staff, from cleaning personnel to security officers, regarding the importance of Code Red and how it would be implemented must be planned.
» Drills regarding Code Red must be conducted at least once a year. Records must be kept about the drill, the results of which must be assessed, and the necessary corrective measures must be taken.

DEFINITIONSAND
ABBREVIATIONS


Definitions
203
Standards of Accreditation in Health - ODHS Kit
Acceptance or Rejection Criteria: In prosthesis laboratory, rules of conduct regarding arrived measure convenience to determined criteria by laboratory management in accordance with scientific requirements.
Accommodation Service: In the health facility, except of the scope of medical services, they are services offering the accommodation, cleaning, washing, eating and drinking the patient, the patient’s relatives and staff and ensuring to give these services in a safety environment which provides life and property safety.
Adverse Event: Events that may or does affect the safety of patient, relatives, employees or the other people negatively in health facilities.
Adverse events related to patient safety may occur in the terms of drug safety, surgical safety, transfusion safety, facility safety, falls, radiation safety and information security.
Adverse events related to employee safety may occur in the terms of stab wounds, facility safety, radiation safety, occupational infections, contact with blood and body fluids.
Antisepsis: Killing of microorganisms in or on living tissue or inhibition of reproduction of these microorganisms is called antisepsis.
Asepsis: The measures taken to avoid the migration of germ to clean surface, medium or material is called asepsis.
Basic Policy: Determining the health facility’s mission and vision with corporate goals and objectives.
Calibration: A number of processes correlating between the values which a measuring device or measuring system show and known values of measured ones under certain circumstances.
Chemical Waste: Gas, solid or liquid waste of chemicals used in medical fields such as treatment or diagnosis and which may be harmful to the health of humans and the environment with various effects.
Code of Document: Providing traceability of the document, the document management system directory refers to the identification system established in accordance with the rules set by institutions and organizations.
Consent Document: Applied for medical Treatment, process will be transferred to the patient by health care providers with information and documents are created to get the consent of the patient.

Definitions
204
Department of Quality, Accreditation and Workers' Rights in Health
Container: Temporary storage unit with 0,8 m3 volume at least, wheel, cap, caps lock, made of stainless metal, plastic or material and so on.
Contamination: Being infected with foreign matter. Transition of bacteria and virus from contaminated surface to another.
Contraindication: Situation that prevents a treatment administration or discovery of patient status/complication that prevents treatment or intervention
Corporate Communications: In the process of production and management; institution that make up the information flow between departments and elements, motivation, integration, education, decisionmaking and control functions such as implemented in the framework of
certain rules in order to ensure, and the process carried out taking into consideration the reputation of the institution while interacting with the external communication.
Date of Publish: the documents was refered to date of publish.
Decontamination: As well as, as a word includes all applications for removal of micro-organisms or organic soils (cleaning, disinfection, sterilization), it is used in the meaning of removal of organic substances and pathogens from a surface or material by pre-cleaning process
comprising physical and / or chemical methods and making the surface or material useable without using any personal protective before sterilization or disinfection in practice.
Disinfection: The process of destruction or stopping reproduction of the majority or all of the pathogenic microorganisms (except bacterial spores) on inanimate surfaces. Disinfection process is considered in 3 three groups high, medium and low disinfection according to the affect levels of bacterial spores and mycobacteria.
Document: Environments containing the information.
External Document: Document not prepared by the institution itself, but benefited from the realization of the activities.
Facility Management: For health facility in order to achieve its purpose, it is coordination of all activities related to planning, application and management of necessary working environment physical and functional

Definitions
205
Standards of Accreditation in Health - ODHS Kit
arrangements which provides the best way to meet the growing health care needs.
Form: Document prepared for filling write the desired data or information.
Functional Structure: Functional structure is classification of activities according to resemblance of used information, skill and resources. As a result of this classification, departments are formed. In this context, functional structure can be considered as classification according to institutional resources. Health institutions adopting this structure generally have the departments of diagnosis, treatment, management and support.
Goal: Refers to the general results that the organisation wants to reach in the long term.
Guide: The document was created for informational purposes and guiding
activities.
Hand Hygiene: It is a general term referring to any action of hand cleansing.
Handover: In order to ensure the patient safety and continuity of care, it is a transfer of patient’s special information from a caregiver to another or from a system featured in an organized team to another with a modern interaction process transferred in a interactive way.
Hazardous Waste: Genotoxic, pharmaceutical and chemical wastes arising from units and wastes containing heavy metals and pressured containers.
Healthcare Associated Infection: These infections are the ones which develop after the patient is admitted to the health facility and which are not on incubation period on admission. Service associated infections after discharge and occupational infections are included in the matter.
High Risk Medicine: These are the medicines that are therapeutics and maximum dosages are close to each other. When used in a wrong way, these can affect the patient negatively irremeable or permanently.
High-Level Disinfection: Some of the chemicals may kill all spores by long term (3-12 hours) treatment In similar concentrations but in a shorter treatment period (e.g. 20 minutes with glutaraldehyde) the same disinfectant kills all microorganisms except bacterial spores. This process is called high-level disinfection.

Definitions
206
Department of Quality, Accreditation and Workers' Rights in Health
Household Waste: Non-contaminated wastes, which is mainly originated from kitchen, garden, and administrative units
IMS: Information Management System. Trained users and devices connected to the computer through a network of institutions, every effort is made to perform (clinic, prosthesis laboratory, radiology etc.), with electronic software to maintain the record.
Indication: It is a term, which refers that situations, in which should be done an application, a treatment or a process.
Indicator: When a topic becomes digitized and measured, this is a tool that contributes to making improvement activities.
Infectious Waste: All kinds of body fluids and human tissues, organs and other pathological material; blankets, sheets, bandages, adhesive tape, tampons, swab and other wastes; bacteria and virus retaining air filters which known as infectious agents carriers or likely to carry them.
Information Security: It means to protect the information from damages and to prevent obtaining the information by unwanted users in any environment using the appropriate technology in the right way for the right purpose.
Inpatient: They are patients whose diagnosis and treatment is conducted during ODHC stay. Daily ODHC stays are also included in this term.
Institutional Structure (Design): Institutional structure includes authorities and responsibilities in institution and forming communication channels. Organizational structure of the health institution is formed after these studies. This structure is shown in the organization scheme. In the organization schemes, positions in the institution, units, departments and authority, responsibility and communication relations between them are shown.
Instruction: A single document containing the steps of the activity.
Intended Population: Employees of the company, people who get the service and all the people that interact with the organization and institutions (media, insurance agencies, suppliers, government agencies, non-governmental organizations, universities, local government units, community leaders, experts, etc.)
Definitions
207
Standards of Accreditation in Health - ODHS Kit
Isolation Precautions: Activities carried out and measures toprevent transmission of apathogen microorganism from person to person, from person to envoirment or vice versa.
List: Similar items listed consecutively document.
Low Level Disinfection: In this process, in a short time (less than 10 minutes) most of the vegetative bacteria, some fungi and some viruses dies.
Matrix Structure: Matrix structure is the use of both functional and sectional structure at the same time in the health institution. For example,services provided in operation room require coordination of people and units that have different functions and from different departments.
Measure Time: It means the date and exact hour of measurement by the dentist.
Measurement (for dentistry field): Creating a copy of mouth part where prosthesis will be placed. A negative of teeth and/or support tissue is captured with the use of soft, half-fluid measurement materials for this purpose.
Medical Gas: Gas that is produced and packed to be used in anesthetic processes or diagnosis and treatment interventions.
Medical Intervention: In the purposes of disease diagnosis/treatment and protecting health, physical and psycological interventions within medicine limits in accordance with occupational responsibilities and standards by people who have authority to practice medicine.
Medical Waste: Infectious, pathologic and penetrating wastes which results from units.
Mission: It is the pure and general object, which determines the reason of health facility’s being, its philosophy with provided products and services that lays down their unique differences and separate them from other health institutions.
Morbidity: incidence of disease
Narcotic Medicine: These are medicines that are like morphine and has painkiller specifications, natural, semi artificial and artificial and these may cause strong physical and psychological addiction.

Definitions
208
Department of Quality, Accreditation and Workers' Rights in Health
Objective: States short term processes for reaching the goals. Objectives are more open and has measurable features comparing to goals.
ODHC: Consists of following institutions of Turkey who provide service actively in oral and dental health field:
• Oral and Dental Health Centers,
• Oral and Dental Health Hospitals,
• Faculties of Dentistry
Organization Scheme: It is a graphic that shows institutional structure as a whole and it also shows various relations between service units in a comprehensive order.
Outpatient: They are the patients without ODHC stay procedures but with necessary diagnostic and therapeutic procedures.
Outsourcing: It’s the method of providing some services which take part in the ODHC but not offered from an institution or organization out of the facility.
Particle: Smallest part of matter or energy
Pathogen Microorganism: Microorganisms that cause infectious diseases
Pathological Waste: Tissues, organs and body parts as a result of surgical intervention
Patient Care: Patient care encompasses the whole health service processes starting from admission of the patient to ODHC to monitoring of the patient after discharge. It also includes service processes of all other relevant occupational groups beside diagnosis/treatment processes provided in policlinics for outpatients and in clinics for inpatients.
Perioperative Period: The period during surgical operation
Personal Hygiene Area: In accordance with the hygiene rules, these are the areas like toilets, baths or sinks, which provides body cleaning and meets hygiene needs.
Plan: the intended purpose ensure achievemant of steps, what, when, why and document that shows how to do it.
Postoperative Period: The period after surgical operation

Definitions
209
Standards of Accreditation in Health - ODHS Kit
Preoperative Period: The period before surgical operation
Primary Facility Resources: It expresses the need of minimum formation of the infrastructure of technologies which will be used in the provision of health care (water, electricity, air conditioning and medical gas systems, etc.).
Privacy: Represents the living area of the patient that has to be clarified for the patients care, treatment (test results, information about the disease and treatment) or for any other reason but hiding them from all other individuals in the society.
Procedure: Document describing how the execution of the activities of a process.
Promotion and Enhancement of Health: is the course in which people increase the control on their health and are able to enhance it. Promotion and enhancement of health represents a social and political progress. It does not only mean the activities that increases the skill and capacity
of individuals but also changing social, environmental and economic conditions, thus it also means the activities aimed at easing their impacts on the health of society and individuals. Promotion and enhancement of health is the course of increasing the control on health determiners (such as biological, environmental, economical, social and life style elements) and thus it is the progress of enhancing their own health.
Prosthesis: In-mouth prostheses consists of all artificial devices which are used to recover worn, damaged teeth, replace unstructured/lost teeth, and get rid of aesthetic defects. These prostheses are artificial matters that correct lost aesthetic and functional needs primarily chewing.
Prosthesis Laboratory Services: All processes that ensures prosthetic material acceptance in convenient conditions, preparation before process, implementation of process and delivery of prosthesis to patient
Prosthetic Material: No matter what kind it is, defines the material used for any prosthesis in all steps such as measurement, material, mid-product and prosthesis
Prosthesis Safety: In processes between measurement and arrival of prosthesis to dentist or patient, evaluation and prevention of all kind of risks that can damage safety and validity of the process

Definitions
210
Department of Quality, Accreditation and Workers' Rights in Health
Psychotrope Medicine: these are the medicines that affect central nervous system and cause some temporal changes in sense, mood, consciousness and behaviors by changing the functions of the brain. And also these may cause physical addiction when used for a long time.
Radioactive Waste: Waste including radioactive material such as fluids left from radiation therapy or laboratory research; contaminated glassware, packaging or paper
Rational Use of Antibiotics: Acting according to the following 5 TRUE bases for the treatment or prophylaxis of an infectious disease.
• Right person
• Right time
• Right way (swallowing, chewing, vascular, etc.)
• Correct amount
• Correct drug
Revision Date: The document was last updated refers to the date.
Revision Number: The document is updated refers to the number of times.
Risk analysis: It refers to identification of risks using methods allowing a comprehensive understanding of the risks, assessment of the severity of the damage in case of risks that may arise. In this context, risk analysis includes following processes; Identification of dangers which patients may be exposed to Determination of the frequency and level of exposure to hazards Assessment of which patient or patient groups are affected.
Risk: It refers to the probability of occurrence and the severity of an event that can damage human health as a result of exposure to a hazard.
Sectional Structure: In this structure type, outcomes are based on and departments (sections) are classified according to these outcomes. Departments in health institutions are formed with respect to certain medical specialties (such as anesthesia, radiology etc.). In this structure, there are functional directors working under department directors. Functional directors are responsible not only to department director but also to higher functional directors of the health facility.
Sharp Waste: Wastes such as injection, injection syringe and all other subcutaneous venture injections, cylinders, cartridges and cans enclosing all the gases used in procedure, lancets, scalpel, knife, serum kit needles, surgical suture needles, biopsy needles, intracath, broken glass, bulbs,

Definitions
211
Standards of Accreditation in Health - ODHS Kit
solid-lamellae, broken glass tubes and petri dishes and these waste may cause stinging, punching, scrape and injuries.
Side Effect: All pharmacological effects, that are unintended, without taking the harm of the medicine into consideration.
Staff/Employee/Personnel: “Staff, employee and personnel” terms in this standard set means all permanent, temporary, volunteer, daily or independent people involved in service provision.
Sterilization: Killing all microorganisms found on anybody or substance by physical or chemical methods including spores.
Supporting Document: Procedure, Direction, Guide, Form, Plan, List, Consent Document, and External Document or this document is supportive documents.
Surgical Prophylaxis: Medical interventions aimed at preventing surgical infections.
Temporary Storage: The process of keeping waste wait in units built in the unit or containers for a temporary period not to exceed 48 hours before the transportation
Transportation: The process of transporting waste by convenient transportation vehicles from temporary storage units to disposal area.
Ultimate Disposal: Destruction or disarmament through incinerating or storing the waste in plants where all measures provided in applicable legislation are taken without any damage to the environment and human health
Value: Defined rules and principle series which directs their members to certain acts for securing the survival of institution.
Verbal Request: verbal request is defined as the doctor’s conveyance of the request to the nurse in a verbal way in the obligatory cases which the physician can not give a written request.
Vision: Expression of health facility’s hope to reach the status under current conditions and its main philosophy for the future with sentences that features excellence and being ambitious
Waste Management Plan: Determining the general principles for not harming the environment and human health when the process of composing waste till disposal of them.

REFERENCES


References
215
Standards of Accreditation in Health - ODHS Kit
• Accreditation Canada Standards, Qmentum International, 2010-2011.• Ağız ve Diş Sağlığı Hizmeti Sunulan Özel Sağlık Kuruluşları Hakkında
Yönetmelik, T.C. Resmi Gazete, Sayı 23846, 14 Ekim1999• Akçabay, M., "Preoperatif Değerlendirme ve Premedikasyon", med.gazi.
edu. tr/posts/download?id=20728, Erişim tarihi: 10.03.2014.• Alp Meşe, E., "Ameliyathane Organizasyonu", http://hastaneler.erciyes.
edu.tr/pdf/Ameliyathanelerde0/o20Enfeksiyon0/o20Kontrol0/oC30/oBC.pdf, Erişim tarihi: 10.03.2014.
• Amsterdam Avrupa Hasta Haklarının Geliştirilmesi Bildirgesi, 28-30 Mart 1994.
• Arslanoğlu, A., "Yönetimde Dış Kaynaklardan Yararlanma Yaklaşımı ve Sağlık Sektöründe Bir Araştırma", İstanbul Marmara Üniversitesi SBE Uluslararası Kalite Yönetimi Bilim Dalı Yayınlanmamış Yüksek Lisans Tezi, 2009.
• Aştı T. Bakım Teknolojisinde Yenilikler, II. Uluslararası IX. Ulusal Hemşirelik Kongresi Kongre Kitabı, 2003
• Atık Yönetimi Genel Esaslarına İlişkin Yönetmelik, T.C. Resmi Gazete, Sayı 26927, 05/07/2008
• Atıkların Düzenli Depolanmasına Dair Yönetmelik, T.C. Resmi Gazete, Sayı 27533, 26/03/2010
• Australian Commission, On Safety and Quality in Health Care, Hospital Accreditation Workbook, Commonwealth of Australia, 2012.
• Australian Commission, On Safety and Quality in Health Care, National Safety and Quality Health Service Standards, 2012.
• Australian Commission, On Safety and Quality in Health Care, Preventing Falls and Harm From Falls in Older People Best Practice Guidelines for Australian Hospitals, Commonwealth of Australia 2009.
• Baskan, S. "Cerrahi Alan Enfeksiyonlarının Önlenmesi: Ameliyathane Koşulları Nasıl Olmalı?", http://www.hastaneinfeksiyonlaridergisi.org/ managete/fu_folder/2003-04/html/2003-7-4-161-167.htm, Erişim tarihi: 10.03.2014.
• Beşeri Tıbbi Ürünlerin Güvenliğinin İzlenmesi ve Değerlendirilmesi Hakkında Yönetmelik T.C.Resmi Gazete Sayı 25763 Tarih:22 Mart 2005
• Binaların Yangından Korunması Hakkında Yönetmelik,T.C. Resmi Gazete, Sayı 24822, 26 Temmuz 2002
• Bird DL, Robinson DS. Modern Dental Assisting. 10th edition, Missouri: Elsevier Saunders Inc.; 2012.
• CDC, "Guideline for Isolation Precautions: Preventing Transmission of Infectious Agents in Healthcare Settings", 2007.

References
216
Department of Quality, Accreditation and Workers' Rights in Health
• CDC, Guideline for Disinfection and Sterilization in Healthcare Facilities, 2008
• CDC, HICPAC, Guidelines for Environmental Infection Control in Health-Care Facilities, Recommendations of CDC and the Healthcare Infection Control Practices Advisory Committee (HICPAC), 2003.
• Çakmakçı, M., "Hastane Enfeksiyonları ve Hastane Tasarımı: Ameliyathanelerin Planlanması", http://www.hastaneinfeksiyonlaridergisi.org/managete/fu_ folder/2001-03/html/2001-5-3-172-177.htm, Erişim tarihi: 10.03.2014.
• Çalıkkocaoğlu S. Tam Protezler Cilt 1. 3. Baskı. İstanbul: Protez Akademisi ve Gnatoloji Derneği 2. Bilimsel Yayını; 1998.
• Çalışanların İş Sağlığı ve Güvenliği Eğitimlerinin Usul ve Esasları Hakkında Yönetmelik, Resmî Gazete, Sayı: 28648, 15 Mayıs 2013.
• Demir, H., Okan, T., "Teknoloji, Örgüt Yapısı ve Performans Arasındaki İlişkiler Üzerine Bir Araştırma", İstanbul, Doğuş Üniversitesi Dergisi, sayı 10 (1), s.57-72, 2009.
• Devlet Arşiv Hizmetleri Hakkında Yönetmelik T.C. Resmi Gazete Sayı 19816 Tarih 16.5.1988
• Devlet Memurları Kanunu, Kanun No:657, Sayı : 12056, 23 Temmuz 1965
• Diş Hekimliği Hizmetlerinin Yeniden Yapılandırılması Makam Onayı, T.C. Sağlık Bakanlığı, Sayı 39939, 06 Ekim 2010
• Diş Protez Laboratuvarları Yönetmeliği Resmi Gazete, Sayı 26016, 07 Aralık 2005
• DUSDATA DUS Hazırlık Merkezleri. Protetik diş tedavisi. 2. Baskı. İstanbul: Klas Ofset ve Tasarım San. Tic. Ltd. Şti.; 2012.
• Eren, E., Stratejik Yönetim ve İşletme Politikası, İstanbul, Beta Basım Yayım Dağıtım A.Ş., 2000.
• Erkoç, Y ve diğerleri, Toplum Sağlığı Merkezi Çalışanlarına Yönelik "Sağlığın Geliştirilmesi Eğitimi" Rehberi, Sağlık Bakanlığı, Ankara, 2011.
• Ertem,G., Standartlara Dayalı Verilen Hemşirelik Bakımının Bakım Kalitesine ve Hasta Memnuniyetine Etkisi, İzmir Kadın Sağlığı ve Hastalıkları ABD Yayımlanmamış Doktora Tezi, 2003.
• Gıda Hijyeni Yönetmeliği, T. C. Resmi Gazete, Sayı 281457, 17 Aralık 2011.
• Glenn M. Rampton, Ian J. Turnbull, J. Allen Doran "Human Resource Management Systems: A Practical Approach", 2nd edition. Ontorio, Carswell Thomson Professional Publishing, s.25, 1999.

References
217
Standards of Accreditation in Health - ODHS Kit
• Groene O., Barbero, M.G., Hastanelerde Sağlığın Geliştirilmesi, Kanıt ve Kalite Yönetimi, çev. Zaralı, F. ve diğerleri, Dünya Sağlık Örgütü (Sağlık Bakanlığı çevirisi), Ankara, Mayıs 2005.
• Güler, H. ve diğerleri, SKS Doküman Yönetim Sistemi, Ankara, Sağlık Bakanlığı, Pozitif Matbaa, 2013.
• Güler, H. ve diğerleri, SKS ve İlaç Güvenliği, Ankara, T.C. Sağlık Bakanlığı, Pozitif Matbaa, 2012.
• Güler, H., Öztürk, A., ADSM Hizmet Kalite Standartları, Ankara, Sağlık Bakanlığı, Pozitif Matbaa, 2011.
• Güllülü U, Özer S, Candan B "Muayenehanelerden Alınan Sağlık Hizmeti Kalitesinin Ölçülmesi Üzerine Bir Saha Çalışması" 5.Ulusal Pazarlama Kongresi: Değişen Tüketici Karşısında Pazarlamada Yeni Yaklaşımlar, Antalya: Akdeniz Üniversitesi, Turizm Araştırma, Geliştirme ve Uygulama Merkezi: 91-109, 2000.
• Hasta Güvenliği: Türkiye ve Dünya, ,Ankara Türk Tabipleri Birliği Yayınları, Ekim 2011.
• Hasta Hakları Yönetmeliği, Resmi Gazete, Tarih: 01.08.1998; Sayı: 23420
• Hasta Hakları Yönetmeliğinde Değişiklik Yapılmasına Dair Yönetmelik, T.C. Resmi Gazete, Sayı 28994 Tarih:8 Mayıs 2014
• Hasta ve Çalışan Güvenliğinin Sağlanmasına Dair Yönetmelik, T.C. Resmi Gazete, Sayı : 27897, 6 Nisan 2011
• Hayran ve diğerleri. “Türkiye Ağız ve Diş Sağlığı Hizmetlerinden Yararlanım Araştırması” Türk Diş Hekimleri Birliği Araştırma Dizisi-4, Ankara, Temmuz 2000
• Hayran ve diğerleri. “Diş Hekimliği Hizmetlerinde Hasta Memnuniyeti Araştırması” Türk Diş Hekimleri Birliği Araştırma Dizisi-6, Ankara, Haziran 2008
• http.www.taek.gov.tr, Erişim tarihi: 10.05.2014.• http://www.ahrq.gov/• http://www.qualitynet.org/dcs/ContentServer?c = Page&pagename=QnetPu
blic%2FPage%2FQnetHomepage&cid=1120143435363• http://www.tard.org.tr/tr-tr/, Erişim tarihi: 16.03.2014.• Inozu, B., Chauncey, D. ve diğerleri, "Performance Improvement for
Healthcare-Leading Change with Lean, Six Sigma and Constraints Management", Novaces,LLC, ISBN 978-0-07-176162-8, 2012.
• Institute of Medicine, To err is human: building a safer health system. Washington, DC: National Academy Press, 1999.
• ISO 31000, "Risk management -- Principles and guidelines", 2009.• ISO 9001, "Quality management systems - Requirements", 2008.

References
218
Department of Quality, Accreditation and Workers' Rights in Health
• İlaçların Güvenliği Hakkında Yönetmelik T.C.Resmi Gazete Sayı 28973, Tarih 15 Nisan 2014
• İş Güvenliği Uzmanlarının Görev, Yetki, Sorumluluk ve Eğitimleri Hakkında Yönetmelik, Resmî Gazete, Sayı:28512, 29.12.2012.
• İş Sağlığı ve Güvenliği Hizmetleri Yönetmeliği, Resmî Gazete, Sayı:28545, 29.12.2012.
• İş Sağlığı ve Güvenliği Kurulları Hakkında Yönetmelik, Resmî Gazete, Sayı: 28532, 18.01.2013.
• İş Sağlığı ve Güvenliği ve Çalışma Ortamına İlişkin 155 Sayılı Sözleşme, International Labour Organization, internet erişimi: http://www.ilo.org/ public/turkish/region/eurpro/ankara/about/soz155.htm
• İş Sağlığı ve Güvenliğine İlişkin İşyeri Tehlike Sınıfları Tebliğinde Değişiklik Yapılmasına Dair Tebliğ, Resmî Gazete, Sayı: 28602, 29.03.2013.Hayran ve diğerleri. “Diş Hekimliği Hizmetlerinde Hasta Memnuniyeti Araştırması” Türk Diş Hekimleri Birliği Araştırma Dizisi-6, Ankara, Haziran 2008
• İş Sağlığı ve Güvenliği Kanunu, T.C. Resmi Gazete, Kanun No: Kanun No. 6331 Sayı 28339, 20 Haziran 2012
• İzolasyon Önlemleri Kılavuzu, Türk Hastane İnfeksiyonları ve Kontrolü Derneği Hastane İnfeksiyonları Dergisi, Cilt 10, Ek 2, 2006.
• Japan Council for Quality Health Care, http://jcqhc.or.jp/pdf/top/english.pdf, ulaşma tarihi: Şubat 2013.
• Joint Commission International Accreditation Hospital, Survey Process Guide, 4th Edition (for Academic Medical Centers), 2013.
• Joint Commission International Accreditation Standards for Hospitals, 4th Edition, 2011.
• Kaya, A., "Türkiye'deki Kamu Hastanelerinde Halkla İlişkiler ve Tanıtım Eksikliği Sorunu", İstanbul Beykent Üniversitesi Hastane ve Sağlık Kurumları Yönetimi Bilim Dalı Yayınlanmamış Yüksek Lisans Tezi, 2010.
• Keskin H, Özdemir T. Çene – yüz protezleri. İstanbul: İstanbul Üniversitesi Yayınlar; 1995.
• Kılıçarslan MA. Dört Elli Diş Hekimliğinde Yardımcı Personel ve Klinik Yöntemi. Ankara: Palme Yayıncılık ; 2013.
• Kılıçarslan MA. Sabit protez X. sınıf ders kitabı. Ankara: Şule Ofset Matbaacılık; 2005.
• Kılıçarslan MA. Sabit protez XI. sınıf ders kitabı. Ankara: Şule Ofset Matbaacılık; 2005.
• Küçükler, N.D. ,Çelebi, G. "Hastane Enfeksiyonları Kontrolünde Çamaşırhane" Sivas, Hastane Enfeksiyonları Eğitim Programı Sözel sunumu, 2009.

References
219
Standards of Accreditation in Health - ODHS Kit
• Külekçi, G. “Diş Hekimliği İnfeksiyon Kontrol Rehberi” Türk Diş Hekimleri Birliği, İstanbul Diş Hekimleri Odası, İstanbul, 2007
• Lizbon Hasta Hakları Bildirgesi, 1981.• Meral, Y, "Sağlık Kuruluşlarında Dış Kaynaklardan Yararlanmanın Hasta
Memnuniyetine Olan Etkisi ve Bu Konuya İlişkin Bir Araştırma", İstanbul Üniversitesi Sosyal Bilimler Enstitüsü Yayınlanmamış Yüksek Lisans Tezi, 2006.
• National Healthcare Disparities Report; 3. Bölüm, "Access to Healthcare". Agency For Healthcare Research And Quality, Washington Yayın no: 09-0002, 2008, Erişim tarihi: 28.03.2014 http://www.ahrq.gov/qual/ nhdr08/Chap3.htm
• National Institute of Standards and Technology, Department of Commerce Baldrige Performance Excellence Program, 2011-2012 Health Care Criteria for Performance Excellence, 2011.
• NIOSH Publication No. 88-119: "Guidelines for Protecting the Safety and Health of Health Care Workers", 1988.
• OECD Health Care Quality Indicators Project: Patient Safety Indicators Report 2009, Health Working Papers No. 47, 2009.
• OECD, Health at a Glance 2011, OECD Indicators, 2011.• Ovayolu, N., Bahar, A. "Hemşirelikte Kalite" Atatürk Üniv. Hemşirelik
Yüksekokulu Dergisi, Cilt: 9 Sayı: 1, 2006.• Öncü, S., "Cerrahide antibiyotik, profilaksisi", Ulusal Cerrahi Dergisi, Cilt
27, Sayı 3, Sayfa 176-181, http://www.ulusalcerrahidergisi.org/text. php3?id=947, Erişim tarihi: 10.07.2013.
• Özlü T. Kuramsal Metinler, "Felsefi Arka Plan ve Örnek Olgularla Hasta Hakları: Hakkınız var, çünkü hastasınız." TİMAŞ Yayınları, İstanbul, Şubat 2005.
• Phillips RL, Dovey SM, Hickner JS, Graham D, Johnson M. The AAFP patient safety reporting system; development and legal issues pertinent to medical error tracking and analysis. In: Advances in patient safety: from research to implementation. Vol. 3.
• Pugh, D. S., ed. "Organization Theory: Selected Readings, Harmondsworth: Penguin.", 1990.
• Radyasyon Güvenliği Komiteleri Çalışma Usul ve Esasları, http://www. taek.gov.tr/belgeler-formlar/rsgd-formlari/usul-esaslar/, Erişim tarihi: 10.05.2014.
• Radyasyon Güvenliği Yönetmeliği, T.C. Resmi Gazete Sayı 23999, 05 Temmuz 2000.
• European Commission, Radiation Protection N° 172, Cone Beam Ct For Dental And Maxillofacial Radiology, Evidence-Based Guidelines, 2012

References
220
Department of Quality, Accreditation and Workers' Rights in Health
• Raju PS, Lonial SC, "The Impact of Service Quality and Marketing on Financial Performance in the Hospital Industry: An Empirical Examination. Journal of Retailing and Consumer Services", 9 (6): 335-348, 2002.
• Restuccia, D.J., Amerika Birleşik Devletlerinde Sağlık Hizmetlerinin Kalitesi: Uygulama ve Gelecek, Çev. Sıdıka KAYA, 2003.
• Rockville, MD: Agency for Healthcare Research and Quality, 2005:121-34. internet erişimi: http://www.ncbi. nlm.nih.gov/bookshelf/br.fcgi?booksaps3&partsA4255. Erişim tarihi: 17.03. 2014.
• Rootman, I. ve diğerleri, "Evaluation in health-Promotion Principles and Perspectives, WHO Regional Publications, European Series, 2001.
• Rosenstiel SF, Land MF, Fujimoto J. Contemporary fixed prosthodontics. China: Mosby Elsevier; 2006.
• Sağlık Bakanlığı ve Bağlı Kuruluşları Atama ve Yer Değiştirme Yönetmeliği T.C. Resmi Gazete Sayı 28599, 26 Mart 2013
• Sağlık Hizmeti Kalitesinin Geliştirilmesi ve Değerlendirilmesine Dair Yönetmelik, T.C. Sağlık Bakanlığı, Sayı 28730, 06 Ağustos 2013
• Sağlık Hizmetleri Genel Müdürlüğü, Sağlıkta Kalite ve Akreditasyon Daire Başkanlığı, Güvenli Cerrahi Kontrol Listesi Uygulama Rehberi, Ankara, Sağlık Bakanlığı, Pozitif Matbaa, 2011.
• Sağlık Hizmetlerinde İyonlaştırıcı Radyasyon Kaynakları ile Çalışan Personelin Radyasyon Doz Limitleri ve Çalışma Esasları Hakkında Yönetmelik, T.C. Resmi gazete, Sayı 28344, 05 Temmuz 2012.
• Sağlıkta Performans ve Kalite Yönergesi, T.C: Sağlık Bakanlığı, Sayı: 2011, 02 Temmuz 2008
• Samastı, M., "Hastanelerde Dezenfeksiyon Kullanım Esasları, Yapılan Hatalar", İ.Ü. Cerrahpaşa Tıp Fakültesi Sürekli Tıp Eğitimi Etkinlikleri Hastane Enfeksiyonları Korunma ve Kontrol Sempozyum Dizisi, 60, s. 143-168, 2008.
• Starfield B, Shi L., "The medical home, access to care, and insurance. Pediatrics.", 113(5 suppl):1493-8., 2004.
• Sterilizasyon Dezenfeksiyon Rehberi, DAS Derneği, 2011.• Sur, H., Gaziantep Zirve Üniversitesi Sağlık Kurumları İşletmeciliği
Uzaktan Eğitim Yüksek Lisans Programı Ders Notları, 2012.• Sur, H., Gaziantep Zirve Üniversitesi Sağlık Kurumları İşletmeciliği
Uzaktan Eğitim Yüksek Lisans Programı Ders Notları, 2012.• Süngü, A., "Ameliyathane Havalandırma Sistemleri IVF ve Genetik
Laboratuvar Havalandırma", http://www.das.org.tr/kitaplar/kitap2007/yazi/ali.sungu- das-2007-yazi.pdf, Erişim tarihi: 10.03.2014.

References
221
Standards of Accreditation in Health - ODHS Kit
• Şencan, İ., Demir, M., SKS Işığında Sağlıkta Kalite 1-2-3 cilt Ankara, Sağlık Bakanlığı, Pozitif Matbaa, 2013.
• T.C. Sağlık Bakanlığı “İlaç ve Tıbbi Sarf Malzemesi Alımları Genelgesi” Sayı: 010-06-7816 Tarih 25 Şubat 2010
• T.C. Sağlık Bakanlığı Çalışan Güvenliğinin Sağlanması Genelgesi, Sayı: 951.99/6665, Tarih:14.05.2012
• T.C. Sağlık Bakanlığı, Akılcı İlaç Kullanımı İnternet Sitesi, http://www.akilciilac. gov.tr/, 25 Haziran 2013.
• T.C. Sağlık Bakanlığı, İnşaat ve Onarım Dairesi Başkanlığı, "Mevcut ve Yeni Yapılacak Sağlık Tesislerinde Uyulması Gereken Asgari Teknik Standartlar Hakkında Genelge, 30.10.2012.
• T.C. Sağlık Bakanlığı, Tedavi Hizmetleri Genel Müdürlüğü, "Yataklı Tedavi Kurumları Enfeksiyon Kontrol Yönetmeliği", Resmi Gazete Sayı: 25903, 11 Ağustos 2005.
• T.C.Sağlık Bakanlığı, Yangın Önleme ve Söndürme Yönergesi, Sayı 2652, 20 Ağustos2008
• Tatar, M.(Editör), Sağlık Kurumları Yönetimi-I, Eskişehir Anadolu Üniversitesi, 2012.
• Tehlikeli Atıkların Kontrolü Yönetmeliği, T.C. Resmi Gazete, Sayı 25755, 14/03/2005.
• Tengilimoğlu, D., Sağlık İşletmeleri Yönetimi, Ankara, 2011.• Tıbbi Atıkların Kontrolü Yönetmeliği, T.C. Resmi Gazete, Sayı 25883,
22/07/2005.• Türk Anesteziyoloji ve Reanimasyon Derneği (TARD), Anestezi Uygulama
Kılavuzları; Preoperatif Hazırlık, Kasım 2005.• Türk Dil Kurumu, www.tdk.gov.tr• Ulusoy M, Aydın K. Diş hekimliğinde hareketli bölümlü protezler. 1. Cilt.
Ankara: Ankara Üniversitesi Basımevi; 2003.• Uztuğ, F. (Editör), Kurumsal İletişim, Eskişehir Anadolu Üniversitesi,
Yayın No 1562, 2012.• WHO Draft Guidelines for Adverse Event Reporting and Learning
Systems: From information to action, 2005.• WHO, Core components for infection prevention and control programmes,
Report of the Second Meeting Informal Network on Infection Prevention and Control in Health Care, 2008.
• WHO, Exploring patient participation in reducing health-care-related safety risks, 2013.
• WHO, Guidelines on Hand Hygiene in Health Care, First Global Patient Safety Challenge Clean Care is Safer Care, 2009.
• WHO, Health Promotion Glossary, 1998.

References
222
Department of Quality, Accreditation and Workers' Rights in Health
• WHO, Milestones in Health Promotion-Statements from Global Conferences, 2009.
• WHO, Prevention of hospital-acquired infections: A practical guide 2nd edition, 2002.
• WHO, Safe Surgery Save Lives, safe Surgery Checklist, Patient Safety Checklists, 2009.
• WHO, World Alliance for Patient Safety, 2009.• Williams SJ, Calnan M. "Convergence and Divergence: Assessing
Criteria of Consumer Satisfaction Across General Practice, Dental and Hospital Care Setting, Social Science and Medicine". 33 (6) :707-716, 1991.
• Yataklı Tedavi Kurumları İşletme Yönetmeliği,T.C. Resmi Gazete, Sayı 17927, 13 Ocak 1983
• Zaimoğlu A, Can G. Sabit protezler. Ankara: Ankara Üniversitesi Basımevi; 2004.

Relevant Legislations of
Standards


Relevant Legislations of Standards
225
Standards of Accreditation in Health - ODHS Kit
Legi
slat
ion
Rela
ted
to S
tand
ards
Chap
ter N
ame
Stan
dard
Co
deSt
anda
rdRe
late
d Le
gisl
atio
n
Orga
niza
tiona
l St
ruct
ure
YO.O
Y.01
.00
An o
rgan
isat
iona
l stru
ctur
e to
cov
er a
ll OD
HC a
ctiv
ities
mus
t be
esta
blis
hed.
• T.
C. S
ağlık
Bak
anlığ
ı, İn
şaat
ve
Onar
ım D
aire
si B
aşka
nlığ
ı, “M
evcu
t ve
Yeni
Ya
pıla
cak
Sağl
ık T
esis
lerin
de U
yulm
ası G
erek
en A
sgar
i Tek
nik
Stan
dart
lar H
akkı
nda
Gene
lge,
30.
10.2
012.
•
Sağl
ık H
izmet
leri
Tem
el K
anun
u, R
esm
i Gaz
ete,
Say
ı:335
9, 1
5.05
.198
7 •
663
Sayı
lı Ka
nun
Hükm
ünde
Kar
arna
me,
Res
mi G
azet
e, S
ayı:2
8103
, 02.
11.2
011
•Ağı
z Ve
Diş
Sağ
lığı H
izmet
i Sun
ulan
Öze
l Sağ
lık K
urul
uşla
rı Ha
kkın
da Y
önet
mel
ik,
Resm
î Gaz
ete,
Say
ı: 29
256,
03
.02.
2015
.
YO.O
Y.02
.00
ODHC
mus
t hav
e al
l nec
essa
ry a
utho
risat
ion
and
perm
its fo
r all
its a
ctiv
ities
Core
Pol
icie
s an
d Et
hica
l Val
ues
YO.P
D.01
.00
Core
pol
icie
s an
d et
hica
l val
ues
of O
DHC
mus
t be
defin
ed.
AĞIZ
VE
DİŞ
SAĞL
IĞI H
İZM
ETİ S
UNUL
AN Ö
ZEL
SAĞL
IK K
URUL
UŞLA
RI H
AKKI
NDA
YÖNE
TMEL
İK, R
esm
i Gaz
ete,
Say
ı: 29
256,
03.
02.2
015
Qual
ity M
anag
emen
t St
ruct
ure
YO.K
Y.01
.00
Plan
ning
, im
plem
enta
tion,
coo
rdin
atio
n an
d co
ntin
uity
of q
ualit
y im
prov
emen
t act
iviti
es m
ust b
e en
sure
d.•
Sağl
ıkta
Kal
iteni
n Ge
liştir
ilmes
i Ve
Değe
rlend
irilm
esin
e Da
ir Yö
netm
elik
, Res
mî
Gaze
te, S
ayı:
2939
9,
27.0
6.20
15.
Docu
men
tM
anag
emen
tYO
.DY.
01.0
0M
anag
emen
t of d
ocum
ents
at O
DHC
mus
t be
ensu
red.
YATA
KLI T
EDAV
İ KUR
UMLA
RI T
IBBÎ
KAY
IT V
E AR
ŞİV
HİZM
ETLE
Rİ Y
ÖNER
GESİ
, 06
.11.
2001
tarih
ve
1058
8 sa
yılı
Adve
rse
Even
t YO
.OB.
01.0
0Re
port
ing
of a
dver
se e
vent
s th
at m
ay o
r doe
s af
fect
the
safe
ty
of p
atie
nts
and
staf
f neg
ativ
ely
mus
t be
ensu
red,
and
nec
essa
ry
mea
sure
s m
ust b
e ta
ken.
• 63
31 S
ayılı
İŞ S
AĞLI
ĞI V
E GÜ
VENL
İĞİ K
ANUN
U, R
esm
î Gaz
ete,
Say
ı : 2
8339
, 30
.6.2
012
•
HAST
A VE
ÇAL
IŞAN
GÜV
ENLİ
ĞİNİ
N SA
ĞLAN
MAS
INA
DAİR
YÖN
ETM
ELİK
,Res
mî
Gaze
te, S
ayı :
278
97, 0
6.04
.201
1
Risk
Man
agem
ent
YO.R
Y.01
.00
Risk
s re
late
d to
ODH
C an
d se
rvic
es p
rovi
ded
mus
t be
man
aged
.•
İŞ S
AĞLI
ĞI V
E GÜ
VENL
İĞİ R
İSK
DEĞE
RLEN
DİRM
ESİ Y
ÖNET
MEL
İĞİ,
Resm
i Ga
zete
, Say
ı: 28
512,
29.
12.2
012
Trai
ning
Man
agem
ent
YO.E
Y.01
.00
In a
ccor
danc
e w
ith q
ualit
y im
prov
emen
t act
iviti
es, t
rain
ing
need
s of
pat
ient
s, c
arer
s an
d st
aff m
ust b
e de
term
ined
, and
it m
ust b
e en
sure
d th
at n
eces
sary
trai
ning
is c
ondu
cted
effe
ctiv
ely.
• Sa
ğlık
ta K
alite
nin
Geliş
tirilş
mes
i Ve
Değe
rlend
irilm
esin
e Da
ir Yö
netm
elik
, Res
mî
Gaze
te, S
ayı:
2939
9,
27.0
6.20
15.
Soci
al R
espo
nsib
ility
YO.S
S.01
.00
ODHC
s m
ust o
rgan
ize p
rogr
ams
for p
rom
otin
g an
d im
prov
ing
heal
th b
y ta
king
hea
lth s
truct
ure
and
gene
ral h
ealth
pro
blem
s of
th
e so
ciet
y in
to a
ccou
nt.

Relevant Legislations of Standards
226
Department of Quality, Accreditation and Workers' Rights in Health
Legi
slat
ion
Rela
ted
to S
tand
ards
Chap
ter N
ame
Stan
dard
Co
deSt
anda
rdRe
late
d Le
gisl
atio
n
Inst
itutio
nal
Com
mun
icat
ion
YO.K
İ.01.
00In
stitu
tiona
l com
mun
icat
ion
activ
ities
mus
t be
carr
ied
out
effe
ctiv
ely.
Mon
itorin
g Of
In
dica
tors
PÖ.G
İ.01.
00In
stitu
tiona
l ind
icat
ors
mus
t be
mon
itore
d an
d ev
alua
ted
in o
rder
to
con
tinuo
usly
impr
ove
proc
esse
s re
late
d to
ser
vice
del
iver
y, le
d by
adm
inis
trativ
e, fi
nanc
ial a
nd m
edic
al s
teps
.
• Sa
ğlık
ta K
alite
nin
Geliş
tirilş
mes
i Ve
Değe
rlend
irilm
esin
e Da
ir Yö
netm
elik
, Res
mî
Gaze
te, S
ayı:
2939
9,
27.0
6.20
15.
Hum
an R
esou
rces
M
anag
emen
t
SÇ.İK
.01.
00A
man
agem
ent s
truct
ure
that
will
fulfi
ll th
e re
quire
men
ts c
once
rn-
ing
plan
ning
of h
uman
reso
urce
s, im
prov
emen
t of w
ork
life
and
the
pers
onne
l mus
t be
esta
blis
hed.
• SA
ĞLIK
BAK
ANLI
ĞI A
TAM
A VE
YER
DEĞ
İŞTİ
RME
YÖNE
TMEL
İĞİ,
Resm
i Gaz
ete,
Sa
yı: 2
8599
, 26.
03.2
013
•
KAM
U KU
RUM
VE
KURU
LUŞL
ARIN
A AÇ
IKTA
N KU
RA İL
E AT
ANAC
AK S
AĞLI
K PE
RSON
ELİN
İN A
TAM
A US
ÛL V
E ES
ASLA
RINA
İLİŞ
KİN
YÖNE
TMEL
İK,
Resm
i Gaz
ete,
Say
ı: 29
412,
10.
07.2
015
•
SAĞL
IK B
AKAN
LIĞI
VE
BAĞL
I KUR
ULUŞ
LARI
492
4 SA
YILI
KAN
UNA
TABİ
SÖ
ZLEŞ
MEL
İ SAĞ
LIK
PERS
ONEL
İ ATA
MA
VE Y
ER D
EĞİŞ
TİRM
E YÖ
NETM
ELİĞ
İ, Re
smi G
azet
e, S
ayı:
2926
4, 1
1.02
.201
5
SÇ.İK
.02.
00Th
e re
quire
men
ts n
eces
sary
to c
onst
antly
impr
ove
recr
uitm
ent
and
com
plia
nce
proc
esse
s of
the
pers
onne
l and
thei
r wor
k lif
e m
ust b
e de
term
ined
and
fulfi
lled.
• SA
ĞLIK
BAK
ANLI
ĞI P
ERSO
NELİ
GÖR
EVDE
YÜK
SELM
E VE
UNV
AN D
EĞİŞ
İKLİ
Ğİ
YÖNE
TMEL
İĞİ ,
Res
mi G
azet
e, S
ayı:
2897
5, 1
7.04
.201
4
• AD
AY M
EMUR
LARI
N YE
TİŞT
İRİL
MEL
ERİN
E İL
İŞKİ
N GE
NEL
YÖNE
TMEL
İK,
Res
mi G
azet
e, S
ayı:
1809
0, 2
7.6.
1983
Empl
oyee
Hea
lth a
nd
Safe
tySÇ
.ÇG.
01.0
0Fa
ctor
s th
reat
enin
g th
e he
alth
and
saf
ety
of e
mpl
oyee
s sh
ould
be
iden
tifie
d an
d ne
cess
ary
prec
autio
ns s
houl
d be
take
n to
est
ablis
h a
heal
thy
and
safe
wor
king
env
ironm
ent.
• Ça
lışan
ların
İş S
ağlığ
ı ve
Güve
nliğ
i Eği
timle
rinin
Usu
l ve
Esas
ları
Hakk
ında
Yö
netm
elik
, Res
mî G
azet
e, S
ayı:
2864
8, 1
5.05
.201
3.
• İş
Güv
enliğ
i Uzm
anla
rının
Gör
ev, Y
etki
, Sor
umlu
luk
ve E
ğitim
leri
Hakk
ında
Yö
netm
elik
, Res
mî G
azet
e, S
ayı:2
8512
, 29.
12.2
012.
•
İş S
ağlığ
ı ve
Güve
nliğ
i Hizm
etle
ri Yö
netm
eliğ
i, Re
smî G
azet
e, S
ayı:2
8545
, 29
.12.
2012
. •
İş S
ağlığ
ı ve
Güve
nliğ
i Kan
unu,
Kan
un N
o:63
31, K
abul
Tar
ihi 2
0.06
.201
2.•
İş S
ağlığ
ı ve
Güve
nliğ
i Kur
ulla
rı Ha
kkın
da Y
önet
mel
ik, R
esm
î Gaz
ete,
Say
ı: 28
532,
18
.01.
2013
. •
İş S
ağlığ
ı ve
Güve
nliğ
ine
İlişk
in İş
yeri
Tehl
ike
Sını
fları
Tebl
iğin
de D
eğiş
iklik
Ya
pılm
asın
a Da
ir Te
bliğ
, Res
mî G
azet
e, S
ayı:
2860
2, 2
9.03
.201
3.

Relevant Legislations of Standards
227
Standards of Accreditation in Health - ODHS Kit
Legi
slat
ion
Rela
ted
to S
tand
ards
Chap
ter N
ame
Stan
dard
Co
deSt
anda
rdRe
late
d Le
gisl
atio
n
Basi
c Pa
tient
Rig
hts
HD.H
H.01
.00
The
serv
ices
pro
vide
d in
ODH
C m
ust b
e or
gani
zed
in s
uch
a w
ay
as to
pro
tect
pat
ient
and
car
er ri
ghts
.•
Hast
a Ha
klar
ı Yön
etm
eliğ
i, Re
smi G
azet
e, S
ayı:
2342
0 Ta
rih: 0
1.08
.199
8;
Patie
nt S
afet
yHD
.HG.
01.0
0Th
e se
rvic
es p
rovi
ded
at O
DHC
mus
t be
orga
nize
d in
suc
h a
way
as
to p
rote
ct th
e sa
fety
of p
atie
nts
and
thei
r car
ers.
Patie
nt
Feed
back
HD.G
B.01
.00
A sy
stem
mus
t be
esta
blis
hed
to re
ceiv
e fe
edba
ck (c
omm
ents
, su
gges
tions
an
d co
mpl
aint
s et
c.) f
rom
pat
ient
s an
d th
eir c
arer
s ab
out t
he
serv
ices
that
are
pro
vide
d.
HAST
A HA
KLAR
I YÖN
ETM
ELİĞ
İ, Re
smi G
azet
e, S
ayı:
2342
0, 0
1.08
.199
8
Acce
ss to
Ser
vice
HD.H
E.01
.00
Nece
ssar
y pr
ecau
tions
mus
t be
take
n in
ord
er to
pro
vide
pat
ient
ab
le to
reac
h se
rvic
es in
tim
e.
Prev
entio
n of
In
fect
ions
SH.E
Ö.01
.00
Nece
ssar
y m
easu
res
mus
t be
take
n fo
r the
pre
vent
ion
of
infe
ctio
ns•
T.C.
Sağ
lık B
akan
lığı,
Teda
vi H
izmet
leri
Gene
l Müd
ürlü
ğü, “
Yata
klı T
edav
i Kur
umla
rı En
feks
iyon
Kon
trol Y
önet
mel
iği”,
Res
mi G
azet
e Sa
yı: 2
5903
, 11.
08.2
005.
Ster
ilizat
ion
Man
agem
ent
SH.S
Y.01
.00
Proc
esse
s co
ncer
ning
ste
riliza
tion
serv
ices
mus
t be
iden
tifie
d an
d ta
ken
unde
r con
trol.
• YA
TAKL
I TED
AVİ K
URUM
LARI
İŞLE
TME
YÖNE
TMEL
İĞİ,
Resm
i Gaz
ete
Sayı
:179
27, 1
3.1.
1983
Med
icin
eM
anag
emen
tSH
.İY.0
1.00
Effic
ient
and
saf
e m
edic
ine
man
agem
ent m
ust b
e en
sure
d in
the
inst
itutio
n.
• Ec
zacı
lar v
e Ec
zane
ler H
akkı
nda
Yöne
tmel
ik,R
esm
i Gaz
ete
Say
ısı
2897
0,
12.0
4.20
14
•İla
çlar
ın G
üven
liliği
Hak
kınd
a Yö
netm
elik
, Res
mi G
azet
e Sa
yı 2
8973
, 15.
04.2
014

Relevant Legislations of Standards
228
Department of Quality, Accreditation and Workers' Rights in Health
Legi
slat
ion
Rela
ted
to S
tand
ards
Chap
ter N
ame
Stan
dard
Co
deSt
anda
rdRe
late
d Le
gisl
atio
n
Patie
nt C
are
SH.H
B.01
.00
Patie
nt c
are
proc
esse
s m
ust b
e co
nduc
ted
in li
ne w
ith th
e ne
eds
of th
e pa
tient
and
so
as to
ens
ure
patie
nt s
afet
y.
• He
mşi
relik
Kan
unun
da D
eğiş
iklik
Yap
ılmas
ına
Dair
Kanu
n, T
.C. R
esm
i Gaz
ete
Sayı
26
510,
02.
05.2
007.
•
SAĞL
IK B
AKAN
LIĞI
VE
BAĞL
I KUR
ULUŞ
LARI
TAR
AFIN
DAN
EVDE
SAĞ
LIK
HİZM
ETLE
RİNİ
N SU
NULM
ASIN
A DA
İR Y
ÖNET
MEL
İK, R
esm
î Gaz
ete,
Say
ı : 2
9280
, 27
.02.
2015
SH.H
B.02
.00
In th
e pa
tient
car
e pr
oces
s, p
atie
nt id
entit
y m
ust b
e ve
rifie
d to
m
ake
sure
that
the
med
ical
pro
cedu
re is
con
duct
ed o
n th
e rig
ht
patie
nt.
SH.H
B.03
.00
Mea
sure
s m
ust b
e ta
ken
to p
reve
nt p
atie
nt fa
lls.
SH.H
B.04
.00
Effe
ctiv
e co
mm
unic
atio
n m
ust b
e en
sure
d in
the
flow
of i
nfor
ma-
tion
amon
g th
e he
alth
pro
fess
iona
ls.
SH.H
B.05
.00
Patie
nts
that
car
ry th
e ris
k of
har
min
g th
emse
lves
or o
ther
s m
ust
be ta
ken
unde
r con
trol.
SH.H
B.06
.00
The
stan
dard
izatio
n of
car
e fo
r spe
cific
pat
ient
gro
ups
mus
t be
ensu
red.
• Ya
takl
ı Sağ
lık T
esis
lerin
de Y
anık
Ted
avi B
irim
lerin
in K
urul
mas
ı ve
İşle
yişi
Hak
kınd
a Yö
nerg
e, 2
202
sayı
lı Ba
kan
olur
u, 1
9.01
.201
0.
• Ya
takl
ı Sağ
lık T
esis
lerin
de Y
oğun
Bak
ım H
izmet
lerin
in U
ygul
ama
Usul
ve
Esas
ları
Hakk
ında
Teb
liğ, T
.C.R
esm
i Gaz
ete
Sayı
280
00, 2
0.07
.201
1.
Radi
atio
n Sa
fety
SH.R
G.01
.00
Mea
sure
s m
ust b
e ta
ken
to e
nsur
e ra
diat
ion
safe
ty fo
r pat
ient
/ca
rers
and
the
pers
onne
l.
• Ra
dyas
yon
Güve
nliğ
i Yön
etm
eliğ
i, T.
C. R
esm
i Gaz
ete
Sayı
239
99, 0
5 Te
mm
uz
2000
. •
Sağl
ık H
izmet
lerin
de İy
onla
ştırı
cı R
adya
syon
Kay
nakl
arı i
le Ç
alış
an P
erso
nelin
Ra
dyas
yon
Doz
Lim
itler
i ve
Çalış
ma
Esas
ları
Hakk
ında
Yön
etm
elik
, T.C
. Res
mi
gaze
te, S
ayı 2
8344
, 05
Tem
muz
201
2.

Relevant Legislations of Standards
229
Standards of Accreditation in Health - ODHS Kit
Legi
slat
ion
Rela
ted
to S
tand
ards
Chap
ter N
ame
Stan
dard
Co
deSt
anda
rdRe
late
d Le
gisl
atio
n
Pros
thes
isLa
bora
tory
Ser
vice
s
SH.P
L.01
.00
Phys
ical
env
ironm
ent o
f the
pro
sthe
sis
labo
rato
ry m
ust b
e ar
-ra
nged
so
as to
ens
ure
safe
ty o
f the
pro
sthe
sis
and
the
pers
onne
l.
• Tı
bbi L
abor
atuv
arla
r Yön
etm
eliğ
i, T.
C. R
esm
i Gaz
ete
Sayı
287
90, T
arih
09
.10.
2013
. •
DİŞ
PROT
EZ L
ABOR
ATUV
ARLA
RI Y
ÖNET
MEL
İĞİ,
Resm
i Gaz
ete,
Say
ı: 26
016,
07
.12.
2005
•
Diş
Prot
ez L
abor
atuv
arla
rı Yö
netm
eliğ
inde
Değ
işik
lik
Yapı
lmas
ı Hak
kınd
a Yö
netm
elik
, Res
mî G
azet
e, S
ayı :
281
59, 3
1.12
.201
1
SH.P
L.02
.00
The
proc
esse
s th
at p
rece
de th
e fa
bric
atio
n of
pro
sthe
sis
mus
t be
che
cked
SH.P
L.03
.00
The
proc
esse
s re
gard
ing
the
fabr
icat
ion
of p
rost
hesi
s m
ust b
e ch
ecke
d.
SH.P
L.04
.00
The
proc
esse
s th
at fo
llow
the
fabr
icat
ion
of p
rost
hesi
s m
ust b
e ch
ecke
d.
SH.P
L.05
.00
Trac
eabi
lity
of th
e pr
oces
ses
rega
rdin
g pr
osth
esis
labo
rato
ry
mus
t be
ensu
red.
Surg
ical
Saf
ety
SH.G
C.01
.00
Patie
nt s
afet
y m
ust b
e en
sure
d in
sur
gica
l pro
cedu
res.
• YA
TAKL
I TED
AVİ K
URUM
LARI
İŞLE
TME
YÖNE
TMEL
İĞİ,
Resm
i Gaz
ete
Sayı
:179
27, 1
3.1.
1983
SH.G
C.02
.00
Cond
ition
s of
the
oper
atin
g ro
om m
ust b
e ap
prop
riate
to e
nsur
e sa
fe s
urge
ry.
Acco
mm
odat
ion
Serv
ices
DH.O
H.01
.00
AYAl
l the
are
as a
t ODH
C m
ust b
e cl
ean
for t
he s
afet
y an
d sa
tis-
fact
ion
of p
atie
nt, c
arer
and
per
sonn
el.
• Gı
da H
ijyen
i Yön
etm
eliğ
i, T.
C. R
esm
i Gaz
ete,
Say
ı 281
457,
17
Aral
ık 2
011.
• T.
C. S
ağlık
Bak
anlığ
ı, Te
davi
Hizm
etle
ri Ge
nel M
üdür
lüğü
, “Ya
takl
ı Ted
avi K
urum
ları
Enfe
ksiy
on K
ontro
l Yön
etm
eliğ
i”, R
esm
i Gaz
ete
Sayı
: 259
03, 1
1.08
.200
5.DH
.OH.
02.0
0Pr
oces
ses
rega
rdin
g ca
terin
g fo
r inp
atie
nt/ c
arer
and
the
pers
on-
nel m
ust b
e id
entif
ied.
DH.O
H.03
.00
Laun
dry
serv
ices
mus
t be
prov
ided
in a
saf
e an
d ef
ficie
nt m
anne
r to
ens
ure
patie
nt a
nd p
erso
nnel
hea
lth a
t ODH
C.•
T.C.
Sağ
lık B
akan
lığı,
Teda
vi H
izmet
leri
Gene
l Müd
ürlü
ğü, “
Yata
klı T
edav
i Kur
umla
rı En
feks
iyon
Kon
trol Y
önet
mel
iği”,
Res
mi G
azet
e Sa
yı: 2
5903
, 11.
08.2
005.
DH.O
H.04
.00
Patie
nt/e
xam
inat
ion
room
s an
d th
e ar
eas
used
by
patie
nts/
care
rs
mus
t be
safe
and
erg
onom
ic.
DH.O
H.05
.00
Safe
ty/s
ecur
ity s
ervi
ces
mus
t be
prov
ided
in O
DHC
to e
nsur
e sa
fety
of l
ife a
nd p
rope
rty
of p
atie
nt/c
arer
and
the
pers
onne
l.•
Özel
Güv
enlik
Hizm
etle
rine
Dair
Kanu
nun
Uygu
lanm
asın
a İli
şkin
Yön
etm
elik
, R
esm
i Gaz
ete
Sayı
: 256
06,
07.1
0.20
04

Relevant Legislations of Standards
230
Department of Quality, Accreditation and Workers' Rights in Health
Legi
slat
ion
Rela
ted
to S
tand
ards
Chap
ter N
ame
Stan
dard
Co
deSt
anda
rdRe
late
d Le
gisl
atio
n
Faci
lity
Man
agem
ent
DH.T
Y.01
.00
A qu
ality
faci
lity
man
agem
ent s
truct
ure
and
proc
ess
mus
t be
es-
tabl
ishe
d to
ens
ure
the
qual
ity a
nd s
afet
y of
hea
lthca
re s
ervi
ces.
İşye
ri Bi
na v
e Ek
lent
ilerin
de A
lınac
ak S
ağlık
ve
Güve
nlik
Önl
emle
rine
İlişk
in Y
önet
me-
lik,T
.C. R
esm
i Gaz
ete,
Say
ı 287
10, 1
7.07
.201
3
Was
te M
anag
emen
tDH
.AY.
01.0
0Sa
fe a
nd e
ffect
ive
man
agem
ent o
f was
te p
rodu
ced
at O
DHC
mus
t be
ens
ured
to p
rote
ct h
uman
and
env
ironm
enta
l hea
lth.
• Tı
bbi A
tıkla
rın K
ontro
lü Y
önet
mel
iği,
T.C.
Res
mi G
azet
e, S
ayı 2
5883
, 22/
07/2
005.
•
Tehl
ikel
i Atık
ların
Kon
trolü
Yön
etm
eliğ
i, T.
C. R
esm
i Gaz
ete,
Say
ı 257
55,
14/0
3/20
05.
• At
ık Y
önet
imi G
enel
Esa
slar
ına
İlişk
in Y
önet
mel
ik, T
.C. R
esm
i Gaz
ete,
Sa
yı 2
6927
, 05/
07/2
008
• At
ıkla
rın D
üzen
li De
pola
nmas
ına
Dair
Yöne
tmel
ik, T
.C. R
esm
i Gaz
ete,
Sayı
275
33, 2
6/03
/201
0
Info
rmat
ion
Man
agem
ent
DH.B
Y.01
.00
A sa
fe a
nd e
ffect
ive
info
rmat
ion
man
agem
ent s
yste
m m
ust b
e pr
esen
t at O
DHC.
• Ki
şise
l Ver
ilerin
Kor
unm
ası K
anun
u, T
.C. R
esm
i Gaz
ete,
Say
ı 296
77, 0
7.04
.201
6
Mat
eria
l and
Dev
ice
Man
agem
ent
DH.M
C.01
.00
Effic
ient
, effe
ctiv
e an
d sa
fe u
se o
f mat
eria
ls a
nd d
evic
es m
ust b
e en
sure
d.•
Tıbb
i Cih
az Y
önet
mel
iği,
T.C.
Res
mi G
azet
e, S
ayı 2
7957
, 07/
06/2
011
Outs
ourc
ing
DH.D
K.01
.00
The
serv
ices
pro
vide
d th
roug
h ou
tsou
rcin
g m
ust b
e in
line
with
th
e co
re p
olic
ies
and
valu
es o
f ODH
C an
d St
anda
rds
of
Accr
edita
tion
in H
ealth
.
•Hizm
et A
lımı İ
hale
leri
Uygu
lam
a Yö
netm
eliğ
inde
Değ
işik
lik Y
apılm
asın
a Da
ir Yö
net-
mel
ik, T
.C. R
esm
i Gaz
ete,
Say
ı 294
28, 2
8/07
/201
5
Emer
genc
yM
anag
emen
t
AD.A
D.01
.00
Mea
sure
s m
ust b
e ta
ken
for t
he n
atur
al
disa
ster
s or
eve
nts
whi
ch re
quire
em
erge
ncy
resp
onse
, stri
ving
, firs
t aid
or
evac
uatio
n.
• Af
et v
e Ac
il Du
rum
Müd
ahal
e Hi
zmet
leri
Yöne
tmel
iği,T
.C. R
esm
i Gaz
ete,
Say
ı 28
855,
18/
12/2
013
• Bi
nala
rın Y
angı
ndan
Kor
unm
ası H
akkı
nda
Yöne
tmel
ik,
T.C.
Res
mi G
azet
e, S
ayı
2673
5, 1
9/12
/200
7
AD.A
D.02
.00
Tim
ely
inte
rven
tions
mus
t be
perf
orm
ed in
the
case
of r
espi
rato
ry
or c
ardi
ac a
rres
t.
AD.A
D.03
.00
Tim
ely
inte
rven
tion
mus
t be
ensu
red
in c
ases
whe
re th
e he
alth
pr
ofes
sion
al is
exp
osed
to a
risk
of v
iole
nce,
or a
n ac
t of v
iole
nce
is d
irect
ed to
war
ds h
im/h
er.
•SA
ĞLIK
BAK
ANLI
ĞI P
ERSO
NELİ
NE K
ARŞI
İŞLE
NEN
SUÇL
AR N
EDEN
İYLE
YA
PILA
CAK
HUKU
Kİ Y
ARDI
MIN
USU
L VE
ESA
SLAR
I HAK
KIND
A YÖ
NETM
ELİK
, Re
smî G
azet
e Sa
yı :
2827
7, 2
8.04
.201
2 •
Çalış
an G
üven
liği G
enel
gesi
, Say
ı: 20
12/2
3, 1
4.05
.201
2
AD.A
D.04
.00
Ther
e m
ust b
e an
arr
ange
men
t in
plac
e to
ens
ure
timel
y re
spon
se
to fi
re.
• Af
et v
e Ac
il Du
rum
Müd
ahal
e Hi
zmet
leri
Yöne
tmel
iği,
T.C.
Res
mi G
azet
e, S
ayı
2885
5, 1
8/12
/201
3 •B
inal
arın
Yan
gınd
an K
orun
mas
ı Hak
kınd
a Yö
netm
elik
, T.
C. R
esm
i Gaz
ete,
Say
ı 26
735,
19/
12/2
007

Annex
Legi
slat
ion
Rela
ted
to S
tand
ards
Chap
ter N
ame
Stan
dard
Co
deSt
anda
rdRe
late
d Le
gisl
atio
n
Faci
lity
Man
agem
ent
DH.T
Y.01
.00
A qu
ality
faci
lity
man
agem
ent s
truct
ure
and
proc
ess
mus
t be
es-
tabl
ishe
d to
ens
ure
the
qual
ity a
nd s
afet
y of
hea
lthca
re s
ervi
ces.
İşye
ri Bi
na v
e Ek
lent
ilerin
de A
lınac
ak S
ağlık
ve
Güve
nlik
Önl
emle
rine
İlişk
in Y
önet
me-
lik,T
.C. R
esm
i Gaz
ete,
Say
ı 287
10, 1
7.07
.201
3
Was
te M
anag
emen
tDH
.AY.
01.0
0Sa
fe a
nd e
ffect
ive
man
agem
ent o
f was
te p
rodu
ced
at O
DHC
mus
t be
ens
ured
to p
rote
ct h
uman
and
env
ironm
enta
l hea
lth.
• Tı
bbi A
tıkla
rın K
ontro
lü Y
önet
mel
iği,
T.C.
Res
mi G
azet
e, S
ayı 2
5883
, 22/
07/2
005.
• Te
hlik
eli A
tıkla
rın K
ontro
lü Y
önet
mel
iği,
T.C.
Res
mi G
azet
e, S
ayı 2
5755
,14
/03/
2005
.•
Atık
Yön
etim
i Gen
el E
sasl
arın
a İli
şkin
Yön
etm
elik
, T.C
. Res
mi G
azet
e,Sa
yı 2
6927
, 05/
07/2
008
• At
ıkla
rın D
üzen
li De
pola
nmas
ına
Dair
Yöne
tmel
ik, T
.C. R
esm
i Gaz
ete,
Sayı
275
33, 2
6/03
/201
0
Info
rmat
ion
Man
agem
ent
DH.B
Y.01
.00
A sa
fe a
nd e
ffect
ive
info
rmat
ion
man
agem
ent s
yste
m m
ust b
e pr
esen
t at O
DHC.
• Ki
şise
l Ver
ilerin
Kor
unm
ası K
anun
u, T
.C. R
esm
i Gaz
ete,
Say
ı 296
77, 0
7.04
.201
6
Mat
eria
l and
Dev
ice
Man
agem
ent
DH.M
C.01
.00
Effic
ient
, effe
ctiv
e an
d sa
fe u
se o
f mat
eria
ls a
nd d
evic
es m
ust b
e en
sure
d.•
Tıbb
i Cih
az Y
önet
mel
iği,
T.C.
Res
mi G
azet
e, S
ayı 2
7957
, 07/
06/2
011
Outs
ourc
ing
DH.D
K.01
.00
The
serv
ices
pro
vide
d th
roug
h ou
tsou
rcin
g m
ust b
e in
line
with
th
e co
re p
olic
ies
and
valu
es o
f ODH
C an
d St
anda
rds
ofAc
cred
itatio
n in
Hea
lth.
•Hizm
et A
lımı İ
hale
leri
Uygu
lam
a Yö
netm
eliğ
inde
Değ
işik
lik Y
apılm
asın
a Da
ir Yö
net-
mel
ik, T
.C. R
esm
i Gaz
ete,
Say
ı 294
28, 2
8/07
/201
5
Emer
genc
yM
anag
emen
t
AD.A
D.01
.00
Mea
sure
s m
ust b
e ta
ken
for t
he n
atur
aldi
sast
ers
or e
vent
s w
hich
requ
ireem
erge
ncy
resp
onse
, stri
ving
, firs
t aid
or
evac
uatio
n.
• Af
et v
e Ac
il Du
rum
Müd
ahal
e Hi
zmet
leri
Yöne
tmel
iği,T
.C. R
esm
i Gaz
ete,
Say
ı 28
855,
18/
12/2
013
• Bi
nala
rın Y
angı
ndan
Kor
unm
ası H
akkı
nda
Yöne
tmel
ik,
T.C.
Res
mi G
azet
e, S
ayı
2673
5, 1
9/12
/200
7
AD.A
D.02
.00
Tim
ely
inte
rven
tions
mus
t be
perf
orm
ed in
the
case
of r
espi
rato
ry
or c
ardi
ac a
rres
t.
AD.A
D.03
.00
Tim
ely
inte
rven
tion
mus
t be
ensu
red
in c
ases
whe
re th
e he
alth
pr
ofes
sion
al is
exp
osed
to a
risk
of v
iole
nce,
or a
n ac
t of v
iole
nce
is d
irect
ed to
war
ds h
im/h
er.
• S
AĞLI
K BA
KANL
IĞI P
ERSO
NELİ
NE K
ARŞI
İŞLE
NEN
SUÇL
AR N
EDEN
İYLE
YAPI
LACA
K HU
KUKİ
YAR
DIM
IN U
SUL
VE E
SASL
ARI H
AKKI
NDA
YÖNE
TMEL
İK,
Resm
î Gaz
ete
Sayı
: 28
277,
28.
04.2
012
• Ça
lışan
Güv
enliğ
i Gen
elge
si, S
ayı:
2012
/23,
14.
05.2
012
AD.A
D.04
.00
Ther
e m
ust b
e an
arr
ange
men
t in
plac
e to
ens
ure
timel
y re
spon
se
to fi
re.
• Af
et v
e Ac
il Du
rum
Müd
ahal
e Hi
zmet
leri
Yöne
tmel
iği,
T.C.
Res
mi G
azet
e, S
ayı
2885
5, 1
8/12
/201
3•B
inal
arın
Yan
gınd
an K
orun
mas
ı Hak
kınd
a Yö
netm
elik
, T.
C. R
esm
i Gaz
ete,
Say
ı 26
735,
19/
12/2
007

232
SAS Indicators
ANNEX – SAS Indicators List SAS Indicators Table 1 – Management and Organisation Aspect
Management and Organisation
Indicator Code
Indicator Obligatory(Z) /Optional (O)
Y.1.Z Target Achievement Rate ZY.2.Z Corrective Preventive Action Completion Rate ZY.3.Z Document Revision Numbers ZY.4.Z Incorrect Use of Adverse Event Reporting System Z
Y.5.Z Monitoring the Realisation Rate of Risks Identified (comparison among periods) Z
Y.6.Z Training Participation Rate of Staff ZY.7.Z Realisation Rate of Trainings Planned Z
Y.8.OLength of Command Line (Number of managers in an hierarchal order, including the top manager, to whom the staff at the bottom unit is accountable)
O
Y.9.O Control Area (Number of people directly accountable to a manager)
O
SAS Indicators Table-2 Healthy Working Life Aspect
Healthy Working LifeIndicator
CodeIndicator
Obligatory(Z) /Optional (O)
Ç.1.Z Staff Satisfaction Rate ZÇ.2.Z Staff Turnover Rate Z
Ç.3.Z Rate of Staff Working in a Department not Compatible with Their Vocational Training Z
Ç.4.Z Exposure Rate of Staff to Sharp Objects ZÇ.5.Z Exposure Rate of Staff to Blood and Body Fluid ZÇ.6.Z Number of Violence Event Against Staff ZÇ.7.Z Completion of Health Scanning towards Staff Z

Performance M
easurement and Quality Im
provement
233
Standards of Accreditation in Health - ODHS Kit
SAS Indicators Table -3 Patient Experience
Patient ExperienceIndicator
CodeIndicator
Obligatory(Z) /Optional (O)
H.1.Z Patient Satisfaction Rate Z
SAS Indicators Table -4 Healthcare Services Aspect
Healthcare ServicesIndicator
CodeIndicator
Obligatory(Z) /Optional (O)
Hasta BakımıS.1.Z Rate of Patient Falls ZS.2.O Timely Transfer of Discharge Summary OS.3.Z Rate of Patient Care Plan Development Z
S.4.ZRate of Not Recording of Verbal Request within the first 24 Hours
Z
S.5.Z
Rate of Completion of First Evaluation by Physicians According to all Components Specified in Patient Evaluation Procedures (For physicians, patient story, physical examination, background, family history, preliminary diagnosis and treatment plan that shall be followed.)
Z
S.6.Z Fissur Sealant implementation rate Z
S.7.Z
Rate of Reapplication with the Same Reason (length should be determined by institution)• Rate of Reapplication due to Prosthesis• Rate of Reapplication due to Filling• Rate of Reapplication due to Root Canal Operation• Rate of Reapplication due to Failure of Antibiotic
Therapy
Z
S.8.Z Rate of Incorrect Impression Taking ZS.9.Z Rate of Retaking Impression Z
Prevention of Infections
S.10.ZRate of Using Appropriate Antibiotics in Surgical Prophylaxis
Z
S.11.Z Hand Hygiene Compliance ZMedication Management
S.12.Z Number of Medication Errors ZS.13.Z Rate of Adverse Effects ZS.14.O Rate of Drug Interaction OS.15.O Amount of Medicines Disposed of O

Performance M
easurement and Quality Im
provement
234
Department of Quality, Accreditation and Workers' Rights in Health
Healthcare ServicesIndicator
CodeIndicator
Obligatory(Z) /Optional (O)
Radiation
S.16.Z Number of Repeated Imaging Z
S.17.Z Duration of Waiting in Radiation Areas Z
S.18.ZNumber of imaging for Pregnant and/or Suspected Pregnant Women
Z
Prosthesis Laboratories
S.19.Z Rate of Refused Impression which has been taken Z
S.20.Z Rate of Incorrect Models Z
S.21.Z
Rate of Impression Taking Matched with Wrong Patient • Rate of Impression Taking Matched with Wrong
Patient which has been realised before working onit
• Rate of Impression Taking Matched with WrongPatient which has been realised after working on it
Z
S.22.Z Rate of Missing Impression Taking/Prosthesis Z
S.23.Z
Rate of Prosthesis Not Delivered on Time • Total Length of Time used for making prosthesis
(Average length of time on the basis of prosthesisis taken) Average length of time passing fromimpression taking to making of prosthesis
• Average length of time passing from takingimpression to modelling
• Average length of time passing from admission tolaboratory to delivery
Z
Surgical Operation
S.24.Z ODHC Rate of Safe Surgery Checklist Use Z
S.25.ZRate of Patients Developing Postoperative Respiratory Failure
Z
S.26.Z Rate of Unplanned Return to Operating Room Z
S.27.OAnaesthesia Complications Rate in Surgical Operations
O

Performance M
easurement and Quality Im
provement
235
Standards of Accreditation in Health - ODHS Kit
SAS Indicators Table -5 Support Services Aspect
Support Services
Indicator Code
Indicator Obligatory(Z) /Optional (O)
D.1.ZNumber of Breakdown Days in Basic Facility Resources Z
D.2.ZTime Past Until Responding to Facility-based Problem Response Z
D.3.ZWaste turnover rate (Determining how frequently the waste is collected from the temporary storing areas by relevant agency /agency in charge) Z
D.4.Z Waste-related Hazardous Accident Rate Z
D.5.ZAverage Response Time for Technical Unit to ODHC Information Management System (HIMS) failures Z
D.6.Z Duration of HIMS down-time ZD.7.Z Time Past Until Responding to Device Breakdown ZD.8.Z Frequency of Device Breakdown ZD.9.Z Number of Days on which Devices were Broken Z
D.10.ZInformation Management System Revision Requests • Rate of response to request• Length of time for responding to requests
Z
SAS Indicators Table -6 Support Services Aspect
Emergency Case Management
Indicator Code
Indicator Obligatory(Z) /Optional (O)
A.1.Z Rate of Completely Filled in Code Blue Event Form Z
A.2.Z Rate of Completely Filled Code White Event Form Z
A.3.ZAverage time of Arrival at the Scene of Event in Code Blue
Z